20180923 prevention is the best medicine - ce.mayo.edu prevention is... · vdt-pace codox-m/ivac...
TRANSCRIPT

©2018 MFMER | slide-1
Prevention is the Best Medicine: Antimicrobial Prophylaxis in the Hematology & Oncology Population
Hilary Teaford, Pharm.D.Pharmacy Grand Rounds 9/25/2018

©2018 MFMER | slide-2
Objectives• Describe considerations for the appropriate
selection of antimicrobial prophylaxis in cancer patients
• Review appropriate dosing, side effects, and duration of antimicrobial agents for antifungal, antibacterial, and antiviral prophylaxis
• Identify some select agents in hematology which require unique antimicrobial prophylaxis considerations

Infection Risk in Cancer Patients
Chemotherapy INFECTION
Impaired Immunity
©2018 MFMER | slide-4
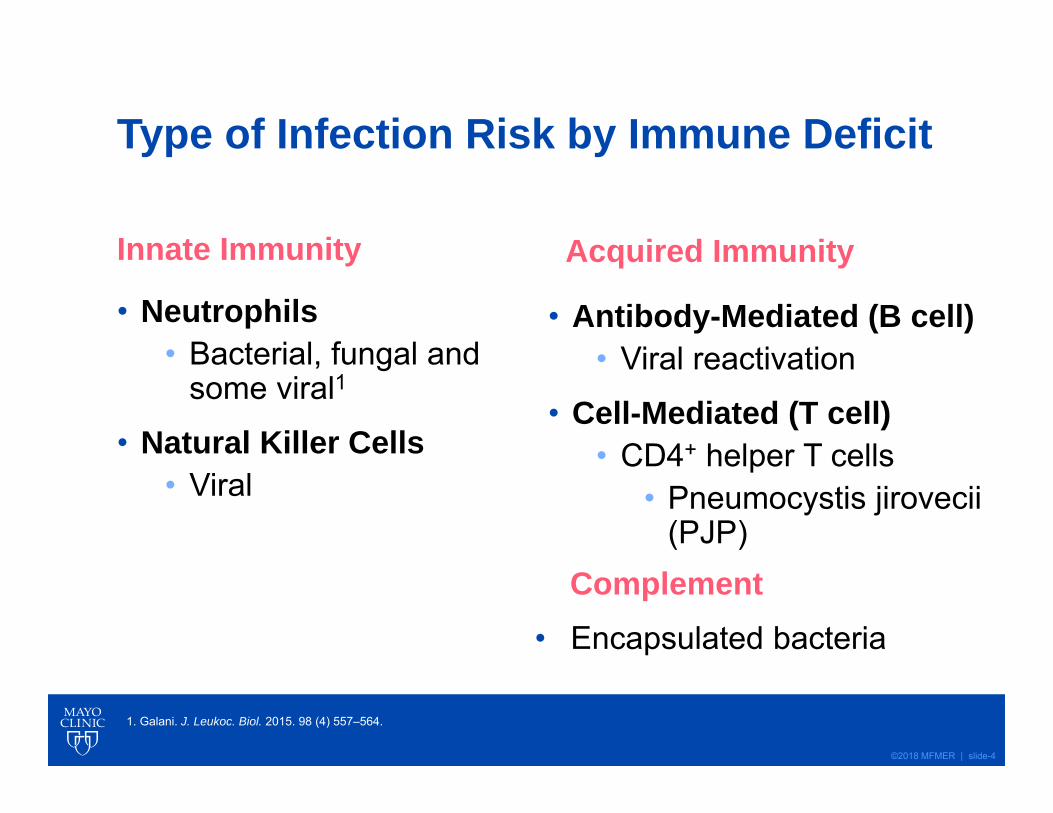
Type of Infection Risk by Immune Deficit
Innate Immunity
• Neutrophils• Bacterial, fungal and
some viral1
• Natural Killer Cells• Viral
Acquired Immunity
• Antibody-Mediated (B cell)• Viral reactivation
• Cell-Mediated (T cell)• CD4+ helper T cells
• Pneumocystis jirovecii (PJP)
1. Galani. J. Leukoc. Biol. 2015. 98 (4) 557–564.
Complement• Encapsulated bacteria

Hematopoiesis
Stem cell
Lymphoma
B
T
CLL
Naive
Myeloid Progenitor
Neutrophils
Eosinophils, Basophils, Monocytes
AML
Lymphoid Progenitor
T
B
ALL
ALL= Acute Lymphocytic Leukemia AML=Acute Myeloid Leukemia CLL= Chronic Lymphocytic Leukemia MM= Multiple Myeloma MDS=myelodysplastic syndrome AA: Aplastic Anemia
Plasma Cells
Myeloid Line = INNATE IMMUNITY
Lymphoid Line = ACQURIED IMMUNITYMM
,MDS, AA

©2018 MFMER | slide-6
Bacterial
Fungal Viral
PJP

©2018 MFMER | slide-7
Bacterial
Fungal Viral
PJP

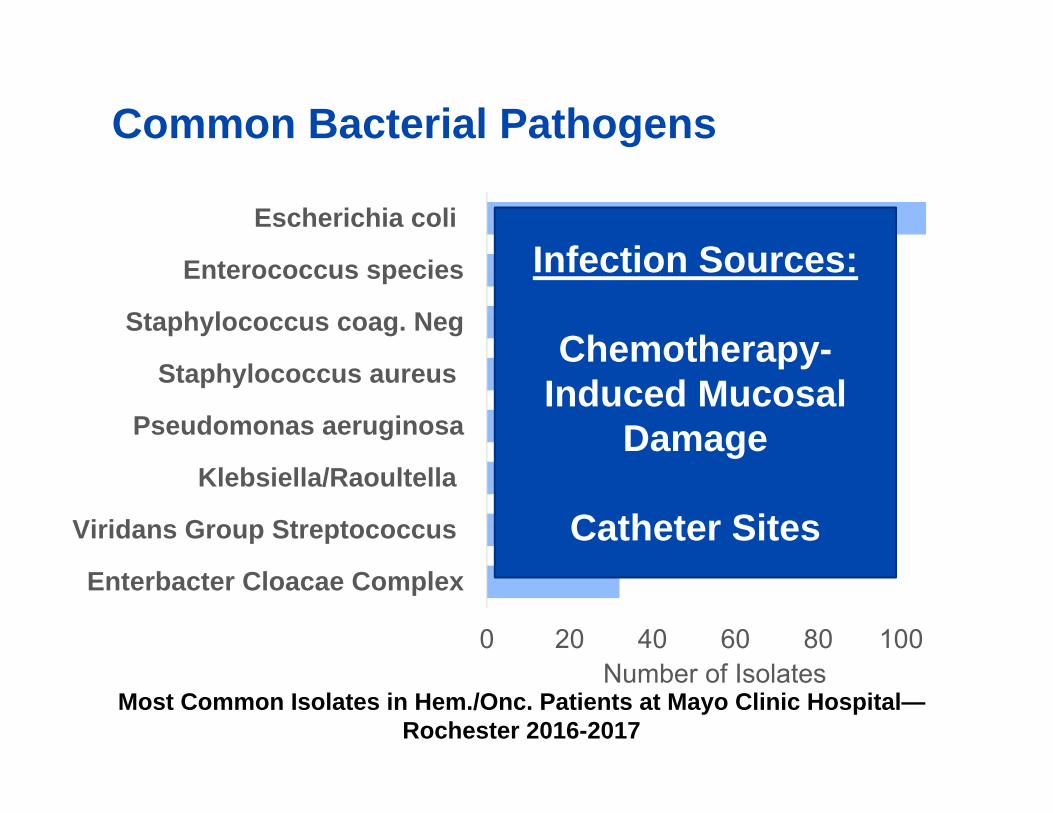
0 20 40 60 80 100
Enterbacter Cloacae Complex
Viridans Group Streptococcus
Klebsiella/Raoultella
Pseudomonas aeruginosa
Staphylococcus aureus
Staphylococcus coag. Neg
Enterococcus species
Escherichia coli
Number of Isolates
Common Bacterial Pathogens
Most Common Isolates in Hem./Onc. Patients at Mayo Clinic Hospital—Rochester 2016-2017
0 20 40 60 80 100
Enterbacter Cloacae Complex
Viridans Group Streptococcus
Klebsiella/Raoultella
Pseudomonas aeruginosa
Staphylococcus aureus
Staphylococcus coag. Neg
Enterococcus species
Escherichia coli
Number of Isolates
Common Bacterial Pathogens
Most Common Isolates in Hem./Onc. Patients at Mayo Clinic Hospital—Rochester 2016-2017
Infection Sources:
Chemotherapy-Induced Mucosal
Damage
Catheter Sites

Optimal Antimicrobial Prophylaxis: Meta-Analysis
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Any Quinolone SMZ-TMP Other Systemic
Rel
ativ
e R
isk
of D
eath
Com
pare
d to
Pla
cebo
Relative All-Cause Mortality Reduction vs. Placebo in Afebrile Neutropenic Patients
SMZ-TMP 800-160 mg PO BID
Gafter-gvili. Cochrane Database Syst Rev. 2014.SMZ-TMP= sulfamethoxazole-trimethoprim
Bacterial Fungal Viral Pneumocystis Unique Agents
SMZ-TMP: sulfamethoxazole-trimethoprim

Bacterial Fungal Viral Pneumocystis Unique Agents
Agents Used in Antibacterial Prophylaxis Line Drug Considerations in Hem./Onc. Patients
Preferred Levofloxacin1 • Reported QTc prolongation (possibly less with Ciprofloxacin2)
• Levofloxacin= more strep. viridans coverageNext preferred
Ciprofloxacin
Alternate
3rd generation cephalosporin3:CefdinirCefpodoxime
• Lacks pseudomonal coverage
Sulfamethoxazole-trimethoprim (SMZ-TMP)
• Lacks pseudomonal coverage• Drug interaction: methotrexate• Myelosuppression• Caution in renal dysfunction
1. Prevention and Treatment of Cancer-Related Infections. NCCN. Version 1.2018 2. Briasoulis. Cardiology. 2011. 120 (2) 103–1103. Yemm. J. Antimicrob. Chemother. 2018. 73 (1) 204–211.

©2018 MFMER | slide-12
Defining Neutropenia• Neutropenia Defined by NCCN:
• Absolute Neutrophil Count (ANC) less then 500 neutrophils/mcL
OR• ANC less than 1000 neutrophils/mcL with expected drop to
<500 neutrophils/mcL within 48 hours
• Profound Neutropenia: <100 neutrophils/mcL
• Prolonged Neutropenia: >7 days
NCCN= National Comprehensive Cancer NetworkPrevention and Treatment of Cancer-Related Infections. NCCN. Version 1.2018
Bacterial Fungal Viral Pneumocystis Unique Agents

Bacterial Fungal Viral Pneumocystis Unique Agents
Risk of Bacterial Infections in Cancer Patients
Solid Tumors Low: less myelosuppressive chemotherapy
Multiple MyelomaCLLLymphoma
Intermediate: regimen specificVDT-PACECODOX-M/IVACR-CHOP14
Acute Leukemia• AML• ALL
High: myelosuppression needed for treatment efficacy
NCCN Guidelines: Consider fluoroquinolone prophylaxis throughout course of neutropenia if expected ANC <1000 for >7 days
Prevention and Treatment of Cancer-Related Infections. NCCN. Version 1.2018
©2018 MFMER | slide-14
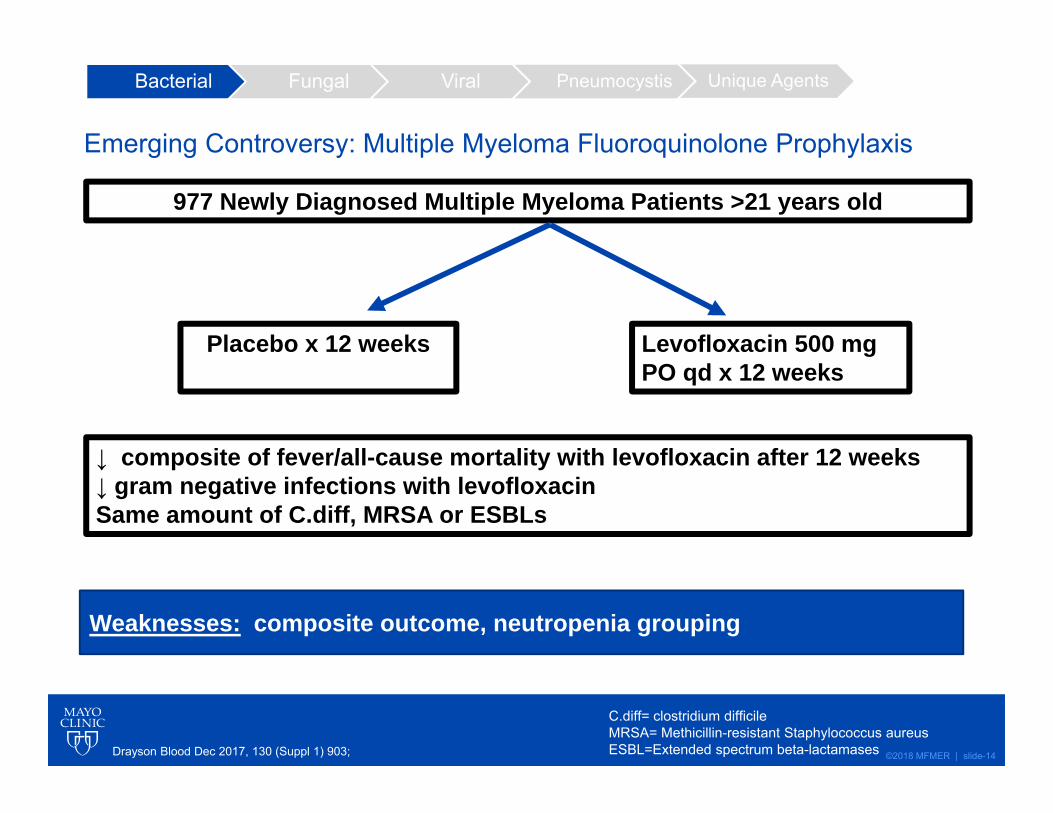
Emerging Controversy: Multiple Myeloma Fluoroquinolone Prophylaxis
Drayson Blood Dec 2017, 130 (Suppl 1) 903;
977 Newly Diagnosed Multiple Myeloma Patients >21 years old
Placebo x 12 weeks Levofloxacin 500 mg PO qd x 12 weeks
↓ composite of fever/all-cause mortality with levofloxacin after 12 weeks ↓ gram negative infections with levofloxacinSame amount of C.diff, MRSA or ESBLs
Weaknesses: composite outcome, neutropenia grouping
C.diff= clostridium difficileMRSA= Methicillin-resistant Staphylococcus aureusESBL=Extended spectrum beta-lactamases
Bacterial Fungal Viral Pneumocystis Unique Agents

©2018 MFMER | slide-15
Fungal
Bacterial Viral
PJP

©2018 MFMER | slide-16
Primary Fungal Organisms of Concern
Organism Mortality in Invasive Infection
Candida (most common) 30%1
Aspergillus 40-90%2
Mucor 54%3
Bacterial Fungal Viral Pneumocystis Unique Agents
1.Cleveland. 2012. 55 (10) 1352–1361.2.Dagenais. Clin. Microbiol. Rev. 2009. 22 (3) 447–465.3.Roden. Clin. Infect. Dis. 2005. 41 (5) 634–653.

Drug Safety and Convenience ConsiderationsSpectrum: most candidaFluconazole Among azoles less potent CYP 3A4 inhibition
Spectrum: candida, aspergillusVoriconazole Hallucinations, vision changes
Itraconzole Inconsistent bioavailability, heart failure exacerbations
Echinocandins Anidulafungin not hepatically or renally cleared
Spectrum: candida, aspergillus, mucor Isavuconazonium/Isavuconazole
Shortens QT interval Seemingly fewer drug interactions
Posaconazole Suspension requires high fat meal, strong CYP3A4 inhibitionTablet has significantly improved bioavailability
Amphotericin B Infusion reactions, electrolyte abnormalities, nephrotoxicity
Agents Used in Fungal Prophylaxis Bacterial Fungal Viral Pneumocystis Unique Agents
Prevention and Treatment of Cancer-Related Infections. NCCN. Version 1.2018
Azole class effects: LFT elevations, most prolong QTc, CYP inhibition

©2018 MFMER | slide-18
Bacterial Fungal Viral Pneumocystis Unique Agents
Recommendations for Select Patient GroupsPopulation Antifungal Prophylaxis Low RiskSolid Tumors
None in most cases
Medium RiskLymphoma Multiple MyelomaCLL
Preferred: fluconazole or an echinocandin during prolonged neutropenia
High-RiskAML
Preferred: posacaonzole during prolonged neutropeniaAlternate: voriconazole, an echinocandin, or amphotericin B during prolonged neutropenia
ALL Preferred: fluconazole or an echinocandin during prolonged neutropeniaAlternate: amphotericin B during prolonged neutropenia
Prevention and Treatment of Cancer-Related Infections. NCCN. Version 1.2018

©2018 MFMER | slide-19
Isavuconazole as Prophylaxis for Invasive Fungal Infections (IFI)
Author Number of Patients
Design and Population Results
Cornely 2015 20 Phase 2 Dose Escalation study in AML primary ppx
No major ADEs, 10% patients had breakthrough IFI
Rausch 2018 100 Retrospective study in primary ppx leukemia patients
18% of primary ppx pts had breakthrough IFI
Fung 2018 5 Case Series 5 cases of breakthrough IFI,3/5 primary ppx
Ppx: Prophylaxis ISA= Isavuconazole ADE= Adverse Drug Event
Cornely et. al. Antimicrob Agents Chemother. 2015;59(4).Rausch. Clin. Infect. Dis. 2018. 11–14.Fung et al. Clin Infect Dis. 2018
Bacterial Fungal Viral Pneumocystis Unique Agents

©2018 MFMER | slide-20
Viral
PJPFungal
Bacterial

©2018 MFMER | slide-21
Bacterial Fungal Viral Pneumocystis Unique Agents
Viral Pathogens of ConcernVirus Pathology
HSV- Herpes Simplex Virus
Skin lesions, meningitis, blindness, encephalitis
VZV- Varicella Zoster Virus
Rash, neuritis, aseptic meningitis, neuropathy, encephalitis, pneumonitis, hepatitis, pancreatitis
HBV- Hepatitis B Virus Acute hepatitis, chronic liver disease, cirrhosis, and hepatocellular carcinoma
CMV-Cytomegalovirus
Colitis, hepatitis, encephalitis, myocarditis, retinitis, Guillen-Barre syndrome
Prevention and Treatment of Cancer-Related Infections. NCCN. Version 1.2018

©2018 MFMER | slide-22
Antiviral AgentsAgent Prophylactic Dosing CommentsHSV/VZVAcyclovir 400-800 mg PO BID OR 5
mg/kg IV qd Need hydration to avoid crystal nephropathy, renally dosed
Valacyclovir 500 mg PO BID or TID Renally dosed
CMV (also covers HSV/VZV)Ganciclovir 5 mg/kg IV q12h x 7-14 days Marrow suppression, renally dosed
Valganciclovir 900 mg PO qdHBVEntecavir: *Preferred*
0.5 mg PO qd Renally dosed
Black box warning: lactic acidosis, hepatomegaly with steatosis
Tenofovir: *Preferred*
TDF: 300 mg PO qdTAF: 25 mg PO qd
Lamivudine 100 mg PO qd
Bacterial Fungal Viral Pneumocystis Unique Agents
Prevention and Treatment of Cancer-Related Infections. NCCN. Version 1.2018
©2018 MFMER | slide-23
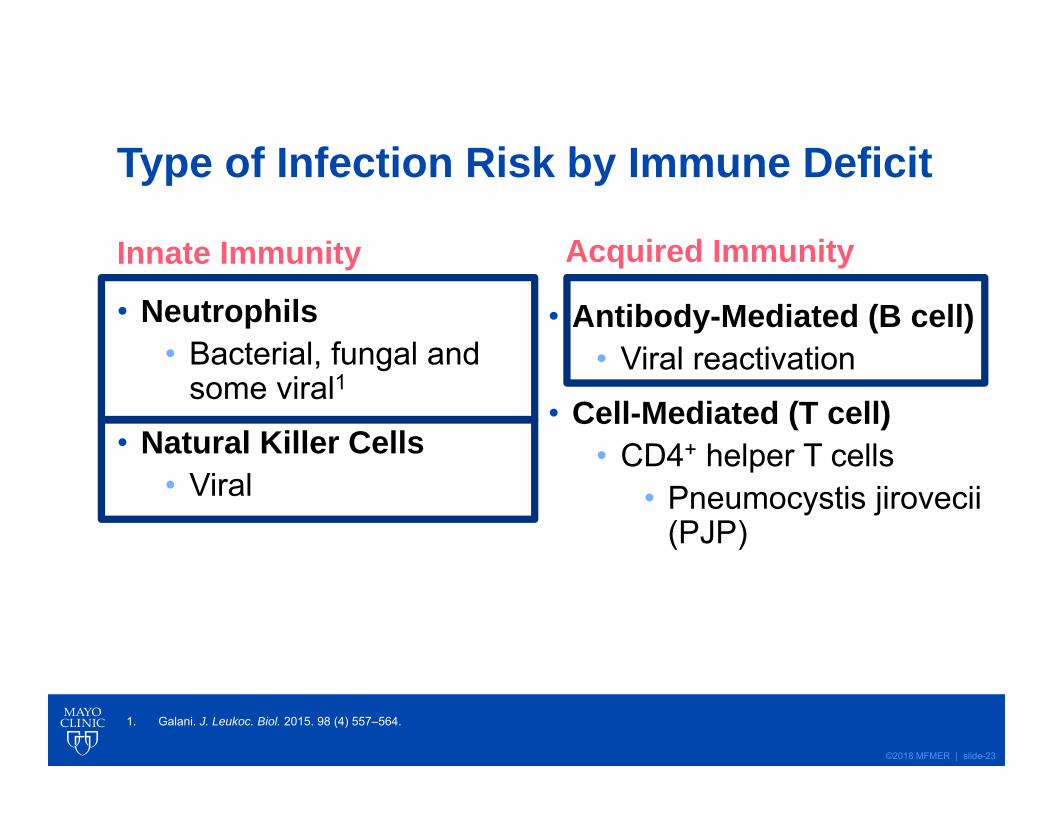
Type of Infection Risk by Immune Deficit
Innate Immunity
• Neutrophils• Bacterial, fungal and
some viral1
• Natural Killer Cells• Viral
Acquired Immunity
• Antibody-Mediated (B cell)• Viral reactivation
• Cell-Mediated (T cell)• CD4+ helper T cells
• Pneumocystis jirovecii (PJP)
1. Galani. J. Leukoc. Biol. 2015. 98 (4) 557–564.
©2018 MFMER | slide-24
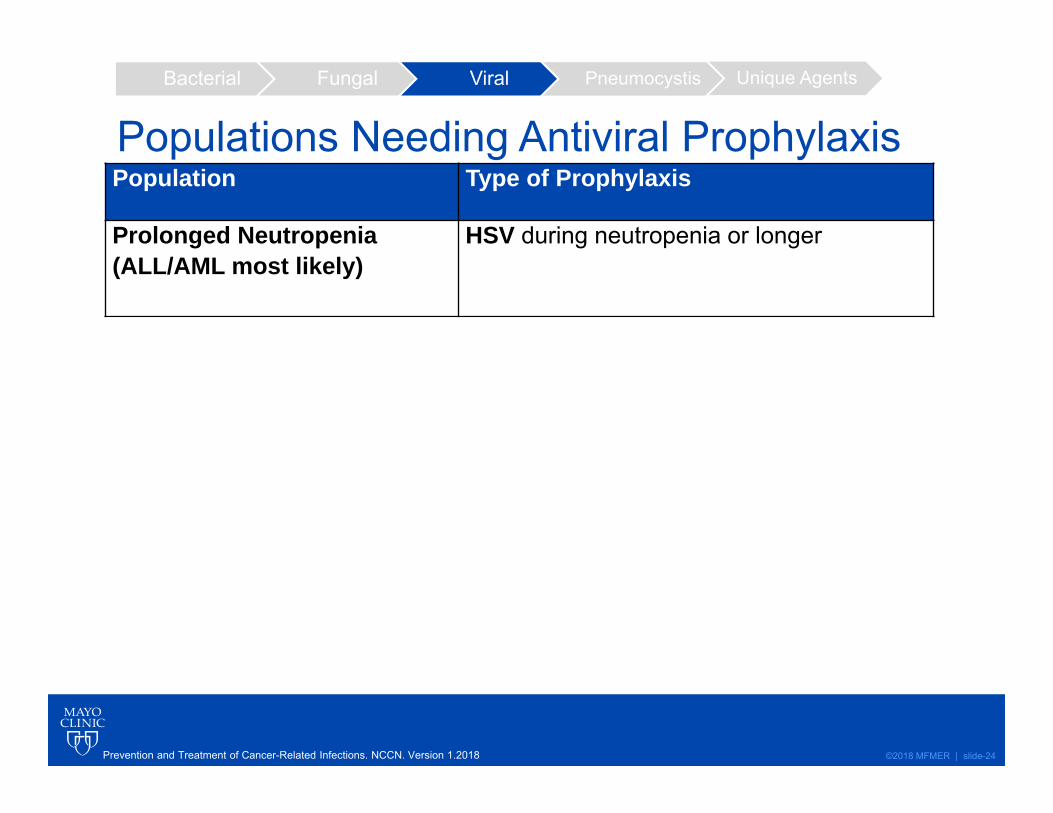
Population Type of Prophylaxis
Prolonged Neutropenia (ALL/AML most likely)
HSV during neutropenia or longer
Multiple Myeloma on proteasome inhibitor (bortezomib or carfilzomib)
VZV throughout therapy
Chronic Lymphocytic Leukemia (CLL) on alemtuzumab
HSV throughout therapyHBV (if HBsAg+) throughout therapyCMV surveillance throughout therapy
Lymphoma on CD-20antibody (rituximab)
HBV (if HBsAg+) throughout therapy
Any patient with previous episode
HSV throughout therapy
Bacterial Fungal Viral Pneumocystis Unique AgentsBacterial Fungal Viral Pneumocystis Unique Agents
Populations Needing Antiviral Prophylaxis
Prevention and Treatment of Cancer-Related Infections. NCCN. Version 1.2018

©2018 MFMER | slide-25
Summary of Antiviral, Antifungal and Antibacterial Prophylaxis • AML
• During neutropenia: levofloxacin, posaconazole & acyclovir*
• ALL • During neutropenia: levofloxacin, fluconazole(or an echinocandin),
acyclovir*
• CML/MM/Lymphoma: • Same as ALL during prolonged neutropenia• Refer to concomitant medications for antivirals to continue
throughout therapy
• Any patient• Acyclovir throughout therapy if past episode of HSV
*Acyclovir may be continued throughout therapy

©2018 MFMER | slide-26
Case for Assessment Question 1A patient with AML, recently discharged following count recovery is admitted due to pneumonia. She is started on cefepime. She is on levofloxacin, posaconazole and acyclovir prior to admission. Her ANC>2000 neutrophils/mcL.

©2018 MFMER | slide-27
What should you do with the levofloxacin & posaconazole?
A) Keep bothB) Keep the levofloxacin, discontinue the
posaconazoleC) Discontinue bothD) Discontinue the posaconzole, keep the
levofloxacin
©2018 MFMER | slide-28
What should you do with the levofloxacin & posaconazole?
A) Keep bothB) Keep the levofloxacin, discontinue the
posaconazoleC) Discontinue bothD) Discontinue the posaconzole, keep the
levofloxacin

©2018 MFMER | slide-29
PJP
Fungal Bacterial
Viral

©2018 MFMER | slide-30
Bacterial Fungal Viral Pneumocystis Unique Agents
Pneumocystis jirovecii (PJP) • Caused by fungus Pneumocystis jirovecii
• Overall mortality in non-HIV patients= 30.6%1
• Prophylaxis leads to 85% reduction in PJP2
1. Liu Y et al. Oncotarget. 2017;8(35)
Line of Therapy3
Drug Dose Reasons to not use
Preferred SMZ-TMP Bactrim SS©: 400-80 mg PO qdBactrim DS©: 800-160 mg PO 3x weekly
• Methotrexate use• May cause
myelosuppression
Alternate Pentamidine 300 mg inhaled through nebulizer every 4 weeks following albuterol neb
Breakthrough PJP in upper lobe
Dapsone 100 mg PO daily G6PD deficiency
Atovaquone 1500 mg daily of oral-suspension with high-fat meal
• Bad taste• Must take with food
SMZ-TMP: sulfamethoxazole-trimethoprim2. Stern. Cochrane Database Syst. Rev. 2014. (10).3. Prevention and Treatment of Cancer-Related Infections. NCCN. Version 1.2018

©2018 MFMER | slide-31
Type of Infection Risk by Immune Deficit
Innate Immunity
• Neutrophils• Bacterial, fungal and
some viral1
• Natural Killer Cells• Viral
Acquired Immunity
• Antibody-Mediated (B cell)• Viral reactivation
• Cell-Mediated (T cell)• CD4+ helper T cells
• Pneumocystis jirovecii (PJP)
1. Galani. J. Leukoc. Biol. 2015. 98 (4) 557–564.
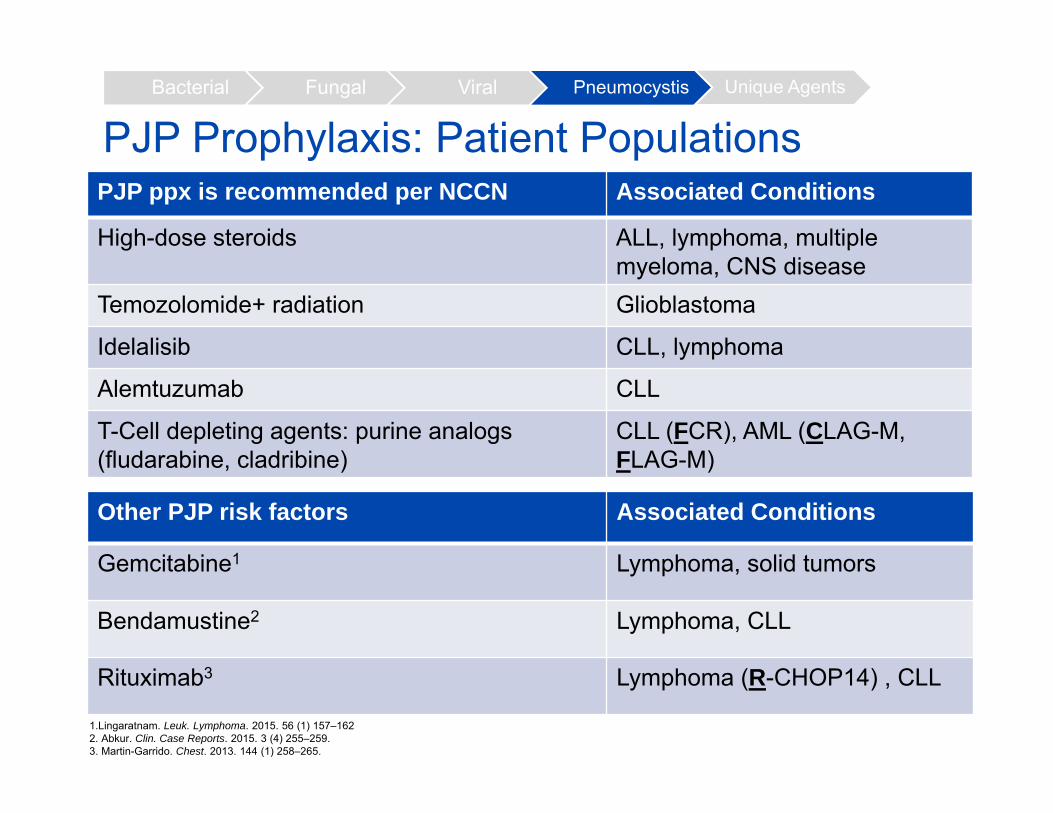
PJP Prophylaxis: Patient PopulationsPJP ppx is recommended per NCCN Associated Conditions
High-dose steroids ALL, lymphoma, multiple myeloma, CNS disease
Temozolomide+ radiation Glioblastoma
Idelalisib CLL, lymphoma
Alemtuzumab CLL
T-Cell depleting agents: purine analogs(fludarabine, cladribine)
CLL (FCR), AML (CLAG-M, FLAG-M)
Other PJP risk factors Associated Conditions
Gemcitabine1 Lymphoma, solid tumors
Bendamustine2 Lymphoma, CLL
Rituximab3 Lymphoma (R-CHOP14) , CLL
Bacterial Fungal Viral Pneumocystis Unique Agents
1.Lingaratnam. Leuk. Lymphoma. 2015. 56 (1) 157–1622. Abkur. Clin. Case Reports. 2015. 3 (4) 255–259.3. Martin-Garrido. Chest. 2013. 144 (1) 258–265.

©2018 MFMER | slide-33
Risk of PJP in Intermittent Steroid Use Intermittent Courses of Corticosteroids Also Present a Risk for Pneumocystis Pneumonia in Non-HIV Patients: Calero-Bernal et. al. 2016
Design Descriptive review of 128 cases of PJP, most without PJP ppx
Results • 50% of patients had hematological disease
• ~20% patients used steroids intermittently with chemotherapy (equiv. 70 mg of prednisone per day)
• Rituximab, methotrexate and everolimus most common other immunosuppressive agents in cases
Takeaway: intermittent steroids with chemotherapy may also be risk factor for PJP
Bacterial Fungal Viral Pneumocystis Unique Agents

©2018 MFMER | slide-34
Duration of Therapy for PJP Prophylaxis Group DurationAlemtuzumab For 2 months and until CD4+ count
is greater than 200 cells/mcLOther T-cell depleting therapies (purine analogs)
Until CD4+ count is greater than 200 cells/mcL
Corticosteroids Throughout active therapy, including taper and for at least 6 weeks after cessation1:
79 out of 113 patients (70%) with PJP were diagnosed with PJP during steroid taper period2
1. Cooley. Intern. Med. J. 2014. 44 (12b) 1350–1363.2. Sepkowitz. J. Am. Med. Assoc. 1992. 267 (6) 832–837.
Bacterial Fungal Viral Pneumocystis Unique Agents
©2018 MFMER | slide-35
Case for Assessment Question #2A Multiple Myeloma patient being treated with weekly CyBorD (Cyclophosphamide-Bortezomib-Dexamethasone) is admitted for pneumonia. Dexamethasone is given 40 mg (267 mg prednisone equivalent) weekly. He has SMZ-TMP and acyclovir as home meds. His ANC is >2000 neutrophils/mcL

©2018 MFMER | slide-36
What should you do with his SMZ-TMP and acyclovir?
A.Discontinue both agents B.Keep SMZ-TMP, stop acyclovir C.Keep both D.Keep both and add fluconazole

©2018 MFMER | slide-37
What should you do with his SMZ-TMP and acyclovir?
A.Discontinue both agents B.Keep SMZ-TMP, stop acyclovir C.Keep both D.Keep both and add fluconazole

©2018 MFMER | slide-38
Agents With Unique
Considerations
©2018 MFMER | slide-39
Type of Infection Risk by Immune Deficit
Innate Immunity
• Neutrophils• Bacterial, fungal and
some viral1
• Natural Killer Cells• Viral
Acquired Immunity
• Antibody-Mediated (B cell)• Viral reactivation
• Cell-Mediated (T cell)• CD4+ helper T cells
• Pneumocystis jirovecii (PJP)
1. Galani. J. Leukoc. Biol. 2015. 98 (4) 557–564.
Complement• Encapsulated bacteria
Bacterial Fungal Viral Pneumocystis Unique Agents

©2018 MFMER | slide-40
Bacterial Fungal Viral Pneumocystis Unique Agents
Eculizumab (Soliris©)
• Mechanism of action: high affinity to compliment protein C5
• Black box warning: meningococcal infections • 1000-2000 fold increase in meningococcal infection risk
• Manufacturer Recommendation: Provide meningococcal vaccines (MenACWY, MenB) 2 weeks prior to starting therapy
• If unable to wait two weeks: • Administer vaccines ASAP and provide 2 weeks of
antibacterial prophylaxis (ciprofloxacin or penicillin VK)
Soliris(Eculizumab) Prescr. Inf. 2018.

©2018 MFMER | slide-41
Bacterial Fungal Viral Pneumocystis Unique Agents
Need for Antibacterial Prophylaxis Throughout Eculizumab Therapy• 80% of eculizumab-treated meningococcal cases
had non-groupable N.meningitidis strains1
• Strains possibly not covered by vaccines1
• Cases reports of fully vaccinated pts with serogroup B meningitis2
• Consider prophylaxis with penicillin while on treatment2
1. Reher. Vaccine. 2018. 36 (19) 2507–2509.
2. McNamara. Am. J. Transplant. 2017. 17 (9) 2481–2484.

©2018 MFMER | slide-42
Bacterial Fungal Viral Pneumocystis Unique Agents
Alemtuzumab (Campath©)• Mechanism: binds to CD52 on surface of B and T lymphocytes,
monocytes, macrophages and natural killer cells
• 18% of patients in approval study had fatal infections (on prophylaxis)
Category Recommendation Duration
Viral HSV: Yes CMV: weekly surveillance HBV: if positive
>2 months after completion & CD4+>200 cells/mcL
PJP Yes
Bacterial No recommendation
Fungal
Campath(Alemtuzumab). Prescr. Inf. 2003

©2018 MFMER | slide-43
True or False: there is some evidence that SMZ-TMP may have value throughout eculizumab therapy

©2018 MFMER | slide-44
True or False: there is some evidence that SMZ-TMP may have value throughout eculizumab therapy

©2018 MFMER | slide-45
Summary• Prolonged neutropenia generally necessitates
antibacterial, antifungal and antiviral prophylaxis and is most common in acute leukemia patients
• Steroids and T-cell depleting agents, such as alemtuzumab, increase risk of PJP
• Assessment of oncology drug interactions, hepatic/renal function, and risk of myelosuppression is key to regimen selection
• Alemtuzumab and eculizumab are two agents with unique antimicrobial prophylaxis considerations

©2018 MFMER | slide-46
Fungal Spectrum vs CostDrug Cost Per Day ($)
Fluconazole 28.64Voriconazole 62.54
Itraconzole 90.56
Isavuconazonium sulfate/isavuconazole
209.58
Posaconazole 234.96
Echinocandins (micafungin & caspofungin & anidulafungin)
Caspo: 112.80Mica: 112.20 Ani: 216
Amphotericin B 3262.27 weekly (466daily)
Bacterial Fungal Pneumocystis Viral

©2018 MFMER | slide-47
Common Viral Pathogens of ConcernPercent of Patients Seropositive
Pathology
HSV- Herpes Simplex Virus
HSV-1: 53.9% in 14-49 year oldsHSV-2: 15.7% in 14-49 year olds
Skin lesions, meningitis, blindness, encephalitis
VZV- VaricellaZoster Virus
98% in 20-49 year olds Rash, neuritis, aseptic meningitis, neuropathy, encephalitis, pneumonitis, hepatitis, pancreatitis
HBV- Hepatitis B Virus
0.27% HBsAg+ Acute hepatitis, chronic liver disease, cirrhosis, and hepatocellular carcinoma
CMV-Cytomegalovirus
58.9% of patients > 6 years>90% of patients > 90 years
Colitis, hepatitis, encephalitis, peri/myocarditis, retinitis, Guillen-Barre syndrome
Bacterial Fungal Pneumocystis Viral