20th annual needham virtual healthcare conference
TRANSCRIPT

20th Annual Needham Virtual Healthcare Conference
NASDAQ: MEIP
April 12, 2021

Forward-Looking Statements
• This presentation contains, and our officers and representatives may from time to time make, statements that are “forward-looking
statements” within the meaning of the safe harbor provisions of the U.S. Private Securities Litigation Reform Act of 1995. Examples of
forward-looking statements include, among others, statements regarding our development strategy; potential advantages of our product
candidates; the initiation and completion of preclinical and clinical studies and the reporting of the results thereof; the timing of regulatory
submissions and actions; the sufficiency of our existing cash; and all other statements relating to our plans, objectives, expectations and
beliefs regarding future performance, operations, financial condition and other future events (including assumptions underlying or
relating to any of the foregoing).
• These forward-looking statements rely on a number of assumptions concerning future events and are subject to a number of risks,
uncertainties, and other factors, many of which are outside of our control. Important factors that could cause our actual results and
financial condition to differ materially from those indicated in forward-looking statements include, among others: uncertainties relating to
the initiation and completion of preclinical and clinical studies; whether preclinical and clinical study results will validate and support the
safety and efficacy of our product candidates; the outcome of regulatory reviews of our product candidates; varying interpretation of
research and development and market data; the impact of the COVID-19 pandemic on our industry and individual companies, including
on our counterparties, the supply chain, the execution of our clinical development programs, our access to financing and the allocation of
government resources; risks and uncertainties relating to intellectual property and the other factors discussed under the caption “Item
1A. Risk Factors” in our most recent annual report on Form 10-K and our most recent quarterly report on Form 10-Q.
• Any forward-looking statement made by us in this presentation is based only on information currently available to us and speaks only as
of the date on which it is made. In addition, we operate in a highly competitive and rapidly changing environment, and new risks may
arise. Accordingly, you should not place any reliance on forward-looking statements as a prediction of actual results. We disclaim any
intention to, and undertake no obligation to, update or revise any forward-looking statement. You are urged to carefully review and
consider the various disclosures in our most recent annual report on Form 10-K, our most recent Form 10-Q and our other public filings
with the SEC since the filing of our most recent annual report.
2
MEI Pharma: Who We Are
• Clinical Development Company Building a Leading
Oncology Franchise with 4 Clinical-Stage Programs:
Focus On HemOnc
• Zandelisib (f/k/a ME-401) Potential Best-in-Class PI3Kδ
Inhibitor in Phase 2 Study Intended to Support Accelerated
Approval with U.S. FDA
• Well Capitalized with ~$180 Million*
* As of December 31, 2020, MEI had $180.1 million in cash, cash equivalents, and short-term investments with no outstanding debt. 3

PROGRAMS INDICATION COMBINATION PHASE 1/1B PHASE 2 PHASE 3COMMERCIAL
RIGHTS
ZandelisibOral P13K Delta
Inhibitor
Follicular & Marginal
Zone Lymphomas
Relapsed/refractoryMonotherapy
U.S. co-promote;
ex-U.S. Kyowa Kirin
exclusive rights
B-Cell Malignancies
Relapsed/refractory
• Monotherapy
• Rituxan®(rituximab)
• Zanubrutinib2
VoruciclibOral CDK Inhibitor
B-Cell Malignancies
& AML
Relapsed/refractory
• Monotherapy
• Venclexta® (venetoclax)3
ME-344Mitochondrial Inhibitor
Solid Tumors Avastin® (bevacizumab)4
PracinostatHDAC Inhibitor
Myelodysplastic
Syndrome
Treatment-naïve
Vidaza® (azacitidine)
Late-Stage Diversified Clinical Pipeline
TIDAL Study1
Clinical Collaboration
1. Phase 2 study intended to support an accelerated approval marketing applications with FDA. 2. Study arm initiated under clinical collaboration with BeiGene, Ltd. 3. Initiation of clinical studies is subject to opening of a new Investigational New Drug Application with FDA 4. Investigator-initiated trial.
4

Zandelisib: Data Driven Advancement in B-cell
Malignancies

The GapNavigating T-reg mediated toxicity to
achieve clinical potential
Zandelisib: Potential to Bridge the Gap and Realize the Promise of PI3Kδ Inhibition
The Challenge The Promise
6

Zandelisib: Potential to Bridge the Gap and Realize the Promise of PI3Kδ Inhibition
* MEI Pharma clinical and preclinical data on file.
**Zandelisib data reported from ongoing Phase 1b study of 57 patients, including ORR and DOR in r/r FL (36) and other B-cell malignancies (21). Data cutoff presented: April 13, 2020.
The Challenge: The Promise:
7
Zandelisib:
Bridging The Gap
• Binding kinetics• Selective inhibition
• Trough Plasma >EC90
• Tumor penetration
• High volume of distribution
• Tumor Accumulation
Properties Supporting Potential Clinical Profile Optimization*
Realize utility of PI3Kδ
in B-cells but limit
toxicity associated with
target in T-regs
Emerging Zandelisib
Profile*
• High Response Rates
• Durable to Date
• Well-tolerated
Daily
x1 week
(60mg)
No therapy
x3 weeks
Daily dosing x2 cycles
(60mg)
Cycles 1 and 2 IS on Cycles ≥3
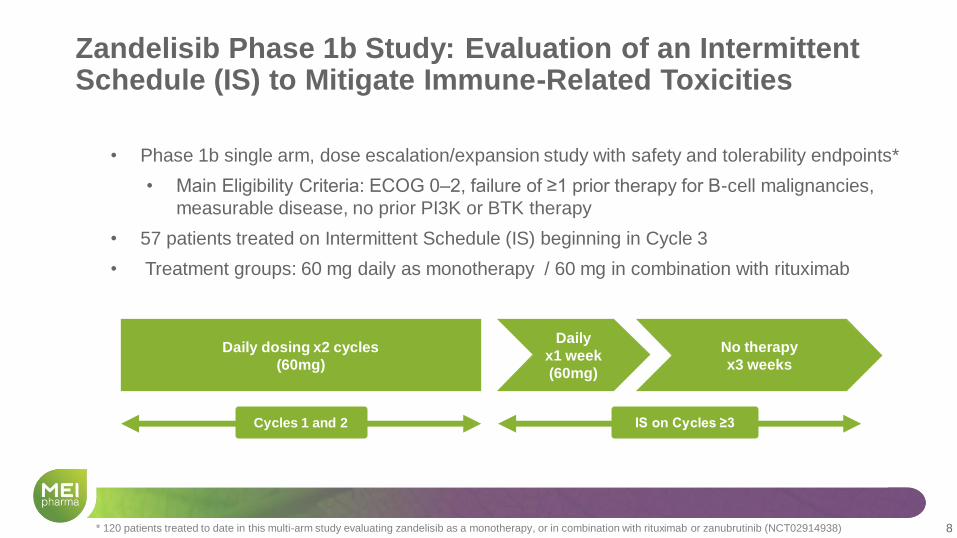
• Phase 1b single arm, dose escalation/expansion study with safety and tolerability endpoints*
• Main Eligibility Criteria: ECOG 0‒2, failure of ≥1 prior therapy for B-cell malignancies,
measurable disease, no prior PI3K or BTK therapy
• 57 patients treated on Intermittent Schedule (IS) beginning in Cycle 3
• Treatment groups: 60 mg daily as monotherapy / 60 mg in combination with rituximab
Zandelisib Phase 1b Study: Evaluation of an Intermittent Schedule (IS) to Mitigate Immune-Related Toxicities
8* 120 patients treated to date in this multi-arm study evaluating zandelisib as a monotherapy, or in combination with rituximab or zanubrutinib (NCT02914938)

Zandelisib Phase 1b Study: Key Findings
• Intermittent Schedule yields a high ORR in R/R FL and CLL/SLL
• FL: 76% as monotherapy (n =17) and 89% with rituximab (n=19)
• CLL/SLL: 89% (n=9)
• Median DOR in FL is not reached with a median follow-up 13.2 months
• Durable responses regardless of prior lines of therapy, treatment group
(± rituximab) or tumor bulk
• Treatment dose and schedule appear to be well tolerated
• Low incidence of Grade ≥3 AESI
• No Grade ≥3 AESI reported after Cycle 3
• Discontinuation rate due to adverse events = 7%
9Zelenetz et al, ASCO 2020. Data cutoff: April 13, 2020.

Low Incidence of AESI: No Increased Toxicity Over Time
Gr3 Adverse Events of
Special Interest (AESI)
Diarrhea
Diarrhea
Colitis
2 (3.5%)
2 (3.5%)
Rash, all Types 1 (1.8%)
ALT/AST elevation 1 (1.8%)
Stomatitis 0
Pneumonia / Infectious
pneumonitis0*
Non-infectious pneumonitis 1 (1.8%)
10
• All Grade 3 AESI occurred in Cycles 1-3
• No Grade 4 AESI
Time to First Grade ≥ 3 AESI (N=57)
No. of
Subjects
with Events
Incidence
Rate
Follow-up Time
Median
(min-max)
7 12.2% 12.5 m ( 0.6 – 28.6)
*1 patient with Grade 5 Covid-19 pneumonia in Cycle 15 not included
• Discontinuations due to AEs in 4 patients (7%)
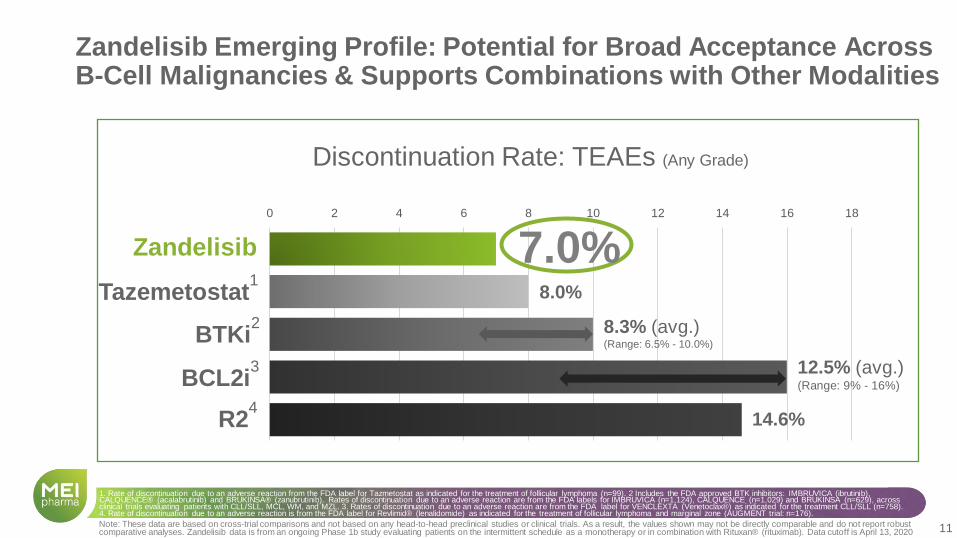
0 2 4 6 8 10 12 14 16 18
Discontinuation Rate: TEAEs (Any Grade)
Zandelisib
BCL2i3
BTKi2
Zandelisib Emerging Profile: Potential for Broad Acceptance Across B-Cell Malignancies & Supports Combinations with Other Modalities
Note: These data are based on cross-trial comparisons and not based on any head-to-head preclinical studies or clinical trials. As a result, the values shown may not be directly comparable and do not report robust comparative analyses. Zandelisib data is from an ongoing Phase 1b study evaluating patients on the intermittent schedule as a monotherapy or in combination with Rituxan® (rituximab). Data cutoff is April 13, 2020
R24
1. Rate of discontinuation due to an adverse reaction from the FDA label for Tazmetostat as indicated for the treatment of follicular lymphoma (n=99). 2 Includes the FDA approved BTK inhibitors: IMBRUVICA (ibrutinib), CALQUENCE® (acalabrutinib) and BRUKINSA® (zanubrutinib). Rates of discontinuation due to an adverse reaction are from the FDA labels for IMBRUVICA (n=1,124), CALQUENCE (n=1,029) and BRUKINSA (n=629), across clinical trials evaluating patients with CLL/SLL, MCL, WM, and MZL. 3. Rates of discontinuation due to an adverse reaction are from the FDA label for VENCLEXTA (Venetoclax®) as indicated for the treatment CLL/SLL (n=758). 4. Rate of discontinuation due to an adverse reaction is from the FDA label for Revlimid® (lenalidomide) as indicated for the treatment of follicular lymphoma and marginal zone (AUGMENT trial: n=176).
8.3% (avg.)(Range: 6.5% - 10.0%)
14.6%
12.5% (avg.)(Range: 9% - 16%)
7.0%
11
8.0%Tazemetostat1
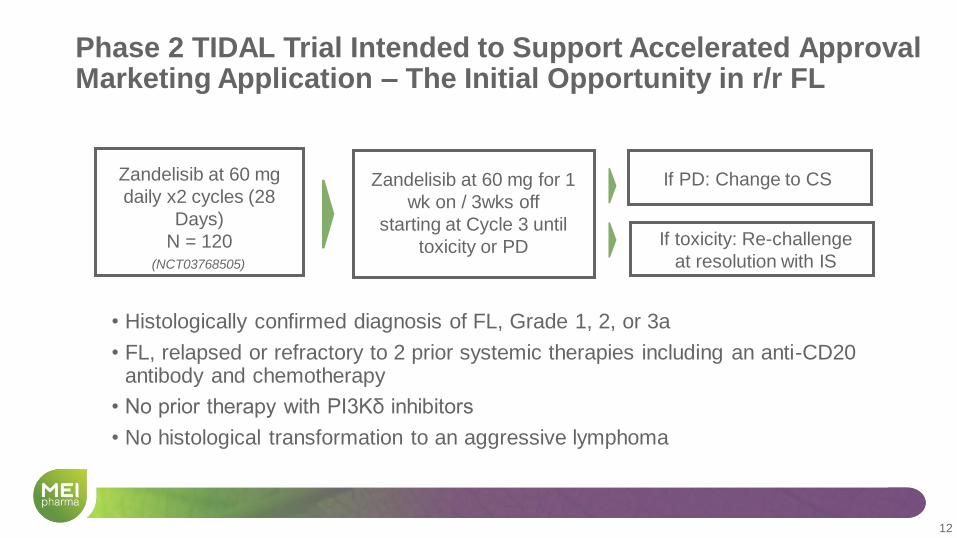
12
Zandelisib at 60 mg
daily x2 cycles (28
Days)
N = 120
Zandelisib at 60 mg for 1
wk on / 3wks off
starting at Cycle 3 until
toxicity or PD If toxicity: Re-challenge
at resolution with IS
• Histologically confirmed diagnosis of FL, Grade 1, 2, or 3a
• FL, relapsed or refractory to 2 prior systemic therapies including an anti-CD20 antibody and chemotherapy
• No prior therapy with PI3Kδ inhibitors
• No histological transformation to an aggressive lymphoma
12
If PD: Change to CS
Phase 2 TIDAL Trial Intended to Support Accelerated Approval Marketing Application – The Initial Opportunity in r/r FL
(NCT03768505)

Expanding Zandelisib Development Activities to Explore Full Potential
• TIDAL study arm evaluating zandelisib monotherapy as ≥3rd line therapy in
marginal zone lymphoma (MZL)
• COASTAL Phase 3 study evaluating zandelisib + rituximab as ≥2nd line therapy in R/R FL and MZL
• Expanding evaluation of combination with zanubrutinib into disease specific B-cell malignancy cohorts
• Japan PMDA registrational Phase 2 study evaluating zandelisib monotherapy in
R/R indolent B-cell lymphoma
• Selective IIT’s (e.g., zandelisib + R-CHOP as 1st line therapy in DLBCL at the Cleveland Clinic)
13
$582Min potential development, regulatory and
commercial milestones
KKC exclusive ex-U.S. rights, MEI to receive escalating tiered royalties starting in teens
U.S. COST SHARING, KKC responsible for incremental ex-U.S. costs
AGREED ON BROAD DEVELOPMENT PLAN for B-cell malignancies
Global License, Development and Commercialization Agreement Optimizes Zandelisib Value (April 2020)
$100M upfront to MEI
50/50U.S. co-promote,
MEI books U.S. sales
14
Market Opportunity
Zandelisib has the Potential to Set the Clinical and Commercial Opportunity Bar for the PI3Kd Class
15
• R/R FL has several treatment
options but no standard of care
Zandelisib Opportunity
15
• PI3Kd inhibitors deliver potent efficacy, but utility limited by the
extensive T-reg mediated toxicity
• PI3Kd inhibitors limited to modest
≥ 3rd Line FL use due to
risk/benefit of current therapies
• Product attributes and novel
treatment schedule could reset
expectations of PI3Kd inhibitors
• Compelling emerging profile
supports best-in-class
opportunity in 3L FL
• Unique zandelisib properties and
combinability could expand utility
to earlier lines of FL and into other
BCMs

Relapsed/Refractory FL: A Significant and Expanding Addressable Market
Company estimates
~15,000: U.S. incidence of
follicular lymphoma
>50% relapse after each
remission
100K: U.S. follicular
lymphoma prevalence
>7,500 U.S. Patients
With Relapsed/Refractory
Follicular Lymphoma
$1B
Addressable
Market
16
ZandelisibConclusion
Multiple
Combination
Regimen
Opportunities
Differentiated
Profile Results in
Best-in-class
Potential
Potential to Meet
Need Across
Multiple B-cell
Malignancies
Zandelisib: Potential to Realize PI3Kδ Promise
17

Voruciclib: Oral CDK Inhibitor with
Potent CDK9 Activity

Voruciclib: Orally Administered CDK Inhibitor with Potent CDK9 Inhibition
Potential Combination Opportunities in Multiple Hematologic and Solid Tumor
Indications
Increased MCL1 is an established
venetoclax resistance mechanism
• Venetoclax inhibits BCL2 but can lead to
stabilization of MCL1
• Voruciclib inhibits MCL1 via CDK9 inhibition
19
CDK9 Regulates MCL1 and MYC
• MCL1 is a pro-survival protein in the BCL-2 family
• MYC is an oncoprotein that drives growth and proliferation in many tumor types
MYC is over expressed in many cancers,
including those with KRAS mutations
• Inhibition of CDK9 leads to reduced transcription
and stability of MYC
• Voruciclib downregulates MYC via CDK9
inhibition

Leveraging CDK9 Regulation of MCL1: Phase 1 Study in R/R B-Cell Malignancies and AML
• Study population• Relapsed/Refractory B-cell Malignancies
• AML After Treatment with Standard Therapy
• Dose escalation with standard 3+3 design
• Endpoints• Safety and tolerability
• Pharmacokinetics
• Biologic correlative studies• BH3 profiling, MCL-1 expression (Dana Farber)
• Molecular mutations analysis (City of Hope)
• Objective response rates
• CR/CRi rate
Voruciclib single agent
dose escalation
Venetoclax + Voruciclib dose
escalation
100
mg
150
mg
200
mg
50
mg
100
mg
150
mg
200
mgV2
20

Leveraging CDK9 Regulation of MYC Transcription and Protein Stability
A. Transcription of MYC B. MYC protein stability
DSIF
HEXIM
NELF
Pol II DSIF Pol II
Inhibitory Complex Cell Stimulatory Signals
Productive elongation of RNA Pol II transcription of target genes
(e.g., MYC, MCL1)
Promoter proximal pausing relieved by PTEFb &
CDK9 activity
KRAS
PI3K
GSK3β
CDK9
P P
PTEFbCDK9
PTEFb
RAF
MEK
MYC
MYC
MYC proteindegradation
by proteasome
SCF-Fbw7Ubiquitin
sotorasibadagrasib
pT58
Pin1
Pin1PP2A
pS62 pS62 pT58
(unstable)
voruciclib
voruciclib
Transcriptionof MYC
(stable)
Transcriptionalactivation of
MYC target genes
MYC MYC
ERK1
CDK9
MePCELARP7
21

Voruciclib Inhibits KRAS Mutant Cell Lines In Vitro and In Vivo in Xenograft Mice
Cell Line Indication KRAS Mut IC50 (µM)
Gp2D CRC G12D 0.8
HCT-116 CRC G13D 1.8
LS-513 CRC G12D 0.6
SW-480 CRC G12V 3.9
SW837 CRC G12C 2.1
KYSE-410 Esoph G12C 1.9
RPMI-8226 MM G12A 2.4
A-549 NSCLC G12S 1.5
Calu-1 NSCLC G12C 2.0
HCC1171 NSCLC G12C 3.0
HCC44 NSCLC G12C 0.8
NCI-H460 NSCLC Q61H 3.1
NCI-H1373 NSCLC G12C 1.2
NCI-H1792 NSCLC G12C 1.4
NCI-H2030 NSCLC G12C 1.1
NCI-H23 NSCLC G12C 1.2
NCI-H358 NSCLC G12C 0.6
TOV-21G Ovarian G13C 1.7
AsPC-1 PDAC G12D 2.3
HPAF-II PDAC G12D 1.9
MIA PaCa-2 PDAC G12C 1.1
Panc 04.03 PDAC G12D 1.4
A. B.
Time (days)
Ave
tum
or
weig
ht
(mg) 600
500
400
100
200
300
0
0 2 4 6 8 10 12 14
1800
1600
1400
1200
1000
800
600
400
200
0
0 2 4 6
Time (days)
Ave
tum
or
weig
ht
(mg)
8 10 12
Control
VOR 100 mg/kg
VOR 50 mg/kg
VOR 200 mg/kg
6000
5000
4000
3000
2000
1000
00 2 4 6
Time (days)
Ave
tum
or
weig
ht
(mg)
8 10 12
Control
VOR 100 mg/kg
VOR 50 mg/kg
VOR 200 mg/kg
Control
VOR 100 mg/kg
VOR 200 mg/kg
HCT-116
(CRC, KRAS G13D)
SW-480
(CRC, KRAS G12V)
H460
(NSCLC, KRAS Q61H)
22

Leveraging CDK9 Regulation of MYC: Exploring Synergy with Direct KRAS Inhibitors
23
Synergy Scores
Cell LineKRASmut
Sensitivity to G12C Inhibitors
Voruciclib + Sotorasib
Voruciclib +Adagrasib
NCI-H23 G12C High
HCC1171 G12C High
MIA Paca-2 G12C High
SW837 G12C Moderate - High
NCI-H2030 G12C High
Calu-1 G12C Moderate - High
HCC-44 G12C Moderate - High
NCI-H1373 G12C Moderate - High
NCI-H358 G12C High
NCI-H1792 G12C Moderate - High
KYSE-410 G12C Low - High
Panc 04.03 G12D Low
Gp2D G12D Low
LS-513 G12D Low - Moderate
AsPC-1 G12D Low
HPAF-II G12D Low
TOV-21G G13C Low Low HighModerate
Esophageal cancer cell lineColorectal cancer cell lines
Non-small cell lung cancer cell linesPancreatic adenocarcinoma cell lines
Ovarian cell line
VORUCICLIB SYNERGIZES WITH KRAS G12C INHIBITORS IN VITRO
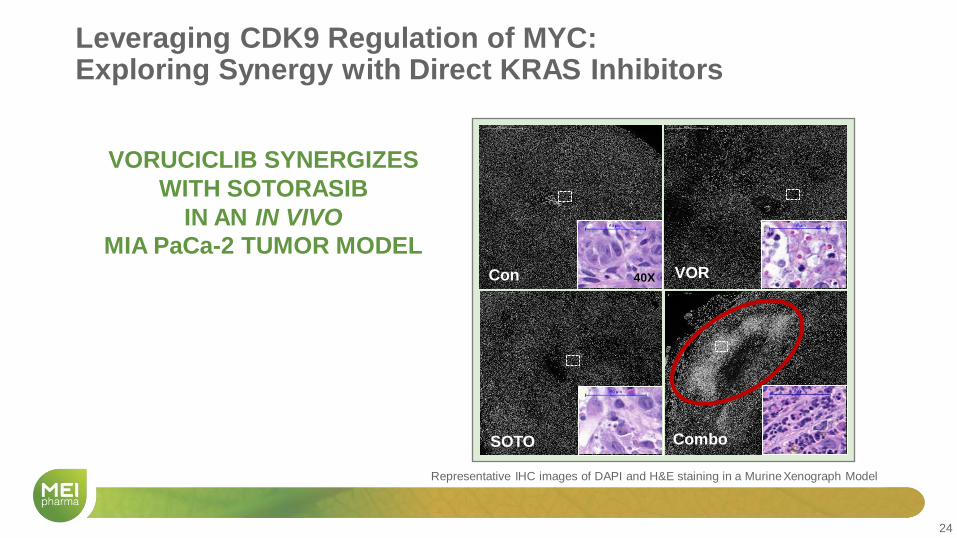
Leveraging CDK9 Regulation of MYC: Exploring Synergy with Direct KRAS Inhibitors
24
VORUCICLIB SYNERGIZES
WITH SOTORASIB
IN AN IN VIVO
MIA PaCa-2 TUMOR MODELCon VOR
SOTO Combo
40X
Representative IHC images of DAPI and H&E staining in a Murine Xenograph Model

Key Upcoming 12 Month Milestones Across Portfolio• Zandelisib
• TIDAL: announce top-line data in Q4 2021
• New clinical studies to expand development, including:• COASTAL, intended confirmatory Phase 3 study + Rituxan® in 2L FL/MZL
• 3L MZL (TIDAL Study arm)
• 1L DLBCL + RCHOP (IIT)
• Initial data of phase 1b evaluating zandelisib with zanubrutinib under
clinical collaboration with BeiGene
• Voruciclib
• Initial data, Phase 1 monotherapy and +BCL2i data updates
• ME-344
• Institute plan to leverage clinically demonstrated anti-tumor activity in
combination with anti-VEGF
• Pracinostat
• Program / Phase 2 MDS Helsinn Update
Timing subject to developments related to the COVID-19 pandemic 25

20th Annual Needham Virtual Healthcare Conference
NASDAQ: MEIP
April 12, 2021