21 july 2011. follow-up to previous reviews tramadol with ssri’s or snri’s potential for...
TRANSCRIPT
Idaho Medicaid Drug Utilization Review Program
21 July 2011
Follow-up to Previous Reviews
Tramadol with SSRI’s or SNRI’s Potential for Serotonin Syndrome
Thiazolidinedione (TZD) Safety
Proton Pump Inhibitors Long Term Continuous Use
2
Tramadol with SSRI’s or SNRI’s: Potential for Serotonin Syndrome
Patients were selected if they had more than one tramadol fill, at least a 30 day overlap with the SSRI or SNRI, and had both a tramadol and an antidepressant claim within the most recent six weeks of data.
179 patient profiles were evaluated.Letters were sent to 174 prescribers about 94 patients
on 2/21/2011.Only prescribers of tramadol, SSRI, or SNRI received
letters.As of 7/5/2011, 42 responses have been received (24%
response rate.)See packet for copy of the letter and the Serotonin
Syndrome Informational sheet. 3
Tramadol with SSRIs or SNRIsPotential for Serotonin Syndrome Response detail as of 7/5/2011Note that providers may choose more than one selection
per response.Reviewed and do not believe adjustment is needed
15Reviewed and have or will modify the treatment 6 Information clinically useful: plan to monitor 11 I will use this information in the care of future pts
10No longer my patient 6My patient, but I did not prescribe this 3Somewhat useful to my practice 5Not useful to my practice 4Very useful to my practice 9
4
Tramadol with SSRIs or SNRIsPotential for Serotonin Syndrome Response detail as of 7/5/2011 “We are actually tapering the tramadol. Used it as a way to stop opioid
use.” “I was not aware that the patient was on tramadol.” “Thank You” “This patient did not report to me that she was on tramadol to the best of
my memory. She has since been fired from my office for med seeking behavior.”
“Defer long term considerations to patient’s primary provider. I am an ER provider only for this patient.”
“tramadol has been discontinued” “Have already started taper and will be off in 30-60 days” “she is only taking tramadol 2 to 3 times a week and we are going to try to
stop completely. She is trying to take Excedrin for migraines. No new order for tramadol was given at last visit.”
“Review with supervising physician. Historically before I started seeing this patient. I only provide follow up care at the facility this report is referring to. Often the patients have been stable on their meds for quite some time and to make any changes could cause decompensation. When possible I attempt to make reductions when appropriate. I will still use the information provided as appropriate.”
5
Thiazolidinediones (TZD’s)
Patients were selected for evaluation if there was a paid claim for a TZD within the last three months.
83 patient profiles were evaluated.Letters were sent to 65 prescribers about 63
patients on 3/22/2011.As of 7/5/2011, 16 responses have been
received (25% response rate.)See packet for copy of the letter and FDA
Drug Safety Communication Insert.6
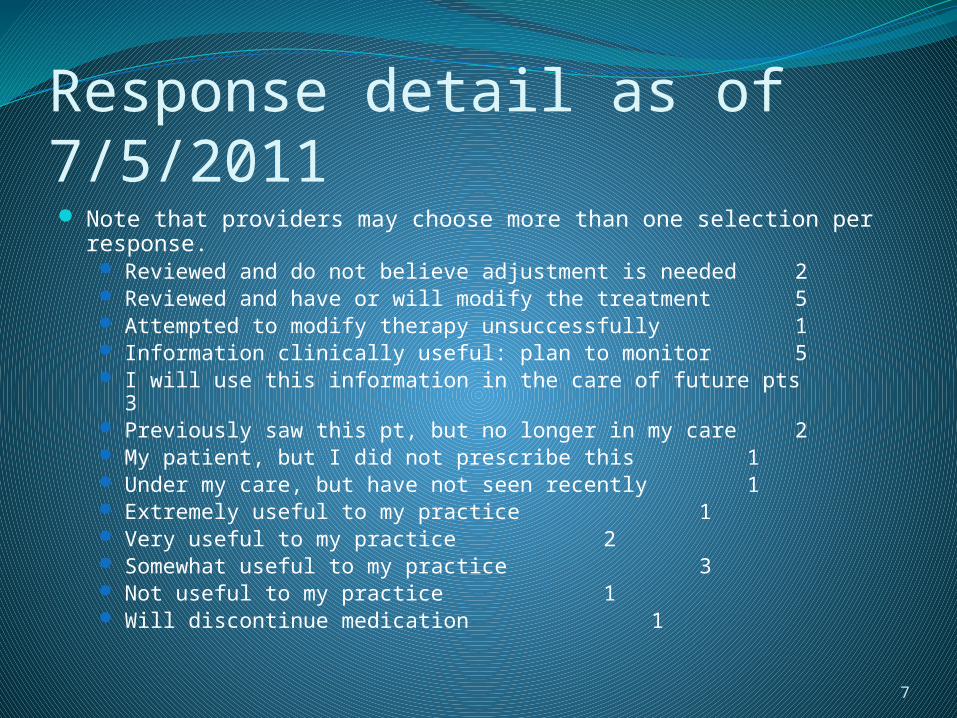
Thiazolidinedione Safety Response detail as of 7/5/2011 Note that providers may choose more than one selection per
response. Reviewed and do not believe adjustment is needed 2 Reviewed and have or will modify the treatment 5 Attempted to modify therapy unsuccessfully 1 Information clinically useful: plan to monitor 5 I will use this information in the care of future pts 3 Previously saw this pt, but no longer in my care 2 My patient, but I did not prescribe this 1 Under my care, but have not seen recently 1 Extremely useful to my practice 1 Very useful to my practice 2 Somewhat useful to my practice 3 Not useful to my practice 1 Will discontinue medication 1
7
Thiazolidinedione SafetyResponse detail as of 7/5/2011 “Patient was already on Avandia® and doing well prior to the drug label
change and guidelines state ok to use in patients already on this med. Patient did not want to change then I will approach him again to consider change to Actos®”
“I am already complying with the above and am no longer prescribing Avandia®”. Note that prescriber also wrote in next to #8 that medication was reordered.
“Control is poor with metformin. Patient is reluctant to try insulin at this time. Her diabetes control is poor.”
“Plan to modify therapy. Actos ®15mg every day” “NO CHANGE” “Patient has been informed of risks and wishes to continue Avandia®” “Review with supervising physician. Historically before I started seeing
this patient. I only provide follow up care at the facility this report is referring to. Often the patients have been stable on their meds for quite some time and to make any changes could cause decompensation. When possible I attempt to make reductions when appropriate. I will still use the information provided as appropriate.”
“Will start Actos®”8
Thiazolidinediones (TZD’s)Risk Evaluation and Mitigation Strategy
(REMS)Rosiglitazone REMS Program
Approved 05/2011 Goals
To restrict access to rosiglitazone-containing medicines so that only prescribers who acknowledge the potential increased risk of myocardial infarction associated with the use of rosiglitazone are prescribing rosiglitazone.
To restrict access to patients who have been advised by a healthcare provider about the potential increased risk of myocardial infarction associated with the use of rosiglitazone and are one of the following: Either already taking rosiglitazone or If not already taking rosiglitazone, they are unable to achieve
glycemic control on other medications and, in consultation with their healthcare provider, have decided not to take pioglitazone for medical reasons
9
Thiazolidinediones (TZD’s)Risk Evaluation and Mitigation Strategy
(REMS)Rosiglitazone REMS Program
Elements to Assure Safe Use Healthcare providers who prescribe rosiglitazone-
containing medicines for outpatient or long-term care use are specifically certified
Rosiglitazone will be dispensed only by specially certified pharmacies Medication will be mailed to the patient
Rosiglitazone will only be dispensed to patients with evidence or other documentation of safe-use conditions Patient must review the Medication Guide and sign the
Patient Enrollment Form with their prescriber Distributors will become certified and all
rosiglitazone medicines will be withdrawn from uncertified pharmacies within 6 months after initial approval of the REMS
10
Thiazolidinediones (TZD’s)Risk Evaluation and Mitigation Strategy
(REMS)Rosiglitazone REMS Program (Avandia-
Rosiglitazone Medicines Access Program™)
www.avandia.com or Phone: 1-800-AVANDIA (1-800-282-6342)Fax: 1-888-772-9404
11
http://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/UCM255624.pdf
Proton Pump Inhibitors: Long Term Continuous UsePatients were selected for evaluation if they
had at least 8 claims for a PPI over the six month period.
167 patient profiles were evaluated.Letters were sent to 473 prescribers about
92 patients on 4/11/2011 (19% lettering rate.)As of 7/5/2011, 113 responses have been
received (24% response rate.)See packet for copy of the letter and
informational sheet.12
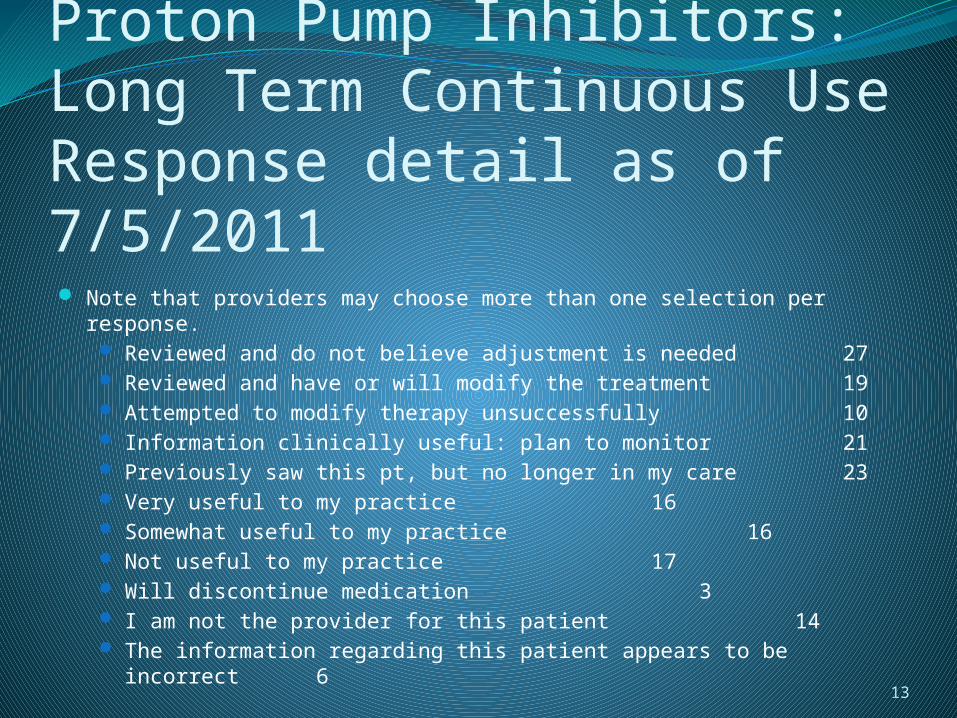
Proton Pump Inhibitors: Long Term Continuous UseResponse detail as of 7/5/2011 Note that providers may choose more than one selection per response.
Reviewed and do not believe adjustment is needed27
Reviewed and have or will modify the treatment19
Attempted to modify therapy unsuccessfully10
Information clinically useful: plan to monitor21
Previously saw this pt, but no longer in my care23
Very useful to my practice 16 Somewhat useful to my practice
16 Not useful to my practice 17 Will discontinue medication
3 I am not the provider for this patient
14 The information regarding this patient appears to be incorrect
6
13
Proton Pump Inhibitors: Long Term Continuous UseResponse detail as of 7/5/2011 “I agreed to refills but did not know how she had done eight refills in six
months” “Patient has seen gastroenterologist and otolaryngologist who
recommended the higher dose.” “I was on call and covering for another provider” “The procedure ID on December 28 2010 is not mine. I never prescribed
Omeprazole to this patient. Please correct error” “Will review in closer detail her symptoms and discontinue of her PPI” “Prescribed this medication for this patient” “Previous NP saw this patient and she has left office” “Try to taper and use H2 blockers for breakthrough symptoms. Patient is
intellectually disabled and lives in a residential treatment center.” “Taper dose and uses H2 blockers for breakthrough. This patient has a
diagnosis of eosinophilic gastritis and is being monitored closely. He can purposely vomit if he is upset for whatever reason possible anxiety. Very complex patient is intellectually disabled and lives in a residential treatment center.” 14

Proton Pump Inhibitors: Long Term Continuous UseResponse detail as of 7/5/2011 “Chronic GERD” “Loves the medication and does not want to stop. Wonders if she can take
medication less often but continues. She will call back after receiving more information.”
“Patient dismissed from clinic and care.” “I cared for this patient in the hospital but not as an outpatient.” “Getting to be annoying.” “I am not the prescriber.” “Increase GERD when off PPI.” “Someone else wrote Nexium”
15
16
Colchicine DURHistorical Perspective
In June 2006, the FDA announced a new drug safety initiative to remove unapproved drugs from the market, including a final guidance entitled “Marketed Unapproved Drugs-Compliance Policy Guide (CPG)”. Notice that any illegally marketed product is subject to FDA
enforcement at any time Clarified that the FDA intends to use a risk-based approach
to enforcementJuly 29, 2009: Colcrys® approved for Familial
Mediterranean Fever (FMF)July 30, 2009: Colcrys® approved for Acute Gout FlaresOctober 16, 2009: Colcrys® approved for Chronic Gout

Colchicine DUR“Outraged Politicians Demand Gout Drug
Price Probe”Article written June 10, 2011 for Medscape
Medical News Colcrys® granted 3 years marketing exclusivity At time of approval, 21 companies were making oral
colchicine with costs as low as $0.04 per tablet. After approval Colcrys® raised the price to $5 per tablet.
2 US Senators and 3 US Representatives are charging the company with price gouging and are demanding an investigation.
Concerns that this may be a new model for drug companies.
17
18
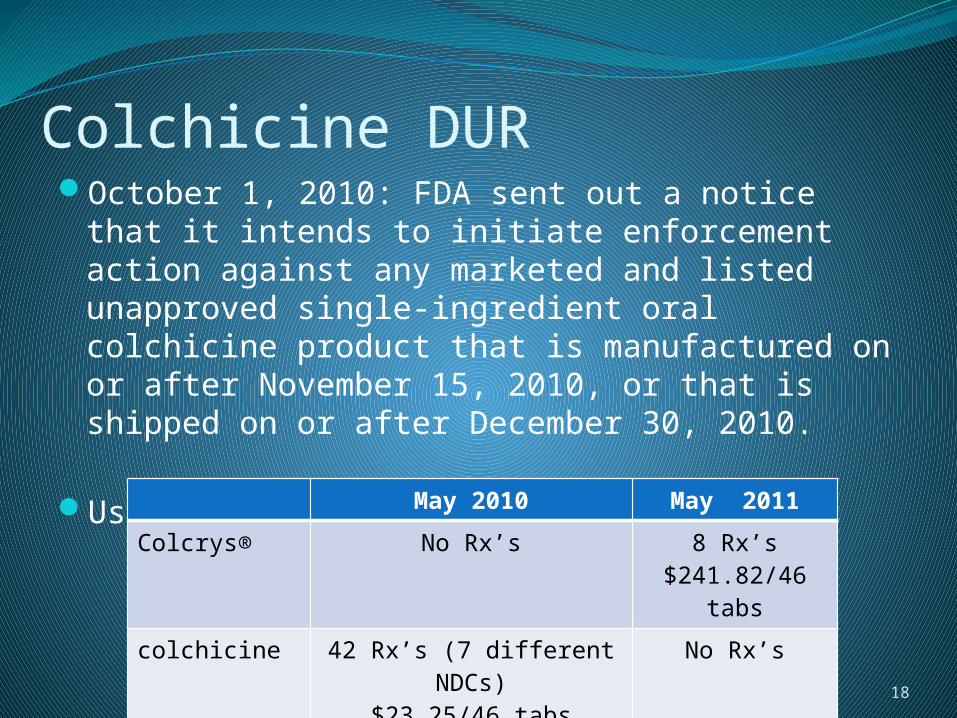
Colchicine DUROctober 1, 2010: FDA sent out a notice that it
intends to initiate enforcement action against any marketed and listed unapproved single-ingredient oral colchicine product that is manufactured on or after November 15, 2010, or that is shipped on or after December 30, 2010.
Use of Colcrys®May 2010 May 2011
Colcrys® No Rx’s 8 Rx’s$241.82/46
tabs
colchicine 42 Rx’s (7 different NDCs)
$23.25/46 tabs
No Rx’s
Colchicine DURCost Avoidance Calculations
34 less colchicine prescriptions per month
34 x $241.82 per Rx = $8221.88 per month
Total cost avoidance of $98,662.56 per year
19
Colchicine DUR
DefinitionsGout is defined as an inflammatory arthritis
induced by the deposition of monosodium urate crystals in synovial fluid and other tissues
Hyperuricemia is defined as a serum urate level ≥ 6.8mg/dl, which is the limit of urate solubility at physiologic temperature and pH
20

Colchicine DUREpidemiology of Gout
6.1 million adults in the USPrevalence increases with ageIncidence higher in men than women (3-4:1 overall)
although decreases at older ages (at least partially due to declining levels of estrogen which has uricosuric effects in women)
Risk Factors: thiazide diuretics, cyclosporine, low dose aspirin (<1000 mg/day), insulin resistance, metabolic syndrome, obesity, renal insufficiency, hypertension, congestive heart failure
Dietary Risk Factors: meat, seafood, ethanol, soft drinks
21
Colchicine DURAcute Gout Attack
Sudden onset of severe debilitating pain with progressive worsening over the first 24 hours
Erythema and swelling in a jointMost attacks resolve within 3-10 days
Management of Acute GoutNon-pharmacologic: joint rest and icing the
affected sitePharmacologic – NSAIDS, corticosteroids,
colchicine22
Colchicine DUR
Pharmacologic Treatment of Acute Gout AttackFirst line – NSAIDS, colchicineRelative efficacy of colchicine as compared
with NSAIDS is unknownIn head-to-head studies between various
NSAIDS, they had similar benefitsAlternative Agent – corticosteroids (all routes
including oral and intra-articular)
23
Colchicine DURTreatment of Acute Gout Attack – NSAIDS
Relative Contra-Indications: renal impairment, risk factors for GI bleeding, congestive heart failure, concomitant anticoagulant therapy
Commonly used agents: indomethacin, naproxen, sulindac
Dose: Start as soon as possible (within 12-24 hours of pain onset). High dose therapy for 2-3 days, then decrease dose. Continue for at least 48 hours after resolution of symptoms
24
Colchicine DURTreatment of Acute Gout Attack – Colcrys®
Dosage First Day – 1.2mg at first sign of gout flare, followed by 0.6mg
one hour later Subsequent Days – 0.6mg twice daily until flare subsides
(typically 3-10 days) For mild (CrCl 50-80ml/min) to moderate (CrCl 30-50ml/min)
renal impairment, no dosage adjustment is needed, but the patient should be monitored for adverse effects.
For severe (CrCl < 30ml/min) renal impairment, a treatment course should be repeated no more than once every 2 weeks. For patients with gout flares requiring repeated courses, consideration should be given to alternate therapy. For patients undergoing dialysis, the total recommended dose for the treatment of gout flares should be reduced to a single dose of 0.6mg (1 tablet).
25
Colchicine DUR
Treatment of Acute Gout Attack – CorticosteroidsCan be given orally, intravenously,
intramuscularly, intra-articularly e.g. prednisone 20mg daily until symptoms resolve,
generally within 5-7 days (taper not necessary after short-term treatment)
Monoarticular attacks are often managed with the use of intra-articular glucocorticoids.
26
Colchicine DURChronic Gout
Chronic tophaceous gout Polyarticular attacks Symptoms between attacks Crystal deposition (tophi) in soft tissues or joints
Who to treat? Patients with hyperuricemia who have at least two attacks per year
or tophi as determined by either clinical or radiographic methodsWhen to treat?
Wait 1-2 weeks after the acute attack has subsided to begin chronic treatment
Goal of therapy Uric Acid Level < 6mg/dl Some patients may require Uric Acid level < 5mg/dl for resolution
of tophi
27
Colchicine DURManagement of Chronic Gout – Allopurinol
Allopurinol is the drug of choice to lower serum uric acid
Mechanism of action Xanthine oxidase inhibitor which blocks the
synthesis of uric acidPrior Authorization is not neededDosage range is 100-800 mg daily (assess renal
function) Mild gout: 200-300 mg daily Moderate gout: 400-600 mg daily Severe gout: 700-800 mg daily
28
Colchicine DUR
Management of Chronic Gout – Allopurinol, con’t.Patient has not failed allopurinol therapy if
only on 300mg daily with normal renal function for severe gout
Allopurinol dosing in renal impairment: If CrCl 10-20ml/min, 200mg daily If CrCl 3-10ml/min, 100mg daily If CrCl <3ml/min, 100mg every other day
29
Colchicine DURManagement of Chronic Gout – Uloric®
Uloric requires prior authorizationMechanism of Action – also a xanthine oxidase inhibitorNo comparative studies done on efficacy between Uloric and
allopurinolCost Comparison to allopurinol
#30 allopurinol 300mg - $7.16 #30 Uloric® 80mg - $168.24
Therapeutic criteria for Uloric® Continuation of gout attacks after three months of allopurinol
therapy at a therapeutic dose (includes assessment of renal function)
Serum urate levels > 6mg/dl after three months of allopurinol therapy at a therapeutic dose
Documented intolerance or allergy to allopurinol
30
Colchicine DUR
Management of Chronic Gout – Colcrys®To prevent an acute attack as a result of
starting allopurinol, low dose NSAID (e.g. naproxen 250mg twice daily) or prophylactic Colcrys® can be used.
Duration of therapy: Without tophi, prophylaxis with Colcrys® for 6
months With tophi, optimal duration of therapy is unknown
31
Colchicine DUR
Management of Chronic Gout – Colcrys®, con’t.Dose: Colcrys® 0.6mg orally once or twice
daily For mild (CrCl 50-80ml/min) to moderate (CrCl 30-
50ml/min) renal impairment, no dosage adjustment is needed, but the patient should be monitored for adverse effects.
For severe (CrCl < 30ml/min) renal impairment, the starting doses should be 0.3mg per day and any increase in dose should be done with close monitoring. For the prophylaxis of gout flares in patients undergoing dialysis, the starting dose should be 0.3mg given twice a week with close monitoring.
32
Colchicine DURManagement of Chronic Gout – Probenecid
Mechanism of action – increases uric acid excretion by blocking urate reabsorption
Prior authorization is not neededManagement of Chronic Gout – Krystexxa®
Not covered by Idaho Medicaid outpatient prescription drug program
Pegylated urate oxidase enzyme – administered IV every 2 weeks by a healthcare professional due to the risk of infusion reactions and anaphylaxis.
Cost is $20,000 annually.
33

Colchicine DURPseudogout
Deposition of calcium pyrophosphate crystals in joints (rather than uric acid crystals).
Causes arthritis characterized by sudden, painful swelling in one or more joints, especially the knee.
Drug of choice – NSAIDsAlternate drug – colchicine (if cannot use NSAID)Other treatments
Joint aspiration Intra-articular corticosteroid Joint rest
34
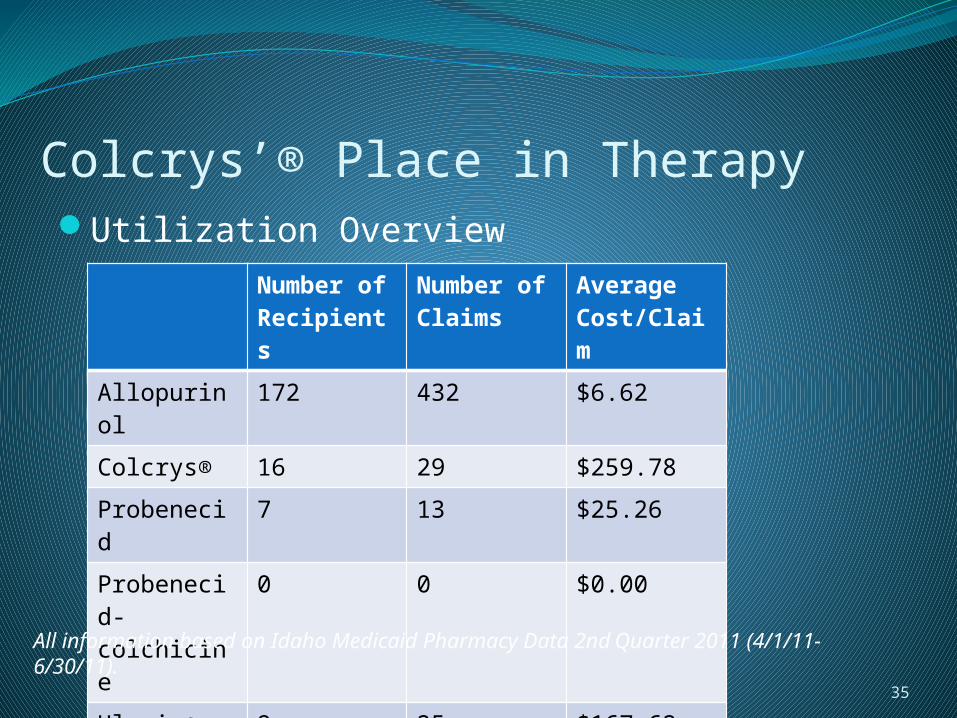
Utilization OverviewNumber of Recipients
Number of Claims
Average Cost/Claim
Allopurinol 172 432 $6.62
Colcrys® 16 29 $259.78
Probenecid 7 13 $25.26
Probenecid-colchicine
0 0 $0.00
Uloric® 9 25 $167.62
Colcrys’® Place in Therapy
35
All information based on Idaho Medicaid Pharmacy Data 2nd Quarter 2011 (4/1/11-6/30/11).
Colchicine DUR
Colcrys®Patients were selected for evaluation if there
was a paid claim for Colcrys® over the six month period 11/1/2010-4/30/2011. A total of 21 patient profiles were evaluated.
2 additional profiles were reviewed which had denied PA requests for Colcrys®, but no paid claims.
36
37
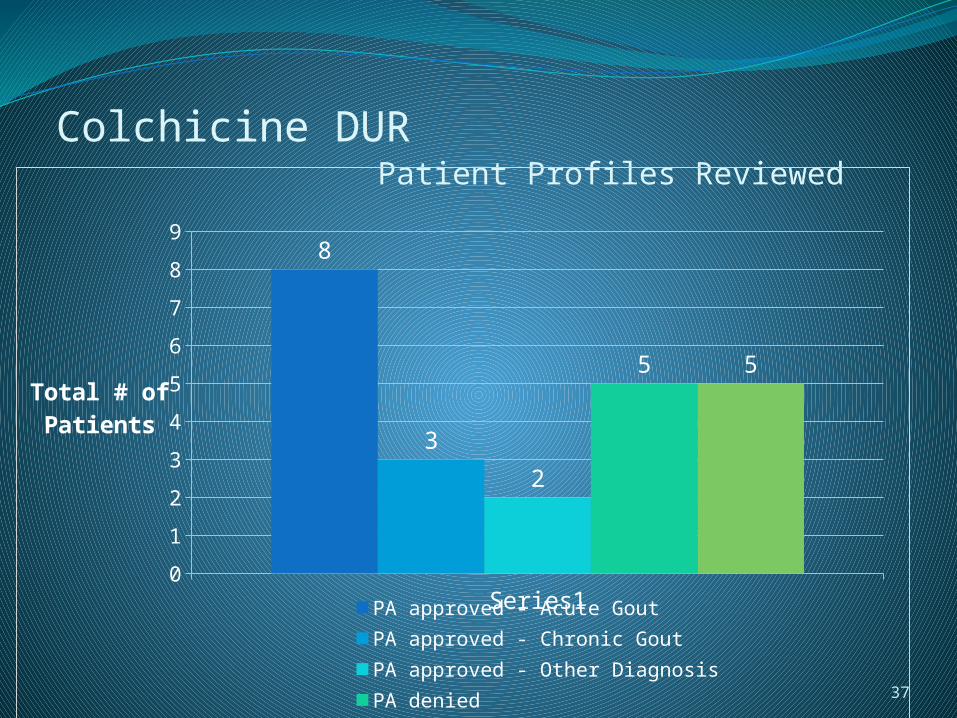
Colchicine DUR Patient Profiles Reviewed
Series10
1
2
3
4
5
6
7
8
98
3
2
5 5
PA approved - Acute Gout PA approved - Chronic Gout
PA approved - Other Diagnosis PA denied
No PA submitted
Total # ofPatients

Colchicine DURColcrys®
Prior Authorization approved for 8 patients with acute gout (*one patient failed both NSAID & corticosteroid)
38
Series10
0.51
1.52
2.53
3.54
4.54
2 2
1
Failed NSAID*
NSAID contra-in-dicated
Failed corti-costeroid*
Acute attack while on allopurinol
Total # of Patients
Colchicine DURColcrys®
3 Prior Authorizations approved for Chronic Gout Patients were already on allopurinol
2 Prior Authorization approved for other Diagnosis 1 : vasculitis (approved for 3 month trial) 1 : Familial Mediterranean Fever (patient has been
on colchicine for years)
39
Colchicine DURColcrys®
5 Prior Authorizations Denied 3 patients with paid Colcrys® claims previously
(Colcrys® would pay if there was a previous paid claim for colchicine in the past 90 days. This AutoPA rule has since been removed.) 2 patients with paid Colcrys® claims had chronic
constipation 1 patient has been on generic colchicine since
2005 1 patient has been on generic colchicine since
2008 (please refer to profile #16 in packet for further review)
1 patient had diagnosis of pseudogout on prior authorization form, but no other information was provided by the prescriber.
40
Colchicine DUR
Colcrys®5 Prior Authorizations Denied (con’t.)
2 patients had no paid Colcrys® claims 1 patient had “possible gout” with uric acid level of
6.6 mg/dl and no contraindications to NSAIDS/corticosteroids
1 patient was subsequently approved the following day when the prescriber phoned into the call center with additional information.
41
Colchicine DURColcrys®
5 patients had at least one paid Colcrys® claim, but a Prior Authorization request was never submitted 3 patients have no paid claims for any other gout
medications (NSAIDs, corticosteroids, allopurinol) Assumption would be off-label use
2 patients also on allopurinol Assumption would be gout diagnosis
42
43
Colcrys® - Summary72.2% (13/18) of the Prior Authorization
requests received were approved.Continue to require Prior Authorization for
Colcrys® with the current therapeutic criteria (listed on next slide)
Off-label use for treatment of chronic constipation was discovered
Turned off Auto Pay rule which approved Colcrys® at point of sale if there was a paid colchicine claim in the past 90 days.

44
Therapeutic Criteria for Colcrys®
1. Acute Gout• Contra-indication and/or failure to NSAIDS or
corticosteroids
2. Chronic Gout• Adjunct to allopurinol AND contra-indication
or failure to NSAIDS
Colchicine DURReferences
Neogi, T. NEJM 2011;364(5):443-452. Management of Gout. Pharmacist’s Letter/Prescriber’s Letter November
2010, Volume 26, Number 261102. Kelly, J. (2011, June 10). Outraged Politicians Demand Gout Drug Price
Probe. Retrieved from http://www.medscape.com/viewarticle/744408 Federal Register/ Vol.75, No. 190/ Friday, October 1, 2010/
Notices:60768-60771. http://fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm227796
.htm http://www.fda.gov/Drugs/GuidanceComplianceRegulatoryInformation/E
nforcementActivitiesbyFDA/SelectedEnforcementActionsonUnapprovedDrugs/ucm118990.htm
45
Ketorolac DURHistorical Perspective:
Discovered that in the drug profiles the Maximum Quantity was set at 10 tablets per day.
The Maximum Quantity was immediately changed to 4 tablets per day as recommended by the package insert.
Report was generated to see how many patients have actually received doses higher than the recommended amount and based on this report it was felt that a Retrospective DUR would be appropriate.
46
Ketorolac DURBlack Box Warnings:
WARNING TORADOL ORAL (ketorolac tromethamine), a nonsteroidal anti-inflammatory
drug (NSAID), is indicated for the short-term (up to 5 days in adults) management of moderately severe acute pain that requires analgesia at the opioid level and only as continuation treatment following IV or IM dosing of ketorolac tromethamine, if necessary. The total combined duration of use of TORADOL ORAL and ketorolac tromethamine should not exceed 5 days.
TORADOL ORAL is not indicated for use in pediatric patients and it is NOT indicated for minor or chronic painful conditions. Increasing the dose of TORADOL ORAL beyond a daily maximum of 40 mg in adults will not provide better efficacy but will increase the risk of developing serious adverse events.
GASTROINTESTINAL RISK Ketorolac tromethamine, including TORADOL, can cause peptic ulcers,
gastrointestinal bleeding and/or perforation of the stomach or intestines, which can be fatal. These events can occur at any time during use and without warning symptoms. Therefore, TORADOL is CONTRAINDICATED in patients with active peptic ulcer disease, in patients with recent gastrointestinal bleeding or perforation, and in patients with a history of peptic ulcer disease or gastrointestinal bleeding. Elderly patients are at greater risk for serious gastrointestinal events.
47

Ketorolac DURBlack Box Warnings con’t.
CARDIOVASCULAR RISK NSAIDs may cause an increased risk of serious cardiovascular thrombotic
events, myocardial infarction, and stroke, which can be fatal. This risk may increase with duration of use. Patients with cardiovascular disease or risk factors for cardiovascular disease may be at greater risk.
TORADOL is CONTRAINDICATED for the treatment of peri-operative pain in the setting of coronary artery bypass graft (CABG) surgery.
RENAL RISK TORADOL is CONTRAINDICATED in patients with advanced renal impairment
and in patients at risk for renal failure due to volume depletion. RISK OF BLEEDING
TORADOL inhibits platelet function and is, therefore, CONTRAINDICATED in patients with suspected or confirmed cerebrovascular bleeding, patients with hemorrhagic diathesis, incomplete hemostasis and those at high risk of bleeding.
TORADOL is CONTRAINDICATED as prophylactic analgesic before any major surgery.
48
Ketorolac DURBlack Box Warnings con’t.
RISK DURING LABOR AND DELIVERY The use of TORADOL in labor and delivery is contraindicated because it may
adversely affect fetal circulation and inhibit uterine contractions. The use of TORADOL is contraindicated in nursing mothers because of the potential adverse effects of prostaglandin-inhibiting drugs on neonates.
CONCOMITANT USE WITH NSAIDS TORADOL is CONTRAINDICATED in patients currently receiving aspirin or
NSAIDs because of the cumulative risk of inducing serious NSAID-related side effects.
SPECIAL POPULATIONS Dosage should be adjusted for patients 65 years or older, for patients under
50 kg (110 lbs) of body weight and for patients with moderately elevated serum creatinine.
http://dailymed.nlm.nih.gov/dailymed/lookup.cfm?setid=c0336606-7366-41ce-9cef-aa6524b92b11
49

Ketorolac DUR
Patients were selected for evaluation if there was a paid claim for ketorolac > 40mg total daily dose over the 3 month period 3/1/2011-5/31/2011.
A total of 29 patient profiles were evaluatedLetters were sent to 9 prescribers about 9
patients on 6/20/2011.As of 7/7/2011, 3 responses have been
received (33% response rate)
50
Ketorolac DURCriteria Paragraph
During a retrospective drug utilization review, it was noted that your patient, (Patient Name), received at least one prescription of more than 20 tablets and/or received multiple consecutive fills of ketorolac. The recommended maximum daily dose of oral ketorolac is 40mg per day (10mg tablet four times daily). Ketorolac is FDA approved for the short term (up to 5 days) management of moderately severe acute pain that requires analgesia at the opioid level and only as continuation treatment following IV or IM dosing of ketorolac. The total combined duration of use of injectable and oral ketorolac should not exceed 5 days. Increasing the dose beyond the recommended daily maximum of 40mg will not provide better efficacy, but will increase the risk of developing serious adverse events. Ketorolac has black box warnings addressing the following risks: Gastrointestinal, Cardiovascular, Renal, Risk of Bleeding, Risk During Labor and Delivery, Concomitant Use with NSAIDs, and in Special Populations.
51
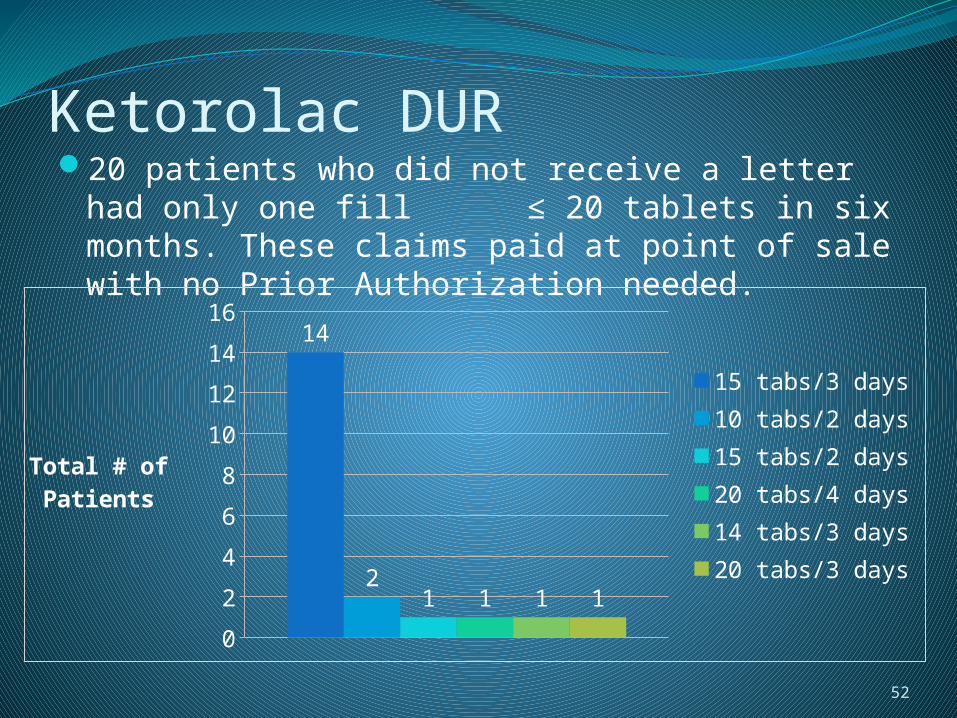
Ketorolac DUR20 patients who did not receive a letter had only
one fill ≤ 20 tablets in six months. These claims paid at point of sale with no Prior Authorization needed.
52
0
2
4
6
8
10
12
14
1614
21 1 1 1
15 tabs/3 days10 tabs/2 days15 tabs/2 days20 tabs/4 days14 tabs/3 days20 tabs/3 days
Total # of Patients
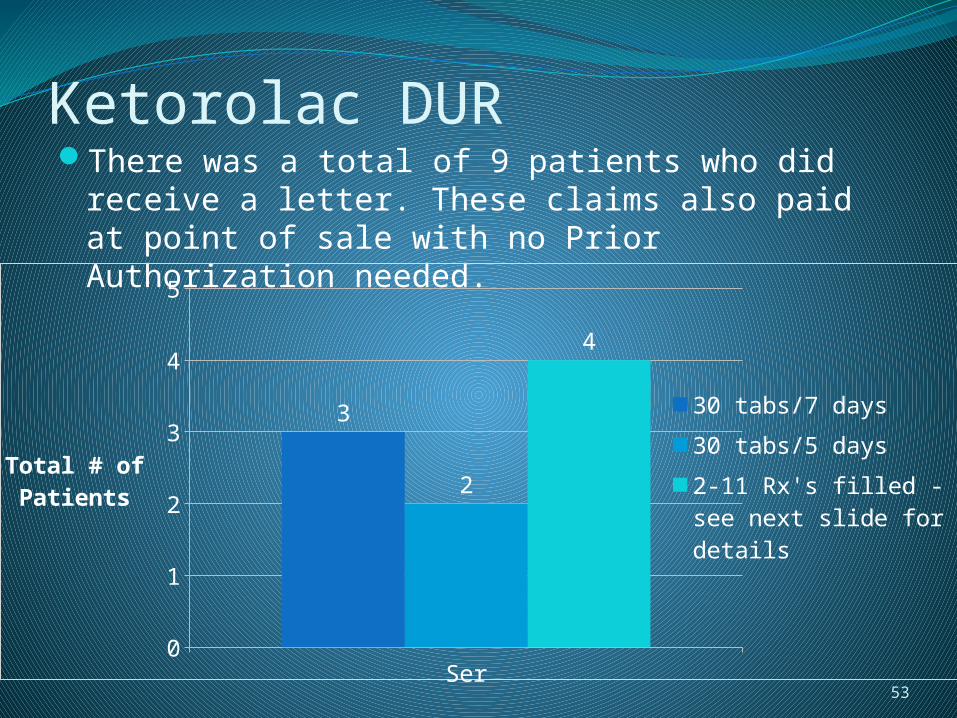
Ketorolac DURThere was a total of 9 patients who did receive a
letter. These claims also paid at point of sale with no Prior Authorization needed.
53Series1
0
1
2
3
4
5
3
2
4
30 tabs/7 days
30 tabs/5 days
2-11 Rx's filled - see next slide for details
Total # of Patients
Ketorolac DURBreakdown of 4 patients with multiple fills:
Patient 1 – 30 tabs/5 days (Dec 6, Dec 20, Feb 13, & Apr 16)
Patient 2 – 30 tabs/7 days (Dec 10, Feb 28, & May 11)
Patient 3 – 40 tabs/20 days (Feb 23) & 15 tabs/3 days (Apr 22)
Patient 4 – 11 fills of 15 tabs/3 days (Jan 12, Feb 10, Feb 25, Mar 6, Mar 15, Mar 29, Apr 6, Apr 11, Apr 22, May 5, & May 11) Please refer to patient’s profile in packet for
detailed profile54
Ketorolac DURResponse detail as of 7/7/2011Note that providers may choose more than one selection
per response. Information clinically useful: plan to monitor
1 I will use this information for care of future patients.
1No longer my patient
1My patient, but I did not prescribe this
1My patient, but I have not seen him/her recently
1Somewhat useful to my practice
1
“The meds were being given in the ER and PCP I believe”
55
Ketorolac DUR - SummaryMaximum quantity per day reduced from 10
to 4 tablets on 5/24/2011
DUR letter sent on 6/20/2011 to 9 prescribers with 3 responses as of 7/7/2011
56
Tramadol with SSRIs or SNRIsPotential for Serotonin SyndromePharmacy Provider Profiling
Profiles are being generated and are currently in the process of being sent out along with the Serotonin Syndrome Handout.
New Response form created to be more relevant to Pharmacists. (Please see form in Packet as well as new prescriber response form).
57
Proposed Studies for Next Quarter:Analysis of Auto Refill PracticeAtypical Antipsychotics: Impact of P&T
RecommendationsHigh Dose Utilization through multiple strengths
of selected medicationAtypical AntipyschoticsFocalin XR®
Injectable Atypical AntipsychoticsP&T Committee Narcotic Analgesic Studies
Further discussed in following slides
58
Proposed Studies for Next Quarter:Synagis 2010-2011 Season
Update on the impact of using the 2009 revised American Academy of Pediatrics (AAP) recommendations for infants with gestational age between 32 to 35 weeks.
RibavirinOnly FDA approved for treatment of hepatitis C
with concomitant interferon.Leukotrienes vs. inhaled corticosteroids in
children with asthma
59
Auto Refill PracticesSome pharmacies are instituting Auto Refill
policies which allow them to automatically dispense refills based on days since last fill
IssuesPotential for stockpilingPotential for continued fill of discontinued
medicationsIncrease cost/waste
Please see Survey in Packet
60
Auto Refill Practices
Fax blast of survey went out to 318 pharmacies on July 8, 2011.
As of 7/11/2011 a total of 48 surveys have been returned (15% response rate)
61
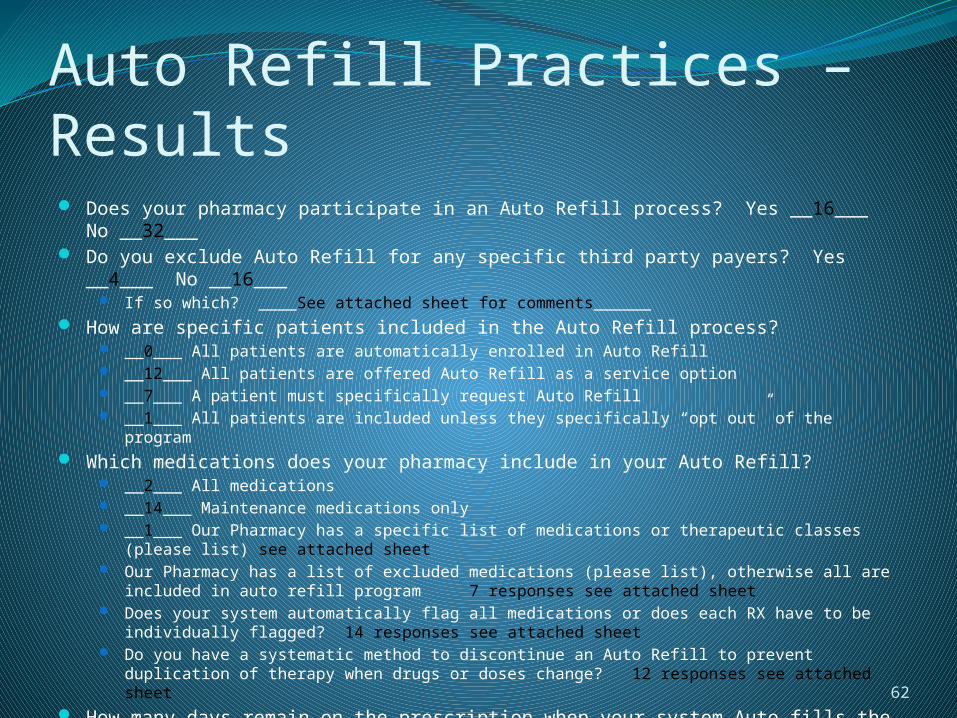
Auto Refill Practices – Results Does your pharmacy participate in an Auto Refill process? Yes __16___ No __32___ Do you exclude Auto Refill for any specific third party payers? Yes __4___ No __16___
If so which? ____See attached sheet for comments______ How are specific patients included in the Auto Refill process?
__0___ All patients are automatically enrolled in Auto Refill __12___ All patients are offered Auto Refill as a service option __7___ A patient must specifically request Auto Refill __1___ All patients are included unless they specifically “opt out” of the program
Which medications does your pharmacy include in your Auto Refill? __2___ All medications __14___ Maintenance medications only __1___ Our Pharmacy has a specific list of medications or therapeutic classes (please list) see
attached sheet Our Pharmacy has a list of excluded medications (please list), otherwise all are included in
auto refill program 7 responses see attached sheet Does your system automatically flag all medications or does each RX have to be individually
flagged? 14 responses see attached sheet Do you have a systematic method to discontinue an Auto Refill to prevent duplication of
therapy when drugs or doses change? 12 responses see attached sheet How many days remain on the prescription when your system Auto fills the
medication? 12 responses average 5 days
62
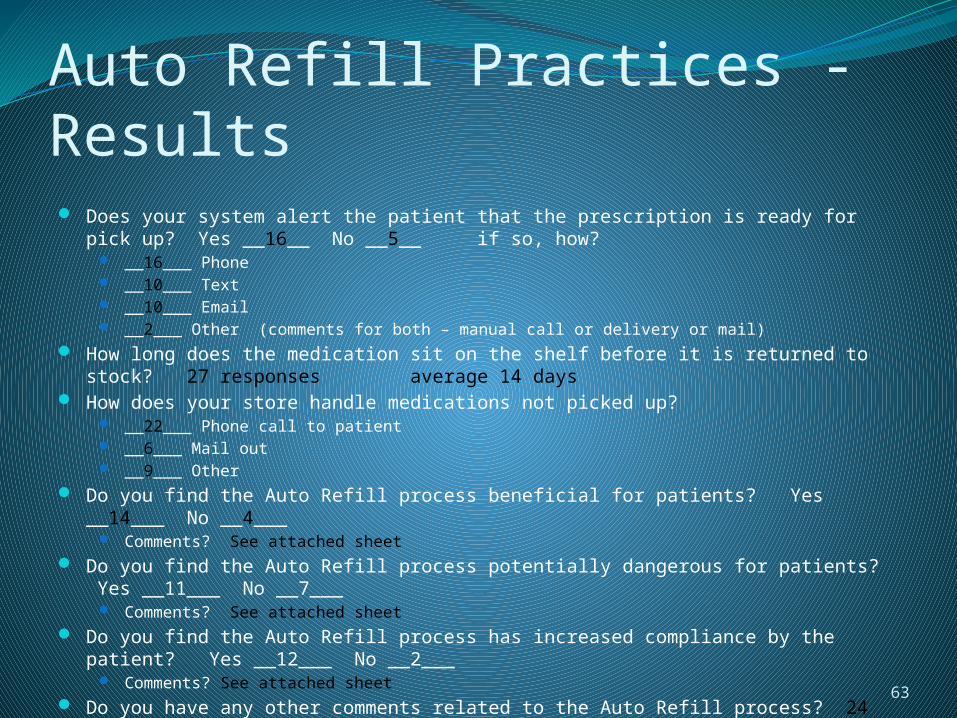
Auto Refill Practices - Results Does your system alert the patient that the prescription is ready for pick up? Yes
__16__ No __5__ if so, how? __16___ Phone __10___ Text __10___ Email __2___ Other (comments for both – manual call or delivery or mail)
How long does the medication sit on the shelf before it is returned to stock? 27 responses average 14 days
How does your store handle medications not picked up? __22___ Phone call to patient __6___ Mail out __9___ Other
Do you find the Auto Refill process beneficial for patients? Yes __14___ No __4___ Comments? See attached sheet
Do you find the Auto Refill process potentially dangerous for patients? Yes __11___ No __7___
Comments? See attached sheet Do you find the Auto Refill process has increased compliance by the patient? Yes
__12___ No __2___ Comments? See attached sheet
Do you have any other comments related to the Auto Refill process? 24 responses see attached sheet
63
Atypical AntipsychoticsP&T RecommendationsApproved for diagnosis per FDA indications or off-label
indications with supporting evidence-based literature.All patients receiving at least 90 days of therapy for the
past 120 days as of implementation date will be grandfathered. No criteria for diagnosis required.
No PDL requirements for patients with schizophrenia and related psychosis.
Bipolar, major depression adjunctive, autism and other designated acceptable diagnoses will require failure of a preferred agent for designated non-preferred agents.
Age, dose and quantity per labeling information on all drugs.
If the medical diagnosis and required drug history have been submitted as prior claims then the prescription will
auto-approve at point of sale. i.e. No written PA required. 64
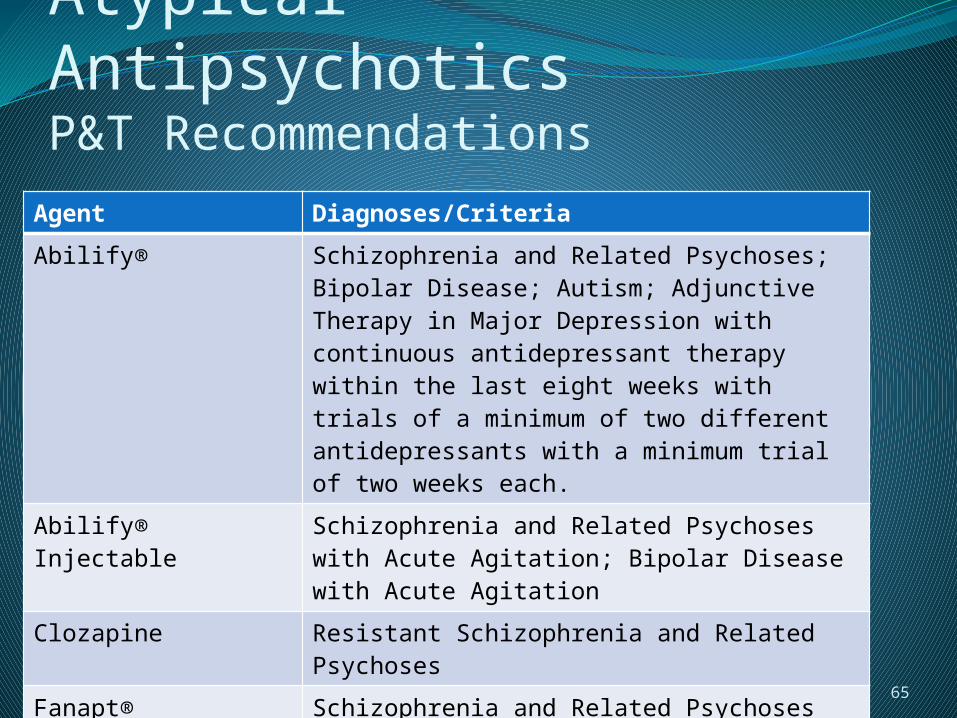
Atypical AntipsychoticsP&T Recommendations
Agent Diagnoses/Criteria
Abilify® Schizophrenia and Related Psychoses; Bipolar Disease; Autism; Adjunctive Therapy in Major Depression with continuous antidepressant therapy within the last eight weeks with trials of a minimum of two different antidepressants with a minimum trial of two weeks each.
Abilify® Injectable Schizophrenia and Related Psychoses with Acute Agitation; Bipolar Disease with Acute Agitation
Clozapine Resistant Schizophrenia and Related Psychoses
Fanapt® Schizophrenia and Related Psychoses
Geodon® Schizophrenia and Related Psychoses; Bipolar Disease – Mania and Mixed State
Geodon® Injectable Schizophrenia and Related Psychoses with Acute Agitation
65

Atypical AntipsychoticsP&T Recommendations (continued)
Adherence RatesAgent Diagnoses/Criteria
Invega® Schizophrenia and Related Psychoses
Invega Sustenna® Schizophrenia and Related Psychoses ANDHistory of Oral Invega® or Risperidone within the past 2 years ANDFailure of Risperdal Consta®
Risperidone Schizophrenia and Related Psychoses; Bipolar Disease – Mania and Mixed State; Autism; Disruptive Behavioral Disorders; Obsessive Compulsive Disorder*Brand name will deny for brand/generic rule
Risperdal Consta® Schizophrenia and Related Psychoses
Saphris® Schizophrenia and Related Psychoses; Bipolar Disease – Mania and Mixed State
66
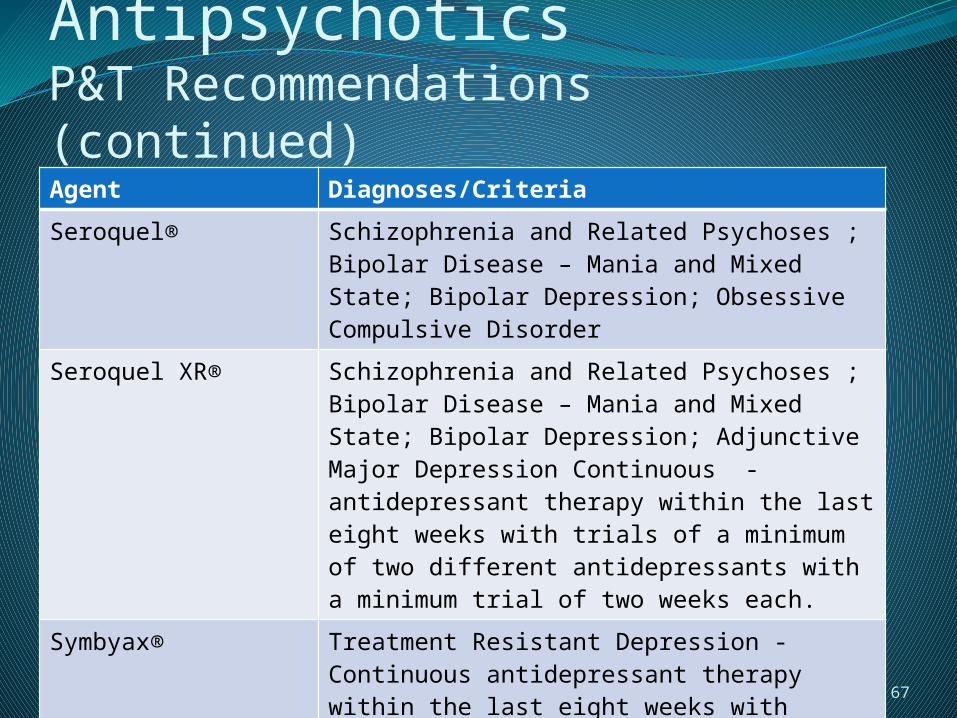
Atypical AntipsychoticsP&T Recommendations (continued)
Adherence RatesAgent Diagnoses/Criteria
Seroquel® Schizophrenia and Related Psychoses ; Bipolar Disease – Mania and Mixed State; Bipolar Depression; Obsessive Compulsive Disorder
Seroquel XR® Schizophrenia and Related Psychoses ; Bipolar Disease – Mania and Mixed State; Bipolar Depression; Adjunctive Major Depression Continuous - antidepressant therapy within the last eight weeks with trials of a minimum of two different antidepressants with a minimum trial of two weeks each.
Symbyax® Treatment Resistant Depression - Continuous antidepressant therapy within the last eight weeks with trials of a minimum of two different antidepressants with a minimum trial of two weeks each. 67
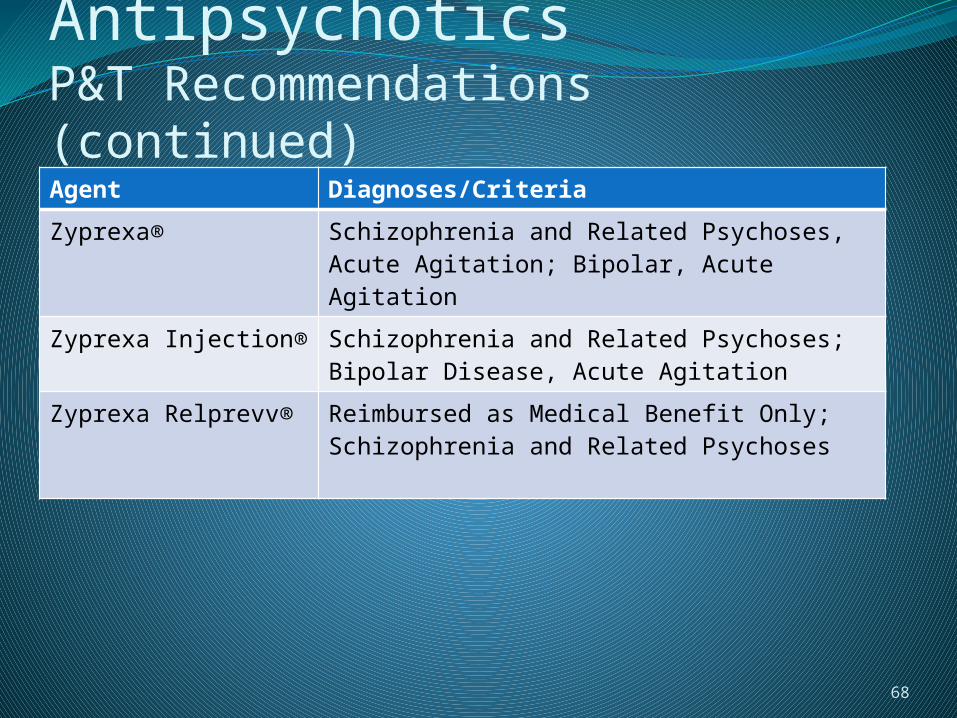
Atypical AntipsychoticsP&T Recommendations (continued)
Adherence RatesAgent Diagnoses/Criteria
Zyprexa® Schizophrenia and Related Psychoses, Acute Agitation; Bipolar, Acute Agitation
Zyprexa Injection® Schizophrenia and Related Psychoses; Bipolar Disease, Acute Agitation
Zyprexa Relprevv® Reimbursed as Medical Benefit Only; Schizophrenia and Related Psychoses
68
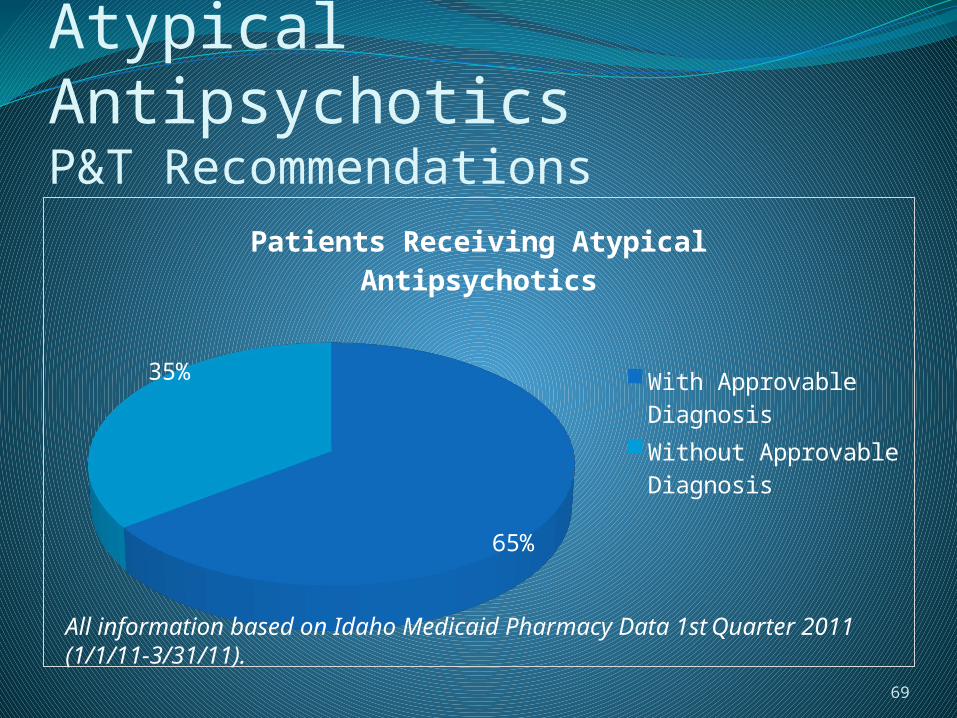
Atypical AntipsychoticsP&T Recommendations
65%
35%
Patients Receiving Atypical An-tipsychotics
With Approvable DiagnosisWithout Approvable Diagnosis
69
All information based on Idaho Medicaid Pharmacy Data 1st Quarter 2011 (1/1/11-3/31/11).
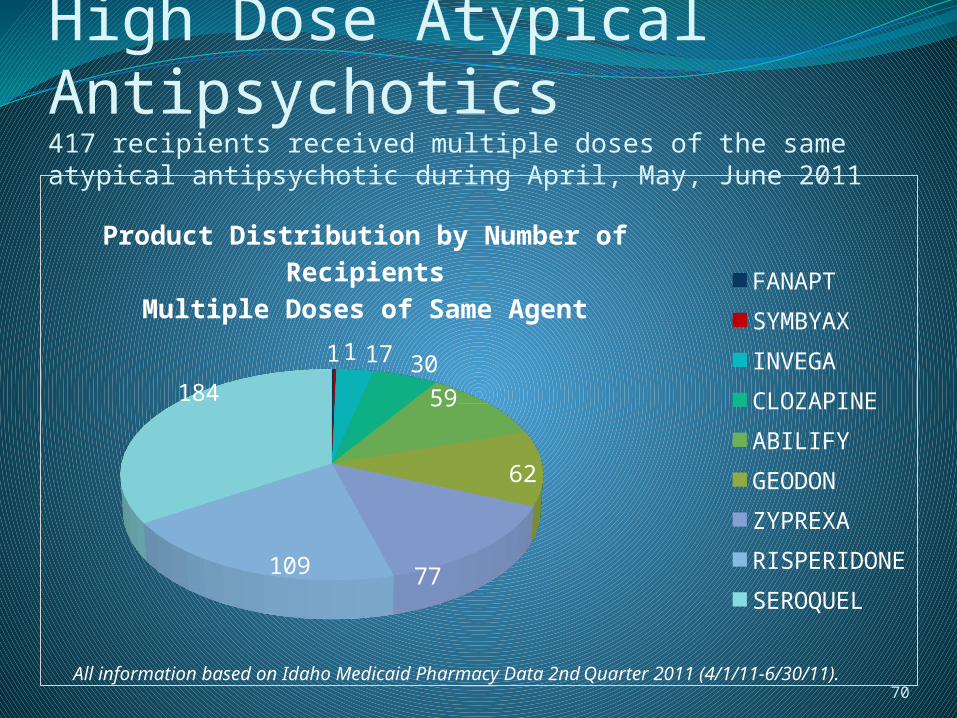
High Dose Atypical Antipsychotics417 recipients received multiple doses of the same atypical antipsychotic during April, May, June 2011
11 17 3059
62
77109
184
Product Distribution by Number of RecipientsMultiple Doses of Same Agent
FANAPT
SYMBYAX
INVEGA
CLOZAPINE
ABILIFY
GEODON
ZYPREXA
RISPERIDONE
SEROQUEL
70All information based on Idaho Medicaid Pharmacy Data 2nd Quarter 2011 (4/1/11-6/30/11).
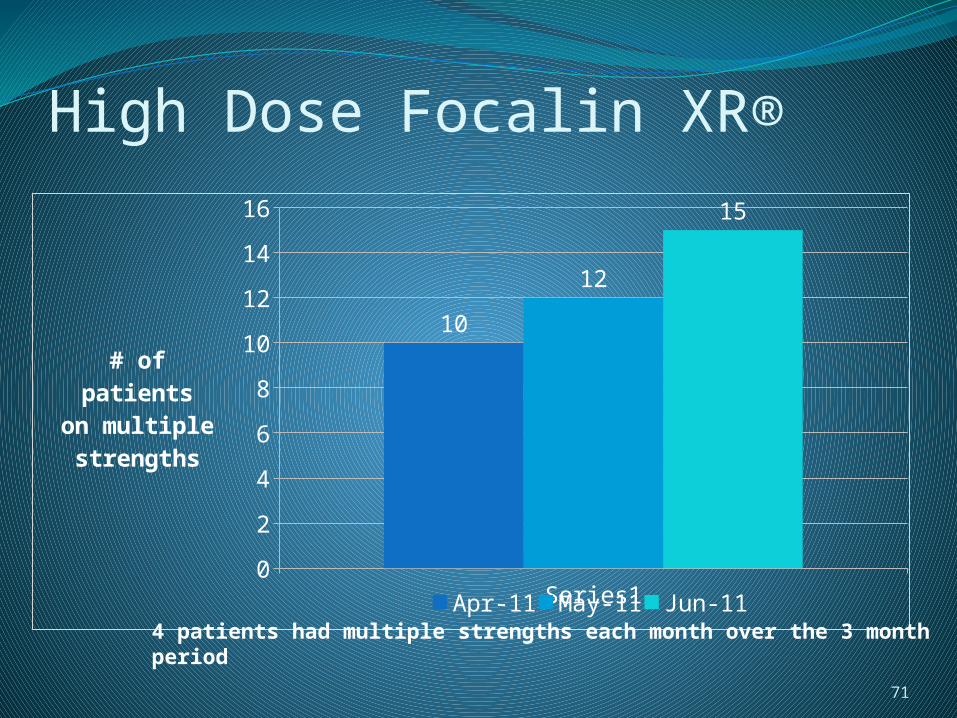
High Dose Focalin XR®
Series10
2
4
6
8
10
12
14
16
10
12
15
Apr-11 May-11 Jun-11
# of pa-tients
on multiplestrengths
71
4 patients had multiple strengths each month over the 3 month period
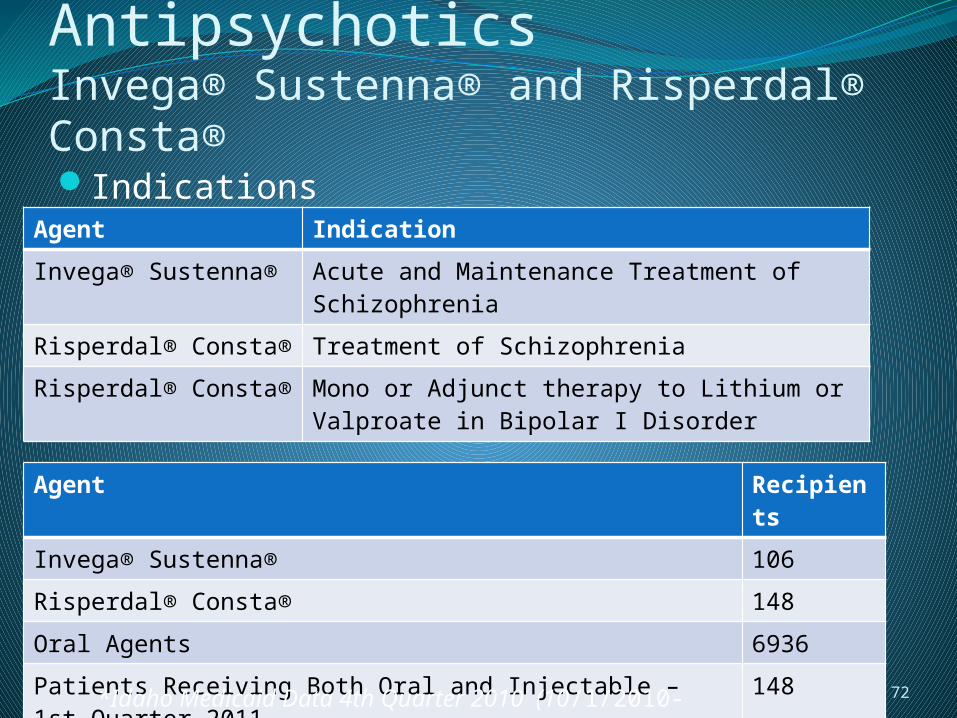
Injectable Atypical AntipsychoticsInvega® Sustenna® and Risperdal® Consta®Indications
Utilization Overview
Agent Indication
Invega® Sustenna® Acute and Maintenance Treatment of Schizophrenia
Risperdal® Consta® Treatment of Schizophrenia
Risperdal® Consta® Mono or Adjunct therapy to Lithium or Valproate in Bipolar I Disorder
Agent Recipients
Invega® Sustenna® 106
Risperdal® Consta® 148
Oral Agents 6936
Patients Receiving Both Oral and Injectable – 1st Quarter 2011
148
*Idaho Medicaid Data 4th Quarter 2010 (10/1/2010-12/31/2010)
72
Injectable Atypical AntipsychoticsInvega® Sustenna® and Risperdal® Consta®Responsibilities of the parties involved
Magellan Run reports to identify Prescribers, Pharmacies,
and PatientsIdaho Medicaid Pharmacy Unit
Analyze reports and identify where intervention is needed
Idaho Medicaid Program Integrity Send out letters requesting documentation of dose
administration
73

P&T Committee Narcotic Analgesic StudiesCommittee Recommendation for Drug
Utilization Review of Narcotic Analgesics The Committee recommended a comprehensive drug
utilization review of short and long-acting narcotics. This was based on concern over the misuse/abuse of these agents that is not addressed through the preferred drug list. Components of the proposed review are outlined below.
Patient ProfilingNumber of patients on monthly (chronic) narcoticsNumber of different agents used by individual
patients Total (cumulative) monthly doses of all concurrent
narcoticsNumber of prescribers per patientAnalysis of multiple scripts from multiple providers
74
P&T Committee Narcotic Analgesic StudiesPatient Profiling Continued
Other addictive drugs prescribed concurrentlyDiagnosis/indication for narcotic use and data
backing that diagnosisPatients with no relevant diagnosis for medicationEvaluation for evidence of illicit drug useRelationships of long-acting narcotic use and
breakthrough narcotics use (lack of long acting and/or breakthrough narcotics given continuously)
Hospital and ER admissions for overdosePrescription fill history, including early refills
75
P&T Committee Narcotic Analgesic StudiesProvider Profiling
Prescribing pattern for non-pain clinic prescribers
They also suggested utilizing several data sources outside Medicaid including outlier reports from the Board of Pharmacy Prescription Drug Monitoring Program, legal/arrest databases and hospital discharge medication records.
76
P&T Committee Narcotic Analgesic Studies
Possible policy changes suggested for consideration after collection and analysis of the data Restriction of prescriptions to prescribers and
pharmacies within Idaho state borders Stricter refill policies (90% rather than current 75%
threshold) Expansion of lock-in program
77
P&T Committee Narcotic Analgesic StudiesDUR Board Suggestions
Propose doing one study per quarter?
What studies would be most beneficial?
What studies would be feasible?
Recommendations?
78
Synagis Utilization Intervention
Update using the 2010-2011 RSV season data on the impact of using the 2009 revised American Academy of Pediatrics (AAP) recommendations for infants with gestational age between 32 to 35 weeks.
Profiles will be reviewed to assess outcomes

RibavirinGeneric ribavirin vs. Ribapak®
Review patient profiles to determine if patients have a diagnosis of hepatitis C and are concomitantly on interferon.
80
Prospective DUR ReportHistory Errors:
• DD – drug-to-drug• PG – drug to pregnancy• TD – therapeutic
duplication• ER – early refill• MC – drug-to-disease
Non-History Errors:• PA – drug-to-age• HD – high dose• LD – low dose• SX – drug-to-gender
81
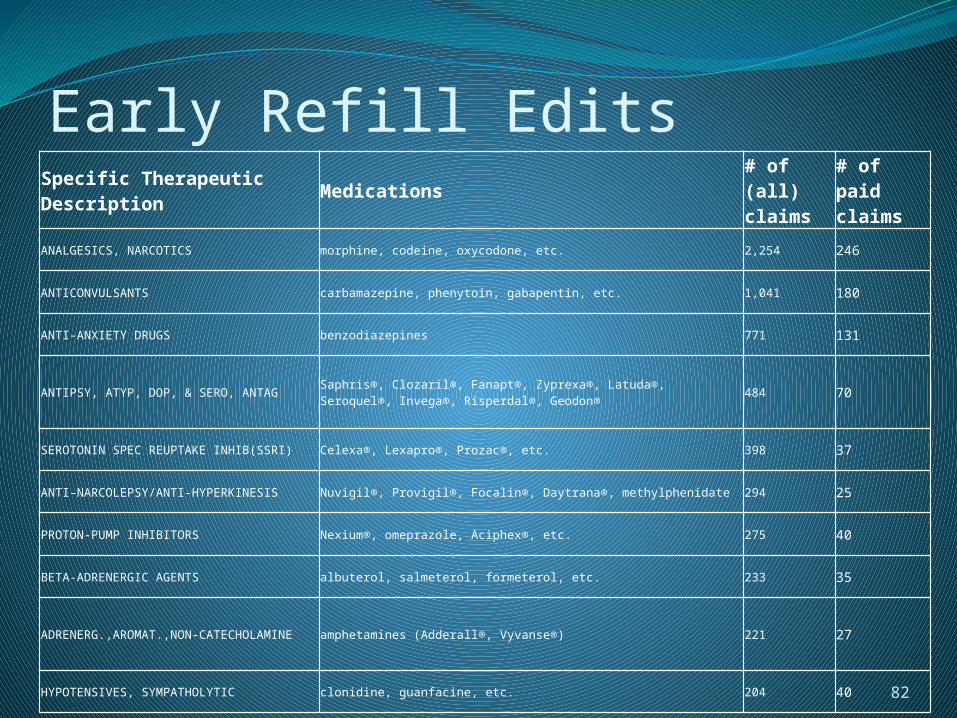
Early Refill EditsSpecific Therapeutic Description
Medications# of (all) claims
# of paid claims
ANALGESICS, NARCOTICS morphine, codeine, oxycodone, etc. 2,254 246
ANTICONVULSANTS carbamazepine, phenytoin, gabapentin, etc. 1,041 180
ANTI-ANXIETY DRUGS benzodiazepines 771 131
ANTIPSY, ATYP, DOP, & SERO, ANTAGSaphris®, Clozaril®, Fanapt®, Zyprexa®, Latuda®, Seroquel®, Invega®, Risperdal®, Geodon®
484 70
SEROTONIN SPEC REUPTAKE INHIB(SSRI) Celexa®, Lexapro®, Prozac®, etc. 398 37
ANTI-NARCOLEPSY/ANTI-HYPERKINESIS Nuvigil®, Provigil®, Focalin®, Daytrana®, methylphenidate 294 25
PROTON-PUMP INHIBITORS Nexium®, omeprazole, Aciphex®, etc. 275 40
BETA-ADRENERGIC AGENTS albuterol, salmeterol, formeterol, etc. 233 35
ADRENERG.,AROMAT.,NON-CATECHOLAMINE amphetamines (Adderall®, Vyvanse®) 221 27
HYPOTENSIVES, SYMPATHOLYTIC clonidine, guanfacine, etc. 204 40
82
DUR Summer NewsletterCopy of Spring Newsletter in packetBrainstorm for new topics
83

Medicaid Update
84