220-dyslipidemia all clogged up - cdn.ymaws.com · ï l í l î ì í õ ð 27+(5 9$6&8/$5...
TRANSCRIPT

3/1/2019
1
ALL CLOGGED UP:DYSLIPIDEMIAS
PRESENTED BY:
KATHY J NOYES, DNP, APRN, FNP-BC, ACNP-BC
HEALTHCARE EDUCATIONAL RESOURCES AND SEMINARS, LLC
NO DISCLOSURES
OBJECTIVES:
• Compare and contrast the different types of dyslipidemias
• Summarize current lipid management guidelines
• Examine specific pharmacologic and non-pharmacologic strategies
for the treatment of patients with various dyslipidemias
DYSLIPIDEMIA: DEFINITION
• American College of Cardiology
• American Heart Association
• National Heart, Lung and Blood Institute
• “ a disorder of lipoprotein metabolism, including lipoprotein overproduction or deficiency. Dyslipidemias may be manifested by elevation of the total cholesterol, the “bad” low density lipoprotein (LDL), and the triglyceride concentrations, AND a decrease in the “good” high-density lipoprotein (HDL) concentrations”
Adult Treatment Panel IV
HYPERLIPIDEMIA: EXCESSIVE AMOUNTS OF LIPIDS IN CIRCULATION
• First thought to be related to atherosclerosis when found in ASHD plagues in 1930’s
• Initial recognition that Hyperlipidemia was a risk factor for CAD began with the Framingham Study in 1979.
• Summary of the Second Report of the National cholesterol Education Program II (NCEP II) Expert Panel on Detection, Evaluation and Treatment of High Cholesterol in Adults. JAMA. 1993.
• Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults: Executive Summary of the Third Report of the National cholesterol Education Program III (NCEP III) . JAMA 2001.
TYPES OF DYSLIPIDEMIAS
• Primary Hyperlipidemia: are all genetically predisposed including:
• Familial Hyperlipidemia: is caused by a mutations of the LDL receptor gene
that prevents the binding and internalization of LDL.
• FH is an autosomal co-dominate disorder whereby homozygotes have
severe hyperlipidemia
• Characterized by elevated LDL, normal triglycerides and FH of premature
CAD
• Tendon Xanthomas (thickening and irregularity of Achilles tendon) and/of
of digit extensor tendons of the metacarpophalangeal joints is diagnostic
of FH
1 2
3 4
5 6
3/1/2019
2
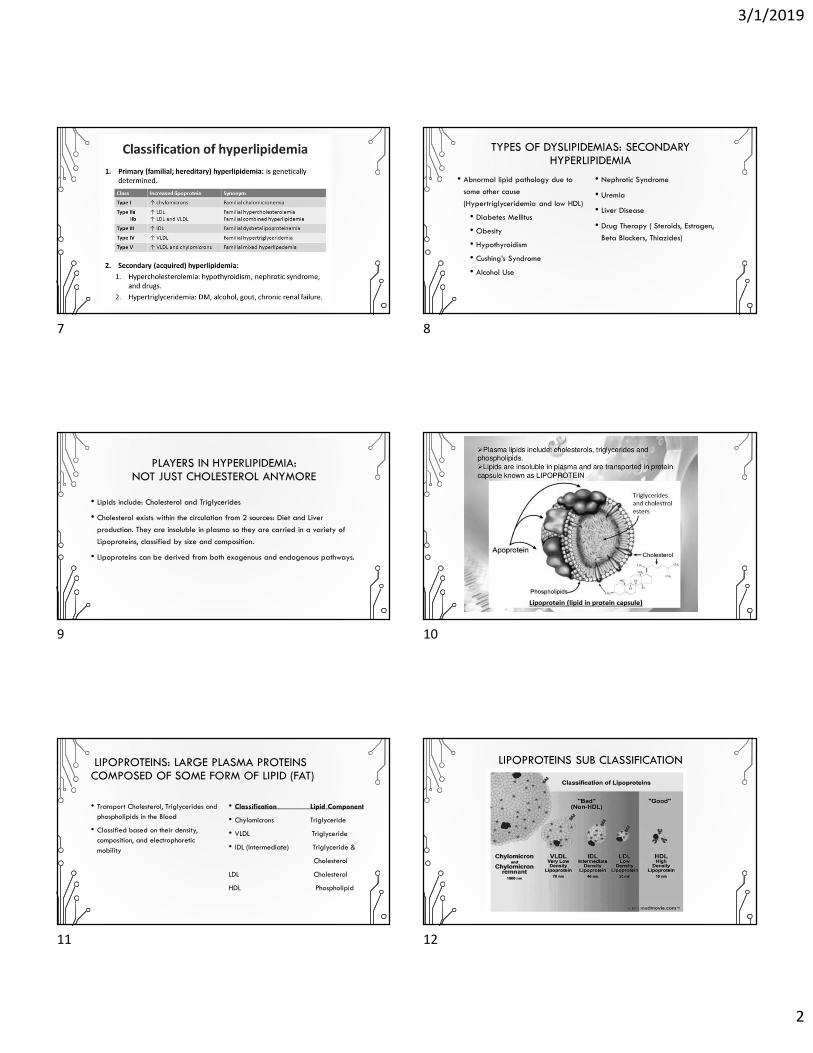
TYPES OF DYSLIPIDEMIAS: SECONDARY HYPERLIPIDEMIA
• Abnormal lipid pathology due to
some other cause
(Hypertriglyceridemia and low HDL)
• Diabetes Mellitus
• Obesity
• Hypothyroidism
• Cushing’s Syndrome
• Alcohol Use
• Nephrotic Syndrome
• Uremia
• Liver Disease
• Drug Therapy ( Steroids, Estrogen,
Beta Blockers, Thiazides)
PLAYERS IN HYPERLIPIDEMIA:NOT JUST CHOLESTEROL ANYMORE
• Lipids include: Cholesterol and Triglycerides
• Cholesterol exists within the circulation from 2 sources: Diet and Liver
production. They are insoluble in plasma so they are carried in a variety of
Lipoproteins, classified by size and composition.
• Lipoproteins can be derived from both exogenous and endogenous pathways.
LIPOPROTEINS: LARGE PLASMA PROTEINS COMPOSED OF SOME FORM OF LIPID (FAT)
• Transport Cholesterol, Triglycerides and phospholipids in the Blood
• Classified based on their density, composition, and electrophoretic mobility
• Classification Lipid Component
• Chylomicrons Triglyceride
• VLDL Triglyceride
• IDL (Intermediate) Triglyceride &
Cholesterol
LDL Cholesterol
HDL Phospholipid
LIPOPROTEINS SUB CLASSIFICATION
7 8
9 10
11 12

3/1/2019
3
LIPID PARTICLE COMPOSITION EXOGENOUS PATHWAY OF LIPID METABOLISM
• Exogenous pathway for lipid
metabolism: Dietary cholesterol and
fatty acids are absorbed.
Triglycerides are formed in the
intestinal cell from free fatty acids
and glycerol and cholesterol is
esterified. Triglycerides and
cholesterol combine to form
chylomicron
ENDOGENOUS PATHWAY OF LIPID METABOLISM
• Endogenous metabolism begins with the liver synthesizing VLDL particles containing Apo B-100 and Cholesteryl esters to form mature VLDL particles. Once released, the VLDL is cleaved (via lipoprotein lipase) into smaller VLDL remnants (IDL) and sub particles that are reabsorbed by the liver or form HDL particles
OTHER INFLAMMATORY MARKERS: APOLIPOPROTEIN B
Apolipoprotein B is the primary
apolipoprotein of chylomicrons, VLDL,
IDL, and LDL particles.
Specific apolipoproteins function in the
regulation of lipoprotein metabolism
through their involvement in the transport
and redistribution of lipids among
various cells and tissues, through their role
as cofactors for enzymes of lipid
metabolism. ApoB is responsible for LDL
“latching onto” blood vessels.
13 14
15 16
17 18

3/1/2019
4
OTHER VASCULAR INFLAMMATORY MARKERS: LP (A)
• Lipoprotein (a): a small particle lipoprotein seen in premature CAD with no risk factors.
• Binds with other Apo B containing lipoproteins
• Enhances LDL entry and accumulation
• Potentiates LDL oxidation
• Digested by Macrophages to produce foam cells
• Stimulates smooth muscle cell proliferation
• Binds Fibrin, platelets to endothelial cells
• Competes with plasminogen for tPA, inhibiting formulation of plasmin (thrombolytic)
• Treatment: Niacin
OTHER VASCULAR INFLAMMATORY MARKERS: C REACTIVE PROTEIN• C-Reactive Protein: is one of a group of
proteins called acute phase reactants that go up in response to inflammation. C-reactive protein (CRP) is produced by the liver. The levels of acute phase reactants increase in response to certain inflammatory proteins called cytokines. These proteins are produced by white blood cells during inflammation and contribute to the genesis and rupture of atheromatous plague.
19 20
21 22
23 24
3/1/2019
5
WHAT WAS NEW IN 2013 ?
• 1. Identification of 4 major statin benefit groups
• 2. Shift away from general treatment to targeted approach
• 3. Definition of Statin intensity identified
• 4. New global risk assessment tool introduced for primary
prevention (http://my.americanheart.org/cvriskcalculator)
• 5. Addition of non-statin drug therapies to further decrease
ASCVD
GROUP 1PATIENTS WITH CLINICAL ASCVD
•Guideline Direction : High intensity statin therapy should
be initiated or continued as first-line therapy in women
and men ≤75 years of age who have clinical ASCVD,
unless contraindicated.
ACC/AHA Guideline 2013/p 22/secondary prevention #1
GROUP 2
PATIENTS WITH PRIMARY ELEVATIONS OF LDL–C ≥190 MG/DL (≥4.9 MMOL/L)
•Guideline Direction : Adults ≥21 years of age with
primary LDL –C ≥190 mg/dL(≥4.9 mmol/L) should be
treated with statin therapy (10- year ASCVD risk
estimation is not required): Use high -intensity statin
therapy unless contraindicated
*ACC/AHA Guideline 2013/p 22/primary prevention ≥21/#2
GROUP 3PATIENTS WITH DIABETES AGED 40 -75 YEARS WITH LDL 70-189 MG/DL (1.8-4.9 MMOL/L) AND WITHOUT CLINICAL ASCVD
•Guideline Direction “Moderate-intensity statin therapy should be initiated or continued for adults 40 to 75 years of age with diabetes mellitus. High-intensity statin therapy is reasonable for adults 40 to 75 years of age with diabetes mellitus with a ≥7.5% estimated 10-year ASCVD risk unless contraindicated
*ACC/AHA Guideline 2013/p 23/primary prevention with diabetes/# 1,2
25 26
27 28
29 30

3/1/2019
6
GROUP 4PATIENTS WITHOUT CLINICAL ASCVD OR DIABETES WITH LDL–C 70 TO 189 MG/DL (1.8 TO 4.9 MMOL/L) AND ESTIMATED 10-YEAR ASCVD RISK ≥7.5%
•Guideline Direction: “Adults 40 to 75 years of age with
LDL–C 70 to 189 mg/dL(1.8 to 4.9 mmol/L), without
clinical ASCVD or diabetes and an estimated 10-year
ASCVD risk ≥7.5% should be treated with moderate-to
high-intensity statin therapy.”
ACC/AHA Guideline 2013/p 23/Primary Prevention w/o Diabetes/#2
RISK ASSESSMENT TOOLS
• https://tools.acc.org/ascvd-risk-estimator-plus/#!/calculate/estimate
• https://professional.heart.org/professional/GuidelinesStatements/Prevention
Guidelines/UCM 457698ASCVD-Risk-Calculator.jsp
• https://reference.medscape.com/calculator/framingham-cardiovascular-
disease-risk
• http://www.reynoldsriskscore.org
Lloyd-Jones DM, Braun LT, Ndumele CE, Smith Jr SC, Sperling LS, Virani SS, Blumenthal RS, Use of Risk Assessment Tools to Guide Decision-Making in the Primary Prevention of Atherosclerotic Cardiovascular Disease, Journal of the American College of Cardiology (2018), doi: https://doi.org/10.1016/j.jacc.2018.11.005.
DISCREPANCIES IN THE GUIDELINES
• 2013 American Diabetic Association Guidelines
• 2013 American Association of Clinical Endocrinologist Guidelines
• 2013 International Atherosclerosis Society
• 2014 U.S. Department of Veterans Administration Dept. of Defense Practice
Guidelines
• 2016 Canadian Cardiology Society Guidelines
• 2016 European Society of Cardiology/European Atherosclerosis Society
• 2016 US Preventive Services Task Force Use of Statin Recommendations
Pallazola, V., Hla, D., Arvantitis, M., et al. (2018) Major Dyslipidemia Guidelines and Their Discrepancies: A Need for Consensus. JACC.
31 32
33 34
35 36

3/1/2019
7
GUIDELINE DISCREPANCIES
• Different CV Risk Estimators: Some used ethnicity, presence of HTN or DM2. Some used
different endpoints (primary and secondary)
• Pooled Cohort Risk Equations
• Framingham Risk Score
• Systemic Coronary Risk Evaluation
• No use of Secondary Diagnostics i.e. Coronary Artery Calcium Scores: What and How to
weigh that data with the numbers, Treatment?
• No consensus on treating Moderate Risk Patients; Most agreed on Lifestyle management but
then what?
• No consensus on what to do with special populations i.e. solid organ transplants, rheumatic
and inflammatory diseases with high potential for drug-drug interactions.
Pallazola, V., Hla, D., Arvanitis, M. et al. (2018) Major Dyslipidemia Guidelines and Their Discrepancies: A Need for Consensus. JACC. April 24.
OTHER PROBLEMS WITH 2013 GUIDELINES
• New global risk Calculator was used that was pooled cohort equations to
develop an estimated 10 year ASCVD risk for AA/Caucasian males/females
• Not evidenced based * Poor attempts at external validation
• No other ethnicity included * No rationale for use of 7.5% as cut off
- No consideration of the inflammatory markers i.e. CRP, Lp (a), Apo B,
LpPLA2
Davidson, MH. Et al. (2011) J. Clinical Lipidology 5: 338-367
2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood CholesterolA Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines
Scott M. Grundy, Neil J. Stone, Alison L. Bailey, Craig Beam, Kim K. Birtcher, Roger S. Blumenthal, Lynne T. Braun, Sarah de Ferranti, Joseph Faiella-Tommasino, Daniel E. Forman, Ronald Goldberg, Paul A. Heidenreich, Mark A. Hlatky, Daniel W. Jones, Donald Lloyd-Jones, Nuria Lopez-Pajares , Chiadi E. Ndumele, Carl E. Orringer, Carmen A. Peralta, Joseph J. Saseen, Sidney C. Smith Jr., Laurence Sperling, Salim S. Virani and Joseph Yeboah
Journal of the American College of Cardiology(2018), doi: https://doi.org/10.1016/j.jacc.2018.11.003
2018 GUIDELINE HIGHLIGHTS
•1) Emphasize a heart healthy life style for ALL individuals
Rubenfire, M., 2018 ACC/AHA Multi-society Guideline on the Management of Blood Cholesterol. JACC. www.acc.org/latest-in-cardiology/ten-points-to-remember/2018
MANAGEMENT OF HYPER/DYSLIPIDEMIAS :LIFESTYLE CHANGES
• Optimize Weight Control BMI < 25
• Optimize BP Control
• Exercise 30=45 min daily x 5 days weekly
• Follow Low Fat, Low Carb Diet (Mediterranean or Dash Diet)
• Stop Smoking
• Sleep 6-9 hours every 24
• Engage in Socialization but Minimize Alcohol
( According to the Dietary Guidelines for AmericansExternal,1 moderate alcohol consumption is defined as having up to 1 drink per day for women and up to 2 drinks per day for men)
2018 GUIDELINE HIGHLIGHTS
• 2) In patients with ASCVD (including CVA, TIA, CAD, ACS, PVD, AAA) reduce
LDL-C with high intensity OR maximally tolerated statins to decrease ASCVD.
This could include low risk with elevated coronary artery calcium scores (CAC)
• 3) In patients with very high-risk ASCVD, with LDL-C > 70, on maximally
tolerated statins, consider adding Ezetimide, then PCSK9 inhibitors
• Major CV Event (MI, CVA, PAD with claudication and ABI <0.85, Amputations, Bypasses
• Heterozygous Familial Hypercholesterolemia (HeFH)
• High Risk Conditions (DM, HTN, CKD with GFR15-59 ml/min/1.2 cm2, Smoking and LDL
> 100
37 38
39 40
41 42

3/1/2019
8
• 2018 Guidelines for
• Very High Risk
• High Risk
2018 GUIDELINE HIGHLIGHTS
• 5) In patients 40-76 yo with DM and LDL-C > 70 mg/dl, begin moderate-
intensity statins
Rubenfire, M., 2018 ACC/AHA Multi-society Guidelines on the Management of Blood Cholesterol.JACC. www.acc.org/latest-in-cardiology/te-points-to-remember/2018
2018 GUIDELINE HIGHLIGHTS
• 6) In patients 40-75 yo evaluated for ASCVD, providers should have a risk
reductions discussion with their patients before beginning a statin. This should
include smoking cessation, BP control, HgA1C and calculated 10 year ASCVD
risk assessment
CLINICIAN – PATIENT RISK DISCUSSION
2018 GUIDELINE HIGHLIGHTS
• 4) In patients with severe primary hypercholesterolemia (LDL-C > 190) begin
high intensity statin therapy. If LDL-C remain > 100 mg/dl add Ezetimibe. If
LDL continues to be high on statin + ezetimibe, consider adding PCSK9
inhibitor
2018 GUIDELINE HIGHLIGHTS
• 7) In patients 40-75 yo w/o DM and with LDL-C>70 mg/dl and a 10 year
ASCVD risk of > 7.5, start a moderate intensity statin if a discussion of
treatment options favors statin therapy to lower LDL-C by > 30%. If risk status
is uncertain, consider using CAC to improve specificity. If 10 yrs. risk is > 20%,
reduce LDL-C by 50%.
• 9) In patients 40-75 yo w/o DM and LDL-C are >70 mg/dl and 10 yrs.
ASCVD risk is >7.5-19.9 % AND statin therapy is uncertain, consider
measuring CAC. If CAC is 1-99, favor statin therapy. If CAC > 100, statin is
indicated unless other risk reductions can be achieved.
43 44
45 46
47 48

3/1/2019
9
CAC MEASUREMENTS: WHEN IS IT APPROPRIATE?
• For patients who are reluctant to initiate statin therapy and want to understand their risk
• For patients concerned about restarting a statin after discontinuing due to statin-related symptoms
• Men (55-80 yo) or Women (60-80 yo) with low burden of risk factors who question benefit of statin
• Adults (40-55 yo)with Pooled Cohort Equation 10 year risk 5-7.5% with CV risk factors, but borderline LDL levels
CORONARY ARTERY CALCIFICATION SCORING• Coronary calcium score 0: No identifiable plaque.
Risk of coronary artery disease very low (<5%)
• Coronary calcium score 1-10: Mild identifiable plaque. Risk of coronary artery disease low (<10%)
• Coronary calcium score 11-100: Definite, at least mild atherosclerotic plaque. Mild or minimal coronary narrowing likely.
• Coronary calcium score 101-400: Definite, at least moderate atherosclerotic plaque. Mild coronary artery disease highly likely. Significant narrowingspossible
• Coronary calcium score > 400: Extensive atherosclerotic plaque. High likelihood of at least one significant coronary narrowing.
2018 GUIDELINE HIGHLIGHTS
• 8) In patients 40-75 yo w/o DM and a 10 year risk of 5-19%, risk enhancing
factors favor initiation of statin therapy. Risk enhancing factors include:
• FH of premature ASCVD *Persistent LDL-C levels > 160
• Metabolic Syndrome *CKD
• H/O Preeclampsia or Early Menopause *Chronic Inflammatory Disorders
• High Risk Ethnic Groups (South Asian) * Elevated Triglycerides > 175 mg/dl
• Elevated Apolipoprotein B > 130 mg/dl * Elevated CPR > 2.0 mg/L
• ABI < 0.9 * Lpa > 50 mg/dl
• Radiation Therapy for L Breast CA whereby coronary arteries are affected
2018 GUIDELINE HIGHLIGHTS• 10) Assess adherence and percentage responses to LDL-C lowering
medications and lifestyle changes with repeat Lipid measurements 4-12 weeks
after statin initiation or dose adjustments, repeating every 3 -12 months
Rubenfire, M., 2018 ACC/AHA Multi-society Guidelines on the Management of Blood Cholesterol.JACC. www.acc.org/latest-in-cardiology/ten-points-to-remember/2018.
LIPID MANAGEMENT: STATINS
• MOA: Competitively inhibit hydroxymethylglutaryl (HMG) CoA reductase, which is an enzyme that aids in cholesterol biosynthesis
• Most statins can lower LDL production within the liver due to LDL receptor turnover allowing increased rate of LDL receptor cycling
• Stains may raise HDL from 5-10% (Simvastatin & Rosuvastatin)
• Statins may decrease triglycerides 10-33% (Atorvastatin & Rosuvastatin)
• Problems:
• Hepatic Dysfunction (ALT increase 0.5-3.0% occurrence)
• Myalgia's due to drug interactions
• Hypothyroidism may cause dyslipidemia and pre-dispose patients to statin-induced myopathy
• Renal proteinuria with high intensity statins
• Renal dosing in patients with CKD
• Diabetes development may occur with high intensity statins as they affect glucose metabolism (conflicting results)
www.uptodate.com/statins-actions-side-effects-and-administration. 3/28/18
STATINS: MECHANISM OF ACTION
• Inhibit the first enzymatic steps in cholesterol synthesis (HMG-CoA)
• Production of this enzyme and of the LDL receptors on Hepatocytes is regulated by the amount of free cholesterol within the hepatocyte
• MOA: Within the hepatocyte: Acetyl CoA binds with HMG-CoA to form free cholesterol within the hepatocyte. When HMG-CoA is blocked a compensatory mechanism is to create more LDL receptors on the hepatocyte to pull more cholesterol out of the plasma
Statins block HMG-CoA
49 50
51 52
53 54

3/1/2019
10
National Lipid Associationhttps://www.lipid.org/sites/default/files/2-_lipid_u-_landmark_clinical_trials-_brown.pdf
National Lipid Associationhttps://www.lipid.org/sites/default/files/2-_lipid_u-_landmark_clinical_trials-_brown.pdf
STATIN EFFECTIVENESS ADVERSE EFFECTS OF STATINS• Myopathy and muscle injury occurs because CoQ10
enzymes are inhibited within the liver also. (CoQ10 is needed for creation of ATP for cellular energy)
• Elevated Liver Enzymes should be monitored to prevent Liver Failure
• GI Upset
• Hyperglycemia (Led to more Dx of Diabetics at higher doses)
• Increased Warfarin levels (bleeding complications)
• Cataracts (in animal toxicity)
• Memory Loss & Confusion (Led to decreased dosages and package warnings in 2012)
Hajar, R. (2011). Statins: Past and Present. Heart Views. 12(3) 121-127
CoQ 10
LIPID MANAGEMENT: EZETIMIBE• MOA: Blocks absorption of lipids in the
small intestine
• When goals are not met in very high-risk patients , when LDL-C levels > 70 g/dl) (or patients who are intolerant of statins) , it is reasonable to add ezetimibe to max tolerated statins.
• IMPROVE-IT trial (Simvastatin & Ezetimibe)
• Ezetimibe can lower LDL-C by additional 20-30%
• Dosing: 10 mg daily w/wo food
• Side Effects:
• Headache * hives, rash
• Dizziness * swelling
• Diarrhea * hoarseness
• sore throat * dyspnea
• runny nose * fatigue
• Sneezing * lack of energy
• joint pain * bruising
• Bleeding
55 56
57 58
59 60
3/1/2019
11
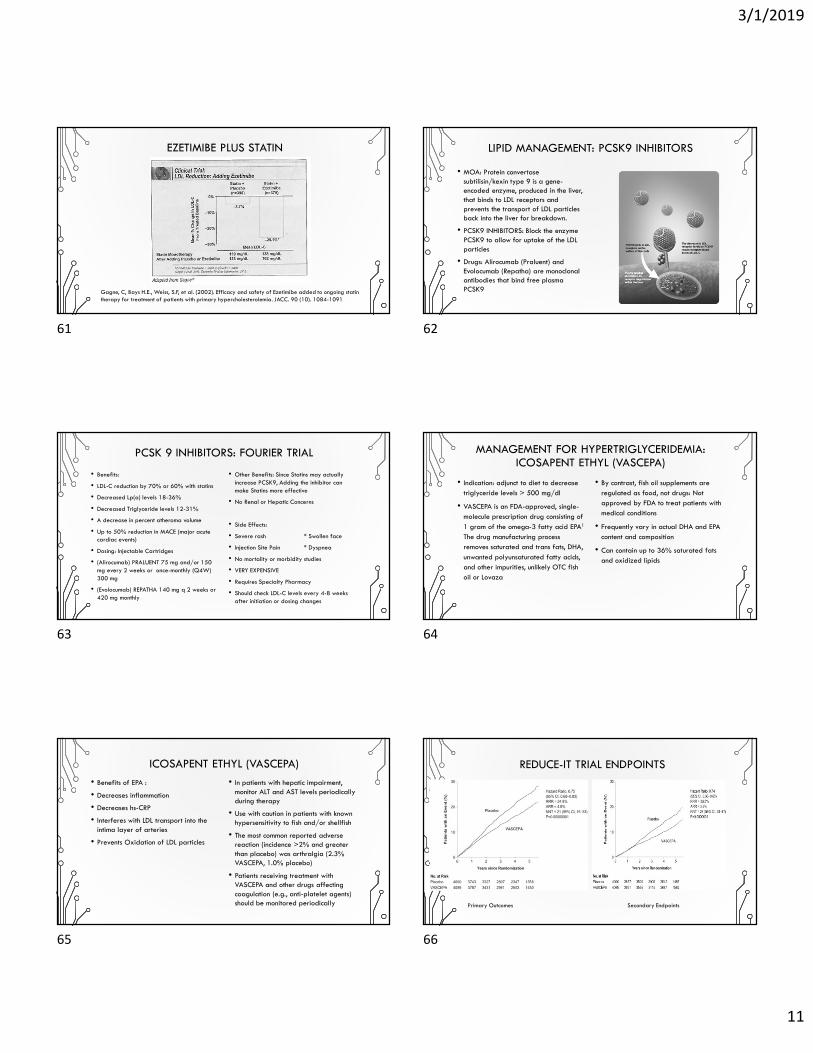
Gagne, C, Bays H.E., Weiss, S.F, et al. (2002). Efficacy and safety of Ezetimibe added to ongoing statin therapy for treatment of patients with primary hypercholesterolemia. JACC. 90 (10). 1084-1091
EZETIMIBE PLUS STATIN LIPID MANAGEMENT: PCSK9 INHIBITORS
• MOA: Protein convertase subtilisin/kexin type 9 is a gene-encoded enzyme, produced in the liver, that binds to LDL receptors and prevents the transport of LDL particles back into the liver for breakdown.
• PCSK9 INHIBITORS: Block the enzyme PCSK9 to allow for uptake of the LDL particles
• Drugs: Alirocumab (Praluent) and Evolocumab (Repatha) are monoclonal antibodies that bind free plasma PCSK9
PCSK 9 INHIBITORS: FOURIER TRIAL
• Benefits:
• LDL-C reduction by 70% or 60% with statins
• Decreased Lp(a) levels 18-36%
• Decreased Triglyceride levels 12-31%
• A decrease in percent atheroma volume
• Up to 50% reduction in MACE (major acute cardiac events)
• Dosing: Injectable Cartridges
• (Alirocumab) PRALUENT 75 mg and/or 150 mg every 2 weeks or once-monthly (Q4W) 300 mg
• (Evolocumab) REPATHA 140 mg q 2 weeks or 420 mg monthly
• Other Benefits: Since Statins may actually increase PCSK9, Adding the inhibitor can make Statins more effective
• No Renal or Hepatic Concerns
• Side Effects:
• Severe rash * Swollen face
• Injection Site Pain * Dyspnea
• No mortality or morbidity studies
• VERY EXPENSIVE
• Requires Specialty Pharmacy
• Should check LDL-C levels every 4-8 weeks after initiation or dosing changes
MANAGEMENT FOR HYPERTRIGLYCERIDEMIA: ICOSAPENT ETHYL (VASCEPA)
• Indication: adjunct to diet to decrease triglyceride levels > 500 mg/dl
• VASCEPA is an FDA-approved, single-molecule prescription drug consisting of 1 gram of the omega-3 fatty acid EPA1
The drug manufacturing process removes saturated and trans fats, DHA, unwanted polyunsaturated fatty acids, and other impurities, unlikely OTC fish oil or Lovaza
• By contrast, fish oil supplements are regulated as food, not drugs: Not approved by FDA to treat patients with medical conditions
• Frequently vary in actual DHA and EPA content and composition
• Can contain up to 36% saturated fats and oxidized lipids
ICOSAPENT ETHYL (VASCEPA)
• Benefits of EPA :
• Decreases inflammation
• Decreases hs-CRP
• Interferes with LDL transport into the intima layer of arteries
• Prevents Oxidation of LDL particles
• In patients with hepatic impairment, monitor ALT and AST levels periodically during therapy
• Use with caution in patients with known hypersensitivity to fish and/or shellfish
• The most common reported adverse reaction (incidence >2% and greater than placebo) was arthralgia (2.3% VASCEPA, 1.0% placebo)
• Patients receiving treatment with VASCEPA and other drugs affecting coagulation (e.g., anti-platelet agents) should be monitored periodically
REDUCE-IT TRIAL ENDPOINTS
Primary Outcomes Secondary Endpoints
61 62
63 64
65 66

3/1/2019
12
ICOSAPENT ETHYL (VASCEPA)
• The REDUCE-IT Trial in 8,179 adult patients at low-density lipoprotein cholesterol (LDL-C) goal, with established cardiovascular disease (CVD) or at high risk for CVD, and hypertriglyceridemia (fasting triglycerides (TG) ≥135 and <500 mg/dL).
• The benefits of VASCEPA were seen on a background of predominately (93.2%) moderate- to high-intensity statin use and median baseline LDL-C levels of 75.0 mg/dL
• 86.9% of patients were exposed for ≥ 12 months.
• Primary Endpoint: The risk for the primary composite endpoint (5-point MACE: time to first occurrence of cardiovascular death, myocardial infarction, stroke, hospitalization for unstable angina, or coronary revascularization; p<0.001): 24.8% RRR
• Secondary Endpoint: The key secondary composite endpoint (3-point MACE: time to first occurrence of cardiovascular death, myocardial infarction, or stroke; p<0.001): 26% RRR
• The decrease in TG at month 12 was 19.7 mg/dl
DYSLIPIDEMIA IN CHILDREN & ADOLESCENTS
• 2018 Recommendations:
• In children and adolescents with obesity
of lipid abnormalities, lifestyle
counseling is first-line therapy
• In children and adolescents 10 year of
age or older with LDL-C > 190mg/dl
or 160 mg/dl with clinical presentation
of FH and DO NOT respond to 3-6
month of lifestyle modifications, it’s
reasonable to start statin therapy
• In children & adolescents with FH of
early CVD and significant
hyperlipidemia, check Lipid profile as
early as 2 years old
• In children & adolescents with moderate
or severe hyperlipidemia, screen all
family members for familial
hyperlipidemia
QUESTIONS ?THANK YOU !
REFERENCES
• Pallazola, V., Hia, D., Arvanitis, M. et al. (2018) Major Dyslipidemia Guidelines and their Discrepancies: a Need for Consensus. www.acc.org/latest-in-cardiology/articles
• Stone, NJ, et al., (2013). 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. JACC. Doi10.1016/jacc2013.11.002
• Davidson, MH., et al. (2011). Clinical utility of Inflammatory Markers and Advanced Lipid Testing. J Clin Lipidology. 5. 338-367.
• NHLBI Expert Panel on Integrated Guidelines for CV Health and Risk Reduction in Children and Adolescents.(2012). www.hnlhi.nih.gov/guidelines/cvd_ped/peds/guidelines_sum.pdf
• Lloyd-Jones DM, et al. (2016) ACC Expert Consensus Decision pathway on the Role of Non-Statin therapies for LDL-cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk.
• Kersten S., (2016). The Genetics of Dyslipidemia—When Less is More. NEJM. 374. 1192.
67 68
69 70
71 72

3/1/2019
13
REFERENCES
• Rosenson, R., et al. (2018). Statins: Actions, side effects and administration.
www.uptodate. Wolters Kluwer. 1-27.
• Rosenson, R., et al (2018). Low Density Lipoprotein Cholesterol Lowering with
Drugs Other Than Statins. www.uptodate. Wolters Kluwer.1-16.
• Rosenson, R., et al (2014). Genetics and causality of triglyceride-rich
lipoproteins in Atherosclerotic Cardiovascular Disease. JACC. 64. 2525.
• Rosenson, R., et (2018). Familial Hypercholesterolemia in Adults: Treatment.
www.uptodate. Wolters Kluwer. 1-12
• Ferranti, S., et (2018). Dyslipidemia in Children: Definition, Screening and
Diagnosis. www.uptodate. Wolters Kluwer. 1-33
73