24-hour blood pressure monitoring to evaluate the effects of nifedipine in pre-eclampsia and in...
TRANSCRIPT

British Journal of Obstetrics and Gynaecology June 1997, Vol. 104, pp. 682-688
24-hour blood pressure monitoring to evaluate the effects of nifedipine in pre-eclampsia and in
chronic hypertension in pregnancy *Chiara Benedetto Professor, *Marina Zonca Research Fellow, *Maurizio Giarola Research Fellow,
*Vincenza Maulh Research Fellow, *Lucian0 Chiarolini Research Fellow, tFranca Carandente Professor *Department of Gynecology and Obstetrics, University of Turin, Italy; fChair of Chronobiology, University of Milan, Italy
Objective To investigate the effect of 7 to 14 days of therapy with nifedipine (sustained-release preparation) on the 24-hour blood pressure patterns of pregnant women with pre-eclampsia or chronic hypertension, and to test the utility of blood pressure monitoring in modulating the timing and dosage of the drug.
Design 24-hour automatic blood pressure monitoring of pregnant women with pre-eclampsia or chronic hypertension before and after nifedipine treatment.
Setting Centre for Prevention, Diagnosis and Treatment of Hypertension in Pregnancy, University of Turin, Italy.
Population Sixteen pregnant women with pre-eclampsia and 17 with chronic hypertension.
Methods 24-hour blood pressure monitoring was performed before the beginning of the therapy and after 7 to 14 days of treatment with sustained-release nifedipine.
Main outcome measures Chronobiological analysis of systolic and diastolic blood pressure values was performed; MESOR, amplitude, acrophase, hyperbaric index, percent time elevation and significance of rhythm were calculated before and after treatment.
Results 6336 blood pressure measurements were analysed. Systolic and diastolic MESOR values were significantly decreased after nifedipine treatment both in pre-eclampsia and in chronic hypertension. However, the antihypertensive effect of nifedipine in pre-eclampsia was especially pronounced during evening and night, while in chronic hypertension it was more constant during the 24-hour period. 24-hour blood pressure monitoring allowed adjustment, when necessary, to the timing and dosage of nifedipine in accordance with the blood pressure patterns of each patient, using the hyperbaric index and percent time elevation as objective parameters for the evaluation of treatment efficacy.
Conclusions 24-hour blood pressure monitoring is a good method to optimise treatment, and confirms that nifedipine is useful for the control of maternal blood pressure in pregnancy.
INTRODUCTION
Calcium channel blockers, such as nifedipine, are used effectively in the treatment of hypertension in non- pregnant women1. However, several investigators have reported improved maternal and perinatal outcome when nifedipine was given to pregnant women as a sec- ond-line antihypertensive in severe pre-eclampsia24. Despite the effect on blood pressure, one study did not find a reduction in the number of days of maternal hospitalisation or an improvement in perinatal outcome when nifedipine therapy was compared with bed rest ~ ~~
Correspondence: Professor C. Benedetto, Dipartimento di Disci- pline Ginecologiche ed Ostetriche, Universith di Torino, Via Ventimiglia 3, 10126 Torino, Italy.
alone in the management of mild pre-eclampsia remote from term5. Nifedipine is superior to hydralazine in the control of severe maternal hyperten~ion~.~ and seems to lower maternal blood pressure without affecting fetal and uteroplacental blood flow"".
Noninvasive automatic blood pressure monitoring is considered by many physicians the ideal way to eval- uate control of hypertension12. However, there are no reports about the effects of nifedipine on the 24-hour blood pressure pattern of pregnant women with pre- eclampsia or chronic hypertension. The aims of this study were twofold: first, to investigate the effect of 7 to 14 days of therapy with nifedipine (sustained-release) on the 24-hour blood pressure patterns of pregnant women with pre-eclampsia or chronic hypertension.
682 0 RCOG 1997 British Journal of Obstetrics and Gynaecology

2 4 - H O U R BLOOD P R E S S U R E M O N I T O R I N G T O E V A L U A T E N I F E D I P I N E 683
Second, to test the utility of blood pressure monitoring in modulating the timing and dosage of the drug.
METHODS Thirty-four pregnant women with pre-eclampsia and 24 with chronic hypertension were recruited. All had been referred to our Centre for the Prevention, Diagnosis and Treatment of Hypertension in Pregnancy, where hyper- tensive patients are generally hospitalised for at least 24 hours to undergo a complete set of biophysical and biochemical analyses.
Before blood pressure monitoring, women were assigned to pre-eclampsia and chronic hypertension groups using traditional sphygmomanometric mea- surements and the criteria reported by Davey and MacGillivray 13. Pre-eclampsia was diagnosed when two consecutive measurements of diastolic blood pressure 2 90 mmHg and proteinuria 2. 300 mg in one 24-hour urine collection were found after the 20th week of pregnancy in a previously normotensive and non- proteinuric woman. Chronic hypertension without proteinuria was diagnosed when two consecutive mea- surements of diastolic blood pressure 2 90 mmHg were found in a woman known to suffer from chronic hyper- tension before pregnancy, or when diastolic blood pres- sure I 9 0 mmHg developed before the twentieth week of pregnancy in the absence of trophoblastic disease.
All women were synchronised to rest-activity and precisely timed meal schedules (breakfast 6:30 am; lunch 12:30 pm; dinner 6:OO pm). They remained in bed for most of the time, and 24-hour blood pressure monitoring was started between 1O:OO am and 1:00 pm. During the 24-hour period, systolic and diastolic arterial blood pressures were measured every 30 minutes, from the right arm, with an automatic oscillometric monitor Dinamap 1846 S X P (Critikon, Ethicon SPA, Pratica di Mare, Rome, Italy) that has been validated in pregnancy14.
All women were monitored once before the begin- ning of therapy and again after 7 to 14 days of treatment with sustained-release nifedipine (dosage 10 to 20 mg given twice a day between 8:OO and 9:OO am and between 8:OO and 9:OO pm). The range of between 7 and 14 days was chosen for practical reasons since women who did not remain hospitalised might have been unable to come back. In 15 women with chronic hyper- tension and in eight with pre-eclampsia blood pressure monitoring were repeated at intervals throughout gesta- tion until delivery and, when necessary, the timing and dosage of nifedipine were adjusted according to the effect of the drug during each 24-hour period.
Systolic and diastolic blood pressure values were downloaded to an IBM personal computer. An observer edited each record, noting missing values and probable
artefacts. Rejected or missing values were replaced by linearly interpolated values, provided that no more than two consecutive samples required editing. The data series of each blood pressure monitoring session were analysed by the single cosinor method to evaluate their circadian rhythmicity, As a rhythm represents a regu- larly recurring oscillation, this procedure consists of a fit of a 24-hour cosine curve to the data series, by the least-squares statistical method. The definition of this mathematical model allows estimation of the following parameters: 1. the midline estimating statistic of rhythm (MESOR), defined as the average value of the rhythmic function fitted to the blood pressure data; 2. the ampli- tude, that is the measure of one half the extent of rhyth- mic variation of blood pressure in a cycle; and 3. the acrophase, a measure of timing, i.e. the lag from a refer- ence timepoint (in this study, local midnight) of the crest-time in the cosine curve appropriately approximat- ing the blood pressure circadian rhythm (Fig. la). The significance value for a rhythm is calculated by the statistical zero amplitude test: where A = 0 in the cosine function
f (t) =M+ A cos (ot+ F) where M = MESOR; A = amplitude; F = acrophase; o = angular frequency; t = time. Rejection of this null hypothesis signifies that the fitted curve (implying rhythmicity) approximates the data more closely than does a straight line with zero slope (implying con- stancy). Acceptance of the hypothesis A = 0 implies either that the data are essentially constant with time or that the single cosine model is otherwise inappr~priate'~.
The parametric endpoints obtained for each individ- ual data series were summarised by the population- mean cosinor method15, obtaining the circadian blood pressure rhythmometric characteristics for each group of subjects and time of monitoring (before and after therapy). The timing and dosage of nifedipine were adjusted if blood pressure data profiles of women suffering from pre-eclampsia or chronic hypertension significantly differed from a time-qualified reference interval (chronodesm). This was calculated with 95% prediction limits from blood pressure data collected for each period of pregnancy from 73 healthy normotensive women with uncomplicated pregnancies, who voluntar- ily underwent 24-hour blood pressure monitorings.
Comparison between the circadian blood pressure profile of each woman and the chronodesm, appropriate for gestational period, allowed calculation of the hyper- baric index16. This corresponds to the total 'area' of blood pressure above the upper limit of the chronodesm (units = mmHg/24 h) and it can be considered a measure of the total pressure load exerted upon the arterial wall. Another important index, calculated to evaluate this load, was the percent time elevation16,
0 RCOG 1997 Br J Obstet Gynaecol 104, 682-688

684 c. BENEDETTO ET AL.
(a) (b) 170- Acrophase Reference 170 -
110- Chronogram 11 0 -
90 - I I I I I 1 90 I 1 I I I 1
08:OO 12:OO 16:OO 20:OO 24:OO 04:OO 08:OO 08:OO 12:OO 16:OO 20:OO 24:OO 04:OO 08:OO
Hours of the day Hours of the day
Fig. 1. Chronobiological parameters, calculated for systolic blood pressure (SBP) values in one pregnant woman with chronic hypertension before the beginning of the therapy. (a) Illustration of the parameters evaluated by least-squares fit of cosine model: MESOR (midline estimat- ing statistic of rhythm), amplitude and achrophase. The chronogram is the individual display of data as a function of time. The continuous sinu- soidal curve is the expression of the mathematical hnction which better approximates the rhythm. (b) The superimposition of the chronogram onto the normal range (chronodesm) of corresponding gestational weeks, which allows calculation of the hyperbaric index (HBI) and percent time elevation (PTE). The chronodesm is the time-qualified reference interval representing the 95% prediction limit.
Table 1. Characteristics of the women included in the study. Values are given as mean f SEM (range) unless otherwise indicated.
Pre-eclampsia (n = 16) Chronic hypertension (n = 17)
Age (years) 30.5 f 1.2 (21-36) 32.9 f 1.0 (24-40) No. primigravidae 7 6 No. multigravidae 9 1 1 Proteinuria at diagnosis (mg/24 h) 1850 f 470 (400-4000) 80 f 20 (0.0-220) Gestational age at the beginning of the therapy (weeks) 30.7 f. 0.9 (25-37) 18.4f 1.8 (8-30) Gestational age at delivery (weeks) 35.1 f 0.9 (29-40) 36.6 f 0-7 (30-40) Newborn weight (g) 2215 f235 (955-3380) 2725 f206 (1050-4080)
which indicates the percent of time during which blood pressure values exceed the threshold constituted by the upper limit of the relevant chronodesm (Fig. lb). The indices hyperbaric index and percent time elevation (expressed as two simple numbers) give information of the dynamic evaluation of 24-hour monitoring of blood pressure and, in our study, were used to compare the effect of different timings and dosages of nifedipine in the same woman. Results were analysed using SPSS, the Statistical Package for Social Science. Statistical differences between pre- and post-therapy values within each group of women were calculated by Student’s t test for paired data.
RESULTS
Eighteen women with pre-eclampsia were delivered before the 7th day of therapy leaving 16 data sets for analysis. Seven women with chronic hypertension post- poned their hospitalisation after the 14th day because of family reasons leaving 17. The characteristics of the women remaining in the study are shown in Table 1.
We analysed a total of 6336 blood pressure measure- ments. In no instance did diastolic oscillometric mea- surement of the Dinamap, corresponding to the fifth phase of Korotkoff sounds, measure zero.
In pre-eclamptic women treatment decreased systolic and diastolic MESOR in 69% (11/16) and 81% (13/16), respectively (Table 2). Considering all women together, both systolic and diastolic MESOR appear to be signifi- cantly decreased after the therapy. In addition, nifedipine tended to anticipate the acrophase of the population- mean cosinor (17:16 h before therapy vs 15:30 h after therapy for systolic blood pressure; 1554 h vs 14:15 h; P < 0.05, for diastolic blood pressure), and to increase the amplitude (4-9 mmHg before therapy vs 6.5 mmHg after therapy, for systolic blood pressure; 4.7 mmHg vs 5.4 mmHg for diastolic blood pressure). However, in each single case, changes in acrophase and amplitude seemed to be independent of each other, and from those of the MESOR.
In pregnant women with chronic hypertension, the drug decreased systolic and diastolic MESOR in 94% (16/17) and 82% (14/17), respectively (Table 3). Considering all women together after treatment, both
0 RCOG 1997 Br J Obstet Gynaecol 104, 682-688

2 4 - H O U R B L O O D P R E S S U R E M O N I T O R I N G T O E V A L U A T E N l F E D l P I N E 685
Table 2. Single values of 24-hour systolic and diastolic blood pres- sure MESOR (mmHg), before and after 7 to 14 days of nifedipine treatment in 16 pregnant women with pre-eclampsia. PMC = popula-’ tion mean cosinor.
Table 3. Single values of 24-hour systolic and diastolic blood pres- sure MESOR (mmHg), before and after 7 to 14 days of nifedipine treatment, in 17 pregnant women with chronic hypertension. Key as for Table 2.
Systolic MESOR Diastolic MESOR Patient no. Pre-therapy Post-therapy Pre-therapy Post-therapy
1 128.0 129.2 86.4 82.6 2 123.3 124.8 77.9 78.1 3 139.5 129.3 87.7 77.4 4 147.4 144.0 95.9 842 5 129.2 127.9 82.6 82.6 6 129.8 132.3 80.4 81.0 7 140.9 134.3 91.6 86.4 8 110.7 105.1 69.4 65.0 9 129.6 11 8.8 79.4 73.0
10 118.6 11 6.4 78.7 77.2 11 135.1 129.8 85.0 78.2 12 129.8 124.5 86.5 77.7 13 131.5 121.2 83.4 75.0 14 121.2 126.1 74.2 77.1 15 142.0 132.1 95.6 90.6 16 124.4 127.1 70.6 70.5
PMC 130.1 f 2.4 127.0 zk 2.2* 82.9 f 2.0 78.8 f 1.6*
*Versus before therapy, P < 0.05.
systolic and diastolic MESOR appeared to be decreased even more significantly than in pre-eclampsia. In addition, nifedipine did not affect the acrophase of the population-mean cosinor (14:53 h before therapy vs 15:08 h after therapy for systolic blood pressure; 14:43 h vs 14:30 h for diastolic blood pressure), and tends to decrease the amplitude (6.7 mmHg, before therapy, vs 5.9 after therapy, for systolic blood pressure; 5.9 mmHg vs 5-0 mmHg for diastolic blood pressure). However, in each single case, changes in amplitude were independent from those of the MESOR.
In both groups of women treatment did not modify the significance of rhythm. Circadian trends of the mean values of systolic and diastolic blood pressure in women with pre-eclampsia or chronic hypertension, before and after therapy, are plotted in Figs 2 and 3. It can be seen that the antihypertensive effect of nifedipine in pre-eclampsia is especially pronounced during evening and night. In chronic hypertension the effect of nifedipine is greater and more constant during the 24-hour period. No difference in the response to nifedipine therapy was found between primigravidae and multigravidae, analysed separately within each of the two groups of hypertensive women,
In women followed longitudinally throughout gesta- tion the 24-hour blood pressure monitoring, before and during treatment, allowed adjustment of the timing and dosage of nifedipine in relation to the blood pres- sure patterns in each case. Figure 4 shows how this approach allows optimisation of treatment, as demon- strated by the progressive decrease in hyperbaric index
Systolic MESOR Diastolic MESOR Patient no. Pre-therapy Post-therapy Pre-therapy Post-therapy
A B C D E F G H I J K L M N 0 P
PMC Q
139.8 128.0 149.9 132.4 1533 141.1 117.4 134.1 1 1 1 . 1 152.9 154.7 153.3 1255 130.4 127.8 165.0 11 8.6 137.4f3.7
123.6 94.0 77.2 108.6 86.7 68.1 133.0 91.4 84.1 131.9 81.2 82.0 154.5 84.3 88.4 128.8 89.2 80.9 103.0 76.0 65.1 120.9 90.9 76.9 106.4 70.8 68.7 136.7 100.9 83. I 148.7 101.4 975 1454 87.3 84.3 119.9 81.3 77.6 125.0 73.6 77.8 11 8.9 87.7 75.7 126.2 102.9 81.2 95.1 74.6 52.0
125.1 f 3.9* 86.7 f 2.4 77.6 f 2.5*
*Versus before therapy, P < 0.005.
and percent time elevation of both systolic and diastolic blood pressure.
DISCUSSION
Automatic blood pressure monitoring increasingly is being used not only to diagnose hypertension but also to monitor therapy. The method is especially helpful in evaluating the ability of drugs to suppress hypertension for the entire day and night since it is well known that single blood pressure samplings can be misleading. To our knowledge this is the first study to report the effect of nifedipine treatment on the 24-hour blood pressure pattern of pregnant women with pre-eclampsia or chronic hypertension. Moreover, the use of objective parameters that qualify and quantify the hypertensive status (i.e. MESOR, acrophase, amplitude, hyperbaric index, percent time elevation) allows comparison between different patients surveys. Correlations with maternal and/or fetal outcome can be more precise than with traditional single sphygmomanometric measure- ments. We found that, in pre-eclampsia, nifedipine significantly decreased systolic and diastolic MESOR in 69% and 8 1% of the cases, respectively. Considering all women together, the drug seemed to anticipate the acrophase to the time (approximately 3 pm) found in normotensive pregnant women of corresponding weeks of gestation”.
The observation that the decrease in blood pressure after treatment was more pronounced during the
0 RCOG 1997 Br J Obstet Gynaecol 104, 682-688

686 C . B E N E D E T T O E T A L .
1601 140
l2OI
0
g 100 E
I I I I 1 I 1
08:OO 12:oo 16:OO 20:oo 24:OO 04:OO 08:OO
Hours of the day
Fig. 2. Circadian trend plot (24-hour) of mean values of systolic (SBP) and diastolic (DBP) blood pressure automatically measured in sixteen women with pre-eclampsia before and after 7 to 14 days of therapy with nifedipine sustained-release. Hatched lines indicate a significant (P < 0.05) difference. Mean values of SBP and DBP obtained in 46 normotensive pregnant women at corresponding weeks of gestation are plot- ted as control reference. Statistical differences were calculated by Student’s t test for paired data.
Before therapy
After therapy
0
g 100- E
80 -
60 -
Controls (SBP)
Before therapy
After therapy Controls (DBP)
4 0 1 I 1 1 I 1 1 1
08:OO 12:oo 16:OO 20:oo 24:OO 04:OO 08:OO
Hours of the day
Fig. 3. Circadian trend plot (24-hour) of mean values of systolic (SBP) and diastolic (DBP) blood pressure automatically measured in seventeen women with chronic hypertension before and after 7 to 14 days of therapy with nifedipine sustained-release. Hatched lines indicate a significant (P < 0.05) difference. Mean values of SBP and DBP obtained in 27 normotensive pregnant women at corresponding weeks of gestation are plot- ted as control reference. Statistical differences were calculated by Student’s t test for paired data.
0 RCOG 1997 Br J Obstet Gynaecol 104, 682-688
2 4 - H O U R BLOOD P R E S S U R E M O N I T O R I N G T O E V A L U A T E N I F E D I P I N E 687
im - im . 140.
120.
100.
M .
60.
10 mg NIFEDIPINE 8.00 h n 20.00 h n
1m 18Weeks 1 DURING THERAPY I 160 1 HBI: 282.9 P I E BOA
60 1 m m 8 10m8 10mg NIFEDIPINE (Lmhn 16.00hn 24.00hn
1w 21 Weeks (WRINGTHERAW]
im 1 HBI: 48.0 PTE: 37.3
IW 28Weeks I DURINCTHERAPY)
HBI: 9.7 &: 9.5 I
10.OOhn 17JJOhn Z3.Whn
+ Ban u r n i6.m mm u.m 4.00 am
HOURS OF THE DAY
DBP ,L\ I")
-Hg l3 W e e k
120 1 6 W e e k I DURING THERAW I 1051 . HBI: 63.0 PTE: 66.7
NIFEDIPINE "' lomi 10 m i
m 18Weeks (DURINGTHEIAW~
105T HBk67.8 -44.9
kM hn 20.00 hn
120 21 Weeks [DURING THERAW ] 1051 I HBI: 8.3 PTE 6.8
10.00hn 17JJOhn U . W h n
I WRINGTHERAW I 120 2 8 W n k 105 I HBk0.0 PT'EO.0
1LWhn 17.00hn SLmhn
o n m 16.m z0.m u.m rao 8.m HOURS OF THE DAY
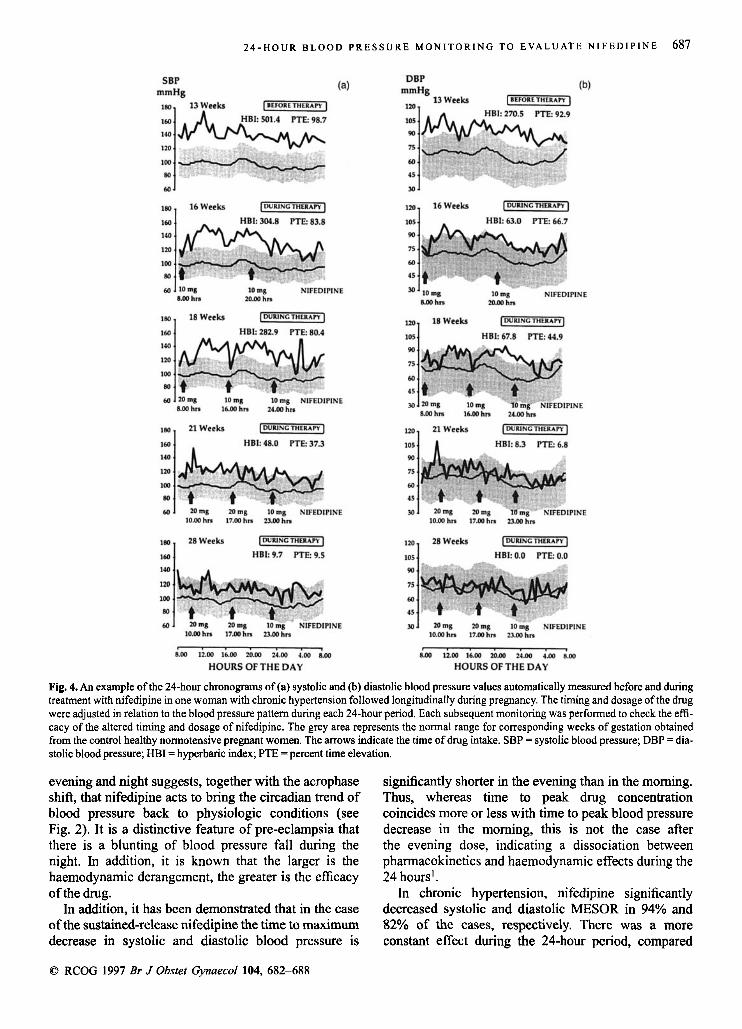
Fig. 4. An example of the 24-hour chronograms of (a) systolic and (b) diastolic blood pressure values automatically measured before and during treatment with nifedipine in one woman with chronic hypertension followed longitudinally during pregnancy. The timing and dosage of the drug were adjusted in relation to the blood pressure pattern during each 24-hour period. Each subsequent monitoring was performed to check the effi- cacy of the altered timing and dosage of nifedipine. The grey area represents the normal range for corresponding weeks of gestation obtained from the control healthy normotensive pregnant women. The arrows indicate the time of drug intake. SBP = systolic blood pressure; DBP = dia- stolic blood pressure; HBI = hyperbaric index; PTE =percent time elevation.
evening and night suggests, together with the acrophase shift, that nifedipine acts to bring the circadian trend of blood pressure back to physiologic conditions (see Fig. 2). It is a distinctive feature of pre-eclampsia that there is a blunting of blood pressure fall during the night. In addition, it is known that the larger is the haemodynamic derangement, the greater is the efficacy of the drug.
In addition, it has been demonstrated that in the case of the sustained-release nifedipine the time to maximum decrease in systolic and diastolic blood pressure is
significantly shorter in the evening than in the morning. Thus, whereas time to peak drug concentration coincides more or less with time to peak blood pressure decrease in the morning, this is not the case after the evening dose, indicating a dissociation between pharmacokinetics and haemodynamic effects during the 24 hours'.
In chronic hypertension, nifedipine significantly decreased systolic and diastolic MESOR in 94% and 82% of the cases, respectively. There was a more constant effect during the 24-hour period, compared
0 RCOG 1997 Br J Obstet Gynaecol 104, 682-688

688 c . B E N E D E T T O E T A L .
with pre-eclampsia (see Fig. 3). These data imply that nifedipine can represent a good pharmacological choice for the control of essential hypertension in pregnancy.
Two explanations can be put forward for the differ- ence in antihypertensive efficacy of nifedipine in pre-eclampsia and chronic hypertension. First, from the hypertensive point of view the cases of pre-eclampsia included in the study were less serious than those of chronic hypertension. In fact, 18 women with severe pre-eclampsia were delivered within a few days of hos- pitalisation and could not be followed for 7 to 14 days after the beginning of the therapy. Second, once the pathogenetic process of pre-eclampsia is primed it dete- riorates despite the therapy. This hypothesis is strength- ened by the observation that in eight women who showed a good response to the antihypertensive effect of nifedipine, platelet count, uric acid, proteinuria and renal function tests did not improve during treatment (data not shown), as already reported by Sibai et aL5.
Finally, our study clearly shows that 24-hour auto- matic blood pressure monitorings, rather than traditional blood pressure measurements, allows appropriate adjustment of the timing and dosage of nifedipine in relation with the blood pressure pattern in individual cases, as shown in Fig. 4. This approach has important clinical implications since it allows for optimal treat- ment with the potential for minimising side-effects of the drug on mother and fetus.
In conclusion, our results demonstrate that in pre-eclampsia nifedipine tends to bring the circadian trend of blood pressure back to physiologic conditions. Nifedipine has a significant effect on both systolic and diastolic blood pressure in a high percentage of cases, especially during the evening and night, whereas in chronic hypertension its efficacy is more constant during the 24-hour period. The use of 24-hour auto- matic blood pressure monitoring in hypertensive women during pregnancy allows optimisation of the timing and dosage of drug therapy.
Acknowledgements This study was supported by the Italian Ministry for University and Scientific and Technological Research (MURST 40%) and the Italian National Research Council (CNR)-targeted project ‘Prevention and
Control Disease Factor’, subproject ‘Maternal-Infant Disease’, contract no. 9300691 .PF41. The authors would like to thank Professor A. Angeli for his encour- agement and Ethicon SPA for technical support.
References 1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
Lemmer B, Nold G, Bebne S, Kaiser R. Chronophannacokinetics and cardiovascular effects of Nifedipine. Chronobiol Int 1991; 8: 485-494. Walters BNJ, Redman CWG. Treatment of severe pregnancy-associ- ated hypertension with the calcium antagonist nifedipine. Br J Obstet Gynaecoll984; 91: 33C336. Constantine G, Beevers DG, Reynolds AL, Luesley DM. Nifedipine as a second line antihypertensive drug in pregnancy. Br J Obstet Gynaecol. 1987; 94: 11361142. Greer IA, Walker JJ, Bjornsson S, Calder AA. Second line therapy with nifedipine in severe pregnancy-induced hypertension. Clin Exper Hyper-Hyper in Pregnancy 1989; B8: 271-292, Sibai BM, Barton JR, Akl S, Sarinoglu C, Mercer BM. Arandomized prospective comparison of nifedipine and bed rest versus bed rest alone in the management of preeclampsia remote from term. Am J Obstet Gynecoll992; 167: 879-884. Seabie SJ, Moodley J, Becker P. Nifedipine in acute hypertension emergencies in pregnancy. SAfr Med J; 76: 248-250. Fenakel K, Fenakel G, Appleman Z et al. Nifedipine in the treatment of severe preeclampsia. Obstet Gynecol. 1991; 71: 331-337. Lindow SW, Davies N, Davey DA, Smith JA. The effect of sublingual nifedipine on uteroplacental blood flow in hypertensive pregnancy. Br JObstet Gynaecoll988; 95: 12761281. Moretti MM, Fairlie FM, Akl S, Khoury AD, Sibai BM. The effect of nifedipine therapy on fetal and placental Doppler waveforms in preeclampsia remote from term. Am J Obstet Gynecol 1990; 163: 1844-1 848. Pirhonen JP, Erkkola RU, Ekblad UU. Uterine and fetal flow velocity waveforms in hypertensive pregnancy: the effect of single dose of nifedipine. Obstet Gynecoll990; 76: 3741. Ismail AAA, Medhat I, Tawfic TAS, Kholeif: A. Evaluation of cal- cium-antagonist (Nifedipine) in the treatment of pre-eclampsia. Int J Gynecol Obstet 1993; 40: 3943. Tamura K. Chronobiologic evaluation of drug efficacy in hyperten- sion. Chronobiollnt. 1991; 8: 511-525. Davey DA, MacGillivray I. The classification and definition of the hypertensive disorders of pregnancy. Clin Exper Hyper-Hyper in Pregnancy 1986; B5: 97-133. Milsom I, Svahn S-0, Forssman L, Sivertsson R. An evaluation of automated indirect blood pressure measurement during pregnancy. Acta Obstet GynecolScand 1986; 65: 721-725. Nelson W, Tong YL, Lee JK, Halberg F. Method for cosinor-rhyth- mometry. Chrunobiologia 1979; 6: 305-323. Carandente F, Halberg F. Chronobiology of blood pressure in 1985 Chronobiologia 1985; 11: 189-321. Benedetto C, Zonca M, Marozio L, Dolci C, Carandente F, Massobrio M. 24-hour blood pressure patterns in physiologic pregnancy and in pregnancy-induced hypertension, preeclampsia and chronic hyperten- sion. Obstet Gynecoll996; 88: 503-512.
Received 30 May 1996 Accepted 12 November 1996
0 RCOG 1997 Br J Obstet Gynaecol 104, 682-688