26 annual clinical symposium on advances in skin and … · page 1 26th annual clinical symposium...
TRANSCRIPT
Page 1
26th Annual Clinical Symposium on Advances
in Skin and Wound CareWashington DC, 2011
James McGuire DPM, PT, CPed, FAPWCACertified in Wound Care by the Council for Medical Education and
Testing, CMET
Total Contact Cast: Is it Really the Gold Standard?
James McGuire DPM, PT, CPed, FAPWCA
Director
Leonard Abrams Center for Advanced Wound Healing
Temple University, Philadelphia, PA
Original Supporting Evidence
Myerson M, Papa J, Eaton K, Wilson K. The total contact cast for management of neuropathic plantar ulceration of the foot. JBJS (Am) 1992;74:261-9.
Helm PA, Walker SC, Pullium G. Total contact casting in diabetic patients with neuropathic foot ulcerations. Arch Phys Med Rehab 1984;65:69l-3.
Pring DJ, Casiebanca N. Simple plantar ulcers treated by below-knee plaster and moulded double-rocker plaster shoe: A comparative study. Lepr Rev 1982;53:261-4.
Pollard JP, LeQuesne LP. Method of healing diabetic forefoot ulcers. Br Med J 1983; 286:436-7. Joseph B, Joshua S, Fritschi EP. The moulded double-rocker plaster shoe in the field treatment of plantar ulcer. Lepr Rev
1983;54:39-44. Diamond JE, Sinacore DR, Mueller MJ. Moulded double-rocker plaster shoe for healing a diabetic plantar ulcer: A case report.
Phys Ther 1987;67:1550-2. Sinacore DR, Mueller MJ, Diamond JE, Blair VP, Drury D, Rose SJ. Diabetic plantar ulcers treated by total contact casting.
Phys Ther 1987;67:1543-9. Walker SC, Helm PA, Pullium G. Total contact casting and chronic diabetic neuropathic foot ulcerations: Healing rates by
wound location. Arch Phys Med Rehabil 1987;68:217-21. Kaplan M, Gelber RH. Care of plantar ulcerations: Comparing applications, materials and non-casting. Lepr Rev 1988;59:59-66. Bossen F, Lethner F. Plantar casts in the management of advanced ischemic and neuropathic diabetic foot lesions. Diabet Med
1989;6:720-3. Birke JA, Novick A, Patout CA, Coleman WC. Healing rates of plantar ulcers in leprosy and diabetes. Lepr Rev 1992;63:365-
74. Sinacore DR. Healing times of diabetic ulcers in the presence of fixed deformities of the foot using total contact casting. Foot
Ankle Int 1998;19:613-8.

Page 2
Sinacore DR. Total contact casting for diabetic neuropathic ulcers. Phys Ther 1996;76:296-301
A review of 13 published studies of total contact casting 0f 526 ulcers found that the ulcers had been present for 182 ± 14 days (mean ± SE), but ∼88% healed in an average of 43 ± 2 days. 11 of the 13 studies had mean healing times of 36–44 days
Total Contact Cast
Still considered by many to be the gold standard for offloading because of improved healing rates (88.9%) and cost savings when compared to standard methods of care
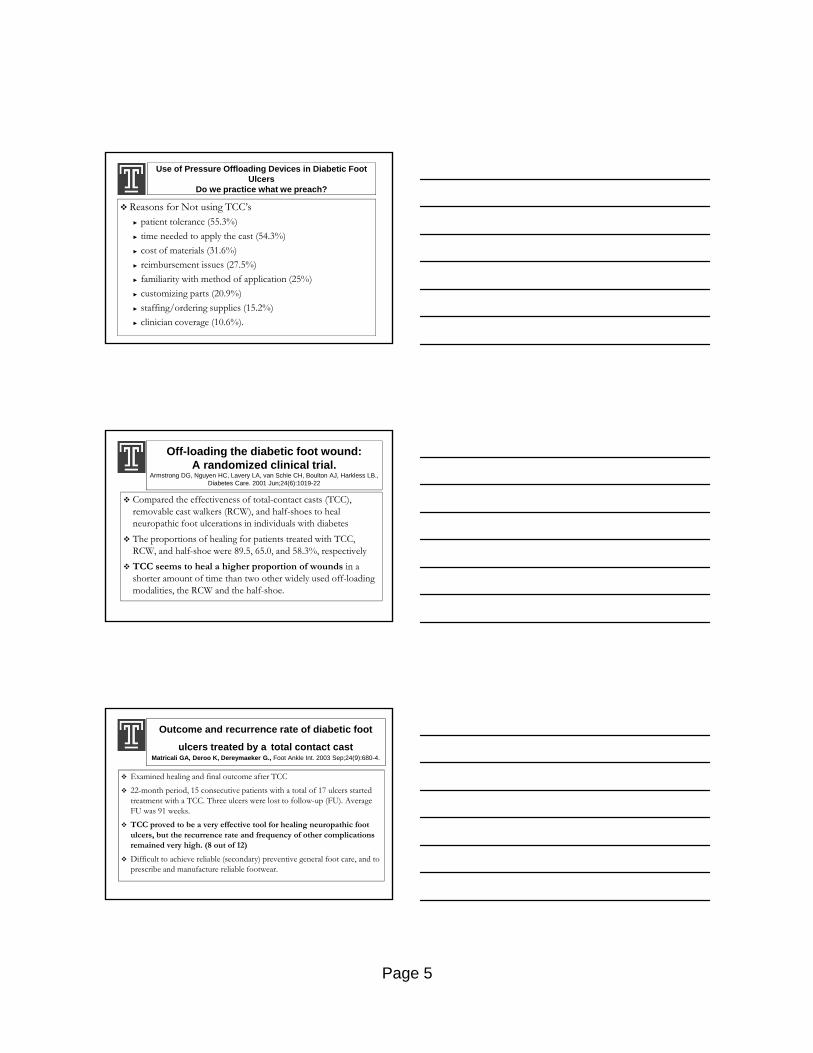
Results of 9 TCC Studies
Average Healing Time:43.73 daysPercent Healed:
88.9%Helm 1984; Sinacore 1987; Walker 1987; Mueller 1989; Meyerson 1992; Birke 1992; Lavery 1997; Armstrong 2001; Birke 2002
Slide Courtesy of Greg Bohn, MD
Page 3
Spencer SA. Pressure relieving interventions for preventing and treating diabetic foot ulcers.
Cochrane Database of Systematic Reviews 2000
There is limited evidence of the effectiveness of orthotic interventions over removal of callus. There is some evidence evaluating the relative effectiveness of two types orthotic devices.There is very limited evidence of the effectiveness of therapeutic shoes.TreatmentThere is very limited evidence of the effectiveness of total contact casts in the treatment of diabetic foot ulcers
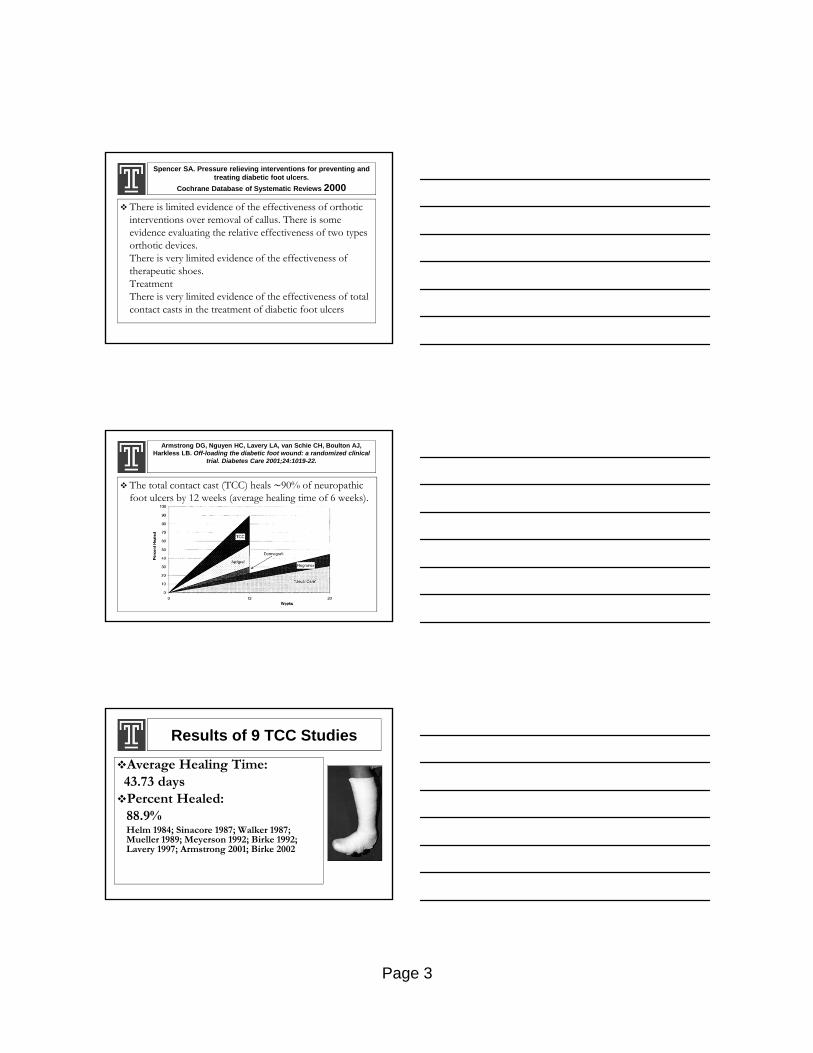
Armstrong DG, Nguyen HC, Lavery LA, van Schie CH, Boulton AJ, Harkless LB. Off-loading the diabetic foot wound: a randomized clinical
trial. Diabetes Care 2001;24:1019-22.
The total contact cast (TCC) heals ∼90% of neuropathic foot ulcers by 12 weeks (average healing time of 6 weeks).
Results of 9 TCC Studies
Average Healing Time:43.73 daysPercent Healed:
88.9%Helm 1984; Sinacore 1987; Walker 1987; Mueller 1989; Meyerson 1992; Birke 1992; Lavery 1997; Armstrong 2001; Birke 2002

Page 4
TCC - Average Outcomes of Studies by Helm 1984; Meyerson 1992; Walker 1987; Birke 1992;
Sinacore 1987; Lavery 1997; Armstrong 2001; Mueller 1989; Birke 2002
Apligraf - Veves, Falanga, et al; Graftskin, a Human Skin Equivalent…, Diabetes Care 2001, 24:290-295.
Dermagraft - Marston, Hanft, et al; The efficacy and safety of Dermagraft…, Diabetes Care 2003, 26:1701-05.
Regranex - Kantor, Margolis; Expected Healing Rates for Chronic Wounds, Wounds 2000, 12:155-158
Slide Courtesy of Dr Greg Bohn
Comparison of Diabetic Wound Treatments
140
44
8484
50.0%
88.9%
30.0%
56.0%
0
20
40
60
80
100
120
140
160
Total Contact Cast Apligraf Dermagraft Regranex
Day
s to
Hea
lin
g
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Per
cen
tag
e H
eale
d
Avg Days to Heal Percent Healed
Use of Pressure Offloading Devices in Diabetic Foot Ulcers
Do we practice what we preach? Wu SC, Jensen JL, Weber AK, DPM, Robinson DE, DPM,3 and
Armstrong DG. Diabetes Care. 2008 November; 31(11): 2118–2119
Of the 895 respondents who treat diabetic foot ulcers, shoe modifications (41.2%, P < 0.03) were the most common form of offloading
15.2% of the centers reported use of removable cast walkers
Total contact casts were used by only 1.7% of the centers.
Use of Pressure Offloading Devices in Diabetic Foot Ulcers
Do we practice what we preach?
58.1% (520 centers) did not consider TCCs as the gold standard to offload the noninfectedplantar diabetic foot
45.5% of the centers nationwide reported no use of TCCs
Page 5
Use of Pressure Offloading Devices in Diabetic Foot Ulcers
Do we practice what we preach?
Reasons for Not using TCC’s► patient tolerance (55.3%)
► time needed to apply the cast (54.3%)
► cost of materials (31.6%)
► reimbursement issues (27.5%)
► familiarity with method of application (25%)
► customizing parts (20.9%)
► staffing/ordering supplies (15.2%)
► clinician coverage (10.6%).
Off-loading the diabetic foot wound: A randomized clinical trial.
Armstrong DG, Nguyen HC, Lavery LA, van Schie CH, Boulton AJ, Harkless LB., Diabetes Care. 2001 Jun;24(6):1019-22
Compared the effectiveness of total-contact casts (TCC), removable cast walkers (RCW), and half-shoes to heal neuropathic foot ulcerations in individuals with diabetes
The proportions of healing for patients treated with TCC, RCW, and half-shoe were 89.5, 65.0, and 58.3%, respectively
TCC seems to heal a higher proportion of wounds in a shorter amount of time than two other widely used off-loading modalities, the RCW and the half-shoe.
Outcome and recurrence rate of diabetic foot
ulcers treated by a total contact castMatricali GA, Deroo K, Dereymaeker G., Foot Ankle Int. 2003 Sep;24(9):680-4.
Examined healing and final outcome after TCC
22-month period, 15 consecutive patients with a total of 17 ulcers started treatment with a TCC. Three ulcers were lost to follow-up (FU). Average FU was 91 weeks.
TCC proved to be a very effective tool for healing neuropathic foot ulcers, but the recurrence rate and frequency of other complications remained very high. (8 out of 12)
Difficult to achieve reliable (secondary) preventive general foot care, and to prescribe and manufacture reliable footwear.
Page 6
Total Contact Casting of the Diabetic Foot in Daily PracticeA prospective follow-up study
Nabuurs-Franssen MH, et al. Diabetes Care February 2005 vol. 28 no. 2 243-247
98 consecutive patients casted and followed until healing; all had polyneuropathy, 44% had PAD, and 29% had infection (PEDIS grade2)
90% of all nonischemic ulcers without infection and 87% with infection healed in the cast (NS).
New ulcers, all superfical, developed in 9% and preulcerativelesions in 28% of the patients while in the cast. All complication wounds healed within 13 days
In patients with PAD but without critical limb ischemia, 69% of the ulcers without infection and 36% with infection healed (P < 0.01).
Diabetic Peripheral Polyneuropathy
The absence of two of five sensory modalities:
Vibration sensation using the 128-Hz tuning fork
Light touch
Sharp-Dull discrimination
Achilles tendon reflex
Semmes Weinstein 10-g monofilament >2 sites tested
Schaper NC: Diabetic foot ulcer classification system for research purposes: a progress report on criteria for including patients in research studies. Diabetes Metab Res Rev 20 (Suppl. 1):S90–S95, 2004
Critical Limb Ischemia
Ankle pressure <50 mmHg
Toe pressure <30 mmHg
TcPo2 < 30 mmHg)
Moderate PAD absence of both pedal pulses
and/or presence of intermittent claudication
and/or ankle brachial index <0.9
and/or toe brachial index <0.6
and/or TcPo2 30–60 mmHg
Page 7
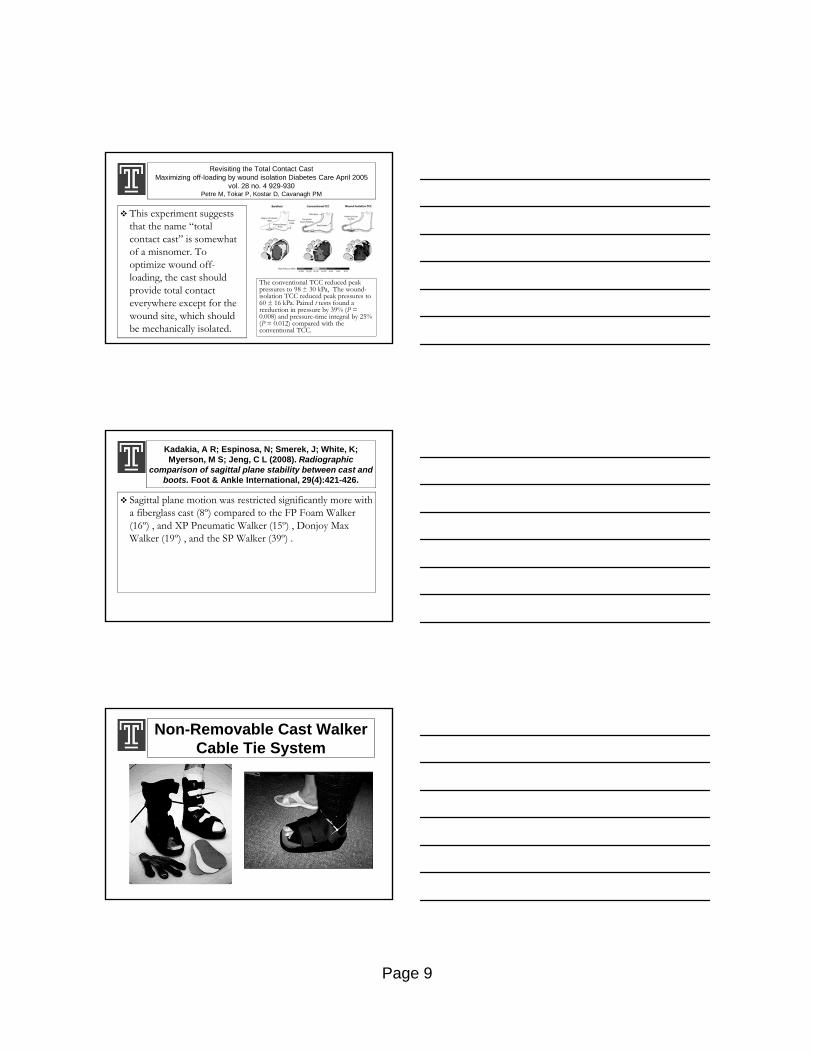
Total Contact Casting of the Diabetic Foot in Daily PracticeA prospective follow-up study
Nabuurs-Franssen MH, et al. Diabetes Care February 2005 vol. 28 no. 2 243-247
Three total contact casting modalities were used: a nonremovable TCC, a removable TCC (RCC), and a shoe-model cast (SMC) that could not be removed by the patient. These casts were applied using a modification of the technique described by Kominsky (13), and the choice of cast was based on both patient and cast characteristics
Cast Criteria
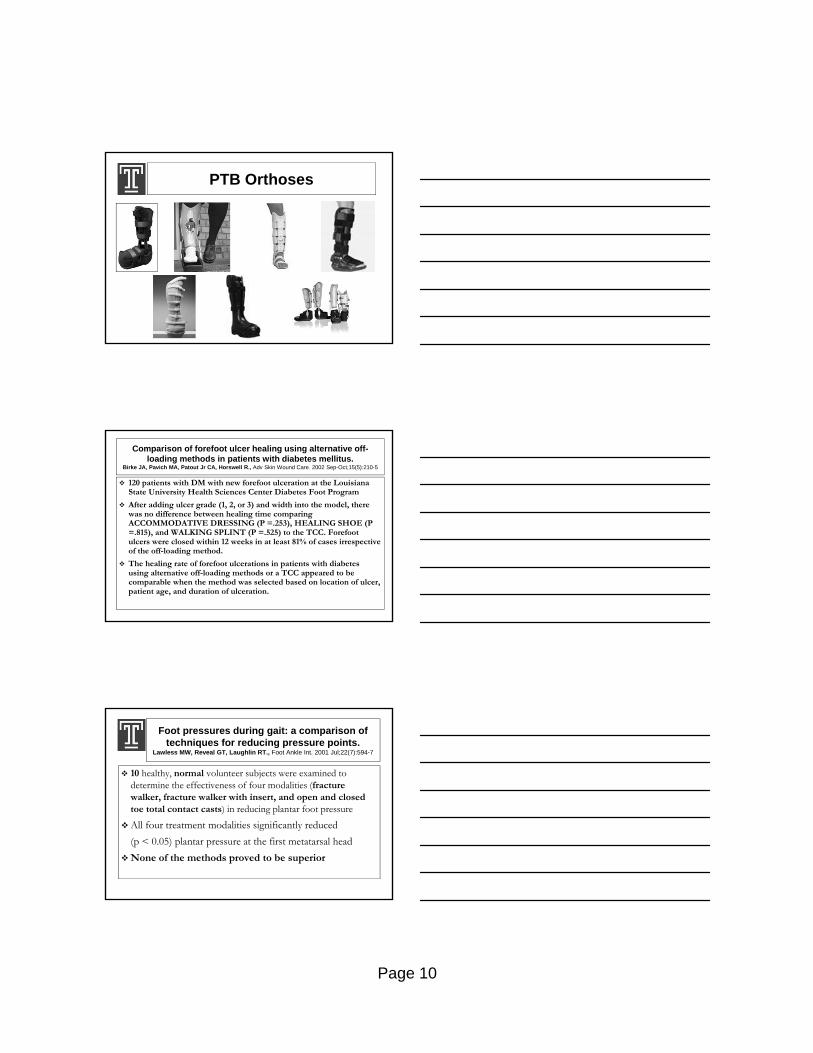
Results
pnp, presence of peripheral neuropathy, no signs of infection of PAD; inf, presence of infection, no signs of PAD; pad, presence of PAD, no signs of infection; inf + pad, presence of both infection and PAD

Page 8
Fife CE, et al; “Why is it so hard to do the right thing in wound care” Wound Rep
Reg : 18 p 154-158 2010
6% DFU patients had “Gold Standard” TCC used
Cost of care was half that of those that did not
TCC is time consuming and poorly reimbursed
Bilaminate skin reimbursed more generously
17% VLU patients received adequate compression
Inadequate reimbursement
Lack of familiarity with Clinical practice Guidelines
TCC - Average Outcomes of Studies by Helm 1984; Meyerson 1992; Walker 1987; Birke 1992; Sinacore 1987; Lavery 1997; Armstrong 2001; Mueller 1989; Birke 2002
Apligraf - Veves, Falanga, et al; Graftskin, a Human Skin Equivalent…, Diabetes Care 2001, 24:290-295.Dermagraft - Marston, Hanft, et al; The efficacy and safety of Dermagraft…, Diabetes Care 2003, 26:1701-05.Regranex - Kantor, Margolis; Expected Healing Rates for Chronic Wounds, Wounds 2000, 12:155-158
Slide Courtesy Dr. Greg Bohn
TCC Systems
Page 9
Revisiting the Total Contact CastMaximizing off-loading by wound isolation Diabetes Care April 2005
vol. 28 no. 4 929-930Petre M, Tokar P, Kostar D, Cavanagh PM
This experiment suggests that the name “total contact cast” is somewhat of a misnomer. To optimize wound off-loading, the cast should provide total contact everywhere except for the wound site, which should be mechanically isolated.
The conventional TCC reduced peak pressures to 98 ± 30 kPa, The wound-isolation TCC reduced peak pressures to 60 ± 16 kPa. Paired t tests found a reeduction in pressure by 39% (P = 0.008) and pressure-time integral by 25% (P = 0.012) compared with the conventional TCC.
Kadakia, A R; Espinosa, N; Smerek, J; White, K; Myerson, M S; Jeng, C L (2008). Radiographic
comparison of sagittal plane stability between cast and boots. Foot & Ankle International, 29(4):421-426.
Sagittal plane motion was restricted significantly more with a fiberglass cast (8º) compared to the FP Foam Walker (16º) , and XP Pneumatic Walker (15º) , Donjoy Max Walker (19º) , and the SP Walker (39º) .
Non-Removable Cast WalkerCable Tie System
Page 10
PTB Orthoses
Comparison of forefoot ulcer healing using alternative off-loading methods in patients with diabetes mellitus.
Birke JA, Pavich MA, Patout Jr CA, Horswell R., Adv Skin Wound Care. 2002 Sep-Oct;15(5):210-5
120 patients with DM with new forefoot ulceration at the Louisiana State University Health Sciences Center Diabetes Foot Program
After adding ulcer grade (1, 2, or 3) and width into the model, there was no difference between healing time comparing ACCOMMODATIVE DRESSING (P =.253), HEALING SHOE (P =.815), and WALKING SPLINT (P =.525) to the TCC. Forefoot ulcers were closed within 12 weeks in at least 81% of cases irrespective of the off-loading method.
The healing rate of forefoot ulcerations in patients with diabetes using alternative off-loading methods or a TCC appeared to becomparable when the method was selected based on location of ulcer, patient age, and duration of ulceration.
Foot pressures during gait: a comparison of techniques for reducing pressure points.
Lawless MW, Reveal GT, Laughlin RT., Foot Ankle Int. 2001 Jul;22(7):594-7
10 healthy, normal volunteer subjects were examined to determine the effectiveness of four modalities (fracture walker, fracture walker with insert, and open and closed toe total contact casts) in reducing plantar foot pressure
All four treatment modalities significantly reduced
(p < 0.05) plantar pressure at the first metatarsal head
None of the methods proved to be superior
Page 11
Pneumatic bracing and total contact casting have equivocal effects on plantar pressure relief.
Hartsell HD, Fellner C, Saltzman CL., Foot Ankle Int. 2001 Jun;22(6):502-6.
Compared plantar pressures produced in healthy subjects wearing a Running Shoe(RS), Total Contact Cast (TCC) and 'customized' pre-fabricated Pneumatic Walking Brace (PWB) [Aircast™]
Unloading of the forefoot was 63.72% for the TCC and 58.77% for the PWB, respectively
Comparison of Offloading Treatments
Lavery LA, Lavery DC, Vela SA, Quebedeaux TL: Reducing dynamic foot pressures in high risk diabetic subjects with foot ulcerations; A comparison of treatments. Diabetes Care. 19(8),August 1996. pp818-821Lavery LA, Lavery DC, Vela SA, Quebedeaux TL: Reducing dynamic foot pressures in high risk diabetic subjects with foot ulcerations; A comparison of treatments. Diabetes Care. 19(8),August 1996. pp818-821
Prefabricated Aircast™ Pneumatic Walker vs Standardized Shoe and TCC
kPakPa
Baunhauer JF, Wervey R, McWilliams J, Harris GF, Shereff MJ: A comparison study of plantar foot pressure in a standardized shoe, TCC, and prefabricated pneumatic walking brace. Foot and Ankle Int, 18(1) Jan 1997. pp26-33
Baunhauer JF, Wervey R, McWilliams J, Harris GF, Shereff MJ: A comparison study of plantar foot pressure in a standardized shoe, TCC, and prefabricated pneumatic walking brace. Foot and Ankle Int, 18(1) Jan 1997. pp26-33
1st MPJ1st MPJ 3rd MPJ3rd MPJ 5th MPJ5th MPJ 5th MTB5th MTB HeelHeel

Page 12
Removable Cast Walker vs. TCC
N/cm²N/cm²
Pollo FE, Crenshaw MS, Brodsky MD, Kirksey BS: Plantar Pressures in Total Contact Casting Verses a Diabetic Walking Boot. Baylor University Medical Center, Dallas, TX. Accepted for presentation, Annual
Meeting of the Orthopedic Research Society, San Francisco, Feb 25-28, 2001
Pollo FE, Crenshaw MS, Brodsky MD, Kirksey BS: Plantar Pressures in Total Contact Casting Verses a Diabetic Walking Boot. Baylor University Medical Center, Dallas, TX. Accepted for presentation, Annual
Meeting of the Orthopedic Research Society, San Francisco, Feb 25-28, 2001
Evaluation of Removable and Irremovable cast walkers in the healing of diabetic foot wounds: a randomized controlled trial. Armstrong DG, Lavery LA, Wu S, Boulton AJ. Diabetes Care, March 2005.
RESEARCH DESIGN AND METHODS-- 50 patients randomly assigned to two groups: an RCW or a RCW wrapped with a cohesive bandage (Instant Total Contact Cast or iTCC) Subjects were evaluated for 12 weeks or healing
RESULTS--An intent-to-treat analysis showed that a higher proportion of patients had ulcers that were healed at 12 weeks in the iTCC group than in the RCW group (82.6 vs. 51.9%, P = 0.02). Of the patients with ulcers that healed, those treated with an iTCC healed significantly sooner (18.7 vs. 15.2 days, P = 0.02).
Armstrong DG, Lavery LA, et al. Activity Patterns of Patients With Diabetic Foot Ulceration: Patients with active ulceration may not adhere to
a standard pressure offloadingregimen. Diabetes Care, Vol. 26, No. 9, September 2003
20 pts.
Recorded total steps per day measured by a waist-worn computerized accelerometer vs. an RCW-mounted accelerometer
1,219 ± 821 steps taken per patient per day
Only 28% of total daily activity was recorded wearing their RCW
Only 30% of the patients recorded more steps on than off
However those patients only wore the device a total of 60% of the total steps they took
Page 13
A randomized trial of two irremovable off-loading devices in the management of plantar neuropathic diabetic foot
ulcerations. Katz IA, Harlan A, Miranda-Palma B, Prieto-Sanchez L, et. al. Diabetes Care, March 2005.
RESEARCH DESIGN AND METHODS--In a prospective, randomized, controlled trial, 41 consecutive diabetic patients with neuropathic plantar foot ulcers were randomly assigned to one of two groups: an irremovable RCW (iTCC) or a standard TCC. Primary outcome measures: ulcers healed at less than or equal to 12 weeks, healing rates, complication rates, cast placement/removal times, and costs.
RESULTS-- Proportions of patients healed within 12 weeks in the iTCC and TCC groups were 94 and 93%, respectively, when patients who were lost to follow-up were excluded. Healing rates were statistically equivalent in the two groups, as were complication rates
The iTCC took significantly less time to place and remove than the TCC. Also an overall lower cost associated with the use of the iTCC compared with the TCC.
An Off-the-Shelf Instant Contact Casting Device for the Management of Diabetic Foot Ulcers: A randomized prospective trial versus traditional
fiberglass cast Diabetes Care March 2007 vol. 30 no. 3 586-590Piaggesi A. et al.
No statistical difference observed in healing rates between groups A (TCC) and B (DM Walker), (95 vs. 85%), healing time (6.5 ±4.4 vs. 6.7 ± 3.4 weeks), and adverse events (6 vs 4) n=40
► Group B, was 78% less expensive compared with group A (P < 0.001)
► Time required for application reduced by 77% and removal 58% compared to group A (P < 0.001)
► Patients’ satisfaction with the treatment was higher in group B (P < 0.01)
Effectiveness of Removable Walker Cast Versus Nonremovable Fiberglass Off-Bearing Cast in the Healing of Diabetic Plantar Foot Ulcer
A randomized controlled trial. Faglia E, et al.Diabetes Care July 2010 vol. 33 no. 7 1419-1423
45 diabetic patients with nonischemic, noninfected neuropathic plantar ulcers were randomly assigned for treatment with a total contact cast [TCC] group or walker cast (Stabil-D group).
Ulcer surface decreased from 1.41 to 0.21 cm2 (P < 0.001) in the TCC group and from 2.18 to 0.45 cm2 (P < 0.001) in the Stabil-D group (P = 0.722).
73.9% in the TCC group and 72.7% in the Stabil-D group achieved healing (P = 0.794).
Average healing time was 35.3 ± 3.1 and 39.7 ± 4.2 days in the TCC and Stabil-D group, respectively (P = 0.708).

Page 14
Stabil-D Orthosis
Total Contact CastIndications
Plantar ulceration Wagner grade I and II,
UTHSC grade A0, 1, 2, or 3
Neuropathic, pressure, traumatic
Avoid: Arterial, Venous
Neuropathic fracture (Charcot)
Post-reconstructive surgery
Sinacore DR: Total contact casting for diabetic neuropathic ulcers. Phys Ther. 1996;76:286-295.
Total Contact CastContraindications
Acute infection
Fever
Palpable lymph nodes
Deep sinus tract or narrow deep wound
Perfuse drainage
Active dermatitis
Excessive/Fluctuating edema
Claustrophobia
Known non-compliance
Arterial insufficiency
ABI <0.8
Wagner Grade III, IV, V None of these are absolute
contraindications to the use of a removable cast walker
Page 15
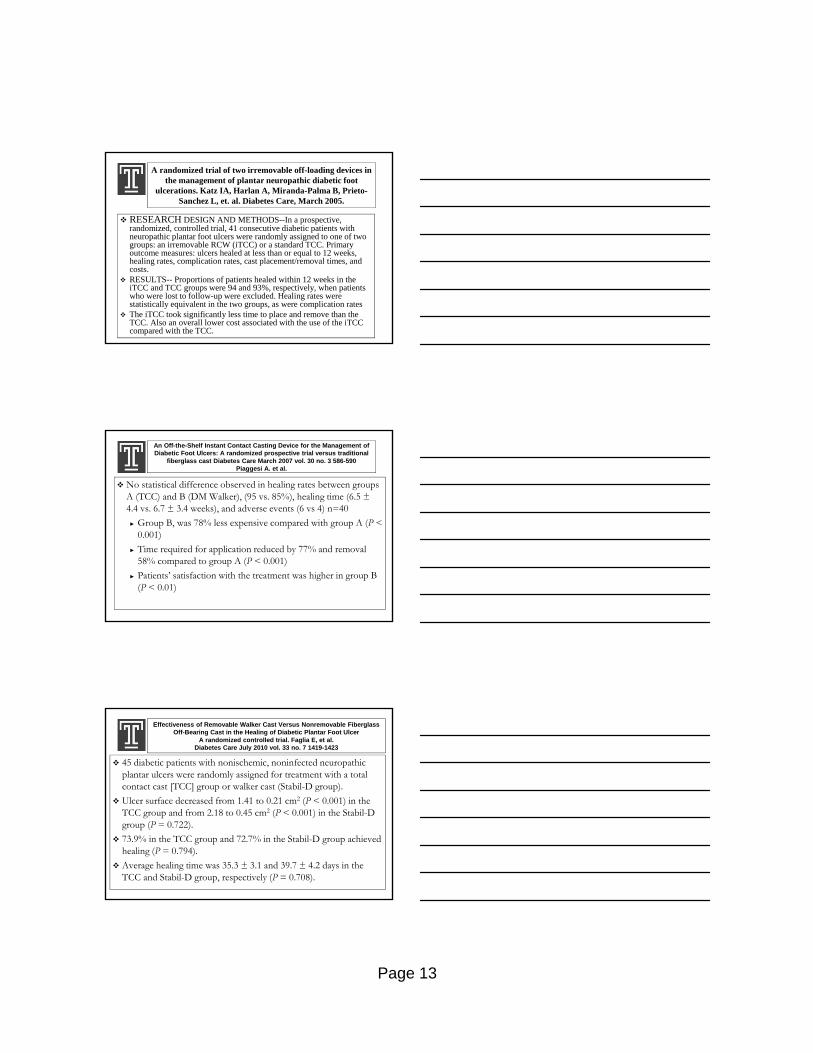
Total Contact CastStockinette, Foam, Light Dressing
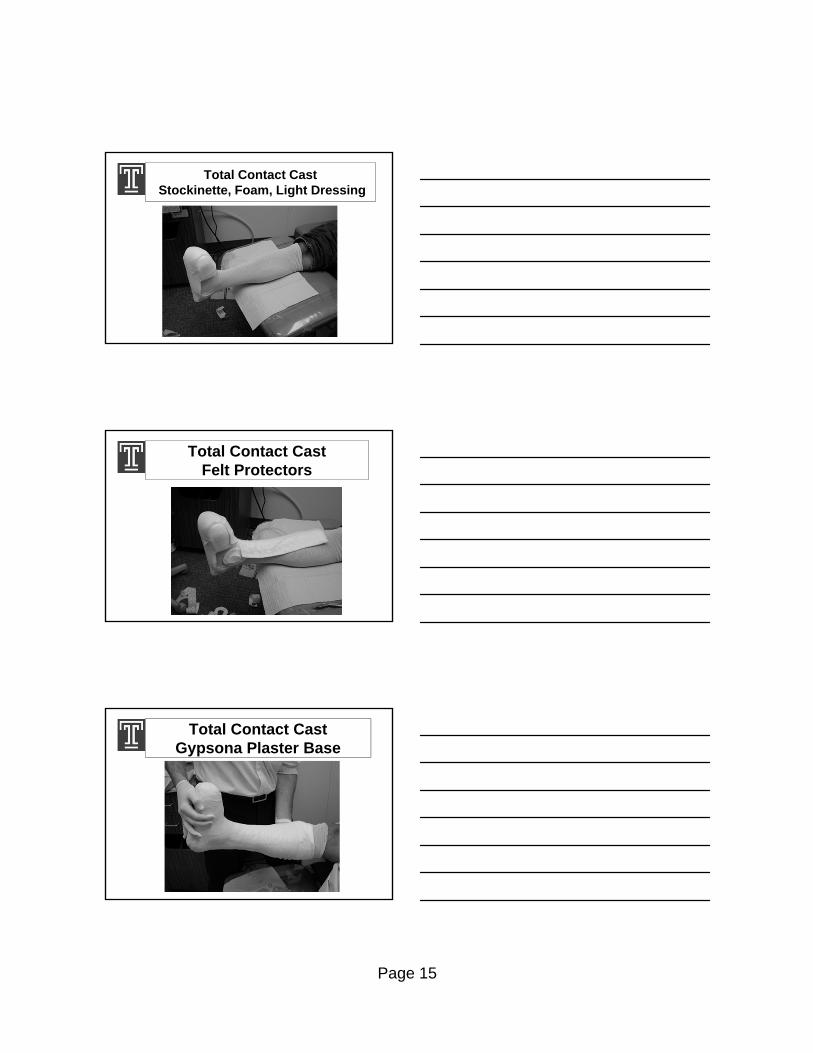
Total Contact CastFelt Protectors
Total Contact CastGypsona Plaster Base

Page 16
Total Contact CastFiberglass Reinforcement
Wound Isolation TCCM Petre, P Tokar, D Kostar, PR Cavanagh
Diabetes Care 28:929-930, 2005
Skive the Foam to Create a Cavity That is More Bowl-like than Cylindrical
TCC Systems
Page 17
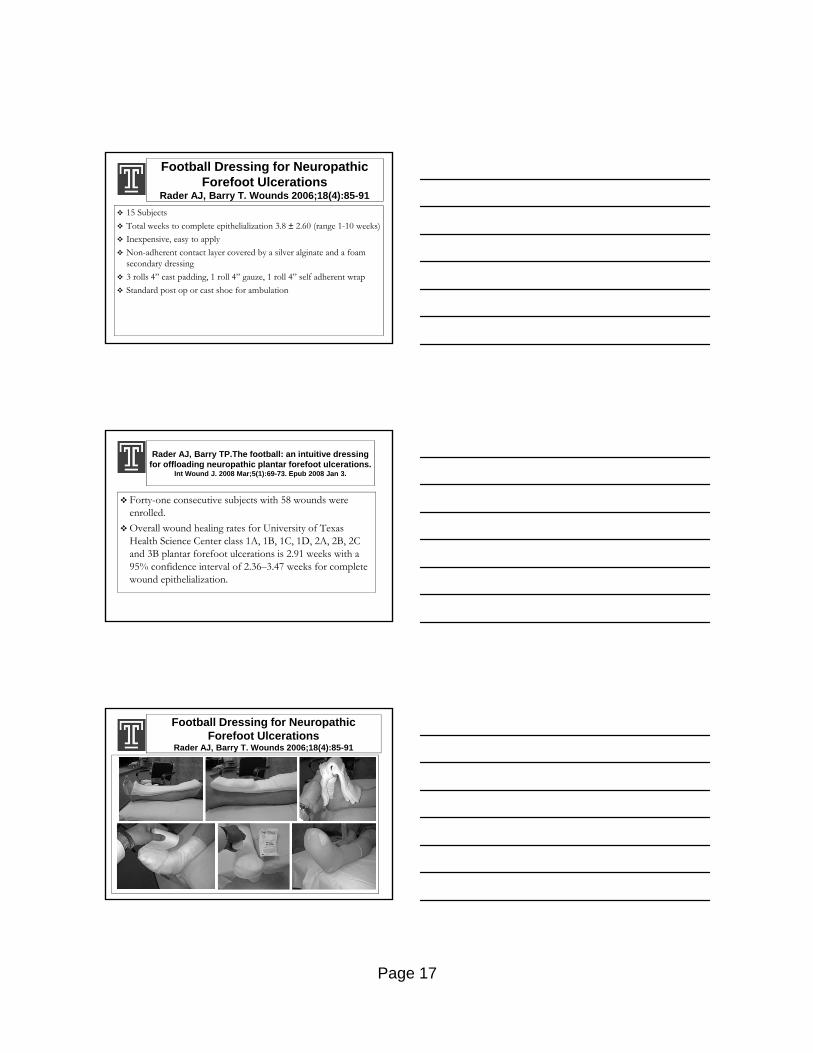
Football Dressing for Neuropathic Forefoot Ulcerations
Rader AJ, Barry T. Wounds 2006;18(4):85-91
15 Subjects
Total weeks to complete epithelialization 3.8 ± 2.60 (range 1-10 weeks)
Inexpensive, easy to apply
Non-adherent contact layer covered by a silver alginate and a foam secondary dressing
3 rolls 4” cast padding, 1 roll 4” gauze, 1 roll 4” self adherent wrap
Standard post op or cast shoe for ambulation
Rader AJ, Barry TP.The football: an intuitive dressing for offloading neuropathic plantar forefoot ulcerations.
Int Wound J. 2008 Mar;5(1):69-73. Epub 2008 Jan 3.
Forty-one consecutive subjects with 58 wounds were enrolled.
Overall wound healing rates for University of Texas Health Science Center class 1A, 1B, 1C, 1D, 2A, 2B, 2C and 3B plantar forefoot ulcerations is 2.91 weeks with a 95% confidence interval of 2.36–3.47 weeks for complete wound epithelialization.
Football Dressing for Neuropathic Forefoot Ulcerations
Rader AJ, Barry T. Wounds 2006;18(4):85-91

Page 18
Football Dressing for Neuropathic Forefoot Ulcerations
Rader AJ, Barry T. Wounds 2006;18(4):85-91