2875
TRANSCRIPT

of a single detector have to be always kept in mind when dealing with very high gradient or very small field sizes formed withmMLC, but within these limitations it can be still used for the verification of these fields.
Author Disclosure: F. Araki, None; S. Tajiri, None; H. Tominaga, None; K. Kawasaki, None; K. Kogo, None; M. Yoshitani,None; L. Muller, None.
2874 Clinical Feasibility of PET/CT Image Guidance After Proton Radiotherapy
H. A. Shih, K. Parodi, H. Paganetti, S. Michaud, J. S. Loeffler, T. F. DeLaney, N. J. Liebsch, J. E. Munzenrider, A. J.Fischman, T. Bortfeld
Massachusetts General Hospital, Boston, MA
Background: Irradiation with high energy protons creates positron emitters such as 11C (t1⁄2 � 20.38 minutes) in target tissues.Detection of this transient radioactivity may be a method for visualizing proton radiation delivered.
Purpose/Objective(s): To evaluate the clinical feasibility of PET/CT imaging as a non-invasive, in-vivo method of treatmentverification following proton radiotherapy.
Materials/Methods: Nine patients undergoing fractionated proton radiation therapy were imaged on a commercial PET/CTscanner following completion of one proton radiation treatment session. Anatomical locations of proton radiation included threecranial bases, four spines (cervicothoracic, two lumbar, and sacral), one orbit, and one eye. Irradiation was delivered in one ortwo fields. Total fraction dose ranged from 1.8 to 10 GyE. PET image acquisition time was 30 minutes and limited to the regionof treatment. For all patients but one, measured PET/CT images were co-registered to the radiation planning CT for comparisonwith (1) the planned dose and (2) its corresponding expected PET image derived from CT-based Monte Carlo calculationsincorporating functional information of tissue-specific perfusion properties. In the case of an ocular melanoma, correlationbetween treatment and imaging position was deduced from radio-opaque reference clips placed in proximity to the target.
Results: All patients were able to easily comply with instructions to proceed from the proton treatment facility immediatelyfollowing their treatment to the PET/CT scanner. In all cases, imaging was initiated within 20 minutes after completion ofradiotherapy. Treatment position was replicated at the PET/CT scan. Based upon the first patient imaged, the importance ofaccuracy of patient set up was recognized and the subsequent 7 patients were imaged with the use of the same custom madetreatment immobilization devices. For the last patient with an ocular melanoma, treatment was delivered with the patient undereyelid retraction and visual fixation on a positioned light. The patient was subsequently imaged in an approximate replicatedeye orientation based upon his recall. The length of PET imaging time made exact set up for this patient impractical becauseof risk for corneal injury with prolonged eyelid retraction and discomfort of continuous visual fixation. Good correlation ofproton radiation delivery field with PET image was obtained in all 9 patients. The best co-registration of images was achievedin the cranial base cases consistent with the greater precision in immobilization inherent to this region. Agreement up to 1–2mm was observed between measurement and prediction, for example within irradiated targets of the clivus or posterior wall ofthe nasal cavity. Both spatial and intensity signal of acquired PET images matched well with the CT-based Monte Carlocalculations.
Conclusions: PET/CT imaging promptly following proton radiation delivery is clinically feasible with good accuracy oftreatment set up replication and image co-registration. Optimizations of this system are underway. This method of treatmentverification may potentially be applied to improving strategies of highly conformal treatment delivery in complex cases suchas in the presence of tissue heterogeneity or metallic implants.
Author Disclosure: H.A. Shih, None; K. Parodi, None; H. Paganetti, None; S. Michaud, None; J.S. Loeffler, None; T.F.DeLaney, None; N.J. Liebsch, None; J.E. Munzenrider, None; A.J. Fischman, None; T. Bortfeld, None.
2875 A Novel Water-Clear, Low-Modulus Bolus Material
J. P. Kirkpatrick1, F. R. Irani2, S. E. Johnston2, A. M. Stalnecker2, T. M. Cooney2, D. L. Georgas1, M. Oldham1
1Duke University Medical Center, Durham, NC, 2Duke University, Durham, NC
Background: Bolus materials are essential tools in radiation therapy, permitting higher surface doses in megavoltage photontreatments and shallower treatment depths in electron therapy. However, most products are not transparent and even thin slabsmay obscure underlying skin structures and set-up marks. These materials also suffer from some combination of odor, volatility,plasticizer migration and/or excessive stiffness.
Purpose/Objective(s): To develop a transparent, low-modulus, stable and odorless material for use as a bolus in radiationtherapy.
Materials/Methods: Candidate constituent materials were selected based on superior stability, clarity, processability andsafety. Mechanical properites were evaluated using a tensile rheometer. Clarity was assessed by the ability to read 12-pointnewsprint through a 1-cm slab of bolus. CT numbers were measured using a CT scanner, and the electron density and effectiveZ calculated from the composition.
Results: A series of soft, water-clear, odorless, colorless elastomeric materials was formulated. Print could be read through allspecimens and underlying landmarks easily discerned, unlike conventional products (Figure 1. below) The materials were stableover a broad temperature range and did not exhibit plasticizer loss or migration, maintaining legible markings from waterproofmarkers for weeks. Tensile modulus and ultimate elongation ranged from 39 t0 122 MPa and from 65 to 165%, respectively.CT numbers ranged from 130 to 160 HU. Calculated mean Z and electron density for these formulations were 5.4 and 3.05x1023 e-/cm3 compared to 7.42 and 3.34 x 1023 e-/cm3 for water. Thus, the current formulations would need to be utilzed atslightly greater thicknesses to achieve build-up equal to water-equivalent materials.
Conclusions: This novel bolus material offers superior clarity, stability and aesthetic properties compared with commerciallyavailable products. Work is underway to fully characterize and optimize the balance of dosimetrc and mechanical properties.
S704 I. J. Radiation Oncology ● Biology ● Physics Volume 66, Number 3, Supplement, 2006
Author Disclosure: J.P. Kirkpatrick, None; F.R. Irani, None; S.E. Johnston, None; A.M. Stalnecker, None; T.M. Cooney, None;D.L. Georgas, None; M. Oldham, None.
2876 A New Method for Real-Time Confirmation of Irradiated Area of Therapeutic Photon Beams
K. Maruyama1, F. Matsubayashi2, T. Magara1, H. Kojima1, M. Ishigami1, K. Hayakawa1,3, M. Hashimoto4
1Graduate School of Medical Science, Kitasato University, Sagamihara, Japan, 2Department of Radiology, KitasatoUniversity Hospital, Sagamihara, Japan, 3Kitasato University School of Medicine, Sagamihara, Japan, 4Department ofRadiology, Chiba University Hospital, Chiba, Japan
Background: External irradiation of energetic photons is used in cancer therapy. There are established methods to estimate theabsorbed dose in the target area, determined by therapeutic planning. It is possible to confirm the irradiated area in advance andin the follow-up, however, no established method is available to confirm it during irradiation therapy.
Purpose/Objective(s): We propose a new method utilizing positron production by incident photons in order to measure theirradiated area directly. This study is to evaluate the method theoretically and to estimate its feasibility by measurements.
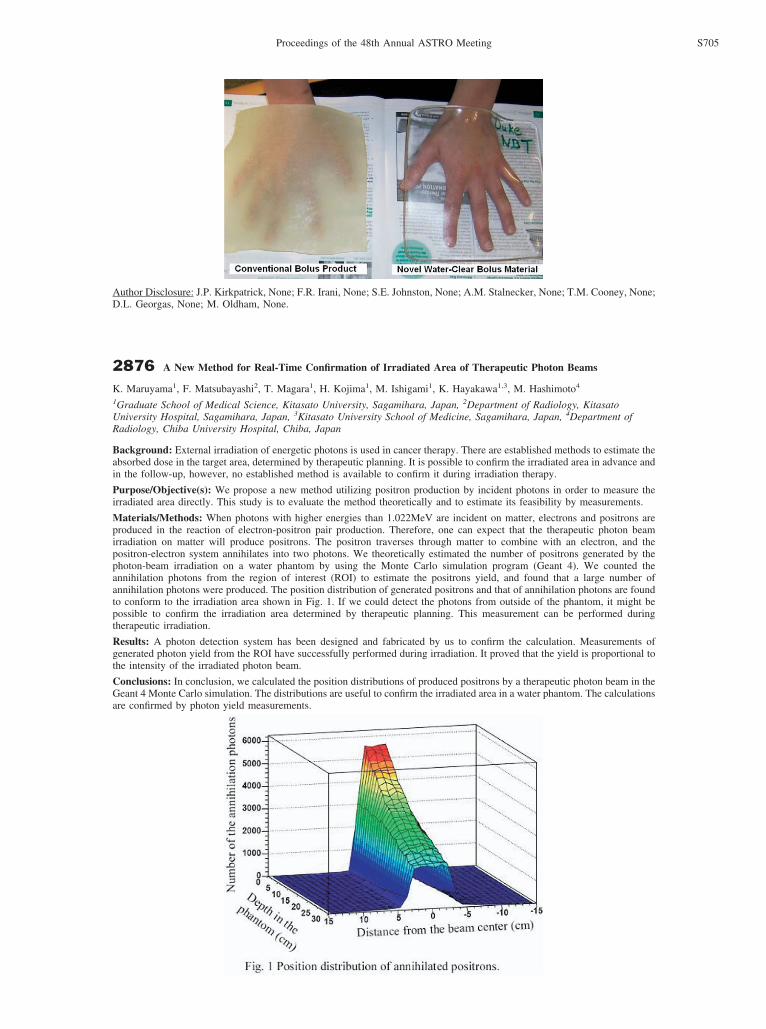
Materials/Methods: When photons with higher energies than 1.022MeV are incident on matter, electrons and positrons areproduced in the reaction of electron-positron pair production. Therefore, one can expect that the therapeutic photon beamirradiation on matter will produce positrons. The positron traverses through matter to combine with an electron, and thepositron-electron system annihilates into two photons. We theoretically estimated the number of positrons generated by thephoton-beam irradiation on a water phantom by using the Monte Carlo simulation program (Geant 4). We counted theannihilation photons from the region of interest (ROI) to estimate the positrons yield, and found that a large number ofannihilation photons were produced. The position distribution of generated positrons and that of annihilation photons are foundto conform to the irradiation area shown in Fig. 1. If we could detect the photons from outside of the phantom, it might bepossible to confirm the irradiation area determined by therapeutic planning. This measurement can be performed duringtherapeutic irradiation.
Results: A photon detection system has been designed and fabricated by us to confirm the calculation. Measurements ofgenerated photon yield from the ROI have successfully performed during irradiation. It proved that the yield is proportional tothe intensity of the irradiated photon beam.
Conclusions: In conclusion, we calculated the position distributions of produced positrons by a therapeutic photon beam in theGeant 4 Monte Carlo simulation. The distributions are useful to confirm the irradiated area in a water phantom. The calculationsare confirmed by photon yield measurements.
S705Proceedings of the 48th Annual ASTRO Meeting