3 architectural design and - nmbl · en 3 architectural design and function of human back muscles...
TRANSCRIPT

En
I
SE
CT
IO
N
57
3 Architectural Design and Function of Human Back Muscles
C H A P T E R Anita Vasavada, PhD
Samuel R. Ward, PT, PhD Scott Delp, PhD
Richard L. Lieber, PhD
Spinal muscles generate movements of the spine and provide the stability needed to protect vital anatomic structures. Muscles must work in coordination with the rest of the neu-romusculoskeletal system (i.e., vertebrae, tendons, ligaments, and the nervous system) to provide these functions. Large movements of the head require appropriate muscle strength, vertebral geometry (e.g., facet joint orientation), ligament compliance, and neural control. The spinal muscles have been described as one of three subsystems (the others are the passive spinal column and neural control) that must work together to stabilize the spine.1
Dysfunction of the spinal musculature is hypothesized to cause various pathologic conditions, such as segmental instability, low back or neck pain, and degenerative disc syndromes. The mechanisms that relate muscle function (or dysfunction) to pathologic processes are unclear, however. Some of the factors that lead to pathologic processes may be elucidated by biomechanical analyses of spine kinematics along with the associated tissue strains and loads. These analyses rely on accurate knowledge of muscle forces, moment arms, and activation patterns to calculate loads and displace-ments, but such values are frequently unavailable for spinal muscles. Often, spinal muscles are ignored or overly simplified (e.g., modeled as one “lumped” muscle) because the anatomy of these muscles is considered too complex to represent realistically. The complex anatomy and architecture of spinal muscles profoundly influence their function, however, and analyses that incorporate these details are required to provide the information necessary to predict more accurately the role of the muscles in spinal function and dysfunction.
This chapter begins with a description of the important and often neglected principles of skeletal muscle architecture and the way in which architecture determines muscle function. Specific information about the anatomy and architecture of the spinal musculature is provided when such information is available. The chapter concludes with a presentation of the implications of spinal muscle anatomy and architecture for motor control and injury.
Muscle Architecture
Skeletal muscle is highly organized at the microscopic level, as evidenced by classic studies that have elucidated the properties of skeletal muscle fibers. With few exceptions, the arrange-ment of muscle fibers within and between muscles has received much less attention. The microscopic arrangement of muscle fibers relative to the axis of force generation is known as the architecture of a muscle.2 Although muscle fiber size (which is directly proportional to force generation) is relatively con-sistent among muscles of different sizes, architectural differ-ences between muscles show much more variability and more strongly affect function. Muscle architecture is a primary determinant of muscle function, and understanding this structure-function relationship has great practical impor-tance. This understanding not only clarifies the physiologic basis for production of force and movement but also provides a scientific rationale for surgery. Muscle architectural studies also provide guidelines for electrode placement during electromyographic measures of muscle activity, explain the mechanical basis of muscle injury during movement, and aid in the interpretation of histologic specimens obtained from muscle biopsies.
Basic Architectural Definitions
The various types of architectural arrangement are as numer-ous as the muscles themselves. For discussion purposes, we describe three general classes of muscle fiber architecture. Muscles composed of fibers that extend parallel to the force-generating axis of the muscle are described as having a parallel or longitudinal architecture (Fig. 3–1A). Muscles with fibers that are oriented at a single angle relative to the force-generating axis are described as having unipennate architec-ture (Fig. 3–1B). The angle between the fiber and the force-generating axis has been measured at resting length in mammalian muscles over different designs and varies from about 0 to 30 degrees. Most muscles fall into the third and most general category, multipennate muscles—muscles
Herkowitz_Chapter 3_main.indd 57 6/4/2010 2:39:08 PM

En
58 BASIC SCIENCE
Pennation angle (θ) is measured by determining the average angle of the fibers relative to the axis of force generation of the muscle. Usually only the pennation angle of fibers on the superficial muscle surface is measured; however, this is only an estimate because pennation angles may vary from superfi-cial to deep and from proximal to distal. This superficial to deep variation in pennation has been documented in several spinal muscles (see later). Although more sophisticated methods could be developed for measurement of pennation angle, it is doubtful they would provide a great deal more insight into muscle function because variations in pennation angle may not strongly affect function.2
Muscle length is defined as “the distance from the origin of the most proximal muscle fibers to the insertion of the most distal fibers.”4 Fiber length represents the number of sarco-meres in series, and experimental evidence suggests that muscle fiber length is proportional to fiber contraction veloc-ity.3,5 Muscle length and fiber length are not the same because there is a variable degree of “stagger” seen in muscle fibers as they arise from and insert onto tendon plates (see Fig. 3–1B). Muscle fiber length can be determined only by microdissec-tion of individual fibers from fixed tissues or by laborious identification of fibers by glycogen depletion on serial sections along the length of the muscle.6 Unless investigators are explicit when they refer to muscle fiber length, they are prob-ably referring to muscle fiber bundle length (also known as fascicle length) because it is extremely difficult to isolate intact fibers, which run from origin to insertion, especially in mam-malian tissue.6,7
Experimental studies of mammalian muscle suggest that individual muscle fibers do not extend the entire muscle
constructed of fibers that are oriented at several angles relative to the axis of force generation (Fig. 3–1C).
These three designations are oversimplified, but they provide a vocabulary with which to describe muscle designs. Because fibers may not be oriented along any of the classic anatomic axes, determination of muscle architecture is impos-sible from a single biopsy specimen or images obtained by magnetic resonance imaging (MRI), computed tomography (CT), or ultrasonography because these methods cannot account for variations in fiber length and orientation changes that occur along the muscle length. Other methods have been developed to characterize the architectural properties of skel-etal muscle.
Experimental Determination of Skeletal Muscle Architecture
Quantitative studies of muscle architecture were pioneered by Gans and colleagues,2,3 who developed precise methodology for defining muscle architecture based on microdissection of whole muscles. The parameters usually included in an archi-tecture analysis are muscle length, fiber or fascicle length, pennation angle (i.e., the fiber angle relative to the force-generating axis), and physiologic cross-sectional area (PCSA). Typically, muscles are chemically fixed in formalin to maintain fiber integrity during dissection. The muscles should be chem-ically fixed while attached to the skeleton to preserve their physiologic length, or physiologic length in the skeleton should be noted. After fixation, muscles are dissected from the skeleton, their mass is determined, and their pennation angle and muscle length are measured.
FIGURE 3–1 Artist’s conception of three general types of skeletal muscle architecture. A, Longitudinal architecture, in which muscle fibers run parallel to the force-generating axis of the muscle. In this case, the natural example is the biceps brachii. B, Unipennate architecture, in which muscle fibers run at a fixed angle relative to the force-generating axis of the muscle. Here the example is the vastus lateralis muscle. C, Multipennate architecture, in which muscle fibers run at several angles relative to the force-generating axis of the muscle. The example here is the gluteus medius muscle. FL, fiber length; ML, muscle length.
FL
FL
Bicepsmuscle
ML = FL
Vastuslateralis
ML
ML
Gluteusmedius
A B C
Herkowitz_Chapter 3_main.indd 58 6/4/2010 2:39:10 PM

En
3 Architectural Design and Function of Human Back Muscles 59
I
SE
CT
IO
N
force relative to a muscle with the same mass and fiber length but with a 0-degree pennation angle.
Mechanical Properties of Muscles with Different Architectures
As stated earlier, muscle force is proportional to PCSA, and muscle velocity is proportional to fiber length. By stating that velocity is proportional to fiber length, it is implicit that the total excursion (active range) of a muscle is also proportional to fiber length. It is important to understand how these two architectural parameters, PCSA and fiber length, affect muscle function.
Comparison of Two Muscles with Different Physiologic Cross-Sectional Areas
Suppose that two muscles have identical fiber lengths and pennation angles but one muscle has twice the mass (equiva-lent to saying that one muscle has twice the number of fibers and twice the PCSA). Also suppose that the two muscles have identical fiber type distributions and that they generate the same force per unit area. The functional difference between these two muscles is shown in Figure 3–2. The muscle with
length and may not even extend the entire length of a fasci-cle.6,7 Detailed studies of individual muscle fiber length have not been conducted in human spinal muscles, but studies in feline neck muscles illustrate that muscle fibers are often arranged in series, ending in tendinous inscriptions within the muscle or terminating intrafascicularly.8,9 Although the terms fiber length and fascicle length are often used interchangeably, technically they are identical only if muscle fibers span the entire length of a fascicle. In muscle architecture studies, bundles consisting of 5 to 50 fibers are typically used to esti-mate fiber length, which may be reported as either fiber length or fascicle length.
The final experimental step required to perform architec-tural analysis of a whole muscle is to measure sarcomere length within the isolated fibers. This is necessary to compen-sate for differences in muscle length that occur during fixation. In other words, to conclude that a muscle has “long fibers,” one must ensure that it truly has long fibers and not that it was fixed in a highly stretched position corresponding to a long sarcomere length. Similarly, muscles with “short fibers” must be investigated further to ensure that they were not simply fixed at a short sarcomere length.
To permit such conclusions, fiber length measurements should be normalized to a constant sarcomere length, which eliminates fiber length variability owing to variation in fixa-tion length. Fiber (or fascicle) lengths are usually normal-ized to the optimal sarcomere length, the length at which a sarcomere generates maximum force. This normalized length is referred to as optimal fiber (or fascicle) length and pro-vides a reference value that can be related back to the physi-ologic length if the relationship between muscle length and joint position is noted. Based on measured architectural parameters and joint properties, the relationship between sarcomere length and joint angle can be calculated. Because sarcomere length strongly influences muscle force genera-tion, an understanding of the relationship between sarco-mere length change and movement has been used in many studies to provide added understanding of muscle design.10-14
The PCSA is calculated next. Theoretically, the PCSA rep-resents the sum of the cross-sectional areas of all the muscle fibers within the muscle, and it is the only architectural param-eter that is directly proportional to the maximum tetanic tension generated by the muscle. The PCSA is almost never the same as the cross-sectional area of the muscle as measured in any of the traditional anatomic planes, as would be obtained using a noninvasive imaging method such as MRI, CT, or ultrasonography. It is calculated as muscle volume divided by fiber length and has units of area.
Because fibers may be oriented at a pennation angle relative to the axis of force generation, it is believed that not all of the fiber tensile force is transmitted to the tendons. Specifically, if a muscle fiber is pulling with x units of force at a pennation angle θ relative to other muscle axis of force generation, only a component of muscle fiber force (x • cosθ) would actually be transmitted along the muscle axis. The volume/length is often multiplied by cosineθ (pennation angle) and is the calculation of PCSA. In other words, pennation causes a loss of muscle
FIGURE 3–2 Schematic drawing of two muscles with different physiologic cross-sectional areas (PCSAs) but identical mass. A, Comparison of isometric length-tension properties. B, Comparison of isotonic force-velocity properties. The effect of increased PCSA with identical fiber length is to shift the absolute length-tension and force-velocity curves to higher values, but with retention of the same range and intrinsic shape.
A
B
Large PCSA
Small PCSA
120
100
80
60
40
20
005 10 15 20 25 30 35 40
Max
imum
tens
ion
(N)
Muscle velocity (mm/s)
120
100
80
60
40
20
005 10 15 20 25 30 35 40
Max
imum
tens
ion
(N)
Muscle length (mm)
Large PCSA
Small PCSA
Herkowitz_Chapter 3_main.indd 59 6/4/2010 2:39:10 PM

En
60 BASIC SCIENCE
through observations of the cat semitendinosus muscle:4 When the proximal semitendinosus head was activated, its Vmax was 224 mm/sec, whereas when only the distal semiten-dinosus head was activated, its Vmax was 424 mm/sec. When both heads were activated simultaneously, the whole muscle Vmax was 624 mm/sec, or the sum of the two velocities. The values for Vmax were proportional to the different lengths of the proximal and distal heads. These data indicate that the longer the fibers in series (equivalent to saying the greater number of sarcomeres in series), the greater the muscle con-traction velocity. As expected, maximum isometric tension was essentially the same regardless of which activation pattern was used.
Interplay of Muscle Architecture and Moment Arms
In addition to its architecture, the potential moment generated by a muscle is influenced by its moment arm. Moment arm, the “mechanical advantage” of a muscle, is the distance from the line of action of a muscle to the joint axis of rotation and is directly related to a muscle’s change in length with joint rotation.15 In other words, the amount of muscle fiber length change that occurs as a joint rotates and, consequently, the range of joint angles over which the muscle develops active force depend on the muscle moment arm. This idea can be explained by comparing the situation in which two muscles with identical fiber lengths have different moment arms at a joint (Fig. 3–4). In the case in which the moment arm is greater, the muscle fibers change length much more for a given change in joint angle compared with a muscle with a shorter moment arm. As a result, the range of joint motion over which the muscle develops active force is smaller for the muscle with the larger moment arm despite the fact that the muscular properties of both muscles are identical.
The architectural design of a muscle and its placement in relation to the skeletal geometry are important determinants of its function. Although muscles with longer fibers can gener-ate force over a greater range of lengths than muscles with shorter fibers (see Fig. 3–3A), this does not indicate that muscles with longer fibers are associated with joints that have larger ranges of motion. Muscles that appear to be designed for speed based on their long fibers may not actually produce large joint velocities if they are placed in the skeleton with a very large moment arm because joint excursion and joint angular velocity are inversely related to moment arm. A large moment arm results in a large joint moment, so that the muscle would be highly suited for torque production but at low angular velocities. Similarly, a muscle that appears to be designed for force production because of the large PCSA, if placed in position with a very small moment arm, may actu-ally produce high joint excursions or angular velocities. Differences between muscle-joint systems require complete analysis of joint and muscular properties. These interrelated concepts of architecture and moment arm (gross anatomy) must be considered when examining the design and function of spinal muscles.
twice the PCSA has an isometric length-tension curve with the same shape, but it is amplified upward by a factor of 2. The maximal tetanic tension (Po) of the larger muscle would be twice that of the smaller muscle. Similarly, comparison of isotonic force-velocity curves indicates that the differences between muscles would simply be an upward shift in Po for the larger muscle.
Comparison of Two Muscles with Different Fiber Lengths
If two muscles have identical PCSAs and pennation angles but fiber lengths that differ, the schematic in Figure 3–3 shows that the effect of increased fiber length is to increase muscle excur-sion and velocity. Peak force of the length-tension curves is identical between muscles, but the range of lengths over which the muscle generates active force is different. For the same reason that an increased fiber length increases active muscle range of the length-tension relationship, it results in an increase in the maximum velocity (Vmax) of the muscle. Exper-imental support for this concept was obtained indirectly
FIGURE 3–3 Schematic drawing of two muscles with different fiber lengths but identical physiologic cross-sectional areas. A, Comparison of isometric length-tension properties. B, Comparison of isotonic force-velocity properties. The effect of increased fiber length is to increase the absolute range of the length-tension curve and absolute velocity of the force-velocity curve, but with retention of the same peak force and intrinsic shape. Dotted vertical line in B shows that, for an equivalent absolute velocity, the muscle with longer fibers generates a greater force.
A
B
120
100
80
60
40
20
05 10 15 20 25 30 35 40
Max
imum
tens
ion
(N)
Muscle velocity (mm/s)
120
100
80
60
40
20
05 10 15 20 25 30 35 40
Max
imum
tens
ion
(N)
Muscle length (mm)
Long fibers
Short fibers
Long fibers
Short fibers
Herkowitz_Chapter 3_main.indd 60 6/4/2010 2:39:10 PM

En
3 Architectural Design and Function of Human Back Muscles 61
I
SE
CT
IO
N
muscles as described earlier, which ultimately influences control and injury mechanisms.
Spinal muscles can be divided into intrinsic muscles, which connect vertebrae with each other, and extrinsic muscles, which attach vertebrae to the limbs. Embryologically, intrinsic muscles originate from the epimere, and extrinsic muscles originate from the hypomere. Intrinsic muscles have innerva-tions from the dorsal rami of spinal nerves, whereas extrinsic muscles are innervated from the ventral rami of spinal nerves and generally have functions related more to the proximal portion of limbs or respiration.
Intrinsic Spinal Muscles Found in the Lumbar, Thoracic, or Cervical Spine
Intrinsic muscles of the spine are dominated by the erector spinae, a group of interdigitated muscles that spans the entire length of the spine, from the sacrum and iliac crest to the skull. Another important group of muscles, the multifidus, are shorter and deeper and are described in more detail later. In the thoracolumbar region, the erector spinae and multifidus muscles constitute the bulk of the spinal musculature. These two distinct functional units have large differences in innerva-tion that probably result in significant functional differences,16 although the detailed biomechanical function of these groups remains only partially elucidated.17 Lying deep to the multifi-dus are even smaller muscles, the rotators, interspinales, and intertransversarii. The cervical region is composed of other intrinsic muscles unique to it (see later).
The erector spinae are commonly considered to be com-posed of three muscles; from medial to lateral, they are the spinalis, longissimus, and iliocostalis. The anatomy and archi-tecture of these muscles vary among different levels of the spine. The words “lumborum,” “thoracis,” “cervicis,” and “capitis” are appended to the muscle name to describe the anatomy more accurately. Although there are varying defini-tions of the composition of the erector spinae, a study by MacIntosh and Bogduk17 provides the most comprehensive descriptive anatomy of the lumbar erector spinae, and Delp and colleagues18 provided the first architectural measurements of these muscles. The continuation of the erector spinae in the cervical region was discussed briefly by Kamibayashi and Richmond.19
The spinalis muscle is the most medial division of the erector spinae. MacIntosh and Bogduk17 described the spinalis as mostly aponeurotic in the lumbar region, but Delp and col-leagues18 obtained architecture measurements from the spina-lis in the thoracic region (Table 3–1). The spinalis is generally absent in the cervical region.
Caudal to rostral, the longissimus consists of the longissimus thoracis, cervicis, and capitis; the longissimus thoracis is divided into lumbar and thoracic portions. The lumbar fascicles of the longissimus thoracis (longissimus thoracis pars lumborum) are composed of five bands that arise from the lumbar transverse processes and attach in a caudal fashion onto the iliac crest (Fig. 3–5A). Each band arising from vertebra L1 to L4 is actu-ally a small fusiform muscle that has an elongated and flat-tened caudal tendon of insertion. Bands from more rostral
Anatomy and Architecture of Spinal Musculature
The architecture of spinal muscles is complex and dramatically different from the architecture of limb muscles. Instead of distinct tendinous attachments to bone, many spinal muscles have very little tendon at their ends and have a complex arrangement of internal tendons and aponeuroses. Their attachments are generally broad; many spinal muscles branch and have insertions at multiple vertebral levels. Some spinal muscles have short fascicles and high pennation, whereas others have long, parallel fascicles. All of these factors affect the force-generating and moment-generating capacity of
FIGURE 3–4 Effect of changing moment arm on active range of motion. In this example, a schematic muscle (shown as a sarcomere in series with some tendon) is attached with two different moment arms. A, 40-degree range of motion for “normal” muscle (from 40 to 80 degrees). B, Moment arm increase results in decrease in range of motion to 25-degree muscle (from 50 to 75 degrees). In B, the active range of motion is smaller because the moment arm is greater, and more sarcomere length change occurs for a given angular rotation. C, Comparison of force versus joint angle (range of motion) for muscles with short (dotted line) or long (solid line) moment arms.
Full flexion(θ = 40°)
Full extension(θ = 80°)
Full flexion(θ = 50°)
Full extension(θ = 75°)
Long moment armShort moment arm
1.0
0.5
0.030 40 50 60 70 80 90
Joint angle (degrees)
Rel
ativ
e m
uscl
e fo
rce
A
B
C
Herkowitz_Chapter 3_main.indd 61 6/4/2010 2:39:10 PM

En
62 BASIC SCIENCE
levels attach more medially on the iliac crest. The juxtaposi-tion of these caudally located tendons form the lumbar inter-muscular aponeurosis.
Fascicles of the thoracic component of longissimus thoracis (longissimus thoracis pars thoracis) arise from all thoracic transverse processes and most ribs and attach to lumbar spinous processes, the sacrum, or the ilium. These are long slender muscles with pronounced caudal tendons that juxta-pose to form the strong erector spinae aponeurosis (see LIA in Fig. 3–5B), which bounds the lumbar paraspinal muscles dorsally. In the upper thoracic and cervical region, the longis-simus cervicis connects transverse processes of thoracic and cervical vertebrae, whereas the longissimus capitis originates on transverse processes and inserts on the mastoid process of the skull (Fig. 3–6).
The lumbar fascicles of the iliocostalis lumborum (iliocosta-lis lumborum pars lumborum) lie lateral to the longissimus thoracis muscles arising from the tip of the transverse pro-cesses of vertebrae L1 to L4 in the lumbar region and are composed of four small, broad bands (see Fig. 3–5C) that attach to the thoracolumbar fascia and the iliac crest. The thoracic fascicles of the iliocostalis lumborum (iliocostalis lumborum pars thoracis) arise from ribs and attach to the iliac spine and crest, forming the lateral part of the erector spinae aponeurosis. In contrast to the more medially located longis-simus thoracis, the caudal tendons are less prominent, giving the iliocostalis lumborum a much more fleshy appearance. Caudal to rib 10, the iliocostalis lumborum and longissimus thoracis lie side by side, forming the erector spinae aponeuro-sis. Rostral to rib 9 or 10, the iliocostalis thoracis separates the iliocostalis lumborum and longissimus thoracis. In the upper thoracic and cervical region, the iliocostalis cervicis connects the ribs to the transverse processes of cervical vertebrae.
MacIntosh and Bogduk17 measured muscle and tendon lengths in the thoracic portions of the longissimus thoracis and iliocostalis lumborum (Table 3–2). Detailed architecture of the lumbar erector spinae, including muscle tendon and
From Delp SL, Suryanarayanan S, Murray WM, et al: Architecture of the rectus abdominis, quadratus lumborum, and erector spine. J Biomech 34:371-375, 2001; Ward, SR, Kim CW, Eng CM, et al: Architectural analysis and intraoperative measurements demonstrate the unique design of the multifidus for lumbar spine stability. J Bone Joint Surg Am 91:176-185, 2009.
TABLE 3–1 Architectural Data of Erector Spinae and Quadratus Lumborum*
MuscleMusculotendon Length (cm)
Muscle Length (cm)
Fascicle Length (cm)
Pennation Angle (°)
Sarcomere Length (µm)
Optimal Fascicle Length (cm)
Muscle Fiber Mass (g) PCSA (cm2)
Rectus abdominis 35.9 (1.9) 34.3 (2.7) 28.3 (3.6) 0 (0) 2.83 (0.28) 28 (4.2) 92.5 (30.5) 2.6 (0.9)
Quadratus lumborum (proximal)
11.7 (1.7) 10.7 (1.3) 7.3 (1.3) 7.4 (2.9) 2.39 (0.21) 8.5 (1.5) 13.3 (5.2) 1.6 (0.6)
Quadratus lumborum (distal)
9.3 (1.3) 8.1 (1.2) 4.7 (0.5) 7.4 (6.2) 2.37 (0.20) 5.6 (0.9) 7.3 (2.4) 1.2 (0.4)
Spinalis thoracis 24.7 (1.5) 18.2 (3.2) 5.2 (0.4) 16 (3.8) 2.26 (0.17) 6.4 (0.6) 10.2 (6) 1.6 (0.9)
Longissimus thoracis 42.6 (5.5) 34.7 (4.8) 9.6 (1.2) 12.6 (5.8) 2.31 (0.17) 11.7 (2.1) 73.4 (31) 5.9 (2.5)
Iliocostalis lumborum 43.8 (4.3) 33.1 (9) 12 (1.7) 13.8 (4.5) 2.37 (0.17) 14.2 (2.1) 60.9 (29.9) 4.1(1.9)
Multifidus NA NA 4.8 (1.7) 18.4 (4.2) 2.26 (0.18) 5.7 (1.8) 73 (12.4) 23.9 (8.4)
NA, not applicable; PCSA, physiologic cross-sectional area.*Table presents mean values (standard deviation).
FIGURE 3–5 A-D, Longissimus thoracis (medial division of erector spinae) schematic of lumbar (A) and thoracic (B) regions and iliocostalis lumborum (lateral division of erector spinae) schematic of lumbar (C) and thoracic (D) regions. ct, caudal tendon; LIA, lumbar intermuscular aponeurosis; mb, muscle belly; rt, rostral tendon. (From Bogduk N: A reappraisal of the anatomy of the human lumbar erector spinae. J Anat 131:525-540, 1980; MacIntosh JE, Bogduk N: The morphology of the lumbar erector spinae. Spine 12:658-668, 1987.)
LIA
Rt
Rt (rib 5)
Rt (rib 8)
Mb
Ct
Mb
Ct
A B
C D
2
Herkowitz_Chapter 3_main.indd 62 6/4/2010 2:39:12 PM

En
3 Architectural Design and Function of Human Back Muscles 63
I
SE
CT
IO
N
fascicle length, sarcomere lengths, and PCSAs, has been mea-sured (see Table 3–1).18 Fascicle lengths were found to be approximately 30% of muscle lengths in these muscles, and sarcomere lengths measured from cadavers in the supine posi-tion were generally shorter than the optimal length, which may imply that the erector spinae are capable of developing greater force in elongated positions (i.e., in flexion).
The lumbar multifidus muscles consist of multiple separate bands arising from each vertebral spinous process and lamina and inserting from two to four segments below the level of origin (Fig. 3–7B). The shortest fascicle of each muscle inserts onto the mammillary process of the vertebra located two seg-ments caudal, whereas longer, more superficial fascicles insert sequentially onto subsequent vertebrae three or more seg-ments lower (see Fig. 3–7). The shortest band of the multifidus arising from L1 inserts on L3, and subsequent bands insert sequentially on L4, L5, and the sacrum. Multifidus muscles
FIGURE 3–6 Posterior view of neck muscles. A, Left side shows superficial muscle, the trapezius. Splenius capitis, splenius cervicis, levator scapulae, and rhomboids lie underneath trapezius. B, Right side shows semispinalis capitis, longissimus capitis, and longissimus cervicis, which lie deep to splenius capitis. Left side shows semispinalis cervicis and suboccipital muscles, which lie under semispinalis capitis. OCI, obliquus capitis inferior; OCS, obliquus capitis superior; RCP maj, rectus capitis posterior major; RCP min, rectus capitis posterior minor. (Adapted from Gray H: Gray’s Anatomy. New York, Gramercy Books, 1977.)
Capitis
Trapezius
Spleniuscapitis
Spleniuscervicis
LevatorscapulaeRhomboids
A
OCS
RCPmaj
RCPmin
OCI
Semispinaliscervicis
Semispinaliscapitis
Longissimuscapitis
Longissimuscervicis
B
From MacIntosh JE, Bogduk N: The morphology of the lumbar erector spinae. Spine 12:658-668, 1987.
TABLE 3–2 Muscle and Tendon Length Data of Lumbar Erector Spinae
MuscleMuscle Belly Length (cm)
Rostral Tendon Length (cm)
Caudal Tendon Length (cm)
Longissimus thoracis pars thoracis
9-12 3-4 Up to 24
Iliocostalis lumborum pars thoracis
10-13 12-15 18-19
FIGURE 3–7 Schematic arrangement of multifidus muscle in cross section (A) and longitudinal section (B). (From Bogduk N: A reappraisal of the anatomy of the human lumbar erector spinae. J Anat 131:525-540, 1980.)
esa
liaMD(LT)
MFLD(IL)
fs fs
apIM
I
lia
L1
L2
L3
L4
L5
S
L1L1
L2L2
L3 L3
L4
L5
S
A
B
Herkowitz_Chapter 3_main.indd 63 6/4/2010 2:39:12 PM

En
64 BASIC SCIENCE
arising from lower lumbar vertebrae consist of fewer fascicles because the number of vertebrae caudal to the origin decreases.
All multifidus muscles that arise from a given level are innervated by the medial branch of the primary dorsal rami of the spinal nerve from a single segment (i.e., each band of multifidus muscle is innervated from a single dorsal ramus). In the cervical region, multifidus fascicles from the spinous processes and laminae of C2, C3, and C4 attach onto facet capsules of two adjacent vertebral articular processes from C4 to C7; fascicles from the spinous processes and laminae of C4 to C7 attach onto transverse processes of upper thoracic ver-tebrae.20 The principal action of the multifidus is extension, but the multisegmental nature of the muscle and the complex three-dimensional orientation in the craniocaudal and medio-lateral directions renders this statement a gross oversimplifica-tion.21 The multifidus is not considered a prime mover of the spine; rather, its function is likely to produce small vertebral adjustments.
A study of the multifidus muscle revealed three major design factors that suit it well for stabilizing the lumbar spine.22 First, the architecture of the multifidus is highly pennated with fibers extending only about 20% of the length of the fascicles. Numerous muscle fibers are packed into a small volume, and even though the multifidus has a smaller mass compared with several other lumbar extensors, it is predicted to create the greatest lumbar extension force by a factor of 2 (see Table 3–1). Second, direct mechanical testing of the multifidus muscle cells and extracellular connective tissue revealed that although the multifidus fibers have the same mechanical properties as other limb muscles, the fiber bundles, which include extracel-lular connective tissue, are about twice as stiff as limb muscles. The multifidus has a high passive elastic capacity that would suit it for passively resisting flexion of the lumbar spine. Third, the multifidus muscle sarcomere length, measured intraopera-tively, is relatively short when the spine is extended, suggesting that the muscle gets stronger as it gets longer. In other words, as the spine flexes, multifidus force increases, suiting it to restore spine angles toward neutral or more extended positions.
Deep to the multifidus are smaller muscles that span one or two vertebral segments. The rotatores attach from caudal transverse processes to the base of rostral spines one or two segments away. Rotators are prominent in the thoracic region, although some authors claim they exist in the lumbar region.23,24 MacIntosh and colleagues25 did not find any muscles deep to the lumbar multifidus. The interspinalis and intertransversarii, found in the lumbar and cervical regions, connect the spines and transverse processes of adjacent vertebrae.
Intrinsic Spinal Muscles Specific to the Cervical Spine
Because of different functional demands in the cervical spine (e.g., large head movements), this region has additional intrin-sic muscles. Kamibayashi and Richmond19 provided details on neck muscle anatomy and quantitative architecture data of the neck muscles (Table 3–3).
Splenius Capitis and Cervicis
The splenius capitis originates at the spinous processes of the lower cervical and upper thoracic vertebrae and inserts on the skull near the mastoid process (see Fig. 3–6A). Contiguous, slightly deeper, and sometimes inseparable is the splenius cer-vicis, which originates on thoracic spinous processes and inserts on cervical transverse processes. Although the splenius capitis and splenius cervicis function in extension, lateral bending, and axial rotation, the splenius capitis is oriented more obliquely than the splenius cervicis, providing more axial rotation capacity for movements of the skull relative to the vertebrae. The fascicle lengths of the splenius capitis and splenius cervicis are similar, but their muscle tendon lengths are not similar; this occurs because the splenius capitis has short aponeuroses, whereas the splenius cervicis has long apo-neuroses (Fig. 3–8A).19
Semispinalis Capitis and Cervicis
The semispinalis capitis originates on the articular processes of the lower cervical vertebrae and transverse processes of the upper thoracic vertebrae and inserts medially on the skull between the inferior and superior nuchal line (see Fig. 3–6A). The semispinalis capitis is characterized by complex patterns of internal tendon and tendinous inscriptions in the medial portion, whereas fascicles in the lateral portion are uninter-rupted (see Fig. 3–8B).19 The semispinalis cervicis (deep to the semispinalis capitis) originates on thoracic transverse pro-cesses and inserts on cervical spinous processes from C2 to C5, with the bulk of its mass inserting on C2.
Longus Capitis and Colli
On the anterior side of the vertebral column, the longus capitis runs from the anterior surface of transverse processes to the baso-occiput (Fig. 3–9). Because it lies close to the vertebral bodies, it has only a small flexion moment arm; the supero-medial orientation could provide ipsilateral rotation. Its coun-terpart, the longus colli, has a more complicated structure. Some fibers run vertically along the anterior vertebral bodies, other fibers run superolaterally from thoracic vertebral bodies to lower cervical transverse processes, and others run supero-medially from transverse processes to the anterior vertebral bodies (see Fig. 3–9). Although all parts of the longus colli have small flexion moment arms, the superomedial and super-olateral portions would have ipsilateral and contralateral rota-tion moment arms. The longus capitis and longus colli are also characterized by an aponeurosis covering much of the super-ficial surface, from which fascicles have long tendons that attach to the vertebrae (Fig. 3–10).19
Suboccipital Muscles
The suboccipital muscles span the region between C2 and the skull (see Fig. 3–6B). The rectus capitis posterior major and minor connect the spinous processes of C2 and C1 with the skull. The obliquus capitis superior is oriented in a
Herkowitz_Chapter 3_main.indd 64 6/4/2010 2:39:12 PM

En
3 Architectural Design and Function of Human Back Muscles 65
I
SE
CT
IO
N
From Kamibayashi LK, Richmond FR: Morphometry of human neck muscles. Spine 23:1314-1323, 1998.
TABLE 3–3 Morphometric Parameters of Human Neck Muscles
Muscle N
MASS (G)Angle (°) Range
MUSCLE LENGTH (CM) NF Length (cm) Mean (SD)
PCSA (CM2)
Range Mean (SD) Range Mean (SD) Range Mean (SD)
Sternocleidomastoideus 9 21-50.5 40.4 (9) 0-20 16.5-21.2 19 (1.6) 10.8 (0.9) 1.81-5.26 3.72 (0.91)
Clavotrapezius 10.7-27.1 18.7 (4.5) 0-30 9-14.8 12 (1.9) 8.4 (2.1) 1.25-2.94 1.96 (0.62)
Acromiotrapezius 68.5-128.4 103.5 (23.5) 0-10 10-14.5 12.6 (1.7) 9.2 (1.8) 7.99-15.26 10.77 (2.38)
Rhomboideus 9 18.8-58.3 40.9 (15.6) 0-5 7.2 (2) 1.76-9.93 5.84 (2.77)
Minor 6.5-12 8.7 (1.9)
Major 5.3-13 8.2 (2.7)
Rectus capitis posterior major
9 1.4-5.5 3.5 (1.2) 0-5 3-4.8 3.7 (0.7) 0.44-1.45 0.93 (0.33)
Rectus capitis posterior minor
9 0.6-1.6 1 (0.3) 0-5 2.6-3.1 1 (0.2) 0.48-0.83 0.50 (0.19)
Obliquus capitis superior
8 1-3.7 2.5 (0.9) 0-20 4.3-5.7 2.5 (0.5) 0.29-1.59 1.03 (0.46)
Obliquus capitis inferior 9 2.1-8.1 5.1 (1.8) 0-5 3.6-5.4 4.4 (0.6) 3.8 (0.8) 0.69-1.73 1.29 (0.54)
Longus capitis 7 2.4-5.6 3.7 (1.2) 0-10 7.8-11.1 9.2 (1.4) 3.8 (1) 0.54-1.63 0.92 (0.35)
Splenius 9 21.6-59.3 42.9 (13.8) 0-5 9.5 (2.3) 2.57-5.48 4.26 (1.04)
Capitis 9.5-15 12.3 (1.5)
Cervicis 11.5-18.5 14.7 (2.3)
Semispinalis capitis 9 21.3-55.8 38.5 (9.4) 0-20 13-20 11.7 (1.9) 6.8 (1.7) 3.93-7.32 5.40 (1.30)
Scalenus anterior 9 5.7-12.4 5.6 (3) 0-20 5.5-7.8 6.8 (0.9) 4.2 (1.3) 0.37-4.51 1.45 (1.23)
Scalenus medius 9 5.6-14.5 10.6 (3.01) 0-30 6.8-9.5 8.1 (1) 5 (0.8) 1.00-3.34 2.00 (0.73)
Scalenus posterior 9 4-23.5 10.6 (7.7) 0-20 7-10 8 (1.1) 6.2 (2.1) 0.59-3.15 1.55 (0.90)
Levator scapulae 8 16.5-38.9 24.6 (8.3) 0-5 13.2-17.5 15.1 (1.6) 11.3 (3.1) 1.39-3.24 2.18 (0.80)
Values in each column represent the range or average of individual values computed on specimen at one time.NF Length, normalized fascicle length; PCSA, physiologic cross-sectional area.
FIGURE 3–8 Architecture of splenius capitis, splenius cervicis, and semispinalis capitis. A, Splenius capitis and splenius cervicis. Note aponeuroses at both ends of splenius cervicis. B, Semispinalis capitis. Medial portion is characterized by tendinous inscriptions and internal aponeuroses interrupting fascicles. (Adapted from Kamibayashi LK, Richmond FJR: Morphometry of human neck muscles. Spine 23:1314-1323, 1998.)
Spleniuscapitis
Spleniuscervicis
Aponeuroses
A
Semispinaliscapitis
Tendinousinscriptions
Internalaponeuroses
B
FIGURE 3–9 Anterior view of deep neck muscles: longus capitis, longus colli, and scalenes. Note three parts of longus colli: superior oblique, vertical, and inferior oblique. (Adapted from Gray H: Gray’s Anatomy. New York, Gramercy Books, 1977.)
Longuscapitis
Scalenusanterior
Longuscolli
Scalenusmedius
Scalenusposterior
Herkowitz_Chapter 3_main.indd 65 6/4/2010 2:39:13 PM

En
66 BASIC SCIENCE
The psoas is the largest muscle in cross section at the lower levels of the lumbar spine.28 Biomechanical analysis shows that the psoas has the potential to flex the lumbar spine laterally, generate compressive forces that increase stability, and create large anterior shear forces at L5 to S1.29 If the psoas were designed for lumbar spine motions, however, one would expect longer fascicles attaching more rostral segments because they would undergo larger excursion. The uniform fascicle lengths suggest that the psoas is actually designed to move the hip,27 and electromyographic studies confirm that its primary function is hip flexion.30
Extrinsic Muscles Linking Vertebrae or Skull to the Shoulder Girdle or Rib Cage
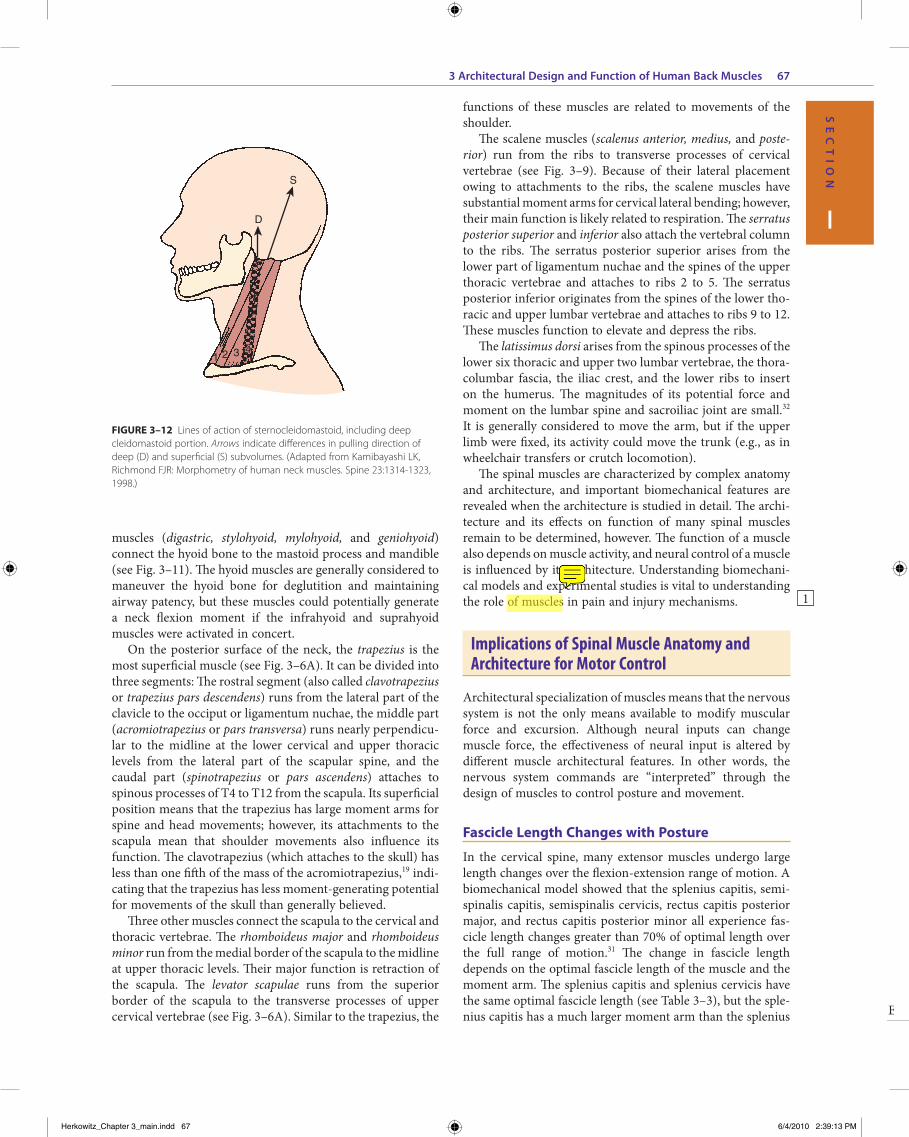
On the anterior and lateral surface of the neck, the sterno-cleidomastoid originates from the sternum and medial clavicle to attach on the skull at the mastoid process and superior nuchal line of the occiput (Fig. 3–11). Kamibayashi and Rich-mond19 divided this muscle into three subvolumes: sternomas-toid, cleidomastoid, and cleido-occipital. The fascicles on the superficial surface (sternomastoid and cleido-occipital por-tions) lie in parallel; however, the cleidomastoid portion on the deep surface, which runs from the clavicle to mastoid process, increases the proportion of muscle fascicles exerting force on the mastoid process (Fig. 3–12).19 Superficial inspec-tion of muscle architecture can neglect the arrangement of these deep fascicles, which would decrease the estimated moment-generating capacity of the sternocleidomastoid in biomechanical models by more than 30%.31 The sternocleido-mastoid has moment arms for flexion, contralateral rotation, and lateral bending and has been found to be active during movements in all three of these directions.
Also on the anterior surface of the neck, the infrahyoid muscles (sternohyoid, sternothyroid, thyrohyoid) link the hyoid bone, thyroid cartilage, and sternum, whereas the suprahyoid
superoinferior direction between the transverse process of C1 and the skull, and the obliquus capitis inferior runs primarily mediolaterally from the spinous process of C2 to the trans-verse process of C1. All four of these muscles can contribute to extension of the head with respect to the neck; in addition, the rectus capitis posterior major and the obliquus capitis inferior are oriented to produce ipsilateral rotation, and the lateral location of the obliquus capitis superior implies a lateral bending function. The obliquus capitis superior has an inter-nal tendon on the deep surface that causes some fascicles to have large pennation angles.19 On the ventral side, the rectus capitis anterior and rectus capitis lateralis are very small muscles that connect the skull to C1, presumably with (small) moment arms for flexion and lateral bending.
Extrinsic Muscles Linking Vertebrae to the Pelvis
The quadratus lumborum attaches from the iliolumbar liga-ment and iliac crest onto the 12th rib and transverse processes of L1 to L4. It assists in lateral bending of the lumbar spine. The proximal component of the quadratus lumborum (i.e., the set of fascicles running from the iliac crest to the 12th rib and L1) has a larger moment arm for lateral flexion and has longer fascicles than the distal component of the muscle. Electromyo-graphic evidence shows that the quadratus lumborum has a dominant role in spine stabilization.26
The psoas major attaches from the anterior surface of the transverse processes, the sides of vertebral bodies, and inter-vertebral discs of all lumbar vertebrae. Together with the iliacus, which arises from the ilium, they form the iliopsoas, which inserts on the lesser trochanter of the femur and is a major flexor of the thigh and trunk. Fascicles of the psoas generally have the same length, regardless of their level of origin. Because of their attachments to a common tendon, bundles from higher levels are more tendinous, whereas the bundle from L5 remains fleshy until it joins the common tendon.27
FIGURE 3–10 Architecture of longus capitis. A, Superficial surface, with long aponeurosis. B, Deep surface, with individual tendons to lower cervical vertebrae. (Adapted from Kamibayashi LK, Richmond FJR: Morphometry of human neck muscles. Spine 23:1314-1323, 1998.)
Longuscapitis
Aponeuroses
C3
C4
C5
C6A B
FIGURE 3–11 Lateral view of sternocleidomastoid and hyoid muscles. (Adapted from Gray H: Gray’s Anatomy. New York, Gramercy Books, 1977.)
Suprahyoids
Infrahyoids
Sterno-cleidomastoid
Herkowitz_Chapter 3_main.indd 66 6/4/2010 2:39:13 PM
En
3 Architectural Design and Function of Human Back Muscles 67
I
SE
CT
IO
N
functions of these muscles are related to movements of the shoulder.
The scalene muscles (scalenus anterior, medius, and poste-rior) run from the ribs to transverse processes of cervical vertebrae (see Fig. 3–9). Because of their lateral placement owing to attachments to the ribs, the scalene muscles have substantial moment arms for cervical lateral bending; however, their main function is likely related to respiration. The serratus posterior superior and inferior also attach the vertebral column to the ribs. The serratus posterior superior arises from the lower part of ligamentum nuchae and the spines of the upper thoracic vertebrae and attaches to ribs 2 to 5. The serratus posterior inferior originates from the spines of the lower tho-racic and upper lumbar vertebrae and attaches to ribs 9 to 12. These muscles function to elevate and depress the ribs.
The latissimus dorsi arises from the spinous processes of the lower six thoracic and upper two lumbar vertebrae, the thora-columbar fascia, the iliac crest, and the lower ribs to insert on the humerus. The magnitudes of its potential force and moment on the lumbar spine and sacroiliac joint are small.32 It is generally considered to move the arm, but if the upper limb were fixed, its activity could move the trunk (e.g., as in wheelchair transfers or crutch locomotion).
The spinal muscles are characterized by complex anatomy and architecture, and important biomechanical features are revealed when the architecture is studied in detail. The archi-tecture and its effects on function of many spinal muscles remain to be determined, however. The function of a muscle also depends on muscle activity, and neural control of a muscle is influenced by its architecture. Understanding biomechani-cal models and experimental studies is vital to understanding the role of muscles in pain and injury mechanisms.
Implications of Spinal Muscle Anatomy and Architecture for Motor Control
Architectural specialization of muscles means that the nervous system is not the only means available to modify muscular force and excursion. Although neural inputs can change muscle force, the effectiveness of neural input is altered by different muscle architectural features. In other words, the nervous system commands are “interpreted” through the design of muscles to control posture and movement.
Fascicle Length Changes with Posture
In the cervical spine, many extensor muscles undergo large length changes over the flexion-extension range of motion. A biomechanical model showed that the splenius capitis, semi-spinalis capitis, semispinalis cervicis, rectus capitis posterior major, and rectus capitis posterior minor all experience fas-cicle length changes greater than 70% of optimal length over the full range of motion.31 The change in fascicle length depends on the optimal fascicle length of the muscle and the moment arm. The splenius capitis and splenius cervicis have the same optimal fascicle length (see Table 3–3), but the sple-nius capitis has a much larger moment arm than the splenius
muscles (digastric, stylohyoid, mylohyoid, and geniohyoid) connect the hyoid bone to the mastoid process and mandible (see Fig. 3–11). The hyoid muscles are generally considered to maneuver the hyoid bone for deglutition and maintaining airway patency, but these muscles could potentially generate a neck flexion moment if the infrahyoid and suprahyoid muscles were activated in concert.
On the posterior surface of the neck, the trapezius is the most superficial muscle (see Fig. 3–6A). It can be divided into three segments: The rostral segment (also called clavotrapezius or trapezius pars descendens) runs from the lateral part of the clavicle to the occiput or ligamentum nuchae, the middle part (acromiotrapezius or pars transversa) runs nearly perpendicu-lar to the midline at the lower cervical and upper thoracic levels from the lateral part of the scapular spine, and the caudal part (spinotrapezius or pars ascendens) attaches to spinous processes of T4 to T12 from the scapula. Its superficial position means that the trapezius has large moment arms for spine and head movements; however, its attachments to the scapula mean that shoulder movements also influence its function. The clavotrapezius (which attaches to the skull) has less than one fifth of the mass of the acromiotrapezius,19 indi-cating that the trapezius has less moment-generating potential for movements of the skull than generally believed.
Three other muscles connect the scapula to the cervical and thoracic vertebrae. The rhomboideus major and rhomboideus minor run from the medial border of the scapula to the midline at upper thoracic levels. Their major function is retraction of the scapula. The levator scapulae runs from the superior border of the scapula to the transverse processes of upper cervical vertebrae (see Fig. 3–6A). Similar to the trapezius, the
FIGURE 3–12 Lines of action of sternocleidomastoid, including deep cleidomastoid portion. Arrows indicate differences in pulling direction of deep (D) and superficial (S) subvolumes. (Adapted from Kamibayashi LK, Richmond FJR: Morphometry of human neck muscles. Spine 23:1314-1323, 1998.)
S
D
1 2 3 44
1
Herkowitz_Chapter 3_main.indd 67 6/4/2010 2:39:13 PM

En
68 BASIC SCIENCE
vary by 2 to 3 cm but remain in the same direction throughout the range of motion (e.g., sternocleidomastoid, splenius capitis) (Fig. 3–15). For other muscles, the direction of moment arm changes with axial rotation. At the neutral position, the right rectus capitis posterior major has a right rotation moment arm; its magnitude increases in left rotated postures. When the head is rotated to the right, the moment arm decreases in magnitude and eventually changes to a left rotation moment arm. These results indicate that the rectus capitis posterior major has an axial rotation moment arm appropriate to restore the head to neutral posture from the most rotated head posi-tions. The moment arms of other muscles such as the semi-spinalis capitis and longissimus capitis show the same pattern, although their moment arms are smaller. The implication of these findings is that the moment arm provides a
cervicis. The splenius capitis undergoes larger fascicle length changes than the splenius cervicis over the same range of motion (Fig. 3–13).
The semispinalis capitis has shorter fascicle lengths, but also a smaller moment arm than the splenius capitis. The semispinalis capitis and splenius capitis experience similar, large fascicle length excursions over the range of flexion-extension motion (see Fig. 3–13). In both muscles, fascicle lengths are extremely short in extended postures; this implies that the central nervous system must compensate for the asso-ciated decrease in force-generating potential by increasing activation or recruiting other extensors of the neck.
Moment Arm Changes with Posture
Different parts of a muscle may have different moment arms, and the magnitude (and in some cases, direction) of these moment arms changes with posture. Muscles that cross mul-tiple joints (as most spinal muscles do) may have different mechanical functions at different joints. A biomechanical model of the neck muscles31 showed that the moment arm of the sternocleidomastoid varies dramatically for flexion-extension movements (Fig. 3–14). For motions of the upper cervical joints, the cleido-occipital segment of the sterno-cleidomastoid actually has an extension moment arm that increases in extended postures (topmost solid line in Fig. 3–14); the other two subvolumes of the sternocleidomastoid (which attach to the mastoid process) have very small moment arms. During flexion of the lower cervical joints, the flexion moment arm of the sternocleidomastoid increases. These results indicate that the function of the sternocleidomastoid depends highly on posture and the joints around which move-ment occurs. The change in sternocleidomastoid flexion moment arm in the lower cervical region indicates a destabi-lizing effect because it potentially increases the flexion moment–generating capacity of the muscle in flexed postures.
The same model31 also showed that for axial rotation of the upper cervical region, many muscles have moment arms that
FIGURE 3–13 Fascicle length excursions over range of neck flexion-extension motion superimposed on normalized muscle active force-length curve. (Adapted from Vasavada A, Li S, Delp S: Influence of muscle morphometry and moment arms on the moment-generating capacity of human neck muscles. Spine 23:412-421, 1998.)
0
0.2
0.4
0.6
0.8
1
0.4 0.6 0.8 1 1.2 1.4 1.6
Nor
mal
ized
forc
e
Normalized fascicle length
0
0.2
0.4
0.6
0.8
1
1.2
0.4 0.6 0.8 1 1.2 1.4 1.6
Nor
mal
ized
forc
e
Normalized fascicle length
Flexion-extensionAxial rotationLateral bending
Splenius cervicisSplenius capitisSemispinalis capitis
FIGURE 3–14 Sternocleidomastoid flexion-extension moment arms. Light lines indicate individual subvolumes (sternomastoid, cleidomastoid, and cleido-occipital), and dark lines indicate mass-weighted average. Solid line indicates moment arm for upper cervical region; dashed line refers to lower cervical region. (Adapted from Vasavada A, Li S, Delp S: Influence of muscle morphometry and moment arms on the moment-generating capacity of human neck muscles. Spine 23:412-421, 1998.)
Flexion Extension
Flexion-extension angle (deg)
Flexion
Extension
−40 −30 −20 −10 0 10 20 30 40 50−4
−3
−2
−1
0
1
2
3
4
Mom
ent a
rm (
cm)
Skull-C2C2-T1
Herkowitz_Chapter 3_main.indd 68 6/4/2010 2:39:13 PM

En
3 Architectural Design and Function of Human Back Muscles 69
I
SE
CT
IO
N
lumbar fascicles, electrodes placed at lumbar vertebral levels may not represent activity of fascicles directly attached to lumbar vertebrae. This could result in inaccurate estimation of lumbar joint and tissue loads.
Muscle Injury and Implications for Neck and Back Pain
Neck and back pain frequently begins with an injury, and in many cases muscle injury is involved. Injury to muscle fibers can occur as a result of trauma, disease, application of myo-toxic agents (e.g., local anesthetics), inflammatory processes, or intense exercise. The degree to which muscle injury relates to low back or neck pain is unknown. Muscle injury and the pain that accompanies it have been studied extensively, however.
Skeletal muscle injury and soreness frequently occur when a muscle is rapidly lengthened while it is activated. Active lengthening of muscle (also called eccentric contraction) has been used to study injuries in animals and humans for more than 20 years.
Muscle pain accompanying eccentric exercise peaks 24 to 48 hours after the exercise bout. Several studies have reported that eccentric exercise results in a significant increase in serum creatine kinase levels 24 to 48 hours after the exercise bout,35,36 and the increase may persist for 3 to 6 days, depending on the precise nature of the exercise. The appearance of creatine kinase in the serum is interpreted as an increased permeability or breakdown of the membrane surrounding the muscle cell.
Training prevents or at least attenuates the magnitude of muscle injury that occurs after eccentric exercise. This training effect is produced only after eccentric training of the specific muscle group being tested. In other words, general increased fitness neither prevents nor attenuates eccentric contraction–induced muscle injury.
Based on experimental studies of skeletal muscles directly subjected to eccentric exercise, it is thought that the early events that cause muscle injury are mechanical ones.37,38 During cyclic eccentric exercise of the rabbit tibialis anterior, significant mechanical changes were observed in the first 5 to 7 minutes of exercise.39 Other studies have revealed structural disruption of the cytoskeleton within the fibers at these earlier time periods40,41 that may provide further insights into the damage mechanism.
Animal and human studies have provided evidence for selective damage of fast fiber types after eccentric exercise.42-44 In human studies, this damage was confined to the type 2 muscle fibers in general; in animal studies, damage has been localized further to the type FG (often equated to type 2B) fast fiber subtype. Because FG fibers are the most highly fatigable muscle fibers,45 it has been speculated that the high degree of fatigability of these fibers may predispose them to injury. Several clinical studies have proposed that the fatigability of back muscles may be a predisposing factor to injury. It is dif-ficult to test this idea directly, however, because many other differences between FG fibers and other muscle fibers exist. Further studies are required to elucidate the basis for fiber
“self-stabilizing” function to assist the central nervous system in maintaining neutrally rotated (i.e., eyes forward) head posture. This function is particularly relevant in the upper cervical region because most axial rotation occurs between C1 and C2.
In the lumbar spine, posture also changes the mechanical function of erector spine muscles. McGill and colleagues33 measured the fiber angles of longissimus thoracic and iliocos-talis lumborum with the lumbar spine in neutral and fully flexed using high-resolution ultrasonography. They found that flexion changes the line of action of these muscles, decreasing their capacity to resist anterior shear forces. This finding is important because anterior shear loads are related to the risk of back injury.34
Electromyography
Knowledge of the complex spinal muscle anatomy is essential for accurate electromyography studies. These studies may be used to detect abnormal muscle activation patterns or to determine input to biomechanical models. MacIntosh and colleagues25 showed the medial fibers of the multifidus (i.e., the fibers immediately lateral to a given spinous process) arise from the spinous process directly above, whereas fibers from higher levels are more lateral. All the fibers of the multifidus arising from a particular vertebra are innervated by the same nerve. This unisegmental innervation has implications for diagnosis of zygapophyseal joint pain related to abnormal activity in the multifidus.
The detailed anatomy of the erector spinae provided by MacIntosh and Bogduk17 also provides important information for electromyography studies. Because thoracic fascicles of the longissimus thoracis and iliocostalis lumborum lie over the
FIGURE 3–15 Axial rotation moment arms for upper cervical region. (Adapted from Vasavada A, Li S, Delp S: Influence of muscle morphometry and moment arms on the moment-generating capacity of human neck muscles. Spine 23:412-421, 1998.)
SternocleidomastoidSplenius capitisRectus capitis posterior major
−4
−3
−2
−1
0
1
2
3Contra-
lateral
Ipsi-lateral
Mom
ent a
rm (
cm)
−40 −30 −20 −10 0 10 20 30 40
Rotation angle (deg)
ContralateralIpsilateral
Herkowitz_Chapter 3_main.indd 69 6/4/2010 2:39:14 PM

En
70 BASIC SCIENCE
the cervical facet joints and ligaments have been clinically isolated as a source of neck pain.53
Muscle Effects on Spinal Stiffness and Stability
It has long been recognized that muscles are necessary for spinal stability. It is unclear, however, which muscles contrib-ute most to spinal stability; this question has been addressed in several theoretical and experimental studies. Crisco and Panjabi54 examined the role of gross muscle architecture (i.e., the number of joints crossed by a muscle) in lateral stabiliza-tion of the lumbar spine using a mathematical model. They calculated minimal muscle stiffness necessary for spinal stabil-ity and found that muscles spanning only one vertebral body required the highest stiffness (i.e., activation) for stability, whereas muscles that spanned the largest number of vertebrae were most efficient (required the least activation). Efficient stabilization (less muscle activation) is important because it implies lower disc loads.
Electromyographically driven modeling by Cholewicki and McGill55 suggested that large muscles may provide the bulk of stiffness to the spinal column, as suggested by Crisco and Panjabi,54 but that the activity of short intrinsic muscles was also necessary to maintain stability. Biomechanical models have shown that buckling (loss of stability) can occur from a temporary reduction in activation to one or more interseg-mental muscles.55 Presumably, small intrinsic muscles are better suited to stabilize displacements at a single joint with a minimum increase in joint loads at other levels. Similarly, Daru56 and Winters and Peles57 used computer and physical models of the cervical spine to show that activating only large, long muscles resulted in instability, especially around the upright posture. The authors also concluded that activation of deep muscles was necessary for spinal stability. These types of analyses show the importance of gross anatomy and architec-ture of spinal muscles on spinal stability. Many important questions remain, however, such as the effect of muscle fatigue on spinal stability and the best muscle activation patterns for stability in the prevention and rehabilitation of low back and neck pain.
Summary
The architecture of a muscle is an important, and often over-looked, determinant of its function. Because muscle architec-ture interacts with the skeletal and nervous systems in complex ways, all of these factors must be examined together to under-stand fully the biomechanical function of a muscle and its contribution to any pain or injury mechanisms. Detailed ana-tomic and architectural studies have yielded insights into spinal muscle functions, but the architecture of many spinal muscles remains to be examined. These data are necessary for accurate biomechanical models, which must be used in con-junction with experimental studies to elucidate the function of spinal muscles and their role in pathologic processes of the spine. This information can ultimately be used in developing improved prevention and rehabilitation strategies.
type–specific injury to skeletal muscle and to document the relationship between muscle injury and back and neck pain.
Implications of Spinal Muscle Anatomy and Architecture for Injury
There are at least three ways in which spinal muscles may be implicated in mechanisms of injury and pain. First, as described earlier, the muscle itself may be injured from eccen-tric contraction during an imposed movement (particularly one in which the kinematics are abnormal). Second, muscle forces may alter the load distribution within anatomic struc-tures that have been clinically linked to pain. Third, muscle activity can alter spinal stiffness and kinematics, which would indirectly affect soft tissue loads and strains. The relationship between muscles and injury can be elucidated by biomechani-cal models, and accurate modeling of anatomy and architec-ture can affect the results of those models.
Muscle Injury Resulting from Eccentric Contraction
As noted earlier, rapid lengthening of muscle is an important mechanism of muscle injury. An example of potential muscle injury secondary to imposed lengthening occurs during whip-lash. During the retraction phase of whiplash injury, when the head translates rearward with respect to the torso, the sterno-cleidomastoid muscle can experience lengthening strains of 5% to 10% while it is active.46,47 During the rebound phase of whiplash injury, when the head translates forward with respect to the torso, the splenius capitis and semispinalis capitis muscles can experience lengthening strains of 10% to 20%. These predictions of muscle strains, based on a biomechanical model that incorporates muscle architecture,31 are above thresholds for strain that causes injury to active-lengthening muscle.37,48,49
Muscles Altering Load Distribution in Other Anatomic Structures
Because muscles are oriented primarily vertically, their activa-tion produces axial compression of the spine. The compressive loads on the discs and facet joints are a function of muscle force, moment arm, and activation. When the detailed anatomy of the lumbar erector spinae was included in a biomechanical model,50 the predicted disc compression and shear loads were reduced compared with a lumped extensor “muscle equiva-lent” commonly used in many models. This study highlights the importance of accurate representation of muscle anatomy in biomechanical models.
Compressive loads may severely alter tissue loads, particu-larly if abnormal vertebral kinematics occur. The synovial fold of the facet joint may become impinged during the abnormal kinematics that occur during whiplash.51 Muscles may also contribute to injury by directly loading passive structures. The cervical multifidus has attachments directly to facet capsular ligaments20,52; the combined loading from joint motion and muscle forces may lead to subcatastrophic injuries in facet capsular ligaments. These observations are important because
Herkowitz_Chapter 3_main.indd 70 6/4/2010 2:39:14 PM

En
3 Architectural Design and Function of Human Back Muscles 71
I
SE
CT
IO
N
4. Lieber RL: Skeletal Muscle Structure and Function: Implications for Physical Therapy and Sports Medicine. Baltimore, Williams & Wilkins, 1992.
5. Bodine SC, Roy RR, Meadows DA, et al: Architectural, histo-chemical, and contractile characteristics of a unique biarticular muscle: The cat semitendinosus. J Neurophysiol 48:192-201, 1982.
6. Ounjian M, Roy RR, Eldred E, et al: Physiological and develop-mental implications of motor unit anatomy. J Neurobiol 22:547-559, 1991.
7. Loeb GE, Pratt CA, Chanaud CM, et al: Distribution and inner-vation of short, interdigitated muscle fibers in parallel-fibered muscles of the cat hind limb. J Morphol 1:1-15, 1987.
8. Armstrong JB, Rose PK, Vanner S, et al: Compartmentalization of motor units in the cat neck muscle, biventer cervicis. J Neu-rophysiol 60:30-45, 1988.
9. Richmond FJR, MacGillis DRR, Scott DA: Muscle-fiber com-partmentalization in cat splenius muscles. J Neurophysiol 53:868-885, 1985.
10. Burkholder TJ, Lieber RL: Sarcomere length operating range of muscles during movement. J Exp Biol 204:1529-1536, 2001.
11. Lieber RL, Ljung B-O, Fridén J: Intraoperative sarcomere mea-surements reveal differential musculoskeletal design of long and short wrist extensors. J Exp Biol 200:19-25, 1997.
12. Lieber RL, Loren GJ, Fridén J: In vivo measurement of human wrist extensor muscle sarcomere length changes. J Neurophysiol 71:874-881, 1994.
13. Rome LC, Choi IH, Lutz G, et al: The influence of temperature on muscle function in the fast swimming scup: I. Shortening velocity and muscle recruitment during swimming. J Exp Biol 163:259-279, 1992.
14. Rome LC, Sosnicki AA: Myofilament overlap in swimming carp: II. Sarcomere length changes during swimming. Am J Physiol 163:281-295, 1991.
15. An KN, Takakashi K, Harrington TP, et al: Determination of muscle orientation and moment arms. J Biomech Eng 106:280-282, 1984.
16. Kalimo H, Rantanen J, Viljanen T, et al: Lumbar muscles: Struc-ture and function. Ann Med 21:353-359, 1989.
17. MacIntosh JE, Bogduk N: The morphology of the lumbar erector spinae. Spine 12:658-668, 1987.
18. Delp SL, Suryanarayanan S, Murray WM, et al: Architecture of the rectus abdominis, quadratus lumborum, and erector spinae. J Biomech 34:371-375, 2001.
19. Kamibayashi LK, Richmond FJR: Morphometry of human neck muscles. Spine 23:1314-1323, 1998.
20. Anderson JS, Hsu AW, Vasavada AN: Morphology, architecture, and biomechanics of human cervical multifidus. Spine 30:86-91, 2005.
21. MacIntosh JE, Bodguk N: The biomechanics of the lumbar mul-tifidus. Clin Biomech 1:205-213, 1986.
22. Ward, SR, Kim CW, Eng CM, et al: Architectural analysis and intraoperative measurements demonstrate the unique design of the multifidus for lumbar spine stability. J Bone Joint Surg Am 91:176-185, 2009.
23. Donisch EW, Basmajian JV: Electromyography of deep back muscles in man. Am J Anat 133:25-36, 1972.
KEy REFERENCES
1. Burke RE, Levine DN, Tsairis P, et al: Physiological types and histochemical profiles in motor units of the cat gastrocnemius. J Physiol (Lond) 234:723-748, 1973.This article is the classic reference that describes the relationship between the anatomic, physiologic, and biochemical properties of the mammalian motor unit. This article helps to explain the orderly recruitment of motor neurons during normal movement.
2. Evans WJ, Meredith CN, Cannon JG, et al: Metabolic changes following eccentric exercise in trained and untrained men. J Appl Physiol 61:1864-1868, 1986.This article is one of the earliest demonstrations of the protective effect of training on muscle injury owing to eccentric exercise. It is also a clear demonstration of the delayed nature of the injury that occurs to muscle after eccentric exercise.
3. Fridén J, Sjöström M, Ekblom B: Myofibrillar damage following intense eccentric exercise in man. Int J Sports Med 4:170-176, 1983.This article is the seminal demonstration of cytoskeletal damage to muscle after eccentric exercise. It contains classic micrographs showing the “Z band streaming” that occurs when muscles are subjected to high-intensity exercise.
4. Macintosh JE, Bogduk N: The biomechanics of the lumbar multifidus. Clin Biomech 1:205-213, 1986; MacIntosh JE, Bogduk N: The morphology of the lumbar erector spinae. Spine 12:658-668, 1987; MacIntosh JE, Valencia F, Bogduk N, Munro RR: The morphology of the human lumbar multifidus. Clin Biomech 1:196-204, 1986.This series of articles describes the complex but highly reproducible anatomy of the lumbar and thoracic spine musculature. Progressing from superficial to deep and thoracic to lumbar, the extraordinary level of organization of this musculature is clearly apparent.
5. Warren GW, Hayes D, Lowe DA, et al: Mechanical factors in the initiation of eccentric contraction-induced injury in rat soleus muscle. J Physiol (Lond) 464:457-475, 1993.This article presents a multiple regression experimental model that describes the relationship between muscle stress, muscle strain, and muscle strain rate as mechanical causal factors in muscle injury. The slow mammalian muscle is used as the experimental model.
REFERENCES
1. Panjabi M: The stabilizing system of the spine: I. Function, dys-function, adaptation, and enhancement. J Spinal Disord 5:383-389, 1992.
2. Gans C, Bock WJ: The functional significance of muscle archi-tecture: A theoretical analysis. Adv Anat Embryol Cell Biol 38:115-142, 1965.
3. Gans C, De Vries F: Functional bases of fiber length and angula-tion in muscle. J Morphol 192:63-85, 1987.
Herkowitz_Chapter 3_main.indd 71 6/4/2010 2:39:14 PM

En
72 BASIC SCIENCE
42. Fridén J: Changes in human skeletal muscle induced by long term eccentric exercise. Cell Tissue Res 236:365-372, 1984.
43. Fridén J, Sjöström M, Ekblom B: Myofibrillar damage following intense eccentric exercise in man. Int J Sports Med 4:170-176, 1983.
44. Lieber RL, Fridén J: Selective damage of fast glycolytic muscle fibers with eccentric contraction of the rabbit tibialis anterior. Acta Physiol Scand 133:587-588, 1988.
45. Burke RE, Levine DN, Tsairis P, et al: Physiological types and histochemical profiles in motor units of the cat gastrocnemius. J Physiol (Lond) 234:723-748, 1973.
46. Brault JR, Siegmund GP, Wheeler JB: Cervical muscle response during whiplash: Evidence of a lengthening muscle contraction. Clin Biomech 15:426-435, 2000.
47. Vasavada AN, Brault JR, Siegmund GP: Musculotendon and fas-cicle strains in anterior and posterior neck muscles during whip-lash injury. Spine 32:756-765, 2007.
48. MacPherson PCK, Schork MA, Faulkner JA: Contraction-induced injury in single fiber segments from fast and slow muscles of rats by single stretches. Am J Physiol 271:C1438-C1446, 1996.
49. Patel TJ, Das R, Fridén J, et al: Sarcomere strain and heterogene-ity correlate with injury to frog skeletal muscle fiber bundles. J Appl Physiol 97:1803-1813, 2004.
50. McGill SM, Norman RW: Effects of an anatomically detailed erector spinae model of L4/L5 disc compression and shear. J Biomech 20:591-600, 1987.
51. Kaneoka K, Ono K, Inami S, et al: Motion analysis of cervical vertebrae during whiplash loading. Spine 24:763-770, 1999.
52. Winkelstein B, McLendon R, Barbir A, et al: An anatomical investigation of the human cervical facet capsule, quantifying muscle insertion area. J Anat 198:455-461, 2001.
53. Barnsley L, Lord S, Wallis B, et al: The prevalence of chronic cervical zygapophysial joint pain after whiplash. Spine 20:20-26, 1995.
54. Crisco JJ, Panjabi MM: The intersegmental and multisegmental muscles of the lumbar spine: A biomechanical model comparing lateral stabilizing potential. Spine 16:793-797, 1991.
55. Cholewicki J, McGill SM: Mechanical stability of the in vivo lumbar spine: Implications for injury and chronic low back pain. Clin Biomech 11:1-15, 1996.
56. Daru KR: Computer simulation and static analysis of the human head, neck and upper torso. MS thesis, Arizona State University, 1989.
57. Winters JM, Peles JD: Neck muscle activity and 3-D head kine-matics during quasi-static and dynamic tracking movements. In Winters JM, Woo SL (eds): Multiple Muscle Systems: Biome-chanics and Movement Organization. New York, Springer-Verlag, 1990, pp 461-480.
24. Gray H: Gray’s Anatomy. New York, Gramercy Books, 1977.25. MacIntosh JE, Valencia F, Bogduk N, et al: The morphology of
the human lumbar multifidus. Clin Biomech 1:196-204, 1986.26. McGill SM, Juker D, Kropf P: Quantitative intramuscular myo-
electric activity of quadratus lumborum during a wide variety of tasks. Clin Biomech 11:170-172, 1996.
27. Bogduk N, Pearcy M, Hadfield G: Anatomy and biomechanics of psoas major. Clin Biomech 7:109-119, 1992.
28. McGill SM, Patt N, Norman RW: Measurement of the trunk musculature of active males using CT scan radiography: Implica-tions for force and moment generating capacity about the L4/L5 joint. J Biomech 21:329-334, 1988.
29. Santaguida PL, McGill SM: The psoas major muscle: A three-dimensional geometric study. J Biomech 28:339-345, 1995.
30. Juker D, McGill SM, Kropf P, et al: Quantitative intramuscular myoelectric activity of lumbar portions of psoas and the abdomi-nal wall during a wide variety of tasks. Med Sci Sports Exerc 30:301-310, 1998.
31. Vasavada A, Li S, Delp S: Influence of muscle morphometry and moment arms on the moment-generating capacity of human neck muscles. Spine 23:412-421, 1998.
32. Bogduk N, Johnson G, Spalding D: The morphology and biome-chanics of latissimus dorsi. Clin Biomech 13:377-385, 1998.
33. McGill SM, Hughson RL, Parks K: Changes in lumbar lordosis modify the role of the extensor muscles. Clin Biomech 15:777-780, 2000.
34. Norman RW, Wells P, Neumann P, et al: A comparison of peak vs. cumulative physical work exposure risk factors for the report-ing of low back pain in the automotive industry. Clin Biomech 13:561-573, 1998.
35. Clarkson PM, Johnson J, Dextradeur D, et al: The relationships among isokinetic endurance, initial strength level, and fiber type. Res Q Exerc Sport 53:15-19, 1982.
36. Evans WJ, Meredith CN, Cannon JG, et al: Metabolic changes following eccentric exercise in trained and untrained men. J Appl Physiol 61:1864-1868, 1986.
37. Lieber RL, Fridén J: Muscle damage is not a function of muscle force but active muscle strain. J Appl Physiol 74:520-526, 1993.
38. Warren GW, Hayes D, Lowe DA, et al: Mechanical factors in the imitation of eccentric contraction-induced injury in rat soleus muscle. J Physiol (Lond) 464:457-475, 1993.
39. Lieber RL, McKee-Woodburn T, Fridén J: Muscle damage induced by eccentric contraction of 25% strain. J Appl Physiol 70:2498-2507, 1991.
40. Lieber RL, Schmitz MC, Mishra DK, et al: Contractile and cel-lular remodeling in rabbit skeletal muscle after cyclic eccentric contractions. J Appl Physiol 77:1926-1934, 1994.
41. Lieber RL, Thornell L-E, Fridén J: Muscle cytoskeletal disruption occurs within the first 15 minutes of cyclic eccentric contraction. J Appl Physiol 80:278-284, 1996.
Herkowitz_Chapter 3_main.indd 72 6/4/2010 2:39:14 PM

EnHSP_003
AUTHOR QUeRy FORMDear Author
During the preparation of your manuscript for publication, the questions listed below have arisen. Please attend to these matters and return this form with your proof.
Many thanks for your assistance.
Query Query RemarksReferences
1 AU: Is the phrase “of muscles” ok as added here?
2 AU: Is “ NA” expanded correctly?
Herkowitz_Chapter 3_main.indd 1 6/4/2010 2:39:14 PM