3. comorbidity network of bd and bpd
TRANSCRIPT
____________________________________________________________________________________________________________www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page30
BridgesBetweenBipolarandBorderlinePerson-alityDisorders:ClarifyingComorbidityThroughtheAnalysisofComplexNetworkofConnectionsBetweenSymptomsDanielCastro1,FilipaFerreira1,AnaSofiaMendes1,TiagoBentoFerreira11UniversityInstituteofMaia(ISMAI),Maia,PortugalCorrespondingauthor:DanielCastro|[email protected]
Received:11December2017Accepted:19July2018
AbstractBackground:ThereasonsforthehighratesofcomorbiditybetweenBipolar(BD)andBorderlinePersonality(BPD)disordersremainelusive,duetothevastarrayofsharedclinicalfeatures,whichmakesthedifferentialdiagnosisdifficult.Thisconstitutesanobstacletoprovidequalityofcareservices,which results indetrimentaleffectson individual’smentalhealth.Theanalysisof thecomplexnetworkof connectionsbetweensymptomsofbothdisorders isapromisingpathway touncover themechanismsunderlying thecomorbiditystructureofbothdisorders.Goals:Inthisstudy,weexploredthecomorbiditynetworkthatrepresentstheconnectionsbetween32DSM-5symptomsofBDandBPDinorderto(1)compareitsmodularstructure(i.e.,theconstitutionofcohesivesubgroupsofsymptomswithinthecomorbiditynetwork)withthenosographicproposaloftheDSM-5;(2)distinguishbetweenthedifferentrolesthosesymptomshaveinthecomor-biditynetworkand identifythesymptomsthatoverlapandbridgebothdisorders,aswellasthedistinctivesymptomsthatbetterdiscriminatethem;(3)identifythemostcentralsymptomsandthosewiththehighestimpactonthestrengthoronthestructureoftheconnectionsonthecomorbiditynetwork;and(4)analyzetheassociationbetweensymptomsrolesandtheircentralityandimpact.Methods:AnepidemiologicalsamplefromtheNationalComorbiditySurvey:Baseline(NCS)wasanalyzed.DataregardingbipolarandborderlinepersonalitysymptomswerecollectedthroughtheCompositeNetworkInternationalDiagnosticInterview(CIDI).Thenet-workofcomplexinteractionsbetweensymptomswasestimatedusingtheIsingmodelwiththeL1-regularizationpenalty(EBIC)andthenosographicstructurewasdetailedwithModulandalgorithms.Results:Dataregardinganoverallsampleof7556individualswasanalyzed(48.6%male,Mage=33.400years,SDage=10.447).ResultsrevealeddifferencesbetweenthemodularstructureofthecomorbiditynetworkandtheDSM-5nosographicproposal,namelyaboutunstablerelationshipsandsubstanceabuse,thatwereassignedtothemoduleconstitutedbysymptomsofmanicepisode(ME).Symp-tomssuchasmoneyspendingandsexual indiscretions,thatoverlapMEandBPDintheDSM-5,wereassignedtotheMEmodule.Psychomotoragitation,whichoverlapsdepressiveepisode(DE)andMEintheDSM-5,wasassignedtotheDEmodule.Additionally,emptinessandworthlessnesswereidentifiedasbridgesymptomsbetweenDEandBPD;angerandsubstanceabusebetweenMEandBPD;andunstablerelationshipsandpsychomotoragitationbetweenDEandME.FatiguewasthemostdistinctivesymptomoftheDEmodule,unstablerelationshipsoftheMEmodule,andangeroftheBPDmodule.Strengthcentrality(r=.61,95%CI[.33,.79],p<.001)andmodularbridgeness(r=.64,95%CI[.38,.81],p<.001)werepositivelycorrelatedwiththeimpactonthestructureofthecomor-biditynetwork;andmodularoverlapwasnegativelycorrelatedwiththeimpactonthestrength(r=-.43,95%CI[-.10,-.68],p=.01)ofitsconnections.Discussion:ResultssuggestasimilarstructureofthecomorbiditynetworktothenosographicproposalofDSM-5.Distinctiveandbridgesymptomswere identifiedforeachdisorderwhichmighthelpwiththedifferentialdiagnosis. Itcanalsohelpustounveilpossibledevelopmentpathwaysofcomorbiditythatmightpromoteanimprovementinpsychologicaltreatments.Keywords:Bipolardisorder,Borderlinepersonalitydisorder,Networkanalysis,Comorbidity.

Castroetal____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page31
IntroductionThe differential diagnosis between Bipolar (BD) andBorderline Personality (BPD) disorders remains con-troversial (Barroilhet, Vohringer, & Ghaemi, 2013;Ghaemi,Dalley,Catania,&Barroilhet,2014).Thiscon-troversyisalsoassociatedwiththehighcomorbidityrate observed in both community-based (McDermidetal,2015)andclinical(Henryetal.,2001;Fonsekaetal., 2015) samples, and constitutes an obstacle forhealth care professionals (Bennazi, 2005; Borda,2016), leads to a high number of misdiagnosed pa-tients (Galione& Zimmerman, 2010) aswell as to alarge lag between diagnosis and beginning of treat-ment(Hirschfeld,Lewis,&Vornik,2003;Zimmerman,Martinez, Young, Chelminski, Morgan & Dalrymple,2014).Thehighcomorbiditybetweenthesedisorderswasattributedtothevastarrayofsharedclinicalfea-tures that span from nuclear diagnostic criteria toetiopathogenic mechanisms (Bayes & Parker, 2017;Paris,Gunderson,&Weinberg,2007)whichledtotheperspectivethatBPDisadisorderofthebipolarspec-trum(e.g.,Akiskal,2004).Inthisperspective,unstabletemperamentisconsideredtoplayamajorroleintheetiologyof thebipolarspectrum,whichmanifests it-self in the emotional instability, unstableinterpersonal relationships, anxiety, and impulsivity,observedinindividualsdiagnosedwithBPD(Hatchett,2010).Contrarytothisperspective,somestudiesob-served marked differences between the clinicalcharacteristicsassociatedwithBDandtheonesasso-ciated with BPD, related, for example, with thedurationoftheepisodes,responsetopharmacologicaltreatments, mood states, mood prognosis and im-pulse reactivity (Soler et al., 2013) and led to theconclusion that these disorders constitute distinctconditions (Koenigsberg et al., 2002; Wilson et al.,2007;Zimmerman,Martinez,Young,Chelminski,Mor-gan, & Dalrymple, 2014). To some extent, thiscontroversyisraisedbythefocusofpreviousresearchonthecomparisonofindividualsdiagnosedwithbothdisorderswithindividualsdiagnosedwithonlyoneofthem, on clinical characteristics related to etiology,treatmentresponseandfamilyhistory(Paris,Gunder-son,&Weinberg,2007).
In exploring alternative pathways to surpass theseproblems,itwassuggestedthatdetailingtheircomor-bidity structure by focusing on symptoms wouldconstituteamajorcontributionbyallowingtheidenti-fication and distinction between overlappingsymptoms,thosesymptomsthataresharedbybothdisorders (e.g. emotional dysregulation and impul-sivity)andwouldbeassociatedwithcomorbidity,anddistinctivesymptoms(e.g.,fearofabandonmentandpsychomotoragitation)thatwouldenablethedistinc-tionbetweenthem(Bayes&Parker,2017;Cassanoetal.,2009;Frías,Baltasar,&Birmaher,2016).Onthesegrounds, a study by Perugi, Angst, Azorin, Bowden,Vieta, and Young (2013) suggested that four out ofninesymptomsofBPDalsopredictBD(unstableandintenseinterpersonalrelations,impulsivity,emotionalinstabilityandreactivityand intenseand inappropri-ate anger), and that fear of abandonment, andrecurringsuicidalityorself-mutilation,arespecificofBPD.Vohringerandcolleges(2016)concludedthatthesymptomsofmanicepisode(e.g.,elevatedmood,in-creasedgoal-directedactivities)andtheirdurationareexclusive of BD. In addition, although the impulsivebehavior is thought to be central to both disorders,mostmanicandhypomanicepisodesdon’tinvolveim-pulsivity (Goodwin & Jamison, 2007). In turn,psychomotoragitationseemstobeamoreprominentfeatureofBDthanofBPD(Cassanoetal.,2009).Ontheotherhand,Benazzi(2008)foundnorelationshipbetween the symptomsofBipolarDisorder II (BD-II)andBPDtraits.Thisbriefoverviewmakesitnoticeablethatalthoughthisapproachisbeginningtocontributetosurpass theongoingcontroversy, someambiguityaround theoverlappinganddistinctive symptomsofbothdisordersremains.Infact,studiesonthecomor-biditybetweenBDandBPD,carriedoutatthelevelofsymptoms, remain scarce (Barroilhet, Vohringer, &Ghaemi,2013).Thisisunfortunate,asinrecentyears,agrowingbodyofresearch,acrossawiderangeofdisorderslikede-pression (Fried, Epskamp, Nesse, Tuerlinckx, &Borsboom, 2016), anxiety (Beard et al., 2016), post-traumaticstress(Armour,Fried,Deserno,Tsai,&Pie-trzack, 2016), psychosis (Isvonaru, Borsboom, Os, &Guloksuz, 2016), substance abuse (Rhemtulla et al.,

Comorbiditynetworkofbipolardisorderandborderlinepersonalitydisorder____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45 page32
2016)andautism(Anderson,Locke,Kretzmann,&Ca-sari,2016),hasprovidedconsistentevidencethattheconnections between symptoms constitute an im-portant dimension of the etiopathogeny of mentalhealthdisorders;andpromotednewinsightsonphe-nomenalikecomorbidity(Cramer,Waldorp,Maas,&Borsboom, 2010) and diversity of clinical presenta-tions (Borsboom & Cramer, 2013) that have adetrimentalimpactonthevalidityofthenosographyof mental health disorders (Boschloo et al., 2015;Eaton,2015).Thosestudiesexplore theconnectionsbetween symptoms by using network models thatrepresentthoseconnections.Thesepsychopathologi-cal networks (see Borsboom, 2017; Borsboom &Cramer,2013;Borsboom,Epskamp,Kievit,Cramer,&Schmittmann,2011;Friedetal.,2017,forreviews)arerepresented through graphs constituted by vertices,representing symptoms, by edges, representing theconnections between symptoms, and by edges-weights,which represent the strengthof these con-nections. Psychopathological networks enable theidentificationofmostcentralsymptoms,theonesthathavemorediverseorstrongerconnectionswithothersymptoms, and/or theones that are involved in theconnections between other symptoms (Borsboom,2017), as well as those symptoms, named bridgesymptoms (Cramer, Waldorp, Mass, & Borsboom,2010),thatconnectdistinctdisorders.Theidentifica-tion of central and bridge symptoms fosters analternative understanding and clarification of thecomorbiditystructuresthatusuallycharacterizemen-talhealthdisorders(Friedetal.,2016),suchastheonebetweenBDandBPD.AlthoughnopreviousstudyhasexploredthecomorbiditynetworkofBDandBPD(i.e.,the network representing the connections betweenthesymptomsofbothdisorders),Richetin,Preti,Cos-tantini,andDePanfilis(2017)exploredthenetworkofconnections between symptoms of BPD and foundthataffectiveinstability,identitydisturbanceandfearofabandonmentarethemostcentralsymptoms.Asinprevious studies on other disorders (e.g., Armour,Fried,Deserno,Tsai,&Pietrzark,2016;Levinsonetal.,2017),theauthorssuggestedthatspecificallytarget-ing these symptoms during treatment can improvetreatmentefficacysincethestrengthandnumberofconnectionsthecentralsymptomsmaintainwiththeothersymptoms isexpectedtobeassociatedwitha
high potential to transform the network. Symptomscentrality is thereforehypothesizedtobeassociatedwiththeirimpactonthenetwork.However,previousstudies on psychopathological networks have pro-vided only partial or indirect support for thishypothesisandfurtherevidenceisnecessarytosup-port it(Friedetal.,2017).This isrelevantbecauseifthisisthecase,thentheidentificationofthesesymp-tomswouldbringmuch-neededbreakthroughsinthedevelopment of precision (Collins & Varmus, 2015;Rugkåsa,Yeeles,Molodynski,&Burns,2015)andindi-vidualized (Fischer, 2015; Fischer & Boswell, 2016)treatments.Anotheropenquestionconcerningtheroleofcentralsymptomsreferstothequestionofknowingifthesesymptomscorrespondtothemostcharacteristic,dis-tinctive symptoms of the disorders being studied.Somestudiesobservedthatsomeofthemostcentralsymptomsinpsychopathologicalnetworksofdepres-sion(vanBorkuloetal.,2015)orpost-traumaticstressdisorder (Armour, Fried, Deserno, Tsai, & Pietrzark,2016)coincidewiththecoresymptomsofthesedisor-ders according to the criteria of the Diagnostic andStatisticalManualofMentalDisorders(DSM),butthisisnotaconsistentobservationasotherstudiesidenti-fiedcentral symptomsthatdonotcoincidewith thecoresymptomsassumedbytheDSM(seeBoschlooetal., 2015 for an example). Moreover, doubts havebeenraisedonthediscriminativepoweroftheDSMcore symptoms (Goekoop&Goekoop, 2014). In thecaseofBD,forexample,impulsivityrelatedsymptoms(i.e.,spending,sexualindiscretions),whicharecriteriaformanicepisodeintheDSM,donotappearinmostmanicepisodes(Goodwin&Jamison,2007).Thesamekindofquestionsalsoapplytothecaseofoverlappingorbridgesymptomssinceitmakesintui-tivesensetohypothesizethatsymptomsthatconnecttwodisorderswouldhaveasignificantimpactonthepsychopathologicalnetworkbydissolvingitinthecaseofbeingremovedduringtreatment.Forexample,anoverlappingsymptombetweenBDandBPDistheen-gagement in activities that have potentiallyunpleasant consequences (e.g., sexual indiscretionsand spending). Thus, in a patientwithBPD that dis-playssexualindiscretionsorspending,alsoassociated

Castroetal____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page33
withBD,targetingthosesymptomscoulddissolvethecomorbidity network and prevent the patient fromalsodevelopingBD.However,nodirectevidenceex-ists to support this hypothesis. In fact, Afzali andcolleagues(2016)comparedthecompletenetworkofconnectionsbetweenthesymptomsofposttraumaticstressdisorderandmajordepressivedisorderwiththenetwork of connections between these disorders’symptoms after removing thebridge symptoms andobservedthatasignificantnumberofconnectionsbe-tweenthesymptomsofbothdisordersemergeevenintheabsenceofbridgesymptoms.Furthermore,todate, the identification of the bridge symptoms hasbeenperformedby identifyingthesymptomsofonedisorderthathavethehighestnumberofconnectionswithsymptomsofadifferentdisorder(e.g.,Afzalietal.,2016;Beardetal.,2016).Thisprocedureassumesthat the empirical structure of the comorbidity net-work reproduces the nosographic proposal of theDSM(i.e.,thesymptomsofbothdisorderscorrespondto identifiable and especially cohesive subgroups ofsymptomsinthecomorbiditynetwork),butthisneedsnotbethecase.Previousstudiesonthepsychopatho-logical networks of other disorders have found onlygeneral correspondence between the DSM noso-graphic proposal and empirical structure of thenetworks(Jones,Mair,Riemann,Mugno,&McNally,2017).Factoranalyticstudiesontheempiricalstruc-tureofBD(Eisner,Johnson,Youngstrom,&Pearlstein,2017;Ferentinosetal.,2017)andBPD(Lewis,Caputi,&Grenyer,2012)observedthatsomesymptomssat-uratemore strongly on a factor corresponding to adifferentdisorder;andpreviousresearchontheem-piricalstructureofBD(Angst,2013)andBPD(Calvoetal.,2016)raisedsomeconcernsoverthevalidityofthenosographicproposaloftheDSMforthesedisorders.Theseobservationssuggestthatitisunlikelythattheempiricalstructureofthecomorbiditynetworkrepli-cates the nosographic proposal of theDSM. This, inturn, suggests that, at least from a methodologicalpointofview, the identificationofbridgesymptomsshould be contingent on the identification of distin-guishable subgroups of symptoms in the empiricalstructureofthecomorbiditynetwork.
Insummary,thereasonsforthehighratesofcomor-bidity between BD and BPD remain elusive(Zimmerman&Morgan,2013).Research focusedoncharacterizingthecomorbidityofBDandBPDbyfo-cusing on their symptomshas begun to identify thesymptomsthatbetterdiscriminatebothdisorders,butpreviousstudiesarescarce,andsomeresultsremainambiguous.Theanalysisofpsychopathologynetworkshasbeenrevealingitselfasoneofthemostpromisingpathways to understanding the role of connectionsbetweensymptomsintheemergenceofcomorbiditybetweenmentalhealthdisordersbutsomeofitscen-tralhypothesesareinneedoffurtherdevelopments.Inthiscontext,thepresentstudyexploredthecomor-bidity between BD and BPD by focusing on thenetwork of connections between the symptoms ofbothdisorders. Itaimed to: (1) compare thecomor-bidity network of BD andBPDwith the nosographicproposaloftheDSM-5(AmericanPsychiatricAssocia-tion, 2013), (2) identify overlapping, bridge anddiscriminativesymptoms,(3)identifythemostcentralandimpactfulsymptoms,and(4)exploretheassocia-tion between symptoms’ centrality and impactwiththeirrolesinthecomorbiditynetwork.
MethodsThisisasecondaryanalysisofdatagatheredinacross-sectionalobservationaldesign.ParticipantsA community-based sample, representative of theUnitedStatesofAmerica,fromapreviousepidemio-logical study, the National Comorbidity Survey:Baseline (NCS-Baseline; Kessler, Borges, & Walters,1999),wasanalyzed.TheNCS-Baselinedatasetcom-prises8098participantswithagesbetween15and61years.Forthisstudy,participantswithoutatleastonesymptomofBDandBPDwereexcluded.Priortothebeginningofeveryinterview,thestudywasexplained,and a verbal informed consentwasobtained. Theseprocedures were approved by the Human SubjectsCommitteesofHarvardMedicalSchoolandoftheUni-versityofMichigan.

Comorbiditynetworkofbipolardisorderandborderlinepersonalitydisorder____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45 page34
SymptomsMeasuresIn the NCS-Baseline study, participants were inter-viewedthroughamodifiedversionoftheCompositeInternational Diagnostic Interview (CIDI; Kessler &Ustun, 2004). This is a structured interview that as-sesses symptoms of depression, mania, dysthymia,panic disorder, agoraphobia, social phobia, simplephobia, generalized anxiety disorder, alcohol abuseanddependence,drugabuseanddependence,antiso-cialpersonalitydisorderandnon-affectivepsychosis.CIDIisatoolcreatedunderthescopeofaWHOinitia-tive, and assesses disorders on basis of thecorrespondingdefinitionsandcriteriafrombothDSM-III-RandICD(Robinsetal.,1998).Forthepresentstudy,CIDIquestionsthatrefertothesymptomsofdepressiveepisode(DE)andmanicepi-sode(ME)wereusedasmeasuresofthesymptomsofBD.Thesequestionsaskparticipantstoratetheoccur-renceofthesesymptomsona“yes”or“no”format.AlthoughtheCIDIdoesnothaveaspecificmeasureforthesymptomsofBPD,ithasasectiondedicatedtotheassessmentofpersonalitytraitsthroughitemsthatre-flect thosetraits.Each item is ratedonaLikert-typescalethatrangesfrom1(“Verytrue”)to4(“Nottrueatall”).Threeof these items,addressingBPDsymp-toms of fear of abandonment, identity disturbance,andemptiness,wereselected for thepresentstudy.ToaccuratelycaptureallthecriteriaproposedbytheDSM-5 for the diagnosis of BPD they were comple-mentedwithotherCIDIquestionsthatassessunstablerelationships, substance abuse, unstable affect andanger.OnlytheDSM-5symptomofcompulsiveeatingismissing from the assessment of the NCS-Baselinestudy. In total, 32DSM-5 symptoms of BD and BPDwereselected(25ofBDand7ofBPD).Whenneces-sary,participants’answersweredichotomizedpriortodata analysis. The CIDI questions selected for thisstudyandthecorrespondingDSM-5criteriaarepre-sentedinTableS1ofthesupplementarymaterials.NetworkEstimationandAnalysisThe Ising model coupled with the L1-regularizationpenalty(EBIC)(vanBorkuloetal.,2014)wasusedtoestimate the network of connections between thesymptomsofBDandBPD.Thematrixcontainingthe
connectionsweightsisincludedinTable2oftheSup-plementary materials. Its graphical representationwas computed using the Fruchterman-Reingold(Fruchterman-Reingold,1991)algorithm.R (RDevel-opment Core Team, 2008) packages bootnet(Epskamp&Fried,2017)andqgraph(Epskampetal.,2012) were used to estimate and represent thecomorbiditynetwork.Threemeasuresof symptoms’centrality were computed: strength, betweenness,andcloseness(Barrat,Barthelemy,Pastor-Satorras&Vespignani, 2004; Opsahl, Agneessens & Skvoretz,2010).Symptomsstrengthisthesumoftheweightsofalltheconnectionsofaspecificsymptomtoallothersymptomsinthenetwork.Betweennessisameasurethatreliesonthenumberoftimesasymptomispre-sent on the shortest path between two othersymptoms.Closeness is theaveragedistance fromaspecific symptom to all the other symptoms in thecomorbidity network. R package qgraph (Epskamp,Cramer,Waldorp, Schmittmann & Borsboom, 2012)wasusedtocomputecentralitymeasures.Theaccuracyandstabilityofthecomorbiditynetworkwere analyzed by estimating the 95% bootstrappedconfidenceintervals(CIs)foreachoftheconnectionsand the correlation stability coefficient (CS-Coeffi-cient; Epskamp, Borsboom, & Fried, 2016). CS-Coefficientestimatesthemaximumnumberofcasesthatcanbedroppedfromthedatatoretainacorrela-tionofatleast.7(95%)betweenthestatisticsoftheoriginal network and the statistics obtained withfewer cases (Epskamp&Fried, 2017).CS-Coefficientmustnotbelowerthan.25andshouldpreferablybehigherthan.5(Epskamp,Borsboom,&Fried,2016).Rpackagebootnet(Epskamp&Fried,2017)wasusedtoestimate the 95% bootstrapped CIs for the connec-tionsweightsandtocomputetheCS-coefficientsforstrength, closeness, and betweenness centrality.ThesearedepictedinFiguresS1andS2inthesupple-mentarymaterials.Additionally,FiguresS4,S5,andS6in the supplementary materials depict the boot-strappeddifferencetestsforthecentralitymeasuresofeverysymptominthenetwork.ThestructureandstrengthimpactofeachsymptominthecomorbiditynetworkwascomputedusingRpack-age networktools (Jones, 2017). Structure impact

Castroetal____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page35
measurestheinfluenceofeachsymptomonthecon-nectionsthatconstitutethecomorbiditynetwork,andstrengthimpactmeasurestheinfluenceofeachsymp-tom on the weights of the connections in thecomorbiditynetwork.Positivevaluesofstrength im-pactsuggestthatsymptomsincreasetheconnectionsweights andnegative values suggest that symptomsdecrease the connections weights. To explore theoverallstrengthimpactofeachsymptomtheabsolutevalueswerecomputed.Afterestimationofthecomorbiditynetwork,itsnet-work structurewas explored in order to compare itwith thenosographicproposal of theDSM-5. Toac-complish this, network modules were identified.Modules are constituted by a set of symptoms thathave a large mutual influence on each other andtherefore form a highly-connected cluster of symp-toms.Thesymptomsineachmoduleareexpectedtocorrespond to the symptomsofeachdisorder if theempiricalstructureofthecomorbiditynetworkcorre-sponds to the nosographic proposal of the DSM-5.Because the nosographic proposal of the DSM-5 in-cludes symptoms that overlap BD and BPD, analgorithmthatallowsnetworkmodulestooverlapwasused.Modulandalgorithm(Szalay-Bekoetal.,2012),implemented in Cytoscape 3.5.1. (Shannon et al.,2003),wasusedtoidentifymodulesinthecomorbid-itynetwork.Eachsymptomgetsmoduleassignmentvalues that represent howmuch it belongs to eachmodule.TableS3inthesupplementarymaterialspre-sentsmoduleassignmentvaluesforthe32symptomsin the comorbidity network. Modular cores are thesymptomsthathavethemaximalmoduleassignmentvalue ineachmodule.Weusedthisasameasureofthedistinctive symptoms (the symptoms thatbettercharacterize amodule and distinguish it from othermodules).Withineachmodule,weconsideredbridgesymptomstobethosesymptomswithhigherassign-ment value to each one of the other modules.Moduland alsomeasuresmodular overlap and brid-geness. Modular overlap is a trans-modularitymeasure of the effective number ofmodules that asymptomisassignedto,andmodularbridgenessisaninter-modularity measure of the overlap of a givensymptombetweentwoormoremodulesrelativetoall
theother symptoms.TableS4 in the supplementarymaterialspresentsthevaluesforsymptomscentrality,impact andmodular roles (bridgeness and overlap).DataanalysisonRwasperformedinRStudio1.1.379(RStudioTeam,2017).Finally,Pearsoncorrelationcoefficientsbetweencen-trality, impact andmodular roleswere estimated inJASP(JASPTeam,2016).
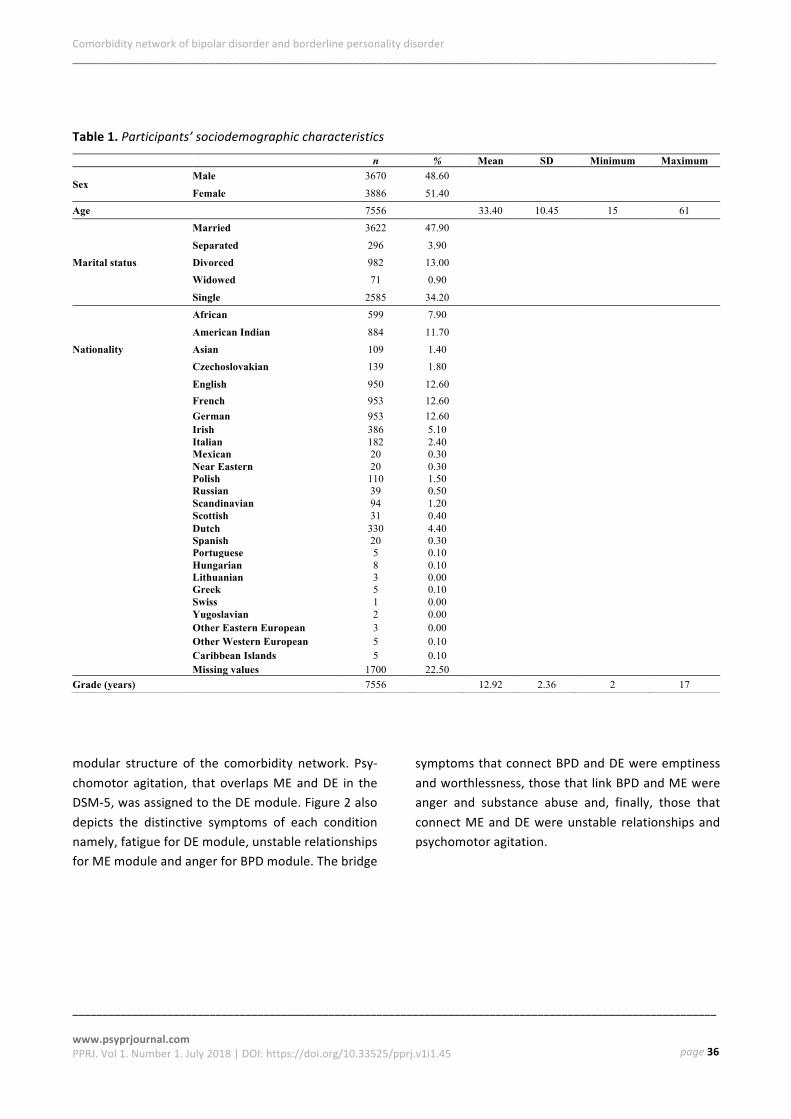
ResultsDatafrom7556participants,whichfulfilledtheinclu-sioncriteria,wereanalyzedandarepresentedbelow.TheseparticipantsarecharacterizedinTable1.Over-all,2473(33%)participantsmetthecriteriaforDE,394(5%)forMEand2471(33%)forBPD.ComorbidityNetworkofBDandBPDThe comorbidity network of BD and BPD is repre-sentedinFigure1.Itisconstitutedby224connectionsbetween the 32 symptoms (density = .45), 220(98.22%) positive, and 4 (1.79%) negative connec-tions.Positiveconnectionsweightsrangefrom.02to3.0 (M = 0.45, SD = 0.451). Negative connectionsweightsrangefrom0.10to1.07(M=0.47,SD=0.42).Theaccuracyandstabilityofthecomorbiditynetworkwereadequate,andtheCS-coefficientswerealsoad-equate for strength (.75), closeness (.52), andbetweenness(.36)ComorbidityNetworkModulesFigure2identifiesthemodulesinthecomorbiditynet-workandthesymptomsthatconstitutethem.Threemodules were observed that broadly correspond tothesymptomsofDE(greendotsinFigure2),ME(or-angedotsinFigure2)andBPD(graydotsinFigure2)in theDSM-5.Differenceswith thenosographicpro-posaloftheDSM-5arevisiblemainlyinMEsymptomswithunstablerelationshipsandsubstanceabusecom-monly associated with BPD being assigned to thismodule. The role of DSM-5 overlapping symptomswas also clarified. The impulsivity criteria that over-laps ME and BPD (i.e., money spending and sexualindiscretions)wereassignedtoMEmoduleinthe.
Comorbiditynetworkofbipolardisorderandborderlinepersonalitydisorder____________________________________________________________________________________________________________
____________________________________________________________________________________________________________www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page36
Table1.Participants’sociodemographiccharacteristics
modular structure of the comorbidity network. Psy-chomotor agitation, thatoverlapsMEandDE in theDSM-5,wasassignedtotheDEmodule.Figure2alsodepicts the distinctive symptoms of each conditionnamely,fatigueforDEmodule,unstablerelationshipsforMEmoduleandangerforBPDmodule.Thebridge
symptomsthatconnectBPDandDEwereemptinessandworthlessness,thosethatlinkBPDandMEwereanger and substance abuse and, finally, those thatconnectMEandDEwereunstable relationshipsandpsychomotoragitation.
n % Mean SD Minimum Maximum
Sex Male 3670 48.60
Female 3886 51.40 Age 7556 33.40 10.45 15 61
Marital status
Married 3622 47.90
Separated 296 3.90 Divorced 982 13.00 Widowed 71 0.90
Single 2585 34.20
Nationality
African 599 7.90
American Indian 884 11.70 Asian 109 1.40 Czechoslovakian 139 1.80
English 950 12.60 French 953 12.60 German 953 12.60
Irish 386 5.10 Italian 182 2.40 Mexican 20 0.30 Near Eastern 20 0.30 Polish 110 1.50 Russian 39 0.50 Scandinavian 94 1.20 Scottish 31 0.40 Dutch 330 4.40 Spanish 20 0.30 Portuguese 5 0.10 Hungarian 8 0.10 Lithuanian 3 0.00 Greek 5 0.10 Swiss 1 0.00 Yugoslavian 2 0.00 Other Eastern European 3 0.00 Other Western European 5 0.10
Caribbean Islands 5 0.10 Missing values 1700 22.50
Grade (years) 7556 12.92 2.36 2 17

Castroetal____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page37
Figure1.Comorbiditynetworkofbipolarandborderlinepersonalitydisorders.GreennodesrepresentthesymptomsofdepressiveepisodeintheDSM-5;orangenodesrepresentthesymptomsofmanicepisodeintheDSM-5;greynodesrepresentthesymptomsofborderlinepersonalitydisorderintheDSM-5;andpurplenodesrepresenttheoverlappingsymptomsaccordingtothenosographicproposaloftheDSM-5:node8(psychomotoragitation)overlapsdepressiveandmanicepisodes;node17(suicidalattempt)overlapsdepressiveepisodeandborderlinepersonalitydisorder;nodes20(moneyspending)and21(sexualindiscretions)overlapmanicepisodeandborderlineperson-ality disorder. Connections between the symptoms (edges) are represented by the blue lines (positive connections), and the red lines(negativeconnections).Thelines’thicknessrepresentsthestrengthoftheconnectionsbetweenthesymptoms(edgesweights).Thethickerthelinesare,thestrongertheconnectionsbetweensymptomsare.
SymptomsModularRoles:BridgenessandOverlap-pingSymptoms’modular bridgeness and overlapping arepresented in Figure 3.A. Symptoms of ME and BPDmodulesrevealedthehighestmodularbridgenessandoverlapping.Unstablerelationships,distractibilityandthought acceleration (ME module), and anger andemptiness(BPDmodule)revealedthehighestmodu-lar bridgeness. Substance abuse (ME module), andunstableaffect, anger, fearofabandonment,empti-nessandidentitydisturbance(BPDmodule)revealedthehighestmodularoverlapping.
Symptoms Centrality: Strength, Betweenness, andClosenessFigure 3.B. presents symptoms centrality. BD symp-toms were the most central symptoms in thecomorbidity network. Unstable relationships (MEmodule)andfatigue(DEmodule)revealedthehigheststrength centrality. The symptoms with the highestbetweennessandclosenesscentralitywereunstablerelationships (MEmodule) anddepressedmood (DEmodule).
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
2728
29
3031
32
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
Depressive Episode1: Depressed Mood2: Decreased Appetite3: Increased Appetite4: Insomnia5: Hypersomnia6: Fatigue7: Psychomotor retardation9: Diminished Interest10: Whorthlessness11: Guilt12: Diminished Concentration13: Slowing Thoughts14: Indecision15: Thoughts of Death16: Suicidal Ideation
Manic Episode18: Euphoria19: Increased Activity22: Distractability23: Decreased Sleep24: Talkative25: Thought Acceleration
Borderline Personality26: Unstable Relationships27: Substance Abuse28: Unstable Affect29: Anger30: Fear of Abandonment31: Identity Disturbance32: Emptiness
Overlapping Symptoms8: Psychomotor Agitation17: Suicide Attempt20: Money Spending21: Sexual Indiscretions
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
Depressive Episode1: Depressed Mood2: Decreased Appetite3: Increased Appetite4: Insomnia5: Hypersomnia6: Fatigue7: Psychomotor retardation9: Diminished Interest10: Whorthlessness11: Guilt12: Diminished Concentration13: Slowing Thoughts14: Indecision15: Thoughts of Death16: Suicidal Ideation
Manic Episode18: Euphoria19: Increased Activity22: Distractability23: Decreased Sleep24: Talkative25: Thought Acceleration
Borderline Personality26: Unstable Relationships27: Substance Abuse28: Unstable Affect29: Anger30: Fear of Abandonment31: Identity Disturbance32: Emptiness
Overlapping Symptoms8: Psychomotor Agitation17: Suicide Attempt20: Money Spending21: Sexual Indiscretions

Comorbiditynetworkofbipolardisorderandborderlinepersonalitydisorder____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45 page38
Figure2.ComorbiditynetworkmodulesbyModulandalgorithm.Threeaxesarerepresentedinthisfigureandeachonecorrespondstothethreeconditionsanalyzed:ingreenisrepresentedthedepressiveepisodemodule;ingray,theborderlinepersonalitydisordermodule;andinorangethemanicepisodemodule.Eachofthethreeaxesshowthemodularcoremeasurevalue.Inthisway,themostdistinctivesymptomswhicharerepresentedinred,are:fordepressiveepisode,fatigue;formanicepisode,unstableinterpersonalrelationships;andforbor-derlinepersonalitydisorder, anger. Thebridge symptomswhichare represented inblueare: formanicanddepressiveepisode,unstableinterpersonalrelationshipsandpsychomotoragitation;formanicepisodeandbor-derlinepersonalitydisorder,substanceabuseandanger;andforborderlineanddepressiveepisode,emptinessandworthlessness.
SymptomsStrengthandStructureImpactSymptoms strength and structural impact are pre-sented in Figure 3.C. Suicidal attempt (DE module),euphoria(MEmodule)andpsychomotoragitation(DEmodule) are those which exhibited the higheststrength impact in thenetwork.On theotherhand,thehigheststructuralimpactwasdisplayedbyunsta-blerelationshipsandeuphoria(MEmodule).
AssociationsBetweenCentrality,ImpactandModu-larRolesToevaluate theassociationsbetweencentrality, im-pact, and modular roles we analyzed the PearsoncorrelationcoefficientsinTable2.Symptomsmodular

Comorbiditynetworkofbipolardisorderandborderlinepersonalitydisorder____________________________________________________________________________________________________________
____________________________________________________________________________________________________________www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page39
Figure3.Symptoms’Centrality,ImpactandModularRole

Comorbiditynetworkofbipolardisorderandborderlinepersonalitydisorder____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45 page40
bridgnesswaspositivelycorrelatedwithstructureim-pact (r = .64,95%CI [.38, .81],p < .001). Symptomsmodularoverlapandstrengthimpactcorrelatedneg-atively(r=-.43,95%CI[-.68,-.10],p=.01).Inaddition,themeasuresof centralitywereassociatedwith im-pact, especially in the structure of the comorbiditynetwork.Strengthcentrality(r=.61,95%CI[.33,.79],
p<0.001)andbetweennesscentrality(r=.37,95%CI[.02,.64],p=.04)correlatedpositivelywithstructureimpact.Closenesscentralityrevealedapositivecorre-lationwithstructureimpact(r=.43,95%CI[.09,0.7],p=.02)andanegativecorrelationwithstrengthim-pact(r=-.35,95%CI[-.63,-.01],p=.05).
Table2.PearsonCorrelationCoefficientsBetweenSymptoms’Centrality,ImpactandModularRoles
Strength Impact
Structure Impact
Strength Centrality
Betweenness Centrality
Closeness Centrality
Modular Bridgeness
Modular Overlap
Strength Impact
Pearson's r — p-value — Upper 95% CI — Lower 95% CI —
Structure Impact
Pearson's r -.33 — p-value .07 — Upper 95% CI .02 — Lower 95% CI -.61 —
Strength Centrality
Pearson's r -.27 .61 *** — p-value .13 < .001 — Upper 95% CI .08 .79 — Lower 95% CI -.57 .33 —
Betweenness Centrality
Pearson's r .05 0.37 * .69 *** — p-value .79 0.04 < .001 — Upper 95% CI .39 0.64 0.84 — Lower 95% CI -.31 0.02 0.45 —
Closeness Centrality
Pearson's r -.35 * .43 * .83 *** .68 *** — p-value .05 .02 < .001 < .001 — Upper 95% CI -.01 .67 .92 .82 — Lower 95% CI -.63 .09 .68 .40 —
Modular Bridgeness
Pearson's r .10 .64 *** .64 *** .57 *** .34 — p-value .57 < .001 < .001 < .001 .06 — Upper 95% CI .44 .81 .81 .77 .62 — Lower 95% CI -.26 .38 .38 .28 -.01 —
Modular Overlap
Pearson's r -.43 * .26 -.21 -.02 -.35 * .50 ** — p-value .01 .16 .25 .91 .05 .00 — Upper 95% CI -.10 .56 .15 .33 -.01 .72 — Lower 95% CI -.68 -.10 -.52 -.37 -.63 .18 —
Note. The absolute values of modular overlap were considered. * p < .05, ** p < .01, *** p < .001.
DiscussionThecomorbiditystructureofBPDandBDremainsun-clearduetosharedclinicalfeatures,whichresultsinenduringuncertaintiesaboutBPDbelongingtothebi-polar spectrum. To contribute to this debate, thispaperpresentsanetworkanalysishavingasmaingoaltoexploretheunderlyingmechanismsofcomorbidityassociatedwith the connectionsbetween the symp-tomsofbothdisorders.Ourresultsshowthreeclear
modules(DE,MEandBPD)suggestingthatthedisor-dersaredistinctentities,whichisinlinewithpreviousstudies(e.g.,diGiacomoetal.,2017).However,afewinconsistencieswereobservedbetweentheempiricalmodularstructureofthecomorbiditynetworkandthenosographicproposaloftheDSM-5.Themostnotice-able difference is that the symptom “unstablerelationships”,asymptomofBPDintheDSM-5,wasassigned to theMEmodule. This supports previous

Castroetal____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page41
studiesthatrecognizeddifficultiesininterpersonalre-lationshipsduringmanicepisodes(Morrisetal.,2013;Siegel et al., 2015). Also, impulsivity-related criteriaforBPD,namelysubstanceabuse,wasassignedtotheMEmodule. This findingmight be explained by thehigh rates of comorbidity between substance abuseand BD (Messer, Lammers, Müller-Siecheneder,Schmidt,&Latifi,2017)andbythehighprobabilityofconsumptionof substancesby individualsdiagnosedwith BD (Grant et al., 2006). In addition, elevatedmoodepisodesareassociatedwithanincreasedlike-lihoodofsubstanceabuse(Messeretal.,2017).Lastly,psychomotoragitation,aDSM-5symptomofbothMEandDE,wasassignedtotheDEmodule,whichisalsoconsistentwithpreviousstudiesthatshowahighfre-quency of psychomotor agitation in depressiveepisodes(Akiskal,Benazzi,Perugi&Rihmer,2005).Asforthedifferentrolesofthesymptomsinthemodularstructureofthecomorbiditynetwork,ourresultssug-gest that in the case of BPD and ME, bridge anddistinctiverolesconverge inthesamesymptom(an-ger), meaning that the symptom that has themostconnectionswithin themodule is also the onewithmostconnectionswiththeothermodules.Infact,an-ger has a high prevalence in both BPD and BD(Fernandez&Johnson,2015),andwasassociatedwiththemisdiagnosisofBD insteadofBPD(Rugero,Zim-merman, Chelminski, & Young, 2010). Unstablerelationshipsalsoseemtoperformbothroles:asadis-tinctivesymptomofMEandbridgesymptomwithDE.Moreover,unstablerelationshipsarethemost inter-modular symptomof the all network and after sub-stance abuse is the symptom that more stronglyconnectsMEwithBPD.Previousstudiessuggestthat“unstable interpersonal relationships” is a non-spe-cific symptom and does not distinguish BPDdiagnostically(Perugietal.,2013).Theinter-modular-ityofthissymptommightexplainthechangesinmoodpolarityand thedevelopmentof somesymptomsofBPDand,therefore,leadtothedifficultiesinthedif-ferentialdiagnosisbetweenBPDandBD.FatiguewasidentifiedasadistinctivesymptomofDE.Thisresultisinlinewithothernetworkstudiesthatindicatefatigueas one of themost central symptoms in depression(Bekhuis,Schoevers,Borkulo,Rosmalen,&Boschloo,2016). Emptiness andworthlessnesswere identified
asbridgesymptomsbetweenDEandBPD.Thisfindingiscongruentwithotherstudiesthatfoundthatempti-nessisoneofthetraitsofBPDthatismostcommonlyobservedinDE(Benazzi,2005).Also,psychomotorag-itationwas identifiedasabridge symptombetweenME andDE,which is linewith previous studies thatconclude thatpsychomotoragitationshouldbecon-sidered a core feature ofmixed states (Mahli et al.,2016).Substanceabuseisalsoabridgesymptombe-tweenBPDandMEandthismightbeexplainedduetothe impulsivity that characterizes both disorders(Messer et al., 2017; Pennay et al., 2011). Globally,thesesymptomsdemonstrateahighinterconnectivitybetween the symptomsof bothdisorders andhelpsexplainthemechanismsofcomorbidity.In addition, our results show the importance of theidentificationofdifferentrolesforthesymptomssincedifferent roles seem to be associatedwith differenttypes of impact in the network. Symptomsmodularbridgeness was associated with structural impact;whilemodularoverlapwasnegativelyassociatedwithstrength impact. This means that symptoms of onedisorderthatinteractthemostwithsymptomsofan-otherdisorder,ifremovedfromthenetwork,causeachangeinhowit isconnected,changingtheconnec-tionsbetweentheremainingsymptoms.Inthecaseofsymptoms that are present in different disorders, iftheyareremovedfromthenetwork,theconnectionsbetween the remaining symptoms stay mostly un-changed, but a reduction in the strength of theconnections takes place. Since a highly and stronglyconnectedpsychopathologicalnetwork is thought tobemoreresistanttochange(Borsboom,2017),theseresults suggest that targeting a specific symptom,more than promoting faster dissolution of the net-work, can have more specific consequences, likehalting the progression of the disorder. Therefore,since acting on inter-modular symptoms breaks theconnectionbetweendisordersandactingonoverlap-pingsymptomsreducestheresistanceofthenetworkto change, more than recognizing the most centralsymptoms, it seems important to identify the symp-toms roles in order to developprecision treatments(i.e. treatments specifically developed for targetingsymptomswithaparticularroleinaspecificnetwork),

Comorbiditynetworkofbipolardisorderandborderlinepersonalitydisorder____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45 page42
that can allow therapists to fasten the resolutionofthe pathology and to prevent the development ofmorecomplexpathologieswithinterventionsdirectedat those symptoms that connected the disorders orthatarestrengtheningthenetworknotallowingforaproper resolution of the pathology. As proposed byprevious studies in network analysis, the centralitymeasures(i.e.strength,betweenness,andcloseness)wereassociatedwiththeimpactonthenetwork(e.g.Friedetal.,2016;Richetinetal.,2017).However,thisimpactismainlystructural;andwithoutawell-definedrole for these symptoms, it is harder to predict theoutcomeofaninterventioninthosesymptoms.Over-all, our results indicate that the identification ofdifferentrolesforthesymptomsmighthelpwiththedifferential diagnosis by distinguishing between dis-tinctiveandbridgesymptoms.Inaddition,itcanalsohelp us to map possible pathways of developmentthat would allow us to foresee the emergence ofcomorbiditywithotherdisordersandpromoteanim-provementinpsychologicaltreatments.Ourresultsshouldbecarefullyinterpretedduetotheuseofacommunity-basedsamplethatmightnotberepresentative of clinical populations. Moreover,symptomsofBDwereassessedbyadiagnosticinter-view which follows a skip logic, meaning that ifparticipantsdonotanswerpositivelytothescreeningquestions of a specific disorder, the following ques-tions pertaining the remaining symptoms are notdone.Wefollowedthesameprocedureusedinprevi-ousstudies(e.g.,Boschlooetal.,2015)andconsideredskip related missing values correspond to absentsymptomsbutthismayhavehadanimpactonthees-timationoftheconnectionsbetweenthesymptoms.Theresultsofthecomparisonbetweenthestructureofthecomorbiditynetworkwiththediagnosticstruc-ture proposed by the DSM-5 should be interpretedcautiouslybecausedatawascollectedonthebasisoftheDSM-III-R.Despitethis,therearenofundamentaldifferencesbetweentheDSM-III-RandtheDSM-5cri-teria for thedisorders studied in thispaper (Mason,Brown,&Croarkin,2016).Theseissues,addedtotheneedtoresorttonon-specificquestionstoencompassall the symptoms of BPDmight have influenced theidentificationof themodules. In thisway, future re-searchshouldaimtoreplicatetheseresults,especially
in clinical samples, and differentiate other roles forsymptomssinceitsplausiblethatmorequalitativedif-ferences exist between them. Another importantresearchtopicistoempiricallytesttheassociationofthe impact in thenetworkwithothermeasuresandrolesbecauseitcanallowustodevelopmoreefficientandprecisetreatments.
ReferencesAfzali,M.,Sunderland,M.,Teesson,M.,Carragher,N.,Mills,
K.,&Slade,T.(2016).Anetworkapproachtothecomorbid-ity between posttraumatic stress disorder and majordepressive disorder: the role of overlapping symptoms.Journal of Affective Disorders, 208, 490-496. doi:10.1016/j.jad.2016.10.037
Akiskal,H.S.,(2004).Demystifyingborderlinepersonality:cri-tique of the concept and unorthodox reflections on itsnaturalkinshipwiththebipolarspectrum.ActaPsychiatricaScandinavica, 110(6), 401–407. doi: 10.1111/j.1600-0447.2004.00461.x
Akiskal,H.S.,Benazzi,F.,Perugi,G.,&Rihmer,Z.(2005).Agi-tated “unipolar” depression re-conceptualized as adepressive mixed state: implications for the antidepres-sant-suicide controversy. Journal of Affective Disorders,85(3),245–258.doi:10.1016/j.jad.2004.12.004
AmericanPsychiatricAssociation(2013).DiagnosticandSta-tistical Manual of Mental Disorders (5th edition).Washington:UnitedStatesofAmerica.
Anderson,A.,Locke,J.,Kretzmann,M.,Kasari,C.(2016).Socialnetwork analysis of childrenwith autism spectrumdisor-der: predictors of fragmentation and connectivity inelementaryschoolclassrooms.Autism,20(6),700–709.doi:10.1177/1362361315603568.Social
Angst,J.(2013).BipolardisordersinDSM-5:strengths,prob-lems and perspectives. International Journal of BipolarDisorders,1(12),1-3.doi:10.1186/2194-7511-1-12
Armour,C.,Fried,E.,Deserno,K.,Tsai,J.,&Pietrzak,H.(2016).AnetworkanalysisofDSM-5posttraumaticstressdisordersymptomsandcorrelatesinU.S.militaryveterans.Journalof Anxiety Disorders, 45, 49–59. doi:10.1016/j.janxdis.2016.11.008
Barrat,A.,Barthelemy,M.,Pastor-Satorras,R.,&Vespignani,A.(2004).Thearchitectureofcomplexweightednetworks.Proceedings of the National Academy of Sciences of theUnited States of America, 101(11), 3747-3752. doi:10.1073/pnas.0400087101
Barroilhet,S.,Vöhringer,P.A.,&Ghaemi,S.N.(2013).Border-line versus bipolar: differences matter. Acta PsychiatricaScandinavica,128(5),385–386.doi:10.1111/acps.12107
Bayes,A.J.,&Parker,G.B.(2017).Clinicalvs.DSMdiagnosisof bipolar disorder, borderline personality disorder andtheir co-occurrence. Acta Psychiatrica Scandinavica,135(3),259–265.doi:10.1111/acps.12678Beard,C.,Millner,J.,Forgeard,C.,Fried,I.,Hsu,J.,Treadway,
T.,&Björgvinsson,T.(2016).Networkanalysisofdepres-sionandanxietysymptomrelationships inapsychiatricsample.PsychologicalMedicine,46(16),3359–3369.doi:10.1017/S0033291716002300

Castroetal____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page43
Bekhuis,E.,Schoevers,A.,vanBorkulo,D.,Rosmalen,M.,&Boschloo,L.(2016).Thenetworkstructureofmajorde-pressive disorder, generalized anxiety disorder andsomatic symptomatology. Psychological Medicine,46(14),1–10.doi:10.1017/S0033291716001550
Benazzi,F. (2005).Borderlinepersonality-bipolarspectrumrelationship.ProgressinNeuro-PsychopharmacologyandBiological Psychiatry, 30(1), 68–74. doi:10.1016/j.pnpbp.2005.06.010
Benazzi,F.(2008).ArelationshipbetweenbipolarIIdisorderandborderlinepersonalitydisorder?Progress inNeuro-Psychopharmacology and Biological Psychiatry, 32(4),1022–1029.doi:10.1016/j.pnpbp.2008.01.015
Borda, J. P. (2016). Self over time: another difference be-tween borderline personality disorder and bipolardisorder.JournalofEvaluationinClinicalPractice,22(4),603–607.doi:10.1111/jep.12550
Borsboom,D.(2017).Anetworktheoryofmentaldisorders.WorldPsychiatry16(1),5–13.doi:10.1002/wps.20375
Borsboom,D.&Cramer,A.O.J.(2013).Networkanalysis:anintegrative approach to the structure of psychopathol-ogy.AnnualReviewofClinicalPsychology,9(1),91–121.doi:10.1146/annurev-clinpsy-050212-185608
Borsboom,D.,Epskamp,S.,Kievit,R.A.,Cramer,A.O.J.,&Schmittmann, V. D. (2011). Transdiagnostic networks.PerspectivesonPsychologicalScience,6(6),610–614.doi:10.1177/1745691611425012
Boschloo,L.,VanBorkulo,C.D.,Rhemtulla,M.,Keyes,K.M.,Borsboom, D., & Schoevers, R. A. (2015). The networkstructure of symptoms of the diagnostic and statisticalmanualofmentaldisorders.PLOSONE,10(9),1–12.doi:10.1371/journal.pone.0137621
Calvo,N.,Valero,S., Sáez-Francàs,N.,Gutiérrez,F.,Casas,M.,&Ferrer,M.(2016).BorderlinepersonalitydisorderandpersonalityinventoryforDSM-5(PID-5):dimensionalpersonalityassessmentwithDSM-5.ComprehensivePsy-chiatry, 70, 105–111. doi:10.1016/j.comppsych.2016.07.002
Cassano,B.,Mula,M.,Rucci,P.,Miniati,M.,Frank,E.,Kup-fer, J., & Fagiolini, A. (2009). The structure of lifetimemanic-hypomanic spectrum. Journal of Affective Disor-ders,112(1–3),59–70.doi:10.1016/j.jad.2008.04.019
Collins,F.S.&Varmus,H.(2015).Anewinitiativeonpreci-sion medicine. The New England Journal of Medicine,372(9),793-795.doi:10.1056/NEJMp1500523
Cramer,A.,Waldorp,L.,Maas,H.,&Borsboom,D. (2010).Comorbidity: a network perspective. Behavioral andBrain Sciences, 33(2), 137–193.doi:10.1017/S0140525X09991567
diGiacomo,E.,Aspesi,F.,Fotiadou,M.,Arntz,A.,Aguglia,E.,Barone,...,Clerici,M.(2017).Unblendingborderlineper-sonality and bipolar disorders. Journal of PsychiatricResearch, 91, 90–97. doi:10.1016/j.jpsychires.2017.03.006
Eaton, R. (2015). Latent variable and network models ofcomorbidity:towardanempiricallyderivednosology.So-cialPsychiatryandPsychiatricEpidemiology,50(6),845–849.doi:10.1007/s00127-015-1012-7
Eisner, R., Johnson, L., Youngstrom, A., & Pearlstein, G.(2017).Simplifyingprofilesofcomorbidityinbipolardis-order.JournalofAffectiveDisorders,220,102–107.doi:10.1016/j.jad.2017.05.045
Epskamp,S.,&Fried,I.(2017).Bootnet:Bootstrapmethodsforvariousnetworkestimationroutines.Rpackagever-sion 1.0.1. Retrieved from http://cran.r-project.org/package=bootnet.
Epskamp, S., Borsboom, D., & Fried, I. (2016). Estimatingpsychologicalnetworksandtheiraccuracy:atutorialpa-per. Behavior ResearchMethods, 50(10), 195-212. doi:10.3758/s13428-017-0862-1
Epskamp, S., Cramer, A.,Waldorp, J., Schmittmann, D., &Borsboom,D. (2012). qgraph: network visualizations ofrelationships inpsychometricdata.JournalofStatisticalSoftware,48(4).doi:10.18637/jss.v048.i04
Ferentinos, P., Fountoulakis, N., Lewis, M., Porichi, E.,Dikeos,D.,Papageorgiou,C.,&Douzenis,A.(2017).Vali-dating a two-dimensional bipolar spectrum modelintegrating DSM-5’s mixed features specifier for majordepressivedisorder.ComprehensivePsychiatry, 77, 89–99.doi:10.1016/j.comppsych.2017.06.007
Fernandez,E.,&Johnson,L.(2015).Angerinpsychologicaldisorders: prevalence, presentation, etiology and prog-nosticimplications.ClinicalPsychologyReview,46,124–135.doi:10.1016/j.cpr.2016.04.012
Fisher,A.J.(2015).Towardadynamicmodelofpsychologi-cal assessment: implications for personalized care.JournalofConsultingandClinicalPsychology,83(4),825–836.doi:10.1037/ccp0000026
Fisher,A.J.,&Boswell,J.F.(2016).Enhancingthepersonal-izationof psychotherapywithdynamic assessment andmodeling. Assessment, 23(4), 496–506. doi:10.1177/1073191116638735
Fonseka, T. M., Swampillai, B., Timmins, V., Scavone, A.,Mitchell,R.,Collinger,K.A.,&Goldstein,B.I.(2015).Sig-nificance of borderline personality-spectrum symptomsamongadolescentswithbipolardisorder.JournalofAf-fective Disorders, 170, 39–45. doi:10.1016/j.jad.2014.08.046
Frías,Á.,Baltasar,I.,&Birmaher,B.(2016).Comorbiditybe-tween bipolar disorder and borderline personalitydisorder: prevalence, explanatory theories, and clinicalimpact.JournalofAffectiveDisorders,202,210–219.doi:10.1016/j.jad.2016.05.048
Fried,E.,Epskamp,S.,Nesse,R.,Tuerlinckx,F.,&Borsboom,D.(2016).Whatgooddepressionsymptoms?comparingthecentralityofDSMandnon-DSMsymptomsofdepres-sioninanetworkanalysis.JournalofAffectiveDisorders,189,314-320.doi:10.1016/j.jad.2015.09.005
Fried, E., van Borkulo, D., Cramer, A., Boschloo, L.,Schoevers,A.,&Borsboom,D.(2017).Mentaldisordersasnetworksofproblems:areviewofrecentinsights.So-cialPsychiatryandPsychiatricEpidemiology,52(1),1–10.doi:10.1007/s00127-016-1319-z
Fruchterman, T., & Reingold, E. (1991). Graph drawing byforcedirectedplacement.Software-PracticeandExperi-ence.21(11),1129-1164.doi:10.1002/spe.4380211102
Galione, J.&Zimmerman,M. (2010).Acomparisonofde-pressedpatientswithandwithoutborderlinepersonalitydisorder: implicationsfor interpretingstudiesoftheva-lidity of the bipolar spectrum. Journal of PersonalityDisorders, 24(6), 763–772. doi:10.1521/pedi.2010.24.6.763

Comorbiditynetworkofbipolardisorderandborderlinepersonalitydisorder____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45 page44
Ghaemi,N.,Dalley,S.,Catania,C.,&Barroilhet,S.(2014).Bi-polarorborderline:aclinicaloverview.ActaPsychiatricaScandinavica,130(2),99–108.doi:10.1111/acps.12257
Goekoop,R.&Goekoop,J.G.(2014).Anetworkviewonpsy-chiatric disorders: network clusters of symptoms aselementary syndromes of psychopathology. PLOS ONE,9(11),1–47.doi:10.1371/journal.pone.0112734
Goodwin,F.&Jamison,K.(2007).Manic-DepressiveIllnessBipolar Disorders and Recorrent Depression. New York:Oxford.
Grant, B., Stinson, F., Dawson, D., Chou, P., Dufour, M.,Compton,W.Pickering,R.,Kaplan,K.(2006).Prevalenceandco-occurrenceofsubstanceusedisordersandinde-pendentmood and anxiety disorders: results from thenational epidemiologic survey on alcohol and relatedconditions.Alcohol Research&Health, 29(2), 107–120.doi:10.1001/archpsyc.61.8.807
Hatchett,G.(2010).Differentialdiagnosisofborderlineper-sonalitydisorderfrombipolardisorder.JournalofMentalHealth Counseling, 32(3), 189–205. doi:10.17744/mehc.32.3.n682682184554445
Henry,C.,Mitropoulou,V.,New,S.,Koenigsberg,W.,Silver-man, J., & Siever, J. (2001). Affective instability andimpulsivityinborderlinepersonalityandbipolarIIdisor-ders: similarities and differences. Journal of PsychiatricResearch, 35(6), 307–312. doi: 10.1016/S0022-3956(01)00038-3
Hirschfeld,M.,Lewis,L.,&Vornik,L.(2003).Perceptionsandimpactofbipolardisorder:howfarhavewereallycome?resultsofthenationaldepressiveandmaniac-depressiveassociation2000surveyofindividualswithbipolardisor-der. Journal of Clinical Psychology, 64(2), 161-74. doi:10.4088/JCP.v64n0209
Isvoranu,M.,Borsboom,D.,vanOs,J.,&Guloksuz,S.(2016).A network approach to environmental impact in psy-chotic disorder: brief theoretical framework.Schizophrenia Bulletin, 42(4), 870–873. doi:10.1093/schbul/sbw049
JASP Team. (2016). JASP (Version 0.8.0.0). Retrieved fromhttps://jasp-stats.org/
Jones,P.(2017).Impact:anewnetworkstatisticfornet-workanalysis(networktools).Rpackageversion1.2.0.Retrievedfromhttp://cran.r-project.org/package=net-worktools.
Jones,J.,Mair,P.,Riemann,B.C.,Mugno,B.L.,&McNally,R.J.(2017).Anetworkperspectiveoncomorbiddepres-sion inadolescentswithobsessive-compulsivedisorder.Journal of Anxiety Disorders, 53, 1-8. doi:10.1016/j.janxdis.2017.09.008
Kessler,B., Borges, E.,&Walters, E. (1999). Prevalenceofand risk factors for lifetime suicide attempts in thena-tionalcomorbiditysurvey.ArchivesofGeneralPsychiatry,56(7),617–626.doi:10.1001/archpsyc.56.7.617
Kessler,R.C.&Üstün,B.B.(2004).Theworldmentalhealth(WMH)survey initiativeversionof theworldhealthor-ganization (WHO) composite international diagnosticinterview(CIDI).InternationalJournalofMethodsinPsy-chiatricResearch,13(2),93–117.doi:10.1002/mpr.168
Koenigsberg,H.W.,Harvey,P.D.,Mitropoulou,V.,Schmeid-ler, J., New,A. S., Goodman,M.,& Siever, L. J. (2002).Characterizingaffectiveinstabilityinborderlinepersonal-itydisorder.AmericanJournalofPsychiatry,159(5),784–788.doi:10.1176/appi.ajp.159.5.784
Levinson,A.,Zerwas,S.,Calebs,B.,Kordy,H.,Hofmeier,S.,Collaborative,V.,&Bulik,M.(2017).Thecoresymptomsof bulimia nervosa, anxiety, anddepression: a networkanalysis. Journal of Abnormal Psychology, 126(3), 340–354.doi:10.1037/abn0000254
Lewis,K.,Caputi,P.,&Grenyer,B.(2012).Boderlineperson-alitydisorder subtypes: a factor analysisof theDSM IVcriteria. Personality and Mental Health, 6(3), 196-206.doi:10.1002/pmh.1183
Malhi,S.,Fritz,K.,Allwang,C.,Burston,N.,Cocks,C.,Devlin,J.,&Lyndon,W.(2016).Aremanicsymptomsthat“dip”intodepressiontheessenceofmixedfeatures?JournalofAffective Disorders, 192, 104–108. doi:10.1016/j.jad.2015.12.009
Mason,B.L.,Brown,E.S.,&Croarkin,P.E.(2016).Historicalunderpinningsofbipolardisorderdiagnosticcriteria.Be-havioralSciences,6(14),1-19.doi:10.3390/bs6030014
McDermid,J.,Sareen,J.,El-Gabalawy,R.,Pagura,J.,Spiwak,R.,&Enns,M.W.(2015).Co-morbidityofbipolardisorderandborderlinepersonalitydisorder:findingsfromthena-tional epidemiologic survey on alcohol and relatedconditions. Comprehensive Psychiatry, 58, 18–28. doi:10.1016/j.comppsych.2015.01.004
Messer, T., Lammers, G.,Müller-Siecheneder, F., Schmidt,R.-F.,&Latifi,S.(2017).Substanceabuseinpatientswithbipolardisorder:asystematicreviewandmeta-analysis.Psychiatry Research, 253, 338–350. doi: 10.1016/j.psy-chres.2017.02.067
Morris, R., Yang,M., Chopra, A., Bentall, R., Paykel, E., &Scott,J.(2013).Differentialeffectsofdepressionandma-niasymptomsonsocialadjustment:prospectivestudyinbipolar disorder. Bipolar Disorders, 15(1), 80–91. doi:10.1111/bdi.12036
Opsahl,T.,Agneessens,F.,&Skvoretz,J.(2010).Nodecen-trality in weighted networks: Generalizing degree andshortest paths. Social Networks, 32, 245-25. doi:10.1016/j.socnet.2010.03.006
Paris,J.,Gunderson,J.,&Weinberg,I.(2007).Theinterfacebetween borderline personality disorder and bipolarspectrum disorders. Comprehensive Psychiatry, 48(2),145–154.doi:10.1016/j.comppsych.2006.10.001
Pennay,A.,Cameron,J.,Reichert,T.,Strickland,H.,Lee,N.K.,Hall,K.,&Lubman,D.I.(2011).Asystematicreviewofinterventions for co-occurring substance use disorderandborderlinepersonalitydisorder.JournalofSubstanceAbuse Treatment, 41(4), 363–373. doi:10.1016/j.jsat.2011.05.004
Perugi,G.,Angst, J.,Azorin, J.M.,Bowden,C.,Vieta,E.,&Young, A. H. (2013). The bipolar-borderline personalitydisordersconnection inmajordepressivepatients.ActaPsychiatrica Scandinavica, 128(5), 376–383. doi:10.1111/acps.12083
RDevelopmentCoreTeam.(2008).R:Alanguageandenvi-ronment for statistical computing. Vienna, Austria: RFoundationforStatisticalComputing.
Rhemtulla,M.,Fried,E.,Aggen,H.,Tuerlinckx,F.,Kendler,S.,&Borsboom,D.(2016).Networkanalysisofsubstanceabuseanddependencesymptoms.DrugandAlcoholDe-pendence, 161, 230–237. doi:10.1016/j.drugalcdep.2016.02.005
Richetin,J.,Preti,E.,Costantini,G.,&DePanfilis,C.(2017).Thecentralityofaffectiveinstabilityandidentityinbor-derline personality disorder: evidence from network

Castroetal____________________________________________________________________________________________________________
www.psyprjournal.comPPRJ.Vol1.Number1.July2018|DOI:https://doi.org/10.33525/pprj.v1i1.45
page45
analysis. PLOS ONE, 12(10). doi: 10.1371/jour-nal.pone.018669
Robins,L.,Wing,J.,Wittchen,U.,Helzer,J,Babor,T.,Burke,J.,Farmer,A.,Jablenski,A.,Pickens,R.,Regier,D.,Sarto-rius,N.&Towle,L. (1998).Thecomposite internationaldiagnostic interviewanepidemiologic instrument suita-ble for use in conjunction with different diagnosticsystemsandindifferentcultures.ArchivesofGeneralPsy-chiatry, 45(12), 1069-1077. doi:10.1001/archpsyc.1988.01800360017003
RStudioTeam(2017).RStudio:IntegratedDevelopmentforR. RStudio, Inc., Boston, MA URL http://www.rstu-dio.com/.
Ruggero,C.J.,Zimmerman,M.,Chelminski, I.,&Young,D.(2010).Borderlinepersonalitydisorderandthemisdiag-nosisofbipolardisorder.JournalofPsychiatricResearch,44(6),405–408.doi:10.1016/j.jpsychires.2009.09.011
Rugkåsa, J., Yeeles,K.,Molodynski,A.,&Burns, T. (2015).Reply.ActaPsychiatrica Scandinavica, 132(4), 310–310.doi:10.1111/acps.12465
Shannon,P.,Markiel,A.,OwenOzier,2,Baliga,N.S.,Wang,J.T.,Ramage,D.,Amin,N.,Schwikowski,B,&Ideker,T.(2003).Cytoscape:asoftwareenvironmentforintegratedmodels of biomolecular interaction networks.GenomeResearch, 13(11), 2498–2504. doi:10.1101/gr.1239303.metabolite
Siegel, R., Hoeppner, B., Yen, S., Stout, R., Weinstock, L.,Hower,H.,Birmaher,B.,Goldstein,T.,Goldstein,B.,Hunt,J.,Strober,M.,Axelson,D.,Gill,M.,&Keller,M.(2015).Longitudinal associations between interpersonal rela-tionshipfunctioningandmoodepisodeseverityinyouthwithbipolardisorder.JournalofNervousandMentalDis-ease, 203(3): 194–204. doi:10.1097/NMD.0000000000000261
Soler,A.,Soler,J.,Elices,M.,Pascual,J.C.,Pérez,J.,Martín-Blanco,A.,&Portella,M.J.(2013).Differencesinatten-tion and impulsivity between borderline personality
disorder and bipolar disorder. Psychiatry Research,210(3),1307–1309.doi:10.1016/j.psychres.2013.09.011
Szalay-Beko, M., Palotai, R., Szappanos, B., Kovács, I. A.,Papp,B.,&Csermely,P.(2012).ModuLandplug-inforcy-toscape: determination of hierarchical layers ofoverlappingnetworkmodulesandcommunitycentrality.Bioinformatics,28(16),2202–2204.doi:10.1093/bioinfor-matics/bts352
vanBorkulo,C.D.,Borsboom,D.,Epskamp,S.,Blanken,T.F.,Boschloo,L.,Schoevers,R.a,&Waldorp,L. J. (2014).Anewmethodforconstructingnetworksfrombinarydata.ScientificReports,4(5918).doi:10.1038/srep05918
van Borkulo, C., Boschloo, L., Borsboom, D., Penninx, H.,Waldorp,J.,&Schoevers,A.(2015).Associationofsymp-tom network structure with the course of longitudinaldepression. JAMA Psychiatry, 72(12), 1219-26.doi:10.1001/jamapsychiatry.2015.2079
Vöhringer,A.,Barroilhet,A.,Alvear,K.,Medina,S.,Espinosa,C.,Alexandrovich,K.,Riumallo,P.,Leiva,F.,Hurtado,E.,Cabrera, J., Sullivan,M.,Holtzman,N.,&Ghaemi, S.N.(2016). The international mood network nosology pro-ject:differentiatingborderlinepersonalitydisorderfrombipolar illness. Acta Psychiatrica Scandinavica, 134(6),504-510.doi:10.1111/acps.12643
Wilson,T.,Stanley,B.,Oquendo,A.,Goldberg,P.,Zalsman,G.,&Mann,J.(2007).Comparingimpulsiveness,hostility,anddepressioninborderlinepersonalitydisorderandbi-polar II disorder. Journal of Clinical Psychiatry, 68(10),1533–9.doi:10.1001/archpsyc.1992.01820080032005
Zimmerman,M.,&Morgan, T. A. (2013). The relationshipbetweenborderlinepersonalitydisorderandbipolardis-order.DialoguesinClinicalNeuroscience,15(2),155–169.doi:10.1176/appi.ajp.163.7.1126
Zimmerman,M.,Martinez,J.,Young,D.,Chelminski,I.,Mor-gan, A., & Dalrymple, K. (2014). Comorbid bipolardisorderandborderlinepersonalitydisorderandhistoryof suicide attempts. Journal of Personality Disorders,28(3),358-364.doi:10.1521/pedi_2013_27_122
.