30. clinical narratives context categorization: the...
TRANSCRIPT
Clinical Narratives Context Categorization: The
Clinician Approach using RapidMiner
Osama Mohammed1, Sabah Mohammed
2, Jinan Fiaidhi
2, Simon Fong
3,
Tia-hoon Kim4
1SimBioSys Laboratory, University of Victoria,
3800 Finnerty Road,Victoria, British Columbia V8W 3P6, Canada 2Department of Computer Science, Lakehead University,
Thunder Bay, Ontario P7b 5E1, Canada 3Department of Computer and Information Science
University of Macau, Av. Padre Tomas Pereira, Taipa, Macau 4Department of Convergence Security, Sungshin W. University, Korea
[email protected], {mohammed,jfiaidhi}@lakeheadu.ca, [email protected],
Abstract. For many years natural language processing (NLP) programming
tools have been used to process information in various applications areas
including medicine. However, most of such systems have been developed by
expert programmers and very little or none by clinicians. The subject under
consideration in this article is automatic categorization of clinical data. This
topic requires great deal of clinical cognition and hence there is a need to let
clinicians develop such systems. This article is an attempt in this direction
where the RapidMiner environment has been used for this purpose. This article
describes how RapidMiner as a visual programming environment can be used
for tokenization and categorization of clinical narratives. It also describes how
to select the best classifier for categorization. K-NN classifier categorizes
clinical narratives with high performance accuracies even for large dataset like
the i2b2 smoking challenge data.
Key words: Clinical Narratives Categorization, Tokenization, RapidMiner,
Context-Awareness
1 Introduction
Automated categorization of textual clinical narratives is an important research
challenge due to the ever-increasing electronic clinical documents. Automatic Text
Categorization (ATC) is formally defined as a classification task: given a textual input,
the categorizer should return a list of categories, which are supposed to provide non-
ambiguous machine-readable information about the input text. ATC assists medical
studies by providing statistically relevant data for analysis [1]. The ATC assigns
semantic labels to the clinical narratives, such as whether a clinical narrative is a
radiology report or a discharge summary. However, the first step to any ATC system
Advanced Science and Technology Letters Vol.51 (SIA 2014), pp.128-138
http://dx.doi.org/10.14257/astl.2014.51.30
ISSN: 2287-1233 ASTL Copyright © 2014 SERSC
is the tokenization of the provided text. Tokenization is the process of separating text
into individual tokens that each conveys some semantic meaning. For English, in
most cases, tokens are equivalent to words. For clinical text, there are often names
and symbols of various types of biomedical entities, such as medications, genes,
proteins, chemicals, etc. The special characters contained in these names and symbols
make it harder to identify meaningful tokens than in normal English text [2]. This
means tokenization should manage language related word dependencies, incorporate
domain specific knowledge and handle morph syntactically relevant specificities [3].
Literature reveals three types of semantically enriched tokenizers:
(1) Rule-Based Tokenizers [4]: Regular Expressions are commonly used for writing
the rules that can identify relevant tokens corresponding to the entity of interest.
Tomanek et al [5] have studied tokenization of biomedical texts by using regular
expression rules for tokenizing biomedical common text. He concluded that this
approach is quite complex, since biomedical authors tend to adopt different, and
sometimes inconsistent, notations. The notation used to write biomedical entity
names, abbreviations, chemical formulas and bibliographic references conflicts
with the general regular expression rules employed for tokenizing common text.
(2) Classification-Based Tokenizers [6]: This tokenization method consists of text
classifiers (e.g. Conditional Random Fields (CRF)) to perform mainly two tasks:
(i) token boundary detection and (ii) sentence boundary recognition. The
classifier is trained by a token sequence when tokens are annotated by single
labels. Tokens are represented by their feature vectors. Typical features are
binary properties, for example, whether the token matches a pattern. Based on the
sequence of labels in training documents and the observed corresponding feature
vectors, the classifier learns the relations between labels and features, and builds
a discriminative model that is applied to predict the most likely label sequence of
unlabeled token sequences. The predictive performance of a classifier model
depends heavily on the dataset applied.
(3) Token Disambiguation Tokenizers [7,8]: This tokenization method uses a
probabilistic model for token disambiguation which chooses the best sense based
on the conditional probability of sense paraphrases given a context.
These three tokenization methods as well as many other hybrid methods lack the
ability to adapt to the document context due to following strict engineering approach
(i.e. one in which developers may focus less (or not at all) on the human factors that
result in or otherwise exhibit learning, memory, expertise, and other features;
cognitive plausibility is not a major concern in such work) [9]. Tokenization requires
several cognitive processing modalities, linguistically-based or otherwise. Our
position in this paper is to integrate some human cognition capabilities as part of the
process of tokenization and document categorization. This integration requires a
promising environment where clinicians can use for implementing, modeling, and
studying document categorization. The integration does not mean that document
categorization will be semi-automatic as it will only be used during the development
process by clinicians. We find RapidMiner as an environment fits this requirement.
2 RapidMiner for Tokenization and Categorization
Advanced Science and Technology Letters Vol.51 (SIA 2014)
Copyright © 2014 SERSC 129

RapidMiner1 is a Java framework that can be programmed via Java
2 and R
3 languages.
RapidMiner provides many built-in processes for data mining (e.g. Text Processing,
Information Extraction) and NLP (e.g. Tokenization, Removal of Stop Words, Part of
Speech Tagging and Stemming). The framework became a leading programming
environment in the paradigm of business intelligence and recently started to be notable
in other fields including in healthcare. The framework offers ease of integration of
various operators (i.e. built in or programmed) using very attractive visual designing
interface. This interface does not requires programming experience and one can use
pipeline and program variety of operators using drag, past and connect approach. This
capability allows for the intervention of experts and developers to envision the
categorization system as well as enhance it and modify it by changing connections and
parameters on the visual interface. Moreover, RapidMiner provides variety of
semantic support through three notable plugins (RMonto4, ISPR
5 and Recommender
Systems6) that can be used for context awareness. These extensions as well as the
programming power of both Java and R, let RapidMiner to be one of the best
environments that we would like to start our investigation with on developing a context
aware tokenization and categorization approach. The following experiments are an
attempt in this direction.
3 Categorizing Clinical Narratives
In order to identify the context of a text written for the purpose of clinical narrative,
need to use samples of such clinical narratives from an authentic and reliable source.
For this purpose we collected equal number of clinical narratives from the
MTSamples.com7 which is a web repository designed to give you access to a big
collection of transcribed medical reports. We collected equal number of samples from
eight different clinical categories (Autopsy, Diet, Discharge Summaries, Chiropractic,
Cosmetic, Dental, ENT and Radiology). We divided our collected samples into
training and testing (80% training and 20% testing) where the textual documents for
each category have been assigned to a specific directory. The task is to tokenize these
documents and generate a vectored document matrix that can be used for categorizing
the context of each of the provided clinical documents. This can be done using the
RapidMiner visual interface by dragging the “Process Document From File” operator
and place it on the design stage. By double clicking this operator, we can start dragging
on it generated design stage all the processes required for tokenization, preprocessing
(e.g. converting to lower cases), tokens identification, elimination of stop words,
stemming and selecting words with min and max number of characters (i.e. NGrams).
Figure 1 describes the tokenization process.
1 http://rapidminer.com/
2 http://www-ai.cs.uni-dortmund.de/SOFTWARE/RMD/index.html
3 http://www.e-lico.eu/r-extension.html
4 http://www.e-lico.eu/rmonto.html
5 http://prules.org/doku.php/download:ispr
6 http://www.e-lico.eu/recommender-extension.html
7 http://www.mtsamples.com/
Advanced Science and Technology Letters Vol.51 (SIA 2014)
130 Copyright © 2014 SERSC
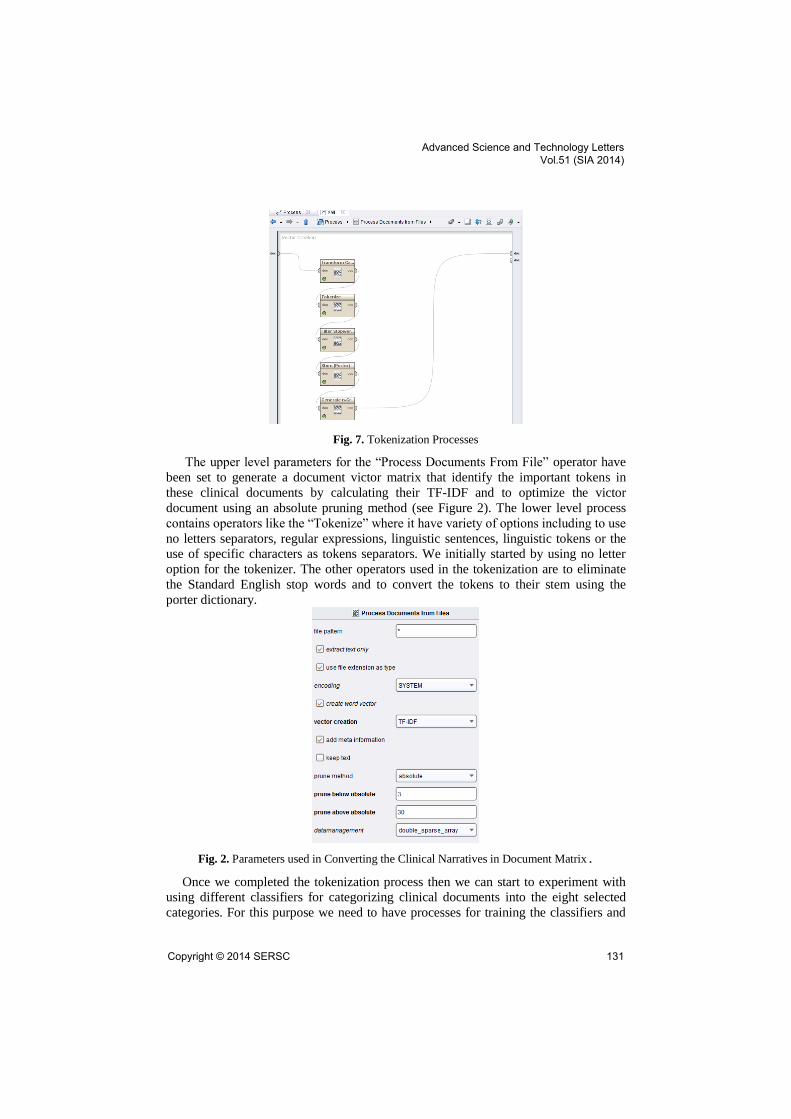
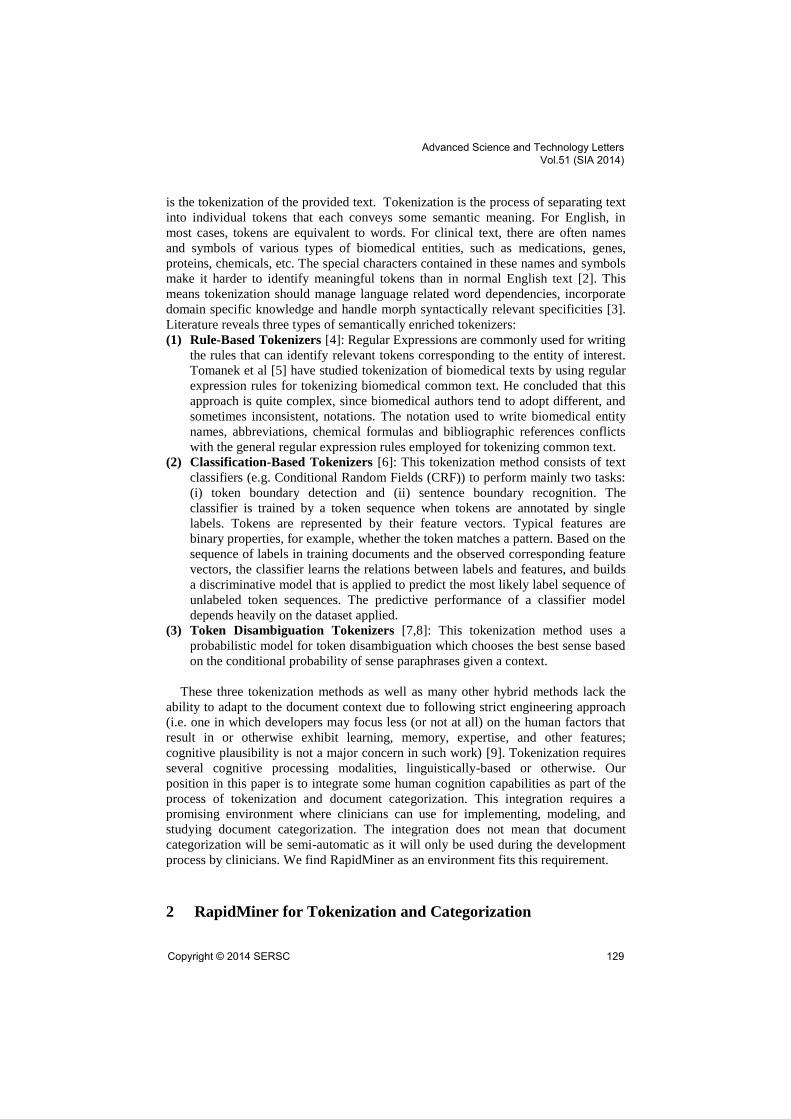
Fig. 7. Tokenization Processes
The upper level parameters for the “Process Documents From File” operator have
been set to generate a document victor matrix that identify the important tokens in
these clinical documents by calculating their TF-IDF and to optimize the victor
document using an absolute pruning method (see Figure 2). The lower level process
contains operators like the “Tokenize” where it have variety of options including to use
no letters separators, regular expressions, linguistic sentences, linguistic tokens or the
use of specific characters as tokens separators. We initially started by using no letter
option for the tokenizer. The other operators used in the tokenization are to eliminate
the Standard English stop words and to convert the tokens to their stem using the
porter dictionary.
Fig. 2. Parameters used in Converting the Clinical Narratives in Document Matrix.
Once we completed the tokenization process then we can start to experiment with
using different classifiers for categorizing clinical documents into the eight selected
categories. For this purpose we need to have processes for training the classifiers and
Advanced Science and Technology Letters Vol.51 (SIA 2014)
Copyright © 2014 SERSC 131

for testing the trained classifier on new provided documents that we need to know its
category. Figure 3 illustrates the upper level for the operators required to be dragged
onto the design stage. In the training part, we need to store the vectored documents and
to use a classification operator container (i.e. the Validation Operator) and to store the
resulted model of training into a store. However, the categorization process starts by
reading both the vectored documents and the stored model of classification and apply
this model on the newly provided clinical document (this requires the use of a “Process
Document from File” operator) to predict its category.
Fig. 3. Training Classifiers and Categorizing New Documents.
The validation operator generates new stage with two windows, one for the
including the classifier and the other for applying the classifier on the new provided
documents and measure the performance statistics. RapidMiner provides huge number
of classifiers (e.g. Naive Bayes, SVM, J48, JRip, ZeroR, Random Tree, K-NN) as well
as wide range of performance measures (e.g. Accuracy, Kappa Statistics, Recall,
Precision, Absolute Error, Cross Entropy and Correlation). Figure 4 illustrates the
classification and categorization container where the K-NN has been used as the
classifier.
Fig. 4. The Classification and Categorization Process of Clinical Narratives.
Based on this container for classification and categorization template, we selected
seven notable classifiers and run them against a sample of 40 clinical narratives for
each the eight different clinical categories where the test data represent 24 clinical
narratives that we need to predict its category (e.g. Autopsy, Diet, Discharge
Advanced Science and Technology Letters Vol.51 (SIA 2014)
132 Copyright © 2014 SERSC
Summaries, Chiropractic, Cosmetic, Dental, ENT and Radiology). Figure 4 illustrates
the overall accuracy of the seven selected classifiers.
Fig. 4. The Accuracy of the Seven Selected Classifiers.
K-NN proves to provide the highest accuracy (95.5%) compared to the other classifiers.
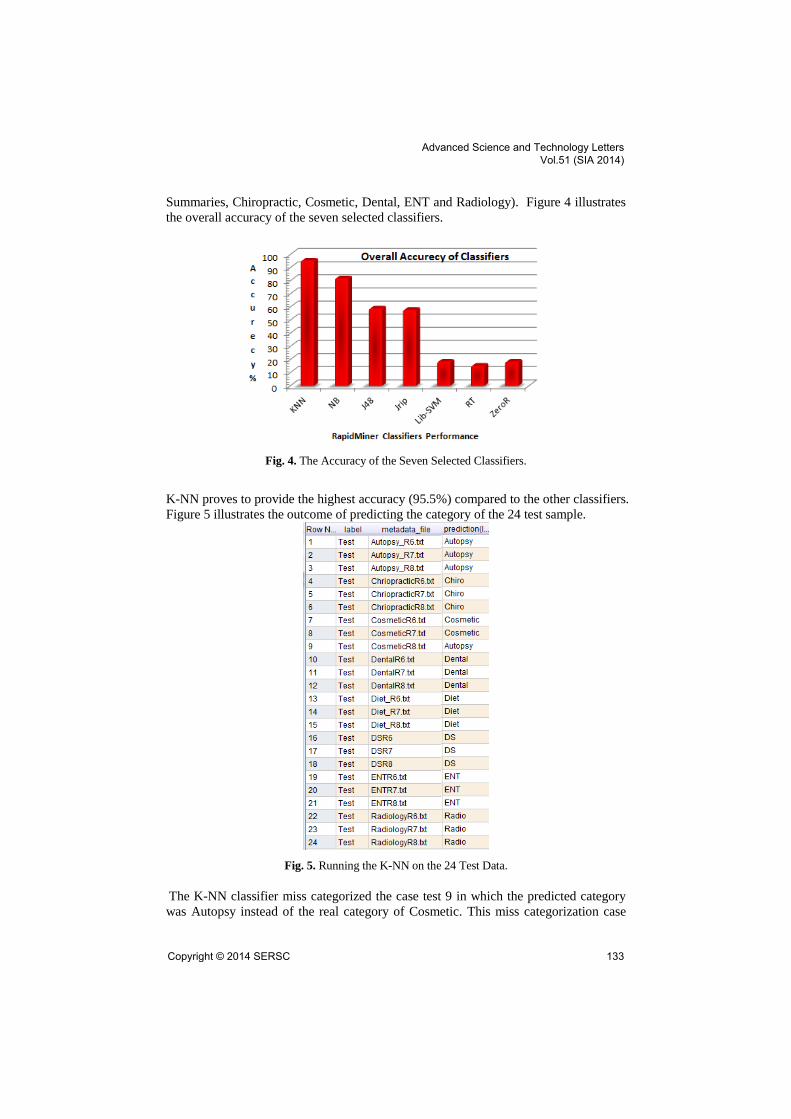
Figure 5 illustrates the outcome of predicting the category of the 24 test sample.
Fig. 5. Running the K-NN on the 24 Test Data.
The K-NN classifier miss categorized the case test 9 in which the predicted category
was Autopsy instead of the real category of Cosmetic. This miss categorization case
Advanced Science and Technology Letters Vol.51 (SIA 2014)
Copyright © 2014 SERSC 133

may be caused by using ill sensitive tokenization as the no letters separators were used
for the purpose of tokenization. However, after using more sensitive tokenization such
as identifying tokens based on the linguistic features, the accuracy have been raised to
97.5%. Moreover, one can enhance the accuracy further by choosing more careful
document vector pruning such as the absolute pruning instead of the traditional
perceptual pruning. The change has raised the accuracy to be 100%. It is also
interesting to note the precision of categorizing each class of clinical narrative. Figures
6 and 7 illustrate the precision of categorizing two classes from the eight classes of the
clinical narratives (Discharge Summaries and Chiropractic Reports).
Fig. 6. The Categorization Precision of Distinguishing Discharge Summaries from the rest of
Clinical Narratives.
Fig. 7. The Categorization Precision of Distinguishing Chiropractic Reports from the rest of
Clinical Narratives.
Moreover, the class recall is another classifier performance measure that provides
information on the goodness of a classifier. Figures 8 and 9 illustrated the class recall
of two classes (Discharge Summaries and Chiropractic Reports).
Advanced Science and Technology Letters Vol.51 (SIA 2014)
134 Copyright © 2014 SERSC
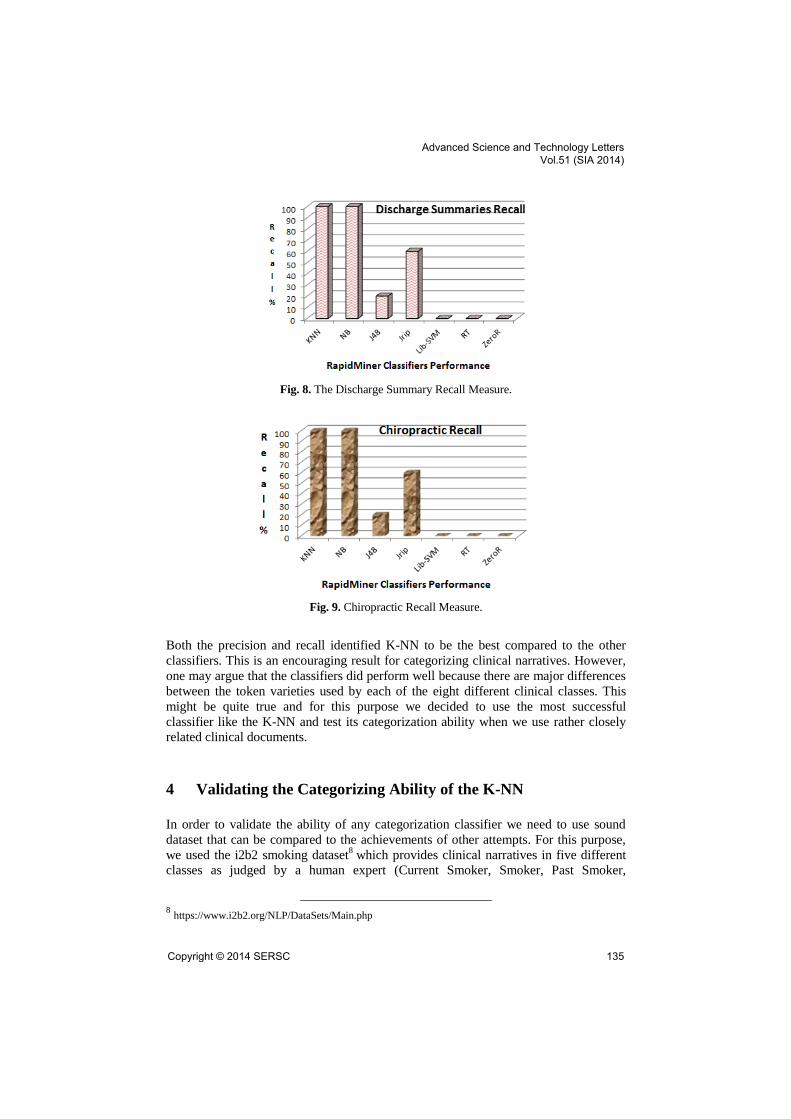
Fig. 8. The Discharge Summary Recall Measure.
Fig. 9. Chiropractic Recall Measure.
Both the precision and recall identified K-NN to be the best compared to the other
classifiers. This is an encouraging result for categorizing clinical narratives. However,
one may argue that the classifiers did perform well because there are major differences
between the token varieties used by each of the eight different clinical classes. This
might be quite true and for this purpose we decided to use the most successful
classifier like the K-NN and test its categorization ability when we use rather closely
related clinical documents.
4 Validating the Categorizing Ability of the K-NN
In order to validate the ability of any categorization classifier we need to use sound
dataset that can be compared to the achievements of other attempts. For this purpose,
we used the i2b2 smoking dataset8 which provides clinical narratives in five different
classes as judged by a human expert (Current Smoker, Smoker, Past Smoker,
8 https://www.i2b2.org/NLP/DataSets/Main.php
Advanced Science and Technology Letters Vol.51 (SIA 2014)
Copyright © 2014 SERSC 135
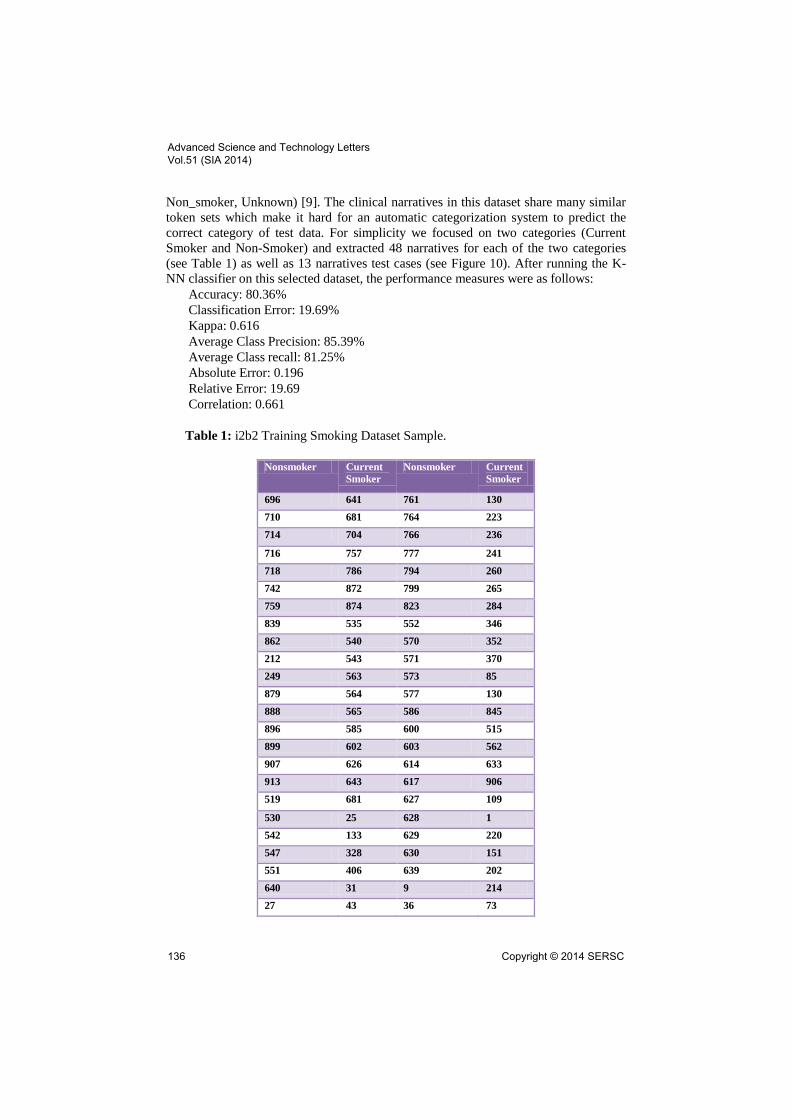
Non_smoker, Unknown) [9]. The clinical narratives in this dataset share many similar
token sets which make it hard for an automatic categorization system to predict the
correct category of test data. For simplicity we focused on two categories (Current
Smoker and Non-Smoker) and extracted 48 narratives for each of the two categories
(see Table 1) as well as 13 narratives test cases (see Figure 10). After running the K-
NN classifier on this selected dataset, the performance measures were as follows:
Accuracy: 80.36%
Classification Error: 19.69%
Kappa: 0.616
Average Class Precision: 85.39%
Average Class recall: 81.25%
Absolute Error: 0.196
Relative Error: 19.69
Correlation: 0.661
Table 1: i2b2 Training Smoking Dataset Sample.
Nonsmoker Current
Smoker
Nonsmoker Current
Smoker
696 641 761 130
710 681 764 223
714 704 766 236
716 757 777 241
718 786 794 260
742 872 799 265
759 874 823 284
839 535 552 346
862 540 570 352
212 543 571 370
249 563 573 85
879 564 577 130
888 565 586 845
896 585 600 515
899 602 603 562
907 626 614 633
913 643 617 906
519 681 627 109
530 25 628 1
542 133 629 220
547 328 630 151
551 406 639 202
640 31 9 214
27 43 36 73
Advanced Science and Technology Letters Vol.51 (SIA 2014)
136 Copyright © 2014 SERSC
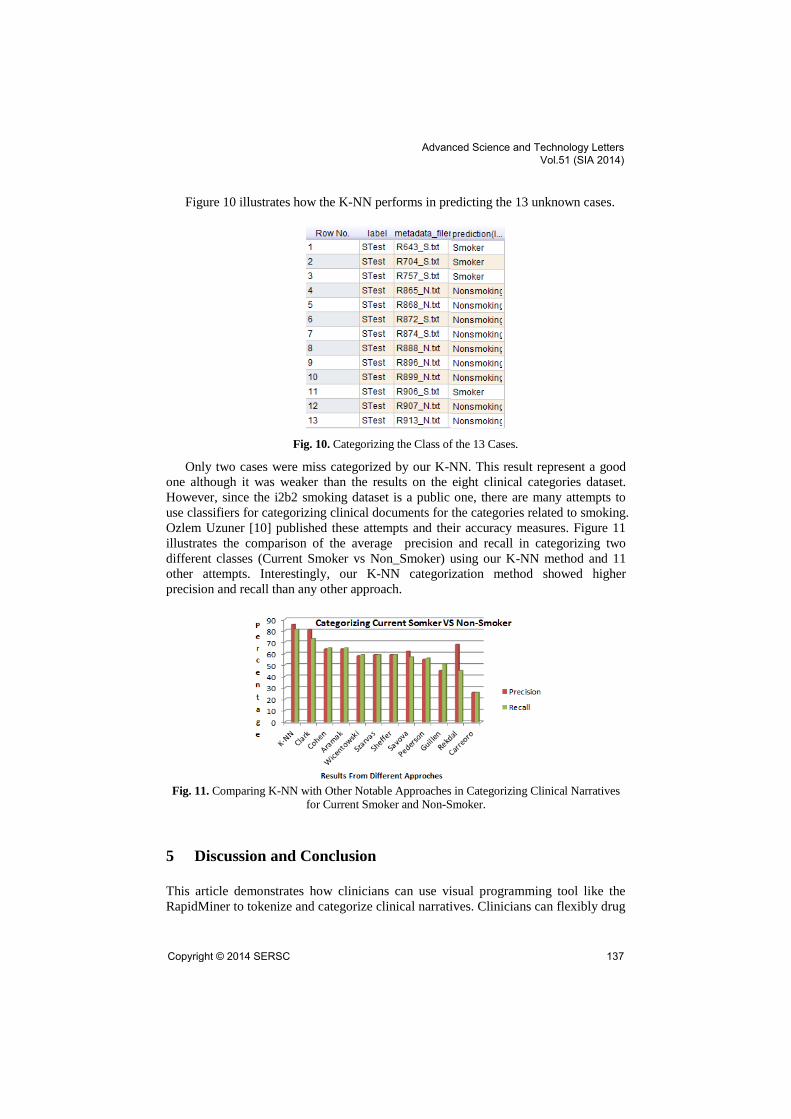
Figure 10 illustrates how the K-NN performs in predicting the 13 unknown cases.
Fig. 10. Categorizing the Class of the 13 Cases.
Only two cases were miss categorized by our K-NN. This result represent a good
one although it was weaker than the results on the eight clinical categories dataset.
However, since the i2b2 smoking dataset is a public one, there are many attempts to
use classifiers for categorizing clinical documents for the categories related to smoking.
Ozlem Uzuner [10] published these attempts and their accuracy measures. Figure 11
illustrates the comparison of the average precision and recall in categorizing two
different classes (Current Smoker vs Non_Smoker) using our K-NN method and 11
other attempts. Interestingly, our K-NN categorization method showed higher
precision and recall than any other approach.
Fig. 11. Comparing K-NN with Other Notable Approaches in Categorizing Clinical Narratives
for Current Smoker and Non-Smoker.
5 Discussion and Conclusion
This article demonstrates how clinicians can use visual programming tool like the
RapidMiner to tokenize and categorize clinical narratives. Clinicians can flexibly drug
Advanced Science and Technology Letters Vol.51 (SIA 2014)
Copyright © 2014 SERSC 137

and past variety of visual operators and change their behaviors’ via parameterizations
even for complex processes like tokenization and classifications. Several experiments
have been conducted for this purpose that reveal major findings for categorization of
clinical narratives. For example K-NN classifier outperform other classifiers in
categorizing diverse clinical reports including those narratives that include high
degree of similarity like the smoking vs nonsmoking discharge summaries. However,
this work is only our initial attempt as we are intending to enrich the categorization
process with higher sense of context-awareness. The next step that we are currently
experimenting with is to enable clinicians through RapidMiner to incorporate
ontologies in the process of tokenizing and categorizing clinical narratives. This
extension is quite possible with the RMonto plugin for RapidMiner. Clinicians can
develop their own ontologies as well as to use an existing one. This work is left to our
next research work.
References
1. Illés Solt, Domonkos Tikk, Viktor Gál and Zsolt T. Kardkovács, Semantic Classification of
Diseases in Discharge Summaries Using a Context-aware Rule-based Classifier, J Am Med
Inform Assoc. 2009 Jul-Aug; 16(4): 580–584.
2. Jing Jiang, ChengXiang Zhai, An empirical study of tokenization strategies for biomedical
information retrieval, Information Retrieval Journal, October 2007, Volume 10, Issue 4-5,
pp 341-363
3. Hassler M, Fliedl G: Text preparation through extended tokenization. In Data Mining VII:
Data, Text and Web Mining and Their Business Applications. Volume 37. Edited by Zanasi,
A and Brebbia, CA and Ebecken, NFF. WIT Press/Computational Mechanics Publications;
2006::13-2
4. Alexandre Manuel Fajardo Vicente, LexMan: a Tokenizer and Morphological Analyzer
with Transducers, https://fenix.ist.utl.pt/downloadFile/395145514800
5. K. Tomanek, J. Wermter, and U. Hahn. Sentence and token splitting based on conditional
random fields. In PACLING 2007 – Proceedings of the 10th Conference of the Pacific
Association for Computational Linguistics, pages 49–57. Melbourne, Australia, September
19-21, 2007. Melbourne: Pacific Association for Computational Linguistics, 2007.
6. Linlin Li, Benjamin Roth and Caroline Sporleder, Topic models for word sense
disambiguation and token-based idiom detection, Proceeding ACL '10 Proceedings of the
48th Annual Meeting of the Association for Computational Linguistics, Pages 1138-1147,
PA, USA 2010.
7. Patrick Ruch et al,Minimal Commitment and Full Lexical Disambiguation: Balancing
Rules and Hidden Markov Models, Proceedings o/CoNLL-2000 and LLL-2000, pages 111-
114, Lisbon, Portugal, 2000.
8. Joshi, A. K., & Srinivas, B. (1994). Disambiguation of super parts of speech (or supertags):
almost parsing. In Proceedings of the 15th Conference on Computational Linguistics -
volume 1 (pp. 154–160). Kyoto, Japan.
9. Deryle Lonsdale, Rebecca Madsen, Unifying language modeling capabilities for flexible
interaction, 9th International Conference on Spoken Language Processing (ICSLP 2006)
Sep 17-21, 2006, Pittsburgh, Pennsylvania.
10. Uzuner Ö., Goldstein I, Luo Y, Kohane I. "Identifying patient smoking status from medical
discharge records". J Am Med Inform Assoc. 2008; 15(1)15-24.
Advanced Science and Technology Letters Vol.51 (SIA 2014)
138 Copyright © 2014 SERSC