30050 gw supplemental credit document …documents.worldbank.org/curated/pt/... · country director...
TRANSCRIPT

Document of
The World Bank
FOR OFFICIAL USE ONLY
Report 30050 - GW
SUPPLEMENTAL CREDIT DOCUMENT
INTERNATIONAL DEVELOPMENT ASSOCIATION
PROPOSED SUPPLEMENTAL CREDIT OF SDR 2.8 MILLION
(US$4.0 MILLION EQUIVALENT)
TO THE REPUBLIC OF GUINEA-BISSAU
FOR THE
NATIONAL HEALTH DEVELOPMENT PROGRAM
November 18,2004
Human Development I1 Country Department 14 Africa Regional Office
This document has restricted distribution and may be used by recipients only in the performance of their official duties. I t s contents may not be otherwise disclosed without W o r l d Bank authorization.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
AfDB AGEOPPE DAF DGPC DRH CAS ERRC EU GDP HIV/AIDS HNSM IDA IEC IMF ISS MAP MoPH NHDP NGO PNDS
PDO PRSP SDR SMP UNDP WAEMU
CURRENCY EQUIVALENTS (Exchange Rate Effective September 2004)
Currency Unit = CFA Franc (CFAF) CFA 1 = US$0.002 U S $ 1 = 500 CFAF
SDR 1 = US$1.46779
WEIGHTS AND MEASURES Metric System
FISCAL YEAR January 1 - December 31
ABBREVIATIONS AND ACRONYMS
African Development Bank Agencia de Criacao de Emprego (Agency for Employment Creation) Directorate o f Administration and Finance Directorate General o f Planning and Coordination Directorate o f Human Resources Country Assistance Strategy Economic Rehabilitation and Recovery Credit European Union Gross Domestic Product Human Immunodeficiency VirudAcquired Immunodeficiency Syndrome Hospital National Simgo Mendes International Development Association Information-Education-Communication International Monetary Fund Interim Support Strategy Multi-country HIV/AIDS Program for the Africa Region Ministry o f Public Health National Health Development Plan Non-governmental Organization Project0 Nacional do Desenvolvimento da Saude (National Development Health Project) Project Development Objective Poverty Reduction Strategy Paper Special Drawing Rights Staff Monitored Program United Nations Development Program West African Economic Monetary Union
Country Director Madani M. Tall Sector Manager Alexandre Abrantes Task Team Leader : Laura Rose
FOR OFFICIAL USE ONLY
This document has a restr icted d is t r ibut ion and may be used by recipients on ly in the performance o f their of f ic ia l duties. I t s contents may n o t be otherwise disclosed Lwithout W o r l d Bank authorization.
THE REPUBLIC OF GUINEA-BISSAU
SUPPLEMENTAL CREDIT TO THE NATIONAL HEALTH DEVELOPMENT PROGRAM
PROJECT SUMMARY
Borrower: Republic o f Guinea-Bissau
Implementing Agency:
Beneficiaries:
Poverty: Poverty-focused interventions
Amount:
Terms:
Ministry o f Public Health
Population o f rural and urban areas
SDR 2.8 mi l l ion (US$4.0 mi l l ion equivalent)
Standard IDA terms with a 40-year maturity, including 10 years o f grace
Financing Plan: IDA: US$4.0 mi l l ion Total: US$ 4.0 mi l l ion
Economic Rate of Return:
Staff Appraisal Report: None
Map: IBRD 272 16
Project ID: PO88282
No t applicable
This document i s based on the findings o f a join Governmen ‘Bank supervision and review mission in March 2004. The Bank team consists o f Messrs/Mmes Laura Rose, Task Team Leader; Johanne Angers, Operations Officer; Fernando Vasco, Public Health Specialist- Consultant; F i l y Sissoko, Financial Management Specialist; Laurent Mehdi Brito, Procurement Analyst; Marie Khoury, Consultant, Finance Officer; and Albert0 Ninio, Legal Counsel.


2
INTERNATIONAL DEVELOPMENT ASSOCIATION
THE NATIONAL HEALTH DEVELOPMENT PROGRAM SUPPLEMENTAL CREDIT TO THE REPUBLIC OF GUINEA-BISSAU FOR
A. INTRODUCTION
1. Country Context. Guinea-Bissau i s a small country on the West African coast wi th a population o f about 1.3 mi l l ion inhabitants. The economy i s based primarily on agriculture, and the country’s main export i s cashew nuts. Guinea-Bissau gained i t s independence from Portugal in 1974 after a protracted liberation war that resulted in the dislocation o f about one-fifth o f the population and the destruction o f important economic infrastructure. In 1998-99, an armed conflict again left a substantial part o f the economic infrastructure in ruins, intensifying the already wide-spread poverty. After two decades o f independence, Guinea-Bissau i s one o f the poorest countries in the world wi th poor infrastructure and low social indicators, and it ranks 172”d out o f 177 countries on the most recent United Nations’ Human Development Index. The percentage o f the population l iv ing on less than two dollars a day i s 64.7 wi th 20.8 percent l iv ing on less than one dollar a day (2002 Br ief Survey o f Poverty - LAP). The gross domestic product (GDP) was estimated at around US$240 mil l ion in 2003 with GDP per capita over the period 1997-2002 averaging US$170 per annum.
2. Legislative elections that took place end o f March 2004 led to the nomination o f a new cabinet. The new Government i s working to restore domestic and international confidence in a country weakened by conflict. The Government’s program focuses on restoring the administration and improving govemance and transparency, as wel l as long term structural reforms. Presidential elections are scheduled for March 2005.
3. The 1997 CAS (Report No. 16568) emphasized that the Bank’s lending and non-lending services would focus on improving access to quality and management o f social services. The project components and activities, as originally planned, remain relevant to the country’s health priorities as reflected in the Government’s second health strategy (National Health Development Plan, 2003-2007). The project i s also consistent with the objectives o f the Interim Support Strategy (ISS), currently under preparation and planned for Board presentation in Spring 2005. The ISS supports the Government’s goal to improve access to basic social services. The Guinea- Bissau Interim Poverty Reduction Strategy Paper (I-PRSP), endorsed by the Boards o f the Bank and the IMF on December 14, 2000, centered around the overarching goals o f poverty reduction, economic growth, good governance, infrastructure and private sector development, and social services delivery. The Full-PRSP covering the period 2004-2006 i s currently being finalized.
4. Health Sector. Much o f the health infrastructure was destroyed during the war and many professionals left the country. Health indicators are correspondingly poor although they have recovered to pre-war levels. Average l i fe expectancy i s 44 years and more than one in ten infants die before their first birthday. Malaria i s the major cause o f death, followed by diarrhea and acute respiratory infections. I t is estimated that 33,900 people are infected by HIV, 4.3 percent o f the total population. Sero-prevalence increased by 40 times between 1989 and 2001. The cities o f Bissau, Gabu and Bafata are the most affected. Service delivery i s also constrained by a shortage o f medical personnel and inadequate financing for even the most basic recurrent costs, including salaries, heating, and drugs. Health services in rural areas are usually l imited to those offered by churches and other non-profit organizations.

3
B. NATIONAL HEALTH DEVELOPMENT PROGRAM
5. The National Health Development Program was approved by the Bank’s Board on November 25, 1997, signed on January 8, 1998, and became effective on May 4, 1998 for the amount o f SDR 8.6 million. As o f November 2004, 84 percent o f the Credit amount had been disbursed and committed with a large part of the remaining procurement being launched. The current closing date i s June 30, 2005.
6. Objectives. The overall development objective o f the National Health Development Program i s to improve the health status o f the population, particularly women and children, through strengthening the national public health system, service delivery, management structures and processes. Specific objectives are (i) to increase the use and effective coverage o f primary health care services and referral centers; (ii) to strengthen the institutional capacity at al l levels; (iii) to improve the quality and the management o f human resources; and (iv) to reinforce intersectoral coordination and action in health-related activities in order to promote better health among the population.
7. Implementation Arrangements. The program i s executed b y the directorates o f the Ministry of Public Health (MoPH) with the support o f technical assistance in key areas o f project management and implementation, including planning, public health, financial management and accounting, and procurement. The General Directorate o f Public Health and i t s various directorates, the Directorate o f Human Resources (DRH), regional health teams, health centers and specialized institutions are responsible for all operational aspects o f the program. The General Directorate o f Planning and Cooperation (DGPC) and i t s various directorates are responsible for planning, monitoring and evaluation, administrative and financial management, and the coordination o f external assistance. In view o f the limited capacity o f the M o P H in the management of c iv i l works, a delegated contract management between M o P H and the Agency for Employment Creation (AGEOPPE) was established for the management and the execution o f the construction and rehabilitation o f health infrastructures.
C. PROJECT IMPLEMENTATION EXPERIENCE
8. Utilization and conversion of primary health care centers and referral centers. This component o f the project aims at (a) ensuring adequate physical coverage o f health facilities accessible to a majority o f the population through the rehabilitation o f health facilities and construction o f staff housing; and (b) ensuring the availability o f a minimum package of activities.
9. The c iv i l work program o f construction originally planned at appraisal experienced various modifications in view of the urgent gaps resulting f rom the military conflict. At the same time, promised donors’ financing to cover the needs evidenced by the health map did not materialize as planned in view of the political situation in the country. Nevertheless, c iv i l works

4
management was delegated to AGEOPPE as foreseen in the Development Credit Agreement, but for reason of lack o f capacity b y the agency to perform i t s mandate, the procurement o f works suffered substantial delays. An Italian non-governmental organization (NGO), Comunidade de Santo Egidio, was given the management for the reconstruction o f Hospital Raoul Folereau (National Hospital for Tuberculosis), which was inaugurated on December 18, 2003. The hospital serves as the country's national hospital for HIV/AIDS and tuberculosis and plays a major teaching role in addition to providing health services. One outstanding issue i s the financing o f recurrent costs for the hospital, which the Government has agreed to assume but i s currently not in financial position to provide.
10. The activities supporting the minimum package o f health care cover immunization, malaria, reproductive health, nutrition, and HIV/AIDS. Immunization coverage rates have increased over the past year and are now comparable to those before the conflict. The malaria program received funding from the Bank, UNICEF, and Ro l l Back Malaria. T o date, Guinea Bissau has a sufficient supply o f mosquito nets through 2006. Decreasing the price f rom CFA 3500 to CFA 1000 increased their uptake. The main priority now i s to develop a network o f impregnation centers. A five-year EU-financed project recently began to address reproductive health issues, particularly maternal mortality. The Bank i s no longer supporting the financing o f these activities in view o f availability o f other sources o f financing. The nutrition program completed all o f i t s activities programmed for 2003 with the exception o f what had been projected for the Islands. The program has identified the following priorities: (i) to work with Hospital National Sim2o Mendes (HNSM) on children's nutrition issues; and (ii) to validate a national plan on nutrition. Once the plan has been completed funding w i l l be provided for discussions with major stakeholders. Prevalence for HIV/AIDS in the 15-64 age group has reached 6.8 percent, wi th 4.1 percent being HIV-1 and 2.7 percent HIV-2. The HIV/AIDS program i s now ful ly funded under the IDA-financed MAP grant.
11. All programs suffer f rom lack o f human resources and inadequate financing for supplies and fuel. The Government intends to introduce incentives, including the construction o f staff housing, in order to encourage placement of staff in remote areas. Cost recovery efforts that have been introduced over the past year are meant in part to supply needed funds for non-salary recurrent costs.
12. In addition to direct support to these programs, the project finances approximately one- third o f the essential drugs required by the country (US $350,000 o f U S $1,000,000). The rest comes from the Government budget and cost recovery under the Bamako Initiative. Drug supply i s not an issue although the cost o f drugs may deter those in need. The appearance o f a strong unregulated private sector in pharmacies has been identified as a problem, requiring more Government regulation. However, the emergence o f the private sector should also be seen as an opportunity for Government to expand i t s coverage.
13. The main constraints identified during implementation that remain to be addressed are the lack of availability and reliability o f data concerning the priority programs and health outcomes in general. Two institutions have responsibility for health information: the Direcpio de Higiene and Epidemiologia (DHE) and the Centro de Znfomza$io Estatistica (CIE). The DHE reported a 93 percent success rate in reporting f rom regions for 2003. However, the results o f this data collection are not analyzed in a meaningful manner. The CIE has yet to define i t s purpose and earlier problems o f coordination between the DHE and C IE persist.

5
14. Institutional Strengthening and Capacity Building. This component aims at helping the Ministry to set up a supervision system and improve the overall management o f the system. Despite additional support through national technical assistance, the capacity o f the General Directorate o f Planning and Cooperation (DGPC) to consult and coordinate remains weak. Donor assistance i s defined by the donors and not by the MoPH. This leads, among other things, to an overlap and inefficiencies in the utilization o f the l imited resources.
15. The project finances a system o f supervision whereby six teams each visit two regions twice a year. Each team produces a report based on established guidelines. The M o P H feels strongly that the added benefit o f this supervision i s substantial, in part by motivating the staff. However, difficulties experienced in the collection and analysis o f data on indicators o f the health status needed for planning and decision-making remain at the forefront o f MoPHs challenges in managing the sector. Data collected to date are often unreliable and inconsistent.
16. The administrative and financial management capacity o f the Directorate o f Administration and Finance (DAF) i s l imited as technical assistance for the financial management and accounting functions required by the project have remained in the Celula da Gestdo rather than being mainstreamed into the responsibility o f the DAF. Very little sharing o f information between the Celula da Gestdo and the DAF occurs in view o f the resentment on the part o f the DAF personnel o f the fees being paid to the technical assistance in carrying out these tasks.
17. As part o f the community financing and management arrangement, the Bamako initiative i s progressing well, with 65.8 percent o f elected management committees in the 114 health zones ful ly functioning. However, several problems have been identified: first, in some areas, public pharmacies are unable to recover cost because o f the inability o f patients to pay (primarily the Bijagos and S. Domingo). Others have difficulty in filling out the paper work required for financial management. Finally, there i s an expectation in the community that members o f the management committees w i l l be paid honoraria for their participation.
18. In addition to the Bamako initiative, intended to primarily finance pharmaceuticals, the Government has introduced user fees for most health services. The Bank team discussed in length with the H N S M their experience since January 2003, and learned that receipts had decreased steadily (from approximately C F A 7.0 mi l l ion to CFA 1.0 million). There are several explanations for this: first, a part o f the fees was intended to be used for staff incentives, but this rarely took place given the acute need o f funding for running expenses and second, beginning in October 2003, the hospital (and other health institutions) was required to pass al l revenue to the Ministry o f Finance. Sixty percent o f these revenues were to be returned to the hospital, which has never occurred. Informal payments for health services are reported to be high and, along with the official user fees, may have had an impact on utilization.
19. Management and Development of Human Resources. This component finances a combination o f technical assistance to develop new human resource incentive systems and training programs to help fill the staffing gaps. Three separate training programs are carried out: (a) for nurses and midwives by the Escola National de Saude (ENS); (b) for administrators b y the Centro Nacional de Fomzapio Administrative (CENFA); and (c) post graduate level training

6
in internal medicine, pediatrics, obstetrics and gynecology, and surgery at the H N S M by an independent Portuguese firm.
20. The introduction o f incentives to encourage a better distribution o f staff has not materialized. Currently, facilities in the Bijagos are closed because o f lack o f staff. Most health centers outside o f Bissau are understaffed (based on existing norms). Staff housing are being financed as a f i rs t attempt to introduce incentives for staff to work in these areas.
21. Management o f human resources. Support to the Direc@io de Recursos Humanos (DRH) has been l imi ted under the project. Analysis o f data on staff b y region and function has been hampered by lack o f a functioning computer. The DRH continues i t s work in coordinating training activities and introducing some sort o f accreditation system to ensure that training programs are endorsed by the Government.
22. This component aims at supporting the H IV /A IDS Prevention and Malaria Control Program. A contract management was established with an international non-governmental organization (NGO) wi th a view to transfer i t s knowledge to a national NGO to take over at the end o f the contract. Most o f the objectives o f the contract under this component have been met: (a) according to the KAP survey, 85.3 percent o f the population recognize that condoms are a form o f protection and 95.9 percent recognize the name "Pante" which i s the name o f the condoms marketed b y PSI; (b) a KAP survey was completed and provides excellent baseline information; (c) many condoms have actually been distributed; and (d) the basic conditions were put in place for a national N G O to take over the program after the international N G O withdrew.
Promotion of Better Health.
23. The MoPH's Dicecqio de Infoma$io EducapTo e Communicapio em Saude (DIECS) also provides support to health promotion activities wi th financing f rom the various health programs such as malaria, TB, HIV/AIDS, and nutrition. I t appears that they have been especially effective with a series o f radio shows highlighting various health priorities on a weekly basis
24. Project Management and Implementation. The project has provided institutional support to the MoPH. Since the mid-term review (April 2002), and with the support o f key technical assistance in project management and implementation, including financial management and accounting and procurement, planning, and public health, the M o P H has been effective at managing and implementing project activities.
D. RATIONALE FOR THE SUPPLEMENTAL CREDIT
25. The project components and activities, as originally planned, remain relevant to the country's health priorities as reflected in the Government's second health strategy (National Health Development Plan, 2003-2007). The proposed supplemental credit would enable the Government to sustain outcomes achieved under the original Credit through ensuring the use and effective coverage o f primary health care services and referral centers, and further strengthening

7
Government’s capacity in the sector. The proposed supplemental i s consistent wi th the project development objectives and meets the conditions stipulated in OP 13.20, namely:
(a ) The cost overrun is due to exceptional circumstances beyond the borrower’s control:
26. The military conflict started in June 1998, only one month after project effectiveness. The subsequent two-year delay in project implementation accounts for the majority of the cost overrun. K e y health infrastructures located in the ci ty o f Bissau were destroyed, namely, the Central Deposit of Drugs, the Public Health Laboratory, the Epidemiology Services, the National I E C Services, the National School o f Health Technicians, the Hospital National Simao Mendes, the National Hospital o f Tuberculosis, the Mental Health Center, a number of health centers, and the MoPH’s building. In accordance with the decision made during the mid-term review in April 2002, the IDA credit financed the unplanned refurbishment o f the National Tuberculosis Hospital (Raoul Folereau) and the Central Drug Deposit in view o f their importance to the functioning o f the health system. Other donors (AfDB, European Union) also contributed to the refurbishment o f other key facilities.
27. The conflict postponed the implementation o f c iv i l works resulting in an increased in the price of primary materials (e.g., a 50 kg. bag o f cement estimated in 1998 at 4,500 CFA i s now at 6,000 CFA). A re-evaluation o f the cost o f c iv i l works and equipment during the mid-term review, including those not originally planned in the project, assessed their total estimated cost to reach US$9.4 mi l l ion as compared to the planned US$3.1 million. The re-evaluation o f the costs pointed out that price contingencies in the Project Appraisal Document (PAD) were insufficient to cover the 150 percent increase in costs.
28. Another contributing factor was the decrease (from US$7.4 mi l l ion to US$2.2 million) in the funding provided b y other donors, particularly the Netherlands, in view o f the country’s political instability. As such, the fol lowing unplanned activities were financed by the IDA credit: construction o f the Hospital Raoul Folereau (US$1.14 million), repair o f the Provisional Drug Deposit (US$0.15 million), support to the priority programs and minimum package o f activities (US$0.52 million), and key training programs (US$O.8 million) that were to be provided b y various bilaterals and United Nations Agencies (France, Portugal, UNICEF, UNFPA, WHO).
29. Finally, due to the fiscal crisis fol lowing the conflict, and as part o f the portfolio restructuring presented to the Board in August 2003, the legal agreement was changed to allow for 100 percent IDA financing, which represented an additional cost to the credit o f approximately US$0.5 million. Additional operating costs related to the first extension o f the original credit by one year are estimated at US$0.2 million.
30. Total cost overrun estimated at this time in relation to the proposed activities that w i l l directly contribute to the Project Development Objectives (PDOs) amounts to US$4.0 mi l l ion as follows: US$2.6 mi l l ion for the coverage o f primary health care centers and referral centers, US$0.7 mi l l ion for institutional capacity, US$0.5 mi l l ion for management and development o f human resources activities, and US$0.2 mi l l ion for the promotion o f better health.

8
(b) The loan is being implemented in compliance with covenants:
31. The project i s in compliance with all the legal covenants. There are no outstanding audit reports and in the 2003 audit report, the auditor issued an unqualified opinion on the financial statement, the special account and the statement o f expenditures.
(c) I t is impossible to reduce the scope of the project to f i t the available resources without significantly impairing the project's economic viability or capacity to achieve its objective:
32. In agreement with the recommendations o f a Quality Enhancement Review (QER) panel, the project was restructured at mid-term to focus more on the financing o f basic services. Further attempts to prioritize were made in 2003 to take into account the closing o f the Dutch funding and the project one-year extension. However, the project may not achieve the PDOs without additional resources, as several o f the activities originally planned, but cut at mid-term, remain clearly necessary to meet the PDOs, namely the refurbishment o f the central drug deposit, the rehabilitation o f health centers and the construction o f staff housing. Other expenses necessary to meet the PDOs include interventions in key public health programs, such as the malaria control and immunizations programs and the purchase o f essential drugs. Continued investments in capacity strengthening are also necessary to improve implementation and management o f these programs and the delivery o f basic health services. These essential inputs are critical to the PDOs that aim at increasing the utilization and effective coverage o f primary health care services and referral centers and ensuring sustainability o f the investments.
(d) The borrower is unable tofinance the additional costs and to obtain additional funds from other lenders on reasonable terms or reasonable time:
33. The Government and the Bank team have explored alternative sources o f financing. The Government i s unable to finance the gap from i t s own resources given the fiscal crisis faced since the conflict. Other external donors are not yet ready to return to the country given the current political climate and fragile situation.
(e) The time available is too short to process a further freestanding Bank loan:
34. The funds under the original project are expected to be fully disbursed by the end o f June 2005. Currently, only a l imited number o f interventions specific to the H IV /A IDS prevention and control program were integrated into the Multi-country H IV /A IDS Program for the Afr ica Region (MAP).
(f3 The borrower is committed to the project, and the implementing agencies have demonstrated competence in carrying it out:
35. Government commitment to the project i s high, as evidenced by the Government's letter requesting the supplemental credit and the aide-memoire o f the appraisal mission that took place in March 2004. Despite extremely dif f icult circumstances, the MoPH, implementing agency for the project, has demonstrated competence in the overall implementation history o f this project. The project has the experience and implementation capacity to fully disburse the supplemental credit within the execution period foreseen.

9
E. THE PROPOSED SUPPLEMENT
36. The proposed supplemental credit, in the amount o f US$4.0 million, would retain the design, basic objectives and operating procedures o f the National Health Development Program. I t would aim to complete the activities o f the original credit. The proposed supplemental credit and original credit would have a closing date o f December 31, 2006, in order to achieve the following:
(a) Utilization and coverage of primary health care centers and referral centers (US$2.6 million)
37. This component w i l l essentially finance the rehabilitation and equipping o f planned health facilities and staff housing, the construction and equipment o f a storage facility for drugs, and the provision o f medical equipment and materials for the health facilities, and technical assistance for the c iv i l works program. As part o f the minimum package o f activities, this component w i l l also provide for essential drugs, technical assistance, and training for Local Health Management Committees.
38. Environmental assessment under the original credit was rated a “C”, wi th no displacement of people. The supplemental w i l l finance the planned rehabilitation o f health facilities. N o one i s expected to be resettled f rom any o f the investments proposed, including the construction o f the storage facility for drugs and staff housing for which the sites have already been identified. Agreement was reached with Government that i t would prepare simple guidelines for the contractors who w i l l be constructing the drug storage building, rehabilitating the health centers, and constructing staff housing. The guidelines w i l l be incorporated into contract documents, a draft o f which w i l l be reviewed by the Bank prior to the f i rs t contract being let.
(b) Strengthening of Institutional Capacity at all Levels (US$0.7 million)
39. This component w i l l strengthen the capacity o f the General Directorate o f Planning and Cooperation (DGPC) through the establishment o f a basic health information system in which information on key sectoral indicators w i l l regularly f low from the health facilities to the center and from the center to the health facilities. Emphasis w i l l also be given on strengthening capacity in (a) data analysis and their use for planning and decision-making; (b) strategic planning; and (c) improving external aid coordination. This component w i l l also contribute to strengthening the Directorate o f Administration and Finance (DAF) in administrative and financial management capacity. This w i l l be achieved through technical assistance, office equipment, training, incremental operating costs, including contractual personnel. In addition, i t w i l l finance technical and financial audits and final evaluation o f the project.
(c) Management and Development of Human Resources (US$0.5 million)
40. This component w i l l finance technical assistance aimed at improving the quality, efficiency and distribution o f human resources through the implementation of specific strategies for personnel management and training. In addition, i t w i l l seek to improve staff motivation (staff housing), working conditions (rehabilitations and equipment) and career prospects
10
(development o f a policy on career development path) o f health personnel as originally planned under the original credit. Outcomes o f these efforts that have been neglected so far in view o f the country’s political instability, w i l l directly contribute to the PDOs and more importantly on improving management (Directorate o f Human Resources) and technical (health facilities) capacity to respond to future health investments in the country. In addition to technical assistance, this component w i l l also finance training and equipment.
(d) Promotion of Better Health (US$0.2 million)
41. This component w i l l provide for the Malaria Control Program through the purchase o f environmentally-approved products for impregnating bed-nets to be distributed b y the Impregnation Centers created under the original credit. The component w i l l also finance the development o f a sector-wide strategy o f communications through technical assistance and workshops.
42. The total project cost i s estimated at US$4.0 mi l l ion equivalent. In view o f the Government’s continued fiscal constraint since the conflict, the current arrangement o f allowing 100 percent IDA financing w i l l be maintained under the supplemental. The breakdown o f the project cost, project financing plan and disbursement plan are shown in Schedules A and B.
Project Cost and Financing.
43. Implementation Arrangements and Procurement. The proposed Supplemental Credit does not require additional implementation capacity beyond what i s already in place in the PNDS. The Supplemental Credit w i l l be subject to the same monitoring and reporting requirements o f the project. Assessment o f PNDS capacity in procurement was carried out in February 2004 and was found satisfactory. Under the original credit, the PNDS had entered into a Convention wi th AGEOPPE, a delegated contract management agency, for the execution o f c iv i l works in view o f the capacity constraint found in the Ministry o f Health at the time o f project approval. C iv i l work activities under this arrangement indicate the weak capacity o f AGEOPPE to adequately control and supervise the c iv i l works. In view o f this, an independent engineering firm, recruited under procedures acceptable to IDA, w i l l manage the technical studies and supervision o f the works while PNDS w i l l manage the procurement. Prior review threshold for c iv i l works w i l l be raised from US$lOO,OOO to US$200,000, and for goods from US$lOO,OOO to US$150,000, according to the outcome o f the procurement capacity assessment. A summary o f the procurement arrangement for the supplement i s found in Schedule C. A timetable o f key project processing events and the status o f Bank operations in Guinea-Bissau are given in Schedules D and E, respectively.
44. Accounting, Financial Reporting and Auditing Arrangements. The PNDS has established an acceptable accounting and reporting system for the project. The contract wi th the current independent auditors have exceeded the three-year limit, and it has therefore been agreed that the PNDS would launch a new selection process for the supplemental credit. Project audit reports, including special accounts and statements o f expenditures, w i l l be submitted to IDA no later than six months after the end o f the fiscal year.
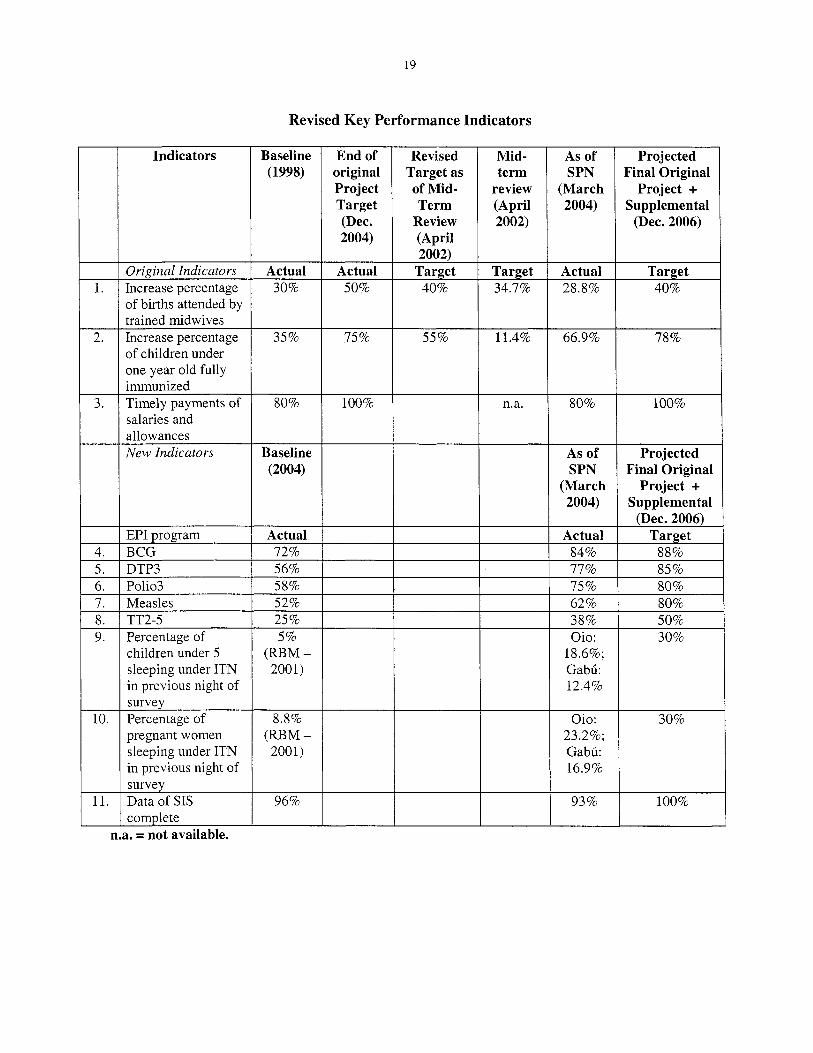
45. The original indicators have been modified to reflect the revised targets according to the new closing date o f December 31, 2006. New indicators have been introduced to monitor (a) the vaccination rate against key communicable diseases o f childhood under the Expanded Program on Immunization (EPI); and (b) the utilization o f
Performance Indicators.

11
Impregnated Bed Nets b y children and pregnant women. These indicators are presented in Schedule F.
46. Closing Date. As part o f this request for a supplemental credit, a concomitant extension o f the closing date f rom June 30, 2005 to December 31, 2006 i s proposed. Without such extension o f the closing date, the project would close at the end o f June 2005, which would make i t difficult to continue implementation of the activities needed to launch those to be financed by the Supplemental Credit. Accordingly, as part o f the amendment o f the legal documentation for the supplemental financing, the Credit Agreement i s amended to reflect the new Closing Date. An Implementation Completion Report (ICR) w i l l be prepared within six months after Credit closing.
47. Effectiveness Conditions. N o conditions o f effectiveness are required except for the submission of: (a) a satisfactory legal opinion on the Agreement Amending the Development Credit Agreement, and (b) a copy o f the Decree ratifying the said Agreement.
48. Economic Analysis. The economic analysis completed for the original project remains valid. Furthermore, international evidence i s overwhelming and undisputable that the programs supported b y the project are the most cost effective interventions to address Africa’s burden o f disease.
49. Environmental and Social Aspects. Experience with the original project indicates that there have not been any significant environmental or social issues. The supplemental does not change the project in ways that would increase the environmental impact. The drug storage facility to be constructed (land already identified) i s a large structure requiring small quantities o f material and i s not adjacent to an environmentally or culturally sensitive area. The rehabilitation and construction of health facilities and staff housing are small-scale and are not going to generate hazardous materials, such as asbestos-containing demolition waste. Finally, the malaria program i s based essentially on the provision o f environmentally-approved products for impregnating bed nets.
50. The Government w i l l prepare simple guidelines for the construction of the drug storage building, rehabilitation o f the health centers, and rehabilitation or construction o f staff housing. The guidelines w i l l be incorporated into contract documents, a draft o f which w i l l be reviewed by the Bank prior to the first contract being awarded. Compliance by contractors on the application o f the guidelines w i l l be part of the supervision tasks carried out by the PNDS staff and the independent engineering firm. For the rehabilitation work, the guidelines w i l l focus on workplace safety and disposal o f demolition debris as well as avoidance o f asbestos or other hazardous materials in the reconstruction work. For the drug storage building and staff housing, again workplace safety w i l l be one issue to cover, as wel l as the application o f good construction practice in land clearing, erosion control, dust control, drainage design, avoidance o f asbestos, scheduling hours o f work to minimize disturbance to local residents, arranging routes and timing o f materials deliveries for the same reason, plus to minimize damage to local roads, etc.
5 1. The proposed supplemental credit should enable the Government to sustain outcomes achieved so far under the original project development objectives. Results to date indicate that the project development objectives are l ikely to be reached and sustained through activities aimed at strengthening the MoPH’s capacity to meet challenges o f the sector in implementing i t s strategy. The sustainability o f the program i s also helped by the sector approach and the close coordination envisaged among key donors.
Sustainability.

12
52. Project Risks. Critical r isks that may negatively impact the success o f the project are: (i) the country’s political situation and potential instability, which may impact service delivery and i t s utilization; (ii) the lack o f resources (financial, human, and materials) to provide and sustain quality basic health services; and (iii) the institutional capacity o f the Ministry o f Public Health to manage and implement i t s strategy. Presidential elections are planned to take place in March 2005, which may impact the health sector by a change o f leadership at the M o P H and o f technical teams at the central and regional levels. Adequate physical, technical and price contingencies have been taken into account in the costing o f the Supplemental Credit in view of recent experience.

13
COMPONENTS 1. Ut i l izat ion and Coverage o f Primary Heal th Care Centers and
SCHEDULE A
LOCAL FOREIGN TOTAL 0.80 1.75 2.55
REPUBLIC OF GUINEA-BISSAU SUPPLEMENTAL CREDIT FOR THE NATIONAL HEALTH DEVELOPMENT
PROGRAM
Referral Centers 2. Strengthening of Institutional
Estimated Costs and Financing Plan (in US$ mi l l ion)
0.60 0.10 0.70
Estimated Costs:
Capacity at a l l Levels 3. Management and Development o f Human Resources
0.30 0.15 0.45
4. Promotion o f a Better Health Total Base Costs Phvsical and m ice contingencies
0.05 0.05 0.10 1.75 2.05 3.80 0.10 0.10 0.20
FINANCIER IDA Total Project Costs
LOCAL FOREIGN TOTAL 1.85 2.15 4.00 1.85 2.15 4.00
14
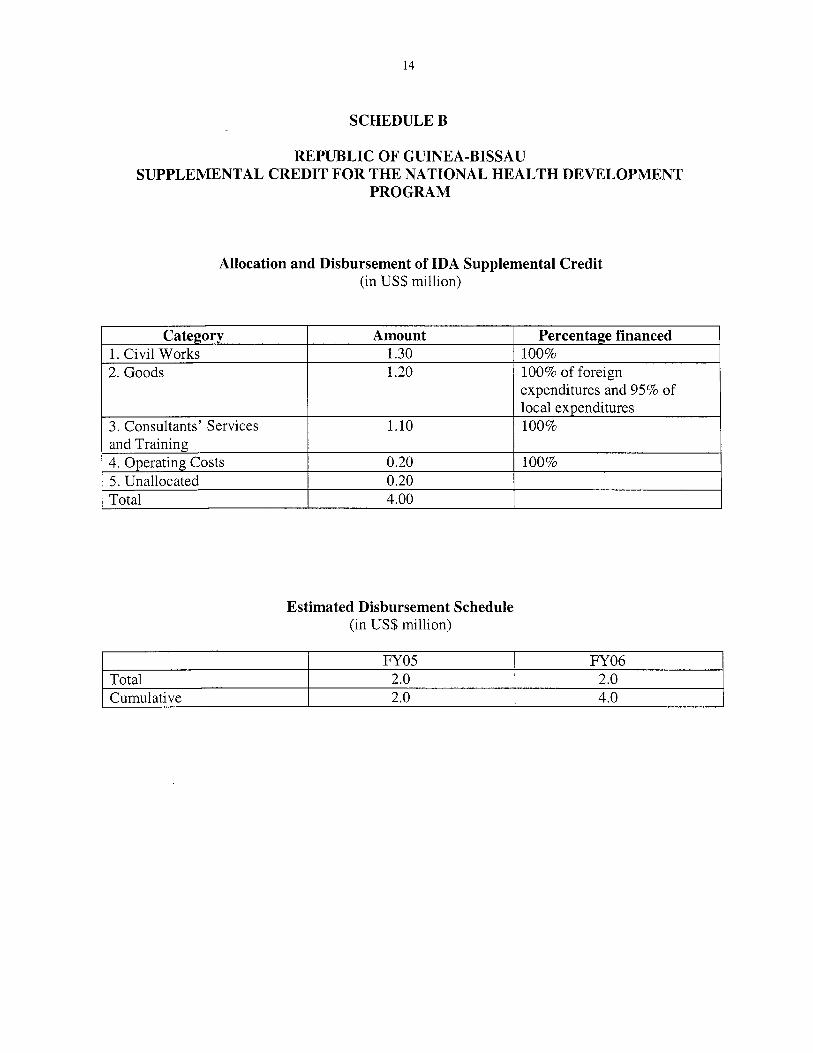
Category 1. Civil Works 2. Goods
3. Consultants’ Services and Training
5. Unallocated Total
4. Operating Costs
SCHEDULE B
Amount Percentage financed 1.30 100% 1.20 100% of foreign
expenditures and 95% of local expenditures
1.10 100%
0.20 100% 0.20 4.00
REPUBLIC OF GUINEA-BISSAU SUPPLEMENTAL CREDIT FOR THE NATIONAL HEALTH DEVELOPMENT
PROGRAM
Total
Allocation and Disbursement of IDA Supplemental Credit (in US$ million)
FY 05 FY 06 2.0 2.0
Estimated Disbursement Schedule (in U S $ million)

15
3. Operating Costs
TOTAL
SCHEDULE C
(1.20) (1.20)
0.20 0.20 (0.20) (0.20)
1.30 1.00 1.70 4.00 (1.30) (1.00) (1.70) (4.00)
THE REPUBLIC OF GUINEA-BISSAU SUPPLEMENTAL CREDIT FOR THE NATIONAL HEALTH DEVELOPMENT
PROGRAM
Summary o f Proposed Procurement Arrangements (US$ million)
16
SCHEDULE D
THE REPUBLIC OF GUINEA-BISSAU SUPPLEMENTAL CREDIT FOR THE NATIONAL HEALTH DEVELOPMENT
PROGRAM
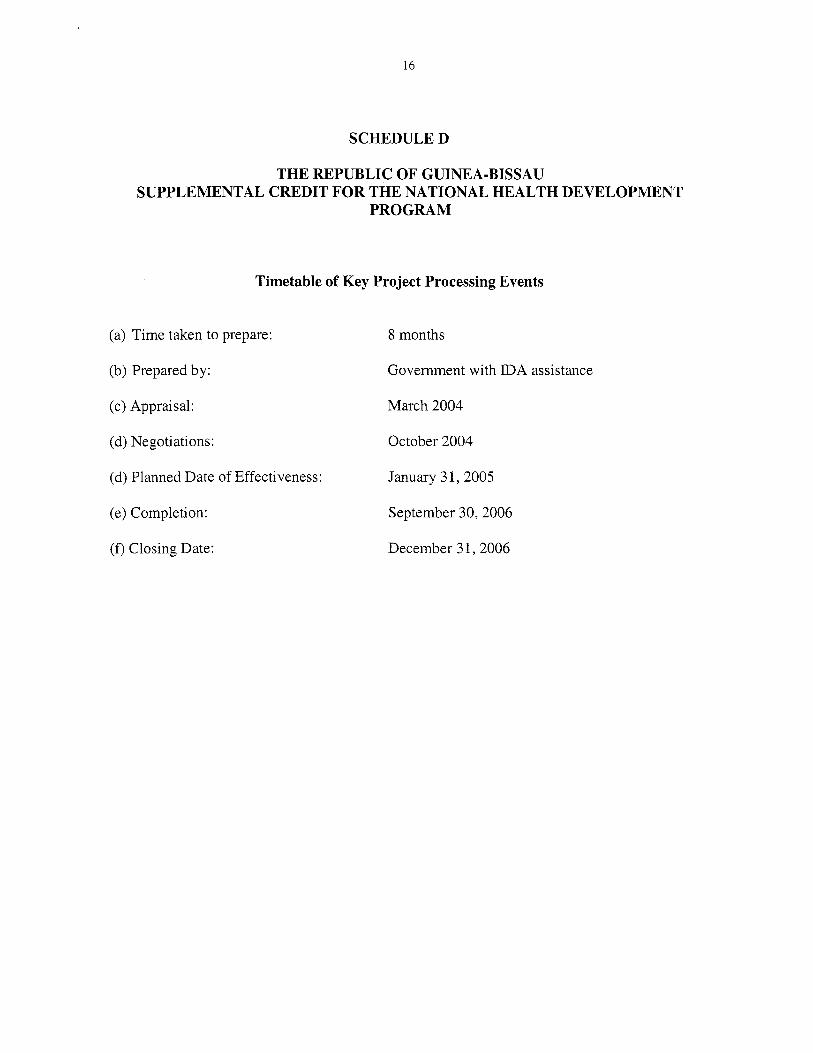
Timetable of Key Project Processing Events
(a) Time taken to prepare:
(b) Prepared by:
(c) Appraisal: March 2004
(d) Negotiations: October 2004
(d) Planned Date o f Effectiveness:
(e) Completion: September 30,2006
(0 Closing Date: December 31,2006
8 months
Government with IDA assistance
January 3 1,2005

17
3 5 ? -
- 4 - 0 0
- O N " ?
F e w = o m N -
z o m
m m m
m m m

18
3.
SCHEDULE F
mortality rate Reduction in total
REPUBLIC OF GUINEA-BISSAU SUPPLEMENTAL CREDIT FOR THE NATIONAL HEALTH DEVELOPMENT
PROGRAM
Original Key Performance Indicators
5.
r Indicators
operational health zones Increase percentage of
Baseline (1998)
6.
7.
8
9.
End of original Project
(Dec. 2004)
births attended by trained midwives Increase percentage of children under one year o ld fu l ly immunized Percentage o f Government’s budget allocated to health per year Percentage o f Ministry o f Health budget allocated to Primary Health Care Timely payments o f salaries and allowances
Mid- term
review (April 2002)
As of SPN
(March 2004)
Revised Target at Mid- Term
Review (April 2002) Target Actual Actual Actual Target
n.a. n.a. n.a.
n.a. n.a. 10%
6%
3% 5%
5.7% 5.7% 6% n.a.
37 96 (83%) n.a. n.a. Increase number o f
30%
35%
50%
75%
40%
55%
34.7%
11.4%
28.8%
66.9%
14.85% n.a. n.a. 11%
53%
100%
n.a. 25 9% (1996)
80%
48%
n.a. 80%
19
Revised Key Performance Indicators
Indicators Baseline (1998)
End of original Project Target (Dec. 2004)
Revised Target as of Mid- Term
Review (April
Mid- term
review (April 2002)
As of SPN
(March 2004)
Projected Final Original
Project + Supplemental
(Dec. 2006)
2002)
34.7% Oriainal Indicators Actual
30% Actual
50% Actual 28.8%
Target 40% 1.
2.
3.
4. 5. 6. 7. 8. 9.
10.
11.
Increase percentage o f births attended by trained midwives Increase percentage o f children under one year old fully immunized Timely payments o f salaries and allowances New Indicators
11.4% 5511 35% 75 % 66.9% 78%
80% 100% 80% 100%
Baseline (2004)
As of SPN
(March 2004)
Projected Final Original
Project + Supplemental
(Dec. 2006) Actual 72%
EPI program BCG
Target 88%
I 77% 85% 56% 58%
DTP3 Polio3 Measles
75% 62%
80% 80% 52%
25 % 5%
TT2-5 Percentage of
38% Oio:
18.6%; Gabti: 12.4%
50% 30%
children h d e r 5 sleeping under ITN in previous night o f
(RBM - 2001)
survey Percentage of Oio:
23.2%; Gabu: 16.9%
30% 8.8% (RBM -
2001) pregnant women sleeping under ITN in previous night o f survey Data of SIS complete
93% 100% 96%
n.a. = not available.