30.trauma musculoskeletal blok 27.ppt
TRANSCRIPT

MUSCULOSKELETAL TRAUMA
Dr.dr. Nur Rachmat Lubis, SpOT.
FRACTURE & DISLOCATION
FRACTUREDefinition :A fracture, whether of a bone, an epiphyseal plate or a cartilaginous joint surface, is simply a structural break in its continuity.
must be consider : surrounding soft tissue around the fracture site

Physical factors in the Production of Fractures
1. Cortical Bone: can withstand compression and shearing forces better
that it can withstand tension forces

2. Cancellous Bone/ spongious:Can’t withstand compression.
Can produced: Crush # / compression # Impacted #

Descriptive Terms Pertaining to Fractures
1. Fracture site : Diaphyseal Metaphyseal Epiphyseal

2. Extent of Fracture:complete Incomplete

3. Configuration of #:1. Transverse2. Oblique3. Spiral4. Comminuted
1 2 3 4

4. Relationship of the Fracture Fragments to Each Other :UndisplacedDisplaced :
1. Overriding2. Angulated3. Rotated4. Distracted5. Impacted6. Shifted
sideways
Relationship of the fracture fragments to each other caused by :
• Effects of Gravity• Effects of muscle pull on the fragments

5. Relationship of the Fracture to the External Environment: Closed # Open #:
Fracture fragment has penetrated the skin ( from within)Sharp object has penetrated the skin to # the bone (from
without)
6. Complication : Uncomplicated Complicated:
Local : InfectionSystemic : Emboli, Sepsis

THE DIAGNOSIS OF FRACTURES
HISTORY :Fall, Direct Trauma.Mechanism of injury.Common symptom of # :
Localized pain.Decreased function of the involved part.

THE DIAGNOSIS OF FRACTURES
PHYSICAL EXAMINATION:INSPECTION ( LOOKING ):
Swelling ( edema )Deformity( angulations, rotation, shortening )Abnormal movementEchymosis( subcutaneous extravasations of blood )
PALPATION ( FEELING ) :Localized tenderness at the # site.Crepitus (not necessary)
RANGE OF MOVEMENT (ROM):Limitation.

THE DIAGNOSIS OF FRACTURES
!!!! CAREFULL ASSESSMENTPatient’s General ConditionSearch for associated injuries:
BrainSpinal CordPeripheral NervesMajor vesselsThoracesAbdominal viscera

THE DIAGNOSIS OF FRACTURES
RADIOGRAPHIC EXAMINATION:# : PHYSICAL EXAMINATIONConfirmation by X-Ray Accurate DiagnosisTo determine extent and configuration of the fracture.Include entire length of the bone and the joints at
each end.2 Projection : AP / Lat, particularly obliqueSpine and pelvis : (+) CT

THE NORMAL HEALING OF FRACTURES1. Cortical bone (diaphyseal bone/ tubular
bone)# torn of blood vessels, canaliculi, Haversian canal
on the # site Osteocyte in the lacunae †↓
A vascular Bleeding from periosteum
1. Fracture Hematoma ↓ Localized on the end of fragment # Osteogenic cells from periosteum formed External callus

From endosteum Internal callusCartilage callus change in to bone by
Endochondral Ossification2 Clinical Union ( fracture line still
apparent)3 Consolidation ( Radiographic Union )4 Remodeling


THE NORMAL HEALING OF FRACTURES
2. CANCELLOUS BONEInternal Fracture Hematoma
osteogenic cells from trabeculae▼
Internal callus▼
Clinical Union▼
Consolidation

THE TIME REQUIRED FOR UNCOMPLICATED # HEALING
FACTOR INFLUENCE:1. Age of the patient Younger age, the healing rate faster.
Example : femur # after birth union 3 weeks
femur # on the age 8 year union 8 weeks femur # on the age 12 year union 12 weeks femur # on the age 20 th/> union 20 weeks

HEALING TIME UNCOMPLICATED #
2. # Site and Configuration # through bones that are surrounded by
muscle >union faster cancellous bone # > union faster than
cortical bone long oblique / spiral # > union faster than
transverse #

WAKTU PENYEMBUHAN # UNCOMPLICATED
3. Initial Displacement of the Fracture :undisplaced #, intact periosteum heal twice as rapidly as displaced #
4. Blood supply to the Fragments :If both fracture fragments have a good blood supply healing faster

ABNORMAL HEALING OF FRACTURES
MALUNION Heal normally expected time but in unsatisfactory
position with residual bone deformity DELAYED UNION
union time longer than normal NON UNION
fractures fail to heal by bone : Fibrous Union False joint (Pseudoarthrosis)

PRELIMINARY CARE FOR PATIENTS WITH #
PRIORITY1. Airway2. Breathing3. Shock4. # and dislocation
Complete PE Splinting Extr # :
To minimize pain Prevent further injury to the soft tissue
INITIAL

CLASSIFICATION OF OPEN #
TYPE IWound Ø < 1 cmClean woundBone penetrated skin with minimal injury
to the muscle (usually from within)Simple #, transverse, short oblique

CLASSIFICATION OF OPEN #
TYPE II:Wound Ø > 1 cmWithout extensive soft tissue damage,
skin flaps or avulsionsimple # transverse, short oblique,mild
comminuted

CLASSIFICATION OF OPEN #
TYPE III:Extensive soft tissue damage ; skin,
muscle, nerve injuries and major arterial injury
Often caused by high speed injuryExample :Traffic accident, farm accidentsGunshot wound> 8 hours

CLASSIFICATION OF OPEN #
TYPE III A :High speed injury, soft tissue can coverage the
woundSegmental # or severe cominuttedTYPE III B :High speed injury> soft tissue lossAvulsion of periosteumWound with severe contaminationTYPE III C :Major arterial injury need to repair

SPECIAL TYPES OF # Stress # (fatigue #) :
March # metatarsal II-III #Prox. Tibia # jumpers and ballet
dancersPathological # :
Occur in abnormal boneWithout major trauma

DISLOCATIONStructural loss of its stability3 structure that prevent normal ROM & also
prevent joint stability
Joint shape ( joint surface )
Capsule and ligament
Muscle that prevent joint stability

DISLOCATION
3 DEGREES OF JOINT INSTABILITY :1st Degree : Occult Joint instability
( apparent only when joint is stressed)2nd Degree : Subluxation ( less than luxation) 3rd Degree : Dislocation (Luxation)
( joint surfaces have completely lost contact)

DISLOCATION
Joint most susceptible to traumatic dislocation:
ShoulderElbowHipInter phalangealAnkle

DIAGNOSIS
Physical Examination :Swelling (edema)Deformity ( angulation, rotation, loss of normal
contour, shortening)Abnormal movementLocal tenderness
Radiographic Examination :Typical features of a subluxationAP / LAT projection

SPECIFIC TYPES OF JOINT INJURIES CONTUSION:
Hemarthrosis (rupture of synovial vessels) Normal X-rayLIGAMENTOUS SPRAIN: Acute sprain, strain sudden stretching of the
ligament withincomplete tears local hemorrhage local swelling tenderness, pain aggravated by movement
Radiographic examination : normal Treatment : strapping / splinting
DISLOCATION : Anatomical reduction immobilization

SPECIFIC FRACTURES AND JOINT INJURIES IN ADULTS
Fracture less common, but more seriousWeaker and less active Periosteum Less rapid fracture healingFewer problems of DiagnosisNo spontaneous correction of residual fracture
deformitiesDifferences in complication:
Open fracture > common in adultMajor arterial trauma Fat embolism

SPECIFIC FRACTURES AND JOINT INJURIES IN ADULTS
Torn ligaments and Dislocations more commonBecause > rigid, child > elasticIf in children make separation in adult dislocation
/ # dislocation
Better tolerance of major blood lossDifferent emphasis on methods of treatment
> frequently require ORIFIf undisplaced # , adult tend to be more cooperative
during treatment, # can be treated by protection alone

SPECIFIC FRACTURES AND DISLOCATIONSTHE HAND
General features: Common Treatment should always deference prevent
disability Edema >> disturbance function elevation
to▼ # digits immobilized as short as possible
never more than 3 weeksfinger Immobilized in the flexed position

SPECIFIC FRACTURES AND DISLOCATIONSTHE HAND
. DISTAL PHALANX :Mallet Finger ( baseball finger, cricket finger )Caused by:
Passive flexion distal of the interphalangeal joint with the extensor tendon under tension may avulse a fragment of bone from the base of the distal phalanx into which the tendon is inserted.
Treatment:Acute : Splinting the finger with DIP joint extended & the
PIP joint flexed 3 weeks. ORIF with wire fixation.

SPESIFIC FRACTURES AND DISLOCATIONSTHE HAND
. METACARPAL S:1.Boxer Fracture ( Street
Fighter # ):# neck metacarpal VStreet fighter’s #
Treatment :Reduction Immobilized in cast not more
than 2 weeksORIF with K-wire fixation if #
unstable

SPESIFIC FRACTURES AND DISLOCATIONSTHE HAND
2. Bennet’s Fracture :# dislocation of the 1st carpo metacarpal joint
Longitudinal force along the axis of the 1st metacarpal with the thumb in flexed
Serious intraarticular fracture dislocation of the CMC joint
Treatment: Closed reduction ORIF K-wire

SPESIFIC FRACTURES AND DISLOCATIONSTHE HAND
3. Rolando # :# base 1st metacarpal with intrarticular T or Y #

SPESIFIC FRACTURES AND DISLOCATIONSTHE WRIST AND FOREARM
1. Distal end of the Radius ( Colles’ # ) Colles’ # :
# radius, 2,5 cm / 1 inch from wrist jointCommonest # in adults, > 50 th ♀ > ♂Fracture occur through bone that has became markedly
weakened by combination senile & post menopausal osteoporosis
Mechanism of injury : fall with lands on outstretched hand positionClinical features:
Dinner fork deformity : posterior displacement or posterior tilt of the distal radial fragment

COLLE’S FRACTURE
CLINICAL FEATURES : DINNER’S FORK DEFORMITY

COLLE’S FRACTURE
Radiographic features :Stable type :
There is 1 main transverse # line with little cortical comminution
Unstable type :Gross comminution, particularly of the dorsal cortex,
and also marked crushing of the cancellous bone

COLLE’S FRACTURE TREATMENT :
Undisplaced # : immobilization with Below Elbow Cast for 4 weeksDisplaced # : Closed Reduction + BE cast Closed Reduction+ External Fixation
COMPLICATION :Usually Colles # had clinical union in acceptable position
within 6 weeksPreventable complication:
Finger Stiffness, Shoulder stiffness, malunionRare complication: Sudeck’s Reflex Symphatetic DystrophyLate rupture EPL

2. Reverse Colles # / Smith’s #
Predominantly in young menOccurs ♂ young adults Fall on the back of the flexed
wrist and hence is a pronation injury
Distal fragment dislocated to the anterior side
SPESIFIC FRACTURES AND DISLOCATIONSTHE WRIST AND FOREARM

SMITH’S #
Treatment : Closed reduction requires strong
supination of the wristAbove Elbow Cast, for 6 weeks, maintain
the position in supination

3.Barton’s #Other form of smith #
Intra articular #
SPESIFIC FRACTURES AND DISLOCATIONSTHE WRIST AND FOREARM

FRACTURE OF THE SHAFT OF THE RADIUS AND ULNA
RADIUS – ULNA :
1. GALEAZZI # : # of the shaft of the radius and
dislocation of the distal radio-ulnar joint. displaced # of distal third of the radial
shaft associated with complete disruption & dislokation of the distal radioulnar joint.
Usually sustained by young adults Distal fragment tilted posteriorly

FRACTURE OF THE SHAFT OF THE RADIUS AND ULNA
Treatment :Open Reduction &
Internal fixation of the radius, the dislocatiwill be on reduced.

FRACTURE OF THE SHAFT OF THE RADIUS AND ULNA
4. MONTEGGIA # :
# of the Prox half of the ulna accompanied by anterior dislocation of the prox radioulnar joint
Dislocation post / antCommon type, hyperextension & pronation
injury. Can also produced by direct trauma over the
ulnar border of the forearm.

FRACTURE OF THE SHAFT OF THE RADIUS AND ULNA
Treatment :Adult ORIF

ELBOW AND ARM
1. # OLECRANON Commonest type is
due to a fall with passive flexion of the elbow combined with powerful contraction of the triceps muscle.
Treatment : ORIF using TBW
(Tension Band Wire)

POSTERIOR DISLOCATION OF THE ELBOW
MECHANISM OF INJURY : Fall on the hand with the
elbow slightly flexed Severe Hyperextension
injury of the elbowCLINICAL FINDING :
Swollen elbow is held in a position of semi flexion
Olecranon is readily palpable posteriorly
RADIOGRAHIC EXAMINATION : Dislocation.

POSTERIOR DISLOCATION OF THE ELBOW
TREATMENT: Closed Reduction Immobilization by cast for at least 3 weeks
COMPLICATION :Elbow stiffnessMedian nerve injury

FRACTURE DISLOCATION OF THE ELBOW
Side swipe injury :Occurs when a driver has his elbow out the
open window of a car at the moment the car is struck from the side by another vehicle.
Usually :Elbow dislocationMultiple comminuted # of the humerus, radius &
ulnaTreatment :
Wait until soft tissue healedORIF

FRACTURES OF THE SHAFT OF THE HUMERUS
> adults Direct trauma # transverse / comminuted Indirect trauma fall on the hand # spiral Clinical Examination :
Flail armPatient tries to support with the opposite hand, Radial Nerve
lesion should always be sought and its presence or absence recorded at the time of the initial examination

FRACTURES OF THE SHAFT OF THE HUMERUS
Treatment :Closed treatmentIndication for ORIF if injury of Brachial artery
which necessitates arterial repairTRANSVERSE # OF THE HUMERAL SHAFT:
Anaesthesia reduction U Slab (Sugar Tong Splint) / Hanging Cast
Clinical union achieved within 6 weeks

FRACTURES OF THE SHAFT OF THE HUMERUS
# SPIRAL & COMMINUTED FRACTURES :Do not require reduction / anaesthesiaGravity alone is adequate to provide alignment
of the fracture fragment immobilized in U shaped plaster slab
COMPLICATION :Radial Nerve InjuryDelayed UnionNon Union

FRACTURES OF THE NECK OF THE HUMERUS
In elderly persons, especially ♀Impacted # relatively commonTreatment :
only protection from further injury by a sling during 6 weeks required for union

SHOULDER JOINT
1. Shoulder Joint Dislocation Anterior Dislocation of the Shoulder
Predominantly of young adults Caused by forced external rotation and extension of the
shoulder Radiographic examination : confirm the diagnosis Treatment :
Reduce as soon as possible, methods : Kocher Method Gravitation HipocratesAfter reduce must immobilized by Velpeau Bandage

SHOULDER JOINT
2. Recurrent Anterior Dislocation of The Shoulder :The stability of the shoulder depend on the integrity of
the joint capsule capsule, capsule & anterior labrum are nearly always avulsed caused the dislocation may recur more and more frequently with less and less violence.
Treatment :Surgical repair with Putti Platt operation capsule as well as
the Subscapularis muscle are divided and then refeed (overlapped) limiting external rotation.

SHOULDER JOINT3. Posterior Dislocation of the ShoulderLess common than anterior dislocationPosterior dislocation can occur :
Fall on the front of the shoulder, with shoulder adducted and internally rotated
Clinical Finding :The patient’s arm seems locked in a position of adduction and
internal rotattedRadiographic finding:
Not readily detected in an AP projection, need special examination :Superoinferior (axillary) projection with the shoulder abducted, is
necessary to confirm that the humeral head is in fact lying posteriorly
Treatment : Closed reduction

SHOULDER JOINT
4. Acromioclavicular Joint Dislocation (AC Joint)
Complains of severe pain over the shoulder
Local tenderness (+) overthe AC joint
Radiolographic examination: Patient standing and holding a
weight in each hand.

SHOULDER JOINT
Treatment :Non operatif : Kenny-Howard Sling, depress the
clavicle and elevate the acromionIf failed ORIF, capsult repair, insertion of a
K-wireK-wire removed after 6 weeks

SHOULDER JOINT5. FRACTURE OF CLAVICLECommon site is the middle third of the clavicleLateral fragment pulled inferiorly and medially by
the weight of the shoulder and upper limbTreatment :
Figure of 8 padded bandageClinical united in 3 weeks
ComplicationMalunionDelayed unionNonunion relative rare

FOOT
2.CALCANEAL #Fall from a considerable height onto one or both heels.High incidence of associated compression # of the spineTreatment
extra-artikular # :Under anaesthesia the two major fragments should
manually compressed from side to side walking cast for 6 weeks
intra-artikular # :ORIF

FOOT
3. FRACTURES OF THE NECK OF THE TALUS No muscle attached to talus> covered by articular cartilageBlood supply not to good# neck talus correlate with ▲ incidence of
avascular necrosis (the body) and non union

FOOT
Mechanism of trauma Severe dorsoflexion injury as may be incurred when the
driver has his foot hard on the brake pedal at the moment of a head-on collision
Treatment :Closed reduction BK cast for at least 8 weeks
Complication:Avascular necrosisDegenerative joint diseaseNonunion

THE ANKLE
# & # DISLOCATIONS OF THE ANKLE1. Isolated # of the Medial Maleolus Abduction injury avulse medial
maleolus below the joint line
Adduction injury shear off the medial maleolus above the joint line
Treatment : Undisplaced : BK cast for 8 weeks Displaced : ORIF

ANKLE
2. Isolated # of the Lateral MaleolusAbduction / external rotation injuryMost common injury of the ankleTreatment :
Closed reduction stable immobilized in BK Cast for 6 weeks
NWB 3 weeks
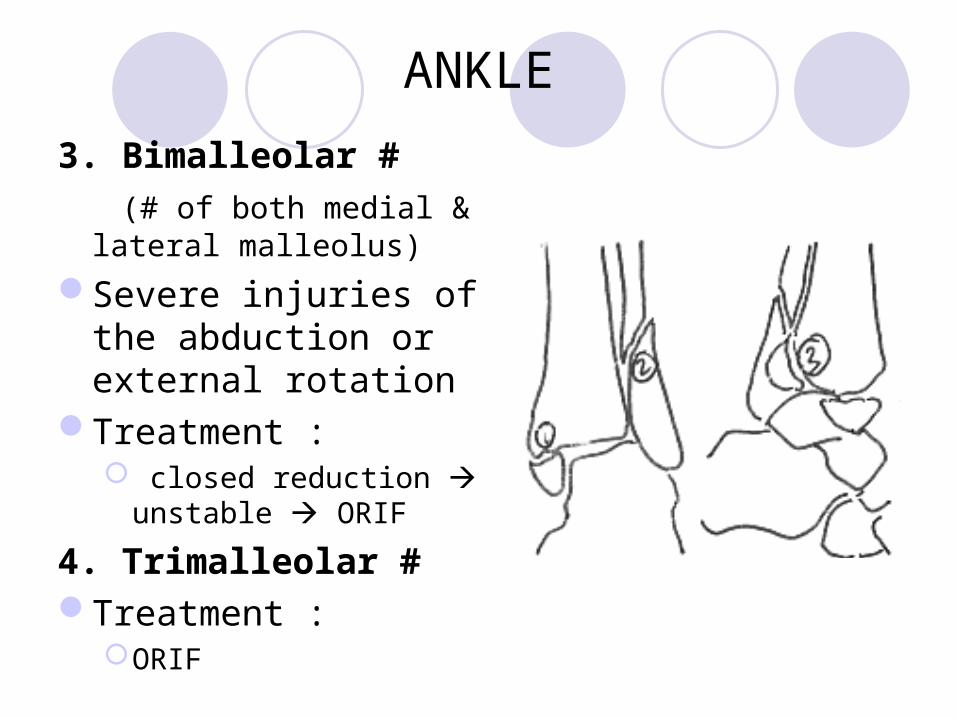
ANKLE3. Bimalleolar # (# of both medial & lateral
malleolus)Severe injuries of the
abduction or external rotation
Treatment : closed reduction
unstable ORIF
4. Trimalleolar #Treatment :
ORIF

ANKLE
Complication :Joint stiffnessnon-union rare>> malunion sbg hsl dari loss of correction
dari fragmen #Degenerative joint disease

LOWER EXTREMITY
# OF THE SHAFTS TIBIA & FIBULA > fractured more frequently Periosteum is thin in adult Frequency open # Rate of union slow Mechanism of injury :
Direct trauma bumper, Traffic accident Clinical features :
Swelling, deformity, Tenderness Radiographic : AP / Lateral
LOWER EXTREMITYTreatment
Reduction of the tibiaOblique & transverse # closed reductionClinical Union after 3-4 weeksUnstable oblique # & spiral # ORIF
ComplicationAnkle stiffnessNerve injuryDelayed unionNon-unionmalunion
KNEE JOINT
1. # of the proximal end of theTibia ( Bumper #) Mechanism of injury :
Usually in elderly A severe abduction injury, usually a direct blow on the
lateral aspect of the limb with the foot fixed on the ground. Treatment:
Closed reduction for elderly If the patient young ORIF

KNEE JOINT
2. Traumatic Dislocation of the knee jointTorn of 4 major ligaments :
CMLCLLACLPCL
Complication:Trauma of the Popliteal Artery risk of gangren in the distal part
Treatment:Reduced as soon as possible
Complete Dislocation of the knee joint
KNEE JOINT
3. FRACTURES OF THE PATELLAIndirect :
Tears of the Quadriceps expansion at the level of the patella produce transverse avulsion fracture of the patella
Direct :Direct trauma comminutted
Clinical finding :Patient can’t extent the lower extremity
Treatment :TBW

KNEE JOINT
4.INTERCONDYLAR FEMUR #Patient fall (knee in flexion position) from
height.Clinical finding : swelling >>Radiolographic :Treatment :
ORIF

FEMUR
FRACTURES OF THE FEMORAL SHAFT
Clinical features: swelling >> deformity
Radiographic examination : Done after ABC stabile

FEMURTreatment:1. Nonoperative treatment :
Longer period in the hospitalLonger period of weight bearingContinuous traction (12 weeks )▼Clinical union▼ active exercise, non weight bearingRadiological union▼Weight bearing
2. Operative treatment : ORIF with intramedullary nail

FRACTURES OF THE FEMORAL SHAFT Indication for intramedullary nail # of the femur :
1. Fail in Closed reduction2. Multiple trauma (head trauma)3. Femoral Artery injury need to repair.4. Elderly, prolonged bed rest is deleterious5. Pathological #
Complication : Shock Fat embolism Knee stiffness Non-union

PELVIS
1. TROCHANTERIC # OF THE FEMUR Include:
Intertrochanter # ( # between the lesser and greater trochanters)
# through the trochanter pertrochanteric # > common in adults over the age of 60 years ♀ > ♂ Clinical features
Lower limb complete external rotation Extremity appears short Upper part of thigh is swollen

PELVIS
Radiolographic examination: extent of the #
Treatment :ORIF Nonoperatif
Complication:Malunion nonoperatif
NECK FEMORAL FRACTURE
1. Subcapital2. Transcervical3. BasilarGarden classification :4 type (intracapsular)Type 1 : incompleteType 2 : complete,
undisplacedType 3 : partially displacedType 4 : complete displaced

NECK FEMORAL FRACTURE
Treatment :Operative : Hemiarthroplasty for the elderly
patientComplication:
Avascular necrosis femoral headNon-union > 30%

TRAUMATIC DISLOCATION &# DISLOCATION OF THE HIP
1. POSTERIOR DISLOCATION Position:
Flexion & adduction, internal rotation
Usually caused by dashboard injury
Extremity became shortens

TRAUMATIC DISLOCATION &# DISLOCATION OF THE HIP
Treatment:Closed ReductionMethods
Complication :Avascular necrosis
femoral headSciatic nerve lesionPost traumatic
degenerative joint disease

TRAUMATIC DISLOCATION &# DISLOCATION OF THE HIP
2. ANTERIOR DISLOCATIONLess commonCaused by a violent injury
which forces the hip into extension, abduction and external rotation.
Radiographical finding: head femur below the
acetabulum

TRAUMATIC DISLOCATION &# DISLOCATION OF THE HIP
Treatment :Closed reduction as soon as possible
Applying traction on the flexed thigh and then internally rotating and adducting the hip.
After reduction, the patient hip should be immobilized in a Hip Spica Cast in its most stable position ( flexion, adduktion, internal rotation)

TRAUMATIC DISLOCATION &# DISLOCATION OF THE HIP
1. Full flexion2. Adduction of the hip3. Internal rotation4. Extension5. Neutral position
