33p. struck by these diseases usually reach death's door after a protracted illness. but...
TRANSCRIPT

ED 422 531
AUTHORTITLE
INSTITUTION
SPONS AGENCYISBNPUB DATENOTEAVAILABLE FROM
PUB TYPEEDRS PRICEDESCRIPTORSIDENTIFIERS
ABSTRACT
DOCUMENT RESUME
CG 028 555
Hinds, Michael deCourcyAt Death's Door: What Are the Choices? An Issue Book forNational Issues Forums.Public Agenda Foundation, New York, NY.; National IssuesForums, Dayton, OH.Charles F. Kettering Foundation, Dayton, OH.ISBN-0-7872-3915-11997-00-0033p.
Kendall/Hunt, 4050 Westmark Dr., Dubuque, IA 52002;toll-free phone: 800-228-0810.Opinion Papers (120)MF01/PCO2 Plus Postage.*Death; Decision Making; Suicide; *Terminal Illness*Assisted Suicide
This paper questions how society should care for people whoare suffering and near death? Underlying this issue are very difficultquestions about the evolving rights of patients, medical standards, andsocietal norms--questions about the American way of death, which ofteninvolves needless pain and unwanted treatment. Three choices are presented ina brief proposal format for use with National Issues Forums. "Choice 1: LetPatients Die with Dignity," holds that physician-assisted suicide is a humaneway of death that is widely and secretly practiced today. "Choice 2: ImproveCare for the Dying," raises the concern that dying patients often sufferneedlessly in our healthcare system, which routinely ignores patient's finalwishes concerning treatment. Correcting the existing system is recommended."Choice 3: Above All, Sustain Life," is based on the premise that life isinvaluable and should be inviolable, and society and the medical communitymust strengthen their commitment to preserving life. References "For FurtherReading" and checklists "In Support" and "In Opposition" are presented witheach choice. A summary that displays comparable points for each viewpoint isincluded. National Issues Formats are described, and ballots to be usedbefore and after attending forum meetings are provided. (EMK)
********************************************************************************
Reproductions supplied by EDRS are the best that can be madefrom the original document.
********************************************************************************

I I I
, C") M
(OIH3)1:131N30 N0I1VI4H0dNI S301:1110S311 lvNolivona3 3H1 01
AC) J
031t4V1:10 N338 SVH 'W1831'1114 SIH1 301100Hd31:1 01 N0ISSINIEI3d"
V
318V11VAV Ad MEI Apgar' Jo uowsoO 11:130
'BOW° luase,, Apuesseaou lou op luau, 4130p slut uo poielssuonnosoio Amon spnod
AUieflb uooanpoioe, eIwOwl 01 apeu, ueep eAseu salueto Jou.V1 0
fougetHINJO 1.101$821U116l0 JO UMW) OW won PCM10,01
se peoopoJoe, SIOQ seo 1uetu0309 SNI. 0 (011:13)1331N30
NOI1VNILIOANI S331:MOS311 1VNOLLV0n03 luatuo.o.oun pus Liam:mod prvon3p3 10 a3.40
NO1131103 O 1N3VIIMIVd30 II
-

NATIONALISSUESFORUMS
A note to the reader about NIF books
Each book in this series for the National Issues Forums outlines an issue and several approaches, or choices, chat address a problem
and its solution. Rather than conforming to any single public proposal, each choice reflects widely held, but contrasting, concerns and
principles. Panels of experts review manuscripts to make sure the choices are presented accurately and fairly.
Unlike most periodicals, issue books do not identify individuals or organizations with partisan labels such as Democrat. Republican,
conservative, or liberal. The goal is to present ideas in a fresh way that encourages readers to judge them on their merit. Issue books
include quotations from experts and public officials when their views appear consistent with the principles of a choice. But these
quoted individuals might not endorse every aspect of a choice as it is described here.

At Death's DoorWhat Are the Choices?
iVT
By Michael deCourcy Hinds
Introduction
How should society care for people who are suffering and near death? That's the issue,and underlying it are very difficult questions about the evolving rights of patients, medicalstandards, and societal norms questions about the American way of death, which ofteninvolves needless pain and unwanted treatment.
Choice I
2
Let Patients Die With Dignity
Physician-assisted suicide is a humane way of death. What'smore, it's widely and secretly practiced today. We shouldlegalize and regulate it to prevent errors and abuses that canoccur in secret and to ensure that all dying patients haveequal access to this practice.
Choice 2
6
What Can Be Done? 7
In Support & In Opposition 10
Improve Care for the Dying 1 I
Dying patients often suffer needlessly in our healthcare system,
which routinely ignores patients' final wishes concerningtreatment. Let's fix the system, and start by giving patientsmore relief from their symptoms and more control overtheir treatment.
Choice 3
What Can Be Done? 12
In Support & In Opposition 15
Above All, Sustain Life 16
Life is invaluable and should be inviolable, and society andthe medical community must strengthen their commitmentto preserving life. Medical science has extended life, butnow some want to abuse that science to shorten life. Thatwould undermine both society and medicine.
What Can Be Done? 17
In Support & In Opposition 20
Summary: What About Claire? 21
Comparing the Choices 22
What Are the National Issues Forums?
Ballots: Register Your Views
Acknowledgments, Credits, and Ordering Information
4
24
25
29
0
At Death's DoorWhat Are the Choices?
Advocates and opponentsof physician-assisted suicide
demonstrate in front of theU.S. Supreme Court.
EClaire S., 68, is a widow. Close friends
and family have moved away from
the small town where she lives,
and terminal illness keeps her house-
bound. Two years ago, she developed
breast cancer. Surgery didn't cure the
disease, but continuing chemotherapy
slows its pace. Painkillers provide some
relief, but often she doesn't have strong
enough medicine or high enough doses to
make her pain bearable. Claire, a retired
accountant, sees no point in continuing
a lonely life of pain and suffering. But she
is afraid to attempt suicide alone, fearing
that she will "botch" it. She wants her
physician's help.
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS
How do Americans want Claire's physicianto respond? The doctor's options include:
o Continuing treatment that sustains life andhope.
o Halting chemotherapy that prolongs her life.
o Treating her for depression.
o Relieving her pain with medication, in highdoses if necessary, despite the chance that anoverdose may unintentionally end her life.
o Prescribing a lethal drug she can use to takeher own life if the doctor is willing to riskprosecution.
Claire's unsettling plea for help was presentedat a symposium on physician-assisted suicide,sponsored by the Ethical Culture Society inNew York. Claire isn't a real person, but a com-posite of dying patients who are crying for help.Symposium participants discussed many wayssociety could help the Claires of America, butthe answers only seemed to spawn new questions.
Physician-assisted suicide, it turns out, is thetip of the iceberg. At first glance, the issue is howsociety can respond humanely to a relativelysmall number of dying patients like Claire whoclearly would like to shorten their lives. Butbeneath the surface is a mountain of questionsabout the evolving rights of patients, medicalethics, societal norms, and the quality of carepatients receive when they become very ill.
The American way of death has become amajor public issue in recent years for many rea-sons. Because of advances in medical technology,death is no longer just a natural event but, inmany cases, it is a medical procedure thatfollows a decision to forego or discontinuelife-sustaining treatment. Meanwhile, patientsare seeking more control over the circumstancesof their death particularly when, for manypatients, the dying process is a gauntlet of high-tech care, unwanted treatments, severe pain, anddepression. The nation's medical establishmenthas advocated for more humane care of terminallyill patients, but reforms have so far proven elusive.
5
To help citizens discuss this emotional,sprawling topic, this guide outlines the issue ofphysician-assisted suicide and three generalapproaches the nation might take.
A Century-Old De ElateOn June 4, 1990, a woman sufferingfrom Alzheimer's disease used Dr.Jack Kevorkian's suicide machine,sparking a national debate aboutthe American way of death. But thiswas really just the latest round in adebate that began as early as the1870s, when physician-assistedsuicide was widely discussed inperiodicals, books, medical societies,and state legislatures. The Ohiolegislature, which took the issue themost seriously, considered and final-ly rejected a 1906 bill to legalizephysician-assisted suicide. Argumentsfor and against physician- assistedsuicide have not changed much in 100 years.
Discussions of physician-assisted suicideebbed and flowed throughout the twentieth cen-tury until Dr. Kevorkian began his crusade tolegalize the practice in 1990. Since then, severalbooks on death have become national best-sellers,including Derek Humphry's Final Exit, a manualwith explicit instructions for committing suicide;it sold 540,000 copies within 18 months of itspublication in 1991. Perhaps the best evidencethat the physician-assisted suicide debate hasentered mainstream America: judges in the 1997Miss U.S.A. beauty pageant asked a contestantto share her views on the subject.
The issue of physician-assisted suicide hasalso re-entered the political arena. Impatientwith legislative inaction, voters initiated ballotmeasures in Washington state in 1991 and inCalifornia in 1992. Both measures, which failedto pass, would have permitted doctors to pre-scribe or administer lethal drugs to terminallyill patients. In 1994, Oregon voters legalizedphysician-assisted suicide and established rulesfor screening patients, intended to make surepatients seeking physician-assisted suicide arecompetent, terminally ill, in great pain, andintent on ending their lives. The law has beenstayed pending review by courts and reconsid-eration by voters in November 1997.
In its first ruling on physician-assisted sui-cide, in June 1997, the U.S. Supreme Courtleft it up to the states to govern the practiceof physician-assisted suicide. The justices
At Death's Door
unanimously upheld laws in New York andWashington that make it a crime for a doctor togive lethal drugs to a terminally ill patient whowants to die. However, the court endorsedcurrent medical practice for treating painaggressively, even if that leads to premature
death as long as the doctor's intentionwas to improve the care of thedying patient.
The justices said that, while thereis no general constitutional right toassisted suicide, they were not"foreclosing" all future claims ofsuch a right for some patients."Throughout the nation, Americansare engaged in an earnest and pro-found debate about the morality,legality, and practicality of physi-cian-assisted suicide," wrote ChiefJustice William H. Rehnquist. Thecourt's inconclusive ruling "permitsthis debate to continue, as it should
in a democratic society," he added.
Saving Lives and Ending ThemSpectacular advances in medicine have given thephysician-assisted suicide debate a new sense ofurgency. Until 1920, pneumonia and influenzawere the leading causes of death and nearly allAmericans died at home. Today, penicillin andother wonder drugs usually cure illnesses likepneumonia, and none of the top five causes ofdeath are infectious diseases. Instead, degenera-tive diseases like cancer lead the list of killers,causing an estimated 70 percent of all deaths.Americans struck by these diseases usually reachdeath's door after a protracted illness.
But instead of going through the door, manypatients pause, their lives artificially sustainedby ventilators, dialysis machines, feeding tubes,and the rest of the miraculous technology in the
I Evidence that the
physician-assisted
suicide debate has
entered mainstream
America: judges in the
1997 Miss U.S.A. beauty
pageant asked a con-
testant to share her
views on the subject.
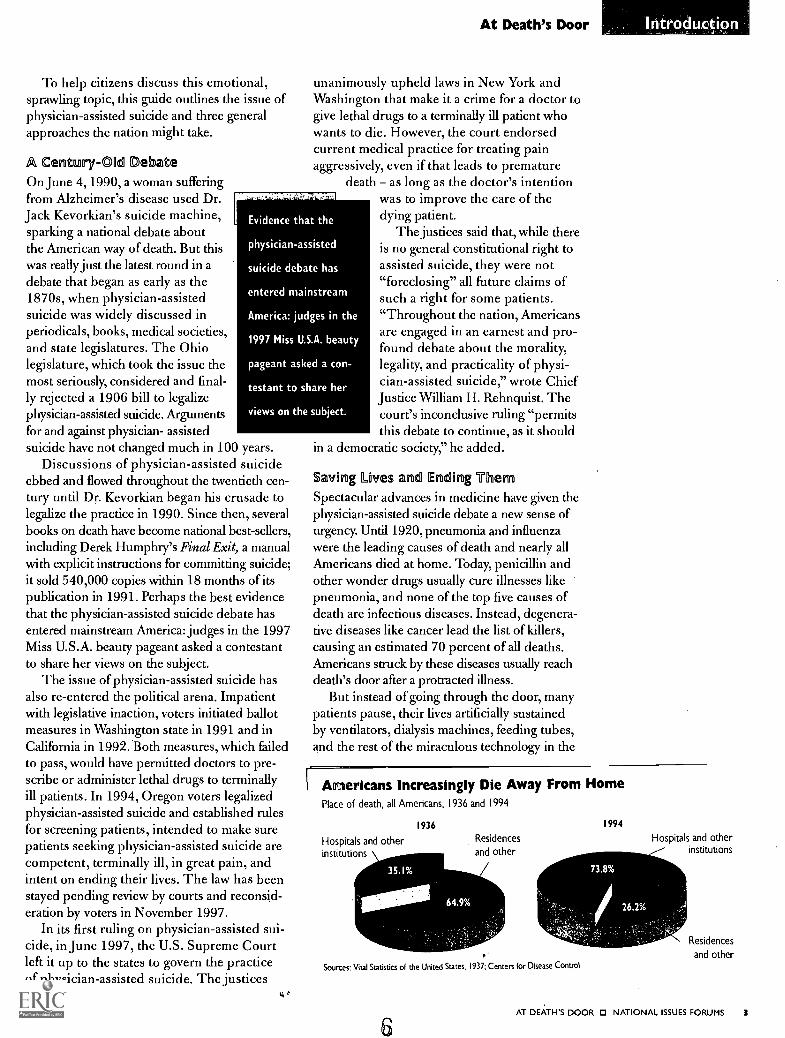
Americans Increasingly Die Away From HomePlace of death, all Americans, 1936 and 1994
1936
Hospitals and otherinstitutions \
Residences
and other
Sources: Vital Statistics of the United States, 1937; Centers for Disease Control
6
1994
Hospitals and otherinstitutions
Residences
and other
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 3

As stark evidence of the growingpublic concern about the way wedie, Derek Humphry's book, FinalExit, made the bestseller list, andmany readers attend his lecturesto learn the best way to commitsuicide.
At Death's Door
intensive care units and hospital wards where mostAmericans die. In this environment, where bio-logical life can be sustained almost indefinitely,death often follows a decision to end treatment.The scope of medical intervention is suggestedby its cost: an estimated 30 percent of thenation's total healthcare budget is spent in thelast six months oflife, much of it in the last month.
It's a perplexing situation: on the one hand,patients want to benefit from all the scientificadvances and optimism that drive medical prac-tice today; on the other hand, modern medicineoften makes death resemble a science experiment,denying patients a peaceful and comfortableparting with families in familiar surroundings.
Recognizing Patient AutonomyTwenty-five years ago, amid a rising public clamorto give patients more control over their bodiesand their treatment, the field of biomedical ethicswas born, and with it, the phrase "patient autono-my" This was the start of the backlash against thetraditional practice of medicine, in which pater-nalistic physicians dictated treatment in what theythought were the best interests of the patient, butoften without informing the patient of the diagno-sis or obtaining consent for the treatment. Today,such behavior would be considered grounds formalpractice, except in medical emergencies.
Medical practice and laws governing terminalcare are in perpetual flux. Here are some majortension points:
o Dying patients may state preferences forreceiving or refusing aggressive treatments suchas resuscitation or emergency surgery; they mayalso write advance directives, living wills, orgive a family member or friend the power ofattorney to make healthcare decisions. But
studies indicate that most doctorsignore these preferences or overrulethem, deeming them medically unsound.By contrast, relatively few healthy peoplemake plans for their end-of-life care, andthose who do plan ahead often change theirminds when they become very sick.
Ea Many dying patients, and most can-cer patients, suffer considerable pain.While the prevalence of unrelievedpain has not been extensively studied,pain management specialists say that agreat many patients suffer needlesslyoften because patients don't knowenough to complain and because doctorsare fearful of giving a lethal overdose of
4 AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS
I Debating the Rights of the Dying
1870s
1906
First major debate about physician-assistedI
suicide in the U.S.
Ohio legislature rejects bill to legalizeassisted suicide.
mu National Society for the Legalization ofEuthanasia is formed.
EnNew York legislature rejects bill to legalizeassisted suicide.
BEIAmerican Hospital Association issuesa "Patient Bill of Rights," which sayspatients should have the right to refuselife-sustaining treatment.
1990
New Jersey Supreme Court permits theparents of comatose Karen Ann Quinlanto disconnect her respirator.
Unitarian-Universalists become the firstreligious body to approve of assistedsuicide for the terminally ill.
Dr. Jack Kevorkian, a retired pathologistin Michigan, begins his crusade to legalizephysician-assisted suicide by helping awoman with Alzheimer's disease endher life.
In its first right-to-die decision, the NancyCruzan case, U.S. Supreme Court rulesthat competent people have a constitu-tional right to refuse treatment, and thatlegal guardians can make that decisionfor incompetent patients.
Voters in Washington narrowly rejecta ballot initiative to legalize physician-assisted suicide.
maCalifornia voters reject a similar measure.
EnziVoters in Oregon approve a ballot initiativeto legalize physician-assisted suicide, but
the law is stayed pending judicial review.
EmTwo federal appellate courts, in overturn-ing state bans on assisted suicide, rulethat terminally ill patients have a consti-tutional right to physician-assisted suicide.
7
U.S. Supreme Court throws out lowercourt decisions, ruling that there is nogeneral constitutional right to assistedsuicide. But the court leaves open thepossibility that some limited right to diecould be claimed in the future.

painkillers. Doctors also worry about patientsbecoming addicted to narcotics. Chronic paincan lead to depression, and sometimes to suicidalthoughts. Studies indicate that most doctors arenot trained to diagnose or adequately treat painor depression.
O The costs of uninsured hospital care candrain the resources of patients and their families.One major study suggests that nearly one in threefamilies with a terminally ill familymember exhausts all or most oftheir savings payinghospital bills insurance
-:$11
f ttt t
doesn't cover.
o The physiciantreating a patientfor pain may inad-vertently end thepatient's life by pre-scribing or adminis-tering an overdose ofpainkillers. But doctorscan also use this legal practice'"---as a cover for intentionally andthus illegally - ending patients' lives.
O Patient autonomy is a major aspect of theassisted-suicide debate. Some advocates ofphysician-assisted suicide see it as a naturalevolution of patients' rights, as the ultimate rightof patients to determine the timing and circum-stances of their own deaths. Some opponentssee physician-assisted suicide as patient auton-omy run amok, where physicians are asked toend lives, in violation of the Hippocratic oathand 2,400 years of professional ethics. Still otheropponents say public demands for the right tophysician-assisted suicide demonstrate, morethan anything else, the high level of frustrationwith a healthcare system that routinely fails tohonor dying patients' preferences for treatmentwhile letting them suffer needless pain anddepression.
At Death's Door
life-support systems should have an equal rightto have a physician help them end their lives.
Opponents see a major difference betweenthe right to refuse a physician's treatment and aright to ask a physician to prescribe lethal drugs.Society has no obligation to end an individual'slife; on the contrary, opponents say, society isobligated to protect life and prevent suicide.
A Framework for DiscussionTo promote an informed discus-
sion of physician-assistedsuicide, this issue book
presents threeapproaches, orchoices, that thenation might take:
Choice One sayssociety must pro-
tect life, but mustalso protect the right
to a humane death. Whennear death and in unbearable
pain, patients should be able toreceive a physician's assistance in ending theirlives. It happens now anyway, but in a secretiveway that spawns error and abuse. Let's regulate it.
Choice Two says the debate about physician-assisted suicide has arisen primarily because thehealthcare system routinely fails to honorpatients' wishes about treatment and failsto relieve their pain and depression. Givingpatients more control over their treatment andrelieving their symptoms is a far better solutionthan supervising suicides.
Choice Three says life is invaluable and shouldbe inviolable, and society and the medical com-munity must strengthen their commitment topreserving it. Medical science has extendedlife, and now some want to abuse that science toshorten life. That would create confusing publicpolicies and weaken public trust in medicine.Assisted suicide is a crime.
ef
A Right to Assisted Suicide?Advocates for physician-assisted suicide assertthat Americans have a sovereign right over theirown bodies. Further, they say citizens should beas free to obtain assistance in suicide as they arenow free to refuse unwanted medical treatmentor to make life-and-death decisions about repro-duction. Advocates also claim that since somepatients already have a legal right to end theirlives by asking a physician to disconnect theirlife-support systems, patients who are not on
For Furrim t=g/At Death's DoorMargaret Pabst Battin, The Death Debate: Ethical Issues in Suicide (Upper
Saddle River, N.J.: Prentice Hall, 1996).
Jonathan D. Moreno, eci., Arguing Euthanasia: The Controversy Over Mercy
Killing (New York: Simon and Schuster, 1995).
Carol Wekesser, ed., Euthana4ia: Opposing Viewpoints (San Diego:
Greenhaven Press, 1995).
8AT DEATH'S DOOR 129 NATIONAL ISSUES FORUMS 5
Let Patients DieWith Dignity
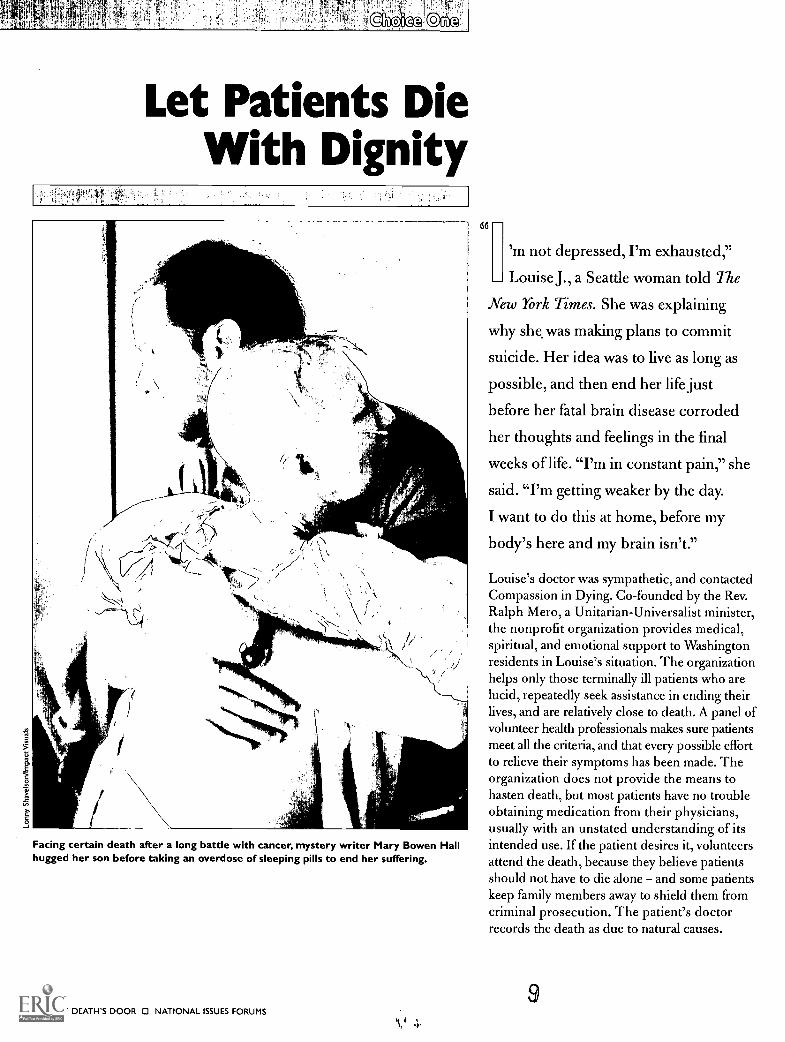
Facing certain death after a long battle with cancer, mystery writer Mary Bowen Hallhugged her son before taking an overdose of sleeping pills to end her suffering.
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS
66
'm not depressed, I'm exhausted,"
Louise J., a Seattle woman told The
New York Times. She was explaining
why she, was making plans to commit
suicide. Her idea was to live as long as
possible, and then end her life just
before her fatal brain disease corroded
her thoughts and feelings in the final
weeks of life. "I'm in constant pain," she
said. "I'm getting weaker by the day.
I want to do this at home, before my
body's here and my brain isn't."
Louise's doctor was sympathetic, and contactedCompassion in Dying. Co-founded by the Rev.Ralph Mero, a Unitarian-Universalist minister,the nonprofit organization provides medical,spiritual, and emotional support to Washingtonresidents in Louise's situation. The organizationhelps only those terminally ill patients who arelucid, repeatedly seek assistance in ending theirlives, and are relatively close to death. A panel ofvolunteer health professionals makes sure patientsmeet all the criteria, and that every possible effortto relieve their symptoms has been made. Theorganization does not provide the means tohasten death, but most patients have no troubleobtaining medication from their physicians,usually with an unstated understanding of itsintended use. If the patient desires it, volunteersattend the death, because they believe patientsshould not have to die alone and some patientskeep family members away to shield them fromcriminal prosecution. The patient's doctorrecords the death as due to natural causes.
9

Louise hung onto life for as long as she could,but her physical health and mental acuity beganto deteriorate rapidly in August 1993. Withpossibly only weeks to live, Louise with hermother, a friend, and the Rev. Mero gathered inher small Seattle apartment crushed 40 sleep-ing pills into a mixture of applesauce and icecream, and swallowed it. As her mother strokedher hand and the Rev. Mero prayed, Louise fellinto a wakeless sleep.
Dying With Dignity"I do think that all human beings have a moralclaim to humane treatment," the Rev. Mero latertold The Times. Supporters of Choice Oneagree. They recognize society's compellinginterest in protecting life, but believe it shouldbe tempered by an individual's right, under cer-tain limited conditions, to choose the time andcircumstances of death. In this view, society hasno interest in protecting the lives of a relativelysmall number of competent patients who are neardeath, suffering unbearable pain, and repeatedlyask for assistance in suicide. In these situations,society's primary obligation is to relieve painand suffering as compassionately as possible.
The best way to accommodate the competingrights and responsibilities of society and patients,in this view, is by legalizing physician-assistedsuicide and closely regulating it to prevent errorsand abuse.
Let patients Die With Dignity
What Can Be Done
Supporters of Choice One generally favor the following measures:
ra Legalize physician-assisted suicide, making it a socially accepted, stigma-free
medical procedure for the relatively few patients who qualify.
m Enact strict rules and medical screening procedures for physician-assisted
suicide. Among other things, rules would restrict these practices to mentallycompetent adults who are terminally ill, suffer unbearable pain, and make
repeated requests for help ending their lives.
63 Permit physicians to practice physician-assisted suicide by administering a
lethal medication when a competent adult meets all the other guidelines
but is physically unable to commit suicide alone.
is Prosecute physicians who violate any of these laws and rules.
B2 Require insurers to provide health and life insurance benefits to people
who die under a doctor's care.
Legalizing assisted suicide would also yieldother benefits; notably, it would free dyingpatients and their families from the stigma ofsuicide, which only adds to their suffering. Foralthough Americans may legally take their ownlives, suicide carries very negative connotationsin our culture, having long been considered acowardly act, a sin, or a symptom of mental illness.
It is tragic when people, still full of productivepotential, kill themselves in fits of depression orbecause of substance abuse. But, in this view,suicide can be a rational medical decision forthose relatively few, mentally competent, termi-nally ill patients who experience life as torture.Documented cases of people who wanted a
physician's help in end-ing their lives include aterminally ill quadri-plegic, who dailyprayed for death; aphysician, who did notwant to be kept aliveon a ventilator but didnot want to die of the
Doctors Already Respond toMany doctors receive requestsPercentage of 828 doctors in Washingtonstate who reported receiving a request from
a patient for help in committing suicide
Doctors who reportedreceiving requests from
patients
Many Assisted-Suicide RequestsMany requests are honoredPercentage of 156 patient requests thatdoctors honored by prescribing a lethal
dose of drugs
Requests that doctorshonored
Source:"Physician-Assisted Suicide and Euthanasia in Washington State:Patient Requests
and Physician Responses:* Journal of the American Medical Association, March 1996
10AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 7

Let Patien s le With Dignity
slow suffocation thatcomes with unplugging themachine; and an AIDSvictim who was losing hissight and memory andwas terrified of what layahead death in a stateof emotional and intel-lectual chaos broughton by AIDS dementia.
Many people feardying more thandeath. "It's notdeath I'm afraidof, it's the processof getting there,"said Mary BowenHall, an author ofpopular mysterybooks including
The QueenAnne Killer
At right and below right:As a painful death from AIDSgrew closer, Pierre Nadeau, aformer trapeze artist, asked aclose friend to give him anoverdose of drugs.
and The SacramentoStalker. In 1989, Hall wasdiagnosed with breast cancer,and in subsequent years, itspread to her bones. She tried many treatments,including bone marrow transplants, but she slow-ly wasted away, suffering bouts of excruciatingpain and panic. She lost control of herbodily functions and had to wear diapers.And, most humiliating of all for her, shehad to be tied to her bed to prevent afall. Before taking her life with a medica-tion prescribed by a compassionate doc-tor in 1994, she said: "There is nothingto be gained by anyone from these nextfew days of misery. It is ridiculous andhumiliating for me to lie here dying fordays. There is no quality left to my lifeand nothing I need to do."
Compassionate Heip in DyingDespite the risk of being charged with afelony and losing their medical licenses,4 in 10 doctors repeatedly say in surveysthat they are willing to help terminally illpatients commit suicide. Three in 10doctors say they are willing to injectpatients with lethal drugs when the pat-ients can't commit suicide themselves.
8 AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS
Doctors aren't just talking. In a landmark 1996study in Washington state, 12 percent of thedoctors surveyed said that in the previous yearthey had received patient requests to help themdie. The doctors acknowledged responding toa quarter of these requests by providing pre-scriptions for lethal drugs or by injecting lethaldrugs, according to the study, done at the U.S.Veterans Affairs Puget Sound Health CareSystem in Seattle.
What's Wrong With This Picture?Compassionate American doctors are beingforced to make life-and-death decisions in ahostile legal environment that isolates them andencourages secrecy and that's bad medicine, inthis view. Consider the impact of secrecy: only 15percent of the patients seeking death obtained asecond opinion; only 24 percent were referred topsychiatrists or psychologists for counseling ormedication; and two patients committed physi-cian-assisted suicide after making only onerequest to die, the Washington study reports.
In normal medical practice, doctors woulddiscuss these difficult cases with their peers andmake referrals to specialists, but as the researchersconclude: "Open, real-time discussion of anindividual patient request is unlikely to occurwhile physician-assisted death remains illegal."
As Choice One supporters see it, Americansshould no longer be asking whether physician-assisted suicide should be allowed, but rather,under what conditions.

Oregon Sets the First StandardA major concern about legalizing physician-assisted suicide is that abuses could occur. Forinstance, society's most vulnerable membersmight feel pressure to choose death rather tharrun up medical bills for relatives, insurers, ortaxpayers to pay. Choice One shares this concertbut says the best way to address it is by legaliz-ing physician-assisted suicide, bringing thenow-secretive practice into the open, and strictiregulating it. In this view, government regulation
lwould set up a comprehensive screening procesito limit physician-assisted suicide to mentallycompetent patients who are near death, sufferunbearable pain, and repeatedly request assis-tance in dying.
As it is now, physician-assisted suicide iswidely practiced, but its avail-ability depends more on thephysician's values and willing-ness to take risks than on thepatient's values and health. Anddoctors who take the risks as amatter of conscience know thatthey have to act alone, violatingprofessional standards that areintended to reduce the chancesof making tragic mistakes.
To remedy this situation,voters in Oregon approved a 1994 ballot mea-sure called the Death With Dignity Act, whichlegalizes physician-assisted suicide and regu-lates it. The law, which has been stayed pendingcourt review, sets many rules that Choice Oneendorses, including the following:
Patients seeking suicide assistance must bementally competent adults with less than sixmonths to live. They must request assistance inwriting and then orally repeat the request 15days later.
o Physicians must ensure that patients havecomplete information about their diagnosis andtherapeutic alternatives, including pain-controltechniques and hospice care.
o A second physician must examine the patientto confirm that the disease is terminal, and thatthe patient is acting voluntarily. Physicians mustrefer the patient for psychological counseling if
Let Patients Die With Dignity
they suspect any emotional disorder is cloudingthe patient's judgment.
IN The patient must be asked to inform his family,but is not required to do so.
Qualified patients who commit suicideunder a doctor's care will not lose anylife or health insurance coverage.
Oregon's regulations are a step in theright direction, but need considerablerefinement, say Choice One supporters.One major problem with the law is that itwrongly forbids physicians from helpingpatients who meet all the requirementsbut are physically unable to commit sui-cide themselves.
When terminally ill patients are also physi-cally immobilized, society must give specialconsideration to their requests for physician-assisted suicide, in this view. These patients wantto escape their suffering by committing suicide,but can't do it alone because they cannot moveor swallow. In these rare cases, physiciansshould be permitted to administer a lethaldrug or, using new computer technology,make it possible for the patient to initiatethe lethal injection by blinking an eyeor spealdng.
Choice One says this practice, whichnow occurs in secret, should be available topatients who meet all the other guidelines.
12
Choice One
Prolonging DeathPercentage of patients dying in
hospitals who spent 10 or moredays in an intensive care unit (ICU)
in a coma or on a ventilator,1989-1994
Source: The Study to Understand Prognoses
and Patient Preferences for Outcomes and
Risk of Treatment (SUPPORT), Robert
Wood Johnson Foundation and National
Institute of Mental Health, 1995
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 9

- * - Let Patients Die With Dignity
Citizens expect society to protect their lives, and thatshould also mean protecting their right to end their lives
in a dignified, humane way. Society must be flexible inresponding to the needs and last wishes of the dying.
No interest is served by prolonging the misery of a rel-atively small number of terminally ill patients who want
to die. They deserve compassionate treatment, and shouldnot have to seek it in secret.
'/ This approach respects patients' autonomy and desire/ for dignity, instead of forcing them to linger on helplessly
and hopelessly.
Since doctors already help many patients die, it wouldbe better for everyone if they did it openly, so that it
could be regulated and made available to eligible patients.
VfAs long as regulations are strict and rigorously en-orced, the danger of abuse will be kept to a minimum.
When a dying patient with intolerable pain wants tocommit suicide but isn't able to move or swallow, it's
only humane for a doctor to help.
'Once a decision has been made to end a life, it is betterto do it quickly and painlessly. Physician-assisted suicide
would be more humane than withdrawing treatment, nutri-tion, water, and air, which is currently allowed.
/57 Recognizing the patient's right to choose the timing/ and circumstances of death eases psychological
suffering. A study in Washington state foundthat many patients who asked for lethalprescriptions never used them.
10 AT DEATH'S DOOR 0 NATIONAL, ISSUES FORUMS
This is a very dangerous choice that threatens society'sability to protect life.
Abuses would be inevitable. Research indicates thatdoctors who support physician-assisted suicide admit
knowing relatively little about pain management and reportrelatively high levels of stress and professional burnout.
-:"Aearly all suicidal people are depressed and needtreatment, not death. Requests for assisted suicide
come mostly from chronically ill, not terminally ill, patientswho suffer more from anxiety than pain.
;Once legal, a right to die could become a duty to diefor patients who feel financial or emotional pressure
from relatives, medical professionals, or insurers.
Given current pressures to ration healthcare, legalizingphysician-assisted suicide would create impossible
conflicts of interest and undermine public trust in medicine.
This choice blurs the critical difference between aphysician who legally withdraws medical treatment to
let nature take its course and a physician who overrides thecourse of nature by prescribing lethal drugs.
V This choice misses the real problem: our healthcaresystem fails to provide humane care for the dying or
to honor patients' final wishes to avoid aggressive treatment.
Some supporters of assisted suicide don't want it\ legalized. They say it's better the way it is: widely
available, but carefully practiced by physicians under threatof criminal prosecution.
Some say government should not decide who qualifiesfor assistance in suicide. They say physicians should
help anyone in pain.
For Further Reading/Let Patients Die With DignityLisa Belkin, "There's No Simple Suicide" (The New York
Times Magazine, November 14, 1993).
Derek Humphry, Final Exit: The Practicalities of Self-Deliverance and Assisted Suicide for the Dying (New York:
Dell Publishing, 1991).
Timothy E. Quill, M.D., Death and Dignity (New York:
W.W. Norton gc Company, 1993).

Improve Carefor the Dying
,..01a0P1'
Home hospice care providescomfort for incurable patientswho do not want to die inpain or suffer through unwantedtreatment.
id
've just plain lived too long," said
the retired teacher in Minneapolis.
She told her doctor that she had buried
her family and outlived most of her
friends as well as her own 83-year-old
body. Crippled by arthritis, she lived
in pain and isolation. "I wish there was
some way you could help me end my
life," she said.
14
Recalling this conversation in the October 1996Minneapolis-St. Paul Magazine, her physician,Dr. Steven Miles, said he replied: "I personallydo not assist patients' suicides. But let's keeptalking. Let's see what we can do in the courseof three months to bring your quality of lifecloser to your criteria for living." Miles, a spe-cialist in geriatrics, put her in touch with asocial worker and a visiting nurse. He replacedher over-the-counter arthritis medicine with anarcotic, which relieved her pain and increasedher mobility. And he prescribed an antidepres-sant, which lifted her dark mood within a month.
When she died of a stroke two years later, itturned out that she had expressed her apprecia-tion in a remarkable way: she asked in her willthat her ashes be shared equally by her socialworker, visiting nurse, and doctor.
Fix the SystemChoice Two says the extraordinary public con-sideration of physician-assisted suicide is thesocietal equivalent of an individual suicideattempt, which is nearly always a depressedperson's cry for relief of pain and suffering, notdeath. Society should respond to this public cryfor help, in this view, by greatly improving thecare of dying patients.
When patients like the retired teacher voice asuicidal wish to escape pain and suffering, theyare convinced that death is the only exit. Butthey are wrong. Doctors like Miles and his teamof healthcare professionals can nearly alwaysdrive away suicidal impulses with adequatetreatment for pain, suffering, and depression.But physicians like Miles are the exceptions tothe rule in American healthcare, a system thatroutinely fails to make patients comfortable,especially dying patients. This is not news tothe medical establishment: the major profes-sional organization, the American MedicalAssociation, with 300,000 members, acknowl-edges in a 1996 report, "Expertise in painmanagement is often not available to patients,
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 11

Hospital Deaths:Often painful,costly, and out ofpatients' controlNote: Data from study of10,000 patients dying in hospitals,1989-1994
Percentage of patients dying inhospitals who experiencedmoderate or severe pain at leasthalf the time during their lastfew days
Percentage of physicians whofailed to find out whether patientswanted to be resuscitated in anemergency
Percentage of dying patients' families
that spent all or most of their savings
on patients' hospital care
Source:The Study to Understand Prognosesand Patient Preferences for Outcomes and
Risk of Treatment (SUPPORT), Robert Wood
Johnson Foundation and National Institute ofMental Health, 1995
Improve Care for the Dying
and comprehensiveand enduring careis the exception." Inthis view, the sys-tem's failure leadsmany Americans todread the dyingprocess and mistak-enly demand a rightto speed it up witha medically super-vised suicide.
According toChoice Two, soci-ety and physiciansare obliged to easethe pain and suffer-ing of death. Thismeans doing every-thing possible tomake terminally illpatients comfort-able, but at thesame time doing nothing to hasten or prolongthe dying process. The operative principle shouldbe: let nature take its course, with healthcare pro-fessionals easing that course as much as possible.
In this view, then, Choice One's call forlegalizing physician-assisted suicide does notaddress Americans' underlying concerns aboutdying namely, that costly hospital care imposesa huge burden on many families and that hospi-tals allow many patients to endure severe pain,depression, and unwanted medical procedures.Studies have repeatedly shown that nearlyall people who express suicidal thoughts aredepressed and respond successfully to treatmentfor depression but most doctors admit theyare unable to diagnose depression.
"We must focus our efforts and attentionon improving the care of the dying," says Dr.Kathleen M. Foley, sounding the main theme ofChoice Two. Foley, co-chief of the Paiti andPalliative Care Service at Memorial Sloan-Ketter-ing Cancer Center in New York, continues: "Realautonomy at the end of life can only be realizedwhen a full range of treatment is available andaffordable, and patients understand all theiroptions." Choice Two calls for improving theend of life with improved comfort care, painmanagement, and mental health treatment. Toaccomplish this, patients must be given moreinformation and more control over their
Supporters of Choice Two generally favor the following measures:
Improve medical training: only 5 of the nation's 126 medical schoolsrequire courses in the care of the dying.
Expand palliative care, which provides as much comfort as possible topatients at every stage of their illness and treatment.
Insist that insurers cover palliative and hospice care.
El Remove barriers to effective pain management, including inadequate train-ing of physicians and nurses and overly restrictive regulation of narcotics.
Provide mental health care for terminally ill patients, who are prone tomental suffering, especially depression.
im Educate patients about end-of-life care. Let patients give legally bindingdirectives, not just preferences, as a way to ensure they don't suffer throughunwanted treatment.
Make ignoring a dying patient's directive or allowing a patient to sufferneedless pain standard grounds for a finding of malpractice.
12 AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS
treatment, and medical professionals need moretraining in the care of the dying. Legal andinsurance reforms are needed to ensure thatpatients receive appropriate care. Once the sys-tem is fixed, suicide will no longer be an issue.
Treat the Patient, Not just the DiseaseAmericans dread the dying process because it'scostly, painful, and filled with unwanted hospitalprocedures and treatment. "If dying patientswant to retain some control over their dyingprocess, they must get out of the hospital," Dr.George J. Annas flatly states. He is director ofthe Law, Medicine, and Ethics Program atBoston University.
Take Hazel Welch, a 92-year-old patient witha perforated stomach. She told her doctor thatshe didn't want surgery, knowing she wouldultimately die without it. But her physician waspersuasive and Miss Welch relented. The opera-tion failed, leaving her at death's door, feelingwretched for two weeks. Before dying, MissWelch reproached her physician for putting herthrough this torment. The physician, SherwinB. Nuland at the Yale-New Haven Hospital inConnecticut, says he regrets only the poor out-come. Not to have tried to save his patient, hewrites in his book How We Die, would haverisked the "scorn of my peers." As he explains:"The code of the profession of surgery demands
4 5
that no patient as salvageable asMiss Welch be allowed to die if astraightforward operation can saveher...mine was strictly a clinicaldecision and ethics should nothave been a consideration."
In a nutshell, that professionalattitude is what's wrong withAmerican medicine, according toChoice Two. Research confirmsthat every facet of medical culture
from the training of doctors toinsurance reimbursement policiesto the over-reliance on high-techtreatment creates an environmentthat ruins the chances for mostAmericans to have gentle, peacefuldeaths. Consider some findings of a landmarkstudy, completed in 1995 arid sponsored by theRobert Wood Johnson Foundation and theNational Institute of Mental Health:
Improve Care for the Dying
in Patients suffer needless pain. Halfof all conscious patients sufferedmoderate to severe pain at least halfof the time during their final daysand weeks. Medical authorities saythis situation is inexcusable.
o Patients' wishes are routinelyignored. Nearly a third of the 10,000dying patients surveyed had notwanted to be resuscitated in a med-ical emergency, but only half of theirdoctors complied with their request by putting"do not resuscitate" orders on their bedsidecharts. When doctors did issue these orders,half of the patients who got them had alreadyspent eight or more days in intensive care units,where mechanical ventilation and invasive pro-cedures are commonly used to keep people alive.
ts Aggressive treatment drains families' resour-ces. Nearly one-third of the patients' familiessaid they spent all or most of their savings onuninsured hospital services.
The way we care for dying patients is deplor-able, the American Medical Association states inits 1996 report: "We are concerned about provid-ing overly aggressive, unwarranted care while care
that is optimally suited to the dyingperson's needs is often not availablein our healthcare system or is notcovered by insurance."
To Comfort APwaysMost Americans die in hospitals,where physicians and nurses
I valiandy fight disease to the death.But in these battles, the pain, suf-fering, and wishes of patients areoften overlooked.
There is an alternative to hospitals: hospicecare. Hospice treatment flows from the belief that
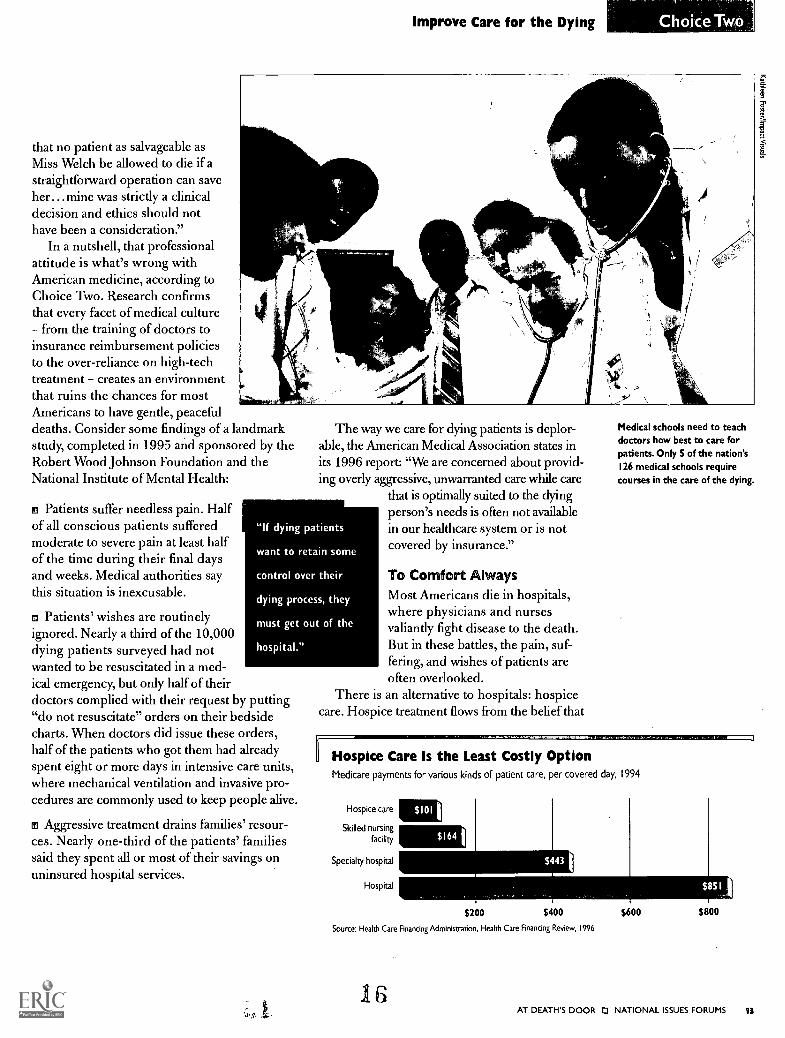
Medical schools need to teachdoctors how best to care forpatients. Only 5 of the nation's126 medical schools requirecourses in the care of the dying.
IHospice Care Is the Least Costly OptionMedicare payments for various kinds of patient care, per covered day, 1994
Hospice care
Skilled nursing
facility
Specialty hospital
Hospital
$164 1
$200 $400
Source: Health Care Financing Administration, Health Care Financing Review, 1996
16
$600 $800
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 13

Comfort CareCan Ease theDying ProcessPercentage of cancer patients
in hospice care who sufferunmanageable pain
2%
Percentage of hospice patientswho die at home
Percentage of hospice patients'
families that are satisfied with
hospice care
Sources: American Medical Council on
Scientific Affairs, 1996; National Hospice
Organization, 1996
Comfort care for terminally illpatients at home is less costly thanhospital care, but many insurersdo not provide adequate coveragefor such essentials as home healthaides or treatment to manage pain.
Improve Care for the Dying
death should neither be hastened nor postponed;an often-cited credo for hospice care is "to curesometimes, to relieve often, to comfort always."
There are about 100 hospice care facilitiesnationwide, serving about 10 percent of the400,000 patients who get hospice care eachyear; the rest get hospice care at home. Hospicecare emphasizes the relief of pain and other symp-toms, and recruits many community volunteersto help improve the patient's quality of life.Consider two major benefits of hospice care:
o Less financial strain on families. As an indi-cator of cost, compare what government insuranceprograms paid in 1994: $101 a day for hospicecare, and $851 a day for general inpatient care ina hospital. But, paradoxically, public and privateinsurers frequently deny coverage for manyhospice care services, often limiting reimburse-ment for such essentials as pain management andhome health aides.
o Greater comfort. Hospice patients knowthat they need not suffer pain, and with their
(lc
agreement, physicians administer as muchmedication as necessary to relieve pain. Everymedical procedure carries a risk, and the risksof aggressively treating pain include a patient'slosing consciousness and even dying. When aphysician's intention is clearly to reduce pain,and not to cause death, aggressively treating painis widely considered morally, medically, andlegally sound.
But hospice care isn't the whole answer. Forone thing, people who are still receiving exten-sive treatment usually aren't eligible for hospices.For another, by the time physicians refer patientsto hospices, many patients have already enduredneedless pain and suffering and have, on average,only a month to live. And finally, most homehospice patients do not receive continuing carefrom physicians trained in comfort care, which isalso called palliative care.
What's needed, in addition to expanding andimproving hospice care, is a system-wide expan-sion of palliative care, which seeks to provide asmuch comfort as possible to patients at everystage of their illness and treatment. And comfortcare must include mental health care, becausethe mental and physical health of the terminallyill often deteriorate together.
'to
94 AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS
If care for the dying were improved, patients would notwant to hasten death.
Americans endure needless pain in hospitals. Studiesrepeatedly indicate that most cancer patients in hospitals
suffer severe pain, compared with only 2 percent of cancerpatients in hospice care.
Nearly all suicidal people suffer from depression; when/ treated, the desire for death nearly always fades away,
studies indicate.
If caregivers consistently honored patients' right to,/ refuse treatment, there would be little demand for theright to physician-assisted suicide, the most extrememeasure of patient control.
Unwanted treatments waste resources that are needed/ to care for others.
/Patients have the legal right to refuse treatment, andthey should be able to exercise that right.
/Legal reforms are needed to force improvements in/patient care, as voluntary efforts over the years have
failed to make enough progress.
We know what works: comfort care is extremelyeffective in addressing the many needs of dying patients
and their families.
Hospice care is less costly than hospital care, and allowspeople to die at home. Insurance policies, paradoxically,
force many patients into higher-cost hospitals by not providingadequate coverage for hospice costs.
41 Because it is far less costly than hospital care, hospicecare relieves some of the financial pressures on families,
which are often cited as a reason patients might considerphysician-assisted suicide.
I orFurtheirteag/& Improve Care for the DyingDaniel.Callahan, The Troubled Dream of Life: LivingWith Mortality (New York: Simon and Schuster, 1993).
Eric J. Cassell, The Nature of Suffering and the Goals ofMedicine (New York: Oxford University Press, 1991).
Judy Foreman and Michele McDonald, "Choosing aGood Death" (The Boston Globe, June 23,1996).Also available on the Internet athttp://www.boston.com/globe/ hospice/home.htm
IL,
Improve Care for the Dying o
In Opposition
If terminally ill people want to die, they should have; /-\:, the right to do so.
XPhysicians can relieve severe pain, but some peopleprefer to end their lives rather than live in a coma-like
state induced by heavy sedation and opiates.
Short of terminally sedating patients, even the mostskillful physicians cannot relieve all the pain suffered
by about 2 percent of cancer patients in hospice care, as thischoice acknowledges.
Choice Two opposes physician-assisted suicide,but supports physicians who treat pain with such
large doses of medication that the patient may die.Medicating patients to the point of death is a way somephysicians disguise mercy killing.
XTreatment cannot help patients who are wasting away,losing control of bodily functions, and feeling utterly
dependent on others. Shouldn't these patients have a right toend their lives?
In calling for more patient control over care, this choiceignores a very important fact: physicians are the
medical experts. Allowing patients to issue directives abouttheir treatment would inevitably cause premature deaths.
'-'When about 40 million Americans lack basic healthinsurance, it's highly questionable whether the
nation can afford to expand coverage for pain management,home nursing, and psychiatric treatment for terminalpatients.
Hospice care is not for most people. Studies suggestthat most patients are unwilling to give up hope for a
cure or a treatment that extends their lives. This means mostpeople will continue to die in hospitals,
accepting all the tradeoffs thataccompany that decision.
SlOP
PA Ncria-4 Sa.!)
NkubeAT DEATH'S. DOOR NATIONAL ISSUES FORUMS IS
Above All,Sustain Life
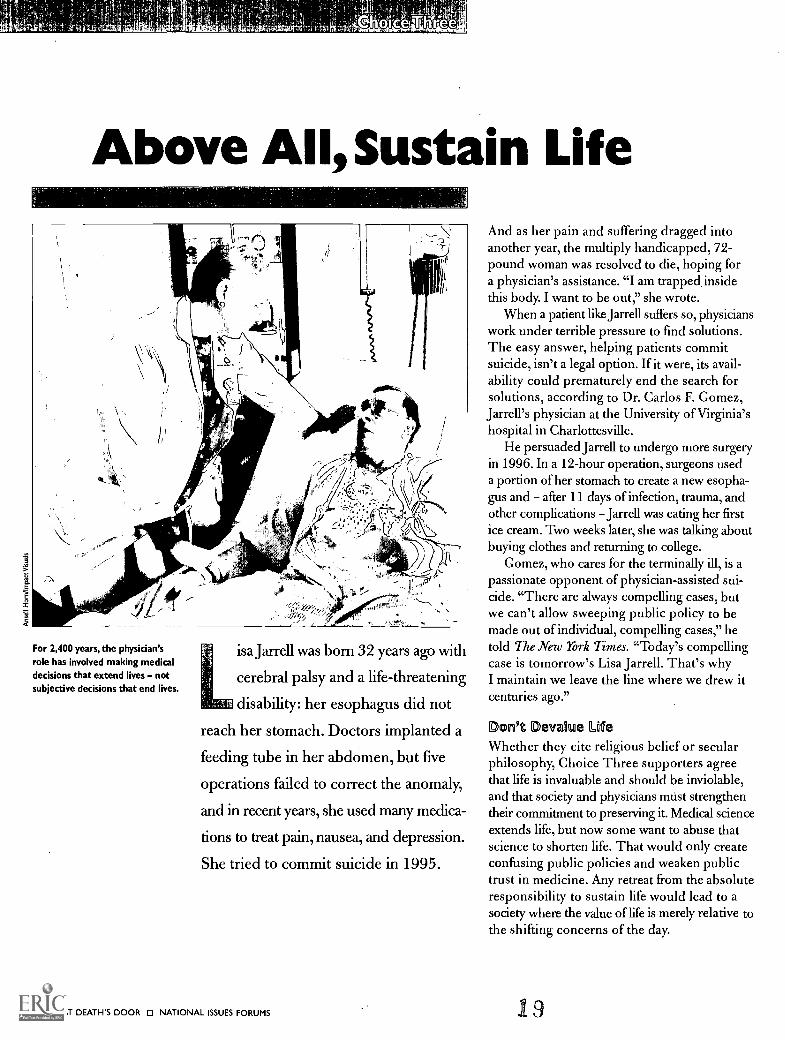
For 2,400 years, the physician'srole has involved making medicaldecisions that extend lives notsubjective decisions that end lives.
isa Jarrell was born 32 years ago with
cerebral palsy and a life-threatening
disability: her esophagus did not
reach her stomach. Doctors implanted a
feeding tube in her abdomen, but five
operations failed to correct the anomaly,
and in recent years, she used many medica-
tions to treat pain, nausea, and depression.
She tried to commit suicide in 1995.
96 AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS
And as her pain and suffering dragged intoanother year, the multiply handicapped, 72-pound woman was resolved to die, hoping fora physician's assistance. "I am trapped insidethis body. I want to be out," she wrote.
When a patient like Jarrell suffers so, physicianswork under terrible pressure to find solutions.The easy answer, helping patients commitsuicide, isn't a legal option. If it were, its avail-ability could prematurely end the search forsolutions, according to Dr. Carlos F. Gomez,Jarrell's physician at the University of Virginia'shospital in Charlottesville.
He persuaded Jarrell to undergo more surgeryin 1996. In a 12-hour operation, surgeons useda portion of her stomach to create a new esopha-gus and after 11 days of infection, trauma, andother complications Jarrell was eating her firstice cream. Two weeks later, she was talking aboutbuying clothes and returning to college.
Gomez, who cares for the terminally ill, is apassionate opponent of physician-assisted sui-cide. "There are always compelling cases, butwe can't allow sweeping public policy to bemade out of individual, compelling cases," hetold The New York Times. "Today's compellingcase is tomorrow's Lisa Jarrell. That's whyI maintain we leave the line where we drew itcenturies ago."
Don't Devalue LifeWhether they cite religious belief or secularphilosophy, Choice Three supporters agreethat life is invaluable and should be inviolable,and that society and physicians must strengthentheir commitment to preserving it. Medical scienceextends life, but now some want to abuse thatscience to shorten life. That would only createconfusing public policies and weaken publictrust in medicine. Any retreat from the absoluteresponsibility to sustain life would lead to asociety where the value of life is merely relative tothe shifting concerns of the day.
1 9

"Human life, as a gift of God, is sacred andinviolable," Pope John Paul II writes in his 1995encyclical, Evangelium Vitae. "Not only musthuman life not be taken, but it must be protectedwith loving concern." Suicide, he adds, is "asobjectionable as murder" and physician-assistedsuicide "can never be excused" and is "gravelyimmoral."
Charles Dougherty, director of the CreightonCenter for Health Policy and Ethics, makes asecular argument that what's best for society isultimately what's best for the individual. Andeven if physician-assisted suicide might makesense in isolated cases, he says, legalizing thepractice would destroy a common bond thatholds society together.
Choice Three calls for recommitting thewhole force of society to each patient's struggleto get well. In this view, Choice One's call forlegalizing physician-assisted suicide is morallyand socially intolerable. Choice Two goes out ofmedical bounds in demanding that patient pref-erences overrule professional judgment in medicalemergencies. And Choice Two goes out of moralbounds by giving a higher priority to patientcomfort than to life itself by promoting theadministration of painkillers in high doses thatcan be life-threatening.
Science's Gift of Life:Medical advances help increase longevityLife expectancy at birth, by gender, 1910-2030
Note: Data for 2010 and 2030 are projections.
1910 1920 1950 1970 1990 2010 2030
El Male Female
Sources: 1996 Greenhook. House Ways and Means Committee,
and National Center for Health Statistics
Above All, Sustain Life
: - -
Supporters of Choice Three generally favorthe following measures:
Respond to requests for physician-assisted suicide the way physicians alwayshave: with mental health treatment and counseling.
Enact a federal law banning all forms of physician-assisted suicide. Opposestate legislation and ballot measures that seek to legalize physician-assistedsuicide.
Require that physicians obtain patients' or families' consent before with-drawing or withholding life-preserving treatment.
Redouble efforts to ensure that physicians do everything possible to sustainlife; it's not their business to decide who should live or die.
Strengthen criminal laws by imposing mandatory minimum penalties andprison sentences for physicians who assist in suicide.
To further deter these practiceS. enact civil laws that make it easier to bringmalpractice suits against physicians who assist in a suicide.
_
Trouble Brewing AlreadyUnfortunately, in this view, society's commitmentto protecting life is already fraying. For example,physicians are authorized to make medical deci-sions often without the consent of patients ortheir families to end patients' lives by withhold-ing or withdrawing life-sustaining treatment,including feeding tubes, that they consider futile.
Choice Three insists that physicians stopmaking these life-and-death decisions about treat-ment, especially since physicians acknowledgethat they can rarely locate the point when treat-ment becomes futile. This is no minor concern:one in three doctors say they have withdrawnlife-support systems without the knowledgeor consent of the patient or a family member;and 3 percent said they had done so over theobjections of a patient or family member, accord-ing to a 1995 national study published in theAmerican Journal of Respiratory and CriticalCare Medicine.
Choice Three also warns that if society grantsterminally ill patients a fundamental right to beassisted in suicide, courts would inevitably beasked to expand this right to patients who aretoo immobilized to commit suicide withoutphysical assistance, or who are chronically ill.And since the law already permits legal guardiansto refuse treatment on behalf of incompetent
20
Any retreat from the
absolute responsibility
to sustain life would
lead to a society
where the value of life
is merely relative to
the shifting concerns
of the day.
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 17

Members of the group Not DeadYet demonstrate against thelegalization of physician-assistedsuicide.They fear that legalizationwould result in pressure on severely
disabled or chronically ill peopleto commit suicide.
'
Above All, Sustain Life
patients, legal guardians might soon find them-selves thrust into the role of deciding whether aphysician should end the lives of relatives whoare demented or in comas, or babies who areborn with severe birth defects.
A right to die might also evolve into a dutyto die, say those who favor Choice Three, espe-cially for elderly or disabled patients who mayfeel or be told that they are a financial andemotional drain on family and society.
Even 'Hopeless' Patients RecoverPercentage of British patients diagnosed with persistent
vegetative state who were misdiagnosed or who emerged
from vegetative state, 1992-1995
Note: Persistent vegetative state is diagnosed when a
patient is thought to have permanently lost function ofthe cerebral cortex, and remains permanently unaware.
Emerged fromMisdiagnosed vegetative state
X
Remainedunconscious
Source:"Misdiagnosis of the Vegetative State: Retrospective Study in a
Rehabilitation Unit," British MedicalJournal, July 1996
tit
MX)t.:AD
58 AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS
n' '' -
And if physician-assisted suicide is redefinedas a medical treatment, society might even cometo view suicide as a cost-effective way to keephealthcare spending down. Farfetched? InOregon, where a 1994 law permitting physician-assisted suicide has for now been stayed bycourt appeals, the legislature has already adopteda rationing plan for the poor: it provides Medicaidfunding for physician-assisted suicide but notfor treatment, unless it is expected to improve adying patient's "low quality of life."
Give No Deadly DrugIn the evolution of modern medicine from prim-itive magic, a historic advance occurred 2,400years ago when Hippocrates, known as thefather of medicine, convinced his colleagues to,stop killing incurable patients who wanted todie, according to the anthropologist MargaretMead. Most medical school graduates still takethe Hippocratic oath, in which doctors swearthey will "give no deadly drug to any, though itbe asked of them, nor suggest any such counsel."
In this view, the physician's only role is tocure illnesses or at least ameliorate their symp-toms. Suicide is not a medical procedure or amedical therapy, and physicians cannot assist insuicides without becoming arbiters of life anddeath and, inevitably, weakening public confi-dence and trust in medicine. "Permitting assistedsuicide would compromise the physician's pro-fessional role, because it would involve physiciansin making inappropriate value judgments aboutthe quality of life," Dr. John Glasson writes in the1994 Report of the Council on Ethical andJudicial Affairs of the American Medical Asso-ciation. By comparison, physicians do not makesuch judgments when a patient or a patient'slegal guardian refuses treatment that artificiallysustains life. In this situation, the physician letsthe underlying disease end the patient's life.
Given the uncertainty of diagnosis and treat-ment, the role of physicians must be limitedto preserving life, in this view. Two researchfindings:
o It's hard to estimate how long patients willlive. According to a 1995 study at the OregonHealth Sciences University in Portland, one intwo Oregon doctors say they can't predict whena patient has less than six months to live, thedefinition of "terminally ill."
o Diagnoses can be wrong. British and Americanstudies in 1996 found that diagnoses of persis-tent vegetative states are often made in error.
21
Consider one near-tragedy: Theresa De Vera,a 21-year-old college student in Los Angeles,had a severe asthma attack in 1996 and slippedinto a coma. After three months, physiciansdiagnosed her condition as a persistent vegetativestate. Then one day, within earshot of De Vera,physicians asked family members to be "realistic"about her chances and to consider having herorgans "harvested" for transplantation beforeremoving life supports, according to The LosAngeles Times. De Vera started to cry. Thenext month, she pulled out of the coma andstarted a journey toward complete recovery.
Slipping Down the SlopePhysician-assisted suicide is openlypracticed in the Netherlands and theDutch experience is debated aroundthe world. Proponents talk aboutthe Netherlands' humane treat-ment of people who want to die;opponents, including ChoiceThree supporters, say theNetherlands provides anexample of a society putting itselfon a slippery moral slope by acceptingphysician-assisted suicide as a social norm.Consider the path the Netherlands has taken:
Above All, Sustain Life
rag Medical guidelines in 1984 goa step further, permitting physi-cians to administer lethal drugsto incurable adults and children(at the request of a legal guardian).
a A 1985 court decision elimi-nates the requirement that apatient be terminally ill, and per-mits physicians to assist in thedeaths of chronically ill patientsas well as babies born with severedefects such as Down's syndromeand spina bifida.
o A 1993 court decision permitsassisted suicide and physician-
assisted suicide forpeople whosuffer psycho-
logical pain, butno physical pain.
A 1973 court case opens the way for physician-assisted suicide to become an accepted medicalpractice for ending the lives of terminally illpatients with unrelenting pain.
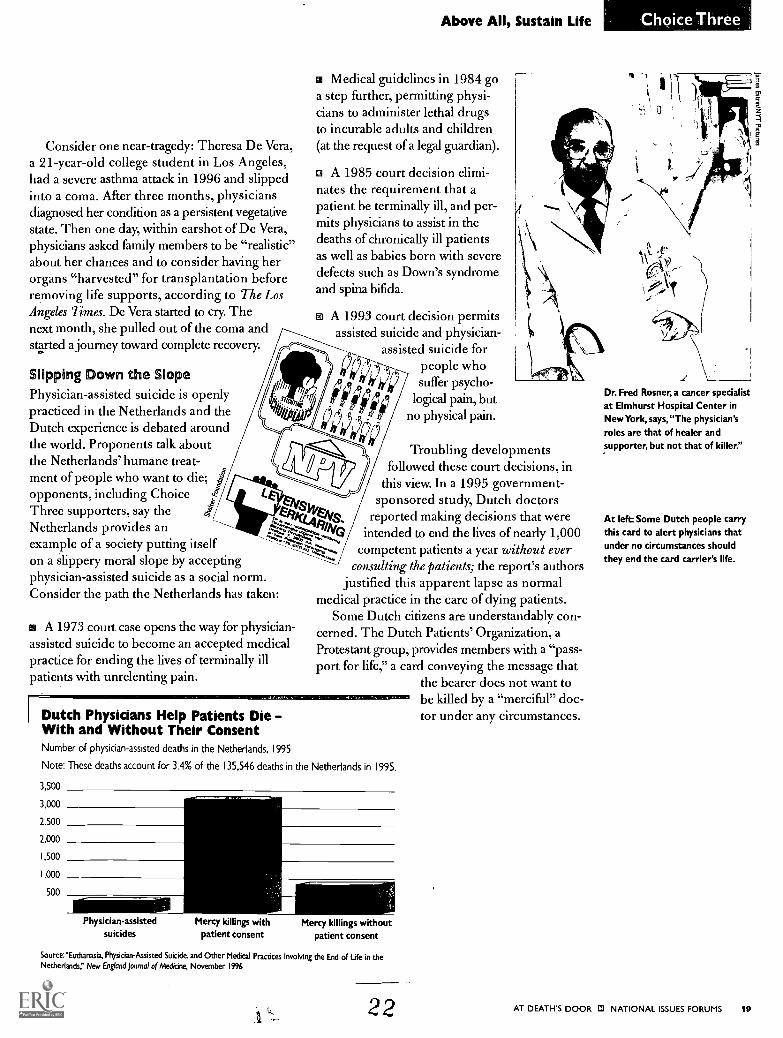
Dutch Physicians Help Patients DieWith and Without Their ConsentNumber of physician-assisted deaths in the Netherlands, 1995
Note: These deaths account for 3.4% of the 135,546 deaths in the Netherlands in 1995.
3,500
3,000
2,500
2000
1,500
1,000
500
Choice Three
Troubling developmentsfollowed these court decisions, in
this view. In a 1995 government-sponsored study, Dutch doctors
reported making decisions that wereintended to end the lives of nearly 1,000
competent patients a year without everconsulting the patients; the report's authors
justified this apparent lapse as normalmedical practice in the care of dying patients.
Some Dutch citizens are understandably con-cerned. The Dutch Patients' Organization, aProtestant group, provides members with a "pass-port for life," a card conveying the message that
the bearer does not want tobe killed by a "merciful" doc-tor under any circumstances.
Physician-assistedsuicides
Mercy killings withpatient consent
Mercy killings withoutpatient consent
Source:"Euchanasia. Physician-Assisted Suicide, and Other Medical Practices Involving the End of Ufe in theNetherlands," New England Journal of Medicine, November 1996
22
Dr. Fred Rosner, a cancer specialist
at Elmhurst Hospital Center inNewYork,says,"The physician'sroles are that of healer andsupporter, but not that of killer."
At left:Some Dutch people carrythis card to alert physicians thatunder no circumstances shouldthey end the card carrier's life.
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 1 9

Above All, Sustain Life
In Supirciii"
VreLife is invaluable and should be inviolable. The primarysponsibility of society is to protect life. Backing away
from this principle would devalue life.
VreThe physician's only proper role is saving lives andlieving symptoms. Asking doctors to assist in suicide
would compromise their role and weaken patient trust.
kliSuicideis a tragic, individual act. Legalizing physician-
assisted suicide would make it the social norm.
VELegalizing physician-assisted suicide would invite thend of abuses that occur in the Netherlands, where it's
widely practiced.
Legalizing physician-assisted suicide would also createV/ a dangerous legal precedent, setting the stage forexpanding this "right" to legal guardians of children andincompetent patients who are chronically or mentally ill.
VtlIf assisted suicide is considered an acceptable medicalreatment, some patients may feel unduly pressured to
end their lives as a way to relieve emotional or financialstrains on their families.
.\/ Asking physicians to help with suicide would forceV them to make subjective and inappropriate decisionsabout the quality of a patient's life.
\iFinancial pressures to ration healthcare would influ-v" ence decisions about providing treatment to dyingpatients. The ink on Oregon's 1994 law was barely drywhen regulators wrote niles limiting treatment for dying,low-income patients thought to have a low quality of life.
Strengthening our laws against physician-assisted sui-\ / cide would clarify society's intolerance for this practice.
Fr=ing/Above All, Sustain LifeCarlos F. Gomez, M.D., Regulating Death (New York:Free Press, 1991).
Herbert Hendin, M.D., Seduced by Death: Doctors,Patients, and the Dutch Cure (New York: W.W.Norton & Company, 1997).
Rita Marker, Deadly Compassion: The Death of AnnHumph?), and the Truth About Physician-Assisted Suicide
(New York: William Morrow and Company, 1993).
n Opposition
XGovernment should not force people to live whenthey suffer unbearable pain and are near death.
XThis choice would expand use of aggressive lifesavingtreatments in a costly and wasteful manner.
The purpose of medicine is to alleviate suffering andsometimes ending a life is the only way to do it.
' Physician-assisted suicide is now widely practiced inz-\\. secret, inviting error and abuse. We should legalize it
and regulate it.
IThere is no meaningful difference between providinga lethal drug to a dying patient and withdrawing life-
sustaining treatment from a dying patient, but only the latteris legal. _
-.,..-?; - Any risk from legalizing physician-assisted suicide is-7 \
1,-% \`-:, outweighed by the right to a humane death.
,i- If terminally ill patients obtain a right to physician-; ;A
::-- ''. assisted suicide, Choice Three worries that courtswould extend this right to other patients in circumstancesdeemed appropriate. Alarming? No, this is the way courtsrefine all our laws over time.
,Some people object to Dutch policies on physician-
;., assisted suicide, but there is no scientific basis forclaims that they have led to abuses, according to a 1996 edi-torial in the New England Journal of Medicine.
When 10 million children have no healthcarecoverage, the nation should not expand life-sustain-
ing treatments that are often futile and unwanted by dyingpatients.
10 AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMSNiculae Asciu

Renovating Public PolicyletaiM
he introduction of this issue book
presented the hypothetical case history
of Claire S., the cancer patient who saw no
point in continuing her painful downward
slide into death. Should society permit her
physician to assist in her suicide?
This once unthinkable question is nowdiscussed in legislatures, courts, and even a tele-vised beauty pageant. Americans are not onlyconsidering making suicide socially acceptable,they are also reconsidering the job descriptionfor physicians, rethinking ethical traditions ofmedicine that have evolved over 2,400 years.There is something very wrong with the Americanway of death, and to fix it, citizens are willing toconsider radical change. How would the threechoices presented in this issue book respondto Claire's plight?
Choice One would say society must preservelife, but should not deny Claire's right to ahumane death. Claire is near death, suffers fromloneliness and pain, and wants to die. Societyserves no interest in prolonging her misery. Acompassionate doctor might give Claire enoughmedication to kill herself but, fearful of legalconsequences, the doctor would likely act insecret. But if physician-assisted suicide waslegalized and regulated, as this choice proposes,medical professionals could evaluate Claire andhelp her one way or another through assistedsuicide or a new program of care.
Choice Two would say that if Claire is likemost suicidal patients, she suffers from depres-sion. She also suffers from severe pain, clearlyindicating that her physician has been inatten-tive. If comfort care was made widely available,as this choice proposes, Claire could obtainrelief from her physical and mental symptoms,and probably a social worker's help to improveher quality of life in other areas. Claire could
24
discontinue chemotherapy, which only prolongsher death. With Claire's consent, her physiciancould take strong measures to ensure that shedoesn't suffer unbearable pain, even though anoverdose of medication might unintentionallyshorten her life.
Choice Three would say society and physiciansshare a commitment to protecting Claire's life.A physician should never give up hope even ifthe patient does, at a low point in treatment.Her physician's responsibility is to continuetreating her cancer and symptoms until there isno further hope of preserving her life. If Clairedecides to discontinue chemotherapy and letthe cancer take its course, her physician mustaccept that decision. Yet studies suggest that 9out of 10 dying patients such as Claire, whoexperience considerable pain and suffering,agree to continue treatment.
In comparing the three approaches, it may helpto consider the following discussion points:
fs Can elements of the three choices becombined? Supporters of each choice findareas of agreement, but see the issue verydifferently and promote very different solutions.Choice One fights for a patient's right to physi-cian-assisted suicide and calls for legalizing thepractice. Choice Two argues that physician-assisted suicide isn't needed, and is discussedonly because the system of care for the dying isbroken and needs fixing. Choice Three defendsthe efforts of society and physicians to preserveall lives and opposes any exceptions as dangerous..
im What are some tradeoffs? Choice One,by having government regulate assisted suicide,would put the state in a new and controversialposition as arbiter of life and death. Choice Two,by giving patients much more say in determiningtheir care, could cause many premature deathswhen patient directives override sound medicaljudgment. Choice Three, by calling on physiciansto preserve all lives, could cause greater sufferingfor dying patients who would rather end theirlives quickly.
AT DEATI-I'S DOOR 0 NATIONAL ISSUES FORUMS 11

Renovating Public Policy
Comparing the Choices
edical technology has greatly extended
American lives, though patients' final days
or months are often spent on artificial life-support
systems. Death often follows a medical decision to
withdraw treatment. Some are demanding a larger
role for patients in making decisions about the time
and manner of their deaths. Do patients have a right
to a physician's assistance in committing suicide?
Lawmakers and jurists are wrestling with this
question, and they need to know what approach
Americans want to take.
22 AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS
Let Patients Die With Dignity
Patients dying in pain have a right to choose the time
and circumstances of their death. But society must
regulate this humane practice to prevent abuse.
What Can Be Done?
co Legalize physician-assisted suicide to give Americans
control over the way they die.
m Enact rules, including one that limits this practice to
terminally ill patients with unbear-able pain.
Swiftly prosecute physicians who violate these regulations.
In Support
m Society's interest in preserving
life must prevail, but not when
death is imminent and painis intolerable.
Many physicians secretly help
incurable patients end their
lives; regulating this practice
would reduce error and abuse.
m There is no meaningful difference between unplugging
a patient's ventilator and prescribing a lethal drug.
In Opposition
o When patients talk about suicide, they're desperatelyasking for care, not death.
o A right to die could easily become a duty to die,
especially for the elderly.
Some opponents say this choice doesn't go far enough;
physicians should help anyone in serious pain, not justthe terminally ill.
A Likely Tradeoff
By having government set eligibility rules, this choice
would put the state in a new and controversial position
as arbiterof life and death.
2 5
Ghoice
Improve Care for the Dying
GI Too many patients suffer from needless pain, depression,
and unwanted treatment. Let's fix the system and give
patients more control over their care.
What Can Be Done?
Allow dying patients to issue directives, not just prefer-
ences, about care and treatment.
Expand comfort care as well as insurance coverage for it.
Relieve pain with
high doses of medi-
cine, even though it
may unintentionally
cause death.
In Support
This choice calls for improving patients' quality of life,
not hastening their death.
Suicidal people usually suffer from depression or pain,
or both. These symptoms can be treated effectively.
Patients need legal authority to control their own care,
because caregivers routinely ignore their needs and
preferences for end-of-life treatment.
In Opposition
This choice promotes what is widely viewed as an
unregulated form of physician-assisted suicide: treating
patients with lethal doses of painkillers.
Some people prefer death to a life blurred by sedatives
and narcotics.
This choice oversimplifies the complexities of health-
care, especially for patients with unpredictable diseases.
A Likely Tradeoff
By giving patients much more say in their care, this
choice would cause premature deaths when patient
directives override sound medical judgment.
, 26
Renovating Public Policy
Above All, Sustain Life
Life is invaluable and should be inviolable, and society
and physicians must strengthen their commitment to
preserving life. Any retreat from this devalues life.
What Can Be Done?
Enact a federal ban on physician-assisted suicide.
Insist that physicians make every effort to sustain life
unless a patient declines treatment.
Respond to requests for physician-assisted suicide
with counseling and mental health treatment.
In Support
Suicide is a tragic, individual act. Legalizing assisted
suicide would make this tragedy the social norm.
Society cannot legalize assisted suicide without invit-
ing the kind of abuses that occur in the Netherlands,
where physician-assisted suicide is widely practiced.
Involving doctors in assisted suicide would further
weaken public confidence in the healthcare system.
In Opposition
Government should
not force people to live
when they want to die.
Any risk involved in
legalizing physician-
assisted suicide is outweighed by the right of
Americans to decide how they want to die.
Insisting on sustaining life even when patients are in
terrible pain would be inhumane.
A Likely TradeoffBy calling on physicians to preserve all lives, this
choice would cause suffering for dying patients who
would prefer to end their lives quickly.
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 23

What Are the National Issues Forums?
How to start a forumForums are initiated at thelocal level by civic andeducational organizations.For information aboutstarting a forum and usingour materials, write theNIF Institute, P.O. Box75306, Washington, D.C.20013-5306, or phone800-433-7834.
Mational Issues Forums bring together citizensaround the nation to discuss challenging
social and political issues of the day. They haveaddressed issues such as the economy, education,healthcare, foreign affairs, poverty, and crime.
Thousands of civic, service, and religiousorganizations, as well as libraries, high schools,and colleges, have sponsored forums. The spon-soring organizations select topics from amongeach year's most pressing public concerns, thendesign and coordinate their own forum programs,which are held through the fall, winter, and spring.
A different kind of discussionNo two forums are alike. They range from smallstudy circles to large gatherings modeled aftertown meetings, but all are different from every-day conversations and adversarial debates.
Since forums seek to increase understandingof complicated issues, participants need notstart out with a close knowledge of an issue.Forum organizers distribute issue books such asthis one, featuring a nonpartisan overviewof an issue and a choice of several publicresponses. By presenting each issue in anonpartisan way, forums encourage par-ticipants to take a fresh look at the issuesand at their own convictions.
In the forums, participants share theiropinions, their concerns, and their knowl-edge. With the help of moderators andthe issue books, participants weigh severalpossible ways for society to address a problem.They analyze each choice, the arguments for andagainst it, and the tradeoffs and other implicationsof the choice. Moderators encourage participants,as they gravitate to one option or another, toexamine their basic values as individuals and ascommunity members.
considered. This happens because the forumprocess helps people see issues from differentpoints of view; participants use discussion todiscover, not persuade or advocate. The bestdeliberative forums can help participants movetoward shared, stable, well-informed public
judgments about important issues.Participants may hold sharply different opin-
ions and beliefs, but in the forums they discusstheir attitudes, concerns, and convictions abouteach issue and, as a group, seek to resolve theirconflicting priorities and principles. In thisway, participants move from making individualchoices to making choices as members of acommunity the kind of choices from whichpublic action may result.
Building communitythrough public deliberationIn a democracy, citizens must come togetherto find answers they can all live with whileacknowledging that individuals have differing
opinions. Forums help people find theareas where their interests and goalsoverlap. This allows a public voice toemerge that can give direction topublic policy.
The forums are nonpartisan and donot advocate a particular solution to anypublic issue, nor should they be con-fused with referenda or public opinionpolls. Rather, the forums enable diverse
groups of Americans to determine together whatdirection they want policy to take, what kinds ofaction and legislation they favor, and what, fortheir common good, they oppose.
NATIISSUFOR
The common groundForums enrich participants' thinking on publicissues. Participants confront each issue head-on,make an informed decision about how to addressit, and come to terms with the likely consequencesof their choices. In this deliberative process,participants often accept choices that are notentirely consistent with their individual wishesand that impose costs they had not initially
14 AT DEATH'S DOOR ID NATIONAL ISSUES FORUMS
ONALESUMS
From agreement to actionForums can lead to several kinds of public action.Generally, a public voice emerges in the resultsof the forums, and that helps set the govern-ment's compass, since forum results are sharedwith elected officials each year. Also, as a resultof attending forums, individuals and groupsmay decide to take action individually or inassociation with others to help remedy a publicproblem, taking actions that citizens can takeoutside of government.
27

At Death's DoorWhat Are the Choices?One of the reasons people participate in the National Issues Forums is that they want leaders to know how they feel about the issues.So that we can present your thoughts and feelings about the issue, we'd like you to fill out this ballot before you attend forum meetings(or before you read this book, if you buy it elsewhere), and to fill out a second ballot after the forum (or after you've read the material).Before answering any of the questions, make up a three-digit number and write it in the box below.
The moderator of your local forum will ask you to hand in this ballot at the end of the session. If you are not attending a forum,send the completed ballot to the National Issues Forums, 100 Commons Road, Dayton, Ohio 45459-2777.
Fill in your three-digit number here.
1. Here is a list of principles on which policy on dying patients mightbe based. How important do you think each one should be?
a. Doctors should be allowed to help dying patients who choose to end theirlives with dignity.
b. Human life is invaluable, and should be preserved for as long as possible.
c. Doctors and hospitals should honor a dying patient's wish to refuse treatment.
d. Doctors should do all they can to ease the pain and suffering of dying patients,but nothing more.
e. Doctors should not be prosecuted if they help dying patients end their lives.
f. A doctor should do everything medically possible to save a patient's life,no matter how hopeless the patient seems.
Veryimportant
Somewhatimportant
Not at allimportant Not sure
0 0 0 00 0 0 00 0 0 0
0 0 0 00 0 0 0
2. Look at the list in Question #1 again. How strongly is each principle reflectedSomewhat
in current policy? Strongly strongly Not at all Not sure
a. Doctors should be allowed to help dying patients who choose to end theirlives with dignity. 0 0 El 0
b. Human life is invaluable, and should be preserved for as long as possible. 0 0 0 0c. Doctors and hospitals should honor a dying patient's wish to refuse treatment. El 0 0 El
d. Doctors should do all they can to ease the pain and suffering of dying patients,but nothing more. El El 0 0
e. Doctors should not be prosecuted if they help dying patients end their lives. 0 0 0 El
f. A doctor should do everything medically possible to save a patient's life,no matter how hopeless the patient seems.
3. Are there other principles that you think should guide policy in this area? Please explain.
4. How concerned are you about the following?
a. Dying patients who are forced to endure needless pain and suffering.
b. Patients who say they want to die but really need treatment for pain and depression.
c. Doctors who violate their oath to preserve life, by helping patients commit suicide.
d. Patients who choose to end their own lives to reduce medical expensestheir families must pay.
e. Doctors and hospitals that disregard patients' wishes to withhold treatment.
f. The huge financial costs to society of keeping dying patients alive.
2R
Very Somewhat Not at all Notconcerned concerned concerned sure
00 0 0 0
0 0 0 00 0 0 0Li 0 0 Li
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 25

5. Do you have any other concerns about public policy in this area? Please explain.
6. How do you feel about these approaches to the problem? Favor Oppose Not sure
a. We should legalize and regulate doctor-assisted suicide, EVEN IF this contradictsthe idea of the doctor as healer. 0 LI 0
b. We should give dying patients more control over their treatment, EVEN IF theirwishes might override sound medical judgment and lead to premature death. LI LI CI
c. We should maintain the current ban on doctor-assisted suicide, EVEN IF thismeans some terminally ill patients will endure needless pain and suffering.
7. Which statement best describes how you feel? (Please choose only one answer.)
a. I am not at all certain what our public policy should be regarding assisted suicide. CI
b. I have a general sense of what our policy should be. LI
c. I have a clear, definite view of what our policy should be. CI
8. Are you male or female? 0 Male CI Female
9. How much schooling have you completed?
CI Less than 6th grade
CI Some college
10. Are you:
LI White
O 6th-8th grade
O College graduate
10 Some high school
0 Graduate school
CI High school graduate
O African-American CI Hispanic 0 Asian-American CI Other (specify)
11. How old are you?
CI 17 or younger 0 18-29 0 30-49 111 50-64
12. Have you attended an NIF forum before? CI Yes El No
13. If you answered "yes" to #12, how many forums have you attended? 0 1-3
14. Do you live in the:
0 NortheastCI Southwest
El South
CI Other
15. What is your ZIP code?
16 AT DEATH'S DOOR Q NATIONAL ISSUES FORUMS
0 Midwest CI West
29
CI 65 or older
111 4 or more

.11.31.....1.111111.u.fgama
At Death's DoorWhat Are the Choices?Now that you've had a chance to read the book or attend a forum discussion, we'd like to know what you think about this issue. Youropinions, along with those of thousands of others who participated in this year's forums, will be reflected in a summary report preparedfor participants as well as elected officials and policymakers working on this problem. Since we're interested in whether you havechanged your mind about certain aspects of this issue, the questions are the same as those you answered earlier. Before answering thequestions, please write in the box below the same three-digit number you used for the Pre-Forum Ballot.
Please hand this ballot to the forum leader at the end of the session, or mail it to: The National Issues Forums, 100 Commons Road,Dayton, Ohio 45459-2777.
Fill in your three-digit number here.
1. Here is a list of principles on which policy on dying patients might be based.How important do you think each one should be?a. Doctors should be allowed to help dying patients who choose to end their
lives with dignity. CI CI 0 CI
b. Human life is invaluable, and should be preserved for as long as possible. CI 0 CI CI
c. Doctors and hospitals should honor a dying patient's wish to refuse treatment. 0 0 CI 0d. Doctors should do all they can to ease the pain and suffering of dying patients,
but nothing more. 0 0 0 0e. Doctors should not be prosecuted if they help dying patients end their lives. 0 CI CI 0
Very Somewhat Not at allimportant important important Not sure
f. A doctor should do everything medically possible to save a patient's life,no matter how hopeless the patient seems.
2. Look at the list in Question #1 again. How strongly is each principle reflectedSomewhat
in current policy? Strongly strongly Not at all Not sure
a. Doctors should be allowed to help dying patients who choose to end theirlives with dignity. CI 0 CI 0
b. Human life is invaluable, and should be preserved for as long as possible. CI 0 0 0c. Doctors and hospitals should honor a dying patient's wish to refuse treatment. 0 CI 0 CI
d. Doctors should do all they can to ease the pain and suffering of dying patients,but nothing more. 0 CI CI 0
e. Doctors should not be prosecuted if they help dying patients end their lives. CI 10 CI 0f. A doctor should do everything medically possible to save a patient's life,
no matter how hopeless the patient seems.
3. Are there other principles that you think should guide policy in this area? Please explain.
4. How concerned are you about the following?
a. Dying patients who are forced to endure needless pain and suffering.
b. Patients who say they want to die but really need treatment for pain and depression.
c. Doctors who violate their oath to preserve life, by helping patients commit suicide.
d. Patients who choose to end their lives to reduce medical expensestheir families must pay.
e. Doctors and hospitals that disregard patients' wishes to withhold treatment.
f. The huge financial costs to society cif, keeping dying patients alive.
3 0
Very Somewhat Not at all Notconcerned concerned concerned sure
0 CI CI CI
0 CI 0 00 CI CI 0
CI 0 CI CI
0 CI CI CI
AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS 17
Post- orum Ballot
5. Do you have any other concerns about public policy in this area? Please explain.
6. How do you feel about these approaches to the problem?
a. We should legalize and regulate doctor-assisted suicide, EVEN IF thiscontradicts the idea of the doctor as healer.
b. We should give dying patients more control over their treatment, EVEN IF theirwishes might override sound medical judgment and lead to premature death.
c. We should maintain the current ban on doctor-assisted suicide, EVEN IF thismeans some terminally ill patients will endure needless pain and suffering.
7. Which statement best describes how you feel? (Please choose only one answer.)
a. I am not at all certain what our public policy should be regarding assisted suicide.
b. I have a general sense of what our policy should be.
c. I have a clear, definite view of what our policy should be.
Favor Oppose Not sure
0 ID iii
El 0 0
111 0 0
000
8. If you answered "c" to Question #7, please explain below what you think our public policy should be.
9. What is your ZIP code?
31
18 AT DEATH'S DOOR 0 NATIONAL ISSUES FORUMS

For the National Issues Forums
Issue books in this series arc prepared by Public Agenda in collaboration \ vith the Kettering Foundation.
Public Agenda
Public Agenda was founded in 1975 by public opinion analyst Daniel Yankelovich and former U.S. Secretary of'
State Cvnis R. Vance. A not [profit. nonpartisan research and education organization based in New York. Public
Agenda lias created mid poiduced issue books in this series sit ice 1982. Its researcli on how citizetts approacli
public issues provides the basis fOr main- innovative educational projects. For more infOrmation. contact Public
Agenda at 6 East :39tli Street. New York. New York 10016. Pholie: 212-686-6610.
Kettering FoundationThe Kettering Foundation. a nonprofit. nonpartisan research institute based in Dayton. Ohio (witli oflices in
Washington. D.C.. and New York) was fimicled in 1927. It has provided books. materials . and moderator train-ing fOr the National Issues Forums since this nationwide network was started in 1982. It is engaged in a wide
range of activities to promote civic participation and enrich public life. For informatioliabout die Kettering
Foinidation. contact the fOundation at 200 Commons Road.- Dayton. Ohio 45459-2799. Phone: 800-221-3657.
Additional CopiesThis issue book is pubhshed by Kendall/11111u PublislMtg Co. This series of issue books covers such topics as
civil justice. Social Security and Nledicare. America's global role. die family. income ineclitality. immigratiomt .
juvenile cii ne. healthcare refOrni, and the public debt. For infiirmation and phone orders. contact Kendal1/1-1 tint.
4050 Westmark Drive. Dubuque. Iowa 52002. Phone: 800-228-0810.
Acknowledgments'Mc editors would like to thank their ci dleagues at Public Agenda and the Kettering Foulidation who helped
define the choice framework and clarify die presentatioir Ed Arnone. Jon Kinghorn. Bob Kingston. and Estus
StMtli at Kettering: and Jean Johnson. Keith chine. and Deborah Wadsworth at Public Agenda. We also appre-
ciate the encouragement and support of Dan Yankelovich. president of Public Agenda, and David Matliews. pres-
ident of the Kettering Foundatitni.
Reviewers
Special thanks to die consultants who reviewed this manuscript: jay E. Kantor. ethicist. New York University
Medical Center; Dr. Russell K. Portenov. Co-Chiel; Pain and Palliative Care Service. Memorial Sloati-Kettering
Cancer Center. New York: Barbara Coombs Lee. Interim Executive Director; Compassion in Dving;Dr. Stephen R. Latham. Deputy Head. Institute fi)r Ethics at the American Medical Association.
At Public Agenda
Project Director: Michael deCourcy Hinds
Writer: Michael deCourcy Hinds
Issues Research: Nancy Beiles. Can dine Corbin
Opinion Research: Steve Farkas
Copy Editor: Ilana Ruin
Design and Graphics
Design: Sundberg K: Associates Inc
Graphics Research: Nancy liciles
Cover illustration: Ju ihn Lytle
Inside Illustrations: Niculae Ascitt
At the Kettering FoundationPublisher: Edward J. Arnone
Production Manager: George Cavanaugh
Doble. Ilse Tebbetts
Circulation Coordinator: Victoria Simpson
At Deaths Door:
What Are die Choices?
Copyright 1997 by National Issues Forums Instituteand Public Agenda
All rights reserved
ISBN: 0-7872-3913-1
BEST COPY AVAILABLE

CI
,
KENDALL/HUNT PUBLISHING COMPANYDubuque, Iowa
9
ISBN 0-7872-3915-1
7 07 7 239152
90000
BEST COPY AVAILABLE

(9/92)
U.S. DEPARTMENT OF EDUCATIONOffice of Educational Research and Improvement (OERI)
Educational Resources Information Center (ERIC)
NOTICE
REPRODUCTION BASIS
ERIC
This document is covered by a signed "Reproduction Release(Blanket)" form (on file within the ERIC system), encompassing allor classes of documents from its source organization and, therefore,does not require a "Specific Document" Release form.
This document is Federally-funded, or carries its own permission toreproduce, or is otherwise in the public domain and, therefore, maybe reproduced by ERIC without a signed Reproduction Releaseform (either "Specific Document" or "Blanket").