4 16 14 vascular disease and respiratory failure small group cases %5bcompatibility mode%5d
TRANSCRIPT
4/14/2014
1
Vascular Disease And Respiratory Failure Case
TutorialsCases and Notes Compiled by
James Allen MD
Case #1
• History: 20 yr old Caucasian woman with acute dyspnea, pleuritic chest pain, and hemoptysis
• PMH: recently started birth control pills• SH: OSU student; non-smoker• FH: father had “phlebitis” after hip surgery• Exam: HR = 122, RR = 24, BP = 92/60,
lungs clear to auscultation
Case #1: ABG
pH 7.50
PCO2 25
PO2 55
HCO3 21
SaO2 90%

4/14/2014
2
Case #1: PFTs
FVC 3.27 liters 100%
FEV1 2.75 liters 100%
FEV1/FVC 92%
TLC 4.98 liters 100%
DLCO 12.3 ml/min/mm 52%
Case #1: Chest X-ray
Case #1: Discussion
• What is the differential diagnosis?
• How would you confirm the diagnosis?
• What are the likely contributing causes of this disease?
• How would you treat her?
• What would you advise her to do regarding future contraception?

4/14/2014
3
Pulmonary Embolus: Chest CT

4/14/2014
4
Pulmonary Embolus: Ventilation/Perfusion (V/Q) scan
Ventilation Perfusion
Pulmonary Embolus: Pulmonary Angiogram
Pulmonary Embolus: Pathology

4/14/2014
5
Pulmonary Infarction: Pathology
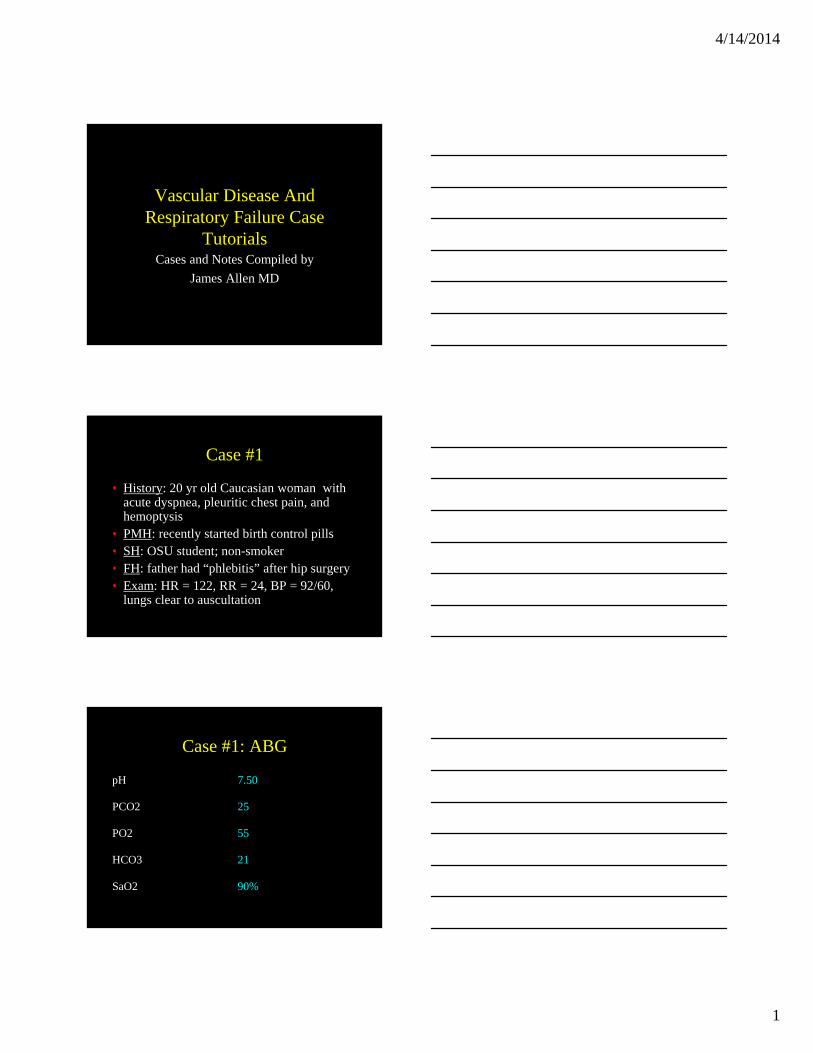
Pulmonary Embolus: Pathology
Pulmonary Embolus
4/14/2014
6
Older Pulmonary Embolus
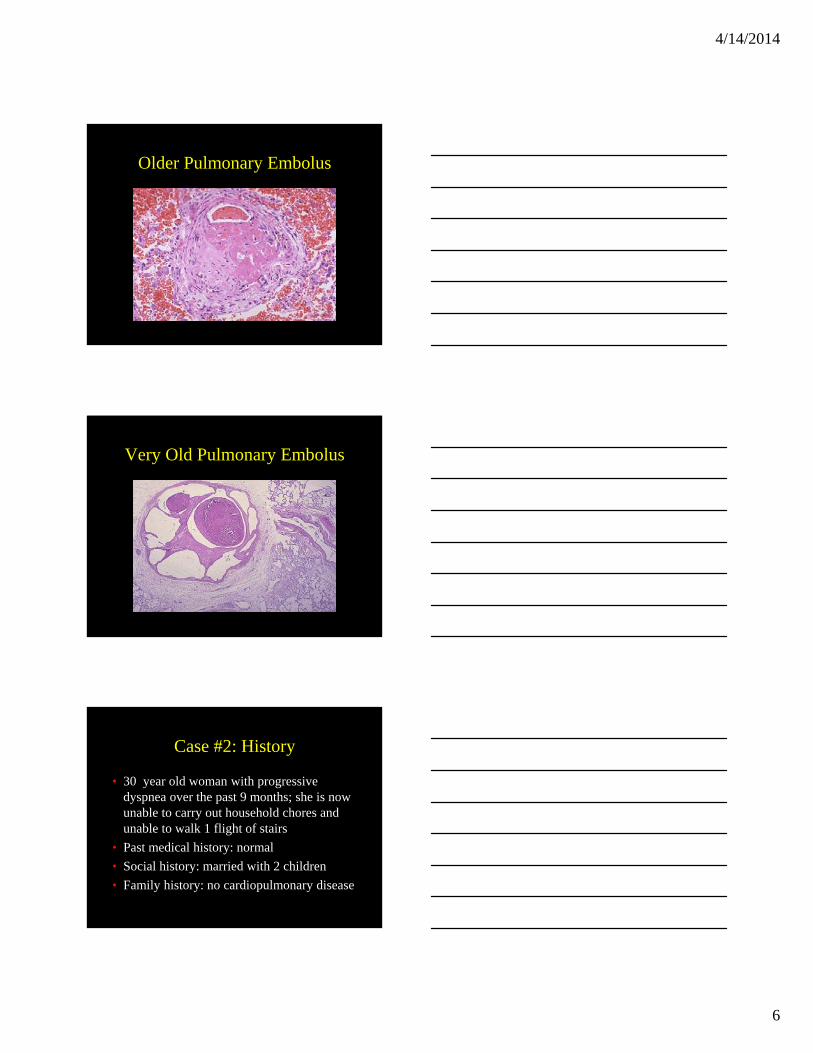
Very Old Pulmonary Embolus
Case #2: History
• 30 year old woman with progressive dyspnea over the past 9 months; she is now unable to carry out household chores and unable to walk 1 flight of stairs
• Past medical history: normal
• Social history: married with 2 children
• Family history: no cardiopulmonary disease

4/14/2014
7
Case #2: Physical Exam
• Vital signs:– 225 pounds– HR 78– BP 130/79– RR 18
• Lungs clear to auscultation• 1/VI systolic murmur, loud pulmonic component
of the second heart sound, elevated jugular venous pressure
• Mild pedal edema
Case #2: Chest x-ray
Case #2: Chest x-ray
29 cm
18 cm

4/14/2014
8
Case #2: PFTs
• FVC 2.95 L (79%)
• FEV1 2.37 L (75%)
• FEV1/FVC 80%
• TLC 4.97 L (90%)
• Diffusing capacity 16.5 (66%)
• 6 minute walk: SaO2 98% at rest and 91% while walking
Discussion Questions
• What does her physical examination suggest?
• How do you interpret the chest x-ray?
• How do you interpret the PFTs?
• What is the significance of the 6 minute walk results?
• What additional studies would you order?
Case #2: Cardiac Echo
• Normal left ventricle
• Dilated, hypokinetic right ventricle
• Dilated pulmonary arteries
• No evidence of intracardiac shunt

4/14/2014
9
Case #2: Right Heart Catheterization
• Before iNO:– PA = 101/43
– Mean PA = 65
– PCWP = 7
– CO = 4.7
– CI = 2.3
• After iNO:– PA = 88/42
– Mean PA = 56
– PCWP = 7
– CO = 4.9
– CI = 2.6
Discussion Questions:
• What is the diagnosis?
• What is the prognosis?
• How would you treat her?
Case #3: History
• 45 year old caucasian man with shortness of breath worsening over the past 3 years.
• Past medical history: scleroderma
• Social history: disabled engineer; married with 2 children; non-smoker

4/14/2014
10
Case #3: Physical Exam
• Vital signs:– HR 104– RR 18– BP 132/72
• Lungs clear to auscultation• Heart = tachycardic but regular; loud P2;
elevated jugular venous pressure; II/VI systolic murmur at right sternal border
Case #3: Chest x-ray
Discussion Questions
• What are the pulmonary complications of scleroderma?
• Which one is most likely in this case?• What additional tests could you do to
confirm your clinical suspicion?• What physical examination findings support
this diagnosis?• What would a cardiac echo show?

4/14/2014
11
Case #3: Right Heart Cath
• Pulmonary artery pressure = 97/41 (mean = 50)
• Pulmonary capillary wedge pressure = 8
• Cardiac output = 3.6
• Cardiac index = 1.8
Case #3: Pathology
Case #3: Pathology

4/14/2014
12
Discussion Questions
• How would you treat him?
• Why is a pulmonary capillary wedge pressure important to measure when evaluating pulmonary hypertension?
Case #4
• 51 year old man with new onset seizures and status epilepticus
• Persistent seizures despite Dilantin, phenobarbital, and Propofol
• Intubated and started on pentobarbital drip for pentobarbital coma
• He developed pneumonia after 1 week that improved with antibiotics
Case #4 (continued)
• After 2 weeks, he continues to have seizures when the pentobarbital is held. He remains comatose on a ventilator.
• On rounds, you note that he has developed hypoxemia resulting in an increase in his inhaled oxygen concentration from 30% to 100%
• On exam, he has new swelling of the right leg

4/14/2014
13
Case #4 (continued)
• What is the most likely diagnosis?
• What test could you do to prove this diagnosis?

4/14/2014
14
Image courtesy of GE Healthcare; used with permission
Image courtesy of GE Healthcare; used with permission
Image courtesy of GE Healthcare; used with permission

4/14/2014
15
Image courtesy of GE Healthcare; used with permission
Case #4 (continued)
• What is this patient’s risk factor(s) for this condition?
• What could have been done to prevent it?
• What other tests could have been used in the diagnosis of this condition?
Case #5
• History: 44 yr old African American woman admitted with diverticulitis. 6 days after admission, she is febrile and dyspneic
• PMH: non-insulin dependent diabetes; prior MI• SH: non-smoker• FH: diabetes• Exam (day 6): temp 102, RR = 32, HR = 136, BP
= 74/52; severe respiratory distress; lungs clear to auscultation

4/14/2014
16
Case #5: ABGs (on 100% supplemental oxygen face mask)
pH 7.24
PCO2 25
PO2 52
HCO3 12 (anion gap = 22)
SaO2 85%
Case #5: Chest X-rays
Admission Hospital Day #6
Case #5: Chest CT

4/14/2014
17
Case #5: Additional Tests
• Cardiac echo: LV ejection fraction = 42%
• Pulmonary artery catheter (Swan-Ganz): pulmonary capillary wedge pressure = 10 mm Hg
• Blood cultures: E. coli
Case #5: Discussion
• What are the possible causes of her pulmonary infiltrates and hypoxemia?
• How do you know if this is acute respiratory distress syndrome (ARDS) vs. heart failure?
• How should she be managed immediately?
ARDS pathology

4/14/2014
18
Case #6: History
• 19 year old man with increasing confusion and morning headaches
• Past medical history: Duchenne’s muscular dystrophy; no surgery, no current medications
• Social history: disabled after high school
• Family history: first degree relatives healthy
Case #6: History
• Review of systems: wheelchair bound; some difficulty swallowing; requires assistance with activities of daily living
Case #6: Physical Exam
• Vital signs:– Afebrile– RR = 16– HR = 102– BP = 100/68
• Diffuse muscle atrophy• Lungs clear to auscultation but both
diaphragms elevated to percussion

4/14/2014
19
Case #6: Chest x-ray
Case #6: PFTs
• FVC 1.76 L (52%)
• FEV1 1.48 L (56%
• FEV1/FVC 84%
• TLC 3.54 L (60%)
• Diffusing capacity 24 (120%)
Case #6: ABG
• pH 7.30
• PO2 62
• PCO2 68
• HCO3 35
• SaO2 91%

4/14/2014
20
Discussion Questions
• Is this hypercarbic or hypoxemic respiratory failure?
• What is the cause of his respiratory failure?
• What is the cause of his confusion?
• How would you treat him?
• What is the prognosis?
Case #7: History
• 60 year old woman with cough and increasing dyspnea for 2 weeks. Her family physician started oral steroids and antibiotics 4 days ago (for presumed exacerbation of COPD) with no benefit yet. For the past 24 hours, she has become much more short of breath
• Past medical history: – Illnesses: emphysema– Surgery: cholecystectomy 10 years ago
Case #7: History
• Medications:– Atrovent (inhaled bronchodilator)
– Serevent (inhaled bronchodilator)
– Prednisone 40 mg/day (oral steroid)
– Doxycycline (oral antibiotic)
• Social history: 60 pack year smoker - still smokes; real estate agent; divorced

4/14/2014
21
Case #7: History
• Family history: mother died of myocardial infarction; father died of stroke
• Review of systems: cough productive of yellow sputum; unable to climb one flight of stairs
Case #7: Physical Exam
• Vital signs:– Afebrile– RR = 32– HR = 112– BP = 134/80
• Severe respiratory distress; only able to speak 2-3 words per breath
• Lungs - barely audible breath sounds; prolonged expiratory phase of respiration
Case #7: Chest x-ray

4/14/2014
22
Case #7: ABG
• Room Air:– pH 7.18
– PO2 52
– PCO2 74
– HCO3 28
– SaO2 85%
• 60% oxygen:– pH 7.12
– PO2 72
– PCO2 80
– HCO3 29
– SaO2 92%
Discussion Questions
• Is the main problem acute hypoxemic or hypercarbic respiratory failure?
• What is the cause of her respiratory failure?
• How would you treat her respiratory failure?
Case #7: Follow-up
• After you successfully manage her in the hospital, her acute illness has resolved and she follows up in your office 2 months later
• Although her dyspnea has improved, she can only walk one flight of steps and is unable to return to work as a realtor because of limiting dyspnea when showing houses

4/14/2014
23
Case #7: Outpatient ABG
• Room Air:– pH 7.38– PO2 52– PCO2 42– HCO3 25– SaO2 87%
• SaO2 while walking in the clinic hallway = 78%
Discussion Questions
• Is her chronic respiratory failure hypercarbic or hypoxemic?
• How would you treat her?