43-338-1-pb
DESCRIPTION
sTRANSCRIPT

İzmir Üniversitesi Tıp Dergisi İzm Üniv Tıp Derg 2014; 2:32-34 Izmir University Medical Journal Izm Univ Med J 2014; 2:32-34
32
CA
SE REP
OR
T
OLG
U SU
NU
MU
Giant kidney tumor: Radiological case report
Dev böbrek tümörü: Radyolojik olgu sunumu
Abstract A 74-year-old man admitted to hospital with abdominal pain and gastrointestinal symptoms. Physical examination was normal except for a large, solid mass lacalized in the right upper quadrant and extending to right lower quadrant. Computed tomography exam revealed a giant kidney tumor; filling right half of the abdominal cavity. In this present case report, we described how the abdominal structures were affected due to this retroperitoneal giant kidney mass. Key words: Abdominal mass, anatomy, kidney tumor. Özet 74 yaşında bir erkek, karın ağrısı ve gastrointestinal sistem belirtileri ile hastaneye başvurdu. Fizik muayene, sağ üst kadranda yerleşmiş ve sağ alt kadrana doğru uzanan büyük, solid kitle dışında normaldi. Bilgisayarlı tomografide, karın boşluğunun sağ yarısını dolduran ve abdominal dev bir böbrek tümörü izlendi. Bu olgu sunumunda, retroperitoneal dev böbrek tümörünün abdominal yapıları nasıl etkilediğini tanımladık. Anahtar kelimeler: Abdominal kitle, anatomi, böbrek tümörü.
Introduction
An abdominal mass is a swelling which
localized in abdomen, and usually detected
during routine physical examination. In
general, abdominal masses develop slowly.
Therefore, patients may have no symptoms
until the mass enlarges and pressurizes on
neighboring anatomical structures (1).
Depending on its’ size, an abdominal mass
may cause change in the shape of the
abdomen (2). Symptoms of abdominal masses
may include abdominal tenderness, pain and
functional disturbances.
The abdomen is divided into four quadrants;
right upper, right lower, left upper and left
lower. Right and left kidneys are located in the
right upper and left upper quadrants,
respectively. Therefore, an abdominal mass
may occur originating from kidney cancer (3).
Papillary renal cell carcinoma (PRCC) is the
second most common histologic type of
kidney cancer (4).
We aimed to present a giant abdominal mass,
originated from the right kidney (PRCC), which
pressurizes on the neighboring anatomical
structures and further changes the anatomical
localization of the abdominal contents.
Case Report
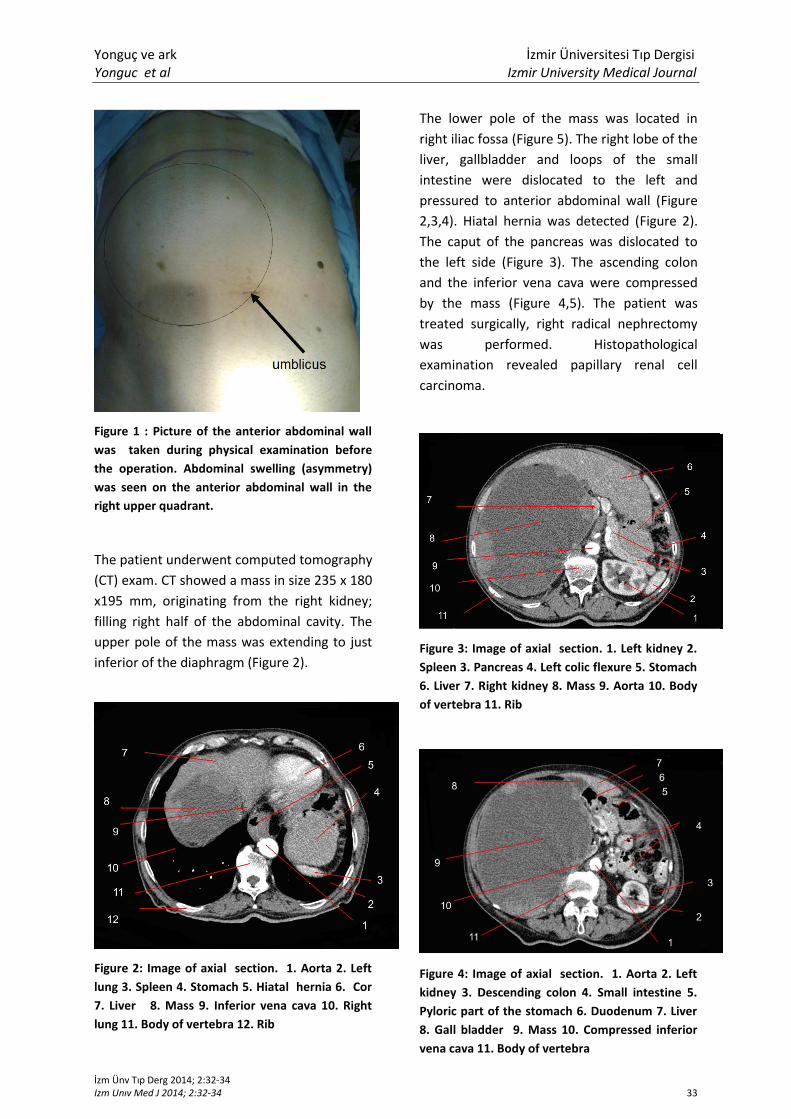
A 74-year-old man presented with a 3-weeks
history of abdominal pain and gastrointestinal
symptoms. In physical examination, a large-
solid mass extending to the right lower
quadrant was detected in the right upper
quadrant (Figure 1).
Gökşin Nilüfer Yonguç1,
Savaş Şahinli2, Esat Adıgüzel
3, Mehmet Bülent Özdemir
3, Şahika Pınar Akyer
3
1Izmir University, Faculty of Medicine, Department of Anatomy, Denizli, Turkey
2Denizli State Hospital, Department of Urology, Denizli, Turkey
3Pamukkale University, Faculty of Medicine, Department of Anatomy, Denizli, Turkey
Sorumlu Yazar/Corresponding Author: Gökşin Nilüfer Yonguç Izmir University, Faculty of Medicine, Department of Anatomy, Denizli, Turkey e-posta: [email protected]
Geliş Tarihi/Received: 15.04.2014 - Kabul Tarihi/Accepted: 07.05.2014
Yonguç ve ark İzmir Üniversitesi Tıp Dergisi Yonguc et al Izmir University Medical Journal
İzm Ünv Tıp Derg 2014; 2:32-34 Izm Unıv Med J 2014; 2:32-34 33
Figure 1 : Picture of the anterior abdominal wall
was taken during physical examination before
the operation. Abdominal swelling (asymmetry)
was seen on the anterior abdominal wall in the
right upper quadrant.
The patient underwent computed tomography
(CT) exam. CT showed a mass in size 235 x 180
x195 mm, originating from the right kidney;
filling right half of the abdominal cavity. The
upper pole of the mass was extending to just
inferior of the diaphragm (Figure 2).
Figure 2: Image of axial section. 1. Aorta 2. Left
lung 3. Spleen 4. Stomach 5. Hiatal hernia 6. Cor
7. Liver 8. Mass 9. Inferior vena cava 10. Right
lung 11. Body of vertebra 12. Rib
The lower pole of the mass was located in
right iliac fossa (Figure 5). The right lobe of the
liver, gallbladder and loops of the small
intestine were dislocated to the left and
pressured to anterior abdominal wall (Figure
2,3,4). Hiatal hernia was detected (Figure 2).
The caput of the pancreas was dislocated to
the left side (Figure 3). The ascending colon
and the inferior vena cava were compressed
by the mass (Figure 4,5). The patient was
treated surgically, right radical nephrectomy
was performed. Histopathological
examination revealed papillary renal cell
carcinoma.
Figure 3: Image of axial section. 1. Left kidney 2.
Spleen 3. Pancreas 4. Left colic flexure 5. Stomach
6. Liver 7. Right kidney 8. Mass 9. Aorta 10. Body
of vertebra 11. Rib
Figure 4: Image of axial section. 1. Aorta 2. Left
kidney 3. Descending colon 4. Small intestine 5.
Pyloric part of the stomach 6. Duodenum 7. Liver
8. Gall bladder 9. Mass 10. Compressed inferior
vena cava 11. Body of vertebra

Yonguç ve ark İzmir Üniversitesi Tıp Dergisi Yonguc et al Izmir University Medical Journal
İzm Ünv Tıp Derg 2014; 2:32-34 Izm Unıv Med J 2014; 2:32-34 34
Figure 5: Image of axial section. 1. Psoas muscle
2. Two common iliac arteries 3. Small intestine 4.
Transverse colon 5. Mass 6. Compressed
ascending colon 7. Inferior vena cava 8. Ilium 9.
Body of vertebra
Discussion
Kidneys are retroperitoneally located lateral to
the vertebral coloumn. They are bean-shaped
and lie in the extraperitoneal connective
tissue of the posterior abdominal region (5).
Our case presented a giant abdominal mass,
caused by PRCC of kidney, with uncommon
clinical condition of filling the right half of the
abdominal cavity; pressurizing and dislocating
abdominal structures.
Papillary renal cell carcinoma (PRCC) is the
second most common histopathologic type of
kidney cancer, and exhibits a large range of
morphologic variants (4,6). Although, PRCC is
one of the common type of kidney cancer,
there is no any case of giant PRCC that leads
dislocation of abdominal structures in the
literature. On the other hand, Taneja and
Singh (7) report a female case of giant renal
angiomyolipoma of the left kidney displacing
the rest of the abdominal contents toward the
other side of the midline. In this
aforementioned case, mass is originited from
left kidney and filling the left abdominal
cavity, hence the abdominal content was
remowed to the right abdominal cavity.
Similarly, Akbulut et al. (8) report a female
case of giant left renal oncocytoma. However,
in these studies, dislocation of anatomical
contents are not explained.
As a conclusion, most of abdominal masses
are determined incidentally during routine
physical examinations. During physical
examination, the clinician must determine the
location of the mass, and describe well its
location (in terms of quadrants). Also clinicians
should be aware of how giant masses can
dislocate the anatomical structures while
performing manipulations.
References
1.http://alexianbrothershealth.adam.com/con
tent.aspx?productId=117&pid=1&gid=003274.
Retrieved July 26, 2014.
2.http://www.healthline.com/symptom/abdo
minal-mass. Retrieved July 26, 2014.
3.https://www.inkling.com/read/hunt-
marshalls-clinical-problems-surgery-smith-
2nd/chapter-7/7-9-abdominal-mass. Retrieved
July 26, 2014.
4.Twardowski PW, Mack PC, Lara PN Jr.
Papillary renal cell carcinoma: current
progress and future directions. Clin Genitourin
Cancer 2014; 12(2):74-79.
5.Drake RL, Vogl W, Mitchell AWM. Gray’s
Anatomy for Students, 2nd edition. Churchill
Livingstone, Elsevier, 2009.
6.Patard JJ, Leray E, Rioux-Leclercq N, Cindolo
L, Ficarra V, Zisman A, De La Taille A, Tostain J,
Artibani W, Abbou CC, Lobel B, Guillé F,
Chopin DK, Mulders PF, Wood CG, Swanson
DA, Figlin RA, Belldegrun AS, Pantuck AJ.
Prognostic value of histologic subtypes in
renal cell carcinoma: a multicenter
experience. J Clin Oncol. 2005; 23:2763–2771.
7.Taneja R, Singh DV. Giant Renal
Angiomyolipoma: Unusual Cause of Huge
Abdominal Mass. J Clin Imaging Sci. 2013; 3:56
8.Akbulut S, Senol A, Cakabay B, Sezgin A.
Giant renal oncocytoma: a case report and
review of the literature. J Med Case Rep.
2010; 4:52.