49 alveolar lung disease on computed tomography
TRANSCRIPT

49 Alveolar Lung Disease on Computed Tomography*
CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
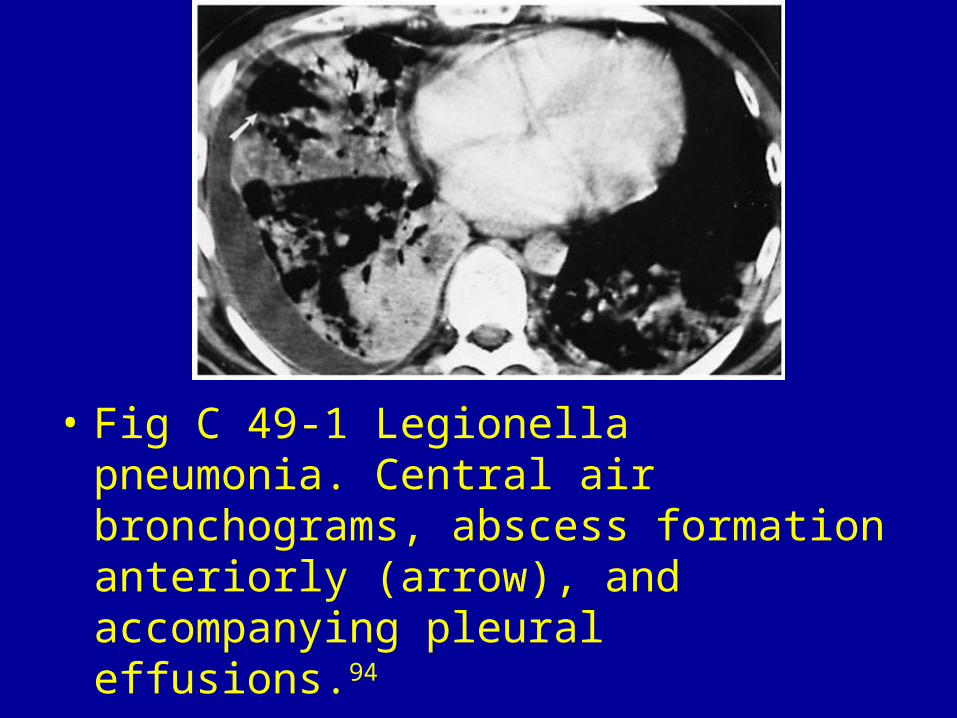
• Fig C 49-1 Legionella pneumonia. Central air bronchograms, abscess formation anteriorly (arrow), and accompanying pleural effusions.94

• Fig C 49-2 Tuberculous pneumonia. Air bronchograms and accompanying hilar lymphadenopathy. (Courtesy of Junpei Ikezoe, MD.)94
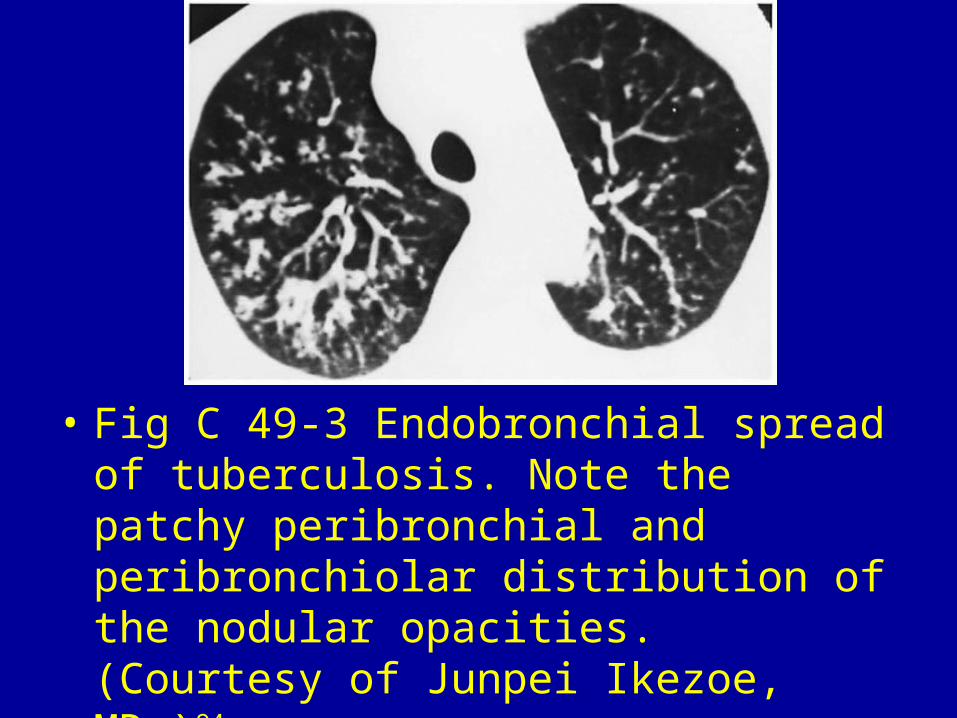
• Fig C 49-3 Endobronchial spread of tuberculosis. Note the patchy peribronchial and peribronchiolar distribution of the nodular opacities. (Courtesy of Junpei Ikezoe, MD.)94
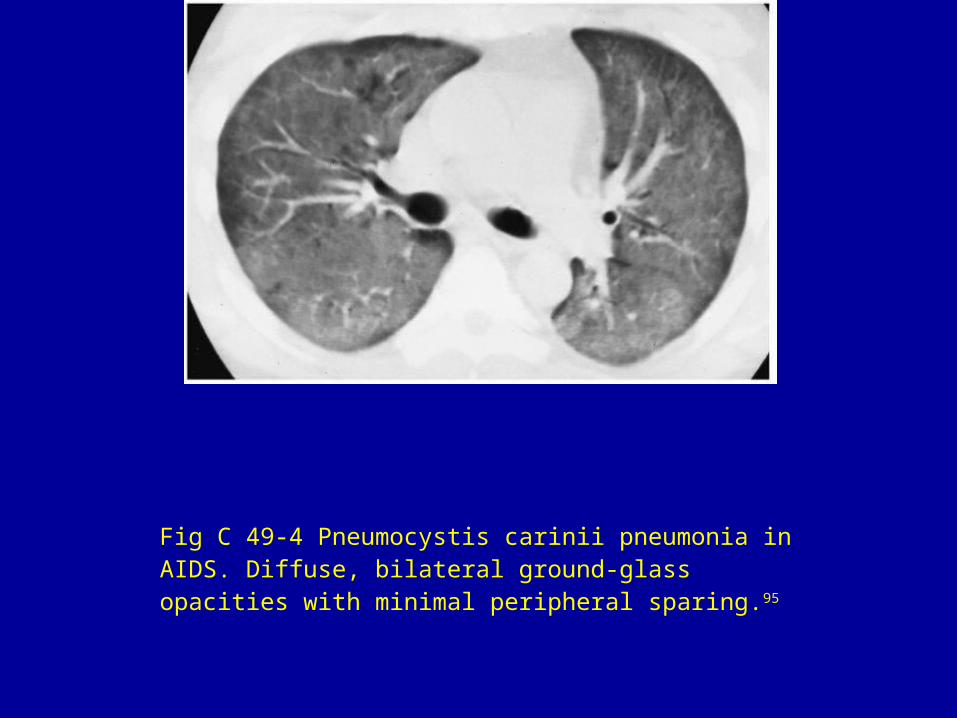
Fig C 49-4 Pneumocystis carinii pneumonia in AIDS. Diffuse, bilateral ground-glass opacities with minimal peripheral sparing.95
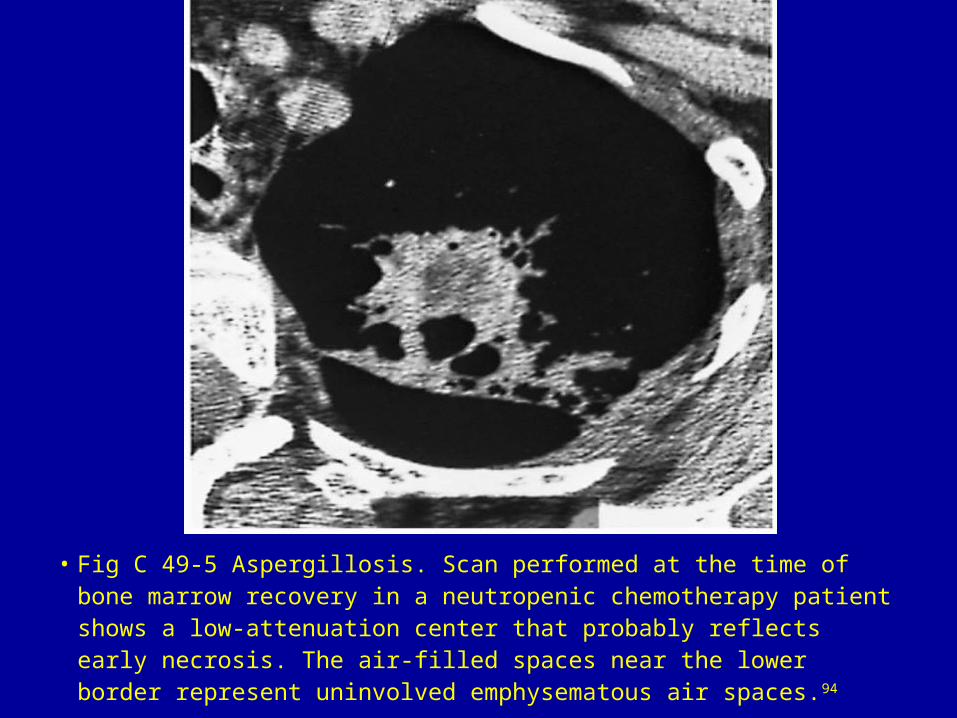
• Fig C 49-5 Aspergillosis. Scan performed at the time of bone marrow recovery in a neutropenic chemotherapy patient shows a low-attenuation center that probably reflects early necrosis. The air-filled spaces near the lower border represent uninvolved emphysematous air spaces.94
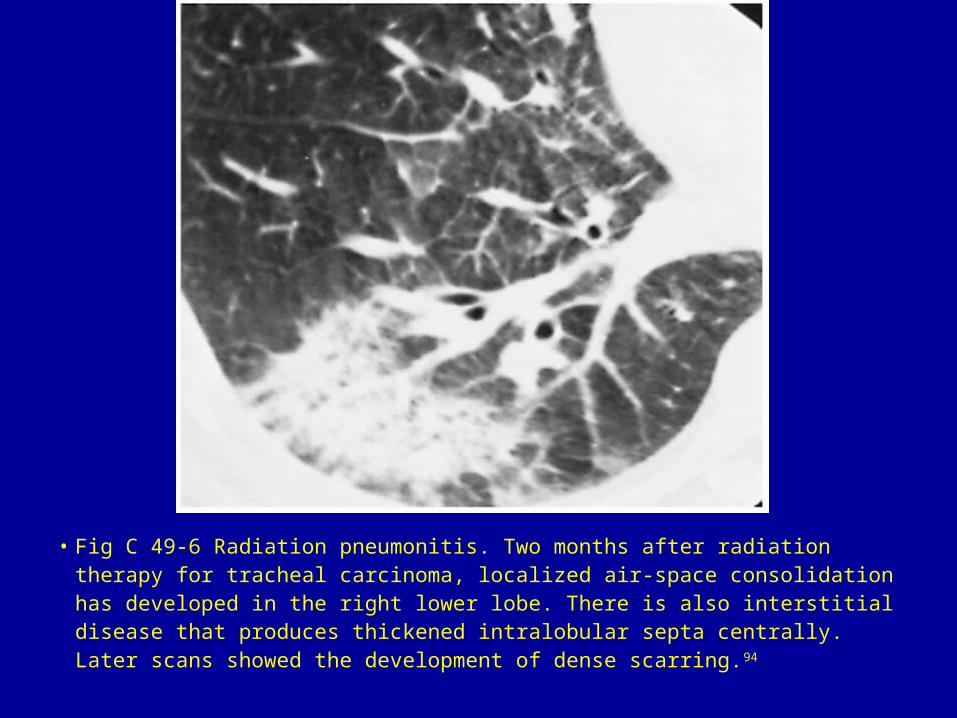
• Fig C 49-6 Radiation pneumonitis. Two months after radiation therapy for tracheal carcinoma, localized air-space consolidation has developed in the right lower lobe. There is also interstitial disease that produces thickened intralobular septa centrally. Later scans showed the development of dense scarring.94
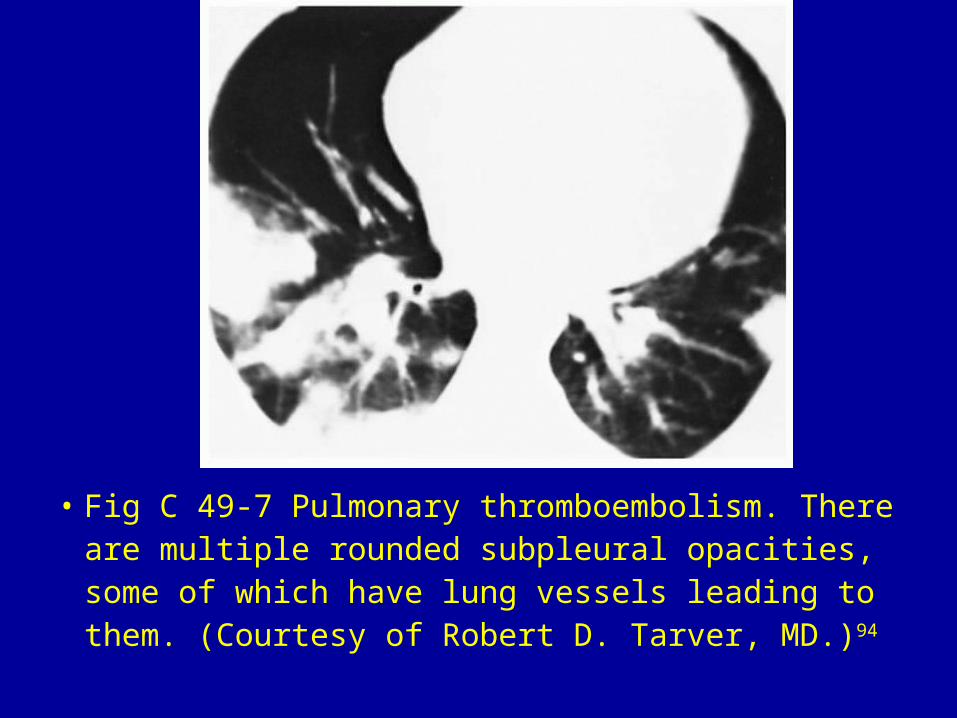
• Fig C 49-7 Pulmonary thromboembolism. There are multiple rounded subpleural opacities, some of which have lung vessels leading to them. (Courtesy of Robert D. Tarver, MD.)94

• Fig C 49-8 Septic emboli. Multiple peripheral cavitating opacities. The vascular connections, particularly in the right middle lobe, indicate their hematogenous origin.96
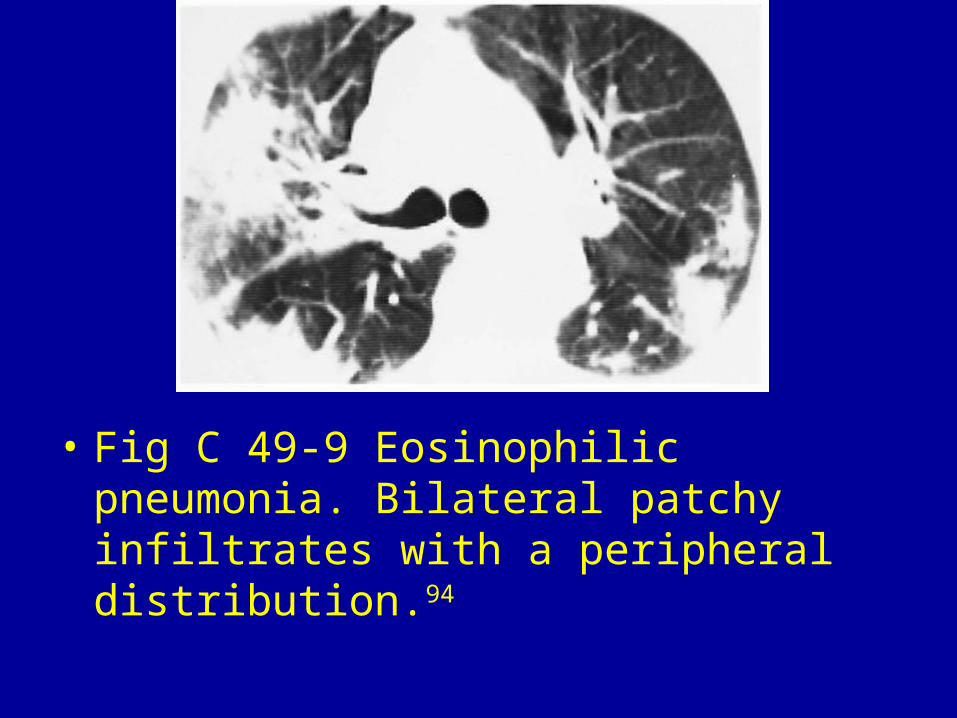
• Fig C 49-9 Eosinophilic pneumonia. Bilateral patchy infiltrates with a peripheral distribution.94
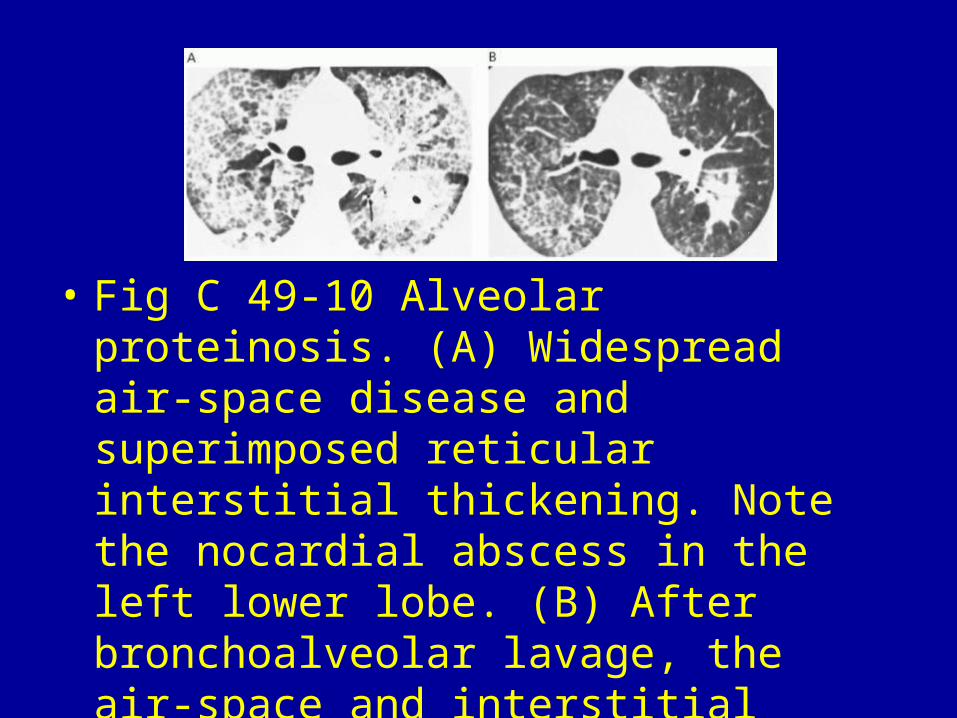
• Fig C 49-10 Alveolar proteinosis. (A) Widespread air-space disease and superimposed reticular interstitial thickening. Note the nocardial abscess in the left lower lobe. (B) After bronchoalveolar lavage, the air-space and interstitial components have diminished.97

• Fig C 49-11 Bronchioloalveolar carcinoma. (A) Widespread air-space filling with geographic margination. (B) Note the presence of air bronchograms. (Courtesy of David P. Naidich, MD.)94

• Fig C 49-12 Lipoid pneumonia. Characteristic dependent location of the consolidation.94

• Fig C 49-13 Alveolar sarcoidosis. (A) Large central masses with partially well-defined and partially ill-defined margins. (B) More peripheral lesions with air bronchograms.94

• Fig C 49-14 Pulmonary contusion. There are accompanying hemothorax, rib fractures, subcutaneous emphysema, and pleural drain.94
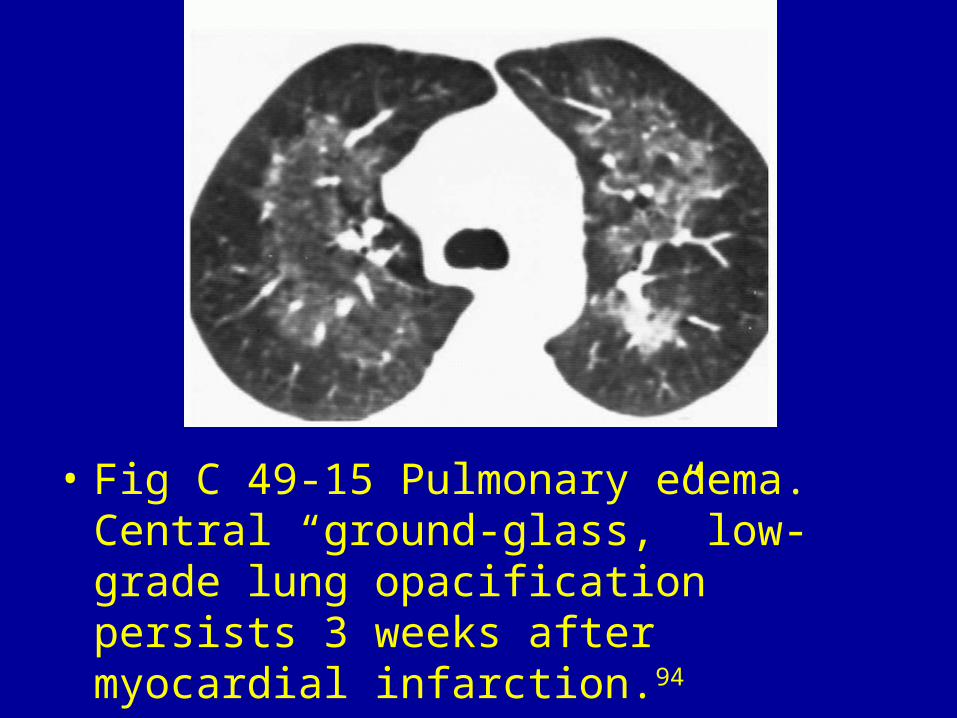
• Fig C 49-15 Pulmonary edema. Central “ground-glass,” low-grade lung opacification persists 3 weeks after myocardial infarction.94

• Fig C 49-16 Cocaine abuse. Acute pulmonary edema with bilateral heterogeneous opacities.11

• Fig C 49-17 Crack lung with pulmonary eosinophilia. Extensive bilateral heterogeneous central and peripheral opacities.

• Fig C 49-18 Pulmonary hemorrhage. Widespread, patchy, and geographic air-space filling in this patient with necrotizing vasculitis.94

• Fig C 49-19 Metastases. Multiple pulmonary nodules with vascular connections indicating their hematogenous origin.96

• Fig C 49-20 Lymphoma. Multiple nodular opacities, some with welldefined and some with ill-defined margins. The major differential diagnostic consideration is fungal infection in this patient with Hodgkin's disease.94

