5% imiquimod cream and reflectance-mode confocal microscopy as adjunct modalities to mohs...
TRANSCRIPT
ORIGINAL ARTICLE
5% Imiquimod Cream and Reflectance-Mode ConfocalMicroscopy as Adjunct Modalities to Mohs MicrographicSurgery for Treatment of Basal Cell CarcinomaABEL TORRES, MD, JD,n AGNIESZKA NIEMEYER, MD,n BEATRICE BERKES, MD,n
DIEGO MARRA, MD, CARL SCHANBACHER, MD,w SALVADOR GONZALEZ, MDz
MARY OWENS, MD,§ AND BLAINE MORGAN, MS§
nLoma Linda University Medical Center, Dermatology Office, Faculty Medical Offices, Loma Linda, California; wDanaFarber Cancer Institute, Boston, Massachusetts; zWellman Laboratories of Photomedicine, Dermatology Department,Harvard Medical School, Boston, Massachusetts; and §3M Pharmaceuticals, St. Paul, Minnesota
BACKGROUND. Imiquimod is an immune response modifier thatup-regulates cytokines and has been shown in clinical studies toreduce or clear basal cell carcinoma tumors when applied topically.
OBJECTIVE. The objectives were to evaluate the efficacy of 5%imiquimod cream in treating basal cell carcinoma precedingexcision by Mohs micrographic surgery and to determine if re-
flectance-mode confocal microscopy is useful to establish theneed for surgical intervention after imiquimod treatment.
METHODS. Subjects applied study cream to one biopsy-con-firmed basal cell carcinoma tumor 5�/week for 2, 4, or 6 weeksin this vehicle-controlled, double-blind study. Confocal micros-copy was used for the 6-week treatment group to examine the
target tumor area at each interval visit and immediately before
Mohs micrographic surgery. After the Mohs micrographic sur-gery excision, the tissue was evaluated histologically, and theexcision area was measured. Confocal microscopy readingswere correlated to the histologic diagnosis.
RESULTS. Tumors cleared or the target tumor area was reducedin subjects in the 4- and 6-week dosing regimens. Confocal
microscopy assessments correlated well with the histologicdiagnosis.
CONCLUSION. Imiquimod improved excision results relative to
vehicle when used for treating basal cell carcinoma before Mohsmicrographic surgery. Confocal microscopy assessments corre-lated well with tumor response to therapy, suggesting that con-
focal microscopy may help determine the need for surgery.
THIS STUDY WAS FUNDED BY A GRANT FROM 3M PHARMACEUTICALS (ST. PAUL, MN), AND THE CONFOCALMICROSCOPE AND SUPPLIES FOR MICROSCOPY WERE SUPPLIED BY LUCID, INC. (HENRIETTA, NY).
MOHS MICROGRAPHIC surgery is one of the mostdefinitive excision options for basal cell carcinoma.1
Mohs micrographic surgery involves excision of theclinically evident neoplastic lesion, microscopic anal-ysis of frozen tumor sections with meticulous mappingof the skin and the excised tissue, and reexcision ofhistologically identified residual neoplasm until tumor-free margins are obtained. Using Mohs micrographicsurgery allows selective excision of basal cell carcino-ma, thereby sparing healthy tissue. Because tumorsfrequently extend beyond their visible borders, orshow dramatic subclinical extension, however, the re-sulting surgical defect following Mohs micrographicsurgery can be significantly larger than the clinicallyapparent lesion and may compromise the final cos-metic outcome.2–4
The immune response modifier, imiquimod, is ap-proved for the treatment of external genital warts andactinic keratosis and has been shown in several studiesto be beneficial for the clearance of both nodular andsuperficial (basal cell carcinoma) lesions and wasrecently approved for the treatment of superficialBCC.5–8 Imiquimod induces interferon and othercytokines locally when applied topically to the tumorsite, producing an antitumor effect.9 Imiquimod couldbe used to reduce the size and the subclinical tumorextensions of primary basal cell carcinoma lesions pri-or to Mohs micrographic surgery, thereby decreasingthe resultant surgical defects and the degree of cos-metic damage caused by Mohs micrographic surgery.
In using a noninvasive therapy such as imiquimodto reduce the size of a basal cell carcinoma lesion, it isimportant to be confident of the treatment outcome sothat the area excised after treatment actually hastumor present or that the area spared is clear of tumor.Confocal microscopy has been effectively used to char-acterize basal cell carcinoma and as an adjunct to sur-
r 2004 by the American Society for Dermatologic Surgery, Inc. � Published by Blackwell Publishing, Inc.ISSN: 1076-0512/04/$15.00/0 � Dermatol Surg 2004;30:1462–1469
Address correspondence and reprint requests to: Abel Torres, MD, JD,
Loma Linda University Medical Center, Dermatology Office, Faculty
Medical Offices, 11370 Anderson Street, Suite 2600, Loma Linda, CA
92354, or e-mail: [email protected].

gery to establish tumor margins.10,11 Confocal mi-croscopy could therefore serve as an adjunct to Mohsmicrographic surgery in evaluating the effectiveness ofimiquimod treatment before surgery.
Methods
Design
This was a randomized, vehicle-controlled, double-blind parallel arm study conducted at two universitylocations in the United States by a single investigator.The protocol and informed consent documents werereviewed and approved by ethics committees at bothlocations. Informed consent was obtained from all sub-jects and the study protocol conformed to the guide-lines of the 1975 Declaration of Helsinki. Subjects wereassigned randomly to dosing regimens that requiredapplying study cream, 5% imiquimod, or vehicle cream(identical formulation cream without imiquimod) oncedaily, 5 days per week, for 2, 4, or 6 weeks.
Subjects and Biopsies
Subjects were informed of study procedures and oftheir rights and responsibilities as study participantsbefore signing an informed consent document. Duringa subject’s prestudy screening visit, up to four clinicallyevident basal cell carcinoma tumors were biopsied toconfirm the diagnosis of basal cell carcinoma if diag-nostic biopsies were not previously performed by areferring physician; biopsies were not repeated for re-ferred subjects. The screening, confirmatory deepshave, or punch biopsy was to penetrate into the re-ticular dermis. The majority of the biopsy was to ex-tend through the entire depth of the tumor but was toremove less than approximately 25% of the clinicallyevident tumor. Lesions were assessed clinically to see ifthe site of the biopsy was clearly evident and appearedclinically to not have removed more than 25% of theclinically assessed lesion including biopsy scarring.Subjects were eligible for the study if they were at least18 years old with a histologically confirmed, primary,superficial, nodular, or mixed superficial and nodularbasal cell carcinoma tumor. The tumor selected fortreatment was required to be consistent with basal cellcarcinoma with no histologic evidence of aggressivegrowth patterns, including severe squamous metapl-asia, morpheaform or infiltrative/desmoplastic fea-tures, or basosquamous features, and suitable fortreatment with Mohs micrographic surgery excision.Micronodular tumors were not specifically excluded.Target tumors were to have a minimum area of 0.5cm2 and a maximum diameter of 2.0 cm and could belocated on an acceptable area of the body as deter-
mined by the investigator. Subjects were excluded ifthey had previous therapy to the target tumor or ifthey had dermatologic conditions that could interferewith skin assessments. Eligible subjects were randomlyassigned 1:1 imiquimod to vehicle into one of sixtreatment groups according to a computer-generatedschedule with a block size of 12.
Safety and Efficacy Measurements
At the treatment initiation visit (2–52 weeks after thescreening biopsy) a baseline of the target tumor areawas determined by measuring and multiplying the twolargest perpendicular dimensions of the tumor. A smallpermanent ink punctum (tattoo) was placed in thecenter of the target lesion to assist in locating the siteafter treatment with imiquimod. In addition, a tem-plate was constructed with a transparent plastic sheetusing anatomic and skin landmarks to delineate thelocation of the tumor.
Subjects returned to the clinic at the end of Week 1,biweekly thereafter for up to 6 weeks, and after theposttreatment excision for safety and efficacy evalua-tions and to determine whether basal cell carcinomawas evident. Confocal microscopy assessments wereincluded for the 6-week group. Before Mohs micro-graphic surgery, the target tumor area was photo-graphed, measured, and assessed for specific local skinreactions that have been seen in other imiquimodstudies. Local skin reactions included erythema, ed-ema, induration, vesicles, erosion, ulceration, scab-bing/crusting, and flaking/scaling. The target tumorarea was then excised for histologic examination usingthe template as a guide to determine the pretreatmenttarget tumor location and to ensure that the treatedarea was accurately selected.
Study Cream Application
Subjects dispensed cream from single-use sachets andrubbed the cream into the target tumor area and ap-proximately 1 cm of the skin surrounding the tumor.The cream was usually applied just before the subject’snormal bedtime, using an estimated amount of studycream determined by the larger diameter of each sub-ject’s tumor, and left in place for at least 8 hr. Thetumor area was not covered with a bandage. Subjectsapplied study cream once per day, 5 days per week, for2, 4, or 6 weeks according to their assigned dosingregimen.
Reflectance-Mode Confocal Microscopy
A reflectance-mode confocal microscope (VS 1000,Lucid, Henrietta, NY) was used to assess the utility of
Dermatol Surg 30:12:December 2004 TORRES ET AL.: IMIQUIMOD AND CONFOCAL MICROSCOPY USED WITH MOHS SURGERY 1463

confocal microscopy to visualize cellular response totreatment with 5% imiquimod cream. The system hasa wavelength of 830 and 30� objective lens of NA0.9, which provided a lateral resolution of approxi-mately 1 mm and an axial resolution (section thickness)of 3 to 5 mm. This system is capable of imaging normalskin to a depth of 200 to 250 mm in vivo.12
When evaluating the images obtained with confocalmicroscopy, the characteristics that were consideredindicative of normal skin were a honeycomb appear-ance of the cellular architectural pattern, consistentratio of nucleus to cytoplasm, and regularly shapednuclei. The following features from the confocal im-ages were considered indicative of tumor: elongatednuclei, focal polarization, parakeratosis, actinic chang-es, monomorphism, prominent nucleoli, high nuclearto cytoplasm ratio, increased vascularity, increased in-flammatory cells, and rolling of white blood cells.11
Confocal microscopy assessments were performedon subjects in the 6-week treatment group beforetreatment, at biweekly (every 2 weeks) clinic visits, andat the Mohs micrographic surgery visit approximately2 weeks after the last treatment visit (just before theMohs micrographic surgery procedure). Results of thepre-Mohs micrographic surgery confocal microscopyevaluations were compared to the Mohs micrographicsurgery histology results.
Mohs Excision
Two to four weeks after the last day of treatment,Mohs micrographic surgery was performed on all sub-jects. Concentric circles were drawn around the visibletarget tumor at 2-mm intervals. The target tumor area,including visible tumor or pretreatment target tumorarea, was excised until no histologic evidence of basalcell carcinoma or suspicious inflammation was seen inthe margins. If the tumor was no longer visible, thetarget tumor location was determined through the useof the pretreatment plastic template together with thecentral punctum tattoo or other skin features recordedin pretreatment photographs; the first excision, in thatcase, consisted of the recorded target tumor area. Theexcised tissue was assessed as accurately as possible todetermine all subclinical extensions, and Mohs sec-tions were performed through the entire block of tissueremoved for completeness. Two measurements werecompared and the differences were tested betweentreatment groups: 1) the posttreatment, presurgicaltumor area was compared to pretreatment tumor areaand 2) the final wound measurement after Mohs mi-crographic surgery, including the wound expansion,was compared to the size of the lesion at study initi-ation.
Analyses
The statistical analysis was performed on the intent-to-treat data set, which included all randomized subjects.All 72 subjects enrolled in this study underwent Mohsmicrographic surgery.
The nonparametric Wilcoxon rank sum test wasused to analyze the change in target tumor area frombaseline. The primary endpoint was the change inclinical assessment of target tumor area from baselineto post-Mohs micrographic surgery excision area.Each of the three active treatment groups was indi-vidually tested against the vehicle group. To controlthe alpha level for these three tests, a step-down (pri-oritization) method of adjustment for multiple testingwas used.13,14 According to this procedure, first the 6-week treatment group was tested against the vehiclegroup at the a50.05 level. If the results of this testwere statistically significant, the 4-week treatmentgroup was then tested against the vehicle group at thea50.05 level. If the results of this test were also sta-tistically significant, the test on the 2-week treatmentgroup relative to vehicle was inspected for significance.
Complete response was a secondary efficacy varia-ble, defined as a subject with no histologic evidence ofbasal cell carcinoma in the posttreatment Mohs mi-crographic surgery tumor excision. Each active treat-ment group was analyzed relative to the vehicle groupon complete response rate using pairwise Fisher’s exacttests. Clinical assessment of response was analyzedsimilarly.
Results
Subjects
Seventy-two subjects (52 men, 20 women) were en-rolled in the study (Table 1). Target tumors ranged insize from 0.2 to 2.9 cm2 after biopsy (Table 1). Thedistribution of target tumor size between the vehicleand imiquimod treatment groups randomly resulted ina greater proportion of the larger tumors assigned tothe vehicle group, although this difference at baselinedid not achieve statistical significance. This is not be-lieved to have affected the analysis of the results of thisstudy, because the primary endpoint was percentchange from baseline to endpoint, which controls forthe baseline values. The median tumor area across alltreatment groups was 1.0 cm2. Two subjects had targettumors outside the range (1 smaller, 1 larger) specifiedin the inclusion criteria but were allowed to continuein the study. The post-Mohs micrographic surgery his-tologic evaluation revealed an aggressive basal cellcarcinoma growth pattern, including severe squamousmetaplasia, morpheaform or infiltrative/desmoplastic
1464 TORRES ET AL.: IMIQUIMOD AND CONFOCAL MICROSCOPY USED WITH MOHS SURGERY Dermatol Surg 30:12:December 2004
features, or basosquamous features in 7 subjects. Thisdiagnosis was possible only on Mohs micrographicsurgery excision because Mohs micrographic surgeryprovides a complete tumor for examination versus asmall sample provided by a biopsy. In addition, somesubjects’ biopsies were performed before initiation ofthe study and the biopsy was not repeated, which mayhave resulted in some subjects being initiated with atumor with an undiscovered aggressive growth pat-tern. Had the aggressive growth pattern been discov-ered upon initiation, the subjects would have beenexcluded from the study. Target tumors were locatedon the face in 47% (34/72) of subjects; on the ex-tremities, excluding hands and feet, in 24% (17/72) ofsubjects; and on the trunk in 19% (14/72) of subjects.No subjects discontinued during the study.
Efficacy
All randomly assigned subjects (n5 72) were includedin the safety and efficacy analysis. For the clinicalevaluation prior to Mohs micrographic surgery, 2 sub-jects in the vehicle 6-week treatment group and 1 inthe imiquimod 6-week treatment group were uneval-uable because the presence of tumor was indetermi-nate. The clinical tumor area was not measured beforeMohs micrographic surgery for these subjects; there-fore, 69 subjects were included in the secondary anal-ysis on pre-Mohs micrographic surgery area.
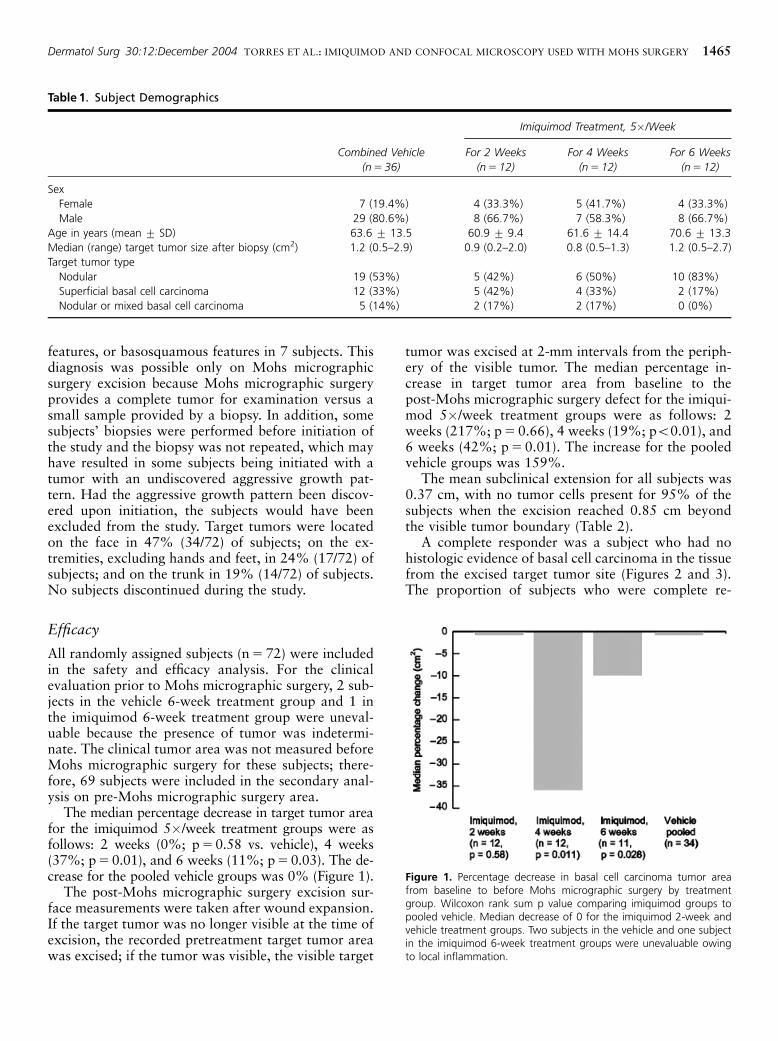
The median percentage decrease in target tumor areafor the imiquimod 5�/week treatment groups were asfollows: 2 weeks (0%; p50.58 vs. vehicle), 4 weeks(37%; p50.01), and 6 weeks (11%; p50.03). The de-crease for the pooled vehicle groups was 0% (Figure 1).
The post-Mohs micrographic surgery excision sur-face measurements were taken after wound expansion.If the target tumor was no longer visible at the time ofexcision, the recorded pretreatment target tumor areawas excised; if the tumor was visible, the visible target
tumor was excised at 2-mm intervals from the periph-ery of the visible tumor. The median percentage in-crease in target tumor area from baseline to thepost-Mohs micrographic surgery defect for the imiqui-mod 5�/week treatment groups were as follows: 2weeks (217%; p5 0.66), 4 weeks (19%; po0.01), and6 weeks (42%; p50.01). The increase for the pooledvehicle groups was 159%.
The mean subclinical extension for all subjects was0.37 cm, with no tumor cells present for 95% of thesubjects when the excision reached 0.85 cm beyondthe visible tumor boundary (Table 2).
A complete responder was a subject who had nohistologic evidence of basal cell carcinoma in the tissuefrom the excised target tumor site (Figures 2 and 3).The proportion of subjects who were complete re-
Table 1. Subject Demographics
Imiquimod Treatment, 5�/Week
Combined Vehicle
(n5 36)
For 2 Weeks
(n512)
For 4 Weeks
(n512)
For 6 Weeks
(n512)
Sex
Female 7 (19.4%) 4 (33.3%) 5 (41.7%) 4 (33.3%)
Male 29 (80.6%) 8 (66.7%) 7 (58.3%) 8 (66.7%)
Age in years (mean � SD) 63.6 � 13.5 60.9 � 9.4 61.6 � 14.4 70.6 � 13.3
Median (range) target tumor size after biopsy (cm2) 1.2 (0.5–2.9) 0.9 (0.2–2.0) 0.8 (0.5–1.3) 1.2 (0.5–2.7)
Target tumor type
Nodular 19 (53%) 5 (42%) 6 (50%) 10 (83%)
Superficial basal cell carcinoma 12 (33%) 5 (42%) 4 (33%) 2 (17%)
Nodular or mixed basal cell carcinoma 5 (14%) 2 (17%) 2 (17%) 0 (0%)
Figure 1. Percentage decrease in basal cell carcinoma tumor areafrom baseline to before Mohs micrographic surgery by treatmentgroup. Wilcoxon rank sum p value comparing imiquimod groups topooled vehicle. Median decrease of 0 for the imiquimod 2-week andvehicle treatment groups. Two subjects in the vehicle and one subjectin the imiquimod 6-week treatment groups were unevaluable owingto local inflammation.
Dermatol Surg 30:12:December 2004 TORRES ET AL.: IMIQUIMOD AND CONFOCAL MICROSCOPY USED WITH MOHS SURGERY 1465

sponders in the imiquimod treatment groups were asfollows: 2 weeks, 3 of 12 (25%; p5 0.09); 4 weeks, 8of 12 (67%; p o 0.01); and 6 weeks, 8 of 12 (67%;p o 0.01). The proportion of subjects who were com-plete responders in the pooled vehicle groups was 2 of36 (6%). The tumors were evaluated for skip areas byMMS processing of the entire excised tissue or absenceof tumor on a pre-MMS biopsy with subsequent tumorfound on MMS peripheral to the biopsy.
When comparing the pre-Mohs micrographic sur-gery investigator clinical assessments with the histo-logic outcome for all subjects, the negative predictivevalue, or the ability of the investigator to correctlydiagnose when basal cell carcinoma was not present,was 80.0% (8/10). The positive predictive value, or theability of the investigator to correctly diagnose whenbasal cell carcinoma was present, was 79.0% (49/62).When comparing the pre-Mohs micrographic surgeryinvestigator clinical assessments with the histologicoutcome for pooled imiquimod groups only, the neg-ative predictive value was 88.9% (8/9). The positivepredictive value was 59.3% (16/27). Confocal micros-copy assessments were made for the 6-week treatmentgroups (Figures 4 and 5). Concordance of the confocal
microscopy assessment with the histologic outcome ofthe excised tumor specimens was calculated for theimiquimod group, the vehicle groups, and all subjectscombined. For confocal microscopy assessmentsacross the pooled imiquimod and vehicle dosing reg-imens (Table 3), the negative predictive value was
Table 2. Excision Radius Beyond Pre-Mohs MicrographicSurgery Visible Tumor Boundary
Statistic
Pooled Vehicle
(n5 34)
Pooled Imiquimod
(n5 35)
All Subjects
(n569)n
Mean (cm) 0.37 0.36 0.37
Minimum –0.45 –0.15 –0.45
Maximum 0.90 1.25 1.25
95th percentile 0.83 1.10 0.85
Median 0.35 0.30 0.30
nThe presence or absence of basal cell carcinoma was indeterminate for threesubjects.
Figure 2. Pretreatment basal cell carcinoma tumor.
Figure 3. Confocal microscopy before treatment: elongated cells withhigh cytoplasm-to-nucleus ratio (consistent with basal cell carcinoma).
Figure 4. Two weeks after treatment: clinically and histologically clear.
1466 TORRES ET AL.: IMIQUIMOD AND CONFOCAL MICROSCOPY USED WITH MOHS SURGERY Dermatol Surg 30:12:December 2004

70.0% (7/10). The positive predictive value was84.6% (11/13). For some subjects, the confocal mi-croscopy assessment could not be determined, becauseof scabbing for example. When a confocal microscopyassessment could be determined, the histologic resultsand the confocal microscopy results were in agreement.
Safety
Subjects in all treatment groups reported adverseevents; 11% (4/36) of subjects using vehicle and42% (15/36) using imiquimod reporting at least oneadverse event. Adverse events were categorized bybody system (Table 4). No serious or severe adverseevents were reported and no subject discontinued be-cause of an adverse event. One subject experiencedfacial swelling and one subject reported flu-like symp-toms that resolved upon discontinuing study drug.
The most frequently reported adverse event (bypreferred term) was application site reaction, reportedby 33% (4/12) of subjects in the imiquimod for 6-weekgroup and by no subjects in any other group. Appli-cation site reactions were defined as discomfort at thetarget site, dryness at target site, erythema at remotesite, itching at target site, pain at remote site, pain at
target site, papule(s) at target site, swollen at remotesite, and swollen at target site. Application site reac-tion was also the most frequently reported adverseevent that was considered to be possibly or probablyrelated to study cream. Flu-like symptoms were re-ported by 1 (8%) subject in the imiquimod 5�/weekfor the 4-week group, a headache was reported by 1(8%) subject in the imiquimod 5�/week for the 6-week group, and procedural site were reported reac-tions by 5 subjects, 2 (17%) in the imiquimod 5�/week for the 4-week group, 1 (8%) in the imiquimod5�/week for the 6-week group, and 2 (6%) in thepooled vehicle groups.
Local skin reactions were evaluated at each treat-ment visit by both the investigator and the subjects.Overall, local skin reactions tended to be more intensein the active treatment groups than the vehicle groups.Subjects in the vehicle groups did experience local skinreactions but of a lower intensity than in the activetreatment groups. Most reactions were mild.
Discussion
The application of 5% imiquimod cream before exci-sion with Mohs micrographic surgery significantly re-duced the size of the target tumor and resulted in asmaller surgical defect from the Mohs micrographicsurgery excision (compared to vehicle groups). Al-though the study may lend credence to a hypothesisthat 4 weeks of imiquimod treatment may be as effec-tive as 6 weeks for the treatment of basal cell carci-noma, the study was not designed and the sample sizeswere not large enough to adequately characterize animiquimod dose–duration response curve.
The post-Mohs micrographic surgery defect mayhave been smaller if more time had been allowed be-tween end-of-treatment and Mohs micrographic sur-gery, because, according to the center’s standardpractice, additional stages were sometimes performedto rule out the presence of tumor if inflammation waspresent that could have been obscuring tumor, even ifno tumor cells were visualized. In most prior studieswith imiquimod for the treatment of basal cell carci-noma, the posttreatment excisions have been conduct-ed approximately 6 weeks after treatment, when localskin reactions (and presumably inflammation) havesubstantially resolved.5–8 Had we waited 6 weeks afterimiquimod treatment there may have been fewer stag-es of Mohs micrographic surgery performed and there-fore more sparing of healthy tissue. Also, depending onthe location of the target tumor, the tissue may havespread open after Mohs micrographic surgery, causingthe resulting defect to appear larger than the actualtissue removed.
Figure 5. Confocal microscopy 2 weeks after treatment: regularhoneycomb and normal epidermis.
Table 3. Pre-Mohs Micrographic Surgery Confocal Micro-scopy Assessment of Tumor Clearance versus HistologicResultsn
Predictive
Value
Imiquimod,
6 Weeks
Vehicle,
6 Weeks
Combined,
6 Weeks
Negative 6/7 (85.7%) 1/3 (33.3%) 7/10 (70.0%)
Positive 3/5 (60.0%) 8/8 (100.0%) 11/13 (84.6%)
nIf subjects with indeterminate confocal microscopy assessments (n5 5) are ex-cluded, all confocal microscopy outcomes matched the histologic results.
Dermatol Surg 30:12:December 2004 TORRES ET AL.: IMIQUIMOD AND CONFOCAL MICROSCOPY USED WITH MOHS SURGERY 1467

For all subjects enrolled in this study, the clinicalevaluation was reliable, with a negative predictive val-ue of determining the absence of tumor that was high-er (80.0%; 8/10) than a noninvasive mechanicalassessment with confocal microscopy (70%; 7/10).The positive predictive value for confocal microscopy(84.6%; 11/13) was higher when establishing tumorpresence than clinical assessments (79%; 49/62)(Table 3). These results suggest that confocal micros-copy may facilitate more accurate noninvasive assess-ments by clinicians. When performing assessments,residual redness or other skin irregularity in the treat-ment area increased the difficulty in determiningwhether tumor was still present. Much of the timethe residual redness or skin irregularity did not indi-cate tumor. For this study, when a diagnosis by con-focal microscopy could be determined, the histologicresults and the confocal microscopy results were inagreement.
Confocal microscopy is a noninvasive means ofevaluating tumor in vivo, its use could lead to tissue-sparing during Mohs micrographic surgery, it couldpotentially be used to evaluate the need for surgeryafter adjunct treatment with imiquimod. Aside frombeing a time-consuming technique, the challenges of
using confocal microscopy include difficulties in ma-nipulating a large machine; maintaining the seal withthe tissue stabilizer ring on convex or concave skinsurfaces, oily skin, or skin at an angle; image varia-bility; and interpretation of images.
This study indicates that clinical evaluations as wellas a noninvasive mechanical assessments with confocalmicroscopy are generally effective and reliable fortumor diagnosis. Imiquimod was effective as an ad-junct therapy in the treatment of primary basal cellcarcinoma lesions by eliminating or reducing thetumor size before Mohs micrographic surgery and de-creasing the resultant surgical defect, thereby poten-tially reducing treatment-associated costs inherent inthe repair of such cosmetic damage. This may be es-pecially useful in the managed care setting or othersituations where treatment delays are common andtreatment with the objective of preventing furthertumor growth could be helpful.
Acknowledgments We acknowledge Cathryn Lloyd (3Mclinical project management), Margo Liberda (3M clinicalstudy management), Jamie Broos (3M data management),Melanie Molin (clinical programming), and Laura Bean Warn-er (3M manuscript preparation).
Table 4. Incidence of Adverse Events
Imiquimod, 5�/week
Body System Preferred Term
For 2 Weeks
(n512)
For 4 Weeks
(n5 12)
For 6 Weeks
(n512)
Vehicle Pooled, 5�/Week
(n536)
No. (%) of subjects with at least one adverse event 2 (17%) 6 (50%) 7 (58%) 4 (11%)
Application site
Disorders 0 (0%) 0 (0%) 4 (33%) 0 (0%)
Reaction 0 (0%) 0 (0%) 4 (33%) 0 (0%)
Body as a whole
General disorders 0 (0%) 1 (8%) 0 (0%) 1 (3%)
Influenza-like symptoms 0 (0%) 1 (8%) 0 (0%) 1 (3%)
Central/peripheral nervous system disorders 1 (8%) 0 (0%) 1 (8%) 0 (0%)
Headache 1 (8%) 0 (0%) 1 (8%) 0 (0%)
Gastrointestinal system disorders 1 (8%) 1 (8%) 0 (0%) 0 (0%)
Nausea 1 (8%) 0 (0%) 0 (0%) 0 (0%)
Stomatitis ulcerative 0 (0%) 1 (8%) 0 (0%) 0 (0%)
Musculoskeletal system disorders 0 (0%) 1 (8%) 0 (0%) 1 (3%)
Arthritis 0 (0%) 0 (0%) 0 (0%) 1 (3%)
Bursitis 0 (0%) 1 (8%) 0 (0%) 0 (0%)
Psychiatric disorders 0 (0%) 0 (0%) 1 (8%) 0 (0%)
Insomnia 0 (0%) 0 (0%) 1 (8%) 0 (0%)
Respiratory system disorders 0 (0%) 1 (8%) 1 (8%) 0 (0%)
Sinusitis 0 (0%) 1 (8%) 0 (0%) 0 (0%)
Upper respiratory tract infection 0 (0%) 0 (0%) 1 (8%) 0 (0%)
Secondary terms 0 (0%) 2 (17%) 1 (8%) 2 (6%)
Procedural site reaction 0 (0%) 2 (17%) 1 (8%) 2 (6%)
Urinary system disorders 1 (8%) 0 (0%) 0 (0%) 0 (0%)
Urinary tract infection 1 (8%) 0 (0%) 0 (0%) 0 (0%)
1468 TORRES ET AL.: IMIQUIMOD AND CONFOCAL MICROSCOPY USED WITH MOHS SURGERY Dermatol Surg 30:12:December 2004

References
1. Rowe DE, Carroll RJ, Day CL. Long-term recurrence rates in pre-viously untreated (primary) basal cell carcinoma: implications forpatient follow-up. J Dermatol Surg Oncol 1989;15:315–28.
2. Wolf DJ, Zitelli JA. Surgical margins for basal cell carcinoma. ArchDermatol 1987;123:340–4.
3. Burg G, Hirsch RD, Konz B, Braun-Falco O. Histographic surgery:accuracy of visual assessment of the margins of basal-cellepithelioma. J Dermatol Surg 1975;1:21–4.
4. Anthony ML. Surgical treatment of nonmelanoma skin cancer.AORN J 2000;71:552–64.
5. Beutner K, Geisse JK, Helman D, et al. Therapeutic response ofbasal cell carcinoma to the immune response modifier imiquimod5% cream. J Am Acad Dermatol 1999;41:1002–7.
6. Shumack S, Robinson J, Kossard S, et al. Efficacy of topical 5%imiquimod cream for the treatment of nodular basal cell carcinoma:comparison of dosing regimens. Arch Dermatol 2002;138:1165–71.
7. Marks R, Gebauer K, Shumack S, et al. Imiquimod 5% cream in thetreatment of superficial basal cell carcinoma: results of a multicen-ter 6-week dose–response trial. J Am Acad Dermatol 2001;44:807–13.
8. Geisse JK, Rich P, Pandya A. Imiquimod 5% cream for thetreatment of superficial basal cell carcinoma: a double-blind, ran-
domized, vehicle-controlled study. J Am Acad Dermatol 2002;47:390–8.
9. Arany I, Tyring SK, Stanley MA, et al. Enhancement of theinnate and cellular immune response in patients with genital wartstreated with topical imiquimod cream 5%. Antiviral Res 1999;43:55–63.
10. Tannous Z, Torres A, Gonzalez S. In vivo real-time confocal re-flectance microscopy: a noninvasive guide for Mohs micrographicsurgery facilitated by aluminum chloride, an excellent contrast en-hancer. Dermatol Surg 2003;29:839–46.
11. Gonzalez S, Tannous Z. Real-time, in vivo confocal reflectance mi-croscopy of basal cell carcinoma. J Am Acad Dermatol 2002;47:869–74.
12. Rajadhyaksha M, Gonzalez S, Zavislan J, et al. In vivo confocalscanning laser microscopy of human skin, II. Advances in instru-mentation and comparison with histology. J Invest Dermatol(1999);113:293–303.
13. Tamhane AC, Hochberg Y, Dunnett CW. Multiple test proceduresfor dose finding. Biometrics (1996);52:21–37.
14. European Committee for Proprietary Medicinal Products (CPMP).Points to Consider on Multiplicity Issues in Clinical Trials [Inter-net]. London: European Agency for the Evaluation of MedicinalProducts, 2002 Sep 19 [accessed 23 Apr 2003]. Available from:http://www.emea.eu.int/pdfs/human/ewp/090899en.pdf
Dermatol Surg 30:12:December 2004 TORRES ET AL.: IMIQUIMOD AND CONFOCAL MICROSCOPY USED WITH MOHS SURGERY 1469