50 encore! pancreas: surgical pathology and cytopathology...
TRANSCRIPT

50 ENCORE! Pancreas: Surgical Pathology and Cytopathology of Pancreatic Neoplasms
N Adsay MD Michelle Reid MD
2011 Annual Meeting – Las Vegas, NV
AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste. 1600
Chicago, IL 60603

50 ENCORE! Pancreas: Surgical Pathology and Cytopathology of Pancreatic Neoplasms With recent advances in imaging and interventional techniques and a dramatic decline in mortality and morbidity of pancreatic operations pancreatic resection specimens are now seen more often by surgical pathologists. Endoscopic ultrasound-guided fine needle aspiration has significantly increased the number of preoperative cytologic specimens reviewed by cytopathologists. Changes in terminology and classifications add to the new information one must now absorb. This session will provide an overview of challenges and practical clues in the diagnosis of pancreatobiliary specimens, with an algorithmic approach to differential diagnosis. Discussions will include: Pancreatic adenocarcinoma and its distinction from its mimics; Differential diagnosis of solid cellular/fleshy tumors of the pancreas; Clinicopathologic characteristics and biologic behavior of cystic tumors of the pancreas; Cytopathologic diagnosis of solid and cystic pancreatic lesions.
• Accurately differentiate problematic cases in surgical pathology of the pancreas, including solid-scirrhous lesions, solid/fleshy circumscribed lesions and cystic and traductal pancreatic tumors.
• Recognize the most common solid and cystic pancreatic lesions/tumors encountered on pancreatic fine needle aspiration; Evaluate the usefulness of ancillary studies in their cytologic diagnosis; Recognize key gastrointestinal contaminants in endoscopic tultrasound-guided pancreatic fine needle aspiration, that may lead to misdiagnosis on cytology.
• Distinguish and diagnose tumors of the ampulla, gallbladder and extrahepatic bile duct; Describe the grossing of pancreatoduodenectomy specimens.
FACULTY: N Adsay MD Michelle Reid MD Practicing Pathologists Surgical Pathology Surgical Pathology (GI, GU, Etc.) 3.0 CME/CMLE Credits Accreditation Statement: The American Society for Clinical Pathology (ASCP) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education (CME) for physicians. This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME). Credit Designation: The ASCP designates this enduring material for a maximum of 3 AMA PRA Category 1 Credits™. Physicians should only claim credit commensurate with the extent of their participation in the activity. ASCP continuing education activities are accepted by California, Florida, and many other states for relicensure of clinical laboratory personnel. ASCP designates these activities for the indicated number of Continuing Medical Laboratory Education (CMLE) credit hours. ASCP CMLE credit hours are acceptable to meet the continuing education requirements for the ASCP Board of Registry Certification Maintenance Program. All ASCP CMLE programs are conducted at intermediate to advanced levels of learning. Continuing medical education (CME) activities offered by ASCP are acceptable for the American Board of Pathology’s Maintenance of Certification Program.

1
EUS‐Guided Fine Needle Aspiration and
Cytopathology of Cystic and Solid Lesions of the Pancreas
Michelle Reid, MDDepartment of PathologyEmory University Hospital
Atlanta, GA
NEEDLE ASPIRATION OF THE PANCREAS
– 1. Percutaneous fine needle aspiration (FNAB) • Performed by a radiologist
– 2. Endoscopic ultrasound‐guided (EUS) FNAB (# 1 technique)• Performed by a gastroenterologist
• An echoendoscope is placed g
• A. Trans‐abdominal ultrasound
• B. CT‐ guided» Better resolution of smaller lesions
p pagainst stomach/duodenum
• High‐resolution image obtained
INTRODUCTION
Endoscopic ultrasound‐guided (EUS) FNAB • Advantages:
– Most cost effective and sensitive diagnostic modality
– Higher resolution of sub‐centimeter (0.5 cm) lesions than CT
Real time visualization of needle during FNA– Real‐time visualization of needle during FNA
– Simultaneously diagnose and stage patients

2
DIAGNOSIS OF PANCREATIC LESIONS
• Can be challenging ‐ SO WHY DO IT?• Because cytologic diagnosis affects surgical management
• Pseudocysts, serous cystadenoma, pancreatitis –NO SURGERY REQUIRED
• All other lesions/neoplasms –SURGERY REQUIRED
• Initial assessment of pancreatic lesions is radiologic – Lesions are either cystic, solid or mixed
ABRIDGED CLASSIFICATION OF SOLID AND CYSTIC PANCREATIC NEOPLASMS
Gross Configuration Neoplasms %
Solid Neoplasms
Ductal Adenocarcinoma 85%
Pancreatic Neuroendocrine Tumor 3‐4%
Acinar Cell Carcinoma 1‐2%
(Solid‐Pseudopapillary Neoplasm) 1‐2%
Pancreatoblastoma <1%
Cystic ‐True cysts Serous Cystadenoma 1‐2%Cystic ‐True cysts Serous Cystadenoma 1‐2%
Mucinous Cystic Neoplasm 1‐2%
Cystic ‐ Intraductal Intraductal Papillary Mucinous Neoplasm 3‐5%
Cystic ‐ DegenerativeSolid‐Pseudopapillary Neoplasm
(Ductal Adenocarcinoma, Acinar Cell Carcinoma, Pancreatic Neuroendocrine Tumor)
Entities in parentheses only rarely exhibit this gross configuration
Modified from Klimstra et al. Archives of Pathology and Laboratory Medicine 2009; 133(3):454‐64.
INTRODUCTION• FNA diagnosis of pancreatic lesions requires correlation of:
• Cytologic and clinical findings
• Radiologic findings
• Ancillary studies» Immunohistochemistryy
» Flow cytometry
» Cyst fluid analysis

3
INTRODUCTIONAccuracy of FNAB
• Immediate cytologic assessment IS A MUST• Best performed by cytopathologist or cytotechnologist
• Reduces number of passes
• Reduces inadequate samples
• Saves time and money
Accuracy of Pancreatic FNAB• Sensitivity for detecting malignancy:
– 86% ‐ 98% for percutaneous FNAB – 75% ‐ 94% for EUS‐FNAB
• Specificity for both approaches 100% • False‐negative and false‐positive results occur• False negative results more common• False‐negative results more common
SAMPLE PREPARATION AND EVALUATION
• 1. Prepare air‐dried and alcohol‐fixed slidesA. Air‐dried slides
• Stain with a Romanowski stain– Diff‐Quik®
• Determine adequacy• Triage specimens
• Flow cytometry (if
• 2. Collect needle rinses for:– Cell blocks (place specimen in
95% alcohol or formalin) • Immunohistochemical stains
Flow cytometry (if lymphoma is suspected)
• Cyst fluid collection for analysis*
B. Alcohol‐fixed slides• Papanicolaou and hematoxylin
and eosin (H&E)
4
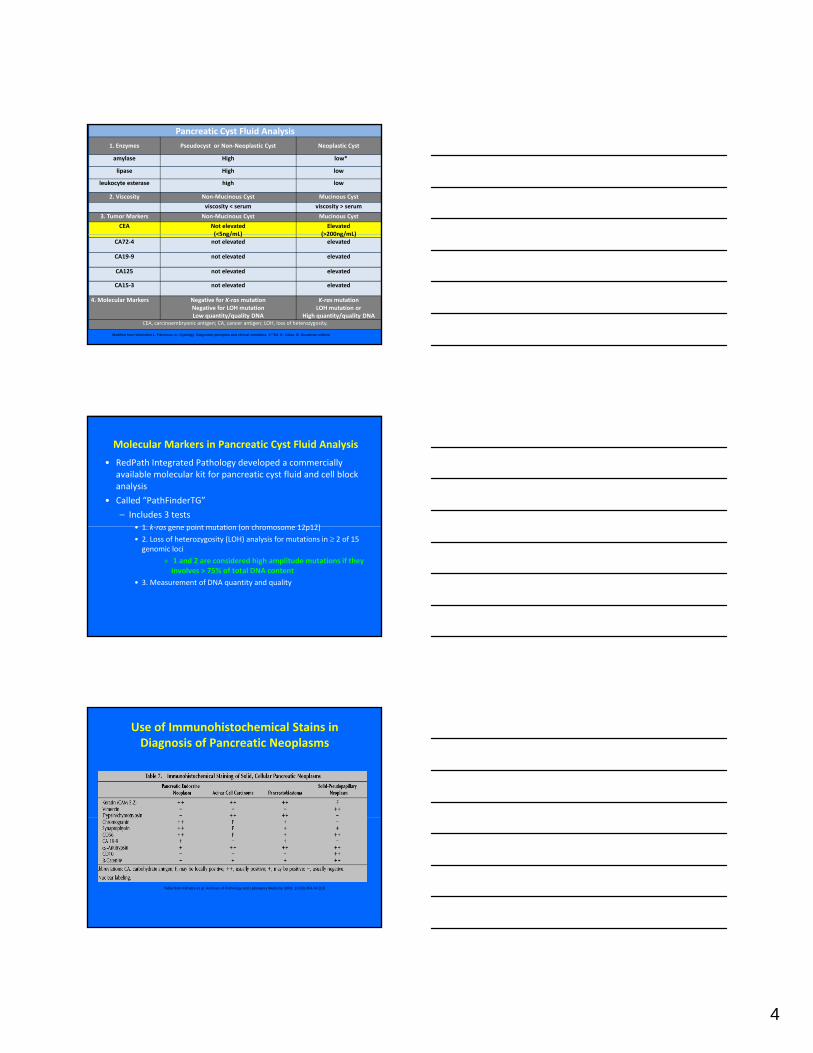
Pancreatic Cyst Fluid Analysis1. Enzymes Pseudocyst or Non‐Neoplastic Cyst Neoplastic Cyst
amylase High low*
lipase High low
leukocyte esterase high low
2. Viscosity Non‐Mucinous Cyst Mucinous Cyst
viscosity < serum viscosity > serum
3. Tumor Markers Non‐Mucinous Cyst Mucinous Cyst
CEA Not elevated (<5ng/mL)
Elevated (>200ng/mL)(<5ng/mL) (>200ng/mL)
CA72‐4 not elevated elevated
CA19‐9 not elevated elevated
CA125 not elevated elevated
CA15‐3 not elevated elevated
4. Molecular Markers Negative for K‐rasmutationNegative for LOH mutation Low quantity/quality DNA
K‐rasmutation LOH mutation or
High quantity/quality DNACEA, carcinoembryonic antigen; CA, cancer antigen; LOH, loss of heterozygosity.
Modified from Weinstein L, Pancreas. In: Cytology. Diagnostic principles and clinical correlates. 3rd Ed. E. Cibas, B. Ducatman editors
Molecular Markers in Pancreatic Cyst Fluid Analysis
• RedPath Integrated Pathology developed a commercially available molecular kit for pancreatic cyst fluid and cell block analysis
• Called “PathFinderTG”
– Includes 3 tests• 1 k ras gene point mutation (on chromosome 12p12)• 1. k‐ras gene point mutation (on chromosome 12p12)
• 2. Loss of heterozygosity (LOH) analysis for mutations in ≥ 2 of 15 genomic loci
» 1 and 2 are considered high amplitude mutations if they involves > 75% of total DNA content
• 3. Measurement of DNA quantity and quality
Use of Immunohistochemical Stains in Diagnosis of Pancreatic Neoplasms
Table from Klimstra et al. Archives of Pathology and Laboratory Medicine 2009; 133(3):454-64.[14]

5
REPORTING TERMINOLOGYSix diagnostic categories
• 1) Non‐diagnostic
• 2) Negative for malignancy
• 3) Atypical cells present
• 4) Suspicious for malignancy
• 5) Positive for malignant cells
• 6) Neoplastic cells present
Diagnostic Categories
1. Non‐diagnostic: • Material is unsatisfactory:
– Because of low cellularity
– Because it does not represent the site biopsied
2. Negative for malignancy: • Benign pancreatic epithelium
p
Diagnostic Categories
3. Atypical cells present:
• Atypia is mild• Background pancreatitis
common
4. Suspicious for malignancy:
• Atypia ≥moderate • Worrisome for malignancy but:
• Qualitatively insufficientcommon
• A COMMENT should be added
Qualitatively insufficient
• Quantitatively insufficient
for a definite diagnosis of malignancy

6
Diagnostic Categories
5. Positive for malignant cells• Cells shows obvious malignant
features
6. Neoplastic cells present: • When the cells are obviously
“neoplastic” but not definitely benign or malignant
• e.g. Mucinous cystse.g. Mucinous cysts
Contaminants in Pancreatic FNAB• EUS‐FNAB introduces gastrointestinal (GI) tract contaminants
• GI tract contaminants include:– 1.Duodenal epithelium
– 2. Gastric epithelium
– 3. GI tract mucin
• Distinguishing GI contaminants from pancreatic ductal adenocarcinoma and neoplastic mucinous cysts can be challenging
CONTAMINANTS IN PANCREATIC FNAB
• Must know location of lesion to determine likely contaminant
• Lesions in head and uncinate process →duodenal epithelial pcontaminants
• Lesions in body/tail →gastric epithelial contaminants

7
1. Duodenal Epithelial Contaminants
• Form flat honeycomb sheets with interspersed goblet cells
• Tissue edges have distinct brush border best seen atbrush border best seen at very high power
• Distinction from well differentiated ductal carcinoma or a neoplastic mucinous cyst can be difficult
Well Differentiated Ductal Adenocarcinoma vs
Duodenal Contaminants
Well differentiated ductal carcinoma ‐ note pleomorphism, overlapping cells and absence of brush border
Duodenal epithelium –note blanduniform cells with 2‐dimensional arrangement and brush border at edge of sheet
Duodenal Contaminants vs Mucinous Neoplasm
Goblet cells
Duodenal epithelium has 2‐dimensional honeycomb sheets with isolated goblet cells interspersed between benign columnar cellsThis helps to distinguish duodenal contaminants from a neoplastic mucinous cyst which has a pure population of mucin‐filled cells which are often
crowded together and overlapping
Duodenal epithelium Neoplastic mucinous cyst
8
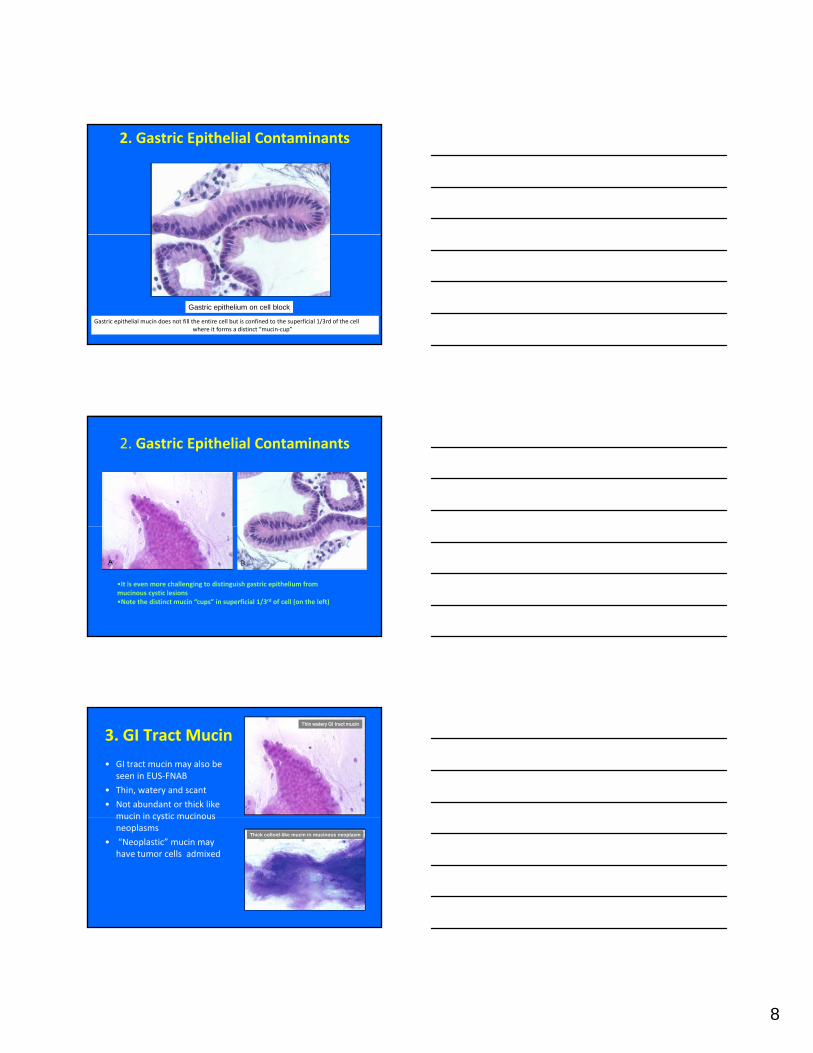
2. Gastric Epithelial Contaminants
Gastric epithelial mucin does not fill the entire cell but is confined to the superficial 1/3rd of the cellwhere it forms a distinct “mucin‐cup”
Gastric epithelium on cell block
2. Gastric Epithelial Contaminants
•It is even more challenging to distinguish gastric epithelium from mucinous cystic lesions•Note the distinct mucin “cups” in superficial 1/3rd of cell (on the left)
3. GI Tract Mucin
• GI tract mucin may also be seen in EUS‐FNAB
• Thin, watery and scant
• Not abundant or thick like mucin in cystic mucinous
Thin watery GI tract mucin
mucin in cystic mucinous neoplasms
• “Neoplastic” mucin may have tumor cells admixed
Thick colloid-like mucin in mucinous neoplasm

9
Normal Exocrine Pancreas ‐ Acinar Cells
– Cells form acinar structures without distinct lumens– Cells are bland, pyramidal/triangular with low N/C ratio, granular (zymogen‐rich) cytoplasm, round nuclei, inconspicuous or prominent nucleoli
CYTOLOGY OF THE NORMAL EXOCRINE
PANCREAS
• Ductal cells– Form monolayer sheets
– Cells are evenly dispersed
– Well‐defined cell borders
Round nuclei with fine– Round nuclei with fine chromatin
– Inconspicuous or absent nucleoli
Ductal cells in honeycomb sheet
CYTOLOGY OF THE
NORMAL PANCREAS
Endocrine pancreas• Islet cells
– Rarely sampled on a FNA
– Form loose aggregates with ill‐defined cell bordersdefined cell borders
– Wispy cytoplasm
– Round nuclei
– Fine chromatin
– Nucleoli are absent or inconspicuous
Endocrine cells are small, monotonous with low N/C ratio and bland nuclei

10
CYSTIC PANCREATIC LESIONS
CYSTIC PANCREATIC LESIONS• The majority are non‐neoplastic or benign
• Pancreatic pseudocysts account for the majority (75%)
• Lymphoepithelial cysts
• Serous cystadenoma
M i ti l• Mucinous cystic neoplasm
• Intraductal papillary mucinous neoplasm
• Solid neoplasms with cystic degeneration
ABRIDGED CLASSIFICATION OF SOLID AND CYSTIC PANCREATIC NEOPLASMS
Gross Configuration Neoplasms %
Solid Neoplasms
Ductal Adenocarcinoma 85%
Pancreatic Neuroendocrine Tumor 3‐4%
Acinar Cell Carcinoma 1‐2%
(Solid‐Pseudopapillary Neoplasm) 1‐2%
Pancreatoblastoma <1%
Cystic True cysts Serous Cystadenoma 1 2%Cystic ‐True cysts Serous Cystadenoma 1‐2%
Mucinous Cystic Neoplasm 1‐2%
Cystic ‐ Intraductal Intraductal Papillary Mucinous Neoplasm 3‐5%
Cystic ‐ DegenerativeSolid‐Pseudopapillary Neoplasm
(Ductal Adenocarcinoma, Acinar Cell Carcinoma, Pancreatic Neuroendocrine Tumor)
Entities in parentheses only rarely exhibit this gross configuration
Modified from Klimstra et al. Archives of Pathology and Laboratory Medicine 2009; 133(3):454‐64.

11
Serous cystadenoma
Solidpseudopapillaryneoplasm
Mucinous CysticNeoplasm
Intraductal
CYSTIC PANCREATIC LESIONS
Pseudocyst
papillarymucinous neoplasm
The primary goal of FNAB of cystic lesions is to distinguish low from
high‐risk pancreatic cystsg p y
• Low‐risk pancreatic cysts– Less likely to harbor malignancy
– Resected only if:• Symptomatic
• When definitive diagnosis
• High‐risk pancreatic cysts– Have a higher risk of high‐
grade dysplasia or malignancy – Managed surgically with
partial/total pancreatectomy
impossible
• Low‐risk pancreatic cysts– Pancreatic pseudocysts
– Serous cystadenomas
– Lymphoepithelial cysts
• High‐risk pancreatic cysts– Intraductal papillary mucinous
neoplasm (IPMN)– 30% harbor carcinoma
– Mucinous cystic neoplasm (MCN)

12
CYSTIC LESIONS OF THE PANCREASSerous cystadenoma
Solidpseudopapillaryneoplasm
Mucinous CysticNeoplasm
Intraductal
LOW-RISK PANCREATIC CYSTS
Pseudocyst
papillarymucinous neoplasm
Pancreatic Pseudocyst ‐ FNA
• Collection of amylase‐rich secretions, debris and blood
• Lacks a true epithelial lining
i ll l i h l d b i• Paucicellular smears with granular debris, macrophages, yellow bile/hematoidin pigment and fat necrosis
Pancreatic Pseudocyst
• Fluid is turbid/necrotic• NOT mucinous or gelatinous• Granular background debris• Inflammatory cells• Pigment is important for
diagnosisY ll i t
Cell blocks• Yellow pigment =
bile/hematoidin• Brown pigment =
hemosiderin
13
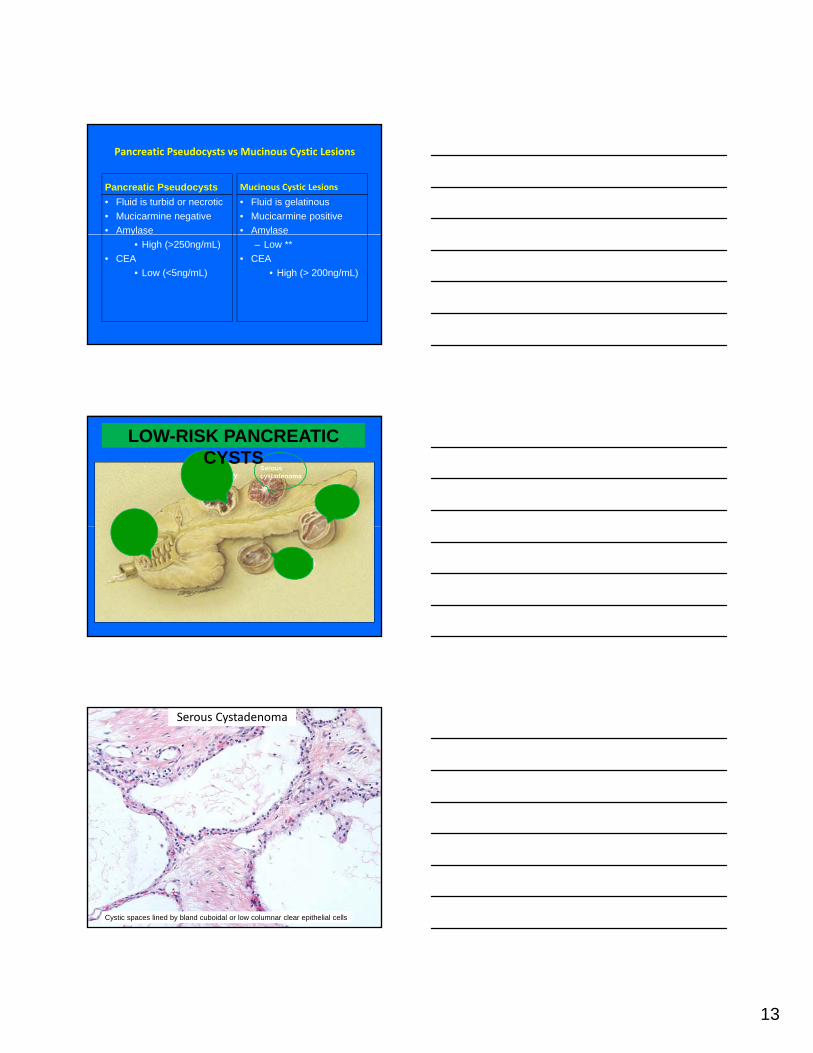
Pancreatic Pseudocysts vs Mucinous Cystic Lesions
Pancreatic Pseudocysts• Fluid is turbid or necrotic• Mucicarmine negative • Amylase
Mucinous Cystic Lesions
• Fluid is gelatinous• Mucicarmine positive• Amylase y
• High (>250ng/mL) • CEA
• Low (<5ng/mL)
y– Low **
• CEA • High (> 200ng/mL)
Serous cystadenoma
Solidpseudopapillaryneoplasm
Mucinous CysticNeoplasm
Intraductal
LOW-RISK PANCREATIC CYSTS
Pseudocyst
papillarymucinous neoplasm
Serous Cystadenoma
Cystic spaces lined by bland cuboidal or low columnar clear epithelial cells

14
Serous Cystadenoma ‐ FNA
• Cyst fluid is usually thin and clear
• Aspirates are often hypocellular
• AE1/AE3 and CA19.9 are +, EMA is focally +
• Amylase and CEA levels are low• Amylase and CEA levels are low
• Mucicarmine negative
• Accuracy of diagnosis by imaging, cytology and chemical analysis is ONLY 20%**
Serous Cystadenoma
Sheets and clusters of cells with clear cytoplasm, defined borders, PAS+ cytoplasm
LOW-RISK PANCREATIC CYSTS
Lymphoepithelial cyst
15
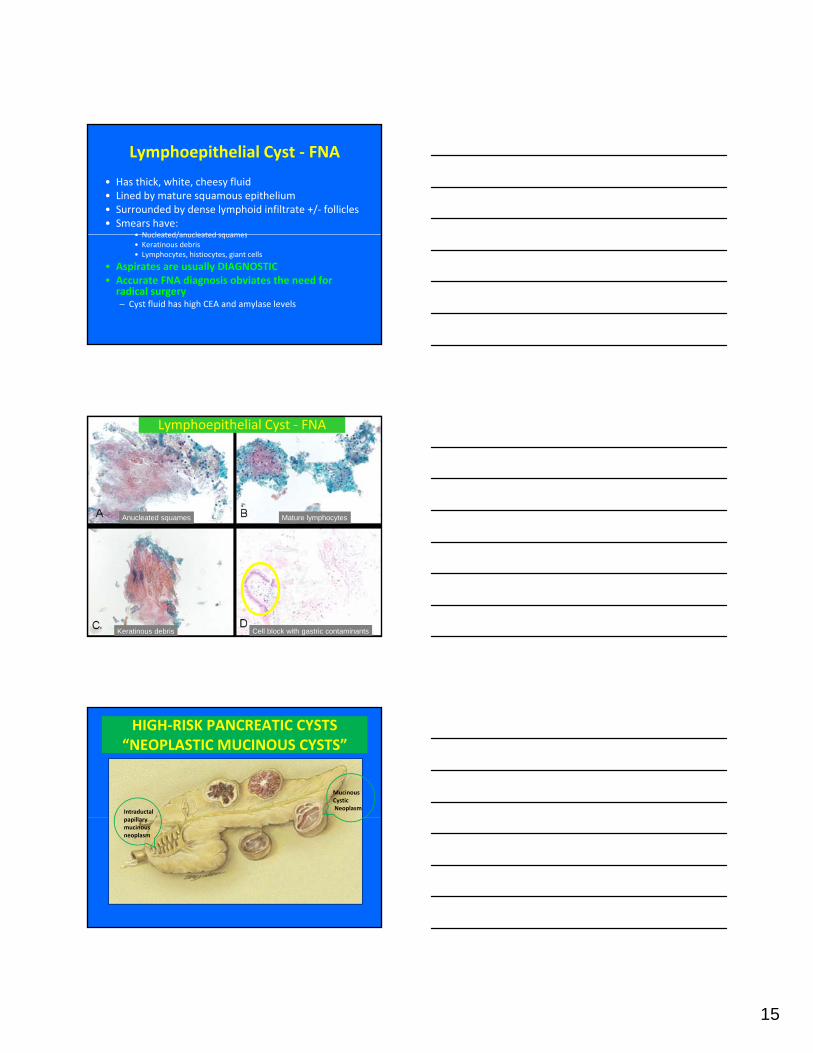
Lymphoepithelial Cyst ‐ FNA
• Has thick, white, cheesy fluid • Lined by mature squamous epithelium• Surrounded by dense lymphoid infiltrate +/‐ follicles• Smears have:
• Nucleated/anucleated squames• Nucleated/anucleated squames• Keratinous debris • Lymphocytes, histiocytes, giant cells
• Aspirates are usually DIAGNOSTIC • Accurate FNA diagnosis obviates the need for radical surgery– Cyst fluid has high CEA and amylase levels
Lymphoepithelial Cyst ‐ FNA
Anucleated squames Mature lymphocytes
Keratinous debris Cell block with gastric contaminants
HIGH‐RISK PANCREATIC CYSTS“NEOPLASTIC MUCINOUS CYSTS”
Mucinous CysticNeoplasmIntraductal
illpapillarymucinous neoplasm

16
NEOPLASTIC MUCINOUS CYSTS
• Mucinous cystic neoplasm (MCN)– Primary mucin‐producing cystic neoplasm – Lined by bland mucin‐filled columnar cells– Has classical sub‐epithelial ovarian‐type ER+, PR + stroma
• Intraductal papillary mucinous neoplasm (IPMN)– Primary mucin‐producing cystic neoplasm – Arises from the main or branch pancreatic ducts– Lined by papillary mucinous epithelium with variable atypia
Key Differences Between the Two Cysts
• MCN– Large, circumscribed, solitary cystic
lesion– Not connected to the main pancreatic
duct or its branches – Because they are not connected to the
main pancreatic duct/branches amylase levels are usually low
– >90% arise in the tail
• IPMN – Diffuse ectasia involving the main
and/or branch pancreatic ducts– Always connected to the main
pancreatic duct or branches – Because they are connected to main
pancreatic duct amylase levels are highin cyst fluid
– >80% arise in the head of the pancreas – Most patients are perimenopausal
females between 40 ‐50 yrs– F : M 20:1 – Has sub‐epithelial ovarian‐type fibrous
stroma– Malignant features include:
• Size >3cm• Thick wall, peripheral calcifications• Intramural mass/nodules
– Most patients are older adults, over the age of 60
– M = F or are slight > females – No sub‐epithelial ovarian‐type stroma
present– Malignant features include:
• Size > 3cm• Dilated main pancreatic duct• Intramural mass/nodules
Cytologic Similarities
• Both IPMN and MCN have abundant thick mucin
• Difficult to express from needle
• Difficult to spread on the slide
• Smear cellularity is variable
Abundant thick colloid-like mucin
Diff‐Quik stainSmear cellularity is variable
• Higher the grade of dysplasia, the greater the cellularity
• Psammomatous calcifications may be seen in IPMN
Pap stain

17
Similarities Between MCN and IPMN
Both contain sheets and clusters ofcolumnar cells with abundant intracytoplasmic mucin
Similarities between MCN and IPMN
The mucin fills the entire cytoplasm and displaces the nucleus peripherally – Note limited nuclear atypia in this example.
NEOPLASTIC MUCINOUS CYSTS
Nuclei are slightly pleomorphic with
Mucin +
coarse chromatin and prominent nucleoli
Macrophages may be present

18
NEOPLASTIC MUCINOUS CYSTS
• Papillary clusters may be seen in IPMN but are not typical in MCN
• Nuclear and architectural atypia can be seen in both IPMN and MCN– Includes hypercellularity
– Nuclear crowding
– Loss of polarity
Papillary structure in an IPMN
Note nuclear atypia with nuclear Crowding and hyperchromasiap y
– Hyperchromasia, pleomorphism
– High N/C ratio and nucleoli
– Single epithelial cells in mucin
• Nuclear atypia is more often seen in IPMN than MCN
Crowding and hyperchromasia
Pancreatic Neoplastic Mucinous Cyst with High‐Grade Dysplasia
Interesting Case - Pancreatic Tail Cyst
19
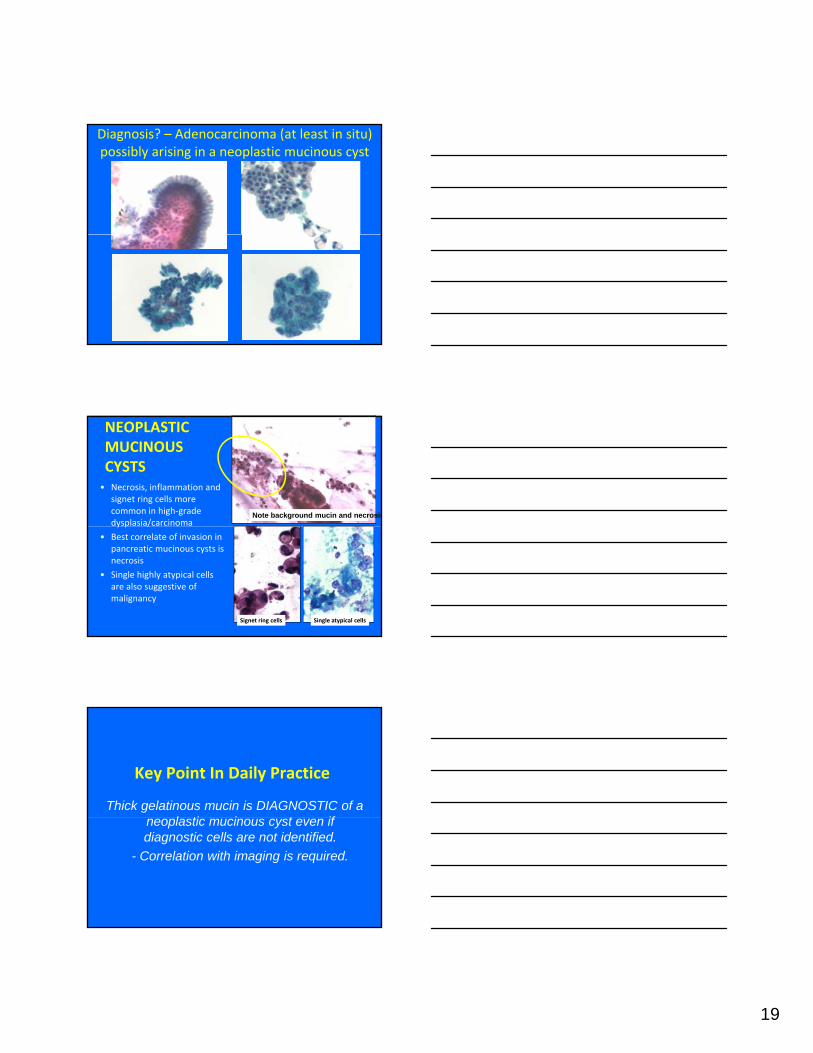
Diagnosis? – Adenocarcinoma (at least in situ) possibly arising in a neoplastic mucinous cyst
NEOPLASTIC MUCINOUS CYSTS• Necrosis, inflammation and
signet ring cells more common in high‐grade dysplasia/carcinoma
Note background mucin and necrosisy p /
• Best correlate of invasion in pancreatic mucinous cysts is necrosis
• Single highly atypical cells are also suggestive of malignancy
Signet ring cells Single atypical cells
Key Point In Daily Practice
Thick gelatinous mucin is DIAGNOSTIC of a l ti i t ifneoplastic mucinous cyst even if
diagnostic cells are not identified.- Correlation with imaging is required.

20
PANCREATIC MUCIN‐PRODUCING CYSTS
• Definitive cytologic distinction between MCN and IPMN is discouraged
• The best diagnosis for such lesions is:• The best diagnosis for such lesions is:– “Neoplastic cells present.”
– “Neoplastic mucinous cyst”
– A comment should be made regarding the presence and grade of cytologic atypia/dysplasia
SOLID PANCREATIC LESIONS
ABRIDGED CLASSIFICATION OF SOLID AND CYSTIC PANCREATIC NEOPLASMS
Gross Configuration Neoplasms %
Solid Neoplasms
Ductal Adenocarcinoma 85%
Pancreatic Neuroendocrine Tumor 3‐4%
Acinar Cell Carcinoma 1‐2%
(Solid‐Pseudopapillary Neoplasm) 1‐2%
Pancreatoblastoma <1%
Cystic True cysts Serous Cystadenoma 1 2%Cystic ‐True cysts Serous Cystadenoma 1‐2%
Mucinous Cystic Neoplasm 1‐2%
Cystic ‐ Intraductal Intraductal Papillary Mucinous Neoplasm 3‐5%
Cystic ‐ DegenerativeSolid‐Pseudopapillary Neoplasm
(Ductal Adenocarcinoma, Acinar Cell Carcinoma, Pancreatic Neuroendocrine Tumor)
Entities in parentheses only rarely exhibit this gross configuration
Modified from Klimstra et al. Archives of Pathology and LaboratoryMedicine 2009; 133(3):454‐64.
21
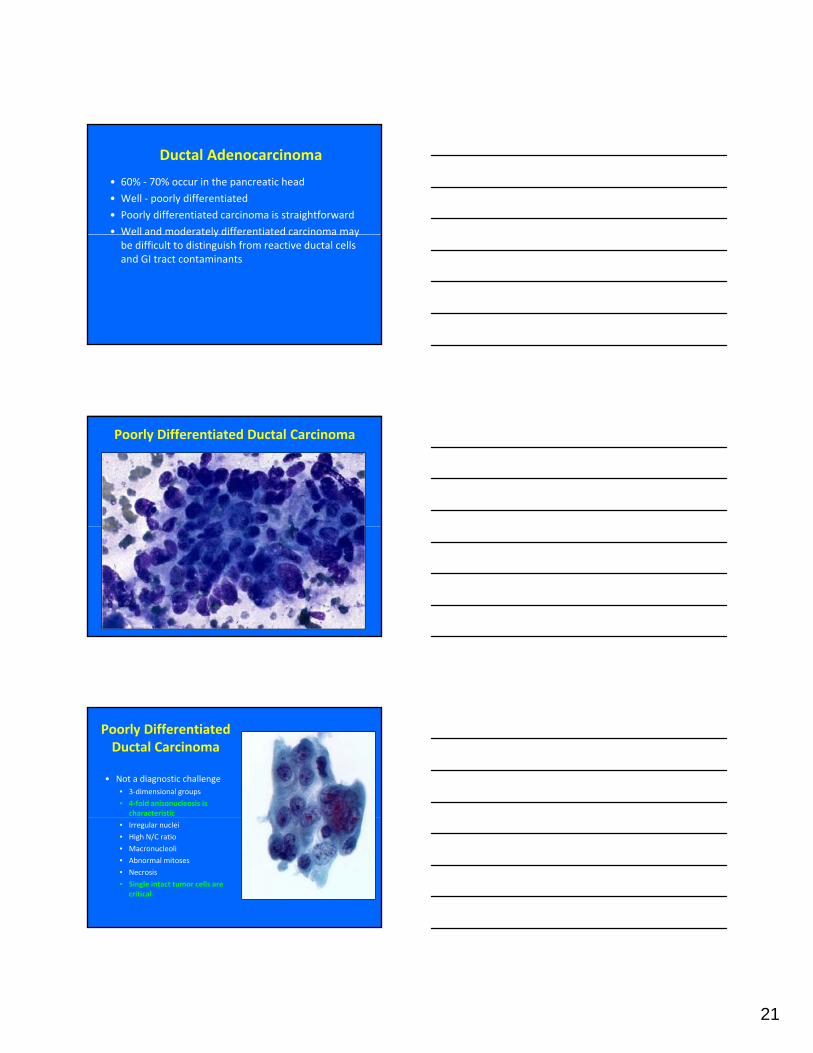
Ductal Adenocarcinoma
• 60% ‐ 70% occur in the pancreatic head
• Well ‐ poorly differentiated
• Poorly differentiated carcinoma is straightforward
• Well and moderately differentiated carcinoma mayWell and moderately differentiated carcinoma may be difficult to distinguish from reactive ductal cells and GI tract contaminants
Poorly Differentiated Ductal Carcinoma
Poorly Differentiated Ductal Carcinoma
• Not a diagnostic challenge• 3‐dimensional groups
• 4‐fold anisonucleosis is characteristic
• Irregular nuclei
• High N/C ratio
• Macronucleoli
• Abnormal mitoses
• Necrosis
• Single intact tumor cells are critical

22
Poorly Differentiated Ductal Adenocarcinoma
3-D crowded groups 4-fold anisonucleosis
Disorganized sheets with hyperchromatic cells with irregular nuclei
MALIGNANT BENIGN
Poorly Differentiated Ductal Adenocarcinoma
Well Differentiated Ductal Carcinoma
• Disorganized sheets similar to normal ductal cells
• Slight nuclear crowding
• “Drunken” honeycomb sheets
• Mild nuclear enlargement• Mild nuclear enlargement
• N/C ratio may remain low
• Anisonucleosis not as pronounced
• Normal pancreatic acini and endocrine cells are rare to absent

23
Interesting Case ‐ FNAB Pancreatic Mass
Slightly “drunken” honeycomb sheet and cellular dissociation
Irregular nuclear contours, hypochromasiaand prominent nucleoli
An extremely bland-appearing well differentiated adenocarcinoma with voluminous foamy cytoplasm
Cells have abundant mucinous vacuoles and very bland almost benign cytologic appearance
Closer examination revealed single intact malignant cells with nuclear irregularity
Diagnosis?
Foamy Gland Variant of Well Differentiated Ductal Adenocarcinoma

24
Foamy Gland Ductal Adenocarcinoma
Ductal Adenocarcinoma• Immunohistochemical markers:
– CK7, CK8, CK18, CK19
– CA 125
– DUPAN‐2 (pancreatic cancer‐associated antigen)
– Mucin glycoproteins are variably expressed • MUC1, 3, 4 and MUC5AC
• Molecular markers:– K‐rasmutation
– Loss of heterozygosity (LOH) mutation
– p53 mutation
Other Variants of DuctalCarcinomaCarcinoma

25
Squamous Cell Carcinoma of Pancreas
• Extremely rare variant of pancreatic carcinoma• Incidence ranges from 0.5% ‐ 5%
• Only diagnose after metastasis has been excluded and after a glandular component has been excluded (i.e. adenosquamous carcinoma)
• Similar biologic behavior to ductal adenocarcinomag
Squamous Cell Carcinoma of Pancreas
Malignant squamous cells are admixed with benign pancreatic ductal cellsThis was a case of primary pancreatic squamous cell carcinoma
Squamous Cell Carcinoma of Pancreas
• Most cases represent metastases – From the lung, followed by
cervix then esophagus
• Correlation with clinical information is paramount to accurate diagnosis

26
Osteoclastic‐ Giant Cell Carcinoma of Pancreas• Extremely rare primary malignant pancreatic tumor
• Associated with ductal adenocarcinoma (40% of cases)• May be focal or predominant
• Prognosis is controversial:• Some say not as dismal as ductal carcinoma
• Others say more aggressive than ductal carcinoma• Others say more aggressive than ductal carcinoma
• Mean survival ≤ 12 months – related to quantity of ductal carcinoma
Osteoclastic‐ Giant CellCarcinoma of Pancreas
• 3 cell types:– 1. Benign‐appearing osteoclast‐
like giant cells– CD68 +, Cytokeratin ‐
– 2 Pleomorphic giant carcinoma
3
2. Pleomorphic giant carcinoma cells
– CD68 ‐, Cytokeratin –– 3. Small ovoid‐spindle histiocyte‐
like carcinoma cells – CD68 +– Cytokeratin +/‐, EMA +/‐
– P53 +, ki‐67 +
1 2
Osteoclastic‐Giant Cell Carcinoma of Pancreas
Conventional ductal adenocarcinoma –same case Cell block with benign giant cells
Benign osteoclast‐like giant cellsAll 3 cell types are represented

27
Mucinous “Colloid” Carcinoma of Pancreas
• Accounts for <1% of pancreatic malignancies
• Commonly associated with IPMN
• Clusters and singly dispersed malignant cells indispersed malignant cells in thick colloid‐like mucin
• Signet ring cells are present• Cytologic diagnosis is
straightforward
Mucinous “Colloid” Carcinoma of PancreasMucinous “Colloid” Carcinoma of Pancreas
Note clusters of slightly pleomorphic, hyperchromatic malignant cells in thick mucin
Chronic Pancreatitis• Can present as solid
pancreatic head lesion• Distinction from carcinoma
challenging on radiology• Reactive ductal cells may
be challengingLymphohistiocytic infiltrates
Stromal fragmentsFat necrosis

28
Chronic Pancreatitis• Atypical reactive ductal cells can be confused with ductal carcinoma
• Distinction between the Reactive ductal cells2 may require immunohistochemistry
Reactive ductal cells
FNA: “Atypical Cells Present”Reactive Ductal Cells vs. Ductal Carcinoma
Note the sheet‐like arrangement, round nuclear contours and similarity between cells.
This is marked reactive atypia
Benign ductal cells – in honeycomb sheets
Drunken HoneycombSheet
Well differentiated ductal carcinomaAbnormal mitosis
Reactive ductal cells – in honeycomb sheetsWell differentiated ductal carcinoma

29
Immunohistochemical Distinction between Adenocarcinoma,
Chronic Pancreatitis and GI Tract Contaminants
Atypical Ductal Cells
SMAD4 p53 CDX‐2
Ductal Adenocarcinoma ‐ + ‐Chronic pancreatitis + ‐ ‐GI tract contaminants + ‐ +SMAD4: Belongs to the SMAD family of cell signaling proteins: It is a homologue of the Drosophila protein: “Mothers against decapentaplegic“ and is also known as DPC4 (Deletion target in pancreatic carcinoma 4); CDX-2, caudal-related homeobox 2 .
Key Point In Daily Practice
• If atypical glandular cells are present and one cannot determine whether they are neoplastic or reactive the best diagnosis is:
• “Atypical cells present” with COMMENT– Correlate clinically and radiologically
Autoimmune Pancreatitis
• “Lymphoplasmacytic sclerosing pancreatitis”
• Can produce a mass effect in pancreas
• Associated with RA IBDAssociated with RA, IBD, primary sclerosing cholangitis
• ↑ serum IgG4 antibody• Antinuclear antibody (ANA) +
• Rheumatoid factor +

30
Autoimmune Pancreatitis (AIP)
• Few reports on cytologic features
• Range from paucicellular to hypercellular aspirates
• Contain stromal fragments• Contain stromal fragments, lympho‐plasmacytic infiltrate, eosinophils
• Minimal ductal epithelium
• IgG4 immunostain is positive in plasma cells
Pancreatic Neuroendocrine Tumors• Range from well ‐ poorly differentiated
• Well differentiated pancreatic neuroendocrine tumor (Pan NET) is the most common
• Poorly differentiated neuroendocrine carcinomaPoorly differentiated neuroendocrine carcinoma (Pan NEC) is extremely rare
• Small cell carcinoma
• Large cell neuroendocrine carcinoma
Well DifferentiatedPancreatic Neuroendocrine Tumor– Hypercellular smears
– Uniform, dyscohesive cells
– Fragile, easily stripped cytoplasm
– Often have eccentric nuclei →plasmacytoid appearance
Well differentiated NET
Plasmacytoid cells– May resemble lymphocytes
– Classical “salt‐n‐pepper” chromatin on Pap/H&E stain
– Indistinct nucleoli usually
– May have prominent nucleoli– Variable nuclear atypia
Plasmacytoid cells
NET with prominent nucleoli

31
Well Differentiated Pancreatic Neuroendocrine Tumor
D
Plasmacytoid cells
Pseudorosettes on cell block
Salt-n-pepper chromatin, small nucleoli
Prominent nucleoli and pseudoacini
Well Differentiated Pancreatic NET
Pseudorosettes are visible both on smear and cell block
Well Differentiated Pancreatic Neuroendocrine Tumor - Pleomorphic Variant
Single plasmacytoid cells and cells with focal degenerative “endocrine” atypia

32
Pancreatic Neuroendocrine Tumor• Immunohistochemistry
• Positive for neuroendocrine
markers
– Synaptophysin, chromogranin, CD56,
CD57
• Positive for keratin, CAM5.2
Poorly Differentiated Pancreatic Neuroendocrine Carcinoma (NEC)
• Extremely rare
• Include small cell and large cell NEC
• Rule out metastasis before making this diagnosis
• Small cell carcinoma resembles small cell carcinoma of the lung– Molding, salt and pepper chromatin,
crush artifact
• Large cell NEC– Resembles poorly differentiated carcinoma
– Expresses neuroendocrine markers
Small cell carcinoma
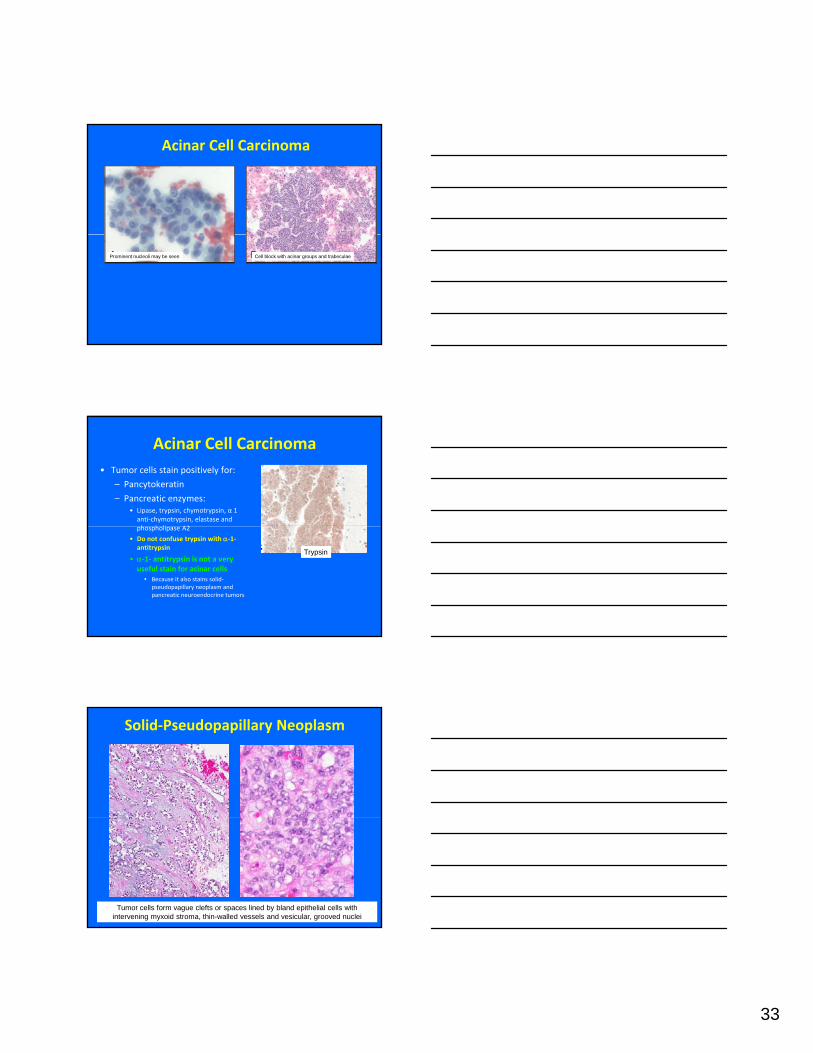
Acinar Cell Carcinoma
Hypercellular smears Acinar formation and naked nuclei
Abundant granular cytoplasmCells have basophilic cytoplasm,Nuclei with fine to coarse chromatin,inconspicuous nucleoli
Normal pancreatic acini
33
Acinar Cell Carcinoma
Prominent nucleoli may be seen Cell block with acinar groups and trabeculae
Acinar Cell Carcinoma• Tumor cells stain positively for:
– Pancytokeratin
– Pancreatic enzymes:• Lipase, trypsin, chymotrypsin, α 1 anti‐chymotrypsin, elastase and h h li A2phospholipase A2
• Do not confuse trypsin with α‐1‐antitrypsin
• α‐1‐ antitrypsin is not a very useful stain for acinar cells
• Because it also stains solid‐pseudopapillary neoplasm and pancreatic neuroendocrine tumors
Trypsin
Solid‐Pseudopapillary Neoplasm
Tumor cells form vague clefts or spaces lined by bland epithelial cells with intervening myxoid stroma, thin-walled vessels and vesicular, grooved nuclei

34
Solid‐Pseudopapillary Neoplasm
– Rare low‐ grade solid and cystic pancreatic
– Usually arises in the pancreatic tail
– Almost exclusively in women (F:M 9:1)
– Third decade (mean age 28 years) or adolescence
– Cytologic features are distinctive
– Accurate diagnosis often made before resection
Solid‐Pseudopapillary Neoplasm
Monomorphic small cells with high N/C Complex branching papillae gratio, fine chromatin, nuclear grooves
g
Papillary fronds with central myxoid stroma (on Diff Quik stain) and blood vessel (H&E)
Solid-Pseudopapillary Neoplasm
Fibrovascular core
Vesicular nuclei with open, fine, powdery chromatin
Nuclear grooves

35
Solid‐Pseudopapillary Neoplasm
• Immunohistochemistry is characteristic and diagnostic• Positive for vimentin:
• Frequently negative for cytokeratin
• Positive for:• Neuron specific enolase
• CD56 (variable)
• CD10
• β‐catenin (nuclear)
• Progesterone receptor
• α ‐1‐ antitrypsin is not helpful because it is positive in SPN, acinar cell carcinoma and pancreatic NETs
Pancreatic Neuroendocrine Tumor (NET) vs Solid‐Pseudopapillary Neoplasm (SPN)
NET SPN
Fine, open chromatinFibrovascular core Salt-n-pepper chromatin
Secondary Pancreatic Neoplasms• Various tumors may metastasize to the pancreas
• Lung (small cell and squamous cell carcinoma)
• Breast
• Kidney
L h• Lymphoma
• Less commonly:• Ovary, colon and stomach
• History of previous malignancy and immunohistochemistry are helpful in diagnosis

36
SUMMARY ‐ PANCREATIC FNAB
– Cytologic evaluation of pancreatic lesions is complex
– Knowledge of types and location of the most common solid and cystic lesions is helpful in diagnosis
– Correlation with clinical, imaging data is paramount
– Cytopathologist /cytotechnologist’s presence during immediate evaluation improves adequacy and diagnostic yield
– Be mindful that chronic pancreatitis and GI tract contaminants (in EUS‐FNAB) may simulate carcinoma
References• 1. Shen j. Kindelberger dw Pancreas and biliary tree. In: Cibas ES DB, editors. Cytology: Diagnostic Principles and Clinical Correlates. 3rd Ed.
Philadelphia: Saunders, 2009: 385‐402.• 2. PitmanM. Pancreas. In: MSidawy, editor. Fine needle aspiration cytology. 1st ed, Foundations in Diagnostic Pathology: Churchhill
Livingstone Elsevier; 2007 p251‐298.• 3. Centeno BA. Fine needle aspiration biopsy of the pancreas. Clin Lab Med 1998;18(3):401‐27, v‐vi.• 4. Ekberg O, Bergenfeldt M, Aspelin P, Genell S, Lindholm K, Nilsson P, Sigurjonsson S. Reliability of ultrasound‐guided fine‐needle biopsy of
pancreatic masses. Acta Radiol 1988;29(5):535‐9.• 5. Erickson RA, Garza AA. Impact of endoscopic ultrasound on the management and outcome of pancreatic carcinoma. Am J Gastroenterol
2000;95(9):2248‐54.• 6. Pitman MB, Deshpande V. Endoscopic ultrasound‐guided fine needle aspiration cytology of the pancreas: a morphological and multimodal
approach to the diagnosis of solid and cystic mass lesions. Cytopathology 2007;18(6):331‐47.• 7. Mitsuhashi T, Ghafari S, Chang CY, Gu M. Endoscopic ultrasound‐guided fine needle aspiration of the pancreas: cytomorphological
evaluation with emphasis on adequacy assessment, diagnostic criteria and contamination from the gastrointestinal tract. Cytopathology 2006;17(1):34‐41.
• 8. Gonzalez Obeso E, Murphy E, Brugge W, Deshpande V. Pseudocyst of the pancreas: the role of cytology and special stains for mucin. Cancer Cytopathol 2009;117(2):101‐7.
• 9. Brandt KR, Charboneau JW, Stephens DH, Welch TJ, Goellner JR. CT‐ and US‐guided biopsy of the pancreas. Radiology 1993;187(1):99‐104.• 10 David O Green L Reddy V Kluskens L Bitterman P Attal H Prinz R Gattuso P Pancreatic masses: a multi institutional study of 364 fine• 10. David O, Green L, Reddy V, Kluskens L, Bitterman P, Attal H, Prinz R, Gattuso P. Pancreatic masses: a multi‐institutional study of 364 fine‐
needle aspiration biopsies with histopathologic correlation. Diagn Cytopathol 1998;19(6):423‐7.• 11. Di Stasi M, Lencioni R, Solmi L, Magnolfi F, Caturelli E, De Sio I, Salmi A, Buscarini L. Ultrasound‐guided fine needle biopsy of pancreatic
masses: results of a multicenter study. Am J Gastroenterol 1998;93(8):1329‐33.• 12. Robins DB, Katz RL, Evans DB, Atkinson EN, Green L. Fine needle aspiration of the pancreas. In quest of accuracy. Acta Cytol 1995;39(1):1‐
10.• 13. Levin DP, Bret PM. Percutaneous fine‐needle aspiration biopsy of the pancreas resulting in death. Gastrointest Radiol 1991;16(1):67‐9.• 14. Klimstra DS, Pitman MB, Hruban RH. An algorithmic approach to the diagnosis of pancreatic neoplasms. Arch Pathol Lab Med
2009;133(3):454‐64.• 15. Belsley NA, Pitman MB, Lauwers GY, Brugge WR, Deshpande V. Serous cystadenoma of the pancreas: limitations and pitfalls of endoscopic
ultrasound‐guided fine‐needle aspiration biopsy. Cancer 2008;114(2):102‐10.• 16. Jimenez‐Heffernan JA, Vicandi B, Lopez‐Ferrer P, Gonzalez‐Peramato P, Perez‐Campos A, Viguer JM. Fine needle aspiration cytology of
endocrine neoplasms of the pancreas. Morphologic and immunocytochemical findings in 20 cases. Acta Cytol 2004;48(3):295‐301.• 17. Gupta RK, Lallu S, Delahunt B. Fine‐needle aspiration cytology of metastatic clear‐cell renal carcinoma presenting as a solitary mass in the
head of the pancreas. Diagn Cytopathol 1998;19(3):194‐7.• 18. Le Borgne J, de Calan L, Partensky C. Cystadenomas and cystadenocarcinomas of the pancreas: a multiinstitutional retrospective study of
398 cases. French Surgical Association. Ann Surg 1999;230(2):152‐61.• 19. Stelow EB, Bardales RH, Shami VM, Woon C et al. Cytology of pancreatic acinar cell carcinoma. Diagn Cytopathol. 2006 May;34(5):367‐
72. • 20. Cohen MB, Egerter DP, Holly EA et al. Pancreatic adenocarcinoma: regression analysis to identify improved cytologic criteria. Diagn
Cytopathol 1991, 7:341‐345• 21. Mitchell ML, Carney CN. Cytologic criteria for the diagnosis of pancreatic carcinoma. Am J Clin Pathol 1985, 83:171‐176• 22. Robins DB, Katz RL, Evans DB et al. Fine needle aspiration of the pancreas. In quest of accuracy. Acta Cytol 1995. 39:1‐10.
QUESTIONS?