504 coincidental multiple asymptomatic intracranial...
TRANSCRIPT

504 Coincidental Multiple Asymptomatic IntracranialAneurysms and Symptomatic Carotid Stenosis
ROBERT D. SHOUMAKER, M.D.,* WILBUR S. AVANT, M.D.,f
AND MAJOR GILBERT H. COHEN, M.C.J
SUMMARY A patient experiencing transient cerebral ische-mic attacks (TIAs) was studied angiographically and found tohave a symptomatic stenosis of the appropriate internal carotid
artery (ICA) and three asymptomatic intracranial aneurysms. Atherapeutic approach to this type of problem is discussed in thisarticle.
IN PATIENTS undergoing cerebral angiographical ex-amination for evaluation of occlusive cerebrovascular dis-ease, about 5% will show an unexpected aneurysm.1'2 Thenumber with multiple aneurysms is difficult to ascertainfrom the literature, but must be considerably less. Thefollowing case illustrates the rare association of threeasymptomatic intracranial aneurysms and a symptomaticcarotid stenosis demonstrated on angiographical evalua-tion.
Case Report
A 67-year-old white woman gave a history of a five-minute episode of left arm numbness occurring three monthsprior to admission. On the day of admission, April 3, 1974,she noted the onset of complete numbness and slightweakness of her left arm and leg lasting about 45 minutes.By the time she was hospitalized, the symptoms had nearlyresolved.
She had a history of hypertension for at least 20 years,which had been under fair control with multiple medica-tions. She also had chronic bronchitis, headaches, and oc-casional depression and was being treated for hypo-thyroidism. There was no history of diabetes mellitus,angina or prior neurological deficits. Family history wasnegative for any neurological disorders.
Examination on admission revealed an alert apprehen-sive woman with a blood pressure of 160/92 mm Hg, regularpulse of 96 per minute. Funduscopic examination showedmild arteriolar narrowing. No hemorrhages, exudates orbright plaques were seen. Ophthalmodynamometry showeda 25% difference in systolic pressures, with the left greaterthan the right. Her neck was supple and bruits were heardover both carotids, most prominent at the midcervicalregion, right greater than the left. Cardiac examinationsuggested left ventricular enlargement but no murmurs orgallops were heard. The rest of the general examination wasnormal. Neurological examination was normal except forsome extinction of the left arm with two-point simultaneousstimulation testing and slight downward drift of her left armwhen extended. No pathological reflexes were elicited.
Complete blood count, urinalysis, blood chemistries, par-tial thromboplastin time, and prothrombin time were allnormal. Cholesterol was 200 mg/dl, and triglyceride was235 mg/dl. Arterial gases showed a pH of 7.44, Po2 of 81
•Department of Neurology, University of Nebraska Medical Center, 42ndand Dewey Avenue, Omaha, Nebraska 68105. tOak Hills Medical Building,Suite 816, San Antonio, Texas 78229. ^Department of Radiology, WilfordHall, USAF Medical Center, Lackland AFB, Texas 78236.
mm Hg, and Pco2 of 32 mm Hg. Chest and skull x-rays werenormal. EKG was suggestive of an old anteroseptal myo-cardial infarct. A radioisotope brain scan and flow studywith 99mtechnetium was normal. During the 12 hours afteradmission, the patient had two more episodes of left armand leg numbness with minimal weakness lasting 20minutes. A lumbar puncture showed an opening pressure of175 mm H2O, clear fluid with two mononuclear cells and noRBCs; glucose and protein were normal. She was treatedwith intravenous heparin, but had two more episodes ofsimilar duration during the next 18 hours. Subsequently, sheunderwent cerebral angiography via transfemoral arterycatheterization. Radiography revealed a 90% stenosis of theright internal carotid artery. In addition, aneurysms of theright middle cerebral artery, right anterior cerebral artery(fig. 1) and left posterior cerebral artery (fig. 2) were noted.There was also a 30% stenosis of the left internal carotidartery at the bifurcation.
The patient then underwent a right carotid endarterec-tomy which revealed an estimated 95% stenosis of the inter-nal carotid artery. Neurosurgical consultants felt that be-cause of the patient's multiple medical problems she was nota good candidate for intracranial surgery at that time. Herpostoperative course was uneventful and ophthalmodyna-mometry revealed equal pressures. She was discharged onacetylsalicylic acid and dipyridamole (Persantin), in additionto her antihypertensive and thyroid medications. Her courseremained stable and she was readmitted seven months afterher surgery for re-evaluation. Cerebral angiography wasperformed via transfemoral catheterization and there was nomeasurable change in the size of the aneurysms. The rightinternal carotid artery was patent; however, the stenosis inthe left internal carotid artery had progressed. A left carotidendarterectomy was successfully performed. Because no in-crease in the size of the aneurysms was noted, intracranialsurgery was not recommended.
Discussion
In a review of the literature by Portnoy and Avellanosa3
on the association of extracranial carotid stenosis or occlu-sion and intracranial aneurysm, no cases showing theassociation with multiple aneurysms were identified. Theyreported one case with a right internal carotid aneurysm andleft internal carotid artery stenosis. Their surgical approachwas identical to that advocated by Pool and Potts,4 i.e., end-arterectomy of the stenotic vessel followed by surgical treat-ment of the aneurysm. Fields and Weibel6 briefly reportedtwo similar cases of ipsilateral symptomatic carotid stenosiswith incidental single intracranial aneurysm, in which they
by guest on June 11, 2018http://stroke.ahajournals.org/
Dow
nloaded from
MULTIPLE ASYMPTOMATIC INTRACRANIAL ANEURYSMS/S/iowma)ter et al. SOS
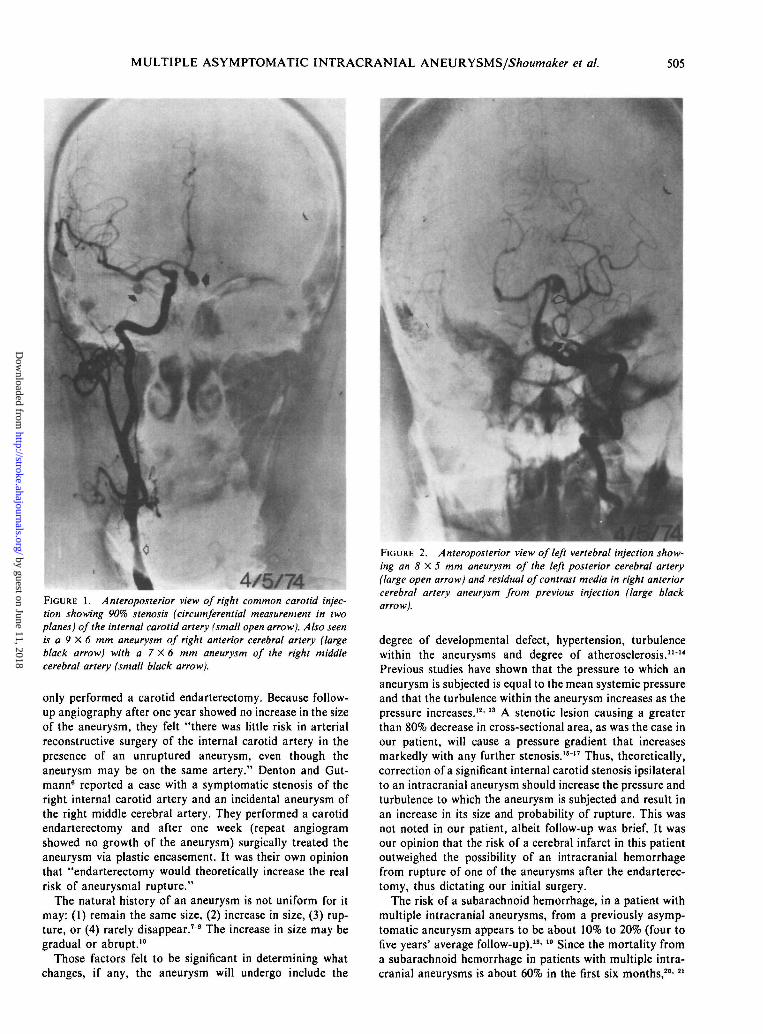
4/5/74FIGURE 1. Anteroposterior view of right common carotid injec-tion showing 90% stenosis (circumferential measurement in twoplanes) of the internal carotid artery (small open arrow). Also seenis a 9 X 6 mm aneurysm of right anterior cerebral artery (largeblack arrow) with a 7 X 6 mm aneurysm of the right middlecerebral artery (small black arrow).
only performed a carotid endarterectomy. Because follow-up angiography after one year showed no increase in the sizeof the aneurysm, they felt "there was little risk in arterialreconstructive surgery of the internal carotid artery in thepresence of an unruptured aneurysm, even though theaneurysm may be on the same artery." Denton and Gut-mann6 reported a case with a symptomatic stenosis of theright internal carotid artery and an incidental aneurysm ofthe right middle cerebral artery. They performed a carotidendarterectomy and after one week (repeat angiogramshowed no growth of the aneurysm) surgically treated theaneurysm via plastic encasement. It was their own opinionthat "endarterectomy would theoretically increase the realrisk of aneurysmal rupture."
The natural history of an aneurysm is not uniform for itmay: (1) remain the same size, (2) increase in size, (3) rup-ture, or (4) rarely disappear.79 The increase in size may begradual or abrupt.10
Those factors felt to be significant in determining whatchanges, if any, the aneurysm will undergo include the
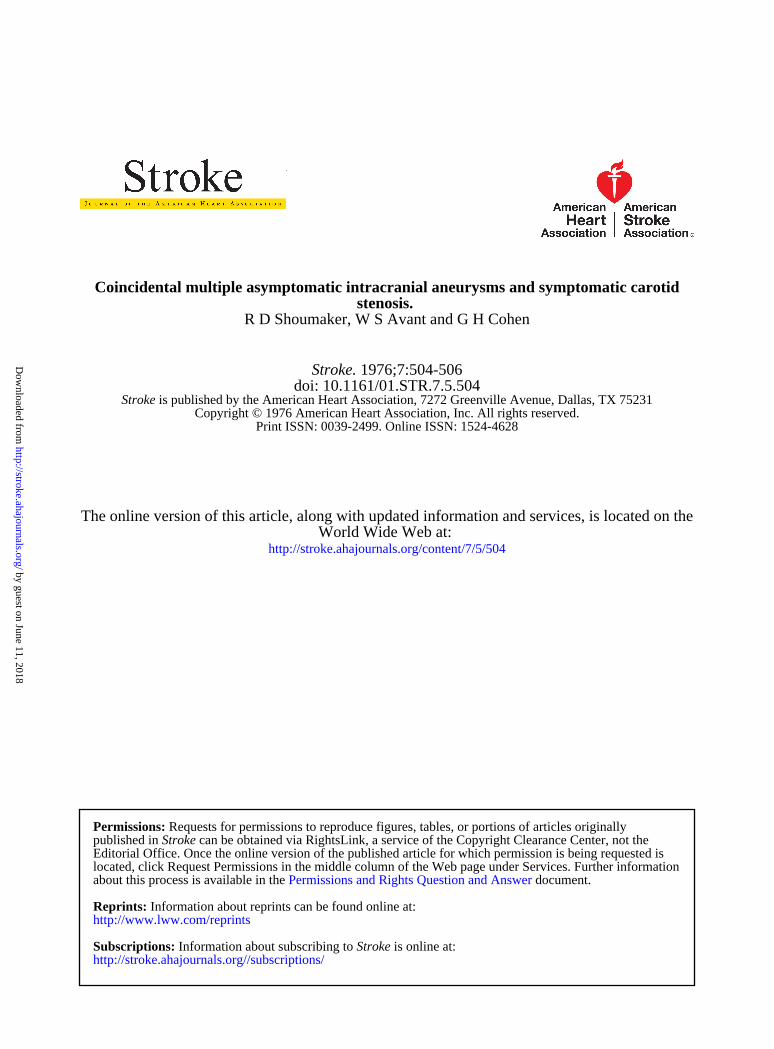
FIGURE 2. Anteroposterior view of left vertebral injection show-ing an 8 X 5 mm aneurysm of the left posterior cerebral artery(large open arrow) and residual of contrast media in right anteriorcerebral artery aneurysm from previous injection (large blackarrow).
degree of developmental defect, hypertension, turbulencewithin the aneurysms and degree of atherosclerosis.11"14
Previous studies have shown that the pressure to which ananeurysm is subjected is equal to the mean systemic pressureand that the turbulence within the aneurysm increases as thepressure increases.12'13 A stenotic lesion causing a greaterthan 80% decrease in cross-sectional area, as was the case inour patient, will cause a pressure gradient that increasesmarkedly with any further stenosis.15"17 Thus, theoretically,correction of a significant internal carotid stenosis ipsilateralto an intracranial aneurysm should increase the pressure andturbulence to which the aneurysm is subjected and result inan increase in its size and probability of rupture. This wasnot noted in our patient, albeit follow-up was brief. It wasour opinion that the risk of a cerebral infarct in this patientoutweighed the possibility of an intracranial hemorrhagefrom rupture of one of the aneurysms after the endarterec-tomy, thus dictating our initial surgery.
The risk of a subarachnoid hemorrhage, in a patient withmultiple intracranial aneurysms, from a previously asymp-tomatic aneurysm appears to be about 10% to 20% (four tofive years' average follow-up).18'19 Since the mortality froma subarachnoid hemorrhage in patients with multiple intra-cranial aneurysms is about 60% in the first six months,20'21
by guest on June 11, 2018http://stroke.ahajournals.org/
Dow
nloaded from

506 STROKE VOL. 7, No. 5, SEPTEMBER-OCTOBER 1976
then the probability of a fatal hemorrhage in the patient withasymptomatic aneurysms should be around 6% to 12%.Thus, any proposed elective surgical procedure for thesepatients should have a mortality risk less than 6% to 12%.Whereas the surgical approach to multiple asymptomaticaneurysms has tended to be relatively conservative,18- "•"others have taken a more aggressive approach.19'23> M If thepatient is properly selected (accessibility and size of theaneurysms; patient's age and neurological, mental andphysical condition; patient's informed consent), and if theexperience and skill of the neurosurgeon are taken into con-sideration, the mortality rate from elective surgery can beless than that of the nonsurgically treated patient.19' M
A patient with symptomatic internal carotid arterystenosis and asymptomatic single or multiple aneurysmsrepresents a therapeutic dilemma. Based on a review of theliterature, this group of patients should first undergo acarotid endarterectomy if clinically and angiographically in-dicated.25' 26 Subsequently, the course is not as certain, but ifall of the very selective criteria are met, the use of one ormore elective intracranial surgical procedure(s) on theaneurysm(s) should be considered. If the patient does notmeet all the criteria but is still a surgical candidate, heshould be followed with angiograms every 6 to 12 months. Ifan increase in the size of the aneurysm(s) is documented,elective intracranial surgery should be reconsidered.
References1. Baker HL: Medical and surgical care of stroke. Circulation 32: 559-562
(Oct) 19652. Silverstein A: Arteriography of stroke. Arch Neurol 12: 387-389 (Apr)
19653. Portnoy HD, Avellanosa A: Carotid aneurysm and contralateral carotid
stenosis with successful surgical treatment of both lesions. J Neurosurg32: 476-482 (Apr) 1970
4. Pool JL, Potts DG: Aneurysms and Arteriovenous Anomalies of theBrain: Diagnosis and Treatment. New York, Harper and Row, 1965
5. Fields WS, Weibel J: Coincidental internal carotid stenosis and intra-cranial saccular aneurysm. Trans Am Neurol Assoc 95: 237-238 (Jun)1970
6. Denton IC, Gutmann L: Surgical treatment of symptomatic carotidstenosis and asymptomatic ipsilateral intracranial aneurysm. JNeurosurg 38: 662-665 (May) 1973
7. Bjorkesten G, Troupp H: Changes in the size of intracranial arterialaneurysms. J Neurosurg 19: 583-588 (Jul) 1962
8. Mount LA, Taveras JM: The results of surgical treatment of intra-cranial aneurysms as demonstrated by progress arteriography. JNeurosurg 13: 618-626 (Dec) 1956
9. Young B, Meacham WF, Allen JH: Documented enlargement and rup-ture of a small arterial sacculation. J Neurosurg 34: 814-817 (Jun) 1971
10. du Boulay GH: Some observations on the natural history of intracranialaneurysms. Br J Radiol 38: 721-757 (Oct) 1965
11. Crawford T: Some observations on the pathogenesis and natural historyof intracranial aneurysms. J Neurol Neurosurg Psychiat 22: 259-266(Nov) 1959
12. Ferguson GG: Turbulence in human intracranial saccular aneurysms. JNeurosurg 33: 485-497 (Nov) 1970
13. Ferguson GG: Direct measurement of mean and pulsatile blood pressureat operation in human intracranial saccular aneurysms. J Neurosurg 36:560-563 (May) 1972
14. Sahs AL: Observations on the pathology of saccular aneurysms. JNeurosurg 24: 792-806 (Apr) 1966
15. Berguer R, Hwang NHC: Critical arterial stenosis: A theoretical and ex-perimental solution. Ann Surg 180: 39-50 (Jul) 1974
16. Brice JG, Dowsett DJ, Lowe RD: Hemodynamic effects of carotid arterystenosis. Br Med J 2: 1363-1366 (Nov) 1964
17. Delin NA, Ekestrom S, Telenius R: Relation of degree of internal carotidartery stenosis to blood flow and pressure gradient. Invest Radiol 3:337-344 (Sep-Oct) 1968
18. Heiskanen O, Marttila I: Risk of rupture of a second aneurysm inpatients with multiple aneurysms. J Neurosurg 32: 295-299 (Mar) 1970
19. Mount LA, Brisman R: Treatment of multiple intracranial aneurysms. JNeurosurg 35: 728-730 (Dec) 1971
20. Locksley HB: Report on the cooperative study of intracranial aneurysmsand subarachnoid hemorrhage; natural history of subarachnoid hemor-rhage, intracranial aneurysms and arteriovenous malformations. JNeurosurg 25: 321-368 (Sep) 1966
21. McKissock W, Richardson A, Walsh L, et al: Multiple intracranialaneurysms. Lancet 1: 623-626 (Mar) 1964
22. Paterson A, Bond MR: Treatment of multiple intracranial arterialaneurysms. Lancet 1: 1302-1304 (Jun) 1973
23. Moyes PD: Surgical treatment of multiple aneurysms and of incidentallydiscovered unruptured aneurysms. J Neurosurg 35: 291-295 (Sep) 1971
24. Stroobandt G, Cornelis G, Tauvoy Ch: Multiple intracranial aneurysms:Evolution and orientation of the surgical treatment. Acta Neurol Belg 73:298-310 (Sep-Oct) 1973
25. Taylor GW, Lumley JSP: Arterial surgery for stroke patients. Br J HospMed 10: 269-277 (Sep) 1973
26. Grindal AB, Toole JF: Surgical treatment of carotid and vertebral arterydisease. Ann Intern Med 81: 647-649 (Nov) 1974
by guest on June 11, 2018http://stroke.ahajournals.org/
Dow
nloaded from
R D Shoumaker, W S Avant and G H Cohenstenosis.
Coincidental multiple asymptomatic intracranial aneurysms and symptomatic carotid
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1976 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.7.5.504
1976;7:504-506Stroke.
http://stroke.ahajournals.org/content/7/5/504World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theStrokepublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on June 11, 2018http://stroke.ahajournals.org/
Dow
nloaded from