6 th international pediatric continuos renal replacement
TRANSCRIPT

1
6 th International Pediatric Continuos Renal Replacement Therapy (pCRRT) Conference
Rome, 8-10 April 2010
Sepsis and AKI
Isabella Guzzo
Department of Nephrology and Urology

2
AKI definition
More than 30 AKI definitions in published literature
hampers comparisons of studies limits generalization of data from
single center studies prevents patients stratification
Akcan-Arikan A. Kidney international 2007; 71: 1028-1035

3
AKI RIFLE Criteria: ADQI II
Bellomo R et al. Crit Care 2004; 8: R204-212

4
Modified RIFLE criteria in critically ill children with acute kidney injury
Estimated CCl Urine output
• Risk eCCl decrease by 25% <0.5 ml/Kg/h for 8 h• Injury eCCl decrease by 50% <0.5 ml/Kg/h for 16 h• Failure eCCl decrease by 75% or <0.3 ml/Kg/h for 24 h or anuric for 12h eCCl <35 ml/min/1.73 m2• Loss persistent failure >4 weeks• End end-stage renal disease
Stage (persistent failure >3 months)
150 pts 82% (n=123) AKI by pRIFLE 18% (n=27) no AKI48.8%(n=60) R26% (n=32) I25.2% (n=31) F
Akcan-Arikan A. Kidney international 2007; 71: 1028-1035
5
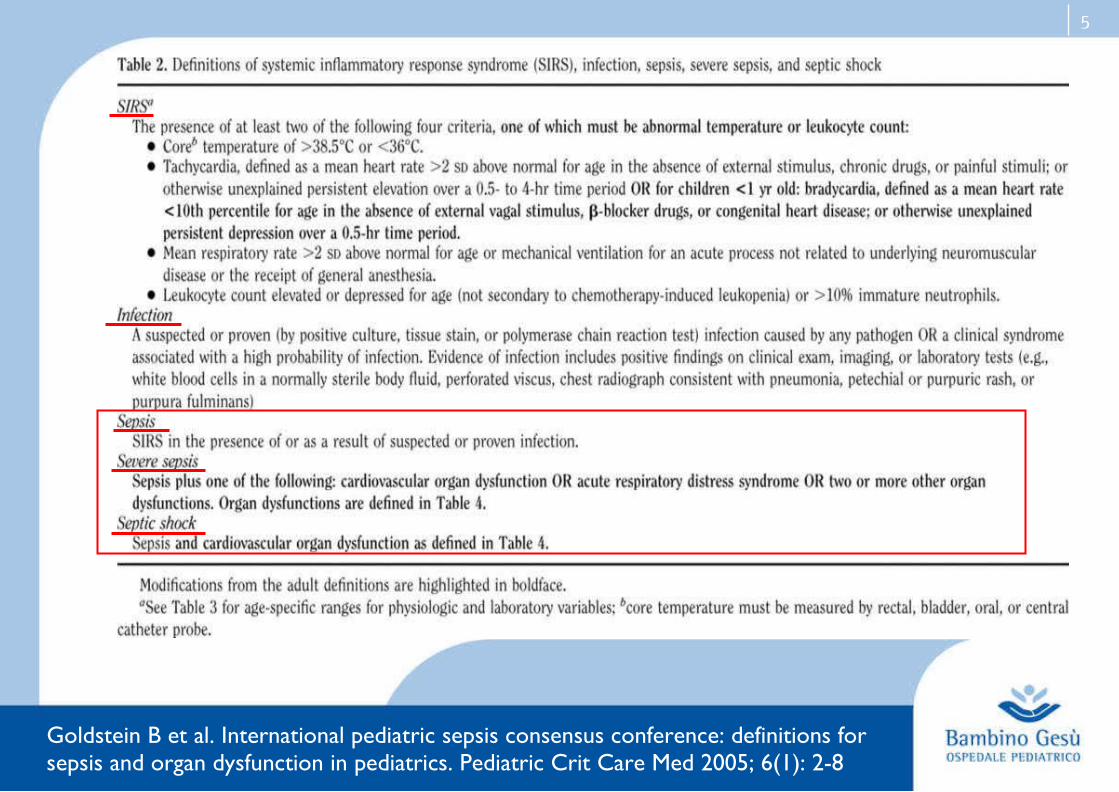
Goldstein B et al. International pediatric sepsis consensus conference: definitions forsepsis and organ dysfunction in pediatrics. Pediatric Crit Care Med 2005; 6(1): 2-8

6
Septic AKI
Septic AKI is defined by the simultaneous presence both of the RIFLE criteria for AKI and the consensus criteria for sepsis and the absence of other clear and established
non-sepsis-related causes of AKI (e.g. radiocontrast, other nephrotoxins)
Wan L. et al, Crit Care Med 2008; 36:S198-203
7
Is sepsis a frequent cause of AKI in children?

8
33 (27)123pRIFLE2005-0
6USAAkcan-
Arikan
Study Location year Definition of
AKIn ptAKI
n (%)AKI + sepsis
Ball New Zealand
2001-06
need for dialysis 226 29 (13)
Hui-Stickle USA 98-01eCCl <75 ml/min/1.73 m2
248 27 (11)
Vachvanichsanong
Thailand 82-04
creat >2 mg/dl or doubling
311 68 (21)
Bailey Canada2000-0
1creat doubling 44 4 (9)
Shaheen UK2000-0
2need for dialysis
83 28 (34)
Williams USA 79-98 creat doubling 228 41 (18)
Incidence of AKI secondary to sepsis

9
Epidemiology of AKI varies between countries
2000-2004N(%)
20(18)
9(8)
20(18)
7(6)
9(8)
5(5)
17(16)
2(2)
3(39
6(5)
8(7)
3(3)
38(35)
109
1995-1999N(%)25(22)
15(13)
7(6)
18(15)
15(13)
12(10)
5(4)
6(5)
2(2)
0(0)
7(6)
4(3)
50(43)
116
< 1995N(%)
23(25)
15(16)
11(12)
7(7)
6(6)
12(13
4(4)
3(3)
2(2)
0(0)
9(10)
1(1)
44(47)
93
Cause
Sepsis
Hypovolemia
PSAGN
SLE
Infectious disease
Malignancies
Hearth failure
CGN
Toxins
KUB anomalies
Miscellaneous
Unknown
Death
Total
Table 2 Distribution of causes and mortality rates of ARF according to the year of admission
Williams DM et al. Arch. Pediatr. Adolesc Med. 2002; 156:893-900
Vachvanichsanong P et al. Pediatrics 2006; 18: 786-91
10
Is the mortality of septic AKI higher than that of AKI secondary
to other causes?

11
Septic AKI and mortality
.0006
.0001
.0003
(2.2-17.0)
(4.1-41.0)
a
6.1
12.9
a
20 (58.8%)
29 (85.3%)
34 (100%)
8 (19.1%)
13 (31%)
29 (69%)
>20%FO
Sepsis
MODS
P value95%CIOdds ratio
Non-survivorsn=34
Survivorsn=42
Variable
a Unable to calculate odds ratio bacause 100% of non-survivors had MODS
Loza R et al. Pediatr Nephrol 2006; 21: 106-09
Hayes LW et al. Journal of Critical Care 2009; 24: 394-400
Sepsis group Mortality
Alive, n (%) Dead, n (%)
Without sepsis (73) 58 (79) 15 (21)
With sepsis (76) 46 (61) 30 (39)
Total (149) 104 (70) 45 (30)
P=0.012
12
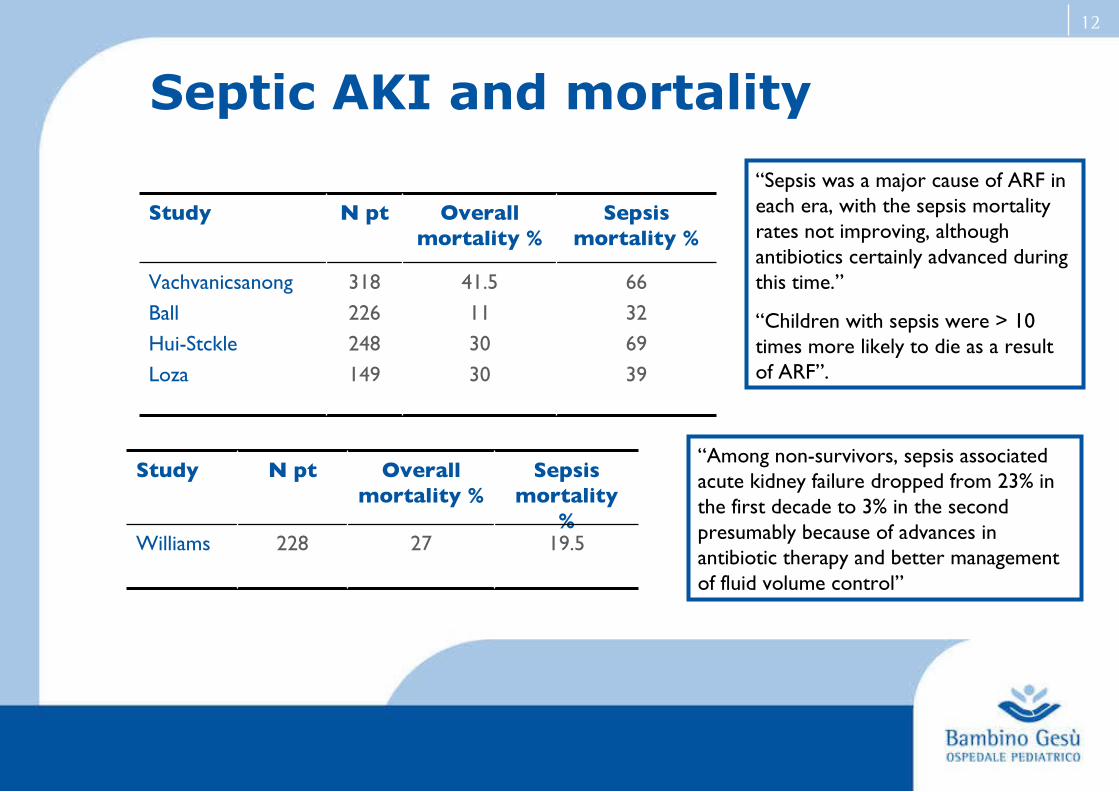
Septic AKI and mortality
66
32
69
39
41.5
11
30
30
318
226
248
149
Vachvanicsanong
Ball
Hui-Stckle
Loza
Sepsis mortality %
Overall mortality %
N ptStudy
19.527228Williams
Sepsis mortality
%
Overall mortality %
N ptStudy“Among non-survivors, sepsis associated acute kidney failure dropped from 23% in the first decade to 3% in the second presumably because of advances in antibiotic therapy and better management of fluid volume control”
“Sepsis was a major cause of ARF in each era, with the sepsis mortality rates not improving, although antibiotics certainly advanced during this time.”
“Children with sepsis were > 10 times more likely to die as a result of ARF”.
13
Is the mortality of septic AKI higher than that of sepsis without
AKI?

14
Acute renal failure in patients with severe sepsis and septic shock-a significant indipendent risk factor for mortality: results from German Prevalence Study
3877 screened patients
415 with severe sepsis/septic
shock 14 with CKD
234 patients w/o ARF
166 patients with ARF
In-hospital mortality 42.8%
In-hospital mortality 67.3%
ARF was the only organ dysfunction that was predictive for mortality (OR 2.112; P=0.0001)
Oppert M. Nephrol Dial Transplant 2008; 23: 904-909

15
Watson RS et al. Am J Respir Crit Care Med 2003 Mar 1; 167(5):695-701
Mortality of children with severe sepsis by age and comorbidity
The risk of death increased with increasing numbers of failing organs, from 7% for those with single-organ system failure to 53.1% for those with four organ systems or more failing
Sepsis and mortality
16
Do patients with septic AKI show evidence of renal
dysfunction at follow up?

17
18(15)
34(87)
11(55)
9(100)
3(60)
1(33)
5(100)
121
39
20
9
5
3
5
202
Post-cardiac surgery
HUS
Sepsis
GN
Ischemia
Nephrotoxic
Other
Total
Survivors with abnormalities at discharge
n (%)
Survivors n
Short-term outcome of survivors
Hypertension, reduced eGFR or abnormal urinalysis were detected in 55% of children with sepsis at the time of discharge
Ball EF et al. J Ped Child Health 2008; 44: 642-6

18
Long-term outcome of survivors
21 children dialysed with meningococcal sepsis: 12 survivors
After a mean follow-up of 4 years 1/3 developed renal abnormalities:
2 abnormal GFR, proteinuria and hypertension 1 isolated proteinuria 1 renal parenchimal defect on DMSA scan
Slack R et al. Pediatr. Crit Care 2005; 6: 477-9

19
Are urinary tests useful in septic AKI?
20
In septic AKI biochemical analysis of urine using standard measurements of sodium,
urea and creatinine calculating various indices of tubular function is not
diagnostically accurate, prognostically valuable or clinically useful
Bagshaw SM et al. Am J Kidney Dis 2006; 48: 695-705
21
Bagshaw SM et al. Intensive Care Med 2007; 33: 1285-96
Urinary biomarkers in septic AKI
Review of 14 studies to assess diagnostic and prognostic value of urinary biomarkers in septic AKI
Urinary IL-18, PAF and NHE3 ● detected early in AKI prior to the development of overt kidney failure● higher in septic than in non-septic AKI patients
Several additional low-molecular-weight proteins and enzymes may be evident early in the urine of patients with AKI. Their value in sepsis remains unclear

22
Urinary interleukin-18 is an acute kidney injury biomarker in critically ill children
Washburn KK et al. Nephrol Dial Transplant 2008; 23: 566-72
In AKI patients, uIL-18 began to rise at day -2, peaked at day 0 and then steadely declined at baseline at day 3, whereas control uIL-18 concentrations remained unchanged
AKI uIL-18 was higher in “non septic” patients than in controls between day -2 and 2.
The sample size was not large enough to evaluate the role of uIL-18 in the subgroup of septic patients

23
Zappitelli M et al. Critical Care, 2007; 11: R84
Urine NGAL is an early marker of acute kidney injury in critically ill children
Mean uNGAL concentrations by pRIFLE max strata
Mean concentrations of uNGAL according to presence or absence of sepsis

24
Why do only some septic patients develop AKI?

25
Perianayagam
incidence of sepsis not significantly
different
incremental increase in serum creat by 0.5, 1, 1.5
mg/dl
200NADPH oxidase p22pho
x
catalase
Wattanathum
IL-10 CGG haplotype
protective from sepsis-associated
AKI
need for dialysis550IL-10
Gordonno association with renal function or
mortality
AKI as part of the SOFA score
213TNF-α/
TNF-αR
Treszlmore often present in AKI (26 vs 6%)
creat > 120 μmol/l, diuresis < 1 ml/Kg/
h
92TNF-α/ IL-6
ReferencesOutcome Definition of AKIPatients
Gene
Genetic polymorphisms in sepsis associated AKI
Haase-Fielitz A et al. Contrib Nephrol 2007; 156: 75-91
26
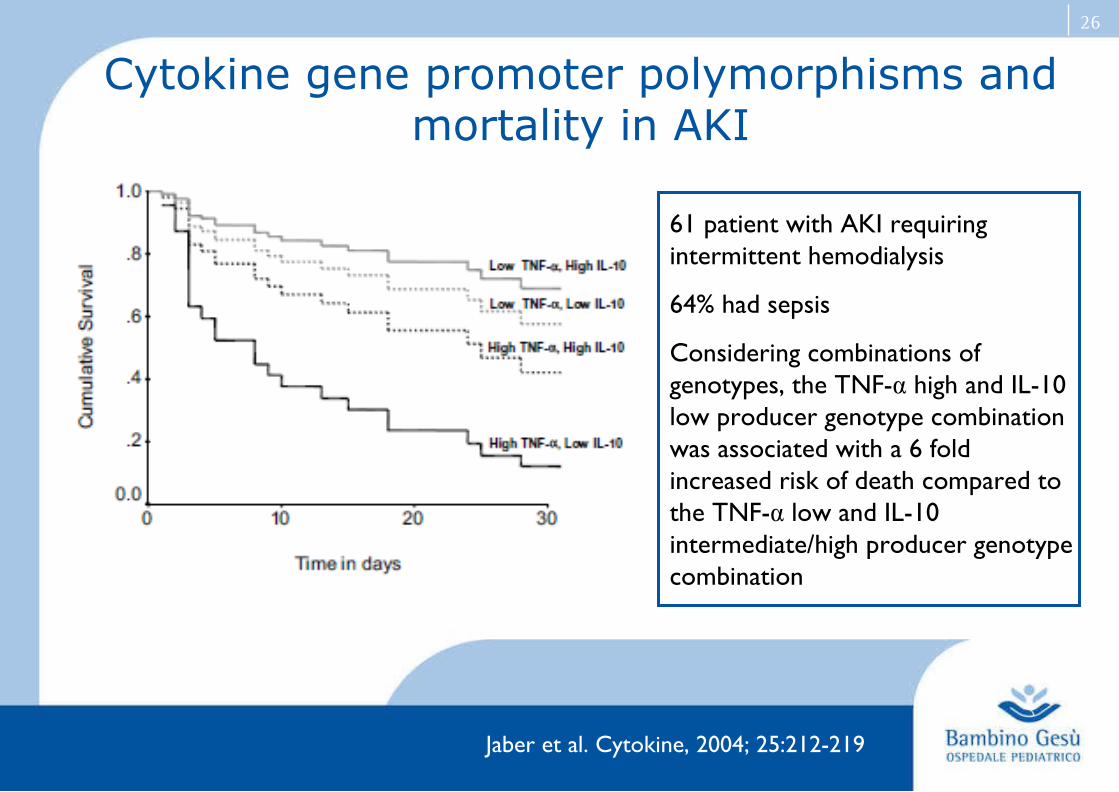
61 patient with AKI requiring intermittent hemodialysis
64% had sepsis
Considering combinations of genotypes, the TNF-α high and IL-10 low producer genotype combination was associated with a 6 fold increased risk of death compared to the TNF-α low and IL-10 intermediate/high producer genotype combination
Cytokine gene promoter polymorphisms and mortality in AKI
Jaber et al. Cytokine, 2004; 25:212-219
27
Can we attenuate or prevent septic AKI?
28
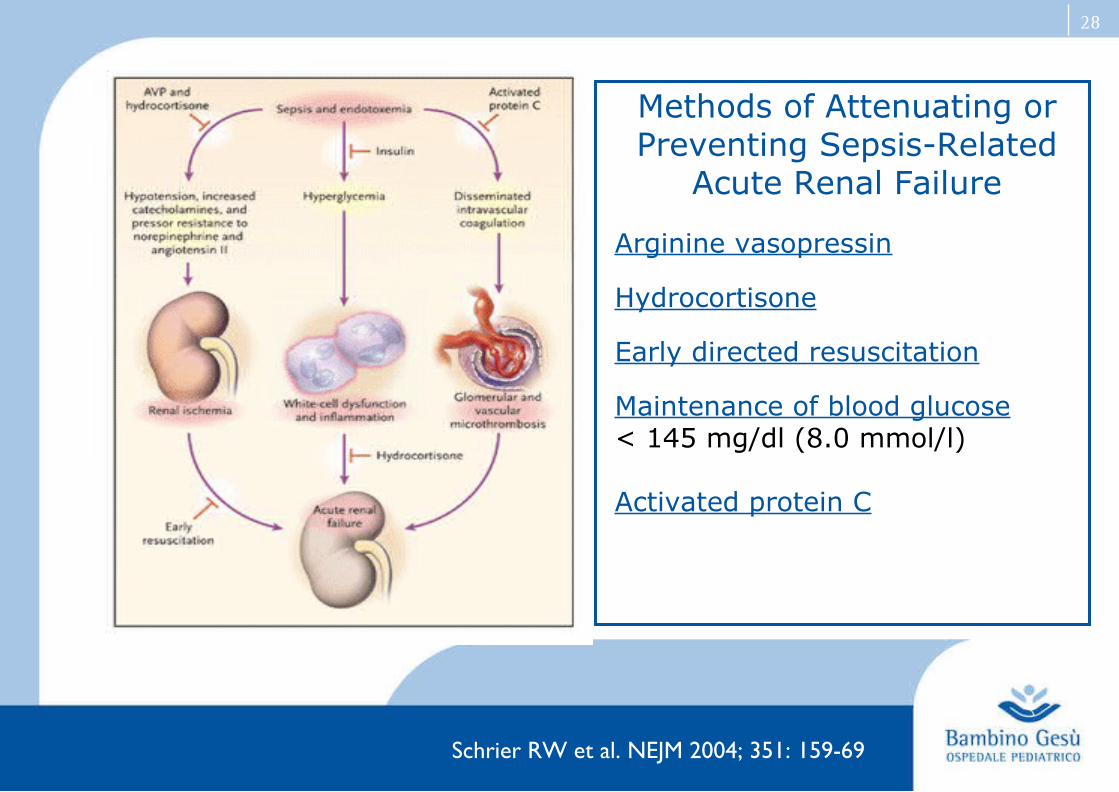
Methods of Attenuating or Preventing Sepsis-Related
Acute Renal Failure
Arginine vasopressin
Hydrocortisone
Early directed resuscitation
Maintenance of blood glucose < 145 mg/dl (8.0 mmol/l)
Activated protein C
Schrier RW et al. NEJM 2004; 351: 159-69

29
A, Shock reversal resulted in 96% survival versus 63% survival among patients who remained in persistent shock state.
B, Resuscitation consistent with the new ACCM-PALS Guidelines resulted in 92% survival versus 62% survival among patients who did not receive resuscitation consistent with the new ACCM-PALS Guidelines.
Early reversal of pediatric-neonatal septic shock by community physicians is associated with improved outcome
Han YY et al. Pediatrics 2003; 112: 793-799
30
Steroids
Hydrocortisone in septic shock → only for children with catecholamine resistance and suspected or proven adrenal insufficiency
No consensus for the best dose
Dose recommendations vary from 1-2 mg/Kg (stress dose) to 50 mg/Kg followed by the same dose as a 24 hr infusion (shock dose)
Dellinger RP et al. Crit Care Med. 2004; 32(3): 858-73
31
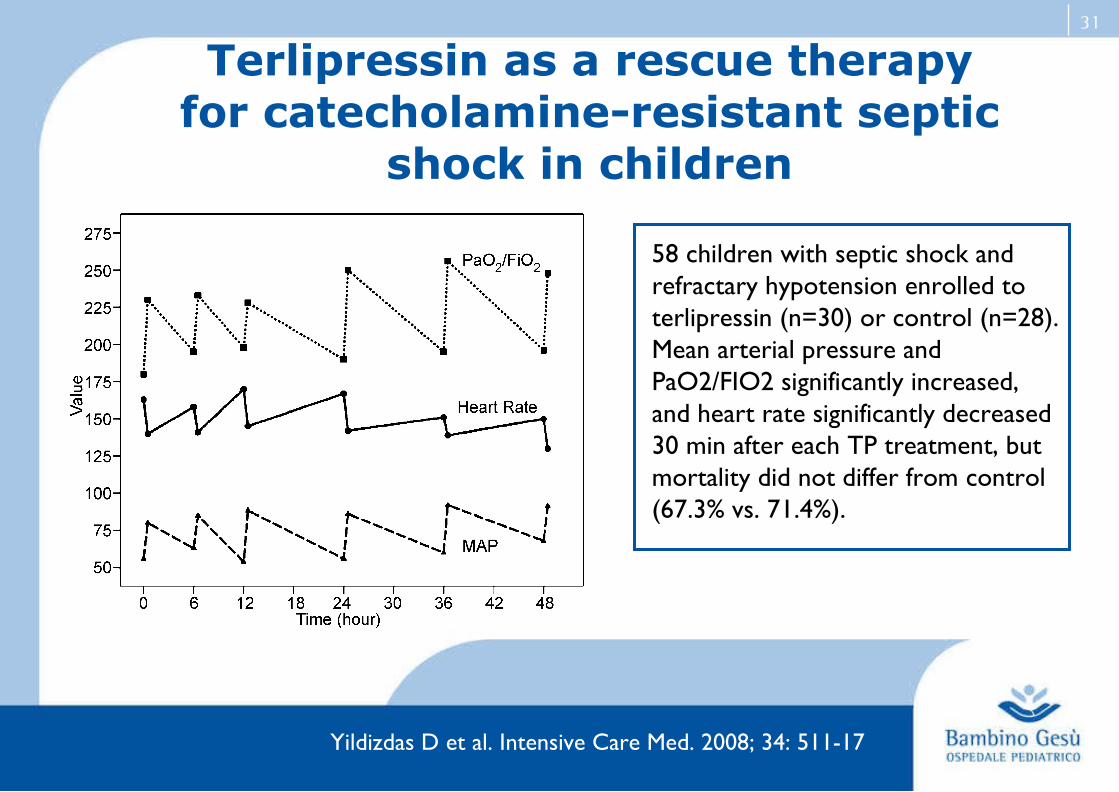
Terlipressin as a rescue therapyfor catecholamine-resistant septic
shock in children
58 children with septic shock and refractary hypotension enrolled to terlipressin (n=30) or control (n=28).Mean arterial pressure andPaO2/FIO2 significantly increased,and heart rate significantly decreased 30 min after each TP treatment, but mortality did not differ from control (67.3% vs. 71.4%).
Yildizdas D et al. Intensive Care Med. 2008; 34: 511-17

32
Drotrecogin alfa in children with severe sepsis
477 patients enrolled. 237 received placebo and 240 DrotAA
No significant difference between groups in 28-day mortality
No difference in overall serious bleeding events
More CNS bleeding events occured in the DrotAA group particularly in children younger than 60 days
Nadel S et al. Lancet 2007; 369: 836-43
33
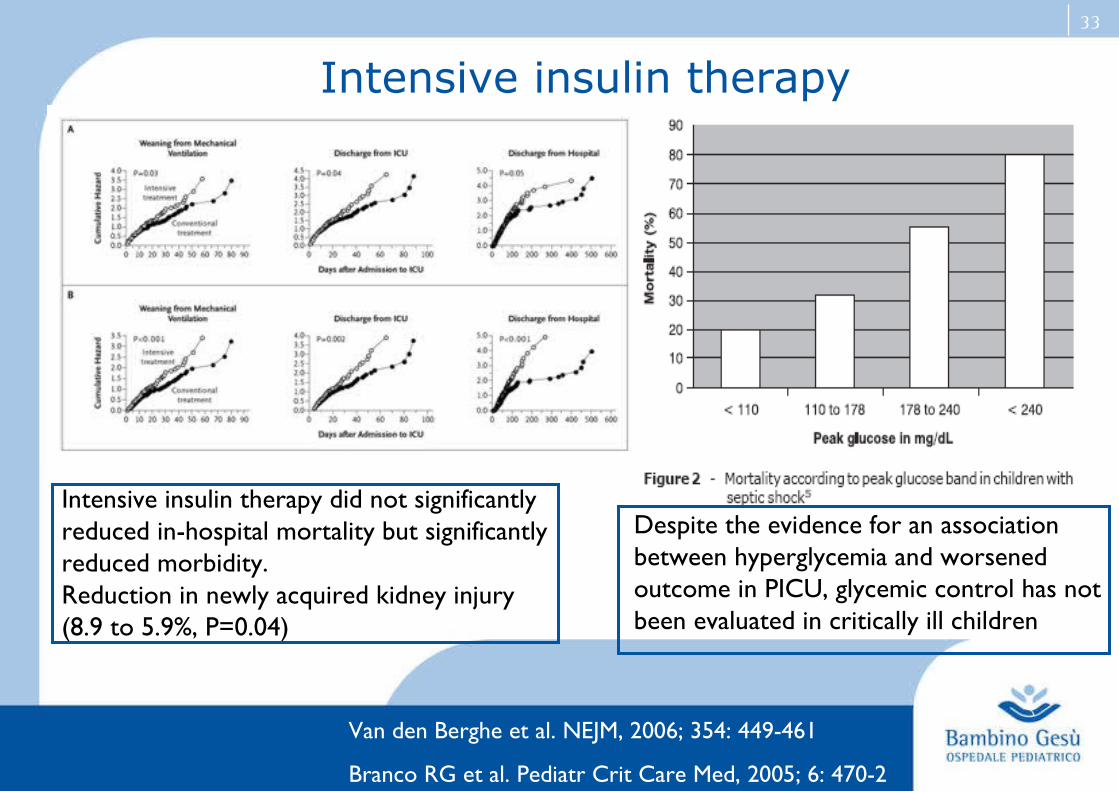
Intensive insulin therapy
Intensive insulin therapy did not significantly reduced in-hospital mortality but significantly reduced morbidity. Reduction in newly acquired kidney injury (8.9 to 5.9%, P=0.04)
Despite the evidence for an association between hyperglycemia and worsened outcome in PICU, glycemic control has not been evaluated in critically ill children
Van den Berghe et al. NEJM, 2006; 354: 449-461
Branco RG et al. Pediatr Crit Care Med, 2005; 6: 470-2
34
Conclusions
Sepsis is a frequent cause of AKI in children Sepsis increases the mortality of AKI AKI increases the mortality of sepsis More than half of children with septic AKI presents renal
dysfunction at discharge and 1/3 develops abnormalities in the long term. Follow-up of these patients is recommended
Genetic risk factors may be involved in the individual susceptibility to septic AKI
Fluid resuscitation avoiding fluid overload, hydrocortisone, terlipressin, drotrecogin alfa and intensive insulin therapy may be useful in the management of septic AKI but further studies are necessary

35
Thank you for your attention