7-risk analysis_b.pdf
TRANSCRIPT

7/27/2019 7-Risk analysis_b.pdf
http://slidepdf.com/reader/full/7-risk-analysisbpdf 1/8
Risk analysis
Pengertian
The development of qualitative and / or quantitative
estimate of risk based on evaluation and mathematical
techniques. (FAA System Safety Handbook, Dec
2000)
The process by which hazards are identified and
analyzed for their likelihood of occurrence and their
potential severity. (GAIN, 2003., Guide to methods
and tools for safety analysis in air traffic
management)
Risk = the expected loss per unit time or activity
Lingkup risk analysis
Looks hazards to determine:
What can happen
When it could happen
Factors associated with their occurrence

7/27/2019 7-Risk analysis_b.pdf
http://slidepdf.com/reader/full/7-risk-analysisbpdf 2/8
Tools untuk risk analysis
Severity assessment -- selecting events for
investigation Root Cause Analysis
Failure mode and effect analysis
Adverse eventManagement process
Risk identification
Risk analysis
Risk evaluation
Risk treatment
Ongoing monitoring
Communication
Audits, complaints,
Claims and incidents
Severity analysis
RCA
Risk registersAction plan
Eliminate or minimizerisk
Review the effectivenessof investigations and
actors
Communicate risks andthe outcomes ofinvestigations
Sumber:Hunter area healthservice
Clinical GovernanceUnit (Agst, 2003)
Preventable harm
Identifying weaknessIn systems
Fixing weakness
In systems
Safety
7/27/2019 7-Risk analysis_b.pdf
http://slidepdf.com/reader/full/7-risk-analysisbpdf 3/8
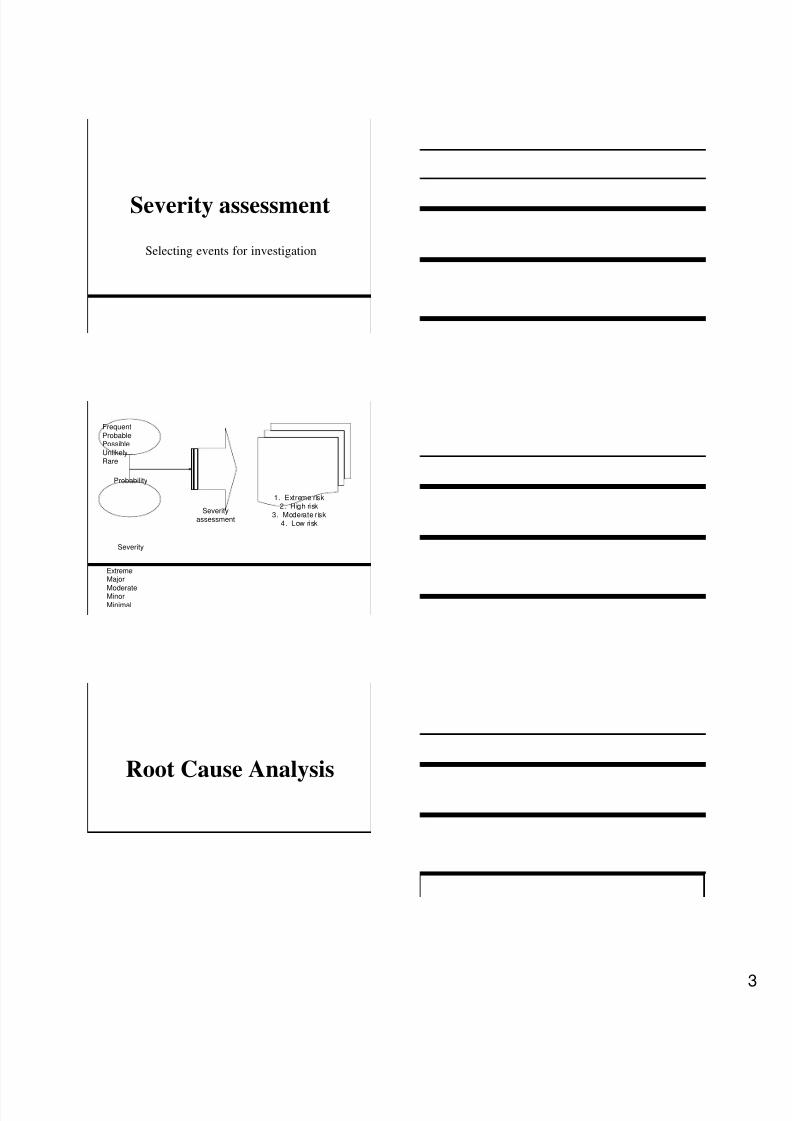
Severity assessment
Selecting events for investigation
Severityassessment
1. Extreme risk2. High risk
3. Moderate risk4. Low risk
Probability
Severity
Frequent
ProbablePossible
UnlikelyRare
ExtremeMajor
ModerateMinor
Minimal
Root Cause Analysis
7/27/2019 7-Risk analysis_b.pdf
http://slidepdf.com/reader/full/7-risk-analysisbpdf 4/8
Steps for root cause analysis
Investigate events
Reconstruct events
Analyze causes
Develop action plans
Report RCA process and findings
Investigate events
Define the problem
Collect pertinent evidence
Conduct interview
Review event environment
Determine contributing factors
Establish a chain of events
Reconstruct events
Define events preceding the adverse event or
near miss
Determine actions and conditions leading up to
these events by developing a causal tree
Continue until you have identified underlying
systems causes or until it is unreasonable to go
further

7/27/2019 7-Risk analysis_b.pdf
http://slidepdf.com/reader/full/7-risk-analysisbpdf 5/8
Analyze causes
Identify root causes within your causal tree
Develop root cause statement
Develop action plans
Identify strategies that are appropriate to the
causes identified and acceptable to the
organization and to those who will be involve
in the changes
Develop a plan for addressing each root cause
and for measuring effectiveness of intervention
Gain agreement form organizational leadership
regarding actions to be taken
Record RCA process and
findings
Record the process and tools uses
The cost of the process
A summary of the events The investigation and analysis process
Findings

7/27/2019 7-Risk analysis_b.pdf
http://slidepdf.com/reader/full/7-risk-analysisbpdf 6/8
Understanding causes of events
Active failure: an intentional violation
committed by an individual Latent condition: a breakdown in process or
systems:
lack of education,
failure to follow procedure,
equipment defect,
poor design, etc
Philosophical viewpoints on human
errors
Human error is not the cause of events, it is a
symptom of deeper troubles in the system
Human error is not the conclusion of an
investigation, it is the beginning
Events are the result of multiple causes
21 steps of RCA (Joint commission)
Communicate the results21
Take additional action20
Run chart, controlchart, histogramEvaluate implementation of improvement plan19
Develop measures of effectiveness and ensure their success18
PDCA, criticalpathImplement the Improvement Plan17
Ensure acceptability of the action plan16
GanttchartDesign improvements15
Evaluate Proposes Improvement Actions14
Brainstorm, flow chart, causeeffect diagramFormulate improvement actions13
FMEAExplore & identify risk-reduction strategies12
Confirm root causes11
Prune the list of root causes10
Flow chart, cause effectdiag, fmea, treeanalysis,
barrier analysisIdentify which systems are involved (the root c auses)9
GanttchartDesign and implement interim changes8
Seeho w to develop indicatorsMeasure, collect and assess data on proximate and underlying causes7
Brainstorm, affinityd iag, cause-effectdiagramIdentify other contributing factors6
Controlch art, treeanalysis, FMEAIdentify contributing factors5
Flow chart, timelineDetermine what happen4
Braintorm, flowchart, pareto, scatter, affinity
diagram, etcStudy the problem3
Brainstorming, multivoting, FMEADefine the problem2
Sizefewer than 10Organize a team1
Note and ToolsDescriptionsSteps

7/27/2019 7-Risk analysis_b.pdf
http://slidepdf.com/reader/full/7-risk-analysisbpdf 7/8
Failure mode andeffect analysis
Apakah FMEA
Suatu alat mutu untuk mengkaji suatu prosedursecara rinci, dan mengenali model-modeladanya kegagalan/kesalahan pada suatuprosedur, melakukan penilaian terhadap tiapmodel kesalahan/kegagalan, dengan mencaripenyebab terjadinya, mengenali akibat darikegagalan/kesalahan, dan mencari solusidengan melakukan perubahan disain/prosedur
Langkah-langkah
Bentuk tim FMEA: orang-orang yang terlibatdalam suatu proses
Tetapkan tujuan, keterbatasan, dan jadual tim
Tetapkan peran dari tiap anggota tim
Gambarkan alur proses yang ada sekarang
Kenalilah Failure modes pada proses tersebut
Kenalilah penyebab terjadinya failure untuk tiapmodel kesalahan/kegagalan
Kenalilah apa akibat dari adanya failure untuktiap model kesalahan/kegagalan

7/27/2019 7-Risk analysis_b.pdf
http://slidepdf.com/reader/full/7-risk-analysisbpdf 8/8
Langkah-langkah….
Lakukan penilaian untuk tiap model kesalahan/kegagalan: Sering tidaknya terjadi (occurrence): (Occ)
0 : tidak pernah, 10 sangatsering Kegawatannya (severity): (SV)
0 : tidak gawat, 10 sangat gawat
Kemudahan untuk terdeteksi: (DT) 0 : mudah dideteksi, 10 : sangat sulitdideteksi
Hitung Risk Priority Number (RPN) dengan mengkalikan: Occ xSV x DT
Tentukan batasan (cut-off point) RPN yang termasuk prioritas
Tentukan kegiatan untuk mengatasi (design action/solution)
Tentukan cara memvalidasi apakah solusi tersebut berhasil
Gambarkan alur yang baru dengan adanya solusi tersebut
Design
Validati
on
Design
action/
Solution
RPNDTSVOCCEffects
of
failure
Cause of
failure
Failure
Mode
Occ : occurrence
SV : severityDT : detectableRPN: risk priority number
Diskusi
Pilih salah satu proses pelayanan klinis
yang bermasalah, yang mungkin
membahayakan pasien
Lakukan analisis dengan FMEA