8 drug resistance
TRANSCRIPT

Drug-Resistance and nosocomial Infection

Section 1 Drug-Resistance
Antibiotics :powerful medicines that fight bacterial infection
Literal translation• anti – against
• biotic – living things
DiscoveryAlexander Fleming in 1928
– He was an extremely messy scientist– Came back from holiday to see a
mould growing on his Staphylococcus agar plates
– Noticed that the Staphylococcus couldn’t grow anywhere near the mould
– The mould prevented bacterial growth!

How antibiotics work Antibiotics can be either• Broad Spectrum
– Kill a wide range of bacteria e.g. Penicillin
• Narrow Spectrum– Kill a specific type or group of bacteria
e.g. Isoniazid Antibiotics work in one of two ways
• Bactericidal – Kills the bacteria
• Bacteriostatic– Prevents the bacteria from dividing

Miracle Cure?– Before the 1930s there were no treatments for
bacterial infections
– Following the discovery of penicillin industry started searching for more antibiotics in nature
– Streptomycin was the first drug to have an effect on tuberculosis – a condition previously untreatable
– Surgeons could attempt more dangerous operations

Sources of Antibiotics
[ɪvə'mektɪn] 伊维菌素利福霉素类
[ˌpɒliː'mɪksɪn] 多粘菌素 [ˌbæsɪ'treɪsɪn] 杆菌肽素双效菌素
[ɒksəzɒ'laɪdɪnwʌnz] 恶唑烷酮类 [laɪ'nezɒlɪd] 利奈唑胺

Miracle Cure?
– Many antibiotics prescribed by the doctor are broad spectrum
– These kill the body’s good bacteria as well as the bad
– With the good bacteria gone there is more room for bad microbes to invade!
Overuse of antibiotics can damage our normal/good bacteria.

Miracle Cure?Antibiotics resistance
– Many bacteria have developed the ability to become resistant to antibiotics.
– These bacteria are now a major threat in our hospitals.
– Antibiotic resistant bacteria include Methicillin 甲氧苯青霉素 Resistant Staphylococcus aureus (MRSA)

Antibiotic Resistance
The Causes
– Overuse
• Antibiotics used to treat infections when they are not needed or not effective i.e. for the flu
– Misuse
• Not completing a prescribed course
• Using antibiotics not prescribed for you

How antibiotic resistance can be prevented
– Antibiotics should be the last line of defence NOT the first
• Most common infections will get better by themselves through time, bed rest, liquid intake and healthy living.
– Only take antibiotics prescribed by a doctor
– If prescribed antibiotics, finish the course.
– Do not use other peoples or leftover antibiotics
• they be specific for some other infection

Antibiotic Resistance APPEARANCE
DRUG INTRODUCTION OF RESISTANCE
Penicillin 1943 1946
Streptomycin 1945 1959
Tetracycline 1948 1953
Erythromycin 1952 1988
Vancomycin 1956 1988
Methicillin 1960 1961
Ampicillin 1961 1973
Cephalosporins 1964 late 1960’s

Origins of ResistanceDrug resistance is a natural by-product of the evolutionary process: natural selection acting on pre-existing genetic variation
400 microbial strains were isolated from natural sources and sealed into vials in 1917, long before the clinical introduction of antibiotics
- Recent analysis: 11 of these 400 strains had antibiotic resistance (at a low level)
-
Origins of ResistanceNearly all clinically useful antibiotics are natural products, or their synthetic derivatives; most were isolated from other microbes
- Fungi (penicillins, cephalosporins)
- Soil bacteria of genus Streptomyces (erythromycin, streptomycin, tetracycline, vancomycin)
In 1999, only 1 class of antibiotic was totally synthetic (Ciprofloxacin)
Antibiotics are an ancient weapon...
[də'revətɪvz]环丙沙星

Origins of ResistanceWhat does the antiquity [æn'tɪkwəti] 古代 of antibiotic resistance tell us?
- There is likely to be considerable genetic variation in natural populations for genes that can potentially confer drug resistance
(i.e., the raw genetic material is there)
- Strong selection will quickly lead to the explosive growth of resistant individuals, especially when most cells are susceptible
Widespread antibiotic use =
- nukes their competition[nuːk] 以核武器攻击 - the fittest survive and reproduce, passing on their resistance both to clonal offspring and to other unrelated bacteria

Inherent Resistance• Darwinian evolution:
– Bacteria that resist an antibiotic's effects are better suited to survive in an environment that contains the antibiotic.
– Genes that confer resistance are transferred to the bacterial progeny.
• Bacteria naturally resistant (e.g., Gram-negative bacteria resistant to penicillins).
• Bacteria may be resistant because – They have no mechanism to transport the drug into
the cell. – they do not contain or rely on the antibiotic’s target
process or protein.

Acquired Resistance
• Bacteria that don’t begin life resistant to a certain antibiotic can acquire that resistance.
• Horizontal evolution:– Resistance genes pass from a resistant strain to a
nonresistant strain, conferring resistance on the latter.
– Presence of an antibiotic is a selective pressure.• Gene transfer mechanisms:
– Conjugation.– Transduction.– Transformation.

Conjugation
• Transmission of resistance genes via plasmid exchange.
• Resistance spreads much faster than simple mutation and vertical evolution would permit.

Transduction and Transformation
• Transduction: Virus transfers gene.
• Transformation: DNA released from a bacterium is picked up by a new cell.

Antibiotic Mechanisms

Antibiotic TargetsThe major classes of antibiotics affect 1 of 3 targets in bacteria cells:
(1) Cell wall biosynthesis
penicillins cephalosporinsvancomycin (non-ribosomal peptide)
(2) Protein synthesis
erythromycin (macrolide ['mækroʊlaɪd] 大环内酯物 polyketides)tetracycline (aromatic [ˌærə'mætɪk] 芳香的 polyketides 聚酮化合物 )
streptomycin, kanamycin (aminoglycosides)
(3) DNA replication
quinolones (Cipro) 盐酸环丙沙星制剂
(-lactams)

Antibiotic TargetsAntibiotics work by exploiting biochemical differences between our eukaryotic cells and the prokaryotic cells of bacteria
(1) Cell wall biosynthesis
- block synthesis of peptidoglycan, the covalently cross-linked peptide/glycan network, which imparts osmotic resistance to cell
(2) Protein synthesis
- target 23S rRNA + associated proteins in peptidyl transferase center of bacterial ribosome
-
(3) DNA replication
- inhibit gyrase, essential enzyme that uncoils intertwined circles of DNA after replication of the circular bacterial chromosome

Antibiotic Target 1: Cell WallCell wall is peptidoglycan, a repeating polymer of di-saccharide, tetra-peptide repeats cross-linked into a 3D matrix
-lactam antibiotics interfere with cell wall biosynthesis of Gram-positive bacteria (Staphylococci, Streptococci)
-

Antibiotic Target 1: Cell WallBacterial transpeptidase enzyme forms crosslinking amide bonds between #3 L-Lysine and #4 D-Alanine residues
TPase cuts off #5 D-Ala residue, then links L-Lys side chain to the remaining D-Ala

Antibiotic Target 1: Cell Wall
Catalytic Serine -OH forms a temporary bond to the substrate
- when Lysine side-chain attacks the temp. ester linkage, the Serine is restored to normal
-

Antibiotic Target 1: Cell Wall

-lactams: Mechanism of Action-lactams inhibit transpeptidase by mimicking its substrate, the terminal D-Ala—D-Ala
Transpeptidase attacks the -lactam ring of penicillin, forms a covalent bond that is slow to hydrolyze; enzyme is deactivated
Normally, the enzyme forms a temporary bond with D-Ala that is rapidly broken by the side chain of Lysine

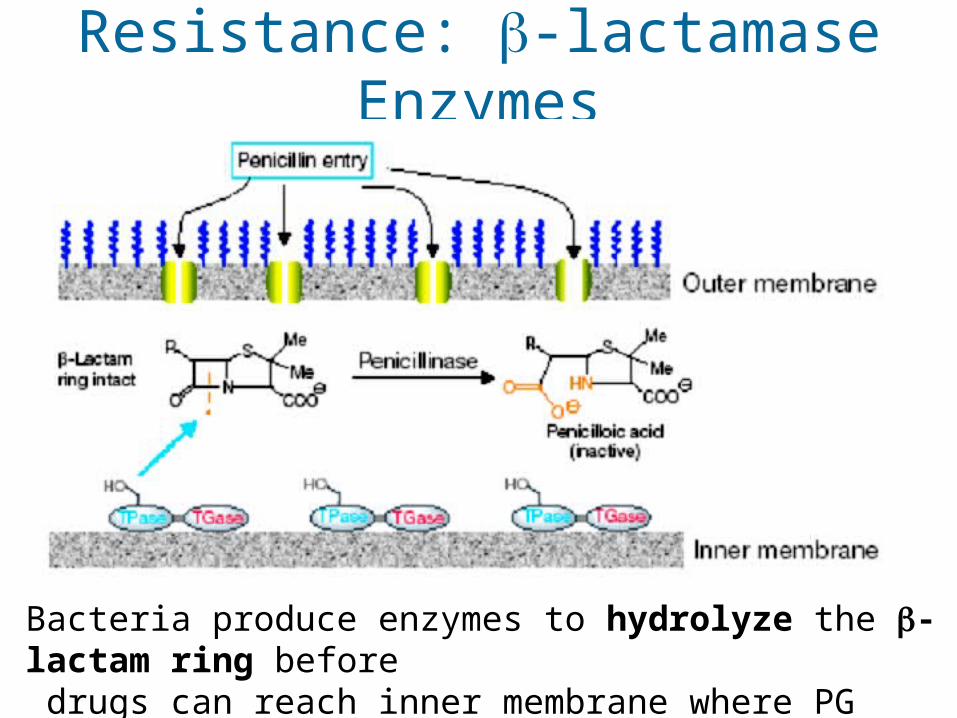
Resistance: -lactamase Enzymes
Bacteria produce enzymes to hydrolyze the -lactam ring before drugs can reach inner membrane where PG synthesis occcurs

Overcoming -lactam Resistance
Augmentin combines -lactam antibiotic w/ clavulanate 克拉维酸钾 , a “suicide” -lactam that occupies the -lactamase enzymes - Allows active drug (amoxacillin, [ m ks 's l n]ə ɒ ɪ ɪ ɪ 阿莫西林 ) to reach target enzymes, PG-synthesizing transpeptidases lining the inner membrane
(resistance) slow tohydrolyze
(cell wall enz.)
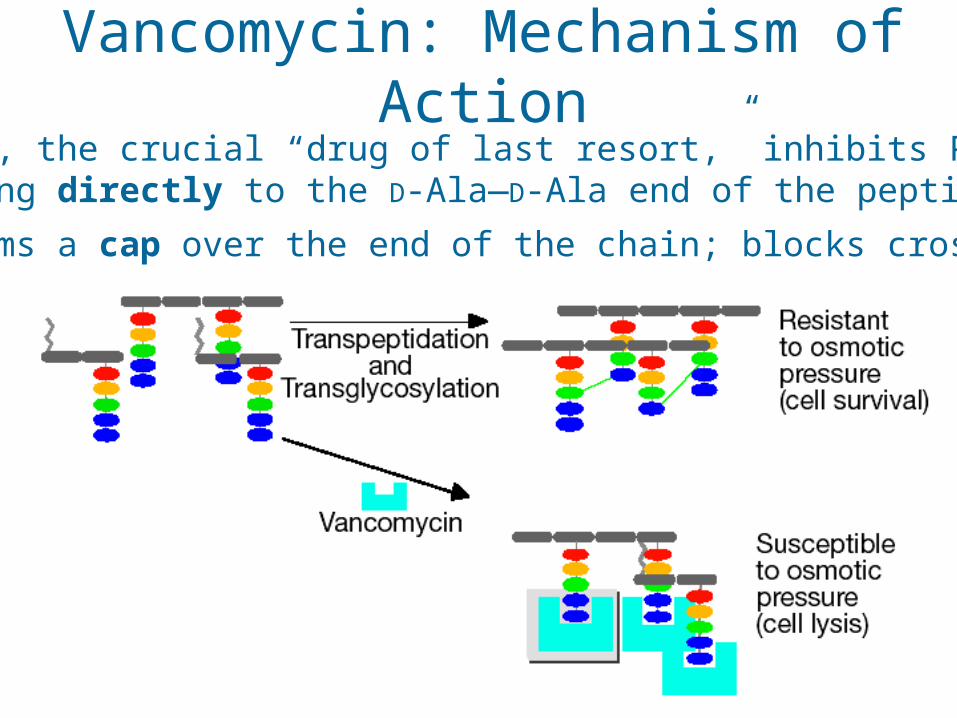
Vancomycin: Mechanism of ActionVancomycin, the crucial “drug of last resort,” inhibits PG synth by binding directly to the D-Ala—D-Ala end of the peptide
- forms a cap over the end of the chain; blocks cross-linking

Vancomycin: Mechanism of Action
Completely surrounds its target peptide, preventing enzymes from reacting with the end of the peptidoglycan chain
3D model of Vancomycin incomplex with D-Ala—D-Ala
note “cup-like” shape of Van

A cell may produce 100,000 lactamase enzymes, each of which can destroy 1,000 penicillins per second
100 million molecules of drug destroyed per second
Resistance: -lactamase Enzymes

Vancomycin makes 5 H-bonds with the D-Ala—D-Ala cap of the PG peptide
- -
Vancomycin
D-Ala D-Ala

Van Resistance: D-Ala-D-LactateVancomycin-resistant bacteria have peptidoglycan chains that end in D-Ala—D-Lactate, instead of the usual D-Ala—D-Ala
(A) What genes are necessary to make this change?
(B) How does this confer resistance?
D-Ala—D-Ala
D-Ala—D-Lactate

Genetics of Van Resistance
VanAVanH
VanX
5 gene products are required to produce Lac-terminal PG
- 2 “sensor” genes detect Van, turn on other 3 genes
- 2 synthesize the critical D-Ala—D-Lactate piece
- 1 destroys the pool of D-Ala—D-Ala in the cell (equilibrium)
reduction
hydrolysis 1,000 fold lower affinity for Van

Vancomycin: Mechanism of Action
D-Ala—D-Ala cap makes 5 H-bonds with Vancomycin
D-Ala—D-Lac makes 1 less H-bond Resistance You die
Genetics of Van ResistanceWhy did penicillin resistance appear in 2 years, but Van resistance take 30 years to become a major health hazzard?
One answer: genetic complexity of resistance mechanism
Penicillin resistance requires the activity of one gene product (-lactamase enzyme)
- usually 2-4 year lag when only 1 gene is involved
Van resistance takes 5 gene products
- apparently delays development of infectious, highly resistant strains when multiple gene products are involved

Overcoming Van Resistance
Approach #1: Screening of semi-synthetic analogues of Van found that hydrophobic derivatives restore potentcy 100-fold
- Partitions drug to membrane surface, thus altering activity and availability to target enzymes
chlorinated bi-phenyl substituent

Overcoming Van ResistanceApproach #2: Screening combinatorial libraries for novel small molecules that cleave the D-Ala—D-Lac depsipeptide [dep'saipepta d]ɪ 缩酚酸肽 - Look for drugs that can effectively function like an enzymeCombinatorial library of 300,000 tripeptide derivatives yielded 3 hits, all w/ an N-terminal serine & an intramolecular H-bondPharmacophore deduced from computer modeling studies
N
HO
NH2
OSProC5 “resensitized” bacteria with Van-resistance, by cleaving their D-Ala—D-Lac depsipeptide
SProC5
Chiosis & Boneca, Science 2001

Protein Synthesis Inhibitors
Erythromycin (macrolide polyketide)
Tetracycline (aromatic polyketide)
Kanamycin(aminoglycoside)

Resistance to Aminoglycosides
Chemical modification of the drug lowers its binding affinity for RNA target in the ribosome
-
(formerly a protein kinase?)

MultiDrug Resistance Pumps
Bacteria use ATP-powered membrane proteins to pump any lipophilic molecule out of the cell
- common in antibiotic-producing bacteria, to get drugs out of their cells without poisoning themselves
Powerful method of resistance, because many different drugs will be equally affected by these efflux pumps

MultiDrug Resistance Pumps
(1) substrate binding: lipophilic drug binds inside cone-shaped chamber; triggers ATP hydrolysis
(2) chamber then closes, substrate flips to opposite orientation
(3) chamber then opens, substrate is expelled to outer face of membrane
outside cell

Erythromycin Resistance
In addition to efflux pumps, erthyromycin resistance can arise from reprogramming the target (akin[ 'k n] ə ɪ 近似的 to Van resistance)Methylation of a specific adenine ['ædənɪn] on the 23S rRNA component of the ribosome - decreases binding affinity of erythromycin-class drugs - does not impair protein synthesis - present as a self-immunity mechanism in erythromycin- producing bacteria
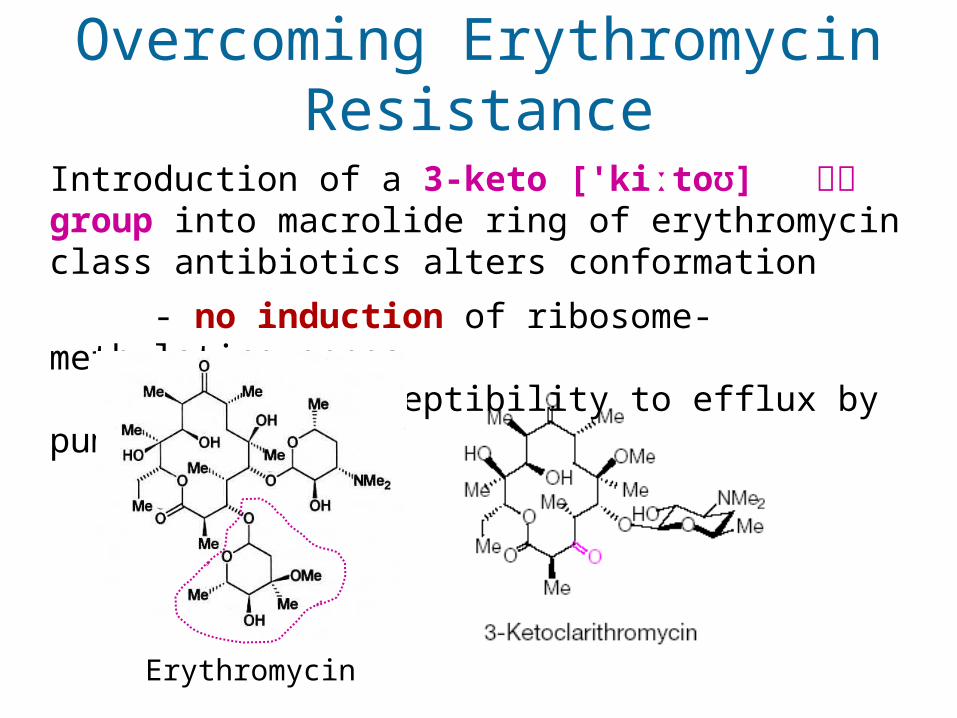
Overcoming Erythromycin Resistance
Introduction of a 3-keto ['kiːtoʊ] 氧化 group into macrolide ring of erythromycin class antibiotics alters conformation
- no induction of ribosome-methylating genes - lower susceptibility to efflux by pumps
Erythromycin

Selection favoring ResistanceWhat causes the rapid occurrence of widespread resistance?
(1) Incomplete treatment: people fail to finish the full course of their medication
- in the 1980’s, tuberculosis was almost wiped out w/ antibiotics - in 1990’s, came back with a vengence['vend ns]ʒə 复仇 , due to resistant strains - 25% of previously-treated tuberculosis patients relapsed with drug resistant strains; most had failed to complete their initial course
(2) Livestock doping['do p ]ʊ ɪŋ 服用禁药 : 50% of antibiotics used by livestock farmers to increase yield of chicken, beef, pork
- high levels of antibiotics used in livestock result in strongly resistant bacterial strains, which can then infect humans

Selection favoring ResistanceWhat causes the rapid occurrence of widespread resistance?
(3) Mis-prescription: my mom demands antibiotics for a cold
- widespread inappropriate use: up to 50% of prescriptions in developing countries are for viral infections that cannot respond
(4) Gene transfer & multi-drug resistance
(a) genes encoding resistance accumulate on plasmids, transposons confer simultaneous resistance to multiple drugs
(b) DNA is easily exchanged between unrelated bacteria - vancomycin-resistant gut bacteria known since 1987 - resistance genes finally transferred to deadly infectious Staphylococcus aureus in a Michigan hospital in 2002

Loss of Resistance...?Resistance carries a cost: resistant bacteria grow more slowly under normal conditions, pay a 10-20% fitness cost
- Replicating extra plasmid DNA is costly to the cell - Ribosomal mutations that confer resistance slow protein production
When we stop using an antibiotic, does resistance go away? - Can we reverse selection, and favor the vulnerable bacteria instead
Experiments show bacteria quickly evolve compensatory mutations that lower the costs of resistance, instead of just losing resistance
-
Levin et al. 2000, Genetics 154: 985-997

Conclusion
• We overuse antibiotics and often neglect to complete a full course of antibiotics once it has been prescribed, leading to the spread of antibiotic resistance.
• Resistance can disappear if there is no
selective pressure to maintain resistance.

Section 2 Nosocomial infections
• The word derives from the Greek nosokomeian, meaning hospital
• These days the terms hospital acquired – and healthcare associated – are used
• A very emotive subject with the public, driven by the press
• Do hospitals really deserve to be blamed for all cases of hospital infection?

Nosocomial infections are…
• Infections that are acquired in hospital (48 hours or more after admission)
• Approx 7% of patients will suffer from an infection whilst in hospital – the risk increases with length of stay
• A significant financial burden on NHS

Impact of nosocomial infections
• Possibly up to100,000 infections per year in UK
• A cause of ~5,000 deaths with nosocomial infections playing a role in ~15,000 others
• Costs the NHS £1 billion – 9% of its in-patient budget
• Cannot be eradicated but it’s thought they could be reduced by up to 30%

Impact of nosocomial infections
• Longer stays in hospital – bed occupancy
• Outbreaks leading to ward closures especially norovirus and C. difficile
• Pain and anxiety for patients and families
• Loss of earnings

Why are we more likely to get an infection in hospital?
Consider 4 important factors…1. The host2. The microbes3. The environment4. Treatment

The host 1
• People in hospital are already sick!• They may have poor general resista
nce to infection• Lack of immunity
– Extremes of age– Immunocompromised (eg cancer chem
otherapy)

The host 2• Reduced immunity
– Diabetes, severe burns• Poor local resistance
– Poor blood supply to tissues • Surgery
– Wounds, sutures • Medical devices
– Catheters, prostheses, tubing etc

The microbes• Virtually any infection can be acquired i
n hospital• However a number of “usual suspect
s” predominate• What are they, where do they come fro
m and why do they cause nosocomial infection?

Opportunistic infections• Nosocomial infections are often caused b
y opportunistic pathogens i.e. those which do not normally cause infection in healthy people
• May be a reflection of reduced defences of host or access to sites not normally colonised by organisms
• May be from normal flora or environment
• Antibiotic resistance is a problem

Opportunistic pathogens• Pseudomonas aeruginosa• staphylococci• E. coli and other coliforms• streptococci and enterococci• Bacteroides fragilis• Candida albicans• Herpes simplex virus• Cytomegalovirus

Biofilms• Biofilms are microbial communities
(cities) living attached to a solid support eg catheters/ other medical devices
• Biofilms are involved in up to 60% of nosocomial infections
• Antibiotics are less effective at killing bacteria when part of a biofilm

The Environment• There are many different sources of pat
hogens when in hospital– Our own normal flora (endogenous infectio
n)– Infected patients– Movement of staff and visitors– Environment e.g. fungi, Legionella– Blood products (v. rare)– Surgical instruments eg vCJD (v. rare)

ENVIRONMENTAL SOURCES OF PATHOGENS IN THE HEALTHCARE SETTING
Source Bacteria Viruses FungiAir Gram-positive cocci (originating from skin)
TuberculosisVaricella zoster (chickenpox),Influenza
Aspergillus
Water (tap and bath)
Gram-negative bacteria (Pseudomonas aeruginosa, Aeromonas hydrophilia, Burkholderia cepacia, Stenotrophomonas maltophilia, Serratia marcescens, Flavobacterium meningosepticum, Acinetobacter calcoaceticus, and Legionella pneumophila) Mycobacteria (Mycobacterium xenopi, Mycobacterium chelonae, or Mycobacterium avium-intracellularae)
Molluscum contagiosum Human papillomavirus (bath water)Noroviruses
AspergillusExophiala jeanselmei
Food Salmonella species, Staphylococcus aureus,Clostridium perfringens,Clostridium botulinum, Bacilluscereus and other aerobic spore-forming bacilli Escherichia coli Campylobacter jejuni ,Yersinia enterocolitica, Vibrio parahaemolyticus, Vibrio cholerae, Aeromonas hydrophilia, Streptococcus species Listeria monocytogenes
Rotavirus Caliciviruses

Treatment
• There is continuous usage of antibiotics in hospitals especially in ICU
• As a result there will be a natural selection for strains that are antibiotic resistant – infections are getting harder to treat
• This has led to problems with multi-resistant bacteria e.g. MRSA, VRE, ESBLs
• Antibiotic treatment can also lead to alterations in normal flora and allow pathogens cause infection eg C. difficile

SummaryDefinitions:
Inherent ResistanceAcquired ResistanceMultiDrug Resistance Pumps
Briefly describe the main antibiotic mechanisms?