920.full
DESCRIPTION
bvfjhTRANSCRIPT

EHRA POSITION PAPER
Management of patients with palpitations: aposition paper from the European HeartRhythm AssociationAntonio Raviele1*, Franco Giada2, Lennart Bergfeldt3, Jean Jacques Blanc4,Carina Blomstrom-Lundqvist5, Lluis Mont6, John M. Morgan7, M.J. Pekka Raatikainen8,Gerhard Steinbeck9, and Sami Viskin10
Document reviewers: Paulus Kirchhof (review coordinator)11, Frieder Braunschweig12, Martin Borggrefe13, Meleze Hocini14, Paolo Della Bella15, and DipenChandrakant Shah16
1Cardiovascular Department, Arrhythmia Center & Center for Atrial Fibrillation, Dell’Angelo Hospital, Via Paccagnella 11, 30170 Mestre-Venice, Italy; 2Cardiovascular Department,PF Calvi Hospital, Noale-Venice, Italy; 3Cardiology Department, Salgrenska University, Gothenburg, Sweden; 4Cardiology Department, Bretagne University, Brest, France;5Cardiology Department, Uppsala University Hospital, Uppsala, Sweden; 6Cardiology Department, Hospital Clinic, University of Barcelona, Barcelona, Spain; 7Wessex CardiacCenter, Southampton University Hospital, Southampton, UK; 8Heart Center, Tampere University Hospital, Tampere, Finland; 9Internal Medicine, Ludwig-Maximilians University,Munich, Germany; 10Tel Aviv Sourasky Medical Center and Sackler School of Medicine, Tel Aviv University, Israel; 11University Hospital Muenster, Muenster, Germany; 12KarolinskaUniversity Hospital, Stockholm, Sweden; 13Universitaetsmedizin Mannheim, Mannheim, Germany; 14Hopital du Haut Leveque, Pessac, France; 15Ospedale San Raffaele, Milan, Italy;and 16Cantonal Hospital, Geneva, Switzerland
Introduction
Aim of the documentPalpitations are among the most common symptoms that promptpatients to consult general practitioners, cardiologists, or emer-gency healthcare services.1 –4 Very often, however, the diagnosticand therapeutic management of this symptom proves to bepoorly efficacious and somewhat frustrating for both the patientand the physician. Indeed, in many cases a definitive, or at leastprobable, diagnosis of the cause of palpitations is not reachedand no specific therapy is initiated.5,6 This means that manypatients continue to suffer recurrences of their symptoms, whichimpair their quality of life and mental balance, lead to the potentialrisk of adverse clinical events, and induce continual recourse tohealthcare facilities.
These difficulties stem from the fact that palpitations are gener-ally a transitory symptom. Indeed, at the moment of clinical evalu-ation, the patient is often asymptomatic and the diagnosticevaluation focuses on the search for pathological conditions thatmay be responsible for the symptom. This gives rise to someuncertainty in establishing a cause–effect relationship betweenany anomalies that may be detected and the palpitations them-selves. Moreover, as palpitations may be caused by a wide rangeof different physiological and pathological conditions, clinicianstend to apply a number of instrumental investigations, laboratorytests, and specialist examinations, which are both time-consumingand costly. Comparable, for example, to syncope, such anapproach is warranted in selected patients, whereas other patients
with palpitations may not require such careful follow-up. The initialclinical assessment should, therefore, include an educated esti-mation of the likelihood of a relevant underlying arrhythmia in apatient with palpitations (‘gatekeeper’ function).
The current management of patients with palpitations is guidedchiefly by the clinical experience of the physician. Indeed, the lit-erature lacks specific policy documents or recommendationsregarding the most appropriate diagnostic work-up to beadopted in individual patients. The aim of this article is topropose expert advice for diagnostic evaluation in order toguide optimal management of patients with palpitations.
DefinitionPalpitations are a symptom defined as awareness of the heartbeatand are described by patients as a disagreeable sensation of pulsationor movement in the chest and/or adjacent areas.7 Implicit in thatawareness is a sense of unpleasantness which may be associatedwith discomfort, alarm, and less commonly pain. As this awarenesscauses the individual to mentally focus on their heartbeat, thenature of the heartbeat, both in terms of its perceived ‘forceful-ness’ and its rate, is assimilated into the term. Therefore, theterm is used to describe a patient’s subjective perception of abnor-mal cardiac activity in a way that may be associated with a sympto-matic cardiac arrhythmia. However, because palpitations are asymptom with a broad range of causes and underlying diseases,it does not have a rigorous and definable clinical correlate.
* Corresponding author. Tel: +39 0419657201; fax: +39 0419657235, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2011. For permissions please email: [email protected].
Europace (2011) 13, 920–934doi:10.1093/europace/eur130
by guest on August 30, 2015
Dow
nloaded from

In normal resting conditions, the activity of the heart is generallynot perceived by the individual. However, during or immediatelyafter intense physical activity or emotional stress, it may be quitenormal to become aware of one’s own heartbeat for briefperiods; these sensations are regarded as physiological palpitations,in that they represent the normal or expected response to acertain challenge or activity leading to an increase in the frequencyand strength of the contraction of the heart. Outside of such situ-ations, instead, palpitations are perceived as abnormal.5– 9
PathophysiologyLittle is known about the events responsible for heartbeat sen-sation, the afferent sensory pathways that are involved, or thehigher-order cognitive processing that filters, modulates, andamplifies these stimuli and brings some to conscious attention.10
Possible sensory receptors are myocardial, pericardial, and periph-eral mechanoreceptors, and/or peripheral baroreceptors withtheir afferent parasympathetic and sympathtic pathways.11,12 Poss-ible brain centres involved in the elaboration of afferent stimuli arethe subcortical areas (thalamus, amygdala) and the base of thefrontal lobes.
From the pathophysiological standpoint, the mechanisms under-lying palpitations are somewhat heterogeneous: contractions of theheart that are too rapid, irregular or particularly slow, as in cardiacarrhythmias including sinus tachycardia secondary to mental dis-turbance, systemic diseases, or the use of certain medications;very intense contractions and anomalous movements of the heart inthe chest, as in the case of some structural heart diseases associatedwith increased stroke volume; anomalies in the subjective perceptionof the heartbeat, whereby a normal heart rhythm or minimal irregu-larities in the cardiac rhythm are felt by the patient and are poorlytolerated, as in the case of some psychosomatic disorders. It isarguable that the pathophysiology of palpitations in these cases isa centrally mediated ‘fright reaction’ that initiates a series ofresponses which include perception of the beating heart.1
It is important to underline the fact that, although cardiacrhythm disorders generally give rise to palpitations (or otherrelated symptoms, such as fatigue, dyspnoea, dizziness, syncope,and angina), in some subjects, for reasons not entirely knownbut probably linked to some clinical characteristics (long-standingarrhythmias with relatively low maximum ventricular rate, malesex, absence of coronary heart disease, and congestive heartfailure) or to the presence of peripheral neuropathy (e.g. diabeticpatients), arrhythmias including prognostically relevant disorderssuch as non-sustained ventricular tachycardias and atrial fibrillationmay remain completely asymptomatic.11,13– 15 Thus, in suchpatients, relevant arrhythmias might not be adequately diagnosedand managed.15
Aetiological classificationFrom the aetiological point of view, the causes of palpitations canbe subdivided into five main groups (Table 1): cardiac arrhythmias,structural heart diseases, psychosomatic disorders, systemic diseases,and effects of medical and recreational drugs.3– 9 It is not uncommon,however, for the patient to have more than one potential cause ortype of palpitation. Electrocardiographic documentation of arhythm disorder during spontaneous symptoms provides thestrongest evidence of causality; whenever this proves possible,therefore, the palpitations are classified as being of arrhythmicorigin. By contrast, they are considered to be of non-arrhythmicorigin when the underlying heart rhythm exhibits sinus rhythmor sinus tachycardia. Thus, according to this aetiological hierarchy,non-arrhythmic causes of palpitations emerge as definitive diag-noses only in cases in which the symptom–electrocardiogram(ECG) correlation excludes the presence of rhythm disorders.8
When it is not possible to document the cardiac rhythm duringpalpitations, non-arrhythmic causes are regarded as probable, butnot definitive.
Palpitations due to arrhythmiasAny type of tachyarrhythmia, regardless of whether or not there isan underlying structural or arrhythmogenic heart disease, can giverise to palpitations: atrial extrasystole, ventricular extrasystole,tachycardias with regular ventricular activity (sinus tachycardia,atrioventricular node reentrant tachycardia, atrioventricular reen-trant tachycardia, atrial flutter, atrial tachycardias), and tachycardiaswith irregular ventricular activity (atrial fibrillation, atrial flutter, or
Table 1 Main causes of palpitations
Cardiac arrhythmias
Supraventricular/ventricular extrasystoles
Supraventricular/ventricular tachycardias
Bradyarrhythmias: severe sinus bradycardia, sinus pauses, second-and third-degree atrioventricular block
Anomalies in the functioning and/or programming of pacemakersand ICDs
Structural heart diseases
Mitral valve prolapse
Severe mitral regurgitation
Severe aortic regurgitation
Congenital heart diseases with significant shunt
Cardiomegaly and/or heart failure of various aetiologies
Hyperthrophic cardiomyopathy
Mechanical prosthetic valves
Psychosomatic disorders
Anxiety, panic attacks
Depression, somatization disorders
Systemic causes
Hyperthyroidism, hypoglycaemia, postmenopausal syndrome, fever,anaemia, pregnancy, hypovolaemia, orthostatic hypotension,postural orthostatic tachycardia syndrome, pheochromocytoma,arteriovenous fistula
Effects of medical and recreational drugs
Sympathicomimetic agents in pump inhalers, vasodilators,anticholinergics, hydralazine
Recent withdrawal of b-blockers
Alcohol, cocaine, heroin, amphetamines, caffeine, nicotine, cannabis,synthetic drugs
Weight reductions drugs
Managing patients with palpitations 921
by guest on August 30, 2015
Dow
nloaded from
atrial tachycardia with variable atrioventricular conduction, torsadesde pointes).16,17 By contrast, bradyarrhythmias are more rarely per-ceived as palpitations: these arrhythmias comprise sinus pauses andsevere sinus bradycardia seen in sick sinus syndrome, sudden onsetof high-degree atrioventricular block, or of intermittent left-bundlebranch block. Anomalies in the functioning and/or programming ofpacemakers and implantable cardioverter defibrillators (ICDs)(pacemaker-mediated tachycardia, pectoral or diaphragmaticstimulation, pacemaker syndrome, etc.) may also be responsiblefor palpitations.
Palpitations due to structural heartdiseaseSome structural heart diseases can give rise to palpitations in theabsence of true rhythm disorders. These include, among others,mitral valve prolapse, severe mitral and aortic regurgitation, conge-nital heart disease with significant shunt, hypertrophic cardiomyo-pathy, and mechanical prosthetic valves.18,19
Palpitations due to psychosomaticdisordersPsychosomatic disorders that are most frequently associated withpalpitations include anxiety, panic attacks, depression, and somati-zation, which can either induce sinus tachycardia or modify thepatient’s subjective perception of a heartbeat that is otherwisenormal or presents minimal irregularities.20–23 If no other poten-tial causes can be identified, the palpitations are considered tobe of psychosomatic origin when the patient fulfils the criteriaspecified in the literature for one or more of the abovementionedpsychosomatic disorders. It must be borne in mind, however, thatcardiac arrhythmias and psychosomatic disorders are not mutuallyexclusive.5,24 In addition, the adrenergic hyperactivation connectedwith intense emotions and anxiety can, in itself, predispose thepatient to supraventricular and/or ventricular arrhythmias.25 –27
Indeed, in the last few years, some studies investigating the corre-lation between anxiety syndrome and the appearance of arrhyth-mias have suggested that anxiety exerts a facilitating effect onarrhythmogenesis28 as well as on the patient’s perception of thearrhythmia.29 Finally, in a study conducted on patients with docu-mented supraventricular tachycardia, it was found that two-thirdshad previously been wrongly diagnosed as suffering from panicattack disorder, and that the diagnosed ‘psychosomatic disease’could be cured by catheter ablation in most of these patients.30
Thus, even in patients affected by psychosomatic disorders, it isimportant to carry out a thorough investigation before excludingan organic cause, particularly arrhythmic, of palpitations.
Palpitations due to systemic causesA sensation of palpitation may stem from sinus tachycardia and/orincreased cardiac contractility, both of which may have variouscauses: fever, anaemia, orthostatic hypotension, hyperthyroidism/thyreotoxicosis, postmenopausal syndrome, pregnancy, hypogly-caemia, hypovolaemia, pheochromocytoma, arteriovenous fistula,postural orthostatic tachycardia syndrome, among others.31 –39
Palpitations due to the effects of medicaland recreational drugsIn such cases, palpitations may be linked to sinus tachycardia; drugsinvolved include sympathomimetics, anticholinergics, vasodilators,and hydralazine.40 The sudden suspension of b-blocker therapymay also give rise to sinus tachycardia and palpitations throughthe induction of a hyperadrenergic state as a result of the‘rebound’ effect. Moreover, palpitations may even occur after theinitiation or dose-increase of b-blockers, due to the perceptionof pulsations caused by increased stroke volume with lowerheart rate, or ventricular ectopic beats if sinus overdrive is with-drawn. Likewise, stimulants such as caffeine and nicotine, or theuse of illicit drugs (cocaine, heroin, amphetamines, LSD, syntheticdrugs, cannabis, etc.) can lead to sympathetic hyperactivation andsinus tachycardia, even in young subjects without heartdisease.41,42 Drugs that prolong QT and predispose patients to tor-sades de pointes and other tachyarrhythmias, such as antidepressivedrugs, besides provoking dizziness or syncope, may also inducearrhythmia-related palpitations.43,44 In the absence of other poten-tial causes, palpitations are regarded as secondary to the use ofdrugs when they are associated temporally to administration ofthe drug and when they cease on suspension of the drug.
EpidemiologyThe prevalence of palpitations is dependent on definitions anddiagnostic methods used and varies substantially in different popu-lations. Nevertheless, there is evidence that palpitations are a veryfrequent symptom in the general population2,9 and, in particular, inpatients suffering from hypertension or heart disease. In studies inprimary care settings, palpitations account for 16% of the symptomsthat prompt patients to visit their general practitioner, and aresecond only to chest pain as the presenting complaint for specialistcardiologic evaluation.1,3,4 This high prevalence of palpitationsemphasizes the need for a structured, ideally evidence-based, step-wise work-up that may allow to distinguish, since the beginning,between patients with benign prognosis and those with poorerprognosis.
With regard to the prevalence of the various causes of palpita-tions, clinical evidence indicates that a considerable number of sub-jects with palpitations have normal sinus rhythm or minor rhythmanomalies, such as short bursts of supraventricular extrasystoles orsporadic ventricular extrasystoles. Nevertheless, clinically signifi-cant arrhythmias such as atrial fibrillation/flutter or paroxysmalsupraventricular tachycardias are also a frequent finding.45,46 In aprospective study by Weber and Kapoor47 in 190 patients present-ing with a complaint of palpitations at an university medical centre,palpitations were due to arrhythmias in 41% of these patients (16%of whom had atrial fibrillation/flutter, 10% had supraventriculartachycardia, and 2% had ventricular tachycardia), to structuralheart disease in 3%, to psychosomatic disorders in 31% (mainlypanic and anxiety disorders), to systemic causes in 4%, and to theuse of a medication, illicit substances, or stimulants in 6%. Accordingto the case records, the prevalence of anxiety syndrome and panicattacks in patients with palpitations ranges from 15% to 31%.20 –22
In the study by Weber and Kapoor,47 male sex, description of an
A. Raviele et al.922
by guest on August 30, 2015
Dow
nloaded from

irregular heartbeat, history of heart disease, and event duration.5 min were found to be independent predictors of a cardiacaetiology. No specific cause of palpitations could be identified in16% of the patients despite a thorough evaluation including theuse of loop recorders. Indeed, it is not always possible to establisha definite cause of palpitations; often, only a likely cause can begiven, and, in some cases, several possible causes have to betaken into consideration.8,42 In the literature, there are insufficientdata about the age and gender distribution of palpitations. Ingeneral, however, older patients and men are more likely tohave an arrhythmic cause of palpitations and younger patientsand women a psychosomatic cause.47– 51
PrognosisThe prognostic implications of palpitations are dependent on theunderlying aetiology as well as clinical characteristics of thepatient. Available data, especially in terms of long-term prognosis,are scarce. Although palpitations are generally associated with lowrates of mortality,4,47 they should bring to attention a potentialserious condition in patients with structural or arrhythmogenicheart disease or a family history of sudden death. This is alsoimportant to keep in mind if the palpitations are associated withsymptoms of haemodynamic impairment (dyspnoea, syncope, pre-syncope, dizziness, fatigue, chest pain, neurovegetative symp-toms).5 On the one hand, depending on the clinical characteristicsof the patient, palpitations due to arrhythmias, in particular of ven-tricular origin, but also atrial fibrillation, are associated with differ-ent prognostic implications.15– 17 On the other hand, in patientswithout relevant heart disease, palpitations (especially ifanxiety-related or extrasystolic) generally have a benign prognosis.A retrospective American study that analysed case recordsobtained from general practitioners found no difference in 5-yearmortality and morbidity between patients with palpitations and agroup of asymptomatic control subjects.4 Also in the abovemen-tioned study by Weber and Kapoor47 on a general population ofpatients presenting with palpitations at an university medicalcentre, despite the high rate of cardiac cause, 1-year mortalitywas only 1.6%. However, even in patients without severe heartdisease, palpitations may be due to significant arrhythmias, suchas atrial fibrillation, atrial flutter, or ventricular ectopic beats, allof which require adequate investigation and treatment. Moreover,clinical characteristics of the patient, such as age, presence of heartdisease, and ECG abnormalities, do not always allow the physicianto identify a priori those cases in which palpitations are caused byclinically significant rhythm disorders.8,47,48,52 –54 An exception tothis is given by changes in the resting ECG that are indicative ofprimary electrical heart diseases.
In athletes, palpitations are not uncommon. Sudden death, inparticular in younger athletes, is rare and mostly associated withunderlying structural heart disease or primary arrhythmic dis-orders, and palpitations may be the initial clinical symptom or anincidental finding possibly leading to the recognition of a previouslyundiagnosed relevant heart disease.55,56 Moreover, because ofpotentially life-threatening haemodynamic consequences of evensupraventricular arrhythmias, such as rapidly conducted pre-excited atrial fibrillation during exertion, careful cardiac evaluation,
in particular of symptomatic competitive as well as recreationalathletes, is warranted.57
Although palpitations display a low mortality rate, the recurrenceof symptoms is, however, very frequent. In the study by Weber andKapoor,47 77% of patients experienced at least one recurrence ofpalpitations, and the effect on their quality of life was unfavourable:one-third of patients reported an impairment of their ability toattend to household chores, 19% claimed that their workingcapacity had diminished, and 12% said that they had taken daysoff work. These findings are confirmed by a prospective study con-ducted by Barsky et al.58 on 145 patients with palpitations, whowere followed up for 6 months and compared with an asympto-matic control group. These authors observed that patients withpalpitations, in spite of having a favourable prognosis in terms ofmortality, remained symptomatic and functionally impaired overtime and exhibited a high incidence of panic attacks and psycho-logical symptoms.58 Frequent and recurrent palpitations, therefore,can impair the patient’s quality of life, giving rise to anxiety and fre-quent visits to the emergency department.3 In many respects, pal-pitations seem to behave like a chronic disorder that has afavourable prognosis, but with periodic attacks followed by transi-tory remission.3,4
Clinical presentation
Duration and frequency of palpitationsWith regard to duration, palpitations may be either short-lasting orpersistent. In short-lasting forms, the symptom terminates spon-taneously within a brief period of time. In persistent forms, the pal-pitations are ongoing and terminate only after adequate medicaltreatment. With regard to frequency, palpitations may occurdaily, weekly, monthly, or yearly.
Types of palpitationsPatients report a wide range of sensations to describe their symp-toms. The most common descriptions, and those most useful inclinical practice in differential diagnoses among the variouscauses of palpitations, enable palpitations to be classified accordingto the rate, rhythm, and intensity of heartbeat5 –9,59,60: extrasystolicpalpitations, tachycardiac palpitations, anxiety-related palpitations,and pulsation palpitations (Table 2). It should, however, be stressedthat patients are not always able to describe the characteristics oftheir symptoms precisely. It may therefore be difficult to identifythe type of palpitation accurately, especially in the case of normal-rate palpitations.5,9,61
Extrasystolic palpitations, due to ectopic beats, generally producefeelings of ‘missing/skipping a beat’ and/or a ‘sinking of the heart’interspersed with periods during which the heart beats normally;patients report that the heart seems to stop and then startagain, causing an unpleasant, almost painful, sensation of a blowto the chest. Linked to the presence of atrial or ventricular extra-systolic beats, this type of palpitation is frequently encounteredeven in young subjects, often in the absence of heart disease,and generally has a benign prognosis. In extrasystolic palpitations,particularly if they are of ventricular origin, the sensation is dueto the increased strength of contraction of the post-extrasystolic
Managing patients with palpitations 923
by guest on August 30, 2015
Dow
nloaded from

beat, which accentuates the movement of the heart inside thechest, or to the post-extrasystolic pause, or to the altered acti-vation of the heart. When the extrasystoles are particularly numer-ous and/or repetitive, it may prove difficult to make a differentialdiagnosis between extrasystolic and tachycardiac palpitations,especially those due to atrial fibrillation.
In the case of tachycardiac palpitations, the sensation described bythe patient is that of a rapid fluctuation like ‘beating wings’ in thechest. The heartbeat is generally perceived to be very rapid (some-times higher than the maximum heart rate estimated on the basisof the patient’s age); it may be regular, as in atrioventricular reen-trant tachycardia, atrial flutter, or ventricular tachycardia, or irregu-lar or arrhythmic, as in atrial fibrillation or post-atrialfibrillation-ablation atypical atrial flutter (Table 3). These palpita-tions are generally linked to supraventricular or ventriculartachyarrhythmias, which begin and usually end suddenly (some-times the termination is gradual due to the increase in sympathetictone during tachycardia that tends to persist and declines slowlyafter its interruption), or to sinus tachycardia due to systemiccauses or to the use of drugs or illicit substances (in these cases,palpitations begin and end gradually).
Anxiety-related palpitations are perceived by the patient as a formof anxiety. The heartbeat is slightly elevated, but never higher thanthe maximum heart rate estimated on the basis of the patient’s age.These palpitations, whether paroxysmal or persistent, begin and
end gradually, and patients describe numerous other associatedunspecific symptoms, such as tingling in the hands and face, alump in the throat, mental confusion, agitation, atypical chestpains, and sighing dyspnoea, that normally precede the palpitations.Anxiety-related palpitations are due to psychosomatic disordersand usually require exclusion of an arrhythmic cause of thesymptoms.
Pulsation palpitations are felt as strong, but regular and not par-ticularly rapid, heartbeats. They tend to be persistent and are gen-erally linked to structural heart diseases, such as aorticregurgitation, or to systemic causes involving a high strokevolume, such as fever and anaemia.
Associated symptoms and circumstancesCertain symptoms and circumstances associated to palpitations areoften connected with the various causes of the palpitations and maybe very helpful in making differential diagnoses.5–9,59,60 Palpitationsarising after sudden changes in posture are frequently due to intol-erance to orthostatis or to episodes of atrioventricular nodal reen-trant tachycardia. The occurrence of syncope or other symptoms,such as severe fatigue, dyspnoea, or angina, in addition to palpita-tions, is much more frequent in patients with structural heartdisease. However, syncope may also occur at the onset of supraven-tricular tachycardia in patients with a normal heart, as the result ofthe triggering of a vasovagal reaction.62,63
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Types of palpitations and their clinical presentations
Type ofpalpitation
Subjectivedescription
Heartbeat Onset andtermination
Triggersituations
Possible associated symptoms
Extrasystolic ‘Skipping/missing abeat’, ‘sinking of theheart’
Irregular, interspersed withperiods of normalheartbeat
Sudden Rest —
Tachycardiac ‘Beating wings’ in thechest
Regular or irregular,markedly accelerated
Sudden Physical effort,cooling down
Syncope, dyspnoea, fatigue, chestpain
Anxiety-related Anxiety, agitation Regular, slightlyaccelerated
Gradual Stress, Anxietyattacks
Tingling in the hands and face, lumpin the throat, atypical chest pain,sighing dyspnoea
Pulsation Heart pounding Regular, normal frequency Gradual Physical effort Asthenia
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 Clinical characteristics of tachycardiac palpitations
Type of arrhythmia Heartbeat Trigger situations Associated symptoms Vagal manoeuvres
AVRT, AVNRT Sudden onset regular with periods ofelevated heart rate
Physical effort, changes inposture
Polyuria, frog sign Sudden interruption
Atrial fibrillation Irregular with variable heart rate Physical effort, cooling down,post meal, alcohol intake
Polyuria Transitory reductionin heart rate
Atrial tachycardia andatrial Flutter
Regular (irregular if A-V conduction isvariable) with elevated heart rate
Transitory reductionin heart rate
Ventriculartachycardias
Regular with elevated heart rate Physical effort Signs/symptoms ofhaemodynamicimpairment
No effect
AVRT, atrio-ventricular reentrant tachycardia; AVNRT, atrio-ventricular node reentrant tachycardia; A-V, atrioventricular.
A. Raviele et al.924
by guest on August 30, 2015
Dow
nloaded from

Polyuria, which is due to the hypersecretion of natriuretichormone, is typical of atrial tachyarrhythmias, particularly atrialfibrillation. By contrast, the sensation of a rapid, regular pulse inthe neck (usually associated with the ‘frog sign’) raises suspicionof supraventricular tachycardia, particularly atrioventricular nodalreentrant tachycardia.64 It is the result of atria contracting againstclosed tricuspid and mitral valves.9,65 An atrioventricular mechan-ical dissociation may also occur in the case of ventricular extrasys-toles. In this case, however, only one or few pulses are felt in theneck, and the rhythm is more irregular. In supraventricular tachy-cardias involving the atrioventricular node, patients often learnto interrupt the episode by themselves by applying vagal stimu-lation through Valsalva’s manoeuvre or carotid sinus massage.
Palpitations that arise in situations of anxiety or during panicattacks are generally due to episodes of more or less rapid sinustachycardia secondary to the mental disturbance. In some cases,however, the patient may have difficulty in discerning whetherthe palpitations precede or follow the onset of the anxiety orpanic attack, and may therefore be unable to suggest whetherthe palpitations are the cause or the effect of the psychologicaldistress.
During physical exercise, due to an increase in the sympatheticdrive, patients may experience, in addition to the normal sensationof a rapid heart rate elicited by intense effort, palpitations due tovarious types of arrhythmia, such as right ventricular outflowtract tachycardia, atrioventricular node reentrant tachycardia, andpolymorphic catecholaminergic ventricular tachycardia. Finally, epi-sodes of paroxysmal atrial fibrillation may occur in the phaseimmediately following the cessation of physical effort, during
which a sudden reduction in sympathetic tone is accompanied byan increase in vagal tone.
Accuracy of clinical features for thediagnosis of arrhythmiasThe utility of the features on history for diagnosing an arrhythmiccause of palpitations has been examined in a recent systematicreview.48 The likelihood ratio of each feature is, in general, lowand only a few features are really predictive. They include historyof cardiac disease, palpitations affected by sleeping, or while thepatient is at work. Other features such as underlying history ofpanic disorder and duration of palpitations less than 5 minappear to be useful for ruling out a clinically significant arrhyth-mia.47 However, data in this regard come from studies withsmall sample sizes.
Diagnostic strategyIn patients with palpitations the diagnostic strategy should aim at:(i) distinguishing the mechanism of the palpitations; (ii) obtainingan electrocardiographic recording during symptoms; and (iii) eval-uating the underlying heart disease. All patients suffering from pal-pitations should therefore undergo an initial clinical evaluationcomprising history, physical examination, and a standard 12-leadECG (Figure 1). This usually should be performed in a primarycare setting.
In specific situations, specialist evaluation and certain specificinstrumental and laboratory investigations should be considered.59
Definitive§ or suspected diagnosis unexplained palpitations
confirmation
+ -
treatment
heart disease or abnormal ECG
-+
treatment ILR
stop
Echo,AECG,MRI*,Stress Test*, EPS*
history, physical examination, ECG, psychosomatic counselling*
frequent or severe
no heart disease and normal ECG
rare or well tolerated
Figure 1 Diagnostic flow-chart of patients with palpitations. *Indicated only in selected cases; § refers to ECG–symptom correlation avail-able. ECG, electrocardiogram (12-lead); Echo, echocardiography; AECG, ambulatory ECG; MRI, magnetic resonance imaging; EPS, electro-physiological study; ILR, implantable loop recorder.
Managing patients with palpitations 925
by guest on August 30, 2015
Dow
nloaded from

Stress testing is indicated if the palpitations are associated withphysical exertion (e.g. right ventricular outflow tract extrasystoles),in athletes and when coronary heart disease is suspected. The roleof echocardiography is of paramount importance to evaluate thepresence of structural heart disease. The need to conductfurther non-invasive cardiologic investigations (particularlycardiac magnetic resonance imaging to evaluate patients withstructural normal heart, palpitations, and frequent ventriculararrhythmias) or invasive investigations (coronary angiography,etc.) will depend on the nature of the heart disease suspectedor ascertained. Comparable to exercise-induced syncope,exercise-induced palpitations should raise suspicion for ischaemic,valvular, or other structural heart disease with the correspondingwork-up. Whenever a systemic or pharmacological cause of palpi-tations is suspected, specific laboratory tests should be performedon the basis of the clinical presentation of the symptom and thepatient’s clinical characteristics (e.g. haemochrome, electrolytes,glycaemia, thyroid function, urinary catecholamines, detection ofillicit substances in the blood or urine). If, on the contrary, a psy-chosomatic cause is suspected, the patient’s mental state must beassessed either by means of specific questionnaires or throughreferral for specialist examination.7,8,20–23
The initial clinical evaluation leads to a definitive or probablediagnosis of the cause of the palpitations in about half of patients,and excludes with reasonable certainty the presence of causes thathave an unfavourable prognosis.47 Moreover, a thorough initialclinical evaluation will indicate which specific investigations, if any,are necessary.
If the initial clinical evaluation proves completely unremarkable—which is more frequent in paroxysmal, short-lastingpalpitations—the palpitations are deemed to be of unknownorigin. In subjects with palpitations of unknown origin who have alow probability of an arrhythmic cause (i.e. patients with gradualonset of palpitations and without significant heart disease and thosewith anxiety-related or extrasystolic palpitations), further investi-gations are often not required. The patient should be reassured and afollow-up clinical examination may be scheduled. It should be under-lined, however, that, in the absence of electrocardiographic record-ing during an episode of palpitations, only a presumed or probablediagnosis can be made.30 By contrast, in instances of subjects withpalpitations of unknown origin presenting with clinical features sug-gestive of an arrhythmic cause66 (Table 4), or when palpitations aresuspected to be related to atrial fibrillation in individuals with riskfactors for thromboembolism,14,67 patients should be referred to
an arrhythmia centre, and second-level investigations should be con-sidered; these include ambulatory ECG monitoring and electro-physiological study (EPS) (Figure 1). Finally, second-levelinvestigations should also be carried out in patients with palpitationsof unknown origin whose symptoms are frequent or associated withimpaired haemodynamic function or impaired quality of life or states ofanxiety.9
Initial clinical evaluation
HistoryIt represents a major part of the initial examination as mostpatients at the time they visit a physician have no palpitationsand the diagnosis has to be performed retrospectively.5– 9,48 Thefirst step is to establish that symptoms described by the patientmatch to palpitations and are not confused with chest pain orother manifestations arising in the chest, but that do not corre-spond to the definition of palpitations described in this article.
When this first step has been achieved several important ques-tions have to be asked, the most important of which are summar-ized in Table 5. Answers to some of these questions may require
Table 4 Clinical features suggestive of palpitations ofarrhythmic origin
Structural heart disease
Primary electrical heart disease
Abnormal ECG
Family history of sudden death
Advanced age
Tachycardiac palpitations
Palpitations associated with haemodynamic impairment
Table 5 Main questions to ask a patient withpalpitations
Circumstances prior to the beginning of palpitations
Activity (rest, sleeping, during sport or normal exercise, change inposture, after exercise)
Position (supine or standing)
Predisposing factors (emotional stress, exercise, squatting orbending)
Onset of palpitations
Abrupt or slowly arising
Preceded by other symptoms (chest pain, dyspnoea, vertigo, fatigue,etc.)
Episode of palpitations
Type of palpitations (regular or not, rapid or not, permanent or not)
Associated symptoms (chest pain, syncope or near syncope,sweating, pulmonary oedema, anxiety, nausea, vomiting, etc.)
End of the episode
Abrupt or slowly decreasing, end or perpetuation of accompanyingsymptoms, duration, urination
Spontaneously or with vagal manoeuvres or drug administration
Background
Age at the first episode, number of previous episodes, frequencyduring the last year or month
Previous cardiac disease
Previous psychosomatic disorders
Previous systemic diseases
Previous thyroid dysfunction
Family history of cardiac disease, tachycardia or sudden cardiacdeath
Medications at the time of palpitations
Drug abuse (alcohol and/or others)
Electrolytes imbalance
A. Raviele et al.926
by guest on August 30, 2015
Dow
nloaded from
inputs from other members of the family or from individuals whohave witnessed an episode of palpitations. Description of the typeof palpitations (regular or not, rapid or not) could help to deter-mine its underlying mechanism (Table 2). It may be useful to askthe patient to mimic the perceived cardiac rhythm, either vocallyor by drumming with the fingers on a table.
Circumstances during which palpitations have occurred are gen-erally helpful to evaluate their cause. Some of these circumstancesare presented in Table 3. When, after this history-taking, itbecomes likely that palpitations are not related to arrhythmiabut rather to psychosomatic disorders, before starting moreextensive cardiovascular procedures, it is judicious to take thehelp of a mental health expert.1,22,23,47,58
It is naturally useless to perform this extensive history-taking ifthe patient has the feeling of palpitation even during the consul-tation. The first examination in these circumstances is to instan-taneously record ECG.
Physical examinationDuring palpitationsThe execution of the physical examination while the patient is stillsymptomatic is not the most frequent situation. However, whenthis occurs it is crucial to have some notions about frequencyand regularity of heart rhythm by listening to the patient’s chestor by palpation of the arterial pulse. The differential diagnosis ofvarious types of tachycardia may be guided by vagal manoeuvres68
such as carotid sinus massage: sudden interruption of the tachycar-dia is highly suggestive of a tachycardia involving the atrioventricu-lar junction whereas a temporary reduction of the frequency issuggestive of atrial fibrillation, flutter, or atrial tachycardia (Table 3).
When this essential stage has been performed, examinationshould aim to evaluate the tolerance of a possible heart rhythmdisturbance (blood pressure, signs of cardiac failure, and so on),to assess the cardiovascular status (i.e. the presence of structuralheart disease), and, in case of a sinus rhythm or sinus tachycardia,to evaluate the presence of systemic diseases potentially respon-sible for palpitations.
In the absence of palpitationsWhen the patient is examined in the absence of the culpritsymptom, the aim is to find signs of structural heart disease thatcould explain the occurrence of palpitations (cardiac murmur,hypertension, vascular diseases, signs of heart failure, and so on).It is also important to search for signs of systemic diseases.
Standard electrocardiogramDuring palpitationsIf the patient is examined during palpitations, 12-lead ECG rep-resents the diagnostic gold standard. Thus, patients should beadvised to come as quickly as possible to an emergency depart-ment or a physician when an ECG has never been recordedduring symptoms. It allows the physician to analyse P and QRSmorphologies and the relationship between these two waves,and the frequency and regularity of the heart rhythm, and finallybrings an accurate diagnosis on the concordance between palpita-tions and the presence or absence of arrhythmia. This distinctionbetween arrhythmic or non-arrhythmic palpitation is of paramount
importance for the future evaluation.1,5– 9,47 Furthermore, preciseanalysis of ECG during arrhythmia either provides the mechanismor gives important data that lead to this diagnosis. It should bestressed, however, that P waves during rapid tachycardia are notalways visible, making the diagnosis difficult. Vagal manoeuvresand pharmacological tests, such as intravenous adenosine or ajma-line, performed during ECG recording are of major interest as theycan unmask the atrial activity or interrupt suddenly the tachycardia,resulting in the diagnosis of the type of arrhythmia.16,68 Alterna-tively, the possibility of taking a transoesophageal ECG duringtachycardia must be considered.
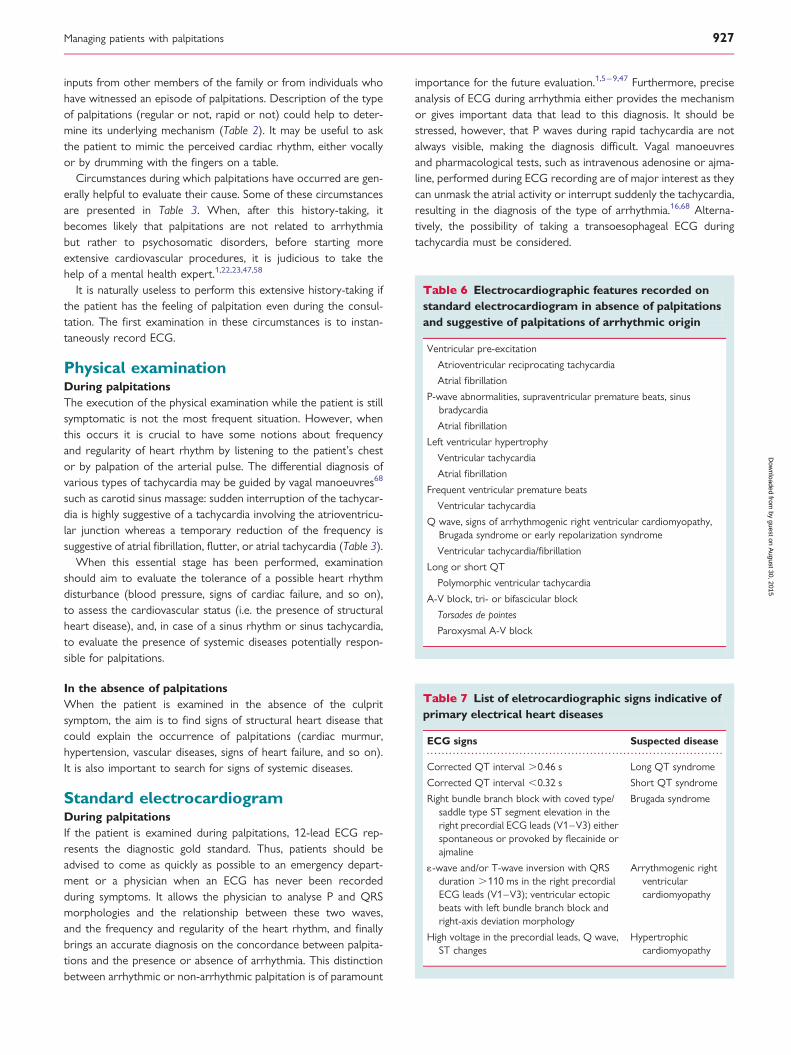
Table 6 Electrocardiographic features recorded onstandard electrocardiogram in absence of palpitationsand suggestive of palpitations of arrhythmic origin
Ventricular pre-excitation
Atrioventricular reciprocating tachycardia
Atrial fibrillation
P-wave abnormalities, supraventricular premature beats, sinusbradycardia
Atrial fibrillation
Left ventricular hypertrophy
Ventricular tachycardia
Atrial fibrillation
Frequent ventricular premature beats
Ventricular tachycardia
Q wave, signs of arrhythmogenic right ventricular cardiomyopathy,Brugada syndrome or early repolarization syndrome
Ventricular tachycardia/fibrillation
Long or short QT
Polymorphic ventricular tachycardia
A-V block, tri- or bifascicular block
Torsades de pointes
Paroxysmal A-V block
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 7 List of eletrocardiographic signs indicative ofprimary electrical heart diseases
ECG signs Suspected disease
Corrected QT interval .0.46 s Long QT syndrome
Corrected QT interval ,0.32 s Short QT syndrome
Right bundle branch block with coved type/saddle type ST segment elevation in theright precordial ECG leads (V1–V3) eitherspontaneous or provoked by flecainide orajmaline
Brugada syndrome
1-wave and/or T-wave inversion with QRSduration .110 ms in the right precordialECG leads (V1–V3); ventricular ectopicbeats with left bundle branch block andright-axis deviation morphology
Arrythmogenic rightventricularcardiomyopathy
High voltage in the precordial leads, Q wave,ST changes
Hypertrophiccardiomyopathy
Managing patients with palpitations 927
by guest on August 30, 2015
Dow
nloaded from

In the absence of palpitationsEven when the ECG is recorded in the absence of palpitations itprovides important data that can suggest the arrhythmic origin ofpalpitations (Tables 6 and 7). In some instances, for example incase of evident pre-excitation when the patient reports rapidregular palpitations, the diagnosis is formal even if tachycardiahas never been recorded.
Ambulatory electrocardiogrammonitoringAmbulatory ECG monitoring serves to document the cardiacrhythm during an episode of palpitations if this cannot be doneby means of standard ECG, as in the case of short-lasting symp-toms. Indeed, ambulatory ECG monitoring utilizes electrocardio-graphic recorders that are able to monitor the patient’s cardiacrhythm for long periods of time or that can be activated by thepatient when symptoms occur.69,70
The devices currently used for ambulatory ECG monitoring canbe subdivided into two main categories: external and implantable.External devices comprise Holter recorders, hospital telemetry(reserved for hospitalized patients at high risk of malignant arrhyth-mias), event recorders, external loop recorders, and, very recently,mobile cardiac outpatient telemetry. Implantable devices comprisepacemakers and ICDs equipped with diagnostic features (usedexclusively in patients requiring such devices for therapeutic pur-poses) and implantable loop recorders (ILRs).
Event recorders or handheld patient-operated ECG systemshave been shown to improve the diagnosis of transient ECGchanges in patients with palpitations.71,72 These devices are reason-ably priced and easy to use. The external and implantable looprecorders, mobile cardiac outpatient telemetry, and pacemakersand ICDs can detect asymptomatic clinically significant arrhythmiasautomatically (i.e. with no activation by the patient) and provide asignificantly higher yield than standard patient-activated loop recor-ders in patients with infrequent palpitations.49,73– 79 Another majorbenefit of the latest diagnostic systems is that many of them notonly allow automatic detection of the arrhythmias but also allowimmediate wireless transmission of pertinent ECG data to a centralmonitoring station via a mobile telephone line or the Internet.The alarms incorporated into the network providing telemetricdata to specialists improve the efficiency of patient management,since the physicians can check their patient’s data remotely withno delay. This permits greater emphasis on documentation andcharacterization of spontaneous arrhythmic episodes, and it isexpected to allow prompt reaction to clinical events as well asto act as a potential for reduced resource use.80 Moreover, theability to detect the onset of the episode provides valuable infor-mation on the mechanism of the arrhythmias. The main technicalcharacteristics of the different ambulatory ECG monitoringsystems are summarized in Table 8.
Diagnostic valueAmbulatory ECG monitoring is regarded as diagnostic only when it ispossible to establish a correlation between palpitations and an elec-trocardiographic recording.69,70 In patients who do not develop
symptoms during monitoring, therefore, this examination is oftennon-contributory. In some patients without palpitations on monitor-ing, the presence of clinically significant arrhythmias that are
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 8 Technical characteristics of the differentambulatory electrocardiogram monitoring devices
Device Characteristics
Holter monitoring Utilizes external recorders connected to thepatient by means of skin electrodes; theserecorders are able to perform continuousbeat-to-beat electrocardiographicmonitoring via several leads (up to 12 inthe latest models).
Event recorders Small, easy-to-use, portable devices that areapplied to the patient’s skin wheneversymptoms are experienced. They provideprospective one-leadelectrocardiographic recording for a fewseconds.
External looprecorders
Connected continuously to the patient bymeans of skin electrodes and equippedwith a memory loop, these devicesprovide one to three-leadelectrocardiographic recording for a fewminutes before and after activation by thepatient when symptoms arise. The latestdevices are also able to self-activateautomatically when arrhythmic eventsoccur.
Mobile cardiacoutpatienttelemetry
Made up of an external loop recorderconnected to the patient by means of skinelectrodes, and of a portable receiver thatis able to transmit an electrocardiographictrace to a remote operating centre or to adedicated website via the telephone. Inthis way, the patient’s rhythm can bemonitored in real time.
Implantable looprecorders
Similar in size to a pacemaker, these devicesare implanted beneath the skin through asmall incision of about 2 cm in the leftprecordial region. They are equipped witha memory loop and, once activated by thepatient through an external activator atthe moment when the symptoms arise,record one-lead electrocardiographictrace for several minutes before and afterthe event. They are also able to record anyarrhythmic event automatically (i.e. withno intervention by the patient). In general,monitoring lasts either until a diagnosis isreached or until the battery runs down.On completion of monitoring, the deviceis removed from the patient.
Pacemakers/ICDs Provided by an internal memory, they areable to detect and store an atrial andventricular IEGM separately (dualchamber devices), and to record anyarrhythmic events automatically. Somemodels may also be activated manually bythe patients when palpitations occur.
IEGM, intracardiac electrogram.
A. Raviele et al.928
by guest on August 30, 2015
Dow
nloaded from

asymptomatic (i.e. not associated with palpitations) may suggest aprobable diagnosis and/or guide the decision to undertake furtherinvestigations.15,59 The specificity of ambulatory ECG monitoring, atleast in formulating a diagnosis of arrhythmic palpitations or non-arrhythmic palpitations, is optimal, whereas the sensitivity is extre-mely variable and depends on the following factors: the monitoringtechniques used, the duration of monitoring, patient compliance,and, most importantly, the frequency of the attacks.
In patients with palpitations of unknown origin, Holter monitor-ing has displayed a rather low sensitivity value (33–35%).81 In ameta-analysis of seven studies conducted on patients withsyncope and/or palpitations of unknown origin, Holter monitoringhas been seen to have a sensitivity value of only 22%.82 By contrast,in patients in whom the symptoms are quite frequent (i.e. daily orweekly), external loop recorders and event recorders have shownboth a higher diagnostic value (66–83%) and a better cost/effec-tiveness ratio than Holter devices.71,83 Finally, in patients withsymptoms of possible arrhythmic origin, mobile cardiac outpatienttelemetry has been seen to exhibit a higher diagnostic value thanthe other external devices.71,84,85
ILRs have been successfully used to study syncope, in which theyhave shown a better cost/effectiveness ratio than the conventionaltests,86,87 and they can be useful in the study of palpitations ofunknown origin.69,88,89 Indeed, the RUP study (recurrent unex-plained palpitations study) recently demonstrated the superiorityof ILR over the conventional diagnostic strategy of Holter andevent recorder monitoring and EPS in the evaluation of a relativelysmall cohort of patients with infrequent palpitations (i.e. monthlyfrequency) reporting both a higher diagnostic value (73% vs. 21%)and a better cost/effectiveness ratio.52 In patients implanted withpacemakers or ICDs, useful information on the origin of palpitationscan be obtained by interrogating the memory of the device.90
Although many patients with palpitations of unknown originwho undergo ambulatory ECG monitoring prove to have rhythmdisorders that are generally benign, such as atrial or ventricularpremature beats, or episodes of sinus rhythm and sinus tachycar-dia, a substantial percentage (6–35%) of the arrhythmias diagnosedprove to be clinically significant, such as supraventricular tachycar-dias and atrial fibrillation.5 Ventricular tachycardia is much lesscommon and is typical of patients with structural or arrhythmo-genic heart diseases. Finally, a small percentage of patients with pal-pitations of unknown origin have major bradyarrhythmic disorders,such as severe sinus bradycardia and paroxysmal advanced atrio-ventricular block.52,71
LimitationsAmbulatory ECG monitoring has some important limitations.Indeed, it is not always possible to formulate a precise diagnosisof the type of arrhythmia recorded, especially when single-leadECG devices are used. For example, it may be difficult to make acorrect differential diagnosis between a supraventricular tachycar-dia with aberrant conduction and a ventricular tachycardia. More-over, ambulatory ECG monitoring is unable to distinguish withcertainty between bradyarrhythmias due to a reflex mechanismand those caused by a disorder of the cardiac conductionsystem, a distinction that has prognostic and therapeutic impli-cations. Finally, ambulatory ECG monitoring requires the patient
to experience a recurrence of symptoms. This delays the diagnosisand, should the palpitations be due to malignant arrhythmias,exposes the patient to the potential risk of adverse events. Themain advantages and limitations of the different ambulatory ECGmonitoring systems are summarized in Table 9.
IndicationsAccording to the ACC/AHA guidelines for the use of ambulatoryECG monitoring,69,70 recurrent palpitations of unknown originconstitute a class-I indication for long-term ECG monitoring. Therecommendations regarding the choice of the ambulatory ECGmonitoring device most suited to the individual patient arereported in Table 9. ILRs are used in selected patients withsevere and infrequent palpitations (inter-symptom interval .4weeks) and when all other investigations, including external ambu-latory ECG monitoring, prove to be negative.66
Electrophysiological studyElectrophysiological study, as an invasive procedure, is usually con-sidered at the end of the diagnostic work-up. However, EPS hassome important advantages over ambulatory ECG monitoring.First of all, it is able to correctly identify the type of arrhythmiaresponsible for the palpitations. Moreover, it enables ablativetherapy of the induced tachyarrhythmias to be performed duringthe same session in which the diagnosis is made. Finally, whileEPS enables a diagnosis to be made and specific therapy to beinitiated immediately, ambulatory ECG monitoring requires thepatient to experience a recurrence of symptoms. This delays thediagnosis and, should the palpitations be due to malignant arrhyth-mias, exposes the patient to the potential risk of adverse events.For this reason, in patients with significant heart disease and inthose with palpitations that precede syncope, in whom the riskof adverse events is higher, electrophysiological evaluation gener-ally precedes the use of ambulatory ECG monitoring. In all othercases, it normally follows ambulatory ECG monitoring when thelatter proves non-diagnostic. For the recommendations of EPS inpatients with palpitations of unknown origin we refer thereaders to the ACC/AHA/ESC 2003 Guidelines on supraventricu-lar arrhythmias16 and the ACC/AHA/ESC 2006 Guidelines formanagement of patients with ventricular arrhythmias and the pre-vention of sudden cardiac death.17
Specific needs in patients at riskof strokeIt is well known that atrial fibrillation is associated with anincreased risk of thromboembolism, especially in patients withcertain risk factors as those considered in the CHA2DS2VAScrisk score.14 It is therefore important to exclude atrial fibrillation asthe underlying cause of the symptoms in patients with palpitationsof unknown origin and a high thromboembolic risk.
However, it must be underlined that once atrial fibrillation hasbeen diagnosed as a cause of palpitations, there is up to nowonly limited data on the importance of assessing atrial fibrillation
Managing patients with palpitations 929
by guest on August 30, 2015
Dow
nloaded from

burden for the evaluation of thromboembolic risk, and more infor-mation is still needed.67,91
TherapyTherapy for palpitations is, of course, directed towards the aetio-logical cause (i.e. treatment of cardiac arrhythmias, structural heartdiseases, psychosomatic disorders, or systemic diseases) wheneverit can be determined. However, many of the suggestions that canbe made are based on clinical experience, without scientific docu-mentation to rely on.
When a clear-cut aetiology is established and a low-risk curativetherapy is available (e.g. ablation for supraventricular arrhythmias),there is no doubt that this is the treatment of choice.92 Moreover,in many benign arrhythmias (e.g. premature beats), a number ofgeneral factors may influence and modulate the frequency andseverity of the symptoms. In this context, changes in lifestyle(e.g. restraining adrenergic substances such as caffeine or alcohol-containing beverages) or non-cardiologic therapies (e.g. anxiolyticdrugs or psychiatric counselling) may be useful to control symp-toms and should be considered. At times, reassurance of thepatient on the benign nature of the disorder can markedlyreduce symptoms.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 9 Advantages, limitations, and indications of the different ambulatory electrocardiogram monitoring devices
Holter monitoring Event recorders External looprecorders/MCOT
Implantable looprecorders
Pacemakers/ICDs
Advantages Low cost; possibility torecord asymptomaticarrhythmias
Low cost; easy to use Retrospective andprospective ECGrecords; possibility torecord asymptomaticarrhythmiasautomatically
Retrospective andprospective ECGrecords; quite goodECG records;monitoring capability upto 36 months; possibilityto record asymptomaticarrhythmiasautomatically
Better discriminationbetween ventricular andsupraventriculararrhythmias, due to dualchamber IEGMrecordings; betterdefinition of arrhythmicburden; monitoringduration for many years(corresponding to theexpected life of thedevice); possibility torecord asymptomaticarrhythmiasautomatically
Limitations Monitoring limited to24 h to 7 days; sizemay preventactivities that maytrigger thearrhythmias; patientsoften fail to completeadequately theclinical diary uponwhich thecorrelation betweensymptoms and thearrhythmiasrecorded is based
Monitoring cannot becarried out for morethan 3–4 weeks; verybrief arrhythmias arenot recorded;arrhythmic triggersare not revealed;poor ECG records
Monitoring cannot becarried out for morethan 3–4 weeks;continualmaintenance isrequired; devices areuncomfortable; quitepoor ECG records
Invasiveness; risk of localcomplications at theimplantation site: highercost; limited memoryand specificity
Invasiveness; risk of earlyand late local andsystemic complications;high costs
Indications From daily to weeklypalpitations; patientswho are unable touse otherambulatory ECGmonitoring devices
From weekly tomonthly, fairlylong-lastingpalpitations notaccompanied byhaemodynamicimpairment;compliant patients
From weekly tomonthly,short-lastingpalpitationsassociated tohaemodynamicimpairment; verycompliant patients
From monthly to yearlypalpitations associatedwith haemodynamiccompromise; when allthe other examinationsprove inconclusive;non-compliant patientswithout haemodynamiccompromise when aclinically significantarrhythmic cause islikely or must be ruledout
Only for patients withconventional indicationsto pacemakers and ICDs
IEGM, intracardiac electrogram; MCOT, mobile cardiac outpatient telemetry.
A. Raviele et al.930
by guest on August 30, 2015
Dow
nloaded from

Clearly, patients with palpitations will benefit from the samepreventive measures recommended to the general populationand to patients with cardiovascular disease.93 Especially in patientswith ventricular ectopy94 and possibly also in patients with atrialectopic beats95, although scientific evidence is lacking, intensifiedreduction of cardiovascular risk factors may be warranted. Thismay comprise, among others, smoking cessation, therapy of dysli-pidemia, management of hypertension, heart failure, and diabetesmellitus, to name but a few. Moderate exercise is a healthy habitthat helps in controlling cardiovascular risk factors. On the otherhand, high-intensity endurance sport practice has been related toan increased risk of atrial fibrillation.96
It is beyond the scope of this paper to discuss in depth thespecific therapy in all arrhythmic conditions causing palpitations.In this regard, we refer the readers to current guidelines.16,17 Inthe case that arrhythmias are found to be related to systemic dis-eases or to the use of pro-arrhythmic drugs, therapy, of course,must aim to remove the underlying conditions. The general rec-ommendations for the treatment of palpitations are listed inTable 10.
When to hospitalize the patient
Diagnostic purposesThe vast majority of patients with palpitations can be assessed in anoutpatient setting. Indeed, most of the investigations required forthe diagnostic evaluation of patients with palpitations can becarried out in an ambulatory or day-hospital setting. In the studyby Weber and Kapoor,47 an EPS and a haemodynamic studywere performed in only 5% of patients.
However, depending on the availability of outpatient ECG moni-toring devices, hospitalization may be considered for patients withvery frequent symptoms, when short-term bed-side monitoring islikely to reveal the underlying diagnosis. Moreover, patients withpalpitations should also be hospitalized when the initial clinicalevaluation suggests an imminent risk for serious arrhythmias(Table 11). For example, patients with primary electrical heartdiseases should be carefully evaluated when presenting withpalpitations.97– 116
Therapeutic purposesThe criteria for the hospitalization of patients with palpitations fortherapeutic purposes are reported in Table 11. Generally, patientswith cardiac arrhythmias and/or structural heart disease will needemergency hospitalization when they complain of palpitationsassociated with haemodynamic compromise, chest pain, orsyncope, as well as if implantation or revision of implanteddevices is indicated.117 – 121
Conflicts of interest: A.R. is a consultant for sanofi-aventis,Boehringer-Ingheleim, Biosense Webster, and St Jude Medical,and has received honoraria from sanofi-aventis, Boehringer Inghe-leim, and Medtronic. L.M. has received honoraria or consulting feesfrom Bard, Biosense Webster, Medtronic, Boston Scientific, St JudeMedical, Sanofi Aventis, Biotronik, and Sorin Group, and hasreceived research grants from Biosense Webster, Medtronic,Boston Scientific, and St Jude Medical. C.B.-L. has received researchgrants from Octopus, AtriCure, and Medtronic. M.J.P.R. is a con-sultant or advisory-board member for Biosense Webster, Boehrin-ger Ingelheim, St Jude Medical, and Stereotaxis. J.M.M. is aconsultant to Medtronic, has received honoraria from BostonScientific and St Jude Medical, and has had research supportfrom all three companies.
References1. Mayou R. Chest pain, palpitations and panic. J Psychosom Res 1998;44:53–70.2. Messineo FC. Ventricular ectopic activity: prevalence and risk. Am J Cardiol 1989;
64:53J–6J.
Table 10 General recommendations for the treatmentof palpitations
Therapy should be directed towards the aetiological cause.
Patients should be reassured in case of a benign cause.
Use of adrenergic substances such as caffeine or alcohol-containingbeverages should be restrained.
Good control of cardiovascular risk factors, specifically ofhypertension, should be ensured.
If there is a recent stressful life-event, psychiatric counselling may be ofhelp.
In patients with symptoms of anxiety and depression, a specific therapyis warranted.
If a specific arrhythmia is found, the appropriate therapy may beantiarrhythmic drugs, ablation, or even an implantable defibrillator.
In the case that arrhythmias are found to be related to systemicdiseases or to the use of pro-arrhythmic drugs, therapy, of course,must aim to remove the underlying conditions.
Table 11 Criteria for the hospitalization of patientswith palpitations
Diagnostic purposes
Severe structural heart disease, suspected or ascertained
Primary electrical heart disease, suspected or ascertained
Family history of sudden death
Need to perform EPS, invasive investigations or in-hospitaltelemetric monitoring
Therapeutic purposes
Bradyarrhythmias requiring implantation of pacemaker
Pacemaker/ICD malfunction not rectifiable by reprogramming
Ventricular tachyarrhythmias requiring immediate interruption and/or ICD implantation or catheter ablation
Supraventricular tachycardias requiring interruption immediately orin a short time, or catheter ablation
Presence of heart failure or other symptoms of haemodynamiccompromise
Severe structural heart diseases requiring surgery or interventionalprocedures
Severe systemic causes
Severe psychotic decompensation
Managing patients with palpitations 931
by guest on August 30, 2015
Dow
nloaded from

3. Kroenke K, Arrington ME, Mangelsdroff AD. The prevalence of symptoms inmedical outpatients and the adequacy of therapy. Arch Intern Med 1990;150:1685–9.
4. Knudson MP. The natural history of palpitations in a family practice. J Fam Pract1987;24:357–60.
5. Zimetbaum P, Josephson ME. Evaluation of patients with palpitations. New Engl JMed 1998;338:1369–73.
6. Giada F, Raviele A. Diagnostic management of patients with palpitations ofunknown origin. Ital Heart J 2004;5:581–6.
7. Brugada P, Gursoy S, Brugada J, Andries E. Investigation of palpitations. Lancet1993;341:1254–8.
8. Pickett CC, Zimetbaum PJ. Palpitations: a proper evaluation and approach toeffective medical therapy. Curr Cardiol Rep 2005;7:362–7.
9. Abbott AV. Diagnostic approach to palpitations. Am Fam Physician 2005;71:743–50.
10. Malliani A, Lombardi F, Pagani M. Sensory innervation of the heart. In: Cervero F,Morrison JFB (eds). Progress in Brain Research. vol. 617. New York: Elsevier; 1986.p39–48.
11. Sugishita K, Shiono E, Sugiyama T, Ashida T. Diabetes influences the cardiacsymptoms related to atrial fibrillation. Circ J 2003;67:835–8.
12. Barsky AJ, Ahern DK, Brener J, Surman OS, Ring C, Dec W. Palpitations andcardiac awareness after heart transplantation. Psychosomatic Med 1998;60:557–62.
13. Kirchhof P, Auricchio A, Bax J, Crijns H, Camm J, Diener HC et al. Outcomeparameters for trials in atrial fibrillation. Europace 2007;9:1006–23.
14. Camm J, Kirchhof P, Lip GYH, Schotten U, Saveliera I, Ernst S et al. Guidelinesfor the management of atrial fibrillation. The task force for the managementof atrial fibrillation of the European Society of Cardiology. Eur Heart J 2010;31:2369–429.
15. Flaker JC, Belew KRN, Beckman K, Vidaillet H, Kron J, Safford R et al. Asympto-matic atrial fibrillation: demographic features and prognostic information fromthe Atrial Fibrillation Follow-up Investigation of Rhythm Management(AFFIRM) study. Am Heart J 2005;149:657–63.
16. Blomstrom-Lundqvist C, Scheinman MM, Aliot EM, Alpert JS, Calkins H,Camm JA et al. ACC/AHA/ESC Guidelines for the management of patientswith supraventricular arrhythmias—executive summary: a report of the Amer-ican College of Cardiology/American Heart Association Task Force on PracticeGuidelines and the European Society of Cardiology Committee for PracticeGuidelines (Writing Committee to Develop Guidelines for the Managementof Patients With Supraventricular Arrhythmias). Circulation 2003;108:1871–909.
17. Zipes DP, Camm AJ, Borggrefe M, Buxton AE, Chaitman B, Fromer M et al.ACC/AHA/ESC 2006 Guidelines for management of patients with ventriculararrhythmias and the prevention of sudden cardiac death: a report of the Amer-ican College of Cardiology/American Heart Association Task Force and theEuropean Society of Cardiology Committee for Practice Guidelines (WritingCommittee to Develop Guidelines for Management of Patients With VentricularArrhythmias and the Prevention of Sudden Cardiac Death): developed in collab-oration with the European Heart Rhythm Association and the Heart RhythmSociety. Circulation 2006;114:385–484.
18. Braunwald E. Valvular heart disease. In Braunwald E (ed.). Heart Disease: A Text-book of Cardiovascular Medicine. 4th ed. Philadelphia: W.B. Sanders; 1992.p1007–65.
19. Deveraux RB, Kramer-Fox R, Kligfield O. Mitral valve prolapse: causes, clinicalmanifestations, and management. Ann Int Med 1989;111:305–17.
20. Chignon JM, Lepine JP, Ades J. Panic disorder in cardiac outpatients. Am J Psychia-try 1993;150:780–5.
21. Barsky AJ, Cleary PD, Coeytaux RR, Ruskin JN. Psychiatric disorders in medicaloutpatients complaining of palpitations. J Gen Intern Med 1994;9:306–13.
22. Barsky AJ, Cleary PD, Sarnie MK. Panic disorder, palpitations and awareness ofcardiac activity. J Nerv Ment Dis 1994;182:63–71.
23. Jeejeebhoy FM, Dorian P, Newman DM. Panic disorder and the heart: a cardiol-ogy perspective. J Psychosom Res 2000;48:393–403.
24. Barsky AJ, Ahern DK, Delameter BA, Clancy SA, Bailey ED. Differential diagnosisof palpitations. Preliminary development of a screening instrument. Arch FamMed 1997;6:241–5.
25. Lampert R, Joska T, Burg MM, Batsford WP, McPherson CA, Jain D. Emotionaland physical precipitants of ventricular arrhythmia. Circulation 2002;106:1800–5.
26. Ziegelstein RC. Acute emotional stress and cardiac arrhythmias. JAMA 2007;298:324–9.
27. Eaker ED, Sullivan LM, Kelly-Hayes M, D’Agostino RB, Benjamin EJ. Anger andhostility predict the development of atrial fibrillation in men in the Framinghamoffspring study. Circulation 2004;109:1267–71.
28. Tavazzi L, Zotti AM, Rondanelli R. The role of psychologic stress in the genesisof lethal arrhythmias in patients with coronary artery disease. Eur Heart J 1986;7(Suppl A):99–106.
29. Domschke K, Kirchhof P, Zwanzger P, Gerlach AL, Breithardt G, Deckert J.Coincidence of paroxysmal supraventricular tachycardia and panic disorders:two case reports. Ann Gen Psych 2010;9:13 (Epub ahead of print).
30. Lessmeier TJ, Gamperling D, Johnson-Liddon V, Fromm BS, Steinman RT,Meissner MD. Unrecognized paroxysmal supraventricular tachycardia. Potentialfor misdiagnosis as panic disorder. Arch Intern Med 1997;157:537–43.
31. Cryer PE, Gerich JE. Glucose counterregulation, hypoglycemia, and intensiveinsulin therapy in diabetes mellitus. N Engl J Med 1985;313:232–41.
32. Klein I. Thyroid hormone and the cardiovascular system. Am J Med 1990;88:631–7.
33. Bravo EL, Giford RW. Pheocromocitoma: diagnosis, localization and manage-ment. N Engl J Med 1984;311:1298–303.
34. Rosenthal DS, Braunwald E. Hematological–oncological disorders and heartdisease. In: Braunwald E (ed.). Heart Disease: A Textbook of Cardiovascular Medi-cine. 4th ed. Philadelphia: W.B. Sanders; 1992. p1742–4.
35. Elkayam U. Pregnancy and cardiovascular disease. In Braunwald E (ed.). HeartDisease: A Textbook of Cardiovascular Medicine. 4th ed. Philadelphia: W.B.Sanders; 1992. p1790–3.
36. Dinardello CA, Wolff SM. Fever. In: Mandell GL, Douglas RG, Bennett JE (eds).Principles and Practices of Infectious Diseases. 3rd ed. New York: Curchill Living-stone; 1990. p464–7.
37. Holman E. Abnormal arteriovenous communications. Great variability of effectswith particular reference to delayed development of cardiac failure. Circulation1966;32:1001–8.
38. Moya A, Sutton R, Ammirati F, Blanc JJ, Brignole M, Dahm JB et al. Guidelines forthe diagnosis and management of syncope. The Task Force for the Diagnosis andManagement of Syncope of the European Society of Cardiology (ESC). Devel-oped in collaboration with European Heart Rhythm Association (EHRA),Heart Failure Association (HFA), and Heart Rhythm Society (HRS). Eur HeartJ 2009;30:2631–71.
39. Thomas JE, Schringer A, Fealey RD, Sheps SG. Orthostatic hypotension. MayoClin Proc 1981;56:117–25.
40. Naranjo Ca, Busto U, Sellers EM. A method for estimating the probabilty ofadverse drug reaction. Clin Pharmacol Ther 1981;30:239–45.
41. Furlanello F, Vitali-Serdoz L, Cappato R, De Ambroggi L. Illicit drugs and cardiacarrhythmias in athletes. Eur J Cardiovasc Prev Rehabil 2007;14:487–94.
42. Lange R, Hillis D. Cardiovascular complications of cocaine use. N Engl J Med2001;345:351–8.
43. Yap YG, Camm AJ. Drug induced QT prolongation and torsades de pointes. Heart2003;89:1363–72.
44. Roden DM. Drug-induced prolongation of the QT interval. N Engl J Med 2004;350:1013–22.
45. Zimetbaum P, Kim KY, Ho KKL, Zebeda J, Josephson ME, Goldberger AL. Utilityof patient-activated cardiac event recorders in general clinical practice. Am JCardiol 1997;79:371–2.
46. Wu CC, Hsieh MH, Tai CT, Chiang CE, Yu WC, Lin YK et al. Utility of patient-activated cardiac event recorders in the detection of cardiac arrhythmias. IntervCard Electrophysiol 2003;8:117–20.
47. Weber BE, Kapoor WH. Evaluations and outcomes of patients with palpitations.Am J Med 1996;100:138–48.
48. Thavendiranathan P, Bagai A, Khoo C, Dorian P, Choudhry NK. Does this patientwith palpitations have a cardiac arrhythmia? JAMA 2009;302:2135–43.
49. Hoefman E, Boer KR, van Weert HCPM, Reitsma JN, Koster RW, Bindels PJE.Predictive value of history taking and physical examination in diagnosing arrhyth-mias in general practice. Fam Pract 2007;24:636–41.
50. Summerton N, Mann S, Rigby A, Petkar S, Dhawan J. New-onset palpitations ingeneral practice: assessing the discriminant value of items within the clinicalhistory. Fam Pract 2001;18:383–92.
51. Mayou R, Sprigings D, Birkhead J, Price J. Characteristics of patients presenting toa cardiac clinic with palpitations. Q J Med 2003;96:115–23.
52. Giada F, Gulizia M, Francese M, Croci F, Santangelo L, Santomauro M et al.Recurrent unexplained palpitations (RUP) study: comparison of implantableloop recorder versus conventional diagnostic strategy. J Am Coll Cardiol 2007;49:1951–6.
53. Fogel RI, Evans JJ, Prystowsky EN. Utility and cost of event recorders in the diag-nosis of palpitations, presyncope and syncope. Am J Cardiol 1997;79:207–8.
54. Krahn AD, Klein GJ, Raymond Y, Norris C. Final results from a pilot study withan implantable loop recorder to determine the etiology of syncope in patientswith negative noninvasive and invasive testing. Am J Cardiol 1998;82:117–9.
55. Pelliccia A, Fagard R, Bjørnstad HH, Anastassakis A, Arbustini E, Assanelli D et al.Recommendations for competitive sports participation in athletes with cardio-vascular disease: a consensus document from the Study Group of Sports Cardi-ology of the Working Group of Cardiac Rehabilitation and Exercise Physiologyand the Working Group of Myocardial and Pericardial Diseases of the EuropeanSociety of Cardiology. Eur Heart J 2005;26:1422–45.
A. Raviele et al.932
by guest on August 30, 2015
Dow
nloaded from
56. Delise P, Guiducci U, Zeppilli P, D’Andrea L, Proto C, Bettini R et al. Cardiolo-gical guidelines for competitive sports eligibility. Ital Heart J 2005;6:661–702.
57. Pelliccia A, Zipes DP, Maron BJ. Bethesda Conference #36 and the EuropeanSociety of Cardiology consensus recommendations revisited: a comparison ofU.S. and European criteria for eligibility and disqualification of competitive ath-letes with cardiovascular abnormalities. J Am Coll Cardiol 2008;52:1990–6.
58. Barsky AJ, Cleary PD, Coeytaux RR, Ruskin JN. The clinical course of palpita-tions in medical outpatients. Arch Intern Med 1995;155:1782–8.
59. Hlatky MA. Approach to the patient with palpitations. In Goldman L,Braunwald E (eds). Primary Cardiology. Philadelphia: W.B. Saunders; 1998.p122–8.
60. Zipes DP, Miles WM, Klein LS. Assessment of patients with cardiac arrhythmia.In Zipes DP, Jalife J (eds). Cardiac Electrophysiology: From Cell to Bedside. Philadel-phia: W.B. Saunders; 1995. p1009–12.
61. Leitch J, Klein G, Yee R. Can patients discriminate between atrial fibrillation andregular supraventricular tachycardia? Am J Cardiol 1991;68:962–6.
62. Leitch JW, Klein GJ, Yee R, Leather RA, Kim YH. Syncope associated with supra-ventricular tachycardia. An expression of tachycardia rate or vasomotorresponse? Circulation 1992;85:1064–71.
63. Brignole M, Gianfranchi L, Menozzi C, Raviele A, Oddone D, Lolli G et al. Role ofautonomic reflexes in syncope associated with paroxysmal atrial fibrillation. J AmColl Cardiol 1993;22:1123–9.
64. Gonzalez-Torrecilla E, Almendral J, Arenal A, Atienza F, Atea LF, del Castillo Set al. Combined evaluation of bedside clinical variables and the electrocardio-gram for the differential diagnosis of paroxysmal atrioventricular reciprocatingtachycardias in patients without pre-excitation. J Am Coll Cardiol 2009;53:2359–61.
65. Gursoy S, Steurer G, Brugada J, Andries E, Brugada P. Brief report: the hemody-namic mechanism of pounding in the neck in atrioventricular nodal reentranttachycardia. N Engl J Med 1992;327:772–4.
66. Brignole M, Vardas P, Hoffman E, Huikuri H, Moya A, Ricci R et al. Indications forthe use of diagnostic implantable and external ECG loop recorders. Europace2009;11:671–87.
67. Botto GL, Padeletti L, Santini M, Capucci A, Gulizia M, Zolezzi F et al. Presenceand duration of atrial fibrillation detected by continuous monitoring: crucialimplications for the risk of thromboembolic events. J Cardiovasc Electrophysiol2009;20:241–8.
68. Brembilla-Perrot B. Pharmacological testing in the diagnosis of arrhythmias.Minerva Cardioangiol 2010;58:505–17.
69. Crawford MH, Bernstein SJ, Deedwania PC, Di Marco JP, Ferrick KJ, Garson AJet al. ACC/AHA Guidelines for ambulatory electrocardiography—executivesummary and recommendations: a report of the American College of Cardiol-ogy/American Heart Association Task Force on Practice Guidelines (Committeeto Revise the Guidelines for Ambulatory Electrocardiography). Circulation 1999;100:886–93.
70. Kadish AH, Buxton AE, Kennedy HL, Knight BP, Mason JW, Schuger JD et al.ACC/AHA clinical competence statement on electrocardiography and ambulat-ory electrocardiography: a report of the ACC/AHA/ACP-ASIM Task Force onClinical Competence (ACC/AHA Committee to Develop a Clinical Compe-tence Statement on Electrocardiography and Ambulatory Electrocardiography),endorsed by the International Society for Holter and Noninvasive Electrocar-diology. J Am Coll Cardiol 2001;38:2091–100.
71. Scherr D, Dalal D, Henrikson CA, Spragg DD, Berger RD, Calkins H et al. Pro-spective comparison of the diagnostic utility of a standard event monitor versusa ‘leadless’ portable ECG monitor in the evaluation of patients with palpitations.J Interv Card Electrophysiol 2008;22:39–44.
72. Kaleschke G, Hoffmann B, Drewitz I, Steinbeck G, Naebauer M, Goette A et al.Prospective, multicentre validation of a simple, patient-operated electrocardio-graphic system for the detection of arrhythmias and electrocardiographicchanges. Europace 2009;11:1362–8.
73. Olson JA, Fouts AM, Padalinam BJ, Prystowsky EN. Utility of mobile outpatienttelemetry for the diagnosis of palpitations, presyncope, syncope, and the assess-ment of therapy efficacy. J Cardiovasc Electrophsiol 2007;18:473–7.
74. Rothman SA, Laughlin JC, Seltzer J, Walia JS, Baman RI, Siouffi SY et al. The diag-nosis of cardiac arrhythmias: a prospective multi-center randomized study com-paring mobile cardiac outpatient telemetry versus standard loop eventmonitoring. J Cardiovasc Electrophysiol 2007;18:248–9.
75. Reiffel JA, Schulhof E, Joseph B. Optimum duration of transtelephonic ECGmonitoring when used for transient symptomatic event detection.J Electrocardiol 1991;24:165–8.
76. Kinlay S, Leitch JW, Neil A. Cardiac event recorders yield more diagnoses andare more cost-effective than 48-hour Holter monitoring in patients with palpita-tions. Ann Intern Med 1996;124:16–20.
77. Scalvini S, Zanelli E, Martinelli G, Baratti D, Giordano A, Glisenti F. Cardiac eventrecording yields more diagnoses than 24-hour Holter monitoring in patientswith palpitations. J Telemed Telecare 2005;11(Suppl 1):14–16.
78. Brown AP, Dawkins KD, Davies JG. Detection of arrhythmias: use of a patient-activated ambulatory electrocardiogram device with a solid-state memory loop.Br Heart J 1987;58:251–3.
79. Antman EM, Ludmer PL, McGowan N, Bosak Fredman PL. Transtelephonic elec-trocardiographic transmission for management of cardiac arrhythmias. Am JCardiol 1988;58:1021–4.
80. Raatikainen MJP, Uusimaa P, van Ginneken MME, Janssen JPG, Linnaluoto M.Remote monitoring of implantable cardioverter defibrillator patients: a safe,time-saving and cost-effective means for follow-up. Europace 2008;10:1145–51.
81. Zimtbaum PJ, Josephson ME. The evolving role of ambulatory arrhythmia moni-toring in general practice. Ann Intern Med 1999;150:848–56.
82. Di Marco JP, Philbrick JT. Use of ambulatory electrocardiographic (Holter) moni-toring. Ann Intern Med 1990;113:53–68.
83. Zimetbaum PJ, Kim KY, Josephson ME, Goldberger AL, Cohen DJ. Diagnosticyield and optimal duration of continuous-loop event monitoring for the diagno-sis of palpitations. Ann Intern Med 1998;28:890–5.
84. Hoefman E, van Weert HCPM, Boer KR, Reitsma J, Koster RW, Bindels PJE.Optimal duration of event recording for diagnosis of arrhythmias in patientswith palpitations and light-headedness in the general practice. Fam Pract 2007;24:11–3.
85. Joshi AK, Kowey PR, Prystowsky EN. First exeprience with a Mobile CardiacOutpatient Telemetry (MCOT) system for the diagnosis and management ofcardiac arrhythmias. Am J Cardiol 2005;95:878–81.
86. Krahn AD, Klein GJ, Yee R, Manda V. The high cost of syncope: cost implicationsof a new insertable loop recorder in the investigation of recurrent syncope. AmHeart J 1999;137:870–7.
87. Krahn AD, Klein GJ, Yee R, Skanes AC. Randomized assessment of syncope trial:conventional diagnostic testing versus a prolonged monitoring strategy. Circula-tion 2001;104:46–56.
88. Waktare JEP, Camm AJ. Holter and event recordings for arrhythmia detection.In: Zareba W, Maison-Blanche P, Locati EH (eds). Noninvasive Electrocardiology inClinical Practice. Armonk, NY: Futura Publishing Company; 2001. p3–30.
89. Paisey JR, Yue AM, Treacher K, Roberts PR, Morgan JM. Implantable loop recor-ders detect tachyarrhythmias in symptomatic patients with negative electro-physiological studies. Int J Cardiol 2005;98:35–8.
90. Epstein AE, Di Marco JP, Ellenbogen KA, Estes MNA III, Freedman RA, Gettes LSet al. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiacrhythm abnormalities: a report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (Writing Committee toRevise the ACC/AHA/NASPE 2002 Guideline Update for Implantation ofCardiac Pacemakers and Antiarrhythmia Devices): developed in collaborationwith the American Association for Thoracic Surgery and Society of ThoracicSurgeons. Circulation 2008;117:e350–e408.
91. Glotzer TV, Daoud EG, Wyse DG, Singer DE, Ezekowitz MD, Hilker C et al. Therelationship between daily atrial tachyarrhythmia burden from implantabledevice diagnostics and stroke risk. The TRENDS Study. Circ Arrhythm Electrophy-siol 2009;2:474–80.
92. Macıas Gallego A, Dıaz-Infante E, Garcıa-Bolao I. Spanish Catheter Ablation Reg-istry. 8th official report of the Spanish Society of Cardiology Working Group onElectrophysiology and Arrhythmias (2008). Rev Esp Cardiol 2009;62:1276–85.
93. Graham I, Atar D, Borch-Jansen K, Boysen G, Burel G, Cifkova R et al. Europeanguidelines on cardiovascular disease prevention in clinical practice: executivesummary. Fourth Joint Task Force of the European Society of Cardiology andother Societies on Cardiovascular Disease Prevention in Clinical Practice (con-stituted by representatives of nine societies and by invited experts). Eur Heart J2007;28:2375–414.
94. Jouven X, Zureik M, Desnos M, Courbon D, Ducimetiere P. Long-term outcomein asymptomatic men with exercise-induced premature ventricular depolariz-ations. N Engl J Med 2000;343:826–33.
95. Binici Z, Intzilakis T, Nielsen OW, Kober L, Sajadich A. Excessive supraventricu-lar ectopic activity and increased risk of atrial fibrillation and stroke. Circulation2010;121:1904–11.
96. Mont L. Arrhythmias and sport practice. Heart 2010;96:398–405.97. Viskin S. The long QT syndromes and torsade de pointes. Lancet 1999;354:
1625–33.98. Kirchhof P, Franz MR, Bardai A, Wilde AM. Giant T-U waves precede torsades de
pointes in long QT syndrome: a systematic electrocardiographic analysis inpatients with acquired and congenital QT prolongation. J Am Coll Cardiol 2009;54:143–9.
99. Keller DI, Huang H, Zhao J, Frank R, Suarez V, Delacretaz E et al. A novelSCN5A mutation, F1344S, identified in a patient with Brugada syndrome andfever-induced ventricular fibrillation. Cardiovasc Res 2006;70:521–9.
Managing patients with palpitations 933
by guest on August 30, 2015
Dow
nloaded from

100. Keller DI, Rougier JS, Kucera JP, Bennamar N, Fressart V, Guicheney P et al.Brugada syndrome and fever: genetic and molecular characterization of patientscarrying SCN5A mutations. Cardiovasc Res 2005;67:510–9.
101. Kum LC, Fung JW, Sanderson JE. Brugada syndrome unmasked by febrile illness.Pacing Clin Electrophysiol 2002;25:1660–1.
102. Morita H, Zipes DP, Morita ST, Wu J. Temperature modulation of ventriculararrhythmogenicity in a canine tissue model of Brugada syndrome. HeartRhythm 2007;4:188–97.
103. Junttila MJ, Gonzalez M, Lizotte E, Benito B, Vernooy K, Sarkozy A et al. InducedBrugada-type electrocardiogram, a sign for imminent malignant arrhythmias. Cir-culation 2008;117:1890–3.
104. Behr ER, Camm AJ. Letter by Behr and Camm regarding article ‘InducedBrugada-type electrocardiogram, a sign for imminent malignant arrhythmias’. Cir-culation 2008;118:e701; author reply e702.
105. Viskin S, Lesh MD, Eldar M, Fish R, Setbon I, Laniado S et al. Mode of onset ofmalignant ventricular arrhythmias in idiopathic ventricular fibrillation. J CardiovascElectrophysiol 1997;8:1115–20.
106. Haissaguerre M, Derval N, Sacher F, Jesel L, Deisenhofer I, de Roy L et al.Sudden cardiac arrest associated with early repolarization. N Engl J Med 2008;358:2016–23.
107. Rosso R, Kogan E, Belhassen B, Rozovki V, Scheinman MM, Zeltser D et al.J-point elevation in survivors of primary ventricular fibrillation and matchedcontrol subjects incidence and clinical significance. J Am Coll Cardiol 2008;52:1231–8.
108. Viskin S. Idiopathic ventricular fibrillation ‘Le Syndrome d’Haissaguerre’ and thefear of J waves. J Am Coll Cardiol 2009;53:620–2.
109. Pasquie JL, Sanders P, Hocini M, Hsu LF, Scavee C, Jais P et al. Fever as a preci-pitant of idiopathic ventricular fibrillation in patients with normal hearts.J Cardiovasc Electrophysiol 2004;15:1271–6.
110. Haissaguerre M, Shah DC, Jais P, Shoda M, Kautzner J, Arentz T et al. Role ofPurkinje conducting system in triggering of idiopathic ventricular fibrillation.Lancet 2002;359:677–8.
111. Haissaguerre M, Shoda M, Jais P, Nogami A, Shah DC, Kautzner J et al.Mapping and ablation of idiopathic ventricular fibrillation. Circulation 2002;106:962–7.
112. Viskin S, Rosso R, Rogowski O, Belhassen B. The ‘short-coupled’ variant of rightventricular outflow ventricular tachycardia: a not-so-benign form of benign ven-tricular tachycardia? J Cardiovasc Electrophysiol 2005;16:912–6.
113. Viskin S, Antzelevitch C. The cardiologists’ worst nightmare: sudden death from‘benign’ ventricular arrhythmias. J Am Coll Cardiol 2005;46:1295–7.
114. Noda T, Shimizu W, Taguchi A, Ajba T, Satomi K, Sujama K et al. Malignant entityof idiopathic ventricular fibrillation and polymorphic ventricular tachycardiainitiated by premature extrasystoles originating from the right ventricularoutflow tract. J Am Coll Cardiol 2005;46:1288–94.
115. Shimizu W. Arrhythmias originating from the right ventricular outflow tract: howto distinguish ‘malignant’ from ‘benign’? Heart Rhythm 2009;6:1507–11.
116. Kirchhof P, Franz MR, Bardai A, Wilde AM. Giant T-U waves precede torsades depointes in long QT syndrome. J Am Coll Cardiol 2009;54:143–9.
117. Colman N, Bakker A, Linzer M, Reitsma JB, Wieling W, Wilde AA. Value ofhistory-taking in syncope patients: in whom to suspect long QT syndrome? Euro-pace 2009;11:937–43.
118. Brignole M, Shen WK. Syncope management from emergency department tohospital. J Am Coll Cardiol 2008;51:284–7.
119. Costantino G, Perego F, Dipaola F, Borella M, Galli A, Cantoni G et al. Short- andlong-term prognosis of syncope, risk factors, and role of hospital admission:results from the STePS (Short-Term Prognosis of Syncope) study. J Am CollCardiol 2008;51:276–83.
120. Brignole M, Alboni P, Benditt DG, Bergfeldt L, Blanc JJ, Bloch-Thomsen PE et al.Guidelines on management (diagnosis and treatment) of syncope: update 2004.Europace 2004;6:467–537.
121. Brignole M, Menozzi C, Bartoletti A, Giada F, Lagi A, Ungar A et al. Anew management of syncope: prospective systematic guideline-based evalu-ation of patients referred urgently to general hospitals. Eur Heart J 2006;27:76–82.
A. Raviele et al.934
by guest on August 30, 2015
Dow
nloaded from