a best practice resource and toolkit - sps the quality of medicines reconciliation: a best practice...
TRANSCRIPT

Winner: Dressings, PrescQIPP Innovation awards 2013; Winner: RPS Pharmaceutical Care Award 2013 Finalist: HSJ Patient safety in primary care award 2013; Winner: UKCPA/Guild Conference Best Poster award 2013
Specialist Pharmacy Service Medicines Use and Safety
Improving the Quality of Medicines Reconciliation
A Best Practice Resource
and Toolkit
Version 1 – June 2015 © Specialist Pharmacy Service

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 2
Medicines Use and Safety
Introduction
The importance and effectiveness of a robust and rigorous Medicines Reconciliation (MR) within all
care settings is vital to ensuring patient safety. Medicines Reconciliation is recognised globally as a
process that supports patient safety. The World Health Organisation (WHO) have identified Medicines
Reconciliation as a priority for action as part of its High 5s Project that was launched in 2006 to address
continuing major concerns about patient safety around the world. Similarly, many national organisations
such as the National Institute for Health and Care Excellence (NICE), National Patient Safety Goals of
the Joint Commission in the USA, the Patient Safety Institute and the Institute for Safe Medication
Practices in Canada have all issued guidance and directives to support the Medicines Reconciliation
agenda. In addition an effective Medicines Reconciliation process significantly supports the delivery of
many of the outcomes associated with the Medicines Optimisation principles as described in the Royal
Pharmaceutical Society Medicines Optimisation Guidance. Medicines Reconciliation is often the first
step or opportunity to understand the patient’s experience of their medicines, this can then lead to
ensuring that patients take their medicines correctly, avoid taking unnecessary medicines, reduce
wastage of medicines, ensure that medicines are prescribed and taken safely and improve outcomes
from medicines use. Despite the high status of Medicines Reconciliation as a patient safety issue and
efforts to implement robust Medicines Reconciliation processes, a consensus statement from key
stakeholders has called for further efforts to identify best practices surrounding Medicines
Reconciliation and their wider dissemination.
Whilst the majority of secondary care NHS providers have Medicines Reconciliation processes in place,
this best practice resource/toolkit will help organisations evaluate the effectiveness of existing
processes, identify and respond to any gaps in service provision and support improvements in current
Medicines Reconciliation processes all with an aim to improve patient safety within the organisation.
The resource is divided into six chapters and aims to:
Allow senior Pharmacists to make a case for resources to support Medicines Reconciliation within
the organisation from a perspective of patient safety and return on investment
Generate discussion between senior Pharmacists and their multidisciplinary colleagues to improve
Medicines Reconciliation processes within the organisation
Allow standardisation and establishment of best practice for Medicines Reconciliation within and
across organisations
Provide tools to audit and evaluate Medicines Reconciliation processes within the organisation
Provide a framework to ensure that staff are fully trained and competent to deliver Medicines
Reconciliation
Provide an introduction to quality improvement methodology in the context of Medicines
Reconciliation
The Medicines Use and Safety team would be grateful if you could provide
feedback on this resource by completing the online feedback survey by clicking
https://www.surveymonkey.com/s/2VHVH6H

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 3
Medicines Use and Safety
Acknowledgements
The development of this best practice resource/toolkit has been supported by a group of talented and
knowledgeable individuals from across the NHS, Academia, Educational Organisations and Health
Research Groups whose expertise, knowledge and contribution has been invaluable. Members of the
working group and their affiliated organisations are detailed below:
Chetan Shah (Project Lead)
Medicines Use and Safety Division, NHS Specialist Pharmacy Service
Chinedu Ahamefula Moorfields Eye Hospital, Moorfields Eye Hospital NHS Foundation Trust
Diane Blunden London Pharmacy Education and Training (LPET)
Fiona Turnbull Northwick Park Hospital, London Northwest Healthcare NHS Trust
Jane Hough Medicines Use and Safety, NHS Specialist Pharmacy Service
Julia Wright Medicines Use and Safety, NHS Specialist Pharmacy Service
Dr Julie Reed Northwest London CLAHRC
Kristi Anderson Northwick Park Hospital, London Northwest Healthcare NHS Trust
Krupa Patel Hounslow CCG
Laura McEwen-Smith Health Education Kent, Surrey & Sussex Pharmacy
Matthew Shaw Centre for Pharmacy Postgraduate Education (CPPE), University of
Manchester
Michelle Sullivan London Chest Hospital, Barts Health NHS Trust
Mildred Johnson Moorfields Eye Hospital, Moorfields Eye Hospital NHS Foundation Trust
Nadine Hall Luton and Dunstable NHS Foundation Trust
Nikki Ayres St George’s Hospital, St George’s University Hospitals NHS Foundation
Trust
Dr Nkiruka Umaru Department of Pharmacy, University of Hertfordshire
Nita Sanghera Kingston Hospital NHS Foundation Trust
Oilin Man Bedford Hospital NHS Trust
Patrick Karikari Newham CCG
Sarah Gray Addenbrooke's Hospital, Cambridge University Hospitals NHS
Foundation Trust
Shirley Kuo Northwest London CLAHRC
Vimal Sriram Northwest London CLAHRC
Wendy Cossey Joint Programmes Board (JPB)

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 4
Medicines Use and Safety
Contents
Introduction Page 2
Acknowledgements Page 3
Chapter 1 Making the Case for Medicines Reconciliation Page 5
Chapter 2 Definition of Medicines Reconciliation and Process Sharing Page 18
Chapter 3 Best Practice Standards Page 36
Chapter 4 Audit and Evaluation Page 59
Chapter 5 Education, Training and Competency Page 76
Chapter 6 Quality Improvement Methodology Page 95 {Authored by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) North West London (NWL)}
Appendices
Appendix 1 Medicines Reconciliation on Admission Audit Data Collection Tool Page 117
Appendix 2 Medicines Reconciliation on Discharge / Discharge Summaries Audit Data Collection
Tool Page 120

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 5
Medicines Use and Safety
Chapter 1 Making the Case for Medicines Reconciliation
The aim of this chapter is to set out an evidence based argument for providing a robust Medicines
Reconciliation service to patients. A crucial element of having a robust and effective Medicines
Reconciliation process/service is to have support within the organisation especially from physicians,
nurses, budget holders and risk managers. In order to gain this support from within the organisation
Medicines Reconciliation should be discussed in the context of (i) being linked to NHS policy and
practice, (ii) being a patient safety issue and lastly as a (iii) return on investment.
1.1 Medicines Reconciliation and NHS Policy and Practice
In 20071 the National Patient Safety Agency (NPSA) and the National Institute for Health and Care
Excellence (NICE) published a patient safety guidance titled “Technical patient safety solutions for
Medicines Reconciliation on admission of adults to hospital”. The guidance recommended that:
All healthcare organisations that admit adult inpatients should make sure that they have policies in
place for Medicines Reconciliation on admission. This includes mental health units, and applies to
elective and emergency admissions.
In addition to specifying standardised systems for collecting and documenting information about
current medications, policies for Medicines Reconciliation on admission should ensure that:
o Pharmacists are involved in Medicines Reconciliation as soon as possible after admission
o The responsibilities of Pharmacists and other staff in the Medicines Reconciliation process
are clearly defined; these responsibilities may differ between clinical areas
o Strategies are incorporated to obtain information about medications for people with
communication difficulties.
Since then organisations have focused Pharmacy resource into delivering Medicines Reconciliation
(MR) within 24 hours of admission. The more recent NICE Guidance - Medicines Optimisation: the safe
and effective use of medicines to enable the best possible outcomes2 which was published in March
2015 states that:
In an acute setting, accurately list all of the person's medicines (including prescribed, over-the-
counter and complementary medicines) and carry out Medicines Reconciliation within 24 hours or
sooner if clinically necessary, when the person moves from one care setting to another – for
example, if they are admitted to hospital
Recognise that Medicines Reconciliation may need to be carried out on more than one occasion
during a hospital stay – for example, when the person is admitted, transferred between wards or
discharged
In primary care, carry out Medicines Reconciliation for all people who have been discharged from
hospital or another care setting. This should happen as soon as is practically possible, before a
prescription or new supply of medicines is issued and within 1 week of the GP practice receiving
the information
In all care settings organisations should ensure that a designated health professional has overall
organisational responsibility for the Medicines Reconciliation process

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 6
Medicines Use and Safety
Organisations should ensure that Medicines Reconciliation is carried out by a trained and
competent health professional – ideally a Pharmacist, Pharmacy technician, nurse or doctor – with
the necessary knowledge, skills and expertise
Involve patients and their family members or carers, where appropriate, in the Medicines
Reconciliation process
When carrying out Medicines Reconciliation, record relevant information on an electronic or paper-
based form.
In addition to the national drivers detailed above Medicines Reconciliation is a key performance
indicator that is measured on the NHS England Medication Safety Thermometer, NHS England
Medicines Optimisation Dashboard and in contract monitoring agreements between Clinical
Commissioning Groups (CCG) and secondary care providers. From a professional perspective
Medicines Reconciliation forms a crucial element of the Royal Pharmaceutical Society (RPS) Hospital
Pharmacy Standards (Standard 2.1) which state that patient’s medicines should be reviewed for an
accurate medication history, for clinical appropriateness and to identify patients of further Pharmacy
support.
1.2 Medicines Reconciliation as a Patient Safety Issue
Medication errors are one of the leading causes of injury to hospital patients, and chart reviews reveal
that over half of all hospital medication errors occur at the interfaces of care3. The prevalence of
medication discrepancies arising at transitions of care have been reported in many different settings
(hospital, community and long-term care facilities) and stages of care (admission, transfer and
discharge). When a patient’s transition from the hospital to home is inadequate, the repercussions can
be far-reaching — hospital readmission, an adverse drug event, and even mortality4, 5.
Several national European studies of adverse events revealed that between 6.3–12.9% of hospitalised
patients have suffered at least one adverse event during their admission and that between 10.8–38.7%
of these adverse events were caused by medications which were preventable6. Similar research
suggests that the average hospitalised patient is subject to at least one medication error per day7, which
confirms previous research findings that medication errors represent one of the most common patient
safety breaches8. Quite pertinently, more than 40 percent of medication errors are believed to result
from inadequate reconciliation in handovers during admission, transfer, and discharge of patients of
which approximately 20 percent are believed to result in patient harm9, 10.
In the UK, the Medicines Use and Safety Division11 conducted a collaborative audit centred on MR
across 56 NHS trusts across East and South East of England covering 33,120 beds. Of the 8621
Medicines Reconciliations audited that includes 49,099 admission drugs (average of 5.7 drugs per MR)
approximately 11,366 unintentional discrepancies (UDs) were identified (mean 1.32 per MR) between
the medications charted at admission and what should have possibly been charted.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 7
Medicines Use and Safety
1.3 Medicines Reconciliation and Return on Investment
Successful implementation of Medicines Reconciliation services requires leadership and adequate
resources to support the process. Therefore a strong business case that demonstrates the patient
safety and financial benefits to the organisation which can justify the resources required is extremely
important. Although there is a significant body of evidence that supports the case for Pharmacist led
MR from a patient safety perspective, it is rather more difficult to quantify the cost benefits derived from
implementing robust Pharmacist led MR. Despite being unable to quantify direct cost savings from
Pharmacist led MR, there is the potential to calculate a monetary figure that might be termed ‘cost
avoidance’. This can be defined as the cost avoided by preventing a preventable ADE which would
result in an increased length of stay or increased use of staff or laboratory or other monitoring resource.
Cost avoidance can be translated into cost effectiveness. Calculations of cost effectiveness
underpinned the review which led to the 2007 Medicines Reconciliation NPSA/NICE Guidance.
In the two figures below, an evidence based attempt is made to demonstrate the return on investment
when pursuing funding for Pharmacy led Medicines Reconciliation support. The examples are focussed
on Pharmacy led MR for unplanned admissions, calculations could be similarly conducted for planned
admissions however, the Pharmacy resource must be adjusted to 5 min per Medicines Reconciliations
as per NICE 2007 guidance.
Fig 1.3.1: Calculating Pharmacist resource and net return on investment for Pharmacy led MR
using detailed published parameters
By using published MR discrepancy/error data it is possible to calculate the number of harmful
medication errors per year that can be avoided by undertaking a Pharmacy led Medicines
Reconciliation. Then by applying a monetary amount (evidence based) to each potential adverse
drug event (ADE) prevented, a gross annual savings amount can be calculated on the premise that
those ADEs are fully avoided by undertaking a Medicines Reconciliation. The costs of a Pharmacy
led MR service can be calculated using the NICE guidance estimations on the time taken to conduct
MR.
By undertaking the above calculations in the context of the admission data for the organisation which
is available from the organisations information team the costs and savings can be calculated in a
bespoke manner for the organisation in a fully evidence based manner and included in any business
cases. By subtracting the costs of the Pharmacy staff from the annual gross savings of preventing
ADEs a net return on investment can be calculated.
The table below sets out the calculations (with evidence based footnotes) that are required to be
followed to achieve the aims sets out above.
Measures Calculations
Average no of MR
discrepancies per patient
1.32

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 8
Medicines Use and Safety
Number of unplanned
admissions per year (X)≠
X
Number of MR medication
errors avoided per year
X(1.32) = Y
Type (categorised by severity
of possible harm) and
frequency of MR
discrepancies¥
Level 1 Errors – 60%
Level 2 Errors – 36%
Serious Errors – 4%
Cost avoided as a result of
medication errors prevented€
Level 1 Errors – £0-6
Level 2 Errors – £65-150
Serious Errors – £713 -£1484
Annual gross savings to
hospital (utilising the absolute
lower end of the above
range)∞
(Y x 0.6 x 0) + (Y x 0.36 x 65) + (Y x 0.04 x 713)
Notes:
0.6 (frequency) and £0 (cost avoided) = Level 1 errors
0.36(frequency) and £65 (cost avoided) = Level 2 errors
0.04(frequency) and £713 (cost avoided) = Level 3 errors
Number of MR that can be
undertaken by a 1.0WTE
member Pharmacy staff per
yearπ
4 x 7 x 5 x 4 x 12 = 6720 MR per year
Cost of Pharmacy staff
resource required
X / 6720 = Z (No of Pharmacy staff required)
Z x AfC salary banding = Pr
Annual Cost Benefit (Y x 0.6 x 0) + (Y x 0.36 x 65) + (Y x 0.04 x 713) – Pr
Notes:
1.32 is based on Dodds L. Results of a Collaborative Audit of Pharmacy-led Medicines Reconciliation (MR) in 56 trusts
across E & SE England. Medicines Use and Safety Division, East and South East Specialist Pharmacy Services 201013. ≠Obtain X from NHS information team (could be for particular care area/ward or entire hospital) ¥Categorisation of errors is based on NRLS rating scale and frequency of error rate is calculated based upon the study
by Dodds L. Which patients benefit most from Medicines Reconciliation? A collaborative evaluation of the outcomes of Pharmacy-led Medicines Reconciliation in various care areas13
€Costs obtained from Campbell F, Karnon J, Czoski-Murray C, Jones R. Systematic review for clinical and cost
effectiveness of interventions in Medicines Reconciliation at the point of admission (2007). The University of Sheffield, School of Health and Related Research12 ∞A very conservative approach has been taken to costs avoided as a result of medication errors prevented, utilising
the absolute lower end of the range πCalculation is based on one Pharmacy staff member taking 15 minutes to undertake a MR for an unplanned admission
(as per NICE guidance1) therefore undertaking 4 MR per hour multiplied by 7 hours in a day multiplied by 5 days per week multiplied by 4 weeks per month multiplied by 12 months per year
When the above calculation pro-forma is applied to an Admissions Unit (In a 400 bedded District
General Hospital) that has an annual unplanned admission rate of 20,807 patients per year the net
return on investment is approximately £1.4million pounds (Pr Value = £116,988 - utilising a Pharmacy
resource of midpoint Band 5 Pharmacy Technician, midpoint Band 6 Pharmacist and midpoint Band
7 Pharmacist).
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 9
Medicines Use and Safety
This could alternatively be expressed as for every £1 spent on Pharmacy staff conducting Medicines
Reconciliation approximately £12 is saved through preventing medication related adverse drug
events.
Despite the evidence based nature of the example set out in in Fig 1.3a there are some limitations to
be mindful of when utilising the example in business cases:
The error type and frequency values utilised in the calculation which are obtained from the study
conducted by Dodds13 relied on individual practitioner self-assessment rather than peer-review of
potential clinical impact which may have introduced bias
There is an assumption that all the identified discrepancies are resolved appropriately and promptly
and so the anticipated preventable ADE is averted
In practice Pharmacy staff do not exclusively undertake MR duties, they are involved in many other
activities that contribute to patient care
The calculations do not factor in cost pressures such as sick leave, annual leave, study leave,
absence etc.
Fig 1.3.2: Model based cost-effectiveness analysis of preventing medication error at hospital
admission through Pharmacist led MR
Some research evidence indicates that medication errors or discrepancies are an imperfect surrogate
for preventable ADEs because they are very common and only a small fraction actually cause harm.
A model developed by Karnon14 et al that proposed a baseline preventable ADE rate of 2.8 (1.5-4.5)
per 1000 prescription orders at a total cost of £4092 (£2072-£6758).
If there is an assumption that on average patients are prescribed 5 drugsӻ this translates into an
average of 0.014 preventable ADE per MR at a cost avoidance of approximately £20/MR.
However, not all of these medication errors will be identified by, or even related to, the MR process,
therefore Karnon14 et al extrapolated from research evidence that Pharmacists reduce the error rate
by 75% and pharmacy technicians/systematic methods of recording drug histories by 50%.
As most pharmacy teams use a mix of pharmacists and pharmacy technicians to undertake MR, then
it would be pragmatic to conclude that Pharmacy led MR reduces the preventable ADE rate at
admission to 0.007 per patient. The cost avoidance is thus £10/MR. Against this must be offset the
cost of the Pharmacy MR itself (15 min of B6 time plus on cost =£5), resulting in a cost avoidance
per Pharmacy led MR of £5 per patient.
In some health economies a proxy cost avoidance of £5/ Pharmacy led MR has been agreed to help
quantify the savings associated with Pharmacy led MR. This can then be applied to admission data
for the organisation. For example if the above calculation is applied to an Admissions Unit (In a 400
bedded District General Hospital) that has an annual unplanned admission rate of 20,807 patients
per year the net return on investment is approximately £104,035.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 10
Medicines Use and Safety
ӻover 75% of patients with discrepancies with the potential for moderate clinical impact in the September 2010 collaborative
service audit were on 5 or more medicines11
Other additional potential benefits of Medicines Reconciliation within a business case that should also
be articulated are the following:
Decrease in readmissions or visits to emergency departments
Decrease in legal costs associated with ADEs
Increased efficiencies due to streamlined processes
Increased patient engagement and patient satisfaction
Increased staff satisfaction
Reduced re-dispensing and thus saving on drug costs and Pharmacy resource
Litigation avoidance
There is significant evidence that demonstrates that implementing effective Medicines Reconciliation
processes are a powerful intervention to reduce medication errors. Some published MR interventions
that have delivered positive outcomes are briefly described:
A series of Medicines Reconciliation interventions, introduced over a seven-month period,
successfully decreased the rate of medication errors by 70% and reduced adverse drug events by
over 15%15.
In another study16, the utilisation of Pharmacy technicians to initiate the reconciliation process by
obtaining medication histories for the scheduled surgical population reduced potential adverse drug
events by 80% within three months of implementation.
A revised Medicines Reconciliation process reduced work and re-works associated with the
management of medication orders. After implementation, nursing time at admission was reduced
by over 20 minutes per patient. The amount of time that Pharmacists were involved in discharge
was reduced by over 40 minutes17.
The implementation of a comprehensive Medicines Reconciliation program to reduce errors in
admission and discharge medication orders at an academic medical centre reduced medication
errors from 90% to 47% in surgical patients18.
A study19 that observed that the introduction of Pharmacy services, which included Medication
Reconciliation, into a hospital’s kidney transplant team created a statistically significant decrease
in the mean length of stay among transplant recipients (from 7.8 days to 3.4 days). The cost savings
attributed to this decrease was estimated at $279,180 USD per year.
A further study14 conducted a cost-effectiveness analysis of interventions aimed at preventing
medication errors at hospital admission. The aim of the study was to assess the incremental costs
and effects (measured as quality adjusted life years) of a range of Medicines Reconciliation
interventions. Findings demonstrated that all five interventions, for which evidence of effectiveness
was identified, were estimated to be extremely cost effective when compared to the baseline
scenario. In this paper, the Pharmacist-led reconciliation intervention had the highest expected net

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 11
Medicines Use and Safety
benefits and a probability of being cost-effective of over 60% by a quality-adjusted life year value
of £10,000.
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 12
Medicines Use and Safety
S
P S
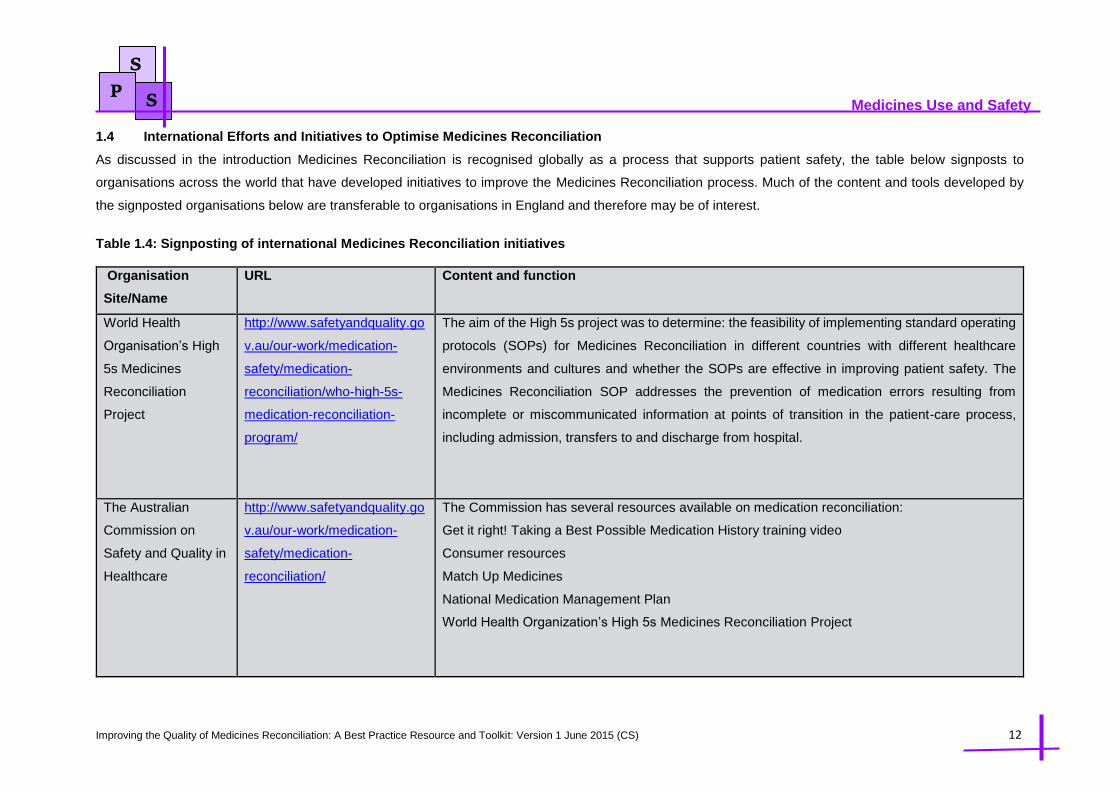
1.4 International Efforts and Initiatives to Optimise Medicines Reconciliation
As discussed in the introduction Medicines Reconciliation is recognised globally as a process that supports patient safety, the table below signposts to
organisations across the world that have developed initiatives to improve the Medicines Reconciliation process. Much of the content and tools developed by
the signposted organisations below are transferable to organisations in England and therefore may be of interest.
Table 1.4: Signposting of international Medicines Reconciliation initiatives
Organisation
Site/Name
URL Content and function
World Health
Organisation’s High
5s Medicines
Reconciliation
Project
http://www.safetyandquality.go
v.au/our-work/medication-
safety/medication-
reconciliation/who-high-5s-
medication-reconciliation-
program/
The aim of the High 5s project was to determine: the feasibility of implementing standard operating
protocols (SOPs) for Medicines Reconciliation in different countries with different healthcare
environments and cultures and whether the SOPs are effective in improving patient safety. The
Medicines Reconciliation SOP addresses the prevention of medication errors resulting from
incomplete or miscommunicated information at points of transition in the patient-care process,
including admission, transfers to and discharge from hospital.
The Australian
Commission on
Safety and Quality in
Healthcare
http://www.safetyandquality.go
v.au/our-work/medication-
safety/medication-
reconciliation/
The Commission has several resources available on medication reconciliation:
Get it right! Taking a Best Possible Medication History training video
Consumer resources
Match Up Medicines
National Medication Management Plan
World Health Organization’s High 5s Medicines Reconciliation Project
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 13
Medicines Use and Safety
S
P S
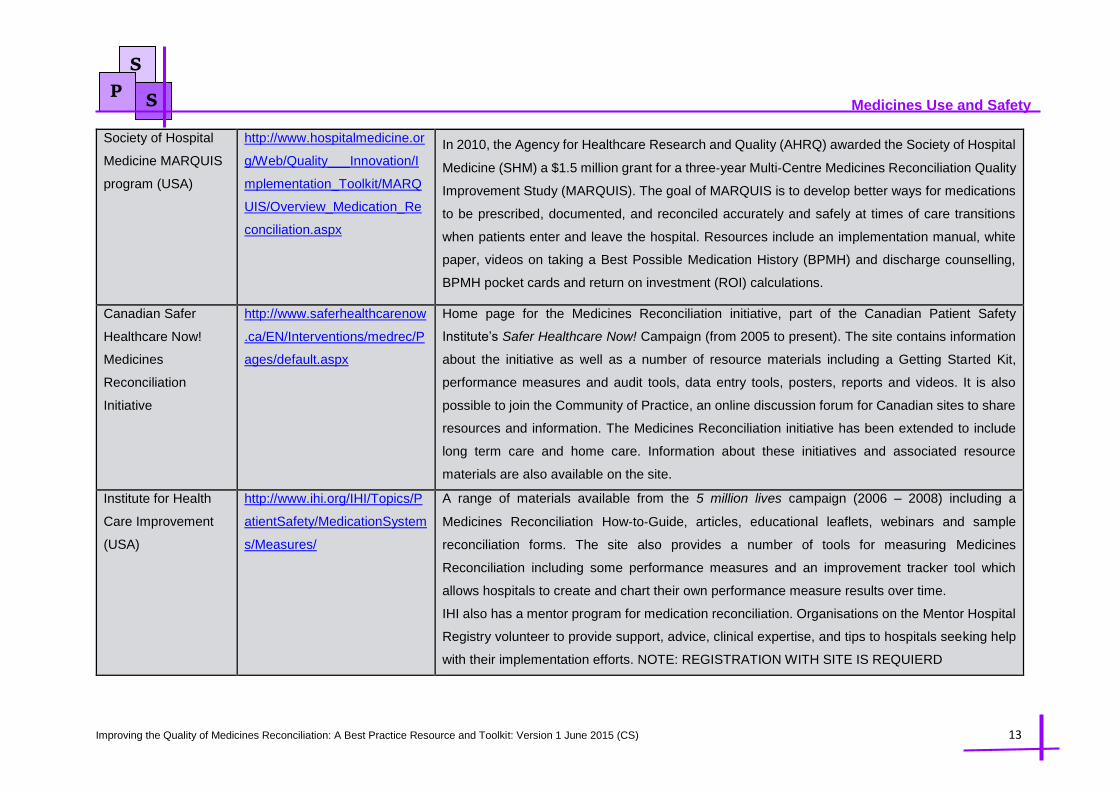
Society of Hospital
Medicine MARQUIS
program (USA)
http://www.hospitalmedicine.or
g/Web/Quality___Innovation/I
mplementation_Toolkit/MARQ
UIS/Overview_Medication_Re
conciliation.aspx
In 2010, the Agency for Healthcare Research and Quality (AHRQ) awarded the Society of Hospital
Medicine (SHM) a $1.5 million grant for a three‐year Multi‐Centre Medicines Reconciliation Quality
Improvement Study (MARQUIS). The goal of MARQUIS is to develop better ways for medications
to be prescribed, documented, and reconciled accurately and safely at times of care transitions
when patients enter and leave the hospital. Resources include an implementation manual, white
paper, videos on taking a Best Possible Medication History (BPMH) and discharge counselling,
BPMH pocket cards and return on investment (ROI) calculations.
Canadian Safer
Healthcare Now!
Medicines
Reconciliation
Initiative
http://www.saferhealthcarenow
.ca/EN/Interventions/medrec/P
ages/default.aspx
Home page for the Medicines Reconciliation initiative, part of the Canadian Patient Safety
Institute’s Safer Healthcare Now! Campaign (from 2005 to present). The site contains information
about the initiative as well as a number of resource materials including a Getting Started Kit,
performance measures and audit tools, data entry tools, posters, reports and videos. It is also
possible to join the Community of Practice, an online discussion forum for Canadian sites to share
resources and information. The Medicines Reconciliation initiative has been extended to include
long term care and home care. Information about these initiatives and associated resource
materials are also available on the site.
Institute for Health
Care Improvement
(USA)
http://www.ihi.org/IHI/Topics/P
atientSafety/MedicationSystem
s/Measures/
A range of materials available from the 5 million lives campaign (2006 – 2008) including a
Medicines Reconciliation How‐to‐Guide, articles, educational leaflets, webinars and sample
reconciliation forms. The site also provides a number of tools for measuring Medicines
Reconciliation including some performance measures and an improvement tracker tool which
allows hospitals to create and chart their own performance measure results over time.
IHI also has a mentor program for medication reconciliation. Organisations on the Mentor Hospital
Registry volunteer to provide support, advice, clinical expertise, and tips to hospitals seeking help
with their implementation efforts. NOTE: REGISTRATION WITH SITE IS REQUIERD
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 14
Medicines Use and Safety
S
P S
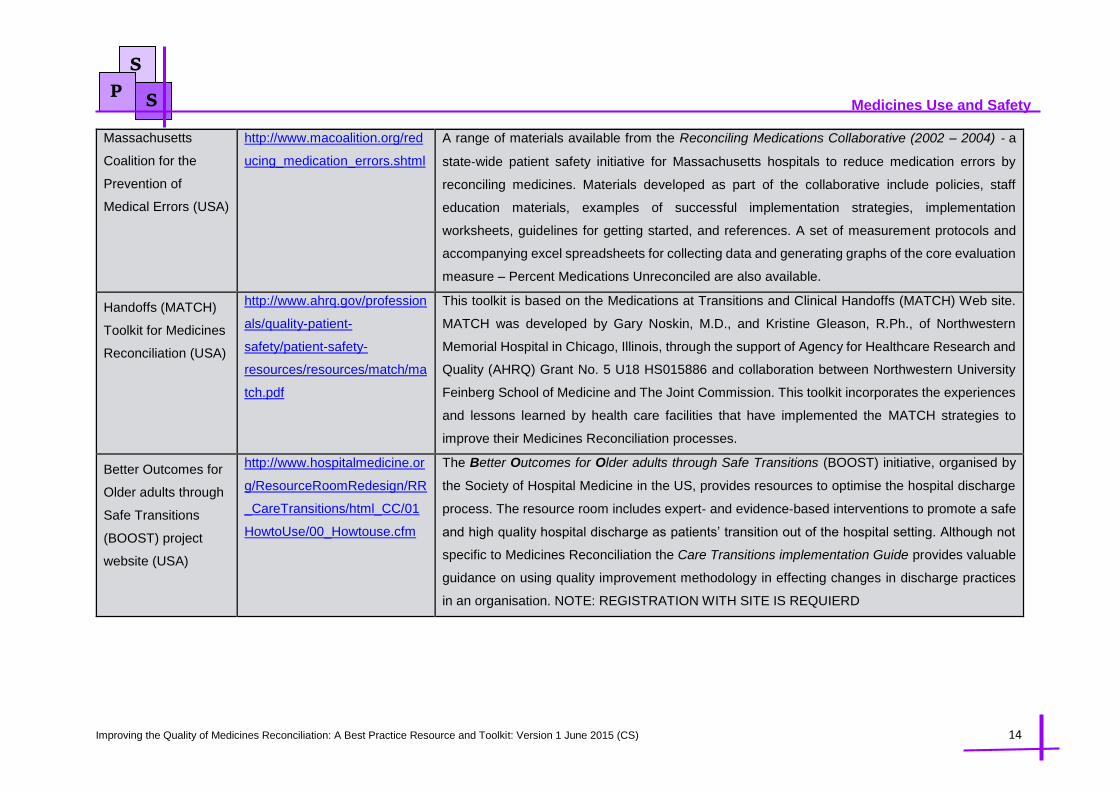
Massachusetts
Coalition for the
Prevention of
Medical Errors (USA)
http://www.macoalition.org/red
ucing_medication_errors.shtml
A range of materials available from the Reconciling Medications Collaborative (2002 – 2004) ‐ a
state‐wide patient safety initiative for Massachusetts hospitals to reduce medication errors by
reconciling medicines. Materials developed as part of the collaborative include policies, staff
education materials, examples of successful implementation strategies, implementation
worksheets, guidelines for getting started, and references. A set of measurement protocols and
accompanying excel spreadsheets for collecting data and generating graphs of the core evaluation
measure – Percent Medications Unreconciled are also available.
Handoffs (MATCH)
Toolkit for Medicines
Reconciliation (USA)
http://www.ahrq.gov/profession
als/quality-patient-
safety/patient-safety-
resources/resources/match/ma
tch.pdf
This toolkit is based on the Medications at Transitions and Clinical Handoffs (MATCH) Web site.
MATCH was developed by Gary Noskin, M.D., and Kristine Gleason, R.Ph., of Northwestern
Memorial Hospital in Chicago, Illinois, through the support of Agency for Healthcare Research and
Quality (AHRQ) Grant No. 5 U18 HS015886 and collaboration between Northwestern University
Feinberg School of Medicine and The Joint Commission. This toolkit incorporates the experiences
and lessons learned by health care facilities that have implemented the MATCH strategies to
improve their Medicines Reconciliation processes.
Better Outcomes for
Older adults through
Safe Transitions
(BOOST) project
website (USA)
http://www.hospitalmedicine.or
g/ResourceRoomRedesign/RR
_CareTransitions/html_CC/01
HowtoUse/00_Howtouse.cfm
The Better Outcomes for Older adults through Safe Transitions (BOOST) initiative, organised by
the Society of Hospital Medicine in the US, provides resources to optimise the hospital discharge
process. The resource room includes expert‐ and evidence‐based interventions to promote a safe
and high quality hospital discharge as patients’ transition out of the hospital setting. Although not
specific to Medicines Reconciliation the Care Transitions implementation Guide provides valuable
guidance on using quality improvement methodology in effecting changes in discharge practices
in an organisation. NOTE: REGISTRATION WITH SITE IS REQUIERD

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 15
Medicines Use and Safety
S
P S
National Institute for
Health and Clinical
Excellence (NICE)
website (UK)
http://www.nice.org.uk/guidanc
e/index.jsp?action=byID&o=11
897
Provides details on the NICE patient safety guidance 1: Technical patient safety solutions for
Medicines Reconciliation on admission of adults to hospital a policy which required all public
hospitals in the UK and Wales to put in place formal systems for admission reconciliation by
December 2008. As well as the guidance document the site provides an audit tool, PowerPoint®
presentation, costing tools and other useful information

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 16
Medicines Use and Safety
References:
1. National Institute for Health and Clinical Excellence (NICE) and the National Patient Safety Agency
(NPSA). Technical patient safety solutions for Medicines Reconciliation on admission of adults to
hospital. December 2007, available at:
http://www.nice.org.uk/resource/uhzwua3ax6lkvnygh5mzybqg5m (Accessed 23rd September 2014)
2. National Institute for Health and Clinical Excellence (NICE). Medicines optimisation: the safe and
effective use of medicines to enable the best possible outcomes. March 2015, available at:
https://www.nice.org.uk/guidance/ng5 (Accessed 28th March 2015)
3. Rozich JD, Resar RK. Medication safety: One organization‘s approach to the challenge. JCOM.
2001;8(10):27-34.
4. Kripalani S, LeFevre F, Phillips CO, et al. Deficits in communication and information transfer
between hospital-based and primary care physicians: implications for patient safety and continuity of
care. JAMA 2007; 297:831–41.
5. Philbert I, Barach P. The European HANDOVER Project: a multi-nation program to improve
transitions at the primary care—inpatient interface BMJ Qual Saf 2012;21:i1–i6. doi:10.1136/bmjqs-
2012-001598.
6. Council of Europe. Creation of a better medication safety culture in Europe: Building up safe
medication practices. Expert Group on Safe Medication Practices (P-SP-PH/SAFE),2006.
7. Institute of Medicine. Preventing medication errors. Washington, DC: National Academies Press;
2006.
8. Bates DW, Spell N, Cullen DJ, et al. The costs of adverse drug events in hospitalized patients.
JAMA1997; 277:307-11.
9. Rozich JD, Howard RJ, Justeson JM, et al. Patient safety standardization as a mechanism to
improve safety in health care. J Qual Saf 2004; 30(1):5-14.
10. Gleason KM, Groszek JM, Sullivan C, et al. Reconciliation of discrepancies in medication histories
and admission orders of newly hospitalized patients. Am J Health Syst Pharm 2004; 61:1689-95
11. Dodds L. Results of a Collaborative Audit of Pharmacy-led Medicines Reconciliation (MR) in 56
trusts across E & SE England. Medicines Use and Safety Division, East and South East Specialist
Pharmacy Services 2010. Available at http://www.acutemedicine.org.uk/wp-
content/uploads/2014/04/Report_Collaborative_MR_Audit_Results_May_2010.pdf. (Accessed 23rd
September 2014)
12. Campbell F, Karnon J, Czoski-Murray C, Jones R. Systematic review for clinical and cost
effectiveness of interventions in Medicines Reconciliation at the point of admission (2007). The
University of Sheffield, School of Health and Related Research. Available at
https://www.nice.org.uk/guidance/psg001/documents/systematic-review-for-clinical-and-cost-
effectiveness-of-interventions-in-medicines-reconciliation-at-the-point-of-admission2 (Accessed 14th
April 2015)
13. Dodds L. Which patients benefit most from Medicines Reconciliation? A collaborative evaluation
of the outcomes of Pharmacy-led Medicines Reconciliation in various care areas. Available at
http://www.medicinesresources.nhs.uk/en/Communities/NHS/SPS-E-and-SE-England/Meds-use-and-

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 17
Medicines Use and Safety
safety/Service-deliv-and-devel/Meds-reconciliation/Which-patients-benefit-most-from-medicines-
reconciliation/?query=reconciliation&rank=81 (Accessed 14th April 2015)
14. Karnon J, Campbell F, Czoski-Murray C. Model-based cost-effectiveness analysis of interventions
aimed at preventing medication error at hospital admission (medicines reconciliation). J Eval Clin Prac
2009; 15: 299-306.
15. Whittington J, Cohen H. OSF Healthcare‘s journey in patient safety. Quality Management in Health
Care. 2004;13(1):53-59.
16. Michels RD, Meisel S. Program using Pharmacy technicians to obtain medication histories. Am J
Health-Sys Pharm. October 1, 2003;60:1982-1986.
17. Rozich JD, Resar RK, et al. Standardization as a mechanism to improve safety in health care:
Impact of sliding scale insulin protocol and reconciliation of medications initiatives. Joint Commission
Journal on Quality and Safety. 2004;30(1):5-14.
18. Murphy EM, Oxencis CJ, Klauck JA et al. Medicines Reconciliation at an academic medical
centre: Implementation of a comprehensive program from admission to discharge. American Journal
of Health-System Pharmacy. 2009;66(23):2126-2131.
19. Maldonado AQ, Weeks DL, Bitterman AN et al. Changing transplant recipient education and
inpatient transplant Pharmacy practices: A single-center perspective. Am J Health Syst Pharm. 2013
May 15; 70 (10): 900-4.
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 18
Medicines Use and Safety
Chapter 2 Definition of Medicines Reconciliation and Process
Sharing
This chapter aims to share the different approaches that organisations have taken to implement
Medicines Reconciliation. The chapter also attempts to define and standardise the concepts and
definitions that underpin effective Medicines Reconciliation.
2.1 Medicines Reconciliation Definition and Guiding Principles
There are several definitions of Medicines Reconciliation within the literature. Although the underlying
principles within the different definitions tend to remain the same the varying definitions can cause some
difficulties in the implementation, resource allocation and measurement of MR. Therefore clarifying the
definition and the processes underpinning MR is critical to ensuring uniform approaches and
measurements to MR are embedded within and across organisations.
The Institute for Healthcare Improvement1 define Medicines Reconciliation as the process of creating
the most accurate list possible of all medications a patient is taking — including drug name, dosage,
frequency, and route — and comparing that list against the physician’s admission, transfer, and/or
discharge orders, with the goal of providing correct medications to the patient at all transition points
within the hospital.
A working definition developed by NHS England Medication Safety team that supports implementation
of MR at a practical level in secondary care is described below (for the purposes of this best practice
resource/toolkit the NHS England definition of MR will be used)
“The collection and accurate identification of a patient’s current list of medicines prior to hospital
admission PLUS the identification AND recording of any discrepancies compared with the list of
medicines prescribed since the hospital admission. Resolution of any discrepancies identified should
occur as soon as possible using clinical judgement to ensure safe and effective patient care”
The World Health Organisation2 have developed several guiding principles that apply to Medicines
Reconciliation implementation which are shown in table 2.1.
Table 2.1: The World Health Organisation Guiding Principles on Medicines Reconciliation
Guiding Principle 1: An up-to-date and accurate patient medication list is essential to ensure
safe prescribing in any setting
The development, maintenance and communication of a complete and accurate medication list
throughout the continuum of care - whenever and wherever medications are used - is essential for
reducing adverse medication events.
Guiding Principle 2: A formal structured process for reconciling medications operates at all
interfaces of care
Having a structured process for reconciling medications at all points of transfer decreases the risk of
communication errors and adverse medication outcomes.
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 19
Medicines Use and Safety
Guiding Principle 3: Medicines Reconciliation on admission is the foundation for
reconciliation throughout the episode of care
The key to the success of Medicines Reconciliation at all interfaces is to first have a process working
effectively at admission to the health care facility. Appropriate admission Medicines Reconciliation is
the foundation to support and facilitate efficient and appropriate reconciliation at internal transfers
and discharge. It should occur early in admission, preferably within 24 hours of admission.
Guiding Principle 4: The process of Medicines Reconciliation is one of shared accountability
with staff aware of their roles and responsibilities
For Medicines Reconciliation to be effective staff need to be aware of their roles and responsibilities
in the process so that patients have their medicines reconciled and discrepancies resolved early
within their admission.
Guiding Principle 5: Medicines Reconciliation is integrated into existing processes for
medication management and patient flow
Effective and efficient implementation of a Medicines Reconciliation process requires integration of
its steps into existing hospital systems.
Guiding Principle 6: Patients and families are involved in the Medicines Reconciliation
Medicines Reconciliation is most effective when patients and families are engaged in the process.
Guiding Principle 7: Staff responsible for reconciling medications are trained to take a best
possible medication history (BPMH) and reconcile
Staff responsible for obtaining and recording the BPMH and reconcile medications should have the
knowledge, skills and attitudes necessary to safely perform the tasks.
2.2 Process of Undertaking Medicines Reconciliation
The National Prescribing Centre (NPC) Guidance Medicines Reconciliation published in 2007 is the key
national document that supported the implementation of MR following the NICE guidance issued in
2007. In addition The East and South East Specialist Pharmacy Service template policy for Medicines
Reconciliation published in 2009 was also a key tool that NHS organisations especially in the East and
South East of England used to implement MR processes. However, these two key documents used
slightly different terminologies in describing the processes through which MR should be undertaken.
For example the NPC document used descriptors such as Stage 1, Stage 2, Basic and Full
reconciliation whereas the East and South East Specialist Pharmacy Service template policy used
descriptors such as Level 1, Level 2, Admission Led and Pharmacy consolidation.
Through consultation with the members of the working group that supported the development of this
best practice resource/toolkit a consensus agreement was reached that indicated that the terms Stage
1, Basic, Level 1, and Admission Led are relatively synonymous with each other as are Full, Stage 2,
Level 2 and Pharmacy consolidation.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 20
Medicines Use and Safety
Stage 1 = Basic = Level 1 = Admission Led
Medicines Reconciliation
Essentially can be described as obtaining a
medication list “Drug History” on admission
at the clerking in stage by the admitting
clinician which is then documented onto the
drug chart.
In the majority of scenarios the admitting
clinician undertaking this “drug history” will
be the admitting Dr or Nurse who has triaged
the patient.
Stage 2 = Full = Level 2 = Pharmacy
Consolidation
Essentially includes Pharmacy staff
involvement (Pharmacists and/or Pharmacy
Technicians) by where the Pharmacy staffs
verify the most accurate medication list for
that patient using two or more sources.
It also involves identifying any discrepancies
(intentional or unintentional) between the
Pharmacy verified list and the medication list
charted by the admitting clinician onto the
drug chart and then resolving the identified
discrepancies accordingly.
Stage 2/Level 2 MR should be conducted by
suitably trained Pharmacists or Pharmacy
Technicians (for example of training
programmes and competency assurance
please see chapter 5)
It is important to recognise that Stage 2/Level
2 MR does not encompass pharmaceutical
review “clinical screen” “medication review”
of the prescription. This must be conducted
by the Pharmacist and is outside the scope
of this best practice resource/toolkit.
This best practice resource/toolkit although generally aimed at Pharmacy staff conducting Medicines
Reconciliation can be used and adapted for use with other healthcare professionals involved in the MR
process. For example in order to improve the quality of stage1/level1 MR clinicians involved in admitting
patients should be a targeted for training and competency assessment as a priority as it would improve
efficiency, patient safety and reduce the risk of ADE.
The detailed process involved in conducting a MR is well described in the literature with individual
organisations usually having their own local policies and processes. The underlying principles of

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 21
Medicines Use and Safety
conducting effective MR are articulated in the National Prescribing Centre (NPC) guidance Medicines
Reconciliation: A guide to implementation published in 2007 and is displayed below:
The Medicines Reconciliation process in detail:
A useful way of remembering the steps in the reconciliation process is to adopt the 3Cs approach.
Collecting
Checking
Communicating
Collecting:
The collecting step involves taking a medication history and collecting other relevant information
about the patient’s medicines. The information may come from a range of different sources (some
potentially more reliable than others).
Checking:
The checking step involves ensuring that the medicines and doses that are now prescribed for the
patient are correct. Obviously, this does not mean that they will be identical to those documented
during the basic reconciliation process. For example, a doctor now responsible for the patient may
make some intentional changes to their medicines but any discrepancies will need to be resolved in
the final step of the process.
Communicating:
Communicating is the final step in the process, where any changes that have been made to the
patient’s prescription are documented and dated, ready to be communicated to the next person
responsible for the medicines management care of that patient.
Below is a flow chart published by the National Prescribing Centre that details the steps involved in the
MR process (The original flow chart in better resolution can be viewed via
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/NPC%2
0Process%20of%20Meds%20Rec_May%2015.pdf). The flow chart is a useful tool that can be used
and adapted by Pharmacy teams who may wish to conduct a process mapping exercise of the MR to
identify any risks or quality improvement initiatives or/and to engage wider multidisciplinary and
management teams.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 22
Medicines Use and Safety
Fig 2.2.1: A flow chart of the Medicines Reconciliation process of patient admission from
primary care to secondary care

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 23
Medicines Use and Safety
Fig 2.2.2: A flow chart of the Medicines Reconciliation process of patient discharge from
secondary care to primary care

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 24
Medicines Use and Safety
S
P S
2.3 Sharing of Medicines Reconciliation Processes, Practices and Documents
Several NHS organisations have kindly shared their Medicines Reconciliation Processes, Practices and Documents so that organisations can look at different
examples and think about what could be incorporated into their own policies and practices to optimise the MR process. The table below provide examples of
drug chart documentation and methods of MR documentation & policy examples.
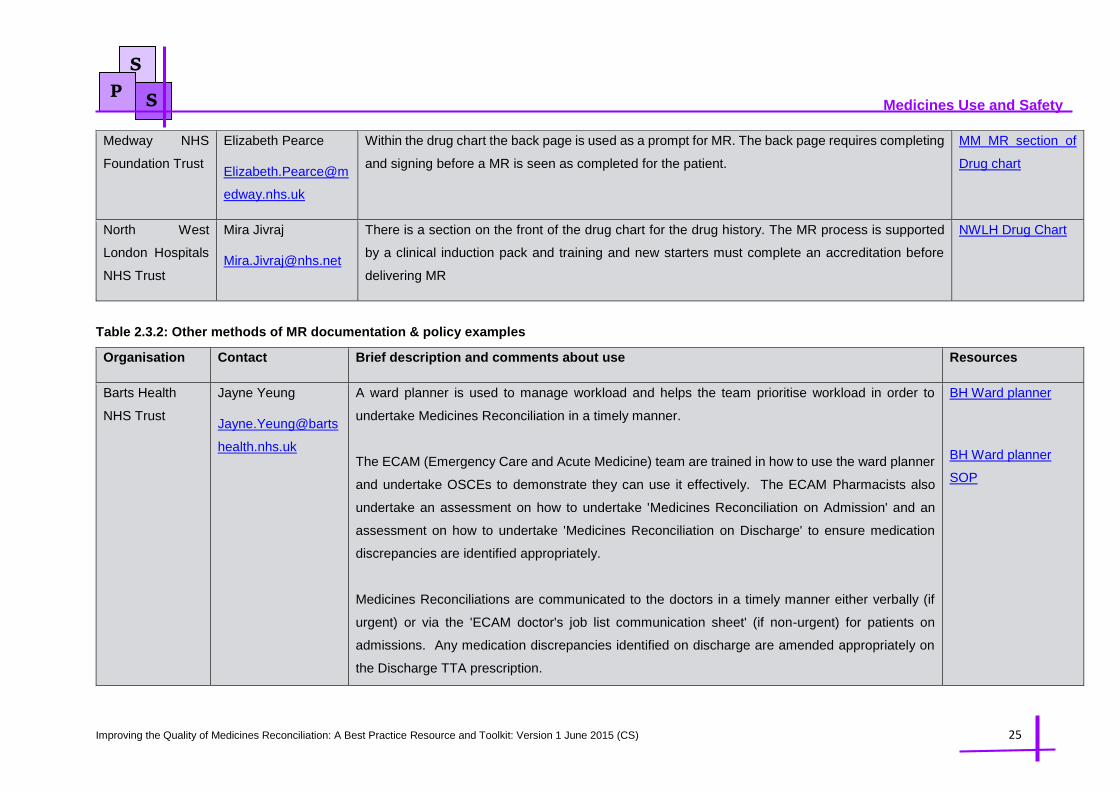
Table 2.3.1: Examples of drug chart documentation of Medicines Reconciliation
Organisation Contact Brief description & comments from contributor about use Resources
Hinchingbrooke
Health Care NHS
Trust
Rachel Waldon
Drug history documentation goes on the front page of the drug chart.
All MR record keeping is on the drug chart. Each drug on the internal sections is marked in the
Pharmacy box (Hx) with dose details and cross referenced to the list on the front for discrepancies
Advantages: Remains with patient / subsequently filed in notes / can easily be transcribed to
subsequent charts when rewritten / easy to transcribe changes onto GP discharge letter
Disadvantages: May be reviewed by a Dr when written by a technician & not validated by a
Pharmacist. This could mean that discrepancies noted are not correct.
Discrepancy Resolution: Policy states how this should be managed. The advantage is it is easy to
track management of unintentional discrepancies; the disadvantage is that it relies on staff
experience to assess the severity of the problem
HH First page drug
chart
HH SOP for MR
(Extract)
Imperial College
Healthcare NHS
Trust
Gavin Miller
Gavin.miller@imperi
al.nhs.uk
The advantage of a specific MR section on the drug chart is that the information is readily available
when the chart is screened at discharge. A disadvantage is that every time the drug chart needs
rewriting, the information needs to be transferred (every 2 weeks)
IH MR section of
drug chart
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 25
Medicines Use and Safety
S
P S
Medway NHS
Foundation Trust
Elizabeth Pearce
Elizabeth.Pearce@m
edway.nhs.uk
Within the drug chart the back page is used as a prompt for MR. The back page requires completing
and signing before a MR is seen as completed for the patient.
MM MR section of
Drug chart
North West
London Hospitals
NHS Trust
Mira Jivraj
There is a section on the front of the drug chart for the drug history. The MR process is supported
by a clinical induction pack and training and new starters must complete an accreditation before
delivering MR
NWLH Drug Chart
Table 2.3.2: Other methods of MR documentation & policy examples
Organisation Contact Brief description and comments about use Resources
Barts Health
NHS Trust
Jayne Yeung
Jayne.Yeung@barts
health.nhs.uk
A ward planner is used to manage workload and helps the team prioritise workload in order to
undertake Medicines Reconciliation in a timely manner.
The ECAM (Emergency Care and Acute Medicine) team are trained in how to use the ward planner
and undertake OSCEs to demonstrate they can use it effectively. The ECAM Pharmacists also
undertake an assessment on how to undertake 'Medicines Reconciliation on Admission' and an
assessment on how to undertake 'Medicines Reconciliation on Discharge' to ensure medication
discrepancies are identified appropriately.
Medicines Reconciliations are communicated to the doctors in a timely manner either verbally (if
urgent) or via the 'ECAM doctor's job list communication sheet' (if non-urgent) for patients on
admissions. Any medication discrepancies identified on discharge are amended appropriately on
the Discharge TTA prescription.
BH Ward planner
BH Ward planner
SOP

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 26
Medicines Use and Safety
S
P S
Chesterfield
Royal Hospital
NHS Foundation
Trust
(Electronic
System)
Andrew hardy
All emergency admissions have their medical clerking written on to a pro-forma. There is a page for
documenting medicines on admission (attached) within the pro-forma. When Pharmacy staffs
undertake Medicines Reconciliation they may find unintentional discrepancies. If these can be
resolved by a prescribing Pharmacist the amendments are made immediately onto the medicines
page of the clerking pro-forma (rather than making an entry into the later chronological paperwork).
This new information is on the right hand side and signed for so it is clear who has added the
information and when. If the Pharmacist is unable to resolve the discrepancy immediately or in face
to face discussion then an entry is made in the chronological notes so it will be seen and acted upon.
The advantage of using the pro-forma is that it is quicker to document changes and it is easy to refer
back to admission medication.
Pharmacy documentation of admission medication is in the form of a free text note linked to the
electronic prescription; this is updated during the admission to note the changes to medication and
reasons for those changes. This note is then used at discharge to ensure the information is
communicated on the discharge summary. The disadvantage is that this is time consuming and the
quality of the note varies considerably.
CR Clerking pro-
forma
East Sussex
Healthcare NHS
Trust
(Electronic
System)
Alan Hopkins
Alan.Hopkins@esht.
nhs.uk
A set template is used to complete MR that can be uses with handheld tablet devices. This allows
the completion of the forms on the ward (either at the nurse’s station or bedside). The form
encompasses medication on admission, additional medication, community Pharmacy services used
and compliance. Because the form is electronic it can be accessed anytime and saved so it can
follow the patient around the hospital during their stay e.g. patient admitted to MAU and had an MR,
then the electronic entry will be saved under the ward folder and transfer to different wards as and
when required. The disadvantage with the system is the need for printing and filing hard copies in
EH Tablet form

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 27
Medicines Use and Safety
S
P S
the notes. Sometimes they get lost, misfiled by other healthcare professionals, or overlooked
because it has no set place within the notes.
Next steps: To integrate this form into the Patient Documentation Booklet. This is used for every
hospital admission and will ensure all health care professionals know where to find MR information
and will support discrepancy resolution.
East London
NHS Foundation
Trust
Alan Cottney
Alan.Cottney@eastl
ondon.nhs.uk
A MR form is used. Advantages are:
Word format, so can be completed electronically- makes MR clear and easy to read, easy to
add rows if more space is required.
Can be printed off and inserted in patients’ notes, or attached to electronic notes.
Useful as a prompt: reminds to use more than one source for MR, reminds to ask about
compliance aid.
Contains space for documenting any discussion that occurred with the patient, and for
highlighting discrepancies.
When filed in notes can help provide clear audit trail, and a reference for future use.
Disadvantages are:
Filed in notes, so no information about MR actually present on drug chart.
A Fax drug history form is also used. There are some advantages we have found with this version:
Clearly asks for a clinical summary - which can help to identify why certain medication is
prescribed - thus potentially sparing another phone call to the GP.
EL MR form
EL Fax form

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 28
Medicines Use and Safety
S
P S
Also clearly asks for allergy information and whether or not the patient is on a compliance aid -
so helps to ensure we get all necessary information first time round.
As the document is in Word format it can be completed electronically, and faxed from NHS Mail
account - making the process quicker and reducing paper burden.
Peterborough
and Stamford
Hospitals NHS
Foundation
Trust
Meb Walji
Meb.Walji@pbh-
tr.nhs.uk
The MR policy has information in the appendix on how to approach a MR consultation and also how
to document information.
PS MR policy
Oxleas NHS
Foundation
Trust
Carol Paton
Carol.Paton@oxleas
.nhs.uk
Oxleas NHS Trust has determined that MR responsibilities lie with the admitting doctor. The
Pharmacist provides a second check that MR has taken place within one week of admission when
any discrepancies which look to be unintentional will be recorded. It was decided that taking the
responsibility for MR away from doctors was deskilling them. Regular audit is used to demonstrate
effectiveness of this approach.
OX MR policy
Sherwood
Forest Hospitals
NHS Foundation
Trust
Cath Fletcher
Catherine.Fletcher@
sfh-tr.nhs.uk
The medication history is documented in the appropriate section of the patients medical clerking.
MR info is also documented on the drug chart in dedicated box(es) on the front with sources used.
If only one source has been obtained the notes are annotated 2nd so it is clear that a second
source should be obtained if possible. Changes made on admission e.g. medication on hold, dose
changes etc. are also documented on the front of the drug chart. If an MMT does the DH and there
are discrepancies they write ‘see clerking ’ on the front of the drug chart so the Pharmacist knows
there are issues to be resolved. The Pharmacist ticks the box, initials and dates once these are
resolved.
SF Drug Chart
SF SOP for MR
SF Enabling policy

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 29
Medicines Use and Safety
S
P S
Pharmacy annotate all prescriptions inside the chart with either ‘DH’ or ‘new’ to assist medical staff
with informing GPs of medication changes on discharge. Also annotate with or dose on DH items
where doses have been changed. This also helps to ensure appropriate transfer of info to GPs on
discharge. Pharmacy patient profiles which are completed at the point of admission also have a tick
box to confirm when MR is complete.
Discrepancy resolution: A trust Enabling Policy is in place which allows Pharmacists to write up
items such as eye drops, creams, salbutamol inhaler, GTN spray etc without the need for them to
be prescribed. The trust approves this and it has been found to be very helpful for items which Drs
do not see as a priority to prescribe.
University
Hospitals of
Leicester NHS
Trust
Hannah Kooner
Hannah.Kooner@uh
l-tr.nhs.uk
Catherine Loughran
Catherine.Loughran
@uhl-tr.nhs.uk
Oncology and Haematology wards currently using electronic prescribing- Medchart.
All Medicines Reconciliation information is added to EPMA only. No documentation in the notes is
needed. Pharmacists will document in the medical notes if changes not actioned from EPMA.
Advantages: All information can be viewed at all times. Previous admissions are easily accessible
if needed. Clear comment can be viewed. Discrepancies easily documented
Electronic handover is used as form of communication and follow up tool. – Can be accessed
anywhere by multiple members of the team- NO sharing of a paper handover. Clear and timely.
Disadvantages: Can be time consuming. Some duplication with documentation on EPMA.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 30
Medicines Use and Safety
S
P S
Discrepancy resolution: When discrepancies occur between the MR and the electronic chart,
medications are added to the medications on admission page and an alert is added to the patients
chart. This alert will appear each time a Pharmacist or doctor accesses the chart until this alert has
been cancelled. This also acts as a reminder for the Pharmacist to follow the issue up if still needed.
East Lancashire
Hospitals NHS
Trust
Alistair Gray
s.uk
Overview: A checklist approach has been developed and evolved to support the Medicines
Reconciliation process by the Pharmacy team. A printed checklist is inserted into the patient notes
at the beginning of the Meds Rec process which prompts the capture of the right information in a
logical order to ensure that an accurate, complete and informative drug history is obtained. The
checklist contains prompts to refer the patient to other health professional e.g. anticoagulant team,
diabetic specialist nurse and acute oncology team when appropriate (NB: an e-patient tracking
system which facilitates referral to other health professionals).
Pharmacists and Pharmacy technicians are also competency assessed prior to conducting
Medicines Reconciliations; the checklist helps maintain their competencies.
In addition changes to prescription stationery complements the MR process making it easy to
identify what medicines the patient has come in on, what has started, stopped, changed and why.
Outcomes: Although not formally audited the checklist intervention and changes in drug chart
stationary has noticeably improved the quality and consistency of information captured during the
MR process compared to pre-introduction of the checklist. It has also improved the quality of
information contained within the discharge letter benefitting transfer of care. Screening a TTA is a
lot more quicker/easier when a patient has been through this checklist process and there is a lot
more confidence in the information contained within the discharge letter (the e-discharge letter
Medicines
Reconciliation
Checklist:
http://www.medicines
resources.nhs.uk/upl
oad/documents/Com
munities/SPS_E_SE
_England/East%20L
ancashire%20Med%
20Rec%20Checklist_
May%2015.pdf
Example of Drug
Chart and Discharge
Stationary:
http://www.medicines
resources.nhs.uk/upl
oad/documents/Com
munities/SPS_E_SE

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 31
Medicines Use and Safety
S
P S
includes a dropdown list to indicate if the drug history has been formally checked or not by a
Pharmacist).
_England/East%20L
ancashire%20Drug%
20Chart%20and%20
Discharge%20Statio
nary_May%2015.pdf
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 32
Medicines Use and Safety
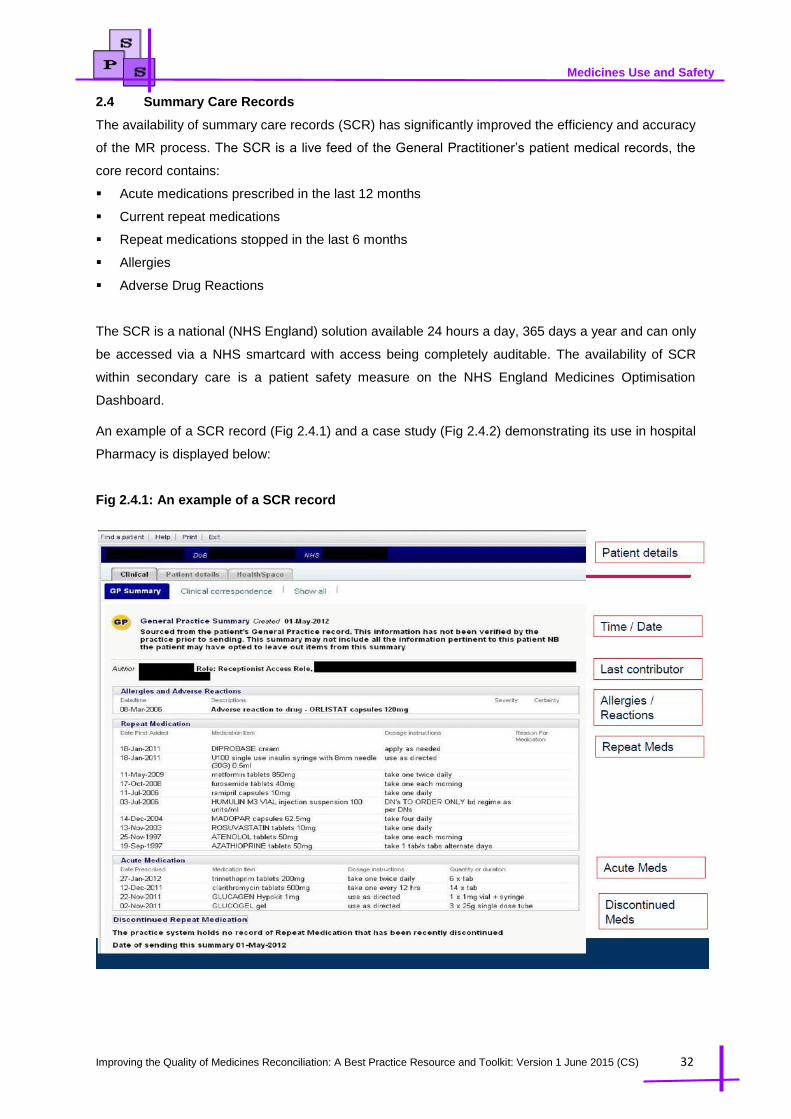
2.4 Summary Care Records
The availability of summary care records (SCR) has significantly improved the efficiency and accuracy
of the MR process. The SCR is a live feed of the General Practitioner’s patient medical records, the
core record contains:
Acute medications prescribed in the last 12 months
Current repeat medications
Repeat medications stopped in the last 6 months
Allergies
Adverse Drug Reactions
The SCR is a national (NHS England) solution available 24 hours a day, 365 days a year and can only
be accessed via a NHS smartcard with access being completely auditable. The availability of SCR
within secondary care is a patient safety measure on the NHS England Medicines Optimisation
Dashboard.
An example of a SCR record (Fig 2.4.1) and a case study (Fig 2.4.2) demonstrating its use in hospital
Pharmacy is displayed below:
Fig 2.4.1: An example of a SCR record

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 33
Medicines Use and Safety
Fig 2.4.2: SCR use in hospital case study

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 34
Medicines Use and Safety
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 35
Medicines Use and Safety
For further information regarding implementing the contact details of the regional implementation teams
are detailed below. They can also offer practical advice and support, including step-by-step guides,
training and engagement materials, alongside other useful resources.
North: [email protected]
Midlands: [email protected]
East: [email protected]
London: [email protected]
South: [email protected]
References:
1. Institute for Healthcare Improvement (IHI) Webpage. Available at
http://www.ihi.org/resources/Pages/Changes/ReconcileMedicationsatAllTransitionPoints.aspx
(Accessed 20th Nov 2014)
2. World Health Organisation (WHO). Assuring medication accuracy at transitions in care: Medication
Reconciliation. Available at http://www.who.int/patientsafety/implementation/solutions/high5s/h5s-
guide.pdf?ua=1 (Accessed 4th April 2015)

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 36
Medicines Use and Safety
S
P S
Chapter 3 Best Practice Standards
This chapter aims to set out the best practice standards that should be observed when conducting robust Medicines Reconciliation. The best practice standards
were developed by the MR working group through a consensus approach.
There are 88 individual best practice standards that have been grouped into 6 overarching standards which have been further separated into 3 main themes
based on the process of conducting a Medicines Reconciliation. These standards aim to support and enable individuals and organisations to improve the quality
of Medicines Reconciliation. The standards although predominantly applicable to secondary care providers are transferable to other care settings (e.g. primary
and community care) and should be used to develop best practice. It should also be noted these standards are equally applicable to the paediatric population.
Theme: Timing of Medicines Reconciliation
Standard 1 – Timing of Medicines Reconciliation on Admission
Much of the guidance centred on Medicines Reconciliation for example the NICE Medicines Optimisation Guidance1, the RPS Professional Standards for
Hospital Pharmacy2 and the World Health Organisation3 guidance indicates that MR should be carried out within 24 hours of admission to a hospital setting.
Within this toolkit and in line with the standards set by NHS England in its medication safety thermometer, this guidance is pragmatically interpreted as standard
1.1 set out below. In terms of best practice this standard is applicable to all hospital settings and care areas, however, it is acknowledged that in certain settings
or care areas e.g. Community Hospitals, Mental Health, Maternity, Day Surgery a limited clinical Pharmacy service may be in operation and that this standard
may not be achievable – in these scenarios Senior Pharmacy Managers should undertake a risk assessment and set safe local standards, have mitigation
strategies in place and/or document the risk on the trust risk register.
Standard Helpful Hints / Comments 1.1 Ensure that patients receive a MR by a member of the Pharmacy team
the day of, or the day following, admission.
It is appreciated that it may be difficult to adhere to the standard where
patients are admitted over a weekend period (e.g.Friday through to
Sunday) however, all patients should receive the same level of care
irrespective of when they are admitted in line with the 7 day working
agenda

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 37
Medicines Use and Safety
S
P S
A member of the Pharmacy team simply requesting a patient’s
medication list from the GP does NOT meet the MR definition unless any
discrepancies have been identified AND recorded (i.e. within the clinical
notes and /or on the prescription chart)
For the standard to be met all of the discrepancies identified DO NOT
need to have been fully resolved (Resolution of any discrepancies
identified should however occur as soon as possible using clinical
judgement to ensure safe and effective patient care)
This measure should be fed into the NHS Medication Safety
Thermometer which is subsequently fed in the NHS Medicines
Optimisation Dashboard. The MO Dashboard can be viewed at
http://www.england.nhs.uk/ourwork/pe/mo-dash/
Theme: Collection and Checking of Medicines Related Information
Standard 2 – Patient Consultation
Consultation skills are of paramount importance during the Medicines Reconciliation process. The RPS Professional Standard 1.1 for Hospital Pharmacy
Services2 states that communication with, and involvement of, patients and carers is an integral component of safe, effective Pharmacy services, therefore
unless it is not physically possible (eg, the patient is unconscious or confused) the patient should always be consulted as part of the MR process — since they
are the ones taking the medicines. The table below outlines the standards required when Pharmacy professionals undertake a consultation with a patient when
conducting a Medicines Reconciliation.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 38
Medicines Use and Safety
S
P S
Standards Helpful Hints / Comments
Structure of the Consultation
2.1 Ensure that the consultation is undertaken in a supportive environment, taking account of safety,
comfort, confidentiality, dignity and respect
2.2 Ensure an introduction takes place and includes name and job role and purpose of the
consultation
2.3 Ensure that the patient’s identity is confirmed using at least two parameters e.g. name and date
of birth
2.4 Ensure the patient has cognition and capacity
2.5 If there are language difficulties consider using NHS Translation Services or other appropriate
services available within the organisation
2.6 Ensure that both open and closed questions are used to elicit a full list of the patient’s medication
regime
2.7 Ensure the discussion includes questions about how the patient manages their medication in their
own home or care setting
For example whether they have a medication
compliance aid or help from relatives or
carers.
2.8 Confirm adherence to medication regime and establish if the patient has difficulty with adhering to
the prescribed medication regime e.g. missed dose(s) of treatment with reasons
Consultation Skills and Behaviours
2.9 Ensure that the scene for the consultation is set professionally and appropriately while building
rapport with the patient
2.10 Ensure and acknowledge the patient’s agenda without interrupting and further balance with your
own agenda before negotiating a shared agenda

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 39
Medicines Use and Safety
S
P S
2.11 Communicate positively and effectively throughout the session, using language that is
appropriate and respectful to the patient
Using non-technical, non-jargon language has
the greatest positive impact on the patient
2.12 Ensure that information is shared and discuss options in an open, honest and unbiased manner
to support the patient in assessing the risks versus benefits in relation to medicines-taking and
making changes to lifestyle
2.13 Ensure that communication and consultation skills are adapted to meet the needs of different
patients
Patient’s may not have English as their first
language or some patients may have capacity,
physical or sensory impairments
2.14 Recognise that patients are diverse; that their behaviour, values and attitudes vary as individuals
and with age, gender, ethnicity and social background, and that you should not discriminate
against people because of those differences
2.15 Ensure that respect for the patient’s perception is considered and support the patient in self-
expression.
2.16 Consider the use of prompting tools to facilitate the consultation (such as checklists) in such a
manner that it does not detract from the patient focus of the consultation
See East Lancashire Hospitals NHS Trust
Checklist in Chapter 2
2.17 Ensure that questioning techniques utilise active listening to draw out the information needed to
gain maximum benefit from the discussion and challenge the patient at a level which is
appropriate for them
2.18 Ensure that patient understanding is checked at points within the consultation while allowing the
patient time and space to reflect
Example Questions/Prompts
“What medications do you take every day?”
“Are there any medicines that you take less frequently e.g weekly or monthly medicines or
medicines just when you need them?”

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 40
Medicines Use and Safety
S
P S
“Do you use any eye drops, ear drops, inhalers, creams, ointments etc?”
“Have you recently taken any antibiotics within the last 2-3 weeks?”
“Is there anything else you take that has not been mentioned?”
“Do you have any allergies to medications?”
“Do you take any over-the-counter medicines?”
“Do you take any multivitamins or herbal supplements?”
“Are you wearing any medication patches?”
“What happens when you take this medication?”
Ask (where appropriate) if the patient uses any of the following?
If on warfarin – where is the yellow book?
If diabetic and on insulin – check insulin device and insulin passport
Other monitoring booklets e.g. DMARD, Chemo
Once weekly medication (state day of week)
Home Oxygen
Over the counter remedies, herbal, sourced from the internet, “recreational”
Standard 3 – Sources of Information
Several sources of information are available to help obtain an accurate medication history, none of which are 100% reliable. Therefore it is often necessary to
use more than one source to confirm the medication history. On occasions one source of information may be sufficient, eg, it would be unnecessary to contact
a GP surgery when an otherwise healthy patient says they do not take any medicines. The table below lists the possible sources of information, the standards
that should be applied when using the information sources with some helpful hints and limitations to be mindful of.
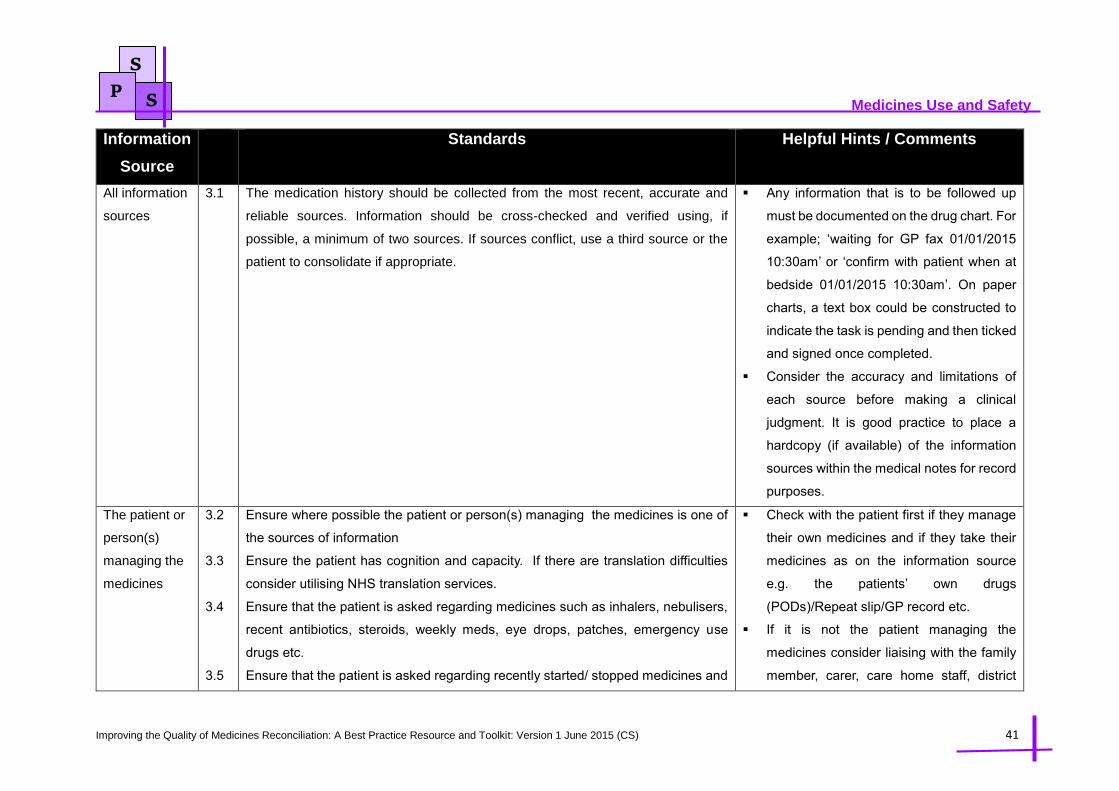
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 41
Medicines Use and Safety
S
P S
Information
Source
Standards Helpful Hints / Comments
All information
sources
3.1 The medication history should be collected from the most recent, accurate and
reliable sources. Information should be cross-checked and verified using, if
possible, a minimum of two sources. If sources conflict, use a third source or the
patient to consolidate if appropriate.
Any information that is to be followed up
must be documented on the drug chart. For
example; ‘waiting for GP fax 01/01/2015
10:30am’ or ‘confirm with patient when at
bedside 01/01/2015 10:30am’. On paper
charts, a text box could be constructed to
indicate the task is pending and then ticked
and signed once completed.
Consider the accuracy and limitations of
each source before making a clinical
judgment. It is good practice to place a
hardcopy (if available) of the information
sources within the medical notes for record
purposes.
The patient or
person(s)
managing the
medicines
3.2
3.3
3.4
3.5
Ensure where possible the patient or person(s) managing the medicines is one of
the sources of information
Ensure the patient has cognition and capacity. If there are translation difficulties
consider utilising NHS translation services.
Ensure that the patient is asked regarding medicines such as inhalers, nebulisers,
recent antibiotics, steroids, weekly meds, eye drops, patches, emergency use
drugs etc.
Ensure that the patient is asked regarding recently started/ stopped medicines and
Check with the patient first if they manage
their own medicines and if they take their
medicines as on the information source
e.g. the patients’ own drugs
(PODs)/Repeat slip/GP record etc.
If it is not the patient managing the
medicines consider liaising with the family
member, carer, care home staff, district

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 42
Medicines Use and Safety
S
P S
recent changes in doses.
nurse etc.
If the patient is temporarily unable to
confirm the medication history for example
due to confusion, document this so that
other members of staff are aware and
leave a prompt to try again sometime later
when the condition may have improved.
This is important as medicines are not
always taken as prescribed.
Check for any hand held medicines related
documents (e.g. methotrexate book,
warfarin book, Insulin passport, My
Medication Passport, medicine/healthcare
apps)
Repeat
prescription
tear-off slips.
3.6
3.7
3.8
Ensure that all the pages of the repeat tear-off slips are available and checked
Confirm details with the patient or person(s) managing the medicines to ensure it
is current
Check the dates when the prescriptions were last issued
Limitations of a repeat prescription tear off
slips:
Does not include information on acute
prescriptions
Prescription may not have been collected/
dispensed/ taken
Some medicines may have stopped
recently

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 43
Medicines Use and Safety
S
P S
Requesting
information
from the GP
3.9
3.10
3.11
3.12
Obtain and document consent from the patient to contact the GP for information
unless the patient is unable to give consent
Confirm the name and designation of the person providing the information from
the GP practice
Obtain a print out from the GP system via a fax or email as opposed to verbal
communication. If possible, request a standard report from GPs regarding
medication (the GP systems have this functionality). This approach will support
requesting and sending essential information easier and more efficient
Ensure GP information is as complete and current as possible and includes:
Details of any acute prescriptions issued in the last 3 months
Regular, on-going treatment including repeat prescriptions
Allergy status
It may be necessary (use clinical judgment) to request the last five
consultations the patient has had with the GP and past medical history as it
may help in revealing recent medication changes
Use discretion on the need to contact the
GP if the information required is minimal
such as to confirm no medication
Information provided by the GP has
several limitations such as it will or may not
include:
o OTC medicines or
o Hospital supplied medication
o Medication supplied via homecare
o Medication prescribed by a Dental
practitioner
o Medication prescribed by an
urgent care centre, walk in centre,
Hospital at Home team, specialist
nurse prescribers, GUM/HIV
medicines
If using a standard report it should contain
repeat medication, acute medication
issues, allergies and display when
medicines were last issued along with
quantities. A template report set up in
System One prescribing system has been
demonstrated to work well in Bedfordshire
Fax or email communication is preferred

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 44
Medicines Use and Safety
S
P S
to reduce the risk of any errors as a result
of miscommunication or omission of
important information
If emailing ensure it is from and to an
encrypted central mailbox e.g. nhs.net
If faxing ensure that only staff have
access to the fax machine and adhere to
any local policies that may be in place
regarding faxing confidential and patient
related information.
Check the dates of issue and quantities of
medicines issued as these may highlight
adherence issues or if a medicine is no
longer being taken
Only viewing the repeat medication is
often insufficient as the patient may have
been issued an acute prescription recently
e.g. An antibiotic for a chest infection that
has then not resolved and resulted in the
hospital admission
Some GP systems may remove items
from repeat list if not issued frequently
In addition GPs may not make an item
available on repeat for a number of

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 45
Medicines Use and Safety
S
P S
reasons
o newly started and the GP wishes
to monitor patient response after
each prescription
o the GP may want to remain in
control of quantities issued
o the GP may have just forgotten/
not yet had time to move item to
repeat
o the medicine may have been
initiated elsewhere but GP may
not yet have received / actioned
letter containing full directions on
continuing therapy
Recently amended/started/stopped
medication may well have contributed to
the reason for admission so this may
affect the decision to
amend/withhold/restart medicines on
admission. This information may be in the
acute prescriptions section or within the
GP consultation section
Verbal requests to patients by the GP to
omit or change medication and/or

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 46
Medicines Use and Safety
S
P S
handwritten prescriptions may not appear
on the prescription record unless a
prescription is issued.
The outcome of a telephone appointment
or home visit with regards to medicine
changes is usually documented in the
consultations section. This information
would otherwise be missed and may help
the Pharmacy team to understand the
intention of the GP and/or explain why the
patient may not be taking their medicine as
prescribed.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 47
Medicines Use and Safety
S
P S
Summary
Care Records
3.13
3.14
3.15
3.16
Ensure that staff members that utilise SCR and have undertaken the relevant face
to face or eLearning training available on the use of SCR
Obtain and document patient consent prior to accessing SCR (check local policy
and guidance)
Check the date the record was updated (should be updated daily)
Print off the information and place in the patient’s notes
The SCR does not always state the last
date the prescription was issued
Sometimes states ‘Date prescribed’ which
could be some time ago therefore clarify if
patient is still taking.
Recent
Hospital
Discharge
Notifications
3.17
3.18
Ensure that hospital discharge is recent (use clinical judgement)
Confirm details with patient/carer to identify any further clinically relevant changes
since discharge
It is important to be mindful that the GP
may not have updated the patient records
or possibly actioned the discharge
notification changes
It is important not to assume that the
discharge notification is accurate as if a
thorough MR was not conducted at the
admission within that episode of care the
discharge notification may be inaccurate
Hospital
Transfer
Letters
3.19 Ensure that a copy of the drug chart in use prior to transfer is faxed across This will allow an appreciation of what
medication the patient has been
administered in the preceding days and
weeks, it may also provide information on
the MR conducted on admission and any
pharmaceutical interventions made
If no MR was completed or unclear, there
may be a need to undertake a full MR and

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 48
Medicines Use and Safety
S
P S
document which medicines were taken
prior to initial hospital admission and
which medicines have been started at the
transferring hospital. This is important as
all changes must be communicated to the
GP upon discharge
Patients Own
Drugs (POD)
3.20
3.21
3.22
Ensure that if a POD SOP is in place and it is being followed
Ensure that all PODs are assessed
Where possible ensure that each POD is confirmed with the patient or person(s)
managing the medicines
Be vigilant for dispensing errors
Confirm that patients can take their
medicines or are taking as labelled.
Confirm the doses being taken as they may
have been changed but not yet reflected on
current supply
Check for additional medicines not listed
on sources checked for example hospital
only medicines, homecare medicines etc.
Check for CDs, fridge / bulky items as
these may not be brought in or the nurse
may already have locked away
Check for medicines that the patient may
keep on their person e.g. topical
preparations, inhalers
Some PODs may no longer be current,
may be recently stopped, may be a family
members medicines or a dispensing error

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 49
Medicines Use and Safety
S
P S
3.23 Ensure PODs are suitable for use, check local POD SOP an example criteria is
detailed below:
o PODs must be clearly labelled with the patient’s name
o PODs that are dispensed must have printed directions on the pack
o Ensure that the packaging corresponds to the content and that the
description of the product or Pharmacy label matches the contents
o If not in original (manufacturer’s) container, it is possible to identify
the product
o Check the patient is able to use any medication devices correctly e.g.
Inhalers
o Confirm the identity of any medicines supplied in a compliance aid
and whether there are any medicines that are not in the compliance
aid e.g. PRN medicines, liquid medicines
o Confirm any discrepancies with the dispensing Community Pharmacy
Be mindful that the patient may have only
brought blister strips with no container or
label
OTC, GSL products, inhalers, insulin,
GTN spray etc. may not be labelled.
Ensure that the medicines belong to the
patient and attach name label if not
labelled.
If dispensed more than 6 months ago,
check for potential non adherence to the
medication regime
Confirm the medicine has been prescribed
for the patient prior to admission.
Nursing or
care home
Medication
administration
record (MAR)
charts.
3.24
3.25
Ensure that all the pages of the MAR chart are available
Check with the patient or care home staff when the last PRN medications were
taken if relevant
Check for any potential transcription
errors
Printed charts from community
Pharmacies maybe more accurate,
however be mindful of medicines that may
not be documented on the MAR chart for
example if a recent hospital discharge has
taken place or an acute prescription has
been supplied
Community 3.26 If possible obtain consent from the patient to call the community Pharmacist Be mindful that the patient may use more

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 50
Medicines Use and Safety
S
P S
Pharmacist 3.27
3.28
3.29
Confirm and document name and designation of the person providing the
information
Notify the community Pharmacist when a patient using a MCA is admitted and
discharged
Ensure that upon discharge all medication changes are communicated
than one community Pharmacy therefore
a complete medication history may not be
available
MCAs are usually dispensed as repeat
prescriptions and community Pharmacies
may attempt to deliver ongoing supplies
whilst a patient is in hospital if not notified
of their admission.
Upon discharge, community Pharmacies
will often arrange collection of MCAs from
a patients home if they have not been
taken into hospital and are no longer
required
Standard 4 – Identification and Resolution of Discrepancies
Resolution of any medication related discrepancies identified is the CRITICAL outcome of the MR process that supports patient safety and good quality care,
therefore processes must be in place to ensure that discrepancies are resolved in a timely manner.
Discrepancies may be intentional or unintentional. Intentional discrepancies can be defined as any difference between the medicines the patient was taking
prior to admission and the medicines prescribed in their new care setting that have been changed intentionally and agreed with the clinician(s) responsible for
the patient's care. Unintentional discrepancies (errors, omissions or unintentional additions) can be defined as any difference between the medicines the patient
was taking prior to admission and the medicines prescribed in their new care setting that is not a conscious change. The table below sets out standards that
must be adhered to when identifying and resolving any medication related discrepancy.
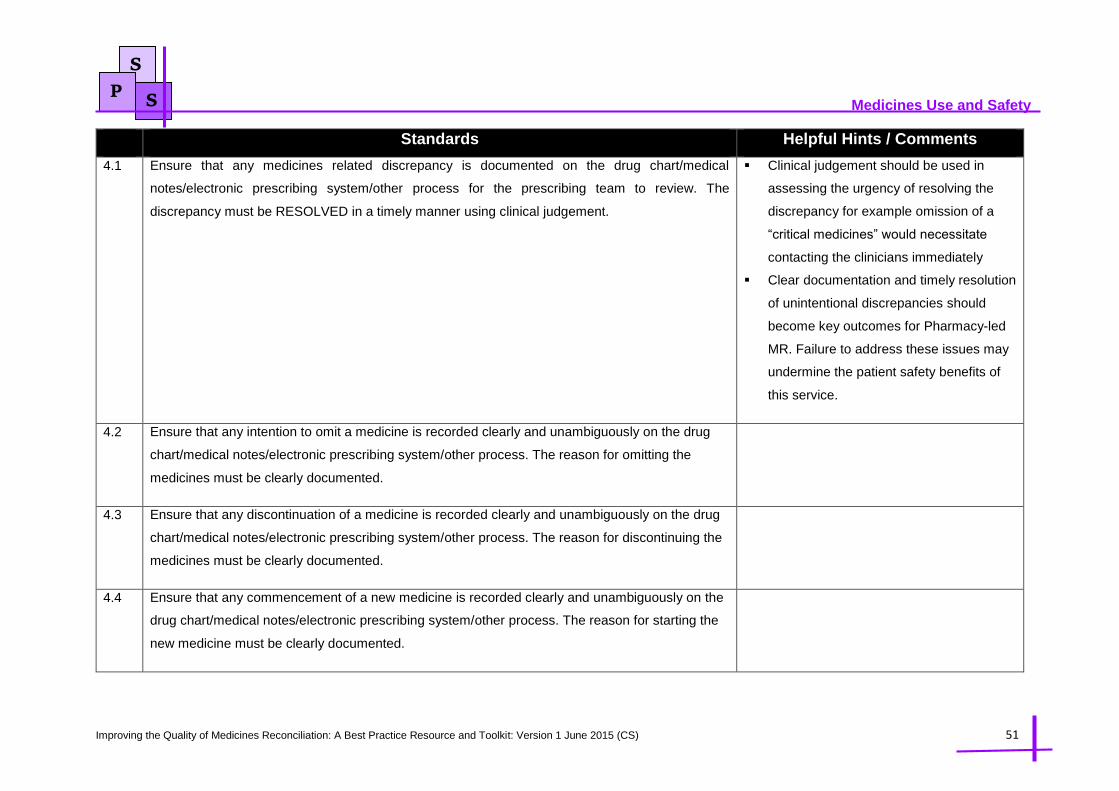
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 51
Medicines Use and Safety
S
P S
Standards Helpful Hints / Comments
4.1 Ensure that any medicines related discrepancy is documented on the drug chart/medical
notes/electronic prescribing system/other process for the prescribing team to review. The
discrepancy must be RESOLVED in a timely manner using clinical judgement.
Clinical judgement should be used in
assessing the urgency of resolving the
discrepancy for example omission of a
“critical medicines” would necessitate
contacting the clinicians immediately
Clear documentation and timely resolution
of unintentional discrepancies should
become key outcomes for Pharmacy-led
MR. Failure to address these issues may
undermine the patient safety benefits of
this service.
4.2 Ensure that any intention to omit a medicine is recorded clearly and unambiguously on the drug
chart/medical notes/electronic prescribing system/other process. The reason for omitting the
medicines must be clearly documented.
4.3 Ensure that any discontinuation of a medicine is recorded clearly and unambiguously on the drug
chart/medical notes/electronic prescribing system/other process. The reason for discontinuing the
medicines must be clearly documented.
4.4 Ensure that any commencement of a new medicine is recorded clearly and unambiguously on the
drug chart/medical notes/electronic prescribing system/other process. The reason for starting the
new medicine must be clearly documented.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 52
Medicines Use and Safety
S
P S
4.5 Ensure that any change in dosing of a medicine is recorded clearly and unambiguously on the
drug chart/medical notes/electronic prescribing system/other process. The reason for the changing
the dose of the medicine must be clearly documented.
e.g. “gliclazide dose reduced due to low BMs,
from 80mg BD to 40mg BD”.
4.6 Ensure that any changes in formulation of a medicine are recorded clearly and unambiguously on
the drug chart/medical notes/electronic prescribing system/other process. The reason for the
change in formulation of the medicine must be clearly documented.
e.g. “medicines converted to liquids whilst the
patient has NG tube in place”.
4.7 Ensure that changes in medicines due to local formulary restrictions are recorded clearly and
unambiguously on the drug chart/medical notes/electronic prescribing system/other process with
detail of the original medicine.
Theme: Communication and Documentation of Medicines Reconciliation
Standard 5 - Documentation of Medicines Reconciliation at Admission
The documentation of the Medicines Reconciliation is an integral part of the MR process as it allows all healthcare professionals to view the changes to the
patient’s medication regime and also allows the final discharge summary to be an accurate list of medications that can be communicated to the next caregiver.
The table below details the standards required when documenting the MR at admission.
Standards Helpful Hints / Comments
5.1 Ensure that all written documentation is legible, clear and in indelible ink or electronic
5.2 Ensure that all allergies or lack of allergies to medicines (NKDA) are clearly documented including the causative
medication and brief description of reaction/outcome
5.3 Ensure that generic drug names are used in all documentation unless otherwise specified for example when
brand names are required for bioavailability issues
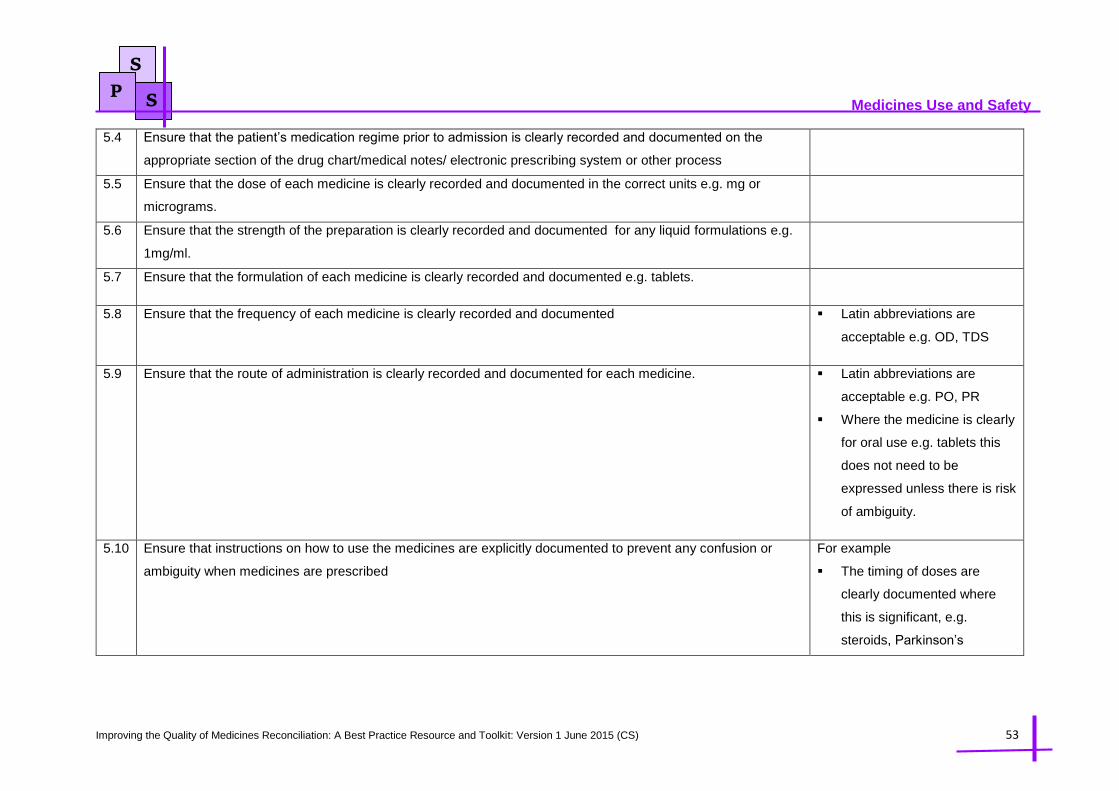
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 53
Medicines Use and Safety
S
P S
5.4 Ensure that the patient’s medication regime prior to admission is clearly recorded and documented on the
appropriate section of the drug chart/medical notes/ electronic prescribing system or other process
5.5 Ensure that the dose of each medicine is clearly recorded and documented in the correct units e.g. mg or
micrograms.
5.6 Ensure that the strength of the preparation is clearly recorded and documented for any liquid formulations e.g.
1mg/ml.
5.7 Ensure that the formulation of each medicine is clearly recorded and documented e.g. tablets.
5.8 Ensure that the frequency of each medicine is clearly recorded and documented Latin abbreviations are
acceptable e.g. OD, TDS
5.9 Ensure that the route of administration is clearly recorded and documented for each medicine. Latin abbreviations are
acceptable e.g. PO, PR
Where the medicine is clearly
for oral use e.g. tablets this
does not need to be
expressed unless there is risk
of ambiguity.
5.10 Ensure that instructions on how to use the medicines are explicitly documented to prevent any confusion or
ambiguity when medicines are prescribed
For example
The timing of doses are
clearly documented where
this is significant, e.g.
steroids, Parkinson’s

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 54
Medicines Use and Safety
S
P S
medicines, day of week for
weekly preparations
For inhaled preparations the
strength and device is clearly
documented
For topical preparations that
the site of application is
clearly documented
For insulin preparations, the
brand, formulation, and type
of device that the patient
normally uses is clearly
documented
For hospital-only or
homecare medicines the
name of the supplier is
clearly documented
For high-risk medicines such
as warfarin or methotrexate
any additional information is
clearly documented
5.11 Ensure any recent changes (within 1-2 months) to the patient’s medication regime is clearly recorded and
documented as part of the MR
5.12 Ensure that the sources used for conducting the MR are clearly recorded and documented

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 55
Medicines Use and Safety
S
P S
5.13 Ensure that any adherence issues identified during the MR process are clearly recorded and documented with
actions taken to resolve the issues
5.14 Ensure that the name and contact details of the person conducting the MR is clearly recorded and documented
along with the date.
Standard 6 - Documentation of Medicines Reconciliation at Discharge
Ensuring that all the all necessary information about the patient’s medicines is accurately documented and communicated to the next healthcare provider is
vital to support safe transfer of care. The Institute of Health Improvement suggested that poor information communication on discharge is responsible for over
50% of all medication errors and up to 20% of adverse events4. The RPS Professional Standard 3.2 for Hospital Pharmacy Services2, the RPS Keeping patients
safe when they transfer between care providers5 – getting the medicines right good practice guidance and Academy of Medical Royal Colleges Standards for
the clinical structure and content of patient records6 collectively set standards of how medicines related information should be communicated at care interfaces.
The table below sets out the standards required when communicating medicines related information on the discharge summary when transferring from
secondary care.
Standards Helpful Hints / Comments
6.1 The discharge summary contains clearly documented details of patients
First & last name
Date of birth
Address
Hospital number
NHS number
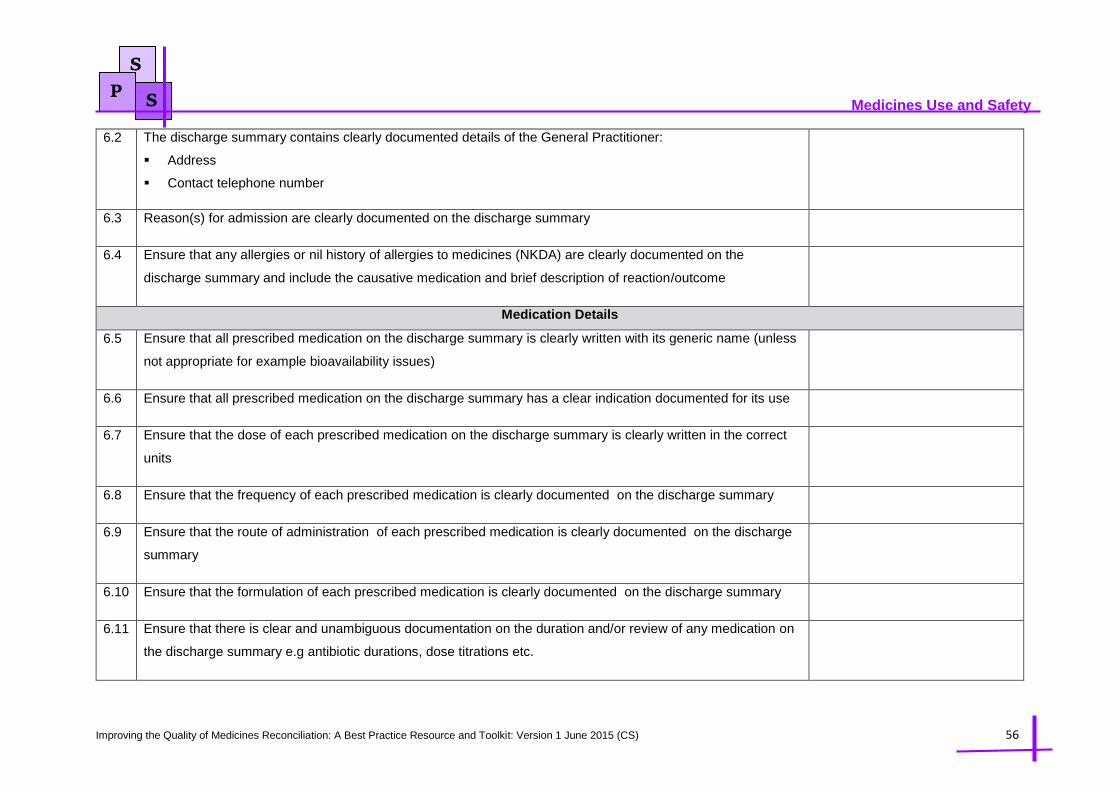
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 56
Medicines Use and Safety
S
P S
6.2 The discharge summary contains clearly documented details of the General Practitioner:
Address
Contact telephone number
6.3 Reason(s) for admission are clearly documented on the discharge summary
6.4 Ensure that any allergies or nil history of allergies to medicines (NKDA) are clearly documented on the
discharge summary and include the causative medication and brief description of reaction/outcome
Medication Details
6.5 Ensure that all prescribed medication on the discharge summary is clearly written with its generic name (unless
not appropriate for example bioavailability issues)
6.6 Ensure that all prescribed medication on the discharge summary has a clear indication documented for its use
6.7 Ensure that the dose of each prescribed medication on the discharge summary is clearly written in the correct
units
6.8 Ensure that the frequency of each prescribed medication is clearly documented on the discharge summary
6.9 Ensure that the route of administration of each prescribed medication is clearly documented on the discharge
summary
6.10 Ensure that the formulation of each prescribed medication is clearly documented on the discharge summary
6.11 Ensure that there is clear and unambiguous documentation on the duration and/or review of any medication on
the discharge summary e.g antibiotic durations, dose titrations etc.
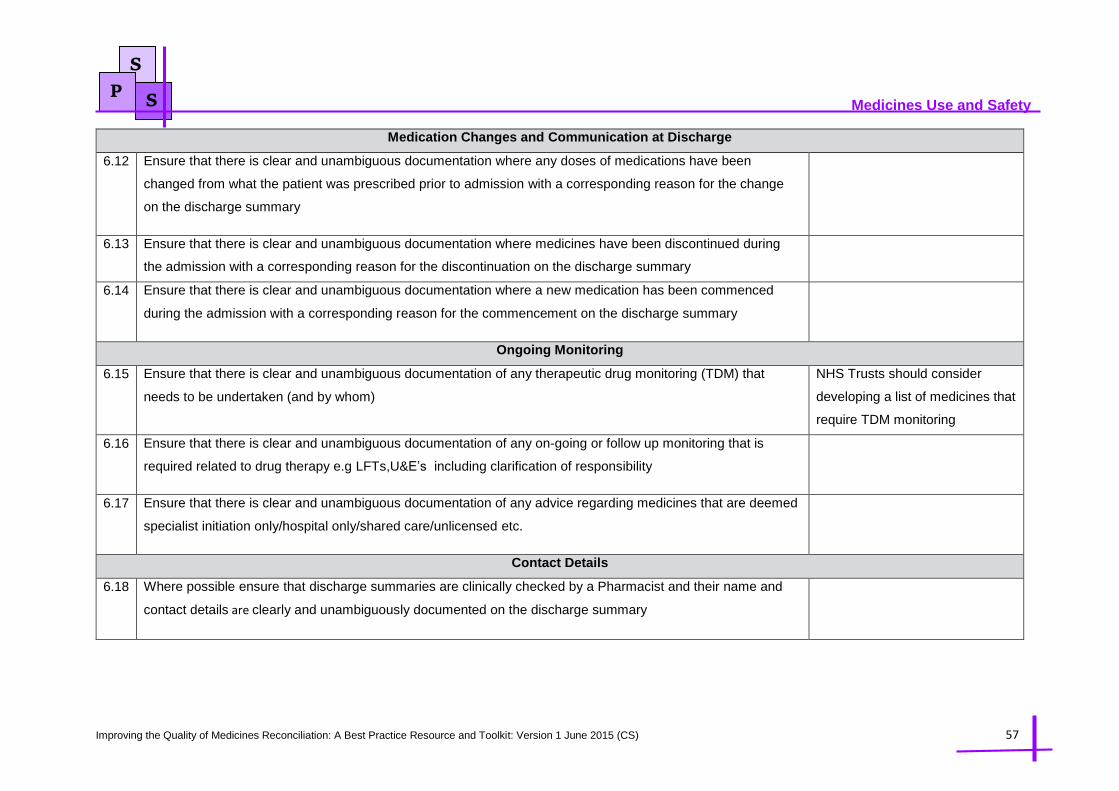
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 57
Medicines Use and Safety
S
P S
Medication Changes and Communication at Discharge
6.12 Ensure that there is clear and unambiguous documentation where any doses of medications have been
changed from what the patient was prescribed prior to admission with a corresponding reason for the change
on the discharge summary
6.13 Ensure that there is clear and unambiguous documentation where medicines have been discontinued during
the admission with a corresponding reason for the discontinuation on the discharge summary
6.14 Ensure that there is clear and unambiguous documentation where a new medication has been commenced
during the admission with a corresponding reason for the commencement on the discharge summary
Ongoing Monitoring
6.15 Ensure that there is clear and unambiguous documentation of any therapeutic drug monitoring (TDM) that
needs to be undertaken (and by whom)
NHS Trusts should consider
developing a list of medicines that
require TDM monitoring
6.16 Ensure that there is clear and unambiguous documentation of any on-going or follow up monitoring that is
required related to drug therapy e.g LFTs,U&E’s including clarification of responsibility
6.17 Ensure that there is clear and unambiguous documentation of any advice regarding medicines that are deemed
specialist initiation only/hospital only/shared care/unlicensed etc.
Contact Details
6.18 Where possible ensure that discharge summaries are clinically checked by a Pharmacist and their name and
contact details are clearly and unambiguously documented on the discharge summary

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 58
Medicines Use and Safety
S
P S
References:
1. National Institute for Health and Clinical Excellence (NICE). Medicines optimisation: the safe and effective use of medicines to enable the best possible
outcomes. March 2015, available at: https://www.nice.org.uk/guidance/ng5 (Accessed 28th March 2015)
2. Royal Pharmaceutical Society. Professional Standards for Hospital Pharmacy Services - Optimising Patient Outcomes from Medicines. Version 2 July 2014.
Available at http://www.rpharms.com/support-pdfs/rps---professional-standards-for-hospital-pharmacy.pdf (accessed 3rd Oct 2014).
3. World Health Organisation. The High 5s Project. Standard Operating Protocol - Assuring Medication Accuracy at Transitions in Care: Medication
Reconciliation. Available at http://www.who.int/patientsafety/implementation/solutions/high5s/h5s-sop.pdf (accessed 4th May 2015)
4. Institute for Healthcare Improvement. Medicines Reconciliation to prevent adverse drug events. Available at
http://www.ihi.org/explore/adesmedicationreconciliation/ Pages/default.aspx (accessed 3rd Jan 2015).
5. Royal Pharmaceutical Society. Keeping patients safe when they transfer between care providers – getting the medicines right. July 2011. Available at
http://www.rpharms.com/current-campaigns-pdfs/1303---rps---transfer-of-care-10pp-professional-guidance---final-final.pdf (accessed 4th Nov 2014)
6. Academy of Medical Royal Colleges. Standards for the clinical structure and content of patient records. July 2013. Available at
https://www.rcplondon.ac.uk/sites/default/files/standards-for-the-clinical-structure-and-content-of-patient-records.pdf (accessed 4th Nov 2014)
6.19 The name and contact details of the discharging Dr is clearly and unambiguous documented on the discharge
summary

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 59
Medicines Use and Safety
Chapter 4 Audit and Evaluation
This chapter aims to provide guidance and tools that allow the audit of the Medicines Reconciliation
process at both admission and at discharge. The chapter provides an overview of the principles
underpinning audit, audit standards, data collection forms for undertaking the audits and some tips on
how the audit results may be presented. Establishing and sustaining reliable Medicines Reconciliation
processes is a challenge and it is imperative to monitor performance and drive improvement through
audit and measurement.
Both the audits described within this chapter are manual retrospective audits conducted through
analysing patient medication charts, medical notes and/or other types of information sources. The
principles of the audit are equally applicable to organisations that have paper based systems or
electronic systems.
4. 1 Principles of Audit
Clinical audit is a quality improvement process that seeks to improve patient care and outcomes through
systematic review of care against explicit criteria. Where indicated changes are implemented at an
individual, team, or service level and further monitoring is used to confirm improvement in healthcare
delivery (NICE 2002). Fig 4.1 below describes the audit cycle, this chapter provides the tools to
complete the audit cycle by identifying the topic to be audited, it sets the standards for the processes
being audited, it provides the methodology and data collection tools along with tips on how the data
may be analysed and presented. The implementing change aspect of the audit cycle is for the
organisation undertaking to consider.
Fig 4.1: The Audit Cycle
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 60
Medicines Use and Safety
Registration of Audit:
It is recommended that the audit is logged and registered with the trust clinical governance/audit
department and a reference number obtained particularly for the Medicines Reconciliation on
Discharge/Discharge Summaries Audit as this will require the audit coordinator to obtain patient medical
records.
Audit Standards:
The audit standards described within this chapter were developed through a consensus approach by
the Medicines Reconciliation working group who kindly volunteered their time to contribute to the
development of this toolkit. The working group discussed local procedures and practices, reviewed
local, regional and national guidelines, policies and directives pertaining to Medicines Reconciliation.
Example of references utilised in drawing up the audit standards include: National Prescribing Centre
(NPC) Medicines Reconciliation - A Guide to Implementation, NHS England Medication Safety
Thermometer, RPS Keeping patients safe when they transfer between care providers guidelines, RPS
Professional Standards for Hospital Pharmacy Services, NHS England Patient Safety Alert: Risks
arising from breakdown and failure to act on communication during handover at the time of discharge
from secondary care and the Academy of Royal Medical Colleges Standards for the structure and
content of medical records.
Patient Confidentiality:
For the purposes of the audits considered within this chapter there should not be any need to collect
patient information that requires identification of the patient details such as name, surname, address or
date of birth and therefore such data should not be collected. The audit coordinator may wish to record
the patient’s hospital number or NHS number that allows data to match to the original patient information
however you must consider how you will ensure the confidentiality of the data.
Sampling Strategy:
The audit standards developed are reflective of the best practice standards detailed in chapter 3. It is
advised that both sets of audit standards are utilised where a comprehensive level 2 MR service is
provided. It is important that your sample contains current or recent patients as audit is about improving
current practices and processes.
Consideration should be given on the timing of the audit particularly for the Medicines Reconciliation on
Admission audit as both the day and the time may affect the results. A suggestion is to capture the
potential best possible scenario by undertaking the audit between Tuesday and Thursday afternoon
during non-school holidays. Similarly a worst case scenario could be audited such as Monday afternoon
and results be compared to observe any differences. This comparison may support any management
decisions and/or business cases for additional resources or 7 day working.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 61
Medicines Use and Safety
Sample Size:
The sample size for both audits will be largely governed by the time that is available and the number of
staff involved in the data collection. The Medicines Reconciliation on Admission audit should allow a
relatively large sample to be audited as the data collection should generally only include review of the
drug chart which should not be time intensive and the audit could be organised such that several
Pharmacists and/or Pharmacy Technicians could undertake the data collection simultaneously. The
Medicines Reconciliation on Discharge / Discharge Summaries Audit may be restricted to a smaller
sample size as the audit will involve reviewing the medical notes of patients retrospectively which may
be a time consuming activity, in addition for more reliable results it would be preferable to have one
individual undertaking the data collection.
Although for research projects it is very important that a sample size is calculated in advance so its
results are generalisable to a larger population, for the purposes of a process based clinical audit there
is no such need, however, the sample should be large enough so that senior clinicians and managers
are willing to implement changes based on the findings. As a general rule of thumb1, a sample size of
greater than 30 allows the accuracy of the final estimate to be reasonable, a sample size of 50 allows
greater confidence in the results however beyond a sample size of 100 there is little to be gained in
terms of confidence in accuracy of results with each extra piece of information that is collected.
Data Collection:
The data collection forms for both audits that have been developed can be found in appendix 1. The
design of the data collection form assumes that the results will be transferred onto a Microsoft excel
spreadsheet for data analysis.
Data Analysis:
Audit data generally comes in three different forms, ‘tick-box’, numerical or free text. The audits
described in this chapter utilise tick box and numerical data forms. In each case the aim is to establish
which standards are being met (% compliance) and which are not (% non-compliance). If a standard is
not being met it is important to identify why and how the practice and/or process can be improved to
ensure that the standard is met in the future. Within the discussion it would be important to consider if
there were other, acceptable reasons for the standard not being met.
The data being collected within this audit generally relates to yes/no options, tick-box options from a
specified list of alternatives or numerical data that is captured as a fraction. It is usual practice to add
up the number of answers recorded for each option and express the total as a raw number and as a
percentage.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 62
Medicines Use and Safety
EXAMPLE 1:
Sample size (n): 50 patients
Audit Standard: The patient’s medication regime prior to admission is clearly documented on the
appropriate section of the drug chart/medical notes/ electronic prescribing system or other
system.
Audit question: Has the patient’s medication regime prior to admission been clearly documented
on the appropriate section of the drug chart/medical notes/ electronic prescribing system or other
appropriate location?
Results: Yes = 32 and No = 18.
A good way of expressing this data is:
The patient’s medication regime prior to admission is clearly documented on the appropriate
section of the drug chart/medical notes/ electronic prescribing system or other
o Yes = (32/50, 64%)
EXAMPLE 2:
Sample size (n): 50 patients that have a total of 250 drugs prescribed between them
Audit Standard: The frequency of each prescribed medication must be clearly documented on
the discharge summary
Audit question: Is the frequency of each prescribed medication clearly documented on the
discharge summary?
Results: 235 medicines did have the frequency of dosing specified clearly whereas 15 medicines
did not
A good way of expressing this data is:
(235/250, 94%) of medicines did have their frequency of dosing clearly
The ‘n=250’ indicates the total number of medicines in the audit sample and is used to calculate
the percentages, i.e. 235/250 = 94%.
The majority if not all of the data generated within the two audits described in this chapter can be
classified as categorical data which is data that can be sorted according to non-overlapping (mutually
exclusive) categories, whereby each subject in a sample can only fit into one category. This type of
data is most commonly presented as a bar chart or a pie chart.
Consideration should be given to whether the data should be collected in a manner that allows
comparison between different hospitals (within a trust) , directorates, care areas, levels of Pharmacy
support and/or resource provided to the care area being audited etc. so that patterns in practice
between different areas/groups can be analysed. Other measures within the Medicines Reconciliation
on Discharge/Discharge Summaries Audit that may allow stratification of data and thus comparison are

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 63
Medicines Use and Safety
whether the discharge summary was screened by a Pharmacist or not, whether the discharge
prescription was electronically generated or hand written and whether a MR was conducted on
admission or not for the discharge summary generated.
Signposting to Audit Support:
Within NHS organisations there may be a specific audit team that can provide support and advice, this
team is usually located within the clinical governance team. The table below signposts readers to
resources that may support the audit process:
Table 4.1: Sources of Audit Support
Audit Resources Description of resource
The Health Quality Improvement Partnership
(HQIP) Intermediate level clinical audit training for
clinicians (Apr 2012)
http://www.hqip.org.uk/guidance-
support/intermediate-level-clinical-audit-training-
for-clinicians.html
This eLearning package is comprised of four
complimentary sessions. Covering 1-2 hours
total study time, these four elements are: 1 -
Thinking about doing clinical audit; 2 -
Identifying and collecting data; 3 - Analysing
and interpreting data; 4 - Feedback and
changing practice.
The Health Quality Improvement Partnership
(HQIP) Criteria and indicators of best practice in
clinical audit
http://www.hqip.org.uk/assets/Downloads/Criteria-
and-indicators-of-best-practice-in-clinical-audit.pdf
The purpose of this guidance is to define the
markers or indicators of good quality clinical
audit, at both national and local level,
conducted by both individuals and more
commonly, by teams.
The Royal Pharmaceutical Society provides its
members with Audit support and guidance. They
also have a useful toolkit available.
http://www.rpharms.com/support/clinical-audit.asp
The Royal Pharmaceutical Society can support
you in preparing for and conducting your clinical
audits so that you can demonstrate your
excellent services and identify areas where you
can enable real improvements.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 64
Medicines Use and Safety
S
P S
4.2 Auditing the Medicines Reconciliation Process
This section provides the tools for organisations to audit their Medicines Reconciliation processes. The section focusses on the two key areas of MR: Medicines
Reconciliation on Admission and Medicines Reconciliation on Discharge. Audit standards that can be easily measured in practice have been developed based
on the standards described in chapter 3. Instructions on how to conduct the audit is detailed and data collection tools are available in the appendices.
Audit Methodology for MR on Admission:
Guidance Notes
The audit should be carried out on wards that are designated to receive a Pharmacy service that includes level 2 MR service as routine (If all wards within
the hospital are audited, results should be broken down by ward in order to contextualise results against Pharmacy resource and patient turnover)
Trusts may choose to audit ALL of the wards/units or just a sample of wards
All patients admitted to the ward/care setting should be audited
The ward/units chosen for audit may admit planned, unplanned or a mixture of patients
If patients are primarily admitted through an admissions unit where Level 2 MR is offered it is suggested that this unit and other ward areas where patients
are transferred are audited
The audit should be carried out on all nominated wards at the same time, this will facilitate an overall picture of the extent of level 2 MR delivery at any
given point in time within the trust. Data should be collected on one day only, as a snap shot audit which could be repeated at intervals that are far enough
apart (e.g. beyond the average length of stay for the care area being audited) so that it has little risk of capturing duplicated data
Consider the day of audit to be Tuesday, Wednesday or Thursday so that it reflects optimal performance. If resources allow it would be worthwhile to audit
Monday as a comparator to observe if there are any differences in results due to possible lower staffing levels over the weekend.
It is anticipated that the audit will require the examination of the drug chart (or electronic prescribing system) and possibly clinical notes if relevant
Instructions for Carrying out the Audit
1. Review Medicines Reconciliation on admission audit standards in Table 5.1.1
2. Review Medicines Reconciliation on admission audit data collection tool (Appendix 1)
3. Print off enough Medicines Reconciliation on admission audit data collection tool forms (appendix 1) for one form per patient being audited
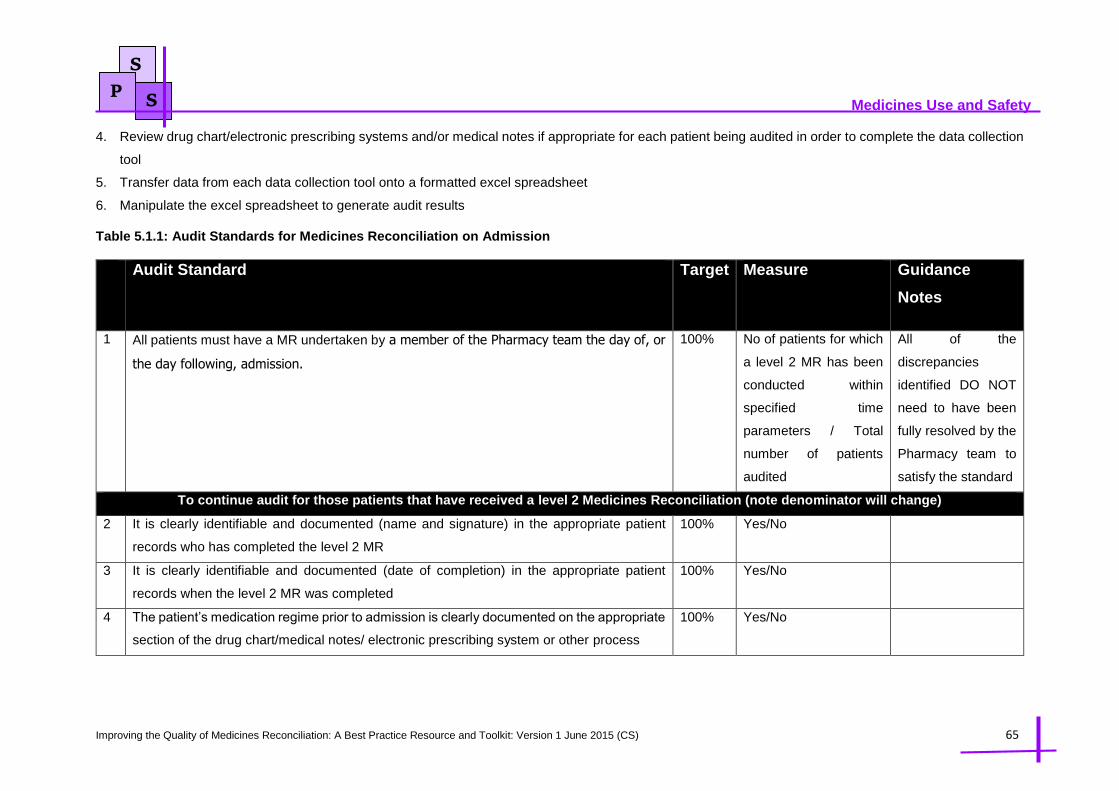
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 65
Medicines Use and Safety
S
P S
4. Review drug chart/electronic prescribing systems and/or medical notes if appropriate for each patient being audited in order to complete the data collection
tool
5. Transfer data from each data collection tool onto a formatted excel spreadsheet
6. Manipulate the excel spreadsheet to generate audit results
Table 5.1.1: Audit Standards for Medicines Reconciliation on Admission
Audit Standard Target Measure Guidance
Notes
1 All patients must have a MR undertaken by a member of the Pharmacy team the day of, or
the day following, admission.
100% No of patients for which
a level 2 MR has been
conducted within
specified time
parameters / Total
number of patients
audited
All of the
discrepancies
identified DO NOT
need to have been
fully resolved by the
Pharmacy team to
satisfy the standard
To continue audit for those patients that have received a level 2 Medicines Reconciliation (note denominator will change)
2 It is clearly identifiable and documented (name and signature) in the appropriate patient
records who has completed the level 2 MR
100% Yes/No
3 It is clearly identifiable and documented (date of completion) in the appropriate patient
records when the level 2 MR was completed
100% Yes/No
4 The patient’s medication regime prior to admission is clearly documented on the appropriate
section of the drug chart/medical notes/ electronic prescribing system or other process
100% Yes/No
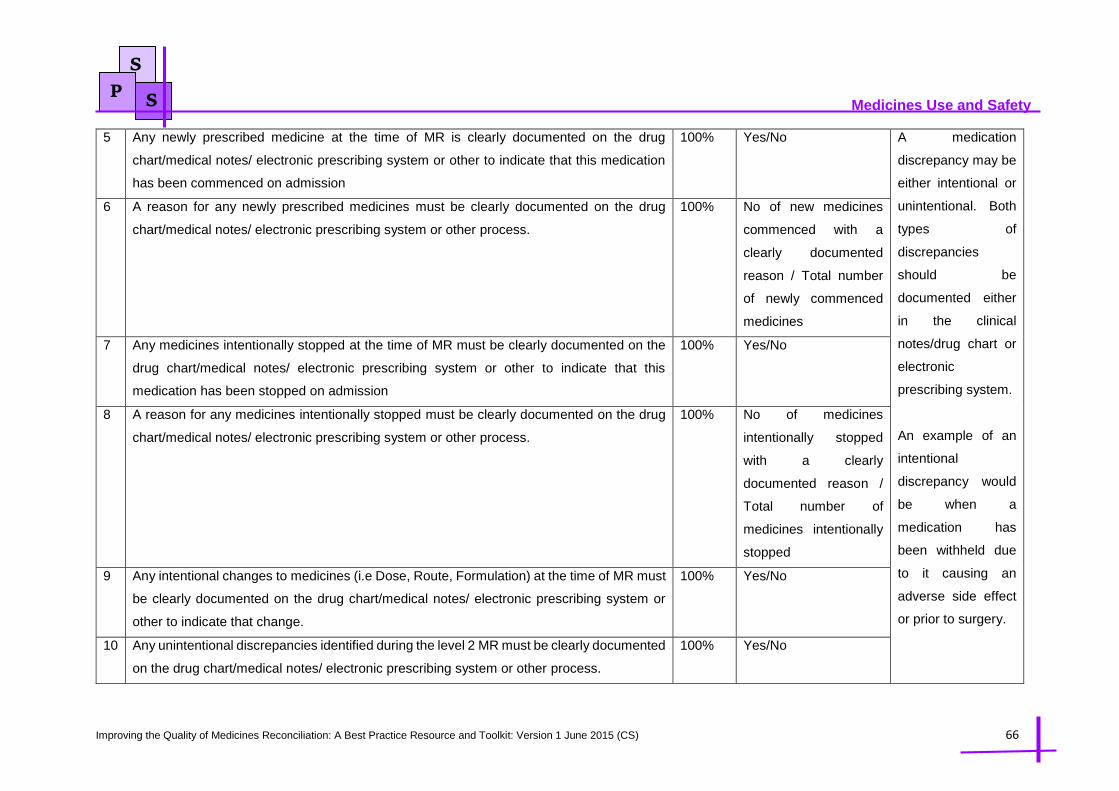
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 66
Medicines Use and Safety
S
P S
5 Any newly prescribed medicine at the time of MR is clearly documented on the drug
chart/medical notes/ electronic prescribing system or other to indicate that this medication
has been commenced on admission
100% Yes/No A medication
discrepancy may be
either intentional or
unintentional. Both
types of
discrepancies
should be
documented either
in the clinical
notes/drug chart or
electronic
prescribing system.
An example of an
intentional
discrepancy would
be when a
medication has
been withheld due
to it causing an
adverse side effect
or prior to surgery.
6 A reason for any newly prescribed medicines must be clearly documented on the drug
chart/medical notes/ electronic prescribing system or other process.
100% No of new medicines
commenced with a
clearly documented
reason / Total number
of newly commenced
medicines
7 Any medicines intentionally stopped at the time of MR must be clearly documented on the
drug chart/medical notes/ electronic prescribing system or other to indicate that this
medication has been stopped on admission
100% Yes/No
8 A reason for any medicines intentionally stopped must be clearly documented on the drug
chart/medical notes/ electronic prescribing system or other process.
100% No of medicines
intentionally stopped
with a clearly
documented reason /
Total number of
medicines intentionally
stopped
9 Any intentional changes to medicines (i.e Dose, Route, Formulation) at the time of MR must
be clearly documented on the drug chart/medical notes/ electronic prescribing system or
other to indicate that change.
100% Yes/No
10 Any unintentional discrepancies identified during the level 2 MR must be clearly documented
on the drug chart/medical notes/ electronic prescribing system or other process.
100% Yes/No

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 67
Medicines Use and Safety
S
P S
An unintentional
discrepancy is
defined as an error
or omission in the
medication history.
The medication may
have been omitted
from the list, or the
wrong drug, dose,
frequency or route
may have been
documented or
prescribed.
11 Any allergies or nil history of allergies to medicines (NKDA) must be clearly documented on
the drug chart/medical notes/ electronic prescribing system or other and include the
causative medication and brief description of reaction/outcome
100% Yes/No
12 A minimum of 2 sources of evidence must be used to confirm the MR and are documented
in the appropriate section of the drug chart/medical notes/ electronic prescribing system or
other process.
100% Yes/No
Data Collection form
breaks down sources
used to identify
prevalence of sources
used

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 68
Medicines Use and Safety
S
P S
Audit Methodology for MR on Discharge/Discharge Summaries Audit:
Guidance Notes
This is a retrospective case note quality audit in which NHS trusts review a random sample of their own discharge summaries that they have sent to the
next caregiver (General Practitioners in the majority of cases)
This type of audit is best suited to be conducted as a project by an individual who has protected time to carry out the audit. The individual in question must
have a good level of clinical knowledge, pharmaceutical skills and ability to navigate the medical notes. Pre-Registration Pharmacists under the supervision
of a Pharmacist would be appropriate candidates to conduct this audit.
When identifying patients/discharge summaries to audit, it would be prudent to exclude:
o Patients Admitted for less than 24 hours
o Planned admissions e.g Surgery, Maternity etc. (the rationale behind the exclusion is that discharge summaries for planned admissions often do
not document the patient’s regular medication, combing this data with unplanned admissions may dilute any findings)
o Deceased whilst in hospital
It may be advisable to audit particular wards (e.g High turnover of medical patients, known risks etc)
It is important to log this audit with the trust audit team and obtain a reference number. This will aid the audit coordinator in obtaining in any information
from medical records.
Instructions for Carrying out the Audit
1. Review Medicines Reconciliation on discharge/discharge summaries audit standards in Table 5.2
2. Review Medicines Reconciliation on discharge/discharge summaries audit data collection tool (Appendix 2)
3. Print off enough Medicines Reconciliation on discharge/discharge summaries audit data collection tool forms (appendix 2) for each discharge summary
being audited
4. Obtain a list (including patient details) of patients discharged from the NHS Trust over the last 3 months from the trust information, audit department or
electronic discharge system. When requesting the information ask the trust information or audit department to remember to exclude patient groups noted
above in the guidance notes

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 69
Medicines Use and Safety
S
P S
5. Number each patient on the list starting from 1. Use consecutive sampling methodology to identify patients to be audited for example choosing every 5th
patient or every 3rd patient to be audited. Consecutive sampling methodology is an example of non-probability sampling and although it is important to
remember that the sample produced may differ in character from the overall population and therefore the audit results may not be representative of the
overall care that is given it is the most practical way of selecting cases for a ‘snapshot’ sample of the population.
6. The total number of patient discharge summaries to be audited (sample size) can be calculated by the NHS Trust dependant on time and resources. As a
guide the sample size selected for a process-based clinical audit project should be large enough so that senior clinicians and managers are willing to
implement changes based on the findings. In terms of clinical audit a ‘snapshot’ sample of roughly 20-50 cases, for a process-based audit this is usually
sufficient. This will enable you to measure whether processes are being followed as per the standards set.
7. Obtain the final discharge summary sent to the next caregiver for all the patients identified. If using an electronic discharge system this should be relatively
simple, if using a paper based discharge system this will involve locating a copy of the paper discharge summary which should be available within the
Pharmacy.
8. Obtain the medical notes/drug chart/electronic system prescribing information regarding each of the patients being audited
9. Complete the data collection tool using the discharge summary, medical notes, drug chart and electronic prescribing information if applicable
10. Transfer data from each data collection tool onto the formatted excel spreadsheet available within the toolkit
11. Manipulate the excel spreadsheet to generate audit results
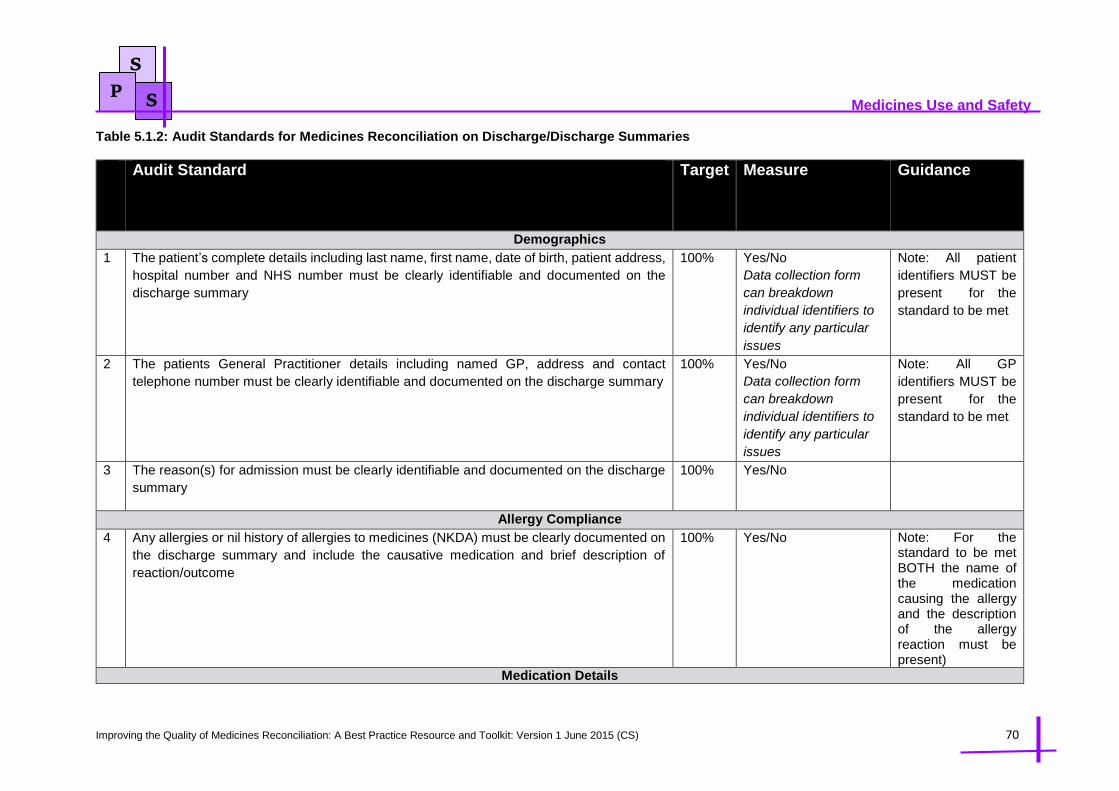
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 70
Medicines Use and Safety
S
P S
Table 5.1.2: Audit Standards for Medicines Reconciliation on Discharge/Discharge Summaries
Audit Standard Target Measure Guidance
Demographics
1 The patient’s complete details including last name, first name, date of birth, patient address,
hospital number and NHS number must be clearly identifiable and documented on the
discharge summary
100% Yes/No
Data collection form
can breakdown
individual identifiers to
identify any particular
issues
Note: All patient
identifiers MUST be
present for the
standard to be met
2 The patients General Practitioner details including named GP, address and contact
telephone number must be clearly identifiable and documented on the discharge summary
100% Yes/No
Data collection form
can breakdown
individual identifiers to
identify any particular
issues
Note: All GP
identifiers MUST be
present for the
standard to be met
3 The reason(s) for admission must be clearly identifiable and documented on the discharge
summary
100% Yes/No
Allergy Compliance
4 Any allergies or nil history of allergies to medicines (NKDA) must be clearly documented on
the discharge summary and include the causative medication and brief description of
reaction/outcome
100% Yes/No Note: For the standard to be met BOTH the name of the medication causing the allergy and the description of the allergy reaction must be present)
Medication Details

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 71
Medicines Use and Safety
S
P S
5 All prescribed medication on the discharge summary must be clearly written with its generic
name (unless not appropriate for example bioavailability issues where brand name is
acceptable)
100% Number of medicines
prescribed
appropriately as
generic / Total number
of medicines
prescribed
The denominator for
all of these
standards is should
remain the same i.e
the total number of
medicines
prescribed on the
discharge summary
6 All prescribed medication on the discharge summary must have a clear indication
documented for its use e.g. Oxybutynin 5mg M/R Tablets PO OD for Urinary Incontinence
100% Number of medicines
prescribed with
indication / Total
number of medicines
prescribed
7 The dose of each prescribed medication on the discharge summary must be clearly written
in the correct units e.g Oxybutynin 5mg M/R Tablets PO OD for Urinary Incontinence
100% Number of medicines
prescribed with clear
and correct dose
instructions / Total
number of medicines
prescribed
8 The frequency of each prescribed medication must be clearly documented on the discharge
summary e.g Oxybutynin 5mg M/R Tablets PO OD for Urinary Incontinence
100% Number of medicines
prescribed with clear
and correct dosing
frequency instructions /
Total number of
medicines prescribed
9 The route of administration of each prescribed must be clearly documented on the
discharge summary e.g Oxybutynin 5mg M/R Tablets PO OD for Urinary Incontinence
100% Number of medicines
prescribed with clear
and correct route of
administration
instructions / Total
number of medicines
prescribed
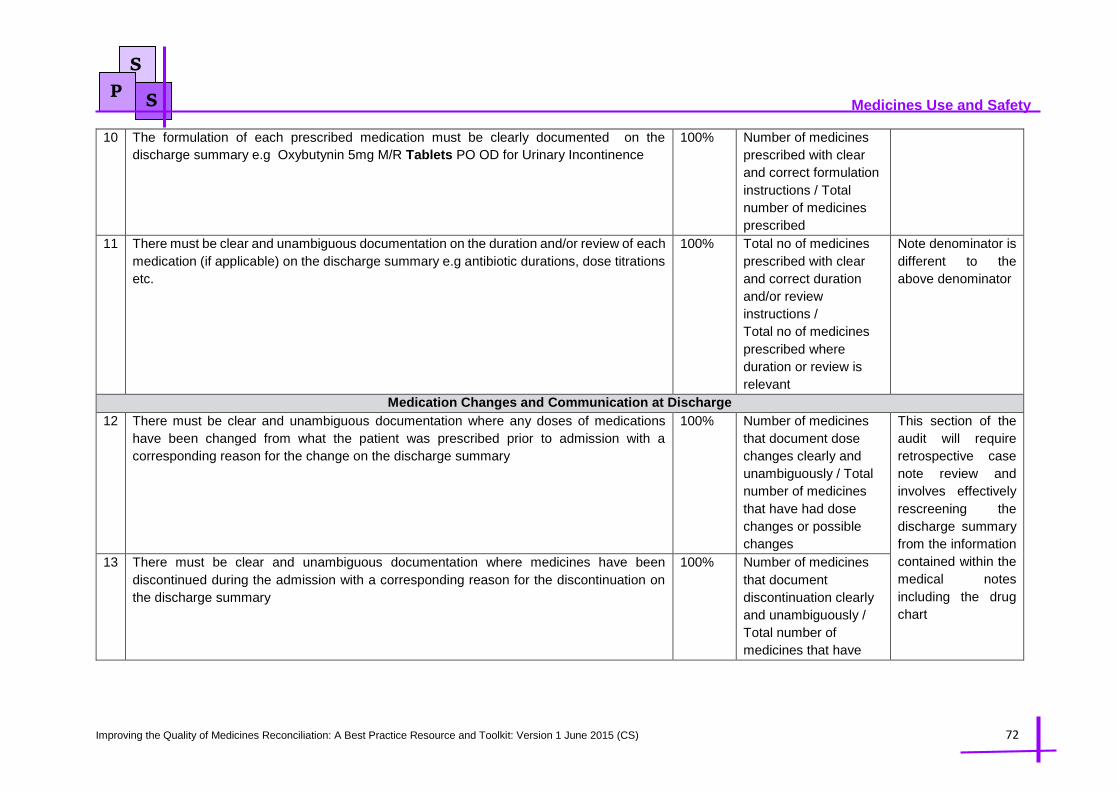
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 72
Medicines Use and Safety
S
P S
10 The formulation of each prescribed medication must be clearly documented on the
discharge summary e.g Oxybutynin 5mg M/R Tablets PO OD for Urinary Incontinence
100% Number of medicines
prescribed with clear
and correct formulation
instructions / Total
number of medicines
prescribed
11 There must be clear and unambiguous documentation on the duration and/or review of each
medication (if applicable) on the discharge summary e.g antibiotic durations, dose titrations
etc.
100% Total no of medicines
prescribed with clear
and correct duration
and/or review
instructions /
Total no of medicines
prescribed where
duration or review is
relevant
Note denominator is
different to the
above denominator
Medication Changes and Communication at Discharge
12 There must be clear and unambiguous documentation where any doses of medications
have been changed from what the patient was prescribed prior to admission with a
corresponding reason for the change on the discharge summary
100% Number of medicines
that document dose
changes clearly and
unambiguously / Total
number of medicines
that have had dose
changes or possible
changes
This section of the
audit will require
retrospective case
note review and
involves effectively
rescreening the
discharge summary
from the information
contained within the
medical notes
including the drug
chart
13 There must be clear and unambiguous documentation where medicines have been
discontinued during the admission with a corresponding reason for the discontinuation on
the discharge summary
100% Number of medicines
that document
discontinuation clearly
and unambiguously /
Total number of
medicines that have
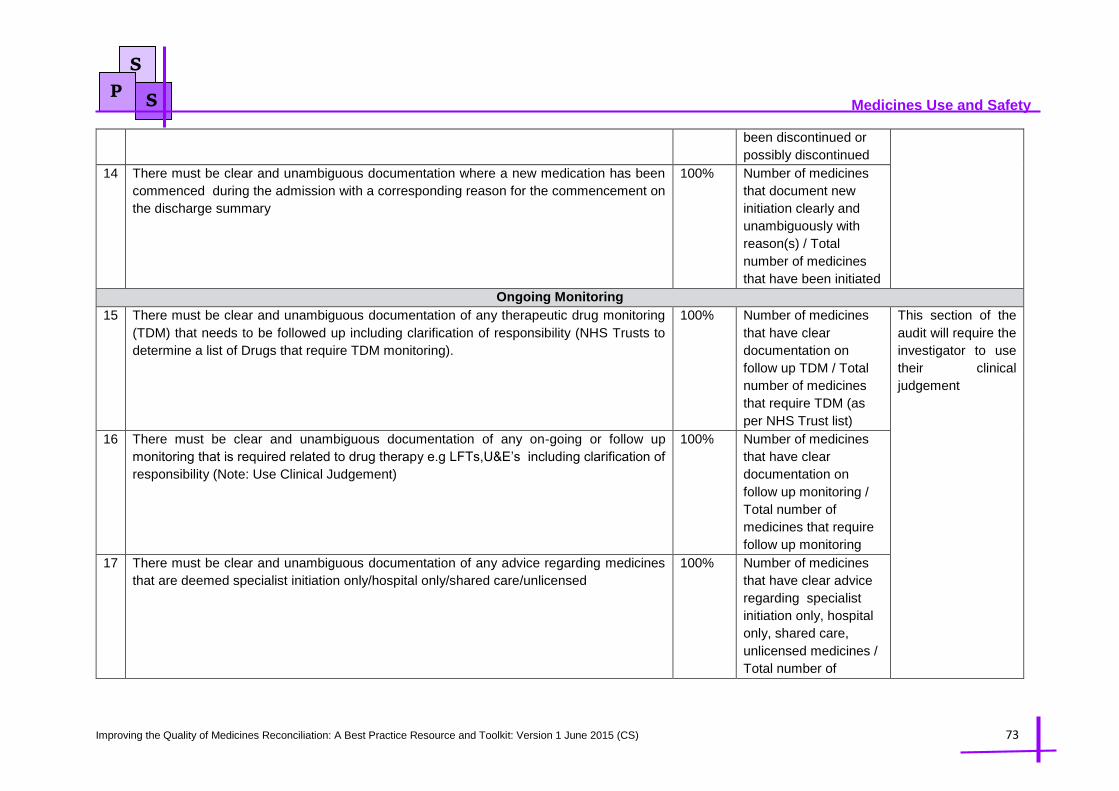
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 73
Medicines Use and Safety
S
P S
been discontinued or
possibly discontinued
14 There must be clear and unambiguous documentation where a new medication has been
commenced during the admission with a corresponding reason for the commencement on
the discharge summary
100% Number of medicines
that document new
initiation clearly and
unambiguously with
reason(s) / Total
number of medicines
that have been initiated
Ongoing Monitoring
15 There must be clear and unambiguous documentation of any therapeutic drug monitoring
(TDM) that needs to be followed up including clarification of responsibility (NHS Trusts to
determine a list of Drugs that require TDM monitoring).
100% Number of medicines
that have clear
documentation on
follow up TDM / Total
number of medicines
that require TDM (as
per NHS Trust list)
This section of the
audit will require the
investigator to use
their clinical
judgement
16 There must be clear and unambiguous documentation of any on-going or follow up
monitoring that is required related to drug therapy e.g LFTs,U&E’s including clarification of
responsibility (Note: Use Clinical Judgement)
100% Number of medicines
that have clear
documentation on
follow up monitoring /
Total number of
medicines that require
follow up monitoring
17 There must be clear and unambiguous documentation of any advice regarding medicines
that are deemed specialist initiation only/hospital only/shared care/unlicensed
100% Number of medicines
that have clear advice
regarding specialist
initiation only, hospital
only, shared care,
unlicensed medicines /
Total number of

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 74
Medicines Use and Safety
S
P S
medicines that are
designated specialist
initiation only, hospital
only, shared care,
unlicensed medicines
Contact Details and Stratification
18 Was the discharge summary clinically screened by the Pharmacist? N/A Yes / No Allows stratification
of results into
Pharmacy screened
TTAs and Non
Pharmacy screened
TTAs
19 If Yes, there must be clear and unambiguous documentation of the name and contact
details of the screening Pharmacist on the discharge summary
100% Yes / No
20 There must be clear and unambiguous documentation of the name and contact details of
the discharging Dr on the discharge summary
100% Yes / No
21 Was the Discharge Summary Electronic or Hand written N/A Electronic / Hand
written
Allows stratification
of results into
electronic or
handwritten
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 75
Medicines Use and Safety
Case Study for MR on Discharge /Discharge Summaries Audit
The Medicines Reconciliation on Discharge/Discharge Summaries Audit Standards was piloted at
Ealing Hospital in West London and Oxford University Hospitals simultaneously to validate the audit
methodology.
Both sites were able to conduct the audit with relative ease, Oxford University Hospitals have an
electronic prescribing system which made data retrieval somewhat easier and reduced the need to
refer back to the medical notes.
The audit investigator at Ealing Hospital kept contemporaneous notes on how they conducted the
audit in a step by step manner, this contemporaneous account may support other audit investigators
when conducting the audit and can be viewed via
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/Cont
amperaneous%20Audit%20Methodology_May%2015.pdf.
At Ealing Hospital the audit results were used as a tool to generate discussion within a focus group
that was set up to improve the quality of Pharmacist TTA screening.
Both audit investigators are happy to be contacted for further information on how they conducted the
pilot audit.
Reena Devit at Ealing Hospital on [email protected]
Cate Leon at Oxford University Hospitals on [email protected]
References and Acknowledgements:
1. Wright D. NHS East of England Audit Package. Version 1 2009
2. University Hospital Bristol NHS Foundation Trust. Clinical Audit - How to Guide? Available at
http://www.uhbristol.nhs.uk/for-clinicians/clinicalaudit/ (Accessed 27th Feb 2015)
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 76
Medicines Use and Safety
Chapter 5 Education, Training and Competency
The NICE Medicines Optimisation Guidance: the safe and effective use of medicines to enable the best
possible outcomes published in March 2015 states that organisations should ensure that Medicines
Reconciliation is carried out by a trained and competent health professional – ideally a Pharmacist,
Pharmacy technician, Nurse or Doctor – with the necessary knowledge, skills and expertise including:
effective communication skills, technical knowledge of processes for managing medicines and
therapeutic knowledge of medicines use. In support of the above guidance this chapter aims to set out
the necessary competencies required to undertake Medicines Reconciliation whilst also signposting to
a variety of educational and training resources that support the development of staff to obtain the
necessary knowledge, skills and competencies to undertake MR.
5.1 Key Competencies for Staff Conducting Medicines Reconciliation
This section shares the key competencies that staff must develop and possess when conducting
Medicines Reconciliation. The competencies are applicable to all Pharmacy staff (Pharmacists,
Pharmacy Technicians and Pre-Registration Pharmacists) and should also be used with Nursing,
Medical or any other staff involved in carrying out Medicines Reconciliation. The competencies and
their behaviours are drawn from three national documents; The Royal Pharmaceutical Society
Foundation Pharmacy Framework, The Foundation Pharmacy Framework for Pharmacy Technicians
developed by the Association of Pharmacy Technicians UK and the Nationally Recognised Competency
Framework for Pharmacy Technicians: Competency Behaviours developed by NHS Pharmacy
Education & Development Committee. The frameworks should be viewed individually and in their
entirety to ensure that practitioners are competent in the all of the underpinning skills and competencies
that are essential for them to deliver any medicines management activity including Medicines
Reconciliation.
Table 5.1.1 below displays these competency frameworks in more detail with links to the full documents.
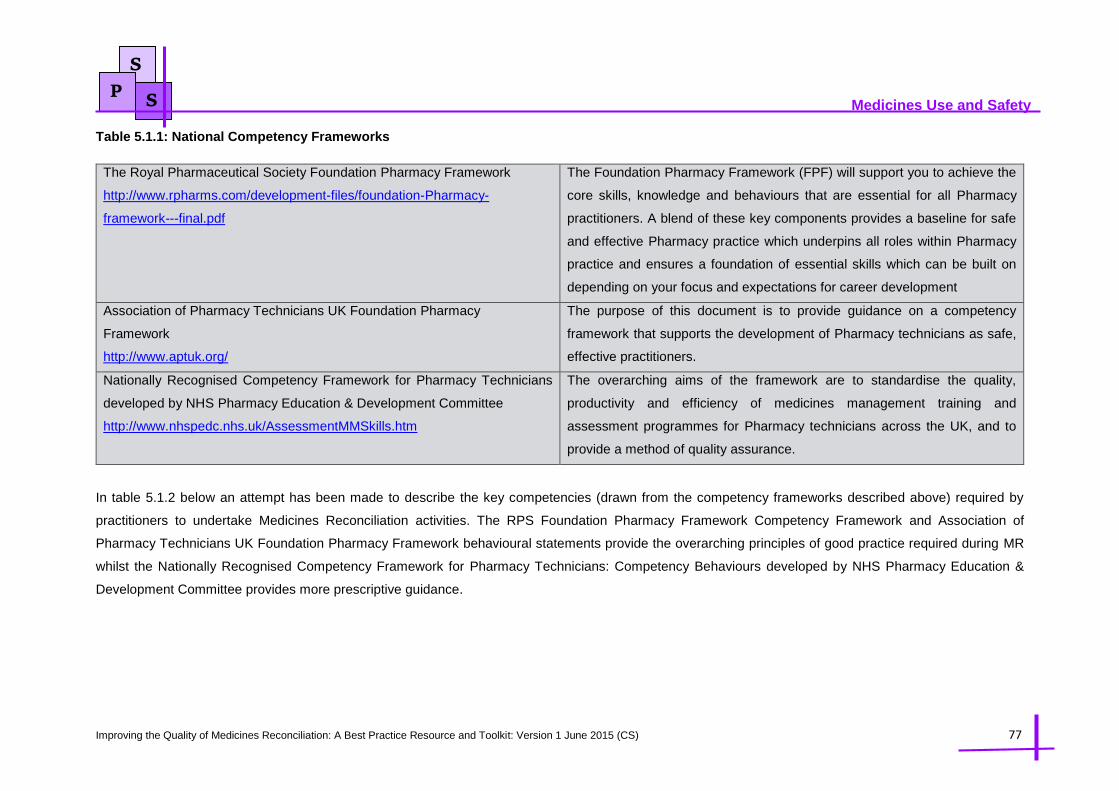
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 77
Medicines Use and Safety
S
P S
Table 5.1.1: National Competency Frameworks
The Royal Pharmaceutical Society Foundation Pharmacy Framework
http://www.rpharms.com/development-files/foundation-Pharmacy-
framework---final.pdf
The Foundation Pharmacy Framework (FPF) will support you to achieve the
core skills, knowledge and behaviours that are essential for all Pharmacy
practitioners. A blend of these key components provides a baseline for safe
and effective Pharmacy practice which underpins all roles within Pharmacy
practice and ensures a foundation of essential skills which can be built on
depending on your focus and expectations for career development
Association of Pharmacy Technicians UK Foundation Pharmacy
Framework
http://www.aptuk.org/
The purpose of this document is to provide guidance on a competency
framework that supports the development of Pharmacy technicians as safe,
effective practitioners.
Nationally Recognised Competency Framework for Pharmacy Technicians
developed by NHS Pharmacy Education & Development Committee
http://www.nhspedc.nhs.uk/AssessmentMMSkills.htm
The overarching aims of the framework are to standardise the quality,
productivity and efficiency of medicines management training and
assessment programmes for Pharmacy technicians across the UK, and to
provide a method of quality assurance.
In table 5.1.2 below an attempt has been made to describe the key competencies (drawn from the competency frameworks described above) required by
practitioners to undertake Medicines Reconciliation activities. The RPS Foundation Pharmacy Framework Competency Framework and Association of
Pharmacy Technicians UK Foundation Pharmacy Framework behavioural statements provide the overarching principles of good practice required during MR
whilst the Nationally Recognised Competency Framework for Pharmacy Technicians: Competency Behaviours developed by NHS Pharmacy Education &
Development Committee provides more prescriptive guidance.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 78
Medicines Use and Safety
S
P S
Table 5.1.2: Key Competencies Required for Staff Conducting Medicines Reconciliation
The RPS Pharmacy Foundation Framework Competency Behaviours and Association of
Pharmacy Technicians UK Foundation Pharmacy Framework
Nationally Recognised Competency
Framework for Pharmacy Technicians:
Competency Behaviours
Consultation and Communication Skills
1.1 Satisfactorily obtains patient consent if appropriate
Obtain valid consent from the patient (or
carer) in accordance with the organisation’s
procedures
Take appropriate actions if consent is not
obtained, not available or declined, in
accordance with organisation’s procedures
1.1 Uses appropriate questioning to obtain all relevant information from the patient
Record the individual’s social habits where
applicable
1.1 Documents consultations where appropriate in the patient’s records
Where applicable, in accordance with
legislation and the organisation’s
procedures relevant to writing in patients’
medical notes
2.3 Communicates clearly, precisely and appropriately with:
- Patient and carer
- Health care professionals
- Others
Introduce self to the patient and explain the
intention of the consultation
Information Gathering and Documentation
1.2 Retrieves relevant or available information
Identify the information needed when
obtaining a medication history
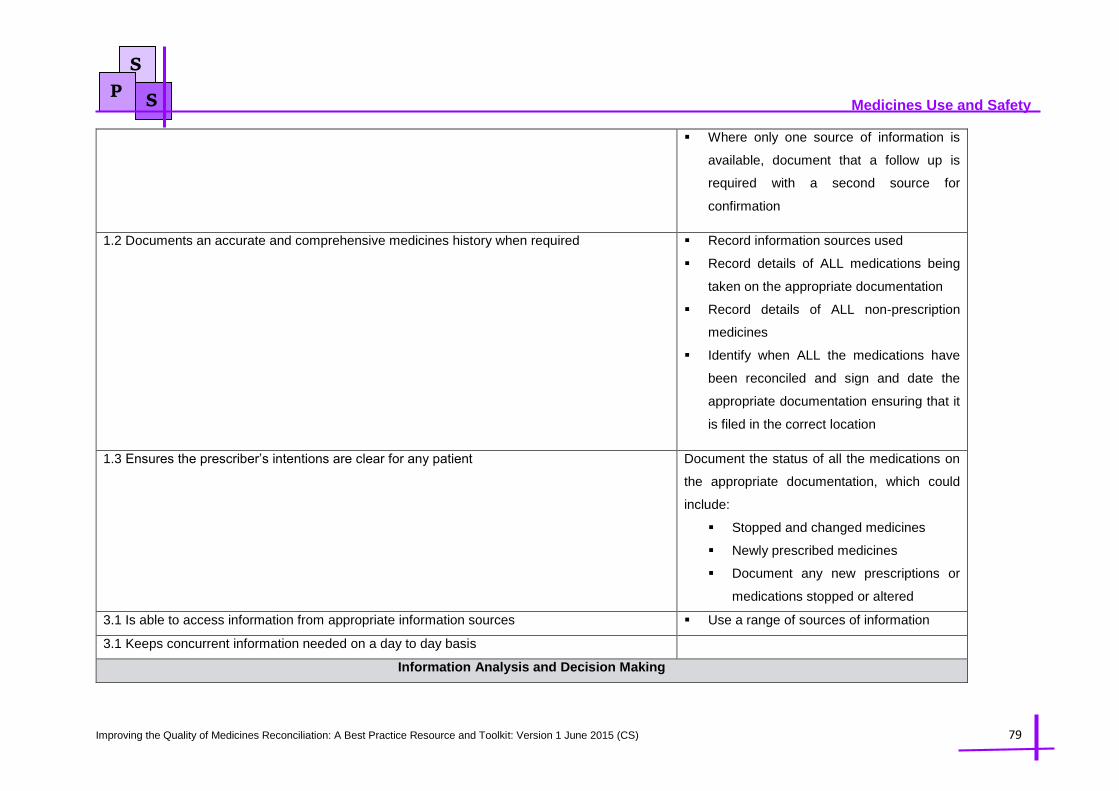
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 79
Medicines Use and Safety
S
P S
Where only one source of information is
available, document that a follow up is
required with a second source for
confirmation
1.2 Documents an accurate and comprehensive medicines history when required
Record information sources used
Record details of ALL medications being
taken on the appropriate documentation
Record details of ALL non-prescription
medicines
Identify when ALL the medications have
been reconciled and sign and date the
appropriate documentation ensuring that it
is filed in the correct location
1.3 Ensures the prescriber’s intentions are clear for any patient
Document the status of all the medications on
the appropriate documentation, which could
include:
Stopped and changed medicines
Newly prescribed medicines
Document any new prescriptions or
medications stopped or altered
3.1 Is able to access information from appropriate information sources Use a range of sources of information
3.1 Keeps concurrent information needed on a day to day basis
Information Analysis and Decision Making

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 80
Medicines Use and Safety
S
P S
3.3 Is able to analyse and synthesise key elements from information gathered
Identify and document any medication
related problems that the patient may have
Compare the verified medication history
obtained with the most recent valid
prescription or documentation available
Identify and document discrepancies
between the accurate medication history
and the medicines prescribed on the
current medication record
Record details of any discrepancies
Sign and date the relevant documentation
and ensure that it is filed in the appropriate
location
3.3 Demonstrates a logical process to problem solving
Take appropriate action if discrepancies
are found between the sources
Recognise the limitations of a single
source and the reasons for always
checking with a further source
Confirm whether the identified changes or
omissions have been made intentionally
Liaise with the appropriate people to
resolve clinical queries and
unexplained/unintentional changes
3.3 Demonstrates clear decision making
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 81
Medicines Use and Safety
S
P S
3.5 Ensures resolution of problem
Document the outcome of the resolution of
any queries
In order to ensure that the skills, knowledge and competencies possessed to undertake MR activities are kept up to date organisations and practitioners may
wish to utilise work based assessment tools such as the Mini Clinical Evaluation Exercise (Mini –CEX) and Medicines Related Consultation Framework (MRCF)
which enable practitioners with the support of a senior colleague or peer to evaluate their own performance with a real patient and have real t ime feedback.
These tools are utilised within the RPS Foundation School Pharmacy Postgraduate Courses and are relatively easy to use. For the tools themselves and
information on how to use them please see the JPB website http://www.jpbsoutheast.org/assessment-tools/. It is acknowledged that Pharmacy technicians that
have completed nationally approved medicines management training and assessment programme are required to undergo a reaccreditation process every 2
years.
5.2 Collation of Education and Training Materials Supporting the Medicines Reconciliation Process
The need for a wide range of people to be trained to deliver Medicines Reconciliation has increased as a result of the increasing national focus on the risks
during transfer of care of patients in all care sectors and the increase in the development of care pathways that deliver care closer to home which may not
always have a dedicated clinical Pharmacy service.
Table 5.2 signposts the reader to a variety of training programmes, training frameworks and educational materials that support the delivery of Medicines
Reconciliation. It also provides an opportunity for organisations/departments/individuals to review their current training provision and compare it to other
examples to ensure that what is provided locally is suitable. Table 5.2 has been divided such that resources are categorised into: A) Nationally available training
and B) Regionally developed training.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 82
Medicines Use and Safety
S
P S
Table 5.2: Collation of National and Regional Education and Training Materials Supporting the Medicines Reconciliation Process
Section A: National MR training programmes and resources
Training Provider Description of Resource
Centre for Pharmacy
Postgraduate Education (CPPE)
https://www.cppe.ac.uk/programm
es/l/medsrecon-h-01/
Training Resource: Learning at Lunch Module: Medicines Reconciliation (Reviewed 2014)
This learning resource is a Level 1 Learning at Lunch Module aimed at pre-registration and registered Pharmacists and
Pharmacy technicians.
Overview: The purpose of this programme is to support Pharmacists and Pharmacy technicians in taking a structured approach
to reconciling medicines for patients in the acute setting. It focuses on the reconciliation of medicines within 24 hours for patients
who are admitted to acute (and mental health) trusts, as required by NICE guidance. It may be used to complement local training
on Medicines Reconciliation within acute trusts.
The programme involves about four hours of study and has a format where participants complete an initial pre-session workbook
(Booklet 1) followed by an on-site workshop. The lunchtime facilitated session involves looking at the case studies in more detail
with questions for participants to work through (Booklet 2). There are suggested answers and also some suggestions for further
practice-based activities.
Complementary resources for running the case studies - a number of sources for drug histories, for example - are being made
available for facilitators to download from the website.
There is no e-assessment for the programme.
Cost: Free for registered and pre-registration Pharmacists and Pharmacy technicians

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 83
Medicines Use and Safety
S
P S
East and South East England
Specialist Pharmacy Services
(MUS Division)
www.nelm.nhs.uk/en/Communit
ies/NeLM/SPS-E-and-SE-
England/Meds-use-and-safety/
Training Resource: A Training Package to support the delivery of Level 2 Medicines Reconciliation by Pharmacy Staff (2009)
Overview: This package is intended to support education and training leads to develop on-site training as well as individual
practitioners in acquiring the knowledge and skills to deliver MR effectively. It is linked to the template MR policy and outcomes
from a MR survey both of which are available on the same web-site. The contents provide a series of learning outcomes needed
to deliver MR. The sections that follow provide information, questions and case scenarios and signposts users to relevant resources
to meet these learning outcomes. Advice is given about how to add in assessments for knowledge and competency. The learning
outcomes are mapped to the General Level Competency Framework (GLF) and the Framework for Pharmacy Technicians (web-
link to CoDEG) which are the previous versions of the RPS Foundation Pharmacy Framework and the Foundation Pharmacy
Framework for Pharmacy Technicians. The package was developed in collaboration with the regional NHS Pharmacy education
and training organisations within the SPS service area.
Cost: Free
NHS Pharmacy and Education
Development Committee
http://www.nhspedc.nhs.uk/
Training Resource: Nationally Recognised Competency Framework for Pharmacy Technicians: The Assessment of Medicines
Management Skills
Overview: The development of this framework was commissioned by the NHS Pharmacy Education and Development
Committee (PEDC) in response to the Department of Health White Paper ‘Equity & Excellence, Liberating the NHS’ and the
Quality, Innovation, Productivity and Prevention (QIPP) agenda. The framework has been developed by a Working Group that
includes medicines management Pharmacy technician specialists and education and development specialists representing all
regions within the United Kingdom.
This framework is intended to be used by training providers who:
Plan to develop medicines management training and assessment programmes for Pharmacy technicians
Currently deliver medicines management programmes and wish to assess the quality of their programmes against a
nationally recognised standard
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 84
Medicines Use and Safety
S
P S
This framework focuses on three aspects of the Pharmacy technician medicines management role and has been developed into
three modules, each following the same format:
The supply of medicines to individual patients
The assessment of Patients’ Own Drugs
Medicines Reconciliation
The framework also describes the underpinning skills that are connected to and interwoven throughout each of the three
modules enabling the medicines management role to be carried out to its full potential and to promote quality of care and patient
safety.
The Medicines Reconciliation module describes learning outcomes, against which competency can be assessed for Pharmacy
technicians undertaking Medicines Reconciliation within the relevant care setting. It also encompasses the identification of
discrepancies and issues that may arise as part of the process and dealing with these in an appropriate manner. A knowledge
and competency-based approach to assessment is recommended and advice is provided about what should be assessed.
Section B: Regional Training Programmes
Training Provider Description of Resource
South West Medicines
Information / Commercial and
Academic Services (CoAcS)
Training Resource: Medicines Reconciliation Training Programme
Overview: The South West Medicines Information and Training / CoAcS system delivers an online programme covering the
process of Medicines Reconciliation and prepares learners with the skills and knowledge necessary to enter into a more detailed
training programme. The learning material comprises four modules which learners have to complete sequentially, taking them

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 85
Medicines Use and Safety
S
P S
SWMiT Website:
http://www.swmit.nhs.uk/TechMed
Man.htm
E Learning Webpage:
http://www.medicinesreconciliatio
n.com/
through the introductory basics, medication history taking, verifying this history (level 1) and reconciling medications prescribed
on admission (level 2).
An assessment system tests learners’ knowledge of both levels in order. Once level one is complete and a certificate issued,
level two assessment becomes accessible. As proof that the learner has demonstrated a suitable level of competence, a
certificate can be printed after passing each assessment. In addition, a reflective diary log is available for each learner to record
their learning experiences.
The activity of each learner is monitored by an assessor who is assigned a number of learners at the same institution. Assessors
can grant or deny access to each learner in their group and authorise the awarding of certificates after evaluating the learners
answers in the level 1 and 2 assessments. They can also give feedback to comments made in learners reflective diary logs.
Assessors are chosen by Organisational leads, of which there is usually only one in each organisation. Leads have substantial
administrative control and have the ability to grant site access to both learners and assessors and assign the latter their
respective groups of learners. Leads can designate authority to capable assessors and need only concern themselves with the
system operation rather than individual assessment.
Cost: One-year subscription for the package: Site Licence £300 + VAT allows 50 users (excluding assessors and organisational
leads)
NHS PE+D (NHS Pharmacy
Education and Development)
Contact: Melanie Boughen:
[email protected] . To
discuss how a Trust uses this
programme contact June Smart at
the West Suffolk Hospital at
Training Resource: Medicines Reconciliation Training Scheme for Pharmacy Staff
Overview: This training scheme has been adapted from a training package originally developed by a partnership between the
Clinical Directorate and E & T Specialists from the East and South East England Specialist Pharmacy Services. The scheme
uses a local trainer (who attends a regional session to support them in delivering the training) and overall programme facilitator
(who attends a regional session for this role). The scheme is aimed at Pharmacists, Pre-registration Trainee Pharmacists and
Pharmacy Technicians who are new to the role and have never received formal training in Drug History Taking, Medicines
Management or Clinical Service and where Medicines Reconciliation is a requirement of their job role

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 86
Medicines Use and Safety
S
P S
Web-site:
http://www.nhsped.uea.ac.uk/
Direct Link to Training:
http://www.nhsped.uea.ac.uk/Phar
macy-technicians/accredited-
medicines-reconciliation/
The Training Scheme consists of two modules with separate learning outcomes that are mapped to the KSF, General Level
Framework, GPhC Registration trainee framework and the Framework for Pharmacy Technicians :
Module 1 – Drug History Taking
– Medicines Reconciliation
Both modules are supported by in-house or regional study days to provide the underpinning knowledge required.
Assessment is both knowledge and competency based. The knowledge is assessed via completion of a questionnaire.
Outcomes from this identify knowledge gaps that can be filled by attending in-house or regional study sessions.
The competency assessment framework is similar for the two modules. It involves observed completion of 10 Drug Histories and
10 MRs with OSCEs available should essential criteria not be covered by the in-practice observed activity.
A portfolio is also completed to document the observed practices that have been undertaken, ensure that a breadth of
experience has been covered and highlight areas where further training is required using reflective practice.
Health Education Kent Surrey
Sussex; Pharmacy Education
Website:
www.kssPharmacy.nhs.uk
Contact: lauramcewen-
discuss how a Trust uses this
programme contact Julie Bole
Training Resource: National Medicines Management Accreditation
Overview: This programme has been developed to support and enhance the delivery of medicines management across the
NHS and in particular the roles of Pharmacy technicians contributing to this agenda. This is a nationally recognised accreditation
and as such will be transferable throughout the United Kingdom. HE KSS recognise that delivery in individual work bases is
diverse; this programme does not attempt to prescribe one single model for the delivery of medicines management. Neither does
it aim to be a clinical knowledge course.
This programme is recommended for Pharmacy Technicians registered with the General Pharmaceutical Council. However, HE
KSS Pharmacy will accept applications from any NVQ2 (or above) qualified Healthcare Professional, depending on the relevance

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 87
Medicines Use and Safety
S
P S
(Western Sussex Hospitals NHS
Trust) [email protected]
to their job role and if supported or nominated by their Trust. Trusts within HE KSS use the course framework as a basis for their
pre-registration Pharmacist MR training.
The training programme combines practice activities, portfolio requirements, practice-based assessments and a summative
OSCE assessment to provide knowledge and competency-based accreditation scheme. The programme also enables trainers to
be accredited to deliver the programme locally. The training is delivered through three modules and the scheme offers Trusts
and candidates a choice in the modules of the Accreditation that they want to complete depending on how relevant the
module is to their job role:
Module 1 – Patient’s Own Drugs (PODs) and Medicines Supply
Module 2 – Medicines Reconciliation
Module 3 – Device Counselling
Cost: KSS Pharmacy training is funded for all staff in Kent, Surrey, East and West Sussex, Hampshire and the Isle of Wight from
NHS Hospitals, NHS Community Trusts Mental Health Trusts and prisons. For all private organisations or NHS staff outside the
KSS and H&IOW region, the cost of this Accreditation is £400. Please visit HEKSS Terms and Conditions page for further
information.
5.3 Local Examples of MR Education and Training
The table below details local examples of training approaches that have been shared by NHS organisations on how they deliver their education, training and
competency assurance with respect to MR.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 88
Medicines Use and Safety
S
P S
Table 5.3: Collation of Local Education and Training Materials Supporting the Medicines Reconciliation Process
Organisation: Northwick Park Hospital
Key Contact: Fiona Turnbull on [email protected] or Mira Jivraj on [email protected]
Junior Doctors Training:
At Northwick Park Hospital clinical Pharmacists carry out training for junior doctors (FY1s) on Medicines Reconciliation annually as part of the FY1 training
program. The one hour mandatory teaching session for FY1 junior doctors is delivered within their first two months at the Trust. This is delivered using
PowerPoint slides and handouts and is combined with brief training on writing TTAs. The presentation covers the types of sources that can be used for
Medicines Reconciliation with advantages and disadvantages. The slides include real examples of sources and ask the doctors to identify the limitations and
include examples of errors that have happened at the Trust. The presentation also includes information on how to document changes made to medication in
hospital.
A Medicines Reconciliation scenario is included in the FY1 prescribing assessment. The assessment is passed if the answer is deemed clinically safe.
Feedback is given verbally during a training session and on an individual feedback form.
Pre-Registration Pharmacists Training:
Clinical Pharmacists carry out training for pre-registration Pharmacists. This includes reading the Medicines Reconciliation policy and observing a clinical
Pharmacist carrying out at least five medicine reconciliations. The pre-registration Pharmacist is then observed and assessed carrying out a minimum of
three Medicines Reconciliations before being signed as competent to complete Medicines Reconciliation without direct observation. Following on from this
they will be asked to complete a further 10 Medicines Reconciliations to gain exposure to different types of patients. If any of the Medicines Reconciliations
are not satisfactory the pre-registration Pharmacist will have to repeat the assessments until the supervising Pharmacist is confident to sign them off. Pre-
registration Pharmacists have a specific clinical training program that includes Medicines Reconciliation.
Newly Employed Pharmacists:
Newly employed Pharmacists are requested to read the Medicines Reconciliation policy, complete the clinical induction pack which includes a section on
Medicines Reconciliation and carry out a ward based Medicines Reconciliation accreditation assessment as part of their departmental induction. The newly

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 89
Medicines Use and Safety
S
P S
employed Pharmacist is requested to undertake a ward based assessment of their clinical Pharmacy skills by one of the senior Pharmacists. Assessment
takes place in the form of the clinical induction pack which includes a series of questions based on the Medicines Reconciliation process. In addition the
newly employed Pharmacist must observe a Pharmacist undertaking 3 Medicines Reconciliation and then themselves must be observed undertaking 3
Medicines Reconciliations to be signed off as competent.
Substantive Pharmacy Staff:
A comprehensive training session is delivered to the entire Pharmacy department every 1-2 years. There is currently no assessment or reaccreditation that
takes place.
Medicines Management Technicians
Medicines Management Technicians (MMT) need to complete an accreditation programme if they undertake Medicines Reconciliations as part of their role.
MMTs who have not previously carried out Medicines Reconciliations are required to complete either an in-house training programme or the London
Pharmacy Education and Training (LPET) AIMM course. Newly employed MMTs with prior experience can complete a fast-track accreditation programme.
Ongoing assessment following accreditation takes place in the form of 6 monthly accompanied ward visits where at least 1 MR is observed each time
In-house training and accreditation
Read MR policy
Candidate observes 10 MR
Candidate is observed completing at least 10 MR receiving feed back
Complete questions and answers in MR accreditation pack
Successfully pass 6 assessed Meds Rec
After accredited has 6 monthly accompanied ward visit
Fast tracked training and accreditation (when employing new staff accredited elsewhere)

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 90
Medicines Use and Safety
S
P S
Read MR policy
Candidate observes 5 MR
Candidate is observed completing at least 2 MR receiving feed back
Complete questions and answers in MR accreditation pack
Successfully pass 3 assessed Meds Rec
After accredited has 6 monthly accompanied ward visit
Resources
Junior Drs Training Resources
Tips for conducting Medicines Reconciliation Junior Drs:
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/Medicines%20Reconciliation%20Junior%20Dr%20Training_
May%2015.pdf
Junior Dr MR Training Slides:
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/Medicines%20Reconciliation%20Junior%20Dr%20Training_
May%2015.pdf
Newly Employed Pharmacists Resources
Accreditation for newly started Pharmacists training programme:
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/Accreditation%20for%20newly%20started%20pharmacists%
20training%20programme_Nov%2013.pdf
Substantive Pharmacy Staff Resources
Pharmacy Department CPD Medicines Reconciliation Presentation:

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 91
Medicines Use and Safety
S
P S
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/Pharmacy%20Departent%20CPD%20Medicines%20Reconci
liation%20Presentation_May%2015.pdf
Medicines Management Technician Training Resources
MMT MR Accreditation Programme:
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/MMT%20MR%20Accreditation%20Programme_Aug%2014.p
df
Fast-tracked accreditation programme for experienced technicians undertaking Medicines Reconciliation:
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/Fast-
tracked%20accreditation%20for%20experienced%20technicians%20already%20carrying%20out%20medicines%20reconciliation_May%2011.pdf
MMT MR Accreditation Checklist:
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/MMT%20MR%20Accreditation%20Checklist_Aug%2014.pdf
Organisation: Lewisham and Greenwich NHS Trust
Key Contact: Richard Pudney on [email protected]
Overview: The programme supports the development of the underpinning knowledge and practical skills to deliver Level 2 Medicines Reconciliation and
includes a competency assessment for pre-registration Pharmacists. The key elements of the programme are delivered over a 4 week period using the
following materials:
Trainee and trainer documents. These provide case scenarios and the information to complete the competency assessments as well as underpinning
knowledge and skills.
A group session lesson plan to support completion of the programme.
Mentoring/shadowing of MR delivery followed by delivery by the learner under observation with a summative assessment using documentation in the
competency training document. The documents available via the links below are for pre-registration Pharmacists but can be applied to other staff
groups.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 92
Medicines Use and Safety
S
P S
Comments:
Strengths:
There is practical evidence collecting, which fits in with pre-registration Pharmacist competencies and gives some practical experience under
supervision.
The programme is fully comprehensive and builds in a competency-based assessment.
Use of a generic MR training template package ensures that the programme covers all the essential requirements, incorporating local practice and
is less time consuming than developing it from scratch.
Weaknesses
Competency-based training is time-consuming to deliver.
Initial training session is still classroom based.
Use of a formal session means that individual learners may need to await session delivery before commencing the training programme as the
training works best as groups being able to discuss ideas (i.e. it is trainee cohort dependent).
Resources
Medicines Reconciliation Training Session - Pre-registration Pharmacist Training (Trainer Copy):
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/Medicines%20Reconciliation%20Training%20(Trainer%20Co
py)_Sept%2014.pdf
Medicines Reconciliation Training Session - Pre-registration Pharmacist Training (Student Copy):
http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/Medicines%20Reconciliation%20Training%20(Student%20C
opy)_Sept%2014.pdf
5.4 Consultation Skills in Medicines Reconciliation
Any training or competency development surrounding MR should consider including or signposting practitioners to materials that support the development of
good consultation skills as this is one of the key skills underpinning MR. The table below signposts to education and training materials and other tools that
support the development of good consultation skills.
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 93
Medicines Use and Safety
S
P S
Table 5.4: Consultation skills training resources
Training or Educational Resource Provider Description of Training or Educational Resource
Centre for Pharmacy Postgraduate Education - Consultation skills for Pharmacy
practice: taking a patient-centred approach
Distance Learning programme
RPS Consultation Skills Assessment tool and guidance
http://www.rpharms.com/help/medication_related_consultation_framework.htm
This reflective tool and guidance can be used to support the development
of your consultation behaviours and skills, and particularly helps you to
develop and demonstrate competencies in cluster 1 of the FPF – Patient
and Pharmaceutical Care. This tool provides a structured approach to
reviewing a patient’s medicines to identify any problems they may have,
including how the patient adheres to their treatment.
Consultation skills for Pharmacy practice website
http://www.consultationskillsforPharmacy.com/
This Consultation skills for Pharmacy practice website supports you
through a learning pathway, as you develop and improve your patient
consultation skills. The website forms part of a national training and
development programme, created in response to the Modernising
Pharmacy Careers (MPC)
Barbara’s story https://www.youtube.com/watch?v=DtA2sMAjU_Y
Created by nurses at Guy's and St Thomas' to raise awareness of dementia
among staff, Barbara's Story is a series of 6 films which has changed
attitudes to dementia in hospitals across the world.
Barnett N, Jubraj B, Varia S (2013). Medicines adherence- are we asking the
right questions and taking the best approach? Pharmaceutical Journal
2013;(291):153-156
Explains how principles of health coaching can facilitate a shift from a
product focused towards a patient centred approach
Emphasises the need to adopt the “Ask Don’t Tell Habit”
Illustrates how to truly acknowledge the patient as an equal expert

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 94
Medicines Use and Safety
S
P S
Consultation Skills for Pharmacy Practice: Practice Standards for England
http://www.consultationskillsforPharmacy.com/docs/docc.pdf
These practice standards have been prepared as part of the modernising
Pharmacy Careers programme to define the knowledge, skills and
behaviours and attitudes that Pharmacy professionals should be able to
demonstrate when communicating and consulting with patients
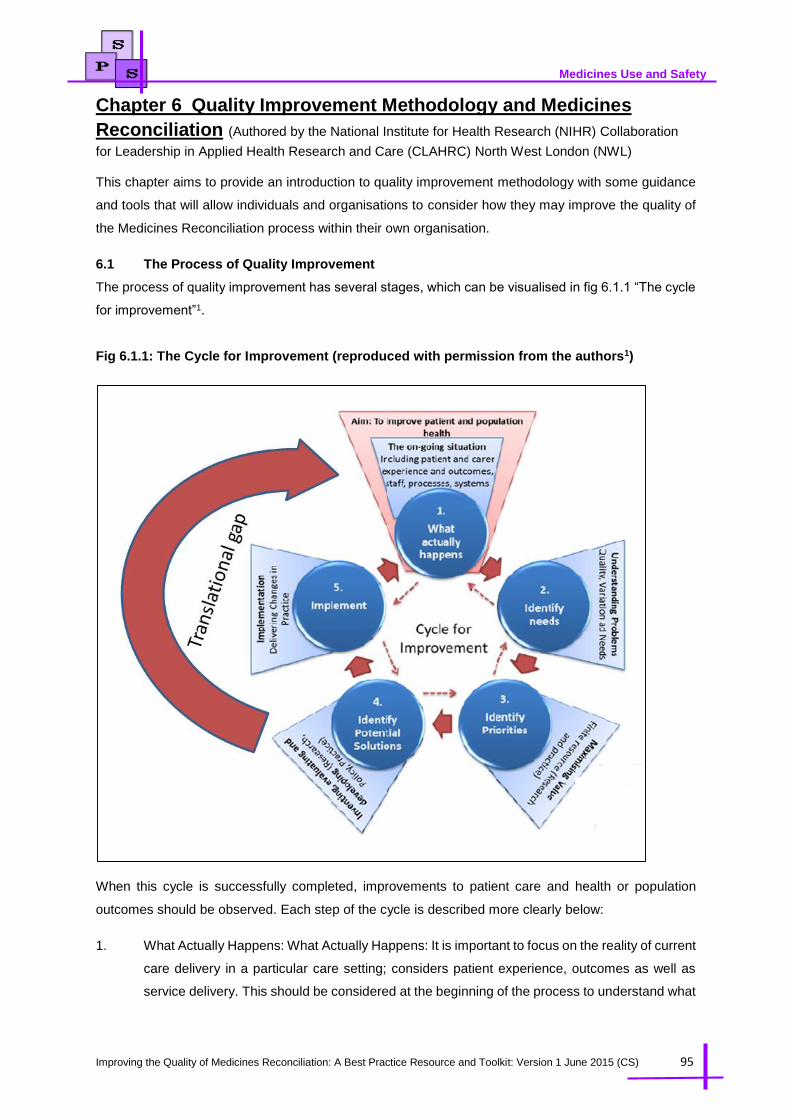
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 95
Medicines Use and Safety
Chapter 6 Quality Improvement Methodology and Medicines
Reconciliation (Authored by the National Institute for Health Research (NIHR) Collaboration
for Leadership in Applied Health Research and Care (CLAHRC) North West London (NWL)
This chapter aims to provide an introduction to quality improvement methodology with some guidance
and tools that will allow individuals and organisations to consider how they may improve the quality of
the Medicines Reconciliation process within their own organisation.
6.1 The Process of Quality Improvement
The process of quality improvement has several stages, which can be visualised in fig 6.1.1 “The cycle
for improvement”1.
Fig 6.1.1: The Cycle for Improvement (reproduced with permission from the authors1)
When this cycle is successfully completed, improvements to patient care and health or population
outcomes should be observed. Each step of the cycle is described more clearly below:
1. What Actually Happens: What Actually Happens: It is important to focus on the reality of current
care delivery in a particular care setting; considers patient experience, outcomes as well as
service delivery. This should be considered at the beginning of the process to understand what
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 96
Medicines Use and Safety
is happening before improvement work is planned, and revisited as changes are being
implemented to ensure that they are making the desired difference.
2. Identify Needs: By understanding the current situation, it is possible to identify areas for
improvement, for instance unmet needs, problems, variations and quality issues.
3. Identify Priorities: It is necessary to prioritise resource investment drawing on knowledge
including patient and population needs, economic and clinical considerations to focus energy
and support successfully delivery of improvements.
4. Identify Potential Solutions: Identifying potential solutions that need to be implemented and
tested to see if they are capable of improving ‘what actually happens’. This stage considers
existing knowledge and interventions or creates new interventions and evidence about what
might work.
5. Implement: Process by which potential solutions are implemented into practice. This is an
iterative process changing in response to emerging evidence to ensure solutions are fit for
purpose and deliver the desired change in ‘what actually happens’.
In reality there is often a gap between the identification of potential solutions and their implementation
and delivery of improvements in care settings. This gap is often described as the translational gap and
results in poor quality patient care. Fig 6.1.2 describes a quality improvement project which had a
significant focus on Medicines Reconciliation that took place at Chelsea and Westminster Hospital and
the challenges the team had to overcome to achieve their desired improvements.
Fig 6.1.2: A project to implement medicines optimisation to support patients with changes made
to medication during an emergency admission into hospital.
A project team was established to address concerns re medicines optimisation including
reconciliation. To start, the project team mapped the actual process of a patient’s journey through
the hospital to discharge home and how this related to their medication needs. They discovered that
four separate professionals were taking medication history from patients (doctors, nurses,
pharmacists and physiotherapists) and that this information was being held in silos and not shared
with the rest of the team. The process map showed inefficiencies, poor patient experience and safety
hazards: For example one patient had arthritis and the physiotherapist was aware she was unable
to open bottles with a child-proof top, but she was given tablets in a bottle with a child-proof top from
pharmacy.
The project team facilitated a number of activities to support staff and patients to redesign the
process, renegotiating the roles of each of the four staff groups so work was coordinated more
effectively. As a result of this work a single Medicines Reconciliation form was introduced for use by
all four professional groups.
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 97
Medicines Use and Safety
The team started collecting data on how well the new Medicines Reconciliation process was working,
including the rate of errors in the reconciliation process. They found that there was a high rate of
errors (24%), although the error rate varied a lot, between 0% and 74%. The team realised that whilst
they had improved the process for Medicines Reconciliation they still needed to improve the rate of
error free Medicines Reconciliation and further reduce variation in how the process was completed.
The team investigated the causes of high or low error rate and how error rates related to patient flow
and staffing levels.
As a consequence of this investigation they decided to redistribute Pharmacy staff to support a 7 day
per week to improve consistency of their service. The team had to negotiate this with several people
including the executive team to secure the appropriate budget and permissions for this change to
take place.
The team realised that information availability on patient level drug history was a systemic problem,
and whilst this hadn't been the original focus of the project, it was fundamentally linked to their ability
to complete high quality Medicines Reconciliation. Patients involved with the project challenged
assumptions about relying on clinicians and healthcare organisations for this information. To support
patients to have greater ownership of their medication histories the team worked with patients to
develop a patient-held ‘My Medications Passport’ that could act as information source to support
Medicines Reconciliation. This led to patients using the My Medications Passport as a platform for
conversations with health care professionals about their drug histories.
The team also worked to increase their profile, identifying how their work related to key hospital
concerns including the importance of Medicines Reconciliation to admissions avoidance, how it
linked to the safe and effective flow of patients through emergency care, and how it contributed cost-
savings by avoiding inappropriate prescribing. Aligning the project to that of the key hospital
concerns took considerable work, but helped to secure vital resources including executive support to
champion the work and permission for team members to be released from daily business.
This example highlights the complexities the project team had to navigate and the wider range of
issues they encountered right from what actually was happening on the wards, identifying the need
for change, identifying priorities and solutions and implementing improvement initiatives. (cycle for
improvement model2). The example also illustrates why effective implementation of new evidence
requires a deep understanding of complex care processes and how they interrelate to form a care
delivery system.
For further information contact Vanessa Marvin at [email protected]

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 98
Medicines Use and Safety
6.2 A Systematic Approach to Quality Improvement:
CLAHRC NWL has developed a systematic approach to quality improvement based on a wide range
of existing research evidence and their experience of delivering, evaluating and researching
improvement projects over the last six years and draws on a diverse set of principles from academic
literature2-6. The methods draw on research literature including basic scientific research, clinical
research, statistics, change management, leadership, and improvement science. Each of the methods
helps teams to addresses a different challenge and using these together will help navigate and make
sense of complexity, incorporate evidence into local practices, overcome barriers and obstacles to
change and maximise the success of the quality improvement project. The approach to quality
improvement is detailed in a stepwise manner table 6.2.
Table 6.2: Quality Improvement Methodology and Tools
1. Representative Team
2. Patient and Public Involvement
3. Stakeholder Management
4. Process Mapping
5. Action Effect Method
6. Plan-Do-Study-Act cycles
7. Measurement for Improvement (including Statistical Process Control)
8. Outcome Measurement
9. Sustainability Model
10. Reviews
11. Finances
Representative Team:
What is a representative team?
In order for the research to be embedded into practice, it is essential to include front line staff members
involved in the day to day 'operational systems' that deliver patient care. To achieve patient centred
care, it is also important to actively involve patients, families and carers who are likely affected by the
research throughout the life of the project.
Why have a representative team within a quality improvement project?
Successful projects are led by strong individuals who are committed to making a difference in bringing
high quality and safer care to patients. It helps to have representation from all staff groups affected by
the project as they can bring insights from their professional perspectives and influence their peers. The
core team will provide oversight and the driving force for the work to proceed. It should be remembered
that they will also need to engage with a wide range of stakeholders (see Patient and Public Involvement
and Stakeholder engagement sections below).
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 99
Medicines Use and Safety
How to choose a representative team?
Involve people who are in key roles that have led successful projects and programmes within your
organisation. Highlight the opportunities for professional development when engaging frontline staff and
define clear roles, responsibilities and time commitments with colleagues and their line managers and
develop a rota for meetings and events to help maintain project momentum.
Example:
Sponsor - Ensures the project is in line with the organisational strategies and can support key
decisions necessary to move the project forward. The more complex the project is the more
involved your executive sponsor should be. (e.g. Chief Pharmacist, Medical Director, Nursing
Director)
Clinical Leads - The clinical champion for the project who coordinates the delivery of the
improvement whilst maintaining high governance standards. (e.g. Senior Clinical Pharmacist,
Care of the Elderly Consultant)
Project Managers - Support the clinical lead and project team members in managing timelines
and coordinating actions, applying improvement methods and the overall delivery of the project.
(E.g. mid-career pharmacist, managers, external project support).
Information Support - Key to collecting routine data and reporting on it. Early collaboration with
Information Technology and Information Services and other relevant departments will support
system changes. (e.g. information analysts, business managers, researchers)
Ward Nursing Staff – Nurses as part of the multi-disciplinary team support the implementation of
the improvement activity, collect and analyse data and support the delivery of the project to
improve patient care (Nurses may be collecting MR data for Med Safety Thermometer already)
Ward Pharmacy Staff - Pharmacists as part of the multi-disciplinary team will support the project
in implementation, providing information on the process and flow and support iterative changes
that need to be implemented as well supporting in data collection and analysis.
Medical Staff, AHPs, receptionists, ward clerks and other healthcare staff may be key people in
bringing your improvement project into practice. Engaging these members from the beginning
will make them feel involved and empowered to make change, and bring useful insights to guide
project direction.
Patient and Public Involvement:
What is Patient and Public Involvement?
The term “Patient and Public Involvement” is to mean activities carried out ‘with’ or ‘by’ members of the
public rather than ‘to’, ‘about’ or ‘for’ them. Individuals can be considered as Patients or Public if they
are: patients; potential patients; informal or family carers; people who use health and social care
services; community and voluntary sector groups or individuals.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 100
Medicines Use and Safety
Why involve patients and the public?
People have a right as citizens and taxpayers, to be involved in shaping services. However, more
importantly involving patients can be transformative and a useful challenge to existing ways of working7.
Working with patients/public can lead to tangible benefits in healthcare improvement as well as
unexpected benefits8-10. Involvement can be at the individual or collective levels – that is, an individual
may be involved as a result of their own care or involvement can be with groups of people to inform
decisions for example at service level. Whether the project team should engage individually or
collectively, should be decided by what the aims are of the quality improvement project.
How to involve patients and the public?
How people are involved in any project needs to be specific to the context. Thinking carefully about the
rationale for patient involvement, identifying the most appropriate methods to use, having clarity on the
role(s) patients will play and ensuring that effective involvement strategies are in place, are important
steps towards facilitating the involvement of patients in ways that harness its full potential, and the
distinctive roles that patients can play in improvement work. It would also be beneficial to reflect on the
experience and expertise across the project team when involving patients and the availability of
resources to support specific methods for example workshops and focus groups. For example, patients
and the public can be involved in emotional mapping of patient journey to understand their perspective
of care or can be involved as part of the project team.
Example:
Patients were part of an improvement team aiming to improve prescribing in the elderly. Interactions
that the patients had in other healthcare settings as well as in their capacities as carers or people
with long-term conditions, led them to suggest a “passport” which would contain all of their current
medication information and would support communication with healthcare professionals. Healthcare
professionals worked with patients as team members and together developed this idea in to a “My
Medication Passport”13.
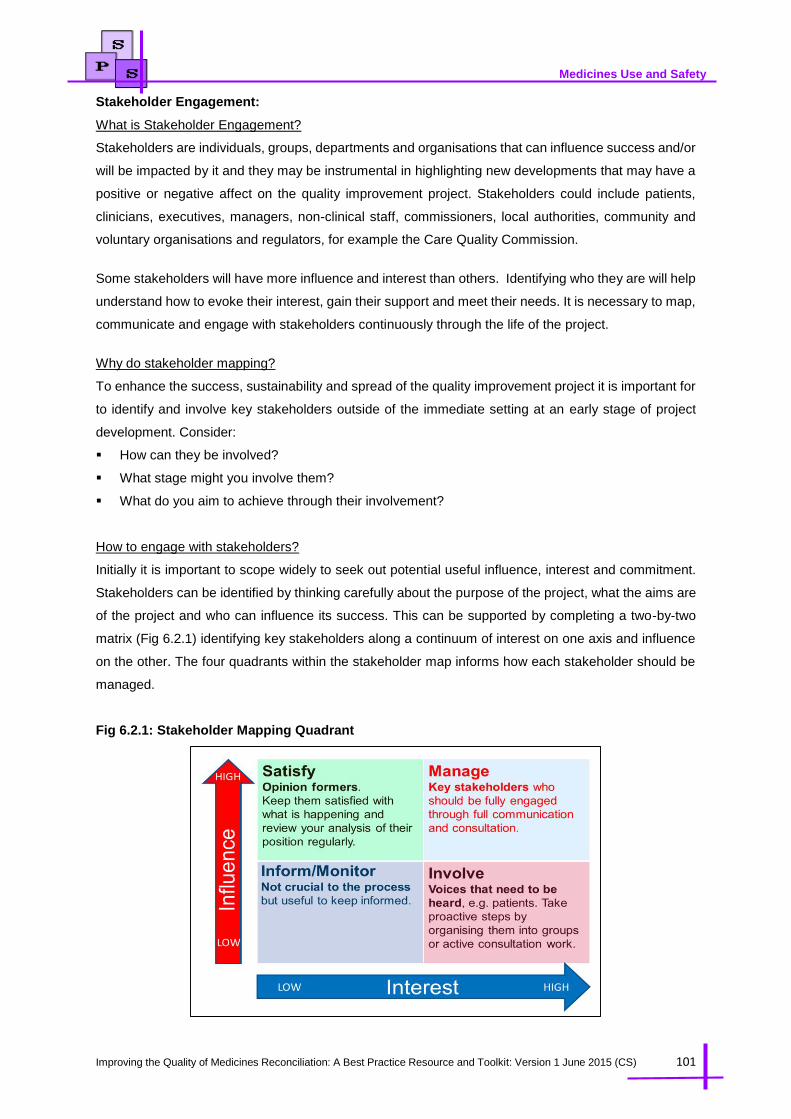
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 101
Medicines Use and Safety
Stakeholder Engagement:
What is Stakeholder Engagement?
Stakeholders are individuals, groups, departments and organisations that can influence success and/or
will be impacted by it and they may be instrumental in highlighting new developments that may have a
positive or negative affect on the quality improvement project. Stakeholders could include patients,
clinicians, executives, managers, non-clinical staff, commissioners, local authorities, community and
voluntary organisations and regulators, for example the Care Quality Commission.
Some stakeholders will have more influence and interest than others. Identifying who they are will help
understand how to evoke their interest, gain their support and meet their needs. It is necessary to map,
communicate and engage with stakeholders continuously through the life of the project.
Why do stakeholder mapping?
To enhance the success, sustainability and spread of the quality improvement project it is important for
to identify and involve key stakeholders outside of the immediate setting at an early stage of project
development. Consider:
How can they be involved?
What stage might you involve them?
What do you aim to achieve through their involvement?
How to engage with stakeholders?
Initially it is important to scope widely to seek out potential useful influence, interest and commitment.
Stakeholders can be identified by thinking carefully about the purpose of the project, what the aims are
of the project and who can influence its success. This can be supported by completing a two-by-two
matrix (Fig 6.2.1) identifying key stakeholders along a continuum of interest on one axis and influence
on the other. The four quadrants within the stakeholder map informs how each stakeholder should be
managed.
Fig 6.2.1: Stakeholder Mapping Quadrant

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 102
Medicines Use and Safety
Example:
In a quality improvement project focussed on Medicines Optimisation at Chelsea Westminster
Hospital the team undertook a stakeholder mapping exercise and started with the example below.
They soon realised that they had not included Physiotherapists and Allied health prescribers within
the project and also realised they needed support from the Chief Pharmacist. They then updated the
stakeholder map to include others who needed to be involved and informed in the project.
Process Mapping:
What is Process mapping?
A process map is a visual representation (a picture or model) that shows all of the current steps in a
process. In a healthcare context, this is often a map of a patient journey - highlighting the relevant
procedures and administrative processes a patient might come across from point A to point B in their
treatment. Importantly the process map should show how things are and what currently happens, rather
than what should happen or what people would like to happen in the future
Why use process mapping?
Process mapping helps users to see what is happening by giving a structured, visual method of
representing tasks and decisions made within a clearly defined context. Setting out a process visually
like this helps anyone involved in the quality improvement project to see other people's tasks and roles.
Process mapping identifies opportunities for improvement towards a more safe, efficient and
coordinated process for patients and staff. It can also help to diagnose problems and identify areas for
improvement. This is necessary to influence how the project will align or ‘fit’ into these systems and
roles to sustain and embed good practice, and should be revisit as the project progresses and changes
are made.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 103
Medicines Use and Safety
How to do a process map?
The most effective approach to building a process map is to work collaboratively as a project group.
The more people that work on the map, the more likely you are to capture the entire process accurately
and from all perspectives. To understand the process, team members must walk through the patient
journey from beginning to end to find out what is actually happening, not what is perceived to be
happening? Outlined below are some tips when conducting a process mapping exercise:
Allow as much time as possible to gather the team and stakeholders together
Planning and preparation for this event is key
Decide who can facilitate and ask the challenging questions that will not disrupt the dynamics. Pre-
meet with senior leaders and managers to discuss your project and invite them to come along to
the process mapping session.
It is important to agree the starting point and end point of your pathway and what is in scope and
out of scope
Start at a high level and drill down
Identify and discuss at each step who is involved in that process or decision point? What are the
parallel processes? Where are the potential ‘trigger’ points that could support your project? Park
issues you cannot solve, to be returned to at a later date.
Be open to ideas and generated by the session.
Document ideas for future use
There may be a need to return to complete more information later that is not available at the initial
time of doing the map.
It is helpful to observe the processes in practice once the initial map has been developed to see if
it accurately reflects what is actually happening in the care setting.
It can be helpful to revisit the process map throughout the improvement project to see if changes
are having the desired impact and to assess any further learning or problems that emerge as
changes are made.
The session will help identify which areas along the pathway require improvement or how they will be
affected by introducing a change. The session will also help the development of key measures, and
identify who is involved in the care processes which may indicate additional people to join the project
team or new stakeholders to engage. The session may identify areas where it is unclear what the
process is and where further investigation needs to take place; for example in collecting data
(observation, speaking to colleagues, quantitative data).
Example: See Fig 2.2.1 and Fig 2.2.2 in chapter 2 for an initial flow chart of the Medicines
Reconciliation process which will support a process mapping exercise.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 104
Medicines Use and Safety
Action Effect Method (AEM):
What is Action Effect Method?
The Action Effect Method14 is a structured way to develop a shared understanding and visual
representation of the three questions in the model for improvement:
(1) Shared aim: What are we trying to accomplish?
(2) Measurement: How do we know that a change is an improvement?
(3) Intervention Ideas: What changes can we make that will result in an improvement?
The Action Effect Method specifies a method of developing the shared aim, then breaking this down
into well-defined contributing factors and connecting these to interventions through cause/effect chains.
The Action Effect Method produces a visual representation known as an Action Effect Diagram, which
depicts the overall aim in a box on the left, and interventions and implementation activities on the right.
The Action Effect Diagram helps you visualise a cause/effect pathway, connected by arrows, from these
interventions to the overall aim. Measurement concepts and links to the evidence are depicted visually
on the diagram as well. This helps the entire project team to keep the whole picture of the project in
mind, and focus on the overall aim, whilst planning specific tasks and implementation efforts.
Why use the Action Effect Method?
The Action Effect Method gives you a clear and structured way to uncover the detail of your project
processes. The finished Action Effect Diagram demonstrates ‘how’ an overall aim might be achieved
by reading left to right, and ‘why’ an intervention is being tested by reading right to left. It can help team
members and other stakeholders to see exactly what is going on in your improvement project. It also
makes sure everyone is focussed on a common aim and help team members to communicate clearly
to others about your project. Interventions are also identified that can be trialled using Plan-Do Study-
Act cycles and predictions made about the potential impact of interventions and how this can be directly
and indirectly measured to assess change efforts success.
How to construct an Action Effect Diagram?
It is helpful to have an initial facilitated session that brings together diverse stakeholders. While taking
time to consider the project in detail is preferable, if needed to, the project team could create an Action
Effect Diagram within a two-hour facilitated session. The initial Action Effect Diagram can then be built
on and developed further over time as the project progresses. The steps below provide some tips on
how to facilitate a session:
Set the scene: Explore the patient and carer experience by using emotional mapping to help remind
stakeholders why this work is important and focus their thinking on what changes need to take
place.
Agree the project aim: Establish a common purpose and shared aim by discussion. Always start
with exploring the overall aim of different people in the group – ‘what do you want to achieve?’ This
is essential to ensure that the whole team are in agreement, and to ensure that the discussion
focuses on the main issue. Try and steer conversations away from ideas for interventions during
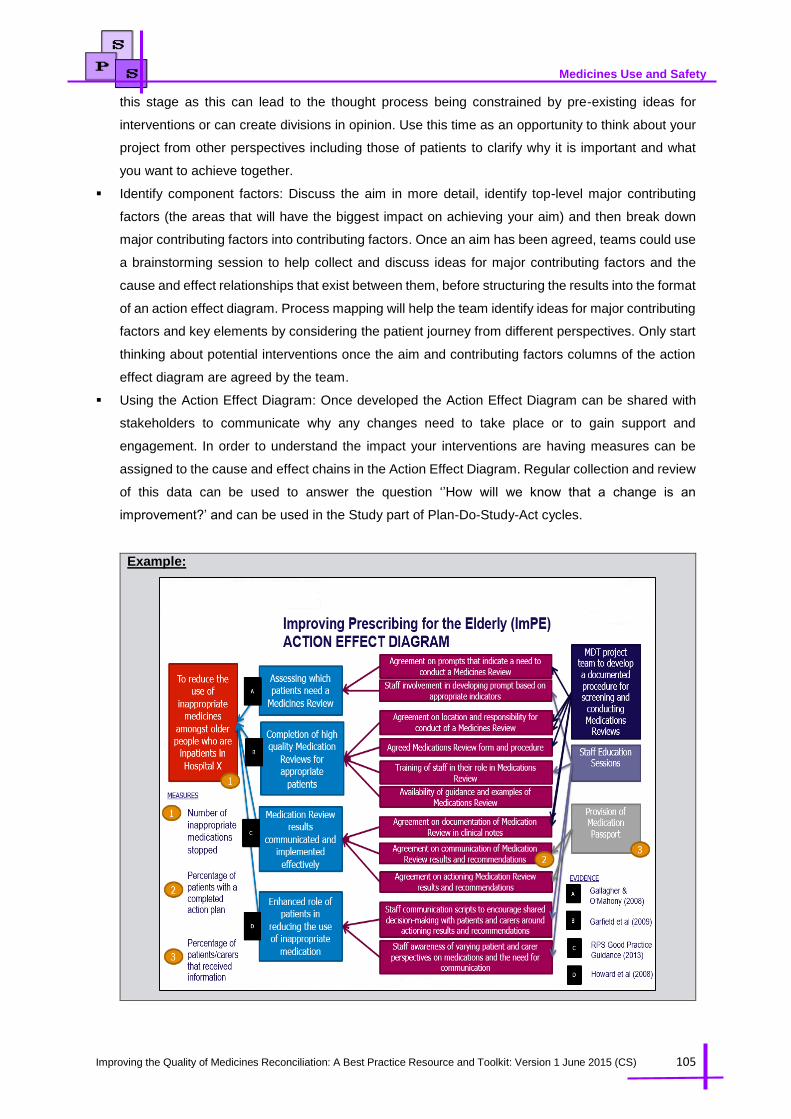
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 105
Medicines Use and Safety
this stage as this can lead to the thought process being constrained by pre-existing ideas for
interventions or can create divisions in opinion. Use this time as an opportunity to think about your
project from other perspectives including those of patients to clarify why it is important and what
you want to achieve together.
Identify component factors: Discuss the aim in more detail, identify top-level major contributing
factors (the areas that will have the biggest impact on achieving your aim) and then break down
major contributing factors into contributing factors. Once an aim has been agreed, teams could use
a brainstorming session to help collect and discuss ideas for major contributing factors and the
cause and effect relationships that exist between them, before structuring the results into the format
of an action effect diagram. Process mapping will help the team identify ideas for major contributing
factors and key elements by considering the patient journey from different perspectives. Only start
thinking about potential interventions once the aim and contributing factors columns of the action
effect diagram are agreed by the team.
Using the Action Effect Diagram: Once developed the Action Effect Diagram can be shared with
stakeholders to communicate why any changes need to take place or to gain support and
engagement. In order to understand the impact your interventions are having measures can be
assigned to the cause and effect chains in the Action Effect Diagram. Regular collection and review
of this data can be used to answer the question ‘’How will we know that a change is an
improvement?’ and can be used in the Study part of Plan-Do-Study-Act cycles.
Example:

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 106
Medicines Use and Safety
Plan-Do-Study-Act cycles:
What is Plan-Do-Study-Act cycles?
The Plan –Do-Study –Act cycle is a framework for an efficient trial and learning methodology (see fig
6.2.2 of PDSA cycle below). The cycle begins with a plan and ends with an action and the use of the
word study emphasises that the purpose of this phase is to build new knowledge. Multiple Plan-Do-
Study-Act cycles are usually needed to make successful changes.
Fig 6.2.2: PDSA Cycle
Why use Plan-Do-Study-Act cycles?
The complexities of healthcare systems make it impossible to do all the design and planning of a change
before it is put into practice. The PDSA cycle13 is a way of developing an intervention over time, testing
changes by starting on a small scale, overcoming barriers that are encountered, and then gradually
ramping up to a full scale intervention. By the time a full scale implementation is reached all the little
unforeseen glitches will have been sorted out and there is a better chance of achieving the aims of the
intervention and sustaining this in the long term.
How to use Plan-Do-Study-Act cycles:
Testing begins with a well laid out plan (to test a change) developed with the project team. Part of
starting any improvement project is to break it down into manageable small steps. These steps will be
the basis for changes to test using Plan-Do-Study-Act cycles. It is important to prioritise changes and
conduct them one at a time: which will provide the biggest impact? From the previous example of the
Action Effect Diagram, the testing would be linked to each the identified interventions on the far right
hand side of the action effect diagram for example the design of a new form for medication review.
Plan: The plan should include predictions made by the project team. Identify potential changes to test
and discuss as a team what predictions will happen because of this change and any difficulties that are
anticipated. Document these to compare back to after your test.
Do: The project team then carries out the agreed plan based on who does what, when and where as
identified in the plan and collect data for analysis.
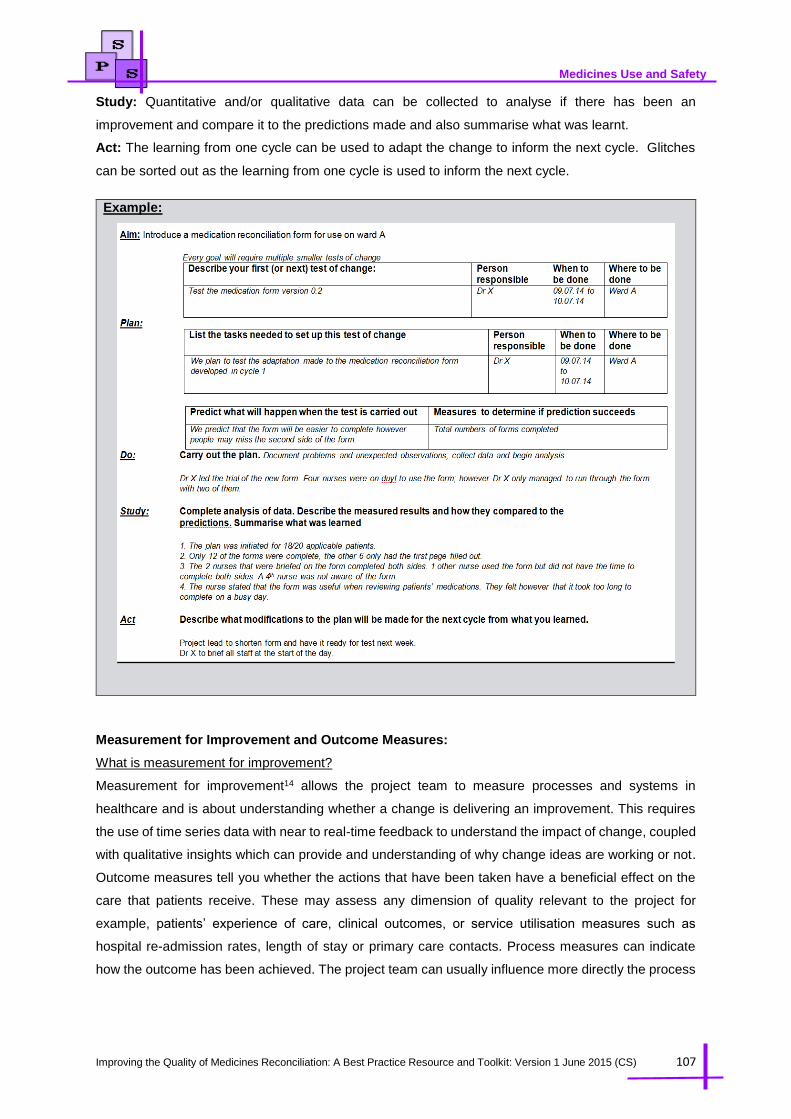
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 107
Medicines Use and Safety
Study: Quantitative and/or qualitative data can be collected to analyse if there has been an
improvement and compare it to the predictions made and also summarise what was learnt.
Act: The learning from one cycle can be used to adapt the change to inform the next cycle. Glitches
can be sorted out as the learning from one cycle is used to inform the next cycle.
Example:
Measurement for Improvement and Outcome Measures:
What is measurement for improvement?
Measurement for improvement14 allows the project team to measure processes and systems in
healthcare and is about understanding whether a change is delivering an improvement. This requires
the use of time series data with near to real-time feedback to understand the impact of change, coupled
with qualitative insights which can provide and understanding of why change ideas are working or not.
Outcome measures tell you whether the actions that have been taken have a beneficial effect on the
care that patients receive. These may assess any dimension of quality relevant to the project for
example, patients’ experience of care, clinical outcomes, or service utilisation measures such as
hospital re-admission rates, length of stay or primary care contacts. Process measures can indicate
how the outcome has been achieved. The project team can usually influence more directly the process
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 108
Medicines Use and Safety
measures than the outcome measures. Linked closely to the project’s aims and objectives, these
measures should be specific, simple, easy to collect and available for weekly use.
Why use measurement for improvement?
Healthcare is complex and however well a new idea works in a trial or in the lab, often it is not known
how effective it will be in real life. To get the most out of the intervention it is important to measure as
the project progresses to understand the variation in the data, using appropriate methods (such as
statistical process control). This enables the project team to know what works and what doesn’t,
improving quality of care in the process. Measurement is a source of learning during implementation
and monitoring of data can help sustain improvement after implementation.
How to measure for improvement?
Define what precisely is being measured including operational definitions
Agree processes or mechanisms by which measurement will take place
Agree who is responsible for data collection, analysis and feedback
Where possible, use existing data and focus on a small number of measures.
Ensure that baseline data are collected before interventions are implemented. They could be
quantitative or qualitative. The purpose of baseline data is to provide information on the current system
of care (which could be done at the process mapping stage), and could include some of the
improvement measures identified. Collecting and analysing baseline data will help inform the starting
point for the project. This will help plan the first actions on the PDSA cycle.
Measurement can also be used over the course of the project to assess how progress is going.
Statistical Process Control is a helpful method to understand what variation is normal and to be
expected, and what is unusual. This analysis method can also signify when a change has been made.
In the example below a quality improvement team identified a weekly average of 24% of medicines
were unreconciled, with wide variation. Interventions to the system of care were made such that this
variation was reduced by half, and the percentage unreconciled medicines fell to 11% on average. At
one point in the new process 40% unreconciled was noted, this would have been “normal” in the
previous care provision, but was unusual now.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 109
Medicines Use and Safety
Example:
Sustainability:
What is sustainability?
Sustainability is when new ways of working and improved outcomes become the norm. Not only have
the process and outcome changed but the thinking and attitudes behind them are fundamentally altered
and the systems surrounding them are transformed in support. There are different models that look at
sustainability including the NHS Institute for Innovation and Improvement Sustainability Model15 and the
CLAHRC NWL ‘Long Term Success Approach’. These models aim to aid teams in reflecting upon long
term success of their initiatives and consider actions they and their teams can take to increase chances
of achieving sustainability over-time. The approach provides a comprehensive analysis of factors
influencing improvement sustainability as well as a tool to examine sustainability within improvement
projects
Why consider sustainability with a quality improvement project?
Significant resources have been dedicated to quality improvement within healthcare services in order
to improve patient outcomes and experience. Unfortunately, many improvements within healthcare fail
to sustain beyond the end of funding and their true benefits are not realised. It is important for teams
to consider sustainability throughout the duration of their projects in order to adequately plan for benefits
to continue after the life time of the project.
How to use the sustainability model?
Sustainability models can be used by individuals but a richer picture can be gained if key members of
the improvement team complete the model and discuss differences in opinions. Individuals within the
team would bring different perspectives and it is important to understand these different perspectives.
In addition to providing further information on sustainability, the act of completing the model can lead to
useful discussions about your improvement initiative. The figure below (fig 6.2.3) shows the ten factors

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 110
Medicines Use and Safety
of sustainability within the three themes of process, staff and organisation from the NHS Institute for
Innovation and Improvement’s sustainability model16.
Fig 6.2.3: NHS Institute for Innovation and Improvement’s Sustainability Model
Reviews:
What are project reviews?
Project reviews provide an overview of the project and can be used to track progress in the project at
different points in time. There is a great deal of literature on the relative merits of both summative and
formative evaluation and review.
Why carry out project reviews?
The review process has both an ‘operational’ purpose and a ‘research’ purpose. From an operational
stand point reviews allow the project team to: Take a step back to consider progress to date and
direction of the project, identify main challenges at this stage and how they can be resolved and identify
support needs of the project team at this stage. From a research standpoint: Use the outputs of review
as one source (among others) to assess - common barriers/facilitators to applying evidence into practice
, an understanding of how projects evolve and to capture your narrative to share with others for example
as a poster in conferences or a peer reviewed journal paper.
How to do a project review?
Structure the review to happen at periodic intervals for the duration of the quality improvement project.
For example, improvement projects that last 18 months, project reviews can happen in windows/periods
of: Window 1 – 6 to 9 months and Window 2 – 12 to 15 months, Window 3 21-24 months after project
has finished to assess sustainability and on-going support requirements. Each review includes a
presentation from the team and a discussion. Part of the purpose of the discussion is to reveal the
extent to which each team has utilised and engaged with the quality improvement methodology. When
preparing a project review consider:
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 111
Medicines Use and Safety
When should a review take place and why?
Scheduling dates & agreeing Chair
Preparing agenda and identifying attendees
Material to bring to review
Actions after the meeting
Capturing progress to share with others
Resources and Funding:
What is resources and funding?
Financial support provides resource through the appointment of specified staff roles or released time
and through non-pay elements such as computers, expenses for focus groups.
Why financial support is needed?
The provision of financial support is a well-established mechanism for generating commitment to
research and development in healthcare. Financial support provides a mandate to act, thereby providing
the freedom to do so. If funding is specifically attached to a learning mandate - this can also support
willingness to learn. Space and time away from busy daily practices is needed for staff to engage with
and explore improvements that can be made. A well written business case can secure resources for a
quality improvement project. This can be used to obtain management commitment and approval for
investment in quality improvement through rationale for the investment and also provides a framework
for planning and management of the business change and the ongoing viability of a project or
programme will be monitored against it.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 112
Medicines Use and Safety
6.3 Medicines Reconciliation Quality Improvement Case Study - North Bristol NHS Trust
Case Study - Improving and Maintaining Medicines Reconciliation on Admission (also
published on the NICE Shared Learning Database)
Aim:
Our aim was to improve medicines reconciliation. Our objective was to exceed 95% of patients
receiving Medicines Reconciliation within 24 hours of admission, in line with NICE recommendation
1.3.1 in NG5 (2015). NICE guidance and other sources evidenced the benefits of carrying out
medicines reconciliation. Our initial problem was what data to collect to prove our performance and
how to collect this. It has taken time to clarify, reach our target and embed practices. Although
"Medicines Optimisation" NG5 has just been published (3/2015) we feel further updated practical
guidance would help hospitals implement, spread and improve consistency between hospitals.
The first issue is the target of "within 24 hours of admission". This is easy to measure for Trusts who
have electronic prescribing, as data can be accurately extracted. For Trusts without this, the
admission date covers 00.01-23.59. Electronic admissions data is not always accessible or accurate
and does not show actual time of prescribing. For clarity we defined that if a patient was admitted on
day 1, then reconciliation had to be completed by 5pm on day 2. NHS England subsequently
confirmed this definition.
The second issue is the definition of 'medicines reconciliation'. Two stages of basic and full
reconciliation were defined by the National Prescribing Centre (2008). This is again easy to measure
for Trusts with electronic prescribing. For Trusts without it, urgent changes to the prescription will be
actioned immediately but non urgent changes will be highlighted and the doctor could address these
at any time between Pharmacist visits. Our work with SPI2 promoted using the easiest method of
data collection. To avoid unnecessary visits to check on this, we defined the completion of medicines
reconciliation as the time when all changes were highlighted but not necessarily acted on. The
benefits of measuring on a run chart using improvement methodology is that results are consistently
measured and the run chart annotated if this changes - and improvements for the individual Trust
clearly demonstrated. Definitions are more important when results from different Trusts are being
compared through benchmarking, as the data may not be comparable. NBT methods ensure robust
auditable data with appropriate sample sizes and reduction of bias in patient selection and
consistency in measurement. Medicines Management Technicians (MMTs) randomly audit 5 patients
per ward per week.
Context:
Medicines Reconciliation ensures that medicines prescribed on patient admissions correspond to
those taken before admissions. This process involves discussion with patients/carers and using
primary care records (NICE/NPSA 2007). Medication errors cause harm to patients, lead to increased
morbidity/mortality and inflate healthcare costs. The importance of Medicines Reconciliation is well
documented:
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 113
Medicines Use and Safety
Globally: (2006) the 'High 5's programme' (World Health Organisation) and the '100K Lives
campaign' [Institute of Healthcare Improvement (IHI)] both targeted Medicines Reconciliation.
Nationally: (2007-2009) the 'Safer Patients Initiative' (SPI) (IHI/Health Foundation) was
introduced.
The key national driver is: 'Technical patient safety solutions for medicines reconciliation on
admission of adults to hospital' (NICE/NPSA 2007).
Medicines Optimisation dashboard (2014) links information from the Medication Safety
Thermometer with Safety information from NHS England.
North Bristol NHS Trust (NBT) and SPI2.
NBT is a large acute NHS Trust in England with approximately 1000 beds. Our work affects 70,000
patients annually via elective and emergency admissions. NBT was selected for ‘SPI2’ (2007-2009)
followed by the Southwest Quality and Patient Safety Improvement Programme (SWQPSI).
Medicines Reconciliation was set as a target.
SPI2 and NICE guidance:
Before we started, we thought that Medicines Reconciliation occurred but could not prove. Our first
task was to introduce processes to enable us to collect data to measure. When we started to
measure, baseline assessments were our first results from 1 ward. We assumed most admissions
would occur on our admissions wards, but found approximately 80% occurred on 30 different wards.
In order to ensure consistency across NBT, we focussed on wards with the greatest number of
admissions (>2%). Patients were involved in the work as in carrying out medicines reconciliation,
patients and their carers were of paramount importance in finding out what drugs had been
prescribed prior to admission and more particularly in finding out what medication they were actually
taking and how. NICE guidance was the first key national driver to support and justify our actions.
The benefits detailed in our results below ensured that medicines reconciliation was carried out as
soon as possible after admission ensuring the patient was prescribed the correct medication reducing
harm from medication errors.
Methods:
SPI2 and SWQPSI use the Model for Improvement and 'Plan, Do, Study, Act' (PDSA) cycles; 'Tests
of change'/'spread' and 'working in collaboration/couplets'. Our work involved spread through various
phases:
Phase 1: Feb 2007-July 2008: SPI (1-8 wards) We liaised with Medical Staff to introduce a Medicines
Admissions Proforma that included drugs on admission/sources of information. Pharmacists audited
Medical staff and we involved frontline ward staff in PDSA cycles. We publicised work using 'Toilet
Top Tips' (captive education!!)
Phase 2: Aug 2008-Jul 2009 (8-11 wards) We consolidated practices and involved more staff to
continue spread. We designed a DVD for training medical students/doctors.

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 114
Medicines Use and Safety
Phase 3: Aug 2009-Feb 2011: (11-30 wards) A new Pharmacist post enabled increased spread and
service to a high risk area.
Phase 4: Feb 2011-Feb 2013: (31-20 wards) Target achieved We re-analysed admissions to ensure
appropriate data collection and audited Sunday admissions to ensure weekend admission did not
adversely affect results.
Phase 5: Feb 2013 -now: (20-15 wards) Target achieved
We are publicising our work to spread good practice. We extended clinical services to the emergency
zone at weekends, benefitting from piloting 'Connecting Care'. New junior medical staff shadow the
Admissions Pharmacist.
In 2008, we submitted a Business case for funding using the NICE/NPSA toolkit but this was not
successful. We did not discontinue any services in implementing but redesigned our clinical services
to ensure that we used more experienced Pharmacists to prioritise and carry out the medicines
reconciliation as soon as possible after admission. These Pharmacists carry out Medicines
Reconciliation more effectively than more junior pharmacists. The more junior Pharmacists could
then focus on queries arising after transfer from the admissions ward knowing the patient had come
to them having been prescribed the correct medication. By demonstrating an improved service we
were supported by funding for a new Pharmacist (2009) for Medicines Reconciliation in a new seated
assessment area and an increased number of specialist posts who contributed to this work as well
as specialty work. These included Pre op Surgical Admissions Pharmacists. Apart from data
collection (as under definitions), motivation was significant as we had not anticipated the timescale
to reach our target, spread and embed. Involving more staff was crucial.
Results and Evaluation:
Our unique results exceeded expectations. Our run chart demonstrates clear and measurable
outcomes that benefit our patients:
2007: 60% reconciled on 1 ward
2011: achieved/maintained/improved: 95% target on 30 wards
Quality, Innovation, Productivity and Prevention (QIPP) benchmarking shows NBT is the best
performing Trust in England/Wales with associated cost avoidance of £350k/yr.
Other outcomes include patients' satisfaction through increased opportunities to discuss medicines
and admissions proformas/electronic data collection tools. Results are accessible to all staff with run
charts displayed via the NBT Ward Quality Synopsis dashboard.
Key learning points:
Various factors that have contributed to our success that we would recommend:
SPI2 was an invaluable arrangement with support from experts and peers to understand
improvement methodology; 'learn from others'; 'Share success' and 'steal shamelessly!'

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 115
Medicines Use and Safety
NBT's successful approach for SPI2 provided strong executive support and each project has a
named executive to support the work.
Clinical audit support has also been invaluable and enabled us to have data portrayed in clear
run charts, broken down to ward level and displayed on the Trust quality dashboard. We ensured
data accurately reflected processes with accessible run chart results.
We annually review patient admissions data to ensure our data is collected from appropriate
wards. When wards achieve consistent results, we reduce but do not stop data collection.
Continuous measurement is ESSENTIAL to know we are achieving results.
SPI2 quoted W. Edwards Deming: 'In God we Trust -all others bring data!'
The "buy-in" of staff is vital, starting with enthusiasts and leaving laggards who often change with
peer pressure. It is tempting to spread too quickly, so important to plan and continue to embed
as the project evolves. Increased staff involvement improves sustainability, embeds into routine
work and lessens the main barrier of time.
We used quality improvement techniques and segmented the patients to develop reliable
processes to ensure that medication reconciliation is completed.
By embedding our work through the Medicines Governance Group we have access to a wide
range of staff and the group has also included patient panel representatives for nearly 5 years
that add a more complete perspective.
Improvement work never stops so we work in continuing phases. Tests of change have focussed
on weekend data and the quality of the medicines reconciliation process. Future work is now
linking in Medicines Reconciliation on discharge and primary care for the complete view.
Contact details:
Jane Smith - Principal Pharmacist Service Development & Governance (NBT Medication Safety Officer) Phone: 0788 443 7780 Email: [email protected]
6.4 The Quality Systems Resource for Pharmacy
The Quality Systems Resource for Pharmacy is a resource that has been developed by the Royal
Pharmaceutical Society to introduce quality systems and quality improvement, acting as a hub to the
fantastic improvement resources of others, and as a platform for sharing pharmacy experiences in
quality improvement. The resource provides further guidance and implementation instructions to many
of the tools discussed in this chapter in addition to other quality improvement tools such as Lean
thinking, Six Sigma etc.
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 116
Medicines Use and Safety
References:
1. Reed JE, Bell D. Making an Impact? The Emergence of Improvement Science in Healthcare. Int J
Sci Soc. 2013:77-92.
2. Langley GJ, Moen RD, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A
Practical Approach to Enhancing Organizational Performance (2nd Edition). 2nd ed. Jossey-Bass
Publishers; 2009.
3. Glasziou P, Ogrinc G, Goodman S. Can evidence-based medicine and clinical quality improvement
learn from each other? BMJ Qual Saf. 2011;20 Suppl 1:i13-17. doi:10.1136/bmjqs.2010.046524.
4. Stetler CB, Mittman BS, Francis J. Overview of the VA Quality Enhancement Research Initiative
(QUERI) and QUERI theme articles: QUERI Series. Implement Sci. 2008;3(1):8. doi:10.1186/1748-
5908-3-8.
5. Gabbay J, le May A. Evidence based guidelines or collectively constructed “mindlines?”
Ethnographic study of knowledge management in primary care. BMJ. 2004;329(7473):1013.
doi:10.1136/bmj.329.7473.1013.
6. J. Rocco P, P. Lloyd P, J. Parry G. Seven Propositions of the Science of Improvement: Exploring
Foundations. Qual Manag Health Care. 2013;22(3)(July/September):170-186.
7. Armstrong N, Herbert G, Aveling E-L, Dixon-Woods M, Martin G. Optimizing patient involvement in
quality improvement. Health Expect. 2013;16(3):e36-47. doi:10.1111/hex.12039.
8. Renedo A, Marston CA, Spyridonidis D, Barlow J. Patient and Public Involvement in Healthcare
Quality Improvement: How organizations can help patients and professionals to collaborate. Public
Manag Rev. 2014;17(1):17-34. doi:10.1080/14719037.2014.881535.
9. Renedo A, Marston CA, Spyridonidis D, Barlow J. Patient and Public Involvement in Healthcare
Quality Improvement: How organizations can help patients and professionals to collaborate. Public
Manag Rev. 2014;17(1):17-34. doi:10.1080/14719037.2014.881535.
10. Renedo A, Marston C. Spaces for Citizen Involvement in Healthcare: An Ethnographic Study.
Sociology. 2014;49(3):488-504. doi:10.1177/0038038514544208.
11. Barber S, Thakkar K, Marvin V, Franklin BD, Bell D. Evaluation of My Medication Passport: a
patient-completed aide-memoire designed by patients, for patients, to help towards medicines
optimisation. BMJ Open. 2014;4(8):e005608. doi:10.1136/bmjopen-2014-005608.
12. Reed JE, McNicholas C, Woodcock T, Issen L, Bell D. Designing quality improvement initiatives:
the action effect method, a structured approach to identifying and articulating programme theory. BMJ
Qual Saf. 2014;23(12):1040-8. doi:10.1136/bmjqs-2014-003103.
13. Taylor MJ, McNicholas C, Nicolay C, Darzi A, Bell D, Reed JE. Systematic review of the
application of the plan-do-study-act method to improve quality in healthcare. BMJ Qual Saf.
2014;23(4):290-8. doi:10.1136/bmjqs-2013-001862.
14. Poots AJ, Woodcock T. Statistical process control for data without inherent order. BMC Med
Inform Decis Mak. 2012;12(1):86. doi:10.1186/1472-6947-12-86.
15. Institute for Innovation and Improvement. Quality Improvement: Theory and Practice in
Healthcare. 2008. Available at:

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 117
Medicines Use and Safety
http://www.institute.nhs.uk/service_transformation/quality_improvement/quality_improvement:_theory
_and_practice_in_healthcare.html. Accessed May 29, 2015.
16. NHS Institute for Innovation and Improvement. Sustainability: Ensuring Continuity in
Improvement.; 2010. Available at:
http://www.institute.nhs.uk/sustainability_model/general/welcome_to_sustainability.html. Accessed
June 3, 2015.
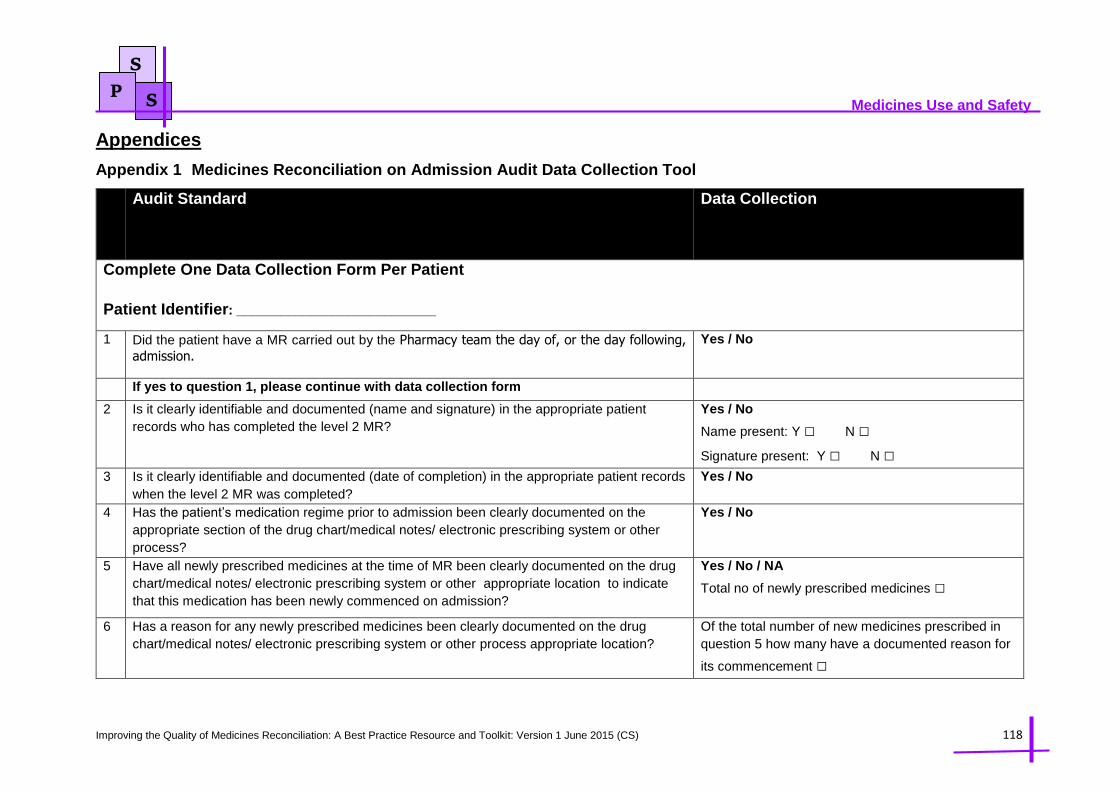
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 118
Medicines Use and Safety
S
P S
Appendices
Appendix 1 Medicines Reconciliation on Admission Audit Data Collection Tool
Audit Standard Data Collection
Complete One Data Collection Form Per Patient
Patient Identifier: ___________________________
1 Did the patient have a MR carried out by the Pharmacy team the day of, or the day following,
admission.
Yes / No
If yes to question 1, please continue with data collection form
2 Is it clearly identifiable and documented (name and signature) in the appropriate patient
records who has completed the level 2 MR?
Yes / No
Name present: Y □ N □
Signature present: Y □ N □ 3 Is it clearly identifiable and documented (date of completion) in the appropriate patient records
when the level 2 MR was completed?
Yes / No
4 Has the patient’s medication regime prior to admission been clearly documented on the
appropriate section of the drug chart/medical notes/ electronic prescribing system or other
process?
Yes / No
5 Have all newly prescribed medicines at the time of MR been clearly documented on the drug
chart/medical notes/ electronic prescribing system or other appropriate location to indicate
that this medication has been newly commenced on admission?
Yes / No / NA
Total no of newly prescribed medicines □
6 Has a reason for any newly prescribed medicines been clearly documented on the drug
chart/medical notes/ electronic prescribing system or other process appropriate location?
Of the total number of new medicines prescribed in
question 5 how many have a documented reason for
its commencement □

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 119
Medicines Use and Safety
S
P S
7 Have all medicines intentionally stopped at the time of MR been clearly documented on the
drug chart/medical notes/ electronic prescribing system or other process in the appropriate
location to indicate that this medication has been stopped on admission?
Yes / No / NA
Total no of medicines stopped □
8 Has a reason for any medicines intentionally stopped been clearly documented on the drug
chart/medical notes/ electronic prescribing system or other process in the appropriate
location?
Of the total number of medicines stopped in question
7 how many have a documented reason □
9 Have all intentional changes to medicines (i.e Dose, Route, Formulation) at the time of MR
been clearly documented on the drug chart/medical notes/ electronic prescribing system or
other process in the appropriate location to indicate that change?
Yes / No / NA
10 Have all unintentional discrepancies identified during the level 2 MR been clearly documented
on the drug chart/medical notes/ electronic prescribing system or other process in the
appropriate location.
Yes / No / NA
11 Have all allergies or nil history of allergies to medicines (NKDA) been clearly documented on
the drug chart/medical notes/ electronic prescribing system or other process in the appropriate
location and include the causative medication and brief description of reaction/outcome?
Yes / No
(Note: For the standard to be met BOTH the name of the
medication causing the allergy and the description of the allergy
reaction must be present)
12 Are there a minimum of 2 sources of evidence that have been used to confirm the MR and are
they documented in the appropriate section of the drug chart/medical notes/ electronic
prescribing system or other process?
Yes / No
Please tick all sources that have been documented
as being used:
FP10 Repeat Slip
GP Fax
PODs
Patient/Carer
Discharge Summary
Summary Care Records
Community Pharmacy PMR
MAR Chart
Other
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 120
Medicines Use and Safety
S
P S
13 Are the sources of evidence that have been used to confirm the MR documented in the
appropriate section of the drug chart/medical notes/ electronic prescribing system or other
process?
Yes / No

Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 121
Medicines Use and Safety
S
P S
Appendix 2 Medicines Reconciliation on Discharge / Discharge Summaries Audit Data Collection Tool
Audit Standard Data Collection
Complete One Data Collection Form Per Patient/Discharge Summary Patient Identifier: __________________________
Demographics
1 Are the patient’s complete details including last name, first name, date of birth, patient
address, hospital number and NHS number clearly identifiable and documented on the
discharge summary?
Yes / No (Note: All details must be present for the standard to be met)
Please tick all identifiers that were present:
Last name
First name
Date of birth
Patient address
Hospital number
NHS number
2 Are the patients General Practitioner details including named GP, address and contact
telephone number clearly identifiable and documented on the discharge summary?
Yes / No (Note: All details must be present for the standard to be met)
Please tick all identifiers that were present:
Named GP Details
Address
Contact Tel No
3 Is the reason(s) for admission clearly identifiable and documented on the discharge
summary?
Yes / No
Allergy Compliance
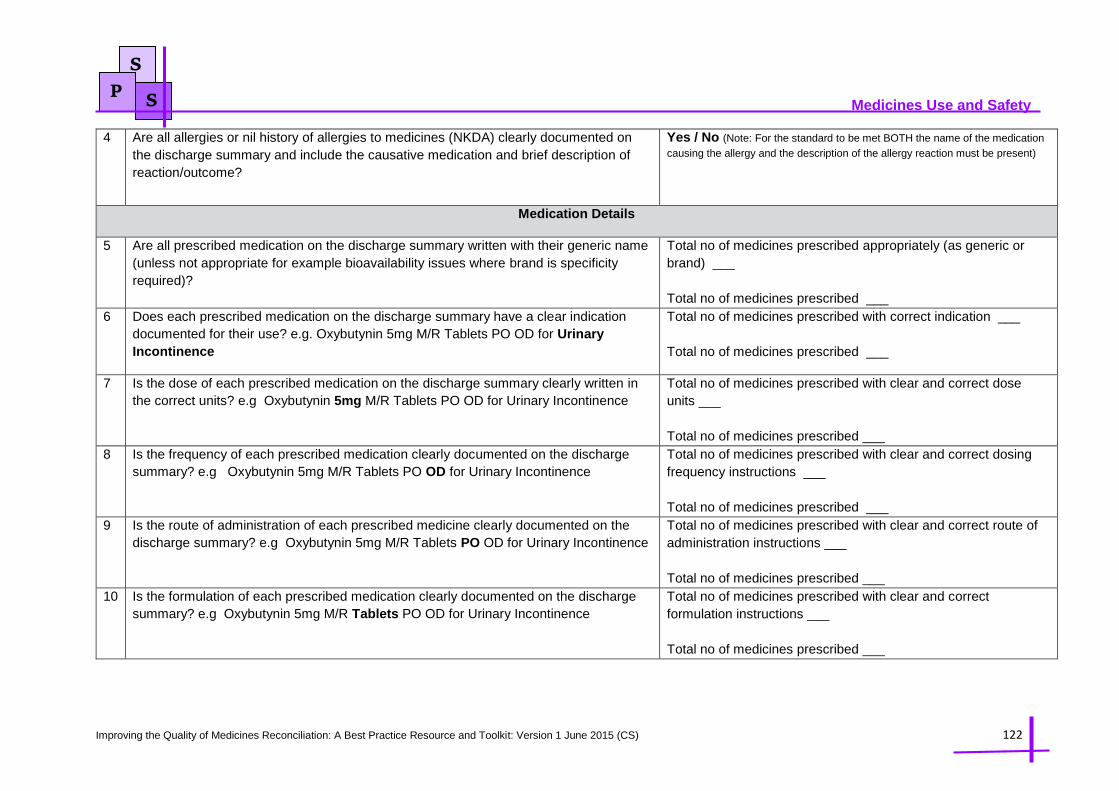
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 122
Medicines Use and Safety
S
P S
4 Are all allergies or nil history of allergies to medicines (NKDA) clearly documented on
the discharge summary and include the causative medication and brief description of
reaction/outcome?
Yes / No (Note: For the standard to be met BOTH the name of the medication
causing the allergy and the description of the allergy reaction must be present)
Medication Details
5 Are all prescribed medication on the discharge summary written with their generic name
(unless not appropriate for example bioavailability issues where brand is specificity
required)?
Total no of medicines prescribed appropriately (as generic or
brand) ___
Total no of medicines prescribed ___
6 Does each prescribed medication on the discharge summary have a clear indication
documented for their use? e.g. Oxybutynin 5mg M/R Tablets PO OD for Urinary
Incontinence
Total no of medicines prescribed with correct indication ___
Total no of medicines prescribed ___
7 Is the dose of each prescribed medication on the discharge summary clearly written in
the correct units? e.g Oxybutynin 5mg M/R Tablets PO OD for Urinary Incontinence
Total no of medicines prescribed with clear and correct dose
units ___
Total no of medicines prescribed ___
8 Is the frequency of each prescribed medication clearly documented on the discharge
summary? e.g Oxybutynin 5mg M/R Tablets PO OD for Urinary Incontinence
Total no of medicines prescribed with clear and correct dosing
frequency instructions ___
Total no of medicines prescribed ___
9 Is the route of administration of each prescribed medicine clearly documented on the
discharge summary? e.g Oxybutynin 5mg M/R Tablets PO OD for Urinary Incontinence
Total no of medicines prescribed with clear and correct route of
administration instructions ___
Total no of medicines prescribed ___
10 Is the formulation of each prescribed medication clearly documented on the discharge
summary? e.g Oxybutynin 5mg M/R Tablets PO OD for Urinary Incontinence
Total no of medicines prescribed with clear and correct
formulation instructions ___
Total no of medicines prescribed ___
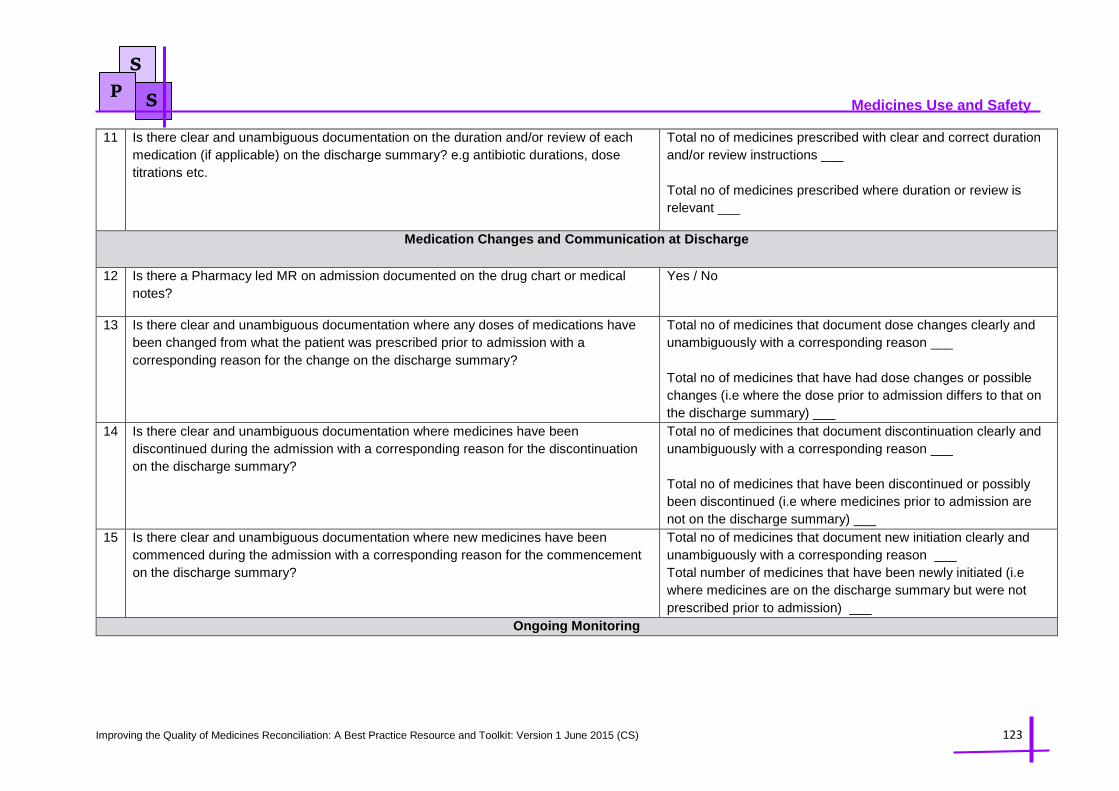
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 123
Medicines Use and Safety
S
P S
11 Is there clear and unambiguous documentation on the duration and/or review of each
medication (if applicable) on the discharge summary? e.g antibiotic durations, dose
titrations etc.
Total no of medicines prescribed with clear and correct duration
and/or review instructions ___
Total no of medicines prescribed where duration or review is
relevant ___
Medication Changes and Communication at Discharge
12 Is there a Pharmacy led MR on admission documented on the drug chart or medical
notes?
Yes / No
13 Is there clear and unambiguous documentation where any doses of medications have
been changed from what the patient was prescribed prior to admission with a
corresponding reason for the change on the discharge summary?
Total no of medicines that document dose changes clearly and
unambiguously with a corresponding reason ___
Total no of medicines that have had dose changes or possible
changes (i.e where the dose prior to admission differs to that on
the discharge summary) ___
14 Is there clear and unambiguous documentation where medicines have been
discontinued during the admission with a corresponding reason for the discontinuation
on the discharge summary?
Total no of medicines that document discontinuation clearly and
unambiguously with a corresponding reason ___
Total no of medicines that have been discontinued or possibly
been discontinued (i.e where medicines prior to admission are
not on the discharge summary) ___
15 Is there clear and unambiguous documentation where new medicines have been
commenced during the admission with a corresponding reason for the commencement
on the discharge summary?
Total no of medicines that document new initiation clearly and
unambiguously with a corresponding reason ___
Total number of medicines that have been newly initiated (i.e
where medicines are on the discharge summary but were not
prescribed prior to admission) ___
Ongoing Monitoring
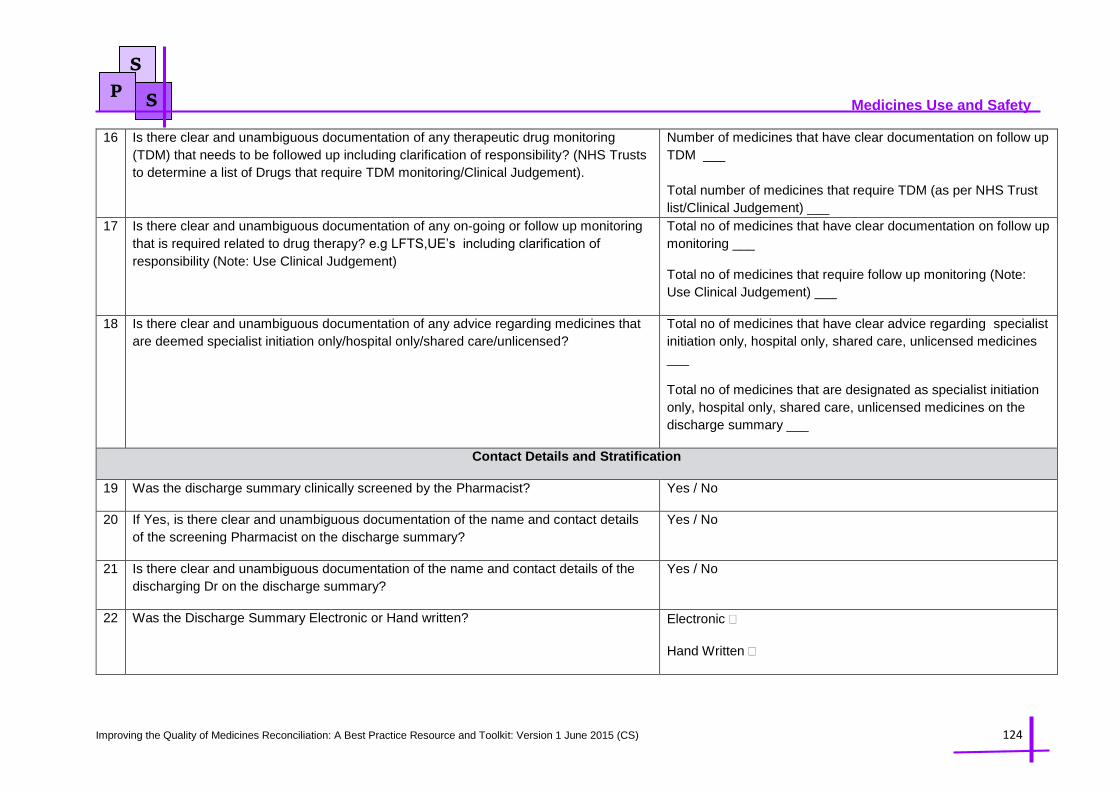
Improving the Quality of Medicines Reconciliation: A Best Practice Resource and Toolkit: Version 1 June 2015 (CS) 124
Medicines Use and Safety
S
P S
16 Is there clear and unambiguous documentation of any therapeutic drug monitoring
(TDM) that needs to be followed up including clarification of responsibility? (NHS Trusts
to determine a list of Drugs that require TDM monitoring/Clinical Judgement).
Number of medicines that have clear documentation on follow up
TDM ___
Total number of medicines that require TDM (as per NHS Trust
list/Clinical Judgement) ___
17 Is there clear and unambiguous documentation of any on-going or follow up monitoring
that is required related to drug therapy? e.g LFTS,UE’s including clarification of
responsibility (Note: Use Clinical Judgement)
Total no of medicines that have clear documentation on follow up
monitoring ___
Total no of medicines that require follow up monitoring (Note:
Use Clinical Judgement) ___
18 Is there clear and unambiguous documentation of any advice regarding medicines that
are deemed specialist initiation only/hospital only/shared care/unlicensed?
Total no of medicines that have clear advice regarding specialist
initiation only, hospital only, shared care, unlicensed medicines
___
Total no of medicines that are designated as specialist initiation
only, hospital only, shared care, unlicensed medicines on the
discharge summary ___
Contact Details and Stratification
19 Was the discharge summary clinically screened by the Pharmacist? Yes / No
20 If Yes, is there clear and unambiguous documentation of the name and contact details
of the screening Pharmacist on the discharge summary?
Yes / No
21 Is there clear and unambiguous documentation of the name and contact details of the
discharging Dr on the discharge summary?
Yes / No
22 Was the Discharge Summary Electronic or Hand written? Electronic
Hand Written