a case of rapid progressive neurosyphilis in …...sang jin lee et al. 280 j rheum dis vol. 26, no....
TRANSCRIPT
278
Received:July 2, 2019, Revised:August 16, 2019, Accepted:August 21, 2019
Corresponding to:Sang Jin Lee http://orcid.org/0000-0002-7892-6482Division of Rheumatology, Department of Internal Medicine, Kyungpook National University Hospital, 130 Dongdeok-ro, Jung-gu, Daegu 41944, Korea. E-mail:[email protected]
Copyright ⓒ 2019 by The Korean College of Rheumatology. All rights reserved.This is an Open Access article, which permits unrestricted non-commerical use, distribution, and reproduction in any medium, provided the original work is properly cited.
Case ReportpISSN: 2093-940X, eISSN: 2233-4718Journal of Rheumatic Diseases Vol. 26, No. 4, October, 2019https://doi.org/10.4078/jrd.2019.26.4.278
A Case of Rapid Progressive Neurosyphilis in Patient with Ankylosing Spondylitis Who Is Treating Anti-interleukin 17A Monoclonal Antibody, Secukinumab
Sang Jin Lee1, Han-Ki Park2, Yong-Sun Kim3
1Division of Rheumatology, Department of Internal Medicine, 2Division of Allergy and Clinical Immunology, Department of Internal Medicine, and 3Department of Neuroradiology, School of Medicine, Kyungpook National University, Daegu, Korea
Anti-interleukin 17A agent, secukinumab is remarkably effective for treating patients with ankylosing spondylitis. However, the main safety concern of secukinumab is an increased risk of infection. Generally, neurosyphilis occurs a few years after the pri-mary syphilitic infection. Rare cases of progressing to neurosyphilis with a much lower latency were reported. We report a case of rapid progressive neurosyphilis involving hearing loss in both ears in a patient with ankylosing spondylitis who was treated with secukinumab. (J Rheum Dis 2019;26:278-281)
Key Words. Ankylosing spondylitis, Interleukin 17A, Neurosyphilis
INTRODUCTION
Prior to the institution of penicillin, syphilis was a com-mon disease and neurosyphilis could develop in the course of syphilis [1]. It was reported that about 20% to 30% of untreated syphilis patients did not clear T. pallidum from the central nervous system (CNS), but the incidence of neurosyphilis decreased and characteristics of the dis-ease changed after use of penicillin [2].Anti-interleukin (IL) 17A monoclonal antibody agent,
secukinumab is highly effective in the treatment of anky-losing spondylitis (AS) and psoriasis. The main safety concern of secukinumab is increased opportunistic in-fection, and mucocutaneous candidiasis is the most fre-quent type; however, the majority of these events have not been difficult to manage [3]. In this case, we present an AS patient with rapid pro-
gressive neurosyphilis who was treated with secukinu-mab, and discuss the principal characteristics of this disease.
CASE REPORT
A 32-year old male patient was admitted with hearing impairment in both sides that started about 5 weeks earlier. He was diagnosed as AS 8 years before admission. The diagnosis was made on inflammatory low back pain, HLA B-27 positivity, limitation of motion in lumbar spine, and bilateral sacroiliitis more than grade 2 by modified New York Criteria. He received biologics, such as tumor necrosis factor (TNF) inhibitors (adalimumab for 16 months, infliximab for 20 months, golimumab for 3 months and then etanercept for 15 months) and IL-17A inhibitor (secukinumab for 10 months). He had a history of being treated with multiple anti-TNF monoclonal anti-bodies, and received the IL-17A monoclonal antibody, se-cukinumab since 1 year ago. Until hospitalization, dis-ease activity of AS was controlled, c-reactive protein level and erythrocyte sedimentation rate were within the nor-mal range and score of Bath Ankylosing Spondylitis Disease Activity Index was 2.61, using secukinumab. Six
Neurosyphilis in Patient with Ankylosing Spondylitis
www.jrd.or.kr 279
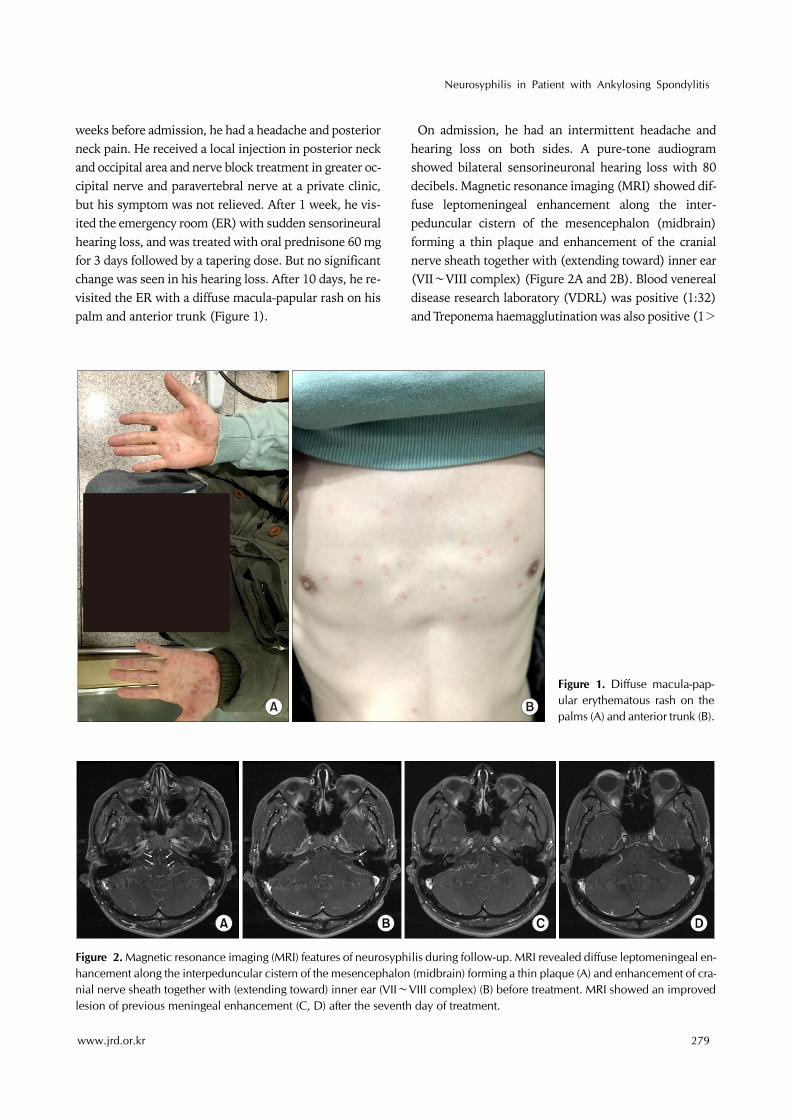
Figure 2. Magnetic resonance imaging (MRI) features of neurosyphilis during follow-up. MRI revealed diffuse leptomeningeal en-hancement along the interpeduncular cistern of the mesencephalon (midbrain) forming a thin plaque (A) and enhancement of cra-nial nerve sheath together with (extending toward) inner ear (VII∼VIII complex) (B) before treatment. MRI showed an improved lesion of previous meningeal enhancement (C, D) after the seventh day of treatment.
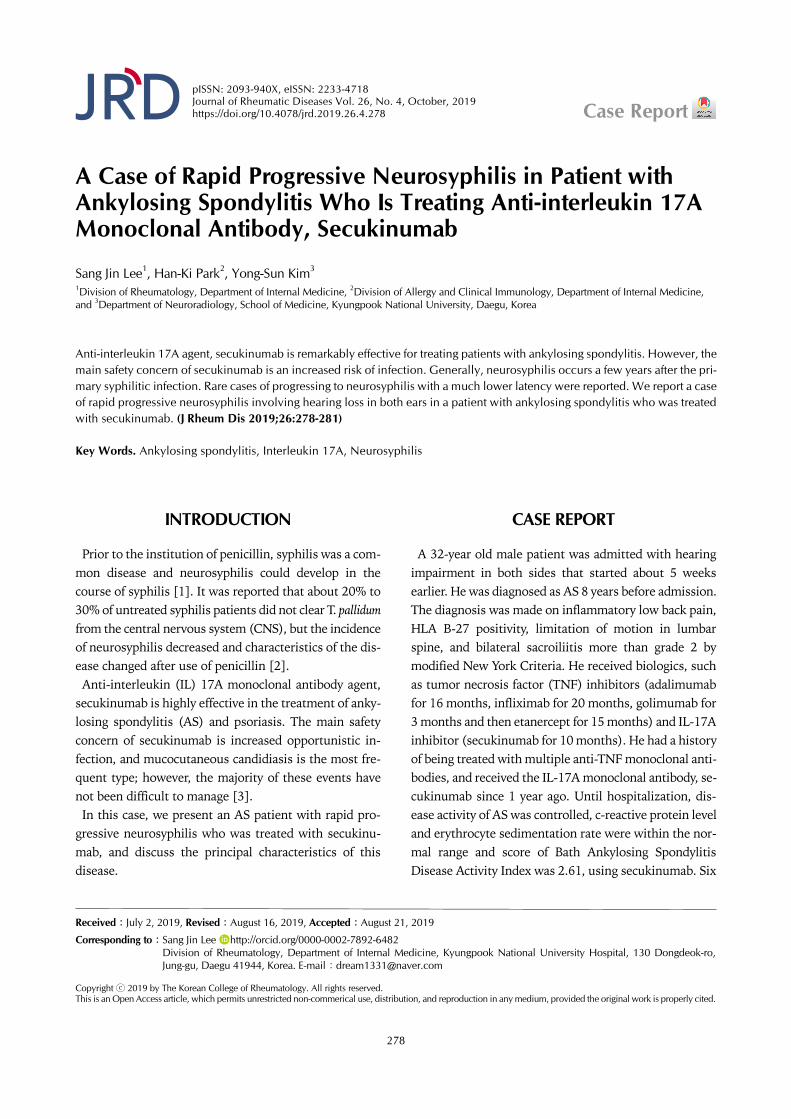
Figure 1. Diffuse macula-pap-ular erythematous rash on the palms (A) and anterior trunk (B).
weeks before admission, he had a headache and posterior neck pain. He received a local injection in posterior neck and occipital area and nerve block treatment in greater oc-cipital nerve and paravertebral nerve at a private clinic, but his symptom was not relieved. After 1 week, he vis-ited the emergency room (ER) with sudden sensorineural hearing loss, and was treated with oral prednisone 60 mg for 3 days followed by a tapering dose. But no significant change was seen in his hearing loss. After 10 days, he re-visited the ER with a diffuse macula-papular rash on his palm and anterior trunk (Figure 1).
On admission, he had an intermittent headache and hearing loss on both sides. A pure-tone audiogram showed bilateral sensorineuronal hearing loss with 80 decibels. Magnetic resonance imaging (MRI) showed dif-fuse leptomeningeal enhancement along the inter-peduncular cistern of the mesencephalon (midbrain) forming a thin plaque and enhancement of the cranial nerve sheath together with (extending toward) inner ear (VII∼VIII complex) (Figure 2A and 2B). Blood venereal disease research laboratory (VDRL) was positive (1:32) and Treponema haemagglutination was also positive (1>

Sang Jin Lee et al.
280 J Rheum Dis Vol. 26, No. 4, October, 2019
640). HIV testing was negative. Cerebrospinal fluid (CSF) contained 473/mm3 white blood cells (WBC) with one-third polymorphonuclear cells, a slightly elevated protein (1.32 g/L) with positive VDRL. The serological test was consistent with neurosyphilis. A careful ques-tioning of the patients revealed that he had sex with pros-titutes about 2 months prior to developing skin rash and after 1 month a painless genital ulcer formed and sponta-neously disappeared. He was treated with ceftriaxone 2 g bid intravenously for 14 days. After the seventh day of treatment, the disease activity was reevaluated. CSF anal-ysis showed a decreased WBC count (131/ mm3) and pro-tein (0.93 g/L), and his headache disappeared and pre-vious meningeal enhancement in MRI improved (Figure 2C and 2D). Three months after treatment, his hearing was gradually restored in pure-tone audiogram with 60 decibels and VDRL titer of serum was decreased (1:2). He was able to talk by hearing aids.
DISCUSSION
This patient had presented hearing loss on both sides si-multaneously with secondary syphilitic cutaneous le-sions following the administration of secukinumab. The cranial nerve palsies in this case were both auditory and likely due to meningeal enhancement of 8th nerve sheath, as shown in MRI. Syphilis in this patient shows a more ag-gressive natural course that included a decreased latency period before the onset of neurosyphilis and increased se-verity of the clinical manifestation in the setting of secuki-numab treatment. To the knowledge of the authors, secondary syphilis was
reported in two patients with AS who had receiving an-ti-TNF monoclonal antibody and neurosyphilis was re-ported in only one patient [4-6]. This case is the first re-port of neurosyphilis in patient with AS under an-ti-IL-17A monoclonal antibody, secukinumab. In the ab-sence of other immune deterioration such as HIV in-fection, secukinumab as well as continuous use of bio-logics seems to have caused rapid progressive neuro-syphilis development.Patients with neurosyphilis are classified into general
paresis, syphilitic meningitis, meningovascular, and ta-betic forms, based on their mode of clinical presentation [7]. General paresis was the most common form, which manifests cognitive impairment and behavior changes. Syphilitic meningitis belongs to this case and was the sec-ond most common form, followed by involvement of the
cranial nerve, mainly ocular and auditory. Meningovas-cular, which manifested as an ischemic event in the brain artery, and tabetic forms, which involved the spinal cord, showed similar incidence in neurosyphilis. While MRI may contribute to an anatomical lesion, neurosyphilis is still best classified by the nature of clinical manifestations [8]. T. pallidum invades to the CSF at a very early stage during
the infection. Because the number of patients with neuro-invasion (based on a CSF study) exceeded the number that developed symptomatic neurosyphilis, early in-vasion of the CNS with T. pallidum may be cleared by an in-flammatory response in most patients with syphilis, even with inadequate therapy [2]. It is reported that adaptive T cell immunity (T cells producing IFN-γ and IL-17) may contribute to the clearance of T. pallidum from the CSF [9,10]. Generally, neurosyphilis follows a few years after the primary infection, but rarely some patients have a much lower latency. The chancre and a maculopapular rash occurred with neurological manifestations at the same time in some immunocompromised patients in-cluding HIV [7,11]. It is reported that neurosyphilis usu-ally develops a more fulminant course in HIV patients, but the course of the disease is more insidious in im-munocompetent patients [1]. Similarly, our patient is al-so shown to have a rapid disease progression due to lack of IL-17.
SUMMARY
We report a case of rapid progressive neurosyphilis in a patient with ankylosing spondylitis who was treating with secukinumab. This case suggests that patients who are receiving the secukinumab should be cautious about the syphilis infection. Further investigations associated between IL-17 and syphilis are needed in the future.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.We received the patient’s consent form about publishing
all photographic materials.
AUTHOR CONTRIBUTIONS
S.J.L. conception and design of study. S.J.L., H.K.P., Y.S.K. acquisition of data. S.J.L., H.K.P., Y.S.K. analysis

Neurosyphilis in Patient with Ankylosing Spondylitis
www.jrd.or.kr 281
and/or interpretation of data. S.J.L., H.K.P., Y.S.K. draft-ing the manuscript. S.J.L., H.K.P., Y.S.K. revising the manuscript.
REFERENCES
1. Timmermans M, Carr J. Neurosyphilis in the modern era. J Neurol Neurosurg Psychiatry 2004;75:1727-30.
2. Marra CM. Neurosyphilis. Continuum (Minneap Minn) 2015;21(6 Neuroinfectious Disease):1714-28.
3. Langley RG, Kimball AB, Nak H, Xu W, Pangallo B, Osuntokun OO, et al. Long-term safety profile of ix-ekizumab in patients with moderate-to-severe plaque psor-iasis: an integrated analysis from 11 clinical trials. J Eur Acad Dermatol Venereol 2019;33:333-9.
4. Iglesias-Plaza A, Iglesias-Sancho M, Quintana-Codina M, García-Miguel J, Salleras-Redonnet M. Syphilis in the set-ting of anti-tumor necrosis factor alpha therapy. Reumatol Clin 2018 Feb 3 [Epub]. DOI: 10.1016/j.reuma.2017. 12.008.
5. Bories-Haffner C, Buche S, Paccou J. Secondary syphilis oc-curring under anti-TNFalpha therapy. Joint Bone Spine
2010;77:364-5.6. Assikar S, Doffoel-Hantz V, Sparsa A, Bonnetblanc JM.
Early neurosyphilis with etanercept treatment. Eur J Dermatol 2013;23:901-2
7. Drago F, Merlo G, Ciccarese G, Agnoletti AF, Cozzani E, Rebora A, et al. Changes in neurosyphilis presentation: a survey on 286 patients. J Eur Acad Dermatol Venereol 2016; 30:1886-900.
8. Nagappa M, Sinha S, Taly AB, Rao SL, Nagarathna S, Bindu PS, et al. Neurosyphilis: MRI features and their phenotypic correlation in a cohort of 35 patients from a tertiary care uni-versity hospital. Neuroradiology 2013;55:379-88.
9. Pastuszczak M, Jakiela B, Wielowieyska-Szybinska D, Jaworek AK, Zeman J, Wojas-Pelc A. Elevated cerebrospinal fluid interleukin-17A and interferon-γ levels in early asymptomatic neurosyphilis. Sex Transm Dis 2013;40: 808-12.
10. Stary G, Klein I, Brüggen MC, Kohlhofer S, Brunner PM, Spazierer D, et al. Host defense mechanisms in secondary syphilitic lesions: a role for IFN-gamma-/IL-17-producing CD8+ T cells? Am J Pathol 2010;177:2421-32.
11. Sadeghani K, Kallini JR, Khachemoune A. Neurosyphilis in a man with human immunodeficiency virus. J Clin Aesthet Dermatol 2014;7:35-40.