a case of successful limb salvage by wire guide thrombectomy
TRANSCRIPT

A case of successful limb salvageby wire guide thrombectomy
Kyoto university Graducate School of Medicine,D t t f C di l M di iDepartment of Cardiovascular Medicine
Nobuya Higashitani, Junichi Tazaki, Hirooki Higami, Yuko Morikami, Hiroki Shiomi, Masahiro Natsuaki, Akihiro Tokushige, Masao Imai, Naritatsu Saito, Takeshi Kimura
Kyoto university Graducate School of Medicine,Department of Cardiovascular Surgery
Senri Miwa, Ryuzo Sakata

Ptient was 74 years old man.
He was admitted to our hospital due to acute onset of rest pain,pallor and paralysis on his right legon his right leg.He had claudication on 100 meter walking 2 month ago.
he had history of esophageal cancer pharyngeal cancer and cervical spondylosis.
he has smoking habit 15/day.
Labo dataWBC:8000/μl, Hb:15.8g/dl, Hct:47.8%, Plt:19.1/μl, CPK:1394IU/l, LDH:236IU/l,/μ , / , / ,CRP:0.3mg/dlABGApH:7 52 pCO2:30 2mmHg pO2:98 2mmHgpH:7.52, pCO2:30.2mmHg, pO2:98.2mmHg,HCO3:24.1mmol, BE:2.3

How should we manage this patient?More than 6 hours had past from the onset but acidosis and necrosis didn’t progress.
•time past occlusion •thrombosis on severe chronic ASO such as collateral developedthrombosis on severe chronic ASO such as collateral developed
→ Emergency PTA
Which site is better for approach?•Antegrade approach is better for total occlusion lesion.•It is difficult to perform EVT with antegrade approach only. •Crossover approach from Lt femoral artery is difficult for occlusion from Rt iliac ostiumostium.
→ Lt brachial artery approach andRt femoral artery approach(US guided puncture)y pp ( g p )
3

Lt Brachial : 4.5Fr 120cm parent plus → Cruise + ExcersiorRt femoral US guided puncture → Cruise + Prograte
PTA
4

PTA Lt Brachial : 4.5Fr 120cm parent plus → Cruise + IVUS Rt femoral → 0.018 Treasure Floppy + Prograte

PTA1 Lt Brachial : 4.5Fr 120cm parent plus Rt femoral Prograte + 0.018 Treasure Floppy 300cm externalization
p/s Bandec 2.0×100mm dilatation

PTA1 Rt Femoral cut down → wire guide Fogary for EIA

PTA Lt Brachial : 4.5Fr 120cm parent plus Rt femoral Prograte + 0.018 Treasure Floppy 300cm externalization
Zilver 9.0×80mm Zilver 9.0×40mm

PTA1 Lt Brachial : 4.5Fr 120cm parent plus
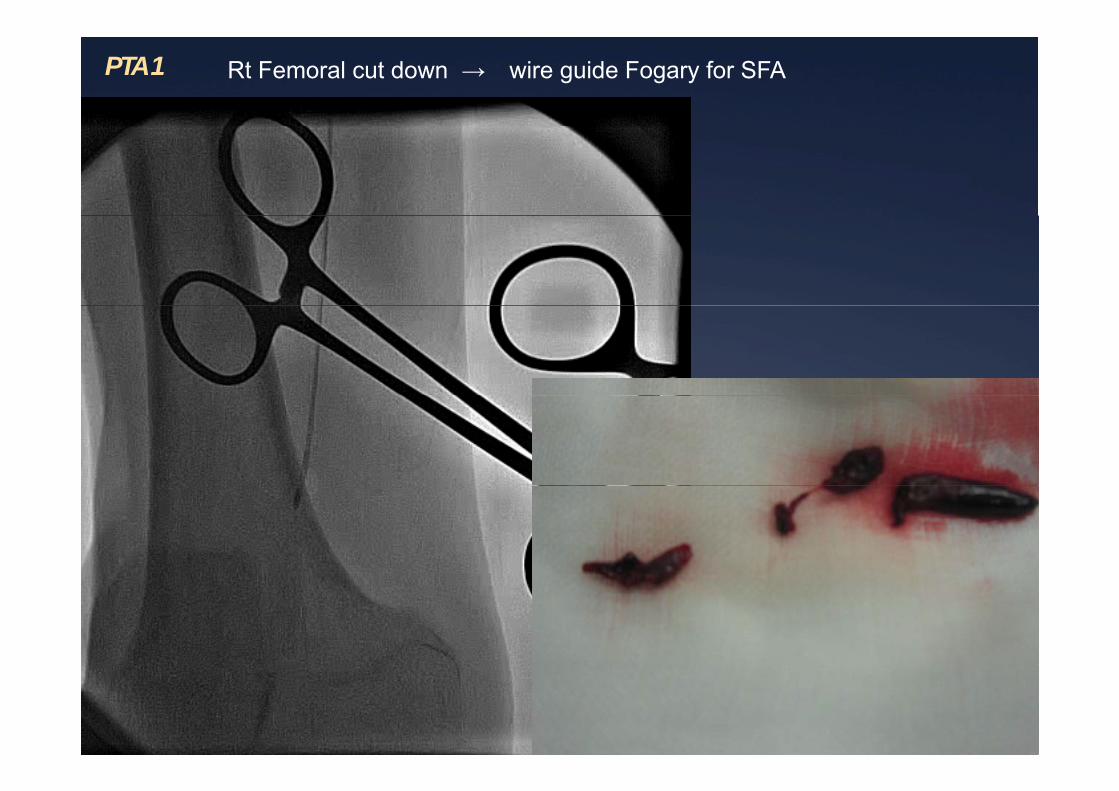
PTA1 Rt Femoral cut down → wire guide Fogary for SFA

Summary day14 CT
This case was not simple acute occlusion ,was thrombosis with chronic organic stenosis.
Therefore, the rich collateral circulation has Therefore, the rich collateral circulation has developed, using a combination of fogarty and PTA, the successful salvage.
After PTA CPK increased but improved After PTA, CPK increased, but improved immediately.
CT angiography on day 14 showed a good contrast to the toes and ABI was getting bettercontrast to the toes and ABI was getting better.
The patient is good and walk on own feet, today
CPK(IU/l)
11
ABI 0.82/0.94
day6day4day2day1 day8 day12

l iconclusion
We reported the successful limb salvage by wire guided thrombectomy
12