a comprehensive plan to preserve your greatest business asset – …/media/prudential/pdf/e... ·...
TRANSCRIPT

Protecting your employees is our priorityA comprehensive plan to preserve your greatest business asset – your employees.
PRUtreasures elite
Your relationships are precious.
Protect them.

Your employees are your organisation’s greatest assets.
Apart from providing them with income stability and career growth, you also want to ensure that their well-being and protection needs are cared for by your organisation.
With PRUtreasures elite, we have solutions to help you protect your employees from the financial impact of unforeseen illnesses and accidents. PRUtreasures elite provides you with the assurance that your employees will receive financial support during difficult times.
Your relationships are precious. Protect them.
Why do employees need help with healthcare?
54.8% of our total health expenditure is paid
out-of-pocket
Each day,
in Singapore are told that they have cancer
Sharp rise in numbers diagnosed with cancer
36 PEOPLESource: Singapore Cancer Society
Source: Aon Hewitt
15%in 2015
Gross Medical Inflation
Source: The World Bank: Out-of-pocket health expenditure, 2014

PRUtreasures elite | 02
How does PRUtreasures elite protect my employees against uncertainties?PRUtreasures elite – a comprehensive plan with affordable premiums.
We offer coverage ranging from protection against death, total and permanent disability, terminal illness and critical illness, as well as for hospitalisation, outpatient clinical and specialist, and even Traditional Chinese Medicine (TCM) treatments.
Comprehensive Solutions• High sum assured of up to $500,000 upon death, total and permanent disability or terminal illness
• Coverage of up to $250,000 upon diagnosis of any of the covered critical illnesses
• Coverage of up to 1-bedded wards in private hospitals
Affordable Premium• Competitive premium for coverage starting with minimal headcount
Guaranteed Coverage• Eligible employees enjoy guaranteed coverage of up to $150,000 for Group Term Life and up to $75,000 for Group Crisis Cover - Accelerated
Portfolio Pricing• Premiums are calculated based on the entire PRUtreasures elite portfolio. This means that claims made by an individual company will not adversely affect their premiums in the subsequent year
Convenience & Ease of Access• Cashless access at Prudential's panel of General Practitioners
• Go paperless and submit your claims online
Terms & Conditions apply. Please refer to www.prudential.com.sg/ptre for more details.

Benefits at a Glance
You can choose between the Group Term Life and Group Hospital & Surgical plans as your core plans. These plans, along with additional optional supplementary benefits, give you more options to customise an employee insurance scheme that can keep pace with their evolving needs.
03 | PRUtreasures elite
BENEFIT TYPE COVERAGE BENEFITS
Group Term Life (GTL) with Group Crisis Cover – Accelerated (GCCA)
(Applicable to Employee only)
• Death• Total and Permanent Disability (TPD)• Terminal Illness (TI)• Critical Illness (CI)
GTL• Lump sum payment of the sum assured upon death due to any cause, including illness and accident• Death, TI and TPD coverage is renewable up to age 74 last birthday• Payment of death benefit upon diagnosis of TI• 24-hour worldwide coverage GCCA• Lump sum payment upon diagnosis of any of the 37 critical illnesses Group Crisis Cover - Accelerated will cease upon payment of full sum assured• CI coverage is renewable up to age 69 last birthday• 24-hour worldwide coverage
Group Hospital & Surgical (GHS) with Group Extended Major Medical (GEMM)
(Applicable to Employee and Dependant)
• Reimbursement of medical expenses incurred as a result of hospitalisation or surgery due to a sickness or injury• Reimbursement of medical expenses in excess of GHS
• Reimbursement up to the respective benefit limits per disability• Covers outpatient kidney dialysis and cancer treatment on per policy year• Flexibility of choice of hospitals• Death benefit available• Reimbursement for medical expenses that exceed limit under the GHS plan
Group Accidental Death & Dismemberment (GADD)(Can be attached to either of the core plans)
(Applicable to Employee only)
• Accidental Death• Total dismemberment resulting from accidental injuries
• Lump sum payment of the sum assured upon accidental death• Lump sum payment (up to 150% of the sum assured) for any permanent disability set out in the Group Accidental Death & Dismemberment – Schedule of Indemnities • 24-hour worldwide coverage
Group Outpatient General Practitioner (GP) withGroup Outpatient Specialist (SP)(Can be attached only to GHS with GEMM)
(Applicable to Employee and Dependant)
• Reimbursement of outpatient medical expenses incurred in GP or SP clinics and diagnostic tests
GP• Clinical consultation at limits as stipulated in the Benefit Schedule SP• Specialist consultation at limits as stipulated in Benefit Schedule, subject to referral by GP• Diagnostic test, x-ray and laboratory test at limits as stipulated in Benefit Schedule, subject to referral by GP or SP
CO
RE
PLA
NS
OPT
ION
AL
SUPP
LEM
ENTA
RY B
ENEF
ITS

PRUtreasures elite | 04
BENEFITS / PLAN TYPE PLAN 11 PLAN 21 PLAN 3 PLAN 4 PLAN 5
Group Term Life (GTL) $500,000 $250,000 $150,000 $80,000 $50,000
Group Crisis Cover - Accelerated (GCCA) $250,000 $125,000 $75,000 $40,000 $25,000
Group Term Life with Group Crisis Cover - Accelerated (GTL+GCCA)
AGE LAST BIRTHDAY PLAN 1 PLAN 2 PLAN 3 PLAN 4 PLAN 5
16 - 19 744.00 388.00 240.00 128.00 80.004
20 - 24 744.00 388.00 240.00 128.00 80.00
25 - 29 744.00 388.00 240.00 128.00 80.00
30 - 34 865.00 451.00 279.00 149.00 93.00
35 - 39 1,163.00 606.00 375.00 200.00 125.00
40 - 44 1,981.00 1,033.00 639.00 341.00 213.00
45 - 49 3,097.00 1,615.00 999.00 533.00 333.00
50 - 54 4,743.00 2,474.00 1,530.00 816.00 510.00
55 - 59 7,998.00 4,171.00 2,580.00 1,376.00 860.00
60 - 64 13,299.00 6,936.00 4,290.00 2,288.00 1,430.00
65 - 693 20,646.00 10,767.00 6,660.00 3,552.00 2,220.00
70 - 743
(Group Term Life renewal only) 20,925.00 10,913.00 6,750.00 3,600.00 2,250.00
3 For renewals only.4 Sub rate.Note: Coverage for Group Crisis Cover - Accelerated benefit ceases at age 69 last birthday.
2 Payment under this condition is limited to 10% of the sum assured, subject to a maximum of $25,000.
Annual Premium Rate (S$)
Group Crisis Cover – Accelerated (GCCA) — List of 37 Critical Illnesses
1. Heart Attack2. Stroke3. Coronary Artery By-pass Surgery4. Major Cancers5. Kidney Failure6. Major Head Trauma7. Major Organ / Bone Marrow Transplantation8. Multiple Sclerosis9. Fulminant Hepatitis10. Primary Pulmonary Hypertension11. Blindness (Loss of Sight)12. Alzheimer’s Disease / Severe Dementia13. Surgery to the Aorta14. Coma15. Deafness (Loss of Hearing)16. Loss of speech17. Heart Valve Surgery18. Major Burns19. HIV Due to Blood Transfusion and Occupationally Acquired HIV
20. Motor Neurone Disease21. Parkinson’s Disease22. End Stage Liver Disease23. End Stage Lung Disease24. Aplastic Anaemia25. Muscular Dystrophy26. Bacterial Meningitis27. Benign Brain Tumour28. Viral Encephalitis29. Angioplasty and Other Invasive Treatment for Coronary Artery2
30. Poliomyelitis31. Systemic Lupus Erythematosus (Systemic Lupus Erythematosus with Lupus Nephritis)32. Other Serious Coronary Artery Disease33. Paralysis (Loss of use of Limbs)34. Apallic Syndrome35. Loss of Independent Existence36. Progressive Scleroderma37. Terminal Illness
1 Health declaration required.

05 | PRUtreasures elite
Group Hospital & Surgical with Group Extended Major Medical (GHS+GEMM)
GROUP EXTENDED MAJOR MEDICAL (GEMM)
BENEFIT SCHEDULE / PLAN TYPE PLAN 1 PLAN 2 PLAN 3 PLAN 4
Provides reimbursement of eligible expenses in excess of GHS if:• Hospitalisation is at least 20 days; or• Surgical Percentage is at least 75% per incision
$80,000 per disability
$60,000 per disability
$40,000 per disability
N.A.
Deductible As per GHS
Co-Insurance by Employee 20%
GROUP HOSPITAL AND SURGICAL (GHS)
BENEFIT SCHEDULE / PLAN TYPE (Maximum per any one disablity) PLAN 1 PLAN 2 PLAN 3 PLAN 4
1. Daily Room and Board Benefit (Maximum 120 days)
1 Bed Ward Private
2 Bed Ward Private
4 Bed Ward Private
4 Bed Ward Government Restructured
2. Intensive Care Unit (ICU) Benefit (Maximum 30 days)
$1,800 per day, up to $54,000 per disability
$1,200 per day, up to $36,000 per disability
$900 per day, up to $27,000 per disability
$15,000 per policy year
subject to 4 Bedded Room in a Singapore
Government or Restructured
Hospital
3. High Dependency Ward (Maximum 30 days)
$1,200 per day, up to $36,000 per disability
$800 per day, up to $24,000 per disability
$600 per day, up to $18,000 per disability
4. Other Hospital Services Benefits (Including implants)
$25,000 per disability for
items 4 to 8
$20,000 per disability for
items 4 to 8
$15,000 per disability for
items 4 to 8
5. Surgical Fees (Subject to Surgical Schedule for private hospitals)
6. In-Hospital Doctor's Consultation Benefit (Maximum 120 days)
7. Pre (90 days) & Post (90 days) Hospitalisation/ Surgery, Specialist Consultation, Diagnostic X-Ray and Lab Test, Traditional Chinese Medicine
8. Emergency Accidental Outpatient Treatment Benefit (Maximum per disability)
9. Miscarriage Benefit Covered under benefits (items 1 to 8), as per the respective benefit limits
10. Overseas Hospitalisation for Accident Benefit 150% of GHS limits (items 1 to 7)
11. Death Benefit $5,000
12. Outpatient Kidney Dialysis / Cancer Treatment (Maximum per policy year) $10,000 per policy year N.A.
Note: Benefits above are on reimbursement basis except item 11. Bed wards entitlements are for standard rooms (as categorised by the hospital) only and not applicable for luxury suites and special rooms.

PRUtreasures elite | 06
AGE LAST BIRTHDAY PLAN 1 PLAN 2 PLAN 3 PLAN 416 - 19 427.00 349.00 267.00 126.006
20 - 24 440.00 353.00 275.00 131.00
25 - 29 476.00 366.00 289.00 136.00
30 - 34 504.00 390.00 309.00 145.00
35 - 39 537.00 413.00 327.00 167.00
40 - 44 584.00 456.00 358.00 216.00
45 - 49 674.00 528.00 416.00 264.00
50 - 54 936.00 739.00 578.00 359.00
55 - 59 1,191.00 947.00 736.00 470.00
60 - 64 1,619.00 1,275.00 983.00 624.00
65 - 69 2,533.00 1,952.00 1,574.00 820.00
70 - 745 3,470.00 2,674.00 2,156.00 1,123.00
AGE LAST BIRTHDAY PLAN 1 PLAN 2 PLAN 3 PLAN 416 - 19 960.75 785.25 600.75 283.50
20 - 24 990.00 794.25 618.75 294.75
25 - 29 1,071.00 823.50 650.25 306.00
30 - 34 1,134.00 877.50 695.25 326.25
35 - 39 1,208.25 929.25 735.75 375.75
40 - 44 1,314.00 1,026.00 805.50 486.00
45 - 49 1,516.50 1,188.00 936.00 594.00
50 - 54 2,106.00 1,662.75 1,300.50 807.75
55 - 59 2,679.75 2,130.75 1,656.00 1,057.50
60 - 64 3,642.75 2,868.75 2,211.75 1,404.00
65 - 69 5,699.25 4,392.00 3,541.50 1,845.00
70 - 745 7,807.50 6,016.50 4,851.00 2,526.75
AGE LAST BIRTHDAY PLAN 1 PLAN 2 PLAN 3 PLAN 416 - 19 1,494.50 1,221.50 934.50 441.00
20 - 24 1,540.00 1,235.50 962.50 458.50
25 - 29 1,666.00 1,281.00 1,011.50 476.00
30 - 34 1,764.00 1,365.00 1,081.50 507.50
35 - 39 1,879.50 1,445.50 1,144.50 584.50
40 - 44 2,044.00 1,596.00 1,253.00 756.00
45 - 49 2,359.00 1,848.00 1,456.00 924.00
50 - 54 3,276.00 2,586.50 2,023.00 1,256.50
55 - 59 4,168.50 3,314.50 2,576.00 1,645.00
60 - 64 5,666.50 4,462.50 3,440.50 2,184.00
65 - 69 8,865.50 6,832.00 5,509.00 2,870.00
70 - 745 12,145.00 9,359.00 7,546.00 3,930.50
Annual Premium Rate (S$) – Group Hospital & Surgical with Group Extended Major Medical (GHS+GEMM)For Employee Only (inclusive of 7% GST)
For Employee and Spouse or Children Coverage Only (inclusive of 7% GST)
For Employees and Spouse and Children Coverage (inclusive of 7% GST)
5 For renewals only.6 Sub rate.

07 | PRUtreasures elite
Group Outpatient General Practitioner (GP)
BENEFIT SCHEDULE / PLAN TYPE PLAN 1 PLAN 2 PLAN 3 PLAN 4
Panel Registered Medical Practitioner Cashless
Non-Panel Registered Medical Practitioner (Covers treatment in Singapore only) Reimburse up to $30 per visit
Singapore Government Polyclinic Full Reimbursement
Accident and Emergency Department in Singapore Hospitals
Reimburse up to $100 per visit (Capped at 2 visits per policy year)
Overseas Registered Medical Practitioner Reimburse up to $100 per visit
Optional: Registered Traditional Chinese Medicine (TCM) Practitioner (Consultation and medication)
Reimburse up to $30 per visit (Capped at 6 visits per policy year)
Co-Payment Option of $0 / $5 co-payment
Group Outpatient Specialist (SP)
BENEFIT SCHEDULE / PLAN TYPE PLAN 1 PLAN 2 PLAN 3 PLAN 4
1. Specialist Consultation at Singapore Government Restructured Hospital (GRH) - GP referral required $2,000 per policy year
Overall policy year
limit of $500
2. Specialist Consultation at Private Hospital (PTE) - GP referral required
$800 per policy year
$400 per policy year
$200 per policy year
3. All other Diagnostic X-Ray and Lab Test - GP or SP referral required
$800 per policy year
$400 per policy year
$200 per policy year
Enhance Your PRUtreasures elite Plan According To Your Needs
PRUtreasures elite offers supplementary benefits to complement the core coverage. Depending on the core plans selected, you can choose up to 2 optional supplementary benefits to suit your company’s budget and needs.
Annual Premium Rate (S$) by Co-Payment and TCM Option – Group Outpatient General Practitioner with Group Outpatient Specialist (GP+SP)
WITH TCM BENEFIT (INCLUSIVE OF 7% GST) PLAN 1 PLAN 2 PLAN 3 PLAN 4
With $5 co-payment 458.00 437.00 420.00 376.00
Without $5 co-payment 495.00 474.00 457.00 413.00
WITHOUT TCM BENEFIT (INCLUSIVE OF 7% GST)
With $5 co-payment 410.00 389.00 372.00 328.007
Without $5 co-payment 447.00 426.00 409.00 365.00
7 Sub rate.
Note: Benefits above are on reimbursement basis.

PRUtreasures elite | 08
Group Accidental Death & Dismemberment (GADD)
BENEFITS / PLAN TYPE PLAN 1 PLAN 2 PLAN 3 PLAN 4 PLAN 5
Group Accidental Death & Dismemberment $500,000 $250,000 $150,000 $80,000 $50,000
Group Accidental Death & Dismemberment (GADD) — Schedule of Indemnities
TYPE OF INJURY PERCENTAGE OF SUM ASSURED
Accidental Death Benefit
1. Accidental Death 100%
Dismemberment Benefits
2. Totally and Permanently Disabled 150%
3. Total and irrecoverable loss of the effective use of sight in one eye and any one limb 150%
4. Total and irrecoverable loss of the effective use of speech and hearing 150%
5. Total and irrecoverable loss of the effective use of all sight in both eyes 150%
Sight: Total and irrecoverable loss of the effective use of:
6. all sight in one eye 100%
7. lens in one eye 50%
Hearing:
8. Total and irrecoverable loss of the effective use of hearing in both ears 75%
9. Total and irrecoverable loss of the effective use of hearing in one ear 25%
10. Loss by physical severance of both ears 6%
11. Loss by physical severance of one ear 3%
Speech:
12. Total and irrecoverable loss of the effective use of power of speech 50%
Limbs: Total and irrecoverable loss of the effective use of:
13. two limbs 150%
14. one limb 125%
Hand: Total and irrecoverable loss of the effective use of:
15. four fingers and thumb of both hands 100%
16. four fingers and thumb of one hand 60%
17. four fingers of one hand 35%
18. both phalanges of one thumb 25%
19. one phalanx of one thumb 12.5%
20. three phalanges of a finger 9%
21. two phalanges of a finger 6.5%
22. one phalanx of a finger 3.5%
Leg:
23. Fractured leg or patella, with established non-union 10%
24. Shortening of leg by at least 5 cm 7.5%
Foot: Total and irrecoverable loss of the effective use of:
25. all toes of one foot 15%
26. two phalanges of one great toe 5%
27. one phalanx of one great toe 3%
28. one toe other than the great toe 1%

09 | PRUtreasures elite
Annual Premium Rate (S$)
Occupational Class 1 (inclusive of 7% GST)
Occupational Class 2 (inclusive of 7% GST)
Occupational Class 3 (inclusive of 7% GST)
AGE LAST BIRTHDAY PLAN 1 PLAN 2 PLAN 3 PLAN 4 PLAN 5
16 - 69 192.00 96.00 57.00 31.00 19.009
70 - 748 820.00 410.00 246.00 131.00 82.00
AGE LAST BIRTHDAY PLAN 1 PLAN 2 PLAN 3 PLAN 4 PLAN 5
16 - 69 240.00 120.00 72.00 38.00 24.00
70 - 748 1,025.00 512.00 307.00 164.00 102.00
AGE LAST BIRTHDAY PLAN 1 PLAN 2 PLAN 3 PLAN 4 PLAN 5
16 - 69 335.00 168.00 101.00 54.00 34.00
70 - 748 1,435.00 717.00 430.00 230.00 143.00
Call your Prudential Financial Consultant or our PruCustomer Line at 1800 333 0 333 today, or visit www.prudential.com.sg
8 For renewals only.9 Sub rate.
Occupational Class
Class 1 : Clerical, administrative or other similar non-hazardous occupations
Class 2 : Occupations where some degree of risk is involved, e.g. supervision of manual workers,
totally administrative job in an industrial environment
Class 3 : Occupations involving regular light to medium manual work but no substantial hazard
which may increase the risk of sickness or accident
Class 4 : Not covered
PRUtreasures elite | 10
Underwriting Guidelines for PRUtreasures elite
Period of Insurance:
• Duration of coverage is for 12 months. Coverage starts from stated effective date upon clearance of required MAS 314 and Compliance checks.
Age Eligibility:
1) Employees• All benefits, except Group Crisis Cover - Accelerated, are available to eligible employees of age 16 to 69 inclusive, and
renewable up to age 74.• Group Crisis Cover - Accelerated is available to eligible employees of age 16 to 64 inclusive, and renewable up to age 69.
2) DependantsA) the Insured Member’s spouse who is: - below 69 years old at his last birthday, and up to 74 years old at his last birthday; and - not an Insured Member under this Policy; orB) the Insured Member’s natural or step child from a legal marriage or legally adopted child who is: - two (2) weeks old; or - up to 25 years old at his last birthday, and is single and unemployed. (Note: National Service Personnel are not covered)
• Based on age last birthday.
Eligibility and Participation Requirements:
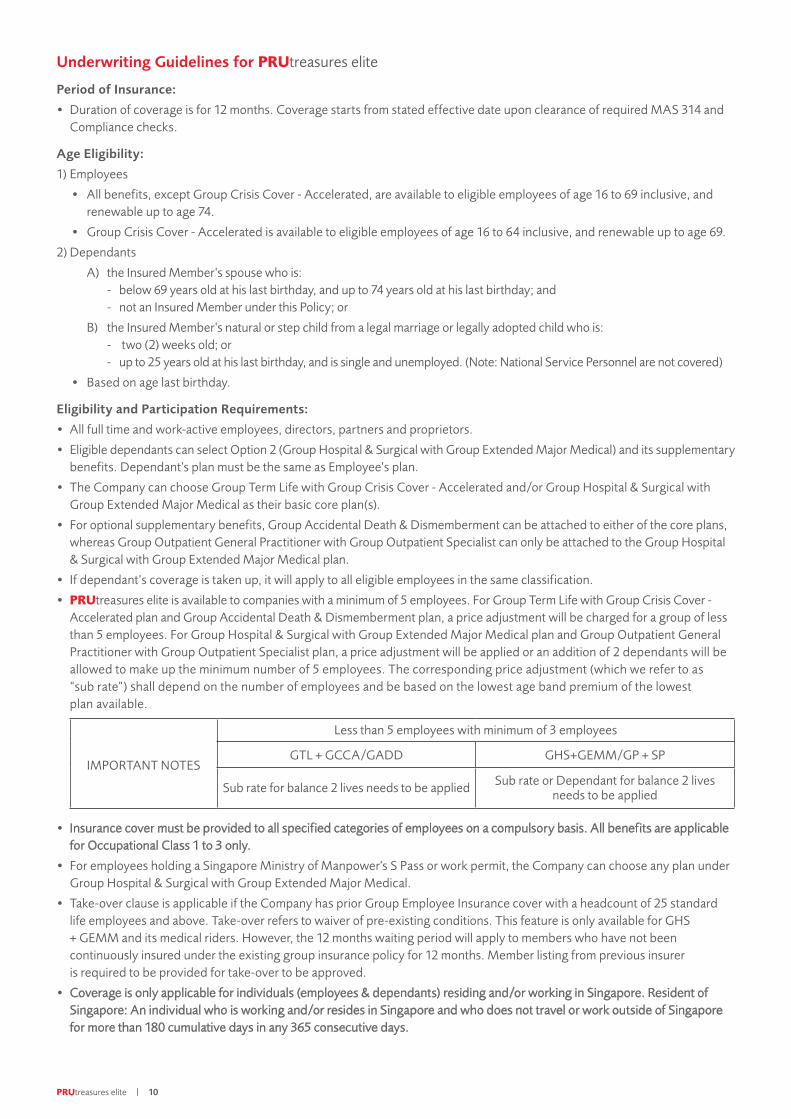
• All full time and work-active employees, directors, partners and proprietors.• Eligible dependants can select Option 2 (Group Hospital & Surgical with Group Extended Major Medical) and its supplementary benefits. Dependant's plan must be the same as Employee’s plan.• The Company can choose Group Term Life with Group Crisis Cover - Accelerated and/or Group Hospital & Surgical with Group Extended Major Medical as their basic core plan(s).• For optional supplementary benefits, Group Accidental Death & Dismemberment can be attached to either of the core plans, whereas Group Outpatient General Practitioner with Group Outpatient Specialist can only be attached to the Group Hospital & Surgical with Group Extended Major Medical plan.• If dependant’s coverage is taken up, it will apply to all eligible employees in the same classification.• PRUtreasures elite is available to companies with a minimum of 5 employees. For Group Term Life with Group Crisis Cover - Accelerated plan and Group Accidental Death & Dismemberment plan, a price adjustment will be charged for a group of less than 5 employees. For Group Hospital & Surgical with Group Extended Major Medical plan and Group Outpatient General Practitioner with Group Outpatient Specialist plan, a price adjustment will be applied or an addition of 2 dependants will be allowed to make up the minimum number of 5 employees. The corresponding price adjustment (which we refer to as “sub rate”) shall depend on the number of employees and be based on the lowest age band premium of the lowest plan available.
IMPORTANT NOTES
Less than 5 employees with minimum of 3 employees
GTL + GCCA/GADD GHS+GEMM/GP + SP
Sub rate for balance 2 lives needs to be applied Sub rate or Dependant for balance 2 lives needs to be applied
• Insurance cover must be provided to all specified categories of employees on a compulsory basis. All benefits are applicable for Occupational Class 1 to 3 only.• For employees holding a Singapore Ministry of Manpower's S Pass or work permit, the Company can choose any plan under Group Hospital & Surgical with Group Extended Major Medical.• Take-over clause is applicable if the Company has prior Group Employee Insurance cover with a headcount of 25 standard
life employees and above. Take-over refers to waiver of pre-existing conditions. This feature is only available for GHS + GEMM and its medical riders. However, the 12 months waiting period will apply to members who have not been continuously insured under the existing group insurance policy for 12 months. Member listing from previous insurer is required to be provided for take-over to be approved.
• Coverage is only applicable for individuals (employees & dependants) residing and/or working in Singapore. Resident of Singapore: An individual who is working and/or resides in Singapore and who does not travel or work outside of Singapore for more than 180 cumulative days in any 365 consecutive days.

11 | PRUtreasures elite
Pre-Existing Conditions – Group Hospital & Surgical with Group Extended Major Medical:
• Shall not pay if the loss or disability arises out of a pre-existing condition, unless the insured member has been insured under this policy continuously for 12 months.• All pre-existing conditions are permanently excluded for outpatient kidney dialysis or outpatient cancer treatment benefits.
Pre-Existing conditions – Group Term Life with Group Crisis Cover - Accelerated:
1) Group Term Life• Shall not pay if the loss or disability arises out of a pre-existing condition, unless the insured member has been insured
under this policy continuously for 12 months.2) Group Crisis Cover - Accelerated
• Shall not pay if the loss or disability arises out of a pre-existing condition.
Premium:
• Premium rates are in Singapore Dollars.• The premium rates are based on age last birthday of individual employees.• Payment of premium is to be made annually.
Medical Underwriting:
• Employee (16 to 64 age last birthday) selecting Plan 1 & 2 of Group Term Life with Group Crisis Cover – Accelerated will require underwriting. The employee will be covered and invoiced at Plan 3 sum assured (i.e $150,000) while pending for fulfillment of underwriting or coverage assessed to be of non-standard rating subsequently.
• Employee (from 65 age last birthday onwards) selecting Group Term Life will require underwriting.• For Group Term Life, employee of 70 to 74 age last birthday will require underwriting at each renewal.
Required Documents:
• Application Form.• A copy of the duly completed, company stamped and signed MAS Notice 314 Declaration on Parties Relevant to the
Policyholder Form.• Business Profile report from the Account & Corporate Regulatory Authority (ACRA).• Health Declaration Form when Medical Underwriting is required.
Note:
You are recommended to seek advice from a qualified Prudential Financial Consultant for a financial analysis before purchasing a policy suitable to meet your needs.
This plan has no cash value. Buying health insurance products that are not suitable for you may impact your ability to finance your future healthcare needs. Premiums are not guaranteed and may be adjusted based on future claims experience.
This brochure is for reference only and is not a contract of insurance. Please refer to the exact terms and conditions, specific details and exclusions applicable to these insurance products in the policy documents that can be obtained from your Prudential Financial Consultant.
This brochure is for distribution in Singapore only and shall not be construed as an offer to sell or solicitation to buy or provision of any insurance product outside Singapore.
Information is correct as at 12 July 2017.

Dec
lara
tio
n
Plea
se re
ad c
aref
ully
bef
ore
signi
ng th
is P
RU
trea
sure
s el
ite a
pplic
atio
n fo
rm.
I und
erst
and
that
the
assu
ranc
e w
ill no
t com
men
ce u
ntil
the
prop
osal
has
bee
n of
ficia
lly a
ccep
ted
by P
rude
ntia
l Ass
uran
ce C
ompa
ny S
inga
pore
(Pte
) Lim
ited
("Pru
dent
ial S
inga
pore
"), p
rem
ium
s ha
ve b
een
paid
and
an
offic
ial l
ette
r ind
icat
ing
cove
r has
com
men
ced
has b
een
issue
d. I
decl
are
that
the
info
rmat
ion
give
n in
this
form
and
any
info
rmat
ion
supp
lied
to P
rude
ntia
l Sin
gapo
re o
r the
Med
ical
Exa
min
er o
f Pru
dent
ial S
inga
pore
is tr
ue, a
nd th
at n
o m
ater
ial f
acts
, tha
t is,
fact
s lik
ely
to in
fluen
ce th
e as
sess
men
t and
acc
epta
nce
of th
is pr
opos
al, h
ave
been
with
held
and
to th
e be
st o
f my
know
ledg
e an
d be
lief t
he in
form
atio
n gi
ven
here
in is
true
and
com
plet
e. I
agre
e to
pay
Pru
dent
ial S
inga
pore
the
amou
nt o
f any
med
ical
fee
incu
rred
shou
ld I
fail t
o ta
ke u
p th
e co
vera
ge a
fter t
he d
ate
of P
rude
ntia
l Sin
gapo
re's
lette
r not
ifyin
g m
e of
the
acce
ptan
ce o
f the
pro
posa
l's st
anda
rd ra
tes.
We
decl
are
and
conf
irm th
at o
ur e
mpl
oyee
s hav
e gi
ven
us th
eir c
onse
nt to
Pru
dent
ial S
inga
pore
, its
offi
cers
and
em
ploy
ees,
in c
olle
ctin
g, u
sing
and
disc
losin
g an
y an
d al
l info
rmat
ion
rela
ting
to th
em in
this
form
to a
ny o
f Pru
dent
ial S
inga
pore
's co
ntra
ctor
s or t
hird
par
ty se
rvic
e pr
ovid
ers o
r dist
ribut
ion
partn
ers,
any
regu
lato
ry, s
uper
viso
ry o
r oth
er a
utho
rity,
cou
rt of
law
, for
the
purp
ose(
s) o
f und
erw
ritin
g, c
laim
s ass
essm
ent a
nd c
usto
mer
serv
icin
g.
Nam
e of
("C
ompa
ny")
:
Com
pany
Add
ress
:
Nat
ure
of B
usin
ess
:
Effe
ctiv
e da
te o
f Pol
icy (D
D/M
M/Y
Y) :
(d
ate
mus
t be
on o
r afte
r the
dat
e of
app
licat
ion)
Effe
ctiv
e da
te o
f new
em
ploy
ees
: □
on
the
date
of e
mpl
oym
ent O
R
□
m
onth
s fro
m th
e da
te o
f em
ploy
men
t
Che
cklis
t of
Req
uire
d D
ocum
ents
□ A
pplic
atio
n Fo
rm
□ A
cop
y of
the
duly
com
plet
ed, c
ompa
ny st
ampe
d an
d sig
ned
MA
S N
otic
e 31
4 D
ecla
ratio
n on
Par
ties R
elev
ant t
o th
e
Polic
yhol
der F
orm
and
MA
S 31
4 D
ecla
ratio
n on
Ben
efic
ial O
wne
r(s)
For
m (i
n th
e ev
ent t
hat t
here
are
Cor
pora
te
Sh
areh
olde
rsOwning
≥25%
ofthe
com
pany).
□Health
Declaratio
n(App
licableifGTL
Plan1or2isse
lected
orm
edicalund
erwritingisrequ
ired)
Nam
e of
Aut
horis
ed S
igna
tory
:
Des
igna
tion
:
HR
Emai
l Add
ress
:
HR
Con
tact
No
: D
ate
of A
pplic
atio
n :
Com
pany
Sta
mp
: S
igna
ture
of A
utho
rised
Sig
nato
ry :
Nam
e of
Fin
anci
al C
onsu
ltant
:
Fina
ncia
l Con
sulta
nt C
ode
: L
ocat
ion
:
Con
tact
No
: S
igna
ture
:
□
Tick
whe
re a
ppro
pria
te
If a
mat
eria
l fa
ct i
s no
t d
iscl
osed
in
this
pro
pos
al,
any
pol
icy
issu
ed m
ay n
ot b
e va
lid.
If y
ou a
re i
n d
oub
t as
to
whe
ther
a f
act
is
mat
eria
l, yo
u ar
e ad
vise
d t
o d
iscl
ose
it. T
his
incl
udes
any
info
rmat
ion
that
you
may
hav
e p
rovi
ded
to
the
agen
t b
ut w
as n
ot in
clud
ed
in t
he p
rop
osal
. Pl
ease
che
ck t
o en
sure
you
are
ful
ly s
atis
fied
wit
h th
e in
form
atio
n d
ecla
red
in t
his
pro
pos
al.
WA
RN
ING
: PU
RSU
AN
T TO
SEC
TIO
N 2
5(5)
OF
THE
INSU
RA
NC
E A
CT
(CA
P 14
2), Y
OU
AR
E TO
DIS
CLO
SE IN
TH
IS A
PPLI
CA
TIO
N F
OR
M F
ULL
Y A
ND
FA
ITH
FULL
Y A
LL T
HE
FAC
TS W
HIC
H
YOU
KN
OW
OR
OU
GH
T TO
KN
OW
, OTH
ERW
ISE
YOU
MA
Y R
ECEI
VE
NO
THIN
G F
RO
M T
HE
POLI
CY.
PRU
trea
sure
s el
ite A
PPLI
CAT
ION
FO
RM
PruC
usto
mer
Lin
e: 1
800-
333
0 33
3
CO
RE
OPT
ION
S
□ G
TL (G
roup
Ter
m L
ife) +
GC
CA
(Gro
up C
risis
Cov
er -
Acc
eler
ated
) A
□ G
AD
D (G
roup
Acc
iden
tal D
eath
& D
ismem
berm
ent)
□ G
HS
(Gro
up H
ospi
tal &
Sur
gica
l Pla
n) +
GEM
M (G
roup
Ext
ende
d M
ajor M
edica
l)A
□ G
AD
D (G
roup
Acc
iden
tal D
eath
& D
ismem
berm
ent)
B □
GP
+ SP
(Gro
up O
utpa
tient
Gen
eral
Pra
ctiti
oner
with
Gro
up O
utpa
tient
Spe
cial
ist)
Cho
ice
of O
ptio
ns

DECLARATION BY COMPANY
I / We hereby declare that, to the best of my / our knowledge and belief, the information given here is true and complete, and agree that if a contract of insurance is effected, all information submitted in connection with this application shall form the basis of such contract between the Company and the Insurer.
___________________________________________________Signature & Name of Authorised Officer
NRIC / Passport no. : ______________________________
Designation : ______________________________
Company Stamp : ______________________________
DECLARATION BY INSURANCE REPRESENTATIVE
I / We hereby declare and acknowledge that I / we have reviewed this form with the authorised officer of the Company, and that I / we have verified that all information in this form is true and complete.
___________________________________________________Signature & Name of Insurance Representative
NRIC / Passport no. : ______________________________
Agency Code : ______________________________
Agency Location : ______________________________
Note: Premium amounts may differ due to the rounding factor. Please pay the stated amount based on the Premium Notice.
No.Name
(Please underline surname)
NRIC / Passport
no.
Gender (M/F)
DOB (DD/MM/
YYYY)
Age Last Birthday
Marital Status Occupation Dependants
(S/C) NationalityBased in
Singapore? (Y/N)
Date of Employment
Corporate Email Address (Please note that e-claims can only be set up for employees
with corporate email
addresses)
GTL + GCCA (Core) (Employee Only) GHS + GEMM (Core)
GADD (Option A) to GTL + GCCA / GHS + GEMM
Core (per pax)
GP+SP (Option B) to GHS + GEMM Core (per pax)
Plan no. Premium Plan no.
Plan Type
No. of Dependants Covered for
GHS (Input if
Plan Type is not
EmployeeOnly)
Total Lives Premium Plan
no.Occupational
Class Premium Plan no.
With TCM (Y/N)
With Co-Payment
(Y/N)
No. of Dependants Covered for
GP+SP
Premium
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
Total Amount Payable: $
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
To be completed
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
(Excel calculator can be used to
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
To be completed
(Excel calculator can be used to
To be completed
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)
replace this hard copy form)

MAS NOTICE 314 DECLARATION ON PARTIES RELEVANT TO THE POLICYHOLDERProposal / Policy Number
The information requested in this form must be provided in order to comply with the mandatory requirements of MAS Notice 314 – Preventing Money Laundering and Countering the Financing of Terrorism – Life Insurance (MAS 314).
The personal data collected in this form, in other documents or provided to Prudential Assurance Company Singapore (Pte) Limited (“Prudential”) shall be used for the purposes stated in the proposal form and Prudential’s Privacy Notice (which is available at www.prudential.com.sg). The personal data may be collected, used and/or disclosed by Prudential, its officers, associated organisation(s) employees, representatires(s), third party distributors and other organisations stated in Prudential's Privacy Notice whether in Singapore or outside Singapore.
(A) Name of Policyholder / Insured Company(ies) / Assignee(s) / Applicant(s) / Beneficiary(ies) (delete accordingly)
(B) Principal Place of Business (“PPOB”) (if different from registered or business address provided). PPOB refers to the main operating office where the senior management of the policyholder resides.
Is the PPOB different from the registered or business address □ Yes □ NoIf yes, please provide PPOB in the space provided
(C) Information on Chairman / CEO / Managing Partner of the company(ies) stated in (A):
Full Name (including any aliases : (1) Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Designation : Chairman / CEO / Managing Partner (delete accordingly) Company Name :
NRIC / Passport No. :
Date of Birth :
Nationality :
(2) Mr / Mrs / Ms / Mdm (delete accordingly)
Chairman / CEO / Managing Partner (delete accordingly)
Full Name (including any aliases : (1) Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Designation : Chairman / CEO / Managing Partner (delete accordingly) Company Name :
NRIC / Passport No. :
Date of Birth :
Nationality :
(2) Mr / Mrs / Ms / Mdm (delete accordingly)
Chairman / CEO / Managing Partner (delete accordingly)
Full Name (including any aliases : (1) Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Designation : Chairman / CEO / Managing Partner (delete accordingly) Company Name :
NRIC / Passport No. :
Date of Birth :
Nationality :
(2) Mr / Mrs / Ms / Mdm (delete accordingly)
Chairman / CEO / Managing Partner (delete accordingly)
Page 1 of 2
PruCustomer Line: 1800-333 0 333
Continued next pageVersion Aug 2016

Page 2 of 2
MAS NOTICE 314 DECLARATION ON PARTIES RELEVANT TO THE POLICYHOLDERProposal / Policy Number
(D) Person(s) authorised to act on matters relating to the purchase of the Policy / assigned Policy
Is the representative(s) signing on the proposal /application / assignment form the only authorised person(s) to act on matters relating to the Policy(s)?□ Yes □ NoIf No, please provide the other authorised person(s) appointed to act on matters relating to the policy(s) in the fields below:
Full Name (including any aliases : Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Designation :
NRIC / Passport No. :
Date of Birth :
Nationality :
Country of Residence :
Signature:
Company Name:
Full Name (including any aliases : Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Designation :
NRIC / Passport No. :
Date of Birth :
Nationality :
Country of Residence :
Signature:
Company Name:
Full Name (including any aliases : Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Designation :
NRIC / Passport No. :
Date of Birth :
Nationality :
Country of Residence :
Signature:
Company Name:
Note: Please complete a separate form, signed by the Representative, if fields provided are insufficient under items (A) - (D).
Declaration
Declaration by Representative of the policyholder / insured company / assignee /applicant / beneficiary / trustee (This Representative could be the CEO, Directors (listed in the ACRA), Managing Director, Partner or Managing Partner of the company/policyholder)
I declare that the information given in this form is complete and accurate. I shall promptly inform Prudential of changes to such natural person’s information in this form. I acknowledge and agree that if the information disclosed in this form is incomplete and/or inaccurate, some or all of the benefits under the policy issued to the Policyholder may not be available. I further acknowledge and agree that Prudential has the right to request supporting documents in relation to the information disclosed in this form.
Full Name (including any aliases as per identification document) :
Designation :
Company Name :
NRIC / Passport No. :
Nationality :
Country of Residence :
Signature with company stamp:
Date:
Version Aug 2016
MAS 314 DECLARATION ON BENEFICIAL OWNER(S)
Page 1 of 2
Continued next page
Proposal / Policy Number
The information requested in this form must be provided in order to comply with the mandatory requirements of MAS Notice 314 – Preventing Money Laundering and Countering the Financing of Terrorism – Life Insurance (MAS 314).
The personal data collected in this form, in other documents or provided to Prudential Assurance Company Singapore (Pte) Limited (“Prudential”) shall be used for the purposes stated in the proposal form and Prudential’s Privacy Notice (which is available at www.prudential.com.sg). The personal data may be collected, used and/or disclosed by Prudential, its officers, associated organisation(s), employees, representative(s), third party distributors and other organisations stated in Prudential’s Privacy Notice whether in Singapore or outside Singapore.
(I) Name of Policyholder / Insured Company(ies) / Assignee(s) / Applicant(s) / Beneficiary(ies) (delete accordingly)
(II) Beneficiary owner(s) is either a
(a) naturalpersonwhoultimatelyownsorcontrolsthebeneficiary proposer assignee applicant(withshareholdingof≥25%ofthecompany’s ordinary shares) or the natural person on whose behalf business relations are established; or
(b) natural person who does not meet the shareholder threshold and who exercises significant influence (i.e. board of directors of corporate shareholder owing the policyholder, person financing the policy) over the beneficiary /proposer /assignee /applicant.
(III) Information on all shareholder(s) or ultimate shareholder who are non-natural person with shareholding of ≥25% of the ordinary shares of company stated in (I):
Section (A): orporateShareholder(s)( SH )directlyowning≥25%ofthepolicyholder
(1) Name of Corporate Shareholder (“CSH”) (2) Percentage of shareholding
A1
A2
A3
A4
( ) %
( ) %
( ) %
( ) %
Section (B): SHsowning≥25%ofthepolicyholderthroughordinarysharesof SHslistedin(A)
(3) Name of CSH(B) owing CSH(A) listed in section (A)
B1
B2
B3
B4
A( )
A( )
A( )
A( )
%
%
%
%
( ) Pleaseindicatewithinthebrac etthecorrespondingnumberinPart Section(A). nthee entthatthereare SHsowning≥25%ofthecompanyinSection please provide their details on a separate form signed by the Representative.
(IV) Details of all beneficial owner(s) as defined in (II) of the companies listed in Part (III) A and/or B or any natural person who exercise significant influence over the Policyholder(s) / Insured Companies / Assignee(s) / Applicant(s) / Beneficiary(ies).
Full Name (including any aliases : Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Relationship to the Policyholder :
NRIC / Passport No. :
Date of Birth :
Nationality :
Country of Residence :
Percentage of Shareholding (ordinary shares):
Name of company:
PruCustomer Line: 1800-333 0 333
Version Aug 2016

Proposal / Policy Number
Full Name (including any aliases : Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Relationship to the policyholder :
NRIC / Passport No. :
Date of Birth :
Nationality :
Country of Residence :
Percentage of Shareholding (ordinary shares):
Name of Company:
Full Name (including any aliases : Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Relationship to the policyholder :
NRIC / Passport No. :
Date of Birth :
Nationality :
Country of Residence :
Percentage of Shareholding (ordinary shares):
Name of Company:
Full Name (including any aliases : Mr / Mrs / Ms / Mdm (delete accordingly) as per identification document)
Relationship to the policyholder :
NRIC / Passport No. :
Date of Birth :
Nationality :
Country of Residence :
Percentage of Shareholding (ordinary shares):
Name of Company:
Note: Please complete a separate form, signed by the Representative, if fields provided are insufficient.
Declaration
Declaration by Representative of the policyholder / insured company / assignee /applicant / beneficiary / trustee (This Representative could be the CEO, Directors (listed in the ACRA), Managing Director, Partner or Managing Partner of the company/policyholder)
I declare that the information given in this form is complete and accurate. I shall promptly inform Prudential of changes to such natural person’s information in this form. I acknowledge and agree that if the information disclosed in this form is incomplete and/or inaccurate, some or all of the benefits under the policy issued to the Policyholder may not be available. I further acknowledge and agree that Prudential has the right to request supporting documents in relation to the information disclosed in this form.
Full Name of Representative (including any aliases as per identification document) :
Designation :
Company Name :
NRIC / Passport No. :
Nationality :
Country of Residence :
Signature with company stamp:
Date:
Page 2 of 2
MAS 314 DECLARATION ON BENEFICIAL OWNER(S)
Version Aug 2016

GROUP HEALTH DECLARATION
WARNING: YOU ARE REQUIRED TO FULLY AND FAITHFULLY DISCLOSE ALL THE FACTS THAT YOU KNOW OR OUGHT TO KNOW. OTHERWISE, YOUR INSURANCE COVERAGE PROVIDED UNDER THIS PLAN MAY BE VOID.
Name of Company Group Policy No.
Details of Employee
Full Name of Employee in Block (as shown in NRIC - underline surname) NRIC/FIN/Passport No.
Date of Birth
Gender
Male / Female
Maritial Status
Occupation Date of Employment
Monthly Salary
S$
Country of Residence Nationality Height (cm) Weight (kg)
Details of Dependant(s) (to be completed if dependants are covered)
Full Name in Block NRIC/FIN/Passport No.
Date of Birth(DD/MM/YYYY)
Gender(M/F) Occupation Height
(cm)Weight
(kg) Nationality
Spouse
Child 1
Child 2
Child 3
Health Declaration
(All questions must be answered and any alteration must be signed) Employee Spouse Child 1 Child 2 Child 3
Yes No Yes No Yes No Yes No Yes No
1. Do you engage in military or private flying other than as passenger travelling solely for transport or in hazardous pursuits such as but not limited to scuba diving, mountain and climbing sport, free fall parachuting, sky diving and motor racing.
If ‘Yes’, please state details on activity, depth dived, locations and frequency in the box provided on the right.
□ □ □ □ □ □ □ □ □ □
2. Have you taken narcotics, any habit forming drugs or ever been treated for drug or alcohol addiction?
If ‘Yes’, please provide details including name of substance, date, treatment, name & address of doctor in the box provided on the right.
□ □ □ □ □ □ □ □ □ □
PTREFOR OFFICE USE ONLY
GTL/TPD GCCA
Sum Assured
Sum Assured (FCL)
Page 1 of 4
PruCustomer Line: 1800-333 0 333
Continued next page

GROUP HEALTH DECLARATIONHealth Declaration
(All questions must be answered and any alteration must be signed) Employee Spouse Child 1 Child 2 Child 3
Yes No Yes No Yes No Yes No Yes No
Page 2 of 4
6. Do you consume alcohol?
If ‘Yes’, please state the type, quantity and frequency
□ □ □ □ □ □ □ □ □ □
Type:
Quantity:
Frequency (per week):
7. Have you or any of your family members, ever been told to have, received any medical advice, counseling or treatment in connection with sexually transmitted disease, AIDS, AIDS Related Complex or any other AIDS related conditions?
If ‘Yes’, please provide details including date, relationship, diagnosis, treatment, name & address of doctor in the box provided on the right.
□ □ □ □ □ □ □ □ □ □
8. In the past 5 years, have you attended to any tests such as X ray, ultrasound, CT scan, biopsy, electrocardiogram (ECG), endoscopy, blood or urine test?
If ‘Yes’, please provide details including date/type/reason/results of test done, treatment, name & address of doctor in the box provided on the right.
□ □ □ □ □ □ □ □ □ □
9. Have either of your natural parents or siblings died or suffered from cancer, heart disease, stroke, high blood pressure, diabetes, kidney disease, mental disorder, dementia, tuberculosis, Down’s syndrome or any hereditary disease?
If ’Yes, please provide full details in the box provided on the right.
□ □ □ □ □ □ □ □ □ □
Relationship Condition/ Cause of Death Age of Onset If Deceased,
Age of Death
3. Do you have any health or life insurance application that has been rejected, postponed or accepted at special rates or terms by any insurance company?
If ‘Yes’, please provide details on date/type of application and reason for special terms in the box provided on the right.
□ □ □ □ □ □ □ □ □ □
4. Have you in the last 3 months had any of the following symptoms for more than one week continuously: fatigue, weight loss, diarrhoea, enlarged nodes or unusual skin lesions?
If ‘Yes’, please provide details including date, diagnosis, treatment, name & address of doctor in the box provided on the right.
□ □ □ □ □ □ □ □ □ □
5. Do you smoke any cigarettes?
If ‘Yes’, please state number of years and the number of sticks per day
□ □ □ □ □ □ □ □ □ □
No. of years:
No. of sticks (per day):

GROUP HEALTH DECLARATION
Health Declaration
(All questions must be answered and any alteration must be signed) Employee Spouse Child 1 Child 2 Child 3
Yes No Yes No Yes No Yes No Yes No
Page 3 of 4
Continued next page
10. Have you EVER had or been told you had or been treated for:
a) asthma, bronchitis, persistent cough, tuberculosis or respiratory disorder?
□ □ □ □ □ □ □ □ □ □
b) epilepsy, fits, stroke, paralysis, weakness of limb, prolonged headache/giddiness, unconsciousness, nervous breakdown, depression or any other nervous/mental disorders or any disease of the brain?
□ □ □ □ □ □ □ □ □ □
c) gastritis, stomach or duodenal ulcer, blood in stools, fistula, piles or any other stomach or bowel disorders?
□ □ □ □ □ □ □ □ □ □
d) blood, protein or sugar in urine, kidney stones, infection or any other disorders of the kidney, bladder or genital organs?
□ □ □ □ □ □ □ □ □ □
e) anaemia, diabetes, thyroid disorders or any other endocrine disorder?
□ □ □ □ □ □ □ □ □ □
f) cancer, tumour, cyst or growth of any kind? □ □ □ □ □ □ □ □ □ □
g) any form of eye, hearing or speech disorder or disease? □ □ □ □ □ □ □ □ □ □
h) jaundice, Hepatitis B carrier or any form of hepatitis, liver or gallbladder disorders? □ □ □ □ □ □ □ □ □ □
i) slipped disc, gout, arthritis, pain or deformity or disorders of the muscles, spine, limbs or joints or severe injury?
□ □ □ □ □ □ □ □ □ □
j) raised cholesterol, high blood pressure, heart attack, heart murmur, irregular or fast heart rate, chest discomfort or pain, diseases or any other disorders of the heart, heart valves or blood vessels?
□ □ □ □ □ □ □ □ □ □
k) any other illness, disorder, injury, disability, operation or hospitalisation not mention above?
□ □ □ □ □ □ □ □ □ □
11. For Female Insured only
a) Have you ever had any abnormal pap smear test or been told by a doctor to have a repeat pap smear within the next 6 months? If yes, advise the date and result of the test and enclose a copy of the result, if available.
□ □ □ □ □ □ □ □ □ □
b) Have you had an abnormal mammogram or been advised to have mammogram,ultrasound, biopsy, operation of the breasts, ultrasound of pelvis or attended to any other gynecological investigations?
□ □ □ □ □ □ □ □ □ □
c) Have you ever consulted a doctor for irregular, painful menstruation or other problems(s) involving the female organs?
□ □ □ □ □ □ □ □ □ □
d) Have any of your family members been diagnosed with breast cancer?
□ □ □ □ □ □ □ □ □ □
If ’Yes, please provide full details in the box provided on the right. Relationship to Insured Age of Diagnosis
e) Are you currently pregnant? If ‘Yes’, please state no of months _________________________ □ □ □ □ □ □ □ □ □ □

Prudential Assurance Company Singapore (Pte) Limited (Reg. No. 199002477Z)Employee Benefit Solutions Address: Singapore Post Centre Post Office PO Box 399 Singapore 914014
Email: [email protected] Fax: 6233-3285
If any of the answer to Questions 10 and 11 is “Yes”, please provide details below for each condition:
Qn No. Name of InsuredName of
Condition /Treatment
Date of Test / Diagnosis
Duration ofIllness / injury
Result / Reasonfor Test done
Name & Address ofDoctors / Clinics / Hospitals
Consent, Declaration and Authorisation - Please read carefully before signing this Group Health Declaration Form.
I/We consent to Prudential Assurance Company Singapore (Pte) Limited (“Prudential”), its officers and employees :
a) Collecting and using at their sole discretion any and all information relating to me/us, including my/our personal particulars, in this Group Health Declaration for the purposes of underwriting;
and
b) Disclosing at their sole discretion any and all information relating to me/us, including my/our personal particulars, in this Group Health Declaration to the servicing intermediary for the above group policy for the purpose of customer service.
I/We declare that no material facts, that are facts likely to influence the assessment and acceptance of my/our group application, have been withheld and the Information given above is true and complete and best to my/our knowledge and they shall be the basis of the issuance of my/our group insurance coverage.
I/We agree to inform Prudential if there is any change in the state of my/our health/activity between the date of this Health Declaration or medical examination and the date of full insurance coverage provided by Prudential to me/us. I/We understand that the terms of accepting me/us as a risk for insurance coverage may vary according to such information received.
I/We agree and authorise any medical source (i.e. physician and hospital), insurance office or organisation that has my/our records to release to Prudential any relevant information at any time for the purpose of underwriting this group application. A photographic copy of this authorisation shall be as valid as the original.
I/We further declare that I/we have read and understood the “Your Guide To Health Insurance” and “Product Summary” (applicable to voluntary coverage only).
Signature of Employee
Date:
Signature of Spouse (if applicable)
Date:
Signature/Name/Designation of Witness (Employer)
Date:
GROUP HEALTH DECLARATION
Page 4 of 4
EBS HD Mar 2017 (PTRE)

Prudential Assurance Company Singapore (Pte) Limited. (Reg. No. 199002477Z)30 Cecil Street #30-01 Prudential Tower Singapore 049712.
Tel: 1800 333 0 333 Fax: 6734 6953Part of Prudential plc