a follow-up study on removable partial dentures in undergraduate
TRANSCRIPT

J Med Dent Sci 2011; 58: 61-67
Corresponding Author: Eiko YoshidaTel: +81-3-5803-5514 Fax: +81-3-5803-5514E-mail: [email protected] January 12;Accepted March 11, 2011
Original Article
A follow-up study on removable partial dentures in undergraduate program: Part I. Participants and denture use by telephone survey
Eiko Yoshida, Kenji Fueki and Yoshimasa Igarashi
Removable Partial Denture Prosthodontics, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan
The aim of this study was to investigate the clinical outcome of removable partial dentures (RPDs) designed to minimize denture mobility during function. Using archived files of the undergraduate program between 2003 and 2005 at Tokyo Medical and Dental University, a list of 169 patients treated with 184 RPDs was created. The RPDs had either an acrylic resin-base or a cobalt-chrome framework-base. Two examiners telephoned all the listed patients and interviewed 118 patients (70%) regarding the use of their RPDs. Of 118 patients, 42 (36%) had stopped using, mainly due to problems with abutment teeth in resin-based dentures, and replacement in cobalt-chrome-based dentures. There was no significant difference in mean age, gender distribution, mean number of remaining/abutment teeth, distribution of denture arch, and Kennedy classification between denture use and nonuse groups (p>0.05). The nonuse group showed a significantly higher percentage of resin-base compared to the use group (p = 0.006). Logistic regression analysis indicated that resin-base was a significant risk factor for nonuse (p = 0.008). The present findings suggest that abutment teeth should be selected carefully, especially in this type of resin-based RPDs, and that the denture base material may be a critical factor which determines denture use.
Key words: follow-up study, removable partial denture, design principle, denture use
1. Introduction
National dental health surveys carried out recently in industrialized countries showed that the mean number of missing teeth is decreasing steadily and the percentage of edentulous people is also declining1,2 and *. These findings suggest that management of partial edentulism in patients with compromised oral or general health status will be increasingly important in industrialized countries3. Implant-supported dentures are becoming popular for prosthetic restorations in partially dentate patients. However, removable partial denture (RPD) is still the primary treatment option from the patients’ view because an implant-supported denture is very expensive and requires a surgical procedure and a longer treatment time compared to treatment with RPD4,5. An RPD is supported by abutment teeth and residual ridges which have different supporting characteristics on force application. It is known that the difference of supporting characteristics generates rotational movements of the RPD when a force is exerted on the extension base, and it results in potentially destructive forces on the abutment teeth and residual ridges. To minimize the undesirable forces and maintain the health of the structures, McCracken proposed biomechanical principles of RPD design which focused on distribution of the forces to the supporting tissues, namely, support, stability, and retention of RPD 6. On the other hand, Marxkors advocated importance of the RPD design principle that takes into account plaque control for prevention of caries and periodontitis 7, which is called the hygienic design principles and is characterized by simplicity and opening of gingival margins. These principles are generally accepted as fundamentals to designing RPDs. Some clinical studies reported that
62 J Med Dent SciE. Yoshida et al.
the hygienic principles are important for long-term oral health8-11. However, there is no sufficient evidence about the biomechanical principles. An RPD design based on the biomechanical principles was employed in the undergraduate dental student programs from 1998 to 2005 at Tokyo Medical and Dental University. To minimize possible rotational movements of the extension-based RPD around the fulcrum line and longitudinal axis formed by the crest of residual ridge, most of the RPDs covered the lingual or palatal sides of direct, indirect abutment teeth and their adjacent teeth with denture plates 12,13. In case of distal extension-based RPDs, mesial rest and back action clasp were designed as direct retainers on teeth adjacent to the edentulous areas for force distribution to the abutment teeth and residual ridges13. In order to investigate the effectiveness of this biomechanical principle-based RPD design, we carried out a follow-up study to investigate the clinical outcome of the RPDs. Denture use, conditions of remaining teeth, masticatory function, and oral health-related quality of life were assessed in partially dentate patients with the RPDs. This paper reports the study outline and determinant factors that affected denture use. *: Survey of dental diseases in 2006 by Ministry of Health, Labour and Welfare. (http://www.mhlw.go.jp/houdou/2006/06/h0602-2.html)
2. Materials and Methods
2.1 Subjects One hundred sixty-nine patients were listed from archived files of undergraduate dental students’ programs between 2003 and 2005 at the Tokyo Medial and Dental University. The patients had been treated with 184 definitive conventional RPDs (acrylic resin-base: 149, cobalt-chrome [Co-Cr]-base: 35) between two and four years previously, at the time of the making of the list. Patients in the undergraduate programs between 1998 and 2002 were excluded because their files were not complete regarding the information about patient-related variables and their treatment.
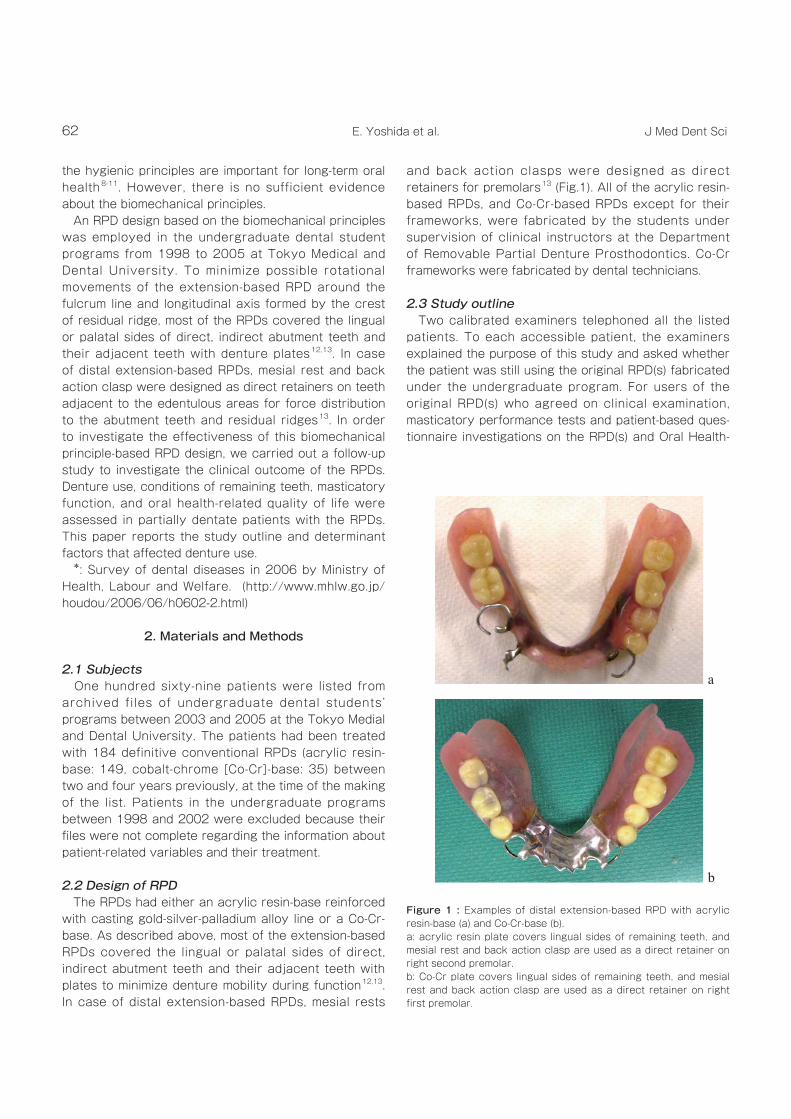
2.2 Design of RPD The RPDs had either an acrylic resin-base reinforced with casting gold-silver-palladium alloy line or a Co-Cr-base. As described above, most of the extension-based RPDs covered the lingual or palatal sides of direct, indirect abutment teeth and their adjacent teeth with plates to minimize denture mobility during function12,13. In case of distal extension-based RPDs, mesial rests
and back action clasps were designed as direct retainers for premolars13 (Fig.1). All of the acrylic resin-based RPDs, and Co-Cr-based RPDs except for their frameworks, were fabricated by the students under supervision of clinical instructors at the Department of Removable Partial Denture Prosthodontics. Co-Cr frameworks were fabricated by dental technicians.
2.3 Study outline Two calibrated examiners telephoned all the listed patients. To each accessible patient, the examiners explained the purpose of this study and asked whether the patient was still using the original RPD(s) fabricated under the undergraduate program. For users of the original RPD(s) who agreed on clinical examination, masticatory performance tests and patient-based ques-tionnaire investigations on the RPD(s) and Oral Health-
a
b
Figure 1 : Examples of distal extension-based RPD with acrylic resin-base (a) and Co-Cr-base (b). a: acrylic resin plate covers lingual sides of remaining teeth, and mesial rest and back action clasp are used as a direct retainer on right second premolar. b: Co-Cr plate covers lingual sides of remaining teeth, and mesial rest and back action clasp are used as a direct retainer on right first premolar.

63Follow-up study on removable partial dentures
Related Quality of Life (OHRQoL) were conducted at the Prosthodontic clinic in Tokyo Medical and Dental Uni-versity Faculty of Dentistry. Prior to the examinations, each patient received a written and verbal description of the experimental procedures and informed consent was obtained. For patients who were not using the original RPD(s) (discarded or replaced), the examiners asked the reason why they stopped using the RPD(s) by telephone. The reason was classified into one of nine categories; RPD fracture, pain, functional problem, discomfort, problem of abutment teeth, aesthetic prob-lem, problem of pronunciation, other, and replacement in cases that the patient could not recall the reason. All experimental procedures were approved by the Ethical Committee of Tokyo Medical and Dental University (No. 236) and implemented between June and December 2007.
2.4 Statistical analyses To analyze demographics of recalled/not-recalled and RPD use/nonuse groups, comparisons were made for the following variables: age, gender, number of remaining teeth and abutment teeth, distribution of denture arch (maxilla/mandible), Kennedy classification, and denture base material. Chi-square test, Fisher’s exact test, and analysis of variance were used to test the distribution of these variables. For RPDs with Kennedy class Ⅰ and Ⅱ to the exclusion of class Ⅲ and Ⅳ because of the small sample size, logistic regression analysis was applied. The null hypothesis was that there was no association between the following outcome and predictors: RPD usage as an outcome, and age, gender, denture arch, Kennedy classification, number of abutment teeth, and denture base material as predictors. Significance level was set at 0.05 and SPSS 11. 0J (SPSS Japan Inc., Tokyo, Japan) was used for all statistical analyses.
3. Results
Flow of the study population is shown in Fig 2. Of the listed 169 patients, 118 patients with 133 RPDs were available for telephonic interview (recall patient-rate: 69.8%). The other patients could not be interviewed mainly due to non-accessibility. Seventy-six of the 118 recalled patients were still using the original 86 RPDs (user rate: 64.4%, used RPD-rate: 64.7%). The used rate of Co-Cr-based RPD (80.0%) was significantly higher than that of acrylic resin-base RPD (60.2%) (p<0.05). Clinical examinations were performed in 46 patients with 55 RPDs (acrylic resin-base: 40, Co-Cr-base: 15).
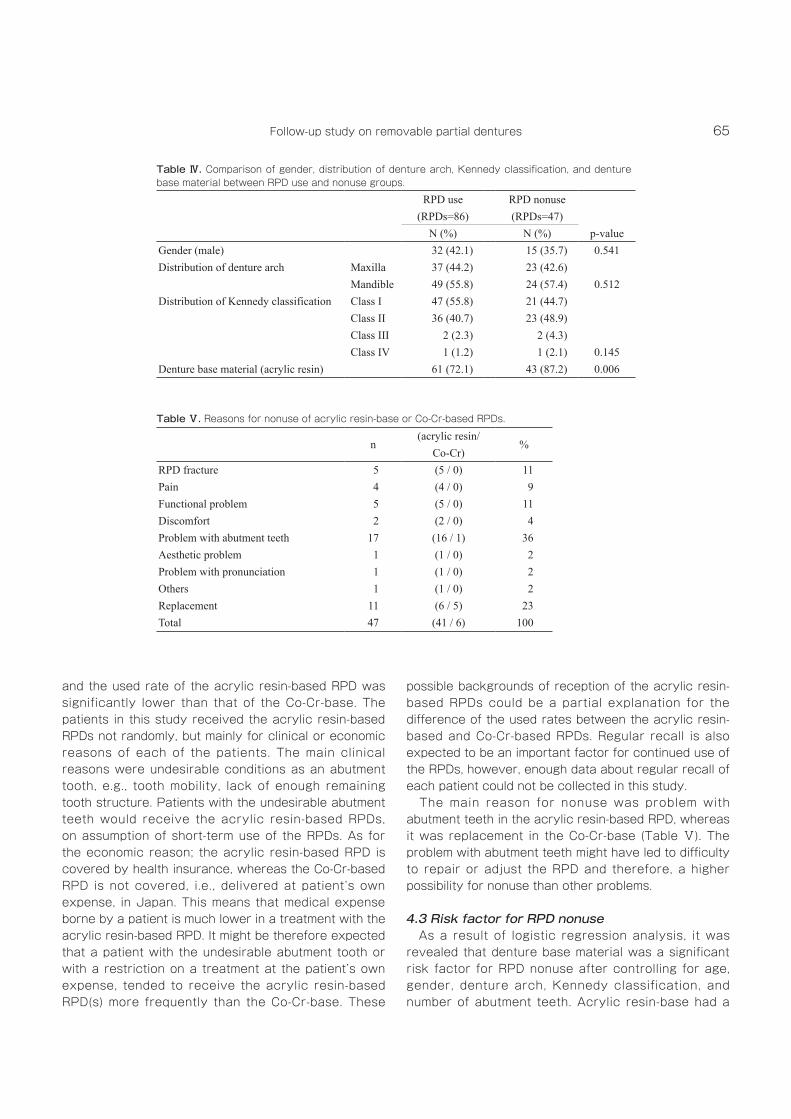
Demographic data in recalled/not-recalled and RPD use/nonuse groups are shown in Tables Ⅰ-Ⅳ. Between recalled and not-recalled groups, significant differences were identified in age, gender, number of remaining teeth, and material distribution (p<0.05). Between RPD use and nonuse groups, a significant difference was identified in denture base material distribution (p<0.01). A total of 47 RPDs (acrylic resin-base: 41, Co-Cr-base: 6) in 42 patients were not in use. The main reason for nonuse was problem of abutment teeth in acrylic resin-based RPDs, whereas it was replacement in Co-Cr-base (Table Ⅴ). As a result of logistic regression analysis, for 127 RPDs with Kennedy class Ⅰ and Ⅱ, denture base material (acrylic resin-base) was identified as a significant risk factor for RPD nonuse (odds ratio of 5.00, p<0.01) (Table Ⅵ).
4. Discussion
4.1 Recall rate In a follow-up study, the recall rate of subjects is important in terms of selection bias. Vanzeveren et al 14 mentioned that high recall rates of around 90% were connected with a relatively low or medium number of patients (<100 patients), with a relatively short period of recall (a few years) and/or the existence
Figure 2 : Flow of the study population.

64 J Med Dent SciE. Yoshida et al.
of systematic recall procedures (sometimes every 6 months). In this study, the recall rate seems not to be high (69.8%). The recalled patients had more advanced age, a higher percentage of females, lower number of remaining teeth, and a lower percentage of acrylic resin-bases than the not-recalled patients (Tables Ⅰ, and Ⅱ), which indicates that there was a certain level of selection bias. These could be partly because of the absence of a systematic recall system. In our undergraduate programs, recall was not systematically organized but was patient-based, although all the patients were instructed to have regular recalls. Additionally, the recalling method by telephone might
also be a factor responsible for this recall rate.
4.2 Used rate of RPD There are some reports about the used rates of acrylic resin-based or Co-Cr-based RPDs. The rate of acrylic resin-base: 67% between six months and five years after their insertion15, Co-Cr-base: around 90% after two years of insertion16, around 50–75%17–19 after five years, 77% after eight to nine years 20, and 50% after ten years19. The used rates of the acrylic resin-based RPDs (60.2%) and the Co-Cr-base (80.0%) between two and four years in this study might not be very different from the previously reported used rates,
Recalled Not-recalled
p-value(patients=118) (patients=51)
Mean (SD) Mean (SD)Age 66.8 (8.1) 58.7 (10.3) <0.001Number of remaining teeth 7.9 (2.9) 9.3 (2.8) 0.003Number of abutment teeth 2.9 (0.9) 2.8 (0.9) 0.647SD: standard deviation
RPD use RPD nonuse(patients=76) (patients=42)Mean (SD) Mean (SD) p-value
Age 66.9 (8.5) 66.5 (7.4) 0.771Number of remaining teeth 7.9 (2.9) 7.7 (3.1) 0.782Number of abutment teeth 2.8 (0.9) 3.1 (0.9) 0.072SD: standard deviation
Recalled Not-recalled(RPDs=133) (RPDs=51)
N (%) N (%) p-valueGender (male) 47 (39.8) 27 (52.9) 0.029Distribution of denture arch Maxilla 58 (43.6) 18 (35.3)
Mandible 75 (56.4) 33 (64.7) 0.305Distribution of Kennedy classification Class I 69 (51.9) 24 (47.1)
Class II 58 (43.6) 25 (49.0) Class III 4 (3.0) 1 (2.0) Class IV 2 (1.5) 1 (2.0) 0.895
Denture base material (acrylic resin) 103 (77.4) 46 (90.2) 0.049
Table Ⅰ. Comparison of age, number of remaining teeth, and abutment teeth between recalled and not-recalled groups.
Table Ⅱ. Comparison of gender, distribution of denture arch, Kennedy classification, and denture base material between recalled and not-recalled groups.
Table Ⅲ. Comparison of age, number of remaining teeth, and abutment teeth between RPD use and nonuse groups.
65Follow-up study on removable partial dentures
and the used rate of the acrylic resin-based RPD was significantly lower than that of the Co-Cr-base. The patients in this study received the acrylic resin-based RPDs not randomly, but mainly for clinical or economic reasons of each of the patients. The main clinical reasons were undesirable conditions as an abutment tooth, e.g., tooth mobility, lack of enough remaining tooth structure. Patients with the undesirable abutment teeth would receive the acrylic resin-based RPDs, on assumption of short-term use of the RPDs. As for the economic reason; the acrylic resin-based RPD is covered by health insurance, whereas the Co-Cr-based RPD is not covered, i.e., delivered at patient’s own expense, in Japan. This means that medical expense borne by a patient is much lower in a treatment with the acrylic resin-based RPD. It might be therefore expected that a patient with the undesirable abutment tooth or with a restriction on a treatment at the patient’s own expense, tended to receive the acrylic resin-based RPD(s) more frequently than the Co-Cr-base. These
possible backgrounds of reception of the acrylic resin-based RPDs could be a partial explanation for the difference of the used rates between the acrylic resin-based and Co-Cr-based RPDs. Regular recall is also expected to be an important factor for continued use of the RPDs, however, enough data about regular recall of each patient could not be collected in this study. The main reason for nonuse was problem with abutment teeth in the acrylic resin-based RPD, whereas it was replacement in the Co-Cr-base (Table Ⅴ). The problem with abutment teeth might have led to difficulty to repair or adjust the RPD and therefore, a higher possibility for nonuse than other problems.
4.3 Risk factor for RPD nonuse As a result of logistic regression analysis, it was revealed that denture base material was a significant risk factor for RPD nonuse after controlling for age, gender, denture arch, Kennedy classification, and number of abutment teeth. Acrylic resin-base had a
RPD use RPD nonuse(RPDs=86) (RPDs=47)
N (%) N (%) p-valueGender (male) 32 (42.1) 15 (35.7) 0.541Distribution of denture arch Maxilla 37 (44.2) 23 (42.6)
Mandible 49 (55.8) 24 (57.4) 0.512Distribution of Kennedy classification Class I 47 (55.8) 21 (44.7)
Class II 36 (40.7) 23 (48.9) Class III 2 (2.3) 2 (4.3) Class IV 1 (1.2) 1 (2.1) 0.145
Denture base material (acrylic resin) 61 (72.1) 43 (87.2) 0.006
n(acrylic resin/
%Co-Cr)
RPD fracture 5 (5 / 0) 11 Pain 4 (4 / 0) 9 Functional problem 5 (5 / 0) 11 Discomfort 2 (2 / 0) 4 Problem with abutment teeth 17 (16 / 1) 36 Aesthetic problem 1 (1 / 0) 2 Problem with pronunciation 1 (1 / 0) 2 Others 1 (1 / 0) 2 Replacement 11 (6 / 5) 23 Total 47 (41 / 6) 100
Table Ⅳ. Comparison of gender, distribution of denture arch, Kennedy classification, and denture base material between RPD use and nonuse groups.
Table Ⅴ. Reasons for nonuse of acrylic resin-base or Co-Cr-based RPDs.

66 J Med Dent SciE. Yoshida et al.
five times greater risk of nonuse compared with Co-Cr-base. The acrylic resin-based RPD in this study covered lingual or palatal surfaces of abutment and its surrounding teeth with an acrylic resin plate. When gingival margins are covered with the acrylic resin plate, plaque accumulation and periodontal damage of the teeth are higher than those not covered or covered with a metal plate 11,21. In addition, the inner surface of the acrylic resin plate is expected to wear out gradually, which could increase denture mobility and result in concentration of mechanical stress on the abutment teeth. Acrylic resin-based RPD consequently might cause problems with the abutment teeth more frequently than Co-Cr-base. On the other hand, rigidity of acrylic resin-based RPD is generally less than that of the Co-Cr-base RPD due to the difference of denture structure and base material, and therefore, failures such as denture fracture are more likely to occur in acrylic resin-base. A series of retrospective cohort studies also reported that increase of abutment teeth mobility22 and fracture of denture base23 were observed more frequently in acrylic resin-based RPD than metal based RPD. This report is based on a telephone survey. Only patients accessible by telephone were involved in the recalled patients, which could be one of the causes of the selection bias described above. Additionally, this retrospective research design might make it difficult for researchers to control quantity and quality of the data. For example, the reasons for nonuse of the RPDs could not be detailed. Therefore, the results should be interpreted on account of these limitations.
Within limitations of this study, it is suggested that in a biomechanical principle-based RPD, abutment teeth should be selected carefully especially for acrylic resin-base and denture base material may be a critical factor which determines denture use.
5. Acknowledgement
The authors would like to thank Dr. H. Furumoto and Dr. K. Mine for their kind assistance with data collection and analyses.
References1. Douglass CW, Watson AJ. Future needs for fixed and
removable partial dentures in the United States. J Prosthet Dent 2002; 87: 9-14.
2. Petersen PE, Bourgeois D, Ogawa H et al. The global burden of oral diseases and risks to oral health. Bulletin of the World Health Organization 2005; 83: 661-669.
3. Wöstmann B, Jørgensen EB, Jepson N et al. Indications for removable partial dentures: A literature review. Int J Prosthodont 2005; 18: 139-145.
4. Nassani MZ, Devlin H, McCord JF et al. The shortened dental arch--an assessment of patients’ dental health state utility values. Int Dent J 2005; 55: 307-312.
5. Ikebe K, Hazeyama T, Kagawa R et al. Subjective values of different treatments for missing molars in older Japanese. J Oral Rehabil 2010; 37: 892-899.
6. McGivney GP, Castleberry DJ. McCracken’s Removable Partial Prosthodontics, ed8. St Louis: Mosby, 1989.
7. Marxkors R. The partial denture with metal framework. Bremen, Germany: BEGO, Bremer Goldschlägarei Wilhelm Herbst, 1984.
Factor β SE p-value Odds ratio 95% CI
Age 0.002 0.024 0.920 1.00 0.96-1.05Gender -0.035 0.431 0.936 0.97 0.42-2.25Maxilla / Mandible -0.083 0.407 0.838 0.92 0.42-2.04Kennedy class I / class II 0.515 0.401 0.199 1.67 0.76-3.67Number of abutment teeth 0.366 0.226 0.104 1.44 0.93-2.25Co-Cr / Acrylic resin-base 1.610 0.606 0.008 5.00 1.52-16.4Constant -3.335 1.916 0.082β: partial regression coefficient, SE: standard error, CI: confidence intervalRPD use; 0, RPD nonuse; 1Male; 0, Female; 1Maxilla; 0, Mandible; 1Class I; 0, Class II; 1Co-Cr-base; 0, Acrylic resin-base; 1
Table Ⅵ. Results of the logistic regression analysis for RPD usage (RPD=127).

67Follow-up study on removable partial dentures
English abstract)16. Schwalm CA, Smith DE, Erickson JD. A clinical study
of patients 1 to 2 years after placement of removable partial dentures. J Prosthet Dent 1977; 38: 380-391.
17. Yeung ALP, Lo ECM, Clark RKF et al. Usage and status of cobalt-chromium removable partial dentures 5-6 years after replacement. J Oral Rehabil 2002; 29: 127-132.
18. Wetherell JD, Amales RJ. Partial denture failures - a long-term clinical survey. J Dent 1980; 8: 333-340.
19. Vermeulen AHBM, Keltjens HMAM, Van’t Hof MA et al. Ten-year evaluation of removable partial dentures: Survival rates based on retreatment, not wearing and replacement. J Prosthet Dent 1996; 76: 267-272.
20. Chandler JA, Brudvik JS. Clinical evaluation of patients eight to nine years after replacement of removable partial dentures. J Prosthet Dent 1984; 51: 736-743.
21. Akaltan F, Kaynak D. An evaluation of the effects of two distal extension removable partial denture designs on tooth stabilization and periodontal health. J Oral Rehabil 2005; 32: 823-829.
22. Amemori H, Hosoi T, Ishiwata Y et al. A clinical survey of partial dentures (Ⅱ) Part 6. Changes in the mobility of the abutment teeth. J Jpn Prosthodont Soc 1971; 15: 134-143. (in Japanese, with English abstract)
23. Shibuya T, Matsumoto M, Kawasaki R et al. A clinical survey of partial dentures (Ⅲ) Part 3. Fractures of partial dentures. J Jpn Prosthodont Soc 1976; 20: 24-30. (in Japanese)
8. McHenry KR, Johansson OE, Christersson LA. The effect of removable partial denture framework design on gingival inflammation: a clinical model. J Prosthet Dent 1992; 68: 799-803.
9. Yeung AL, Lo EC, Chow TW et al. Oral health status of patients 5-6 years after placement of cobalt-chromium removable partial dentures. J Oral Rehabil 2000; 27: 183-189.
10. Öwall B, Jörgensen EB, Davenport J et al. Removable partial denture design: A need to focus on hygienic principles? Int J Prosthodont 2002; 15: 371-378.
11. Zlataric DK, Čelebić A, Valentić-Peruzović M. The effect of removable partial dentures on periodontal health of abutment and non-abutment teeth. J Periodontol 2002; 73: 137-144.
12. Matsuo E, Ohki K. Standard textbook of dentistry; Standard partial denture. Tokyo: Igakushoin publishers, Inc, 1990. (in Japanese)
13. Ohyama T. At las of removable part ia l denture prosthodontics -Design theories and practice of extension base dentures-. Tokyo: Ishiyaku publishers, Inc, 2005. (in Japanese)
14. Vanzeveren C, D’Hoore W, Bercy P et al. Treatment with removable partial dentures: a longitudinal study. PartⅠ. J Oral Rehabil 2003; 30: 447-458.
15. Amemori H, Okuno M, Gunzi K et al. A clinical survey of partial dentures (Ⅱ) Part 2. Long-term observations on clinical effects of wearing partial dentures. J Jpn Prosthodont Soc 1968; 12: 155-171. (in Japanese, with