a g e n d a - south warwickshire ccg
TRANSCRIPT

Governing Body - 22 May 2019
Governing Body
22 May 2019, 9.30 – 11.30 Committee Room, Westgate House, Warwick
A G E N D A
Item Lead Enc Time
1. Apologies:
Dr David Spraggett
Chair
2. Declarations of Interest.
Where possible, any conflict of interest should be declared to the Chair of the meeting as soon as it is identified in advance of the meeting. Please see guidance below.
3. Minutes of the Previous Meeting Enc 01
4. Matters Arising from the Previous Minutes
5. Action Log Enc 02
6. Questions from the Public
7. Chief Officer’s Report Gillian Entwistle Chief Officer
Enc 03 9.35
8. Financial Position at Month 12 (March 2019) Paul Sheldon Chief Finance Officer
Encs 04-04c
9.40
9. Performance Report, 2018/19, Month 11 Ali Cartwright Chief Delivery Officer
Enc 05 9.45
10. Nursing, Quality and Governance Report Alison Walshe Chief Nurse
Enc 06 9.55
11. Proposal for Clinical Commissioning for Coventry and Warwickshire
Dr David Spraggett Enc 07+07a
10.00
12. (Item removed)
13. Safeguarding Children & Adults at Risk of Abuse Policy
Alison Walshe Enc 09+09a
10.50
14. Operational Plan 2019/20 Anna Hargrave Chief Strategy Officer
Enc 10+10a
10.55
15. Primary Care Networks Anna Hargrave Enc 11+11a
11.05
16. CCG 360° Stakeholder Survey 2018/19 Anna Hargrave
Enc 12+12a
11.10

Governing Body - 22 May 2019
Item Lead Enc Time
17. Primary Care Network Clinical Directors and Potential Conflicts of Interest
Alison Walshe Enc 13 11.15
18. 2016-2020 Strategic Plan Progress Update Anna Hargrave Enc 14-14b 11.20
19. Assurance Framework Alison Walshe
Encs 15+15a
11.25
20. Any Other Business Dr David Spraggett
FOR INFORMATION
Note: Information items are only provided to Governing Body members in the electronic pack and are not provided in hard copy
21. Minutes of the Performance Committee (February and March 2019)
Rodney Pitts Lay Member & Committee Chair
Enc 16+16a
22. Minutes of the Clinical Quality & Governance Committee (February and March 2019)
Elaine Strachan-Hall Registered Nurse & Committee Chair
Enc 17+17a
23. Minutes of the Primary Care Committee (February 2019)
Robin Verso Lay Member & Committee Chair
Enc 18
24. Procurement Update – April 2019 Ali Cartwright Enc 19
25. Minutes of the Audit Committee (December 2018) Rodney Pitts Enc 20
26. Resolution: “That pursuant to the provisions of Section 1(2)
of the Public Bodies (Admission to Meetings) Act 1960, the public be now excluded from the meeting by reason of the confidential nature of the business about to be transacted”.
Dr David Spraggett
Future Meetings: Date
Time
Venue
17-July-19+AGM 09.30 am - 11.30 am Committee Room, Westgate House, Warwick
18-Sept-19 09.30 am - 11.30 am Committee Room, Westgate House, Warwick
20-Nov-19 09.30 am - 11.30 am Committee Room, Westgate House, Warwick
22-Jan-20 09.30 am - 11.30 am Committee Room, Westgate House, Warwick
18-Mar-20 09.30 am - 11.30 am Committee Room, Westgate House, Warwick
Declarations of Interest:
Under the Health and Social Care Act 2012, there is a legal obligation to manage conflicts of interest appropriately. Where possible, any conflict of interest should be declared to the Chair of the meeting as soon as it is identified in advance of the meeting. Where this is not possible, it is essential that at the beginning of the meeting a declaration is made if anyone has any conflict of interest to declare in relation to the business to be transacted at the meeting. An interest relevant to the business of the meeting should be declared whether or not the interest has previously been declared. Where a declaration is made, the following should be recorded:
Name of the person declaring the interest;
Position within, or relationship with, the CCG;
Type of interest eg, financial interests, non-financial professional interests;

Governing Body - 22 May 2019
Description of interest, including for indirect interests details of the relationship with the person who has the interest;
Dates interest relates to, from to; and
The actions to be taken to mitigate risk.
Type of Interest Description
Financial Interests
This is where an individual may get direct financial benefits from the consequences of a commissioning decision. This could include being:
A director, including a non-executive director, or senior employee in a private company or public limited company or other organisation which is doing, or which is likely, or possibly seeking to do, business with health or social care organisations;
A shareholder (of more than 5% of the issued shares), partner or owner of a private or not for profit company, business or consultancy which is doing, or which is likely, or possibly seeking to do, business with health or social care organisations.
A consultant for a provider;
In secondary employment;
In receipt of a grant from a provider;
In receipt of research funding, including grants that may be received by the individual or any organisation in which they have an interest or role; and
Having a pension that is funded by a provider (where the value of this might be affected by the success or failure of the provider).
Non-Financial Professional Interests
This is where an individual may obtain a non-financial professional benefit from the consequences of a commissioning decision, such as increasing their professional reputation or status or promoting their professional career. This may include situations where the individual is:
An advocate for a particular group of patients;
A GP with special interests e.g., in dermatology, acupuncture etc.
A member of a particular specialist professional body (although routine GP membership of the RCGP, BMA or a medical defence organisation would not usually by itself amount to an interest which needed to be declared);
An advisor for CQC or NICE;
A medical researcher.
Non-Financial Personal Interests
This is where an individual may benefit personally in ways which are not directly linked to their professional career and do not give rise to a direct financial benefit. This could include, for example, where the individual is:
A voluntary sector champion for a provider;
A volunteer for a provider;
A member of a voluntary sector board or has any other position of authority in or connection with a voluntary sector organisation;
A member of a political party;
Suffering from a particular condition requiring individually funded treatment;
A financial advisor.
Indirect Interests
This is where an individual has a close association with an individual who has a financial interest, a non-financial professional interest or a non-financial personal interest in a commissioning decision (as those categories are described above). This should include:
Spouse / partner;
Close relative e.g., parent, [grandparent], child, [grandchild] or sibling;
Close friend;
Business partner.

Governing Body - 22 May 2019
Blank page
End of report

Enc 01
Governing Body Meeting Minutes of 20 March 2019 Page 1 of 6 Governing Body – 22 May 2019
NHS SOUTH WARWICKSHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY
Minutes of the public meeting held on
Wednesday 20 March 2019 9:30 am – 11:00 pm, Westgate House, Warwick
Present:
Dr David Spraggett Chair DS
Gillian Entwistle Chief Officer GE
Paul Sheldon Chief Finance Officer PS
Dr Richard Lambert Assistant Clinical Chair RL
Rodney Pitts Lay Member RP
Robin Verso Lay Member RV
Catherine White Lay Member CW
Dr Gareth Rowland GP Member Representative GR
Dr Karen Clarke GP Member Representative KC
Dr Jill Crowfoot GP Member Development JC
Dr Sukhi Dhesi GP Member Representative SD
Dr Ian Allwood GP Member Representative IA
Elaine Strachan-Hall Registered Nurse ESH
John Linnane Director of Public Health JL
In Attendance
Alison Walshe Chief Nurse AW
Anna Hargrave Chief Strategy Officer AH
Alison Cartwright Chief Delivery Officer AC
Claire Jones Corporate Governance Manager CJ
Carolyn Bennett Note taker CB

Enc 01
Governing Body Meeting Minutes of 20 March 2019 Page 2 of 6 Governing Body – 22 May 2019
Ref Note Actions
1. 1.1
Apologies (Item 1) No apologies were received.
2. 2.1
Declarations of Interest (Item 2) No interests were declared.
3. 3.1
Minutes of the previous meeting held on 23 January 2019 (Item 3, Enc 01) The minutes of the previous meeting were accepted as a true and accurate record of the meeting.
4. 4.1
Matters Arising of the previous meeting held on 23 January 2019 (Item 4) There were no matters arising from the previous minutes.
5. 5.1 5.2 5.3
Action Log (Item 5, Enc 02) Actions 182+183 – PS confirmed the Task and Finish Group had been established and had met frequently and would now transfer into the scrutiny process. ACTION CLOSED. Action 184 – Further information regarding CYP waiting time will be included in the next report. ACTION CLOSED Action 185 – Information was still awaited from Wolverhampton however updates were being received via finance reports. ACTION TO REMAIN OPEN
PS
6. 6.1
Questions from the Public (Item 6) There were no questions from the public.
7. 7.1 7.2
Chief Officer’s Report (Item 7, Encs 03-03C) GE advised that work continued on the ICS development and that a number of changes were under way as NHSE and NHSI come together as one organisation. The Governing Body noted the content of the report and agreed to delegate authority to the Audit Committee to approve the annual accounts 2018/19 and the Annual Report 2018/19 due to the non-alignment of submission date with the Governing Body meeting.
8. 8.1
Finance Report – Month 10, 2018-19 (Item 8, Enc 04) PS talked through the report and set out the key pressures and risks during the year and the value of current forecast year-end deficit. The Task and Finish Group had been reviewing the unmitigated risks and a small number of changes had been made to the last reported year end position to reflect this work. There were no other changes to the previous forecast to report.

Enc 01
Governing Body Meeting Minutes of 20 March 2019 Page 3 of 6 Governing Body – 22 May 2019
Ref Note Actions
8.2 8.3
PS confirmed the GP IT in year overspend was due to timing of receiving allocation funding and expenditure. The Governing Body noted the content of the report.
9. 9.1 9.2 9.3 9.4 9.5 9.6 9.7
Opening Budgets 2019-20 (Item 9, Enc 05) PS presented the report. PS reminded members that the approval of the budget is reserved to the CCG Members per the Constitution and will be presented to the Members’ Council next week, subject to recommendation today. The budgets contained the uplift of 5.22% which it was noted was quite low compared with other CCGs. The QIPP requirement is £17.2m and as contracts are still to be signed, there is still a risk that could be increased. Attention was drawn to the risks listed in section 8 of the report and noted the risk related to the acute contract value as the contract with SWFT is still to be settled. PS explained there were few opportunities to increase QIPP programme without impacting on the acute service. Further discussion over the next few weeks with SWFT about pathway redesign and efficiency generation is critical. A discussion took place regarding the different financial data. GE reiterated that a large proportion of QIPPs will only be deliverable with the co-operation of providers. This was the main focus of the Coventry & Warwickshire system escalation meeting held last week with NHSE/I and it was recognised therefore this was not just an issue for South Warwickshire CCG but the whole footprint. The Governing Body noted the risks inherent in the opening budgets as presented and in particular the risk of successfully delivering the large QIPP programme 2019/20 and approved the opening budgets for 2019/20.
10. 10.1 10.2 10.3
Medium Term Financial Plan 2019-2024 (Item 10, Enc 06) PS stated the plan incorporated the strategic aims of the CCG as set out in its strategy and complied with all NHS business rules, plus repayment over the next 2/3 years of the 2018-19 deficit. RV commended PS for the much improved and most useful document. The Governing Body noted the following:- • The content of the report; • The risks inherent in the plan as presented and in particular the risk of
successfully delivering the significant QIPP programme; • The number of variables in delivering the early years of the 5 year plan
which may affect the robustness of the expenditure plan for later years.
11. 11.1
Performance Report – Month 9, 2018-19 (Item 11, Enc 07) AC highlighted the following:- • 9 out of 17 indicators had been achieved for month 9;

Enc 01
Governing Body Meeting Minutes of 20 March 2019 Page 4 of 6 Governing Body – 22 May 2019
Ref Note Actions
11.2 11.3 11.4
• Areas of concern for delivery of targets included; A&E, referral to treatment (RTT) where the CCG had just missed the position for December but was now improving, and children’s wheelchairs where NHSE was now providing support.
With regard to autism, SD reported some work had been outsourced however this would not clear the backlog. An action plan was in the process of being developed. JL reported that constitution performance was now being requested more regularly by the County Council’s Health Overview and Scrutiny Committee and agreed to speak to the Committee clerk in an attempt to get the meeting dates changed so they did not clash with CCG governance meetings to allow attendance. The Governing Body noted the areas of performance improvement and deterioration and the actions being taken to address these.
12. 12.1 12.2 12.3
Nursing, Quality and Governance Report (Item 12, Enc 08) AW presented the report and highlighted the following points: • SWFT was maintaining a strong position on mortality measures. Worcester
acute trust figures were outside the expected range and these are being reviewed.
• Despite a further recruitment process, no appointment was made to the Designated Doctor for Child Protection/Child Death Overview post. AW commented that this made a stronger case to review the model across Coventry and Warwickshire.
• Personal Health Budgets (PHBs) were a focus of activity as numbers continued to increase as planned.
• Transforming Care target performance was showing improvement however due to a number of recent adult admissions it is unlikely the trajectories set by NHSE will be met.
It was agreed AW would provide further SHMI data at the next meeting. The Governing Body noted the content of the report.
AW
13. 13.1 13.2 13.3
NHS Continuing Healthcare Policy (Item 13, Encs 09-09c) AW presented the proposed new policy which had been developed per guidance from NHSE. The policy was proposed for all three CCGs in Coventry & Warwickshire and was recommended to the Governing Body by the Clinical Quality & Governance Committee (CQ&GC). AW confirmed feedback was gained from those moving from child to adult care. The Governing Body approved the new NHS Continuing Healthcare policy which would be added to the website along with FAQs.
14. 14.1 14.2
EU Exit Assurance Report (Item 14, Enc 10) AW confirmed the CCG had put in place all NHSE reporting requirements to date. Both the CCG and SWFT had delivered a fully compliant position. The Governing Body noted the positive assurances detailed in the report.

Enc 01
Governing Body Meeting Minutes of 20 March 2019 Page 5 of 6 Governing Body – 22 May 2019
Ref Note Actions
15. 15.1
Information Governance Year-End Report (Item 15, Enc 11) The Governing Body approved the report and delegation of authority to the SIRO to submit the Data Security and Protection Toolkit.
16. 16.1 16.2 16.3 16.4
Equality Delivery System (EDS2) Portfolio (Item 16, Encs 12-12a) AH presented the report which had been endorsed by the CQ&GC. AH confirmed that relevant groups were targeted with regard to ensuring direct outcomes and actions. GE commended those that had worked on the report. The Governing Body noted the content of the EDS2 Portfolio for 2018 and approved the document for publication to the CCG website.
17. 17.1
GDPR and Data Protection Act 2018 – amendments to CCG policy and procedure documents and workplan updates (Item 17, Encs 13 – 13k) The Governing Body approved the eleven remaining category 3 documents listed in section 2.1 and noted that the CCG is on schedule for completing all GDPR and DPA 2018 workplans by its deadline of 31 March 2019.
18. 18.1 18.2
Performance Development Review Framework (PDR) (Item 18, Enc 14-14b) CJ presented the new Framework for approval. The Governing Body approved the PDR Framework.
19. 19.1
Data Security and Protection: Staff Awareness 2018/19 – Outcomes and Management Response (Item 19, Encs 15-15a) The Governing Body noted the and approved the management response to the actions suggested.
20. 20.1
2016-2020 Strategic Plan Progress Report The Governing Body noted the content of the report.
21. 21.1 21.2 21.3
NHS Staff Survey 2018 AH stated this was the third time the survey had been undertaken and the first time two years in a row and a 100% response rate had been recorded. The overall response was positive and the Chief Officers’ Team had reviewed the report and passed it to the Staff Forum for consideration and actions. The Governing Body noted the content of the report.

Enc 01
Governing Body Meeting Minutes of 20 March 2019 Page 6 of 6 Governing Body – 22 May 2019
Ref Note Actions
22. 22.1 22.2
NHSE Evidence Based Interventions Guidance – Policy Amendments and Additions It was agreed the policies should be made easily available to GPs, perhaps via the Extranet, with easily identifiable labelling. In line with the NHSE Evidence Based Interventions Guidance, the Governing Body approved the 3 new commissioning policies and the amendments to 13 existing policies as detailed in appendix 1.
23. 23.1 23.2
Commissioning Policy Approval: Freestyle Libre Flash Continuous Glucose Monitoring System RL noted there may be some operational issues with the new policy and some risk. The Governing Body agreed the removal of the local Freestyle Libre Flash Continuous Glucose Monitoring System Policy and adoption of the national eligibility criteria on 1 April 2019.
24. 24.1 24.2
Assurance Framework 18/19 and 19/20 Refresh It was agreed the blank boxes under further action should be completed where relevant. The Governing Body noted the risks, improvements and positive assurances detailed in the final Assurance Framework for 2018/19 and approved the draft Assurance Framework for 2019/20.
AW
25. 25.1
Any Other Business On behalf of the CCG DS thanked JL for all his help over the years and wished him well in his retirement.
Date of next meeting: Wednesday 22 May 2019 at 9:30am – 11:30 am – Committee Room, Westgate House, Warwick. Confirmed as a true and accurate record of the meeting: Signature of Chair/Date:
Print Name:
David Spraggett
End of Report


NHS South Warwickshire Clinical Commissioning Group Enc 03
Chief Officer’s Report Governing Body - 22 May 2019
Page 1 of 2
Report To: Governing Body For decision
Report Title: Chief Officer’s Report For discussion √
Report From: Gillian Entwistle For information
Date: 22 May 2019 Confidential
Purpose of the Report:
To provide a briefing to the Governing Body on priority issues and a range of emerging issues and key business items.
Key Points:
Briefing on current position relating to emerging/ongoing issues.
Recommendation (s):
Members are asked to note the report.
Previously Considered By: Date:
N/A
CCG Objectives:
To build relationships with patients and our communities √
To improve health and reduce health inequalities √
To improve the quality of care and transform services √
To make best use of resources √
Governance and Assurance √
Management of Conflict of Interests: n/a
Financial Implications: Resource implications for future planning.
Performance Implications: References national constitutional objectives.
Quality Implications: References national and local quality standards.
Equality and Diversity Considerations: Part of the planning process.
Patient and Public Engagement: Engagement undertaken or within plans.
Risk Assessment: In-year risks will be added to Risk Register.

NHS South Warwickshire Clinical Commissioning Group Enc 03
Chief Officer’s Report Governing Body - 22 May 2019
Page 2 of 2
Integrated Care System Development 1.1 The five year plan for the Coventry & Warwickshire health and care system is to be
refreshed for the autumn, per the requirements of the NHS Long Term Plan and the ground work, including the development of the engagement strategy, has commenced via the Better Health, Better Care, Better Value Board. The current strategies of the three local CCGs and the two Health & Wellbeing Boards will feed in to this process.
1.2 Establishing mechanisms for non-executive, lay and local authority member involvement in
the refresh is part of the current governance review being led by Professor Sir Chris Ham.
1.3 Member and stakeholder engagement on the development of local commissioning in light of the NHS Long Term Plan and in the context of an integrated care system has been undertaken in recent months. The process to take this forward will be a time consuming and challenging one for commissioners and the building blocks of Primary Care Networks (PCNs) and Place Partnership critical in the success of delivering any changes.
1.4 A transition team to lead the operational aspects of the commissioner development work is
in place, reporting to the three CCG Chairs. At the same time, substantial work to establish PCNs per the national timetable, and continue the Place development has proceeded at pace. PCN development and approval is subject to a further paper later on this agenda.
Health & Wellbeing Board 2.1 The Warwickshire Health & Wellbeing Board met on 1st May and the full minutes of the
meeting are available on the County Council website. Of note was the Delivery Plan and the following minute extract:
Health and Wellbeing Board Annual Review 2018/19 and Delivery Plan 2019/20 The Board considered its Annual Review for 2018/19 and Delivery Plan for 2019/20. The Annual Review highlighted the continued achievements in health and wellbeing across the system, building on previous reports. The achievements had been sourced from across the Health and Wellbeing Board (HWB) partnership and reflected the breadth of effort in delivering the outcomes in the HWB Strategy. The second part of the report looked forward, covering elements to support the delivery of the refreshed HWB Strategy and the focus of activity for 2019/20. The key elements were outlined: • Prioritising prevention; • Strengthening communities; • Coordinating services; • Sharing responsibility. Feedback was sought on the draft document, which would then be updated and submitted to the Board in September 2019 for final approval, alongside the annual performance report.
2.2 The full minutes of the meeting and copies of the reports are available on the County Council
website via this link. Recommendation 3.1 Governing Body Members are requested to note the report.
End of Report

NHS South Warwickshire Clinical Commissioning Group Enc 04
Finance Report Month 12 2018/19 Governing Body – 22 May 2019
Page 1 of 8
Report To: Governing Body For decision
Report Title: 2018/19 Financial Position at Month 12 (March 2019) For discussion √
Report From: Paul Sheldon Chief Finance Officer
For information
Date: 22 May 2019 Confidential Purpose of the Report:
To update the Governing Body on the reported 2018/19 outturn financial position of the CCG.
Key Points:
• The CCG has reported an in-year deficit of £4.3m in 2018/19 (subject to audit). This will be partially offset by the cumulative surplus of £981k, resulting in an overall cumulative deficit of £3.3m.
• The reported QIPP delivery for 2018/19 is £15.6m (90% of the plan); this includes a number of
non-recurrent mitigations.
• The draft accounts were submitted on time and the external audit of the draft accounts were completed by the middle of May. An Audit Committee meeting to approve the accounts will be held on 23rd May, with submission of the final accounts to NHS England by the 29th May deadline.
Recommendation(s):
It is recommended that the Governing Body note the contents of the report.
Previously Considered By: Date:
Executive Team 1 May 2019
CCG Strategic Objective(s) this report relates to:
Out of Hospital
Personalisation
Specialist Provision
Delivering Today X
Management of Conflicts of Interest: No conflicts of interest.
Financial Implications: The CCG’s ability to achieve its financial targets in 2018/19.

NHS South Warwickshire Clinical Commissioning Group Enc 04
Finance Report Month 12 2018/19 Governing Body – 22 May 2019
Page 2 of 8
Performance Implications: No direct impacts on performance.
Quality Implications: Potential impact on the CCG’s ability to commission high quality services for its population.
Equality and Diversity Considerations: No direct impacts on equality and diversity.
Patient, Public and Stakeholder Engagement: No direct impacts on patient, public and stakeholder engagement.
Risk Assessment: No direct impacts on risk.

NHS South Warwickshire Clinical Commissioning Group Enc 04
Finance Report Month 12 2018/19 Governing Body – 22 May 2019
Page 3 of 8
Objectives and Key Messages
1.1. The CCG’s key financial objectives as per the plan and approved by NHS England (NHSE) prior to the start of the financial year are outlined in Table 1 below.
1.2. The CCG is monitored by NHS England against the metrics in table 1 agreed within the CCG 2018/19 financial plan.
• The CCG was required to deliver an in-year balanced position, however it has overspent by £4.3m.
• The cumulative surplus of £981k will be fully utilised to offset the in year overspend leaving a cumulative deficit if £3.3m going into 2019/20.
• The CCG has achieved 90% of the QIPP plan i.e. a shortfall of £1.7m in achieving the target.
• The CCG is has remained within its annual running cost limit of £5.8m.
Summary Financial Position
2.1. The CCG summary financial position reported to NHSE is outlined in table 2 below.
Column1 Plan target
18/19 Outturn position
Financial Performance Metric £'000's £'000's
In year( Surplus)/Deficit- Full year Forecast 0 4,326
In-Year (Surplus) / Deficit - Underlying (695) 4,600
Cumulative Surplus 981 981
QIPP Saving - Full year Forecast 17,296 15,596
Annual Running Costs Limit 5,853 5,525
Table 1: Key Financial Objectives 2018/19
NHS South Warwickshire Clinical Commissioning Group Enc 04
Finance Report Month 12 2018/19 Governing Body – 22 May 2019
Page 4 of 8
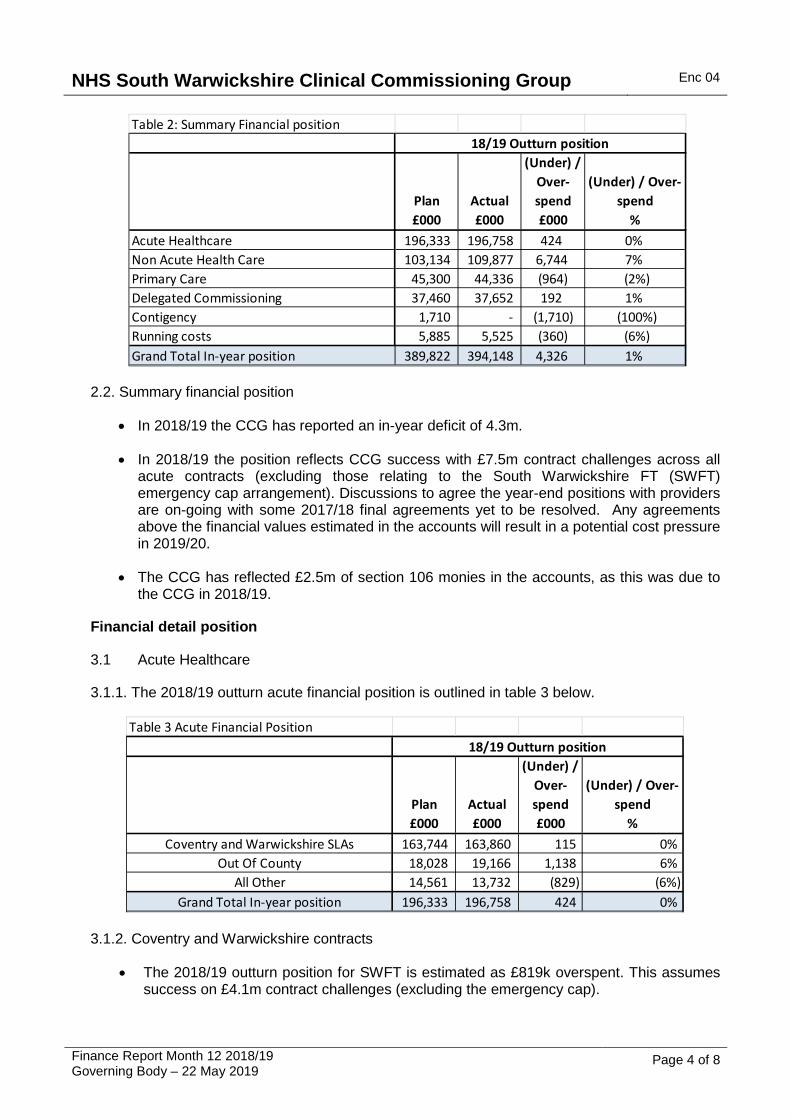
2.2. Summary financial position
• In 2018/19 the CCG has reported an in-year deficit of 4.3m.
• In 2018/19 the position reflects CCG success with £7.5m contract challenges across all acute contracts (excluding those relating to the South Warwickshire FT (SWFT) emergency cap arrangement). Discussions to agree the year-end positions with providers are on-going with some 2017/18 final agreements yet to be resolved. Any agreements above the financial values estimated in the accounts will result in a potential cost pressure in 2019/20.
• The CCG has reflected £2.5m of section 106 monies in the accounts, as this was due to the CCG in 2018/19.
Financial detail position
3.1 Acute Healthcare
3.1.1. The 2018/19 outturn acute financial position is outlined in table 3 below.
3.1.2. Coventry and Warwickshire contracts
• The 2018/19 outturn position for SWFT is estimated as £819k overspent. This assumes success on £4.1m contract challenges (excluding the emergency cap).
Table 2: Summary Financial position
Plan£000
Actual£000
(Under) / Over-spend£000
(Under) / Over-spend
%Acute Healthcare 196,333 196,758 424 0% Non Acute Health Care 103,134 109,877 6,744 7% Primary Care 45,300 44,336 (964) (2%)Delegated Commissioning 37,460 37,652 192 1% Contigency 1,710 - (1,710) (100%)Running costs 5,885 5,525 (360) (6%)Grand Total In-year position 389,822 394,148 4,326 1%
18/19 Outturn position
Table 3 Acute Financial Position
Plan£000
Actual£000
(Under) / Over-spend£000
(Under) / Over-spend
%Coventry and Warwickshire SLAs 163,744 163,860 115 0%
Out Of County 18,028 19,166 1,138 6% All Other 14,561 13,732 (829) (6%)
Grand Total In-year position 196,333 196,758 424 0%
18/19 Outturn position

NHS South Warwickshire Clinical Commissioning Group Enc 04
Finance Report Month 12 2018/19 Governing Body – 22 May 2019
Page 5 of 8
• University Hospitals Coventry & Warwickshire (UHCW) is anticipated to be underspent by £1m and assumes success on £1.9m of risk adjusted contract challenges.
3.1.3. Out of County contracts.
Worcester Acute Hospitals is forecast to overspend overall by £525k while Gloucester Hospital Foundation Trust is forecast to underspend by £126k, with the reminder out of county contracts are showing a cumulative forecast overspend of £739k.
3.1.4. All other Acute
The “other Acute” underspend reflects slippage in planned developments and additional income received in year and reflects section 106 income.
Non-Acute position
3.2.1. The Non-Acute position is outlined in the table 5 below.
3.2.2. Mental Health & Learning Disability Services
• The overspend relates to an increase in individual packages of care. The activity data shows an average increase of 11% in 2018/19 compared to 2017/18.
• The CCG has entered into risk share agreement with Coventry & Warwickshire Partnership Trust (CWPT) which agrees to share any costs or reductions against the agreed financial baseline up to a cap of £1m. £500k income has been assumed in the final position.
3.2.3. Personalisation/ Continuing Healthcare (CHC)
• In 2018/19 the cost pressure relate to an increase in joint funded packages and fast track packages. CHC expenditure remains stable.
• Children’s packages have had a significant increase of £1.1m from 2017/18 outturn. • The CCG has succeeded in clearing the backlog of CHC referrals. This has resulted in a
non-recurrent cost pressure to the CCG of £325k.
Table 4 Non Acute Financial Position
Plan£000
Actual£000
(Under) / Over-spend£000
(Under) / Over-spend
%Community Services 38,063 37,710 353- (1%)
Mental Health & Learning Disability Services 35,773 37,645 1,872 5% Continuing Healthcare 27,696 32,578 4,881 18%
Other Services 1,601 1,944 343 21% Grand Total In-year position 103,134 109,877 6,744 7%
18/19 Outturn position
NHS South Warwickshire Clinical Commissioning Group Enc 04
Finance Report Month 12 2018/19 Governing Body – 22 May 2019
Page 6 of 8
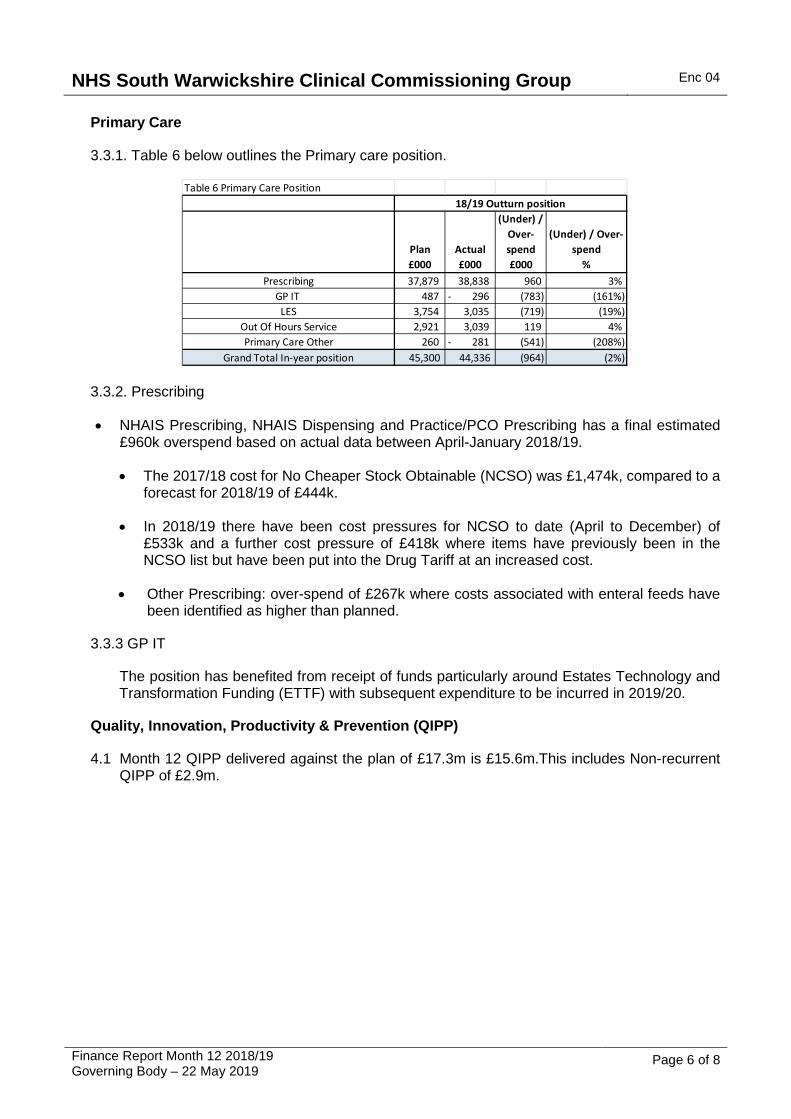
Primary Care
3.3.1. Table 6 below outlines the Primary care position.
3.3.2. Prescribing
• NHAIS Prescribing, NHAIS Dispensing and Practice/PCO Prescribing has a final estimated £960k overspend based on actual data between April-January 2018/19.
• The 2017/18 cost for No Cheaper Stock Obtainable (NCSO) was £1,474k, compared to a forecast for 2018/19 of £444k.
• In 2018/19 there have been cost pressures for NCSO to date (April to December) of £533k and a further cost pressure of £418k where items have previously been in the NCSO list but have been put into the Drug Tariff at an increased cost.
• Other Prescribing: over-spend of £267k where costs associated with enteral feeds have been identified as higher than planned.
3.3.3 GP IT
The position has benefited from receipt of funds particularly around Estates Technology and Transformation Funding (ETTF) with subsequent expenditure to be incurred in 2019/20.
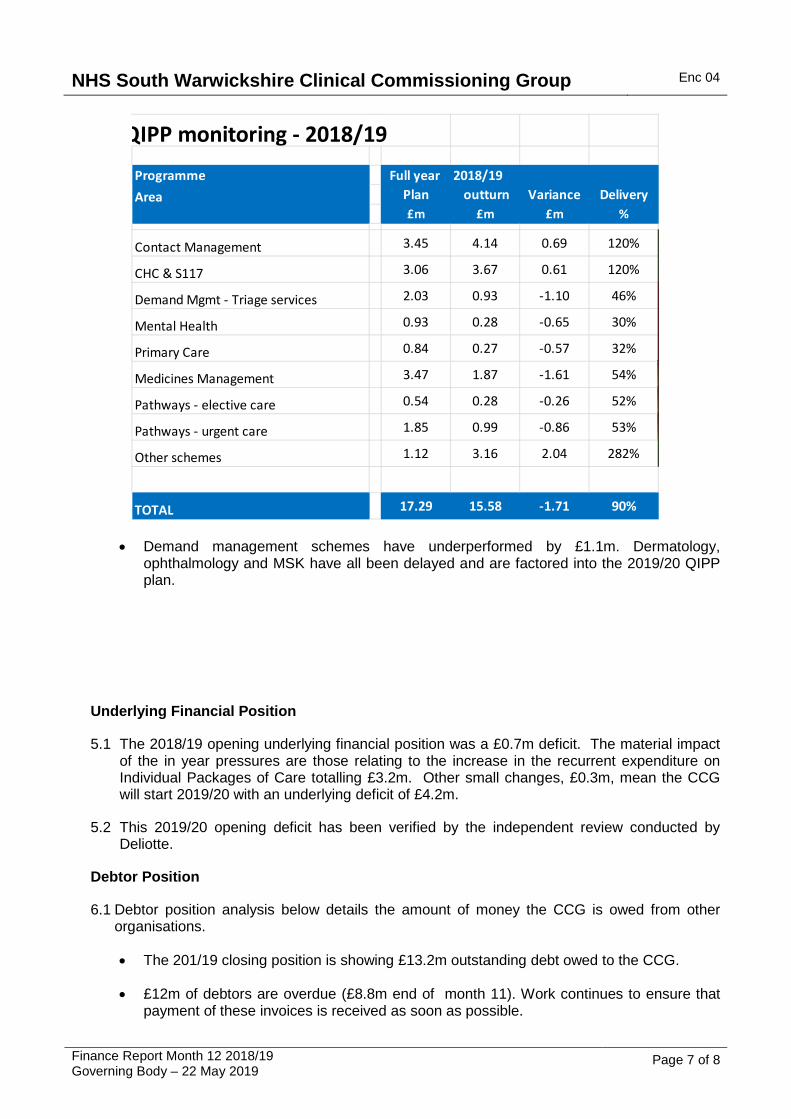
Quality, Innovation, Productivity & Prevention (QIPP)
4.1 Month 12 QIPP delivered against the plan of £17.3m is £15.6m.This includes Non-recurrent QIPP of £2.9m.
Table 6 Primary Care Position
Plan£000
Actual£000
(Under) / Over-spend£000
(Under) / Over-spend
%Prescribing 37,879 38,838 960 3%
GP IT 487 296- (783) (161%)LES 3,754 3,035 (719) (19%)
Out Of Hours Service 2,921 3,039 119 4% Primary Care Other 260 281- (541) (208%)
Grand Total In-year position 45,300 44,336 (964) (2%)
18/19 Outturn position
NHS South Warwickshire Clinical Commissioning Group Enc 04
Finance Report Month 12 2018/19 Governing Body – 22 May 2019
Page 7 of 8
• Demand management schemes have underperformed by £1.1m. Dermatology, ophthalmology and MSK have all been delayed and are factored into the 2019/20 QIPP plan.
Underlying Financial Position
5.1 The 2018/19 opening underlying financial position was a £0.7m deficit. The material impact of the in year pressures are those relating to the increase in the recurrent expenditure on Individual Packages of Care totalling £3.2m. Other small changes, £0.3m, mean the CCG will start 2019/20 with an underlying deficit of £4.2m.
5.2 This 2019/20 opening deficit has been verified by the independent review conducted by Deliotte.
Debtor Position
6.1 Debtor position analysis below details the amount of money the CCG is owed from other organisations.
• The 201/19 closing position is showing £13.2m outstanding debt owed to the CCG.
• £12m of debtors are overdue (£8.8m end of month 11). Work continues to ensure that payment of these invoices is received as soon as possible.
QIPP monitoring - 2018/19
Programme Full year 2018/19 Area Plan outturn Variance Delivery
£m £m £m %
Contact Management 3.45 4.14 0.69 120%
CHC & S117 3.06 3.67 0.61 120%
Demand Mgmt - Triage services 2.03 0.93 -1.10 46%
Mental Health 0.93 0.28 -0.65 30%
Primary Care 0.84 0.27 -0.57 32%
Medicines Management 3.47 1.87 -1.61 54%
Pathways - elective care 0.54 0.28 -0.26 52%
Pathways - urgent care 1.85 0.99 -0.86 53%
Other schemes 1.12 3.16 2.04 282%
TOTAL 17.29 15.58 -1.71 90%

NHS South Warwickshire Clinical Commissioning Group Enc 04
Finance Report Month 12 2018/19 Governing Body – 22 May 2019
Page 8 of 8
• £5.4m debtors relate to packages of care and responsible commissioner issues.
• The table below shows the movement in debtors throughout the year.
Cash Flow analysis
7.1. The table below shows that CCG had £139k cash remaining at the end of March. This was below the maximum threshold set by NHSE of £362k.
Table 9: Cash flow efficiency
Financial Accounts Metrics
8.1 There are a number of key financial accounting performance metrics which are reviewed on a monthly basis e.g. Better Payment Practice Code (BPPC) and cash management.
8.2 The CCG achieved all four BPPC targets at year-end. Further details of these are in Appendix 2 and the Statement of Financial Position (Balance Sheet) is at Appendix 3.
Recommendation
9.1 The Governing Body is recommended to note the contents of the report.
End of Report
Debtor summary NHS Non TotalDebtors 1/4/18 6,081 1,181 7,262 Invoices raised YTD 13,324 13,961 27,284 Credit notes YTD 31- 271- 302- Settled YTD 8,402- 12,616- 21,018-
Current Balance 10,972 2,254 13,226
Mar-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19£000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s
Opening Balance 1,830 75 1,986 3,140 138 624 2 5 10 5 1,158 468 484Cash Drawn 32,405 33,600 29,300 29,300 32,500 28,400 33,100 32,400 31,500 32,000 28,000 25,300 30,500Cash Spent 32,330 31,539 24,174 26,022 31,738 29,022 33,097 32,395 31,505 30,847 28,690 25,284 30,845Cash Balance 75 1,986 3,140 138 624 2 5 10 5 1,158 468 484 139
Cash Efficiency Apr-18 May-18

Enc 04a
Plan£000
Actual£000
(Under) / Over-spend£000
(Under) / Over-spend
%
Acute HealthcareCoventry and Warwickshire SLAs 163,744 163,744 163,860 115 0.1% Out Of County 18,028 18,028 19,166 1,138 6.3% All Other 14,561 14,561 13,732 (829) (5.7%)
Total Acute Healthcare 196,333 196,333 196,758 424 0.2%
Non Acute HealthcareMental Health & LD 35,773 35,773 37,645 1,872 5.2% Continuing Care 27,696 27,696 32,578 4,881 17.6% Community 38,063 38,063 37,710 (353) (0.9%)All Other 1,601 1,601 1,944 343 21.4%
Total Non Acute Healthcare 103,134 103,134 109,877 6,744 6.5%
Primary CarePrescribing 37,879 37,879 38,838 960 2.5% GP IT 487 487 (296) (783) (160.8%)LES 3,754 3,754 3,035 (719) (19.1%)Out of Hours 2,921 2,921 3,039 119 4.1% Primary Care Other 260 260 (281) (541) (208.1%)
Total Primary Care 45,300 45,300 44,336 (964) (2.1%)
Contingency 1,710 1,710 0 (1,710) (100.0%)1% Non-recurrent Reserve 0 0 0 0 0.0%
TOTAL PROGRAMME 346,477 346,477 350,971 4,494 1.3%
Delegated Commissioning 37,460 37,460 37,652 192 0.5%
TOTAL PROGRAMME INC. DEL. COMMISSIONING 383,937 383,937 388,624 4,687 1.2%
Running Cost Allowance 5,885 5,885 5,525 (360) (6.1%)
In-year Planned Surplus 0 0 0 0 0.0%
TOTAL IN-YEAR POSITION 389,822 389,822 394,148 4,326 1.1%
Brought Forward Surplus 981 981 0 (981) (100.0%)
TOTAL CUMULATIVE POSITION 390,803 390,803 394,148 3,345 0.9%
TOTAL RESOURCE LIMIT AVAILABLE 390,803
VARIANCE 0
Plan Actual(Under) /
Over spend
% variance
Coventry & Warwickshire SLAs £000's £000's £000's £000's %South Warwickshire NHS FT (M05) 133,275 133,275 134,094 819 0.6% University Hospitals Coventry & Warwickshire NHST (M06) 19,021 19,021 18,019 (1,002) (5.3%)West Midlands Ambulance Service NHS FT (M06) 8,531 8,531 8,693 161 1.9% Coventry and Warwickshire Pathology Services (M06) 2,917 2,917 3,054 137 4.7%
Sub total - Warwickshire 163,744 163,744 163,860 115 0.1%
Out Of County SLAsWorcestershire Acute Hospitals NHST (M06) 8,602 8,602 9,127 525 6.1% Heart of England NHS FT (M06) 2,085 2,085 2,114 29 1.4% University Hospital Birmingham NHS FT (M06) 1,863 1,863 2,138 275 14.8% Birmingham Women and Children's NHS FT (M06) 483 483 609 126 26.1% Royal Orthopaedic Hospital NHS FT (M06) 459 459 668 209 45.5% Sandwell & West Birmingham Hospitals NHST (M05) 343 343 347 4 1.2% Oxford University Hospitals NHS FT (M06) 3,825 3,825 3,920 95 2.5% Gloucestershire Hospitals NHS FT (M06) 368 368 242 (126) (34.3%)
Sub total - Out Of County 18,028 18,028 19,166 1,138 6.3%
Other BMI - The Meriden Hospital 751 751 1,003 252 33.5% Ramsay Healthcare UK 946 946 742 (204) (21.5%)
South Warwickshire Clinical Commissioning GroupSummary
Period : April 2018 to March 2019 (Month 12)
AnnualPlan£000
MONTH-END POSITION
South Warwickshire Clinical Commissioning GroupAcute Services
Period : April 2018 to March 2019 (Month 12)
AnnualPlan
MONTH-END POSITION

Nuffield Health 2,374 2,374 2,135 (240) (10.1%)SWFT AQP 3,795 3,795 4,065 270 7.1% Other Acute 6,695 6,695 5,788 (907) (13.5%)
Sub total - Other & NCAs 14,561 14,561 13,732 (829) (5.7%)
Total 196,333 196,333 196,758 424 0.2%
Plan Actual(Under) /
Over spend
% variance
£000's £000's £000's £000's %Community Services
South Warwickshire NHS FT 29,632 29,632 27,532 (2,100) (7.1%)ICES - WCC Charge 2,021 2,021 2,020 (1) (0.1%)ICES - SWFT Recharge (1,416) (1,416) 0 1,416 (100.0%)Other Providers 694 694 1,159 465 67.0% Palliative Care 1,085 1,085 952 (132) (12.2%)Better Care Fund 6,048 6,048 6,048 (0) (0.0%)
Sub total - Community Services 38,063 38,063 37,710 (353) (0.9%)
Mental Health & Learning Disability ServicesCoventry and Warwickshire Partnership NHST 27,453 27,453 27,454 1 0.0% Other Mental Health & LD 8,320 8,320 10,191 1,871 22.5%
Sub total - Mental Health & LD 35,773 35,773 37,645 1,872 5.2%
Continuing HealthcareFunded Nursing Care 3,284 3,284 3,161 (123) (3.7%)Continuing Care Other 24,412 24,412 29,417 5,004 20.5%
Sub total - Continuing Care 27,696 27,696 32,578 4,881 17.6%
Other ServicesPatient Transport 1,598 1,598 1,922 324 20.3% Other Non Acute 3 3 22 19 630.8%
Sub total - Other 1,601 1,601 1,944 343 21.4%
Total 103,134 103,134 109,877 6,744 6.5%
Plan Actual(Under) /
Over spend
% variance
£000's £000's £000's £000's %
NHAIS Prescribing 1,234 1,234 990 (244) (19.8%)NHAIS Dispensing 6,060 6,060 5,580 (480) (7.9%)Practice/PCO Prescribing 28,444 28,444 30,173 1,729 6.1% Central Drugs 906 906 954 48 5.3% Home Oxygen Therapy 326 326 308 (18) (5.5%)Other Prescribing 910 910 834 (76) (8.3%)
Sub total - Prescribing 37,879 37,879 38,838 960 2.5%
GP IT 487 487 (296) (783) (160.8%)
LES 3,754 3,754 3,035 (719) (19.1%)
Out Of Hours Service 2,921 2,921 3,039 119 4.1%
Primary Care Other 260 260 (281) (541) (208.1%)
45,300 45,300 44,336 (964) (2.1%)
Plan Actual(Under) /
Over spend
% variance
£000's £000's £000's £000's %
General Practice (GMS) 24,666 24,666 24,947 281 1.1% QOF 3,612 3,612 3,726 114 3.2% Enhanced Services 1,124 1,124 887 (237) (21.1%)Premises Cost Reimbursement 4,133 4,133 3,424 (709) (17.2%)Other Premises Costs 18 18 179 161 893.9%
South Warwickshire Clinical Commissioning GroupNon Acute Services
Period : April 2018 to March 2019 (Month 12)
AnnualPlan
MONTH-END POSITION
South Warwickshire Clinical Commissioning GroupPrimary Care Services
Period : April 2018 to March 2019 (Month 12)
AnnualPlan
MONTH-END POSITION
South Warwickshire Clinical Commissioning GroupDelegated Commissioning
Period : April 2018 to March 2019 (Month 12)
AnnualPlan
MONTH-END POSITION

Dispensing/Prescribing Fees 2,036 2,036 2,055 19 0.9% Other 1,377 1,377 1,766 389 28.2% PMS Premium for Investment 309 309 484 175 56.7% Contingency 185 185 185 0 0.0%
37,460 37,460 37,652 192 0.5% 0
Plan Actual(Under) /
Over spend
% variance
£000's £000's £000's £000's %
Pay 3,467 3,467 2,921 (546) (15.8%)
Non pay 789 789 778 (11) (1.4%)
CSU 1,160 1,160 1,328 168 14.5%
Estates 469 469 497 28 6.1%
5,885 5,885 5,525 (360) (6.1%)
£000's £000's £000's £000's £000's £000'sPROGRAMME RESOURCES
Initial CCG Programme Allocation Month 1 335,853 335,853 Market rents Month 1 (223) (223)HSCN Month 1 140 140 Paramedics Month 1 83 83 Surplus/Deficit Carry Forward - Planned Month 2 981 981 Moved from Delegated to Programme - GPFV Month 3 292 292 GP WIFI Maintenance 2018/19 Month 3 22 22 18/19 Increased Flu Vacc costs baseline realignment Month 3 614 614 LWBC Revenue Funding Q1 for West Midlands Cancer Alliance Month 3 596 596 ED Revenue Funding Q1 for West Midlands Cancer Alliance Month 3 1,017 1,017 Diabetes Transformation Fund: SE DTCM05 Month 3 7 7 Diabetes Transformation Fund: MDFT DTCM05 Month 3 16 16 GPFV-Improving Access to General Practice Month 3 733 733 CCG Grants ICESS Month 3 1,753 1,753 2018-19 GPFV Extended Access Funding Month 4 292 292 LWBC Q2 West Midlands Alliance Month 4 596 596 ED Q2 West Midlands Alliance Month 4 1,017 1,017 Main Capital grants ICES additional grant Month 5 268 268 Recurring impact of 17/18 alteplase transfer for BWCH Month 6 (8) (8)2018 GP OOH Services Funding Allocation Month 6 1 1 M06 IAT Adjustment for IR Changes - Made recurrent Month 6 2 2 Diabetes Transformation Fund: SE DTCM05 Month 6 7 7 Diabetes Transformation Fund: MDFT DTCM05 Month 6 16 16 South Warwickshire CCG Seasonal Flu Allocation Transfer Month 7 (421) (421)Transformation Funding Month 7 1,066 1,066 Excess Treament Programme. Gateway ref: 08385 & 08558 Month 7 (8) (8)Q3 ED Revenue Funding for West Midlands Cancer Alliance Month 7 1,444 1,444 Q3 LWBC Revenue Funding for West Midlands Cancer Alliance Month 7 1,189 1,189 SWCCG - Oncology allocation for SWBH Month 8 (3) (3)Charge Exempt Overseas Visitor (CEOV) Adjustment Month 8 598 598 SWCCG - Cancer Alliance monies Month 9 (4,136) (4,136)Diab Transf: DTCM05 SE Month 9 7 7 Diab Transf: DTCM05 MDFT Month 9 16 16 CYP Green Paper Project Initiation costs 18/26 Month 9 75 75 Q4 ED Revenue Funding for West Midlands Cancer Alliance Month 10 1,444 1,444 Q4 LWBC Revenue Funding for West Midlands Cancer Alliance Month 10 1,189 1,189 Q4 ED Revenue Funding West Midlands Cancer Alliance - Digital Pathology ProMonth 11 450 450 GPFV Workforce Retention MOU Month 11 50 50 CHC - NHS Continuing Healthcare (CHC) Month 11 7 7 SWCCG CHE Month 11 40 40 SWCCG CHE Month 11 30 30 SWCCG CHE Month 11 44 44 SWCCG CHE Month 11 16 16 Diab Transf: DTCM05 SE Month 12 8 8 Diab Transf: DTCM05 MDFT Month 12 14 14 HSCN incentive funding Month 12 15 15 Contribution to MHIS indepdent review fees Month 12 10 10 Additional concenssionary stock/NCSO funding for CCGs Month 12 239 239
11,644 11,644
South Warwickshire Clinical Commissioning GroupRunning Cost Allowance
Period : April 2018 to March 2019 (Month 12)
AnnualPlan
MONTH-END POSITION
South Warwickshire Clinical Commissioning GroupRevenue Resource Limit
Period : April 2018 to March 2019 (Month 12)
Recurrent Non-recurrent Total
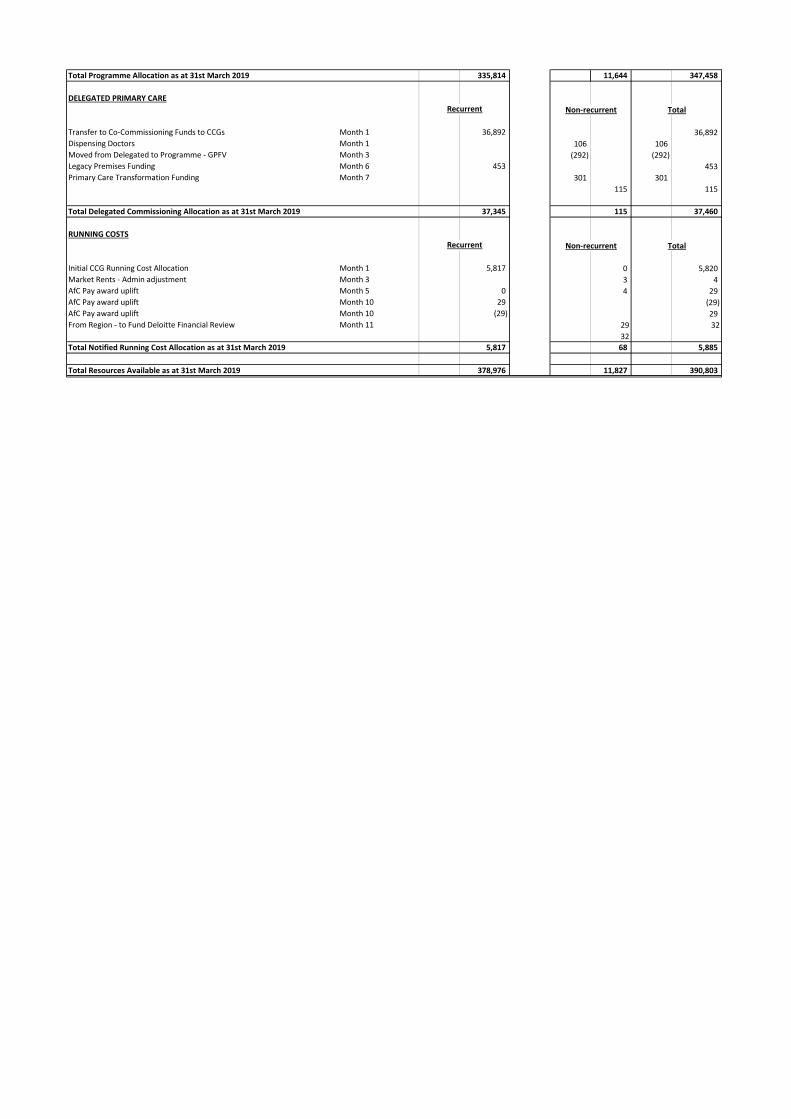
Total Programme Allocation as at 31st March 2019 335,814 11,644 347,458
DELEGATED PRIMARY CARE
Transfer to Co-Commissioning Funds to CCGs Month 1 36,892 36,892 Dispensing Doctors Month 1 106 106 Moved from Delegated to Programme - GPFV Month 3 (292) (292)Legacy Premises Funding Month 6 453 453 Primary Care Transformation Funding Month 7 301 301
115 115
Total Delegated Commissioning Allocation as at 31st March 2019 37,345 115 37,460
RUNNING COSTS
Initial CCG Running Cost Allocation Month 1 5,817 0 5,820 Market Rents - Admin adjustment Month 3 3 4 AfC Pay award uplift Month 5 0 4 29 AfC Pay award uplift Month 10 29 (29)AfC Pay award uplift Month 10 (29) 29 From Region - to Fund Deloitte Financial Review Month 11 29 32
32Total Notified Running Cost Allocation as at 31st March 2019 5,817 68 5,885
Total Resources Available as at 31st March 2019 378,976 11,827 390,803
Recurrent Non-recurrent Total
Recurrent Non-recurrent Total
Enc 04b
Governing Body – 22 May 2019
APPENDIX 2
Financial Accounts Metrics
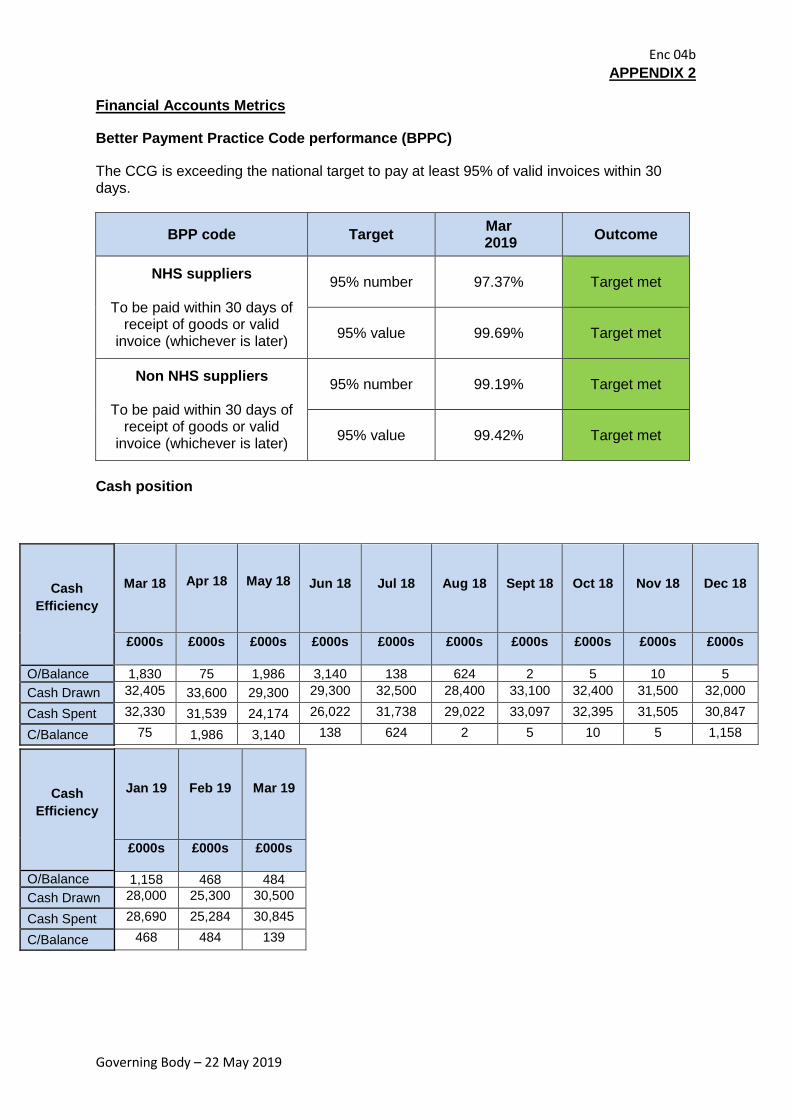
Better Payment Practice Code performance (BPPC)
The CCG is exceeding the national target to pay at least 95% of valid invoices within 30 days.
BPP code Target Mar 2019 Outcome
NHS suppliers
To be paid within 30 days of receipt of goods or valid
invoice (whichever is later)
95% number
97.37%
Target met
95% value
99.69%
Target met
Non NHS suppliers
To be paid within 30 days of receipt of goods or valid
invoice (whichever is later)
95% number
99.19%
Target met
95% value
99.42%
Target met
Cash position
Cash Efficiency
Mar 18 Apr 18 May 18
Jun 18
Jul 18
Aug 18
Sept 18
Oct 18
Nov 18
Dec 18
£000s £000s £000s £000s £000s £000s £000s £000s £000s £000s
O/Balance 1,830 75 1,986 3,140 138 624 2 5 10 5 Cash Drawn 32,405 33,600 29,300 29,300 32,500 28,400 33,100 32,400 31,500 32,000
Cash Spent 32,330 31,539 24,174 26,022 31,738 29,022 33,097 32,395 31,505 30,847
C/Balance 75 1,986 3,140 138 624 2 5 10 5 1,158
Cash Efficiency
O/Balance Cash Drawn Cash Spent C/Balance
Jan 19
Feb 19
Mar 19
£000s £000s £000s
1,158 468 484 28,000 25,300 30,500 28,690 25,284 30,845
468 484 139

Enc 04b
Governing Body – 22 May 2019
Blank Page
End of Report
Enc 04c
Governing Body – 22 May 2019
APPENDIX 3
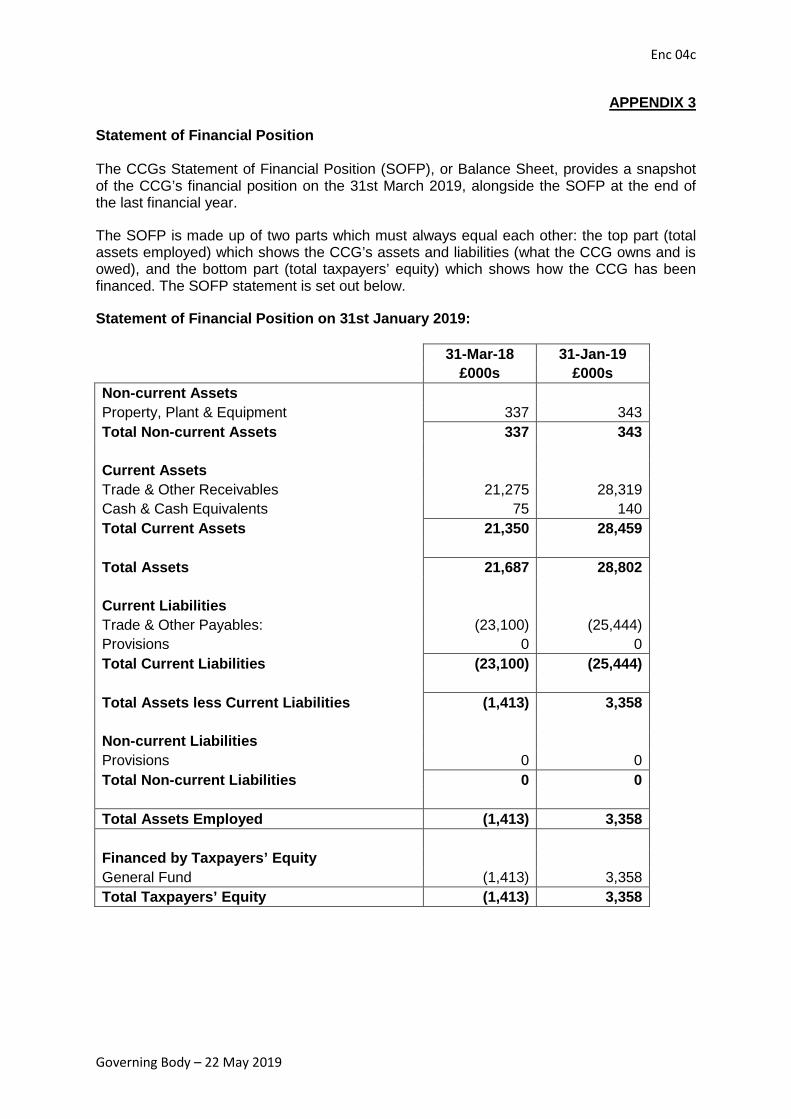
Statement of Financial Position The CCGs Statement of Financial Position (SOFP), or Balance Sheet, provides a snapshot of the CCG’s financial position on the 31st March 2019, alongside the SOFP at the end of the last financial year.
The SOFP is made up of two parts which must always equal each other: the top part (total assets employed) which shows the CCG’s assets and liabilities (what the CCG owns and is owed), and the bottom part (total taxpayers’ equity) which shows how the CCG has been financed. The SOFP statement is set out below.
Statement of Financial Position on 31st January 2019:
31-Mar-18 31-Jan-19
£000s £000s Non-current Assets Property, Plant & Equipment 337 343 Total Non-current Assets 337 343
Current Assets Trade & Other Receivables 21,275 28,319 Cash & Cash Equivalents 75 140 Total Current Assets 21,350 28,459 Total Assets 21,687 28,802 Current Liabilities Trade & Other Payables: (23,100) (25,444) Provisions 0 0 Total Current Liabilities (23,100) (25,444) Total Assets less Current Liabilities (1,413) 3,358 Non-current Liabilities Provisions 0 0 Total Non-current Liabilities 0 0 Total Assets Employed (1,413) 3,358 Financed by Taxpayers’ Equity General Fund (1,413) 3,358 Total Taxpayers’ Equity (1,413) 3,358

Enc 04c
Governing Body – 22 May 2019
Blank Page
End of Report
NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 1 of 20
Report To: Governing Body For decision
Report Title: Performance Report, 2018/19, Month 11 For discussion √
Report From: Alison Cartwright Chief Delivery Officer
For information
Date: 22 May 2019 Confidential
Purpose of the Report:
To update Governing Body Members on the February 2019 position regarding performance against national targets and priority indicators for NHS South Warwickshire CCG (the CCG).
Key Points:
NHS Constitution indicators in February 2019: • Good progress has been sustained/improved for the following indicators:
• Cancer – Two week wait • Cancer – Two week wait (Breast Symptoms) • Cancer – 31 day standard and subsequent treatments • Ambulance Handover Local Threshold • Delayed Transfer of Care (Acute)
• Areas of concern:
• A&E 4 hour waits • Referral to Treatment (RTT) pathway (incomplete aggregate target) • RTT over 52 week waits (Incomplete pathway) • Diagnostics • Cancer – 31 day Standard and drug regimen • Cancer – 62 day standard and consultant upgrade • Cancer – 104 day waits
• The CCG breached 7 out of the 16 Acute priority indicators with Delayed Transfers of Care
(Non-Acute), Wheelchairs, and E-Referral utilisation remaining an issue. • The CCG breached 7 out of the 17 Mental Health indicators with Dementia and IAPT remaining
an issue. • Where applicable Contract Performance Notices have been served to the relevant providers for
these indicators and Remedial Actions Plans and recovery trajectories have been agreed. Progress against these plans is detailed in the report.
Recommendation (s): Governing Body members note the areas of performance improvement and deterioration and the actions being taken to address these. Previously Considered By: Date:
Executive Team 1 May 2019

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 2 of 20
CCG Strategic Objective(s) this report relates to:
Out of Hospital Personalisation Specialist Provision
Delivering Today √
Management of Conflicts of Interest: Not applicable.
Financial Implications: Financial penalties and with-holds utilised as per the national contract to lever improvements in performance.
Performance Implications: See detail within the report.
Quality Implications: See detail within the report.
Equality and Diversity Considerations: Not applicable.
Patient, Public and Stakeholder Engagement: Not applicable.
Risk Assessment: High risk area given current performance challenges.

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 3 of 20
Executive Summary 1.1 The report details February 2019 performance for the NHS Constitution Rights & Pledges
and priority indicators for both the CCG and its main providers of services. Actions being taken to address any areas of non-achievement are detailed in section 5.
1.2 There were 8 separate NHS Constitution CCG indicators breaching during the month.
Acute Performance at a glance
Performance Summary Indicators achieved
Indicators breaching
Total Indicators
NHS Constitution – CCG 9 8 17
Priority Indicators not in the NHS Constitution 7 9 16
Good Progress Basis Target Feb-19
A&E: 12 hour trolley waits SWFT 0 0
Cancer 2 week wait – GP Referral CCG 93% 97.1%
Cancer 2 week wait – Breast Symptoms CCG 93% 96.5%
Cancer – 31 day standard CCG 96% 97.2%
Cancer 31 day – subsequent treatment surgery CCG 94% 100%
Cancer 31 day – subsequent treatment radiotherapy CCG 94% 97.4%
Cancer 31 day – subsequent treatment Drug regimen CCG 98% 100%
Number of operations cancelled for a second time SWFT 0 0 DTOC % of delayed bed days as percentage of occupied beds –Acute SWFT 3.5% 3%
Ambulance Handover Local Threshold SWFT 98% 99.8%
Ellen Badger – Community Average length of stay SWFT 28 26.2
CHC: % DSTs completed in acute setting (Mar 2019) CCG <15% 13.2%
CHC: 12+ week cases open at month end (Mar 2019) CCG 0 0 CHC: % eligibility decisions made within 28 days from receipt of Checklist (Mar 2019) CCG 80% 100%
NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 4 of 20
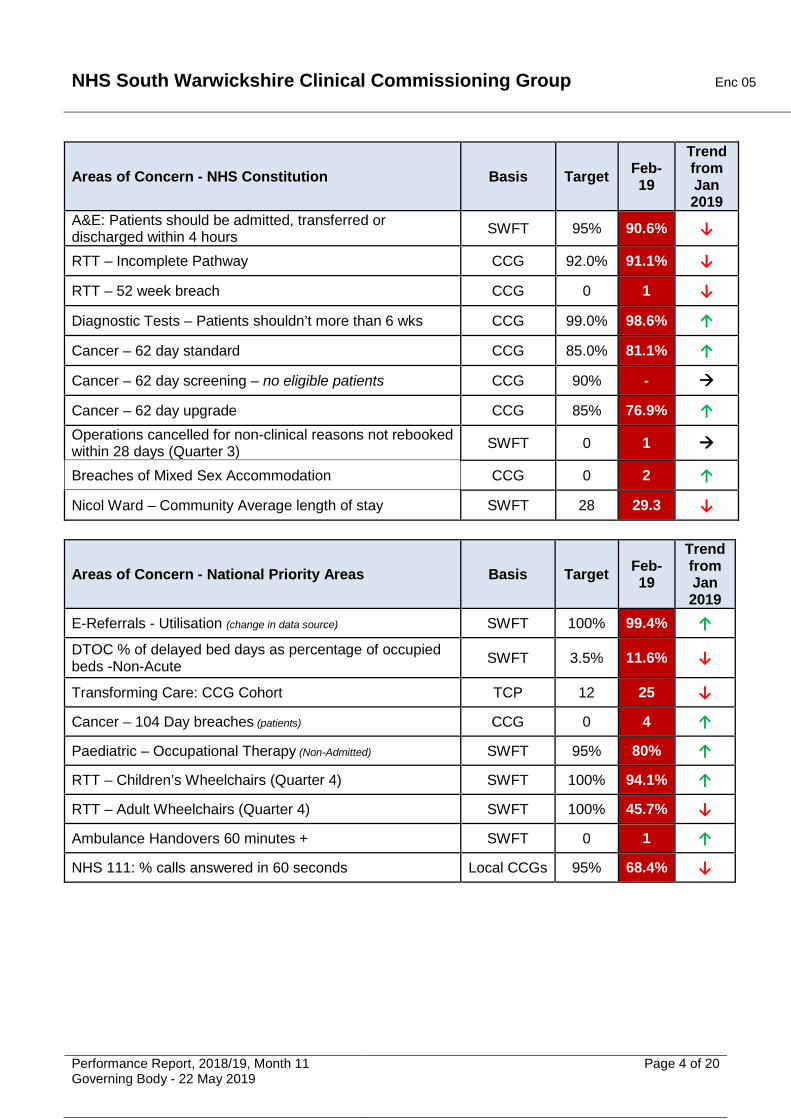
Areas of Concern - NHS Constitution Basis Target Feb-19
Trend from Jan 2019
A&E: Patients should be admitted, transferred or discharged within 4 hours SWFT 95% 90.6% ↓
RTT – Incomplete Pathway CCG 92.0% 91.1% ↓
RTT – 52 week breach CCG 0 1 ↓
Diagnostic Tests – Patients shouldn’t more than 6 wks CCG 99.0% 98.6% ↑
Cancer – 62 day standard CCG 85.0% 81.1% ↑
Cancer – 62 day screening – no eligible patients CCG 90% -
Cancer – 62 day upgrade CCG 85% 76.9% ↑ Operations cancelled for non-clinical reasons not rebooked within 28 days (Quarter 3) SWFT 0 1
Breaches of Mixed Sex Accommodation CCG 0 2 ↑
Nicol Ward – Community Average length of stay SWFT 28 29.3 ↓
Areas of Concern - National Priority Areas Basis Target Feb-19
Trend from Jan 2019
E-Referrals - Utilisation (change in data source) SWFT 100% 99.4% ↑ DTOC % of delayed bed days as percentage of occupied beds -Non-Acute SWFT 3.5% 11.6% ↓
Transforming Care: CCG Cohort TCP 12 25 ↓
Cancer – 104 Day breaches (patients) CCG 0 4 ↑
Paediatric – Occupational Therapy (Non-Admitted) SWFT 95% 80% ↑
RTT – Children’s Wheelchairs (Quarter 4) SWFT 100% 94.1% ↑
RTT – Adult Wheelchairs (Quarter 4) SWFT 100% 45.7% ↓
Ambulance Handovers 60 minutes + SWFT 0 1 ↑
NHS 111: % calls answered in 60 seconds Local CCGs 95% 68.4% ↓

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 5 of 20
Mental Health Performance at a glance
Performance Summary Indicators achieved
Indicators breaching
Total Indicators
NHS Constitution – CCG 9 8 17
Priority Indicators not in the NHS Constitution 9 7 16
Good Progress Basis Target Feb -19 Care Programme Approach: Proportion of patients followed up within 7 days of discharge from psychiatric inpatient care (Quarter 3)
CCG 95% 100%
% of patients physically reviewed by Place of Safety clinician within 3 hours of admission (Quarter 3) CCG 90% 100%
% of patients contacted within (4 hours) of referral to the Crisis Team CCG 95% 100%
Response to emergency assessment bed areas by AMHAT (Quarter 3) CWPT 95% 99.5%
Improving Access to Psychological Therapies (IAPT): Recovery Rate (Dec 2018) CCG 50% 58.3%
CAMHS - Referral to Treatment (Emergency - 48 hrs) CWPT 100% 100% CAMHS - Referral to Treatment (Urgent - 5 working days) CWPT 100% 100%
CAMHS - Referral to Treatment (Routine - 18 weeks) CWPT 95% 100% % AMHAT referrals received from A&E commencing assessment within 90 mins (Quarter 3) CWPT 90% 94.1%
% AMHAT referrals received from wards commencing assessment within 36 hours from AMHAT (Quarter 3) CWPT 90% 96.2%
Areas of Concern - National Priority Areas Basis Target Feb-19
Trend from Jan 2019
Dementia diagnosis percentage (65 + years) CCG 66.7% 59.3% ↓ Improving Access to Psychological Therapies (IAPT): Access Rate (Dec 2018) CCG 4.75% Q3 4.03% ↓
Mental Health: Early Intervention in Psychosis (EIP) – complete patients CCG 53% 0% ↓
Areas of Concern- Local Priority Areas Basis Target Feb-19 Trend from Jan 2019
CAMHS - % of LAC to have an initial health assessment within 13 days (Quarter 3) CWPT 95% 29.6% ↓
Children and Young People’s Emotional Well-Being and Mental Health Follow-ups (over 12 weeks) – provisional data CCG 12
weeks 24 ↓
Children and Young People’s Autism Spectrum Disorder Waits (CYP ASD) (over 12 weeks - proxy) – provisional data CCG 12
weeks 443 ↓
CAMHS - Review of LAC health plan and a written report for each review and a copy sent to social care (Quarter 3) CWPT 95% 44.9% ↓

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 6 of 20
NHS Constitution Rights and Pledges 3.1 February 2019 performance for the CCG and its main providers is shown below:
Target Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19
Patients should be admitted, transferred or discharged within 4 hours of their arrival at an A&E department - SWFT 95% 90.5% 94.6% 96.1% 95.6% 96.6% 95.0% 97.7% 95.4% 92.0% 90.2% 90.6%
A&E Trolley Waits of greater than 12 hours (from DTA to admission) - SWFT 0 0 0 0 0 0 0 0 0 0 0 0
Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks from referral 92% 90.3% 91.4% 91.1% 90.9% 89.8% 88.8% 89.5% 90.4% 90.7% 91.3% 91.1%
Incomplete pathways of greater than 52 weeks 0 5 5 5 9 7 6 3 2 1 0 1
Diagnostics Patients waiting for a diagnostic test should have been waiting no more than 6 weeks from referral 99% 92.7% 95.7% 97.0% 94.9% 94.1% 94.8% 99.2% 98.8% 98.4% 97.9% 98.6%
Maximum two-week wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP 93% 92.3% 95.5% 92.9% 90.0% 93.6% 95.3% 96.2% 97.7% 98.2% 97.1% 97.1%
Maximum two-week wait for first outpatient appointment for patients referred urgently with breast symptoms (cancer not initially suspected) 93% 98.9% 100.0% 93.9% 94.1% 93.2% 98.6% 99.4% 95.9% 97.0% 96.8% 96.5%
Maximum one month (31-day) wait from diagnosis to first definitive treatment for all cancers 96% 98.3% 95.2% 98.5% 97.9% 99.2% 95.9% 94.5% 96.2% 99.2% 95.5% 97.2%
Maximum 31-day wait for subsequent treatment where that treatment is surgery 94% 94.1% 100.0% 89.5% 86.7% 92.9% 78.6% 95.7% 95.7% 100.0% 95.5% 100.0%
Maximum 31-day wait for subsequent treatment where that treatment is an anti-cancer drug regimen 98% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 93.1% 100.0%
Maximum 31-day wait for subsequent treatment where the treatment is a course of radiotherapy 94% 100.0% 95.7% 94.8% 96.2% 97.3% 100.0% 100.0% 100.0% 96.1% 96.3% 97.4%
Maximum two month (62-day) wait from urgent GP referral to first definitive treatment for cancer 85% 81.2% 74.4% 75.0% 74.3% 72.7% 78.1% 73.1% 71.1% 80.0% 72.1% 81.1%
Maximum 62-day wait from referral from an NHS screening service to first definitive treatment for all cancers 90% 90.0% 83.3% 88.9% 83.3% 100.0% 100.0% 85.7% 87.5% 50.0% 80.0% 0 patients
Maximum 62-day wait for first definitive treatment following a consultant's decision to upgrade the priority of the patient (all cancers) 85% 86.7% 100.0% 85.7% 92.9% 85.7% 91.7% 89.5% 81.3% 85.0% 72.7% 76.9%
MSA Breaches of Mixed Sex Accommodation guidelines - Instances 0 5 2 6 1 2 3 4 2 4 3 2
All patients who have operations cancelled, on or after the day of admission for non-clinical reasons to be offered binding date within 28 days, or the treatment to be funded at the time and hospital of the patient's choice - SWFT 0
Number of operations cancelled for a second time - SWFT 0 0 0 0 0 0 0 0 0 0 0 0
Mental Health Care Programme Approach (CPA): The proportion of people under adult mental illness specialties on CPA who were followed up within 7 days of discharge from psychiatric in-patient care during the period 95%
1
100.0%
NHS Constitution MeasuresNHS South Warwickshire CCG
Measure
A&E
RTT
Cancer - 2WW
N/A
N/A100.0%
Cancer - 31 day
1
Cancer - 62 days
Cancelled Operations
96.1%
9

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 7 of 20
NHS Local Mental Health Priorities 3.2 February 2019 performance for the CCG at CWPT is shown below. Exception reports for non-compliant standards are detailed further on in the
report.
Ref Indicator Target Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19
C10 Adult - % of service users experiencing a first episode of psychosis or ARMS (at risk mental state) who waits less than two weeks to start a NICE recommended package of care - Completed Pathways 50% 0.0% 0.0% 33.3% 0.0% N/A 0.0% N/A 0.0% N/A N/A 0.0%
CON29 % of patients contacted within (4 hours) of referral to the Crisis Team 95% 100.0% 100.0% 99.3% 94.1% 99.0% 100.0% 93.2% 96.2% 99.4% 100.0% 100.0%
CON30 Adult - % of patients who have a crisis plan agreed which has been developed in consultation with Community IPU, CRHT, patient and carer
Q1 -25%Q2 - 50%
CON36 Adult - % seen, physically reviewed and examined by CWPT POS clinician (Junior Doctor) within 3 hrs of admission to the unit from time of arrival at POS
Q1 - 90%Q2 - 90%
SQ92a Adult - 90% of all appropriate referrals received from A&E which have had their assessment commenced within 90 minutes from AMHAT receiving the referral. 90%
SQ93 Adult - Response to emergency assessment bed areas will be within 12 hours from receipt of appropriate referrals during the service hours of operation. 95%
SQ94 Adult - 90% of all appropriate referrals received from wards have had their assessment commenced within 36 hours from AMHAT receiving the referral. This will be subject to clinical availability and existing clinical priorities. 90%
CON176 Adult - Number and % of s136 detentions prevented and/or diverted TBC
From NHSE Adult - Dementia diagnosis percentage (65 + years) 66.7% 59.70% 59.80% 60.1% 59.9% 60.1% 58.9% 58.6% 59.0% 59.4% 59.0% 59.3%
Adult - Improving Access to Psychological Therapies (IAPT): Access Rate 4.75% 4.17% 4.03% 3.92% 3.94% 4.14% 4.33% 4.58% 4.39% 4.03%
Adult - Improving Access to Psychological Therapies (IAPT): Recovery Rate 50% 53.6% 44.4% 52.0% 59.5% 53.3% 57.1% 53.6% 55.9% 58.3%
CAMHS - Referral to Treatment (Emergency - 48 hours) 100% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
CAMHS - Referral to Treatment (Urgent - 5 working days) 100% 100.0% N/A 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
CAMHS - Referral to Treatment (Routine - 18 weeks) 95% 100.0% 100.0% 100.0% 97.8% 100.0% 100.0% 98.0% 100.0% 100.0% 100.0% 100.0%
CAMHS - Referrals Received by Navigation Hub (All CAMHS) 122 150 145 166 103 96 184 127 123 128 132
CON149 CAMHS - Waiting time from initial appointment to follow up appointment (12 weeks) 95% 25.8% 55.8% 64.1% 63.3% 51.1% 48.3% 41.0% 32.7% 43.3% 68.0% 66.7%
CON63 CAMHS - ASD Waiting time from referral to assessment (Average wait) TBC 59 61 64 64 63 60 59 51 52 53 55
CON64 CAMHS - Number of ASD assessments undertaken each month 20 18 9 4 10 8 9 10 16 13 12 10
CYP ED from NHS E
CAMHS - referrals for an assessment or treatment of any eating disorder will access NICE concordant treatment within 1 week for urgent cases 90% for 18/19
CYP ED from NHS E
CAMHS - referrals for an assessment or treatment of any eating disorder will access NICE concordant treatment within 4 weeks for routine cases 90% for 18/19
(CON10) CAMHS - patients will have an assessment within 48 hours of referral to ALT where medically fit 95% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%
CON144 CAMHS - Number and % of newly looked after children to have an initial health assessment within 13 days post receipt of notification 95% 23.0% 37.0% 33.0%
CON144a CAMHS - Review of LAC health plan and provide a written report for each review and a copy sent to social care, 0-5 years at least 6 monthly and to 18 years at least 12 months - Reported Quarterly 95% 79.2% 88.2% 82.4% 82.2% 79.2% 34.4% 28.8% 39.7% 68.5%
94.1%
98.5%
96.2%
7.6%
report not due
report not due
report not due
report not due
report not due
report not due
report not due
63.2% 13.9%
81.1%
100.0%
100.0% 99.0%
78.4% 83.3%
report not due
report not due
CON10
66.7% 100.0%
88.8% 84.8%
86.9%
report not due
Mental Health Dashboard
48.6% 53.2%
100.0% 100.0%
55.3%
100.0%
report not due
report not due
89.7%
95.4% 97.5%

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 8 of 20
Issues: • 10.2% (+575) rise in attendances in February ‘18 vs February ‘19. • Stranded (7 day) and Super Stranded (21 day) stay patients rose
steadily over the winter and have maintained this level.
Ongoing Actions: • GP in A&E, working as part of the ED team, and commissioned by
SWFT, is reportedly working well. Increased support during March to ensure delivery of the 4 hour target, and has been extended until the end of May, with a business case being developed for future use.
• The A&E Delivery Plan continues to be worked through and monitored via the SWFT A&E Delivery Board. All actions continue to be monitored and progressed, focusing on flow through the department and hospital, and for delayed transfers of care.
• Review and scoping of national requirement for all Minor Injury Units to be assigned as Urgent Treatment Centres or Primary Care facilities has commenced.
o SWFT have completed a gap analysis and are now costing the project.
o An updated plan with a timeline is anticipated to be presented to the C&W A&E delivery board in April.
o Workforce scoping has been undertaken Early indications from the daily data is that the 95% standard has been achieved for March.
Recovery Date: March 2019
EMERGENCY CARE TARGETS: 4 Hour Wait

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 9 of 20
111 Outcomes Performance
Out of Hours Performance: % A&E/Admission Referrals
111 Update • Call volumes have decreased slightly from January, which is in line with
previous trends. • There has been a small increase in the percentage of patients
recommended to attend A&E, however a slight reduction in how many are referred to OOH.
111 Service Improvement Actions: • The *5 service, continues to improve utilisation, with only 10%
paramedic calls through this service conveyed to ED. • The new national 111 online service in the West Midlands went
live in March. It will direct patients to the right healthcare, including whether they need to see a GP or seek urgent care; get advice on self-care and in most areas, get a call back from a nurse, doctor or other health professional if they need it. Impact is to be assessed.
• Refreshed improvement plan agreed and being monitored for calls answered in 60 seconds KPI, due to decrease in performance.
OOH Update • There has been a slight decrease in the number of calls from January to
February (92) this is expected as it is a shorter month. • This slight reduction is in line with the previous year trends. OOH Service Improvement Actions: • 4 Contract Performance Notices remain in place for;
o Time taken to call back a healthcare professional o Calls triaged within 60 minutes; discussions to amend the KPI
and therefore close CPN are in progress. o Urgents consulted within 2 hours o Urgents visited within 2 hours
• The performance of all KPIs with a CPN continue to improve and are still on track to deliver by May 2019.
• Revised action and improvement plan with narrative around ongoing work and internal actions and improvements made to support delivery.
EMERGENCY CARE TARGETS: 111 and OOH

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 10 of 20
SWFT Actions: • Capacity issues persist in Ophthalmology at the Warwick site, led by
eRS referrals into Warwick, rather than Stratford. Recruitment is underway for a substantive consultant, and a locum is also in place.
• General Surgery breaches relate to a small number of patients, which is being monitored by the senior team.
• Work between SWFT and NHS England on Orthodontic capacity is ongoing, and are continuing to advertising for a locum for additional sessions.
Out of Area Trusts Recovery Actions: • University Hospitals Coventry and Warwickshire:
o Currently not meeting trajectory agreed with NHS Improvement, the Trust is focussing on prioritising 45+ weeks.
• Worcestershire Acute Hospitals: o A specialty based trajectory, based on known and planned
capacity to meet on-going demand is being worked on to reduce the number of patients waiting over 40 weeks.
• University Hospitals Birmingham (HGS Sites): o Significant improvements over the last few months in ENT and
Ophthalmology backlogs, due to a recruitment drive. • Oxford University Hospitals:
o A harm review process is in place to review all patients waiting over 52 weeks
52 Week Waits • 1 x breach at Midland Eye Clinic, Ocular-Plastics
o Patient outsourced by UHB due to long waiting times. o Clock stop 6th March 2019.
CCG Issue: • Underachievement at out of area Trusts. SWFT Issues: • Specialties failing target are General Surgery, Gynaecology and
Ophthalmology. • The aggregate standard continues to be achieved through over-
performance in other specialties, including 95.6% in Orthopaedics.
Recovery Date: Quarter 4 2018/19
REFERRAL TO TREATMENT: Overview
NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 11 of 20
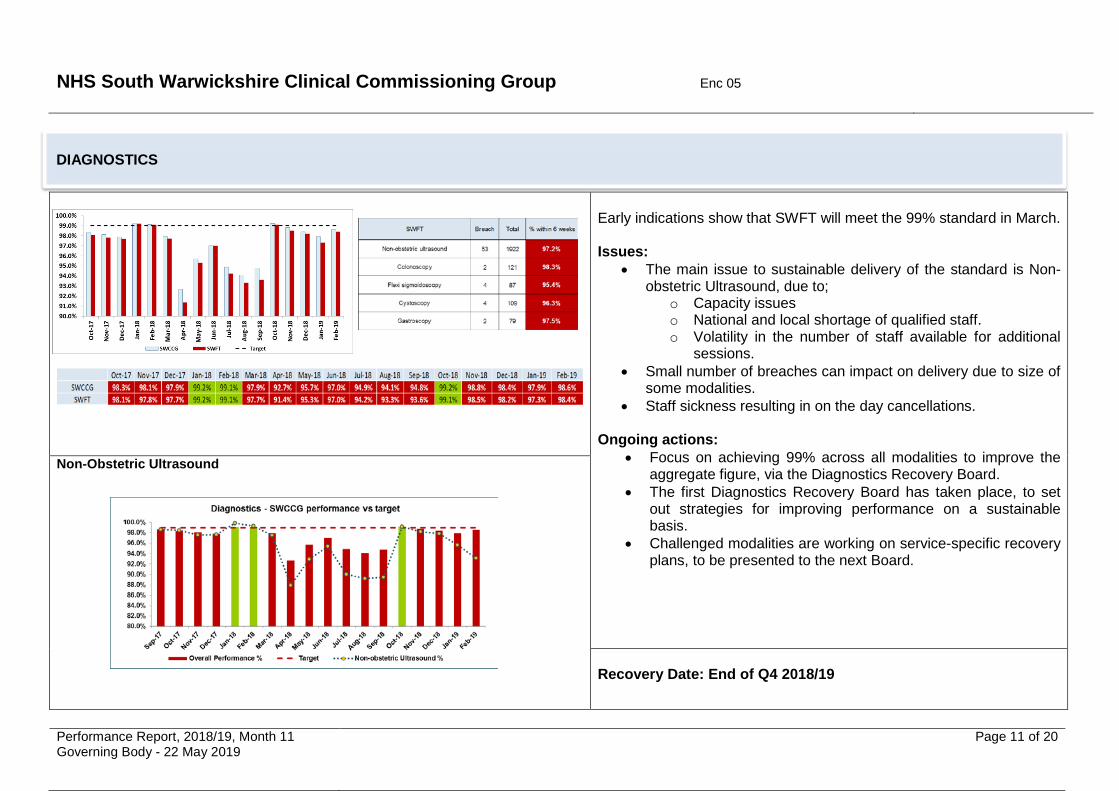
Early indications show that SWFT will meet the 99% standard in March. Issues:
• The main issue to sustainable delivery of the standard is Non-obstetric Ultrasound, due to;
o Capacity issues o National and local shortage of qualified staff. o Volatility in the number of staff available for additional
sessions. • Small number of breaches can impact on delivery due to size of
some modalities. • Staff sickness resulting in on the day cancellations.
Ongoing actions:
• Focus on achieving 99% across all modalities to improve the aggregate figure, via the Diagnostics Recovery Board.
• The first Diagnostics Recovery Board has taken place, to set out strategies for improving performance on a sustainable basis.
• Challenged modalities are working on service-specific recovery plans, to be presented to the next Board.
Non-Obstetric Ultrasound
Recovery Date: End of Q4 2018/19
DIAGNOSTICS

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 12 of 20
62 day Cancer Performance
14 patients (out of 74) have breached the 62 day standard in February 2019.
Issues:
• Delays at diagnostic stage due to a lack of diagnostic capacity. • Complex pathways for some specialties with onward referral to
tertiary centres, leading to late referrals. • Issues with the escalation of breached patients. • An increase in breaches during January, due to patients
postponing their treatment over the holiday period. Recovery Actions:
• SWFT have invited the NHS Interim Management And Support Team to review Cancer delivery at the Trust. The review will include;
o A diagnostic assessment of the Cancer action plan as to its sustainability.
o Recommendations for additional actions to improve performance.
• Additional support for Haematology Oncology from UHCW remains in place.
• Radiology clinicians continue to attend MDT. • Increased scrutiny on pathway has been sustained through the
Cancer Patient Tracking List meeting. • SWFT are still aiming to reduce 2ww times to 7 days • Oncology and Haematology service sustainability review is due in
April 2019. Performance has improved in March, and SWFT are still aiming to achieve 85% by March 2019.
62 day Breach Reasons – All Providers
104 Day Breaches – 4 in February:
o SWFT x 2 – delay in diagnostic testing o SWFT/UHCW – complex diagnostic pathway o SWFT/UHB – Reason not known
Recovery Date: End of Quarter 4 2018/19
CANCER
First Seen Provider
Adm
inis
trat
ive
dela
y
Com
plex
dia
gnos
tic
path
way
Inad
equa
te P
rovi
der
capa
city
Oth
er re
ason
(not
list
ed)
PATI
ENT
Cho
ice
Trea
tmen
t del
ayed
for
med
ical
reas
ons
Del
ay to
Dia
gnos
tic T
est
Gra
nd T
otal
1 3 1 1 3 91 1 2
1 1UHCW 1 1UHB 1 1
1 4 1 3 1 1 3 14
First Treatment Provider
UHCW
SWFTUHCW
Grand Total
SWFT
SWFT
UHB
NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 13 of 20
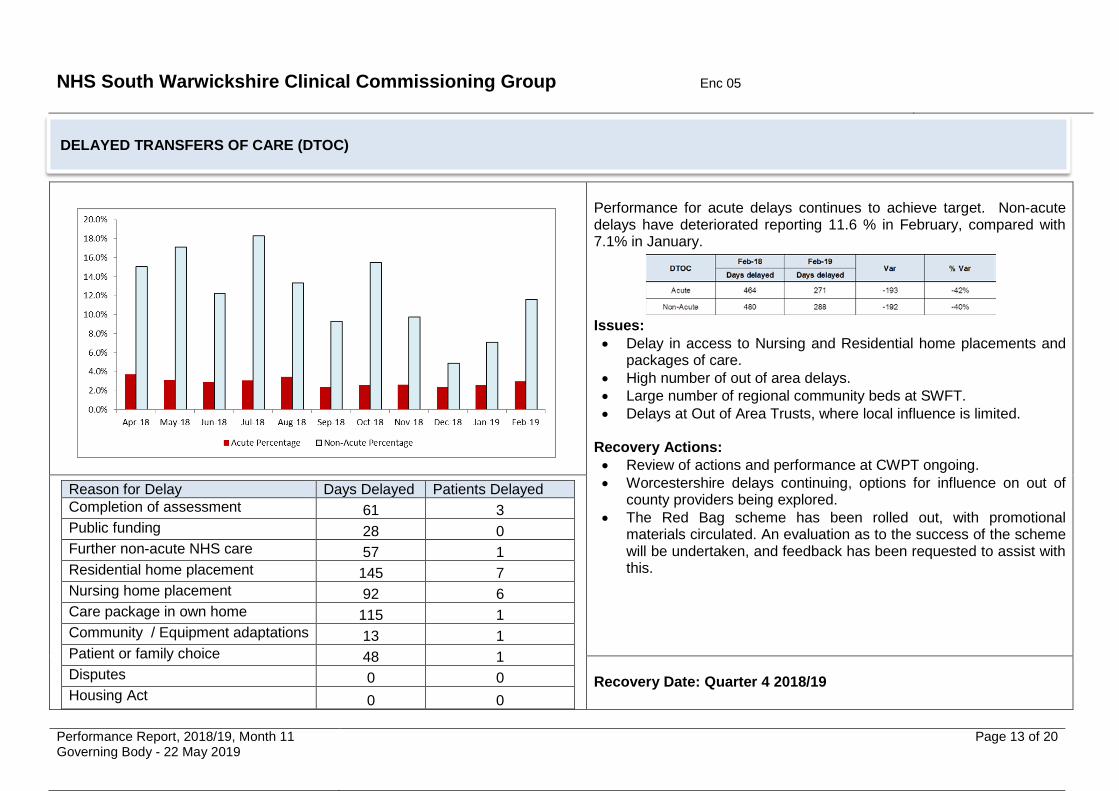
Performance for acute delays continues to achieve target. Non-acute delays have deteriorated reporting 11.6 % in February, compared with 7.1% in January. Issues: • Delay in access to Nursing and Residential home placements and
packages of care. • High number of out of area delays. • Large number of regional community beds at SWFT. • Delays at Out of Area Trusts, where local influence is limited.
Recovery Actions: • Review of actions and performance at CWPT ongoing. • Worcestershire delays continuing, options for influence on out of
county providers being explored. • The Red Bag scheme has been rolled out, with promotional
materials circulated. An evaluation as to the success of the scheme will be undertaken, and feedback has been requested to assist with this.
Reason for Delay Days Delayed Patients Delayed Completion of assessment 61 3 Public funding 28 0 Further non-acute NHS care 57 1 Residential home placement 145 7 Nursing home placement 92 6 Care package in own home 115 1 Community / Equipment adaptations 13 1 Patient or family choice 48 1 Disputes 0 0 Housing Act 0 0
Recovery Date: Quarter 4 2018/19
DELAYED TRANSFERS OF CARE (DTOC)
NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 14 of 20
Contract Performance Reported by Exception
Indicator Issue Action Recovery
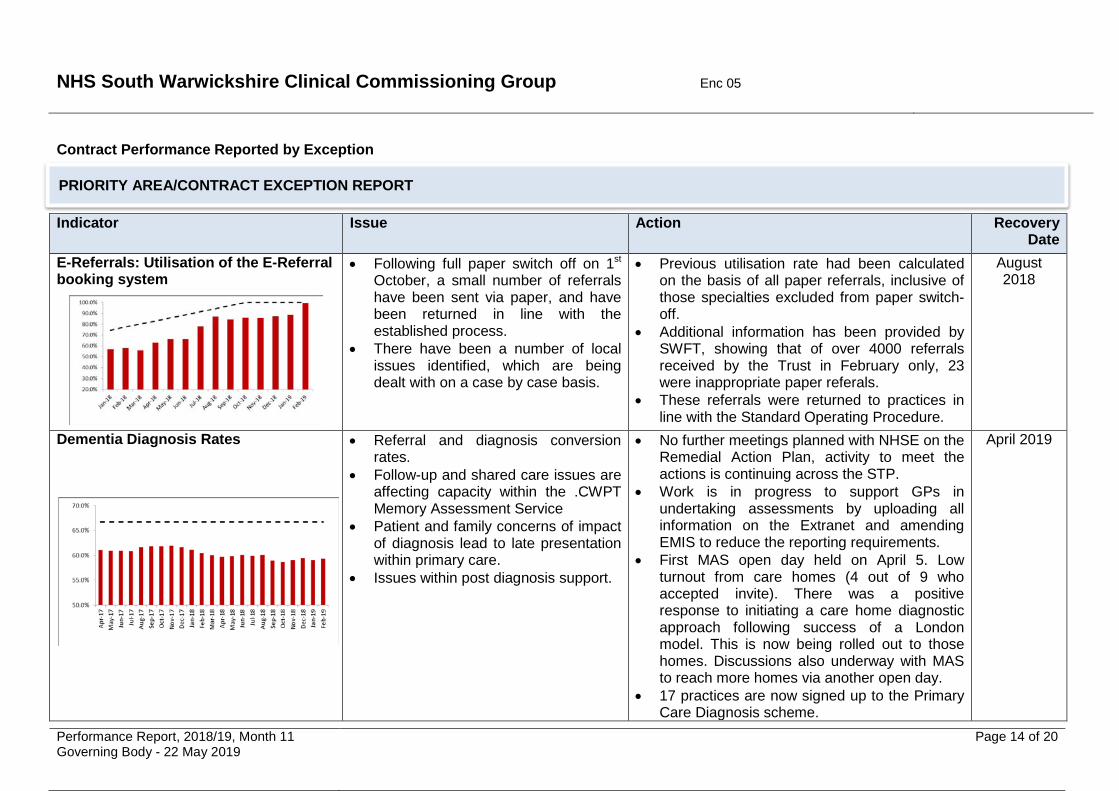
Date E-Referrals: Utilisation of the E-Referral booking system
• Following full paper switch off on 1st October, a small number of referrals have been sent via paper, and have been returned in line with the established process.
• There have been a number of local issues identified, which are being dealt with on a case by case basis.
• Previous utilisation rate had been calculated on the basis of all paper referrals, inclusive of those specialties excluded from paper switch-off.
• Additional information has been provided by SWFT, showing that of over 4000 referrals received by the Trust in February only, 23 were inappropriate paper referals.
• These referrals were returned to practices in line with the Standard Operating Procedure.
August 2018
Dementia Diagnosis Rates
• Referral and diagnosis conversion rates.
• Follow-up and shared care issues are affecting capacity within the .CWPT Memory Assessment Service
• Patient and family concerns of impact of diagnosis lead to late presentation within primary care.
• Issues within post diagnosis support.
• No further meetings planned with NHSE on the Remedial Action Plan, activity to meet the actions is continuing across the STP.
• Work is in progress to support GPs in undertaking assessments by uploading all information on the Extranet and amending EMIS to reduce the reporting requirements.
• First MAS open day held on April 5. Low turnout from care homes (4 out of 9 who accepted invite). There was a positive response to initiating a care home diagnostic approach following success of a London model. This is now being rolled out to those homes. Discussions also underway with MAS to reach more homes via another open day.
• 17 practices are now signed up to the Primary Care Diagnosis scheme.
April 2019
PRIORITY AREA/CONTRACT EXCEPTION REPORT

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 15 of 20
Indicator Issue Action Recovery Date
Improving Access to Psychological Therapies (IAPT): Access
• Workforce issues, leading to increased caseloads for existing staff.
• Accommodation issues related to increased requirement for staff, and therefore clinic space.
• Increase in awareness of, and referrals to, the service is required.
• Service Development Improvement Plan is being developed within the new 2019/20 contract, to focus on IAPT access.
• The group is intending to review IAPT access and produce a system-wide recovery plan.
• Commissioners liaising with NHS England regarding the expectations on co-locating IAPT and primary care for 2019/20.
• CWPT have drafted the trajectory, which will be shared with commissioners once data validation is complete.
March 2019
Early Intervention in Psychosis Waits
• Care Coordinators experiencing capacity issues and increased caseloads due to workforce.
• Due to workforce issues, treatment pathways are shorter than recommended by NICE.
• The Intensive Support Team report, was circulated on 1st April.
• Recommendations from the report are split into themes, including Model Fidelity, Information and Reporting, Investment, Service Users and Carers.
• Following on from this, and acting on one of the recommendations from the report, a working group is being convened to review the recommendations and produce an action plan.
• 2 care coordinators are due to commence in post in April and May 2019. Interviews for the third post have been held, but the outcome is not yet known.
March 2019
PRIORITY AREA/CONTRACT EXCEPTION REPORT

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 16 of 20
Indicator Issue Action Recovery Date
Looked After Children (Quarterly)
• For Month 9, 37 out of 54 children had received a LAC Health Plan Review and Report within 12 months, and 7 out of 21 children had received an initial health assessment within 13 days.
• The workforce reviewing Looked After Children is within the same pool as other core CAMHS activities, and therefore is subject to similar issues of workforce and complex patients.
• KPIs are not reflective of the work of the LAC service.
• Percentage figures provided relate to CWPT as a provider, and cannot be supplied at Commissioner level. CWPT has received 4 South Warwickshire CCG referrals, to Q3.
• LAC Recovery Plan has been submitted to CRCCG, key areas for focus are; o Review current position for Health
Assessments, Plan Reviews and Reports; o Review reporting requirements; o Reassess initial capacity and demand
modelling undertaken; o Benchmarking against other areas; o Review how demand is managed within
the service; o Recovery trajectory to be modelled and
submitted to Commissioners. •
March 2019
PRIORITY AREA/CONTRACT EXCEPTION REPORT

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 17 of 20
Indicator Issue Action Recovery
Date Children and Young People’s Emotional Well-Being and Mental Health (CYP)
• Acute Liaison (ALT) capacity issues impacting on core CAMHS staffing, as staff are being used to cross-cover ALT.
• There is significant, ongoing pressure on clinical capacity, which is being outstripped by demand.
• Increased utilisation of the navigation hub impacting on workforce and triage timeframes.
• Workforce issues due to maternity leave across CAMHS services.
• Work is ongoing to improve waiting times at the front end of the pathway, which will benefit follow up waiting times, due to additional capacity within the system as a whole.
• Risk stratification of long waiting patients is continuing, to ensure that patients are treated in order of clinical priority.
• Review of Navigation Hub processes is ongoing.
TBC
Children and Young People’s Autism Spectrum Disorder Waits (CYP ASD)
• Due to the requirements for a multi-professional and multi-agency approach to assessments, developing remedial plans is complex.
• Demand for assessments is exceeding capacity available.
• Shortage of qualified staff to undertake assessments nationally.
• Following the Children and Young People’s ASD workshop in January, a number of immediate actions have been adopted by the Integrated Commissioning Team.
• Outputs from the workshop are still expected to be discussed at the next Transforming Care Commissioners Group meeting on 25th April to determine what the next steps should be.
• Work is progressing to identify an SRO to lead on a system wide approach to CYP ASD
• Any work undertaken will also link in with the ASD Joint Strategic Needs Assessment that is in development within Warwickshire County Council.
TBC
PRIORITY AREA/CONTRACT EXCEPTION REPORT
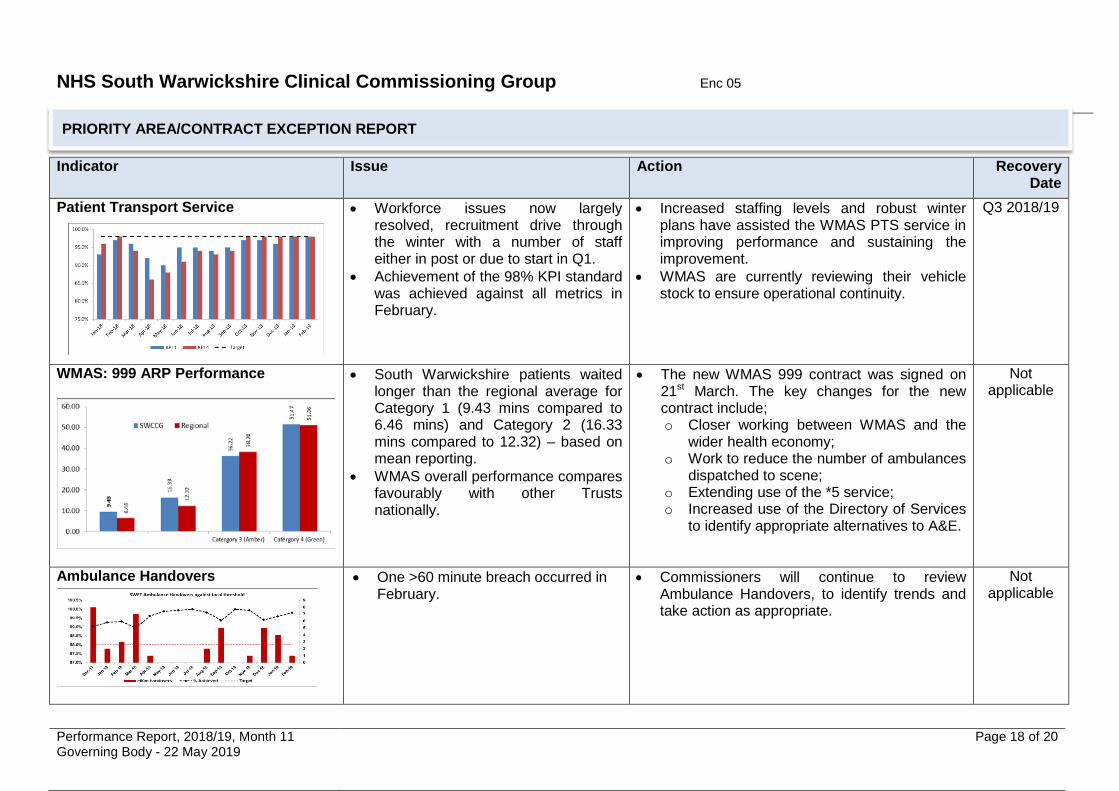
NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 18 of 20
Indicator Issue Action Recovery Date
Patient Transport Service
• Workforce issues now largely resolved, recruitment drive through the winter with a number of staff either in post or due to start in Q1.
• Achievement of the 98% KPI standard was achieved against all metrics in February.
• Increased staffing levels and robust winter plans have assisted the WMAS PTS service in improving performance and sustaining the improvement.
• WMAS are currently reviewing their vehicle stock to ensure operational continuity.
Q3 2018/19
WMAS: 999 ARP Performance
• South Warwickshire patients waited longer than the regional average for Category 1 (9.43 mins compared to 6.46 mins) and Category 2 (16.33 mins compared to 12.32) – based on mean reporting.
• WMAS overall performance compares favourably with other Trusts nationally.
• The new WMAS 999 contract was signed on 21st March. The key changes for the new contract include; o Closer working between WMAS and the
wider health economy; o Work to reduce the number of ambulances
dispatched to scene; o Extending use of the *5 service; o Increased use of the Directory of Services
to identify appropriate alternatives to A&E.
Not applicable
Ambulance Handovers
• One >60 minute breach occurred in February.
• Commissioners will continue to review Ambulance Handovers, to identify trends and take action as appropriate.
Not applicable
PRIORITY AREA/CONTRACT EXCEPTION REPORT

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 19 of 20
Indicator Issue Action Recovery Date
Transforming Care: CCG Cohort (Overall TCP) Of 25 adult CCG patients, 10 are SWCCG patients.
Transforming Care: NHSE Cohort (Overall TCP) Of 29 people in NHSE commissioned beds, 6 are SWCCG patients.
The Transforming Care Partnership is on red escalation by NHSE due to the number of people in hospital above the trajectory. Contributing factors: • High number of children and young
people in Tier 4 CAMHS inpatient services.
• Increase in admissions to CCG assessment, treatment and MH beds. This follows a reduction in 2016/17 and Q1-3 2017/18 following new community intensive support service for adults with LD.
• In 2017/18, 90% of CCG admissions did not have a community care and treatment review prior to admission, highlighting a gap in local systems to identify admission risks. 59% had an emergency pre-admission review - community CTRs and CETRs provide more opportunity to prevent admissions.
• Challenges with finding the right community provider - some discharges have been delayed for complex patients.
The TCP has identified priority areas that will have most impact in supporting delivery (programme, commissioning, clinical, and operational). Associated delivery actions include: • Admission of adults to CCG beds continues to be
above the level required to achieve trajectory and RCA reveals system gaps in ensuring people with ASD and mental health needs can access support that is reasonably adjusted.
• Arden is an accelerator site for CYP and is mobilising additional support in the community for young people with ASD as well as developing a single planning framework for health, social care and education.
• A Workforce Strategy has been developed and funding identified to commission ASD awareness training for 650 people across health, social care, independent and voluntary sector and family carers.
• An All Age ASD strategy is being co-produced across the TCP with associated needs analysis due for completion Q1.
• NHS England has confirmed that the Transforming Care Programme is continuing in 2019/20. As the Arden TCP team resource will not be continuing, the TCP is focussing on establishing business as usual processes during the Quarter 1 handover period.
End of Quarter 2 2018/19 (revised
June 2018 from Q1)
PRIORITY AREA/CONTRACT EXCEPTION REPORT

NHS South Warwickshire Clinical Commissioning Group Enc 05
Performance Report, 2018/19, Month 11 Governing Body - 22 May 2019
Page 20 of 20
End of Report
Indicator Issue Action Recovery Date
Referral to Treatment Waiting Times: Wheelchairs Children’s Wheelchair Performance:
Adult’s Wheelchair Performance:
Demand and Capacity • Increase in demand and
complexity due to an aging population.
Workforce • The service has staffing issues
primarily due to vacancies and long term sickness.
• Up to 20% clinical capacity reduction due to recruitment issue.
Data Quality • Initial Lorenzo RTT and Best
System review identified a variance in backlog numbers linked to re-opening of RTT pathways in the Best (Community) System.
Specialist Chair Prescriptions • The Trust have identified that there
are an outlier for the % of Specialist Chairs prescribed.
• The prescribing of specialist chairs is highly labour intensive and complex, further reducing the capacity to manage the service.
• Following improved children’s performance in March, NHS England and the CCG are assured that the changes made to the operational management of the service have had a positive effect on performance, which is to continue into 2019/20.
• The service has made significant changes to the way patients are managed which has meant improved performance.
• NHS England have confirmed that they have received sufficient assurance to reduce the level of their oversight of the service, but will be monitoring performance.
• The CPN and associated Remedial Action Plan will remain in place for 2019/20, with a refresh of the action plan to align to the updated actions and focus.
End of Quarter 4
PRIORITY AREA/CONTRACT EXCEPTION REPORT

NHS South Warwickshire Clinical Commissioning Group Enc 06 ___________________________________________________________________________
_________________________________________________________________________________________ Nursing, Quality and Governance Report Governing Body – 22 May 2019
Report To: Governing Body For decision
Report Title: Nursing, Quality and Governance Report For discussion √
Report From: Alison Walshe Chief Nurse
For information
Date: 22 May 2019 Confidential
Purpose of the Report:
To update Governing Body members regarding nursing, quality and governance matters.
Key Points:
This report provides an overview of current nursing, quality and governance matters, as discussed in detail at Clinical Quality and Governance Committee and Performance Committee.
Recommendation (s):
That Governing Body members note the content of this report.
Previously Considered By: Date:
- -
CCG Strategic Objective(s) this report relates to:
Out of Hospital Personalisation √ Specialist Provision
Delivering Today √
Management of Conflicts of Interest: Not applicable.
Financial Implications: Not applicable
Performance Implications: The CHC targets relating to acute assessments and 28 days fall within the Quality Premium scheme.
Quality Implications: Report focused on nursing, quality and governance.
Equality and Diversity Considerations: Not applicable.
Patient, Public and Stakeholder Engagement: Not applicable.
Risk Assessment: Quality and Governance are areas of high priority for the CCG.

NHS South Warwickshire Clinical Commissioning Group Enc 06
Nursing, Quality and Governance Report Governing Body – 22 May 2019
Page 2 of 10
Introduction 1.1 This report provides an update to Governing Body on nursing, quality and governance
matters. Nursing and Quality Contractual Quality 2.1 The latest quality dashboards for SWFT were discussed at Clinical Quality and Governance
committees at the end of March and early May (Appendix 1 shows the position at the end of February). The committee noted the improvement in A&E response rates and will continue to monitor these carefully to determine whether further contractual action is required. Patient satisfaction with the A&E service at SWFT remains well above the national average. Inpatient satisfaction levels at SWFT have reduced to below the national average in recent months. This will be discussed with SWFT at a forthcoming clinical quality review meeting and continue to be monitored. Satisfaction with maternity services, meanwhile, is higher than the national average, as is the case for outpatient services.
Infection Prevention and Control 2.2 The end of year C difficile rates for south Warwickshire showed a significant improvement on
previous years with the CCG ending the year at 65 cases against the target of 59, of which 10 are attributable to the acute trust and 55 are attributable to the community. This continues to compare favourably to the equivalent period during 2017/18 and to date there have been 17 fewer cases during 2018/19, representing a 20% reduction. Of the cases acquired by SWFT, no lapses in care have been identified. Whilst it is disappointing we missed our target the performance is a testament to the hard work undertaken across the whole health economy to reduce C difficile infections.
2.3 New guidance on C difficile objectives has now been released for 2019/20. The CCG’s
tolerance targets have increased from 59 cases in 2018/19 to 68 cases for 2019/20. 24 cases are allocated to the acute sector and 44 to the community. The emphasis is on avoiding a culture of blame but identification of any lapses in care in which CDI is acquired is still required. The objectives are based on the forecast outturn from 1 April 2018 – 31 December 2018 using the new case definitions.
Mortality 3.1 Table 1 below demonstrates mortality figures (SHMI) at the CCG’s major acute providers.
Please note that there is no change from the previous report as the next publication is due sometime during May 2019.
3.2 As can be seen, SHMI rates at OUH and SWFT are stable and within the anticipated range.
Rates at both UHCW and WAHT have, however, been increasing steadily since October 2016, albeit the SHMI for UHCW showed a slight reduction in June and September 2018. Host
TRUSTSHMI Value
published 22/3/18 (Oct 16 - Sept 17)
SHMI Value published 19/7/18 (Jan 17 - Dec 17)
SHMI Value published 20/9/18 (Apr 17 - Mar 18)
SHMI Value published 22/11/18
(Jul 17 - Jun 18)
SHMI Value published 14/02/19 (Oct 17 - Sept 18)
OUH (Oxford University Hospitals NHS Foundation Trust) 0.9228 0.9309 0.9202 0.9187 0.9210
SWFT (South Warwickshire NHS Foundation Trust) 1.0333 1.0103 1.0051 1.0030 0.9912
UHCW (University Hospital Coventry and Warwickshire NHS Trust) 1.0928 1.1197 1.1333 1.1203 1.1202
WHAT (Worcestershire Acute Hospitals NHS Trust) 1.0453 1.0476 1.0584 1.0921 1.1132

NHS South Warwickshire Clinical Commissioning Group Enc 06
Nursing, Quality and Governance Report Governing Body – 22 May 2019
Page 3 of 10
commissioners (Coventry and Rugby CCG and Worcestershire CCGs) take a lead in working with the Trusts to address mortality rates.
3.3 LeDeR steering group meetings continue on a quarterly basis in 2019/20. Up until the 31
March 2019 there have been 71 notifications across the Arden Transforming Care Partnership (TCP) footprint since the LeDeR programme commenced on 1 October 2017. South Warwickshire CCG have had 23 notifications of deaths of people with a learning disability and out of the 23 reviews: 18 (78%) have been completed and signed off by Bristol University, 3 are with allocated reviewers but remain incomplete, one LeDeR notification was noted as a child death and will be managed by the child death process and 1 is unassigned. Through the LeDeR steering group, numbers will continue to be monitored against the trajectory submitted to NHSE.
3.4 The monies from NHSE have been agreed to be used for an independent reviewer and a post
holder is now in post with an allocated review. The allocation of cases to this reviewer will be monitored to ensure equal access for all 3 CCGs.
3.5 Learning from the local reviews has been categorised, as detailed in Table 2 below. For some
patients learning will span a number of categories but access to annual health checks, inadequate end of life care, provision of general inpatient care, poor liaison with or support for family, and insufficient social services support are emerging so far as key areas of concern. This learning will be taken into relevant forums for action: e.g. clinical quality review meetings with providers; Transforming Care Partnership Board; learning disabilities commissioning group.

NHS South Warwickshire Clinical Commissioning Group Enc 06
Nursing, Quality and Governance Report Governing Body – 22 May 2019
Page 4 of 10
Safeguarding 4.1 A separate paper is on the Governing Body agenda for approval in relation to proposals for
future arrangements for both the Adults’ and Children’s Safeguarding Boards.
4.2 Tracy Redgate, Adults’ Safeguarding Lead Nurse, has recently indicated her decision to retire at the end of June. Work is underway between the three CCGs to determine the most appropriate way to fill this statutory post but I would like to formally thank Tracy for her significant contribution to adult safeguarding in Warwickshire over a number of years.
4.2 Discussions continue with SWFT in respect of recruitment to the post of Designated Doctor for Child Protection/Child Death Overview in the context of required changes to the Child Death Overview Panel where revised national guidance was published last year. Current interim arrangements (supported by a community paediatrician at SWFT) continue whilst options are re-considered.
Looked After Children
5.1 At their meeting in March, Clinical Quality and Governance Committee discussed, in detail, the Health of Looked After Children Annual Report.
5.2 A workshop was held earlier in May between key partners to discuss how to prioritise and take forward the recommendations of this report, some of which relate to the quality of existing services and some of which relate gaps in commissioning. An action plan is being developed to ensure the recommendations of the Designated Doctor and Nurse are taken forward so that the needs of this vulnerable group of children are appropriately met. The action plan will be reported back to Clinical Quality and Governance Committee in due course.
Continuing Healthcare 6.1 The CCG continues to achieve the two quality premium targets in relation to acute hospital
assessments and 28 day assessments. The table below provides detail of the 28 day performance for the whole of 2018/19.
April May June July Aug Sept Oct Nov Dec Jan Feb Mar Trajectory 50% 50% 54% 70% 80% 80% 80% 80% 80% 80% 80% 80% % Achieved
45.61 48.57 35.29 63.38 84.21 91.49 95.77 97.26 97.44 97.67 98.08 100
6.2 Whilst work on appeals and retrospective cases is prorgressing, regrettably staff sickness and
vacancies are once against compromising progress in this area. Regular, detailed, updates are provided to Performance committee and the CCG continues to try to recruit additional RGN and RMN staff.
Personal Health Budgets 7.1 The CCG ended 2018/19 with a cumulative position of 45 Personal Health Budgets (PHB).
The current PHBs are held by 25 adults who are eligible for Continuing Healthcare and 1 child within the Transforming Care programme, 27 of whom have a notional budget and 18 a direct payment/third party budget.
Transforming Care 8.1 The Transforming Care programme includes individuals who have a Learning Disability and/or
Autism with behaviour that challenges who are at risk of admission or are admitted to learning disability/mental health inpatient beds. As at the end of March CCG had 8 adults in hospital in CCG commissioned beds, although late notification of a March discharge meant that the figure

NHS South Warwickshire Clinical Commissioning Group Enc 06
Nursing, Quality and Governance Report Governing Body – 22 May 2019
Page 5 of 10
reported to NHS England was 9. All individuals at risk of an admission receive a Care and Treatment Review (CTR) to avoid an admission where possible or agree that an admission is appropriate. During Quarter 4 there were 2 admissions,1 new diagnosis during an existing admission, 1 child who turned 18 and moved to an adult inpatient bed and 2 discharges.
8.2 As of 31st March there were also 6 south Warwickshire residents meeting Transforming Care
criteria currently in beds within services commissioned by NHS England. There has been an improvement in the number of children and young people in the Transforming Care cohort in CAMHS tier 4 beds, with no admissions during Quarter 4.
Low secure
Medium secure
High secure
CAMHS Tier 4
Adult 0 2 0 0
Child 0 0 0 4
8.3 During Quarter 4 there were 2 CAMHS Tier 4 (Transforming Care cohort) children’s discharges and 1 young person who turned 18 and moved into the adult cohort.
8.4 In March 2019 the Coventry, Warwickshire and Solihull Transforming Care Partnership remained on red escalation by NHSE as a result of under performance against the trajectories to reduce the number of people in hospital. A recovery action plan remains in place at both local and partnership levels and new trajectories have been agreed for the next two years. The table below details performance against the CCG trajectory for inpatient admissions by the end of the programme in March 2019.
People in SWCCG beds as at 31/3/19
Target March 2019
People in NHSE beds as at 31/3/19
Target March 2019
9 3 6 5
Governance 9.1 A key focus of March and April has been the creation of the 2018/19 Annual Report, with the
official draft being submitted to NHSE ahead of the 18 April deadline. Following minor feeback from NHSE, the draft was submitted to Members’ Council for approval. Final approval will be sought from Audit Committee (which has delegated authority from Governing Body), with submission scheduled for 24 May.
9.2 The 2018/19 Data Security and Protection Toolkit was completed in March with the CCG
confirming full compliance. 9.3 Weekly and Daily EU-exit SitRep returns to NHSE began in March, ceasing in mid-April with
the decision to delay the UK’s exit. 9.4 The CCG submitted a fully compliant annual Conflicts of Interest return, with over 95% of staff
and Governing Body members completing the annual training. 9.5 Training for staff and line managers is underway in respect of:
• rolling out ESR (Employee Staff Record system) self-service; and • implementing the Performance Development Review Framework following Governing
Body approval in March.

NHS South Warwickshire Clinical Commissioning Group Enc 06
Nursing, Quality and Governance Report Governing Body – 22 May 2019
Page 6 of 10
Recommendation 10.1 That Governing Body members note the content of this report.

NHS South Warwickshire Clinical Commissioning Group Enc 06 ___________________________________________________________________________
_________________________________________________________________________________________ Nursing, Quality and Governance Report Governing Body – 22 May 2019
Appendix 1 Quality Dashboard 2018/19 (Contract quality data relates to reporting period of December 2018 to February 2019)
MONTHLY HIGHLIGHT QUALITY DASHBOARD Trend / Graph /
CommentsData as of 25.04.19
Organisation
Data Source Jan-19 Feb-19 Mar-19 Trend from Feb 2018 -Feb 2019 position
Patient SafetySWFT 7 5 5UHCW 0 0 1CWPT 2 2 1
Serious Incidents- overall number per month at local providers relating to SWCCG patients
SWCCG Total 9 7 7
NHS111 1 0 0MSI 0 0 0
Serious Incidents- overall number per month at other contracted providers relating to SWCCG patients SWCCG Total 1 0 0
Serious Incidents at out of area providers relating to SWCCG patients: 0 0 0
Never Events SWFT 1 0 0Included in the SWFT total
figure of 7 for Jan 19
Infection Control Jan-19 Feb-19 Mar-19C Difficile - Total monthly number reported by SWFT SWFT 0 0 0C Difficile - Total number reported by SWFT YTD 2018/19 (Nb: tolerance = total of 5 avoidable cases for the year) SWFT 8 8 8
MRSA SWFT 0 0 0Patient Experience Dec-18 Jan-19 Feb-19Friends & Family Test (FFT) at SWFTInpatient Areas Trajectory (Threshold Dec 18 to Feb 19 =>25% )
SWFT Response Rates 24.3% 19.3% 25.3%NHSE Average Response Rates NHSE NHSE 21.7% 23.7% 24.2%
SWFT % patients recommending the service SWFT NHSE 95.0% 94.0% 95.0%NHSE Average % patients recommending the service NHSE NHSE 95.0% 95.0% 96.0%
A&E Department (Response Rate Trajectory Threshold Dec 18 =>9% / Jan 19 =>10% / Feb 19 =>11% )
SWFT Response Rates SWFT NHSE 3.3% 7.9% 14.2%NHSE Average Response Rates NHSE NHSE 11.4% 11.9% 12.2%
SWFT % patients recommending the service SWFT NHSE 95.0% 92.0% 91.0%NHSE Average % patients recommending the service NHSE NHSE 86.0% 86.0% 85.0%
Maternity Services (Response Rate Trajectory Threshold =>23.3% ) Birth Question 2 SWFT Response Rate % 23.0% 29.0% 18.0%
Birth Question 2 NHSE Average Response Rate % NHSE NHSE 18.4% 21.8% 22.2%SWFT % patients recommending the service SWFT NHSE 96.0% 97.0% 98.0%
NHSE Average % patients recommending the service NHSE NHSE 97.0% 97.0% 97.0%All Community Health Areas (Threshold =>97 %)
SWFT % patients recommending the service SWFT NHSE 95% 98% 96%
NHSE Average % patients recommending the service NHSE NHSE 96% 96% 96%All Outpatient Areas (Threshold => 95%)
SWFT % patients recommending the service SWFT NHSE 93% 96% 96%
NHSE Average % patients recommending the service NHSE NHSE 94% 94% 94%
Complaints SWFT 11 24 13Clinical Outcomes at SWFT Dec-18 Jan-19 Feb-19SHMI (rolling 12 months Oct 17 to Sept 18 ) SWFT SWFT 0.99RAMI ( rolling 12 months Mar 18 to Feb 19 ) SWFT SWFT 76 73.7 74.4
SWCCG Patient Safety Team
Serious Incidents at local providers relating to SWCCG patients:
Serious Incidents other contracted services relating to SWCCG patients:
1.00

NHS South Warwickshire Clinical Commissioning Group Enc 06
Nursing, Quality and Governance Report Governing Body – 22 May 2019
Page 8 of 10
Contract Exceptions & Notes Threshold Dec-18 Jan-19 Feb-19
Trustwide
TW2C Perform local audits to identify the percentage of patients receiving appropriate prophylaxis
According to agreed audit programme
Action plan and second audit of patients on surgical w ards due
TW28 Staff ing: Reduction in Sickness Absence: All directorates including Out of Hospital Care (Community) & Women and Children's (Acute and Community).
Trust w ide Division total threshold <4.0% 5.11% 5.96% For details please refer to report
TW29 Staff ing: Personal Development Review : Percentage of PDR compliance Threshold >80%
Corporate Division 61.69%
Elective Care Division 85.67%
Emergency Care Division 78.70%
Out of Hospital Services 88.88%
Support Services Division 81.27%
Women & Children Service 82.51%
TW30 Achieve ESR Turnover rate target by all directorates including Out of Hospital Care (Community) & Women and Children's (Acute and Community). Threshold: <13.5%
All Divisions together Average 14.47% For details please refer to report
TW26 Mandatory training To achieve an combined mandatory training compliance of 85%
For details please refer to report
TW31a Trust-w ide: Acute and Community inpatients and CERT Teams. Dementia & Delirium; Find, Assess and Investigate Dementia & Delirium
% Total compliance for screening 82.50% 80.80% 82.50%
% Total compliance for investigation 50.00% 71.00% 16.70%
Safeguarding
Corporate Division Level 3 100%
Elective Care Division Level 3 100%
Emergency Care Division Level 3 94%
Out of Hospital Services Level 3 77%
Support Services Division Level 3 100%
Womens & Children Service Level 3 97%
Overall Total Compliance 90%
For details please refer to report.
SW9 & SG11 Safeguarding Vulnerable Children and Young people Compliance . Mandatory Training. All staff are trained to an appropriate level in safeguarding and promoting the w elfare of children and young people Threshold 90%
Contract Performance Notice issued 23/10/17. Compliance levels improved. Please refer to report for further details.
90% or more at the end of each quarter
For details please refer to report

NHS South Warwickshire Clinical Commissioning Group Enc 06
Nursing, Quality and Governance Report Governing Body – 22 May 2019
Page 9 of 10
Acute
A1 Safer Surgery Checklist - continued compliance 100% 100% 100% 100%
A2 Safer Surgery Checklist - full completion 98% 99.38% 97.37% 100%
A5 A maximum tw o w eek w ait standard for rapid access chest pain clinic 98% to be seen w ithin 2 w eeks 98% 98% 96.00% For details please refer to report.
Stroke
STR17 Stroke 90% stay on stroke unit 90% 81% 73% 71% Contract Performance Notice issued 23/10/17. Joint Investigation undertaken. Please refer to report for further details.
Maternity
MT2 Breastfeeding status to be recorded at discharge from Trust inpatient services 95% 95.71% 95.85% 93.15%
MT5 Promoting Vaginal Birth. Reduction in caesarean section rate.Previously not to exceed 26.5% /
Revised Nov 18 not to exceed 28% 38.82% 28.51% 28.83% For details please refer to report
MT8 Detection on foetal grow th restriction 68% 42% Quarterly reporting. For details please refer to report.
MT9 All w omen know n to midw ifery to be referred to Health Visiting Service at booking 100% of w omen know n to midw ifery referred to Health Visiting
95.12% 98.10% 94.21% For details please refer to report.
MT10 Breast feeding – increase in breast feeding initiation rates 81% 78.10% 83.80% 77.80% For details please refer to report
MT15A All w omen w ho smoke should be offered referral to Smoking Cessation Service (includes signposting to smoking cessation)
100%
MT15B All w omen w ho smoke should be offered Carbon Monoxide Testing at 36 w eeks gestation
65.47%
MT17 Appropriate inpatient staff ing levels to provide 1-2-1 midw ifery care in established labour
100% of w omen 89% 93% 98.80% For details please refer to report
For details please refer to report100% of w omen

NHS South Warwickshire Clinical Commissioning Group Enc 06
Nursing, Quality and Governance Report Governing Body – 22 May 2019
Page 10 of 10
Blank Page
End of Report

NHS South Warwickshire Clinical Commissioning Group Enc 07
Transition Case for Change Governing Body Meeting – 22 May 2019
Page 1 of 2
Report To: Governing Body For decision
Report Title: Proposal for Clinical Commissioning in Coventry & Warwickshire - Transition Case for Change
For discussion
Report From: David Spraggett, Chair
Liz McLean, Programme Lead
For information
Date: 22 May 2019 Confidential
Purpose of the Report:
To provide information on which the CCG can recommend a preferred option on future commissioning organisation arrangements to CCG member practices for decision.
Key Points:
In response to the requirements in the NHS Long Term Plan, a case for change to evolve health commissioning in Coventry & Warwickshire has been developed covering the three local CCGs covering that footprint.
The Governing Body is asked determine a preferred option to be recommended to the Member Practices for decision, following the requirements set out in the CCG’s Constitution.
The NHS South Warwickshire CCG Constitution sets out in the Terms of Reference for the CCG Members’ Council that it; ‘Approve any proposal to merge or federate with any other CCG’. (Constitution Appendix 6)
Recommendation (s):
1. That the Governing Body support Option 3;
2. That Member Practices are invited to choose (by voting) Option 2 or Option 3.
Previously Considered By: Date:
Not applicable -
CCG Strategic Objective(s) this report relates to:
Out of Hospital Not applicable
Personalisation Not applicable
Specialist Provision Not applicable
Delivering Today
Management of Conflicts of Interest:
All Governing Body Members have a Financial and Professional conflict of interest in the proposal as the positions they currently hold may be at risk should either Option 2 or 3 be put forward by the Governing Body for approval by the CCG Membership.
The control on this conflict of interest is the Governing Body’s consideration and recommendation of a preferred option in the public meeting.
Financial Implications: Requirement to deliver 20% reduction in running costs by 2021
Performance Implications: Not applicable
Quality Implications: Not applicable

NHS South Warwickshire Clinical Commissioning Group Enc 07
Transition Case for Change Governing Body Meeting – 22 May 2019
Page 2 of 2
Equality and Diversity Considerations:
Not applicable
Patient, Public and Stakeholder Engagement:
Stakeholder engagement has taken place and is described in detail in the paper.
Risk Assessment:
Should the Governing Body not support the recommendation of Option 3 to the Members, the CCG would be at risk of: not achieving the NHS Long Term Plan’s aspiration of a single commissioning voice for an Integrated Care System; and not achieving the 20% reduction in running costs by 2021.

TRANSITION CASE FOR CHANGE
PROPOSAL FOR CLINICAL COMMISSIONING IN COVENTRY &
WARWICKSHIRE
Liz McLean [email protected]
Abstract This document aims to outline the Case for Change for the future working arrangements of NHS Coventry & Rugby Clinical Commissioning Group (CCG), NHS South Warwickshire CCG,
and NHS Warwickshire North CCG, currently acting as commissioning partners in the Coventry & Warwickshire Sustainability and Transformation Partnership (STP)
It describes the context and identifies the engagement feedback and overall narrative for the process of considering the options for change. It recommends a preferred option. It also
includes information addressing the 11 tests required by NHS England for mergers of CCGs as defined in April 2019.
It is drafted for an intended audience of high-level, informed stakeholders.
Enc 07a
Page 2 of 39
DOCUMENT HISTORY COVER SHEET
DOCUMENT TITLE CCGs Case for Change
VERSION / DATE CREATED 16 May 2019
VERSION DATE SAVED BY NOTES 0 05 05 19 LM Initial Draft 1 9.05.19 GE Inclusion of comments from GE 2 12.05.19 LM Inclusion of comments from GE, AG, & Region
3 14.05.19 LM Inclusion of comments and material from AG, AH, S’OH, CH, PS, AW
4 15.05.19 LM Inclusion of provider feedback & restructuring 5 15.05.19 LM Inclusion of comments from AG, GE 6 16.05.19 LM Addition of further ONS data
FINAL 16.05.19 LM Paper approved for submission to Governing Bodies by AG and GE

Page 3 of 39
Table of Contents
Introduction ............................................................................................................................... 5
Background ............................................................................................................................... 6
The CCGs ................................................................................................................................... 7
CCG profiles .............................................................................................................................. 8
Current joint working arrangements in relation to contracts and services ............. 9
Local population .................................................................................................................... 11
Local health needs ................................................................................................................ 13
Sustainability and Transformation Partnership ............................................................ 15
Primary Care Networks ........................................................................................................ 16
Delivery at Place .................................................................................................................... 17
Vision ........................................................................................................................................ 19
Integrated Care Systems ..................................................................................................... 19
Future arrangements ............................................................................................................ 21
Expected benefits of greater alignment ........................................................................... 21
Current progress .................................................................................................................... 22
Future aspects of working together in Place ................................................................. 24
Financial position .................................................................................................................. 24
Stakeholder engagement ..................................................................................................... 25
Stakeholder events ................................................................................................................ 26
Governing bodies .................................................................................................................. 27
Members ................................................................................................................................... 27
Local health and wellbeing leads ...................................................................................... 28
Staff ........................................................................................................................................... 28
Patients ..................................................................................................................................... 28
Criteria for reviewing scenarios ......................................................................................... 28
Stakeholder responses ........................................................................................................ 29
Support for change ............................................................................................................... 29
A full merger was the most preferred scenario ............................................................. 29
Joint management team across three CCGs first before moving to full merger .. 29
Building robust “Places” – and not losing local identity – is critical to success 30
Involving the local population and their representatives is seen as another critical measure of success .............................................................................................................. 30
Supporting staff is vitally important ................................................................................. 30
“Do nothing” is not a viable scenario .............................................................................. 30
Criteria to select final options ............................................................................................ 31
Options for the future direction of health commissioning arrangements .............. 32
o Option one: No change ............................................................................................... 32
o Option two: Retain three CCGs but with a single management structure ...... 32
o Option three: Merger of the three CCGs .................................................................. 33

Page 4 of 39
Conclusions ............................................................................................................................ 33
Recommendations................................................................................................................. 34
Delivery timeline .................................................................................................................... 34
Membership engagement .................................................................................................... 35
Future financial management ............................................................................................. 35
ANNEX ONE ....................................................................................................................................... 37
NHS England tests on a decision in principle for the formation of one CCG ........ 37
I. Alignment with (or within) the local STP/ICS .......................................................... 37
II. Co-terminosity with local authorities........................................................................ 37
III. Strategic, integrated commissioning capacity and capability ........................... 37
IV. Clinical leadership ......................................................................................................... 37
V. Financial management ................................................................................................. 37
VI. Joint working................................................................................................................... 38
VII. Ability to engage with local communities ............................................................... 38
VIII. Cost savings .................................................................................................................... 38
IX. CCG Governing Body approval .................................................................................. 38
X. GP members and local Healthwatch consultation ................................................ 38
Abbreviations used in this document ........................................................................................ 39
Page 5 of 39
Introduction The NHS Long Term Plan (LTP) was released in early January 2019. Of note for the local population is the requirement for a plan to address local health inequalities, and clarity of a new service model for the NHS. This new model will comprise of Primary Care Networks (PCNs), facilitated by a new type of General Medical Services (GMS) network contract. Every Sustainability and Transformation Partnership (STP) area in the country is to be, or be part of, an Integrated Care System (ICS) by 2021. With less than two financial years to deliver this change, discussions have centred around the development of the local PCNs and the transition of the three individual clinical commissioning groups (CCGs) to a single strategic commissioner as required by the LTP. This has led to several scenarios for strategic commissioning being put forward which are explained in this document. Proposals for PCNs and updated Primary Care Strategy are the subject of other documents. This document describes current challenges and commissioning arrangements and sets out the thinking for changing the way the CCGs could work together in the future to underpin the transition into an ICS. It explains the possible alternative options; including their advantages and disadvantages. Governing Body members are asked to discuss the options set out in this paper and the recommendation of the option which will best fit and most rapidly begin to deliver the requirements of the LTP within the timescale required nationally. The approved recommendation will be put to a vote of the members in line with the required constitutional arrangements for each CCG.

Page 6 of 39
Background The NHS Long Term Plan (LTP) sets out an intention to continue to develop Integrated Care Systems across England and that, by April 2021, ICSs will cover the whole country. NHS England describes an ICS as an arrangement in which NHS organisations, in partnership with local councils and others, take collective responsibility for planning and commissioning care, managing resources, delivering NHS standards, and improving the health of the population they serve.
Figure 1: Population Health Care delivery
The LTP (p.29) describes how the commissioning environment will continue to evolve and that it is in this context that CCGs will operate in future.
‘Each ICS will need streamlined commissioning arrangements to enable a single set
of commissioning decisions at system level. This will typically involve a single CCG
for each ICS area. CCGs will become leaner, more strategic organisations that
support providers to partner with local government and other community
organisations on population health, service redesign and Long Term Plan
implementation.’
Across England there is a growing appetite for formal CCG mergers. Several, for example in Birmingham & Solihull and around Bristol, became new statutory bodies on 1 April 2018. This reduced the total number of CCGs from 211 in 2013 to 195 in 2018. The drive and ambition to respond is leading to rapid change with many other CCGs implementing new structures by

Page 7 of 39
1 April 2020. Many have already set up shared management teams and innovative structures across STP areas to help tackle the issues they face and facilitate the shift from competition to collaboration. A range of solutions are being implemented around the country from:
• formally merged CCGs, • further integration with local government, • smaller Place-based systems involving commissioners and providers in a Place and
providers taking on commissioning responsibilities. No ‘one size fits all’ approach is mandated by NHS England. The ICS needs health commissioning to change to support development of two critical capabilities:
• Better, faster service integration by better alignment of commissioning resources e.g. pathway redesign, contracting expertise, case management etc. with providers around discreet populations known as a ‘Place’;
• Streamlined, single commissioning resources for a population approach focusing on assurance, financial management, strategic change, and outcomes-based commissioning. CCGs have been told, by NHS England, to reduce their running costs by 20% as part of these new structures by 2020/21
In the future, the strategic commissioners will contract with a single organisation or partnership of organisations to manage a single budget and deliver a range of services for the local population, focusing on the population’s health and wellbeing. This means that CCGs will have a more strategic role in overseeing the local health system, focusing more on overall performance and less on individual services. Providers will take on delivery commissioning currently carried out by commissioners, such as sub-contracting for and monitoring the performance of individual services. Commissioners identified a number of scenarios for the future of health commissioning across Coventry and Warwickshire, and criteria against which to assess them. These have been tested with staff and stakeholders to inform selection and weighing of the assessment criteria, the preferred option and the case for change that is the subject of this paper. To make this transition successful, there are several important factors to consider:
• What is already in place that demonstrates working in the ICS way; • What, and where, are potential opportunities for this change to further benefit patients
and the public, improving population health through integration, and/or to address inefficiencies or financial challenges;
• Full assessment of the risk vs benefit of potential changes; and • Availability of the resource required to achieve the changes in an appropriate
timescale.
The CCGs The local CCGs were formed in April 2013 taking over responsibility for planning, paying for, and monitoring, local health services from Primary Care Trusts (PCTs). These were new organisations combining the expertise of local family doctors and NHS managers putting local doctors and nurses at the heart of deciding which health services to provide, and where and

Page 8 of 39
how they would be provided. Each CCG is led by a Governing Body. All general practices in a CCG area are members of that CCG and have clinical representatives elected to their respective governing bodies. The CCG membership retains the authority to set the strategy and direction for the organisation and to hold their governing body to account. CCGs are responsible for commissioning services including:
• Planned hospital care • Rehabilitative care • Urgent and emergency care (including out-of-hours) • Most community health services • Mental health and learning disability services.
The CCGs also have delegated authority from NHSE for commissioning general practice primary care services. The three CCGs have a long history of working together to commission hospital, community, children's and mental health services working in partnership with social care.
CCG profiles NHS Coventry & Rugby Clinical Commissioning Group Accountable officer: Andrea Green Address: Parkside House, Quinton Road, Coventry, CV1 2NJ Local authority: Coventry City Council (for Coventry)
Warwickshire County Council (for Rugby) 2019/20 budget: £729.4 million Number of staff: 256 (this includes several directly provided services)
NHS South Warwickshire Clinical Commissioning Group Accountable officer: Gillian Entwistle Address: Westgate House, Market Street, Warwick, CV34 4DE Local authority: Warwickshire County Council 2019/20 budget: £404 million Number of staff: 52 NHS Warwickshire North Clinical Commissioning Group Accountable officer: Andrea Green Address: Heron House, Nuneaton, Newdegate Street, Nuneaton, CV11 4EL Local authority: Warwickshire County Council 2019/20 budget: £282.7 million Number of staff: 53
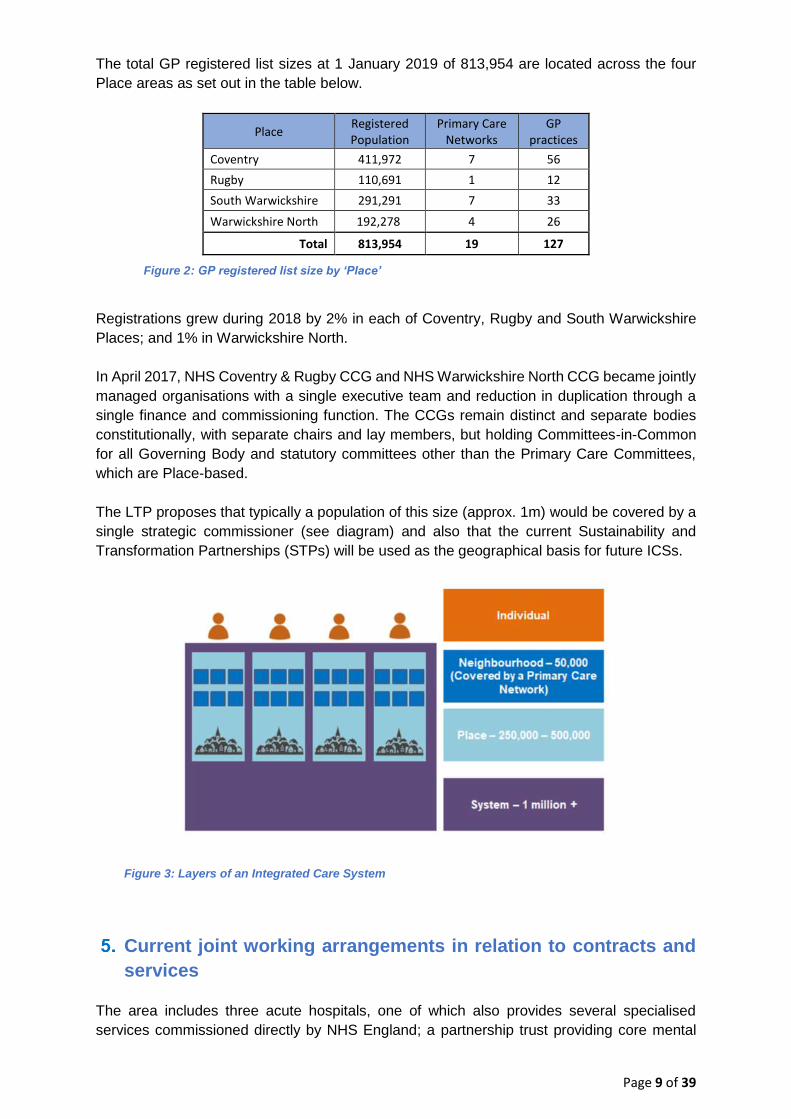
Page 9 of 39
The total GP registered list sizes at 1 January 2019 of 813,954 are located across the four Place areas as set out in the table below.
Place Registered Population
Primary Care Networks
GP practices
Coventry 411,972 7 56
Rugby 110,691 1 12
South Warwickshire 291,291 7 33
Warwickshire North 192,278 4 26
Total 813,954 19 127
Figure 2: GP registered list size by ‘Place’
Registrations grew during 2018 by 2% in each of Coventry, Rugby and South Warwickshire Places; and 1% in Warwickshire North. In April 2017, NHS Coventry & Rugby CCG and NHS Warwickshire North CCG became jointly managed organisations with a single executive team and reduction in duplication through a single finance and commissioning function. The CCGs remain distinct and separate bodies constitutionally, with separate chairs and lay members, but holding Committees-in-Common for all Governing Body and statutory committees other than the Primary Care Committees, which are Place-based. The LTP proposes that typically a population of this size (approx. 1m) would be covered by a single strategic commissioner (see diagram) and also that the current Sustainability and Transformation Partnerships (STPs) will be used as the geographical basis for future ICSs.
Current joint working arrangements in relation to contracts and services
The area includes three acute hospitals, one of which also provides several specialised services commissioned directly by NHS England; a partnership trust providing core mental
Figure 3: Layers of an Integrated Care System

Page 10 of 39
health services for the whole population and community services in Warwickshire operated by one of the acute trusts; and 127 general medical practices, serving a total of approximately 960,000 local residents.
• University Hospitals of Coventry & Warwickshire: general and tertiary (specialised) acute
• George Eliot Hospital: general acute • South Warwickshire Foundation Trust: general acute and Out of Hospital services for
Warwickshire • Coventry & Warwickshire Partnership Trust: Mental Health and Learning Disability plus
Out of Hospital services for Coventry.
Figure 4: Location map
• NHS Coventry & Rugby CCG is the co-ordinating commissioner for UHCW and CWPT
and leads negotiations on behalf of all 3 CCGs. It carries out activity analysis and raises challenges on behalf of all 3. It also hosts the IFR team and management of the commissioning policies reform group.
• NHS South Warwickshire CCG is the co-ordinating commissioner for SWFT and leads negotiations on behalf of all 3 CCGs for the trust’s acute and other Warwickshire-wide services, including the Out of Hospital contract. The CCG is also lead commissioner for Out of Hours services.
• NHS Warwickshire North CCG is the co-ordinating commissioner for the George Eliot
Hospital Trust and other Warwickshire-wide services. • The Arden-Gem Commissioning Support Unit (CSU) provides services to all three CCGs:

Page 11 of 39
Information Governance, Communications & Engagement, Business Intelligence (DSCRO) and other functions such as HR, estates and information technology. The CCGs vary in their utilisation of these services with Coventry & Rugby commissioning fewer services than the other two.
• West Midlands Ambulance Service NHS Foundation Trust; NHS 111 are contracted by
Sandwell and West Birmingham CCG as the co-ordinating commissioner for the area consortium. The staff who manage this process are funded by the three CCGs.
• The CCGs have experience of working together on joint ‘at scale’ procurements, namely:
Any Qualified Provider (AQP) and CSU procurements.
Local population
The area of Coventry and Warwickshire is home to a population with wide and diverse needs together with areas of rurality and urban conurbations. Despite the focus of population within the main towns of the county, a significant part of Warwickshire is rural in nature. In the past ten years, Coventry’s population has grown by a fifth, making it the second-fastest growing local authority outside of London. In 2016-17 its growth rate was the seventh highest. Growth is particularly high amongst 18-29 year olds. The county of Warwickshire has five Districts. The larger population bases are Nuneaton & Bedworth, Stratford-on-Avon and Warwick. Nuneaton & Bedworth is an area of significant urban deprivation, being some of the most deprived in the country. The North Warwickshire District is a more rural area. The Nuneaton & Bedworth and Stratford-on-Avon Districts have experienced the largest numerical population increases, with North Warwickshire, Warwick and Rugby Districts experiencing much lower, but approximately the same numerical increases as each other. Generally, the rate of population growth in the county of Warwickshire is below that experienced nationally (0.83%) but there is variation between the five districts.
Figure 5: ONS population and growth by District
ONS 2014-based projections suggest the population of the county of Warwickshire is
Area 2015 2016 2017 2015-2016 2016-2017 2015-17
Coventry (City) 344,300 353,200 360,100 2.6% 2.0% 4.6%
Warwickshire (total) 555,200 559,000 564,600 0.7% 1.0% 1.7%
North Warwickshire 62,800 63,200 64,100 0.6% 1.4% 2.1%
Nuneaton & Bedworth 126,600 127,700 128,700 0.9% 0.8% 1.7%
Rugby 104,500 105,300 106,400 0.8% 1.0% 1.8%
Stratford 122,400 123,300 125,200 0.7% 1.5% 2.3%
Warwick 138,900 139,500 140,300 0.4% 0.6% 1.0%
% changePopulation / Year

Page 12 of 39
projected to increase by an overall 11.1% from 2016 to 2039, lower than the equivalent national increase of 15.0%. However, this masks considerable variation when looking at broad age bands:
• 0-14 years expected growth by 4.9% between 2016 and 2039; • 16-64 years expected growth by 2.1%; • 65+ years expected to increase by almost half (49.0%); and • 90+ years is expected to increase substantially.
Figure 6: Warwickshire County Council - ONS 2014 population projections
Although age profiles for NHS Warwickshire North CCG and NHS South Warwickshire CCG are broadly similar there is a greater proportion of residents aged between 0-19 (23%) in NHS Warwickshire North CCG and a greater proportion of residents aged 70 years or over (16%) in NHS South Warwickshire CCG. The age profile for NHS Coventry and Rugby CCG is comparatively different due to the large student population residing in Coventry City; 56% of residents are aged 20-59 but the greatest proportion of residents are aged 20-29 years. The city has experienced a high rate o_international migration.
Figure 7: Population Profiles for each CCG

Page 13 of 39
Coventry is one of the fastest growing local authority areas in recent years due to more births than deaths and growing migrant and student populations (attending the two local universities). The number of full time students at the universities has doubled during the last 10-15 years. The growth in over-65s is expected to accelerate and outpace other groups within the next 10-15 years. The city is diverse with around one third of the population and just under half of school aged children from minority ethnic groups. It is a relatively deprived city, ranking 55th out of 326 local authority areas and with significant differences between wards. Almost a third of the children live in low-income families. Life expectancy is lower than the national average though similar to other areas with the same level of deprivation. There is an inequality gap between the least and most deprived areas, with a difference in life expectancy of 9.4 years for men and 8.7 years for women. The city has higher rates of premature deaths (under the age of 75) from cardiovascular disease, cancer and respiratory disease. Rugby residents are predominantly in the ‘white British’ ethnic group and account for approximately 84% of the population (2011 data), and just over 1 in 10 of the population recorded as being born outside of the UK. The variation between wards of most vs least deprived is 5.7 years lower life expectancy for men and 4.0 years life expectancy for women. South Warwickshire has an older age profile with its 65+ years population size significantly larger than that of both Coventry & Warwickshire as a whole, and nationally. Although its total future population growth is significantly lower, its 65+ years population’s growth will be
significantly higher than that of both Coventry & Warwickshire as a whole and nationally by 2035. This raises a considerable financial challenge with fewer working age people in the CCG area and increased adult health and social care responsibilities associated with an aging population. Warwickshire North is an extremely diverse locality, with some neighbourhoods experiencing high levels of deprivation, some with high numbers of BME communities, and several new housing developments alongside more traditional urban town and rural village communities. Like South Warwickshire, both Nuneaton & Bedworth and the North Warwickshire Districts have significant numbers of older people as a proportion of their communities which is significantly larger than that of both Coventry & Warwickshire as a whole and nationally. Its total future population growth is significantly lower but its more rapid growth in those over 65 years will be significantly higher than that of both Coventry & Warwickshire as a whole and nationally by 2020. This raises a considerable financial challenge with fewer working age people in the CCG area and increased adult health and social care responsibilities associated with an aging population.
Local health needs The map which follows shows the index of multiple deprivation (IMD) for the STP area. The IMD in 2015 was 19.87 against a national average of 21.67.
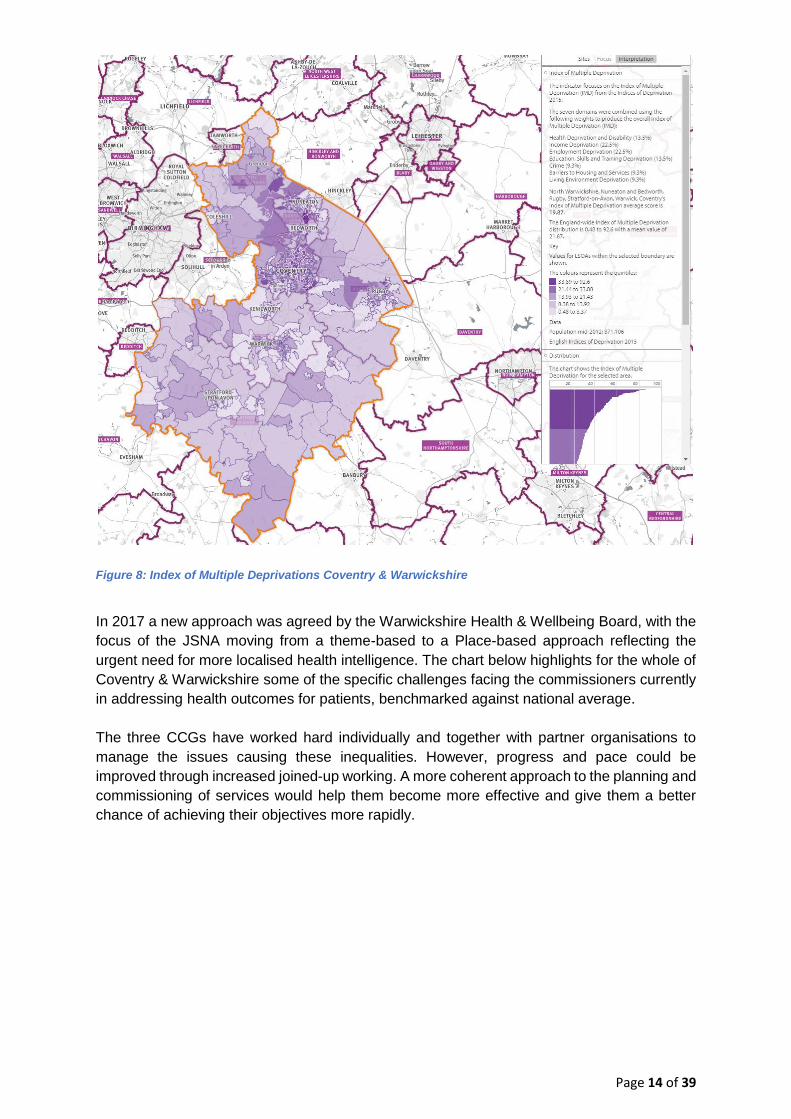
Page 14 of 39
Figure 8: Index of Multiple Deprivations Coventry & Warwickshire
In 2017 a new approach was agreed by the Warwickshire Health & Wellbeing Board, with the focus of the JSNA moving from a theme-based to a Place-based approach reflecting the urgent need for more localised health intelligence. The chart below highlights for the whole of Coventry & Warwickshire some of the specific challenges facing the commissioners currently in addressing health outcomes for patients, benchmarked against national average. The three CCGs have worked hard individually and together with partner organisations to manage the issues causing these inequalities. However, progress and pace could be improved through increased joined-up working. A more coherent approach to the planning and commissioning of services would help them become more effective and give them a better chance of achieving their objectives more rapidly.

Page 15 of 39
Figure 9: Challenges in health outcomes across all three CCGs
Sustainability and Transformation Partnership In 2016, the Government asked NHS organisations and local councils to formalise their working relationships by forming STPs to deliver NHS England’s Five Year Forward View at a
local level. The LTP now builds on the Five Year Forward View to completely transform local health and social care across the NHS in England. This can only be achieved if everyone who has a stake in health and social care - the NHS, Local Authorities, the voluntary sector and other public sector agencies - work together to

Page 16 of 39
achieve change. This change is about providing better quality care, improving health, social care and wellbeing services and making sure that services can be delivered in a sustainable way. Other than the three CCGs, the members of the local STP ‘Better Health, Better Care, Better
Value’ Board are: • University Hospitals Coventry & Warwickshire NHS Trust (UHCW) • George Eliot NHS Trust (GEH) • Coventry and Warwickshire Partnership NHS Trust (CWPT) • South Warwickshire NHS Foundation Trust (SWFT) • Coventry City Council • Warwickshire County Council • Healthwatch
The local providers have recently joined together in a Provider Alliance in order to improve patient pathways and reduce duplication in local service provision. One of the main aims of the STP is to create more effective and efficient organisations, releasing a greater proportion to be spent on frontline services, to the greater benefit of patients. The ambition is to strengthen the voice of commissioning, improve the quality of services across the whole system, meet financial targets and be a stronger commissioner to match local provider partners. A number of high level goals can be realised, at least in part, by the proposal to change. For example:
• More effective system management underpinned by comprehensive information system;
• More effective and efficient commissioning processes with less duplication; • Greater focus on outcomes based commissioning; • Better value through improved efficiency and reduced costs of commissioning function; • Simpler and more effective governance of commissioning and decision making; • Stronger service transformation approaches, decommissioning and re-commissioning; • Aligned budgets (as a minimum) and agreed risk share arrangements.
Primary Care Networks One of the key challenges general practice has faced in the past is the lack of a single, representative provider voice to engage in system level strategic planning and decision making. CCGs have improved this but still not managed to achieve a single voice of general practice. This has led to a perception of lack of representation and influence of general practice at a strategic level. Nominated GP leaders have worked closely with individual GP contractors, local LMC and GP Federations, to develop a mechanism for securing the One Voice of General Practice. This development provides one aspect of the foundation for future PCN Clinical Directors to play their crucial role in shaping and influencing the ICS and in ensuring that general practice feels fully engaged. Member practices have already formed geographically aligned Primary Care Networks

Page 17 of 39
(PCNs) typically serving natural communities of around 30,000 to 50,000, though some are significantly larger reflecting local conditions. They will now progress through the NHSE maturity matrix for PCNs and identify population health priorities, including focused action to reduce variation, and extend the range of services available in out of hospital settings. The developing Primary Care Strategy will aim to ensure that the PCNs in each of the four Places can:
• Co-ordinate out of hospital care. • Facilitate and promote peer review and sharing of good practice • Provide additional resilience • Develop arrangements to join up extended hours • Improve outcomes for patients by delivering the seven mandated national service
specifications contributing to NHS Long Term Plan • Innovate and collaborate to deliver system benefits • Utilise investment in new roles to expand general practice workforce • Support PCN Accountable Directors • Agree an approach across Coventry and Warwickshire to achieve sustainable GP one
voice within the ICS and at Place.
Delivery at Place The Coventry & Warwickshire Health and Wellbeing Place Forums led by local authorities and working with all system partners have developed a model for the future of health and care for the population in Coventry and Warwickshire. They also agreed that within this area there would be four “Places”; these are Coventry, Rugby, Warwickshire North and South
Warwickshire.
Figure 10: System of care

Page 18 of 39
This model puts people at its heart and builds the system around them. It places much more emphasis on what the system will offer to people around promoting independence, early intervention, self-help and prevention, as this is where the most beneficial and long-lasting outcomes and positive impacts on health and wellbeing can be made. The new model looks to move services closer to where people live, removing some of the barriers to access. It helps to remove unnecessary trips to hospital and the stress that goes with it i.e. parking, appointment times. Finally, it builds on existing partnership working by bringing those commissioning and providing services into even stronger alignment. In order to best support this new model, there need to be changes to how services are prioritised, planned and commissioned. There needs to be a move away from an income-driven commissioning style, where local providers compete for CCG resources, and a move to an outcomes-based commissioning approach. This means focusing less on paying for performance based on targets and processes, and more on the impact that services have on the health and wellbeing of people living in Coventry and Warwickshire. Coventry and Warwickshire CCGs have agreed a model of care (depicted in the diagram below). These contracts require community providers to organise their community service offer around GP registered patient lists of around 30k - 50k populations, and to establish integrated teams working in collaboration with general practice and social care. The action taken to implement Out of Hospital care provides a solid foundation for breaking down historical barriers between primary, community and social care services, and for providing assessment and support for ‘higher risk’ patients to remain independent later in life.
This is achieving system benefits and responding to the requirements of the NHS long term plan by establishing an Integrated Care System with general practice at its core.
Figure 11: Integrated Care system model

Page 19 of 39
Vision Throughout the engagement with key stakeholders across the STP area, we have learnt that the following objectives are consistently important to them in the CCGs pursuing a single commissioning voice:
• Overall improved health and better outcomes for patients; • A more sustainable local NHS; • Better integration of provision and commissioning at Place • Better integration with the local authorities, especially for social care and preventing
poor health outcomes; • Consistency for patients; • Ensuring that all patients can access the same high quality service, regardless of
where they live in the area; • A strong and strategic NHS commissioning voice to match that of the provider
organisations and local authority; • A larger and stronger pool of clinical expertise; and • Building on the existing partnerships the three CCGs currently have.
While finalising proposals, feedback from staff and stakeholders recognised that ‘Place’ is a
key issue. The area of Coventry and Warwickshire is made up of many different natural communities and a key consideration will be how a new organisation can respond to that, whilst still delivering high quality services and addressing and reducing health inequalities.
Integrated Care Systems Despite the legislative framework moving increasingly towards a quasi-competitive market, the policy objective in recent years has been to increase integration and a statement that ICSs will effectively end the purchaser / provider split, bringing about integrated funding and delivery for a given geographical population. The LTP is clear that local NHS organisations will increasingly focus on population health – moving to Integrated Care Systems everywhere. The most recent definition describes their function as
“… bringing together local organisations to redesign care and improve population
health, creating shared leadership and action.”
In an ICS, NHS organisations, in partnership with local councils and others, take collective responsibility for managing resources, delivering standards, and improving the health and wellbeing of the population they serve. For example, ICSs are expected to improve health and care by:
• Supporting the coordination of services, with a focus on those at risk of developing acute illness and being hospitalised;
• Providing more care in a community and home-based setting, including in partnership with council social care, and the voluntary and community sector;
• Ensuring a greater focus on population health and preventing ill health; • Allowing systems to take collective responsibility for how they best use resources to
improve health results and quality of care, including through agreed cross-system spending totals.

Page 20 of 39
As the national direction of travel moves away from competition and toward collaboration and integration, commissioners and providers will work more closely together making shared decisions. This will necessitate a different type of commissioning organisation, that aligns strategic commissioning functions to a system level, and tactical commissioning activities to a place level, integrated with provision. The LTP outlines that:
1.51. We will continue to develop ICSs, building on the progress the NHS has already
made. By April 2021 ICSs will cover the whole country, growing out of the current
network of Sustainability and Transformation Partnerships (STPs).
ICSs will have a key role in working with Local Authorities at ‘place’ level and through ICSs,
commissioners will make shared decisions with providers on how to use resources, design
services and improve population health (other than for a limited number of decisions that
commissioners will need to continue to make independently, for example in relation to
procurement and contract award).
Every ICS will need streamlined commissioning arrangements to enable a single set of
commissioning decisions at system level. This will typically involve a single CCG for each
ICS area.
CCGs will become leaner, more strategic organisations that support providers to partner
with local government and other community organisations on population health, service
redesign and Long Term Plan implementation.
Developing the model outlined above will be a continuous journey, with many achievements and small milestones along the way. There are three major stages as outlined in the figure below. These major stages are: A. Current: This first describes the current position and the progress already made within the STP system.
B. Greater alignment: The second describes the proposed next step and includes greater alignment between the CCGs (through the bringing together of functions, leadership and governance), alongside greater alignment of the appropriate commissioning activities to integrate with providers at each Place.
C. Integrated care at system and Place level: the third describes a foreseeable end-state D. Legislative changes: to underpin local requirements but currently unclear. Proposals for possible changes to legislation were published on 28th February 2019. The earliest time for legislative change is 2022 and CCGs have been encouraged to move forward with implementing the LTP and not wait for legislation.

Page 21 of 39
Figure 12: Major stages in moving to strategic commissioning
Future arrangements
There is a need to establish appropriate governance arrangements with transparency over where decisions are made when the change in structure is being implemented ahead of any legislation change. Shared management structures have demonstrated many advantages to date, including greater capacity and resilience, economies of scale and an enhanced skills base. The move to joint working and shared responsibility helped those CCGs who were currently struggling to tackle common issues with NHS providers or social services. The benefits of aligning the boundaries of NHS commissioning areas with existing administrative boundaries at other levels are widely acknowledged. The proposed boundary is aligned and coterminous with both the existing Local Authorities and CCGs. There is no requirement to adjust boundaries or change the relationship of any GP practices to the developing PCNs. The four Place health delivery systems are coterminous with City, District and Borough Council boundaries and the four groups of PCNs. Local Providers focus on delivery of services to their Place-based populations and, in the case of UHCW, provide some tertiary services to the whole population.
Expected benefits of greater alignment Greater alignment of the health and care organisations will allow creation of a health and social care system that works better for patients and their families and which makes best use of scarce resources. Through minimising the structural barriers that exist between organisations

Page 22 of 39
there is removal of competing priorities of individual organisations and development of aligned objective to improving the quality of health services across the whole of the ICS. The ultimate goal of this greater alignment is to improve the health of the population, provide better quality care for patients, improve ways of working and return the system to financial balance, by a more effective and efficient use of assets and resources. This will be achieved through transforming clinical services across both primary and secondary care, and also improving organisational alignment and system performance across other areas, including shared functions and shared governance. There is no technical reason as to why the benefits outlined above cannot be achieved by three separate organisations. However, the practicalities of this arrangement, and learnings from other systems, suggests that this would be extremely difficult to achieve. Without a single leadership team, it will be challenging to achieve the transformative change required to improve the quality of care provided, whilst ensuring financial stability to the system. This is supported by a wealth of learnings from other systems, where organisations (both commissioners and providers) have attempted to collaborate but where separate leadership has created material, and in some cases insurmountable, barriers to alignment. Alignment will have, a positive impact on financial stability, through:
• Reduction in duplication – the appointment of joint/single roles will realise savings • More efficient use of resources across the system • Improved relationships across the total Coventry and Warwickshire footprint • Aligning the financial objectives of all organisations removes incentives to act in the
interest of individual organisations and encourages activity which benefits the entire system.
Current progress A temporary, dedicated transition team has been convened to manage the transition to a future state, develop and implement a detailed plan e.g. communications, risk and issues and management. We are confident that the proposal follows a natural progression, building on joint working arrangements and collaborations such as:
• Lead commissioner contract arrangement/joint clinical commissioner groups • Better Care Fund arrangements through the Better Health, Better Care, Better Value
Partnership • Hosted team arrangements • System Resilience Groups/A&E Delivery Boards
Furthermore, there are already in place some of the following shared functions across two or more of the existing CCGs:
• Single senior management team in two CCGs • Committees in common e.g. all Governing Body committees included the Governing
Bodies of two of the CCGs, but with the exception of the Primary Care Committee • Joint Strategic Commissioning Committee • Individual Funding Requests

Page 23 of 39
• Clinical Policy Group. The strategic delivery plan across the three CCGs is set out in the table below:
Programme Deliverables for 2019/20 By St
rate
gic
Com
mis
sion
ing
Strategic Framework for the C&W HWB partnership 30 September 2019
Strategic Commissioner Strategy & yr1 commissioning intentions (including financial strategy) 30 September 2019
Agreed governance and reporting for strategic commissioning team 30 June 2019
Strategic Commissioning Process for MCYP; Planned Care; and MH Throughout 2019/20
Develop the strategic commissioning clinical leadership function/s 30 June 2019
Establish an assurance framework that can be used to inform readiness of Place for ICP contract 30 September 2019
Undertake a baseline assessment of readiness and work with the Places (both provider and delivery commissioning) on a development plan that enables the progression to an ICP contract
31 November 2019
Develop the system 5-year plan Autumn 2019
Plac
e B
ased
Tr
ansf
orm
atio
n Pr
ogra
mm
e
Develop Place based commissioning transformation resources focused on priority areas – MH; Frailty; Planned Care; Maternity and Paediatrics; CIP/QIPP/Value Boards
31 May 2019
Support the delivery of Place Based 5 year plans 30 June 2019
Develop Commissioning at Place transformation and continuous improvement methodology with Provider Alliance 30 September 2019
On behalf of the 4 Places deliver system wide enabling programmes Throughout 2019/20
Plac
e B
ased
G
over
nanc
e
Develop, for each Place, an agreed Governance mechanism governance for reporting into existing CCGs for 2019/20 31 May 2019
Ensure governance enables effective participation in the ICS development and enables CCGs to deliver statutory responsibilities
31 May 2019
Design governance for place-based commissioning 31 December 2019
Popu
latio
n H
ealth
M
anag
emen
t
System wide clinical leadership development – stage 1 31 March 2020
Baseline assessment of analytical capacity and capacity for PHM 31 May 2019
Develop the C&W methodology/approach in line with regional approach and obtain agreement with BHBCBV Board 30 June 2019
Develop PHM capacity and capability resources in line with the regional approach 31 March 2020
Primary Care Transformation Programme
Mechanisms in place for NHS organisations in each place to work with PCNs 30 June 2019
Figure 13: Joint development plan
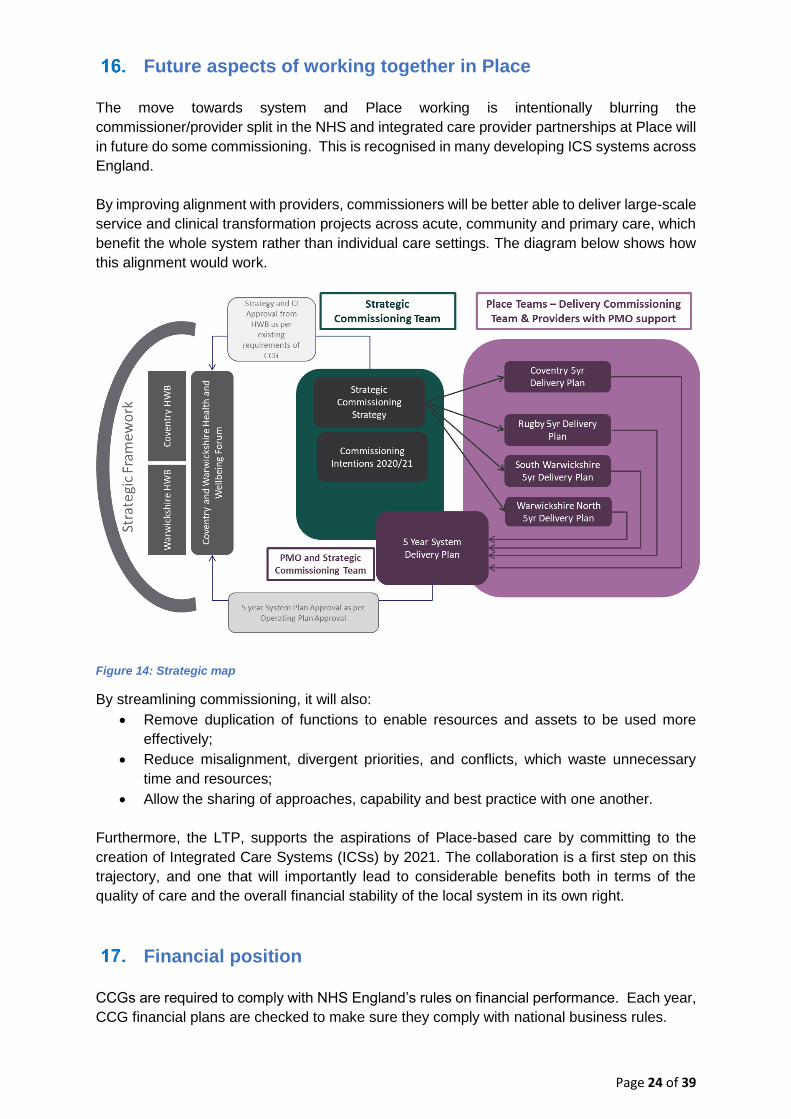
Page 24 of 39
Future aspects of working together in Place The move towards system and Place working is intentionally blurring the commissioner/provider split in the NHS and integrated care provider partnerships at Place will in future do some commissioning. This is recognised in many developing ICS systems across England. By improving alignment with providers, commissioners will be better able to deliver large-scale service and clinical transformation projects across acute, community and primary care, which benefit the whole system rather than individual care settings. The diagram below shows how this alignment would work.
Figure 14: Strategic map
By streamlining commissioning, it will also: • Remove duplication of functions to enable resources and assets to be used more
effectively; • Reduce misalignment, divergent priorities, and conflicts, which waste unnecessary
time and resources; • Allow the sharing of approaches, capability and best practice with one another.
Furthermore, the LTP, supports the aspirations of Place-based care by committing to the creation of Integrated Care Systems (ICSs) by 2021. The collaboration is a first step on this trajectory, and one that will importantly lead to considerable benefits both in terms of the quality of care and the overall financial stability of the local system in its own right.
Financial position CCGs are required to comply with NHS England’s rules on financial performance. Each year, CCG financial plans are checked to make sure they comply with national business rules.
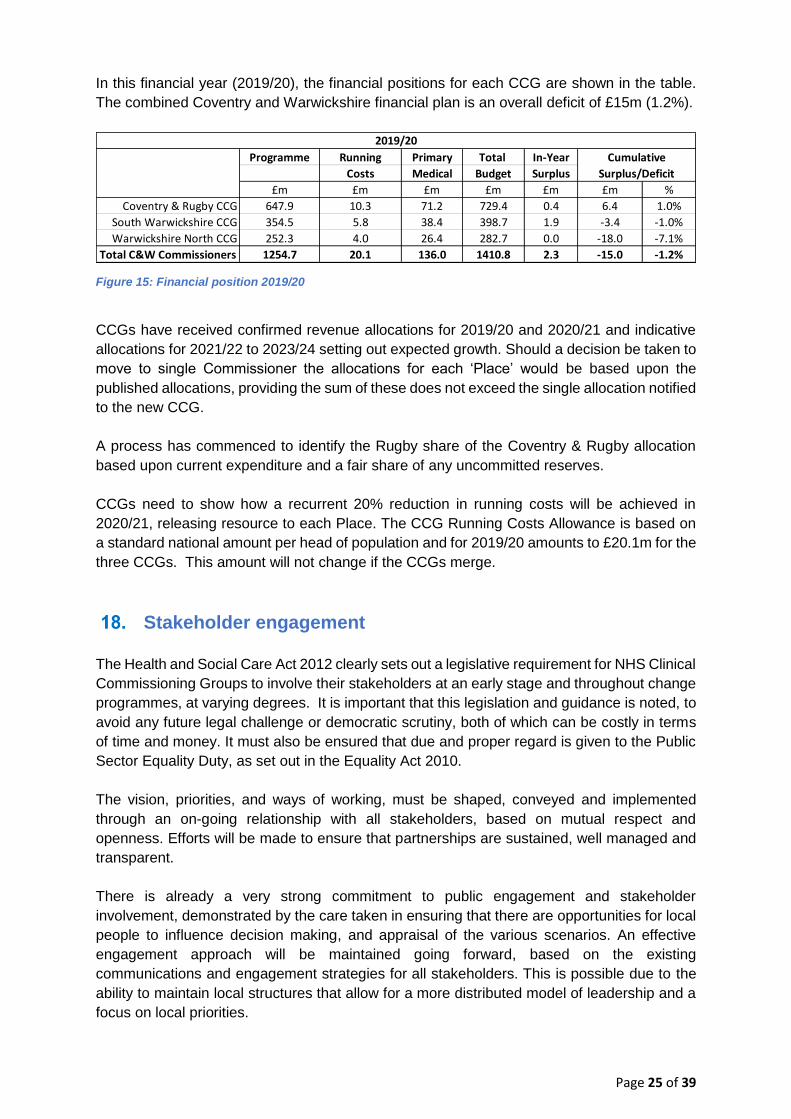
Page 25 of 39
In this financial year (2019/20), the financial positions for each CCG are shown in the table. The combined Coventry and Warwickshire financial plan is an overall deficit of £15m (1.2%).
Figure 15: Financial position 2019/20
CCGs have received confirmed revenue allocations for 2019/20 and 2020/21 and indicative allocations for 2021/22 to 2023/24 setting out expected growth. Should a decision be taken to move to single Commissioner the allocations for each ‘Place’ would be based upon the published allocations, providing the sum of these does not exceed the single allocation notified to the new CCG. A process has commenced to identify the Rugby share of the Coventry & Rugby allocation based upon current expenditure and a fair share of any uncommitted reserves. CCGs need to show how a recurrent 20% reduction in running costs will be achieved in 2020/21, releasing resource to each Place. The CCG Running Costs Allowance is based on a standard national amount per head of population and for 2019/20 amounts to £20.1m for the three CCGs. This amount will not change if the CCGs merge.
Stakeholder engagement The Health and Social Care Act 2012 clearly sets out a legislative requirement for NHS Clinical Commissioning Groups to involve their stakeholders at an early stage and throughout change programmes, at varying degrees. It is important that this legislation and guidance is noted, to avoid any future legal challenge or democratic scrutiny, both of which can be costly in terms of time and money. It must also be ensured that due and proper regard is given to the Public Sector Equality Duty, as set out in the Equality Act 2010. The vision, priorities, and ways of working, must be shaped, conveyed and implemented through an on-going relationship with all stakeholders, based on mutual respect and openness. Efforts will be made to ensure that partnerships are sustained, well managed and transparent. There is already a very strong commitment to public engagement and stakeholder involvement, demonstrated by the care taken in ensuring that there are opportunities for local people to influence decision making, and appraisal of the various scenarios. An effective engagement approach will be maintained going forward, based on the existing communications and engagement strategies for all stakeholders. This is possible due to the ability to maintain local structures that allow for a more distributed model of leadership and a focus on local priorities.
Programme Running Primary Total In-Year
Costs Medical Budget Surplus
£m £m £m £m £m £m %
Coventry & Rugby CCG 647.9 10.3 71.2 729.4 0.4 6.4 1.0%
South Warwickshire CCG 354.5 5.8 38.4 398.7 1.9 -3.4 -1.0%
Warwickshire North CCG 252.3 4.0 26.4 282.7 0.0 -18.0 -7.1%
Total C&W Commissioners 1254.7 20.1 136.0 1410.8 2.3 -15.0 -1.2%
Cumulative
Surplus/Deficit
2019/20

Page 26 of 39
Those charged with the authority to set the direction for clinical commissioning are local GPs as is articulated in the CCG Constitutions. GPs are connected to the NHS and see every aspect of it; they are also connected to their local populations. Their input into the process of how to get more from local NHS clinical commissioning is critical to achieving the ambitions set out. The members and governing bodies of all three CCGs have been informed and involved from the outset and contributed to the planning at each stage. The Governing Bodies confirmed this as the correct strategic direction of travel, but like other stakeholders, there are issues that have been raised (see below). These views and insight will be more important than ever during transition towards a new model and need to be taken into account. Stakeholders have so far raised issues that need to be discussed during the programme of involvement and used as the basis for further conversations that will influence and inform future decisions. Issues raised for discussion included:
• Need to retain patient-focused pathways of care. • The role of a single commissioner in an ICS and links to the new PCNs and Place. • Delivery of a single Commissioning Voice. • Clarity on the financial impact and management across Coventry and Warwickshire as
a whole and at Place. • How NHS England deadlines for merger applications fit with the need for local
engagement and democratic processes. • Maintaining good relationships at all levels with hospitals and other health and care
providers. • Clarity on the combined vision and priorities for the new organisation, not just its size
and shape. • The need for consistent commissioning strategies across the Coventry & Warwickshire
footprint delivering localised implementation at Place.
Stakeholder events Some scenarios were developed to determine the best way of commissioning health services going forward, making the most of the CCGs resources and working more closely with providers and the community and voluntary sector. Stakeholder events were held with staff, representatives of the GP membership, the CCG governing bodies and key stakeholders, including representatives from patient groups and the community and voluntary sector, as well as colleagues working in health and social care. In the period since December 2018 there have been a number of briefings and engagement events with staff, Members and Governing Bodies. Other events have also been held with key stakeholders between March and May 2019. The purpose of the engagement activity was to bring together a wide range of key stakeholders from across Coventry and Warwickshire, including colleagues working in health and social care, voluntary and community organisations, councillors, carers and patients and their representatives with the aim of:
• Providing clarity that this piece of engagement was specifically around the future of health commissioning as it pertains to meeting the needs of a future integrated care

Page 27 of 39
system for Coventry and Warwickshire. • Giving attendees some background information and putting things in context to help
them understand why we are considering changing health commissioning. • Capturing their initial thoughts and reactions to this information to input into the case
for change document, due to be presented to the CCG governing bodies in late May 2019.
These events were not:
• A platform to persuade people of our thinking; it was a listening exercise as part of the engagement process
• Aimed at the wider public; rather, they were targeted and focused events with CCG staff and membership, and representatives from various key stakeholder groups from across Coventry and Warwickshire
• A platform to make decisions but a chance for people to further inform thinking.
A wide range of stakeholders were invited to the events. To ensure that the stakeholders were fully representative, we took into account the demographics of our population, previous engagement equality findings and recommendations in how to engage seldom heard and protected characteristic groups. To ensure there was representation from across Coventry and Warwickshire stakeholders were identified and invited to nominate representatives to attend the events. These external stakeholders included:
• Patients and patient representatives – individuals who had contributed to previous engagement activities, including underrepresented groups of people identified as part of other wider communications and engagement strategies
• Voluntary and community sector representatives including those representing underrepresented groups
• MPs and local Councillors • Both local Healthwatch organisations
Those who were unable to attend any of the events were offered the chance to contact the team to share their views or request a link to an online survey, although to date no such requests have been received.
Governing bodies The three CCGs’ governing bodies were given an opportunity to feed into the case for change during a governing body development session. Following a presentation to provide background and context, a series of questions was asked. Responses and feedback were captured via an online tool (mentimeter.com).
Members The same information was presented to each CCG’s membership and feedback was captured
using an online tool (www.mentimeter.com) where possible. For NHS Coventry and Rugby CCG, CCG representatives attended a Protected Learning Time (PLT) event for the Coventry membership, and a Delivery Group meeting for Rugby. NHS Warwickshire North CCG holds monthly membership meetings and the April meeting was used to deliver a brief presentation and then capture feedback using the same online tool.

Page 28 of 39
NHS South Warwickshire CCG conducted a meeting with their membership at a Members’ Council engagement session in March 2019. One of the key themes from this meeting was that a “larger, stronger GP voice” needed to be added to the assessment criteria, which was agreed.
Local health and wellbeing leads Letters were sent to the Chief Executives of all the local providers, as well as leaders for local GP federations/alliances and Local Medical Committee Chairs, Deputy Chairs and Secretaries. The letters outlined the approach and requested feedback, in writing, to the proposals and timelines, as well as any other feedback or concerns they had.
Staff NHS Coventry and Rugby CCG and NHS Warwickshire North CCG staff attended an all-staff team brief, led by the Accountable Officer, on 30th April 2019. An update was given on progress since the last briefing in December 2018, then attendees were asked to provide their feedback and views using the mentimeter tool. Likewise, NHS South Warwickshire CCG held an equivalent staff engagement session on 7th May 2019.
Patients NHS South Warwickshire CCG spoke with members of its 3PG group - comprised of patient representatives, GPs and the CCG Lay Member for Patient and Public involvement. Feedback from this event suggested that the presentation and subject matter were very complex and needed to be simplified for wider audiences. This was adjusted ahead of the stakeholder events. It was also felt that “patient voice” needed to be added to the assessment criteria alongside “larger, strong GP voice” and this was actioned.
Criteria for reviewing scenarios Various scenarios were considered and through the process of the stakeholder engagement these were refined. When asked, out of 174 people, only three (all staff members) said they were not happy/satisfied with the scenarios identified. At the Warwickshire North stakeholder event, only one attendee felt they had sufficient information to respond to this question. In particular, the majority wanted more information on how each scenario would be costed. They also preferred “Don’t have enough information” to “don’t know”, from a wording standpoint. The initial criteria used by SWCCG with members were subsequently combined with the criteria used elsewhere, with some additions. These were:
• Progress already made towards a single commissioning voice; • Realisation of possible efficiencies; • Potential to address the financial challenge; and • Level of disruption and speed of change.
After adaptation the following criteria were finally used to evaluate various scenarios:
• Improved clinical quality • More effective use of resources • Better access to services

Page 29 of 39
• Development of services • Ease of delivery • Improved strategic fit • Meeting training, teaching, research needs • Improved environmental quality • Meeting national/regional policy
Broadly speaking, most of those engaged agreed that all the appraisal criteria were important. Improved clinical quality, more effective use of resources and better access to services were agreed as the highest priorities across all engagement sessions, with the remaining options changing depending on the audience. Generally, meeting national and regional policy was seen as the least important criterion for the majority of stakeholders, with improved environmental quality often in second-to-last place.
Using best practice criteria for assessing more general scenarios, members were asked to rank which of these criteria should be prioritised, and whether these should be sensitised for this subject matter, or if anything was missed by using this set of criteria.
Stakeholder responses The key messages which emerged from the engagement programme were as follows (in no particular order of priority): Support for change The vast majority of those engaged were in agreement that there was a need for change to both an integrated care system (ICS), and also that health commissioning needed to change to help enable development of the ICS. However, there was some feeling that much of this had been discussed and promised before and not taken hold in various forms including previous iterations of CCGs (e.g. Primary Care Trusts, Strategic Health Authority). So there was some scepticism that it would work this time around, particularly when it came to integrated the health and social care agenda, finances and accountability. A full merger was the most preferred scenario At each session most agreed that a full merger made the most sense and would be the best scenario for achieving the objectives set out in the future model of health and wellbeing for Coventry and Warwickshire, though it was widely recognised it would not be an easy, quick or cheap process. Local provider’s feedback to date has also been broadly supportive of a full merger. Joint management team across three CCGs first before moving to full merger At each session some questions were raised over whether, due to the tight timeframes, there was a possibility of doing a “best of both worlds” approach, which would involve first moving
to a joint management team to build the foundation of the new commissioning structure before moving to a full merger.
Page 30 of 39
Building robust “Places” – and not losing local identity – is critical to success All agreed that success or failure of the health and wellbeing system was dependent on building and supporting strong “Places”. Loss of local voice and identity were highlighted as being of large concern when thinking about moving to a strategic commissioning structure. Involving the local population and their representatives is seen as another critical measure of success Local people, and those that represent them (whether that be in the community and voluntary sector or elected officials), were eager to be involved as much as possible in the future development of systems to improve the health and wellbeing of the local population. Transparency, openness and the opportunity to feed into and influence planning and delivery were considered of vital importance. Supporting staff is vitally important Any change to the status quo will introduce uncertainty, worry and potential changes for staff. All stakeholders agreed the importance of supporting them during any change couldn’t be
overstated. Understandably, amongst staff groups job security was a chief concern. “Do nothing” is not a viable scenario Only one person felt that “do nothing” was a viable scenario. All others considered it was not;
either due to pressures from NHS England or for achieving the aspirations of the future model of health and wellbeing for the area. A full report will be available on the website of each of the three CCGs.

Page 31 of 39
Criteria to select final options
OPTIONS
1: Do nothing 2: Single Management 3: Full merger
Criterion Three statutory bodies
Three statutory bodies & joint commissioning One statutory body
Improved clinical quality No change
All the clinical expertise in the STP area would be
available to the whole STP area
All the clinical expertise in the STP area would be
available to the whole STP area
More effective use of resources No advantage
More stable arrangement than no change
Stable arrangement.
Single legal entity. Single executive team -
loss of some senior posts Single executive team –
loss of some senior posts
Better access to services No advantage No advantage
Single voice for strategic commissioning of local
services
Development of services No advantage No advantage
Single voice for strategic commissioning of local
services
Ease of delivery No change No advantage No advantage
Timeframe 3-6 months Timeframe 9-22 months
Improved strategic fit No advantage Some economies of scale
Maximises potential for economies of scale
Eliminates commissioning duplication and inconsistent
approaches Allows single financial and
service strategy Strong basis for negotiation
and approach to STP Meeting training,
teaching, research needs
No advantage No advantage No advantage
Improved environmental
quality No advantage No advantage No advantage
Meeting national / regional policy
Does not achieve
requirement
Joint alignment to STP / ICS
Full alignment to STP / ICS for providers / provider
alliance and local authorities to engage with
Retains three commissioning bodies and
three sets of statutory requirements to be
delivered
Move from three sets of statutory requirements to
one
No advantage – influence across STP not
maximised

Page 32 of 39
Options for the future direction of health commissioning arrangements
As a result of the discussions and consideration of the criteria the following options are set out below for Governing Body consideration: o Option one: No change
Three separately accountable CCGs and current, separate management arrangements. Until recently, each of the three CCGs had separate management teams, planning processes, priorities, budgets, and reporting responsibilities. Within the last two years NHS Warwickshire North and NHS Coventry & Rugby CCGs have shared an executive team and aligned work programmes focussed on the relevant lead acute provider for the CCG. This has enabled some streamlining of staff time involved. While there are lead commissioning arrangements in place for contracting purposes, providers in the STP area work with the views of three CCGs, as does Warwickshire County Council. Coventry City Council has the benefit of working solely with Coventry & Rugby CCG, though the CCG works with both Local Authorities. Management and governance arrangements are duplicated. The CCGs have two accountable officers, two chief finance officers, two executive teams and hold two sets of committee meetings in public. But they have three sets of offices, complete all their legal responsibilities separately three times (such as accounts), commissioning plans, production of three annual reports and maintenance of three websites. Implementing this option would maintain the status quo and would not fulfil the vision of becoming a strategic commissioner nor the development of an ICS. It does not offer any benefit in terms of economies of scale nor deliver the required reduction in costs. It does not improve recruitment and retention and creates the potential to lose clinical leadership and key staff. There would remain three commissioning voices, with potentially divergent associated commissioning priorities. This would appear to duplicate decision making at Place and potentially hinder progress. This option has therefore been discounted. o Option two: Retain three CCGs but with a single management structure
A single joint management team established following the immediate appointment of a single
Accountable Officer for the three CCGs with retention of the three existing statutory bodies
In this arrangement, the current CCGs would remain separate organisations that share some staff and structures to help them work more efficiently. This model would deliver marginal benefit in cost reduction in areas such as joint committees or holding committees-in-common to undertake aligned priorities and responsibilities. Each CCG would retain its own constitution, governing body and membership arrangements for all statutory functions. The CCGs would work toward this arrangement by appointing a single Accountable Officer and Chief Financial Officer in the first instance. The timescale for this has already been approved
Page 33 of 39
by the Governing Bodies and recruitment will commence shortly. Implementing this option would require the CCGs to co-design and implement new non-statutory governance arrangements. Comparing this option to the current arrangements in Option 1, there are no material advantages. Implementing this option would incur little disruption for staff and have no significant impact on the current level of duplication. Meetings-in-common would need to be held in a rotation of the three sets of CCG offices which might disadvantage some stakeholder and public attendance.
o Option three: Merger of the three CCGs A single commissioning voice, management team, constitution, and governance arrangements following merger; with a single, joint management team established following the immediate appointment of a single Accountable Officer for the three CCGs up to the date of merger This option establishes an entirely new CCG, with a single management team, governing body and one set of statutory duties to be delivered, coterminous with the whole STP area and including both Local Authorities. It would provide the foundation of the future ICS and do so within the timeframe required nationally. The arrangement would be stable, permanent and align to existing local authority health scrutiny and Health and Wellbeing Board arrangements. This alternative would allow more effective partnership work within the STP, including with NHS England, on areas outside of the CCG’s scope e.g. specialised commissioning. Implementing this option would require the early recruitment of a Accountable Officer and a Chief Financial Officer to appoint a single executive team and to design and implement new statutory governance arrangements leading on the merger application to NHSE England and delivery of the merger programme arrangements. Compared to current arrangements, this arrangement would be significantly more sustainable and substantially reduce duplication because there would be one statutory body, rather than three; a single legal entity for providers, third sector and local authorities to engage with; and a single set of reporting and policy approaches to deliver consistency for the people of Coventry and Warwickshire. These arrangements would make all the clinical expertise available in the area available to the whole of the area, with the single CCG working together with the recently established Provider Alliance which itself covers those within the STP footprint.
Conclusions
1. It is considered that, due to the lack of any demonstrable benefits, Option 1 is discounted entirely.
2. Option 2 is a viable option but fails to deliver a single commissioning voice and retains
three statutory organisations and overheads in management and requirements.
3. Option 3 creates a single management structure whilst moving the organisations to full
Page 34 of 39
merger. It gives the best chance of achieving the national target of becoming an ICS by 2021 and delivers the requirements of full coterminosity with the STP area and boundary alignment with the local authorities. It also provides the greatest potential for achieving the financial reduction in management costs required by the NHS Long Term Plan and the ability to develop a strategic commissioning function to support a single co-ordinated approach to the commissioning and delivery of health care at Place.
Recommendations
1. That the Governing Body support Option 3 2. That CCG member practices are asked to choose (by voting) either Option 2 or Option
3
Delivery timeline Following the Governing Bodies’ decision on the recommended option, planning to deliver the this will continue in the meantime. The CCGs will proceed to engage with members and stakeholders during the next few months to ensure that the planning is robust. If it becomes clear during the engagement that the preferred option is not sustainable and/or does not deliver the required benefits a further report will be brought back to the Governing Bodies with a revised recommendation and next steps. If Option 3 (Full Merger) is supported there will be a requirement to formally apply to NHS England for formal merger to take place. Annex 1 sets out the NHSE / NHSI criteria for assessing CCG mergers. Whilst there are many other documents that will need to be developed or refined to support the case for change for merger, these criteria will need to be assured within that case. Formal application would be required in September for transition on 1 April following. In each of the change options (Options 2 and 3), the three Governing Bodies will have a single Accountable Officer and will work towards a single management team. This approach offers clear executive leadership and economies of scale. There is every intention of retaining strong clinical leadership under changed arrangements and envisage retaining a robust executive function incorporating the Accountable Officer role. However, adjustments will be needed such as determining the required skills and capacity in accordance with NHSE guidance. This would include the establishment of the correct balance of clinical, lay member and executive roles. It is recognised that clinical leadership has two distant parts; those involved in strategy, governance and accountability (e.g. Governing Body members), and those driving delivery, patient centred care pathways, implementing new evidence, building relationships with clinicians in provider organisations. The approach will be to get the balance between these two roles and ensure those clinicians with the right skills are in the right roles. In developing the new operating structure, there would need to be decisions on how to establish the function of Clinical Chair and the wider clinical engagement and leadership structures. Since these are well-regarded/trusted mechanisms in each of the existing CCGs
Page 35 of 39
it has significance in terms of continuity. The new leadership will need to finalise the proposals, but the intention would be to agree the core principles with the respective memberships to underpin new arrangements in a merged organisation. These plans will be firmed up and made available for scrutiny after the final decision on the option is reached. Steps will also be taken to mitigate any risks associated with changes for example using necessary shadow committees/arrangements where committee structures are to be altered.
Membership engagement
As set out in the CCGs’ constitutions, the memberships of each organisation are required to agree changes to their organisation. The following membership engagement principles will be followed:
• Engagement will continue to build on the clinical led model; where local GPs are at the heart of the conversation, being visible and their presence sustained
• Engagement will have a shared focus for the future, where the goal is to be a strong strategic commissioner
• The arrangements by which GPs are engaged will be flexible and will be able to adapt to small and larger networks
• Engagement with GPs will be supported by a common message, with common materials so that all GPs throughout Coventry and Warwickshire receive consistent, timely and relevant information
• There will be a commitment to using and building upon existing networks for engagement, so that there is minimum disruption to business as usual
• An evidence-based approach will be used • The overall approach to engagement should be informed by the Local Medical
Committees.
Future financial management It is too early to draw together the detail of this plan but there are several components of the financial control arrangements which will be essential in delivering proper stewardship and accountability for public funds in a new structure or new CCG. These are set out below in such a way which incorporates a transition phase if required:
• Audit Committee: If Option 2 is adopted, jointly agreed terms of reference and holding meetings in common. Robust audit arrangements would be expected to be adopted by a new CCG in order to ensure clear oversight of financial governance.
• Chief Finance Officer and Finance Team: financial planning, management and reporting is provided in-house with AGEM Commissioning Support Unit providing financial systems and transactions support. There is a need to ensure continuity with regard to these arrangements. The appointment of a single Chief Financial Officer will be undertaken prior to the remaining leadership team. The structure and functions of the finance team for the new arrangements will be determined following that appointment.
• Financial policies: adoption of a common set of prime financial policies. These policies would become the prime financial policies for a new CCG. Harmonisation of

Page 36 of 39
the scheme of delegated financial limits used by the individual CCGs would be adopted by a new CCG.
• Financial planning: the three CCGs developed joint working arrangements for the completion of the most recent contracting process. This included common assumptions for financial planning purposes and lead commissioner arrangements for contract negotiation processes.
• Financial system/budgetary controls: the CCGs operate a common financial system (ISFE) and use the business intelligence reporting functionality from ISFE to support budgetary control and financial management. Further work will be undertaken to continue to harmonise detailed working practices to ensure financial control operates effectively under new arrangements.
• Internal audit: Coventry and Warwickshire Audit Services (CWAS) currently provides internal audit and counter fraud services to all three CCGs. CWAS would deliver a jointly agreed single audit plan as approved during any transition phase by each Audit Committee. This approach is expected to facilitate a smooth transition of internal audit arrangements into the first year of a new CCG which may then choose to re-procure internal audit and counter fraud services in future.
• External audit: external audit arrangements would need to be confirmed or procured depending on the option selected.
In the longer term, the establishment of new models of care and structures will see deployment of resources in new settings. In addition, the future commissioning function will continue to evolve, with a wider range of potential partners including local authority and other statutory agencies, and there is an expectation that greater efficiencies will be available over time as these new structures develop.
Page 37 of 39
ANNEX ONE
NHS England tests on a decision in principle for the formation of one CCG1 The application procedure for CCGs proposing to merge has been revised in light of the NHS Long Term Plan, and the learning from previous mergers. The revised procedure sets out the legal requirements, and how CCGs should work together to prepare merger applications. The revised procedure builds in benefits realisation from the outset, so that the proposed benefits of joint working and merger (streamlined commissioning across systems, efficiencies, financial savings, etc) are clearly articulated and measured. As CCGs merge and cover larger areas, they will need to show how they will retain local focus and involve members and communities. In accordance with the legal requirements and the NHS Long Term Plan, NHS England will consider the following criteria in deciding whether to approve a proposed merger:
I. Alignment with (or within) the local STP/ICS To provide the most logical footprint for local implementation of the NHS Long term Plan, and
to provide strategic, integrated commissioning to support population health.
II. Co-terminosity with local authorities
There is a presumption in favour of CCGs being coterminous with one or more upper-tier or
unitary local authorities. They should also show how they have/will put in place suitable
arrangements with local authorities to support integration at ‘place’ level (population of
between 250,000 and 500,000).
III. Strategic, integrated commissioning capacity and capability In line with the legal requirements, the existing CCGs must demonstrate that they have/will
develop the leadership, capacity and capability for strategic, integrated commissioning for their
population. This will include population health management, new financial and contractual
approaches that encourage integration, and developing place-based partnerships. In
accordance with the legal requirements, the application must demonstrate how any
commissioning support services to be procured will be of an appropriate nature and quality.
IV. Clinical leadership
In line with the legal requirements, the existing CCGs must demonstrate how the proposed
new CCG will be a clinically led organisation, and how members of the new CCG will
participate in its decision-making.
V. Financial management
In accordance with the legal requirements, the existing CCGs must show how the new CCG
will have financial arrangements and controls for proper stewardship and accountability for
public funds.
1 Procedures for clinical commissioning groups to apply for constitution change, merger or dissolution NHS England & NHS Improvement April 2019

Page 38 of 39
VI. Joint working
Ideally, a merger should build on collaborative working between the existing CCGs and
represent a logical next step from current arrangements. The merger application should show
progress on joint working to date and must show how the existing CCGs intend to resource
and manage the merger process itself.
VII. Ability to engage with local communities
Assurance is required that the move to a larger geographical footprint will not be at the
expense of the proposed new CCG’s ability to engage with - and consider the needs of - local
communities.
VIII. Cost savings Where possible, the existing CCGs should show how collaboration and joint working to date
has contributed to cost savings; they must also show any further cost savings projected to
result from the merger, and when, and how cash released will be re-invested.
IX. CCG Governing Body approval
The merger application must show evidence of approval for the merger by the Governing Body
of each of the existing CCG governing bodies.
X. GP members and local Healthwatch consultation
Evidence is required that each of the existing CCGs have engaged with, and seriously
considered the views of, their GP member practices, and local Healthwatch, in relation to the
merger. The merger application must record the level of support and the prevailing views of
each existing CCG’s member practices and local Healthwatch, and the existing CCGs’
observations on those views.

Page 39 of 39
Abbreviations used in this document BME Black and minority ethnic CCG Clinical Commissioning Group CRCCG NHS Coventry & Rugby CCG GMS General Medical Services (contract) ICS Integrated Care System IMD Index of Multiple Deprivation JSNA Joint Strategic Needs Assessment LTP NHS Long Term Plan (10 year Plan) PCN Primary Care Network (of GPs) STP Sustainability & Transformation Partnership SWCCG NHS South Warwickshire CCG WNCCG NHS Warwickshire North CCG

NHS South Warwickshire Clinical Commissioning Group Enc 09
Safeguarding Children & Adults at Risk of Abuse Policy Governing Body – 22 May 2019 Page 1 of 2
Report To: Governing Body For decision X
Report Title: Safeguarding Children & Adults at Risk of Abuse Policy
For discussion
Report From: Alison Walshe Chief Nurse For information X
Date: 22 May 2019 Confidential
Purpose of the Report:
To seek approval of the adoption of the Safeguarding Children & Adults at Risk of Abuse Policy.
Key Points:
• This policy sets out the Clinical Commissioning Group’s arrangements for safeguarding and promoting the welfare of children and adults at risk. It should be read in conjunction with local multi-agency procedures, which outline, in detail, actions to be undertaken where safeguarding concerns arise.
• This policy covers the CCG’s safeguarding role and responsibilities as a commissioner of health services for children and adults. The policy aims to ensure that no act or omission by the CCG as a commissioning organisation, or via the services it commissions, puts an individual at risk; and that robust systems are in place to safeguard and promote the welfare of children, and to protect adults at risk of harm.
Recommendation (s):
Governing Body is requested to note the contents of this report and approve the adoption of the attached Safeguarding Children & Adults at Risk of Abuse Policy.
Previously Considered By: Date:
Clinical, Quality & Governance Committee 27 March 2019
CCG Strategic Objective(s) this report relates to:
Out of Hospital Personalisation Specialist Provision
Delivering Today √
Management of Conflicts of Interest: Not applicable
Financial Implications: Not applicable
Performance Implications: Not applicable
Quality Implications: Not applicable
Equality and Diversity Considerations: Not applicable
Patient, Public and Stakeholder Engagement: Not applicable
Risk Assessment: Not applicable

NHS South Warwickshire Clinical Commissioning Group Enc 09
Safeguarding Children & Adults at Risk of Abuse Policy Governing Body – 22 May 2019 Page 2 of 2
Blank Page
End of Report
Enc 09a
Safeguarding Children and Adults at Risk of Abuse Policy
NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 2 of 12
VERSION CONTROL
Version: 0.8
Ratified by: Governing Body
Date ratified: TBC
Name of originator/author: Tracy Redgate, Lead Nurse Safeguarding Adults
Name of responsible committee: Clinical Quality and Governance Committee
Date issued: TBC
Review date: May 2022
VERSION HISTORY
Date Version Comment / Update
27/03/2019 0.7 Subject to specified amendments, recommended to the Governing Body by the Clinical Quality and Governance Committee.
30/04/2019 0.8 Specified amendments made by Tracy Redgate and reviewed by Alison Walshe, Chief Nurse.
22/05/2019 0.8 Submitted to the Governing Body.

NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 3 of 12
Contents
1. Introduction ................................................................................................................................ 4
2. Legislation .................................................................................................................................. 4
3. Definitions .................................................................................................................................. 5
4. Purpose of the Policy ................................................................................................................. 6
5. Scope of the Policy .................................................................................................................... 7
6. Principles ................................................................................................................................... 7
7. Roles and Responsibilities ......................................................................................................... 8
8. CCG Responsibility for Ensuring Safeguarding Arrangements with Commissioned Provider Organisations ............................................................................................................................. 9
9. Complaints against a CCG Employee ...................................................................................... 10
10. Personal Health Budgets (PHBs) and Health Funded Long Term Placements (Continuing Health Care)............................................................................................................................. 11
11. PREVENT ................................................................................................................................ 11
12. Monitoring and Review ............................................................................................................. 12

NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 4 of 12
1. Introduction
It is the responsibility of every NHS funded organisation and each individual healthcare professional working in the NHS to ensure that the principles and duties of safeguarding adults and children are holistically, consistently and conscientiously applied, with the well-being of those adults and children at the heart of what we do. For adult safeguarding this also needs to respect the autonomy of adults and the need for empowerment of individuals’ decision-making, in keeping with the Mental Capacity Act and its Code of Practice (Safeguarding Vulnerable People in the NHS – Accountability and Assurance Framework, 2015).
As an NHS funded organisation the CCG has statutory responsibilities set out in the Safeguarding Vulnerable People in the NHS - Accountability and Assurance Framework (2015). The CCG needs to be assured not only that its own staff understand and fulfil their safeguarding responsibilities but that those organisations from which it commissions services have effective safeguarding arrangements in place. To support the CCG to fulfil its statutory safeguarding responsibilities, it secures the services of Designated Professionals and Adult Safeguarding Leads. The Designated Professional’s role is to work across the local health system to support other professionals in their agencies on all aspects of safeguarding and child protection. Designated Professionals are clinical experts and strategic leaders for safeguarding and as such are a vital source of advice and support to health commissioners in CCGs, the local authority and NHS England, other health professionals in provider organisations, quality surveillance groups (QSG), regulators, the LSCB/SAB and the Health and Wellbeing Board. The full detail of Designated Professionals’ and Adult Safeguarding Leads’ roles is set out in relevant inter-collegiate guidance. Safeguarding is everybody’s business and all staff should be appropriately trained to identify and raise potential safeguarding concerns, thus ensuring appropriate and timely action. All directors and staff working for the CCG in any capacity, including as a volunteer, are required to adhere to this policy and any associated procedures and guidelines that may be appended during the lifetime of this policy. The CCG is a statutory partner on the Children and Adults’ Safeguarding Boards (and in the future Safeguarding arrangements outlined in Working Together 2018) and is represented in these arrangements by the Chief Nurse. The CCG will ensure actively contribute to the strategic and assurance agendas for safeguarding and ensure the Health voice is appropriately represented and will ensure there are robust processes in place to learn and disseminate lessons for Health from cases where children or adults at risk have been seriously harmed or have died through abuse or neglect. The Local Safeguarding Children and Adults’ Boards (and in the future Safeguarding arrangements outlined in Working Together 2018) have a role in holding the CCG to account for fulfilling its statutory duties in respect of safeguarding.
2. Legislation
A number of legislative frameworks and statutory guidance underpin the CCG’s statutory responsibilities regarding safeguarding, and this policy should be read in conjunction with:
Caldicott Committee - Report on the Review of Patient-Identifiable Information (1997)
Care Act 2014
NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 5 of 12
Children and Social Work Act 2017
Domestic Violence, Crime and Victims Act 2004 Safeguarding Vulnerable Groups Act 2006 Mental Health Act 1983
House of Commons Education Committee Mental health and well-being of looked- after children Fourth Report of Session 2015–16.
Information Sharing: Advice for practitioners providing safeguarding services to children, young people, parents and carers (2018)
Looked After Children: Knowledge, Skills and Competences of health care staff. Intercollegiate Role Framework, 2015).
Mental Capacity Act 2005: Code of Practice (Department for Constitutional Affairs 2007)
Mental Capacity Act 2005 Equality Act 2010
National Tariff Payment System.
NHA Act 2006
NHS Safeguarding Assurance Framework (NHSE 2015)
Not Seen Not Heard: A review of the arrangements for Child Safeguarding and health care of Looked After Children in England (CQC, 2016)
Promoting the health and wellbeing of looked after children: Statutory Guidance for Local Authorities, Clinical Commissioning Groups and NHS England (2015)
Sexual Offences Act 2003
Statutory Guidance on Joint Strategic Needs Assessments and Joint Health and Wellbeing Strategies (2013)
Statutory guidance on making arrangements to safeguard and promote the welfare of children under section 11 of the Children Act 2004 (HM Government 2007)
Statutory Guidance on promoting the Health and well-being of Looked After Children (DH 2009)
The Children Act 1989 Guidance and Regulations Volume 2: Care Planning, Placement and Case Review
The Children Act 1989 Guidance and Regulations Volume 3: Transition to Adulthood
The Children Act 1989 Guidance and Regulations Volume 4: Fostering Services. Who Pays? Determining responsibility for payments to providers (2013)
Working Together to Safeguard Children (2018).
At a local level these legislative frameworks have directed the development of the policies and procedures of the Local Safeguarding Children Board (LSCB) and in the future Safeguarding arrangements outlined in Working Together 2018; and the Local Safeguarding Adults Board (LSAB)
The CCG has an additional statutory duty to adhere to the Human Rights Act 1998 and uphold fundamental rights contained within the Act for those who are unable to do this for themselves.
3. Definitions
For the purposes of this policy the following definitions provide clarity of terms.
Commissioning - The process of planning, buying and continuously improving services in order to achieve the best quality health outcomes for patients in accordance with population need and the funding available.

NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 6 of 12
Children - As defined in the Children Act 1989 and 2004, a child is anyone who has not yet reached their 18th birthday. ‘Children’ therefore means children and young people throughout.
Safeguarding children and Child protection are defined in ‘Working Together to Safeguard
Children (2018)’:
Safeguarding children is defined as:
Protecting children from maltreatment;
Preventing impairment of a child’s health or development;
Ensuring that children are growing up in circumstances consistent with the provision of safe and effective care;
Taking action to enable all children to have the best outcomes in their lives.
Child protection is part of safeguarding and promoting welfare but refers to:
Activity that is undertaken to protect specific children who are suffering, or are likely to suffer, significant harm.
Looked after Children (LAC) – CCGs have specific Corporate Parenting roles and responsibilities in relation to children and young people who are in the care of the Local Authority, as outlined in the Children and Social Work Act 2017. The Originating CCG remains the responsible commissioner regardless of where the child is placed, as per statutory guidance (‘Promoting the health and well-being needs of looked after children, 2015 and Who Pays (2014’).
Safeguarding adults - Safeguarding adults includes:
Prevention of harm and abuse through the provision of high quality care;
Effective responses to allegations of harm and abuse in line with local guidance;
Using learning to improve services to patients.
Adult at risk - The Care Act 2014 revises the definition of ‘adult at risk’ to be an adult who:
Has needs for care and support (whether or not the authority is meeting any of those needs);
Is experiencing, or is at risk of, abuse or neglect, and;
As a result of those needs is unable to protect himself or herself against the abuse or neglect or the risk of it.
Safeguarding is a continuum of responses that seek to prevent or respond to abuse and neglect. It is an umbrella term for both ‘promoting welfare’ and ‘protecting from harm’.
4. Purpose of the Policy
This policy sets out the Clinical Commissioning Group’s arrangements for safeguarding and promoting the welfare of children and adults at risk. It should be read in conjunction with local multi-agency procedures, which outline, in detail, actions to be undertaken where safeguarding concerns arise.
NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 7 of 12
This policy is aimed at CCG employees. Member practices, as individual healthcare providers, are required to have their own safeguarding policies.
5. Scope of the Policy
This policy covers the CCG’s safeguarding role as a commissioner of health services for children and adults. The policy aims to ensure that no act or omission by the CCG as a commissioning organisation, or via the services it commissions, puts an individual at risk; and that robust systems are in place to safeguard and promote the welfare of children, and to protect adults at risk of harm.
6. Principles
The CCG recognises that safeguarding children and adults at risk is a shared responsibility requiring effective joint working between agencies and professionals who have different roles and expertise in protecting vulnerable groups in society from harm. In order to achieve effective joint working there must be constructive relationships at all levels, promoted and supported by:
The commitment of the CCG’s Governing Body members and senior managers to safeguard children and adults at risk;
Clear lines of accountability within each organisation for safeguarding;
Staff training and continuing professional development (as outlined in the 3 Intercollegiate Competency documents for Children (2019), LAC (2015) and Adult (2018) to ensure an understanding not only of their own roles and responsibilities in respect of safeguarding, but also of those other professionals and organisations (see training strategy for details of staffing and the level of training required);
Safe recruitment and working practices, including disclosure and barring functions, and dealing with allegations against people who work with children and adults, where appropriate, in line with the Safeguarding Boards’ safer recruitment and employment policies (or the alternative Safeguarding arrangements);
Effective interagency working with local authorities, the police and third sector organisations, including appropriate arrangements to cooperate with local authorities in the operation of Safeguarding Children Board, Safeguarding Adults Board and Health and Wellbeing Boards;
Effective information sharing across organisations and agencies in line with GDPR (2017);
Employing or securing the expertise of Designated Safeguarding and Looked After Children’s Doctors and Nurses, and best practice Named GP/Professional (see section 7 roles and responsibilities);
Commissioning systems and processes that ensure services and care placements for individual adults and children provide adequate safeguards against abuse and neglect, including taking account of the requirements of the Mental Capacity Act 2005;
Effective systems for responding to abuse and neglect of adults and children;
Supporting the development of a positive learning culture across organisations to ensure that organisations are not unduly risk averse;
Working with the Local Authority and other partners to enable access to community resources that can reduce social and physical isolation for adults.

NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 8 of 12
7. Roles and Responsibilities
Accountable Officer: The ultimate accountability for safeguarding sits with the CCG’s Accountable Officer who has responsibility for ensuring that the health contribution to safeguarding and promoting the welfare of children and adults is discharged effectively across the whole health economy through commissioning arrangements.
Chief Nurse: The Chief Nurse is the Governing Body’s executive lead for safeguarding, and
has responsibility for providing leadership of the safeguarding agenda within the CCG. Specifically, the Chief Nurse will ensure:
Robust constitutional and governance arrangements are in place, including sufficient capability/capacity and lines to accountability, to ensure compliance with safeguarding responsibilities as set out in the NHS England Safeguarding Assurance Framework (2015).
Executive-level attendance at Adult and Children’s Safeguarding Board meetings (or alternative arrangement in line with Working Together 2018);
CCG participation, as required, in Domestic Homicide Reviews, Safeguarding Adult Reviews and Serious Case Reviews (or alternative arrangement in line with Working Together 2018), ensuring timely dissemination of learning and implementation of recommendations (holding providers to account, as required);
The securing of expertise from Designated and Named Professionals, as per Intercollegiate Guidance;
Governing Body members and CCG staff are appropriately trained (as per Inter-collegiate Guidance) and updated regarding their safeguarding responsibilities. This includes PREVENT and Mental Capacity Act
Commissioned providers are appropriately held to account for their safeguarding responsibilities via CCG contracting agreements;
That the voice of the service user is at the forefront of service planning and commissioning to ensure the voice and experience of vulnerable adults and children shapes the service delivery;
Provide regular reports to Governing Body and Clinical Quality and Governance Committee;
The provision of safe services to Looked After Children, for those placed in- area, as well as outside its borders.
Designated and Named Professionals
The following professional roles will be established in accordance with the Intercollegiate Guidance for Children’s Safeguarding (2019), Looked After Children (2015) and Adults’ Safeguarding (2018). Capacity within roles will be consider both the Intercollegiate Guidance and local need:
Designated Doctors and Nurses for Safeguarding Children and Looked After Children;
Designated Paediatrician for unexpected deaths in childhood;
Adults’ Safeguarding Lead;
Named Professional for Primary Care *(Best Practice);
Named Professional for Mental Capacity Act;
Named Professional for Prevent;
Strategic Lead for Child Sexual Exploitation.

NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 9 of 12
The roles will be supported by relevant policies and training, as per Intercollegiate competencies.
Individual CCG Members of staff are required to:
Be alert to the potential indicators of abuse or neglect for children and adults and know how to act on these concerns in line with local guidance;
undertake training in accordance with their roles and responsibilities;
understand the principles of confidentiality and information sharing in line with national and local guidance;
Contribute, if required, to multi-agency meetings established to safeguard children and adults at risk.
CCG Member Practices: As independent contractors, each Member Practice is required to have its own Safeguarding Policy and a named GP Safeguarding Lead (with Level 3 training Adults, Children and LAC). All staff within the practice are required to have undergone safeguarding training and updates to the required level and frequency (as per the Inter-Collegiate Guidance) and to work to the local safeguarding procedures.
8. CCG Responsibility for Ensuring Safeguarding Arrangements with Commissioned Provider Organisations
There are mechanisms in place to ensure the CCG is compliant with its responsibilities for safeguarding of children and adults with care and support needs who are at risk of abuse and neglect. These mechanisms include:
Annual reports, providing a review of activity with regard to children, LAC and adult safeguarding, to be presented to the CCG’s Governing Body.
Contribution to Audit/Review/ Inspection processes as required, such as Section 11 audits or Safeguarding Board quality assurance/improvement audits.
Regular safeguarding reports to Clinical Quality and Governance committee meetings and Governing Body meetings including the provision of Serious Case and Domestic Homicide review reports.
Completion of NHS England Safeguarding Assurance Tool or newest iteration
Review of provider safeguarding compliance through themed reviews/visits (utilising a suitable quality assurance review framework), attendance at safeguarding meetings, contractual KPI monitoring, safeguarding incident monitoring.
Assurance reports will include evidence of:
Children (Safeguarding), Looked after Children and Adult Safeguarding training appropriate to staff roles and responsibilities. This will include Mental Capacity Act and Deprivation of Liberties Safeguards (DoLS) and PREVENT training (see Safeguarding training strategy for further details);
Promotion of well-being and prevention of abuse and neglect with a focus on outcomes rather than just the process of safeguarding;
Participation in local safeguarding arrangements;
System/process change in response to learning from audits, reviews, inspections and safeguarding adults reviews;

NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 10 of 12
Provision of an accredited WRAP facilitator and sufficient resources to deliver the training programme.
9. Complaints against a CCG Employee
Children Working Together to Safeguarding Children (2018) explicitly states that where a complaint is received against an employee and that complaint has a child protection/child concern component, the organisation’s Safeguarding Lead must be notified and involved in reviewing the case and reporting it to the Local Authority Designated Officer (LADO). To deliver this responsibility the CCG will work within the local guidance and the CCG’s Disciplinary Policy. Adults Adults at risk can be subjected to abuse by those who work with them in any and every setting. For the purposes of this policy, a Person in a Position of Trust (PIPOT) is someone who works with or cares for adults at risk in a paid or voluntary capacity, including ‘shared lives carers’ (previously known as ‘adult foster carers’). All allegations of abuse, neglect or maltreatment of adults at risk by a PIPOT will be taken seriously and treated in accordance with the organisation’s procedures. All adults at risk are entitled to the same level and standard of protection from harm, regardless of whether they are receiving statutory or other services or if they are receiving none. To deliver this responsibility the CCG will work in conjunction with the West Midlands Adult Position of Trust Framework and the CCG’s Disciplinary Policy. PIPOT local arrangements will be followed in all cases in which there is an allegation that an individual has:
Behaved in a way that has harmed or may have harmed an adult at risk;
Possibly committed a criminal offence against or related to an adult at risk;
Behaved towards an adult at risk in a way that indicates she or he is unsuitable to work with such adults;
Behaved in a way that has harmed children or may have harmed children which means their ability to provide a service to adults at risk must be reviewed;
Been subject to abuse themselves, which means their ability to provide a service to adults at risk must be reviewed.
The scope of PIPOT procedures applies to all cases where concern, suspicion or allegation arises in connection with:
The PIPOT's own work/voluntary activity;
The PIPOT's life outside work (i.e. concerning adults at risk in the family or the social circle, risks to children, whether the individual's own children or other children).
Investigations regarding an employee of the CCG who fulfils the definition of PIPOT and about whom an allegation of adult abuse has been made will be undertaken in line with local safeguarding policies and procedures. Any associated management following investigation will be in line with the CCG Disciplinary policy/procedures. The CCG will ensure that information relating to PIPOT investigations is stored securely and

NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 11 of 12
may be accessed by the Safeguarding Executive Lead and Designated Nurse. In the event of change of organisational arrangements from the CCG to another organisation, arrangements will be made with the Caldicott Guardian for information to be retained indefinitely in line with national guidance.
10. Personal Health Budgets (PHBs) and Health Funded Long Term Placements (Continuing Health Care)
Safeguarding awareness will be an integral part of delivering personal health budgets and agreeing long term, health-funded placements. Person-centred approaches and self-care should work hand in hand with safeguarding principles through the process of shared decision making. When considering personal health budgets and/or long term placement requests the CCG will keep in mind the six principles of safeguarding adults (DH 2011):
Empowerment – Presumption of person led decisions and informed consent.
Protection – Support and representation for those in greatest need.
Prevention – It is better to take action before harm occurs.
Proportionality – Proportionate and least intrusive response appropriate to the risk presented.
Partnership – local solutions through services working with their communities. Communities have a part of play in preventing, detecting and reporting neglect and abuse.
Accountability – accountability and transparency in delivering safeguarding.
Personal health budgets will have checks and balances during the consideration and approvals process to ensure appropriate risk identification and management. A well-designed process from assessment to review will provide a more person- centred, outcome-focused mechanism for determining what the issues are that face the person, exploring any existing or potential risks and opening a dialogue about how these can be positively managed. With good information and planning people can be enabled to manage selected risks that enhance their quality of life and supported to eliminate or manage risks that are unacceptable. In considering options for long term placements the CCG will:
Demonstrate it is meeting its responsibilities to safeguard and promote the welfare of vulnerable adults; in so doing, supporting and complying with the Safeguarding Vulnerable Adults Board’s policies and procedures.
Have processes in place to ensure it can make safe adult care placements (such as in care homes, nursing homes or independent hospitals) based on knowledge of standards of care and safeguarding concerns and staff are aware of the escalation process if there is cause for concern.
Ensure that any systems and processes that include decision making about an individual (e.g. funding panels) take account of the requirements of the Mental Capacity Act 2005; this includes ensuring that action and decisions are documented in a way that demonstrates compliance with the Act.
11. PREVENT
The PREVENT Strategy (HM Government 2011) and updated Counter Terrorism Strategy (Contest) 2018 sets out the government’s commitment to understand factors which encourage people to support terrorism and then to engage in terrorism-related activity.

NHS South Warwickshire Clinical Commissioning Group Safeguarding Children and Adults at Risk of Abuse Policy – v0.8
Page 12 of 12
The health sector has a non-enforcement approach to PREVENT and focuses on support for vulnerable individuals and health care organisations. The PREVENT agenda requires healthcare organisations to work with partner organisations to contribute to prevention of terrorism by safeguarding and protecting vulnerable individuals and making safety a shared endeavour. Three national objectives have been identified for the PREVENT strategy:
Objective 1: respond to the ideological challenge of terrorism and the threat we face from those who promote it;
Objective 2: prevent people from being drawn into terrorism and ensure that they are given appropriate advice and support;
Objective 3: work with sectors and institutions where there are risks of radicalisation which we need to address.
“Building Partnerships, Staying Safe: The health sector contribution to HM Government’s PREVENT strategy: guidance for healthcare organisations” (DH Nov 2011) sets out guidance and toolkits for leaders, managers and workers in healthcare organisations. PREVENT awareness training within provider organisations is now included within the NHS Standard Contract within Service Conditions (SC32: Safeguarding). As such, it is mandated for all providers who deliver NHS services including non-NHS organisations. The CCG has a PREVENT lead, as required by NHS England CCG Prevent responsibility and duties (2015).
12. Monitoring and Review
The CCG will be held to account for its safeguarding statutory duties by the Local Safeguarding Boards (Children and Adult, or alternate arrangements as per Working Together 2018). This will be through the use of NHS England Safeguarding Assurance Tool (or newest iteration) which will support the CCG to comply with the Section 11 audit in respect of children; Self-Assessment Framework in respect of adults. This policy will be reviewed 3 yearly or earlier if there are significant changes to safeguarding legislation. End of Policy

NHS South Warwickshire Clinical Commissioning Group Enc 10
Operational Plan 2019/20 Governing Body - 22 May 2019
Page 1 of 2
Report To: Governing Body For decision √
Report Title: Operational Plan 2019/20 For discussion
Report From: Anna Hargrave
Chief Strategy Officer
For information
Date: 22 May 2019 Confidential
Purpose of the Report:
To inform the Governing Body of the outcome of the period of engagement undertaken in relation to NHS South Warwickshire Clinical Commissioning Group’s (“the CCG”) Operational Plan for 2019/20 and to ask the Governing Body to approve the Plan.
Key Points:
The NHS Long Term Plan was published on 7 January 2019. The associated NHS Shared Planning Guidance for 2019/20 (NHS Operational Planning and Contracting Guidance 2019/20) was published on 10 January 2019.
The Planning Guidance confirms that every CCG is required to agree an organisation level Operational Plan for 2019/20.
Section 4 of the Planning Guidance sets out the key deliverables which must be addressed within the Operational Plan, with Annex B providing a full list of deliverables.
The duty to publish an Operational Plan is also set out in section 14Z11 of the National Health Service Act 2006 (duty to prepare and publish a commissioning plan). The NHS Act specifies that the Plan must describe how the CCG intends to discharge specific statutory duties as they relate to quality, inequalities, public involvement and consultation and financial performance.
In order to ensure that NHS England, our population and stakeholders have maximum clarity:
o In Section 4 of the Operational Plan, the CCG confirms how it proposes to exercise the relevant statutory functions in the coming financial year.
o In Sections 5a-5g of the Operational Plan, the CCG confirms its priorities and deliverables for 2019/20 against the deliverables identified in the Planning Guidance.
The Operational Plan reflects the CCG’s Strategy for the period 2016-2020, the 2019/20 Commissioning Intentions and the Better Health, Better Care, Better Value Programme.
Engagement Process
A period of engagement on the Operational Plan was undertaken from 10 April to 6 May 2019.
As part of the engagement process, the Operational Plan was shared with key stakeholders and published to the CCG website. Those interested in doing so were able to provide feedback by completing a short survey.
The opportunity to engage with the CCG on the content of the Operational Plan was promoted though a number of different channels; the GP newsletter, email to the CCG Public and Patient Participation and Gateway Groups, feature on the CCG website and social media output.
Results of Survey
4 survey responses were received. While some positive feedback was noted, other feedback (both via the survey and verbal) highlighted that the Plan is lengthy and deals in complex subject matter, meaning that it does not feel accessible from a patient perspective.
In response to this feedback, it is proposed that an infographic summary of the Plan is developed.
Recommendation (s):
The Governing Body is asked:
To note the context and process undertaken to date to develop the CCG’s Operational Plan for 2019/20;

NHS South Warwickshire Clinical Commissioning Group Enc 10
Operational Plan 2019/20 Governing Body - 22 May 2019
Page 2 of 2
To note the outcome of the period of engagement undertaken and approve the proposed response; and
To approve the Operational Plan.
Previously Considered By: Date:
Executive Team
Performance Committee
Members’ Council
3 April 2019
24 April 2019
8 May 2019
CCG Strategic Objective(s) this report relates to:
Out of Hospital
Personalisation
Specialist Provision
Delivering Today
Management of Conflicts of Interest:
None relevant to this report.
Financial Implications: The Operational Plan aligns with the financial plan for 2019/20 and the medium term financial plan which have been developed by the CCG Finance Team.
Performance Implications:
The Operational Plan sets out activities that will improve the performance of the south Warwickshire system. Examples of areas where the Plan is expected to contribute to improved performance are; the NHS Constitution rights and pledges, progress against the NHS Long Term Plan, Better Care Fund targets, NHS Outcomes Framework targets and Public Health Outcomes Framework targets.
Quality Implications: As above.
Equality and Diversity Considerations:
The Operational Plan supports the CCG’s work to address the issues set out in the Joint Strategic Needs Assessment (JSNA) for Warwickshire and the emerging place-based JSNAs, including the need to reduce health inequalities.
Patient, Public and Stakeholder Engagement:
The Operational Plan describes the specific programmes and projects required to deliver year four of the CCG’s Strategy. The Strategy was developed with the support of and feedback from our key stakeholders including; our Member Practices, local health partners including South Warwickshire NHS Foundation Trust and Coventry and Warwickshire Partnership NHS Trust, Warwickshire County Council, patients and members of the public.
The Operational Plan was published on the CCG website for a period of engagement from 10 April to 6 May 2019.
Risk Assessment: Section 6 of the Operational Plan identifies the key risks to the delivery of the Plan, together with the mitigating actions that are in place.

Enc 10a
DRAFT
Operational Plan 2019/20
Operational Plan 2019/20 FINAL
Page 2 of 70
Contents
1. Overview …………………………………………………………………. page 3
2. Our System ………………………………………………………………… page 6
3. Our Place ………………………………………………………………… page 8
4. Our Plan …………………………………………………………………. page 15
4a. Assurance ………………………………………………………………... page 15
4b. Performance………………………………………………………………. page 15
4c. Quality……………………………………………………………………… page 16
4d. Equality……………………………………………………………………… page 17
4e. Finance ………………………………………………………………….. page 18
4f. Engagement …………………………………………………………. page 19
5. Our Response to the NHS Planning Guidance for 2019/20…………. page 22
5a. Cancer …………………………………………………………………… page 22
5b. Maternity Care……………………………………………………………. page 25
5c. Mental Health…………………………………………………………….. page 29
5d. Out of Hospital …………………………………………………………… page 37
5e. Personalisation……………………………………………………………. page 48
5f. Planned Care……………………………………………………………… page 58
5g. Urgent and Emergency Care…………………………………………….. page 61
6. Managing Key Risks ………………………………………………………… page 66

Operational Plan 2019/20 FINAL
Page 3 of 70
SECTION 1: Overview
“Since the CCG’s last Operational Plan was published there have been a number of significant achievements made – most notably our local Out of Hospital Transformation Programme has begun to fundamentally reshape the out of hospital system across Coventry and Warwickshire in line with the new model described in the NHS Long Term Plan. Looking forward to 2019/20 and beyond, this Operational Plan outlines the key work programmes that the CCG, and partner organisations, will focus on to enable us to deliver improvements in the health and wellbeing of our population. Health and care organisations in Coventry and Warwickshire see the next five years as a challenging, but pivotal period. Our combined ambition is to create a more efficient and effective health and care system, which is orientated towards prevention and early intervention, able to provide the best treatment and care and stay in financial balance. We want to ensure that services are co-ordinated, work with people’s own resources and are committed to achieving the best possible outcomes for people. To achieve our ambition, we need to adopt ways of working and models of care that boost people’s sense of control, capability and independence. Better Health, Better Care, Better Value, the local partnership of NHS organisations and Councils, has already provided an opportunity to tackle challenges, develop innovative approaches and transform services. In this Operational Plan we commit to seizing the momentum and impetus that the partnership has created to explore how much further and faster we can move towards realising a truly joined up, high quality, sustainable, modern and accessible health and care system in Coventry and Warwickshire.” Dr David Spraggett Chair of the CCG
This document sets out NHS South Warwickshire Clinical Commissioning Group’s (‘the CCG’) Operational Plan for 2019/20. Developed in response to the publication of the NHS Long Term Plan (‘the NHS LTP’) and the associated NHS Operational Planning and Contracting Guidance (‘the NHS OP&CG’), this Plan recognises that 2019/20 will be a pivotal year for the CCG and the wider Coventry and Warwickshire health and care system. Just as the NHS LTP describes 2019/20 as a ‘transitional year’ for the NHS, this Operational Plan gives a clear signal that 2019/20 will be a year of transition in Coventry and Warwickshire – one in which the architecture of our system will begin to change, a new governance structure will emerge and both CCGs and Providers will redefine their ‘business as usual’ ways of working. All of this with the aim of creating conditions in which, over the coming five years, real progress can be made to transform the way that health and care services are commissioned and delivered, and, in turn, to improve outcomes for individuals and populations, so that over time the people of Coventry and Warwickshire are able to live healthier and more fulfilled lives. As this Plan will demonstrate, we have strong foundations to build from moving into 2019/20. The NHS LTP describes a new world of system working, in which, by April 2021, Integrated Care Systems cover the whole country. Section 2 outlines what has already been achieved in 2018/19 in relation to the development of an Integrated Care System (‘ICS’) for Coventry and Warwickshire and how we will build on this during 2019/20. The formation of the Coventry and Warwickshire Better Health, Better Care, Better Value (‘BHBCBV’) Partnership in 2016 is recognised as a critical milestone in the local ICS journey. As a consequence of the experience gained over the last two years through the development and delivery of the BHBCBV Programme, Commissioner and Provider organisations from across the Coventry and Warwickshire system are firmly of the belief that if we are going to secure the greatest possible health gain for our population within the resources available to us:
We cannot keep doing things the way that we have always done them; and
Greater collaboration between organisations (be that between Commissioners, between Providers or between Commissioners and Providers) is needed to transform services and manage resources.
The work (both completed and planned) described in Section 2 demonstrates not only how far relationships between the BHBCBV partner organisations have strengthened and matured, but also each organisation’s commitment to accelerating the development of an ICS in 2019/20, driving the transition of our system from its current form to a new one which both enables and prioritises collaboration.
Operational Plan 2019/20 FINAL
Page 4 of 70
Section 2 provides an overview of the BHBCBV Programme identifying the key workstreams within the Programme. Each workstream has established its priorities for 2019/20 aligned to the key deliverables in the NHS OP&CG. Section 2 also highlights the work undertaken by the BHBCBV Clinical Design Authority (made up of senior clinical leaders from across Coventry and Warwickshire) during 2018/19 to develop a system-wide clinical strategy. The clinical strategy identifies three priority areas for the local system which are frailty, mental health and musculoskeletal (MSK) services; these are areas where there is a clear opportunity to deliver improved outcomes for patients and a recognised need to test whether the financial investment being made by the system represents value in relation to the outcomes being achieved. Throughout 2019/20, the Clinical Design Authority will oversee work to develop best practice pathways for the three priority areas. Work will then be undertaken at Place level to redesign pathways in line with these best practice examples. Ultimately this will allow the CCG to be confident that pathways are being delivered in a way that is evidence-based, demonstrably high quality and cost effective. As we have already signalled in our commissioning intentions for 2019/20, the future Coventry and Warwickshire ICS will be a place-based system, made up of four Places including south Warwickshire. Section 3 sets out what we expect to be happening at Place level in 2019/20. Our experience through the on-going local Out of Hospital Transformation Programme tells us that Place will be the level where most service change will take place in the future ICS, where decisions about how money is spent will be made and where opportunities to get better value will be identified. As such, Place development will be an area of focus in 2019/20. We will again be able to build on the foundation of work completed in 2018/19. Design principles agreed in December 2018 will provide a framework for the three CCGs to work with Providers in each Place in a way that will ensure that there is consistency of purpose across the Places whilst allowing local variation, recognising the need to reflect different populations and Provider landscapes in each Place. In line with the NHS LTP, and as part of Place development, supporting GP Networks will also continue to be a priority in 2019/20. Networks will be the building blocks of the future ICS and much progress has already been made. Seven Networks are established in south Warwickshire, broadly aligned to the Place Based Teams, which are the on the ground delivery mechanism for the new Out of Hospital service. Section 3 recaps what has been achieved locally in relation to Network development to date and what we will be focusing on in 2019/20. We acknowledge that considerable effort and resource will need to be directed into expanding engagement with our GP and broader general practice workforce during 2019/20 to ensure that they understand and are confident in the purpose of their participation in both Networks and Place. We expect that the publication of the new national Network contract (Directed Enhanced Service) during 2019 will provide additional impetus for this engagement. As set out in Sections 2 and 3, both CCGs and Providers will need to devote time, resource and energy to reshaping the architecture of the local system in 2019/20. For CCGs the focus will, in part, be on developing a single commissioner for Coventry and Warwickshire. A key objective for the so-called ‘Strategic Commissioner’ will be to develop ‘strategic commissioning’ – this will move the Strategic Commissioner away from commissioning volume and activity to commissioning improved outcomes for defined groups of people or populations, as well as focusing on health inequalities within the population. Strategic commissioning will be fundamentally driven by engagement with patients and the public to understand what outcomes matter most and are meaningful to them. The new place-based Joint Strategic Needs Assessments (‘JSNAs’) for Warwickshire will be a key resource for the Strategic Commissioner to be able to understand population need at a more local level than ever before and to determine priorities accordingly. Whilst the development of a single commissioner will accelerate the CCG’s ability to act as a Strategic Commissioner, it is not contingent on it; indeed our commissioning intentions clearly articulate our intent to act as a Strategic Commissioner as our standard approach in 2019/20. Already we have done this within the local Out of Hospital and CAMHS (Child and Adolescent Mental Health Services) Transformation Programmes, which have delivered two new outcomes-based contracts. Section 3 sets out how, acting as a Strategic Commissioner and as the system architecture gradually evolves to that of a fully functioning ICS, we will focus on a number of ‘developmental’ contracts during 2019/20. Not only will this enable the CCG to further develop and embed the competencies and capabilities that will be required within the future

Operational Plan 2019/20 FINAL
Page 5 of 70
ICS, it will also allow us to drive improvements in quality, outcomes and financial sustainability in the short to medium term. A number of national and local priorities (including frailty, mental health and MSK services) will ultimately sit in one the developmental contracts. The developmental contracts should not, however, in themselves be seen as a solution; what they will enable us to do is put in place the financial and contractual incentives for transformation to happen at Place level. As we have signalled in our commissioning intentions, it is not only the three CCGs that will need to develop different competencies and capabilities to operate effectively within the future ICS. Over time functions and tasks that CCGs have undertaken historically will transfer from the Strategic Commissioner to sit with Providers. These so-called ‘delivery commissioning’ functions (for example, service redesign at pathway level) will, at a future point, be undertaken by Providers at Place level. During 2019/20, the CCG will continue to undertake delivery commissioning functions, while at the same time working closely with individual Providers and the Provider Alliance established in 2018/19 to ensure that the Provider Alliance develops in tandem with the Strategic Commissioner and is supportive of the evolution process, in terms of both stages of development and the end goal. In Sections 4 and 5 we confirm that we will not be distracted from the need to remain focused on the delivery of our statutory functions as a CCG (as these relate to performance, quality, finance and engagement) and the continued delivery of priorities set out in our 2016-2020 strategy Translating our 2020 Vision into Reality during the coming year of transition. Although 2019/20 is the final year of the strategy, the key drivers for it remain relevant and the priorities that it identifies are aligned to national priorities set out in the NHS LTP and reflected in the NHS OP&CG. The strategy’s focus on the transformation of out of hospital care is particularly noteworthy. Through the local Out of Hospital Transformation Programme, which was a major area of focus within the CCG’s previous 2 year Operational Plan, the out of hospital system in south Warwickshire is already being fundamentally reshaped in line with the new model described in the NHS LTP. The Out of Hospital Transformation Programme also gives us local proof of the effectiveness of contracts delivered through an outcomes-based approach to drive integrated, person-centred care. Our strategy will continue to be a focal point for the CCG’s work in 2019/20 and we remain committed to finishing what we have started across the four cornerstones (Out of Hospital, Personalisation, Specialist Provision and Delivering Today), even as we work on the development of the ICS and begin to pave the way for a seamless transition to a new system wide Strategic Framework, underpinned by a Five Year Plan. Since 2016 the Delivering Today cornerstone of our strategy has clearly focused the CCG on the delivery of financial targets and business rules required by NHS England. As set out in Section 4e delivering an in-year financial surplus of £1.9m in line with our medium term (five year) financial plan will be a key priority for the CCG in 2019/20. The CCG has developed its Quality, Innovation, Productivity and Prevention (‘QIPP’) Programme for 2019/20 – successful delivery of the various projects within the Programme will be critical to the overall delivery of the CCG’s financial plan for 2019/20. In support of the broader system aspiration to ‘live within our means’ that all BHBCBV partner organisations have endorsed, and recognising the stretching QIPP and Cost Improvement Programme (CIP) targets that all CCGs and Providers will be working to in 2019/20, the CCG and main Acute Provider within each Place will agree and take joint ownership of a Value Programme for that Place. In south Warwickshire, the Programme will focus the CCG and South Warwickshire NHS Foundation Trust on demand management as a key lever for driving efficiency and reducing costs. In order to ensure that our population and stakeholders have maximum clarity regarding our response to the NHS OP&CG, in Sections 5a-5g we confirm our priorities and deliverables for 2019/20 against the key areas identified in the NHS OP&CG. We have sought to ensure that there is a clear read across between the priorities identified in Section 5 and the deliverables outlined in the NHS OP&CG. Finally, in Section 6 we set out the key risks and issues that are likely to impact the delivery of our Operational Plan in 2019/20 and describe our approach to risk management.

Operational Plan 2019/20 FINAL
Page 6 of 70
Key Messages:
During 2019/20 the CCG’s overarching priorities will be:
To remain focused on the delivery of our strategy Translating our 2020 Vision into Reality and our vision to ‘build relationships with patients and our communities to improve health, transform care and make the best use of our resources’.
To continue to support the delivery of the Coventry and Warwickshire Better Health, Better Care, Better Value Programme.
To work with system partners to put in place the building blocks of an Integrated Care System. This will involve the CCG focusing on the development of a single commissioner for Coventry and Warwickshire, alongside supporting the development of delivery commissioning, south Warwickshire as a Place and the seven local GP Networks.
To work with system partners to develop a new system wide Strategic Framework, which will be the anchor for the Five Year Plan required by NHS England in the autumn of 2019.
This Operational Plan should be read in conjunction with other published documents including our strategy and commissioning intentions for 2019/20. These documents are available on the CCG website: https://www.southwarwickshireccg.nhs.uk/.

Operational Plan 2019/20 FINAL
Page 7 of 70
SECTION 2: Our System
As we have clearly signalled in our commissioning intentions for 2019/20 there is consensus across Commissioner and Provider organisations in Coventry and Warwickshire that our direction of travel at system level in the coming year will be towards the development of an ICS. The anticipated benefits of forming an ICS are set out in the NHS LTP and it is not our intention to rehearse those here. Locally the formation of the Coventry and Warwickshire BHBCBV Partnership in 2016 is recognised as a critical milestone in our ICS journey. As a consequence of the experience gained over the last two years through the development and delivery of the BHBCBV Programme, Commissioner and Provider organisations from across the Coventry and Warwickshire system are firmly of the belief that if we are going to secure the greatest possible health gain for our population within the resources available to us:
We cannot keep doing things the way that we have always done them; and
Greater collaboration between organisations (be that between Commissioners, between Providers or between Commissioners and Providers) is needed to transform services and manage resources – such collaboration is fundamentally characteristic of the BHBCBV Programme.
The BHBCBV Programme consists of a number of key workstreams; five transformational workstreams (Planned Care, Urgent and Emergency Care, Mental Health and Emotional Wellbeing, Maternity and Paediatrics and Proactive and Preventative Care) and three enabling workstreams (Productivity and Efficiency, Digital Transformation and Estates). These workstreams are driving a number of system-wide transformational projects which provide both proof of concept and (in their delivery) the foundations for the future ICS. The BHBCBV Clinical Design Authority (‘CDA’) is an important part of the overall governance structure of the BHBCBV Programme. During 2018/19 the CDA has developed a system-wide clinical strategy, which identifies three priority areas for the local system: frailty, mental health and MSK services. As part of the local journey towards becoming an ICS, BHBCBV partner organisations participated in an ICS Development Programme across the summer of 2018. The outputs of the Programme are a set of roadmaps which will continue to guide the system journey in 2019/20. Through participation in the Development Programme, there is now a clearer shared vision of the end state or design model that we are looking to achieve in Coventry and Warwickshire:
As agreed by the Coventry and Warwickshire Place Forum (made up of the Health and Wellbeing Boards of Coventry and Warwickshire), the future ICS will be made up of four Places, including south Warwickshire.
There will be a single commissioner for Coventry and Warwickshire. This Strategic Commissioner will move away from commissioning volume and activity to commissioning improved outcomes for defined groups of people or populations, as well as focusing on health inequalities within the population.
Both CCGs and Providers will need to develop different competencies and capabilities to operate effectively within the future ICS. Over time functions and tasks that CCGs have undertaken historically will transfer from the Strategic Commissioner to sit with Providers. These so-called delivery commissioning functions will, at a future point, be undertaken by Providers at Place level.
A Provider Alliance will be established. The Provider Alliance will have a shared sense of ownership with the Strategic Commissioner about what needs to happen across the system.
Ultimately, and in line with emerging information at national level relating to Integrated Care Provider (ICP) contracts, the Strategic Commissioner will place a contract with a single organisation or partnership of organisations within a Place to manage a single budget and deliver a range of services for the local population, focusing on the population’s health and wellbeing.
If you carry the above logic through, the end state in Coventry and Warwickshire will consist of the Strategic Commissioner placing four ICP contracts (one per Place), with the four Integrated Care Providers working collaboratively through the Provider Alliance to deliver the outcomes set by the Strategic Commissioner.
Another key action at system level during 2019/20 will be the development of a new system wide Strategic Framework. The anchor for the Strategic Framework will be the Concordat agreed by the Coventry and Warwickshire Place Forum in July 2018:

Operational Plan 2019/20 FINAL
Page 8 of 70
Prioritising prevention: We will tackle the causes of health-related problems to reduce the impact of ill-health on people’s lives, their families and communities. We will seek to address the root causes of problems, listening to local people’s priorities and acting on their concerns. Strengthening communities: We will support strong and stable communities. We will listen to residents to understand what they want from the services we provide and encourage them to lead change themselves where possible. Co-ordinating services: We will work together to design services which take account of the complexity of people’s lives and their over-lapping health and social needs. We will focus on the best way to achieve good outcomes for people, reducing the number of interactions people have with our services and avoiding multiple interventions from different providers. Sharing responsibility: We value the distinct contributions made by all the organisations that are part of this Concordat. We will maintain partnerships between the public sector, voluntary and community sector, local businesses and residents, recognising that we share a responsibility to transform the health and well-being of our communities. We will pool resources, budgets and accountabilities where it will improve services for the public.
In turn the Strategic Framework will be the anchor for the Five Year Plan required by NHS England in the Autumn of 2019 – it will articulate a clear narrative for the system as a whole which builds on the design model set out on page 7.
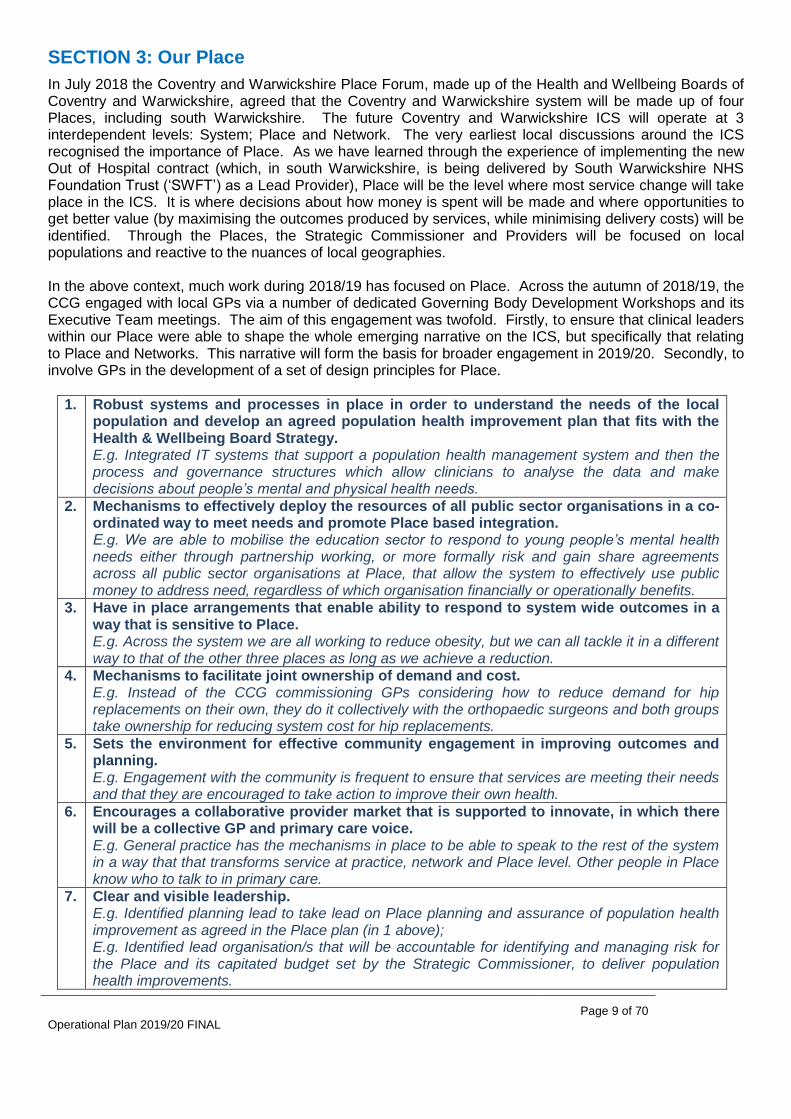
Operational Plan 2019/20 FINAL
Page 9 of 70
SECTION 3: Our Place
In July 2018 the Coventry and Warwickshire Place Forum, made up of the Health and Wellbeing Boards of Coventry and Warwickshire, agreed that the Coventry and Warwickshire system will be made up of four Places, including south Warwickshire. The future Coventry and Warwickshire ICS will operate at 3 interdependent levels: System; Place and Network. The very earliest local discussions around the ICS recognised the importance of Place. As we have learned through the experience of implementing the new Out of Hospital contract (which, in south Warwickshire, is being delivered by South Warwickshire NHS Foundation Trust (‘SWFT’) as a Lead Provider), Place will be the level where most service change will take place in the ICS. It is where decisions about how money is spent will be made and where opportunities to get better value (by maximising the outcomes produced by services, while minimising delivery costs) will be identified. Through the Places, the Strategic Commissioner and Providers will be focused on local populations and reactive to the nuances of local geographies. In the above context, much work during 2018/19 has focused on Place. Across the autumn of 2018/19, the CCG engaged with local GPs via a number of dedicated Governing Body Development Workshops and its Executive Team meetings. The aim of this engagement was twofold. Firstly, to ensure that clinical leaders within our Place were able to shape the whole emerging narrative on the ICS, but specifically that relating to Place and Networks. This narrative will form the basis for broader engagement in 2019/20. Secondly, to involve GPs in the development of a set of design principles for Place.
1. Robust systems and processes in place in order to understand the needs of the local population and develop an agreed population health improvement plan that fits with the Health & Wellbeing Board Strategy. E.g. Integrated IT systems that support a population health management system and then the process and governance structures which allow clinicians to analyse the data and make decisions about people’s mental and physical health needs.
2. Mechanisms to effectively deploy the resources of all public sector organisations in a co-ordinated way to meet needs and promote Place based integration. E.g. We are able to mobilise the education sector to respond to young people’s mental health needs either through partnership working, or more formally risk and gain share agreements across all public sector organisations at Place, that allow the system to effectively use public money to address need, regardless of which organisation financially or operationally benefits.
3. Have in place arrangements that enable ability to respond to system wide outcomes in a way that is sensitive to Place. E.g. Across the system we are all working to reduce obesity, but we can all tackle it in a different way to that of the other three places as long as we achieve a reduction.
4. Mechanisms to facilitate joint ownership of demand and cost. E.g. Instead of the CCG commissioning GPs considering how to reduce demand for hip replacements on their own, they do it collectively with the orthopaedic surgeons and both groups take ownership for reducing system cost for hip replacements.
5. Sets the environment for effective community engagement in improving outcomes and planning. E.g. Engagement with the community is frequent to ensure that services are meeting their needs and that they are encouraged to take action to improve their own health.
6. Encourages a collaborative provider market that is supported to innovate, in which there will be a collective GP and primary care voice. E.g. General practice has the mechanisms in place to be able to speak to the rest of the system in a way that that transforms service at practice, network and Place level. Other people in Place know who to talk to in primary care.
7. Clear and visible leadership. E.g. Identified planning lead to take lead on Place planning and assurance of population health improvement as agreed in the Place plan (in 1 above); E.g. Identified lead organisation/s that will be accountable for identifying and managing risk for the Place and its capitated budget set by the Strategic Commissioner, to deliver population health improvements.

Operational Plan 2019/20 FINAL
Page 10 of 70
8. Clear and effective governance arrangements that allow effective decision making at Network, Place and System levels.
Table 1: Coventry and Warwickshire Place Design Principles The design principles were approved by the CCG’s Governing Body in December 2018 and have also been endorsed by the BHBCBV Board. During 2019/20 the CCG will work closely with our Member GP Practices, SWFT and Coventry and Warwickshire Partnership NHS Trust (‘CWPT’) to shape how we want to operate in south Warwickshire to deliver the eight principles. Not only will this involve SWFT, CWPT and the GP Practices needing to establish strong and effective partnerships amongst themselves, they will also need to consider how they will work with communities – seeing the people who they deliver services to as assets and partners. The participation of our two Local Authorities (Stratford-on-Avon District Council and Warwick District Council), voluntary, community and social enterprise organisations and many others in local partnerships will also be essential if we are to improve the health of our communities by tackling the wider issues that can affect health (ranging from alcohol and diet, to poverty, housing quality, leisure services and employment) and find ways of connecting people to the wide range of resources that communities can offer. Engagement with the District Councils will also be fundamental in developing the strategic approach that will be taken at Place level in relation to prevention, early intervention, self-help and self-care. The design principles will ensure that there is consistency of purpose across the four Places in Coventry and Warwickshire in undertaking this work, whilst allowing local variation on the delivery of the purpose, recognising the need to reflect different populations and Provider landscapes in each Place. It is important to remember that south Warwickshire already has many building blocks for Place established. The process that we will work through in 2019/20 needs to build on these, not start from scratch if they are working well and are owned by key partners in the Place. A notable example is the South Warwickshire Health and Wellbeing Partnership; a forum which already brings together CCG, District Council and County Council representatives, along with Healthwatch, to advance the health and wellbeing of local people and to encourage people and organisations who arrange for the provision of health and social care services in the area to work in an integrated manner.
As we note in Section 1, another key part of our plan for 2019/20 at Place level is to work on practical examples and learn as we do. Section 2 describes the end state that we are envisioning at the current time as consisting of the Strategic Commissioner placing four outcomes-based ICP contracts – one contract per Place. To get to this end state, CCGs and Providers will need to develop and embed the competencies and capabilities that will be required within the future ICS so that, in the future, the Strategic Commissioner can be confident in placing the ICP contract. To this end, the BHBCBV Board has agreed a Transformation Programme which will be enacted through a number of developmental contracts. This Programme will allow CCGs and Providers to work in sequence to make the shift to outcomes-based contracts in readiness for a single ICP contract per Place and will provide the framework for the development of strategic commissioning, delivery commissioning, Place and the Provider Alliance in a co-ordinated and systematic way. The Transformation Programme will also allow us to drive improvements in quality, outcomes and financial sustainability in the short to medium term. A number of national and local priorities (including frailty, mental health and MSK services) will ultimately sit in one the developmental contracts. The developmental contracts should not, however, in themselves be seen as a solution; what they will enable us to do is put in place the contractual and financial incentives for transformation to happen at Place level.
Area Status
Out of Hospital The commissioning process which led to the award of the new Out of Hospital contract provides a good example of the transformation methodology that will need to be applied to other areas. This methodology is now being replicated in relation to Planned Care and Maternity, Children and Young People Services.
A common outcomes framework is in place across the system but how it is delivered locally reflects differences in each Place.
The 3 new contracts (1 per CCG) implemented from April 2018 provide the basis for the future operating model at Place level. The Strategic Commissioner will

Operational Plan 2019/20 FINAL
Page 11 of 70
challenge Providers to build on this.
The Out of Hospital model of care promotes health and wellbeing, independence, community support and self-care in or close to people’s homes.
Some differences exist in scope particularly between Coventry and Warwickshire and these will be addressed in 2019/20.
Opportunity to expand the scope in general e.g. NHS Continuing Healthcare, mental health services and Local Authority commissioned services. These opportunities will be reviewed during 2019/20.
Addresses local priority (frailty).
Planned Care Transformation Programme established and being progressed using the same methodology as Out of Hospital.
The scope will include Cancer services.
Initial phase of engagement completed in south Warwickshire.
The Programme will now expand across the whole system with a second phase of engagement planned to commence in April 2019.
Each Place will agree a phased redesign programme to systematically work through the specialities over a two year period based on Place priorities.
Reducing activity that is not adding value will be a key driver.
Learning will be shared across the system to maximise benefit.
All places will include MSK as phase 1 priority. Dermatology and Ophthalmology are the other phase 1 priorities in south Warwickshire.
The phased implementation approach will allow each Place to take early efficiencies and resize demand.
Addresses local priority (MSK services).
Maternity, Children and Young People Services
Transformation Programme established in relation to Maternity and Paediatrics and being progressed using the same methodology as Out of Hospital.
Phase 1 completed (including engagement and development of desirable criteria and draft outcomes framework).
Phase 2 planned to commence in May 2019. This phase will build on the work being undertaken simultaneously, led by the Local Maternity System.
A separate element of this programme will seek to deliver improved collaboration between all service providers (both health and social care) for women, children and young people.
Mental Health During 2018/19 a new outcomes based contract for CAMHS (Child and Adolescent Mental Health Services) was awarded, establishing the ‘RISE’ Transformation Programme jointly commissioned by the 3 CCGs and Warwickshire County Council.
Commissioners plan to begin broader engagement on mental health services during 2019/20. The objective of the engagement will be to determine how to effectively commission mental health services to ensure integration with physical health.
Addresses local priority (Mental Health).
Urgent and Emergency Care
As per Mental Health, Commissioners will initially undertake engagement to determine the most effective scope and mechanism for this contract.
Table 2: Coventry and Warwickshire ICS Transformation Programme – Developmental Contracts As the CCG recognises in its 2019/20 commissioning intentions a proliferation of evidence tells us that successful outcomes based commissioning is only possible if appropriate contracting and payment mechanisms are in place. With this in mind, an area of focus within the Transformation Programme set out in Table 2 will be to innovate our contracting and payment approaches in tandem with our approach to commissioning.
As we highlight in Section 1, as part of Place development, supporting the development of GP Networks will also continue to be a high priority in 2019/20. Networks will be the building blocks of the future ICS and

Operational Plan 2019/20 FINAL
Page 12 of 70
much progress has already been made. Seven Networks are established in south Warwickshire, broadly aligned to the Out of Hospital Place Based Teams. The CCG has directed considerable energy into Network development during 2018/19, with dedicated staff resource identified to focus on this agenda. The Networks have been meeting together regularly to share learning and progress via an All GP Networks meeting established in June 2018. Each Network has developed an action plan and in areas where new place-based JSNAs are available these have been used to inform and shape the plans. A structured process has also been introduced to enable the Networks to bring forward proposals which address a population need that they have identified at Network level and which require resource support. A recent proposal led to the CCG funding 25 places for Practice Nurses to receive training relating to the care of those with paediatric respiratory conditions. As noted earlier in this section, engagement with Governing Body members and the CCG Executive Team has taken place around Networks and the CCG has also run a number of Focus Groups aimed specifically at securing the engagement of some of our Member GP Practices who we hear from less often. The outputs of this engagement have helped us to develop a narrative on the case for change as it relates to Networks specifically, which will form the basis for broader engagement in 2019/20. It has also allowed us to deepen our understanding of some of the barriers that our GP practices perceive in relation to Network participation – a key one being how the associated language around ‘moving care out of the hospital’ lands with GPs as an assumption that they will need to do more at a time when they already stretched. There are now examples from within south Warwickshire that counter this idea; for example, our Member GP Practice Croft Medical Centre identified diabetes as a priority and subsequently worked with the local Diabetes Specialist Nurse and a SWFT consultant to establish a small local multi-disciplinary team focused on improving the outcomes of a targeted group of patients. The on-going development of the Out of Hospital Place Based Teams during 2019/20 will continue to move us towards this kind of collaborative model of out of hospital care across south Warwickshire. GP Practices can expect to see community services and resources tailored to meet the needs of their patients; with a clear focus on putting robust management plans in place for the most high-risk patients and co-ordinating care. As well as delivering benefits for patients, this approach aims to reduce burden on practices and release capacity. We strongly acknowledge that more effort and resource will need to be directed into expanding engagement with our GP and broader general practice workforce during 2019/20 to ensure that they understand and are confident in the purpose of their participation in both Networks and Place. We expect that the publication of the new national Network contract (Directed Enhanced Service) during 2019 will provide additional impetus for this engagement.
Workforce Working with the other Coventry and Warwickshire CCGs, in 2017 we developed a General Practice Workforce Strategy for Coventry and Warwickshire. The Strategy is premised on the shared value that: ‘A growing and ageing population, with complex, multiple conditions, means that personal and population-orientated primary care is central to our local health system. It is our belief that if general practice fails, the whole NHS fails.’ As a CCG we are clear that some workforce challenges will require system wide action whilst others require focus and action at Place level. The Workforce Strategy identifies our key system challenges as follows:
Almost a quarter of GPs in Coventry and Warwickshire and over a third of nurses are aged over 54;
Workload in general practice is increasing at a greater rate than the workforce;
Significant health inequalities exist across the footprint;
Our population is aging and increasing (in part as a consequence of significant planned housing growth).
In the above context, the Strategy sets four strategic objectives which we will continue to focus on in 2019/20:
Stabilising the current general practice workforce – by implementing a range of recruitment and
retention activities, with the Practice Nurse workforce being a particular focus group in south
Warwickshire.

Operational Plan 2019/20 FINAL
Page 13 of 70
Putting in place the foundations for a more robust approach to workforce planning – so that we not only have a clear understanding of workforce demand and supply trajectories, but also integrate other key processes such as succession planning, career development and talent management.
Investing in the development of the wider primary care workforce – challenging the boundaries of traditional roles and supporting clinical and non-clinical staff to extend their scope of practice in order to most effectively manage the growing demands on general practice teams. Also exploring how new roles (clinical pharmacists, Advanced Nurse Practitioners, social prescribers, etc.) can improve access to care, enhance patient safety and streamline patient pathways, ensuring that holistic care is delivered more efficiently.
Supporting the continuing development of Networks – focusing on the development of Network workforces through population health-based workforce redesign.
Significant progress has already been made and we will build on this. In 2018/19, we have:
Worked with the other Coventry and Warwickshire CCGs to deploy national funding to develop a local GP retention scheme. The scheme incorporates 3 elements: GP mentors, #careforyourcareer and GP transformational posts. 20 GP mentors have been recruited across Coventry and Warwickshire. Funding was secured from the Coventry and Warwickshire Local Workforce Action Board (‘the LWAB’) to create a development programme for the mentors in conjunction with Coventry University. The #careforyourcareer campaign has launched on social media and a dedicated website will go live in 2019/20. A series of videos have been produced to support the social media campaign, engaging local GPs, Practice Nurses and Practice Managers: https://vimeo.com/318988448/da5741ddc5.
Supported the local Training Hub in the delivery of the General Practice Nursing 10 point action plan – with the main focus being on supporting recruitment, training, retention and return to work for all nurses. This includes encouraging Member GP Practices to support the training, mentoring and preceptorship of student nurses, new practice nurses, Advanced Nurse Practitioners and those returning to the nursing profession.
Secured funding from Health Education England (via the LWAB) to develop and implement a local Primary Care Leadership Programme. Successful applicants are working through the NHS Leadership Academy Mary Seacole Programme. This programme will be expanded to Advanced Nurse Practitioners in 2019/20.
Worked with the Training Hub to deliver a training programme for Practice Managers.
Secured support from NHS England to run a training needs analysis. 26 Member GP Practices responded and the outputs are now being analysed – this analysis will support more targeted workforce planning in 2019/20.
Continued to support successful local social prescribing schemes which are enabling our Member GP Practices to test the effectiveness of new roles. The Active Monitoring scheme (which is being implemented in Bidford-on-Avon and Stratford-upon-Avon) offers an early intervention approach for people experiencing mild to moderate mental health problems and is being delivered by mental health practitioners working across five GP practices.
Deployed funding from the General Practice Resilience Fund to provide backfill for nurse and Health Care Assistant training.
Maintained close links with the local General Practice Nurse Development Nurse with the aim of ensuring that her work complements and is informed by the Primary Care Workforce Strategy – as a consequence we now have 11 mentors supporting student nurse placements (an increase from 2 previously).
Progressed plans for a new approach to Protected Learning Time and Practice Nurse Forum sessions to commence in 2019/20.
Throughout 2019/20 the Primary Care Workforce Strategy will continue to drive the CCG’s work in this area. The delivery of the Strategy and associated delivery plan will be overseen by a Local Workforce Group, which engages the GP Federation (South Warwickshire GP) and SWFT. The Group will maintain strong links with the BHBCBV Workforce Group and the LWAB.

Operational Plan 2019/20 FINAL
Page 14 of 70
Estates Alongside other Sustainability and Transformation Partnership (STP) areas nationally, Coventry and Warwickshire produced a single estates strategy that was submitted to NHS England and NHS Improvement in July 2018. Feedback on this submission has been provided and will be addressed by the BHBCBV Estates Group ahead of any future submission deadline. The CCG will continue to be an active member and support the work of the BHBCBV Estates Group in 2019/20. Locally, the CCG has developed an Interim General Practice Estates Strategy for south Warwickshire. The process of developing the Interim Strategy included a baseline review of the general practice estate within south Warwickshire, in line with the following methodology:
Stocktake – to establish baseline data (including functional suitability, condition and utilisation) for the existing estate. Member GP Practices were fully engaged in this process.
Current Capacity Analysis – utilising the data gathered at the stocktake stage, to establish the current capacity of the existing estate for delivery of General Medical Services (GMS) in line with the methodology outlined in Health Building Note 11-01: Facilities for Primary and Community Care Services.
Demand Projection – taking account of both the Warwick and Stratford-on-Avon District Council Local Plan housing trajectories and assumptions around natural demographic growth, to produce future demand projections at both individual practice and locality levels.
Future (2030) Capacity Analysis – by comparing future demand projections at locality level versus current capacity, to identify ‘hotspot’ areas (i.e. priority localities where a capacity gap will emerge over time) and to define the future capacity requirement for GMS delivery at both individual practice and locality levels.
The conclusion of the above work established a number of important headline messages, which continue to underpin the CCG’s approach to estates planning:
As to be expected from an estate of mixed age and type (ranging from purpose built primary medical care facilities to converted former residential buildings), the review produced variable results in relation to condition, compliance and functionality, with space standards issues identified at some practices and variable utilisation rates evidenced between practices. It should be noted that no premises have been identified as non-compliant by the Care Quality Commission via its programme of inspections.
Analysis of current capacity demonstrated capacity broadly meeting demand. However, as noted above, there was variation in utilisation rates between practices and it was recognised that those practices operating at a high utilisation rate, particularly those located in areas already being impacted by housing growth, would start to experience issues meeting demand in the shorter term.
The population growth arising across the CCG geography in the period to 2030 as a result of the housing delivery projected within the District Council Local Plans will generate significant increased demand on general practice services. The Warwick and Stratford-on-Avon District Council Local Plans set a combined housing requirement of circa. 31,000 dwellings in the period to 2030. In combination with other factors (most notably the strategic direction of travel, reinforced in the NHS LTP, towards the fundamental redesign and reimagining of out of hospital care), the projected population growth will have the impact of increasing the number of patient interactions being delivered in general practice premises. To create sufficient capacity to accommodate this increase, additional built space will be required.
While the current estate in some localities is sufficient to meet future demand, in other localities demand will outstrip capacity in the absence of development work being undertaken; be that via improvements to existing premises or the development of new premises.
The breadth of the work being undertaken by the CCG in relation to estates incorporates targeted work in individual prioritised localities to develop options appraisal studies, input to projects that have secured support from the CCG’s Primary Care Committee via the submission of business cases, engagement with Member GP Practices at both individual practice and locality level to support the development of potential estates schemes and on-going engagement with the two District Councils.

Operational Plan 2019/20 FINAL
Page 15 of 70
During 2019/20 the CCG will continue to focus on the above areas, alongside undertaking a refresh of the demand and capacity analysis on the seven new GP Network footprints. The outputs of this analysis will be shared with the Networks who are expected to play an increasing role in driving estates planning, working with SWFT.
Digital Innovation The Coventry and Warwickshire Digital Transformation Board (‘DTB’) is leading the implementation of the Coventry and Warwickshire Interim Digital Health Strategy which identifies five priority areas for the system:
Information and Communication Technology Fundamentals – focusing on standardisation, interoperability and connectivity amongst the IT estate, and reducing the digital maturity variation.
Patient and Public Facing Services – focusing on empowerment and availability of tools that meet health and care service requirements.
Partners/Organisational Interaction – focusing on enhanced electronic record sharing, and a move towards a seamless integrated health and social care system.
Workforce and Flexible Working Development – focusing on providing staff with the right tools at the right time to enable efficient and effective service delivery.
Management Information and Data – focusing on implementing a robust data quality strategy, generating evidence-based insights, and supporting the transformation of data into intelligence.
The CCG will continue to be an active member and support the work of the DTB in 2019/20. All BHBCBV partner organisations have published their digital ambitions via strategies or plans at organisation level, and there is a degree of commonality between them around sharing and making better use of data, information and insights, improving the digital experience, operational efficiency, productivity, continuous improvement, innovation, creating transparency between organisations and empowering patients and service users. The anchor for the CCG’s work in this area is our General Practice Information and Communication Technology (‘GPICT’) Strategy. The CCG’s vision, as set out in the GPICT Strategy, is: ‘To have a robust, resilient, accessible, secure and high performing GP ICT infrastructure that provides the platform to enable and deliver the transformation of general practice; to deliver integrated person centred care; to support new ways of working and put general practice in the best possible position to seize upon future opportunities.’ During 2018/19 the GPICT Strategy has delivered against many of its priorities, with significant funding from the national Estates and Technology Transformation Fund being deployed in support. Programmes and projects being implemented under the strategy are broadly divided into three categories: infrastructure, tools and support. In relation to infrastructure, building on the legacy position of all 33 Member GP Practices being on EMIS Web and the replacement of N3 lines with HSCN lines installed on a 100 Mbps bearer (which provide the option of increasing speed at very low cost over time), has created a solid platform for future strategic change (e.g. vertical integration, horizontal integration and implementing different models of working). At the same time, the CCG has sought to support our Member GP Practices to maximise efficiency and reduce the burden of bureaucracy by deploying specific solutions (including dual screens, a digital dictation solution and a document management solution) and offering all practices the opportunity to access support from a ‘digital angel’. Throughout 2019/20 the GPICT Strategy will continue to drive the CCG’s work in this area. The CCG has developed a GPICT plan on a page which charts the progress made to date in relation to the delivery of the Strategy and sets out our priorities for 2019/20. The delivery of the plan will be overseen by a Local GPICT Group, which engages both GP and Practice Manager representation. The Group will maintain strong links with the DTB to ensure that innovation and developments happening in general practice are aligned to and support the broader system direction travel.

Operational Plan 2019/20 FINAL
Page 16 of 70
SECTION 4: Our Plan
4a. Assurance
Every year the CCG holds an Annual General Meeting. The meeting offers an opportunity for us to look back on the previous financial year; to celebrate achievements and successes but equally to reflect on areas where work is required to improve our performance and/or to deliver expected standards. To date we have been a high performing organisation – something that we are determined to maintain through the period of this Operational Plan. We are accountable to the people of south Warwickshire, as well as to NHS England, for planning and ensuring the delivery of high quality care that meets the needs of our population. As a CCG we hold ourselves to account through the governance structure described in our Constitution. To help our population and stakeholders understand how we are performing, we communicate and engage with them regularly (as described in Section 4f). There are also a range of objective measures that we are assessed against.
NHS Constitution Rights and Pledges The NHS Constitution sets out rights to which patients, public and staff are entitled, and pledges which the NHS is committed to achieve. These translate into a set of indicators designed to provide assurance that the CCG is delivering quality outcomes for patients, as well as to provide a basis for assessing that we are continuously improving. We report our performance against these indicators to our Governing Body in public. NHS England has announced that during 2019-20 a national review of clinical standards will be completed, with the aim of ensuring that the standards and targets underpinning the delivery of NHS care prioritise what is most important to patients and their families, support the goals of the NHS LTP and are fit for the future. On completion of the review, the CCG will implement the new standards across contracts.
CCG Improvement and Assessment Framework The NHS England CCG Improvement and Assessment Framework draws together NHS Constitution and other core performance and finance indicators, outcome goals and transformational challenges in a single framework, which is used by NHS England to assess how effectively the CCG works with others (including the Warwickshire Health and Wellbeing Board) to improve quality and outcomes for patients. The Framework includes 58 indicators structured around four domains:
Assurance Component
Better Health: this domain looks at how the CCG is contributing towards improving the health and wellbeing of its population, and bending the demand curve.
Better Care: this domain principally focuses on care redesign, performance of NHS Constitution standards, and outcomes, including in important clinical areas.
Sustainability: this domain looks at how the CCG is remaining in financial balance, and is securing good value for patients and the public from the money it spends.
Leadership: this domain assesses the quality of the CCG’s leadership, the quality of its plans, how the CCG works with its partners, and the governance arrangements that the CCG has in place to ensure it acts with probity, for example in managing conflicts of interest.
The Framework provides the basis for the annual Assurance Review between the CCG and NHS England. The CCG reports its performance in this Review within its Annual Report. The result is also made available by NHS England via their website: https://www.england.nhs.uk/commissioning/regulation/ccg-assess/iaf/.
4b. Performance
As we have highlighted in Section 4a, the CCG has a duty to act in a way that promotes the NHS Constitution. To this end, the CCG ensures that delivery of the NHS Constitution rights and pledges is

Operational Plan 2019/20 FINAL
Page 17 of 70
included within all relevant Provider contracts and these are monitored and performance managed through well-established contract management processes. The CCG’s performance against NHS Constitution indicators continues to be strong; where performance issues have been identified in 2018/19, the CCG has worked closely with the relevant Providers and has agreed remedial actions plans and associated recovery trajectories. Section 5 confirms that CCG plans have been developed to ensure delivery of all NHS Constitution targets in 2019/20. Throughout 2019/20, the Delivering Today cornerstone of our strategy will continue to focus the CCG on robust management of the delivery of local and national performance standards and targets across all Provider contracts.
Development of 2019/20 Contracts Activity Assumptions Working with other BHBCBV partner organisations, the CCG has pursued a co-ordinated approach to planning for 2019/20 – this has involved each CCG working with the main Acute Provider within its Place/s to align activity assumptions and plans. In south Warwickshire, activity plans have been developed using the likely outturn position for 2018/19 and adjusted to account for both demographic and non-demographic growth. Non-demographic growth takes into account year-on-year linear assumptions, combined with a non-recurrent element of additional activity required to meet predicted 2019/20 demand levels and enable the delivery of NHS Constitution targets. Demand prediction modelling considers the current maturity, and accounts for the expected impact of, local and system projects and programmes aimed at demand management. The essential approach within south Warwickshire has been to develop plans based on realistic levels of activity with appropriate phasing – so, for example, the 2019/20 plan includes phasing to ensure that elective activity is front loaded into the first half of the year in order to allow winter pressures to be fully managed across the system by the CCG’s main Providers. Capacity Planning Working with SWFT, the CCG has ensured that capacity and workforce arrangements are appropriate to meet activity assumptions and to maximise achievement of NHS Constitution targets. This will be continuously monitored via the contract governance structure throughout the year. To support this during 2019/20 the CCG will contribute to the development of a system-wide capacity planning tool. This application will provide detailed insight into the use of clinical resources, service structure and unwarranted variation that disrupts patient care.
4c. Quality
The CCG has a clear governance process for monitoring the delivery of continuous improvement in the quality and safety of the services that we commission through our Performance and Clinical Quality and Governance Committees, and onwards to the Governing Body and the Members’ Council. The CCG’s Systematic Approach to Quality is our well-established quality oversight and improvement framework and sets out the approach that we take in pursuit of our goal of improving the quality of care for the population of south Warwickshire. Our approach acknowledges that getting the basics right in terms of robust data collation, analysis and reporting is fundamental to achieving our core aim to ‘improve patient safety, patient experience and clinical outcomes through a systematic approach to quality improvement across primary, secondary and community services’. The CCG’s approach has, at its heart, the collection and triangulation of robust and timely quantitative and qualitative data. Regular standard format reports, including the Integrated Quality and Safety report and the Primary Medical Care Performance and Quality report, convert the data into meaningful information and include recommended actions to address any areas of concern. The reports are presented to the Clinical Quality and Governance Committee, which determines priority areas for action and approves action plans. The impact of implementing identified actions is reviewed through subsequent reporting.

Operational Plan 2019/20 FINAL
Page 18 of 70
During 2019/20 we are committed to working with the other Coventry and Warwickshire CCGs to progress the development of a system-wide approach to continuous quality improvement and quality assurance to support the transition to an ICS. This work will include:
Working with health and care partners to develop a System and Place-based model and transition plan to support continuous quality improvement and assurance.
Identification and agreement of system quality priorities.
Development of a system quality dashboard and Quality Assurance Framework (‘QAF’). The use of a system wide QAF will demonstrate to external stakeholders including NHS England, NHS Improvement, Providers, patients and the wider public, the approach being taken to fulfil the CCG’s statutory duties with regard to quality.
4d. Equality
The Warwickshire Health and Wellbeing Board is a forum for councillors, commissioners (including CCGs) and communities to work together with other partners to improve the health and wellbeing of our local population and reduce health inequalities. The Health and Wellbeing Board is the local leader on tackling health inequalities. Among its key responsibilities is the production of the local JSNA. By drawing on both ‘hard’ data (i.e. statistics) and ‘soft’ data (i.e. the views of local people and professionals), the JSNA highlights Warwickshire’s priority groups in relation to health and social care need. The JSNA aims to establish a shared, evidence-based consensus on the key local priorities across health and social care and was used to develop both the Warwickshire Health and Wellbeing Strategy and the CCG’s own strategy. The CCG has been able to demonstrate how our strategy aligns with the priorities of the JSNA and the Health and Wellbeing Strategy and there is clear support for our strategy from the Health and Wellbeing Board.
“South Warwickshire CCG makes a significant contribution to the working of the Health and Wellbeing
Board and strategy delivery. In the last 12-18 months, the CCG has made important contributions within the on-going process of developing new place-based Joint Strategic Needs Assessments (JSNAs) for Warwickshire. Initially via participation in the working group responsible for making recommendations in relation to shaping the place geographies and subsequently via the JSNA Strategic Group, which is providing oversight of the delivery of the new JSNAs. The CCG has made a clear commitment to using the evidence base that is generated to inform the future design, commissioning and delivery of services at the local level, and has already shared the first wave assessments with the emerging local GP networks in order to drive their planning.” Councillor Izzi Seccombe. Leader of Warwickshire County Council.
During 2018/19 and 2019/20, new place-based JSNAs are being rolled out. The first of the new JSNAs (for the South Leamington, Bishops Tachbrook & Whitnash and Alcester, Henley, Studley & Bidford JSNA places) were completed and published in February 2019. These highlighted key priorities for each area and uncovered local inequalities which would have been masked by looking at the needs of south Warwickshire residents as a whole or if priorities were set based solely on population age structures. For example, the Alcester, Henley, Studley and Bidford area has an older age-profile than Warwickshire as a whole but a key priority emerging from the JSNA process was children and young people’s mental health, with some local areas having particularly high rates of hospital admissions related to self-harm among 10 to 24 year olds. The South Leamington, Whitnash and Bishops Tachbrook JSNA identified local geographies with higher than average rates of emergency hospital admissions for diabetes and circulatory disease, highlighting opportunities for increasing prevention activities and for improving the management of the conditions in the community. The place-based JSNAs will fundamentally shape and guide the work of the Strategic Commissioner in the coming years and be a key resource for the GP Networks.

Operational Plan 2019/20 FINAL
Page 19 of 70
Working relationships between the CCG and Warwickshire County Council are close and continue to be formally recognised through the following mechanisms:
The Director of Public Health and the Strategic Director of the People Group are members of the CCG Governing Body;
The Director of Public Health presents the JSNA and the Health and Wellbeing Board Annual Report to the Governing Body and the Members’ Council;
The Chair of the CCG is a member of the Health and Wellbeing Board;
The Chief Officer of the CCG is a member of two Health and Wellbeing Board sub-committees (the Executive Board and the Commissioning Board);
The Head of Planning and Policy is a member of the JSNA Strategic Group;
The Associate Director of Public Health is a joint appointment between the CCG and Warwickshire County Council.
The CCG has in place an Equality, Diversity and Human Rights policy which is publically available on its website together with:
The CCG’s Equality and Diversity Objectives for 2016-2020;
The NHS Equality Delivery System (‘EDS2’) report for 2018 published in March 2019; and
Our commitment to the Workforce Race Equality Standard (WRES). Together these documents demonstrate how the CCG complies with the Public Sector Equality Duty and that we work in ways which ensure equality and inclusion are embedded in all of our functions and activities. Tackling inequalities is one of our key priorities as a CCG and we are committed to ensuring that equality and inclusion is a priority when planning and commissioning local healthcare. To help us do this, we engage with local communities (as described Section 4f) to understand their needs and how best to commission the most appropriate services to meet those needs. Our Annual Reports provides specific examples of initiatives focused on reducing health inequalities. All of the CCG’s commissioning decisions are subject to thorough equalities analysis. The CCG further demonstrates evidence of ‘due regard’ by embedding equality consideration in the decision making processes of the Governing Body and its Committees.
4e. Finance
Financial Plan for 2019/20 In 2019/20 the CCG has an overall commissioning budget of £403.6m to spend on healthcare for the population of south Warwickshire. The CCG is expected to deliver a £1.9m in-year surplus in 2019/20. The CCG’s medium term (5 year) financial plan also assumes an in-year surplus in 2020/21 and 2021/22 to bring the cumulative surplus to 1% (in line with NHS England business rules). The CCG’s financial plan for 2019/20 assumes delivery of the financial targets and business rules required by NHS England, including increased investment in mental health services (in line with the Mental Health Investment Standard) and investment in primary care. Overall delivery of the 2019/20 plan is predicated on the delivery of a QIPP Programme of £17.2m (this figure may be subject to change pending the outcome of contract negotiations). This efficiency target represents 4.3% of the CCG’s anticipated funding in 2019/20. Contract offers have been made to Providers in line with the national timetable. These offers are built up from agreed activity levels, costed for the 2019/20 published National Tariff prices, adjusted for the impact of the QIPP Programme.

Operational Plan 2019/20 FINAL
Page 20 of 70
CCG Management/Running Costs In 2019/20 the total administrative/management costs of undertaking commissioning activities are planned to be £5.5m. This equates to 1.4% of the total cost of commissioned healthcare services. During 2019/20 the CCG will be planning for and taking actions to achieve the required 20% real terms reduction against its 2017/18 running cost allocation by 2020/21. The CCG is working jointly with the other Coventry and Warwickshire CCGs to align work programmes and provide efficiencies to achieve this target.
Healthcare Expenditure Planned healthcare expenditure for 2019/20, net of savings/efficiencies, contingencies/reserves and running costs, is £392.4m. The split of this expenditure across the various healthcare services is set out below:
Quality, Innovation, Productivity and Prevention Programme for 2019/20 The CCG’s QIPP Operational Pipeline Policy describes how the CCG operationalises its QIPP Programme, from initial generation of ideas, through to implementation and then on to business as usual. During 2019/20 the Financial Delivery Board (chaired by the CCG’s Chief Officer) will maintain oversight of QIPP delivery. Board meetings will consider the progress of QIPP schemes at different stages of delivery taking action as required to ensure that the schemes remain on track. As outlined in Section 1, the CCG and SWFT will agree and take joint ownership of a Value Programme for south Warwickshire via the establishment of a Joint Value Board, with a reporting line into the relevant Committee/Board of each organisation. This is in alignment with the agreed design principles for Place which include establishing ‘mechanisms to facilitate joint ownership of demand and cost’. The Place level Value Programme will triangulate a broad range of available benchmarking information (including NHS RightCare) to set priorities. The CCG will also support and contribute to the work of the Finance Workstream of the BHBCBV Programme which will ultimately deliver a system-wide Financial Strategy for Coventry and Warwickshire.
4f. Engagement
The CCG’s core value set confirms our commitment to putting patients, carers and the wider public at the heart of everything that we do and to understanding what matters the most to them. Communication and
Operational Plan 2019/20 FINAL
Page 21 of 70
engagement will remain priorities for us in 2019/20. Our Communications and Engagement Strategy is based on the principle of open and continuous communication with patients, the public, our Member GP Practices, staff and key stakeholders. It acknowledges our statutory responsibilities and the NHS commitment to involving patients in the way in which health services are planned and managed. The CCG is committed to putting people first and will continue to strive to improve communication and increase participation and engagement with all in as many aspects of our work as possible. The Communications and Engagement Strategy describes an overarching set of ten principles which will continue to underpin the work that we do in 2019/20. It also articulates three specific key objectives:
Objective How will this be achieved?
1. To proactively engage with stakeholders and enable people to contribute to shaping future health services commissioned by the CCG.
Using a wide variety of methods and approaches;
Working with the CCG’s Public and Patient Participation and the Gateway Groups;
Actively engaging with minority community groups;
Actively promoting and recruiting Health Champions;
Working with key partners to share information;
Reporting feedback to public meetings of the CCG.
2. To develop a culture that promotes open communication and engagement with patients and the public.
Communicating the organisation’s priorities; Ensuring the organisation’s vision and values, statutory requirements and aspiration for public engagement are known by every member of staff;
Delivering proactive and reactive media relations;
Ensuring all project managers are aware of expectations regarding communication and engagement and are suitably trained to deliver them;
Project plans describe stakeholder engagement.
3. To ensure Member Practices and staff are informed, engaged and involved in the work of the CCG and participate in commissioning activities for the benefit of patients.
Providing opportunities for GPs to influence commissioning and the provision of services through Member Council meetings;
Promoting clinical involvement in commissioning;
Maintaining and developing the CCG website;
Developing feedback mechanisms for issues and concerns raised by GPs and other stakeholders;
Ensuring staff briefings are focused on key topics and there are opportunities for feedback.
Our engagement approaches target the whole population, including less often heard groups. We want local people to have genuine involvement in our decisions to transform and improve services and we recognise that it is only by having a conversation with and listening to people who use services that we will be able to succeed in delivering our vision of ‘better healthcare for everyone’. During 2019/20 we will remain focused on creating opportunities for patients, the public and our stakeholder partners to engage with us. We will continue to provide a range of opportunities for individual and collective engagement and we will ensure that our approaches are effective in both informing and

Operational Plan 2019/20 FINAL
Page 22 of 70
listening. In support of Place development, we expect to ramp up our engagement activities with our Member GP Practices as we work together to embed and develop the seven GP Networks. There are a number of methods and forums that we will continue to draw on to deliver engagement, which include:
Health Champions – members of the public can apply to be a Health Champion.
All GP Network Meetings – these meetings bring together representatives of each of the seven Networks.
GP Practice level Patient Participation/Reference Groups (‘PPGs’/’PRGs’);
CCG Public and Patient Participation Group (‘3PG’) – this group includes a member of each existing practice level PPG or PRG;
CCG Gateway Group – six representatives from the 3PG attend Gateway meetings where commissioning activity is discussed with CCG staff and representatives of our Member Practices;
Warwick District Faith Forum;
Warwickshire Third and Public Sector Partnership Group;
Social Media – social media, particularly Twitter, is an important platform for the promotion of both CCG activities and national initiatives such as #StayWellThisWinter;
GP Feedback System – our Member Practices can provide feedback on an ad-hoc basis via this portal;
The annual CCG 360º Stakeholder Survey.
In progressing individual projects and work programmes, the CCG maintains a robust approach to public involvement and engagement. One of the functions of our Gateway Group is to assure the CCG that projects have been reviewed from a public and patient communications and engagement perspective. A locally developed Engagement Assessment Tool is used to ensure a consistent approach. There will be occasions when engagement with patients, the public and stakeholders will suffice; however, there will also be circumstances where we will need to undertake a full consultation. The circumstances that will trigger a full consultation are not set out in statute or guidance. The CCG will use the test in section 244 of the NHS Act 2006 (together with the Local Authority (Public Health, Health and Wellbeing Boards and Health Scrutiny) Regulations 2013) to assess whether a requirement to consult is triggered. The CCG has a duty to inform both the local regional team for NHS England and the Health Overview and Scrutiny Committee before a consultation is launched. As appropriate, engagement activities will take an integrated approach. Planned Care and Maternity, Children and Young People Services are two areas where the CCG will work with the other Coventry and Warwickshire CCGs to develop and implement engagement plans during 2019/20.

Enc 10a
SECTION 5: Our Response to the NHS Planning Guidance for 2019/20
5a. CANCER
Priorities Key deliverables Baseline Position 2019/20 Actions/Milestones (steps to delivery)
Success Measure
Relationship to Other System Programmes
Action Owner
Maintain active participation in the Cancer Alliance.
Implement place elements of System wide plan to meet Cancer Alliance priorities.
System wide plan in place. Develop a local strategy and system wide plan with key stakeholders. Formal sign off by C&W Cancer Board STP and CCGs/providers
High level plan with agreed STP trajectories Continued monitoring of plan
Cancer Planned Care
Joint
Implement national timed pathway for oesophago-gastric cancer.
Establish baseline position across the STP Agree implementation plan to implement new pathway.
Pathway implemented by the end of 2019/20.
Cancer Planned Care
Provider
Support roll out of Rapid Diagnostic Centres.
Baseline position to be established Understand national/WMCA requirements & local implications and agree implementation.
1 RDC established in Alliance area.
Cancer Planned Care
Provider/CCG
As part of the Coventry and Warwickshire Cancer Board, continue to drive delivery of the National Cancer Strategy and recommendations from the cancer task force
Implementation of the Cancer Group’s identified work programmes which span: Prevention, screening and early diagnosis; Demand and capacity; and Living with and beyond cancer
System wide work programme in development
Participate in System wide Task and Finish Groups established to address national/WMCA requirements and to support delivery of local trajectories. Develop local place based plan to support delivery of system wide plan and implement place based actions identified.
Workstreams achieve planned objectives and milestones as evidenced via reporting to the Cancer Board.
Cancer Planned Care
Provider/CCG
Deliver eight NHS Constitution Standards for cancer waiting times.
Deliver 2 week wait from GP urgent referral to first consultant appointment standard.
Nov 18 performance 97.7% Maintain delivery of 2 week wait performance.
Delivery of 93% target for whole year at aggregate level.
Cancer Provider
Deliver 2 week wait breast symptomatic (where cancer not initially suspected) from GP urgent referral to
Nov 18 performance 95.9% Maintain delivery of 2 week wait performance.
Delivery of 93% target for whole year at aggregate level.
Cancer Provider
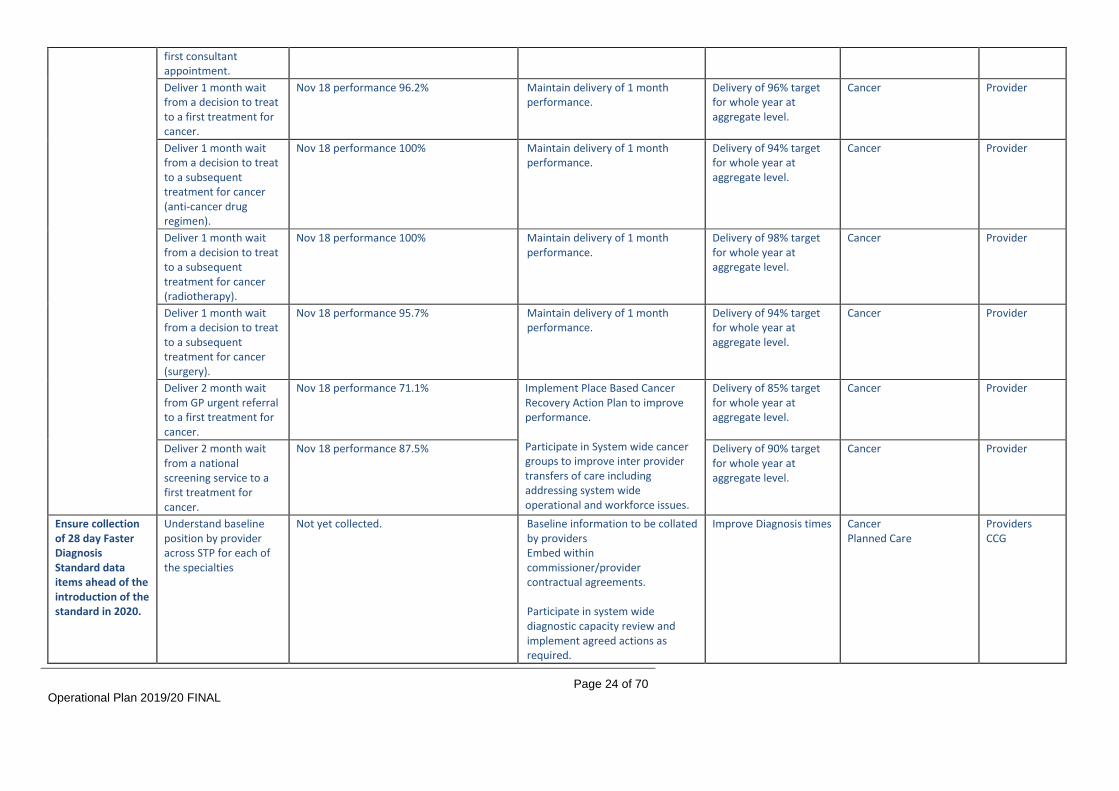
Operational Plan 2019/20 FINAL
Page 24 of 70
first consultant appointment.
Deliver 1 month wait from a decision to treat to a first treatment for cancer.
Nov 18 performance 96.2% Maintain delivery of 1 month performance.
Delivery of 96% target for whole year at aggregate level.
Cancer Provider
Deliver 1 month wait from a decision to treat to a subsequent treatment for cancer (anti-cancer drug regimen).
Nov 18 performance 100% Maintain delivery of 1 month performance.
Delivery of 94% target for whole year at aggregate level.
Cancer Provider
Deliver 1 month wait from a decision to treat to a subsequent treatment for cancer (radiotherapy).
Nov 18 performance 100% Maintain delivery of 1 month performance.
Delivery of 98% target for whole year at aggregate level.
Cancer Provider
Deliver 1 month wait from a decision to treat to a subsequent treatment for cancer (surgery).
Nov 18 performance 95.7% Maintain delivery of 1 month performance.
Delivery of 94% target for whole year at aggregate level.
Cancer Provider
Deliver 2 month wait from GP urgent referral to a first treatment for cancer.
Nov 18 performance 71.1% Implement Place Based Cancer Recovery Action Plan to improve performance. Participate in System wide cancer groups to improve inter provider transfers of care including addressing system wide operational and workforce issues.
Delivery of 85% target for whole year at aggregate level.
Cancer Provider
Deliver 2 month wait from a national screening service to a first treatment for cancer.
Nov 18 performance 87.5% Delivery of 90% target for whole year at aggregate level.
Cancer Provider
Ensure collection of 28 day Faster Diagnosis Standard data items ahead of the introduction of the standard in 2020.
Understand baseline position by provider across STP for each of the specialties
Not yet collected. Baseline information to be collated by providers Embed within commissioner/provider contractual agreements. Participate in system wide diagnostic capacity review and implement agreed actions as required.
Improve Diagnosis times Cancer Planned Care
Providers CCG
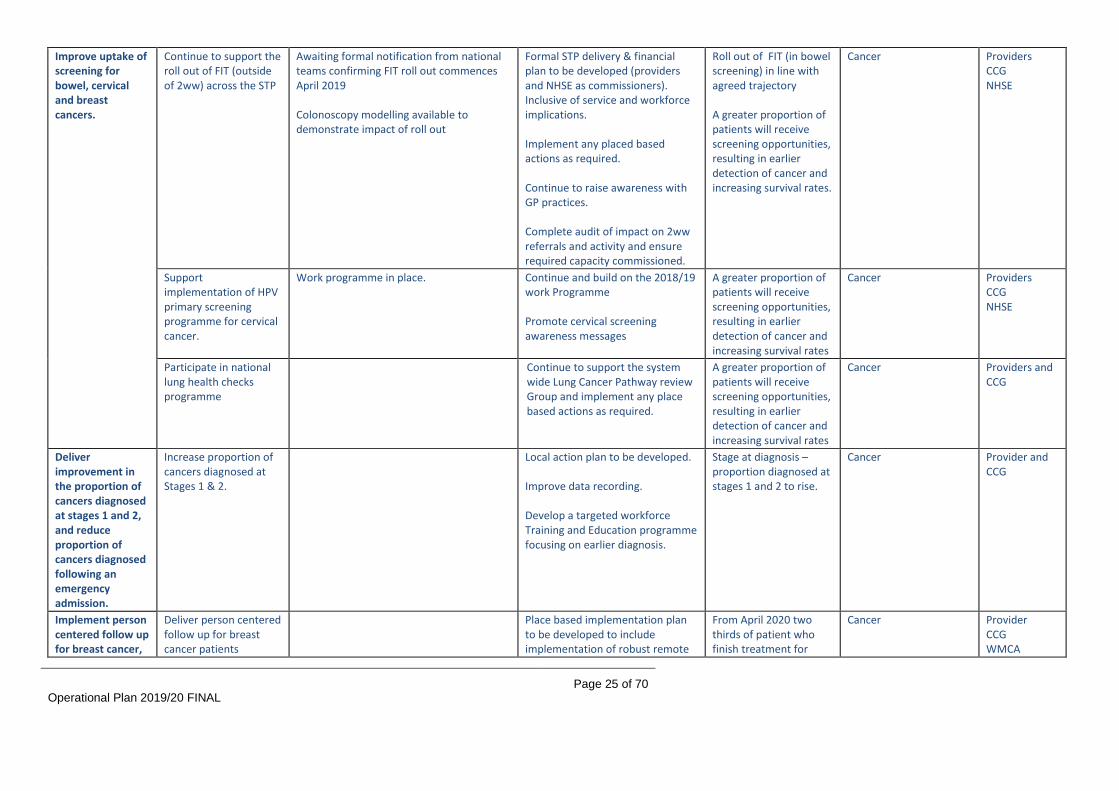
Operational Plan 2019/20 FINAL
Page 25 of 70
Improve uptake of screening for bowel, cervical and breast cancers.
Continue to support the roll out of FIT (outside of 2ww) across the STP
Awaiting formal notification from national teams confirming FIT roll out commences April 2019 Colonoscopy modelling available to demonstrate impact of roll out
Formal STP delivery & financial plan to be developed (providers and NHSE as commissioners). Inclusive of service and workforce implications. Implement any placed based actions as required. Continue to raise awareness with GP practices. Complete audit of impact on 2ww referrals and activity and ensure required capacity commissioned.
Roll out of FIT (in bowel screening) in line with agreed trajectory A greater proportion of patients will receive screening opportunities, resulting in earlier detection of cancer and increasing survival rates.
Cancer Providers CCG NHSE
Support implementation of HPV primary screening programme for cervical cancer.
Work programme in place. Continue and build on the 2018/19 work Programme Promote cervical screening awareness messages
A greater proportion of patients will receive screening opportunities, resulting in earlier detection of cancer and increasing survival rates
Cancer Providers CCG NHSE
Participate in national lung health checks programme
Continue to support the system wide Lung Cancer Pathway review Group and implement any place based actions as required.
A greater proportion of patients will receive screening opportunities, resulting in earlier detection of cancer and increasing survival rates
Cancer Providers and CCG
Deliver improvement in the proportion of cancers diagnosed at stages 1 and 2, and reduce proportion of cancers diagnosed following an emergency admission.
Increase proportion of cancers diagnosed at Stages 1 & 2.
Local action plan to be developed. Improve data recording. Develop a targeted workforce Training and Education programme focusing on earlier diagnosis.
Stage at diagnosis – proportion diagnosed at stages 1 and 2 to rise.
Cancer Provider and CCG
Implement person centered follow up for breast cancer,
Deliver person centered follow up for breast cancer patients
Place based implementation plan to be developed to include implementation of robust remote
From April 2020 two thirds of patient who finish treatment for
Cancer Provider CCG WMCA

Operational Plan 2019/20 FINAL
Page 26 of 70
and prepare for subsequent stratification of follow up approaches for prostate and colorectal cancer.
including systems for remote monitoring.
monitoring system with clear process for re-entry in each Trust Implement revised follow-up pathways
breast cancer are on a supported self-management follow up pathway.
Develop person centered follow up protocols for prostate and colorectal cancer patients including systems for remote monitoring.
Work in collaboration with WMCA to develop protocols. Place based implementation plan to be developed to include implementation of robust remote monitoring system with clear process for re-entry in each Trust. Implement revised follow-up pathways by Q4 2019/20.
Clinically agreed protocols and remote monitoring systems in place by the end of 2019/20.
Cancer Provider CCG WMCA
Ensure all elements of the Recovery Package (RP) are in place.
Ensure all elements of the recovery package are commissioned namely:
Timely Holistic Needs Assessments and Care Plans at Trust level
Electronic Treatment Summaries required across Trusts and Primary Care
Health and Wellbeing Support required across STP footprint
Cancer Care Reviews (holistic) in primary care
Baseline undertaken. Considerable variation across the STP and many elements are not currently in place.
Place based implementation plan to be developed and implemented. Deliver primary care nurse training. Complete patient engagement event to understand cancer patient experiences whilst LWBC Collaborate with Digital Transformation Board to scope the IT requirements for the LWBC programme.
Every person with cancer has access to the elements of the Recovery Package by 2020.
Cancer Digital Transformation
Provider/CCG/LA
5b. MATERNITY Priorities Key deliverables Baseline Position 2019/20 Actions/Milestones
(steps to delivery) Success Measure
Relationship to Other System Programmes
Action Owner
Continue to work Implement an enhanced Pilot projects for Continuity of Carer (CoC) The LMS Quality & Safety By March 2020, 35%+ of Provider

Operational Plan 2019/20 FINAL
Page 27 of 70
with Commissioner and Provider partners from across the system to deliver the recommendations in the National Maternity Review 'Better Births' and the West Midlands Neonatal Review through the implementation of the Coventry and Warwickshire Local Maternity System Transformation Plan.
and targeted continuity of carer model to help improve outcomes for the most vulnerable mothers and babies. Ensure that continuity of carer is provided to groups that experience the poorest outcomes, such as women from ethnic minorities and the most deprived socio-economic groups.
are underway at each provider trust within the LMS. Pilot project estimate achieving 20% of women booked onto a CoC pathway by March 2019. Current trajectory Baseline 2015 = 0 March 2019 = 2,219 – 20% of births March 2020 = 3,884 - 35% of births (Long Term Plan) The long term plan requires 75% of the most vulnerable women to experience CoC by March 2024 . In order to meet this we will focus the work of the emerging Maternity Voices Partnership to engage with these communities to inform the Quality and Safety workstream enabling the workstream to develop clear plans to roll out CoC .
workstream with support from the PMO confirm a plan to deliver continuity at scale to meet the confirmed trajectory of 35% by March 2020 Trajectories will be developed during 2019/20
women experience a continuity of carer pathway.
Make progress against trajectory to deliver improvements in safety towards the 2020 ambition to reduce stillbirths, neonatal deaths, maternal death and brain injuries by 20% and by 50% in 2025.
StillBirths Baseline 2015 = 5.2 per 1,000 Trajectory: March 2019 = 5/1,000 March 2020 = 4.1/1,000 March 2021 = 3.9/1,000 Intrapartum Brain Injury 2015 = 5/1,000 March 2019 = 5/1,000 March 2020 = 4/1,000 March 2021 = 4/1,000
The Quality & Safety and Health & Wellbeing workstreams across the LMS both contain plans that support the reduction in deaths. These include: - Agreeing & adopting
uniformed care pathways across the LMS
- Developing a parent education programme
- Increasing the support offered to women to stop smoking
- Implement v2 of the Saving Babies Lives Care Bundle.
- Increasing the rate of CoC - Improving access to perinatal
mental health services
- Uniform Care Pathways adopted across the LMS
- Implementation of V2 of the Saving Babies Lives Care Bundle.
- Increase the number of pregnant women who stop smoking during pregnancy.
Provider
Deliver full implementation of the Saving Babies’ Lives Care Bundle (v2) by 31 March 2020.
All recommendations within V1 of the Saving Babies’ Lives Care Bundle are met. Performance is measured across the LMS and reported to the LMS Board.
The Quality & Safety workstream have a task and finished group focussed on Safety. This group will develop and implement plans to meet the additional
Full implementation of the Saving Babies’ Lives Care Bundle (v2) at each provider unit.
Provider

Operational Plan 2019/20 FINAL
Page 28 of 70
recommendations found in V2 of the Saving Babies Lives Care Bundle across the LMS.
Continue against trajectory to deliver improvements in choice and personalisation so that by March 2021 all women have a personalised care plan.
Current trajectory* Baseline 2015 = 0 March 2019 = 2,433 March 2020 = 4,485 March 2021 = 11,213
During review in 2018/19 the Choice & Personalisation workstream have identified that the current use of the Perinatal Institute Antenatal Record at UHCW and GEH and the electronic Badgernet system at SWFT both contain a personalised care plan. Therefore performance is already at 100%. However in the spirit of continuous improvement and in line with meeting the digital aim for maternity care, the LMS will be focussing on delivering a uniformed electronic care record that offers an online portal for women to access and personalise their own care record, this is currently available at SWFT through the Badgernet system. GEH are finalising a business case to implement a maternity EPR within 2019/20. UHCW is in the process of confirming their trusts approach to a trustwide EPR, and the LMS will revisit the pace needed to deliver a an electronic Maternity Record, and ensure that all three records interface and meet the same capability standards.
Roll out of a uniformed or at least an interfaced Maternity Electronic Patient Record.
Provider / CCG
Continue against trajectory to deliver improvements in choice and personalisation so that by March 2021
Current trajectory* Baseline 2015 = 590 March 2019 = 800 March 2020 = 1000 March 20221 = 2450
In July 2018 SWFT opened their Co-Located Midwifery Led Birth Unit (MLU) Bluebell. This is the second MLU in the LMS with UHCW already supporting women in the
Increase birth rate in low risk settings to achieve agreed trajectory.

Operational Plan 2019/20 FINAL
Page 29 of 70
more women can give birth in midwifery settings.
Lucina MLU. There are currently no further plans to develop additional birth settings. Focus is now on agreeing uniform care pathways and safely increasing the number of women supported to birth in the MLU or at home.
Offer all women who smoke during their pregnancy, specialist smoking cessation support.
Baseline 2018 =
* No electronic referral system currently available in Coventry.
KPI's
UHC
W
SWF
T GEH
CO at Booking >95%
100
%
>75
%
CO at 36/40 >70%
100
%
>75
%
Smokers
referred to
SSiPS *
100
%
>75
%
The Health & Well-being workstream have a dedicated Smoking Cessation task and finish group delving improvements in the care pathway. Currently the ambition is to secure E-referrals for Coventry so that all trusts can electronically refer to Specialist Smoking cessation services. The health and Well-being workstream has a task and finish group focused on smoking cessation that will work up action plans to increase each trusts performance in the indicator CO testing at 36 weeks gestation.
Achievement of the following targets: * CO at booking recorded, greater that 95% at all Trusts * Smokers referred to SSIPS 90% for all Trusts. Implementation of a uniformed Smoking cessation care pathway and guideline.
Provider/CCG
Continue to work with Commissioner partners from across the system through the Maternity and Children's Strategic Commissioning Programme Board to progress the Coventry and Warwickshire Maternity, Children and
To develop an Outcomes Framework for Maternity and Paediatric Services
There are no agreed set of outcomes for the maternity and paediatrics across the system. There is significant variation in health outcomes and therefore an opportunity to reduce health inequalities by focusing on a common set of outcomes.
During Qtr 4 of 2018/19 and Qtr 1 staff engagement will be undertaken Final Outcomes Framework finalised at the end of Q1
Approved Outcomes Framework
Maternity Transformation Group
Commissioners
To design a delivery model for maternity and paediatrics across Coventry and Warwickshire that delivers a clinical and financially sustainable service that improves the outcomes for women, babies and
The current services are not effectively meeting the needs of the population as evidenced by lower than expected outcomes on key measures and variability across the system. Providers have workforce challenges that cannot be resolved without a significant redesign of the delivery model. Phase One has been completed by
Qtr 4 2018/19 Provider Alliance will undertake a Current Service Analysis to provide a baseline position. Qtr 1-3 Following the launch of Phase Two the Provider Alliance will undertake a process to develop a delivery model that delivers the commissioners outcomes within a
New delivery model ready to implement in Qtr 2 2020/21
Maternity Transformation Group
Providers

Operational Plan 2019/20 FINAL
Page 30 of 70
Young People Transformation Programme.
children. Commissioners who have undertaken public and patient engagement to determine desirable criteria and the first draft of the outcomes Framework.
financial envelope. Providers will undertake public and patient engagement as part of the design process. Qtr 3 Commissioners will assess the delivery model and subject to satisfactory response will commission the model.
5c. MENTAL HEALTH Priorities Key deliverables Baseline Position 2019/20 Actions/Milestones
(steps to delivery) Success Measure
Relationship to Other System Programmes
Action Owner
Deliver in full the local plan which responds to the Five Year Forward View for Mental Health and Implementing the Mental Health Forward View.
Additional baseline funding deployed in support of delivery of identified priorities.
Funding agreed to support MHFYFV priorities; the funding is recurrent so will support delivery into 2019/20:
EIP
IAPT
Perinatal
CAMHS 3.5
Discussions and action plans agreed with local MH provider. Periodic monitoring
Implementation of plans/ trajectories achieved.
N/A CCG
Continue to focus on expanding access to Improving Access to Psychological Therapies (IAPT) services for adults and older adults with common mental health problems, with a focus on those with long-term conditions (LTC).
IAPT service in place for individuals aged 16+years, delivering evidence based treatment pathways, which meets current KPIs. The service is exploring how access can be increased for a wide range of patient cohorts such as BME; older adults; new parents and patients with LTCs. Transformational funding was secured in 2017/18 to develop IAPT-LTC pathways, with agreement from CCGs to fund on a recurrent basis. An evaluation plan is being developed between the CCGs and CWPT to demonstrate the impact of the LTC expansion in relation to health outcomes, financial savings and impact on healthcare utilisation
Develop a system wide plan with trajectories to track and monitor increases in:
Meeting the access rate and maintaining the recovery rate;
Expansion in LTC pathways and treatment;
Co-location of therapists;
Uptake of trainee courses for PWPs, HITs and LTC trainees.
IAPT services providing timely access to treatment for at least 22% of those who could benefit (people with anxiety disorders and depression) by March 2020, (increasing to 25%by 2020/21) with two thirds of the increase in access anticipated to be delivered within the IAPT for LTC service. At least 75% of people referred to the IAPT programme begin treatment within six weeks of referral.
Establish an IAPT steering group. Reporting by exception to the MH STP Primary care workstream and/or MH STP Board.
STP

Operational Plan 2019/20 FINAL
Page 31 of 70
At least 95% of people referred to the IAPT programme begin treatment within 18 weeks of referral. At least 50% of people who complete IAPT treatment recover.
Expand capacity for people experiencing a first episode of psychosis.
EIP service is in place for individuals aged 14 – 65years. The service has pathways in place for ARMS (At Risk MH State) and over 35years. Additional investment has been approved in 2018/19 to recurrently fund an additional 8 WTE Care Coordinators.
Develop a system wide plan with trajectories to explore how to:
Increase referrals from individuals experiencing first episode of Psychosis;
Reduce duration of untreated psychosis.
Increase length of treatment to align with national average of 36 months
At least 56% of people aged 14-65 experiencing their first episode of psychosis start treatment within two weeks. Ensure the 2018/19 commitment for NICE concordance for EIP is met; then deliver against the further ambition for 50% of services to be graded at level 3 by the end of 2019/20.
Development of an EIP steering group. Reporting by exception to the MH STP Specialists care work stream and/or MH STP Board.
STP
Increase access to high-quality mental health services for children and young people (CYP).
Current position (Q2): SWCCG: 18.8% Projected year end position: SWCCG: 32.3%
Monitor the following areas through the collaborative, C&W-wide CAMHS operational group.
Refresh the referral to treatment pathway;
Undertake further system capacity and demand modelling and generate proposals to best manage the system pressures;
Continue with collaborative waiting list management arrangements;
Continue to increase the scale of available multi-agency early help opportunities in schools and in the
At least 32% of children and young people with a diagnosable mental health condition receive treatment from an NHS-funded community mental health service.
N/A STP

Operational Plan 2019/20 FINAL
Page 32 of 70
community;
Ongoing development of the digital offer;
Remodelled multi-agency “targeted” support with strengthened partnership working with PMHT and which is closely aligned to Warwickshire Health & Wellbeing Hubs;
Continued development of the Warwickshire Rise Community Partnerships to increase access to a range of information, training, advice and support, from a range of agencies;
Implement a refreshed framework for Mental Health Interventions for School-aged Children (MHISC)
Community eating disorder teams for children and young people meet access and waiting time standards.
Latest 2018/19 position as follows:
Routine
Q1 Routine
Q2 Routine
Q3
SWCCG 100% 100% 78.75%
STP 90% 100% 88.75%
Urgent
Q1 Urgent
Q2 Urgent
Q3
SWCCG 100% 100% N/A
STP 100% 100% N/A
Monthly monitoring of contract KPI.
By March 2021, at least 95% of children and young people with an eating disorder are seen within one week of an urgent referral. By March 2021, at least 95% of children and young people with an eating disorder are seen within four weeks of a routine referral.
N/A STP
Continue to focus on working with Warwickshire County Council and other system partners to progress the implementation of the 2016-2020
2015-17 Local Authority figures show that there were 245 deaths by suicide across Coventry and Warwickshire. NB. there is variation between ONS and NCISH figures, STP are checking this with NCISH.
Work with providers to ensure that plans are in place for a zero-suicide ambition for mental health inpatients. A driver diagram has been created; 10 change ideas are currently in progress across the
At least 10% reduction in suicides by 2020/21.
Emergency and crisis care/acute work streams
STP

Operational Plan 2019/20 FINAL
Page 33 of 70
Warwickshire Suicide Prevention Strategy.
system with further ideas currently being developed for 19/20.
Continued reduction in out of area placements for acute mental health care for adults, in line with agreed trajectories.
Reporting and monitoring arrangements established.
CCG actions for 2019/20:
Continued CQUIN for out of area co-ordinator;
Director-level oversight. CWPT key areas of focus for 2019/20 (supporting action plan with more detail available):
Improve patient flow;
Ensure timely discharge;
Improve patient experience;
Digital technology to support management and oversight in real time (Cambio).
Joint actions:
Joint reviews of all OAPs;
Joint task and finish group to maintain system grip;
Engagement with NHSI collaborative on OAPs;
Fortnightly face to face meeting to review inpatient capacity, flow and in turn the out of area placements.
To eliminate all inappropriate Out of Area Placements (OAPs) by December 2021 through a series of service improvements.
Acute/crisis care work streams
STP
Continued reduction in out of area placements for acute mental health care for CYP, in line with agreed trajectories.
Coventry and Warwickshire identified as having high numbers of tier 4 bed usage. Extension made to Acute Liaison Team as precursor to Home Treatment Team
Establishing operational Crisis Home Treatment Team.
Reduction in T4 occupied bed days in Coventry and Warwickshire
New service to link with NHSE New Care Models for regional T4 commissioning approach
CCG
Continue to focus on support for adults and older adults with severe mental illnesses (SMI).
People with a SMI receive a full annual physical health check.
Across the STP, 17.5% of people with a SMI currently receive a full annual physical health check
Complete evaluation of delivery options.
At least 60% people with SMI receive a full annual physical health check.
Primary Care CCG
Undertake preparatory work for the
This activity currently forms part of the block contract.
Strengthen local relationships between primary care, secondary
Effective redesign and reorganisation of core
Primary Care STP

Operational Plan 2019/20 FINAL
Page 34 of 70
mobilisation of a new integrated primary and community model (as per the Long Term Plan).
care, local authorities and VCS services. Develop understanding of local need through information and data. Clear KPIs to be developed for this cohort in order for a baseline to be established.
community mental health teams that enable us to move towards a new place-based, multidisciplinary service across health and social care, aligned with primary care networks.
Increase access to Individual Placement and Support (IPS) services in line with STP trajectory.
IPS service in place delivered by Rethink. The service is integrated within CWPT and receives many referrals from IPUs and Crisis Team alongside the Job shop.
Current provision in place until March 2020. Continued monitoring and development of the service to ensure is delivering to targets. A commitment from the CCGs that the wave of IPS funding for STPs to be applied for.
Targets for Warwickshire as follows: 300 to commence service; 90 into employment; 30 into training and education.
Community capacity/resilience STP work stream
STP
Develop plan to establish baselines and track access to psychological therapies for people with SMI.
Liaise with the C&W IAPT service to explore how access to psychological therapies can be increased for people with SMI
Baseline current access to psychological therapies for patients with SMI. Plan joint actions to increase access for SMI patients. Review any training implications.
An increase in the uptake of psychological therapies for patients with SMI. Outcome measures. Recovery rates.
Establish an IAPT steering group. Reporting by exception to the MH STP Primary care workstream and/or MH STP Board.
Develop plan to establish baselines and track access to psychological therapies for people with SMI.
Dementia diagnosis, care and support.
Diagnosis rates across STP at December 2018: SWCCG 59.4%
Continue to implement detailed Dementia Diagnosis Action Plan across STP area.
At least two thirds (66.7%) of people with dementia, aged 65 and over, receive a formal diagnosis.
Out of hospital transformation programme taking on responsibility for post-diagnostic support from April 2019.
CCG Diagnosis rates at December 2018: SWCCG 59.4%
Review and recommission post-diagnostic support offer to ensure those diagnosed and their families and carers receive the necessary
Range of post diagnostic support services including: - MAS Community Team; - Dementia Navigators; - Admiral Nurses (CRCCG); - Dementia Cafes; - Dementia Portal.
Review of current provision March 2019. Agree public and stakeholder engagement plan with WCC and CCC April 2019.
Improve post diagnostic care in line with published guidance and quality standards (NICE NG97 and QS30 and QS1)
(see above) Aligned recommissioning across CCG and Local Authorities (WCC and CCC)
CCG

Operational Plan 2019/20 FINAL
Page 35 of 70
support to live well with dementia
Dementia Action Alliances in place across the STP with work to build on and increase to number of Dementia Friends Contracts aligned in 2018 to enable comprehensive review and recommissioning activity in 2019/20.
Recommissioning plan June 2019. Develop and implement improved training for carers August 2019.
Monitor using service level data from commissioned services, including waiting times, service outcomes for clients and carer wellbeing; NHS Rightcare figures of deaths of people with dementia by usual place of residence, rate of emergency admissions aged 65+ with dementia, etc.
Dementia also forms part of the End of Life Work Programme.
Increase access to high-quality perinatal mental health services.
The Perinatal MH service supports women who are pregnant, or in the postnatal year, who are experiencing serious perinatal mental health difficulties. Through Wave 2 funding the team are expanding capacity and capability to reach more women.
Consider opportunities to use additional baseline investment through roles such as:
Team administration;
Paid peer support workers;
Clinical Pharmacists
Parent-infant or Family Therapists.
Increase access for at least 4.5% of population birth rate.
Increase access to evidence-based care for women with moderate to severe perinatal mental health difficulties and a personality disorder diagnosis
Extend services to preconception to 24 months after birth, in line with the cross-government ambition for women and children focusing on the first 1,001 critical days of child’s life.
Expand access to evidence-based psychological therapies to also include parent-infant, couple, co-parenting and family interventions.
Implement maternity outreach clinics.
Ensure partners of women accessing specialist perinatal mental health services receive evidence-based assessment of their mental
A Perinatal MH steering group is in place. Reporting by exception to the MH STP Specialists care work stream and/or MH STP Board.
N/A STP
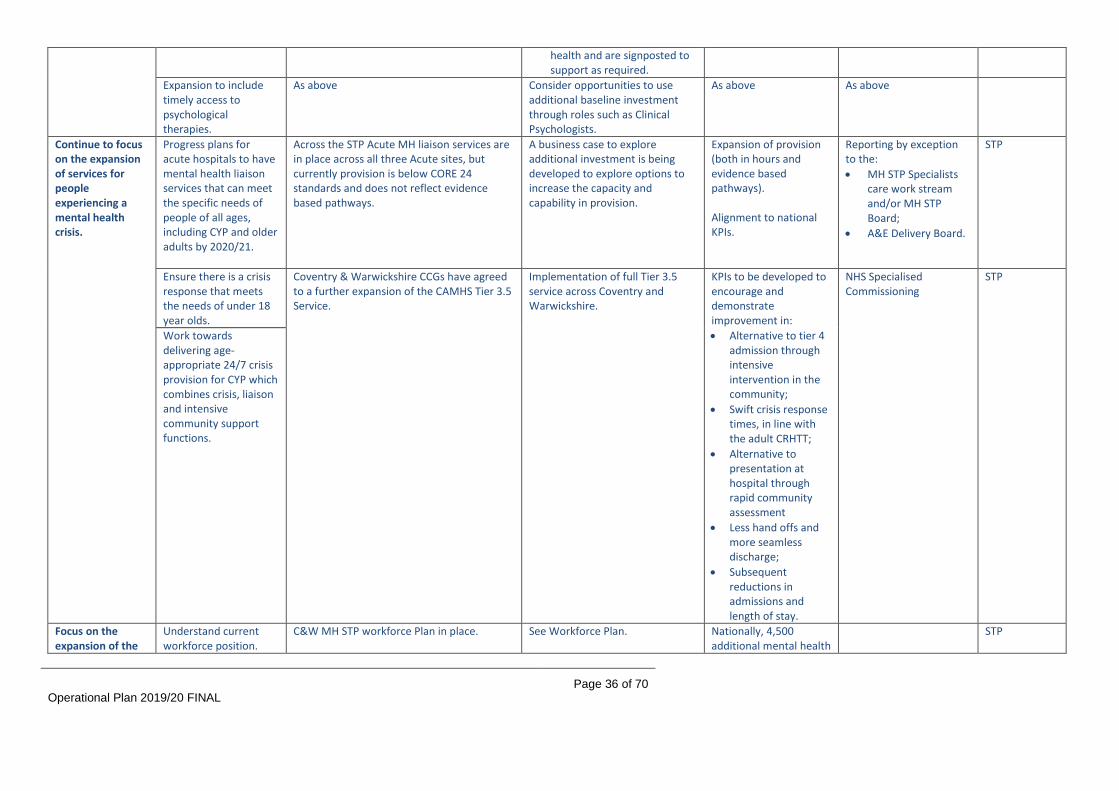
Operational Plan 2019/20 FINAL
Page 36 of 70
health and are signposted to support as required.
Expansion to include timely access to psychological therapies.
As above Consider opportunities to use additional baseline investment through roles such as Clinical Psychologists.
As above As above
Continue to focus on the expansion of services for people experiencing a mental health crisis.
Progress plans for acute hospitals to have mental health liaison services that can meet the specific needs of people of all ages, including CYP and older adults by 2020/21.
Across the STP Acute MH liaison services are in place across all three Acute sites, but currently provision is below CORE 24 standards and does not reflect evidence based pathways.
A business case to explore additional investment is being developed to explore options to increase the capacity and capability in provision.
Expansion of provision (both in hours and evidence based pathways). Alignment to national KPIs.
Reporting by exception to the:
MH STP Specialists care work stream and/or MH STP Board;
A&E Delivery Board.
STP
Ensure there is a crisis response that meets the needs of under 18 year olds.
Coventry & Warwickshire CCGs have agreed to a further expansion of the CAMHS Tier 3.5 Service.
Implementation of full Tier 3.5 service across Coventry and Warwickshire.
KPIs to be developed to encourage and demonstrate improvement in:
Alternative to tier 4 admission through intensive intervention in the community;
Swift crisis response times, in line with the adult CRHTT;
Alternative to presentation at hospital through rapid community assessment
Less hand offs and more seamless discharge;
Subsequent reductions in admissions and length of stay.
NHS Specialised Commissioning
STP
Work towards delivering age-appropriate 24/7 crisis provision for CYP which combines crisis, liaison and intensive community support functions.
Focus on the expansion of the
Understand current workforce position.
C&W MH STP workforce Plan in place.
See Workforce Plan.
Nationally, 4,500 additional mental health
STP

Operational Plan 2019/20 FINAL
Page 37 of 70
mental health workforce, including through the implementation of training and retention schemes.
Understand required expansion numbers. Provider level expansion plan/s in place. Understand key local pressure points for service areas or staff groups, and identify mitigation. Expansion and enabling of training schemes. Expansion and enabling of retention schemes.
Commissioner intentions reflect investment and continued scrutiny in key areas such as perinatal, IAPT, CYP, etc.
therapists recruited and trained by 2020/21. Increased number of mental health therapists co-located in primary care by 2020/21 to support increase in access to be delivered through IAPT-Long Term Conditions services. Capacity and capability of CYP workforce expanded.
Ensure Providers submit comprehensive data to the Mental Health Services Dataset (MHSDS)/Improving Access to Psychological Therapies (IAPT) dataset.
Routine monitoring of data sets, with outputs used to inform Commissioner to Provider discussions.
CWPT submits the MHSDS and the IAPT dataset national dataset on a monthly basis in line with their statutory requirements.
Continue to monitor submissions in line with current contract systems and processes.
N/A STP/CSU
Ensure operational plans reflect understanding of local health inequalities.
MHSDS/IAPT datasets available. Contracting teams will work with BI to understand how MHSDS can be used to understand health inequalities and how the data can be utilised in informing commissioning decisions.
N/A STP/CSU
Mid-year review undertaken with Providers.
There is no mid- year review undertaken currently with CWPT to review the MHSDS/ IAPT.
Contracting teams will await and implement any guidance from NHSE in relation to a requirement to undertake a mid-year review with providers. IAPT and MHSHS submissions are monitored monthly as a matter of routine and this will continue.
N/A STP/CSU
Contract penalties applied as appropriate i.e. where data reporting or quality standards are not being met.
Financial sanctions for 2018/19 linked to reporting via MHSDS. Development of new sanctions for 2019/20 in line with new NHS contract requirements for IAPT and Data Quality Maturity Index.
Continued monitoring and implementation of penalties where appropriate, issuing of quarterly financial sanctions. Continuation of DQIP for EIP data. Implementation of a DQIP for the Data Quality Maturity Index, as per the 2019/20 NHS standard contract.
N/A STP/CSU

Operational Plan 2019/20 FINAL
Page 38 of 70
Deliver Mental Health Digital Strategy, which addresses digital record sharing and the integration of digital tools and digitally-enabled therapies.
Board level sign off achieved.
No joint digital strategy for MH currently in existence.
Develop a joint digital strategy covering the integration of digital tools and digitally-enabled therapies. Implement new NHS contract guidance around e-referrals into MH services.
Board level sign off achieved. CWPT digital delivery group
STP
Increase baseline spend on mental health.
Meet Mental Health Investment Standard (MHIS).
Routine monitoring against plan in place. Monthly monitoring to assess achievement of MHIS.
NHSE mandated requirement to meet MHIS.
Any MH/LD related expenditure through OOH (IPU 18-21) will be included as part of calculation.
CCG
Undertake joint review of MHIS investment plan (review to engage identified lead mental health provider).
No current joint review planned. To be discussed with CWPT.
Plans on how to undertake review to be determined.
Joint review made. Review of all MH expenditure
CCG
5d. OUT OF HOSPITAL (PREVENTION, GENERAL PRACTICE SERVICES & COMMUNITY SERVICES) Priorities Key deliverables Baseline Position 2019/20
Actions/Milestones (steps to delivery)
Success Measure
Relationship to Other System Programmes
Action Owner
Continue working with our Member Practices to focus on the sustainability of general practice here and now, and how general practice in south Warwickshire will transform over time to remain sustainable for the future.
Primary Care Strategy incorporated as part of wider System Strategy.
The CCG’s Primary Care Strategy ‘Transforming General Practice Together’ was published in May 2017. The Strategy is built around the pillars of the General Practice Forward View and runs for 3 years. The Strategy was assured by NHS England in April 2017. Regular progress reporting is established to the CCG Primary Care Committee. Plans are being developed to deliver a new System Strategy and associated 5 year System Delivery Plan.
Identify resource to support System Strategy and System Delivery Plan development, including engagement. Establish System Strategy Development Group to design and have oversight of the delivery of the development process. Plan and deliver engagement activities.
System Strategy in place. 5 year System Delivery Plan in place in line with mandated national timetable (currently due Autumn 2019). In relation to the Primary Care strategy, the CCG continues to be able to demonstrate to Member Practices, other stakeholders and our population how practices have benefited from the opportunities flowing from the General Practice Forward View.
All Programmes
CCG

Operational Plan 2019/20 FINAL
Page 39 of 70
Effective use of £1.50 per head of population recurrent investment.
Total one off non-recurrent investment of £3 per head made across 2017/18 and 2018/19 (£1.50 per head in each year). Engagement commenced in relation to 2019/20 funding, including via the All GP Network meeting.
Review schemes associated with the investment in 2017/18 and 2018/19. By July 2019 determine how £1.50 investment will be used in 2019/20 aligned to the requirements of the new Network directed enhanced service (DES).
Recurrent investment until 31 March 2024. Associated schemes are aligned to the national Network DES. Evaluation of associated schemes identifies positive impact against General Practice Forward View objectives and local priorities.
CCG
Continue to focus on the development of the GP Networks (groupings of CCG Member Practices) established in 2018/19 as the foundation for future Out of Hospital service delivery models.
Maintain active support to GP Network development, including by supporting the implementation of the Network DES.
7 GP Networks established. Regular All GP Network meeting established and agreed schedule of meetings in place for 2019/20. Action plan in place for each Network. Place based Joint Strategic Needs Assessments being shared with Networks as they are produced. Work programme in place to deliver all JSNAs by 2020/21, being overseen by the JSNA Strategic Group with reporting to the Health and Wellbeing Board. GP Network Development Plan in development.
Continue to Chair and participate in the local All GP Network meeting, which brings together the Chairs/nominated representatives of each GP Network and CCG representatives. Continue to track the progress of the action plans that the GP Networks have set for themselves through the All GP Network meeting. Through the General Practice Investment Proposal process established in 2018/19, continue to consider requests from the GP Networks to provide resource support and/or other identified input to proposed projects which address priorities that they have identified at Network level.
100% population coverage of GP Networks. Clinical Director in place for each Network. Objectives and milestones within the GO Network Development Plan being met, as demonstrated though reporting. 6 Out of Hospital Place Based Teams in place, aligned to GP Networks. The CCG is able to demonstrate to Member Practices, other stakeholders and our population the benefits that the GP Networks have delivered.
Proactive and Preventative Care Productivity and Efficiency
CCG GP Networks

Operational Plan 2019/20 FINAL
Page 40 of 70
Continue to support the development of the relationship between the GP Networks and the Out of Hospital Place Based Teams. Continue to develop future system leaders from within general practice by expanding the local General Practice Leadership and Development Programme commenced in 2018/19. Work with the GP Networks to respond to the publication of the national network contract and any other new guidance on the future direction of Networks. Finalise GP Network Development Plan.
Provide GP Networks with data analytics for population segmentation and risk stratification to allow them to understand their populations’ needs, including for symptomatic and prevention programmes.
Place based Joint Strategic Needs Assessments being shared with Networks as they are produced. Work programme in place to deliver all JSNAs by 2020/21, being overseen by the JSNA Strategic Group with reporting to the Health and Wellbeing Board. The GP Federation (South Warwickshire GP) provides support to practices in relation to data analytics and has links into the CCG Business Intelligence Team.
Ensure every GP Networks has reviewed the place based JSNA relevant to their network area. Review GP Network action plans to verify that they address JSNA priorities. Continue to engage with the GP Federation to support data
GP Network action plans address priorities identified in the new place based JSNAs. Improved uptake and coverage of national screening and immunisation programmes at Network level.
Proactive and Preventative Care
CCG GP Networks
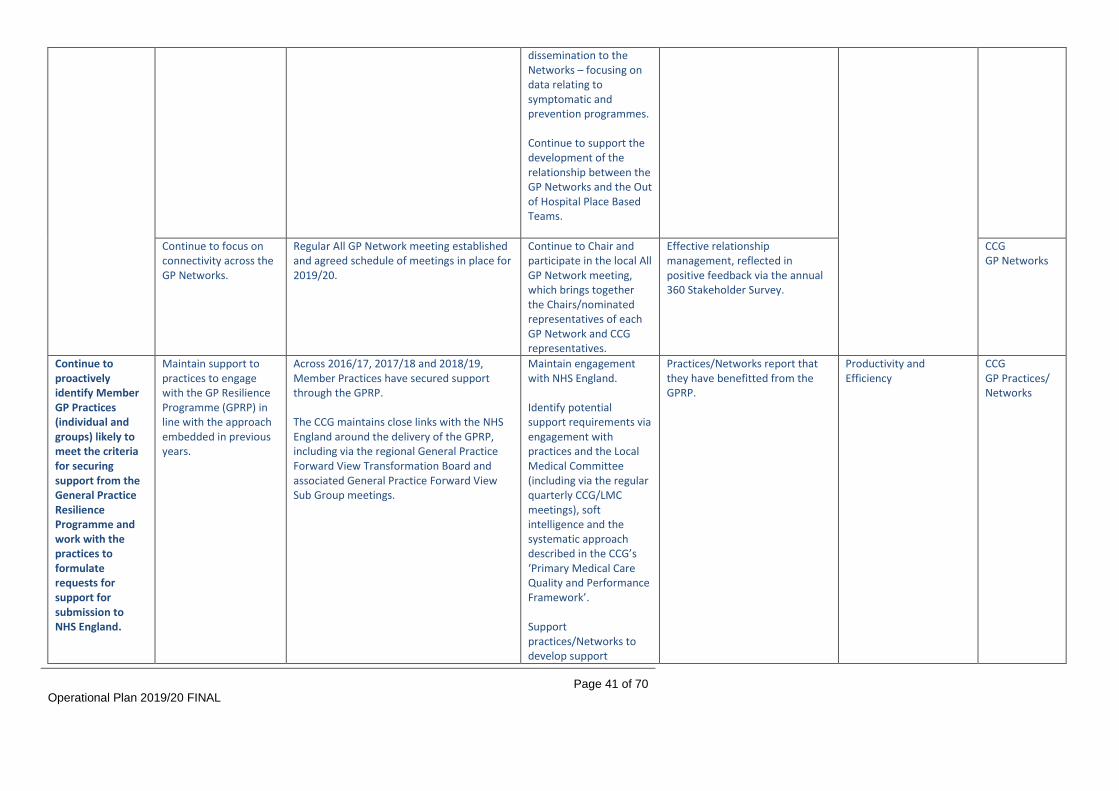
Operational Plan 2019/20 FINAL
Page 41 of 70
dissemination to the Networks – focusing on data relating to symptomatic and prevention programmes. Continue to support the development of the relationship between the GP Networks and the Out of Hospital Place Based Teams.
Continue to focus on connectivity across the GP Networks.
Regular All GP Network meeting established and agreed schedule of meetings in place for 2019/20.
Continue to Chair and participate in the local All GP Network meeting, which brings together the Chairs/nominated representatives of each GP Network and CCG representatives.
Effective relationship management, reflected in positive feedback via the annual 360 Stakeholder Survey.
CCG GP Networks
Continue to proactively identify Member GP Practices (individual and groups) likely to meet the criteria for securing support from the General Practice Resilience Programme and work with the practices to formulate requests for support for submission to NHS England.
Maintain support to practices to engage with the GP Resilience Programme (GPRP) in line with the approach embedded in previous years.
Across 2016/17, 2017/18 and 2018/19, Member Practices have secured support through the GPRP. The CCG maintains close links with the NHS England around the delivery of the GPRP, including via the regional General Practice Forward View Transformation Board and associated General Practice Forward View Sub Group meetings.
Maintain engagement with NHS England. Identify potential support requirements via engagement with practices and the Local Medical Committee (including via the regular quarterly CCG/LMC meetings), soft intelligence and the systematic approach described in the CCG’s ‘Primary Medical Care Quality and Performance Framework’. Support practices/Networks to develop support
Practices/Networks report that they have benefitted from the GPRP.
Productivity and Efficiency
CCG GP Practices/ Networks

Operational Plan 2019/20 FINAL
Page 42 of 70
requests.
Work in partnership with our Member Practices, the other Coventry and Warwickshire CCGs, South Warwickshire NHS Foundation Trust and the wider training and education system (including the Local Workforce Action Board, Health Education England and the local Training Hub) to implement the Coventry and Warwickshire Primary Care Workforce Strategy.
Continue to focus on GP and nurse retention, including by supporting eligible GPs to access the national GP Retention Scheme. Continue to support the delivery of the General Practice Nursing Ten Point Action Plan in partnership with the local Training Hubs and other stakeholder partners. Ensure all staff working in general practice have access to the support of a training hub. Develop and implement a learning and development programme for general practice. Continue to expand the range of professionals working within general practice teams.
Primary Care Workforce Strategy in place. The Strategy identifies four strategic objectives:
Stabilising current primary care workforce.
Putting in place the foundations for a more robust approach to workforce planning.
Investing in the development of the wider general practice workforce.
Supporting the continuing development of GP Networks.
Baseline workforce demand and supply data established, with regular reporting to NHS England against identified trajectories by role type. Delivery Plan in place, with regular reporting to NHS England established.
Continue to Chair and participate in the South Warwickshire Local Workforce Group. Maintain links with the Coventry and Warwickshire Local Workforce Action Board. Co-ordinate activities at a Coventry and Warwickshire level where applicable – for example, the deployment of relevant national funding e.g. Practice Manager Development funding. Seek to take maximum advantage of relevant funding opportunities as they become available. Work with our Member Practices to increase the number of staff working in new roles in general practice (clinical pharmacists, Advanced Clinical Practitioners, apprentices, etc.), including by participating in relevant national schemes. Work with the local Training Hub to deliver quality training for staff working in general
Key objectives and milestones within the Delivery Plan are delivered, as evidenced via reporting to NHS England.
Productivity and Efficiency
CCG GP Practices/ Networks

Operational Plan 2019/20 FINAL
Page 43 of 70
practice in south Warwickshire based on the Learning Needs Analysis completed in 2018/19. Enhance the skill set of the local general practice workforce in specific areas – including frailty, end of life and Mental Health, including dementia. Work with South Warwickshire NHS Foundation Trust to introduce ‘blended’ roles working across general practice and the Out Hospital Transformation Programme. Focus on recruitment and retention, including through the implementation of both national and bespoke local approaches (GP Mentors, #careforyourcareer campaign, etc.)

Operational Plan 2019/20 FINAL
Page 44 of 70
In line with the GPICT Strategy, make progress to deliver a robust, resilient, accessible, secure and high performing GP ICT infrastructure that provides the platform to enable and deliver the transformation of general practice locally; to deliver integrated person centred care; to support new ways of working and to put Member Practices in the best position to seize on future opportunities.
Implement online consultations across all GP practices. Implement pipeline of projects being funded via the national Estates and Technology Transformation Fund (ETTF). Ensure all Member GP Practices are able to provide all of the functionality offered through the NHS App.
GP ICT Strategy in place, built around 3 pillars: infrastructure, tools and support. Project Initiation Documents (PIDs) and delivery plans in place for ETTF projects, with regular reporting established to NHS England.
Maintain links with the Coventry and Warwickshire Digital Transformation Board. Deliver the key trajectories and milestones identified in the ETTF project plans.
Key trajectories and milestones identified in the ETTF project plans delivered, as evidenced via reporting to NHS England. Projects delivered within planned timescales as evidenced via reporting to NHS England regional team. 100% of population able to access NHS App by 31 July 2019.
Digital Transformation CCG GP Practices/ Networks
Continue to implement our Primary Care Estates Strategy.
New build schemes delivered. Improvement schemes delivered. Options appraisal process progressed in various localities.
Interim Primary Care Estates Strategy in place. Locality position statements submitted to Primary Care Committee in February 2019.
Provide input and support to progress relevant schemes (new development or improvement). Continue to engage with Warwick and Stratford-on- Avon District Councils to secure developer funding contributions as appropriate (either via Section 106 planning obligations or the Community Infrastructure Levy).
Demonstrable progress on the delivery of the Primary Care Estates Strategy as evidenced in reporting to the CCG’s Primary Care Committee and onwards to the Governing Body.
Estates CCG GP Practices/ Networks
Continue to Continue to manage Service went live on 3 September 2018. Maintain participation on Maintain 100% population Productivity and CCG

Operational Plan 2019/20 FINAL
Page 45 of 70
provide extended access to general practice services for 100% of the population.
the extended access contract awarded in 2018/19 against the agreed Service Development and Improvement Plan.
Service has been assured by NHS England via an assurance visit. 2 hubs established initially. 4 additional hubs rolled out during Q4 2018/19.
the Service Delivery Board. Business as usual contract management.
coverage of extended access. Maintain delivery of the seven core requirements for extended access identified by NHS England, as evidenced via NHS England assurance process
Efficiency
Provider
Working closely with South Warwickshire NHS Foundation Trust, fully complete and embed the redesign, implementation and transition to a new Out of Hospital model of care, aligned to the new model described in the NHS Long Term Plan.
An Integrated Single Point of Access (iSPA) for professionals, patients and carers which will achieve a streamlined referral process, ensure patient flow through the system is seamless and improve the management of the highest acuity patients.
To evaluate and continue to evolve the iSPA introduced in 2018/19 and to maximise opportunities for the iSPA to be integrated with other system partners including social care.
To continue to build and evolve the iSPA model, implementing a clinical triage system which supports delivery of a 2 hour rapid response in the community to avoid admission where appropriate. Establish Technology Plan to support vision to keep people in home e.g. direct booking/online assessment. Development of digital offer and telehealth opportunities. Build relationships and integration between general practice, community services and other key stakeholders to ensure the Out of Hospital model delivers improved case management and outcomes for its patient population, and supports the wider system objectives.
Out of Hospital model demonstrates improvement against agreed range of system wide metrics, and patient and stakeholder outcome measures.
Urgent and Emergency Care
Provider
Implementation of To continue and complete the roll out and Implementation of Out of Hospital model Out of Hospital Provider
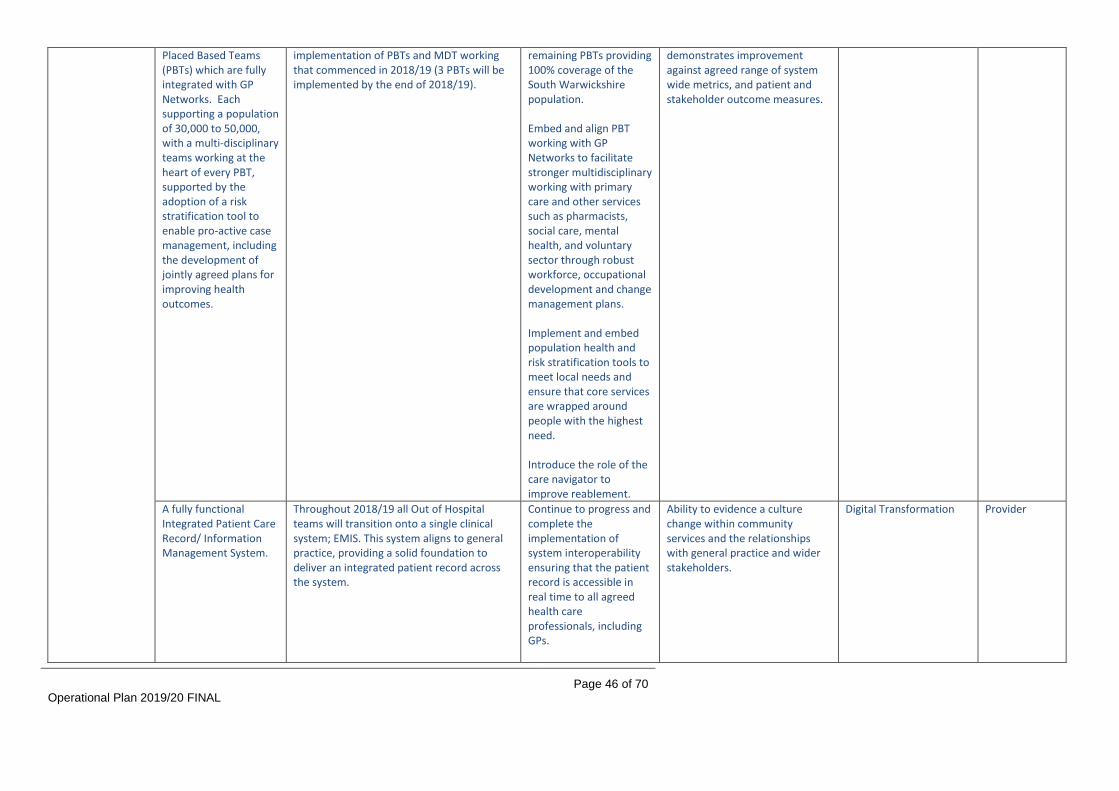
Operational Plan 2019/20 FINAL
Page 46 of 70
Placed Based Teams (PBTs) which are fully integrated with GP Networks. Each supporting a population of 30,000 to 50,000, with a multi-disciplinary teams working at the heart of every PBT, supported by the adoption of a risk stratification tool to enable pro-active case management, including the development of jointly agreed plans for improving health outcomes.
implementation of PBTs and MDT working that commenced in 2018/19 (3 PBTs will be implemented by the end of 2018/19).
remaining PBTs providing 100% coverage of the South Warwickshire population. Embed and align PBT working with GP Networks to facilitate stronger multidisciplinary working with primary care and other services such as pharmacists, social care, mental health, and voluntary sector through robust workforce, occupational development and change management plans. Implement and embed population health and risk stratification tools to meet local needs and ensure that core services are wrapped around people with the highest need. Introduce the role of the care navigator to improve reablement.
demonstrates improvement against agreed range of system wide metrics, and patient and stakeholder outcome measures.
A fully functional Integrated Patient Care Record/ Information Management System.
Throughout 2018/19 all Out of Hospital teams will transition onto a single clinical system; EMIS. This system aligns to general practice, providing a solid foundation to deliver an integrated patient record across the system.
Continue to progress and complete the implementation of system interoperability ensuring that the patient record is accessible in real time to all agreed health care professionals, including GPs.
Ability to evidence a culture change within community services and the relationships with general practice and wider stakeholders.
Digital Transformation Provider
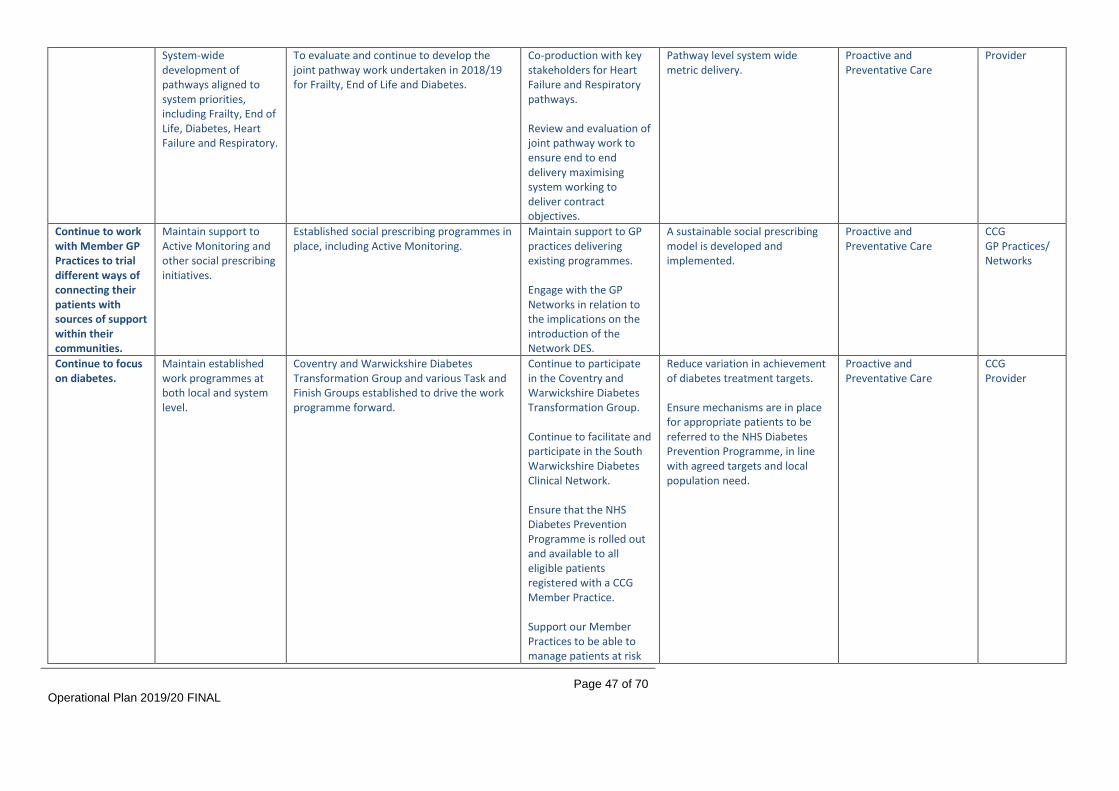
Operational Plan 2019/20 FINAL
Page 47 of 70
System-wide development of pathways aligned to system priorities, including Frailty, End of Life, Diabetes, Heart Failure and Respiratory.
To evaluate and continue to develop the joint pathway work undertaken in 2018/19 for Frailty, End of Life and Diabetes.
Co-production with key stakeholders for Heart Failure and Respiratory pathways. Review and evaluation of joint pathway work to ensure end to end delivery maximising system working to deliver contract objectives.
Pathway level system wide metric delivery.
Proactive and Preventative Care
Provider
Continue to work with Member GP Practices to trial different ways of connecting their patients with sources of support within their communities.
Maintain support to Active Monitoring and other social prescribing initiatives.
Established social prescribing programmes in place, including Active Monitoring.
Maintain support to GP practices delivering existing programmes. Engage with the GP Networks in relation to the implications on the introduction of the Network DES.
A sustainable social prescribing model is developed and implemented.
Proactive and Preventative Care
CCG GP Practices/ Networks
Continue to focus on diabetes.
Maintain established work programmes at both local and system level.
Coventry and Warwickshire Diabetes Transformation Group and various Task and Finish Groups established to drive the work programme forward.
Continue to participate in the Coventry and Warwickshire Diabetes Transformation Group. Continue to facilitate and participate in the South Warwickshire Diabetes Clinical Network. Ensure that the NHS Diabetes Prevention Programme is rolled out and available to all eligible patients registered with a CCG Member Practice. Support our Member Practices to be able to manage patients at risk
Reduce variation in achievement of diabetes treatment targets. Ensure mechanisms are in place for appropriate patients to be referred to the NHS Diabetes Prevention Programme, in line with agreed targets and local population need.
Proactive and Preventative Care
CCG Provider

Operational Plan 2019/20 FINAL
Page 48 of 70
of and living with diabetes in general practice, including by enabling professionals working in general practice to access education, training and relevant resources. Ensure that people at risk of and living with diabetes in south Warwickshire are able to access high quality education and self-care resources, including the Diabetes Education and Self-Management for Ongoing and Newly Diagnosed (DESMOND) education programme. Evaluate the outcomes associated with education and self-care interventions implemented locally. Focus on maintaining a 100% participation rate in relation to the National Diabetes Audit.
Continue to discharge relevant functions in line with the Delegation Agreement for full delegation of primary medical care services.
Continue to evidence performance of functions via reporting to the Primary Care Committee. Participate in internal audits.
Delegated commissioning arrangements in place since April 2015. Primary Care Committee and Primary Care Operations Group established and meeting regularly to conduct business within their respective terms of reference. First audit completed during Q4 2015/16, with a finding of “significant assurance”
Primary Care Committee to maintain oversight.
Compliance evidenced via reporting to the Primary Care Committee. Positive audit results achieved.
N/A CCG

Operational Plan 2019/20 FINAL
Page 49 of 70
reported in April 2016. Second audit ongoing and due to conclude March 2019.
Local investment, including deployment of funding associated with development offers within the General Practice Forward View.
Effective use of £1.50 per head of population recurrent investment.
See above. See above. See above. N/A CCG
Effective use of other funding flows (practice manager training, training for receptionists and clerical staff, etc.)
Care navigation and clinical correspondence programmes rolled out across practices to support efficiencies and new ways of working. Practice Manager Training Programme has been co-developed with the local Training Hub.
Maintain regular reporting to NHS England to provide assurance of delivery.
Every Member Practice has delivered at least 2 high impact actions by 31 March 2020. Practices are supported to optimise workflow. Increased competency of staff working in general practice.
5e. PERSONALISATION (LEARNING DISABILITIES AND AUTISM, PERSONAL HEALTH BUDGETS, CONTINUING HEALTHCARE) SOUTH WARWICKSHIRE Priorities Key deliverables Baseline Position 2019/20
Actions/Milestones
Success Measure
Relationship to Other System Programmes
Action Owner (CCG or Provider)
Continue transforming care for people with a learning disability, autistic spectrum condition or both by implementing ‘Transforming Care for People with Learning Disabilities’, the joint plan developed through the Arden Transforming Care Partnership.
Continue to reduce reliance on inpatient care (both CCG and NHS England funded).
Dynamic risk stratification process in place with clear function of identifying those at risk of admission Intensive support for adults with LD and ASD in place and recurrently funded Forensic support for adults in place and funded to 2020 Intensive support for children and young people with ASD in place and funded to 2020 CCG Inpatients as at 31/12/18 - 21 NHSE adult inpatients as at 31/12/18 - 20 CAMHS inpatients as at 31/12/18 - 12 SWCCG - 6
Evaluate intensive support service for children and young people and secure recurrent funding from April 2021 Evaluate forensic support service for adults and secure recurrent funding from April 2021 Implement new service specifications and review capacity of community learning disability services to ensure people are supported to live in the community
Achieve planned trajectory of 18.5 inpatients per million population for CCG commissioned inpatient services by March 2020. By March 2021, reduce adults in CCG commissioning inpatient services to 9 individuals across the TCP – each CCG will also have their own target to meet. Achieve planned trajectory of 18.5 inpatients per million population for NHSE commissioned inpatient services by March 2020. By March 2021, reduce adults in NHSE commissioned inpatient services to 12 individuals across the TCP – each CCG will also have
Mental Health and Emotional Well-being
CCG

Operational Plan 2019/20 FINAL
Page 50 of 70
Improve admission avoidance offer including exploring potential to develop bed based and in-reach emergency respite services Working collaboratively with social care, education and health providers, clarify key worker arrangements for children and young people with a learning disability, autism or both who are in mental health hospital or at risk of admission to mental health hospital, including defining roles and responsibilities in relation to care coordination and process for agreeing who the key worker is. Undertake review of readmissions for children and young people and implement recommendations Deliver Accelerator Programme, including evaluation of impact of ASD outreach service for children and young people and co-production of single planning framework for children and young
their own target to meet. Achieve planned trajectory for children and young people in Tier 4 inpatient services by March 2020. All Age Autism strategy is signed off and in place Functions of support outlined in Building the Right Support are recurrently funded.

Operational Plan 2019/20 FINAL
Page 51 of 70
people at risk of admission to hospital. Work with education to conduct a needs assessment for young people with ASD who are out of school or on limited timetable. Develop and deliver multi-agency response to needs assessment in order to prevent hospital admission. Develop pathway for children and young people with ASD who present with self-harming and self-injurious behaviour
Reduce length of stay for those who do require inpatient care.
12 point discharge plans in place for all inpatients Additional case management resource in place in all CCGs to progress discharge Average length of stay for children and young people in tier 4 is 8 months, 1 month longer than the regional average Average length of stay for adults in assessment and treatment is 6 months 17 adults have been in hospital for more than 5 years
Continue to promote use of 12 point discharge plans to progress discharges Improve care coordination for children and young people in CAMHS tier 4 inpatient settings by agreeing with health providers, social care and education and key worker roles and responsibilities and how key workers will be assigned. Review capacity of intensive support services to support young people stepping
Reduce length of stay for young people in CAMHS Tier 4 to be in line with regional average Reduce number of people in hospital with length of stay for over 5 years (for adults) and for over 1 year (for children)
Mental Health and Emotional Well-being
CCG

Operational Plan 2019/20 FINAL
Page 52 of 70
down from hospital Progress planned discharges for long stay adults Work collaboratively with West Midlands commissioners to develop pathways for people with autism, commission in patient services in least restrictive setting with reduced length of stay, and implement the respond pilot.
Improve the quality of inpatient care across the NHS and independent sector.
Pre-admission CETR compliance is below 90%. Advocacy organisation commissioned to deliver experts by experience hub to support delivery of CTR and CETR.
CCG to be represented at Care, Education and Treatment Reviews (CETRs) for children and young people who are inpatients Alongside Birmingham and Solihull CCG, implement new specification for assessment and treatment services. Strengthen process to proactively identify children and young people and adults who are subject to regular and or prolonged restrictive practices including the use of seclusion/long term segregation and ensure that appropriate
Care and Treatment Reviews (CTRs) carried out in line with policy both pre- and post-admission. Uptake of CETRs increased – 90% of under-18s admitted to hospital to have either a community CETR or a CETR post-admission. Demonstrable increase in compliance and quality of CETRs. Reduction in use of prolonged or regular restrictive practices
Mental Health and Emotional Well-being
CCG

Operational Plan 2019/20 FINAL
Page 53 of 70
safeguarding and review measures are followed. Ensure inpatient service specifications include requirement to reduce the use of restrictive practices. Ensure commissioned services are aware of and working towards national improvement standards for learning disability services.
Continue to focus on tackling the causes of morbidity and preventable deaths in people with a learning disability, autistic spectrum condition or both.
Improve uptake of annual health checks in general practice for people aged over 14 years with a learning disability
2017/18 figures: SWCCG = 52.8%
Specify requirements for Health Facilitation Resource to support delivery. Promote AHCs with client group, formal and informal carers. Support primary care in delivery of DES.
At least 75% of people on the learning disability register have had an annual health check.
Mental Health and Emotional Well-being
CCG
Increase identification of people who should be on the GP LD register and consequently benefitting from enhanced services.
2017/18 figures: SWCCG – 0.37% of GP registered population is on register National average (0.49%)
Awareness raising, including formal and informal carers. Support the workforce to identify those individuals eligible for the register. Specify contractual requirements for Health Facilitation Resource to support delivery.
Registered population on the GP LD register increases in line with the national ambition for the LD register to grow year on year.
Mental Health and Emotional Well-being
CCG
Continued learning and action from Learning Disabilities Mortality
Steering group established, chaired by the SWCCG Chief Nurse. Local area contact for each CCG attends.
Bi-monthly steering groups scheduled.
Annual report submitted to appropriate local Boards and Committees to demonstrate
Mental Health and Emotional Well-being
CCG

Operational Plan 2019/20 FINAL
Page 54 of 70
Reviews (LeDeRs). NHSE LeDeR trajectory developed and reported against. As at end 2018 40% of reviews complete. Administration support in place to assist in obtaining documentation for analysis. Themes, recommendations and best practice examples identified and reported to Steering Group.
Reviewer allocation system to continue with internal monthly monitoring by CCG. Scheduled updates provided to provider CQRMs and CCG governing body committees. Communication strategy to be developed to ensure that all learning outcomes, required actions and quality improvement requirements are shared with stakeholders.
action taken and outcomes from LeDeR reviews. Learning shared with stakeholders, recommended actions implemented.
Implement the National Disability Improvement Standards and apply to all NHS funded services over the next 5 years
CCG aware of requirements. Standards being built into service specifications as developed
Begin work to ensure that all commissioned service providers are aware of the standards. Require local providers to review current practice in line with the four improvement standards and to produce plans that outline how sustained quality improvement will be developed in line with the standards. Agree mechanisms for reporting progress towards delivering improvement standards for all providers Ensure that all contracts
Plans are established demonstrating baseline position against standards guidance. Improvement measures are outlined. Patient experience of NHS funded services is improved. Progress to be picked up within TCP assurance and monitoring processes
Mental Health and Emotional Well-being
CCG

Operational Plan 2019/20 FINAL
Page 55 of 70
with NHS providers include reference to the National Disability Improvement Standards and that progress monitoring is built in to quality assurance processes.
The whole NHS to improve its understanding of the needs of people with LD/ASD
Working group in place with CCG and CWPT representation to address reasonable adjustment requirements for children and adults with mental health and learning disabilities.
With CWPT, co-produce and deliver plan to improve reasonable adjustments in mental health services for children and adults with LD/ASD or both. Scope the potential to roll out reasonable adjustments programme to other NHS providers including primary care. Deliver Transforming Care workforce plan, including ASD training for providers and development of self-assessment tool for Autism Friendly Services With social care, education and health providers, clarify keyworker arrangements for people with LD, ASD or both who are in hospital or at risk of admission to hospital. Identify any gaps and develop plan to address gaps.
Plan in place and implemented Coventry and Warwickshire wide strategy developed encompassing range of activity for delivery
Mental Health and Emotional Well-being
CCG

Operational Plan 2019/20 FINAL
Page 56 of 70
Review and share appropriate training resources including e-learning packages. Co-produce Coventry and Warwickshire All Age Autism Strategy and ensure associated work-plan is owned by all partners.
Expand the STOMP-STAMP programmes to stop the overmedication of people with a learning disability, autism or both.
STOMP established within secondary care - active steering group and action plan for delivery established.
Develop all-age STOMP-STAMP plan for the STP to expand beyond secondary care. Increase local intelligence with regard to levels of use of psychotropic medicine amongst LD cohort, particularly those not supported by secondary care services. Work with primary care and medicines optimisation colleagues to develop and establish a programme for medication reviews and appropriate specialist pharmacy support. Consider inclusion in the primary care incentives scheme (quality component) for 2020/21. Ensure that STOMP-STAMP is embedded in
Use of psychotropic medication is reduced. Use of appropriate non-medical intervention increases, subsequently avoiding need for/use of medication. STOMP-STAMP embedded in quality assurance processes across health and social care.
Proactive and Preventative
CCG
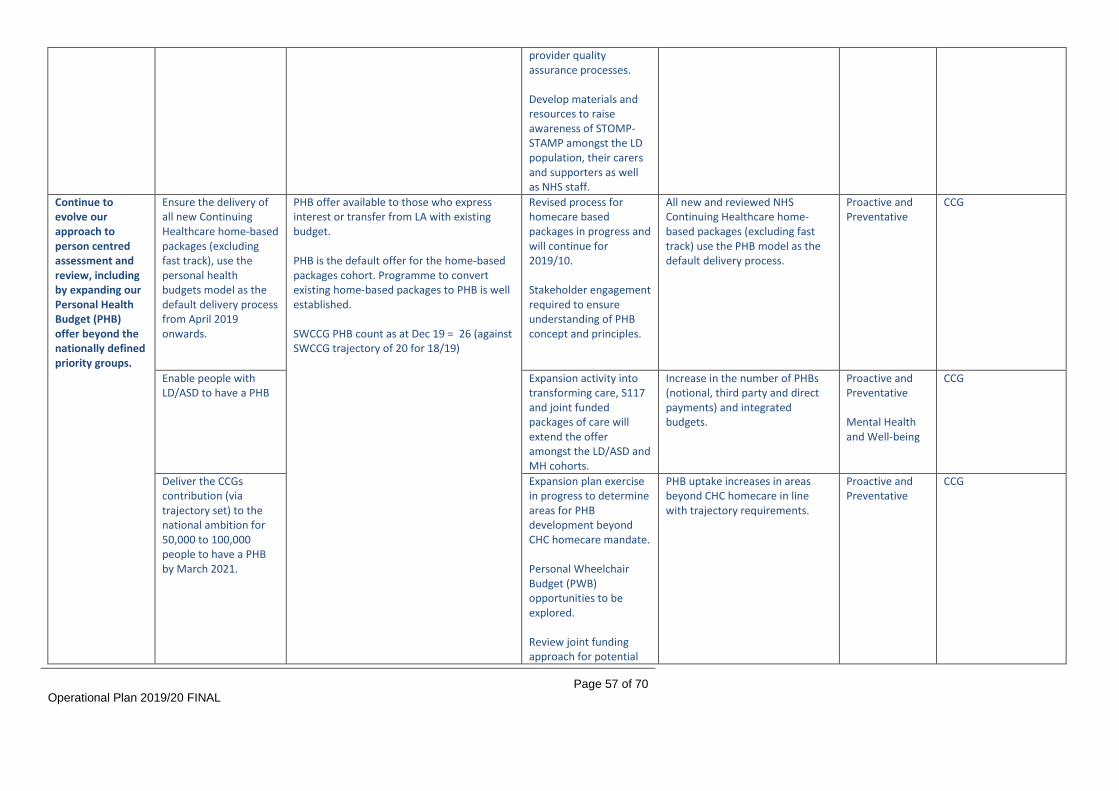
Operational Plan 2019/20 FINAL
Page 57 of 70
provider quality assurance processes. Develop materials and resources to raise awareness of STOMP-STAMP amongst the LD population, their carers and supporters as well as NHS staff.
Continue to evolve our approach to person centred assessment and review, including by expanding our Personal Health Budget (PHB) offer beyond the nationally defined priority groups.
Ensure the delivery of all new Continuing Healthcare home-based packages (excluding fast track), use the personal health budgets model as the default delivery process from April 2019 onwards.
PHB offer available to those who express interest or transfer from LA with existing budget. PHB is the default offer for the home-based packages cohort. Programme to convert existing home-based packages to PHB is well established. SWCCG PHB count as at Dec 19 = 26 (against SWCCG trajectory of 20 for 18/19)
Revised process for homecare based packages in progress and will continue for 2019/10. Stakeholder engagement required to ensure understanding of PHB concept and principles.
All new and reviewed NHS Continuing Healthcare home-based packages (excluding fast track) use the PHB model as the default delivery process.
Proactive and Preventative
CCG
Enable people with LD/ASD to have a PHB
Expansion activity into transforming care, S117 and joint funded packages of care will extend the offer amongst the LD/ASD and MH cohorts.
Increase in the number of PHBs (notional, third party and direct payments) and integrated budgets.
Proactive and Preventative Mental Health and Well-being
CCG
Deliver the CCGs contribution (via trajectory set) to the national ambition for 50,000 to 100,000 people to have a PHB by March 2021.
Expansion plan exercise in progress to determine areas for PHB development beyond CHC homecare mandate. Personal Wheelchair Budget (PWB) opportunities to be explored. Review joint funding approach for potential
PHB uptake increases in areas beyond CHC homecare in line with trajectory requirements.
Proactive and Preventative
CCG

Operational Plan 2019/20 FINAL
Page 58 of 70
to deliver joint funded packages as integrated PHBs.
NHS Continuing Healthcare (CHC) delivery.
Develop plan to incorporate CHC strategic improvement programme opportunities into QIPP for 2019/20 through continued standardisation of process and adoption of best practice including the implementation of digital solutions, use of CHC SIP tools and guidance, and use of the CHAT assurance tools.
QIPP CHC related programme for 19/20 agreed to include: - Personal Health Budgets in CHC - OT Therapist within CHC - CHC Reviews SIP tools (Finance, workforce, Digitalization, etc) - Webex sessions completed - CHAT assurance – implementation of
the CHAT tool is in progress System wide group to align processes with WCC established and Memorandum of Understanding agreed.
QIPP schemes delivered in line with project plans, monitored monthly via assurance processes. Detailed delivery plan reviewed throughout 2019/20 and submitted to NHS England regional team. Achievement against plan reviewed at least quarterly. Liaison with other CCGs to review use of CHAT tool/resource requirements to inform implementation planning Ensure stakeholder engagement via provider forums and feedback from customers regards process and flow.
QIPP schemes delivered successfully, meeting savings targets and achieving intended quality benefits. SIP tools successfully implemented and embedded within CHC processes. Improved patient experience and reduction in complaints 80%+ of cases with a positive NHS CHC Checklist, receive an eligibility decision within 28 days from receipt of the Checklist (or other notification of potential eligibility). Improved relations with LAs result in less disputes.
Productivity and Efficiency Mental health and well-being
CCG
Continue to focus on delivery of standards within the National Framework.
Agreement to implement system-wide multi-agency training plan Project initiated to improve DToC process
Training needs assessment to be completed and development of rolling training programme to include understanding and implementation of the framework and Warwickshire Memorandum of Understanding for all
80%+ of cases with a positive NHS CHC Checklist, receive an eligibility decision within 28 days from receipt of the Checklist (or other notification of potential eligibility). Zero referrals breaching 28 days by more than 12 weeks in each reporting quarter.
Productivity and Efficiency Mental health and well-being
CCG
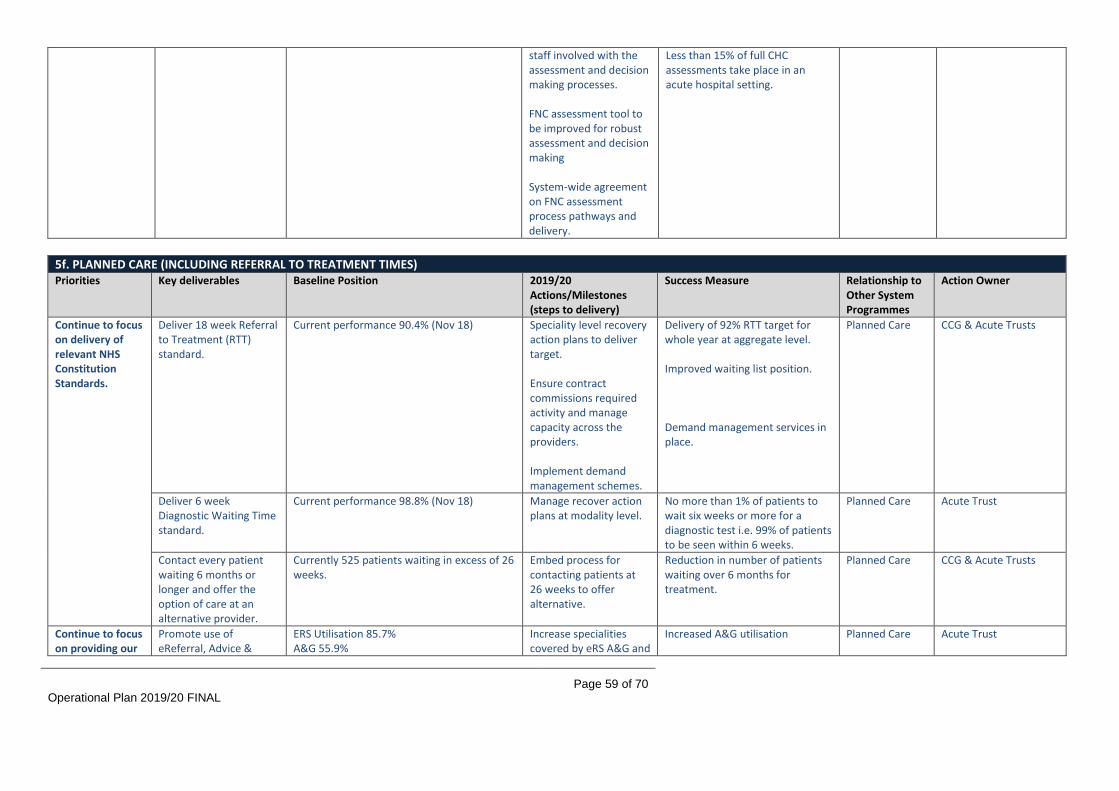
Operational Plan 2019/20 FINAL
Page 59 of 70
staff involved with the assessment and decision making processes. FNC assessment tool to be improved for robust assessment and decision making System-wide agreement on FNC assessment process pathways and delivery.
Less than 15% of full CHC assessments take place in an acute hospital setting.
5f. PLANNED CARE (INCLUDING REFERRAL TO TREATMENT TIMES) Priorities Key deliverables Baseline Position 2019/20
Actions/Milestones (steps to delivery)
Success Measure
Relationship to Other System Programmes
Action Owner
Continue to focus on delivery of relevant NHS Constitution Standards.
Deliver 18 week Referral to Treatment (RTT) standard.
Current performance 90.4% (Nov 18) Speciality level recovery action plans to deliver target. Ensure contract commissions required activity and manage capacity across the providers. Implement demand management schemes.
Delivery of 92% RTT target for whole year at aggregate level. Improved waiting list position. Demand management services in place.
Planned Care CCG & Acute Trusts
Deliver 6 week Diagnostic Waiting Time standard.
Current performance 98.8% (Nov 18) Manage recover action plans at modality level.
No more than 1% of patients to wait six weeks or more for a diagnostic test i.e. 99% of patients to be seen within 6 weeks.
Planned Care Acute Trust
Contact every patient waiting 6 months or longer and offer the option of care at an alternative provider.
Currently 525 patients waiting in excess of 26 weeks.
Embed process for contacting patients at 26 weeks to offer alternative.
Reduction in number of patients waiting over 6 months for treatment.
Planned Care CCG & Acute Trusts
Continue to focus on providing our
Promote use of eReferral, Advice &
ERS Utilisation 85.7% A&G 55.9%
Increase specialities covered by eRS A&G and
Increased A&G utilisation Planned Care Acute Trust

Operational Plan 2019/20 FINAL
Page 60 of 70
population with choice and control over their elective care.
Guidance and Consultant Connect.
Consultant Connect.
Continue to embed First Contact Practitioner services.
FCP Pilot in 1 network due to commence in Q4 201/20
Expand FCP service across Networks.
Increased number of patients having direct access to MSK First Contact Practitioners.
Planned Care Primary Care
CCG & Provider
Continue to deliver Clinical Peer Review.
91% of practices undertake a clinical peer review of secondary care referrals.
Review current scheme Q2 2019/20. Implement revised scheme as appropriate for Q3 2019/20.
Increased number of referrals reviewed.
Planned Care Primary Care
CCG
Use capacity alerts within the NHS e-Referral Service (e-RS) to support shifts in flows of activity.
Not in use at present. Implement capacity alerts where provider capacity is available within system to support shifts in flows of activity.
Capacity Alerts in use. Planned Care Acute Providers
Continue to focus on streamlining elective care pathways, including through outpatient redesign and avoiding unnecessary follow-up.
Ensure redesign/transformation plans reflect recommendations in the elective care speciality based handbooks.
Dermatology and Ophthalmology handbooks reviewed and redesign programmes in place.
Review local services against new handbooks and develop transformation plans as required.
Reduced variation in services. Planned Care Urgent Care Out of Hospital Primary Care
CCG & Providers
Expand the use of non-face-to-face alternatives e.g. virtual clinics and telehealth.
Non face to face virtual clinics in place in some specialities and for some pathways.
Speciality level and provider based action plans to be developed for mobilisation.
Increase in non face to face activity. Reduction in outpatient attendances.
Planned Care Primary Care Out of Hospital
CCG & Providers
Review system wide MSK services.
Clinical Design Authority commencing review of all MSK services across system.
Support the requirements of the system wide review at place. Implement any agreed place based changes as required.
To be conformed following outcome of the review.
Planned Care CCG & Providers
Implement Dermatology Demand Management Service.
No current service
Implement an Integrated Community Dermatology Triage and Treatment Service by Q3 2019/20.
Service in place. Reduction in acute care outpatient attendances.
Planned Care Primary Care Out of Hospital
CCG

Operational Plan 2019/20 FINAL
Page 61 of 70
Implement Ophthalmology Demand Management Service.
No current service
Implement an Integrated Community Ophthalmology Triage and Treatment Service by Q3 2019/20.
Service in place. Reduction in acute care outpatient attendances.
Planned Care
CCG
Continue to focus on delivery of planned care schemes within the South Value Programme.
Schemes in development. Develop and implement required actions plans as appropriate.
To be identified for individual schemes.
Planned Care CCG & Providers
Ophthalmology High Impact Interventions
Maintain failsafe prioritisation processes and policies in all areas to manage the risk of harm to ophthalmology patients.
Processes and Policies in place. Processes and Policies to continue to be followed.
No reported harm for patients due to inappropriate prioritisation.
Planned Care Providers
Act on the outcomes from the eye health capacity reviews.
Capacity review to be completed by March 19.
Consider outcomes of capacity review and develop and implement actions as appropriate.
To be confirmed following outcome of the review.
Planned Care CCG
Implement system wide capacity and demand model for 3 specialities
Support the development and implementation of a system wide capacity and demand model across Coventry and Warwickshire.
Model in development. Finalisation of model by Q2 2019/20. Implementation at place during Q2 2019/20. Review system wide impacts for Q3 2019/20.
Increased efficiency at place and system. Improved RTT performance for place and system.
Planned Care CCG & Acute Providers
Develop planned care outcomes based contract.
Planned Care Outcome measures and Critical Success Factors identified for new contracting approach for 2020/21.
Phase 1 Engagement for South completed. Alignment of approach across System. Phase 2 Engagement to commence. Development and finalisation of patient outcome measures and system critical success factors. Contracting approach to be agreed.
Planned Care patient outcome measures and system critical success factors defined.
Planned Care CCG

Operational Plan 2019/20 FINAL
Page 62 of 70
5g. URGENT AND EMERGENCY CARE Priorities Key deliverables Baseline Position 2019/20
Actions/Milestones (steps to delivery)
Success Measure
Relationship to Other System Programmes (Out Of Hospital, Planned Care, etc.)
Action Owner (CCG or Provider)
Continue to focus on the redesign of urgent care services outside of A&E, providing more opportunities for patients to be seen without going to A&E.
Patients are supported to navigate to the optimal urgent care service.
Range of urgent care services in place with access to be supported through utilisation of NHS 111. Over 50% of NHS 111 calls receive clinical assessment.
Communication plan to support national and reginal Choose Well and NHS 111 marketing campaigns. Continue to promote the ASK NHS app. Implementation of High Intensity User service to reduce unnecessary attendance at A&E through focused support to repeat attenders. Improve GP and community practitioner use of advice and deflection phone-lines e.g. GP Liaison, iSPAs. Support consent uptake and use of eSCR, Castle Register (EoL) and other shared records. Increase utilisation of direct to NHS 111 clinical assessment service calls for other
Maintain a 50%+ proportion of NHS 111 calls receiving clinical assessment. Over 40% of people triaged by NHS 111 that are booked into a face-to-face appointment, where this is needed, by 31 March 2020. Reduction in ‘A&E by default’ selections on DOS to less than 1% by March 2020. Increase Consultant Connect utilisation. Increase OOH iSPA calls. Increase health professional calls to NHS 111 Reduction in A&E attendances and emergency admissions.
Urgent Care Digital Transformation Primary Care Mental health Out of Hospital
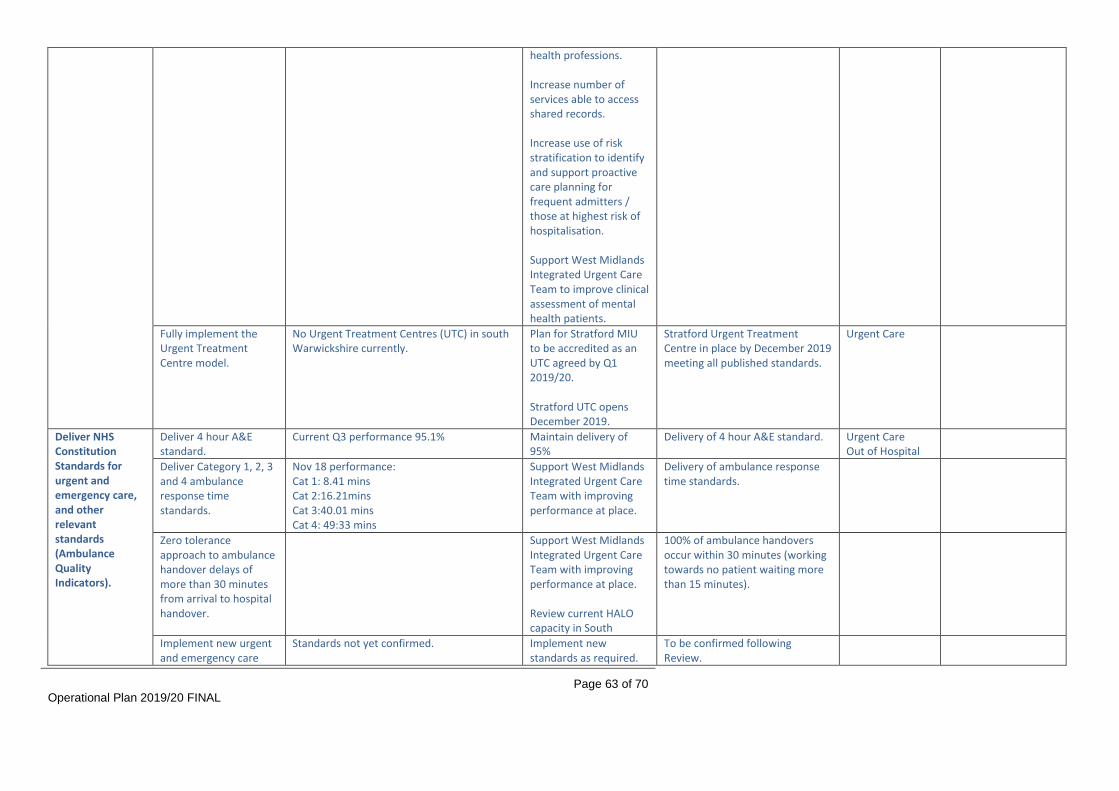
Operational Plan 2019/20 FINAL
Page 63 of 70
health professions. Increase number of services able to access shared records. Increase use of risk stratification to identify and support proactive care planning for frequent admitters / those at highest risk of hospitalisation. Support West Midlands Integrated Urgent Care Team to improve clinical assessment of mental health patients.
Fully implement the Urgent Treatment Centre model.
No Urgent Treatment Centres (UTC) in south Warwickshire currently.
Plan for Stratford MIU to be accredited as an UTC agreed by Q1 2019/20. Stratford UTC opens December 2019.
Stratford Urgent Treatment Centre in place by December 2019 meeting all published standards.
Urgent Care
Deliver NHS Constitution Standards for urgent and emergency care, and other relevant standards (Ambulance Quality Indicators).
Deliver 4 hour A&E standard.
Current Q3 performance 95.1% Maintain delivery of 95%
Delivery of 4 hour A&E standard. Urgent Care Out of Hospital
Deliver Category 1, 2, 3 and 4 ambulance response time standards.
Nov 18 performance: Cat 1: 8.41 mins Cat 2:16.21mins Cat 3:40.01 mins Cat 4: 49:33 mins
Support West Midlands Integrated Urgent Care Team with improving performance at place.
Delivery of ambulance response time standards.
Zero tolerance approach to ambulance handover delays of more than 30 minutes from arrival to hospital handover.
Support West Midlands Integrated Urgent Care Team with improving performance at place. Review current HALO capacity in South
100% of ambulance handovers occur within 30 minutes (working towards no patient waiting more than 15 minutes).
Implement new urgent and emergency care
Standards not yet confirmed. Implement new standards as required.
To be confirmed following Review.

Operational Plan 2019/20 FINAL
Page 64 of 70
standards (arising from the Clinical Standards Review) from October 2019.
Implement the recommendations in the Carter review on operational productivity and performance in ambulance trusts.
Agree trajectory for safe reduction in avoidable conveyances to emergency departments.
Support West Midlands Integrated Urgent Care Team to work with provider to deliver the outcomes of the Carter Review. Trajectory to be agreed by April 2019. New service specification in development.
Trajectory to deliver reduction in avoidable conveyances agreed by Lead Commissioner.
Ambulance services meet a baseline level of digital maturity.
Ambulance services are able to access and use patient and service information at scene. Electronic prescribing deployed.
Implement comprehensive model of Same Day Emergency Care (SDEC) in both medical and surgical specialties.
Services to be in place 12hrs per day, 7 days a week.
Ambulatory care currently in place 5 days a week for 12hrs per day.
Undertake independent review of system wide SDEC functions. Implement recommendation of above service review ensuring 12hrs and 7 day coverage. Increase utilisation of SDEC/Ambulatory Care.
SDEC delivered 12 hours per day, seven days a week by September 2019. 30% of non-elective admissions delivered via SDEC by March 2020.
Providers to record SDEC activity via standard core dataset.
Not in use yet. Providers to implement Core Dataset.
Reduce avoidable admissions through the establishment of acute frailty
Comprehensive geriatric assessments via MDTs in A&E and acute receiving units.
Frailty assessment service in place 60hrs hours per week.
Review current Acute Frailty services across system and implement any recommendations made at place.
Acute frailty service being provided for at least 70 hours a week by December 2019.

Operational Plan 2019/20 FINAL
Page 65 of 70
services. Work in progress towards achieving clinical frailty assessment within 30 minutes of arrival.
Frailty pathway review Range of frailty services in place. Full Frailty pathway review including, Primary Care, Out of Hospital and Acute Services. Develop and implement primary care frailty services for all patients including additional clinical support for those in care homes. Out of Hospital Frailty pathway to be implemented.
Reduction in emergency admissions.
Review care pathways for those patients with the most serious illness and injury (heart attack, major trauma, severe asthma attack or with sepsis).
Current pathways in place Review current pathways. Agree and sign-off revised pathways. Agree and deliver additional operational actions when identified.
Revised pathways in place
Continue to improve performance at getting people home without unnecessary delay.
Continue to reduce ALOS figures for admitted patients following unscheduled admission.
Reductions in ALOS seen in first part of 2018/19 (excluding 0 LOS) SWFT fell from 7.5 to 6.9
Providers to agree local targets for reduction in 7-day or more lengths of stay.
Bed occupancy by long stay patients reduced by 25% versus 2017/18 baseline.
Providers to agree local targets for reduction in 14-day or more lengths of stay.
Once above achieved, reduce by 40% versus 2017/18 baseline by March 2020.
Continue to work with system partners to
Nov 18 performance Acute: 2.7%
DTOCs below 3.5% Patients in hospital over
DToC targets delivered in line with Better Care Fund Plan.
Operational Plan 2019/20 FINAL
Page 66 of 70
address Delayed Transfers of Care (DToC) performance.
Community beds: 9.8%
21 days within nationally set targets for each provider

Enc 10a
SECTION 6: Managing Key Risks
This section sets out the key risks to the delivery of the Operational Plan, together with the mitigating actions that are in place. The CCG’s approach to risk management is broadly set out in its Constitution. An Assurance Framework is presented and discussed at every Governing Body meeting and is under-pinned by an Operational Risk Register, which is discussed at every Executive Team and Clinical Quality and Governance Committee meeting. The Audit Committee also has oversight of the Assurance Framework. The Assurance Framework provides the CCG with a comprehensive framework for the effective identification and focused management of risk across the organisation and wider system. The Assurance Framework identifies which of the organisation’s strategic objectives may be at risk because of inadequacies in the operation of controls, or where the CCG has insufficient assurance. At the same time, it encompasses the control of risk, provides structured assurances about where risks are being managed and ensures that objectives are being delivered. This allows the Governing Body to determine how to make the most efficient use of resources and address the issues identified. Risk Area Causes Mitigations
Failure to effectively deliver day to day commissioning responsibilities whilst at the same time contributing to the development of the Integrated Care System at System, Place and Network level.
Operational Plan describes 2019/20 as transitional year – CCG will be required to balance delivering its business as usual responsibilities and supporting the development of the ICS.
Insufficient staff resource is one area of risk.
Staff not having the competencies and capability to work differently in a changing environment is another.
Operational Plan and Commissioning Intentions document establish delivery priorities for 2019/20.
Rationalisation of functions across organisations e.g. single project teams to be established drawing human resource from across BHBCBV partner organisations. Planned Care and Maternity, Children and Young People Services Transformation Programmes will be delivered in this way.
Non-traditional ways of working across and between organisations will increasingly be the norm.
Work to develop a single commissioner will likely identify additional opportunities for the three CCGs to work together in a different way, even before the establishment of a single Strategic Commissioner.
Governing Body and BHBCBV Board oversight.
Failure to achieve the 2019/20 Financial Plan (including delivering a £1.9m in-year surplus), and failure to deliver the QIPP Programme target.
Efficiency opportunities may under-deliver against plan; the currently CCG has a QIPP Programme target of £17.2m in 2019/20 (this figure may be subject to change pending the outcome of contract negotiations). The £17.2m target represents 4.3% of the CCG’s anticipated funding in 2019/20.
The CCG has a robust governance structure in place relating to QIPP Programme delivery – the structure includes the Finance Delivery Board, which engages senior manager and clinician input.
The Financial Plan includes the 0.5% contingency (£2.0m) which will provide in year

Operational Plan 2019/20 FINAL
Page 68 of 70
Risk Area Causes Mitigations
Final 2018/19 pressures – any pressures that emerge relating to the final weeks of 2018/19 could impact on the exit rate and thus place further pressure on 2019/20 e.g. unexpected growth in prescribing, increased acute contract performance or unachieved QIPP.
Individual Packages of Care packages – this expenditure continues to be a financial risk for the CCG moving into 2019/20.
mitigation for non-recurrent use.
Benchmarking and horizon scanning will be undertaken to identify additional QIPP opportunities over-and-above the budgeted plan to provide mitigation for slippage in delivery of those schemes identified.
The CCG and SWFT will agree and take joint ownership of a joint Value Programme. This will provide additional impetus and traction for a number of schemes within the QIPP Programme.
Failure to achieve NHS Constitution standards and targets.
A broad range of factors have the potential to impact performance. For example, winter pressures may impact delivery of the A&E waiting time target. In relation to targets relevant to planned care activity (Referral to Treatment Time target, Diagnostic Waiting Time target, etc.), poor alignment between demand and capacity is the key factor.
The CCG’s performance against NHS Constitution targets has continued to be strong in 2018/19.
The CCG will continue to utilise all contractual levers to improve performance.
Where performance issues are identified a robust management process is initiated which includes the implementation of recovery plans. The CCG’s Performance Committee has oversight of the delivery of these plans.
The CCG and SWFT will agree and take joint ownership of a Value Programme 2019/20. This will provide additional impetus and traction for a number of schemes within the QIPP Programme, including those aimed at demand management.
Planned Care Transformation Programme will be an area of focus in 2019/20.
Workforce Set out in full in the Primary Care Workforce Strategy.
Primary Care Workforce Strategy in place and being implemented.
On-going assurance process in place with NHS England.
The CCG will maintain engagement with and, as appropriate, seek support from Health Education England and the Local Workforce Action Board in relation to the implementation of the Strategy.

Operational Plan 2019/20 FINAL
Page 69 of 70
Digital Innovation Potential for lack of alignment between local direction of travel (as set out in the GPICT Strategy) and national direction; specifically in relation to schemes being mandated at a national level (with associated funding available).
GPICT Strategy in place and being implemented.
Programme structure and governance in place for GPICT projects.
The CCG will maintain close engagement with the NHS England Midlands & East Regional Team via the Head of Digital Technology
The CCG will maintain engagement with and, as appropriate, seek support from the Digital Transformation Board in relation to the implementation of the Strategy.

Operational Plan 2019/20 FINAL
Page 70 of 70
Blank Page
End of Report
NHS South Warwickshire Clinical Commissioning Group Enc 11
Primary Care Networks Governing Body - 22 May 2019
Page 1 of 2
Report To: Governing Body For decision
Report Title: Primary Care Networks For discussion
Report From: Alison Cartwright, Chief Delivery Officer Anna Hargrave, Chief Strategy Officer
For information
Date: 22 May 2019 Confidential
Purpose of the Report
The Governing Body is being asked to approve the registration applications from the 7 Primary Care Networks (PCNs) in south Warwickshire details of which are shown in attachment 1.
Key Points:
• CCGs are required to confirm that the registration requirements for the formation of PCNs have been met as required in the Network Contract Directed Enhanced Service Contract Specification 2019/20 by 31st May 2019.
• In The NHS Long term Plan, PCNs are an essential building clock of every Integrated Care System (ICS).
• The GP five-year framework published in January 2019 describes how general practice will implement The NHS Long Term Plan and includes the mandated requirements of PCNs.
• In summary these are:- o All GP practices are expected to be in a PCN; o PCNs are required to a minimum of 30,000 population; o The PCN area must cover a boundary that makes sense to its constituent members;
community providers and local community and cover a geographically contiguous area; o The PCN will be required to appoint a named accountable Clinical Director, who will be a
practicing clinician from within the PCN members practices who will represent the PCN at CCG-level clinical meetings and the ICS/STP;
o Identify a single nominated practice or provider to receive PCN funding; o Submit their application to the CCG for approval by 15th May 2019.
• The registration requirements have been received from all 7 PCNs.
Recommendation (s):
Governing Body approve the applications and confirm this in writing to the PCNs by 31st May 2019.
Previously Considered By: Date:
Not applicable
CCG Strategic Objective(s) this report relates to:
Out of Hospital √ Personalisation Specialist Provision
Delivering Today √
NHS South Warwickshire Clinical Commissioning Group Enc 11
Primary Care Networks Governing Body - 22 May 2019
Page 2 of 2
Management of Conflicts of Interest: As per CCG Managing Conflicts of Interest policy
Financial Implications: Funding has been clearly identified within the Network Contract Directed Enhanced Service (Network DES).
Performance Implications: N/A
Quality Implications: N/A
Equality and Diversity Considerations: N/A
Patient, Public and Stakeholder Engagement:
Key stakeholders have been engaged regarding The Long Term Plan so are aware of the Network DES.
Risk Assessment: No risks have been identified at this time.

Enc 11a
Governing Body – 22 May 2019
Network Clinical Director Network List Size Network Member Practices ODS
code Practice’s registered
list size (as at 1 January 2019)
Arden Dr Gareth Rowland Dr Mansur Ahmad 37,723
The Pool Medical Centre M84002 7,429 Henley-in-Arden Medical Centre M84024 6,630 Tanworth-in-Arden Medical Centre M84047 4,576 Alcester Health Centre M84049 5,687 Arrow Surgery M84060 5,820 Budbrooke Medical Centre M84069 4,981 Lapworth Surgery M84620 2,600
Stratford Surrounds Dr Karen Clarke 39,383
Bidford Health Centre M84018 12,026 Hastings House Surgery M84030 11,438 Meon Medical Centre M84066 4,693 Shipston Medical Centre M84025 11,226
Stratford Central Dr Michael Cordner 44,908
Arden Medical Centre M84617 2,768 Bridge House Medical Centre M84014 9,013 Rother House Medical Centre M84021 14,925 Trinity Court Surgery M84043 18,202
Warwick and Kenilworth
Dr Nick Yeats 60,980
Abbey Medical Centre M84036 13,928 Avonside Medical Centre M84010 9,784 Priory Medical Centre M84028 18,047 The Castle Medical Centre M84013 12,055 The New Dispensary M84063 7,166
Leamington South Dr Sukhi Dhesi 34,135
Croft Medical Centre M84015 15,895 Spa Medical Centre M84059 3,833 Warwick Gates Family HC M84070 8,020 Whitnash Medical centre M84064 6,387
Leamington North Dr Oliver Lawton 43,731 Clarendon Lodge M84017 13,604 Cubbington Road Surgery M84029 7,193

Enc 11a
Governing Body – 22 May 2019
Sherbourne Medical Centre M84040 9,736 Waterside Medical Centre M84032 13,198
East Dr Melinda Wood 30,431
Fenny Compton Surgery M84009 5,438 Harbury Surgery M84044 5,818 Kineton Surgery M84062 5,309 Southam Surgery M84026 8,008 St Wulfstan Surgery M84629 5,858
TOTAL 291,291