a l i a n dis t r i c t h - parliament of victoria - home · shared intern position at the end of...
TRANSCRIPT

Nat
halia
D istr ict Ho
spit
al
Providing Quality Care
Annual Report& Quality of Care report 2012/13
Leading our community towards better health
Nathalia District Hospital

Contents
Relevant Minister 1
Mission & Vision 1
About Nathalia District 2 Hospital
Chair Report 3
Director of Medical Services Report 4
Board Members 6
Attendance at Meetings 6
Senior Officers 7
Organisational Chart 8
Workforce Data 9
Statutory Requirements 10
Summary of Financial Results 13
Statement of Priorities 14
Financial and Service Performance Reporting 16
Highlights for 2012-2013 18
Disclosure Index 19
Annual Financial Report 21
Quality of Care Report 69
INTRODUCTION
In accordance with the Financial Management Act 1994, I am pleased to present the Report of Operations for the Nathalia District Hospital for the year ended 30 June 2013.
Sue Logie Chair – Board Of Management Nathalia26 August 2013
Annual Reporting
Nathalia District Hospital reports on its annual performance in two separate documents. This Annual Financial and Performance Report fulfills the statutory reporting requirements to Government by way of an Annual Report and the Quality of Care Report reports on quality, risk management and performance improvement matters. Both documents are presented to the Annual General Meeting and then distributed to the community.

ANNUAL REPORT
VisionLeading our community towards better health.
MissionWorking collaboratively to provide quality health and well-being services for our community
ValuesIntegrity
We engage others in a respectful, fair, and ethical manner, fulfilling our commitments as professionals. We ensure highest degree of dignity, equity, honesty, and kindness.
Accountability We ensure quality patient care, and use resources appropriately in an open and transparent manner.
Collaboration We work as a team in partnership with our staff, our community, and other healthcare providers.
Knowledge
We create opportunities for education and health promotion.
Excellence
We are committed to achieving our goals and improving quality of care by delivering efficient, safe, person-centred, innovative, knowledge-based healthcare.
NATHALIA DISTRICT
HOSPITAL 2012/13
n a t h a l i a D i s t r i C t h o s p i t a l - a n n u a l r e p o r t 2 0 1 2 / 1 3 3
Nathalia District Hospital was established under the Health Service Act 1988.
Relevant Minister
The responsible Ministers during the reporting period was:
The Honourable David Davis, MLC, Minister for Health and Ageing.
The Honourable Mary Wooldridge, MLA, Minister for Mental Health.

4 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
The Objectives, Functions, Powers and Duties of Nathalia District Hospital are described in the Operational Practices and By-laws of the
organisation.
Established under the Health Services Act 1988, Nathalia District Hospital is the major regional health provider for Nathalia.
Nathalia District Hospital continues to operate under the Department of Health Small Rural Health Services model. This model gives the hospital flexibility to tailor services to meet the changing needs of our community. These programs are reviewed annually in consultation with our community.
The hospital services the residents of Nathalia and District, which encompasses the small townships and districts of Waaia, Barmah, Picola, Kotupna, Bearii and Yalca. It provides a 24-hour urgent care service with a medical practitioner on call, and a range of services within the Acute Care Unit to cater for adults and children. Outpatients services are conducted in Radiology, Pathology, Physiotherapy, Speech Pathology, Occupational Therapy, Dietetics, Palliative Care, Residential Aged Care and Generalist Counselling. Community Health staff and District Nurses provide a wide range of health promotion and domiciliary programs to our community.
About Nathalia District Hospital
4 n a t h a l i a D i s t r i C t h o s p i t a l - a n n u a l r e p o r t 2 0 11 / 1 2

N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3 5
Chair Report
The 2012-2013 financial year had hospital boards across the country struggling with the Commonwealth Government’s announcement
of a reduced allocation of funding mid financial year due to the Australian Bureau of Statistics review of Estimated Resident Population figures. Hospitals across Australia were informed that hospitals were facing a funding cut. I attended a meeting with The Honorable David Davis, MLC, Minister for Health and Ageing, with other rural health board members to discuss the funding crisis. With a loud and clear message from the Victorian Healthcare Association and healthcare providers the Commonwealth decision to cut the funding midyear was overturned.
We had a change of key personnel with the CEO Kerryn Healy resignation resulting in Andrew Stripp being appointed as Acting CEO.
Thanks to Alan Sage, who as chair of the Nathalia and District Hospital board was successful in the realisation of the current building. Alan did not apply for re appointment to the Board.
Madeline Keil resigned from the board due to ill health. We also were saddened that Marion Hando also resigned for health reasons. Marion’s input as a community representative on the patient care review committee was highly valued and will be missed. Thank you for your time and contribution.
We welcome the challenge of accreditation under the new National Safety and Quality Health Service Standards. The Nathalia and District Hospital board appreciates that the changes can increase the workload of individual staff members, and is encouraged by the support for the accreditation process.
Our Board members were able to attend a workshop conducted by Steven Bowman on Advanced Governance and Strategic Awareness. Liam Bourke, Kevin Pell and Sue Logie took the time to attend the
workshop and report back to the board. I attended the Auditor General’s Regional Client Forum, and the Hume Health Services Chair’s forum.
I acknowledge the collaborative work of all Nathalia and District Hospital directors, staff, and volunteers throughout the year. I thank you for the opportunity to chair over the past three years and appreciate the assistance of the Department of Health and the staff at GV Health who assist our Hospital in our vision to lead our community towards better health.
Bernadette Brooks Chair – Board of Management 2012-2013

6 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
As I said last year in my report, my appointment at Nathalia District Hospital requires little time at the hospital itself. In fact, my appointment requires me to actually work one day a month. However, as the Director of Medical Services for all four Moira health services as well as being Director of Clinical Training for Murray to the Mountains Intern Training Program, there is a certain synergy in what I do across all the health services.
One clear example of this is that of Chair of the Moira Health Credentialing and Privileging Committee whereby the whole process of assuring that the doctors have the appropriate qualifications, are duly registered to practise and have medical indemnity and then through the link between scope of practice and privileging assuring the knowledge and competency of each doctor.
It has been an eventful year. Dr Chuck Fong has obtained his FRACGP; Dr Nyorora Mogeke is almost there; Dr Peter Poon has clearly demonstrated his ongoing commitment to training, reinforced by the shared intern position at the end of last year, whereby the then intern at Cobram District Health, Dr Alison Mahony, undertook some of her training at Nathalia District Hospital. Dr John Drenen has continued to provide the solid face of rural general practice and his influence in the education program was amply demonstrated in the Grand Round presentation . Here the theme was of a young woman where modern medicine has enhanced her life expectancy, and where a generation or so ago, she would not have faced adulthood. It is such Grand Rounds which are important to delineating through case presentations the clinical and ethical dilemmas which health professionals face.
Recently Dr Rajani Nandakumar has joined the practice to undertake 26 days in a second practice as required by her training program as a general practice registrar. She is based primarily in the Kialla practice in Shepparton, but being in Nathalia has provided her with a glimpse of working in a rural practice outside a regional centre.
The other advancement in medical practice has seen the commencement of regular visits by Dr Arup Bhattacharya, consultant geriatrician at Goulburn Valley Health. Over the past two years, consultant geriatricians from Western Health have been visiting on a six week basis providing a mixed clinical/education program, which has been very successful.
Hopefully Nathalia, together with Numurkah, in association with the University of Melbourne Medical Clinic in Shepparton, will get its own intern placement in 2015. Nathalia has provided a very useful teaching space and hosted a number of memorable videoconferences.
Dr Mark Harris provided one of these on the night that the tornado ripped down along the Murray River through Cobram and Mulwala despite the buffeting of the building from the maelstrom outside, the two Yarrawonga interns received this videoconference with great clarity.
Other notable videoconferences from Nathalia were Professor Charles Guest, the President of the Australasian Faculty of Public Health Medicine, speaking on his experiences in revisiting the Goulburn Valley region where he did his research thesis on public health some thirty years before; and Mr Andrew Warden, who described his ten year experience as a patient/consumer with the rare condition of Waldenstrom’s Macroglobulinaemia.
Director of Medical Services Report

N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3 7
Videoconferencing has both facilitated despite a number of correctable glitches communication across the region and in so doing emphasised that one of the major reasons for education is to engender a degree of collegiality between the various health services through education.
Finally, I would like to thank Leigh Giffard, Lynne Peterson and all the staff for providing me with the opportunity to work in this pleasant environment, which is Nathalia!
Dr John Best OA Director of Medical Services
n a t h a l i a D i s t r i C t h o s p i t a l - a n n u a l r e p o r t 2 0 1 2 / 1 3 7

8 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Chair Ms Bernadette Brooks Committees:
• Audit Committee
• Medical Appointments Committee
• Moira Healthcare Alliance
• Patient Care Review Committee
Senior Vice Chair Ms Sue Logie Committees:
• Audit Committee
• Medical Appointments Committee
• Patient Care Review Committee
Treasurer and Junior Vice Chair Mr David Vaughan Committees:
• Audit Committee
• Patient Care Review Committee
Other Members
Mr Alan Sage Committees:
• Patient Care Review Committee
Mr Kevin Pell Committees:
• Medical Appointments Committee
• Patient Care Review Committee
Mr David McKenzie Committees:
• Patient Care Review Committee
Ms Madeleine Keil (resignation 01/03/2013) Committees:
• Patient Care Review Committee
Ms Kerry-anne Rappell (appointment 01/01/2013) Committees:
• Patient Care Review Committee
Mr Liam Bourke (appointment 01/01/2013) Committees -
• Audit Committee
• Patient Care Review Committee
Attendance at MeetingsJUN JUL AUG SEP NOV DEC JAN FEB MAR APR MAY JUN
Ms. B. Brooks NM A
Mr. A. Sage A NM A
Ms. S. Logie A NM (Chair) A A
Mr. D. McKenzie A NM
Mr. K. Pell NM
Mr. D. Vaughan A NM
Ms. M. Keil A NM A
Ms. K. Rappell NM
Mr. L. Bourke NM A A
= In Attendance A = Apology NM = No Meeting
Honorary Solicitors - Dawes & Vary Auditors - Auditor - General Victoria Bank - Bendigo Bank
Board Members

N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3 9
Chief Executive Officer Ms Kerryn Healy B. Bus (Acc), CPA, AFCHSE, CHE, FHFM (until 8 March 2013)
Chief Executive Officer Mr. Andrew Stripp (March 2013 to June 2013) BBSc(Hons)MSc
The Chief Executive Officer (CEO) is responsible to the Board of Management for the efficient and effective management of Nathalia District Hospital. Prime responsibilities include the development and implementation of operational and strategic planning, maximising service efficiency and quality improvement, and minimising risk. The CEO is also CEO of the Yea & District Memorial Hospital and Goulburn Valley Health and chairs the Nathalia District Hospital Executive. The CEO represents Nathalia District Hospital on a number of State committees, the Hume Regional Integrated Cancer Service, and the Hume Rural Health Alliance Executive Committee, and is also a member of the Hume Health Partnership.
Chief Finance Officer Mr Shaun Eldridge B.Bus (Acc) MBA, CPA
The Chief Finance Officer has responsibility for the financial management and reporting requirements to the Board of Management, Managers and external bodies including the Department of Health.
Director of Nursing/Manager Ms Leigh Giffard RN, RM, BN, Grad Dip Advanced Nursing (Management), Master of Health Service Management, MRCNA
The Director of Nursing/Manager is responsible for the management of all clinical and non-clinical services within the organisation. This includes Nursing, Hospitality, Maintenance, Allied Health Services and
the Nathalia Medical Clinic. Leigh also oversees the operational management of Quality Improvement, Risk Management, Occupational Health and Safety, and Complaints Management. She maintains strong links with the community and its representatives to ensure the services provided by our Hospital meet Community needs.
Assistant Director of Nursing Mr Grant Hutchins RN, Bachelor of Public Health, BN
The Assistant Director of Nursing holds a key management and leadership role within the Hospital coordinating the quality of clinical care delivered to our residents and patients. Major responsibilities include Clinical Leadership and Standards of Practice, Nursing Recruitment and Retention, Clinical Risk Management, and Quality Improvement. Grant oversees the placement of nursing, allied health and medical students as well as the ongoing professional development of our own clinical staff. Where necessary, Grant relieves the Director of Nursing/Manager to ensure seamless service delivery.
Director of Medical Services Dr John Best OA MBBS (USyd), FRACP, FRACMA
The Chief Medical Officer has overall professional responsibility for Visiting Medical Officers, biomedical engineering services and medico legal advice. The Chief Medical Officer co-ordinates medical credentialing of VMOs and provides advice to the Board of Management about the appointment of Visiting Medical Officers.
Senior Officers

10 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Org
anis
atio
nal C
hart
Boa
rd o
f Man
agem
ent
Nat
halia
Dis
tric
t Hos
pita
l & B
anaw
ah
Nur
sing
Hom
e
Chi
ef E
xecu
tive
Offi
cer
Dire
ctor
of N
ursi
ng/M
anag
erQ
ualit
y C
oord
inat
orC
hief
Fin
ance
Offi
cer
Dire
ctor
of M
edic
al S
ervi
ces
Ass
ocia
te D
irect
or o
f Nur
sing
Adm
inis
trat
orV
isiti
ng M
edic
al O
ffice
rs
NAT
HA
LIA
ME
DIC
AL
CLI
NIC
Pra
ctic
e N
urse
Pra
ctic
e M
anag
erR
ecep
tion
HO
SP
ITA
LITY
S
ER
VIC
ES
C
OO
RD
INAT
OR
Adm
inis
trat
ive
Sup
port
Hea
lth In
form
atio
n M
anag
emen
tS
tore
sC
ater
ing
Cle
anin
gLa
undr
yM
aint
enan
ceIn
depe
nden
t Liv
ing
Uni
ts
DIS
TRIC
T N
UR
SIN
G
UN
IT M
AN
AG
ER
Dis
tric
t Nur
ses
HIT
HP
ost A
cute
Car
eD
omic
iliary
Pos
t Nat
al
Vis
itsP
allia
tive
Car
e H
ome
Ser
vice
s
CO
MM
UN
ITY
HE
ALT
H
CO
OR
DIN
ATO
R
Wom
en’s
Hea
lthH
ealth
Pro
mot
ion
Pla
nned
Act
ivity
Gro
upG
ym a
nd S
tren
gth
Trai
ning
Volu
ntee
r C
oord
inat
ion
Allie
d H
ealth
Dia
bete
s C
linic
Cou
nsel
ling
Ser
vice
sV
isiti
ng S
ervi
ces
incl
udin
g R
adio
logy
and
Pat
holo
gy
CLI
NIC
AL
SE
RV
ICE
S
and
RE
SID
EN
TIA
L A
GE
D C
AR
E
NU
RS
E U
NIT
M
AN
AG
ER
Em
erge
ncy
Acu
te C
are
Pal
liativ
e C
are
Res
iden
tial A
ged
Car
eR
esid
ent L
ifest
yle
AC
FI D
ocum
enta
tion

N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3 11
Labour Category June Current Month June YTD FTE
2012 2013 2012 2013
Nursing 33.21 30.44 32.60 30.76
Administration & Clerical 6.47 7.79 6.06 7.59
Medical Support 0.04 0.05 0.06 0.05
Hotel & Allied Health Services 12.60 12.63 13.22 12.57
Hospital Medical Officers 1.00 0.79 0.95 0.97
Ancillary Staff (Allied Health) 3.16 2.67 2.44 2.66
Nursing 30.44
Hotel & Allied Health Services 12.63
Medical Support 0.05
Administration & Clerical 7.79
Ancillary Staff (Allied Health) 2.67
Workforce Data
Hospital Medical Officers 0.79
Nathalia District Hospital is committed to applying merit and equity principles when appointing staff. The selection processes ensure that applicants are assessed and evaluated fairly and equitably on the basis of the key selection criteria and other accountabilities without discrimination.
All Nathalia District Hospital staff are required to abide by the Code of Conduct, which is based on the Code of Conduct for Victorian Public Sector Employees.

12 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Consultancies
No consultancies were commissioned by Nathalia District Hospital during the year 2012/13.
Occupational Health and Safety
Nathalia District Hospital complies with the Occupational Health and Safety (OH&S) Act 2004. The health and safety of our staff, residents, patients and visitors is paramount at the Hospital. All staff make a commitment on commencement of work at the Hospital to diligently create and maintain a safe environment.
During the 2012/13 financial year, no work injuries or days lost were recorded.
Occupational Health and Safety is supported by an appropriate incident and hazard identification system in a ‘No Blame’ environment, as well as an open disclosure policy. All incidents are reported using the Victorian Health Incident Management System. Identified OH&S risks have key performance indicators in place, which are monitored and reported monthly to relevant committees who ensure those risks are managed.
Compliance with Building Act
Nathalia District Hospital complied fully with the building and maintenance provisions of the Building Act 1993 – Guidelines issued by the Minister for Finance for publicly owned buildings.
During 2012-13, the following have been undertaken: Regulation 1209 & 1215 - Annual Essential Safety Measures Report.
Key Performance Indicators exist across a range of OH&S services, including:
Topic No. of KPIs Results
Fire and Emergency 8 94% of staff completed competency in fire and emergency training – a decrease of 3.6% on previous year. Those staff who have not completed the competency are on maternity leave.
Manual Handling 5 94% of staff completed competency in manual handling, with no time lost due to manual handling incidents in 2012/13.
Infection Control 9 All KPIs were achieved in this area in 2012/13.
Safe Chemical Management 4 100% of non-clinical staff completed chemical safety competency.
Radiation Safety 2 Achieved all outcome measures in all areas.
Waste Management 3 Achieved all outcome measures in all areas.
Security 5 Achieved outcome measures in all areas. Additional surveillance cameras have been installed to increase safety after hours.
Noise 3 No documented complaints about noise received in 2012/13.
Contractor Management 4 Achieved all outcome measures in all areas.
Statutory Requirements

13N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Occupancy Permits and Certificates of Final Inspection.
Nathalia District Hospital Occupancy Permits and Certificates of Final Inspection are all current.
Building Works
No new Occupancy Permits and Certificates of Final Inspection were issued.
Essential Safety MeasuresNathalia District Hospital buildings constructed after 1994 have been designed to conform to The Building Act 1993 and its Regulations, as well as to meet other statutory regulations that relate to health and safety matters. All have been issued with Occupancy Permits.
Irrespective of the age of each building, Nathalia District Hospital is obliged to maintain essential safety measures, so far as is practicable, in accordance with the Building Regulations 2006.
Compliance involves ensuring that all essential safety measures covered by the Regulations are being maintained to fulfil their purpose. It also involves keeping records of maintenance checks, completing an Annual Essential Safety Measures Report, and retaining records and reports on the premises for inspection by the Municipal Building Surveyor or the Chief Fire Officer on request.
Essential Safety Measures Reports are prepared annually for properties owned by Nathalia District Hospital to confirm that all of the essential safety services are operating at the required level of performance.
Fire Audit Compliance The Nathalia District Hospital Fire Audit is current.
Freedom of Information Requests
Nathalia District Hospital is an agency subject to the Freedom of Information Act (Victoria) 1982. There were two formal requests for information received by Nathalia District Hospital under the Act during 2012-13.
The Nathalia District Hospital Freedom of Information/Medico-Legal Officer is under the Clinical Services Division at Nathalia District Hospital. A legislated fee of $25.10 per application and an excess charge of $20 are applied for a search fee when required.
Competitive Neutrality
Nathalia District Hospital has complied with all government policies regarding competitive neutrality.

14 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Victorian Industry Participation Policy
Nathalia District Hospital abides by the principles of the Victorian Industry Participation Policy Act 2003. In 2012-13, there were no procurement or project activities under the Victorian Industry Participation Policy above the threshold of $1 million.
Environmental Performance
Nathalia District Hospital has a total of 5 fleet vehicles in its fleet. Fuel consumption and greenhouse gas emissions are monitored bi-monthly as part of our Environmental Management Plan by the OH&S Committee.
Each vehicle has an individual ‘green’ rating, which includes our air pollution and greenhouse ratings; our overall ‘green’ score for this financial year is 12.5 out of 20.
Description Number Percentage of fleet
4 cylinder vehicles 5 100%
Diesel vehicles 3 60%
Unleaded vehicles 2 40%
Additional Information
In compliance with the requirements of FRD 22C Standard Disclosures in the Report of Operations, details in respect of the items listed below have been retained by Nathalia District Hospital and are available to the relevant Ministers, Members of Parliament and the public on request (subject to the freedom of information requirements, if applicable):
a. A statement of pecuniary interest has been completed;
b. Details of shares held by senior officers as nominee or held beneficially;
c. Details of publications produced by the Department about the activities of the Health Service and where they can be obtained;
d. Details of changes in prices, fees, charges, rates and levies charged by the Health Service;
e. Details of any major external reviews carried out on the Health Service;
f. Details of major research and development activities undertaken by the Health Service that are not otherwise covered either in the Report of Operations or in a document that contains the financial statements and Report of Operations;
g. Details of overseas visits undertaken including a summary of the objectives and outcomes of each visit;
h. Details of major promotional, public relations and marketing activities undertaken by the Health Service to develop community awareness of the Health Service and its services;
i. Details of assessments and measures undertaken to improve the occupational health and safety of employees;
j. General statement on industrial relations within the Health Service and details of time lost through industrial accidents and disputes, which is not otherwise detailed in the Report of Operations;
k. A list of major committees sponsored by the Health Service, the purposes of each committee and the extent to which those purposes have been achieved;
l. Details of all consultancies and contractors including consultants/contractors engaged, services provided, and expenditure committed for each engagement.
Statutory Requirements continued

15N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Relevant Financial Information
Summary of Financial Results
Financial Analysis of Operating Revenues and Expenses 2013 2012 2011 2010 2009
Total Revenue 6,227,662 5,848,139 5,620,155 10,504,238 4,019,233
Total Expenses 6,655,300 6,344,655 6,377,494 5,497,230 4,348,046
Net Result for the year (inc. Capital & Specific Items) (427,638) (496,516) (757,339) 5,007,008 (328,813)
Retained Surplus/ (Accumulated Deficit) 3,424,478 3,999,122 4,386,060 5,080,701 264,413
Total Assets 18,010,127 18,053,963 18,227,142 18,904,848 13,752,767
Total Liabilities 1,900,102 1,516,300 1,192,963 1,113,330 968,257
Net Assets 16,110,025 16,537,663 17,034,179 17,791,518 12,784,510
Total Equity 16,110,025 16,537,663 17,034,179 17,791,518 12,784,510
Nathalia District HospitalSummary of Financial Results For the Year Ended 30 June 2013
Revenue IndicatorsAverage Days
to Collect2012/13 2011/12
Private Inpatients 27.39 27.63
Residential Aged Care 34.07 33.70
Significant Changes in Financial Position
The cash and investment assets of Nathalia District Hospital have increased this financial year. This is largely due to receipt of resident accommodation bonds during the financial year.
Equity has decreased during the year by the entity result for 2012-13 of $427,638 deficit, due in the main to depreciation.
Operational & Budgetary Objectives & Factors Affecting Performance
The Board budgeted for a break even result in financial position before capital items and depreciation for the 2012-13 year. The final result for the year was a deficit of $35,355 before capital items and depreciation.
Events subsequent to balance date
Nathalia District Hospital negotiated the sale of the former hospital site in Elizabeth Street during the year, the proceeds realised at settlement in the 2013/14 financial year.

16 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Statement of Priorities 2012-2013
Priority Action Deliverable Outcome
1. Developing a system that is responsive to people’s needs
In partnership with other providers within the local area apply existing service capability frameworks to maximise the use of available resources across the local area.
Build on current partnerships with other Moira health services to deliver a community rehabilitation program across the shire
In Progress-
Moira CRC hub is currently being built in Cobram. Building works due for completion December 2013. Spoke services at Nathalia due to commence approximately 12-18mths later.
Liaise with Nathalia community association to improve the current model of care by incorporating social wellbeing into our health programs
Completed-
Community well being programs commenced including monthly carers lunch and weekly ‘people supporting people’ community barbecue.
2. Improving every Victorian’s health status and experiences
Consider new models of care and more coordinated services to respond to the specific needs of people with priority clinical conditions
Expand community health programs to include audiology services to improve outcomes for clients with hearing deficits
Completed-
Visiting Audiology services commenced fortnightly from August 2012.
Increase access to videoconferencing to provide increased options for specialist involvement in patient care.
Completed-
Videoconferencing sessions are held monthly with medical specialists to provide education for our health care staff and opinion/involvement in patient care.

17N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
3. Expanding service, workforce and system capacity
Develop collaborative approaches to deliver professional education, training and support.
Introduce the ‘advanced practice nurse’ model to improve after hours emergency treatment when there is no doctor available on call.
Completed-
Rural and Isolated Practice Endorsed Nurses commenced practicing at the organisation in February 2013.
Support the partnership with the Murray to Mountains (M2M) program to provide placement for interns in the Nathalia Medical Clinic.
In Progress-
Ongoing-The organisation continues to receive and support medical intern placements, assisting the currency of their knowledge and skills
4. Increasing the system’s financial sustainability and productivity
Identify opportunities for efficiency and better value service delivery.
Maintain a sound financial position by working towards a break even budget.
In Progress-
New budget developed aimed at achieving a 2% surplus
Examine and reduce variation in administrative overheads.
Work towards the sale of the old hospital site to improve the overall financial position of the health service.
In Progress-
Offer received and accepted in June 2013.
Analyse consumables for administrative purposes.
Completed-
Review of ordering systems to manage stock control, February 2013.
5. Implementing continuous improvements and innovation
Develop and implement strategies that better support patient flow and the quality and safety of hospital services
Work towards a patient centred care model by introducing the identify- situation-observations-background-agreed plan- read back (ISoBAR) handover technique and hourly rounding.
Completed-
ISoBAR Handover and hourly rounding introduced in October 2012. Falls incidences have reduced significantly post introduction of the new system.
Review the quality processes to ensure compliance with the National Safety and Quality Standards
Completed-
Preparations complete for National Standard Review scheduled for September 2013

18 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Financial and Service Performance Reporting
18
FINANCIAL PERFORMANCE
Operating Result Target 2012-13 actuals
Annual Operating result ($m) $0 -$35,355
Cash management Target 2012-13 actuals
Creditors <60 days 38
Debtors <60 days 48
Quality and Safety Target 2012-13 actuals
Health service accreditation Full compliance Full compliance
Residential aged care accreditation Full compliance Full compliance
Cleaning standards Full compliance Full compliance
Submission of data to VICNISS Full compliance Full compliance
Hand Hygiene (rate) 70 78.5%
Victorian Patient Satisfaction Monitor (OCI) 73 83.8%
Consumer Participation Indicator 75 80.5%
People Matter Survey Full compliance Full compliance
ACUTE PERFORMANCE
Service Campus Type of Activity Activity Levels
Medical inpatients Bed days 1327
Urgent Care Presentations 214
Nursing home type patients Bed days 363
Non-admitted patients Occasions of service 7158
Radiology Number of clients 253
District nursing Occasions of service 4715

19N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
ATTESTATION OF DATA INTEGRITY
I, Dale Fraser, certify that Nathalia District Hospital has put in place appropriate internal controls and processes to ensure that reported data reasonably reflects actual performance. Nathalia District Hospital has critically reviewed these controls and processes during the year.
Dale Fraser Chief Executive Officer 23 August 2013
ATTESTATION FOR COMPLIANCE WITH THE MINISTERIAL STANDING DIRECTION 4.5.5.1 - INSURANCE
I, Dale Fraser, certify that Nathalia District Hospital has complied with Ministerial Direction 4.5.5.1 - Insurance
Dale Fraser Chief Executive Officer 23 August 2013
ATTESTATION OF COMPLIANCE WITH AUSTRALIAN/NEW ZEALAND RISK MANAGEMENT STANDARD
I, Dale Fraser, certify that Nathalia District Hospital has risk management processes in place consistent with the Australian/New Zealand Risk Management Standard and an internal control system is in place that enables the executives to understand, manage and satisfactorily control risk exposures. The audit committee verifies this assurance and that the risk profile of Nathalia District Hospital has been critically reviewed within the last 12 months.
Dale Fraser Chief Executive Officer 23 August 2013
PRIMARY HEALTH CARE
Activity levels
Service Outpatient Inpatient Nursing Home
Physiotherapy 1172 95 356
Occupational Therapy 106 47 113
Dietitian 60 10 29
Footcare 246 2 19
Diabetes Education 55 2 0
Optometry 89 0 2
Counselling 546 38 207
Domiciliary 14 0 0
Well Womens Clinic 71 0 0
Pathology 2408 0 0
Community Health 1618 0 0
Music Therapy in the Home 9 26 202

20 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Highlights for 2012-2013Implementation of the Rural and Isolated Practice Endorsed Registered Nurse (RIPERN) Program
Our health service has been working towards improving patient access to timely, safe and appropriate care for people in Nathalia in the event that there is no Medical Officer available to provide care. With the support and assistance of the Victorian Department of Health, Nathalia District Hospital commenced the RIPERN program in February 2013.
The RIPERN function means that RIPERN qualified nurses may administer or supply medicines approved by the Minister for Health, according to the health management protocols contained in the Primary Clinical Care Manual. We currently have three RIPERN qualified nurses, and a further two nurses working towards completion. The RIPERN nurses will complement our existing clinical team’s capacity to provide urgent and primary healthcare to people who make unplanned visits to the Urgent Care Centre.
New Strategic Plan for 2013-15
Following consultation with our community, consumers and staff, the Board of Management at Nathalia District Hospital has developed a Strategic Plan to lead the health service for the next three years. This follows a review of the organisation’s vision, mission and values in early 2012.
The new Strategic Plan has six strategic directions to guide our progress and development over the next three years.
Increased Consumer Involvement through the Discharge Planning Process
Following feedback through the Victorian Patient Satisfaction Monitor that patients do not feel they are sufficiently involved in their care planning, a new discharge planning process has been developed that is patient driven. With support from clinical staff, the patient plans their discharge, identifying any area they may require assistance or support for. The patient takes ownership of the plan they are developing.
Staff meet with the patient each day and provide additional information to support the plan if required, such as discharge information on current medication and their side effects, additional information about the patient’s illness or further referrals to other services.

21N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Disclosure Index The annual report of the Nathalia District Hospital is prepared in accordance with all relevant Victorian legislation. This index has been prepared to facilitate identification of the Department’s compliance with statutory disclosure requirements.
Legislation Requirement Page Reference
Ministerial DirectionsReport of OperationsCharter and purposeFRD 22C Manner of establishment and the relevant Ministers 1FRD 22C Objectives, functions, powers and duties 2FRD 22C Nature and range of services provided 2
Management and structureFRD 22C Organisational structure 8
Financial and other informationFRD 10 Disclosure index 19FRD 11 Disclosure of ex-gratia payments 68FRD 15B Executive officer disclosures 67FRD 21B Responsible person and executive officer disclosures 67FRD 22C Application and operation of Freedom of Information Act 1982 11FRD 22C Compliance with building and maintenance provisions of Building Act 1993 11FRD 22C Details of consultancies over $100,000 10FRD 22C Details of consultancies under $100,000 10FRD 22C Major changes or factors affecting performance 13FRD 22C Occupational health and safety 10FRD 22C Operational and budgetary objectives and performance against objectives 13FRD 22C Significant changes in financial position during the year 13FRD 22C Statement of availability of other information 12FRD 22C Statement on National Competition Policy 11FRD 22C Subsequent events 13FRD 22C Summary of the financial results for the year 13FRD 22C Workforce Data Disclosures including a statement on the application of employment
and conduct principles 9FRD 25 Victorian Industry Participation Policy disclosures 12SD 4.2(j) Sign-off requirements Inside CoverSD 3.4.13 Attestation on Data Integrity 17SD 4.5.5.1 Attestation on Insurance 17SD 4.5.5 Attestation on Compliance with Australian/New Zealand Risk Management Standard 17
Financial Statements Financial statements required under Part 7 of the FMASD 4.2(a) Statement of changes in equity 27SD 4.2(b) Operating statement 25SD 4.2(b) Balance sheet 26SD 4.2(b) Cash flow statement 28
Other requirements under Standing Directions 4.2SD 4.2(a) Compliance with Australian accounting standards and other authoritative pronouncements 29SD 4.2(c) Accountable officer’s declaration 24SD 4.2(c) Compliance with Ministerial Directions 29SD 4.2(d) Rounding of amounts 31
LegislationFreedom of Information Act 1982 11Victorian Industry Participation Policy Act 2003 12Building Act 1993 11Financial Management Act 1994 29

22 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
This page has been left blank intentionally

23N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Nathalia District
Hospital
ANNUAL FINANCIAL REPORT
2012/13
n a t h a l i a D i s t r i C t h o s p i t a l - a n n u a l r e p o r t 2 0 1 2 / 1 3
24 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3

25N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3

26 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
We certify that the attached financial statements for Nathalia District Hospital have been prepared in accordance with Standing Direction 4.2 of the Financial Management Act 1994, applicable Financial Reporting Directions, Australian Accounting Standards, Australian Accounting Interpretations and other mandatory professional reporting requirements.
We further state that, in our opinion, the information set out in the comprehensive operating statement, balance sheet, statement of changes in equity, cash flow statement and notes to and forming part of the financial statements, presents fairly the financial transactions during the year ended 30 June 2013 and the financial position of Nathalia District Hospital at 30 June 2013.
At the time of signing, we are not aware of any circumstance which would render any particulars included in the financial statements to be misleading or inaccurate.
We authorise the attached financial statements for issue on this day.
Nathalia District Hospital Board member’s, accountable
officer’s and chief finance & accounting officer’s declaration
Shaun Andrew Eldridge Chief Finance & Accounting Officer
Shepparton 26 August 2013
Dale Fraser Accountable Officer
Shepparton 26 August 2013
Sue Logie Chairperson
Shepparton 26 August 2013

27N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Nathalia District HospitalComprehensive Operating StatementFor the Financial Year Ended 30 June 2013
Note
Total2013
$
Total2012
$
Revenue From Operating Activities 2 5,927,933 5,587,461
Revenue From Non-Operating Activities 2 96,501 110,478
Employee Expenses 3 (4,181,342) (3,924,858)
Non Salary Labour Costs 3 (526,811) (593,233)
Supplies and Consumables 3 (262,403) (239,317)
Other Expenses 3 (1,089,233) (926,127)
Net Result Before Capital & Specific Items (35,355) 14,404
Capital Purpose Income 2 203,228 150,200
Depreciation 4 (592,112) (642,146)
Finance Costs 3 - (1,641)
Expenditure Using Capital Purpose Income 3 (2,205) (17,333)
Share Adjustment in Hume Rural Health Alliance Joint Venture 3 (1,194) -
Net Result for the Year (427,638) (496,516)
Comprehensive Result (427,638) (496,516)
This statement should be read in conjunction with the accompanying notes

28 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Nathalia District HospitalBalance SheetAs At 30 June 2013
Note
Total2013
$
Total2012
$Current AssetsCash and Cash Equivalents 5 2,445,130 2,137,267 Receivables 6 203,269 157,097 Other Assets 7 20,803 26,486 Total Current Assets 2,669,202 2,320,850
Non Current AssetsReceivables 6 173,372 103,010 Property, Plant & Equipment 8 15,167,553 15,630,103 Total Non Current Assets 15,340,925 15,733,113
TOTAL ASSETS 18,010,127 18,053,963
Current LiabilitiesPayables 9 522,934 465,499 Provisions 10 912,836 905,880 Other Liabilities 12 288,263 56,931 Total Current Liabilities 1,724,033 1,428,310
Non Current LiabilitiesProvisions 10 176,069 87,990 Total Non Current Liabilities 176,069 87,990
TOTAL LIABILITIES 1,900,102 1,516,300
NET ASSETS 16,110,025 16,537,663
EQUITYProperty, Plant and Equipment Revaluation Surplus 13a 239,977 239,977 General Purpose Surplus 13a 1,179,136 1,032,130 Restricted Specific Purpose Surplus 13a 162,466 162,466 Contributed Capital 13b 11,103,968 11,103,968 Accumulated Surpluses/(Deficits) 13c 3,424,478 3,999,122 TOTAL EQUITY 16,110,025 16,537,663
Contingent Assets and Contingent Liabilities 20
This statement should be read in conjunction with the accompanying notes
29N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
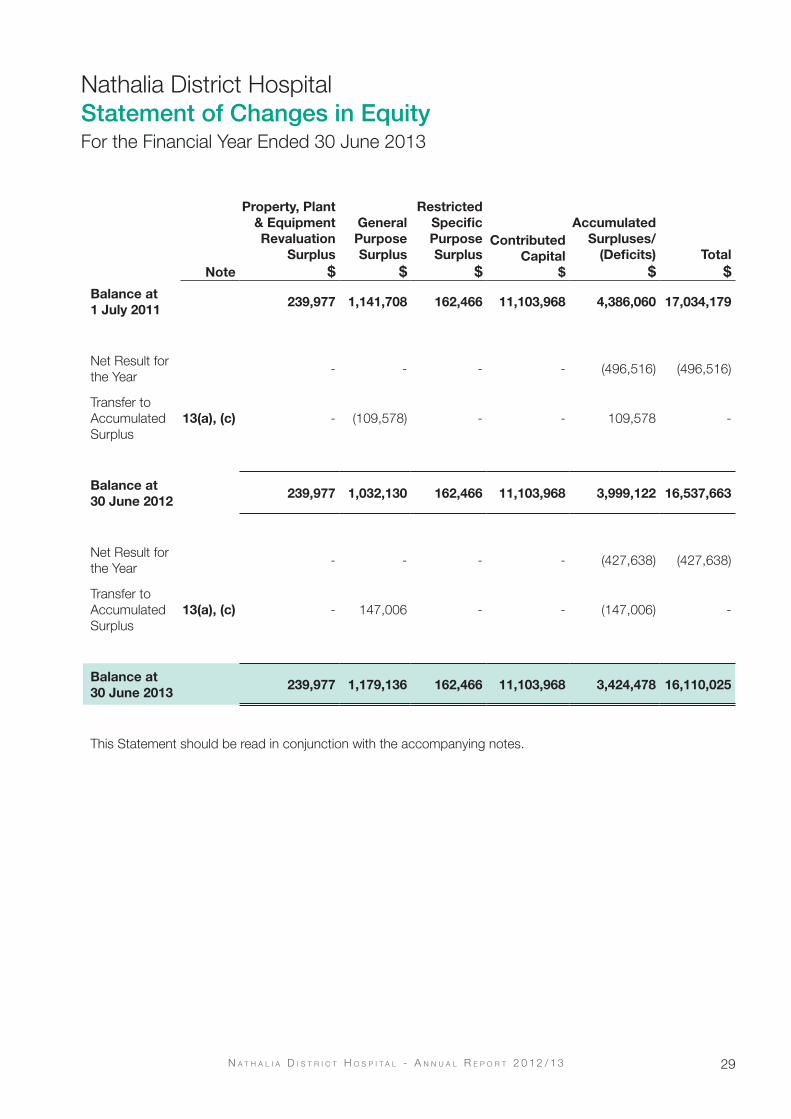
Nathalia District HospitalStatement of Changes in EquityFor the Financial Year Ended 30 June 2013
Note
Property, Plant& EquipmentRevaluation
Surplus $
GeneralPurposeSurplus
$
RestrictedSpecificPurposeSurplus
$
Contributed Capital
$
AccumulatedSurpluses/
(Deficits) $
Total $
Balance at 1 July 2011
239,977 1,141,708 162,466 11,103,968 4,386,060 17,034,179
Net Result for the Year
- - - - (496,516) (496,516)
Transfer to Accumulated Surplus
13(a), (c) - (109,578) - - 109,578 -
Balance at 30 June 2012
239,977 1,032,130 162,466 11,103,968 3,999,122 16,537,663
Net Result for the Year
- - - - (427,638) (427,638)
Transfer to Accumulated Surplus
13(a), (c) - 147,006 - - (147,006) -
Balance at 30 June 2013
239,977 1,179,136 162,466 11,103,968 3,424,478 16,110,025
This Statement should be read in conjunction with the accompanying notes.
Note
Total2013
$
Total2012
$Current AssetsCash and Cash Equivalents 5 2,445,130 2,137,267 Receivables 6 203,269 157,097 Other Assets 7 20,803 26,486 Total Current Assets 2,669,202 2,320,850
Non Current AssetsReceivables 6 173,372 103,010 Property, Plant & Equipment 8 15,167,553 15,630,103 Total Non Current Assets 15,340,925 15,733,113
TOTAL ASSETS 18,010,127 18,053,963
Current LiabilitiesPayables 9 522,934 465,499 Provisions 10 912,836 905,880 Other Liabilities 12 288,263 56,931 Total Current Liabilities 1,724,033 1,428,310
Non Current LiabilitiesProvisions 10 176,069 87,990 Total Non Current Liabilities 176,069 87,990
TOTAL LIABILITIES 1,900,102 1,516,300
NET ASSETS 16,110,025 16,537,663
EQUITYProperty, Plant and Equipment Revaluation Surplus 13a 239,977 239,977 General Purpose Surplus 13a 1,179,136 1,032,130 Restricted Specific Purpose Surplus 13a 162,466 162,466 Contributed Capital 13b 11,103,968 11,103,968 Accumulated Surpluses/(Deficits) 13c 3,424,478 3,999,122 TOTAL EQUITY 16,110,025 16,537,663
Contingent Assets and Contingent Liabilities 20
This statement should be read in conjunction with the accompanying notes

30 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Nathalia District HospitalCash Flow StatementFor the Financial Year Ended 30 June 2013
Note
Total2013
$
Total2012
$Cash Flows from Operating Activities
Operating Grants from Government 4,077,787 4,069,125
Patient and Resident Fees Received 472,945 400,778
Donations and Bequests Received 63,539 12,388
Interest Received 98,877 110,447
Other Receipts 1,213,571 1,220,458
Total Receipts 5,926,719 5,813,196
Employee Expenses Paid (4,086,306) (3,792,725)
Non Salary Labour Costs (526,811) (593,233)
Payments for Supplies and Consumables (1,441,439) (1,307,025)
GST Received from ATO 134,102 143,733
Total Payments (5,920,455) (5,549,250)
Cash Generated from Operations 6,264 263,946
Capital Grants from Government 29,264 71,211
Residential Accommodation Payments Received 96,704 82,376
Expenditure Using Capital Purpose Income (3,399) (18,974)
Net Cash Flow from/(used in) Operating Activities 14 128,833 398,559
Cash Flows from Investing Activities
Payments for Non Financial Assets (65,407) (216,635)
Proceeds from Sale of Non Financial Assets 13,105 14,182
Proceeds from Sale of Investments - -
Net Cash Flow from/(used in) Investing Activities (52,302) (202,453)
Net Increase/(Decrease) in Cash and Cash Equivalents Held 76,531 196,106
Cash and Cash Equivalents at Beginning of Financial Year 2,080,336 1,884,230
Cash and Cash Equivalents at End of Financial Year 5 2,156,867 2,080,336
This statement should be read in conjunction with the accompanying notes

31N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 1: SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
These annual financial statements represent the audited general purpose financial statements for Nathalia District Hospital for the period ending 30 June 2013. The purpose of the report is to provide users with information about the Health Services’ stewardship of resources entrusted to it.
a. Statement of compliance
These financial statements are general purpose financial statements which have been prepared in accordance with the Financial Management Act 1994 and applicable AASs, which include interpretations issued by the Australian Accounting Standards Board (AASB). They are presented in a manner consistent with the requirements of AASB 101 Presentation of Financial Statements.
The financial statements also comply with relevant Financial Reporting Directions (FRDs) issued by the Department of Treasury and Finance, and relevant Standing Directions (SDs) authorised by the Minister for Finance.
The Health Service is a not-for profit entity and therefore applies the additional Aus paragraphs applicable to “not-for-profit” Health Services under the AASs.
The annual financial statements were authorised for issue by the Board of Nathalia District Hospital on 26th August 2013.
b. Basis of accounting preparation and measurement
Accounting policies are selected and applied in a manner which ensures that the resulting financial information satisfies the concepts of relevance and reliability, thereby ensuring that the substance of the underlying transactions or other events is reported.
The accounting policies set out below have been applied in preparing the financial statements for the year ended 30 June 2013, and the comparative information presented in these financial statements for the year ended 30 June 2012.
The going concern basis was used to prepare the financial statements.
These financial statements are presented in Australian dollars, the functional and presentation currency of the Health Service.
The financial statements, except for cash flow information, have been prepared using the accrual basis of accounting. Under the accrual basis, items are recognised as assets, liabilities, equity, income or expenses when they satisfy the definitions and recognition criteria for those items, that is they are recognised in the reporting period to which they relate, regardless of when cash is received or paid.
The financial statements are prepared in accordance with the historical cost convention, except for:
• Non-current physical assets, which subsequent to acquisition, are measured at a revaluation amount being their fair value at the date of the revaluation less any subsequent accumulated depreciation and subsequent losses. Revaluations are made and are re-assessed with sufficient regularity to ensure that the carrying amounts do not materially differ from their fair values;
• Available-for-sale investments which are measured at fair value with movements reflected in equity until the asset is derecognised (i.e. other comprehensive income – items that may be reclassified subsequent to net result).
Historical cost is based on the fair values of the consideration given in exchange for assets.
In the application of AASs, management is required to make judgments, estimates and assumptions about carrying values of assets and liabilities that are not readily apparent from other sources. The estimates and associated assumptions are based on professional judgements derived from historical experience and various other factors that are believed to be reasonable under the circumstances. Actual results may differ from these estimates.
The estimates and underlying assumptions are reviewed on an ongoing basis. Revisions to accounting estimates are recognised in the period in which the estimate is revised if the revision affects only that period or in the period of the revision, and future periods if the revision affects both current and future periods. Judgements and assumptions made by management in the application of AASs that have significant effects on the financial statements and estimates, with a risk of material adjustments in the subsequent reporting period, relate to:
• The fair value of land, buildings, infrastructure, plant and equipment (refer to Note 1(j);
Nathalia District Hospital Notes to the Financial Statements 30 June 2013
Note
Total2013
$
Total2012
$Cash Flows from Operating Activities
Operating Grants from Government 4,077,787 4,069,125
Patient and Resident Fees Received 472,945 400,778
Donations and Bequests Received 63,539 12,388
Interest Received 98,877 110,447
Other Receipts 1,213,571 1,220,458
Total Receipts 5,926,719 5,813,196
Employee Expenses Paid (4,086,306) (3,792,725)
Non Salary Labour Costs (526,811) (593,233)
Payments for Supplies and Consumables (1,441,439) (1,307,025)
GST Received from ATO 134,102 143,733
Total Payments (5,920,455) (5,549,250)
Cash Generated from Operations 6,264 263,946
Capital Grants from Government 29,264 71,211
Residential Accommodation Payments Received 96,704 82,376
Expenditure Using Capital Purpose Income (3,399) (18,974)
Net Cash Flow from/(used in) Operating Activities 14 128,833 398,559
Cash Flows from Investing Activities
Payments for Non Financial Assets (65,407) (216,635)
Proceeds from Sale of Non Financial Assets 13,105 14,182
Proceeds from Sale of Investments - -
Net Cash Flow from/(used in) Investing Activities (52,302) (202,453)
Net Increase/(Decrease) in Cash and Cash Equivalents Held 76,531 196,106
Cash and Cash Equivalents at Beginning of Financial Year 2,080,336 1,884,230
Cash and Cash Equivalents at End of Financial Year 5 2,156,867 2,080,336
This statement should be read in conjunction with the accompanying notes

32 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
• Superannuation expense (refer to Note 1(g)); and
Actuarial assumptions for employee benefit provisions based on likely tenure of existing staff, patterns of leave claims, future salary movements and future discount rates (refer to Note 1(g)).
c. Reporting entity
The financial statements include all the controlled activities of Nathalia District Hospital. Its principal address is:
36-44 McDonell StreetNathaliaVictoria 3638.
A description of the nature of Nathalia District Hospital’s operations and its principal activities is included in the report of operations, which does not form part of these financial statements.
Objectives and funding
Nathalia District Hospital’s overall objective is to work collaboratively to provide quality health and well-being services for our community, as well as improve the quality of life to Victorians.
Nathalia District Hospital is predominantly funded by accrual based grant funding for the provision of outputs.
d. Principles of consolidation
Nathalia District Hospital does not control any other
entities.
Jointly controlled assets or operations
Interests in jointly controlled assets or operations are not consolidated by Nathalia District Hospital, but are accounted for in accordance with the policy outlined in Note 1(j) Financial Assets.
e. Scope and presentation of financial statements
Fund Accounting
Nathalia District Hospital operates on a fund accounting basis and maintains three funds: Operating, Specific Purpose and Capital Funds. Nathalia District Hospital’s Capital and Specific Purpose Funds include unspent capital donations and receipts from fund-raising activities conducted solely in respect of these funds.
Services Supported By Health Services Agreement and Services Supported By Hospital and Community Initiatives
Activities classified as Services Supported by Health Services Agreement (HSA) are substantially funded by the Department of Health and includes Residential Aged Care Services (RACS) and are also funded from other sources such as the Commonwealth, patients and residents, while Services Supported by Hospital and Community Initiatives (H&CI) are funded by Nathalia District Hospital’s own activities or local initiatives and/or the Commonwealth.
Residential Aged Care Service
Nathalia District Hospital’s Residential Aged Care Service operations are an integral part of the entity and shares its resources. An apportionment of land and buildings has been made based on floor space. The results of the two operations have been segregated based on actual revenue earned and expenditure incurred by each operation in Note 2b to the financial statements.
Nathalia District Hospital’s Residential Aged Care does not have a separate Committee of Management and is substantially funded from
Commonwealth bed-day subsidies.
Comprehensive operating statement
The comprehensive operating statement includes the subtotal entitled ‘net result before capital & specific items’ to enhance the understanding of the financial performance of Nathalia District Hospital. This subtotal reports the result excluding items such as capital grants, assets received or provided free of charge, depreciation, expenditure using capital purpose income and items of an unusual nature and amount such as specific income and expenses. The exclusion of these items is made to enhance matching of income and expenses so as to facilitate the comparability and consistency of results between years and Victorian Public Health Services. The ‘net result before capital & specific items’ is used by the management of Nathalia District Hospital, the Department of Health and the Victorian Government to measure the ongoing operating performance of Health Services.
Capital and specific items, which are excluded from this sub-total, comprise:
• Capital purpose income, which comprises all tied grants, donations and bequests received for the purpose of acquiring non-current assets, such as capital works or plant and equipment. It
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

33N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
also includes donations of plant and equipment (refer Note 1 (g)). Consequently the recognition of revenue as capital purpose income is based on the intention of the provider of the revenue at the time the revenue is provided.
• Depreciation and amortisation, as described in Note 1 (g);
• Finance costs which comprises interest payments payable on the refund of accommodation bonds for residents who have departed the entity’s Residential Aged Care Facilities; and
• Expenditure using capital purpose income, comprises expenditure which either falls below the asset capitalisation threshold or does not meet asset recognition criteria and therefore does not result in the recognition of an asset in the balance sheet, where funding for that
expenditure is from capital purpose income.
Balance sheet
Assets and liabilities are categorised either as current or non-current (non-current being those assets or liabilities expected to be recovered/settled more than 12 months after reporting period), are disclosed in the notes where relevant.
Statement of changes in equity
The statement of changes in equity presents reconciliations of each non-owner and owner changes in equity from opening balance at the beginning of the reporting period to the closing balance at the end of the reporting period. It also shows separately changes due to amounts recognised in the comprehensive result and amounts recognised in other comprehensive income.
Cash flow statement
Cash flows are classified according to whether or not they arise from operating activities, investing activities, or financing activities. This classification is consistent with requirements under AASB 107 Statement of Cash Flows.
Rounding
All amounts shown in the financial statements are expressed to the nearest $1 unless otherwise stated.
Minor discrepancies in tables between totals and sum of components are due to rounding.
f. Income from transactions
Income is recognised in accordance with AASB 118 Revenue and is recognised as to the extent that it is probable that the economic benefits will flow to Nathalia District Hospital and the income can be reliably measured. Unearned income at reporting date is reported as income received in advance.
Amounts disclosed as revenue are, where applicable, net of returns, allowances and duties and taxes.
Government Grants and other transfers of income (other than contributions by owners)
In accordance with AASB 1004 Contributions, government grants and other transfers of income (other than contributions by owners) are recognised as income when the Health Service gains control of the underlying assets irrespective of whether conditions are imposed on the Health Service’s use of the contributions.
Contributions are deferred as income in advance when the Health Service has a present obligation to repay them and the present obligation can be reliably measured.
Indirect Contributions from the Department of Health
• Insurance is recognised as revenue following advice from the Department of Health.
• Long Service Leave (LSL) – Revenue is recognised upon finalisation of movements in LSL liability in line with the arrangements set out in the Metropolitan Health and Aged Care Services Division Hospital Circular 05/2013 (update for 2012-13).
Patient and Resident Fees
Patient fees are recognised as revenue at the time invoices are raised.
Private Practice Fees
Private practice fees are recognised as revenue at the time invoices are raised.
Revenue from commercial activities
Revenue from commercial activities such as commercial laboratory medicine is recognised at the time invoices are raised.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

34 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Donations and Other Bequests
Donations and bequests are recognised as revenue when received. If donations are for a special purpose, they may be appropriated to a surplus, such as the specific restricted purpose surplus.
Interest Revenue
Interest revenue is recognised on a time proportionate basis that takes in account the effective yield of the financial asset.
Sale of investments
The gain/loss on the sale of investments is recognised when the investment is realised.
Fair value of assets and services received free of charge or for nominal consideration
Resources received free of charge or for nominal consideration are recognised at their fair value when the transferee obtains control over them, irrespective of whether restrictions or conditions are imposed over the use of the contributions, unless received from another Health Service or agency as a consequence of a restructuring of administrative arrangements. In the latter case, such transfer will be recognised at carrying value. Contributions in the form of services are only recognised when a fair value can be reliably determined and the service would have been purchased if not received as a donation.
g. Expense recognition
Expenses are recognised as they are incurred and reported in the financial year to which they relate.
Employee expenses
Employee expenses include:
• Wages and salaries;
• Annual leave;
• Sick leave;
• Long service leave; and
• Superannuation expenses which are reported differently depending upon whether employees are members of defined benefit or defined contribution plans.
Defined contribution superannuation plans
In relation to defined contribution (i.e. accumulation) superannuation plans, the associated expense is simply the employer contributions that are paid or payable in respect of employees who are members of these plans during the reporting
period. Contributions to defined contribution superannuation plans are expensed when incurred.
Defined benefit superannuation plans
The amount charged to the comprehensive operating statement in respect of defined benefit superannuation plans represents the contributions made by the Health Service to the superannuation plans in respect of the services of current Health Service staff during the reporting period. Superannuation contributions are made to the plans based on the relevant rules of each plan, and are based upon actuarial advice.
Employees of the Nathalia District Hospital are entitled to receive superannuation benefits and the Nathalia District Hospital contributes to both the defined benefit and defined contribution plans. The defined benefit plan provides benefits based on years of service and final average salary.
The name and details of the major employee superannuation funds and contributions made by the Nathalia District Hospital are as follows:
Depreciation
All infrastructure assets, buildings, plant and equipment and other non-financial physical assets that have finite useful lives are depreciated. Depreciation begins when the asset is available for use, which is when it is in the location and condition necessary for it to be capable of operating in a manner intended by management.
Depreciation is generally calculated on a straight line basis, at a rate that allocates the asset value, less any estimated residual value over its estimated useful life. Estimates of the remaining useful lives and depreciation method for all assets are reviewed
Fund
Contributions Paid or Payable for the year
2013 $
2012 $
Defined benefit plans:
Health Super – revised and new
5,236 7,028
Defined contribution plans:
Health Super 230,811 220,384
Hesta Super 86,740 86,901Total 322,787 314,313
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

35N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
at least annually, and adjustments made where appropriate. This depreciation charge is not funded by the Department of Health. Assets with a cost in excess of $1,000 are capitalised and depreciation has been provided on depreciable assets so as to allocate their cost or valuation over their estimated useful lives.
The following table indicates the expected useful lives of non-current assets on which the depreciation charges are based.
Finance Costs
Finance costs are recognised as expenses in the period in which they are incurred. Finance costs include:
• interest on the refund of Residential Aged Care accommodation bonds.
Grants and other transfers
Grants and other transfers to third parties (other than contribution to owners) are recognised as an expense in the reporting period in which they are paid or payable. They include transactions such as: grants, subsidies and personal benefit payments made in cash to individuals.
Other operating expenses
Other operating expenses generally represent the day-to-day running costs incurred in normal
operations and include:
Supplies and consumables
Supplies and services costs which are recognised as an expense in the reporting period in which they are incurred. The carrying amounts of any inventories held for distribution
are expensed when distributed.
Bad and doubtful debts
Refer to Note 1 (j) Impairment of financial assets.
Fair value of assets, services and resources provided free of charge or for nominal consideration
Contributions of resources provided free of charge or for nominal consideration are recognised at their fair value when the transferee obtains control over them, irrespective of whether restrictions or conditions are imposed over the use of the contributions, unless received from another agency as a consequence of a restructuring of administrative arrangements. In the latter case, such a transfer will be recognised at its carrying value.
Contributions in the form of services are only recognised when a fair value can be reliably determined and the services would have been purchased if not donated.
h. Other comprehensive income
Other comprehensive income measures the change in volume or value of assets or liabilities that do not result from transactions.
Net gain/(loss) on non-financial assets
Net gain/(loss) on non-financial assets and liabilities includes realised and unrealised gains and losses
as follows:
Revaluation gains/(losses) of non-financial physical assets
Refer to Note 1(j) Revaluations of non-financial physical assets.
Disposal of non-financial assets
Any gain or loss on the disposal of non-financial assets is recognised at the date of disposal and is determined after deducting from the proceeds the carrying value of the asset at that time.
Net gain/(loss) on financial instruments
Net gain/(loss) on financial instruments includes:
Realised and unrealised gains and losses from revaluations of financial instruments at fair value;
Impairment and reversal of impairment for financial instruments at amortised cost (refer to Note 1 (j)); and
Disposals of financial assets and derecognition of financial liabilities
2013 2012
Buildings 30 to 40 Years 30 to 40 Years
Plant & Equipment 10 Years 10 Years
Medical Equipment 5 Years 5 Years
Computers & Communications 3 Years 3 Years
Furniture & Fittings 5 Years 5 Years
Motor Vehicles 7 Years 7 Years
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

36 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Revaluations of financial instrument at fair value
Refer to Note 1 (i) Financial instruments.
Other gains/(losses) from other comprehensive income
Other gains/(losses) include:
the revaluation of the present value of the long service leave liability due to changes in the bond interest rates; and
transfer of amounts from the reserves to accumulated surplus or net result due to disposal or derecognition or reclassification
i. Financial instruments
Financial instruments arise out of contractual agreements that give rise to a financial asset of one Health Service and a financial liability or equity instrument of another Health Service. Due to the nature of Nathalia District Hospital’s activities, certain financial assets and financial liabilities arise under statute rather than a contract. Such financial assets and financial liabilities do not meet the definition of financial instruments in AASB 132 Financial Instruments: Presentation. For example, statutory receivables arising from taxes, fines and penalties do not meet the definition of financial instruments as they do not arise under contract.
Where relevant, for note disclosure purposes, a distinction is made between those financial assets and financial liabilities that meet the definition of financial instruments in accordance with AASB 132 and those that do not.
The following refers to financial instruments unless otherwise stated.
Categories of non-derivative financial instruments
Receivables
Receivables are financial instrument assets with fixed and determinable payments that are not quoted on an active market. These assets are initially recognised at fair value plus any directly attributable transaction costs. Subsequent to initial measurement, receivables are measured at amortised cost using the effective interest method, less any impairment.
Receivables category includes trade receivables and other receivables, but not statutory receivables.
Financial liabilities at amortised cost
Financial instrument liabilities are initially recognised on the date they are originated. They are initially measured at fair value plus any directly attributable transaction costs. Subsequent to initial recognition, these financial instruments are measured at amortised cost with any difference between the initial recognised amount and the redemption value being recognised in profit and loss over the period of the interest-bearing liability, using the effective interest rate method.
Financial instrument liabilities measured at amortised cost include all of the Health Service’s contractual payables, deposits held and advances received.
j. Assets
Cash and Cash Equivalents
Cash and cash equivalents comprise cash on hand and cash at bank, deposits at call and highly liquid investments with an original maturity of three months or less, which are held for the purpose of meeting short term cash commitments rather than for investment purposes, which are readily convertible to known amounts of cash and are subject to insignificant risk of changes in value.
Receivables
Receivables consist of:
• contractual receivables, which includes mainly debtors in relation to goods and services and accrued investment income; and
• statutory receivables, which includes predominantly amounts owing from the Victorian Government and Goods and Services Tax (“GST”) input tax credits recoverable.
Receivables that are contractual are classified as financial instruments and categorised as receivables. Statutory receivables are recognised and measured similarly to contractual receivables (except for impairment), but are not classified as financial instruments because they do not arise from a contract.
Trade debtors are carried at nominal amounts due and are due for settlement within 30 days from the date of recognition. Collectability of debts is reviewed on an ongoing basis, and debts which are known to be uncollectible are written off. A provision for doubtful debts is recognised when there is objective evidence that the debts may not be collected and bad debts are written off when identified.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

37N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Property, plant and equipment
All non-current physical assets are measured initially at cost and subsequently revalued at fair value less accumulated depreciation and impairment. Where an asset is acquired for no or nominal cost, the cost is its fair value at the date of acquisition. Assets transferred as part of a merger/machinery of government are transferred at their carrying amount.
Crown land is measured at fair value with regard to the property’s highest and best use after due consideration is made for any legal or constructive restrictions imposed on the asset, public announcements or commitments made in relation to the intended use of the asset. Theoretical opportunities that may be available in relation to the asset(s) are not taken into account until it is virtually certain that any restrictions will no longer apply.
Land and buildings are recognised initially at cost and subsequently measured at fair value less accumulated depreciation and impairment.
Plant, equipment and vehicles are recognised initially at cost and subsequently measured at fair value less accumulated depreciation and impairment. Depreciated historical cost is generally a reasonable proxy for fair value because of the short lives of the assets concerned.
Revaluations of non-current physical assets
Non-current physical assets are measured at fair value and are revalued in accordance with FRD 103D Non-current physical assets. This revaluation process normally occurs at least every five years, based upon the asset’s Government Purpose Classification, but may occur more frequently if fair value assessments indicate material changes in values. Independent valuers are used to conduct these scheduled revaluations and any interim revaluations are determined in accordance with the requirements of the FRDs. Revaluation increments or decrements arise from differences between an asset’s carrying value and fair value.
Revaluation increments are recognised in ‘other comprehensive income’ and are credited directly to the asset revaluation surplus, except that, to the extent that an increment reverses a revaluation decrement in respect of that same class of asset previously recognised as an expense in net result, the increment is recognised as income in the net result.
Revaluation decrements are recognised in ‘other comprehensive income’ to the extent that a
credit balance exists in the asset revaluation surplus in respect of the same class of property, plant and equipment.
Revaluation increases and revaluation decreases relating to individual assets within an asset class are offset against one another within that class but are not offset in respect of assets in different classes.
Revaluation surplus is not transferred to accumulated funds on derecognition of the relevant asset.
In accordance with FRD 103D, Nathalia District Hospital’s non-current physical assets were assessed to determine whether revaluation of the non-current physical assets was required and did not identify any significant movement that would require a re-valuation.
Prepayments
Other non-financial assets include prepayments which represent payments in advance of receipt of goods or services or that part of expenditure made in one accounting period covering a term extending beyond that period.
Disposal of non-financial assets
Any gain or loss on the sale of non-financial assets is recognised in the comprehensive operating statement. Refer to Note 1(h) – ‘comprehensive income’.
Impairment of non-financial assets
All non-financial assets are assessed annually for indications of impairment, except for:
• assets arising from construction contracts.
If there is an indication of impairment, the assets concerned are tested as to whether their carrying value exceeds their possible recoverable amount. Where an asset’s carrying value exceeds its recoverable amount, the difference is written-off as an expense except to the extent that the write-down can be debited to an asset revaluation surplus amount applicable to that same class of asset.
If there is an indication that there has been a change in the estimate of an asset’s recoverable amount since the last impairment loss was recognised, the carrying amount shall be increased to its recoverable amount. This reversal of the impairment loss occurs only to the extent that the asset’s carrying amount does not exceed the carrying amount that would have been determined, net of depreciation or amortisation, if no impairment loss had been recognised in prior years.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

38 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
It is deemed that, in the event of the loss or destruction of an asset, the future economic benefits arising from the use of the asset will be replaced unless a specific decision to the contrary has been made. The recoverable amount for most assets is measured at the higher of depreciated replacement cost and fair value less costs to sell. Recoverable amount for assets held primarily to generate net cash inflows is measured at the higher of the present value of future cash flows expected to be obtained from the asset and fair value less costs to sell.
Investments in jointly controlled assets and operations
In respect of any interest in jointly controlled assets, Nathalia District Hospital recognises in the financial statements:
• its share of jointly controlled assets;
• any liabilities that it had incurred;
• its share of liabilities incurred jointly by the joint venture;
• any income earned from the selling or using of its share of the output from the joint venture; and
• any expenses incurred in relation to being an investor in the joint venture.
For jointly controlled operations, Nathalia District Hospital recognises:
• the assets that it controls;
• the liabilities that it incurs;
• expenses that it incurs; and
• the share of income that it earns from selling outputs of the joint venture.
Impairment of financial assets
At the end of each reporting period Nathalia District Hospital assesses whether there is objective evidence that a financial asset or group of financial asset is impaired. All financial instrument assets, except those measured at fair value through profit or loss, are subject to annual review for impairment.
Receivables are assessed for bad and doubtful debts on a regular basis. Bad debts considered as written off and allowances for doubtful receivables are expensed. Bad debt written off by mutual consent and the allowance for doubtful debts are classified as ‘other comprehensive income’ in the net result.
The amount of the allowance is the difference between the financial asset’s carrying amount and the present value of estimated future cash flows, discounted at the effective interest rate.
k. Liabilities
Payables
Payables consist of:
• contractual payables which consist predominantly of accounts payable representing liabilities for goods and services provided to the Health Service prior to the end of the financial year that are unpaid, and arise when the Health Service becomes obliged to make future payments in respect of the purchase of those goods and services. The normal credit terms for accounts payable are usually Nett 30 days.
• statutory payables, such as goods and services tax and fringe benefits tax payables.
Contractual payables are classified as financial instruments and are initially recognised at fair value, and then subsequently carried at amortised cost. Statutory payables are recognised and measured similarly to contractual payables, but are not classified as financial instruments and not included in the category of financial liabilities at amortised cost, because they do not arise from a contract.
Provisions
Provisions are recognised when the Health Service has a present obligation, the future sacrifice of economic benefits is probable, and the amount of the provision can be measured reliably.
The amount recognised as a liability is the best estimate of the consideration required to settle the present obligation at reporting date, taking into account the risks and uncertainties surrounding the obligation. Where a provision is measured using the cash flows estimated to settle the present obligation, its carrying amount is the present value of those cash flows, using a discount rate that reflects the time value of money and risks specific to the provision.
When some or all of the economic benefits required to settle a provision are expected to be received from a third party, the receivable is recognised as an asset if it is virtually certain that recovery will be received and the amount of the receivable can be measured reliably.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

39N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Employee benefits
This provision arises for benefits accruing to employees in respect of wages and salaries, annual leave and long service leave for services rendered to the reporting date.
Wages and salaries, annual leave, sick leave and accrued days off
Liabilities for wages and salaries, including non-monetary benefits, annual leave, accumulating sick leave and accrued days off which are expected to be settled within 12 months of the reporting date are recognised in the provision for employee benefits in respect of employee’s services up to the reporting date, and are classified as current liabilities and measured at their nominal values.
Those liabilities that are not expected to be settled within 12 months are also recognised in the provision for employee benefits as current liabilities, but are measured at present value of the amounts expected to be paid when the liabilities are settled using the remuneration rate expected to apply at the time of settlement.
Long service leave The liability for long service leave (LSL) is recognised in the provision for employee benefits.
Current liability – unconditional LSL (representing 10 or more years of continuous service) is disclosed in the notes to the financial statements as a current liability even where Nathalia District Hospital does not expect to settle the liability within 12 months because it will not have the unconditional right to defer the settlement of the entitlement should an employee take leave within 12 months.
The components of this current LSL liability are measured at:
• present value – component that Nathalia District Hospital does not expect to settle within 12 months; and
• nominal value – component that Nathalia District Hospital expects to settle within 12 months.
Non-current liability – conditional LSL (representing less than 10 years of continuous service) is disclosed as a non-current liability. There is an unconditional right to defer the settlement of the entitlement until the employee has completed the requisite years of service. Conditional LSL is required to be measured at present value.
Consideration is given to expected future wage and salary levels, experience of employee departures and periods of service. Expected future payments are discounted using interest rates of Commonwealth Government guaranteed securities in Australia.
Termination benefits
Termination benefits are payable when employment is terminated before the normal retirement date or when an employee accepts voluntary redundancy in exchange for these benefits.
Liabilities for termination benefits are recognised when a detailed plan for the termination has been developed and a valid expectation has been raised with those employees affected that the terminations will be carried out. The liabilities for termination benefits are recognised in other creditors unless the amount or timing of the payments is uncertain, in which case they are recognised as a provision.
On-costs
Employee benefit on-costs, such as workers compensation and superannuation, are recognised together with provisions for employee benefits.
Superannuation liabilities
Nathalia District Hospital does not recognise any unfunded defined benefit liability in respect of the superannuation plans because the Health Service has no legal or constructive obligation to pay future benefits relating to its employees, its only obligation is to pay superannuation contributions as they fall due.
l. Equity
Contributed capital
Consistent with Australian Accounting Interpretation 1038 Contributions by Owners Made to Wholly-Owned Public Sector Entities and FRD 119 Contributions by Owners, appropriations for additions to the net asset base have been designated as contributed capital. Other transfers that are in the nature of contributions or distributions that have been designated as contributed capital are also treated as contributed capital.
Property, plant & equipment revaluation surplus
The asset revaluation surplus is used to record increments and decrements on the revaluation of non-current physical assets.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

40 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
General purpose surplus
These are accumulated funds of surplus revenue over expenditure from fund raising activities and community support programs.
Specific restricted purpose surplus
A specific restricted purpose surplus is established where the Health Service has possession or title to the funds but has no discretion to amend or vary the restriction and/or condition underlying the funds received.
m. Contingent assets and contingent liabilities
Contingent assets and contingent liabilities are not recognised in the balance sheet, but are disclosed by way of note and, if quantifiable, are measured at nominal value. Contingent assets and contingent liabilities are presented inclusive of GST receivable or payable respectively.
n. Goods and Services Tax (“GST”)
Income, expenses and assets are recognised net of the amount of associated GST, unless the GST incurred is not recoverable from the taxation authority. In this case, the GST payable is recognised as part of the cost of acquisition of the asset or as part of the expense.
Receivables and payables are stated inclusive of the amount of GST receivable or payable. The net amount of GST recoverable from, or payable to, the taxation authority is included with other receivables or payables in the balance sheet.
Cash flows are presented on a gross basis. The GST components of cash flows arising from investing or financing activities which are recoverable from, or payable to the taxation authority, are presented as an operating cash flow.
Commitments for expenditure and contingent assets and liabilities are presented on a gross basis.
o. AASs issued that are not yet effective
Certain new Australian accounting standards have been published that are not mandatory for the 30 June 2013 reporting period. DTF assesses the impact of all these new standards and advises the Health Service of their applicability and early adoption where applicable.
As at 30 June 2013, the following standards and interpretations had been issued by the AASB but were not yet effective. They become effective for the first financial statements for reporting periods commencing after the stated operative dates as detailed in the table below. Nathalia District Hospital has not and does not intend to adopt these standards early
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

41N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Standard/ Interpretation
Summary Applicable for Annual Reporting periods beginning on
Impact on Public Sector Entity Financial Statements
AASB 9 Financial instruments
This standard simplifies requirements for the classification and measurement of financial assets resulting from Phase 1 of the IASB’s project to replace IAS 39 Financial Instruments: Recognition and Measurement (AASB 139 Financial Instruments: Recognition and Measurement).
1 Jan 2015 Subject to AASB’s further modifications to AASB 9, together with the anticipated changes resulting from the staged projects on impairments and hedge accounting, details of impacts will be assessed.
AASB 10 Consolidated Financial Statements
This Standard forms the basis for determining which entities should be consolidated into an entity’s financial statements. AASB 10 defines ‘control’ as requiring exposure or rights to variable returns and the ability to affect those returns through power over an investee, which may broaden the concept of control for public sector entities. The AASB has issued an exposure draft ED 238 Consolidated Financial Statements – Australian Implementation Guidance for Not-for-Profit Entities that explains and illustrates how the principles in the Standard apply from the perspective of not-for-profit entities in the private and public sectors.
1 Jan 2014 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date. Subject to AASB’s final deliberations on ED 238 and any modifications made to AASB 10 for not-for-profit entities, the entity will need to re-assess the nature of its relationships with other entities, including those that are currently not consolidated.
AASB 11 Joint Arrangements
This Standard deals with the concept of joint control, and sets out a new principles-based approach for determining the type of joint arrangement that exists and the corresponding accounting treatment. The new categories of joint arrangements under AASB 11 are more aligned to the actual rights and obligations of the parties to the arrangement.
1 Jan 2014 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date. Subject to AASB’s final deliberations and any modifications made to AASB 11 for not-for-profit entities, the entity will need to assess the nature of arrangements with other entities in determining whether a joint arrangement exists in light of AASB 11.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

42 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Standard / Interpretation
Summary Applicable for annual reporting periods beginning on
Impact on public sector entity financial statements
AASB 13 Fair Value Measurement
This Standard outlines the requirements for measuring the fair value of assets and liabilities and replaces the existing fair value definition and guidance in other AASs. AASB 13 includes a ‘fair value hierarchy’ which ranks the valuation technique inputs into three levels using unadjusted quoted prices in active markets for identical assets or liabilities; other observable inputs; and unobservable inputs.
1 Jan 2013 Disclosure for fair value measurements using unobservable inputs are relatively onerous compared to disclosure for fair value measurements using observable inputs. Consequently, the Standard may increase the disclosures for public sector entities that have assets measured using depreciated replacement cost.
AASB 119 Employee Benefits
In this revised Standard for defined benefit superannuation plans, there is a change to the methodology in the calculation of superannuation expenses, in particular there is now a change in the split between superannuation interest expense (classified as transactions) and actuarial gains and losses (classified as ‘Other economic flows – other movements in equity’) reported on the comprehensive operating statement.
1 Jan 2013 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date. While the total superannuation expense is unchanged, the revised methodology is expected to have a negative impact on the net result from transactions of the general government sector and for those few Victorian public sector entities that report superannuation defined benefit plans.
AASB 128 Investments in Associates and Joint Ventures
This revised Standard sets out the requirements for the application of the equity method when accounting for investments in associates and joint ventures.
1 Jan 2014 Not-for-profit entities are not permitted to apply this Standard prior to the mandatory application date. The AASB is assessing the applicability of principles in AASB 128 in a not-for-profit context. As such, impact will be assessed after the AASB’s deliberation.
AASB 1053 Application of Tiers of Australian Accounting Standards
This Standard establishes adifferential financial reportingframework consisting of twotiers of reporting requirementsfor preparing general purposefinancial statements.
1 Jan 2013 The Victorian Government is currently considering the impacts of Reduced Disclosure Requirements (RDRs) for certain public sector entities and has not decided if RDRs will be implemented in the Victorian public sector.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

43N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
p. Category groups
Nathalia District Hospital has used the following category groups for reporting purposes for the current and previous financial years.
Admitted Patient Services (Admitted Patients) comprises all recurrent health revenue/expenditure on admitted patient services, where services are delivered in public hospitals.
Aged Care comprises revenue/expenditure from
Home and Community Care (HACC) programs and
Allied Health and support services.
Primary Health comprises revenue/expenditure
for Community Health Services including health
promotion and counselling, physiotherapy, speech
therapy, podiatry and occupational therapy.
Residential Aged Care comprises those
Commonwealth-licensed residential aged care
services in receipt of supplementary funding from DH.
Other Services excluded from Australian Health
Care Agreement (AHCA) (Other) comprises
revenue/expenditure for services not separately
classified above, including Public Health Services.
Standard / Interpretation
Summary Applicable for annual reporting periods beginning on
Impact on public sector entity financial statements
AASB 1055 Budgetary Reporting
AASB 1055 extends the scope of budgetary reporting that is currently applicable for the whole of government and general government sector (GGS) to NFP entities within the GGS, provided that these entities present separate budget to the parliament.
1 July 2014 This Standard is not applicable as no budget disclosure is required.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

44 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 2: REVENUE
Revenue from Operating Activities
HSA2013
$
HSA2012
$
H&CI2013
$
H&CI2012
$
Total2013
$
Total2012
$Government GrantsDepartment of Health 2,897,592 2,752,825 - - 2,897,592 2,752,825 Commonwealth Government:Residential Aged Care Subsidy 1,176,238 1,200,544 - - 1,176,238 1,200,544 Total Government Grants 4,073,830 3,953,369 - - 4,073,830 3,953,369
Indirect Contributions by Department of HealthInsurance 8,619 19,996 - - 8,619 19,996 Long Service Leave 70,362 (18,471) - - 70,362 (18,471)Total Indirect Contributions by Department of Health
78,981 1,525 - - 78,981 1,525
Patient and Resident FeesPatient & Resident Fees (Refer Note 2b)
117,418 115,696 - - 117,418 115,696
Residential Aged Care (Refer Note 2b)
348,206 320,756 - - 348,206 320,756
Total Patient and Resident Fees 465,624 436,452 - - 465,624 436,452
Commercial Activities & Specific Purpose FundsMedical Clinic - - 899,459 927,326 899,459 927,326 Caféteria and Catering - - 52,854 43,511 52,854 43,511 Rental Properties - - 15,936 23,605 15,936 23,605 Total Commercial Activities & Specific Purpose Funds
- - 968,249 994,442 968,249 994,442
Donations & Bequests 12,539 12,388 51,000 - 63,539 12,388 Other Revenue from Operating Activities 277,710 189,285 - - 277,710 189,285
Total Revenue from Operating Activities 4,908,684 4,593,019 1,019,249 994,442 5,927,933 5,587,461
Revenue from Non-Operating ActivitiesInterest 495 900 96,006 109,578 96,501 110,478
Capital Purpose IncomeState Government Capital Grants:
Targeted Capital Works and Equipment - - 22,853 - 22,853 - Other Capital Grants - - 6,411 71,211 6,411 71,211
Assets Received Free of Charge (Refer Note 2d)
- - 75,900 - 75,900 -
Net Gain on Disposal of Non-Current Assets (Refer Note 2c)
- - 1,360 (3,387) 1,360 (3,387)
Residential Accommodation Payments (Refer Note 2b)
- - 96,704 82,376 96,704 82,376
Total Capital Purpose Income - - 203,228 150,200 203,228 150,200
Total Revenue (Refer Note 2a) 4,909,179 4,593,919 1,318,483 1,254,220 6,227,662 5,848,139
Indirect contributions by Department of Health: Department of Health makes insurance and long service leave payments on behalf of Nathalia District Hospital. These amounts have been brought to account in determining the operating result for the year by recording them as revenue and expenses.This note relates to revenues above the net result line only, and does not reconcile to comprehensive income.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

45N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 2A: ANALYSIS OF REVENUE BY SOURCE
AdmittedPatients
2013$
ResidentialAged Care
2013$
Aged Care2013
$
PrimaryHealth
2013$
Other2013
$
Total2013
$
Revenue from Services Supported by Health Service Agreement
Government Grants 1,969,503 1,780,431 282,156 - 41,740 4,073,830
Indirect Contributions by Department of Health
8,503 81 35 - 70,362 78,981
Patient and Resident Fees (Refer Note 2b)
68,741 348,306 26,602 21,905 70 465,624
Donations (Non Capital) 12,289 50 - 200 - 12,539
Interest - - - - 495 495
Other Revenue from Operating Activities
99,273 38,430 1,924 6,637 131,446 277,710
Total Revenue From Services Supported By Health Service Agreement
2,158,309 2,167,298 310,717 28,742 244,113 4,909,179
Revenue from Services Supported by Hospital and Community Initiatives
Commercial Activities & Specific Purpose Funds
- - - - 968,249 968,249
Donations (Non Capital) - - - - 51,000 51,000
Interest - - - - 96,006 96,006
Capital Purpose Income (Refer Note 2)
- - - - 203,228 203,228
Total Revenue From Services Supported By Hospital and Community Initiatives
- - - - 1,318,483 1,318,483
Total Revenue 2,158,309 2,167,298 310,717 28,742 1,562,596 6,227,662
Indirect contributions by Department of Health: Department of Health makes insurance and long service leave payments on behalf of Nathalia District Hospital. These amounts have been brought to account in determining the operating result for the year by recording them as revenue and expenses.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013
NOTE 2: REVENUE
Revenue from Operating Activities
HSA2013
$
HSA2012
$
H&CI2013
$
H&CI2012
$
Total2013
$
Total2012
$Government GrantsDepartment of Health 2,897,592 2,752,825 - - 2,897,592 2,752,825 Commonwealth Government:Residential Aged Care Subsidy 1,176,238 1,200,544 - - 1,176,238 1,200,544 Total Government Grants 4,073,830 3,953,369 - - 4,073,830 3,953,369
Indirect Contributions by Department of HealthInsurance 8,619 19,996 - - 8,619 19,996 Long Service Leave 70,362 (18,471) - - 70,362 (18,471)Total Indirect Contributions by Department of Health
78,981 1,525 - - 78,981 1,525
Patient and Resident FeesPatient & Resident Fees (Refer Note 2b)
117,418 115,696 - - 117,418 115,696
Residential Aged Care (Refer Note 2b)
348,206 320,756 - - 348,206 320,756
Total Patient and Resident Fees 465,624 436,452 - - 465,624 436,452
Commercial Activities & Specific Purpose FundsMedical Clinic - - 899,459 927,326 899,459 927,326 Caféteria and Catering - - 52,854 43,511 52,854 43,511 Rental Properties - - 15,936 23,605 15,936 23,605 Total Commercial Activities & Specific Purpose Funds
- - 968,249 994,442 968,249 994,442
Donations & Bequests 12,539 12,388 51,000 - 63,539 12,388 Other Revenue from Operating Activities 277,710 189,285 - - 277,710 189,285
Total Revenue from Operating Activities 4,908,684 4,593,019 1,019,249 994,442 5,927,933 5,587,461
Revenue from Non-Operating ActivitiesInterest 495 900 96,006 109,578 96,501 110,478
Capital Purpose IncomeState Government Capital Grants:
Targeted Capital Works and Equipment - - 22,853 - 22,853 - Other Capital Grants - - 6,411 71,211 6,411 71,211
Assets Received Free of Charge (Refer Note 2d)
- - 75,900 - 75,900 -
Net Gain on Disposal of Non-Current Assets (Refer Note 2c)
- - 1,360 (3,387) 1,360 (3,387)
Residential Accommodation Payments (Refer Note 2b)
- - 96,704 82,376 96,704 82,376
Total Capital Purpose Income - - 203,228 150,200 203,228 150,200
Total Revenue (Refer Note 2a) 4,909,179 4,593,919 1,318,483 1,254,220 6,227,662 5,848,139
Indirect contributions by Department of Health: Department of Health makes insurance and long service leave payments on behalf of Nathalia District Hospital. These amounts have been brought to account in determining the operating result for the year by recording them as revenue and expenses.This note relates to revenues above the net result line only, and does not reconcile to comprehensive income.

46 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 2A: ANALYSIS OF REVENUE BY SOURCE
AdmittedPatients
2012$
ResidentialAged Care
2012$
Aged Care2012
$
PrimaryHealth
2012$
Other2012
$
Total2012
$
Revenue from Services Supported by Health Service Agreement
Government Grants 1,903,721 1,762,329 256,818 - 30,501 3,953,369
Indirect Contributions by Department of Health
17,895 1,303 798 - (18,471) 1,525
Patient and Resident Fees (Refer Note 2b)
73,436 320,756 38,004 4,256 - 436,452
Interest - - - - 900 900
Donations (Non Capital) 11,900 388 - 100 - 12,388
Other Revenue from Operating Activities 50,049 10,229 2,058 4,414 122,535 189,285
Total Revenue From Services Supported By Health Service Agreement
2,057,001 2,095,005 297,678 8,770 135,465 4,593,919
Revenue from Services Supported by Hospital and Community Initiatives
Commercial Activities & Specific Purpose Funds
- - - - 994,442 994,442
Interest - - - - 109,578 109,578
Capital Purpose Income (Refer Note 2) - - - - 150,200 150,200
Total Revenue From Services Supported By Hospital and Community Initiatives
- - - - 1,254,220 1,254,220
Total Revenue 2,057,001 2,095,005 297,678 8,770 1,389,685 5,848,139
Indirect contributions by Department of Health: Department of Health makes insurance and long service leave payments on behalf of Nathalia District Hospital. These amounts have been brought to account in determining the operating result for the year by recording them as revenue and expenses.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013
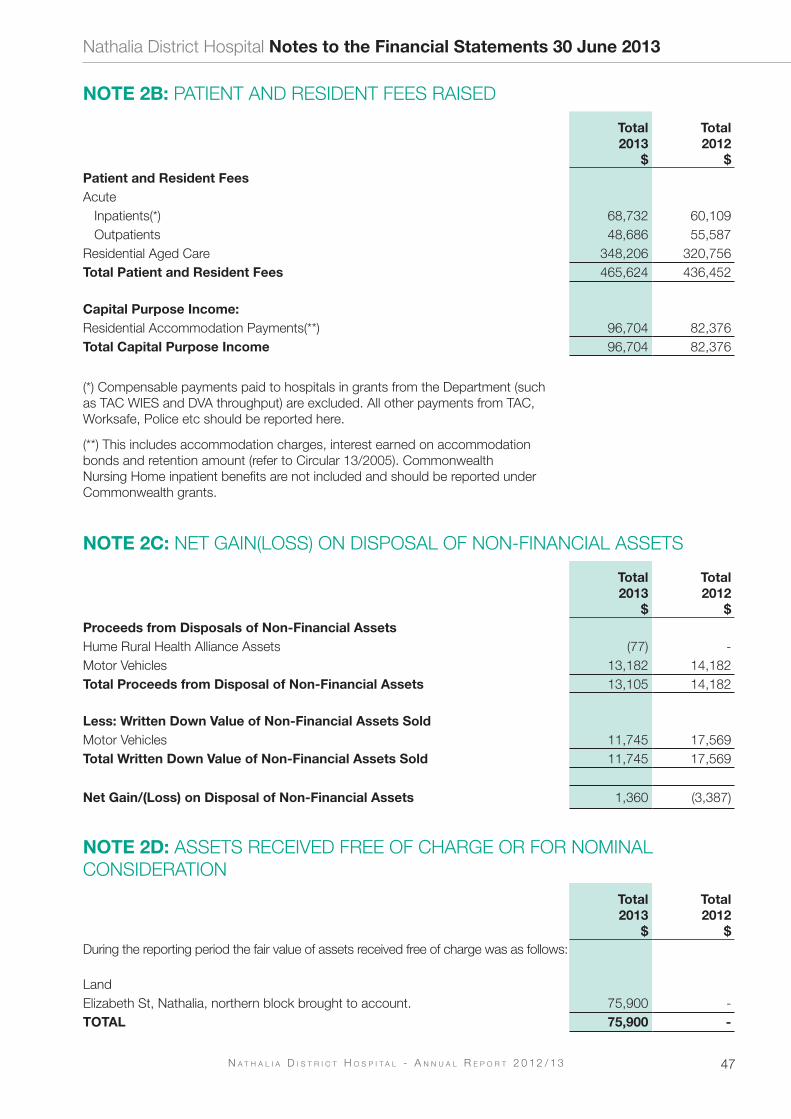
47N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 2B: PATIENT AND RESIDENT FEES RAISED
Total2013
$
Total2012
$Patient and Resident FeesAcute
Inpatients(*) 68,732 60,109 Outpatients 48,686 55,587
Residential Aged Care 348,206 320,756 Total Patient and Resident Fees 465,624 436,452
Capital Purpose Income:Residential Accommodation Payments(**) 96,704 82,376 Total Capital Purpose Income 96,704 82,376
(*) Compensable payments paid to hospitals in grants from the Department (such as TAC WIES and DVA throughput) are excluded. All other payments from TAC, Worksafe, Police etc should be reported here.
(**) This includes accommodation charges, interest earned on accommodation bonds and retention amount (refer to Circular 13/2005). Commonwealth Nursing Home inpatient benefits are not included and should be reported under Commonwealth grants.
NOTE 2C: NET GAIN(LOSS) ON DISPOSAL OF NON-FINANCIAL ASSETS
Total2013
$
Total2012
$Proceeds from Disposals of Non-Financial AssetsHume Rural Health Alliance Assets (77) - Motor Vehicles 13,182 14,182 Total Proceeds from Disposal of Non-Financial Assets 13,105 14,182
Less: Written Down Value of Non-Financial Assets SoldMotor Vehicles 11,745 17,569 Total Written Down Value of Non-Financial Assets Sold 11,745 17,569
Net Gain/(Loss) on Disposal of Non-Financial Assets 1,360 (3,387)
NOTE 2D: ASSETS RECEIVED FREE OF CHARGE OR FOR NOMINAL CONSIDERATION
Total2013
$
Total2012
$During the reporting period the fair value of assets received free of charge was as follows:
LandElizabeth St, Nathalia, northern block brought to account. 75,900 - TOTAL 75,900 -
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

48 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 3: ExPENSES
HSA2013
$
HSA2012
$
H&CI2013
$
H&CI2012
$
Total2013
$
Total2012
$Employee ExpensesSalaries & Wages 3,338,306 3,228,279 321,666 282,285 3,659,972 3,510,564 Long Service Leave 155,495 59,201 7,404 5,287 162,899 64,488 Superannuation 287,742 288,543 28,384 25,770 316,126 314,313 Workcover Premium 32,330 32,583 3,190 2,910 35,520 35,493 Departure Packages 6,825 - - - 6,825 - Total Employee Expenses 3,820,698 3,608,606 360,644 316,252 4,181,342 3,924,858
Non Salary Labour CostsFees for Visiting Medical Officers 98,149 107,521 428,662 485,712 526,811 593,233 Total Non Salary Labour Costs 98,149 107,521 428,662 485,712 526,811 593,233
Supplies & ConsumablesDrug Supplies 40,087 36,976 190 215 40,277 37,191 Medical, Surgical Supplies and Prosthesis 83,895 77,538 10,900 6,839 94,795 84,377 Food Supplies 124,310 114,386 120 115 124,430 114,501 Pathology Supplies 2,901 3,248 - - 2,901 3,248 Total Supplies & Consumables 251,193 232,148 11,210 7,169 262,403 239,317
Other ExpensesTransfer Pricing (105,278) (61,804) 105,278 61,804 - - Insurance Cost Funded by DH 387 8,290 - - 387 8,290 Administrative Expenses 423,052 384,045 46,075 45,654 469,127 429,699 Domestic Services 107,259 97,428 703 1,537 107,962 98,965 Fuel, Light, Power and Water 161,320 134,896 13,517 9,272 174,837 144,168 Motor Vehicle Expenses 32,161 32,452 - - 32,161 32,452 Repairs and Maintenance 137,968 67,718 2,710 6,152 140,678 73,870 Maintenance Contracts 89,828 101,825 1,574 1,530 91,402 103,355 Patient Transport 10,397 6,510 - - 10,397 6,510 Patient & Client Purchased Services 43,083 10,621 - - 43,083 10,621 Bad & Doubtful Debts - - 253 327 253 327 Audit Fees - VAGO Audit of Financial Statements
12,180 10,500 - - 12,180 10,500
Audit Fees - Other 6,766 7,370 - - 6,766 7,370 Total Other Expenses 919,123 799,851 170,110 126,276 1,089,233 926,127
Expenditure using Capital Purpose Income - - 2,205 17,333 2,205 17,333
Interest Expense - Accommodation Bond Refunds
- - - 1,641 - 1,641
Depreciation (Refer Note 4) - - 592,112 642,146 592,112 642,146 Share Adjustment in Hume Rural Health Alliance Joint Venture
- - 1,194 - 1,194 -
Total Expenses 5,089,163 4,748,126 1,566,137 1,596,529 6,655,300 6,344,655
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

49N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 3A: ANALYSIS OF ExPENSES BY SOURCE
AdmittedPatients
2013$
ResidentialAged Care
2013$
Aged Care2013
$
PrimaryHealth
2013$
Other2013
$
Total2013
$
Services Supported By Health Service Agreement
Employee Expenses 783,109 1,367,191 220,627 239,041 1,210,730 3,820,698
Non Salary Labour Costs 98,149 - - - - 98,149
Supplies & Consumables 82,843 40,648 1,957 4,100 121,645 251,193
Other Expenses from Continuing Operations
714,451 918,053 136,838 102,585 (952,804) 919,123
Total Expenses from Services Supported by Health Service Agreement
1,678,552 2,325,892 359,422 345,726 379,571 5,089,163
Services Supported By Hospital & Community Initiatives
Employee Benefits - - - - 360,644 360,644
Non Salary Labour Costs - - - - 428,662 428,662
Supplies & Consumables - - - - 11,210 11,210
Other Expenses from Continuing Operations
- - - - 170,110 170,110
Total Expenses from Services Supported by Hospital and Community Initiatives
- - - - 970,626 970,626
Expenditure Using Capital Purpose Income
Equipment Purchases - - - - 2,205 2,205
Interest Expense on Accommodation Bond Refunds
- - - - 1,194 1,194
Depreciation (Refer Note 4) - - - - 592,112 592,112
Total Expenditure from Services supported by Health Services Agreement and by Hospital and Community Initiatives
- - - - 1,566,137 1,566,137
Total Expenses 1,678,552 2,325,892 359,422 345,726 1,945,708 6,655,300
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

50 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 3A: ANALYSIS OF ExPENSES BY SOURCE
AdmittedPatients
2012$
ResidentialAged Care
2012$
Aged Care2012
$
PrimaryHealth
2012$
Other2012
$
Total2012
$
Services Supported By Health Service Agreement
Employee Expenses 878,638 1,217,203 219,814 254,131 1,038,820 3,608,606
Non Salary Labour Costs 107,521 - - - - 107,521
Supplies & Consumables 77,343 41,970 1,958 135 110,742 232,148
Other Expenses from Continuing Operations
725,469 928,247 136,939 6,271 (997,075) 799,851
Total Expenses from Services Supported by Health Service Agreement
1,788,971 2,187,420 358,711 260,537 152,487 4,748,126
Services Supported By Hospital & Community Initiatives
Employee Expense - - - - 316,252 316,252
Non Salary Labour Costs - - - - 485,712 485,712
Supplies & Consumables - - - - 7,169 7,169
Other Expenses from Continuing Operations
- - - - 126,276 126,276
Total Expenses from Services Supported by Hospital and Community Initiatives
- - - - 935,409 935,409
Expenditure Using Capital Purpose Income
Equipment Purchases - - - - 17,333 17,333
Interest Expense on Accommodation Bond Refunds
- - - - 1,641 1,641
Depreciation (Refer Note 4) - - - - 642,146 642,146
Total Expenditure from Services supported by Health Services Agreement and by Hospital and Community Initiatives
- - - - 1,596,529 1,596,529
Total Expenses 1,788,971 2,187,420 358,711 260,537 1,749,016 6,344,655
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

51N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 3B: ANALYSIS OF ExPENSES BY INTERNALLY MANAGED AND RESTRICTED SPECIFIC PURPOSE FUNDS FOR SERVICES SUPPORTED BY HOSPITAL AND COMMUNITY INITIATIVES
Total2013
$
Total2012
$
Commercial Activities
Medical Clinic 896,659 862,041
Catering Services 52,533 50,851
Rental Properties 21,435 22,517
Total 970,627 935,409
NOTE 4: DEPRECIATION
Total2013
$
Total2012
$
Buildings 386,304 397,049
Computers & Communications 34,027 62,671
Furniture & Fittings 7,543 6,508
Medical Equipment 94,234 92,735
Motor Vehicles 18,171 21,007
Plant & Equipment 11,582 11,164
Non-Medical Equipment 39,753 50,308
Hume Rural Health Alliance Equipment 498 704
Total Depreciation 592,112 642,146
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

52 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 5. CASH AND CASH EQUIVALENTS
For the purposes of the Cash Flow Statement, cash assets includes cash on hand and in banks, and short-term deposits which are readily convertible to cash on hand, and are subject to an insignificant risk of change in value, net of outstanding bank overdrafts.
Total2013
$
Total2012
$
Cash on Hand 500 500
Cash at Bank 540,589 524,106
Short Term Deposits 1,904,041 1,612,661
Total Cash and Cash Equivalents 2,445,130 2,137,267
Represented by:
Total Cash for Health Service Operations (as per Cash Flow Statement) 2,156,867 2,080,336
Cash for Monies Held in Trust
Term Deposits 288,263 56,931
Total Cash and Cash Equivalents 2,445,130 2,137,267
NOTE 6: RECEIVABLES
Current
Total2013
$
Total2012
$
Contractual
Trade Debtors 101,108 39,805
Patient Fees 69,789 77,110
Accrued Investment Income 11,451 13,827
Other Accrued Revenue - 4,836
182,348 135,578
Statutory
GST Receivable 20,921 21,519
Total Current Receivables 203,269 157,097
Non-Current
Statutory
Debtor - Department Human Services Long Service Leave 173,372 103,010
Total Non-Current Receivables 173,372 103,010
Total Receivables 376,641 260,107
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

53N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 7: OTHER ASSETS
Current
Total2013
$
Total2012
$
Prepayments 20,803 26,486
Total Other Assets 20,803 26,486
NOTE 8: PROPERTY, PLANT & EQUIPMENT
Total2013
$
Total2012
$
LandLand at Fair Value 641,148 537,450 Total Land 641,148 537,450
BuildingsBuildings at Fair Value 15,338,630 15,347,716 Less Accumulated Depreciation 1,176,554 790,250 Total Buildings 14,162,076 14,557,466
Plant and EquipmentPlant and Equipment at Fair Value 65,945 56,456 Less Accumulated Depreciation 37,968 26,386 Total Plant and Equipment 27,977 30,070
Motor VehiclesMotor Vehicles at Fair Value 159,238 160,329 Less Accumulated Depreciation 84,162 77,423 Total Motor Vehicles 75,076 82,906
Medical EquipmentMedical Equipment at Fair Value 488,237 476,477 Less Accumulated Depreciation 326,943 232,709 Total Medical Equipment 161,294 243,768
Computers and CommunicationComputers and Communication at Fair Value 199,079 197,485 Less Accumulated Depreciation 197,751 163,724 Total Computers and Communication 1,328 33,761
Non-Medical EquipmentNon-Medical Equipment at Fair Value 211,493 210,272 Less Accumulated Depreciation 147,714 107,961 Total Non-Medical Equipment 63,779 102,311
Furniture and FittingsFurniture and Fittings at Fair Value 59,303 59,303 Less Accumulated Depreciation 24,983 17,440 Total Furniture and Fittings 34,320 41,863
Rural Health Alliance - Share of Plant and Equipment at Fair Value 555 508
TOTAL 15,167,553 15,630,103
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

54 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Nat
halia
Dis
tric
t Hos
pita
l No
tes
to t
he F
inan
cial
Sta
tem
ents
30
June
201
3
NO
TE
8: P
RO
PE
RTY
, PLA
NT
& E
QU
IPM
EN
T (C
ontin
ued)
Rec
onci
liatio
n of
the
carr
ying
am
ount
s of
eac
h cl
ass
of a
sset
at t
he b
egin
ning
and
end
of t
he p
revi
ous
and
curr
ent fi
nanc
ial y
ear
is s
et o
ut b
elow
.
Land
$B
uild
ing
s $
Pla
nt &
Eq
uip
men
t $
Med
ical
Eq
uip
men
t $
Co
mp
uter
s &
Co
mm
unic
atio
n $
Furn
itur
e&
Fit
ting
s $
Mo
tor
Vehi
cles $
No
n M
edic
al
Eq
uip
men
t $
Hum
eR
ural
Hea
lth
Alli
ance $
Tota
l $
Bal
ance
at
1 Ju
ly 2
011
537,
450
14,8
22,9
62
40,
094
298,
050
96,4
32
47,
276
98,
367
131,
340
1,2
12 1
6,07
3,18
3
Add
ition
s-
131,
553
1,1
40
38,
453
-
1,0
95
23,
115
21,
279
-
216,
635
Dis
posa
ls-
- -
-
- -
(17,
569)
-
- (1
7,56
9)
Dep
reci
atio
n (n
ote
4)-
(397
,049
)(1
1,16
4)(9
2,73
5)(6
2,67
1) (
6,50
8)(2
1,00
7)(5
0,30
8) (
704)
(6
42,1
46)
Bal
ance
at
1 Ju
ly 2
012
537,
450
14,5
57,4
66
30,
070
243,
768
33,7
61
41,
863
82,
906
102,
311
508
15,
630,
103
Add
ition
s 7
98
17,
914
9,4
89
11,
760
1,5
94
- 2
2,08
6 1
,221
5
45
65,
407
Dis
posa
ls-
- -
-
- -
(11,
745)
-
- (1
1,74
5)
Net
Tra
nsfe
rs b
etw
een
Cla
sses
27,
000
(27,
000)
Ass
ets
Rec
eive
d Fr
ee o
f Cha
rge
75,
900
- -
-
- -
- -
-
75,
900
Dep
reci
atio
n (n
ote
4)-
(386
,304
)(1
1,58
2)(9
4,23
4)(3
4,02
7) (
7,54
3)(1
8,17
1)(3
9,75
3) (
498)
(5
92,1
12)
Bal
ance
at
30 J
une
2013
641,
148
14,1
62,0
76
27,
977
161,
294
1,3
28
34,
320
75,
076
63,
779
555
15,
167,
553
Land
and
bui
ldin
gs
carr
ied
at
valu
atio
nA
n in
depe
nden
t val
uatio
n of
the
Hea
lth S
ervi
ce's
land
and
bui
ldin
gs w
as p
erfo
rmed
by
the
Valu
er-G
ener
al V
icto
ria to
det
erm
ine
the
fair
valu
e of
the
land
and
bui
ldin
gs.
The
valu
atio
n, w
hich
con
form
s to
Aus
tral
ian
Valu
atio
n S
tand
ards
, was
det
erm
ined
by
refe
renc
e to
the
amou
nts
for
whi
ch a
sset
s co
uld
be e
xcha
nged
bet
wee
n kn
owle
dgea
ble
part
ies
in a
n ar
ms
leng
th tr
ansa
ctio
n. T
he v
alua
tion
was
bas
ed o
n in
depe
nden
t ass
essm
ents
. The
effe
ctiv
e da
te o
f val
uatio
n w
as 3
0th
June
200
9.
Pla
nt a
nd E
qui
pm
ent
carr
ied
at
fair
val
ueA
n in
depe
nden
t val
uatio
n of
the
Hea
lth S
ervi
ce's
maj
or m
edic
al e
quip
men
t was
per
form
ed b
y th
e D
omin
ion
Gro
up to
det
erm
ine
thei
r fa
ir va
lue.
An
inde
pend
ent
valu
atio
n w
as a
lso
perfo
rmed
on
mot
or v
ehic
les
by th
e H
ealth
Ser
vice
's fl
eet m
anag
er W
ebfle
et M
anag
emen
t Ser
vice
s to
det
erm
ine
thei
r fa
ir va
lue.
The
val
uatio
ns,
whi
ch c
onfo
rm to
Aus
tral
ian
Valu
atio
n S
tand
ards
, was
det
erm
ined
by
refe
renc
e to
the
amou
nts
for
whi
ch a
sset
s co
uld
be e
xcha
nged
bet
wee
n kn
owle
dgea
ble
willi
ng
part
ies
in a
n ar
m's
leng
th tr
ansa
ctio
n. T
he v
alua
tions
wer
e ba
sed
on in
depe
nden
t ass
essm
ents
. The
effe
ctiv
e da
te o
f the
val
uatio
ns w
as 3
0th
June
201
0.

55N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 9: PAYABLES
Total2013
$
Total2012
$Current
Contractual
Trade Creditors 234,461 273,789
Capital Creditors - -
Accrued Expenses 170,200 76,591
Income In Advance - Other 45,315 -
449,976 350,380
Statutory
GST Payable 1,443 2,246
FBT Payable - -
Income In Advance - DHS 65,159 112,873
Income In Advance - Other - -
Income In Advance - Commonwealth 6,356 - 72,958 115,119
TOTAL PAYABLES 522,934 465,499
(a) Maturity analysis of payables
Please refer to Note 15c for the ageing analysis of contractual payables
(b) Nature and extent of risk arising from payables
Please refer to note 15c for the nature and extent of risks arising from contractual payables
NOTE 10: PROVISIONS
Total2013
$
Total2012
$Current Provisions
Employee Benefits (i)Unconditional and expected to be settled within 12 months (ii) 409,851 428,793 Unconditional and expected to be settled after 12 months (iii) 427,178 412,873
837,029 841,666 Provisions related to employee benefit on-costsUnconditional and expected to be settled within 12 months (ii) 61,885 51,293 Unconditional and expected to be settled after 12 months (iii) 13,922 12,921
75,807 64,214 Total Current Provisions 912,836 905,880
Non-Current ProvisionsEmployee Benefits (i) 160,476 80,137 Provisions related to employee benefit on-costs 15,593 7,853 Total Non Current Provisions 176,069 87,990
Total Provisions 1,088,905 993,870
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

56 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 10: PROVISIONS (Continued)
Total2013
$
Total2012
$(a) Employee Benefits and Related On-Costs
Current Employee Benefits and Related On-Costs
Accrued Salaries & Wages 69,607 146,985
Accrued Days Off 8,500 7,020
Annual Leave Entitlements 393,629 326,081
Unconditional Long Service Leave Entitlements 441,100 425,794
Non-Current Employee Benefits and Related On-Costs
Conditional Long Service Leave Entitlements 176,069 87,990
Total Employee Benefits and Related on-Costs 1,088,905 993,870
(b) Movement in Provisions
Total2013
$
Total2012
$
Movement in Long Service Leave:
Balance at start of year 513,784 479,675
Provisions made during the year
- Revaluations (9,377) 29,082
- Expense recognising employee service 172,276 35,406
Settlement made during the year (59,514) (30,379)
Balance at end of year 617,169 513,784
(i) Provisions for employee benefits consist of amounts for annual leave and long service leave accrued by employees, not including on-costs.(ii) The amounts disclosed are nominal amounts
(iii) The amounts disclosed are discounted to present value
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

57N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 11: SUPERANNUATION
Employees of the Health Services are entitled to receive superannuation benefits and the Health Services contributes to both defined benefit and defined contribution plans. The defined benefit plan provides benefits based on years of service and final average salary.
The Health Service does not recognise any defined benefit liability in respect of the plan(s) because the entity has no legal or constructive obligation to pay future benefits relating to its employees; its only obligation is to pay superannuation contributions as they fall due. The Department of Treasury and Finance discloses the States' defined benefits liabilities in its disclosure for administered items.
However superannuation contributions paid or payable for the reporting period are included as part of employee benefits in the comprehensive operating statement of the Health Service. The name, details and amounts expense in relation to the major employee superannuation funds and contributions made by the Health Services are as follows:
Total2013
$
Total2012
$Defined Benefit Plans:
First State Super 5,328 7,028
Defined Contribution Plans:
First State Super 230,811 220,384
Hesta Superannuation 86,740 86,901
Other
Total 322,879 314,313
NOTE 12: OTHER LIABILITIES
Total2013
$
Total2012
$Current
Monies Held in Trust
Employee Parental Leave Funds 1,851 832
Accommodation Bonds (Refundable Entrance Fees) 259,570 -
Government Grants - Hume Region Programs 26,842 56,099
Total Current 288,263 56,931
Total Monies Held in Trust
Represented by the following assets:
Cash at Bank 288,263 56,931
Total 288,263 56,931
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

58 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 13: EQUITY
Total2013
$
Total2012
$(a) Surpluses
Property, Plant and Equipment Revaluation Surplus (1)
Balance at the Beginning of the Reporting Period 239,977 239,977
Increase in the Value of Land - -
Increase in the Value of Buildings - -
Balance at the End of the Reporting Period 239,977 239,977
Represented by:
Land 234,487 234,487
Plant & Equipment 5,490 5,490
Total 239,977 239,977
General Purpose Surplus
Balance at the Beginning of the Reporting Period 1,032,130 1,141,708
Transfer to and from Accumulated Surplus 147,006 (109,578)
Balance at the End of the Reporting Period 1,179,136 1,032,130
Restricted Specific Purpose Surplus
Balance at the Beginning of the Reporting Period 162,466 162,466
Transfer to and from Accumulated Surplus - -
Balance at the End of the Reporting Period 162,466 162,466
Total Surpluses 1,581,579 1,434,573
(b) Contributed Capital
Balance at the Beginning of the Reporting Period 11,103,968 11,103,968
Capital Contributions received from Victorian Government - -
Balance at the End of the Reporting Period 11,103,968 11,103,968
(c) Accumulated Surpluses / (Deficits)
Balance at the Beginning of the Reporting Period 3,999,122 4,386,060
Net Result for the Year (427,638) (496,516)
Transfers to and from General Reserves (147,006) 109,578
Transfers to and from Restricted Purpose Reserves - -
Balance at the End of the Reporting Period 3,424,478 3,999,122
Total Equity At End Of Financial Year 16,110,025 16,537,663
(1) The property, plant and equipment asset revaluation reserve arises on the revaluation of property, plant and equipment.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

59N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 14: RECONCILIATION OF NET RESULT FOR THE YEAR TO NET CASH INFLOW/(OUTFLOW) FROM OPERATING ACTIVITIES
Total2013
$
Total2012
$
Net Result for the Period (427,638) (496,516)
Non-cash movements:
Depreciation 592,112 642,146
Assets Received Free of Charge - Other (75,900) -
Movements included in investing and financing activities
Net (Gain)/Loss from Disposal of Non Financial Physical Assets (1,360) 3,387
Movements in assets and liabilities:
Change in Operating Assets and Liabilities
Increase/(Decrease) in Payables 57,435 134,273
Increase/(Decrease) in Provisions 95,035 132,133
(Increase)/Decrease in Other Assets 5,683 (8,648)
(Increase)/Decrease in Receivables (116,534) (8,216)
Net Cash Inflow/(Outflow) from Operating Activities 128,833 398,559
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

60 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 15: FINANCIAL INSTRUMENTS
15(a) Financial Risk Management Objectives and Policies
Nathalia District Hospital's principal financial instruments comprise of:
Cash Assets
Term Deposits
Receivables (excluding statutory receivables)
Payables (excluding statutory Payables)
Details of the significant accounting policies and methods adopted, including the criteria for recognition, the basis of measurement and the basis on which income and expenses are recognised, with respect to each class of financial asset, financial liability and equity instrument are disclosed in note 1 to the financial statements.
The Health Service's main financial risks include credit risk, liquidity risk, interest rate risk and foreign currency risk. The Health Service manages these financial risks in accordance with its financial risk management policy.
The Health Service uses different methods to measure and manage the different risks to which it is exposed. Primary responsibility for the identification and management of financial risks rests with the financial risk management committee of the Health Service.
The main purpose in holding financial instruments is to prudentially manage Nathalia District Hospital's financial risks within the government policy parameters.
Categorisation of Financial Instruments
Financial Assets
CarryingAmount
2013$
CarryingAmount
2012$
Cash and Cash Equivalents 2,445,130 2,137,267
Receivables 182,348 135,578
Total Financial Assets 2,627,478 2,272,845
Financial Liabilities
At Amortised Cost 449,976 350,380
Other Liabilities 288,263 56,931
Total Finanical Liabilities 738,239 407,311
Net holding gain/(loss) on financial instruments by category
Financial Assets
Net HoldingGain/(Loss)
2013$
Net HoldingGain/(Loss)
2012$
Cash and Cash Equivalents (i) 96,501 110,478
Total Financial Assets 96,501 110,478
Total Financial Liabilities - -
(i) For cash and cash equivalents, loans or receivables and available-for-sale financial assets, the net gain or loss is calculated by taking the movement in the fair value of the asset, interest revenue, plus or minus foreign exchange gains or losses arising from revaluation of the financial assets, and minus any impairment recognised in the net result.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

61N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 15: FINANCIAL INSTRUMENTS (Continued)
15(b) Credit Risk
Credit risk arises from the contractual financial assets of Nathalia District Hospital which comprise cash and deposits, non-statutory receivables and available for sale contractual financial assets. Nathalia District Hospital's exposure to credit risk arises from the potential default of a counter party on their contractual obligations resulting in financial loss to Nathalia District Hospital. Credit risk is measured at fair value and is monitored on a regular basis.
Credit risk associated with the Nathalia District Hospital's contractual financial assets is minimal because the main debtor is the Victorian Government. For debtors other than the Government, it is Nathalia District Hospital's policy to only deal with entities with high credit ratings of a minimum Triple-B rating and to obtain sufficient collateral or credit enhancements, where appropriate.
In addition, Nathalia District Hospital does not engage in hedging for its contractual financial assets and mainly obtains contractual financial assets that are on fixed interest, except for cash assets, which are mainly cash at bank. As with the policy for debtors, Nathalia District Hospital's policy is to only deal with banks with high credit ratings.
Provision of impairment for contractual financial assets is recognised when there is objective evidence that Nathalia District Hospital will not be able to collect a receivable. Objective evidence includes financial difficulties of the debtor, default payments, debts which are more than 60 days overdue, and changes in debtor credit ratings.
Except as otherwise detailed in the following table, the carrying amount of contractual financial assets recorded in the financial statements, net of any allowances for losses, represents Nathalia District Hospital's maximum exposure to credit risk without taking account of the value of any collateral obtained.
Credit Quality of contractual financial assets that are neither past due nor impaired
2013
Financial Institutions (AAA credit
rating)$
Other$
Total$
Financial Assets
Cash and Cash Equivalents - 2,445,130 2,445,130
Receivables:
Debtors and Patient Fees - 170,897 170,897
Other Receivables - 11,451 11,451
Total Financial Assets - 2,627,478 2,627,478
2012
Financial Assets
Cash and Cash Equivalents 465,068 1,672,199 2,137,267
Receivables:
Debtors and Patient Fees - 116,915 116,915
Other Receivables - 18,663 18,663
Total Financial Assets 465,068 1,807,777 2,272,845
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

62 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 15: FINANCIAL INSTRUMENTS (Continued)
15(b) Credit Risk (continued)
Ageing Analysis of Financial Assets as at 30 June
Past Due but Not Impaired
$
2013
CarryingAmount
$
Not PastDue and
Not Impaired
$
Less than 1month
$
1-3 Months
$Financial Assets
Cash and Cash Equivalents 2,445,130 2,445,130 - -
Receivables:
Debtors and Patient Fees 170,897 150,478 9,587 10,832
Accrued Revenue 11,451 11,451 - -
Total Financial Assets 2,627,478 2,607,059 9,587 10,832
2012
Financial Assets
Cash and Cash Equivalents 2,137,267 2,137,267 - -
Receivables:
Debtors and Patient Fees 116,915 - 116,915 -
Accrued Revenue 18,663 - 18,663 -
Total Financial Assets 2,272,845 2,137,267 135,578 -
There are no material financial assets which are individually determined to be impaired. Currently Nathalia District Hospital does not hold any collateral as security nor credit enhancements relating to any of its financial assets.
There are no financial assets that have had their terms renegotiated so as to prevent them from being past due or impaired, and they are stated at the carrying amounts as indicated. The ageing analysis table above discloses the ageing only of contractual financial assets that are past due but not impaired.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

63N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 15: FINANCIAL INSTRUMENTS (Continued)15(c) Liquidity Risk
Liquidity risk is the risk that Nathalia District Hospital would be unable to meet its financial obligations as and when they fall due.Nathalia District Hospitals's maximum exposure to liquidity risk is the carrying amounts of financial liabilities as disclosed in the face of the balance sheet.
The following table discloses the contractual maturity analysis for Nathalia District Hospital's financial liabilities.
Maturity Analysis of Financial Liabilities as at 30 June
2013
CarryingAmount
$
NominalAmount
$
Less than 1 month
$
3 Months- 1 Year
$Financial Liabilities
Payables 449,976 449,976 449,976 -
Other Financial Liabilities
- Other 28,693 28,693 1,851 26,842
Total Financial Liabilities 478,669 478,669 451,827 26,842
2012
Financial Liabilities
Payables 350,380 350,380 350,380 -
Other Financial Liabilities
- Other 56,931 56,931 56,931 -
Total Financial Liabilities 407,311 407,311 407,311 -
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

64 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 15: FINANCIAL INSTRUMENTS (Continued)
15(d) Market Risk
Nathalia District Hospital's exposures to market risk are primarily through interest rate risk with only insignificant exposure to foreign currency and other price risks. Objectives, policies and processes used to manage each of these risks are disclosed in the paragraph below.
Currency Risk
Nathalia District Hospital is exposed to insignificant foreign currency risk through its payables relating to purchases of supplies and consumables from overseas. This is because of a limited amount of purchases denominated in foreign currencies and a short time-frame between commitment and settlement.
Interest Rate Risk
Exposure to interest rate risk might arise primarily through the Nathalia District Hospital's interest bearing liabilities. Minimisation of risk is achieved by mainly undertaking fixed rate or non-interest bearing financial instruments. For financial liabilities, the hospital mainly undertakes financial liabilities with relatively even maturity profiles.
Interest Rate Exposure of Financial Assets and Liabilities as at 30 June
Interest Rate Exposure
2013
WeightedAverageEffective Interest
Rate (%)
CarryingAmount
$
FixedInterest
Rate$
VariableInterest
Rate$
Non InterestBearing
$Financial Assets
Cash and Cash Equivalents 3.60% 2,445,130 1,904,041 540,589 500
Receivables:
Patient Fees and Trade Debtors - 170,897 - - 170,897
Other Receivables - 11,451 - - 11,451
Total Financial Assets 2,627,478 1,904,041 540,589 182,848 Financial Liabilities
Payables - 449,976 - - 449,976
Other Financial Liabilities
- Other - 28,693 - - 28,693
Total Financial Liabilities - 478,669 - - 478,669
2012
Financial Assets
Cash and Cash Equivalents 5.12% 2,137,267 1,612,661 524,106 500
Receivables:
Patient Fees and Trade Debtors - 116,915 - - 116,915
Other Receivables - 18,663 - - 18,663
Total Financial Assets 2,272,845 1,612,661 524,106 136,078 Financial Liabilities
Payables - 350,380 - - 350,380
Other Financial Liabilities
- Other - 56,931 - - 56,931
Total Financial Liabilities - 407,311 - - 407,311
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

65N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 15: FINANCIAL INSTRUMENTS (Continued)
(d) Market Risk (continued)
Sensitivity Disclosure Analysis
Taking into account past performance, future expectations, economic forecasts, and management's knowledge and experience of the financial markets,Nathalia District Hospital believes the following movements are 'reasonably possible' over the next 12 months (Base rates are sourced from the Reserve Bank of Australia) - A Shift of +1% and -1% in markets interest rates (AUD) from year-end rates of 3.6%; - A parallel shift of +1% and -1% in inflation rate from year-end rates of 2%;The following table discloses the impact on net operating result and equity for each category of financial instrument held by Nathalia District Hospital at year end as presented to key management personnel, if changes in the relevant risk occur.
Interest Rate Risk
-1% +1%
2013
CarryingAmount
$Profit
$Equity
$Profit
$Equity
$
Financial Assets
Cash & Cash Equivalents 2,445,130 (24,451) (24,451) 24,451 24,451
Receivables
- Trade Debtors 170,897 - - - -
- Other Receivables 11,451 - - - -
Financial Liabilities
Payables 449,976 - - - -
Other Financial Liablities
- Other Financial Liablities 28,693 - - - -
(24,451) (24,451) 24,451 24,451
2012
Financial Assets
Cash & Cash Equivalents 2,137,267 (21,373) (21,373) 21,373 21,373
Receivables
- Trade Debtors 116,915 - - - -
- Other Receivables 18,663 - - - -
Financial Liabilities
Payables 350,380 - - - -
(21,373) (21,373) 21,373 21,373
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

66 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
Nathalia District Hospital Notes to the Financial Statements 30 June 2013
NOTE 15: FINANCIAL INSTRUMENTS (Continued)15(e) Fair Value
The fair values and net fair values of financial instrument assets and liabilities are determined as follows:
*Level 1 - the fair value of financial instrument assets and liabilities with standard terms and conditions and traded in active liquid markets are determined with reference to quoted market prices;
* Level 2 - the fair value is determined using inputs other than quoted prices that are observable for the financial asset or liability, either directly or indirectly; and
* Level 3 - the fair value is determined in accordance with generally accepted pricing models based on discounted cash flow analysis using unobservable market inputs.
The Health Services considers that the carrying amount of financial instrument assets and liabilities recorded in the financial statements to be a fair approximation of their fair values, because of the short-term nature of the financial instruments and the expectation that they will be paid in full.
The following table shows that the fair values of most of the contractual financial assets and liabilities are the same as the carrying amounts.
Comparison between carrying amount and fair value
2013
Carrying Amount
2013$
Fair Value2013
$
Carrying Amount
2012$
Fair Value2012
$Financial Assets
Cash and Cash Equivalents 2,445,130 2,445,130 2,137,267 2,137,267
Receivables:
Patient Fees and Trade Debtors 170,897 170,897 116,915 116,915
Other Receivables 11,451 11,451 18,663 18,663
Total Financial Assets 2,627,478 2,627,478 2,272,845 2,272,845
Financial Liabilities
Payables 449,976 449,976 350,380 350,380
Other Financial Liabilities
- Other 28,693 28,693 56,931 56,931
Total Financial Liabilities 478,669 478,669 407,311 407,311

67N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 16: JOINTLY CONTROLLED OPERATIONS AND ASSETS
Ownership Interest
Hume Rural Health Alliance - Information Systems 2013 2012
1.81% 1.79%
Nathalia District Hospital interests in the above jointly controlled operations and assets is detailed below. The amounts are included in the financial statements under their respective asset categories.
Total2013
$
Total2012
$Current Assets
Cash and Cash Equivalents 25,397 18,520
Receivables 19,995 16,495
Other Assets 936 531
Total Current Assets 46,328 35,546
Non Current Assets
Plant and Equipment 552 508
Current Liabilities
Payables 18,282 17,615
Total Liabilities 18,282 17,615
Nathalia District Hospital's interest in revenue and expenses resulting from jointly controlled operations and assets is detailed below:
Revenues
Operating Revenue 61,441 41,883
Non Operating Revenue 418 900
Total Revenue 61,859 42,783
Expenses
Non Salary Labour Costs 34,431 32,339
Operating Expenses 72,094 61,988
Depreciation 495 704
Capital Expenditure - 3,572
Total Expenses 107,020 98,603
Net Result (45,161) (55,820)
Contingent Liabilities and Capital Commitments
The jointly controlled operation has no known contingent liabilities or capital commitments
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

68 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 17: OPERATING SEGMENTSResidential Aged
Care Services Other HSA &
H&CI Services
2013$
2012$
2013$
2012$
Total2013
$
Total2012
$
REVENUE
Total Revenue (External Segment Revenue)
2,167,298 2,095,005 4,060,364 3,642,656 6,227,662 5,737,661
EXPENSES
Total Expenses (External Segment Revenue)
(2,325,892) (2,187,420) (4,329,408) (4,157,235) (6,655,300) (6,344,655)
Net Result From Ordinary Activities
(158,594) (92,415) (269,044) (514,579) (427,638) (606,994)
Interest Income - - 96,501 110,478 96,501 110,478
Net Result for Year (158,594) (92,415) (172,543) (404,101) (331,137) (496,516)
Other Information
Segment Assets 37,721 31,702 17,972,406 18,022,261 18,010,127 18,053,963
Total Assets 37,721 31,702 17,972,406 18,022,261 18,010,127 18,053,963
Segment Liabilities - - 1,900,102 1,516,300 1,900,102 1,516,300
Total Liabilities (Unallocated) - - 1,900,102 1,516,300 1,900,102 1,516,300
The major services from which the above segments derive income are:
Residential Aged Care Services
Other HSA & H&CI Services - Acute and Community Services
Pricing between inter-segments is at cost
Nathalia District Hospital operates predominantly in Nathalia, Victoria. More than 90% of revenue, net surplus from ordinary activities and segment assets relate to operations in Nathalia, Victoria.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

69N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE 18A: RESPONSIBLE PERSON RELATED DISCLOSURESIn accordance with the Ministerial Directions issued by the Minister for Finance under the Financial Management Act 1994, the following disclosures are made regarding responsible persons for the reporting period.
Period
Responsible Ministers: From To The Honourable David Davis, MLC, Minister for Health and Ageing 1/07/2012 30/06/2013
The Honourable Mary Wooldridge, MLA, Minister for Mental Health 1/07/2012 30/06/2013
Board of Directors
Mr A Sage 1/07/2012 30/06/2013
Mrs B Brooks 1/07/2012 30/06/2013
Mr D Vaughan 1/07/2012 30/06/2013
Ms S Logie 1/07/2012 30/06/2013
Mr K Pell 1/07/2012 30/06/2013
Mr D McKenzie 1/07/2012 30/06/2013
Ms M Keil 1/07/2012 10/03/2013
Mr L Bourke 19/02/2013 30/06/2013
Ms K Rappell 19/02/2013 30/06/2013
Accountable Officer
Ms KM Healy 1/07/2012 8/03/2013
Mr A Stripp 9/03/2013 30/06/2013
Remuneration of Responsible Persons
Total2013
$
Total2012
$
Nil Nil
Other Transaction of Responsible Persons and their Related Parties
Mr A Sage is a partner of Nathalia Printers. The business provided printing services to the Hospital on normal terms and conditions. The aggregate value of these services was $6,203 (2012 $5,777)
NOTE 18B: ExECUTIVE OFFICER DISCLOSUREThe Chief Executive Officer is employed by Goulburn Valley Health (GVH) and information relating to her/his remuneration is disclosed in the financial statements of GVH. During the year Nathalia District Hospital paid $89,452 to GVH in relation to the service provided by the CEO and other Administration staff.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

70 N a t h a l i a D i s t r i c t h o s p i t a l - a N N u a l r e p o r t 2 0 1 2 / 1 3
NOTE:19: EVENTS OCCURRING AFTER THE BALANCE SHEET DATEA contract has been signed for the sale of the old hospital site at 35-37 Elizabeth Street, Nathalia for $155,000 inclusive of GST.
NOTE 20: CONTINGENT ASSETS AND LIABILITIESThere are no known contingent liabilities or assets at the date of this report.
NOTE 21: Ex-GRATIA PAYMENTSThere were no ex-gratia payments made by Nathalia District Hospital during the 2012/2013 financial year.
Nathalia District Hospital Notes to the Financial Statements 30 June 2013

Nat
halia
D istr ict Ho
spit
al
Providing Quality Care
Quality of Care report 2012/13Nathalia District Hospital

72 N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3
Quality of Care Report 2012/13
The Quality of Care Report is produced by Nathalia District Hospital so we can inform our community about the health services we provide, and the standard at which they are provided at. We monitor our performance against other similar sized hospitals (E sized) within Victoria to ensure our care is of the highest quality. We aim to provide an informative report that is of interest to all members of our community and provides them with a useful reference document.
This report gives an overview of the work we have undertaken in 2012/13. The report also details how we have performed on a number of key performance indicators and outlines the safety and governance systems we have in place to ensure we continue to improve.
While producing an annual Quality of Care Report is a requirement of the Victorian Department of Health we are committed to making it as valuable a reporting tool to the community as possible. We encourage you to take the time to fill in the feedback form available within the Hospital, or online to assist us to reach this goal. We unfortunately did not receive any feedback in regard to last year’s report.
A diverse group of staff, with input from volunteers from the Community and members of our Board of Management have worked together to gather the information to write this year’s Quality of Care Report. We take this opportunity to thank everyone involved with the production of the report and welcome any ideas and comments that you may have. We hope that you enjoy reading our report and find it interesting and useful.
Who is Our Community
Our Hospital services the residents of Nathalia and District, which encompasses the small townships and districts of Waaia, Barmah, Picola, Kotupna, Bearii and Yalca.
Demographically our population is ageing, with the most recent Australian Bureau of Statistics (2011) listing our population at the median age of 45 years, significantly higher than the national average of 37 years. We have 23% of our community over 65 years of age compared to an Australian average of 13.2% however we also meet the Australian average of 19% of our population less than 15 years of age. This creates challenges for our small rural health service to be creative and proactive in providing primary health services across the continuum to ensure our community’s wellbeing.
Nathalia District Hospital is one of the larger employers in the town, currently employing 86 staff. It operates under the Victorian Department of Health Small Rural Health Service Funding Program. This program allows us flexibility for our organisation to decide the balance of services to be provided. We continue to expand and grow our primary health services to include occupational therapy, physiotherapy, dietetics, diabetes education, asthma education, generalist counselling, pathology collection, medical imaging, optometry, audiology and podiatry. These programs are reviewed annually to meet the changing needs of our community.
The health service has not been without its challenges in 2012/2013. Financial challenges remain a constant concern as we attempt to deliver maximum services whilst containing costs in this tight economic environment.

N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3 73
Clinical Governance
Governance is the manner in which an organisation is controlled, and kept on track to achieve its overall aims and objectives. In regards to the Nathalia District Hospital the governance we talk about most often is Clinical Governance. Clinical governance is the system by which the Hospital’s Board of Management, managers, clinicians and staff share responsibility and accountability for safety and quality of healthcare provided. That is, the structure we use to make things better and safer.
Good clinical governance requires a planned and integrated approach to:
• defining and delegating responsibility for clinical safety and quality;
• establishing well-designed systems capable of supporting safe, high quality clinical care;
• monitoring clinical quality;
• reporting on performance;
• risk management, and
• a strong organisational culture of safety, quality and compliance.
Clinical Governance at NDH is delivered through a framework based on the four domains of quality and safety set out in the Victorian Government Clinical Governance Policy Framework. The Clinical governance domains are:
• Consumer participation.
• Clinical effectiveness.
• Risk Management
• Effective workforce
Strategic Plan & Goals
In February this year, we released the Nathalia District Hospital Strategic Plan 2013–2015. It identifies six strategic areas, each with a defined goal as follows:
1. To ensure the governance structure and performance of the Board of Management is effective and efficient.
2. To promote the newly developed vision, mission and values statements of Nathalia District Hospital.
3. Develop processes for involving consumers in the governance and planning processes whilst, at the same time, partnering with other health providers to strengthen service delivery
4. To have a mix of skilled staff to meet needs and demands of consumers.
5. To provide quality evidence based care for all consumers.
6. To remain viable, relevant and reliable in order to service the community and its needs now and into the future.
Credentialing
To support our strategic goal of “Safe and Effective Patient Centred Care” we must ensure our staff are appropriately skilled, trained and credentialed. Being credentialed means that you have the right skills and experience to be able to practice as a clinician i.e. if you are a doctor, you have been to medical school, passed, undergone additional training, and you are registered to practice as a doctor in Australia. It is important that all our clinical staff have both the right qualifications to practice, and that the scope of their practice is limited to the experience they bring with them to the organisation.
Our Credentialing and Scope of Clinical Practice Policy ensures all health professionals we employ are appropriately credentialed and have their scope of practice defined. There is a requirement for all staff to meet the National Registration for Heath Professionals legislation as well as the Department of Health requirements.
Promoting Consumer Participation
Consumer participation occurs when consumers, carers and community members are meaningfully involved in decision making regarding health service planning.
Consumers, including persons living with disability, persons from diverse cultural and religious backgrounds, sexual orientation, socio economic status and social circumstance assist to determine health service priorities, assist with quality issues, and provide input into policy development, planning of care and treatments for themselves and the community.
Nathalia District Hospital’s consumer participation model has a focus on incorporating consumer involvement in service planning and delivery. This ensures that health care is delivered effectively and appropriately, and that the health service remains accountable to the needs of the community.
Formal and informal ways consumers are involved include:
Each consumer is involved with the planning of their care and treatment.
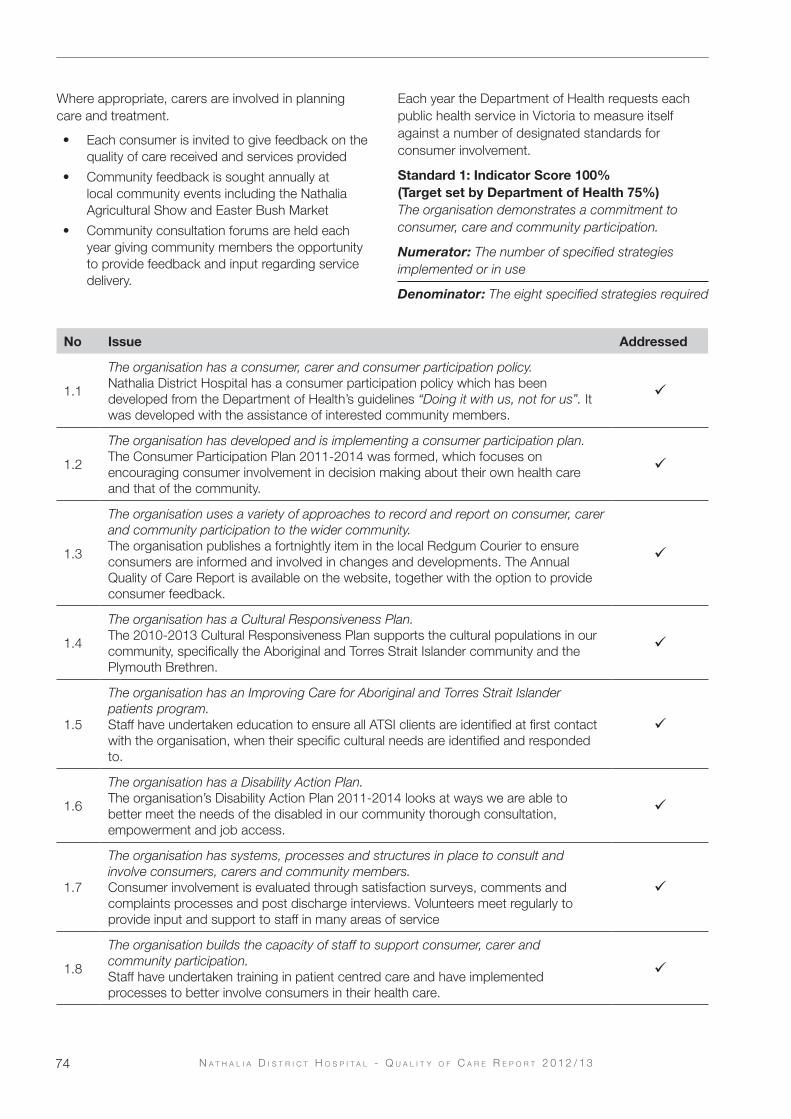
74 N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3
Where appropriate, carers are involved in planning care and treatment.
• Each consumer is invited to give feedback on the quality of care received and services provided
• Community feedback is sought annually at local community events including the Nathalia Agricultural Show and Easter Bush Market
• Community consultation forums are held each year giving community members the opportunity to provide feedback and input regarding service delivery.
Each year the Department of Health requests each public health service in Victoria to measure itself against a number of designated standards for consumer involvement.
Standard 1: Indicator Score 100% (Target set by Department of Health 75%)The organisation demonstrates a commitment to consumer, care and community participation.
Numerator: The number of specified strategies implemented or in use
Denominator: The eight specified strategies required
No Issue Addressed
1.1
The organisation has a consumer, carer and consumer participation policy.Nathalia District Hospital has a consumer participation policy which has been developed from the Department of Health’s guidelines “Doing it with us, not for us”. It was developed with the assistance of interested community members.
1.2
The organisation has developed and is implementing a consumer participation plan.The Consumer Participation Plan 2011-2014 was formed, which focuses on encouraging consumer involvement in decision making about their own health care and that of the community.
1.3
The organisation uses a variety of approaches to record and report on consumer, carer and community participation to the wider community.The organisation publishes a fortnightly item in the local Redgum Courier to ensure consumers are informed and involved in changes and developments. The Annual Quality of Care Report is available on the website, together with the option to provide consumer feedback.
1.4
The organisation has a Cultural Responsiveness Plan.The 2010-2013 Cultural Responsiveness Plan supports the cultural populations in our community, specifically the Aboriginal and Torres Strait Islander community and the Plymouth Brethren.
1.5
The organisation has an Improving Care for Aboriginal and Torres Strait Islander patients program.Staff have undertaken education to ensure all ATSI clients are identified at first contact with the organisation, when their specific cultural needs are identified and responded to.
1.6
The organisation has a Disability Action Plan. The organisation’s Disability Action Plan 2011-2014 looks at ways we are able to better meet the needs of the disabled in our community thorough consultation, empowerment and job access.
1.7
The organisation has systems, processes and structures in place to consult and involve consumers, carers and community members.Consumer involvement is evaluated through satisfaction surveys, comments and complaints processes and post discharge interviews. Volunteers meet regularly to provide input and support to staff in many areas of service
1.8
The organisation builds the capacity of staff to support consumer, carer and community participation.Staff have undertaken training in patient centred care and have implemented processes to better involve consumers in their health care.

N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3 75
Bedside Handover
As part of our commitment to involving patients in their care, we commenced a bedside clinical handover for all acute patients in March 2013. Bedside clinical handover is the sharing of clinical information between the patient, the nurses who have been providing care over the past 8 hours, and the nurses who will be taking over that care for the next 8 hours.
The aim of the bedside handover is to improve communications with those staff providing care through open discussion with each patient. Recent feedback from the trial of clinical handover has been very positive, with patients feeling greater involvement in their care by being given the opportunity to comment and ask questions at handover.
Standard 2: Indicator Score 81%(Target set by Department of Health 75%)A consumer participation indicator score on the Victorian Patient Satisfaction Monitor (VPSM).
Using the five point Likert scale, where 1=poor, 2=fair, 3=good, 4=very good and 5=excellent the following responses were provided by consumers in Wave 23 of the VPSM:
• Opportunity to ask questions about your condition or treatment scored 4.15, a decrease of 0.22 on the previous year
• Willingness of staff to listen to your health care problems scored 4.08, unchanged from the previous Wave improvement of 0.33 on the previous year
Consumers, whether residents in our nursing home, patients in acute care, or community health clients, are encouraged to become directly involved in their care from earliest point of contact to the service. Consumers take an active role in goal setting their aims for treatment, and assisting the health professionals by working together to achieve the goals set.
Consumer Participation Index Wave 21-23
Standard 3: Indicator Score 81.60%(Target set by Department of Health 75%)Consumers and, where appropriate, carers are provided with evidence based, accessible information to support key decision making along the continuum of care.
Numerator: Number of VPSM respondents rating Question 20(b) “good” or “excellent”
Denominator: Total number of respondents to the above question
Question 20(b) asks how you would rate the written information you were given about how you manage your condition and recovery at home as “good” or “excellent”.
All written information for consumers is reviewed by a consumer representative before it is approved for use by the health service. This consumer representative provides feedback as to whether the brochure is easy to understand, is free from “health jargon” the consumer would find difficult to interpret, and that we have not omitted any important information. The consumer representative uses a score sheet which rates presentation, language, content, and treatment information and outcomes. Once this feedback has been given, the brochure is approved through the quality meetings.
There were 5 brochures reviewed in 2012/13, all had alterations made to them following consumer review.
General Patient Infomation Wave 21-23
NDH
E Size
All Hospitals
80
82
84
86
88
90NDH
E Size
All Hospitals
Wave 21 Wave 22 Wave 23
7476
78808284868890
Wave 21 Wave 22 Wave 23

76 N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3
Standard 4: Indicator Score 100%(Target set by Department of Health 75%)Consumers, carers and community members are active participants in the planning, improvement and evaluation of services and programs on an ongoing basis.
Numerator: Number of dimensions of specified activities where consumers, carers and community members are actively involved
Denominator: The six dimensions of specified activities
Dimension Issue Addressed
1
Strategic planning: During development of the organisation’s new vision, mission and value statements, a number of community consultations were held to gain consumer involvement.
2Service, program and community development:As a result of feedback received, the Nathalia Medical Clinic has gained funding to support an evening consultation from 6pm to 9pm every Wednesday.
3
Quality Improvement Activities:All acute patients are invited to take part in the Victorian Patient Satisfaction Monitor after discharge. In Wave 23, 31 patients were invited to give feedback, with 14 accepting the offer. This resulted in a 45% return rate.
4
Developing and monitoring feedback, complaints and appeals systems, and in the review of complaints: Patient Care Review Committee meets every second month to oversee the clinical governance of the health service. This Committee consists of community representatives and community members of the Board of Management, staff and medical officers. One of the Committee’s roles is to review all comments and complaints.
5Ethics, quality, clinical and corporate governance committees: The Hospital does not have an Ethics Committee, but uses the expertise of Goulburn Valley Health for advice and support when required.
6
Consumers, carers and community members are involved in the development of consumer information:All consumer documents are reviewed by a consumer representative to ensure the information provided does not include health jargon and meets the needs of the consumer.
1.8
The organisation builds the capacity of staff to support consumer, carer and community participation.Staff have undertaken training in patient centred care and have implemented processes to better involve consumers in their health care.
Dealing with Complaints
Nathalia District Hospital has a policy of open disclosure when dealing with complaints modelled on the guidelines of the Australian Commission on Quality and Safety in Health Care. Every complaint is taken seriously and dealt with as soon as possible. Complaints may be verbal or written and may be made anonymously. The Quality Coordinator oversees our complaints process. Complaints are a measure for us to improve our service provision and in this respect are always welcomed.
Nathalia District Hospital received 8 written complaints during 2012/13 and 10 verbal complaints. Of the 18 complaints, 33% were about staff direct care delivery to consumers and another 33% were found to be because the hospital policy was not clear. In the same time period the organisation received 17 written positive comments and 11 suggestions for improvement through its comments, suggestions and complaints program. All complaints were addressed to the satisfaction of the person making the complaint within 7 days.
100% of staff have completed a competency on open disclosure in 2013.

N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3 77
Standard 5: The organisation actively contributes to building the capacity of consumers, carers and community members to participate effectively.
Community members regularly request to be involved in their Hospital. We have a small but dedicated band of volunteers who continually donate their time and expertise to assist us to deliver services to our residents, patients and community members. We are grateful for their dedication and commitment.
Our Community continues to benefit from the use of the community car, which is owned and maintained by the hospital. Community members, under the skilled guidance of Mrs Joan Dohnt, drive thousands of kilometres each year to take people to medical appointments as far away as Melbourne.
We are continuing to work on developing this area by encouraging consumers to be involved in the operational and strategic directions of our Hospital.
Cultural Responsiveness Plan (CRP)
The Cultural Diversity Framework designed by the Department of Health aims to improve and extend the cultural responsiveness performance of Victorian health services. The cultural responsiveness framework specifies six clear standards across the four quality and safety domains of organisational effectiveness, risk management, consumer participation and effective workforce.
The framework encompasses a strategic and whole-of-organisation approach and is designed to be aligned with health services’ strategic planning processes.
It specifies six standards and improvement measures for culturally responsive practice.
A whole of organisation approach to cultural responsiveness is demonstrated.
NDH has developed a CRP which it is in the process of implementing, with the aim of becoming compliant by end of year 2013. The plan is inclusive of; Key Performance Indicators (KPIs), annual review and reporting of outcomes, a defined reporting chain and is culturally appropriate to the Nathalia district community. A clause will be entered into the terms of reference for the Patient Care Review Committee (PCRC).
Leadership for cultural responsiveness is dem-onstrated by the health service
PCRC has endorsed the role of this committee to manage and evaluate CRP and its KPIs.
Accredited interpreters are provided to patients who require one
The organisation ensures that current documentation identifies CALD clients at each presentation to Nathalia District Hospital, and gains feedback on their experiences during their time accessing the service. International signage is used within all locations of the facility and that information regarding interpreter services is available at both the Hospital and Medical Clinic reception areas.
Inclusive practice in care planning is demon-strated, including but not limited to dietary, spiritual, family, attitudinal and other cultural practices.
The organisation has purchased a dietary manual for catering staff to meet the dietary needs of CALD patients and residents.
CALD consumer, carer, and community mem-bers are involved in the planning, improvement, and review of programs and services on an ongoing basis.
Community groups are invited to nominate a representative to drive cultural awareness programs through PCRC, which will also function as CDC/CAC for Nathalia District Hospital. The Consumer Participation policy will have a clause added to facilitate the inclusion of personnel from diverse backgrounds.
Staff at all levels are provided with professional development opportunities to enhance their cultural responsiveness.
The education staff have overseen the development of a self directed learning package relevant to each service area of the Hospital. This learning package will align with the CRP intentions, domains and measures, and is to be completed by all personnel.
Improving Care for Aboriginal Patients Program - ICAP Reporting
The 2011 Australian Bureau of Statistics figures indicate there are 1920 people in the Nathalia postcode area, of which 44 (or 2.3%) identify themselves as of Aboriginal or Torres Strait Islander decent.
Nathalia District Hospital is working towards improving service access for this group by working closely with the Cultural Diversity Officer at Moira Shire.

78 N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3
Key Result Area Demonstration of Achievement
Establish and maintain relationships with Aboriginal Communities and services.
Involvement of Aboriginal people in health service activities relevant to the identification and care of Aboriginal patients.-
NDH routinely screens all patients on admission to the health service to identify those identifying as being of Aboriginal descent.
Due to the small size of the organisation the service works closely with the Moira Shire Cultural Diversity Officer to ensure services are tailored to the client needs.
Provide or coordinate cross cultural training for hospital staff
Senior staff have undertaken external cultural training.
This will be expanded to all clinical staff in the near future.
Set up and maintain service planning processes that ensure that the cultural needs of Aboriginal people are addressed when referrals and service needs are being considered, particularly in regard to discharge planning.
Involvement of Aboriginal staff in development, review and refinement of discharge planning arrangements, and views of Aboriginal organisations and Aboriginal service users have been sought.
NDH places an emphasis on involving and seeking the views of local Aboriginal people to ensure their care needs and cultural needs are being considered, especially in regard to discharge planning.
Established referral arrangements to support all hospital staff to make effective primary care referrals and seek the involvement of Aboriginal workers and agencies.
Involvement of Aboriginal Staff in development, review and refinement of referrals to primary care, and the views of Aboriginal community controlled health organisations have been sought.
NDH does not have the resources to employ a dedicated Aboriginal liaison officer, thus expert advice is sought from the Moira Shire to provide guidance to staff to ensure that referral principles are being consistently applied.
The local aboriginal community is also surveyed annually to determine their levels of satisfaction in regard to services provided.
Consumer Feedback
The Victorian Patient Satisfaction Monitor provides patients with the opportunity to provide anonymous feedback about the services and care received whilst an inpatient in our Hospital.
In the most recent Wave 23 survey the following responses were received:
What is the best thing about your stay in hospital:
• I was able to relax, knowing that doctors and nurses were taking care of me so efficiently
• The warmth and consideration from all staff.
What was the worst thing about your stay in hospital:
• Just the fact that I had to be there
• Not being at home.
What could the hospital do to improve the care and services:
• Do not really know as everything seemed OK to me.
• Not aware of the immediate needs.
Australian Safety and Quality Framework for Health Care
The Australian Safety and Quality Framework for Health Care, describes a vision for safe and high quality care for all Australians, and sets out the actions needed to achieve this vision. It specifies three core principles for safe and high quality care. These principles of care are:
• consumer centred,
• driven by information, and
• organised for safety.
The Framework was endorsed by Health Ministers as the national safety and quality framework for Australia

N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3 79
in November 2010. It provides areas of action that all people in the health system can take to improve the safety and quality of care provided in all healthcare settings over the next decade.
This framework can be used as the basis of strategic and operational safety and quality plans, providing a mechanism for refocusing current safety and quality improvement activities and designing goals for health service improvement, and be used as a guide for reviewing investments and research in safety and quality.
Aged Care Standards and Accreditation AgencyThe Aged Care Standards and Accreditation Agency conducted their three yearly two day accreditation audit of Banawah in May 2012. In November 2012, we received an unannounced visit where assessors reviewed incident management and specialised nursing care needs of residents. On both occasions our nursing home was found compliant in all 44 standards.
Australian Council on Healthcare StandardsThe Australian Council on Healthcare Standards conducted an Organisation Wide Survey in September 2011 in which all criteria under the three ACHS functions of Clinical, Support and Corporate were reviewed, together with any recommendations from the previous organisation-wide survey. The results were of an exceptionally high standard, with a total of 11 Extensive Achievement ratings being received. We are due for a Periodic Review under EQuIPNational in September 2013.
Home and Community Care National Service StandardsMonitoring of the accreditation for HACC service standards was last undertaken by the Australian Council on Healthcare Standards in September 2009, when Nathalia District Hospital District Nursing Service received a perfect 20/20 score. This external survey is due to be repeated in September 2013, and will incorporate the values of the Active Service Model which is being implemented across all health services.
Risk Management
Understanding what can go wrong and how to best prevent it from reoccurring is important. We are able to identify and monitor incidents through the Victorian Health Incident Management System (VHIMS) which allows us to track incidents, analyse them and make improvements to our care.
NDH runs an extensive risk register which monitors all identified risk to the organisation, and put strategies in place to alert us if the risk is not being effectively managed.
Medication Safety
Reducing harm from medications remains an important element of our work. Reducing errors and harm through safe and timely administration of medications is vital to ensure the safety of our residents, patients and staff.
All medication incidents and errors which occur at NDH are reported through the VHIMS electronic reporting tool, in 2012-13 a total of 41 incidents were reported in the facility, 26% of which were failure to remove a medication patch from a resident/patient after the prescribed time.
Each incident reported is reviewed at the time to determine whether improvements can be made to prevent incidents from reoccurring. Examples of improvements made during the past 12 months include; education to nursing staff regarding the reporting requirements of VHIMS (regarding what needs to be reported), the development of a system to ensure medication patch’s are removed from patients/residents post the prescribed time frame and the development of clinical guidelines for the antibiotic drug Gentamycin.
In the Public Sector Residential Aged Care Aged Care Quality Indicator Reports Banawah was below the state average of the use of nine or more medications with a prevalence of 3.87 per 1000 occupied bed days.
Preventing Falls and Harm From Falls
Nathalia District Hospital’s falls minimisation protocol uses the World Health Organisations definition of a fall; an event which results in a person coming to rest inadvertently on the ground or floor or a lower level.
Although falls are an inevitable part of ageing, our aim is to reduce the incidence of falls amongst our patients, clients and residents, and the associated injuries that may occur. Each patient is assessed for falls risk on admission to the facility regardless of whether they are a home based, hospital based or residential aged care client.
The service monitors a number of indicators regarding falls including falls frequency, and any resident who has repeated falls is reviewed by a multidisciplinary team in an attempt to identify triggers and reduce falls.

80 N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3
During the past 12 months NDH recorded 45 falls occurring within the facility, with 3 resulting with fractures. 28 of these falls occurred within a 3 month period (July, August, and September 2012).
In October 2012, in a response to the fall rate in the 3 months prior, NDH introduced an hourly rounding system aimed at reducing the amount of falls occurring within the facility. Hourly rounding is a program which requires staff to check on the patient or resident each hour and ask them a series of questions designed to limit their risk of falls. Questions include whether the person needs to go to the toilet or needs pain relief. The introduction of this system has been a success, with falls reducing by from an average of just under 4 falls a month down to 1.4 falls a month.
In the Public Sector Residential Aged Care Aged Care Quality Indicator Reports Banawah was below the state average of falls frequency with a prevalence of 5.34 falls per 1000 occupied bed days.
Pressure Ulcer Prevalence
A pressure ulcer is an area of skin that has been damaged due to unrelieved pressure and is commonly referred to as a pressure sore or bed sore. Pressure ulcers may only look minor, exhibiting only a redness of the skin, but they commonly hide further damage under the skin surface. Individuals confined to bed or chair, unable to move themselves, have a loss of sensation, loss of bowel or bladder control, poor nutrition, or are unwell, are at risk of developing pressure ulcers.
A skin integrity risk assessment is completed on all residents and patients in our care. Those indentified as “at risk” will then have preventative strategies implemented. Ongoing assessment ensures that risk management strategies are working as a part of the day to day care of the resident/patient.
Staff are also educated regarding early recognition of pressure ulcers and are provided with the knowledge to implement early preventative measures.
In the Public Sector Residential Aged Care Aged Care Quality Indicator Reports Banawah was above the state average of Stage 1 pressure injuries with a prevalence of 3.31 incidents per 1000 occupied bed days, but below the state average for all other stages of pressure injuries.
Safe Use of Blood and Blood Products
In 2012, Nathalia District Hospital took part in an audit of consent for blood transfusions, completed by the Blood Matters program from the Victorian Department of Health.
The Blood Matters Program Patient Blood Management Steering Group identified the area of ‘blood transfusion consent’ to audit to determine current practice across the State. The audit identified minor changes were needed to be made to policy and forms at NDH in regard to blood transfusion consent, which are in the process of being amended. In addition, all registered nurses are required to complete a competency on blood and blood products every 2 years using the Blood Safe e-learning education package.
Preventing and Controlling Healthcare Associated Infections
Nathalia District Hospital has a well documented and resourced infection control program which is monitored regularly to determine its ongoing effectiveness. Policies and procedures have been developed in accordance with Department of Health guidelines and the organisation has close links with the Hume Region Infection Control Practitioners Group for additional support and expertise when required.
Clinical staff complete regular audits on waste management, cleaning, food services, hand hygiene, linen, personal protective equipment, blood and body fluid spills, and occupational exposures, which helps the facility monitor performance and identify any potential areas of concern and need for improvement.
Results of audits are reported through both the Quality Improvement Committee and Patient Care Review Committee, where it is determined whether further action is required to improve outcomes.
Hand Hygiene Hand Hygiene is the term used to describe the cleaning of hands aimed at preventing the spread of infection by the use of soap and water, or a waterless antibacterial agent. Alcohol hand rub is available at the entrance to our health service for use by visitors as they enter and leave, and throughout the building in strategic places.
Our health service audits compliance every 4 months to ensure we achieve, at the very least, the minimum standard of compliance as set by the Department of Health at 70%. Audit results during 2012/2013 saw the health service achieve an average score for
Staff HealthWe have maintained staff immunisation to Hep B at 100%. 88% of staff accepted the offer to become immunised for Influenza in 2012/2013, an increase of 2.5% on the previous year.
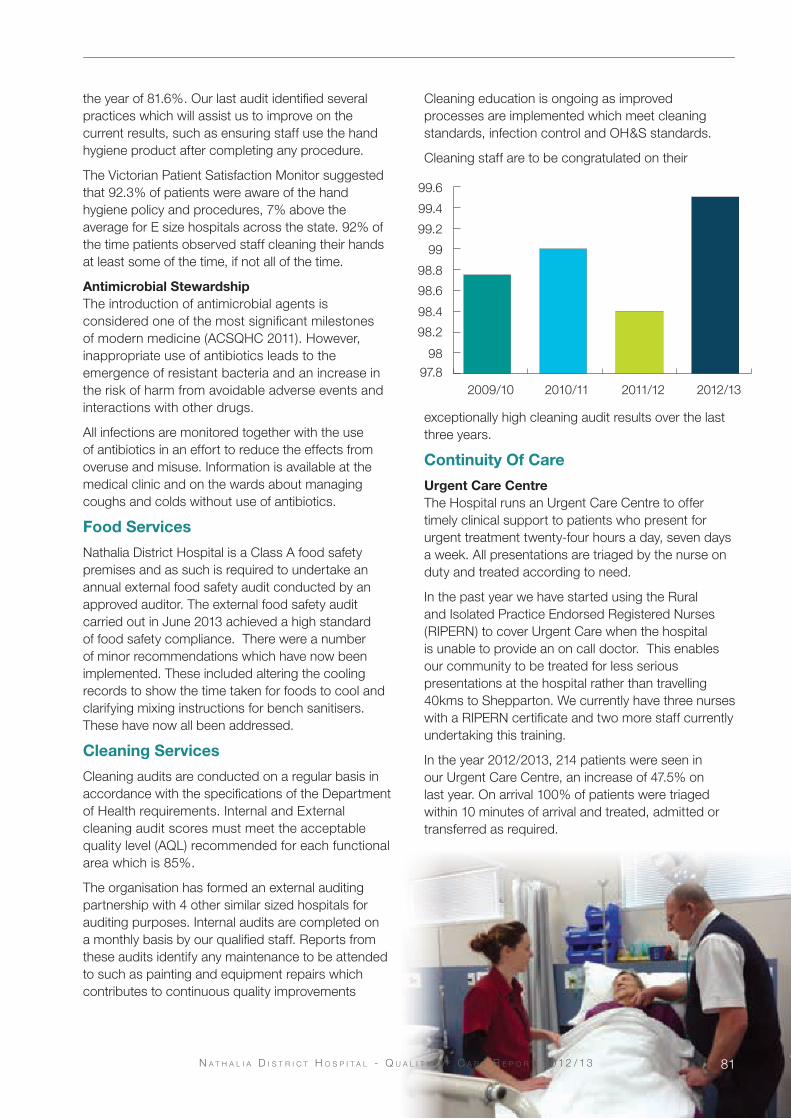
the year of 81.6%. Our last audit identified several practices which will assist us to improve on the current results, such as ensuring staff use the hand hygiene product after completing any procedure.
The Victorian Patient Satisfaction Monitor suggested that 92.3% of patients were aware of the hand hygiene policy and procedures, 7% above the average for E size hospitals across the state. 92% of the time patients observed staff cleaning their hands at least some of the time, if not all of the time.
Antimicrobial StewardshipThe introduction of antimicrobial agents is considered one of the most significant milestones of modern medicine (ACSQHC 2011). However, inappropriate use of antibiotics leads to the emergence of resistant bacteria and an increase in the risk of harm from avoidable adverse events and interactions with other drugs.
All infections are monitored together with the use of antibiotics in an effort to reduce the effects from overuse and misuse. Information is available at the medical clinic and on the wards about managing coughs and colds without use of antibiotics.
Food Services
Nathalia District Hospital is a Class A food safety premises and as such is required to undertake an annual external food safety audit conducted by an approved auditor. The external food safety audit carried out in June 2013 achieved a high standard of food safety compliance. There were a number of minor recommendations which have now been implemented. These included altering the cooling records to show the time taken for foods to cool and clarifying mixing instructions for bench sanitisers. These have now all been addressed.
Cleaning Services
Cleaning audits are conducted on a regular basis in accordance with the specifications of the Department of Health requirements. Internal and External cleaning audit scores must meet the acceptable quality level (AQL) recommended for each functional area which is 85%.
The organisation has formed an external auditing partnership with 4 other similar sized hospitals for auditing purposes. Internal audits are completed on a monthly basis by our qualified staff. Reports from these audits identify any maintenance to be attended to such as painting and equipment repairs which contributes to continuous quality improvements
Cleaning education is ongoing as improved processes are implemented which meet cleaning standards, infection control and OH&S standards.
Cleaning staff are to be congratulated on their
exceptionally high cleaning audit results over the last three years.
Continuity Of Care
Urgent Care CentreThe Hospital runs an Urgent Care Centre to offer timely clinical support to patients who present for urgent treatment twenty-four hours a day, seven days a week. All presentations are triaged by the nurse on duty and treated according to need.
In the past year we have started using the Rural and Isolated Practice Endorsed Registered Nurses (RIPERN) to cover Urgent Care when the hospital is unable to provide an on call doctor. This enables our community to be treated for less serious presentations at the hospital rather than travelling 40kms to Shepparton. We currently have three nurses with a RIPERN certificate and two more staff currently undertaking this training.
In the year 2012/2013, 214 patients were seen in our Urgent Care Centre, an increase of 47.5% on last year. On arrival 100% of patients were triaged within 10 minutes of arrival and treated, admitted or transferred as required.
97.898
98.2
98.4
98.6
98.8
99
99.4
99.2
99.6
2009/10 2010/11 2011/12 2012/13
n a t h a l i a D i s t r i C t h o s p i t a l - Q u a l i t y o f C a r e r e p o r t 2 0 1 2 / 1 3 81

Acute CareOur doctors have continued to provide a dedicated service to the local community and Nathalia District Hospital. We have a total of six acute beds, one shared room and four single rooms all with ensuite. There were a total of 1129 acute bed days and 106 separations for the 2012/13 financial year.
The Hospital runs a Transition Care Program (TCP) in partnership with Goulburn Valley Health in Shepparton. This program has now been running for two years. TCP provides restorative services for up to 12 weeks for older people who are ready for discharge from hospital. The Transition Care Team includes the coordinator, physiotherapist, occupational therapist, dietitian and medical specialist. We had 390 bed days attributed to this program in 2012/13; an increase of 44% from the previous year.
The Discharge Planning Team continues to review the support patients have been given post discharge, and evaluate the effectiveness of our discharge planning process. This is a multidisciplinary team who review all patients admitted and recently discharged to effectively provide them with a seamless transition back into the community once they recover from their illness.
Palliative CareOur Palliative Care Suite has a kitchenette, fold out bed and its own garden; this allows families to stay with their loved ones during an acute episode or terminal stages of a patient’s illness if the patient chooses a Hospital admission. The District Nursing Service provides the majority of palliative care services to clients in their own home, with support from the Hume Region Palliative Care Service.
Residential Aged CareOur residential aged care facility, Banawah, has 20 high care beds all with single room accommodation for our residents. Each room has access to an ensuite, overhead tracking for lifting residents, piped oxygen, a television and data cabling for computer access. In 2012/13 we had a total of 7,269 bed days from a possible 7,300 giving us a 99.6% occupancy rate.
The Aged Care Standards and Accreditation Agency (ACSAA) had an unannounced visit in November 2012, where there were no issues of any concern raised by the auditors. We also had one Aged Care Funding Instrument (ACFI) audit in June 2013 to check our documentation for funding for the Nursing Home.
This year our activities program has been very active with weekly outings on the bus for our residents. This has lifted the spirits of the residents who look forward to these outings. We have purchased a pool table at the residents request and many of them have become quite skilled over the past few months.
We are grateful to our local schools for providing a number of visits to put on plays and sing to our residents. This builds a bond between our older and younger generations. Volunteer groups have entertained our residents with poetry readings or nostalgia from the Historical Society. The regular activity program includes bingo, music therapy, massage, gardening, pet therapy, craft and cooking. Special events and holidays are celebrated with theme days for occasions like Melbourne Cup, Christmas in July, ANZAC Day and Valentine’s Day.
We sincerely thank the volunteers who assist our residents throughout the year. They continue to provide much needed support and companionship.
District Nursing Services
The District Nursing Service is offered daily to people in the community to assist them to achieve their individual goal/aims and maintain their independence. Nursing care can include assistance with medicines, wound care, end of life care and assistance to carers to care for loved ones with life limiting conditions. The District Nurses also coordinate a carer program with carer day outings, an in home music and a diversional
therapy program.
The nurses work closely with other services such as the Moira Palliative Care Service and
82 n a t h a l i a D i s t r i C t h o s p i t a l - Q u a l i t y o f C a r e r e p o r t 2 0 1 2 / 1 3

N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3 83
Goulburn Valley Health Hospital in The Home Service and demonstrate their commitment to assisting nursing students with their community placement and have completed further training to be competent to assess students.
Nathalia Medical Clinic
There have been several major changes within the clinic over the last 12 months. Dr Kyi Wann resigned his position in September 2012 to take up a position closer to his family in Melbourne. In March 2013 we were pleased to welcome back Dr Mogeke Nyorora after he had completed 12 months working at Tatura Medical Clinic and Dr Chuck Kong has recently obtained his fellowship through the Royal Australian College of General Practice.
After 35 years servicing Nathalia and District, Dr Peter Poon has recently scaled back his clinic hours to two and a half days per week. We are lucky to have such a devoted team of doctors in our current line up of Dr Peter Poon, Dr John Drenen, Dr Chuck Kong and Dr Mogeke Nyorora along with the great support of our practice nurses and administration staff.
During the latter half of 2012, the clinic hosted Intern Dr Alison Mahony for a 10 week period through M2M (Murray to the Mountains) Training Program. In conjunction with Cobram District Health, Dr Mahony gained experience in General Practice in Nathalia under the supervision of Dr Poon and Dr Drenen. Staff from the hospital and clinic have had the opportunity to attend further education organised through the M2M Program via both videoconference and on site, including sessions on Paediatric and Geriatric health issues.
The After Hours Clinic has continued to fill a much needed service in the community with another 12 months of grant money secured through the Department of Health and Ageing and very positive feedback received from the local community. Along with the ongoing clinic driven health checks, used as an early detection tool for chronic disease, Nathalia Medical Clinic continues to strive for good health in the community.
Community Health
Nathalia District Hospital Community Health Team provides education, assistance and advice on a wide range of health issues to community members.
In 2012/13 these included:
• Breast Feeding Friendly
• Smiles 4 Miles
• International Women’s Day
• Women’s Health Clinics including pap tests / cervical screening
• Moira Food Bank
• Rotary Guest Speakers
• People Supporting People Community BBQ’s
• Connectingcare
• Early Intervention into Chronic Disease
• Cert 111 Allied Health Assistant Project
• Asthma, Diabetes, QUIT, Anaphylaxis Management are offered and school health programs
Breast Feeding FriendlyThe Moira Shire has mapped breast feeding friendly businesses throughout the shire. Nathalia Community Health has been working with 11 businesses in Nathalia. These businesses have been screened and registered with the Australian Breast Feeding Association. The location and details of these businesses can be found on the Australian Breast Feeding Association website.
Approved businesses in Nathalia have the Australian Breast Feeding Association recognised sticker displayed.
International Women’s Day 2013The theme for International Women’s Day 2013 was Preventing Violence Against Women and Children: promoting equal and respectful relationships and non violent norms”. A representative from Centre Against Sexual Assault (CASA) spoke to community members on Family Violence. An informative session was presented on educating women about physical and verbal bullying, “control of people”, being other forms of violence. This prompted great discussion. The presentation was followed by morning tea provided by the local Women’s Group. A member of the Women’s Group spoke on the “Look Good, Feel Good” program facilitated by the Cancer Council and finished the presentation with a makeup demonstration.
People Supporting People Community BBQ’sNathalia Community Health worked in partnership with Nathalia Community House to initiate and assist with facilitating a free weekly community BBQ for those in need in Nathalia. The initial request came from People Supporting People in Shepparton, due to calls they had received for assistance, from Nathalia community

84 N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3n a t h a l i a D i s t r i C t h o s p i t a l - a n n u a l r e p o r t 2 0 11 / 1 284
members. All equipment & supplies are funded through People Supporting People and volunteers assist with the BBQ.
ConnectingcareConnectingcare is a comprehensive web-based directory providing secure messaging and e-referral. Primary Care Partnerships over Victoria have been using Connectingcare which enables agencies to securely and easily send referrals and other secure messages.
Over 23,000 Victorian services based on the Human Services directory data model are listed with Connectingcare as an online service. This enables service providers to accept electronic referrals and messages from Connectingcare. By completing the standard referral template within the Connectingcare website, staff send e-referrals. No patient or client identifying information is stored in the Connectingcare system.
Nathalia has just implemented this service, and will be providing training sessions for staff in the near future to use Connectingcare services.
Allied Health & Support
The following Allied Health and Support Services have been provided in 2012/13, funded through the Department of Health, Small Rural Health Service funding initiative:
• McGrath Breast Care Nurse
• Optometry
• Audiology
• Physiotherapy
• Dietetics
• Speech Pathology – at request only
• Diabetes Education
• Generalist Counselling
Support Services
Support Services has provided catering and cleaning services for patients/residents, staff and visitors to our organisation during 2012/13. Catering, environmental, maintenance and gardening staff deliver high quality goods and services which meet all Victorian and Australian Standards in healthcare and ensure patients/residents stays are of the highest quality.
Education
Following the introduction of the National Health Care Standards in January 2013, all public Hospitals are subject to a requirement to maintain the professional standard of their services. All employees in public Hospitals must receive ongoing education to maintain the currency of their professional and vocational knowledge and skills.
To ensure that the organisation continues to achieve excellence in this area, Nathalia District Hospital has a strong commitment to the promotion of learning and the professional development of its staff. All staff at Nathalia District Hospital are required to maintain mandatory competencies as fundamental skills essential to safe practice. Competencies are individualised to work roles and work areas, and include; Advanced Life Support (Registered Nurses), Basic Life Support (all other staff), medication administration, manual handling, food safety, fire and emergency training, hand hygiene & bullying & harassment training.
The organisation employs a nurse educator to manage the professional development and ongoing education of its nursing staff.

N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3 85
Following an annual education needs analysis being completed in 2012, an education plan was developed for the 2012/13 year, which now provides weekly education opportunities for all staff. Internal training is delivered via a number of different platforms utilising tried and trusted methods of training such as face to face and visual delivery, to the latest technology including online training, and tele & videoconferencing. These education sessions help staff to maintain their skills and to further expand their knowledge base.
Work Placements & Experience for StudentsThe organisation continues to support the development of the health workforce of the future by supporting student placement.
The organisation continues to accept students from various education providers, ranging from higher education institutions such as La Trobe & Charles Sturt Universities to local schools, Nathalia Secondary College & St. Mary of the Angels Secondary College.
Staff have supported the placement and development of students at many levels and differing disciplines, including; medical students, physiotherapy students, nursing students (both enrolled and registered), through to work experience students, VCAL and community placement students.
External StudyWithin the organisation staff continue to be supported to upgrade their qualifications. Many staff have undertaken different types of external training, including: nursing traineeships, Diploma of Nursing, OH&S training, Certificate IV in Training & Assessment, infection control, Food Safety auditing, cleaning auditing etc.
The Hospital continues to support the up-skilling of enrolled nurses to registered nurses through a partnership with Charles Sturt University.
n a t h a l i a D i s t r i C t h o s p i t a l - a n n u a l r e p o r t 2 0 11 / 1 2

86 N a t h a l i a D i s t r i c t h o s p i t a l - Q u a l i t y o f c a r e r e p o r t 2 0 1 2 / 1 3
This page has been left blank intentionally


www.nathaliahospital.org.au
Nathalia District Hospital & Banawah Nursing Home36-44 McDonell St, Nathalia, VIC 3638
Phone: (03) 5866 9444
Fax: (03) 5866 2042
E-mail: [email protected]
Nat
halia
D istr ict Ho
spit
al
Providing Quality Care