a mini thesis in partial fulfilment of the …s3.amazonaws.com/zanran_storage/ · development...
TRANSCRIPT

A MINI THESIS IN PARTIAL FULFILMENT OF THE MASTER IN
DEVELOPMENT STUDIES (MDS)
ASSESSMENT OF THE IMPACT OF HIV/AIDS ON RURAL LIVELIHOODS
CENTRE FOR DEVELOPMENT SUPPORT
P O Box 339
University of the Free State
BLOEMFONTEIN
9310
Willys C Simfukwe January 2003

2
ACKNOWLEDGEMENTS Willys Simfukwe, a Project Manager with Catholic Relief Service (CRS) in Zambia, together with
Mathews Ngosa, the Agricultural Coordinator for the Catholic Diocese of Ndola, have been
responsible for facilitating the study.
The study has been conducted both as dissertation for a Masters of Development Studies (MDS),
with the Center for Development Support (CDS), University of the Free State, Bloemfontein, and
as a community assessment for designing a long-term food security project in the rural areas of the
Diocese of Ndola. Funding for the study has been provided by CRS, under the direction of
Michele Broemmelsiek, the Country Representative in Zambia.
The study has been made possible by high investment of time and energy. Fifty-eight people who
included Community Health Workers and Clinical Staff from Fiwale Mission Hospital, Mishikishi
Rural Clinic, Kafulafuta settlement, and Kafubu Health Center. The contributions of Mathews
Ngosa and Chanda ChimpwenA throughout the stages from design to monitoring the research
process are highly appreciated. I would also like to thank Joackim Kasonde for the encouragement
and interest in the study. I cannot forget to appreciate the inputs of Mrs. Kunda who typed the
translated version of the questionnaire.
I would like to express my sincere gratitude to Michele Broemmelsiek and John Donahue for the
financial support and allowing me time to conduct the study in Masaiti. Special thanks to Dorie
Olivier, Professor Lucius Botes and Professor Herman van Schalkwyk for the timely support and
advice. Lastly, my sincere gratitude go to my wife Brenda who endured the lonely moments
without complaints when I was away conducting the study. Bravo to my son Alinani who always
jumped on my laps and joined in typing with his toddler fingers.

3
ABSTRACT Because of lack of data to inform the design of a food security project in an HIV/AIDS
environment in Masaiti District in Zambia, a Study was conducted in three farming blocks of
Mishikishi, Kafubu and Fiwale. The objective was to explore and review literature on the impact
of HIV/AIDS on rural livelihoods and food security, establish steps to build the capacity of rural
communities in analyzing and mitigating the impact of HIV/AIDS on their livelihood systems,
and generate information for designing a long-term Livelihoods and food security program in the
rural areas of the Diocese of Ndola. The study shows that applying the Sustainable Livelihoods
Approach (SLA) provides a holistic and participatory approach to engage local rural households in
analyzing the impact of HIV/AIDS on their livelihoods. The study provides some insights on the
impact of HIV/AIDS on livelihood assets and activities. It proposes a number of coping and
mitigation strategies.

4
ACRONYMS AND ABBREVIATIONS AIDS : Acquired Immune Deficiency Syndrome BMI : Body Mass Index CBO : Community Based Organization CBOH : Central Board of Health CCZ : Christian Council of Zambia CDS : Center for Development Support CHAZ : Christian Health Association of Zambia CIDA : Canadian International Development Agency CMAZ : Christian Medical Association of Zambia COPE : Community-based Options for Protection and Empowerment CRS : Catholic Relief Services DANIDA : Danish International Development Agency EFZ : Evangelical Fellowship of Zambia FAO : Food and Agriculture Organization of the United Nations GDP : Gross Domestic Product GTZ : German Technical Assistance to Zambia HBC : Home-Based Care HIV : Human Immuno Virus INGO : International Non Governmental Organizations JACH : Jerusalem Association Children’s Home in RSA MOH : Ministry of Health MSF : Medicien San Frontier NGO : Non-Governmental Organization NHAC : National HIV/AIDS Council NPO : Non-Profit Organization PLA : Participatory Learning and Action PRA : Participatory Rural Appraisal PRS : Poverty Reduction Strategies ROSCAs : Rotating Savings and Credit Associations SAP : Structural Adjustment Programme SARO : Southern Africa Regional Office for CRS SL : Sustainable Livelihoods SLA : Sustainable Livelihoods Approach STD : Sexually Transmitted Disease STI : Sexually Transmitted Illness TAC : Treatment Action Campaign in South Africa TB : Tuberculosis UNAIDS : Joint UN Programme on HIV/AIDS UNDP : United Nations Development Programme UNICEF : United Nations Children Emergency Fund USA : United States of America USAID : United States Agency for International Development VSO : Volunteer Services Organization WHO : World Health Organization ZEC : Zambia Episcopal Conference

5
CONTENTS ACKNOWLEDGEMENTS ........................................................................................................ 2 ABSTRACT................................................................................................................................ 3 ACRONYMS AND ABBREVIATIONS ...................................................................................... 4 LIST OF TABLES...................................................................................................................... 7 LIST OF FIGURES ................................................................................................................... 7 MAPS .........................................................................................Error! Bookmark not defined. CHAPTER ONE........................................................................................................................ 8 1. Introduction......................................................................................................................... 8 1.1 General Background......................................................................................................... 8 1.2 The sustainable livelihoods approach .............................................................................. 9 1.2.1 Livelihood definition ...................................................................................................... 9 1.3. The HIV/AIDS situation in Zambia................................................................................. 12 CHAPTER TWO: THE STUDY .............................................................................................. 14 2.1 Rationale of the study.................................................................................................. 14 2.2 Aims and Objectives of the study ................................................................................ 15 2.3. Methodology ................................................................................................................. 15 2.3.1 Study Design ................................................................................................................ 15 2.3.2 Data sources, collection tools and techniques............................................................. 16 2.3.3 Site Selection................................................................................................................ 17 2.3.4 Sample size and sampling ............................................................................................ 18 2.3.5 Ethical Considerations................................................................................................. 19 2.3.6 Study management and Quality Control...................................................................... 19 2.3.7 Data Analysis ............................................................................................................... 20 2.4.7 Limitations of the study................................................................................................ 20 Chapter 3: Literature Review ................................................................................................ 21 3.1. AIDS as a development Issue...................................................................................... 21 3.2 AIDS as a rural Issue.................................................................................................. 23 3.3 Impact of HIV/AIDS on rural households................................................................... 25 3.3.1 Impact on rural women................................................................................................ 25 3.3.2 Impact on nutrition and food security.......................................................................... 26 3.3.3 Labour Loss or Stress .................................................................................................. 29 3.3.4 Loss of agricultural knowledge and management skills .............................................. 30 3.3.5 Declining yields. .......................................................................................................... 31 3.3.6 Loss of Income ............................................................................................................. 32 3.3.7 Increased Household expenditure................................................................................ 32 3.3.8 Impact on the livestock sector................................................................................. 34 3.3.9 Impact on natural resources .......................................................................................... 38 3.4 Household and community responses to the impact of HIV/AIDS ............................. 38 3.4.1 Household responses aimed at improving food security ............................................... 40 3.4.2 Household responses aimed at raising income and maintaining expenditure .............. 40 a. Income diversification......................................................................................................... 40 b. Shifting, reducing or cutting back expenditure................................................................... 41 c. Sale of farm produce, assets and use of savings ................................................................. 41 d. Loans................................................................................................................................... 42 e. Role of the extended family ................................................................................................. 43 3.4.3 Household responses aimed at alleviating the loss of labour........................................ 43 a. Intra-household reallocation of labour and taking children out of school ........................ 43 b. Hiring labour ...................................................................................................................... 45 c. Changing household crop production and substitution of crops ........................................ 45

6
d. Decreasing the area cultivated .......................................................................................... 45 e. Lengthening of the working day.......................................................................................... 46 3.4.4 Other household responses ............................................................................................ 46 3.5 Vulnerability of rural households to the impact of HIV/AIDS.................................... 47
CHAPTER FOUR: STUDY FINDINGS............................................................................ 50 4.1 Background information (Demographics)........................................................................ 50 4.2 Livelihoods........................................................................................................................ 52 4.2.1 Physical Assets............................................................................................................... 54 4.2.2 Social Capital................................................................................................................. 55 4.2.3 Financial Assets ............................................................................................................. 56 4.2.4 Intra-household asset control and use of Assets............................................................ 57 4.2.5 Livelihoods activities and labour distribution. .............................................................. 58 4.3 Impact of HIV/AIDS on Livelihood assets and activities (shocks and stresses) ............... 60 4.3.1 HIV/AIDS Prevalence and people’s perceptions........................................................... 61 4.3.2 Impact of HIV/AIDS on the households and their livelihoods....................................... 62 4.2.3 Coping Strategies and Building Resilience.................................................................... 64 4.2.4 Lessons Learnt in Applying SLA to analyze the impact of HIV/AIDS ........................... 65 Chapter 5: Recommendations................................................................................................ 67 REFERENCES ........................................................................................................................ 68

7
LIST OF TABLES Table 1. Zambia’s trends in growth rate with and without AIDS 2002 and 2010.......................... 21 Table 2 potential impacts of AIDS on households ..........................Error! Bookmark not defined. Table 3 The three stages of loss management ................................................................................ 39 Table 4. Household coping strategies ............................................................................................. 40 Table 5: Community responses towards HIV/AIDS.........................Error! Bookmark not defined.
LIST OF FIGURES Figure 3.1 Relationship between poverty and HIV/AIDS .............................................................. 22

8
CHAPTER ONE
1. Introduction
1.1 General Background Southern Africa is one of the regions most severely affected by HIV/AIDS. Although HIV/AIDS
epidemic started late in Southern Africa, it has been explosive, reaching prevalence rates of above
30 percent in some countries such as Botswana and Swaziland. In the midst of many other
challenges, Southern Africa has the world’s worst HIV epidemic, and indeed some analysts
suggest that all developmental activities in the region should be seen through an HIV/AIDS lens.
Roughly one-third of HIV-infected people — 11 million, the majority of them women — live in
Southern Africa. While HIV-prevalence ranges from 0.15 percent in Madagascar to 35.8 percent
in Botswana, Malawi, Zambia, Zimbabwe and South Africa have prevalence rates greater than 15
percent (CRS SARO, 2002). In Swaziland, 33.4 percent of the Swazis aged 15 – 49 years are
affected by HIV/AIDS (Muwanga, 2002). A CORDAID country situational analysis 2001 report
indicates that 139 people die every day from an AIDS-related illness in Malawi (Kapwepwe and
Siamwizia, 2001).
The impact of HIV/AIDS is challenging the development gains in Sub-Saharan Africa. Based on
the Millennium goal of halving the proportion of people living in absolute poverty by 2015, there
is increasing focus on the critical importance of poverty reduction for people-centered sustainable
development. This calls for a shift in the definition of development from purely economic growth
to socioeconomic and human development. The recent debate on the measurement of poverty has
led to emphasis on the use of poverty indicators and human development indexes rather than
measurement purely in terms of per capita income or economic growth. This has resulted in the
development of Poverty Reduction Strategies (PRS) that are linked with macroeconomic and
structural reforms. It is important to note that the PRS follow on to the Structural Adjustment
Programmes (SAP), which had a knocking-effect on the livelihoods of the majority of people in
Sub-Saharan Africa. The PRS address three key elements: a) economic growth with use of labour
of the poor as one of their most important assets; b) investment in human capital; and c) creation
of safety nets for the most vulnerable.
In addition to that PRS are macro oriented, meso and micro level strategies are required to
adequately mitigate the impact of HIV/AIDS on the individuals, households and local
communities. These meso and micro level strategies should be formulated on the basis of
community and household level empirical data. This study seeks to explore the information on the

9
impact of HIV/AIDS on rural livelihoods, to establish steps to build the capacity of rural
communities in analyzing and mitigating the impact of HIV/AIDS on their livelihood systems. It
is anticipated that the application of the Sustainable Livelihood Approach (SLA) in the study, will
generate information for designing a long term Livelihood and food security program in the rural
areas of the Diocese of Ndola. The following section provides an overview of the SLA.
1.2 The sustainable livelihoods approach The Sustainable Livelihood Approach puts people at the center of development. It recognizes that
the poor are the managers of complex asset portfolios. It seeks to understand the multiple
livelihoods that people pursue and the changes occurring over time, the resources used in
livelihood activities, the constraints faced and available opportunities. The approach aims to build
the capacity of local people, for them to be better able to pursue their own livelihood strategies.
The SLA requires action in enhancing the participation of people in devising their livelihood
intervention options and adopting people-centered strategies; raising the human capital status of
households and communities; combating the devastating impact of HIV/AIDS epidemic;
promoting formal and informal employment; and ensuring appropriate utilization of natural
resources (UNDP, 2001).
1.2.1 Livelihood definition
A livelihood is combination of activities, assets (natural, physical, financial, human, social), and
the access to these, and capabilities that are mediated by institutions and social relations to enable
an individual or household to gain a living (de Satge, 2002). The figure below provides a simple
pictorial view of livelihood definition
A livelihood is depicted by a triangle formed by the interaction of capabilities, assets (and access
them), and activities that are influenced by institutional and social relations. Every livelihood is
one way or the other exposed to, and affected by shocks and stresses (see figure 1.1 below).
Assets are the resources used for gaining a livelihood. Capabilities are the combined knowledge,
skills, state of health and ability to labour or command labour of a household (de Satge, 2002)

10
FIGURE 1.1 LIVELIHOOD MODEL Source: Adapted from CARE, DFID, Oxfam and LAL livelihood frameworks Assets are subdivided into five categories. The categories include
Natural assets these include water, rainfall, forests, wildlife, and land. Natural assets can
be enhanced or augmented when brought under human control and usage that increases
productivity.
Human assets refer to the labour available to the household, skills, education and health
status, and the ability to find and use information to cope with, recover from and adapt to
shocks and stresses. Investing in education and training increase it. The human assets in a
household are dynamic, constantly changing due to internal demographic changes (death,
birth, marriage, etc) or external pressures.
LIVELIHOOD
A S S E T S
CAPABITILITIES
ACTIVITIES
ACCESS Shocks Stresses
Shocks Stresses
Shocks Stresses

11
Physical assets refer to the basic infrastructure (housing, buildings, transport, energy,
communication, etc.) and production equipment and inputs (tools, seeds, etc.) that enable
people or households to pursue livelihoods.
Financial assets refer to cash, loans, savings, gifts, regular remittances or pensions, and
other financial instruments, which are available to people and provide them with diverse
livelihood options.
Social assets refer to networks, membership of groups, relationships of trust, access to
wider institutions in society, freedom from violence. It also includes reciprocity within and
between families, and in communities, the support provided by religious, cultural and
informal organizations. Social assets are enhanced and maintained by a culture of human
rights and democracy and by vibrant local institutions. Political capital should be
considered as a sixth asset. It refers to citizenship, enfranchisement and membership
political parties (Adato & Meinzen-Dick, 2002).
In addition to assets, shocks, risks, vulnerability and sustainability are common terms in the
livelihoods vocabulary. These terms are defined below
Shocks are sudden events, which undermine household livelihoods. These include loss of
employment, death of an economically active household member, as well as impact of
natural hazards like drought, floods or extreme weather conditions that are often made
worse by mismanagement of the environment. Stresses are ongoing pressures, which face
households and individuals. They include long-term food insecurity and limited access to
essential services and facilities. The degradation of the natural resource base is another
stress that may force people to travel long distances for fuel and other natural resources (de
Satge, 2002).
Risk is the chance of a shock or disaster event occurring or the chance of a loss or the loss
itself.
Vulnerability refers to the capacity of an individual or household to deal with a risky event.
The capacity to deal with risks depends on the resources available to an individual or
household to protect against risks and manage losses afterwards. Vulnerability also refers
12
to the characteristics that limit an individual, a household or a community to anticipate,
manage, resist or recover the impact of shocks (a hazard or natural trigger).
Sustainability refers to specific characteristics and values in relation to the way people
carry out their activities as well as utilize assets and resources. Households have
sustainable livelihoods when they can cope with, and recover from shocks and stresses.
Livelihood sustainability entails that the natural resource base is maintained and
capabilities are enhanced now and for future generations (UNDP, 2002).
Gender is a key component of livelihoods analysis. It refers to the socially constructed roles
ascribed to males and females. It is important because the entitlements to resources and
vulnerability to shocks and stresses vary within the household based on gender. Entitlements are
resources, which people have the right to access.
1.3. The HIV/AIDS situation in Zambia
In Zambia, the first cases of AIDS-related sicknesses and deaths were reported in the early 1980s.
However, limited knowlegde about HIV/AIDS at that time coupled with lack of acceptance and
political will, delayed the response to the HIV/AIDS epidemic. At the time of wake up call, in the
early 1990s, the epidemic had spread to every corner of the country. The HIV/AIDS prevalence in
Zambia is among the highest in Southern Africa - almost 20 percent of the adult population is
infected with HIV virus (MOH/CBOH, 1999).
HIV/AIDS is a major social and economic challenge to the development process in Zambia. More
and more adults and children are getting infected every day. An estimated 25,000 babies are
infected each year with HIV through their mothers either during pregnancy or at birth, or through
breast milk. High rates of HIV prevalence have now been followed by sharp increases in mortality
due to AIDS. Women typically become infected with HIV much earlier than men, reflecting their
lack of knowledge about HIV/AIDS and their inability to protect themselves, and their
physiological vulnerability (MOH/CBOH, 1999). With its direct impacts on people’s health
(increased illnesses) and socioeconomic well being, HIV/AIDS is contributing to rising workload
especially for women, increasing costs in the health services and the depletion of human capital in
the Zambian economy. Vast differences in HIV prevalence are obvious both between urban and
rural areas and between regions. In urban areas, the prevalence rate among 15-49 year olds is

13
more than 28 percent while in rural areas it is 13.6 percent. In 1999, the highest HIV prevalence
was reported in the Lusaka and Copperbelt provinces (27.3 percent and 26.3 percent respectively).
Prevalence rates range between 15 percent to19 percent in the other five provinces – Luapula
(16.2 percent), Eastern (16.5 percent), Central (18.7 percent), Southern (15.7 percent) and Western
(18.9 percent). Prevalence is slightly lower in the Northern (13.5 percent) and Northwestern (11.7
percent) Provinces (MOH/CBOH, 999).
The determinants of the HIV prevalence in Zambia have been identified as: a largely young
population; high mobility and internal migrations; high levels of poverty; high prevalence of
sexually transmitted illnesses (STIs); multiple sexual relations; lack of male circumcision; low
social and economic status of women; early sexual activity and some cultural practices. Among
the macro determinants is the impact of the Structural Adjustment Program (SAP) and the high
debt burden (Kapwepwe and Siamwizia, 2001)
14
CHAPTER TWO: THE STUDY
2.1 Rationale of the study Despite Zambia being one of the highly urbanized countries, the majority of the people in Zambia
still lives in rural areas and depends mainly on agriculture for their livelihoods. Achieving food
security is one of the main objectives of the agricultural policy in Zambia. The need for food and
livelihood security in a country where almost fifty percent of child deaths are caused by
malnutrition cannot be overemphasized (UNICEF, 2001). The failure of agricultural policies and
extreme weather conditions has had a detrimental effect on the food security in Zambia. The
HIV/AIDS pandemic has exacerbated the poverty situation among rural households making them
more prone to food insecurity. The rural areas in Zambia are overwhelmed with high levels of
poverty- as high as 89 percent in some parts of the country (UNDP, 2001).
Since the early 1990s, anti-HIV/AIDS programs have been designed and implemented mainly in
the urban areas. The anti-AIDS programs have focused on HIV/AIDS awareness (information on
the causes and the spread of HIV/AIDS), while efforts to mitigate the impact of HIV/AIDS have
emphasized on the care for the sick (Home-Based Care and Community-Based Care) and support
of orphaned children. The anti-HIV/AIDS programs have resulted in the reduction of HIV/AIDS
infection rates especially in urban areas. Although there is a general stabilization and reduction in
HIV infections rates in urban areas, the rate of HIV infections in rural areas is rising rapidly
(UNDP, 2001). The rising rates of HIV/AIDS infections and the high levels of poverty are major
threats to the sustainability of rural livelihoods.
This study is important both as an explorative activity to understand the impact of HIV/AIDS on
rural livelihoods, and as capacity building activity to enhance the local communities’ capacity to
improve and sustain food security. The study is based on the principles of applied development
research, which emphasize a holistic approach and community ownership of the development
process and outputs. The study focuses on involving the local communities in analyzing their own
situations and determining their own courses of action. It is anticipated that the completed study
will provide useful information to organizations and individuals involved in HIV/AIDS
programming for rural areas in Zambia.
The application of the Sustainable Livelihood Approach (SLA) is based on the understanding that
while HIV/AIDS affects or impacts on every aspect of human life, the livelihoods approaches
offer a holistic way of addressing the HIV/AIDS epidemic which promotes joined up thinking

15
across sectors and disciplines, that can look not just at the impact on health but also at the impact
on social support, finances, housing, land-use and land tenure (Steely and Pringle, 2001). The
study is based on the premise that the impact of HIV/AIDS on agricultural production systems and
rural livelihoods cannot be generalized, even within one country, but must be disaggregated into
spatial and temporal dimensions. Studies conducted in Uganda, Tanzania and Zambia shows that
HIV/AIDS follows a different pattern in each village and district. Geographic and ethnic factors,
religion, gender, age, marriage customs and agro-ecological conditions play a role in the pattern
and impact of HIV/AIDS and in people's perception of the disease (FAO, 2001).
2.2 Aims and Objectives of the study
The study aims at the applying the Sustainable Livelihoods Approach in understanding the impact
of HIV/AIDS. It seeks to ascertain how to involve rural communities in incorporating HIV/AIDS
in livelihood analyses in order to improve the food security of HIV/AIDS affected households.
The specific objectives of the study were
1. To explore and review literature on the impact of HIV/AIDS on rural livelihoods and
food security.
2. To establish steps to build the capacity of rural communities in analyzing and
mitigating the impact of HIV/AIDS on their livelihood systems
3. To generate information for designing a long-term Livelihood and food security
program in the rural areas of the Diocese of Ndola
2.3. Methodology
2.3.1 Study Design
The study was designed as an explorative and interventional study. Firstly, it was designed to
explore and review information on HIV/AIDS and its impact on rural livelihoods and food
security. Secondly, the study was designed as a participatory intervention - involving local
communities in analyzing the impact of HIV/AIDS on their lives, and in designing long-term
strategies to mitigate its impact. The involvement of local community members in the study was
based on the appreciation of the extant local knowledge and initiatives in mitigating the impact of
HIV/AIDS. Local communities are already responding to the HIV/AIDS challenge in their own
way (home and community care systems, moral support to affected, etc). It was intentional that

16
this study should build on the existing local capacity to analyze and develop interventions to
mitigate the effects of HIV/AIDS.
2.3.2 Data sources, collection tools and techniques
For the literature review, published data was obtained from Zambian government agencies that
included the Ministry of Agriculture and Cooperatives, Ministry of Community Development and
Social Services; UN agencies FAO, UNDP, UNICEF; and CRS library. The key words used on
the Internet searches included HIV, AIDS, rural, livelihoods, food security, impact, and
agriculture in various combinations. A data compilation checklist was developed to focus the
literature review and Internet search on the necessary information needed for the study and to
avoid being swamped with too much information.
In addition to literature review and Internet searches, Participatory Rural Appraisal tools were
applied to engage the community and collect qualitative data. Key informant and normative
interviews were used to get information in the study areas - Fiwale, Mishikishi and Kafubu rural
settlements in Masaiti District. The initial process involved preliminary discussions and meetings
in communities for almost a month. Follow up meetings were then held with the Ndola Diocese
Development and Agricultural Team, Masaiti District Health Management Team, Fiwale Mission
Hospital, Mishikishi and Kafubu Health Center staff, and the Community Health Neighborhood
Committees. A second series of community meetings involved the selection and training of the
research teams. The research teams comprised of community health volunteers, staff from health
centers, the Diocesan Deanery Coordinator, and Agricultural Coordinator. The selection of the
community health workers to be involved in the study was based on the number of health
neighborhood committees in each study area. The minimum requirement for the team member
was the ability to read and write, and to translate the local language into English and vice versa.
Gender equity and wider community representation were key elements in assembling the research
teams. The table below shows the HIV prevalence in the study area.

17
TABLE 2.1. HIV PREVALENCE ESTIMATES FOR COPPERBELT PROVINCE OF ZAMBIA 1999
Province/District HIV HIV+ HIV+ HIV+ HIV+ HIV+ Prevalence Total Urban Rural Total 15 and 15-49 15-49 15-49 15-49 50+ Older
______________________________________________________________________________________________
Provincial 26.2% 197,543 185,618 11,917 12,591 210,125
Chililabombwe 25.8% 7,666 7,177 489 417 8,083
Chingola 28.1% 23,757 23,714 43 1,465 25,223
Kalulushi 24.4% 8,511 7,614 897 479 8,990
Kitwe 28.7% 54,762 54,762 - 3,502 58,264
Luanshya 26.6% 20,463 19,570 893 1,304 21,767
Lufwanyama* 12.8% 3,128 462 2,666 281 3,410
Mpongwe* 12.8% 2,294 339 1,956 207 2,501
Mufulira 26.9% 20,845 20,138 707 1,188 22,034
Masaiti* 12.8% 5,006 740 4,266 450 5,456
Ndola Urban 28.4% 51,100 51,100 - 3,297 54,397
______________________________________________________________________________________________
Source: Ministry of health and Central Board of Health 1999. * These are rural districts in province. The study sites are in Masaiti District.
2.3.3 Site Selection
Site selection was a three-step process; the selection of a district from among the three rural
districts in the province, followed by the settlements or villages within the district, then the Health
Neighborhood Zone in the village. The Lead Investigator based on the existence of the CRS
partner’s agricultural and rural resettlement activities chose the district. The Diocesan Agricultural
Team and local Community Health Volunteers who were more conversant with district and
settlement characteristics chose the farm settlements and Health Neighborhood Zones. The sample
sites for the study covered Fiwale, Kafubu and Mishikishi farm settlements in Masaiti district. The
three farm settlements were selected on the basis of:
i) Availability of a Rural Health Center;

18
ii) Existence of Community Health Committees;
iii) HIV/AIDS prevalence as recorded by the RHC and MOH/CBOH;
iv) Proximity and easier access to the urban centers; and
v) Existence of CRS partner agricultural activities
TABLE 2.2 STUDY SITES Farm Settlement
Mishikishi Kafubu Fiwale Health
Neighborhood
Zones
Kango-Moni
Nkumbwe
Mabungo/Mpangamumba
Fipempele/Chankute
Busalala
Kalalangabo-Matipa
Fipwika-Mushitu
Kashilalyashi
Zone 1
Zone 2
Zone 4
Zone 6
Makubi-Kanshiwa
Munkulungwe
Nkomesha 1
Ngwenya
Lumano West
Mwelemuka-Chikoti
Chinkuli-Mbalashi
Kangwena
Own source
2.3.4 Sample size and sampling
The household was used as a unit of measure. Sample size calculations were based on the percent
of the local population as recorded by the RHC. The Ministry of Health in collaboration with the
Central Statistics Office (CSO) has established standard population counts for every RHC in all
districts in Zambia. The research team conducted the mapping and demarcation of Health
Neighborhood (HN) zones to allow for a systematic random sampling. The households in each of
the HN zones were selected based on:
i) Presence of a terminally ill person for a period of six months or more;
ii) Death of a terminally ill person within the last five years;
iii) Membership in the community home-based care program
iv) Female headed and or child headed household; and
v) Well being of the household as classified by the local community members
The sample included female-headed, child-headed, and male-headed households. The study
targeted a total 498 households in the three selected sites. Community health workers and
volunteers in the Home-Based Care (HBC) programs were the key informants on the households
to target for interviews and focused discussions.

19
TABLE 2.3 TARGETED AND ACTUAL INTERVIEWS Site/Area Targeted Actual
Mishikishi 202 181
Kafubu 100 87
Fiwale 196 168
Total 498 436
Own source
2.3.5 Ethical Considerations Discussions were also held with research teams and general community to avoid reinforcing of
stigma and discrimination. In addition to that sensitive information regarding HIV/AIDS was
only obtained after establishing good rapport with informants and with their consent. The
inclusion of a household on the interview list was done after consultations with, and gaining
consent from the members of the household. Pre-survey discussions with provincial and district
health management officials ensured that ethical concerns were considered and properly addressed
during the study.
2.3.6 Study management and Quality Control
A clinical officer at each of the three health centers in the study area was selected as team leader
and process supervisor. In each study area, the research team provided their daily or weekly
feedback on the field experiences to the Clinical officer. The Diocesan Deanery Coordinator and
the Diocesan Agricultural Coordinator provided the supervisory back up to clinical officers and
monitored research process in the field. The lead investigator did the overall coordination and
management of the research process.
In order to avoid complacence and bias during field interviews, the interviewers within the
research teams were swapped so that they interviewed in the areas, which they knew but were not
too familiar with the people that they interviewed. The diversity of research team members
ensured that wide aspects were covered with minimal omissions of vital information. The
interviewing of several members in a household helped to clarify or refute uncertain responses. In
addition to that the Supervisors provided assistance in interpreting the responses. Apart from the

20
targeted HIV/AIDS affected households, interviews were also conducted with some that had no
terminally ill person or experienced AIDS related deaths
2.3.7 Data Analysis The analysis of data was done in two phases. Firstly, community level analysis was done through
group meetings. This provided a chance for community members to ascertain the data collected by
the research teams and appreciate the similarities and differences in selected sites. Secondly, the
lead investigator applied Microsoft Excel and Access for quantitative analysis.
2.4.7 Limitations of the study A number of problems were encountered and noted in this study. The high level of poverty in the
study sites provided a potential source of bias. It was not easy to differentiate the households
impacted by poverty from those impacted by HIV/AIDS. The limited number of in-country
studies and reports on impact of HIV/AIDS on rural households, made the lead researcher to rely
more on literature from other countries for review.
The second limitation relates to the selection of study sites. The study sites chosen could not
ensure complete representation at district or national level. The study sites were chosen on the
basis of the existing geographic coverage of the Catholic Diocese of Ndola agricultural
department, and the need to establish a long-term livelihoods improvement programme. Only a
full-scale district or national survey could provide complete and good representative data.

21
CHAPTER 3: LITERATURE REVIEW
The study design was based on the understanding that some work has been done on the subject
matter by other researchers. Reviewing what has already been done on HIV/AIDS and its impact
on rural livelihoods formed part of the study. The following section provides the results of the
literature review focusing on HIV/AIDS as development and rural issue, its impact on rural
households, and the household and community responses.
3.1. AIDS as a development Issue
AIDS is not just a health problem though it is often presented as one (Loevinsohn et al, 2001:7).
The UN Special Session on HIV/AIDS indicates that by killing so many people in the prime of
their lives, AIDS poses a threat to development. By reducing growth, weakening governance,
destroying human capital, discouraging investment and eroding productivity, AIDS undermines
countries’ efforts to reduce poverty and improve living standards (UN Fact sheet, 2001).
HIV/AIDS has a profound impact on growth, income and poverty. Over (1998) notes that the third
major impact of the epidemic is on households and, in the aggregate on the extent and depth of
national poverty. The UN estimates that the annual per capita growth, in half the countries of sub-
Saharan Africa is falling by 0.5-1.2 percent as a direct result of HIV/AIDS. It is also projected that
by 2010, per capita GDP in some of the hardest hit countries may drop by 8 percent and per capita
consumption may fall even further (UN Fact Sheet, 2001). The table below shows trends in
economic growth in Zambia with and without HIV/AIDS in 2002 and 2010.
TABLE 3.1. ZAMBIA’S TRENDS IN GROWTH RATE WITH AND WITHOUT HIV/AIDS 2002 AND 2010
Growth rate YEAR With HIV/AIDS Without HIV/AIDS Net Decrease 2002 1.6 2.9 1.3 2010 1.0 2.6 1.5 Source: adapted from Stanecki. K.A. Draft report July 2002, Barcelona Conference on AIDS People at all income levels are vulnerable to the economic impact of HIV/AIDS with the poor
suffering more acutely. HIV/AIDS pushes people deeper into poverty as households loose their
breadwinners to AIDS, livelihoods are compromised, and savings are consumed by the cost of
health care and funerals. The number of people living in poverty has increased up to 5 percent in
some countries as a result of AIDS. The AIDS epidemic is jeopardizing the efforts to reach the
Millennium Summit goal of halving the proportion of people living in extreme poverty by 2015
(UN Fact Sheet, 2001)

22
With increased poverty as a result of HIV/AIDS, impoverished people resort to commercial sex
and other coping strategies that increase the chances of contracting HIV/AIDS and hence creating
a vicious cycle. The links between HIV/AIDS and poverty are presented figure 3.1 below.
FIGURE 3.1 RELATIONSHIP BETWEEN POVERTY AND HIV/AIDS Source: adapted from UNAIDS/World Bank 2001, A Toolkit for Mainstreaming HIV/AIDS in Development Instruments As a result of the impact of HIV/AIDS on household economics, poverty is likely to deepen as the
epidemic takes its course. The above aspects of the socio-economic impact of HIV/AIDS
combine to create a vicious cycle of poverty and HIV/AIDS in which affected households are
caught up. As adult members of the household become ill and are forced to give up their jobs,
household income will fall. To cope with the change in income and the need to spend more on
health care, children are often taken from school to assist in caring for the sick or to work so as to
contribute to household income. Because expenditure on food comes under pressure, malnutrition
often results, while access to other basic needs such as health care, housing and sanitation also
comes under threat.
Consequently, the opportunities for children for their physical and mental development are
impaired. This acts to further reduce the resistance of household members and children
(particularly those that may also be infected) to opportunistic infections, given lower levels of
immunity and knowledge, which in turn leads to increased morbidity and mortality (Tanya, 2002).
Households headed by AIDS infected widows are also particularly vulnerable, because women
Structural vulnerability -> high-risk situations Lack of access to preventive interventions Lack of access to affordable care Lower education status -> reduced access to information on AIDS
POVERTY HIV/AIDS
Lost productivity Catastrophic cost of health and death Increased dependency ratio Orphans with worse nutrition, lower school enrolment Decreased capacity to manage households headed by orphans, elderly Reduced national income Fewer national resources for HIV/AIDS control

23
have limited economic opportunities and traditional norms and customs may see them severed
from their extended family and denied access to an inheritance (UNDP, 1994). In many third
world situations, therefore, HIV/AIDS exposes already vulnerable, resource-poor households to
further shocks (Tanya, 2002). The impact is worse if the family is a low-income household,
because such households generally possess few resources, and thus are less able to cope with
increased medical care and other related expenses (Pitayanon et al. 1997).
At national level, governments lose valuable skilled staff and are faced with mounting expenses
for health and orphan care, reduced revenues and lower return on social investment (UN Fact
Sheet, 2001). World Bank studies indicate that the average cost of treating an AIDS patient from
time of diagnosis to death ranges from US $100 to US $1100 in Africa. In Zambia, AIDS care
expenditures are projected to increase from US $3.4 million in 1989 to US $18.3 million in 2004
and to US $22.1 million (MOH/CBOH, 1999). The AIDS epidemic has increased the prevalence
of opportunistic infections such as tuberculosis, which was contained before the 1980s. The
interaction of tuberculosis and HIV infections has contributed to almost a five-fold increase in the
TB rate (UNDP, 2001).
As result of HIV/AIDS, the public, private, and civil society sectors are faced with higher costs in
training, insurance, benefits, absenteeism and illness (UN Fact sheet, 2001). Productivity falls
even among people not living with HIV/AIDS as they have to take time off their productive
activities to care for sick relatives and friends or attend funerals. Absenteeism and death have
plagued the labour force, and have affected the quality of education, food security and quality of
health care (UNDP, 2001). The ultimate result is reduction in annual per capita growth in GDP. If
AIDS epidemic trend continues, productivity growth may be cut by as much as 50 percent in hard-
hit countries. HIV/AIDS overburdens social systems and hinders health and educational
development. It undermines social cohesion in many countries and is increasingly recognized as a
threat to social and political stability.
3.2 AIDS as a rural Issue
One of the common characteristics of developing countries is the substantial dependence on
agricultural production for food and income. The vast majority of people in developing countries
lives and works in rural areas. Over 65 percent are rural based, compared to less than 27 percent in
economically developed countries (Todaro, 1997). HIV/AIDS, which was once an urban

24
problem, has moved to rural areas. Chief David Lingazwe of Amambisi Tribal Authority in South
Africa said the AIDS epidemic had taken every one by surprise. “…We thought it was a town
thing, we didn’t know it would kill our families like this…” (IRIN-SA 2001 quoted in Steely and
Pringle, 2001). In Zambia, the UNDP observes that the rate of HIV infections is rising faster in
rural areas than in urban areas where it is stabilizing (UNDP, 2001). The Food and Agricultural
Organization (FAO, 2001) reports that HIV/AIDS was no longer restricted to cities. The disease
was spreading with alarming speed into rural areas and affects the farming population, especially
people in their most productive years (ages 15 to 45). More than two-thirds of the population in
25 most affected African countries lives in the countryside.
Although interrelations between the epidemic and overall development have been acknowledged,
the linkages to agriculture have received less attention because the epidemic was perceived as
being largely urban. The existing evidence of the spread of the epidemic to rural areas was often
overlooked because of poor data, the irregular patterns of spread and lower prevalence than in
urban areas (FAO, 2001). Pitayanon, Kongsin and Janjaroen (1997) noted that the largest
proportion of AIDS cases had been reported in Thailand’s Northern Province mainly in rural
areas. Labourers and agricultural workers, who are generally the poorest and least educated, are
the most vulnerable to HIV/AIDS. In Sub-Saharan Africa, millions of rural people suffer from
chronic poverty, socio-economic marginalization, food insecurity and, most recently, the
devastating impact of the HIV/AIDS epidemic. In a study in Malawi, Loevinsohn et al (2001)
reported HIV to be more prevalent in urban than non-urban areas in early stages of the epidemic.
Though the differences in prevalence have remained, the gap is steadily narrowing. The median
prevalence among non-urban sentinel sites (antenatal clinics) increased in relation to urban sites
from about 20 percent in 1992 to 70 percent in 1998. Gari (2002) reports that the combined threat
of the food insecurity and the impact of AIDS are leading to a rural development crisis. In poor
rural households, HIV/AIDS causes severe labour and economic constraints that disrupt
agricultural activities, aggravate food insecurity, and undermine the prospects for rural
development. The HIV/AIDS pandemic is undoing the decades of economic and social
development causing rural disintegration.

25
3.3 Impact of HIV/AIDS on rural households
3.3.1 Impact on rural women
From the gender perspective, women and girls are more vulnerable to HIV/AIDS and shoulder the
largest burden. Girls are removed from school to care for sick relatives. The reduced education for
girls and women further impedes national development (UN Fact sheet, 2001). Since HIV/AIDS
is above all a sexually transmitted disease, very often more than one family member is affected
and dies. As a result, the entire assets and savings of many families, which are generally meager
before the onset of the disease are completely depleted, leaving the surviving family members
without means of support. A study in Uganda has shown that the burden of the socio-economic
impact of HIV/AIDS is disproportionately affecting rural women. In the districts studied, more
households were found to be headed by AIDS widows than by AIDS widowers. Widows with
dependent children became entrenched in poverty as a result of the socio-economic pressures
related to HIV/AIDS. Widows lost access to land, labour, inputs, credit and support services.
HIV/AIDS stigmatization compounded the widow’s situation further as assistance from the
extended family and the community; their main safety net was discontinued.
The loss of productive labour force in agriculture - the mainstay of rural areas, excessive use of
natural resources, lack of good policies, and extreme weather conditions have had a devastating
effect on the food security in rural areas. As stated earlier, the socioeconomic impact of
HIV/AIDS includes among others the loss of livelihood at household level; increased vulnerability
to food insecurity and increased malnutrition; and the break up of family structures. The lack of
food in already impoverished rural populations is reinforcing the effect of HIV/AIDS by
weakening long established rural survival mechanism of subsistence agriculture thereby trapping
the rural communities in a poverty vicious cycle. The inter linkages between the increase of
HIV/AIDS-related mortality and morbidity, the lack of farm inputs and labour force, the
deterioration of household economy and the impact on education, health and the social system,
which eventually lead to a breakdown of the traditional coping mechanisms, are presented in
figure 3.2 below. The figure indicates that immediate effects of increased HIV/AIDS morbidity
and mortality on rural economies are shortage of labour; loss of agricultural and community
organization skills; and a marked increase in poverty among women. With increased
stigmatization, the immediate effects are followed with severance of assistance from extended
family and the community. As a result affected households become more impoverished, education

26
for children is discontinued, and health status declines, and social values are eroded leading to the
collapse of both nuclear and extended families.
FIGURE 3.2 THE IMPACT OF HIV/AIDS ON TRADITIONAL COPING MECHANISMS IN RURAL ECONOMIES (ADAPTED FROM FAO)
3.3.2 Impact on nutrition and food security The trend towards increasing food insecurity in Zambia and the region as a whole should be
viewed within the context of a deepening HIV/AIDS crisis, just as the HIV/AIDS pandemic must
be understood as inter-related on many levels to the region’s food security situation (CRS SARO,
2002). The HIV/AIDS epidemic in Sub-Saharan Africa is strongly intertwined with issues of food
and nutrition. On one hand, malnutrition and food insecurity may force households to adopt
Increase of HIV/AIDS mortality and morbidity
Loss of agriculture and community organization skills Shortage of labour Marked increase in poverty
among women
Farm households lose access to cash, income, credit, farm inputs and supply services
AIDS widows lose access to land, labour, cash, income, credit, farm outputs and support services
AIDS stigmatisation
Severance of assistance from the extended family and community
Breakdown of nuclear family
Household economy impoverished
Education discontinued
Health status declines
Social values eroded
Extended family network strained to breaking point

27
livelihoods that increase the risk of HIV transmission, such as migration to find work. On the
other, HIV/AIDS may precipitate or exacerbate malnutrition and food insecurity (Gillespie and
Haddad, 2002). The extent to which malnutrition rates in affected households rise depends on the
type of coping mechanisms, household resource constraints, socio-cultural context and emotional
stress. As the ability to produce and accumulate food and income decreases, the household falls
into a downward spiral of increasing dependency ratios, poorer nutrition and health, increasing
expenditure of resources (time and money) on health problems, more food shortages, decreasing
household viability, and increasing reliance on support from extended family and the wider
community. The effects of HIV/AIDS on rural households, and the likely impact of the disease on
farmers’ health and the nutrition of farm families are depicted in figure 3.3 below.
FIGURE 3.3 IMPACT OF HIV/AIDS ON THE FOOD AND NUTRITION SITUATION OF RURAL HOUSEHOLDS (ADAPTED FROM FAO)
Reduced labour
Reduced land use
Reduced extension
Increased sale of farm assets
Reduced agricultural production
Loss of other income sources
Increased health costs
Reduction in schooling
Increased funeral costs
Reduced clothing & shelter
etc…
Reduced access to wild food
Reduced income
Increased non-food expenses
Reduction in food available at farm level
Reduced food purchases
Reduced K.A.P
Reduced time
Reduced access to water
Poor sanitation
Reduced access to food (household food security)
Reduction in food selection, preparation and distribution Reduced health
services Poor hygiene
Reduced food intake
Reduced Health status
Poor Nutrition

28
The risk of HIV transmission may precipitate or exacerbate malnutrition and food insecurity
(Gillespie and Haddad, 2002). The main link between HIV/AIDS and food security is the potential
for people living with HIV/AIDS to use nutrition to enhance the quality and longevity of life.
Conversely, malnutrition leads to an impaired immune response, which accelerates AIDS (CRS
SARO, 2002). Gillespie and Haddad (2002) state that HIV/AIDS has direct impacts on nutrition
for the individual, the household, and the community. HIV infection, compounded by inadequate
dietary intake, rapidly leads to malnutrition. They further state that people living with HIV have
higher than normal nutritional requirements: as high as 50 percent more protein and 15 percent
more calories. However, they are likely to suffer from loss of appetite and anorexia, which
reduces the dietary intake at the time when nutritional requirements are greatest. Loevinsohn et al.
(2001) state that AIDS strain already meager diets and pushes many into a vicious cycle – failure
to maintain nutrition status weakens immunity and increases susceptibility to opportunistic
infection, which in turn undermine the nutritional status.
Research in Zambia, for example, has indicated that the labour loss resulting from AIDS deaths
are particularly critical in rural areas, with deaths often resulting in increased food insecurity
(Nampanya-Serpell, 2000). The four in-depth profiles of affected families in rural Uganda
presented by Topouzis and Hemrich (1994) paint a similar picture. Ikamari (1991, in Forsythe
and Rau, 1998: S51 quoted in Tanya 2002), in a survey of the families of 52 individuals who had
died of AIDS, found that these deaths had a significant impact on the household's nutritional
status. It, however, is unclear how exactly changes in nutritional status were monitored in these
two studies. The impact of HIV/AIDS on nutritional status has been explored extensively in the
household impact study the World Bank conducted in Kagera district in Tanzania between 1991
and 1994. Increased consumption on health care and burials saw per capita food consumption
drop by 16 percent amongst the poorest half of households affected by an adult death. Stunting
amongst AIDS orphans was higher than amongst other children (Over, 1998b).
HIV/AIDS undermines food security through its impact on: households’ ability to produce food
due to labour shortages or stress. The cumulative scale of morbidity and mortality due to
HIV/AIDS causes increasing labour losses in affected households (Gari, 2002). AIDS morbidity
forces infected individuals within households to cut back the number of hours that they work. A
study in Rwanda showed that 56 percent of HIV-positive household members lost or missed at
least one day of work in within two weeks due to ill-health, nearly 35 percent missed one week or
more, while 20 percent could not work at all (Nandakumar et al, 2000, as quoted in Tanya, 2002).

29
In Tanzania, it is estimated that a sick man will loose 297 days of work and a sick woman 429
days over an 18-month period (Rugamela, 1999). The estimates were based on the assumption that
the AIDS illness is 18 months in duration and that 12 of the 18 months are spent in bed. Rural
households affected by AIDS suffer labour stresses that affect farm, off-farm, and domestic work.
Labour loss disrupts agricultural practices and, hence aggravates livelihood vulnerability and food
insecurity (Gari, 2002).
3.3.3 Labour Loss or Stress Rapid population growth has often been considered the greatest population problem in Africa.
However, in some rural communities HIV/AIDS is now causing labour shortages for both farm
and domestic work. HIV/AIDS has quantitative and qualitative impacts on labour in rural
communities by reducing the household's workforce, as people die or spend time on mourning,
attending funerals and caring for sick household members; and by reducing skills and changing
the gender division of labour depending on how the farm-household members are affected (du
Guerny, 2000). HIV/AIDS escalates the morbidity and mortality predominantly on the most active
and productive segment of the rural society (Gari, 2002). The impact of HIV/AIDS on the
households has three stages – illness, death and the longer-term consequences of AIDS morbidity
and mortality (Loewenson and Whiteside, 1997). When HIV/AIDS strikes, it strips away assets of
all forms – human, financial, social, physical, and natural. Human capital is the first casualty.
Infected individuals die prematurely, before which their productivity declines progressively as
they succumb to opportunistic infections (Gillespie et al, 2002).
A study by FAO in East Africa found that labour-intensive farming systems with a low level of
mechanization and agricultural input were particularly vulnerable to the impact of AIDS. Some of
the effects of labour shortage in full impact communities in Eastern Africa were: reduction in the
acreage of land under cultivation; delay in farming operations such as tillage, planting and
weeding; reduction in the ability to control crop pests; decline in crop yields; loss of soil fertility;
shift from labour-intensive crops (e.g. banana) to less labour-intensive crops (such as cassava and
sweet potatoes); shift from cash-oriented production to subsistence production; reduction in the
range of crops per household; and decline in livestock production (FAO, 2001).

30
Figure 3.4 Projected Labour Loss: source FAO
The figure indicates that the loss in agricultural labour force in the nine hardest hit African
countries will range from 13 percent in Tanzania to 26 percent in Namibia between 1985-2020.
3.3.4 Loss of agricultural knowledge and management skills
Agro biodiversity and indigenous knowledge represent locally available agricultural assets with
enormous value and potential in rural food and livelihood security (Gari, 2002). HIV/AIDS leads to
loss of agricultural knowledge. People die before passing knowledge and expertise to the next
generation. A study in Kenya showed that only seven percent of agricultural households headed by
orphans had adequate knowledge of agricultural production. In Kenya's Ministry of Agriculture, 58
percent of all staff deaths are caused by AIDS, and in Malawi's Ministry of Agriculture and
Irrigation at least 16 percent of the staff is living with the disease. One study found that up to 50
percent of the time of agricultural extension staff was lost through HIV/AIDS in sub-Saharan
Africa (FAO, 2002).

31
HIV/AIDS generates a paradox regarding agro biodiversity and indigenous knowledge. It disrupts
customary agricultural systems, socio-demographic structures, and community dynamics; it further
impairs the maintenance of agro biodiversity and indigenous knowledge (Gari, 2002). Gillespie and
Haddad (2002) indicate that AIDS drastically abbreviates that the ability of parents and other elders
to transfer knowledge, both within their own generation and to the next. AIDS impairs the ability of
children to acquire and use information even through formal education, as children are pulled out of
school to reinforce the family’s ability to care for the sick, to maintain its current livelihood, or to
develop new livelihoods. In many areas, the usual way for children to learn the required
agricultural skills is by working with their parents. Given the AIDS pandemic, this is often no
longer possible and, owing to the gender division of labour and knowledge, the surviving parent is
not always able to transfer the skills of the deceased one.
In a study in Namibia, Du Guerny et al. (2000) note that in households where both the husband and
wife died there was total inability of the child-headed households to produce enough food for their
own consumption. This was a result of both inadequate resources and inability to use and manage
the limited available resources for optimum crop production. In addition to poor crop and weed
management, the children also lacked skills for livestock management resulting in the death of the
few livestock inherited. Such events ill intensified the food security problems of the child-headed
households unless appropriate mitigating interventions are put in place. Muwanga (2002) states that
the death of parents may signal the end of farming in the household. This illustrates also the limits
of community and family solidarity.
3.3.5 Declining yields.
Du Guerny (1999) noted that reduction in yields are less immediately visible but important and are
caused by a variety of factors including delays or poor timing in such essential farming operations
as tillage, planting and weeding. Delays occur because of sickness or dependency on outside
labour, which is not always available when needed (e.g. relatives who assist through solidarity
first care for their own fields). It also seems that the fertility of the soil is affected negatively
owing to the priority given to immediate survival concerns over longer-term land conservation
measures. In Swaziland, Muwanga (2002) found that households that had experienced an AIDS
related death had 54.2 percent reduction in maize production and 29.6 percent reduction in cattle
herd growth. In Zimbabwe, households that experienced an AIDS death had 61 percent reduction
in maize production.

32
3.3.6 Loss of Income HIV/AIDS damages financial capital in number of ways. Expenses on drugs, funerals, burial and
related transport costs strain already limited family budgets (Gillespie and Haddad, 2002). A study
in the rural areas of Thailand indicated that the economic impact of an HIV/AIDS death on a rural
household measured in terms of direct and indirect costs per death were substantial, and were
greater than costs of death from other causes that occurred in the community during the same
period. The negative impact of an HIV/AIDS related death on the household labour supply for
family production was substantial, and affected about 52 percent of households that engage in
economic activities. The loss was almost 50 percent, leading to about a 47 percent loss in
household income (Pitayanon et al, 1997). Households living in rural Chanyanya in Kafue district
in Zambia that were affected by chronic illness had an annual income 46 percent lower than
households in the same area that were not affected by chronic illness (Mutangadura and Webb,
1999). Nampanya-Serpell (2000) shows that households in Zambia that had suffered a paternal
death had experienced a drop in monthly disposable income in excess of 80 percent.
The FAO study showed that the second factor of household agricultural production that
HIV/AIDS would affect was the availability of disposable cash income. During episodes of
illness, household financial resources may be diverted to pay for medical treatment and eventually
to meet funeral costs. Such resources may otherwise be used to purchase agricultural inputs, such
as occasional extra labour or other complementary inputs (e.g. new seeds or plants, fertilizer,
pesticides, etc.). In Rakai district in Uganda, families with orphans, which in most cases were
female headed, had a lower household income compared to families without orphans. In terms of
financial capital services (credit, savings, and insurance), poor families either have to borrow or
sell stores of value. A family affected by HIV/AIDS is less able to avoid default, and hence is less
attractive to group-based liability schemes (Gillespie and Haddad, 2002)
3.3.7 Increased Household expenditure HIV/AIDS will cause affected households to spend more on medical care and funerals. In the
Democratic Republic of the Congo, the cost of hospital care for a child with AIDS amounts to
three times the average monthly household income (Davachi et al, 1988, as quoted in Tanya,
2002). In Burkina Faso, the cost of the lifetime care of an AIDS patient equals twice the country's
per capita income. A study in New Zealand, which required respondents to keep a diary of their
HIV/AIDS-related expenditure over a period of one month, found that private direct costs increase
sharply as the illness progresses (FAO, 1997).
33
The changes in the supply of household labour caused by AIDS morbidity and mortality, which is
accompanied by a drop in household income, will also result in changes in the aggregate level of
expenditure. In affected households, aggregate levels of expenditure will increase initially as
households need to spend more on medical care and funerals. In the Kagera study, the total level
of expenditure was the only statistically significant difference between affected and non-affected
households. The total level of expenditure was 25 percent higher in households suffering an adult
death than in household where no adult death occurred. However, levels of expenditure will also
depend on the ability of the affected household to finance these expenses from transfers of income
received from outside the household, which, as explained elsewhere, is ultimately dependent on
the socio-economic status of the affected household. There is evidence for this in the published
findings from household impact studies. In Kagera, Tanzania, consumption dropped dramatically
in poor households following an adult death (decreased 11 percent among poorest 10 percent),
while the total level of expenditure in less poor households actually increased (Tanya, 2002).
Tanya (2002), reports that differences in per capita equivalent adult expenditure are small and are
not statistically significant, except when controlling for socio-economic status and vulnerability
by for example allowing for differences in education of the household, gender of the deceased and
the duration of illness. In the longer term, as households meet these expenses but are still faced
with a reduction in labour supply, affected households will spend less, an argument supported by
evidence from household impact studies. In rural Thailand, the per capita expenditure in
households affected by an adult death dropped by 43.5 percent with the drop being worse when
the deceased was an adult woman than when it was an adult man (Kongsin et al, 2000; Parker et
al, 2000).
Changes in the level and pattern of household expenditure have wider impacts. The decline in
expenditure on food and other basic needs described above may affect the nutritional status of
household members negatively. Children and the elderly are particularly vulnerable to cutbacks
on expenditure on food. Substantial reductions in the nutritional status of children will in turn
cause changes in infant and child mortality within affected households.
34
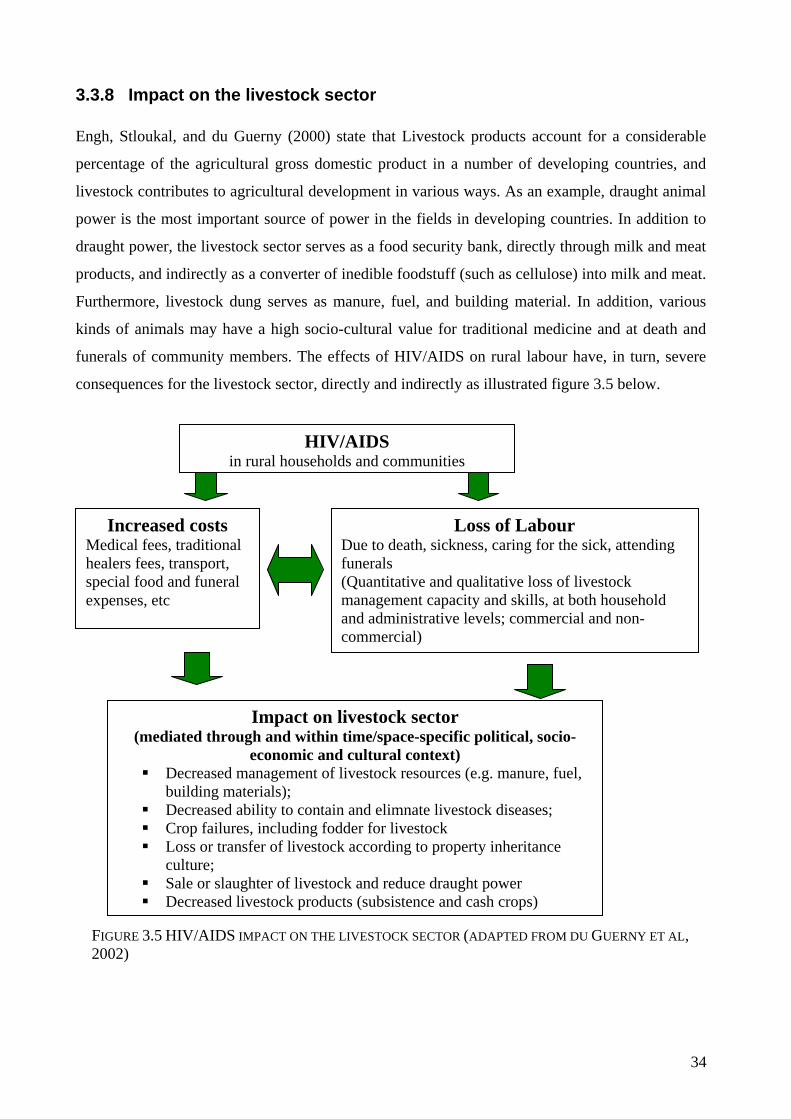
3.3.8 Impact on the livestock sector Engh, Stloukal, and du Guerny (2000) state that Livestock products account for a considerable
percentage of the agricultural gross domestic product in a number of developing countries, and
livestock contributes to agricultural development in various ways. As an example, draught animal
power is the most important source of power in the fields in developing countries. In addition to
draught power, the livestock sector serves as a food security bank, directly through milk and meat
products, and indirectly as a converter of inedible foodstuff (such as cellulose) into milk and meat.
Furthermore, livestock dung serves as manure, fuel, and building material. In addition, various
kinds of animals may have a high socio-cultural value for traditional medicine and at death and
funerals of community members. The effects of HIV/AIDS on rural labour have, in turn, severe
consequences for the livestock sector, directly and indirectly as illustrated figure 3.5 below.
FIGURE 3.5 HIV/AIDS IMPACT ON THE LIVESTOCK SECTOR (ADAPTED FROM DU GUERNY ET AL, 2002)
HIV/AIDS in rural households and communities
Increased costs Medical fees, traditional healers fees, transport, special food and funeral expenses, etc
Loss of Labour Due to death, sickness, caring for the sick, attending funerals (Quantitative and qualitative loss of livestock management capacity and skills, at both household and administrative levels; commercial and non-commercial)
Impact on livestock sector (mediated through and within time/space-specific political, socio-
economic and cultural context) Decreased management of livestock resources (e.g. manure, fuel,
building materials); Decreased ability to contain and elimnate livestock diseases; Crop failures, including fodder for livestock Loss or transfer of livestock according to property inheritance
culture; Sale or slaughter of livestock and reduce draught power Decreased livestock products (subsistence and cash crops)

35
Du Guerny et al. (2000) noted that the various factors are interlinked, the figure above is therefore
highly simplified. Furthermore, the political, socio-economic and cultural context makes time and
space-specific impacts on the linkages illustrated. The impact of HIV/AIDS on the rural livestock
sector is at three levels namely
Reduced capacity for livestock management and production
Du Guerny et al. (2000) state that in addition to the quantitative reduction of the household
workforce, which occurs when adults fall ill or die, the remaining household members may
lack the skills or physical strength to maintain livestock management and production.
Naturally, this has the strongest impact on households which are child-headed or where the
majority of the members are children and older people. Furthermore, mourning and attending
funerals are both time- and energy-consuming. During the mourning period work is reduced or
postponed, including the production of crops and fodder. In a study in Oshana and Caprivi in
Namibia, du Guerny et al. (2000) observed that mourning time for relatives was reported to
range from four to eight days, and for immediate neighbours, it was estimated that they
sympathized and consoled the bereaved family for about half the mourning period. The rest of
the community had to stop work on the funeral day. It was also important to take into account
the time perspective. HIV/AIDS had both short- and long-term effects as daily care was
reduced as well as the capacity to make plans and investments regarding future agricultural
and livestock production.
It was estimated that extension staff in north-central Namibia spent at least 10 percent of their
time attending funerals. Farmers were also spending an equal proportion of their time to attend
the funerals of their relatives. To this must be added the extended mourning time in the village
as well as the time for consoling and sympathizing with bereaved neighbours and attending
funerals of dead community members. Therefore, the lost production time may be more than
25 percent of short critical production periods such as sowing and weeding. Moreover,
delayed weeding demands higher labour inputs. Consequently, in situations where labour is
becoming scarce due to HIV/AIDS morbidity and mortality, the reduction of potential crop
yields due to poor weed management can be severe.
Du Guerny et al. (2000) further stated that apart from HIV/AIDS killing part of the active
workforce involved in livestock and crop tending, it also has serious effects on the veterinary
service, and thus on the country's ability to contain and eliminate livestock diseases. Where

36
local veterinarians and experienced livestock inspectors have been claimed to AIDS, this may
seriously compromise the veterinary service's ability to react to epidemic diseases. In countries
such as Namibia, which are dependent on livestock exports for much of their foreign
exchange, this may have serious consequences. There is reason to believe that these countries
may, in the long run, risk losing markets if they are not effectively able to monitor, control and
eliminate trade-threatening diseases.
Inheritance systems and livestock management
Du Guerny et al. (2000) noted some difference on the impact of AIDS related death on
livestock ownership depending on the cultural practices. In Oshana, immediate effects of an
AID related death on household resources, including livestock, were distinctly different for
households where husbands died and those where wives died. This was probably due to the
matrilineal property inheritance culture, as a result of which there may be a substantial re-
distribution of family property following the death of the male spouse. No such distinctions
were obvious in the Caprivi where the inheritance culture is patrilineal. A common
observation in Oshana households where the husband died of HIV/AIDS was the practice of
taking livestock away from the remaining family (wife and children), although there was
legislation, which should have prevented this. In extreme cases all cattle were taken. Besides
the immediate loss of the mobile bank constituted by livestock for use in times of crop failure,
household food security was also threatened due to loss of draught power which precluded
timely sowing and loss of an organic fertilizer source. Consequently, the levels of grain
produced by the affected households fell despite the maintenance of the cropped area.
Besides cattle, sheep and goats as well as chickens are also taken. A striking case in a
relatively poor household was where all small stock was taken. Where the relatives of the
deceased were more considerate, they only took some of the livestock leaving the wife and
children with some. While this was less disruptive, the effect on crop production was seen
through reduced cropped area and grain production. The trauma associated with the death of
the husband and lack of resources to hire casual labour would also be factors contributing to
the reduction in the intensity of cropping activities.
A prominent feature of the affected households where the wife died was the lack of disruption
of production resources and assets. The assets were less affected than when the husband died
and the household grain production levels were usually maintained. However, in some
situations there was a decline in cropping intensities, crop and weed management.

37
Coverage of HIV/AIDS-related costs by sale and slaughter of livestock
Family assets including livestock might be sold off to meet AIDS related costs. The findings
of Du Guerny et al. (2000) obtained in Caprivi and Oshana in Namibia, indicated that a
common strategy for covering direct costs associated with sickness and death was the sale of
livestock followed by the sale of crops. Borrowing and savings was the least common. Among
the affected households in Oshana, sale of crops and livestock had occurred in 10 cases, while
benefits from insurance and the National Social Security Fund had been used in five cases.
Savings and pension had only helped meet direct costs in two cases each. In Caprivi all four
affected households interviewed cited sale of livestock as the means of meeting direct costs of
sickness and death. One household had sold both crops and livestock. One of the
consequences of high sales of livestock was that production resources were taken out of the
farming system. The important contribution of livestock through draught power, manure, food
security bank, meat and milk products is compromised when large numbers are diverted to
support increasing costs of sickness and death.
In the case of the Oshana region, in addition to the sale of the livestock, the cultural norm is to
slaughter at least one ox during the funeral to feed the mourners. Where the number of cattle
owned allows, several oxen may be slaughtered during the mourning period. In the absence of
oxen, sheep may be slaughtered at the funeral while goats are not culturally acceptable. In
Caprivi, providing meat at funerals was a recent development as tradition considers eating
meat on such occasions as taboo. There is normally less feasting at funerals in the Caprivi
region. Widespread sale and slaughter of livestock to support the sick and to provide food for
the mourners at funerals do not only jeopardize the livestock sub-sector but also the crop
production sub-sector due to reduced availability of draught power and manure. Thus, when
the forced expenses due to HIV/AIDS-associated sicknesses and deaths are met by the sale of
livestock, this is generally setting the stage for serious future household food security and
malnutrition problems. The loss of draught animal power in areas where integration of crop
and livestock is prominent - as in sub-humid eco-zones in southern Africa - strongly hits the
livelihood of rural communities as less draught power results in reduced cultivated areas. The
sacrifice or sale of cattle might be regarded as one of the most destructive processes related to
HIV/AIDS in the livestock sector (du Guerny et al, 2000).

38
3.3.9 Impact on natural resources
Land, forests, water, crops and animals are all affected by the HIV/AIDS epidemic. Land may not
be cultivated and certain crops may not be grown because of the loss or lack of labour, and land
may also be sold to pay the increased medical fees, funeral costs or other household expenses.
Forests may not be managed, with some areas being over harvested because they are close to
home of labour starved households. Water bodies may be over-exploited as households with sick
persons who require frequent washing take more than the usual share (Steely, 2002). The
conservation workforce in Africa has been particularly vulnerable to HIV/AIDS. Both its “formal”
side, i.e. protected area authorities, university/research specialists, non-governmental
organizations staff and its partners in rural natural resource-dependent communities are affected
(Dwasi, 2002).
Gillespie et al (2001) summarize the impact of HIV/AIDS on rural and agricultural dependent
households as follows:
The following chapter gives a review of some of the coping mechanisms and support systems that
rural households have adopted to mitigate AIDS.
3.2.10 Coping mechanisms and support systems
Households and communities for developed various responses to mitigate the impact of
HIV/AIDS. The following section outlines of some of the households and community responses.
3.4 Household and community responses to the impact of HIV/AIDS
Jackson, Mutangadura and Mukurazita (1999) state that households adopt a range of strategies to
cope with effect of HIV/AIDS. Coping strategies not requiring any cash are the most frequently
adopted. These include intra-house labour relocation, taking children out of school, diversifying
household crop production and decreasing the area cultivated. The coping mechanisms employed
by households affected by HIV/AIDS can be categorized into responses that deal with practical
realities such as income loss due to loss of labour and those more personal mechanisms with
regards to care and support by other household members. In an analysis of the literature Donahue
An adult becomes sick; sick adult reduces work; replacement labour is “imported”; all adults work longer hours on the farm; healthcare expenses rise; household reduces food consumption; household switches to less intensive crops and farming systems, small livestock; nutrition status of the sick adult deteriorates; sick adult stops work; family members spend more time caring for sick adult, less time on childcare; divisible assets are sold (e.g., livestock); debts increase; children drop out of school to help with household labour; sick adult dies; household incurs funeral expenses; household may fragment as other adults migrate for work; household reduces cultivation of land (more is left fallow); inappropriate natural resource management may lead to increased spread of pests and disease; effects of the loss of farming knowledge intensify; mining of common property resources increases; access to land and property (particularly for surviving widows) may be affected; solidarity networks are strained or totally collapse; surviving partner becomes sick; and the downward spiral continues and accelerates.

39
(1998) reveals that most loss-management strategies are employed in stages. The first phase
involves the use of reversible mechanisms and disposal of self-insuring assets. Secondly, affected
households dispose productive assets. In the final phase, the household enters into destitution.
The table 3 below highlights the three stages of loss-management to mitigate the impact of AIDS.
TABLE 3.2 THE THREE STAGES OF LOSS MANAGEMENT Stage Loss-management strategies
1. Reversible
mechanisms and
disposal of self-insuring
assets
♦ Seeking wage labour or migrating temporarily to find work
♦ Switching to producing low-maintenance subsistence food crops
(which are usually less nutritious)
♦ Liquidating savings accounts or stores of value such as jewelry or
livestock (excluding draft animals)
♦ Tapping obligations from extended family or community members
♦ Soliciting family or marriage remittances
♦ Borrowing from informal or formal sources of credit
♦ Reducing consumption
♦ Decreasing spending on education, non-urgent health care, or
other human capital investments
2. Disposal of
productive assets
♦ Selling land, equipment, or tools
♦ Borrowing at exorbitant interest rates
♦ Further reducing consumption, education, or health expenditures
♦ Reducing amount of land farmed and types of crops produced
3. Destitution ♦ Depending on charity
♦ Breaking up household
♦ Distress migration Source: Donahue, J. (1998); Tanya, A. (2002)
In addition to the three coping phases noted by Donahue, Jackson et al. (1999) report that the
household coping strategies can be divided into three basic categories. The categories include
strategies aimed at improving food security; Strategies aimed at raising and supplementing income
so as to maintain household expenditure patterns; and Strategies aimed at alleviating the loss of
labour. The table below provides a summary of the household coping mechanism categories
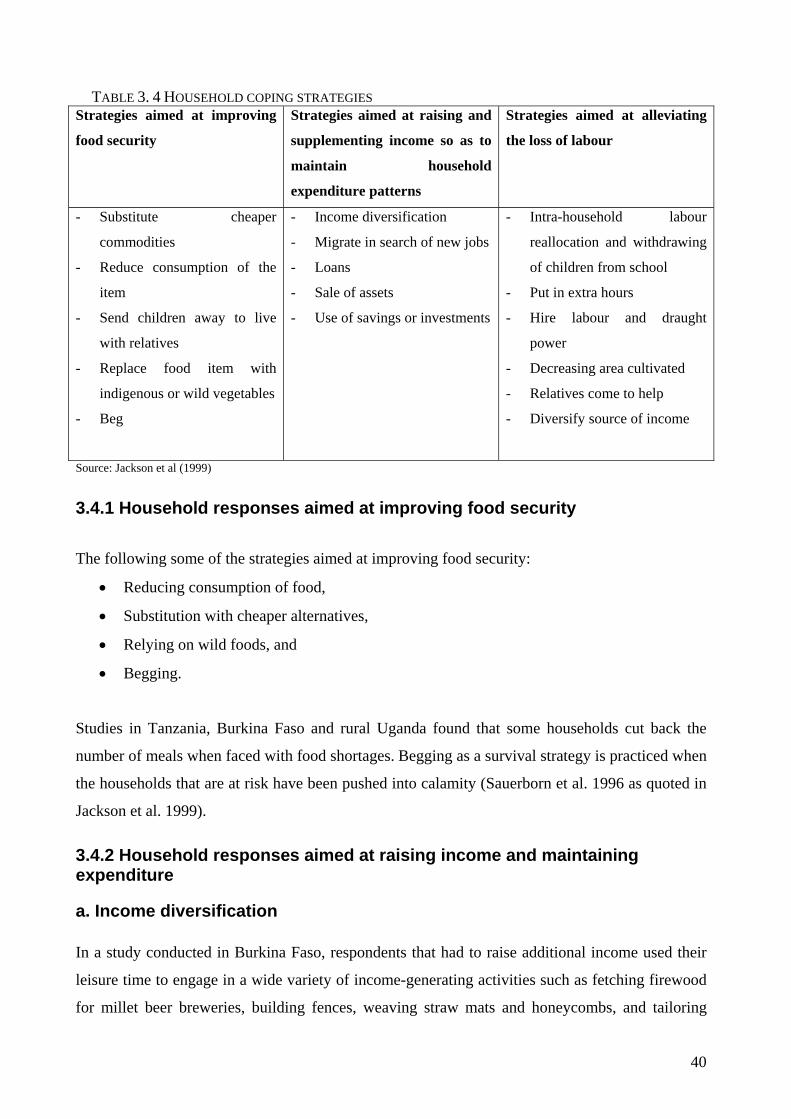
40
TABLE 3. 4 HOUSEHOLD COPING STRATEGIES Strategies aimed at improving
food security
Strategies aimed at raising and
supplementing income so as to
maintain household
expenditure patterns
Strategies aimed at alleviating
the loss of labour
- Substitute cheaper
commodities
- Reduce consumption of the
item
- Send children away to live
with relatives
- Replace food item with
indigenous or wild vegetables
- Beg
- Income diversification
- Migrate in search of new jobs
- Loans
- Sale of assets
- Use of savings or investments
- Intra-household labour
reallocation and withdrawing
of children from school
- Put in extra hours
- Hire labour and draught
power
- Decreasing area cultivated
- Relatives come to help
- Diversify source of income
Source: Jackson et al (1999)
3.4.1 Household responses aimed at improving food security
The following some of the strategies aimed at improving food security:
• Reducing consumption of food,
• Substitution with cheaper alternatives,
• Relying on wild foods, and
• Begging.
Studies in Tanzania, Burkina Faso and rural Uganda found that some households cut back the
number of meals when faced with food shortages. Begging as a survival strategy is practiced when
the households that are at risk have been pushed into calamity (Sauerborn et al. 1996 as quoted in
Jackson et al. 1999).
3.4.2 Household responses aimed at raising income and maintaining expenditure
a. Income diversification In a study conducted in Burkina Faso, respondents that had to raise additional income used their
leisure time to engage in a wide variety of income-generating activities such as fetching firewood
for millet beer breweries, building fences, weaving straw mats and honeycombs, and tailoring

41
(Adams et al.’s 1996, as quoted in Tanya, 2002). Migration to urban areas in search of
employment is common. In Zambia, some members of rural households were reported to have
migrated to urban areas in search of employment so that they can remit some income in their rural
area, while some work in neighbours’ fields as casual labour so as to earn some income (Jackson
et al. 1999). In ability to diversify income sources increases the vulnerability of affected
households to the epidemic. Prevailing poverty drives women into sex work as a course of
income. In Malawi, girls as young as 12 years old were driven to fulfill short-term income needs
(Little, 1996 as quoted in Jackson et al. 1999)
b. Shifting, reducing or cutting back expenditure Increased spending on medical care and funerals crowds out other household expenditure, which
may see a drop in expenditure on food and other basic needs. In Rwanda, 73, 82, 86 and 57
percent of affected households could respectively not meet their clothing, housing, education and
nutritional needs or could only do so with difficulty The death of an adult female in Zimbabwean
households caused the consumption of most food items to decrease, with the drop in consumption
being particularly pronounced in the case of meat, bread, milk and eggs (Mutangandura, 2000). In
Kagera district in Tanzania the expenditure on food by the poorest half of households affected by
an adult death fell by 32 percent in the short term. The impact of HIV/AIDS on expenditure on
medical care and funerals has been documented extensively, while fewer studies have reported on
changes in expenditure on other items. This suggests that many household impact studies have
perhaps collected detailed data on HIV/AIDS-related expenditure only, in the process failing to
collect data on other types of household expenditure, which is crucial in determining how the
epidemic causes consumption patterns to change (Tanya, 2002).
c. Sale of farm produce, assets and use of savings Households affected by AIDS morbidity and mortality, and the resulting drop in household
income and increased pressure on household expenditure, normally cut back on savings and even
dissave in order to cope with these pressures on household finances. Kawaramba (1997) in
Zimbabwe reported that the sale of agricultural produce was a predominant coping strategy to
raise income to meet additional health costs (Jackson et al. 1999). Drinkwater (1993) in Zambia
and Barnett et al. (1995) reported similar findings and indicate the sale of farm produce as a
widely coping strategy. Some households pledge future crops to meet immediate cash needs

42
(Rugalema, 1998, in Jackson et al. 1999). Households that do not have enough income to buy food
or to pay for health care, funeral expenses or education costs sale assets in response to the crises
(Tibaijuka, 1997; and Rugalema, 1998 as quoted in Jackson et al. 1999). A SAfAIDS study in
Zambia indicates the range of assets commonly sold as cattle, bicycles, chickens, furniture,
carpentry tools, radios and wheelbarrows. When AIDS strikes, it stripes away assets of all forms.
To meet large health and funeral expenses, poor families may sell productive equipment or
mortgage land (Gillespie and Haddad, 2002). Twenty-four percent of Zimbabwean households
affected by an adult female death sold assets to cope with the death (Mutangadura, 2000, as
quoted in Tanya, 2002). In Burkina Faso found that most households in a study used any
available cash or savings to pay for medical expenses. The sale of assets was the second most
common method of meeting medical costs. Livestock was the primary asset sold, with villagers
emphasizing the dangers of selling cereal to overall food security (Adams et al. 1996, quoted in
Tanya, 2002)
d. Loans To cushion the impact of AIDS on household income rural families resort to borrowing. The
informal financial sector is an important source of income used during the times of need
(Sauerborn et al. 1996, Aryeetey and Hyuha, 1990 as quoted in Jackson et al. 1999:20). The
informal financial sector includes 1) relatives friends and neighbours, 2) rural cooperatives, 3)
rotating and savings club associations, 4) rural traders, and 5) rural moneylenders. Adams et al.
(1996 as quoted in Tanya, 2002) report that in both of the villages sampled in the Burkina Faso
study, it was customary to take loans. In one village debtors had to pay interest on their loans
whereas the loan was interest free in the other village. Loans were seen as short-term solutions to
tide the cash-strapped households over until their financial status improved. Loans were seen as
less of a risk than selling livestock or other assets. In Rwanda, 18 percent of affected household
had to resort to borrowing in order to finance health care expenses, of which 64 percent borrowed
from friends or neighbors and 16 percent from family (Nandakumar et al, 2000). In Kagera,
Tanzania, households affected by adult deaths made limited use of credit (Lundberg and Over,
2000), which may be because households lack access to credit facilities and/or because
households prefer to adopt alternative coping mechanisms available to the household (Tanya,
2002).

43
e. Role of the extended family The extended family plays a crucial role in mitigating the impact of AIDS on rural households.
Mukoyogo and Williams (1991, as quoted in Jackson et al, 1999) state that the extended family as
a safety net is still by far the most effective community response to the AIDS crisis. Pitayanon et
al. (2000) state that during difficult times households may receive monetary support from relatives
or their extended family members living away from home. In their study in Thailand, 15 percent
of the households affected by an HIV/AIDS – related death received transfers-in from outside.
The average amount received was US$328 per year. The people who provided the money were
mainly adult children of the household head working away from home or the siblings of the head
of the household.
Based on evidence from Uganda (Rakai) and Zambia, the extended family has been described as
the national strength of African countries in terms of coping with the orphan problem. Affected
households that are need of food send their children to live with relatives. Relatives and friends
provide may provide both moral and material support to the sick on the assumption of future
reciprocation (Jackson et al. 1999). Existing family support systems have also been found to
continue to function before and after the death of household members thus underlining their
importance as a coping mechanism (UNAIDS, 1995). Ryder et al. (1994, as quoted in Tanya,
2002) argues that the presence of a concerned extended family substantially minimizes the adverse
impact of HIV/AIDS on the health and socio-economic status of orphans. The threat to extended
family as a safety net is that over time the ability of families and social networks to absorb these
demands will decrease as more adults die of young of HIV/AIDS (Jackson et al. 1999). The
traditional family-care system may further be undermined as demands on time and resources
increase and as stigma and the danger of infection forces the extended family to shy away from
fulfilling their traditional role.
3.4.3 Household responses aimed at alleviating the loss of labour
a. Intra-household reallocation of labour and taking children out of school
Over (1998) reports that to cope with the loss of adults in prime of life to AIDS, households and
extended families often reallocate their resources including the withdrawing of children from
school to help at home, working longer hours and adjusting household membership. Pitayanon et

44
al. (2000) in Thailand observed that many households tried to cope by reallocating the time
household members spent on various activities. Most of the reallocation involved other members
taking on more work than previously to make up the lost income, helping with family business to
substitute for the lost labour, reducing the time spent at work to help the family, needing to find
work, changing to a new job that paid more, needing to find supplementary work, or quitting a job
to help with family chores and take care of the sick person. In addition, children of the deceased as
well as other school-aged members of the households were in some cases withdrawn from school
to start work and to help with family production. Jackson et al. (1999) highlights the importance
of the removal of children from school as a common coping strategy of households. The uptake
of schooling requires both cash and time. Hence, the fact that AIDS morbidity often results in
children being taken out of school to care for the ill is also at stake here. Gillespie and Haddad
(2002) state that HIV/AIDS impairs the children to acquire and use information through formal
education as younger generations are pilled out of school to bolster the family’s ability to provide
care for the ill, to maintain its current livelihood, or to develop new livelihoods. In Zambia,
researchers found that changes in school enrolment resulting from AIDS deaths are more
pronounced in urban than in rural areas. In urban areas, respectively 21 and 17 percent of females
and males dropped out of school following an AIDS death, compared to only 8 and 6 percent of
females and males that dropped out of school in rural areas following an AIDS death (Nampanya-
Serpell, 2000). This is a destructive coping strategy as it undermines the children’s future income
earning potentials. The children in 13 percent of Zimbabwean households where an adult female
had died were unable to attend school following the death, with 75 percent of these children being
absent from school for more than six months due to financial constraints (Mutangadura, 2000).
Jackson et al. (1999) state that girls are more likely to be withdrawn from school than boys, either
to take on the labour role of the mother whilst the latter cares for the sick person, or to be the
primary caregiver.
Another strategy involved changing the sick person’s task from physically demanding ones to
more sedentary ones such as weaving or sewing clothes. The four in-depth profiles of affected
families in rural Uganda presented by Topouzis and Hemrich (1994) present similar evidence of
the impact of HIV/AIDS on the division of labour within the household. One impact study,
though, has not found a significant change in the division of labour within affected households. A
large proportion of households in rural Thailand did not change the allocation of activities
between household members significantly following an adult death (Tanya, 2002)
45
b. Hiring labour Gillespie and Haddad (2002) note that human capital is the first casualty to AIDS. Infected
individuals die prematurely, before which their productivity declines progressively as they
succumb to opportunistic infections. In Zambia, Burkina Faso, Tanzania, Malawi and Zimbabwe,
affected households reported hiring labour and draught power to meet their production
requirements (SAfAIDS, in press; Sauerborn et al. 1996; Rugalema, 1998; Kwaramba, 1997 as
quoted in Jackson et al. 1999). Only households with stable income or source of remittance were
able to hire labour and draught power. Pitayanon et al. (2000) in Thailand, report that 10 percent
of all the households that experienced an HIV/AIDS related death, or 40 percent of the households
that had a family business, hired substitute labour to replace the ill and deceased person.
Furthermore, they state that with rising household expenses and falling income, the additional
expenditure on hiring substitute labour could result in a shortage of production capital of the
household, leading to an adverse impact on family production in future.
c. Changing household crop production and substitution of crops
In a study in Swaziland reported by Muwanga (2002) 42.3 percent of the households that
experienced an AIDS death showed changes in cropping patterns. This involved substitution of
labour intensive crop like cotton with less intensive crops like maize, and moving from cash crops
to purely subsistence crops Jackson et al. (1999) report on research done in East Africa that
reports that households involved in agricultural production may cultivate a mixture of subsistence
and cash crops. Crops that are sensitive to timing services were substituted for those that were
not. Where there was a threat to the agricultural production of a household due to temporary
labour loss, families substituted cash crops for crops that required less labour and expensive inputs
such as fertilizer and pesticides. The four in-depth profiles of affected families in rural Uganda
presented by Topouzis and Hemrich (1994 as quoted in Tanya 2002) support these arguments. Du
Guerny (1999) states that cash crops are often abandoned owing to the inability to maintain
enough labour for both cash and subsistence crops. Switching from labour-intensive crops, to less
labour-intensive ones, is observed. This could have an impact on the nutritional quality of the diet.
d. Decreasing the area cultivated
Jackson et al. (1999) in their research review report that in Burkina Faso, Uganda and the Ivory
Coast the amount of land being cultivated by households that were struck by morbidity and
mortality decreased. Du Guerny (1999) notes that reduction in area of land under cultivation is

46
common among AIDS affected rural households. Community authorities often allocate land to
families on the basis of their size. He reports that the sickness and death of an adult can result in
the inability of the household to cultivate all the land at its disposal. Tending for the sick can take
a considerable amount of time, which is no longer available for agriculture. Thus, more remote
fields tend to be left fallow and the total output of the agricultural unit consequently declines. In a
study in Swaziland, Muwanga (2002) found that there was a significant reduction in area under
cultivation in households that experienced an AIDS related death. The average reduction in land
under cultivation was 51 percent compared to 15.8 percent in households that experienced a non-
AIDS related death. The reduction in land area under cultivation attributed to the study in
Swaziland was 34.2 percent.
e. Lengthening of the working day
Jackson et al. (1999) found that many households put in extra hours of labour per day to make up
for losses due to illness. In a study in Thailand, Pitayanon et al. (1997) report that many
households tried to cope with impact of AIDS by reallocating the time household members spent
on various activities. This involves taking up more work and working longer hours to make for the
lost income.
3.4.4 Other household responses The other notable household responses are migration of members in affected households and
family displacement. Tanya (2002) notes that few household impact studies have explored the
impact of HIV/AIDS on migration, which is a loss-management strategy adopted by affected
households that become destitute and which is not included in Jackson et al.'s (1999) typology of
coping strategies. Over (1995, in WHO, 1997) noted in a study in Kegare region in Tanzania that
at the level of individual households, movements of household/family members into and out of the
household were evident both in the six months prior to death and in the period immediately
following the death of a household member. These movements, which frequently commence in
apparent anticipation of death, most probably have an important role to play in household coping.
In a study in Zambia, Nampanya-Serpell (2000) reports that 61 percent of urban households in
Zambia that were affected by an AIDS death had to move to cheaper housing where access to
public services was worse than where they lived before. Of the 141 households who had moved 31
(almost 22 percent) had lost electricity when they moved while, 55 (approximately 39 percent)
lost access to piped water in their homes. In Uganda, urban children orphaned by AIDS were often
47
uprooted from their places of birth and sent back to villages where their extended family resided.
Other orphans have run away from home in order to escape the stigma and poverty (Topouzis et
al, 1994 in UN Economic Commission for Africa, 2002). The four in-depth profiles of affected
families in rural Uganda presented by Topouzis and Hemrich (1994 quoted in Tanya, 2002) paint
a similar picture.
Some causes of vulnerability to the impact of HIV/AIDS and community responses are discussed
in the following section.
3.5 Vulnerability of rural households to the impact of HIV/AIDS
Topouzis and du Guerny (1999) state that awareness with regard to the magnitude and impact of
HIV/AIDS on project target groups and operations is important for sustainable rural development.
They further state that an analysis of factors contributing to vulnerability to the spread of HIV is
very instrumental. They noted that vulnerability to poverty, food/livelihoods insecurity, gender
inequality, migration, war and civil conflict etc. has a catalytic effect on vulnerability to HIV.
In a study in Zambia, Drinkwater (1993) described the underlying causes of vulnerability in
household (and cluster) livelihoods security with reference to three factors – production, social
and health. The relative diversity of the farming system did have a bearing on household food
security and the relative position and vulnerability of women within the household. In situations
were divorce generally increased the vulnerability of women, the vulnerability was heightened in
the context of maize based farming system. In addition to relative diversity of the farming system,
ill health and mortality had effects on production systems and hence provided the lead to a more
specific and detailed look at the impact of HIV/AIDS. Drinkwater (1993) identified maize based
production system driven by credit and inorganic fertilizer, lack of draught power, and lack of
crop diversification as causes of vulnerability in agricultural production. Lack of crop
diversification as a cause of vulnerability has been observed in Swaziland as well. Muwanga
(2002) identified the limited range of crops in an area with erratic rainfall and poor soils as one of
the factors pointing to the vulnerability of subsistence farming to impact of HIV/AIDS. The
Swaziland subsistence farm systems predominantly have maize as the main crop cultivated.
On the social side, high divorce rate was a major cause of vulnerability to HIV/AIDS. One
obvious consequence of high divorce rate is that both men and women commonly through their
lives have a large number of sexual partners. This practices leads to the spread of HIV/AIDS even

48
among older men. The other factor that exacerbated the break up families and had negative
impact on agricultural production was the inferior status of sons-in-law. In Mpongwe in Zambia,
the sons-in-law go to live in their in-laws village. The son-in-law has an inferior status and is
rarely motivated to work hard even on the field of his own wife. In clusters dominated by women,
it was observed that any sons-in-law married to junior daughters nearly always engaged in income
activities elsewhere – working at private farming company, doing piecework for others, or going
fishing. Inheritance practices and the nature of kin was another social custom that affected
production negatively, and increased the vulnerability of women and children. The general
practice among the matrilineal Lamba in Zambia, is that women do not inherit property from their
husbands, and children receive only a limited amount at the mercy of the husband’s kin. Even in
patrilineal communities husband do commit adultery and divorce does occur. This also increased
exposure to HIV/AIDS. The relationships between men and women in Zambia’s rural, matrilineal
societies are quite clearly difficult and fraught with tension. In patrilineal societies, the tension
arises from the greater authority that women have – women have more means to livelihoods and
food security and therefore a better basis to negotiate working relationships with men
(Drinkwater, 1993).
In a study in Swaziland, Muwanga (2002) identified several factors that point to the vulnerability
of subsistence farm systems to the impact of HIV/AIDS. In addition to lack of crop
diversification, other factors include
• The dependence of production on labour input means that as the younger members who are
disproportionably affected by HIV/AIDS dies, the reduction in labour supply will affect
production
• The dependence on remittances for survival in many households, means that as member of the
household that remit money die of HIV/AIDS the reduction in income will lead to reduced
production on the farm
• The wide use of hired labour on the farms. Dependence on hired labour means that farms or
households are vulnerable to changes in income, which is used to hire the labour. The income
could be from remittances, sale of farm produce or sale of household labour. These sources of
income are affected by increased morbidity and mortality of the productive members of the
household. The makes hired labour an unsuitable household labour saving technology when
faced with epidemic

49
• Female headed household. The death of heads of households – usually men, means loss of
institutional memory that is vital to sustain production on the farm. As women take over as
heads of households, they do so with limited skills and knowledge of the farm systems. It is
therefore difficult for them to cope with reductions in labour supply and interruption of flow of
remittances. In the study in Swaziland, a female head of household lamented that she did not
even know how many herds of cattle and land they owned since it was her husband who
managed the farm. In Malawi, it was found that female-headed households were especially
vulnerable to changes in labour supply and to reductions in the flow of remittances.
• Increase in number of orphans. With the death of parents, knowledge, skills and experience of
agricultural practices, farm management and marketing are lost. The young member of the
household may not have the necessary knowledge, skills and experience in farming to
continue managing the household farm. In households were parents had died, the orphans
lamented that they did not have the necessary knowledge to continue with farm activities.
The findings of the study are presented in the following chapter.

50
CHAPTER FOUR: STUDY FINDINGS
This chapter presents the findings of the study. It provides information the demographics,
livelihoods assets and activities as well as some indicators of the impact of HIV/AIDS on the
livelihoods and food security of households in the study sites. Its also outlines some of the lessons
learnt in analyzing the impact of HIV/AIDS using the SLA.
4.1 Background information (Demographics)
There were 436 respondents in the study as indicated in table 4.1 below. Female respondents
accounted for 58.3% of the total sample. The households included 44.7% female headed and
48.9% male headed. The age of the heads of households ranged from 15 to 89 years, with an
average age of 47 years. Twenty-eight households (6.4%) were child headed. The family size
ranged from 1 to 14 members. Almost 68% of households had 4 – 9 family members. The average
family size was 6.6. Of the total 436 respondents, 22.7% were single, 45.5% married, and 9.9
divorced. Widows and widowers accounted for 15.1% and 6.9% respectively. Of the married 198,
seven were child couples (wife and husband below 18 years). A total of 204 households (47.7%)
reported that they were sad while 162 were happy and 66 were very happy respectively.
TABLE 4.1 DEMOGRAPHIC INFORMATION RESPONDENT HOUSEHOLDS Variable Mishikishi
Kafubu
Fiwale
Total
Gender N % N % N % N %
Male 77 42.5 31 35.6 74 44.0 182 41.7
Female 104 57.5 56 64.4 94 56.0 254 58.3
436 100.0
Age N % N % N % N %
< 18 4 2.2 3 3.4 6 3.6 13 3.0
19 – 24 13 7.2 6 6.9 16 9.5 35 8.0
25 – 29 36 19.9 13 14.9 20 11.9 69 15.8
30 – 39 45 24.9 20 23.0 37 22.0 102 23.4
40 – 49 43 23.8 21 24.1 31 18.5 95 21.8

51
50 – 59 22 12.2 17 19.5 38 22.6 77 17.7
60 – 69 7 3.9 4 4.6 11 6.5 22 5.0
> 70 11 6.1 3 3.4 9 5.4 23 5.3
436 100.0
Marital Status N % N % N % N %
Single 49 27.1 14 16.1 36 21.4 99 22.7
Married 77 42.5 34 39.1 87 51.8 198 45.4
Divorced 19 10.5 13 14.9 11 6.5 43 9.9
Widow 25 13.8 19 21.8 22 13.1 66 15.1
Widower 11 6.1 7 8.0 12 7.1 30 6.9
436 100.0
Household Type N % N % N % N %
Female headed 87 48.1 35 40.2 73 43.5 195 44.7
Male headed 83 45.9 44 50.6 86 51.2 213 48.9
Child headed 11 6.1 8 9.2 9 5.4 28 6.4
436 100.0
Family Size N % N % N % N %
1 – 3 17 9.4 7 8.0 13 7.7 37 8.5
4 – 6 56 30.9 32 36.8 59 35.1 147 33.7
7 – 9 68 37.6 29 33.3 52 31.0 149 34.2
10 – 12 22 12.2 11 12.6 23 13.7 56 12.8
12+ 18 9.9 8 9.2 21 12.5 47 10.8
436 100.0
Well-being N % N % N % N %
Sad 81 44.8 46 52.9 81 48.2 208 47.7
Happy 75 41.4 28 32.2 59 35.1 162 37.2
Very happy 25 13.8 13 14.9 28 16.7 66 15.1
436 100.0

52
Migration Status N % N % N % N %
Non-migrant 58 32.0 29 33.3 65 38.7 152 34.9
Trading migrant 69 38.1 33 37.9 58 34.5 160 36.7
Employment migrant 54 29.8 25 28.7 45 26.8 124 28.4
436 100.0
Level of Education N % N % N % N %
No formal 98 54.1 28 32.2 83 49.4 209 47.9
Primary 55 30.4 41 47.1 67 39.9 163 37.4
Secondary 19 10.5 14 16.1 10 6.0 43 9.9
College 9 5.0 4 4.6 8 4.8 21 4.8
436 100.0
A total of 152 (34.9%) households reported that there was no migration for livelihoods activities.
Of those that migrated, 36.7% were in trading while 28.4% migrated for seasonal formal
employment. Households with college level accounted for 4.8%, secondary level 9.9%, primary
37.4% while non-formal educated households represented 47.9% of the total 436.
4.2 Livelihoods
Agriculture is the main source of livelihoods for the people in Fiwale, Mishikishi and Kafubu. The
main agriculture activities include rainfed crop growing (maize, sunflower, beans, paprika, sweet
potatoes, soya beans, sorghum, pumpkins, and beans); livestock rearing (goats, cattle, pigs, and
poultry); and dambo gardening (rape, cabbage, tomato, onion, impwa – local egg plants, carrots,
and green maize). Mangoes and bananas are the other agriculture products that provide food and
income especially in the rain season. Table 4.2 below shows the characteristics of the study areas
in Masaiti District.

53
TABLE 4.2 CHARACTERISTIC OF SAMPLED AREAS IN MASAITI DISTRICT Areas Fiwale Kafubu Mishikishi
Areas population 7781* 6465* 8841*
No of Households
Ethnic grouping Lamba-Lima mixed with
settler
Lamba-lima mixed with
settlers
Lamba-Lima mixed with settlers
District HIV
prevalence
12.8%** 12.8%** 12.8%**
Rural Health center
prevalence record
- - -
Disease prevalence adult and child malnutrition.
Malaria, TB, Pneumonia,
Diarrhea, Skin rashes, STIs
Malaria, TB, Malnutrition,
Diarrhea, Pneumonia,
High malnutrition, malaria, TB,
STIs, Diarrhea
Village wealth Low - High Low High
Access to social
services
Good
Baptist Mission Hospital,
four primary and one basic
schools, Postal agency,
Hammermill; CHAZ and
local HBC activities,
agriculture extension office.
Good
Rural health center, one
primary and basic school; a
market with local shops.
Health neighborhood HBC
program; Orphanage and
OVC hospices;
Good
Rural health center with
laboratory and surgery. Primary
and basic school. Big market
place, Ndola Diocese micro
finance program.
State of road
infrastructure
Good year round feeder
roads connected to tarred
high way
Year round feeder roads
connected a dilapidated tarred
road
Feed roads with easy access to a
tarred highway.
Migration patterns In and out-migration In and out-migration In and out-migration
Farming systems
and ecological
areas
Rain fed and dambo farming
Food crops: maize, sorghum, sweet
potatoes, beans, cucurbits
Cash crops: maize,
vegetables, soybean, paprika
and groundnuts
Free-range and Intensive
poultry production
Rain-fed and dambo farming
Food crops: maize, sorghum,
beans, cucurbits and
groundnuts
Cash crops: maize, fresh
vegetables, groundnuts
Free-range small livestock
(goat, poultry, pigs)
Rain fed and dambo farming
Food crops: maize, sorghum,
cucurbits and sweet potatoes
Cash crops: vegetables,
groundnuts, maize, sweet
potatoes, paprika,
Free range small livestock (goat,
poultry, guinea fowls
Food security Often insecure to highly
secure
Insecure to secure Insecure to secure

54
Own source: * Rural Health Centre 2002 statistics, ** Ministry of Health/Central Board of Health 2003
Maize, sorghum and sweet potatoes are the major crops grown in Mishikishi, Fiwale and Kafubu.
Maize, beans, cucurbits and sweet potatoes are grown by almost all households largely for
subsistence and surplus is for sale. Other crops such as paprika, soya bean, groundnuts, paprika
and vegetables are grown as cash crops. Most households employ at least three cultivation types:
Upland flat production of maize, sorghum, groundnuts, and soya beans;
Upland mound production of sweet potatoes, beans ad paprika;
Dambo cultivation of maize, beans, cucurbits and vegetables
The agricultural production in the study is labor based and is highly labor intensive. In addition to
agriculture, the households also depend on charcoal, wild fruits, mushroom, and remittances from
relative, pensions and trading. The livelihood assets are shown in the sections below.
4.2.1 Physical Assets
Almost all the households possess hoes, axes, kitchen utensils and chairs. Of the total 436
respondents, 424 (97.2%) own houses while 342 (78.4%) have access to land. Of the 94
households (21.6%) that had no access to land 84 (89%) were female headed and 8 (8.5%) were
child headed. Other assets included bicycles (26.4%), radios (36.2%), cupboards (28.7%) and
wheelbarrows (6.9%). The ownership of Hammer mill, oil presses and carpentry tools accounted
for 1.4% of the total 436 households.
TABLE 4.3 MATERIAL ASSETS IN STUDY AREAS Variable Mishikishi Kafubu Fiwale Total
Material Assets N % N % N % N %
Hoes & axes 181 100 87 100 168 100 436 100.0
House 175 97 87 100 162 96 424 97.2
Wheelbarrow 7 4 15 17 8 5 30 6.9
Radio 68 38 39 45 51 30 158 36.2

55
Bicycle 65 36 23 26 27 16 115 26.4
oil press 2 1 0 0 1 1 3 0.7
pots + other kitchen utensils 181 100 87 100 168 100 436 100.0
Bed 173 96 85 98 165 98 423 97.0
Hammermill 1 1 0 0 0 0 1 0.2
Chairs 181 100 87 100 168 100 436 100.0
Cupboard 67 37 34 39 24 14 125 28.7
Land 108 60 79 91 155 92 342 78.4
Carpentry tools 1 1 1 1 0 0 2 0.5
Oil press 2 1 0 0 1 1 3 0.7
4.2.2 Social Capital
The social assets are list in table 4.4 below. Church and agricultural extension groups are the most
popular social groupings. Of the total 436 respondents, 83.5% reported having household
members who belonged to Church and agricultural extension groups. Other sources of social
capital are health and market committees, Parent and Teachers Associations (PTA), and political
parties.
TABLE 4.4 SOCIAL NETWORKS AND GROUPS Membership in community
groups
Mishikishi
Kafubu
Fiwale Total
N % N % N % N %
Church and church groups 160 88 68 78 136 81 364 83.5
Village Health committee 58 32 23 26 45 27 126 28.9
School PTA 67 37 28 32 44 26 139 31.9
Market committee 25 14 17 20 15 9 57 13.1
Agriculture extension group 136 75 76 87 152 90 364 83.5
Political party 57 31 11 13 19 11 87 20.0

56
4.2.3 Financial Assets
In addition to the physical and social assets, the following were identified financial assets:
• Savings
• Remittances from relatives
• Pension schemes
• Sale of crops
• Sale of Livestock
• Mango and Bananas
• Charcoal
• Other forest products (mushroom and wild fruits)
• Hammer mill
• Oil press
TABLE 4.5 FINANCIAL ASSETS Mishikishi
Kafubu
Fiwale
Total
Financial Capital N % N % N % N %
Savings 8 4 6 7 7 4 21 4.8
Remittances from family
members
29 16 34 39 22 13 85
19.5
Pension scheme 35 19 18 21 14 8 67 15.4
Crops 176 97 81 93 162 96 419 96.1
Livestock 123 68 67 77 78 46 268 61.5
Mango & banana 97 54 72 83 54 32 223 51.1
Charcoal 14 8 8 9 13 8 35 8.0
Other forest products 99 55 56 64 102 61 257 58.9
Hammer mill 1 1 0 0 0 0 1 0.2
Oil press 2 1 0 0 1 1 3 0.7

57
Crops, fruits, and livestock are the main sources of income. Crop sales accounts for 96.1% as a
source of income for the 436 households while livestock accounts for 61.5%. The livestock
includes mainly goats, poultry and pigs. None of the households included in the study had cattle.
The sale of forest products (mushroom and wild fruits) is another important source of income or
financial capital. Pension schemes and family remittances account for 34.9% as income sources.
Of the 436 households, 21 (4.8%) had savings in the bank. The processing of crops milling and oil
pressing were the least in terms of income sources. The following section looks at the access and
control of assets within the studied households.
4.2.4 Intra-household asset control and use of Assets
The control and use of resources varied among the types of household table 4.6. Among male
headed and child headed households, men have more power and control on the access to and use
of physical and financial resources, while women have big voice on the type of social grouping to
belong to. Of the 213 male headed households, 55% and 86% men were the sole decision makers
on the use of physical and financial asset respectively, while 48% women made decision on social
grouping. Among the 195 female headed households, 39% had men as key decision makers on
physical assets, 30% and 44% on social assets and financial assets respectively.
TABLE 4.6 ASSET CONTROL AND USE Control and
Use of Assets
Male headed
Household
Female Headed
Household
Child Headed
Household
Male Female All Male Female All Male Female All
Physical 117 86 10 75 104 16 18 7 3
55% 40% 5% 39% 53% 8% 64% 25% 11%
Social 86 102 25 58 101 36 13 5 10
40% 48% 12% 30% 52% 18% 46% 18% 36%
Financial 184 17 12 85 97 13 21 2 5
86% 8% 6% 44% 50% 6% 75% 7% 18%
The table above indicates that women have more control on the use of physical, social and
financial assets in female headed households. However, even in female headed households the

58
female heads have to consult some male relative in case of asset transfer or sale. Households that
reported consultative family decisions on use of assets accounted for 10% to 12% among the male
headed, 13 to 18 % of female headed, and 11 to 36% of child headed. The livelihood activities are
outlined in the section below.
4.2.5 Livelihoods activities and labour distribution.
In addition to agricultural production activities (land preparation, planting, weeding, harvesting,
tending livestock, and selling crops or livestock), the household members are involved in caring
for and visiting the sick, attending funerals and other community ceremonies. Other activities
include household maintenance (cooking, sweeping, washing clothes, nursing children) and
harvesting and collection of forest products (firewood, charcoal, mushroom and fruits). Other
household members are involved trading and doing piecework.
Except for the age group 18years and below in which the male spend more time in agriculture,
women above 18 years spent more time in agricultural activities than men. Among the 18 to 60
years category, women spend 30% of their time on agriculture activities while men spend 23% of
their time on the same activities. Figure 4.1 illustrates the percentage time spent of agriculture
production by age and gender.
Labour input in Agriculture Production
05
101520253035
Agricultural production
Age and Gender
% T
iime
Male < 18Female <18Male 18 -60Female 18 - 60male > 60Female > 60
FIGURE 4.1 PERCENTAGE OF TIME SPENT ON AGRICULTURE PRODUCTION ACTIVITIES
Compare to females, males in all types households spend less time on household maintenance and
childcare activities. Figure 4.2 shows that while women there is decrease in time spent on child

59
care as women get above 60 years, there is an increase in time spent on caring for the sick, visiting
the sick and attending funeral by both gender (male and female) in over 60 years category. Girls
below 18 ages spend almost equal time on childcare, household maintenance and caring for the
sick. The study found that boys in the same age category spent more time on visiting the sick.
Time spent of household maintenance and health care and funerals
02468
101214161820
Male <
18
Female
<18
Male 18
-60
Female
18 - 6
0
male >
60
Female
> 60
Age and gender
% ti
me
spen
t child carehousehold maintenancecaring for the sickvisiting the sickattending funerals
FIGURE 4.2 PERCENTAGE OF TIME SPENT ON CHILDCARE, HEALTH CARE AND HOUSEHOLD MAINTENANCE
The percentage of time spent by respondent households on harvesting forest products, community
maintenance and piecework is indicated in figure 4. 3 below.

60
Harvesting Forest products, community maintenance and Piecework
05
10152025303540
Fore
stpr
oduc
tha
rves
ting
Com
mun
itym
aint
enan
ce
Gar
deni
ng
Pie
cew
ork
Activity
% T
ime
spen
t Male < 18
Female <18
Male 18 -60
Female 18 - 60
male > 60
Female > 60
FIGURE 4.3 PERCENTAGE OF TIME SPENT ON HARVESTING FOREST PRODUCTS, COMMUNITY MAINTENANCE
The male under the age of 18 and below spend 36% of their time doing piecework while the
female of the same age group spend about 11%. Men in age group 18 – 60 spend 23% of their
time on piecework while womenfolk spend less than 5% of their time on the same activity. Like
agriculture production, women and girls spend more time than men and boys in harvesting forest
products. The only exception is the production of charcoal that is dominated by men. Men in the
18 – 60 year age group spend more time on community maintenance than women in the same age
group.
4.3 Impact of HIV/AIDS on Livelihood assets and activities (shocks and stresses)
This section seeks to show identify the links between HIV/AIDS and the elements of the
livelihood systems in the study sites. While the study deliberately focused on HIV/AIDS, it is not
the only shock or stress that the households are exposed. The relationship HIV/AIDS to other
shocks and stress factors is not captured in this study. The following section shows the prevalence
and perceptions about HIV/AIDS in the study sites

61
4.3.1 HIV/AIDS Prevalence and people’s perceptions
Proxy Indicators were used to separate AIDS affected from non-affected households. The proxy
indicators included presence of chronically ill adult and household head, and death of adult or
household head from terminal illness in the past 12 months. The targeting of households was
based on information from the Health Neighbourhood Committee and the village home care. This
increased the prevalence rate in the study when compared to the national prevalence that indicated
12.8%. Table 4.8 shows the prevalence rate among the study sample.
TABLE 4.8 HIV/AIDS PREVALENCE AMONG THE STUDY SAMPLE
Proxy Indicator Male Headed
Female Headed
Child Headed
Total
N % N % N % N %
Chronically ill adult 56 26 37 19 0 0 93 21
Household head chronically ill 34 16 57 29 0 0 91 21
Adult died from Chronic illness 28 13 16 8 2 7 46 11
Household head died from Chronic illness 18 8 9 5 26 93 53 12
Not affected 77 36 76 39 0 0 153 35
Total 213 100 195 100 28 100 436 100
Of the 213 male-headed households, 136 (64%) were affected by HIV/AIDS. Among the 136
affected households, 56 (26%) of the total had an adult who was chronically ill while 34 (16%)
had a household head who was ill. Male-headed households that had lost a person from a long
illness were 28 (13%) and 18 (8%) for adult and household death respectively. Non-affected male
headed households were 77 representing 36% of 213.
Among the 195 female-headed households, 111 (61%) were affected by HIV/AIDS. These
included 37 (19%) who had an adult suffering from chronic illness, 57 (29%) that had a sick
household head, 16 (8%) that had lost an adult from chronic illness and 9 (5%) that lost a
household from a terminal illness. Non-affected households among the female-headed households
accounted for 39%.
The entire 28 child headed households had been affected by HIV/AIDS mainly through the death
of household heads and adult family members.

62
The affected households attributed the deaths and sicknesses of household members to malaria,
diarrhea, TB, pneumonia, hunger/malnutrition, witchcraft, and HIV/AIDS. This is show in figure
4.4 below. Of the 283 affected households, 25% mentioned malaria, 24% diarrhea, 16% hunger
and malnutrition, 12% TB, and 9% pneumonia. Witchcraft and TB accounted for 8% and 6%
respectively. It is interesting to note that some household members are able to mention
HIV/AIDS is a cause of death or illness of their family members. The impact of death HIV/AIDS
related sickness and death on the household is discussed in the following section.
Perception on causes of death and illness
Malaria25%
TB12%
Pnuemonia, 9%
Witchcraft6%
hunger/malnutrition16%
HIV/AIDS8%
Diarrhea24%
MalariaTBPnuemonia, Witchcrafthunger/malnutritionHIV/AIDSDiarrhea
FIGURE 4.4 PERCEPTION OF CAUSES OF DEATH AND CHRONIC ILLNESSES
4.3.2 Impact of HIV/AIDS on the households and their livelihoods
The impact of HIV/AIDS ranged from perception and attitude change among household members
to changes in asset use and control and in application of family labour. Of the 283 affected
households, 48% reported that the illness and sickness of their relative had changed their own
thinking about HIV/AIDS. One household member said that “..I thought it was out in the streets
but it has now entered our bedrooms. We all need to be careful and do something to stop it from
spreading...”. Another 36% reported changes in use of material and financial assets. There was
increased depletion of savings and sale of assets to meet both the food and medical needs of the

63
sick person. In addition to the patient, more money was required to feed other relatives that came
to visit the sick person.
Figure 4.5 shows the household observations on the effect of the HIV/AIDS sickness and death on
their physical assets. Of the 283 affected households, 66 said the physical asset status was the
same, 20 reported an increase through contributions of relatives and friends while 165 reported a
reduction in physical assets. The other 32 were not sure of the status of the physical assets. The
later was common in situation were the sick person still remained in control of assets and hence
other household members were aware of what assets had been transferred sold. Among the child
headed households 21(75%) had reduction in physical assets, 7% had not change while 18% were
not sure.
33
13
78
12
31
7
66
1520
21
50
1020304050607080
Number
N N N
MaleHeaded
FemaleHeaded
ChildHeaded
change
Changes in Physical Assets
sameincreasedreducednot sure
FIGURE 4.5 EFFECT OF HIV/AIDS ON PHYSICAL ASSETS
In addition to changes in physical assets, all the 283 affected households reported a reduction in
both financial and social capital. Increased costs of nursing and feeding the sick and funeral
expenses eroded the financial base. The reduction in social capital was attributed to lack of time as
the patient needed more attention and to stigma that made affected household members reduce or
cut off their interaction with other community group members. Consequently, there was reduced
capacity to engage in household and community livelihood activities. Non-affected households
reported the changes in relationships and disintegration of some community groups has a major

64
effect of HIV/AIDS. In parts of Mishikishi and Kafubu, the communal lending groups have
collapsed as a result of members being sick or caring for the sick.
The death or sickness of the head of household also led to reduced inflow of food and income. The
adult was supplementing household food and income source was no longer able to do so. As result
there were reduction in food stock and food consumption. Of the 283 affected households, 67%
reported a reduction in food available at home and eventually in the amount of food consumed in
the household.
The other effect of HIV/AIDS on households is the increase in the number of orphans and the
emerging child couple scenario. Among the 408 male and female headed households, 52%
reported having taken an orphan in the past 18 months. This has contributed to the increase child
care role among aged (above years old). The following section outlines some of the coping and
resilience building strategies.
4.2.3 Coping Strategies and Building Resilience
The households and communities in study sites have developed diverse coping mechanism. The
coping strategies being applied by affected households include
Reallocation of household labour on livelihood activities. This includes increased use of
both child and adult labor for selected activities.
Reducing land under cultivation and focusing on easy to grow crops. HIV/AIDS has led to
changes both in land under cultivation and the types of crops grown. Affected households
are slowly shifting from high input cash crops to low input food crops. In some cases there
was total abandoning of on-farm production in preference to selling labour (doing piece at
other farms).
Working longer hours than before to cover for lost labour and time
Adopting new cultivation techniques – minimum and conservation tillage
Shifting to traditional healers instead of medical institutions
Sale of household assets to raise money for medical and household needs
Engaging in small scale trading with increase use of children in vending

65
Increased utilization of forest resources
Early and forced marriages
Many of the coping strategies have a negative effect on the long-term sustainability of livelihoods.
While they meet immediate needs of the households, they undermine the future income earning
potential of households and individual members. Mitigation strategies should overcome the
negative effects of HIV/AIDS at the household and community levels.
The next section provides the lessons learnt in applying the Sustainable Livelihoods Approach to
assess the impact of HIV/AIDS on rural households
4.2.4 Lessons Learnt in applying the SLA to analyze the impact of HIV/AIDS
Working with communities and attempting to elicit livelihoods strategies is complex and time
consuming. It requires a multi-disciplinary and talented team. The livelihoods approach generates
a large amount of information making compiling difficult. The pre-assessment survey and
collection of secondary data is critical to the success of the final study. Involvement of the
community from the start in terms clarification of objectives, approaches and community role is
equally important.
Despite being complex and time consuming, the SLA can be used as an icebreaker on sensitive
issues like HIV/AIDS. It was noted during the study that the analysis opened a way and provided
an opportunity for community members to talk openly about HIV/AIDS and relate it to their own
livelihoods. It also builds the momentum that is needed for communities to move forward with
development interventions.
The SLA provides the opportunity to learn and build on the strengths of what is already known,
tried and tested. The ‘livelihoods lens’ enables us to look ‘cross-sectorally’ being able to
recognize with the HIV/AIDS epidemic that it is inappropriate to look at rural households or areas
in isolation. We can and must learn with people who have ‘mainstreamed HIV/AIDS’ in their own
lives out of necessity, and have developed successful ways to mitigate the impact of the AIDS
epidemic. The SLA allows for a good systems approach in targeting action to prevent and mitigate
the impact in rural communities. Although national responses to the AIDS pandemic in most
developing countries are multi-sectoral, there is a need to further integrate the holistic perspective

66
by increasing the understanding of the complete cause-effect relationships. This will enable local
communities to develop appropriate activities to remove the root causes identified.
The SLA could be useful in facilitating the complete understanding of cause-effect relationships.
This study has led into the formulation of an HIV/AIDS and food security pilot project. The
project targets 75 AIDS affected female headed household. The objective is to extend the
production period from six months to year round through small-scale irrigation technology. In
addition to the women, the project is testing the involvement of the rural youth in agriculture and
HIV/AIDS activities.
The combination of quantitative and qualitative assessments provides a good mix to triangulate
and reduce biases and errors in the study.

67
CHAPTER 5: RECOMMENDATIONS
Many of the findings of this study are similar to what other people have found before. However, it
the participatory process and approach to the analysis that provides another window of doing
things. The multi-sectoral and participatory nature of the study encouraged and educed
enthusiastic community involvement.
Addressing the impact of HIV/AIDS on rural household required a multi-sectoral approach that
allows linkages across sectors and the interaction of shocks and stresses. The following should be
considered to prevent asset loss and build resilience in rural households
Increasing land ownership and improving management:
Increasing access to land control over land use is one of the building blocks of resilience.
Ownership induces stewardship. This means rural households will be motivated to improve
and maintain soil productivity.
Extending the crop growing season: promotion of low-labour water harvesting techniques
is necessary to increase food and income security especially among female headed
households
Crop diversification to reduce the risk of crop failure and diversify the income source.
Linking agricultural production to forest resources: Allow communities to appreciate the
interdependence of agricultural production on the ecological system. This will reduce over
exploitation of environment for either agriculture or forest products.
Strengthen social networks: institutional support to strength community groups and create
networks for information sharing
Development of human assets through farmer training and consolidation of local
knowledge transfer systems
Promote behavior change: Negative cultural practices and community behavior that
promote the spread of HIV/AIDS and reinforce stigma should be discarded. Gender equity
is key factor in facilitating behavior change in rural communities. Encourage openness
about HIV/AIDS in communities
Promoting community based operations research that allow communities to learn by doing
and as result maintain the skills to address the HIV/AIDS problems at community level.
Integrating HIV/AIDS and agriculture with other sectors, and providing linkages to wide
national and regional interventions.

68
REFERENCES
Barnett. T, Whiteside. A, and Smart. R (2000) Eds. AIDS Brief for sectoral planners and
managers: Subsistence Agriculture Sector.
Carney, D. and Ashley, C. (2000). Sustainable Livelihoods: lessons from early experience. DFID,
London.
CRS (2002). Regional Strategy for Southern Africa. Harare, Zimbabwe
De Satge. R, (2002). Learning about livelihoods: insights from Southern Africa. Periperi
publications and Oxfam publishing.
Donahue, J. (1998). “Community-Based Economic Support for Households affected by AIDS,”
Health Technical Services (HTS) Project, for USAID, June 1998.
Donahue, J. and Williamson, J. (1999). “Community Mobilization to Mitigate the Impacts of
HIV/AIDS,” Displaced Children and Orphan Fund, September 1999.
Donahue, J. (2002). Children, HIV/AIDS and Poverty in Southern Africa, SARPN April 9 and 10th
2002.
Drinkwater, M. (1993). The Effects of HIV/AIDS on Agricultural Production Systems in Zambia:
An analysis and field reports of case studies carried out in Mpongwe, Ndola Rural District
and Teta, Serenje District. A study undertaken by the Adaptive Research Planning Team,
Ministry of Agriculture, the FAO of the United Nations
Du Guerny, J. (1999). Aids and agriculture: Can agricultural policy make a difference? in Food,
Nutrition and Agriculture, No. 25 , FAO, Rome
Du Guerny, J, Engh, I. and Stloukal, L. (2000). HIV/AIDS in Namibia. The impact on the livestock
sector, FAO, Rome.
Du Guerny, J. (2002). Agriculture and HIV/AIDS UNDP South East Asia HIV and Development
Project.
Dwasi, J. (2002). Working together to help conserve Africa’s biodiversity. Contributed Paper
Sessions (http//www.ecosystemhealth.com/hehp/papersessions/session3-5.htm)
FAO (1995). The effects of HIV/AIDS on Farming Systems in Eastern Africa. FAO Farm
Management and Production Economics Service, Rome.
FAO, (1997). The rural people of Africa confronted with AIDS: A challenge to development.
Rome, December 1997.
FAO (2002). Rural Livelihoods. FAO message to the Barcelona AIDS conference.
Gillespie, S, Haddad, L. and Jackson, R. (2001). HIV/AIDS, Food and Nutrition Security: Impacts
and Actions. IFRPI and WFP.

69
Gari, J. (2002). Agrobiodiversity, Food Security and AIDS mitigation in sub-Saharan Africa.
Strategic issues for agricultural policy and programme responses. SD:People:Population.
FAO, Rome.
Gillespie, S. and Haddad, L. (2002). IFPRI 2001-2002 Annual Report Essay—Food Security as
a Response to AIDS
ITDG (2002). ITDG Southern Africa 2002 Annual report.
(http://www.itdg.org/html/itdg_southernafrica/annual_report/annual_report_2002.htm)
Kapwepwe, M. and Siamwiza, R. (2001). CORDAID HIV/AIDS Programmes Assessment:
Zambia.
Martin, A. (2002). Southern Africa Regional Poverty Network (SARPN), HIV/AIDS and its
Impacts on Land Tenure and Livelihoods in Lesotho: Comments on Lesotho Country
Study. (http://www.eldis.org/static/DOC10745.htm)
Ministry of Health/Central Board of Health, (1999). HIV/AIDS in Zambia. Background
Projections, Impacts, Interventions.
Mutangadura, G, Mukuratiza, D. and Jackson, H. (1999). A review of household and community
responses to the HIV/AIDS epidemic in the rural areas of sub-Saharan Africa. UNAIDS
best practice collection. Geneva, Switzerland. (http://www.unaids.org)
Muwanga, F.T. (2002). Impacts of HIV/AIDS on Agriculture and the Private Sector in Swaziland:
The Demographic, Social and Economic Impact on Subsistence Agriculture, Commercial
Agriculture, Ministry of Agriculture and Cooperatives and Business.
Nampanya-Serpell. N, (2000). Social and Economic Risk Factors for HIV/AIDS Affected Families
in Zambia. Paper presented at the AIDS and Economic symposium in Durban 7 – 8 July
2000. (http://www.iaen.org/library/files.cgi/196_67nampanya.pdf)
Ngwira, N, Bota, S. and Loevinsohn, M. (2001). HIV/AIDS, Agriculture and Food Security in
Malawi. RENEWAL working paper number one. Lilongwe and The Hague.
Over, M. (1998). Coping with the Impact of AIDS. Article based on a World Bank Policy
Research Report, Confronting AIDS: Public Priorities in a Global Epidemic. New York:
Oxford University Press for World Bank 1997
Over, M. (1995). The Economic Impact of Fatal Adult Illness from AIDS and Other Causes in
sub-Saharan Africa. A study conducted jointly by the World Bank and the University of
Dar es Salaam, Tanzania.
Pitayanon S, Kongsin , and Janjareon WS (1997). The economic impact of HIV/AIDS mortality
on households in Thailand, in Bloom, David and Peter Godwin, eds, “The economics of
70
HIV and AIDS: The case of South East Asia.” UNDP 1997.
(http://www.iaen.org/impact/thai/thai.pdf)
Staneck, K.A (2002). Draft report on the Barcelona AIDS conference.
Steely, J. and Pringle, C. (2001). Sustainable Livelihoods Approaches and HIV/AIDS. A
preliminary resource paper
Steely, J. (2002). Co-editor, Khanya-Managing Rural Change. Sustaining Livelihoods in Southern
Africa Issue: 6 June 2002. HIV/AIDS and Sustainable Livelihoods.
Tanya, A. (2002). The Social and Economic Impact of HIV/AIDS. A review of literature. Centre
for Health Systems Research and Development, University of the Free State,
Bloemfontein.
Todaro, M. (1997). Economic Development. Addison Wesley Longman Limited, UK (Chapter 2
– Diverse structures and Common Characteristics of Developing Nations)
Topouzis, D. (1998). The implications of HIV/AIDS for rural development policy and
programming: Focus on sub-Saharan Africa. FAO, Rome.
(http://www.fao.org/sd/WPdirect/WPre0074htm)
UN (2001). Fact sheet: Global crisis-Global action: HIV/AIDS, Food Security and Rural
Development. UN special session on HIV/AIDS 25-27 June, 2001. New York.
UN (2001). Fact sheet: Global crisis-Global Action: HIV/AIDS and Development. UN special
session on HIV/AIDS 25 – 27 June 2001. New York.
UN (2001). Fact sheet: Global crisis-Global action: An overview of the HIV/AIDS Epidemic. UN
special session on HIV/AIDS 25 – 27 June 2001. New York.
UNAIDS/World Bank (2001). A Toolkit for Mainstreaming HIV/AIDS in Development
Instruments
UNDP (2001). Zambia Human Development Report 1999/2000. Mission Press, Ndola, Zambia
USAID, (2002). Coming Together, Caring Together: A report on the Communities Responding to
HIV/AIDS Epidemic (CORE) Initiative, January 2001 – June2002. Washington, DC
World Bank, (2001). Indigenous Knowledge and HIV/AIDS: Ghana and Zambia. IK Notes No.
30 March 2001. (http://worldbank.org/afr/ik/default.htm)

71
QUESTIONNAIRE OR CHECKLIST FOR THE HIV/AIDS AND LIVELIHOODS STUDY Name of Data Collector(s)________________________ Date____/___/______ Location/Site: ________________________
SECTION A. HOUSEHOLD DETAILS
1. Respondent/Interviewee:_Male/Female____________________ Age:_____ Marital Status. ______________ List the names of family members present during the interview 2. Relationship of Interviewee to the Household: Mother Father Son Daughter Uncle Aunt Grandmother Grandfather Other (specify). _______________________ 3. Family Type: (Mark with X) CHILD HEADED ___, FEMALE HEADED (WIDOR)___, FEMALE HEADED(UNMARRIED) ____, MALE HEADED (WIDOWER) ____, MALE HEADED (UNMARRIED) MALE HEADED (MARRIED) ____ 4. Family Size: ____ No. of Adult Male ____ No. of Adult female _____ No. of female children ____ No. of Male children ____ 5. Household Well-being Category (mark X) Sad _______ Happy___________ Very Happy________ 6. Household Migration: How long does each youth and adult member reside permanently in the household? Where do they reside when they are away from the household? Why do they spend the other time residing away from the household? 7. Education Levels What is the education level of the all members of the household?

72
NB. The information on the names will be used for follow up but will not included in the report on ethical grounds
SECTION B. LIVELIHOOD ASSESSMENT
1. Assets A. What material assets does the household possess or own? List all the assets
Who in the household owns each of these assets? Who in the household has the access to the assets? Who decides how the assets should be used? How is the decision made? What is the quality of each of these material assets?
B. What social groupings does the household have access to? List all the assets Who in the household belongs to each of the social groups? Who decides on family member to join thegroups? How is the decision made? What is the quality of each of these social assets? Do any members of the household have specific social status? List and indicate the status.
C. What financial capital does the household possess or access to? List all.
Who in the household has access to each of these financial assets? Who in the household has the control over the use of these assets? Who decides how to use these assets? How is the decision made? What is the quality of each of these assets?
2. Livelihood activities in the households (indicate who is involved in the activity) a. Productive Activities Activity Male Adult Male Child Female
Adult Female Child
Include other activities in the notebook.

73
b. Reproductive Activities Activity Male adult Male child Female
Adult Female Child
Include other activities in the notebook c. Community development or maintenance Activities. Record as in a and b above Community Activities Activity Male adult Male child Female
Adult Female Child
3. CAPABILITIES a. What skills does the household possess? Indicate who in the household has the skill Skills Male adult Male children Female adult Female
child
b. What knowledge does the household possess? Indicate who has the knowledge within the household. c. Who in the household is able to work productively? Indicate the type work each member can do.

74
d. What is the quality of each of the capabilities that household members possess?
4. Resource Flows What resources (food and goods) does the household have access to? What are the sources of these resources? How do these resources flow in and out of the household over time (year)? How do individual household members gain control or access to the resources? What is the composition of household meals? How many meals are consumed per day by the household? one two three > three Total Fiwale Kafubu Kafulafuta
5. Shocks and Stresses (Impact of HIV/AIDS) a. How many members of the household died in the recent past or are suffering from a terminal illness? What illness were or are they suffering from? c. What does the household attribute the illness or death to?

75
d. What changes have been seen in the household since the illness and or death of the family member or members? e. What has been or is the impact of the terminal illness and or death of a family member or members on Household material/physical assets Same Increased Reduced Not sure Total Fiwale Kafubu Kafulafuta Household social assets Same Increased Reduced Not sure Total Fiwale Kafubu Kafulafuta Household financial assets Same Increased Reduced Not sure Total Fiwale Kafubu Kafulafuta Household capabilities Same Increased Reduced Not sure Total Fiwale Kafubu Kafulafuta

76
f. Has the death and or terminal illness changed the food resource flow in and out of the Household? If yes how has the food resource flow changed? Same Increased Reduced Not sure Total Fiwale Kafubu Kafulafuta g. What is the current income expenditure? h. What was the expenditure pattern before the terminal illness and or death of the family member? Expenditure patterns Same Increased Reduced Not sure Total Fiwale Kafubu Kafulafuta I. What factors have contributed to the situation in which the household is? list micro and macro environmental factors. 6. Coping and building Resilience
a. How is the household coping with the current situation? List the coping strategies and the role of each household member.

77
b. How would the household like to prepare itself to a handle similar situation in future? List the suggested interventions and the role of each household member. c. How would the household like the community to prepare itself to assist the households affected with terminal illness and death of family members? d. Which other stresses and shocks apart from terminal illness and or death has the household experienced or is experiencing now? e. How can the factors micro and macro that contribute to the current household situation be adequately addressed? Indicate the role of individuals, households, community, government, International actors.