a new protocol for the treatment.. epidermolysis
TRANSCRIPT

91
© Socidtd d'/~dition de l'Association d'Enseignement Mddical des Hdpitaux de Paris, 1997
A new protocol for the treatment of hand deformities in recessive dystrophic epidermolysis bullosa (13 cases)
G.L. CAMPIGLIO, G. PAJARDI, G. RAFANELLI
SUMMARY: The recessive form of dystrophic epidermolysis bullosa creates severe hand deformities with disabling functional limitations in the main daily acti- vities. Typically, the thumb is contracted in adduction, the first web space is oblite- rated, the palm and digits are contracted in flexion and interdigital spaces are lost (pseudo-syndactyly). In this paper, we present our experience with a protocol based on the association of various internationally developed techniques : brachial plexus anesthesia with ketamine sedation, dynamic splinting and coverage of the wounds with allogenie keratinocytes sheets. The overall results obtained in the first 13 patients showed a good tolerance of the procedure, no anesthesiologic compli- cation and marked improvement of the hand deformities. The long-term follow-up revealed a recurrence before 2 years in 2 hands, between 2 and 4 years in 7 hands and after 4 years in 6 hands. The conclusion is that an aggressive surgical attitude, along with an adequate intra and post-operative rehabilitation, ensures a good restoration of hand function and a satisfying delay of inevitable recurrence.
Ann Chir Main (Ann Hand Surg), 1997, 16, n ° 2, 91 -101 .
K E Y - W O R D S : E p i d e r m o l y s i s b u l l o s a . - H a n d su rge ry . - Sp l in t .
INTRODUCTION
The term Epidermolisys Bullosa (EB) refers to a group of heterogeneous non-inflammatory diseases whose principal common feature is an unusual susceptibility of the tegument to frictional stress with blistering following the slightest mechanical trauma, the so-called Nikolsky sign [1, 2, 3].
CLASSIFICATION
Since 1870, when EB was firstly described and separa ted f rom pemph igus by von Hebra [4], various classification schemes have been proposed but the most reasonable clinical distinction was reported by Pearson only in 1971 [5]. According to this classification, two broad categories of EB are
Manuscrit rec~u b la R6daction le 3 fdvrier 1997. Accept6 le 21 mars 1997. Viale Papiniano 44, 20123 MILAN (Italy).

92 RECESSIVE DYSTROPHIC EPIDERMOL I/SIS BULLOSA
A N N A L E S DE C H I R U R G 1 E
DE L A M A I N 1 9 9 7 , E~ Du MEm.rr suPerlEur
16, n ° 2 ANNALS OF HAND AND UPPER LIMB
S U R G E R Y
TABLE I. - Classification of epidermolysis bullosa (Pearson, 1971).
TABLEAU I. - Classification de I '~pidermolyse bulleuse. TABLA I. - Classificaci6n de la epidermo lisis arnpollar.
A) Non scarring forms Epidermolysis simplex Cockayne's disease Junctional bullous epidermatosis
B) Scarring forms Dominant dystrophic epidermolysis bullosa Recessive dystrophic epidermolysis bullosa Acquired dystrophic epidermolysis bullosa
recognized on the basis of clinico-pathological dif- ferences (table I). Those forms resulting from bulls formation above the epidermal basement membrane are termed non-scarring in that the lesions heal without significant fibrosis unless secondary infec- tion occurs. On the contrary, the scarring or dystro- phic varieties are characterized by a shear level just beneath the basement membrane , intradermal connective tissue degenerat ion and absence of anchoring fibrils in the papillary dermis which results clinically in severe and disabling deformi- ties. Both scarring and non-scarring types include separate forms that can be genetically transmitted as either autosomal dominant or recessive traits [3] ; indeed, indirect evidence suggests that some of these different diseases may be expressions of varying degrees of intensity of allelic mutation at a particular gene locus [6, 7].
Although any dystrophic type of EB can produce hand deformities, the recessive form is the most severe. All patients treated with the following surgi- cal and physiotherapeutic protocol suffered from this form of EB.
PATHOGENESIS
The exact pathogenesis of recessive dystrophic epidermolysis bullosa (RDEB) has not been fully elucidated: Eisen, in 1969, proposed that dystrophic types may result from dermal destruction by an abnormal amount of a collagenase [8]. This hypo- thesis was subsequently confirmed by Bauer in 1977 who demonstrated increased collagenase levels in skin samples taken from patients with RDEB [9]. Whether elevated collagenase levels are the result of increased synthesis or decreased degra- dation is still unknown. Other researchers reported that dystrophic epidermolysis bullosa may be caused by the production of an abnormally structu- red protein which is incorporated in the epidermal- dermal junction [ 10].
CLINICAL PICTURE
The recessive dystrophic epidermolysis bullosa is a disease with an es t imated incidence of 1 in 300,000 live births [11] which commonly involves both the cutaneous and mucosal surfaces. The blisters heal slowly and produce scarring and milia formation. Repeated injury and healing may also play an important role in the development of squa- mous cell carcinoma which has been observed in some patients, expecially in the fourth-fifth decade [12, 131.
Lesions of the mouth, esophagus and anus are particularly disabling as they make eating and defe- cation painful and difficult, resulting in an inade- quate dietary intake, so that patients, even with added supplements, are usually quite thin and small [14].
Nails are dystrophic and are lost in infancy. Repeated friction and subsequent secondary healing produce a characteristic triad of hand deformities: adduction contracture of the thumb with oblitera- tion of the first web space, volar contractures of the palm and digits and pseudosyndactyly (fig. 1). Fine manipulation of the objects is markedly reduced and independent digital function is lost, resulting in significant impairment of important everyday acti- vities.
MATERIALS AND METHODS
Patients
A group of 13 patients (9 males and 4 females) affected by RDEB were treated between 1990 and 1995 at our Institute using the protocol described below. The average age was 6 years (range 3-9 years) and both hands were treated simulta- neously in 70 % of cases. The follow-up ranged from 1 to 5 years.
Preparation
Special precaution in the daily care of these patient is required and an educational program is required both for the parents and nurses. No rubbing or taping is tolerated. Prevention of frictional trauma by frequent lubrification of the skin is of paramount importance in these patients. Beds with flotation mattresses are also routinely used to prevent skin-shearing stresses. In case of mucosal involvement of the digestive tract a soft or semili- quid diet is administered with a protein supplement.
Established lesions can be treated using non- adherent dressings while topical antibiotics are limited to infected wounds.

ANNALES DE CHIRURG1E
DE L A M A I N ET DU MEMBRE SUPERIEUR
ANNALS OF HAND ANI) UPPER LIMB
SURGERY
1997, 16, n°2
RECESSIVE DYSTROPHIC EPIDERMOL YSIS B ULLOSA 93
Fig. 1. - The typical hand deformities in a young patient affected by recessive dystrophic epidermolysis bullosa.
Fig. 1. - D~formation typique des mains chez un jeune patient atteint d'6pidermolyse bulleuse.
Fig. 1. - Deformaci6n tipica de las manos en una paciente j6ven quien presenta una epidermolisis ampollar.
Systemic corticosteroids and vitamin E therapy are not effective, as also reported by others, and their use is rarely justified [5, 15].
Anesthesia
The procedures are performed under brachial plexus anesthesia with ketamine sedation. Atropine (0.5 rag) is administered 45 minutes before surgery. In the operating room, the patient is sedated with ketamine at the dose of 5 mg/kg using a percuta- neous IV catheter fixed without tape or adherent strips [16]. After careful disinfection of the axilla, the block is performed using lidocaine 0.5-1% with ep inephr ine 1:200,000 (0.33 ml /kg) [16]. Throughout the procedure, both blood pressure and cardiologic activity are monitored and supplemen- tary doses of ketamine are adminis tered when necessary.
Surgical technique
In contrast with other recent reports [17] all our procedures were performed under a pneumatic tourniquet. This is not applied directly to the skin, which is protected with a cotton pad in order to
eliminate any additional source of trauma. Skin is dis infected very gently using povidone iodine solution. Conventional frictional scrubbing is absolutely avoided because of the fragility of the skin.
The procedure begins with epidermal degloving of the hand which is performed by incising the epidermis at the wrist and peeling it off distally (fig. 2, 3). The adducted thumb is then released and the first web space is recreated. As also evidenced by Cuono in 1978, the thumb adduction contracture involves the adductor pollicis brevis and the first dorsal interosseous muscle, its correction therefore requires a long incision (from the base of the web at the level of the carpometacarpal joint dorsally, across the web and up to the palm volarly) and deep release through the muscular aponeurosis [1]. Release of the palm is obtained by continuing this incision over the volar surface. A full thickness skin graft, usually taken form the groin, is used to cover the defects created by release of the contractures. Proximal and distal interphalangeal joint contrac- tures are released surgically using a transverse inci- sion and avoiding exposure of the tendons. Finally, the hand is splinted, as explained below, and all the de-epithelialized wounds are dressed using alloge- nic in vitro cultured keratinocytes.

94 RECESSIVE DYSTROPHIC EPIDERMOL YSIS B ULLOSA
ANNALES DE CFIIRURGIE
DE LA MAIN 1 9 ~1 / , ET DU M EP, IBRE SL'PERIEUR
--16, n ° 2 ANNALS OF HAND AND UPPER LIMB SURGERY
Fig. 2. - T h e , epidermal cocoon ,, is gently removed starting at the wrist.
Fig. 2. - Ab la t ion du <, cocon ,, ep ide rm ique & part i r du po ignet .
Fig. 2. - Ext i rpac i6n de la ,, coca , , ep ide rm ica desde la muf ieca.
Fig. 3. - All of the epidermis is peeled off exposing the deep dermal layer.
Fig. 3. - L'6piderme superficiel est enleve, exposant la couche dermique profonde.
Fig. 3. - Ablaci6n de la capa epid6rmica superficial, Io que permite exporter la capa d6rmica profunda.
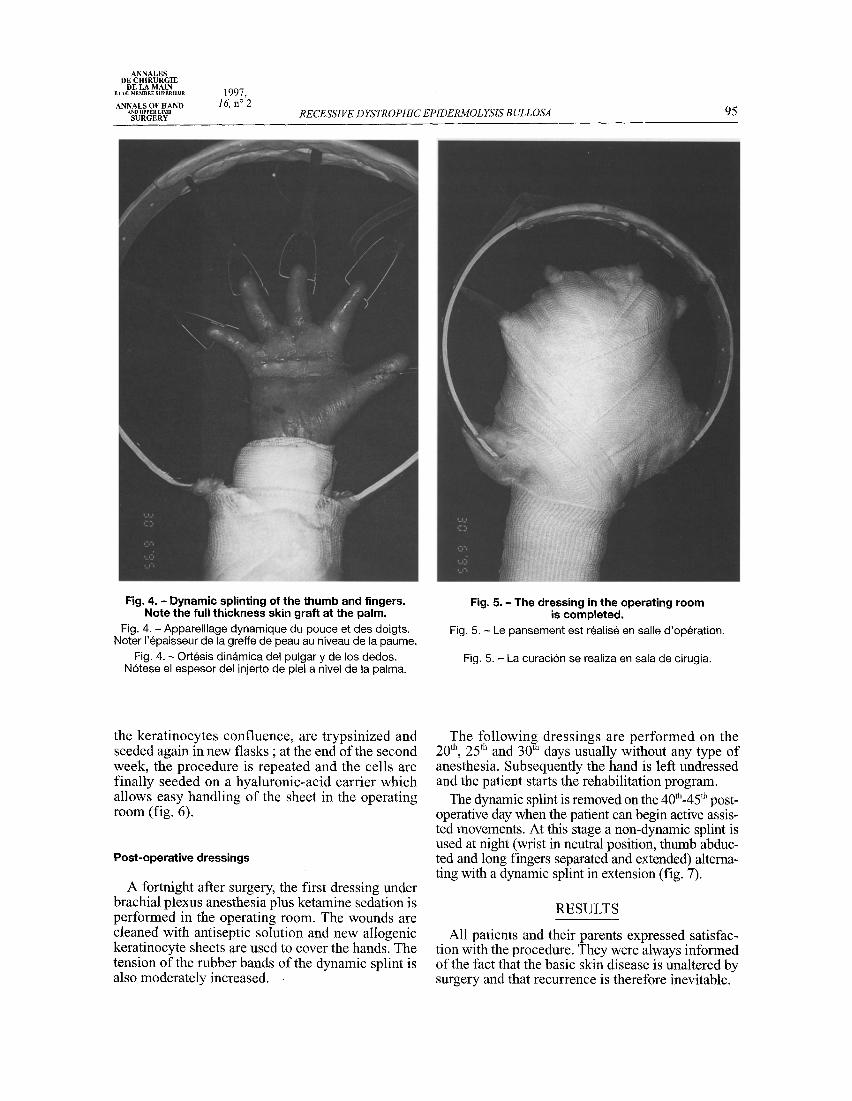
Splinting
Intraoperative and postoperative splinting of the thumb and long fingers is not performed by rigid stabilization with Kirshner wires but using a new dynamic device, consisting of an horseshoe-shaped plastic loom which maintains in calibrated tension a rubber band fixed to P3 of each finger with intra- osseous steel clips (fig. 4, 5). The splint maintains opening of the hand and allows progressively increasing extension of the joints during the post- operative period.
In vitro cultured allogenic keratinocytes
Although uncovered de-epithelialized hands can heal spontaneously from the residual skin appen- dages this predisposes to more fibrosis and rapid
recurrence of the contracture [1]. After having successfully used allogenic in vitro cultured kerati- nocyte sheets in the treatment of IInd degree burns for many years at our Institute [ 18, 19] we decided to also dress the wounds of patients with RDEB using the same method, as biological dressing with allogenic keratinocytes has been show to accelerate spontaneous healing of non-surgical burns and skin graft donor sites, probably because of the release of cytokines which act as growth factors and modula- tors of the immune response [18, 19]..
The method consists of obtaining a small sample from the foreskin of newborn infants (negative to a battery of blood tests for infectious diseases) and cultured on an irradiated murine (3T3) fibroblast feeder-layer. The skin of newborn infants is used because of its greater growth capacity. After 1 week,
ANNALES DE CH1RURGIE
DE LA MAIN ET DO MEMBRE SUPERIEUR
ANNALS OF HAND AND UPPER LIMB SURGERY
1997, 16, n ° 2
RECESSIVE DYSTROPHIC EPIDERMOL YSIS B ULLOSA 95
Fig. 4. - Dynamic splinting of the thumb and fingers. Note the full thickness skin graft at the palm.
Fig. 4. - Apparei l lage dynamique du pouce et des doigts. Noter I 'epaisseur de la greffe de peau au niveau de la paume.
Fig. 4. - Ortesis din~tmica del pulgar y de los dedos. N6tese el espesor del injerto de piel a nivel de la palma.
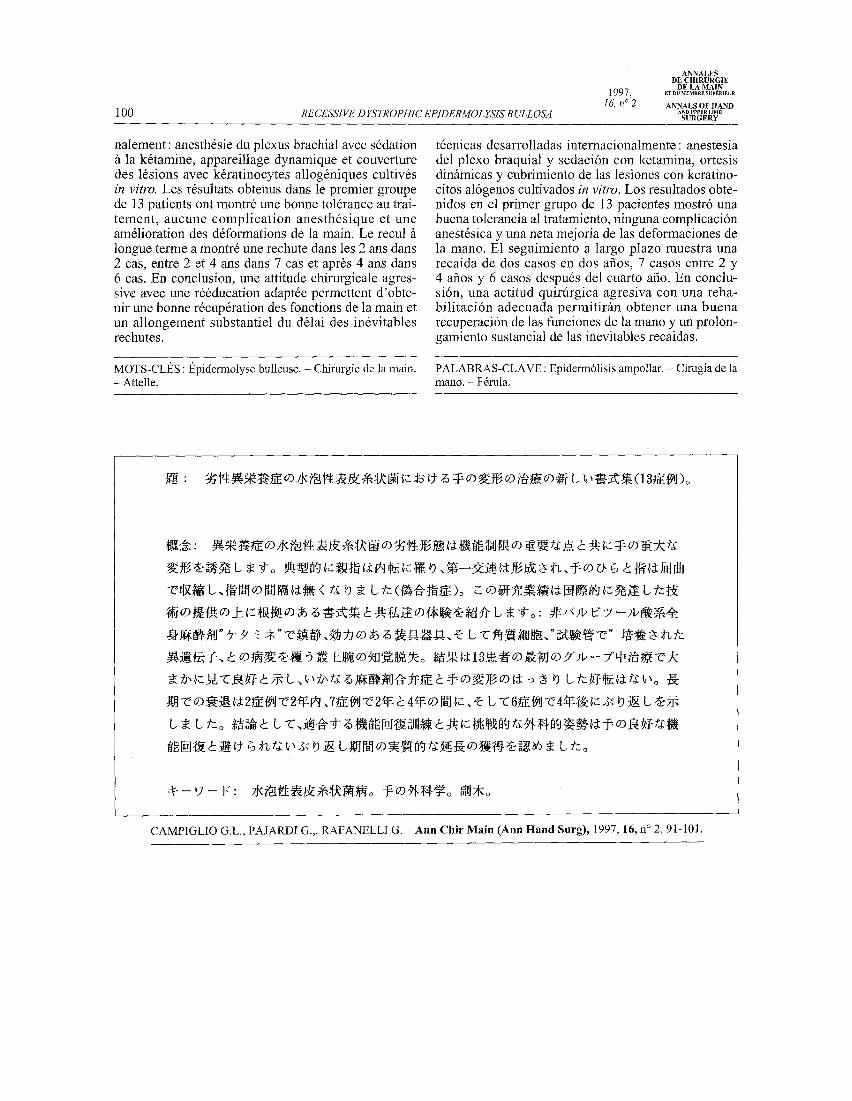
Fig. 5. - The dressing in the operating room is completed.
Fig. 5. - Le pansement est realis6 en salle d 'op6rat ion.
Fig. 5. - La curaci6n se realiza en sala de cirugia.
the keratinocytes confluence, are trypsinized and seeded again in new flasks ; at the end of the second week, the procedure is repeated and the cells are finally seeded on a hyaluronic-acid carrier which allows easy handling of the sheet in the operating room (fig. 6).
Post-operative dressings
A fortnight after surgery, the first dressing under brachial plexus anesthesia plus ketamine sedation is performed in the operating room. The wounds are cleaned with antiseptic solution and new allogenic keratinocyte sheets are used to cover the hands. The tension of the rubber bands of the dynamic splint is also moderately increased.
The following dressings are performed on the th th ~tla 20 , 25 and 30 days usually without any type of
anesthesia. Subsequently the hand is left undressed and the patient starts the rehabilitation program.
The dynamic splint is removed on the 40th-45 tu post- operative day when the patient can begin active assis- ted movements. At this stage a non-dynamic splint is used at night (wrist in neutral position, thumb abduc- ted and long fingers separated and extended) alterna- ting with a dynamic splint in extension (fig. 7).
RESULTS
All patients and their parents expressed satisfac- tion with the procedure. They were always informed of the fact that the basic skin disease is unaltered by surgery and that recurrence is therefore inevitable.

96 RECESSIVE DYSTROPHIC EPIDERMOL YSIS B ULLOSA
ANNALES DE CHIRURGIE
DE LA MAIN 1 9 9 7 , ET ou ~ B . ~ s~P~.,Eu.
16, n o 2 ANNALS OF HAND AND UPPER LIMB
SURGERY
No anesthetic complications were observed.
As far as the surgical technique is concerned the skin graft to the first web and palm showed a mean tacking of 85-90 %. Thumb abduction was good and resulted in excellent opposition and grasping (fig. 8, 9). Comple te extens ion of one or more fingers was not obtained in 7 cases.
From a functional point of view, the mean recur- rence-free interval was 42 months, with values ran- ging from 22 to 50 months (table II).
Fig. 6. - Histological section of a keratinocyte sheet at the end of culture. The hyaluronic carrier
has been removed (HE x 200) Fig. 6. - C o u p e h is to log ique d 'une b a n d e de k6ra t inocy tes
en fin de culture, Le suppo r t en ac ide hya lu ron ique a 6t6 en lev&
Fig. 6. - Cor te h is to l6g ico de una b a n d a de quera t inoc i tos al te rmino del cul t ivo. La base de ac ido h ia lurdnico
ha s ido ret i rada.
TABLE II. - Results. TABLEAU II. - R6sultats. TABLA II. - Resultados.
Insufficient (recurrence before 2 years) : 3
Good (recurrence between 2 and 4 years) : 7
Excellent (recurrence after 4 years) : 5
Total hands treated 15
CONCLUSIONS
The recessive dystrophic epidermolysis bullosa creates severe hand deformities with disabling func- tional limitations to perform important everyday activities. Since surgery does not address the etio- logy of the RDEB the objective of hand reconstruc- tion in these patients is only to restore pinching and grasping function and delay as much as possible recurrence of the deformities. For this reason, the procedure should only be performed when hand function is significantly deteriorated [3].
In this paper, we have presented our experience with a protocol based on the association of various in ternat ional ly deve loped techniques : brachial plexus anesthesia with ketamine sedation, dynamic splinting and coverage of the wounds with allogenic keratinocyte sheets.
Fig. 7. - Once the hand is healed, the patient wears a static splint at night. Fig. 7. - Apr~s c icatr isat ion, le pat ient por te une attel le s ta t ique nocturne.
Fig. 7. - Despu6s de la c icatr izaci6n, el pac ien te uti l iza una or tes is est f i t ica nocturna.

ANNALES DE CHIRURGIE
DE LA MAIN ET DU MEMBRE SUPERIEUR
ANNALS OF HAND AND UPPER LIMB SURGERY
1997 , 16, n ° 2
RECESSIVE D }'STROPHIC EPIDERMOL YSIS BULLOSA 97
Fig. 8. - a) Preoperative view of the hand in a young patient, b) Postoperative view 17 months after surgery. Note the good grasp of the right hand.
Fig. 8. - a) Vue preoperatoire chez un jeune patient, b) Vue postop6ratoire & 17 mois de recul. Noter la qualit6 de la prehension de la main droite.
Fig. 8. - a) Aspecto pre operatorio en un j6ven, b) Aspecto post operatorio a 17 meses de evolucidn. N6tese la calidad de la 3rensi6n de la mano derecha.
Brachial plexus anesthesia associated with keta- mine sedation is effective, well tolerated by the patients, can be repeated for the frequent postopera- tive dressings and, most of all, avoids the risks of endotracheal inmbation [20, 21]. Regional anesthe-
saa is not useful beause of the age of the patients and risk of skin trauma and infection [22].
We prefer to use a full thickness instead of split thickness skin graft to cover defects of the first web and palm because of the difficulty in graft harves-

98 RECESSIVE D IZSTR OPHIC EPIDERMOL YSIS B ULLOSA
1997, 16, n°2
ANNALES DE CH1RURGIE
DE LA MAIN ET I)U MEMBRE SUP~RIEUR
ANNALS OF HAND AND UPPER LIMB SURGERY
Fig. 9. - a) Preoperative view. b) Follow-up a t 4 years. The hand functions are well preserved.
Fig. 9. - a) I~tat pr~op6ratoire, b) R~sultat a 4 ans. Les fonction$ de la main sont prbserv~es.
Fig. 9. - a) Aspecto pre operatorio. Io) Resultado a 4 afio$. Las funciones de la mano estan preservadas.
ting due to the fragility of the skin [1, 23, 24] and because of the minor tendency to postoperat ive contracture of full thickness grafts. We also agree with Rees and Cuomo that flap coverage of these defects is unnecessary and overambitious [ 1, 25].
The use of allogenic in vitro cultured keratino- cytes to cover d e - e p i t h e l i z e d hands p r e s e n t s two advantages : it does not require skin grafts thus reducing the surgical trauma and accelerating the p o s t o p e r a t i v e r ecove ry ; the cel ls re lease

A N N A L E S DE CHIRURGIE
DE L A MAIN ET DIJ MEMBRE SUPERIEUR
A N N A L S OF H A N D AND UPPER LIMB
S U R G E R Y
1997, 16, n ° 2
RECESSIVE DYSTROPHIC EPIDERMOL YSIS B ULLOSA 99
various cytokines which promote spontaneous re-epithelization. Moreover, the possibility of bin- ding certain phamacological molecules (antibiotics, antiseptics, growth factors) to the synthetic carrier is currently studied at the laboratories of our Institute.
The dynamic splint allows very early mobiliza- tion of the hand to prevent recurrence of the defor- mities, but does not interfere with wound healing
and dressings. It also presents the advantages of being easily prepared, inexpensive and avoids the use of intra-articular Kirschner wires which can cause postoperative stiffness of interphalangeal joints [3].
The overall results in this group of patients show that an aggressive attitude along with adequate intra and postoperative rehabilitation allows good resto- ration of hand function and a satisfactory delay of inevitable recurrence.
REFERENCES
1. CUONO C., FINSETH F. - Epidermolysis bullosa : current concepts and management of the advanced hand deformity. Plast. Reconstr. Surg., 1978, 62, 280.
2. GOODMAN H. -Nikolsky sign. Arch. Dermatol. Syph., 1953, 68, 334.
3. GREIDER J., FLATT A. - Care of the hand in recessive epider- molysis bullosa. Plast. Reconstr. Surg., 1983, 72, 222.
4. VON HEBRA F. - Pemphigus. Arzl icher Bericht des K.K. Allgemeinen Krankenhauses zu Wein vom Jahre. 1870 Vienna.
5. P E A R S O N R.S. - The mechanobu l lous diseases . In: FITZPATRICK T., Dermatology in general medicine. New York, McGraw Hill Co, 1971.
6. GEDDE-DAHL T. - Epidermolysis bullosa. A clinical, genetic and epidemiological Study. Baltimore, John Hopkins Press, 1971.
7. GEDDE-DAHL T. - Phenotype-genotype corrections in epider- molysis bullosa. Birth Defects, 1971, 7, 107.
8. EISEN A. - Human skin collagenase : relationship to the pathoge- nesis of epidermolysis bullosa dystrophica. J. Invest. Dermatol., 1969, 52, 449.
9. BAUER E. - The role of human skin collagenase in epidermolysis bullosa. J. Invest. Dermatol., 1977, 68, 119.
10. PEARSON R. - Studies on the pathogenesis of epidermolysis bullosa. J. Invest. Dermatol., 1962, 39, 551.
11. DAVISON B. - Epidermolysis bullosa. J. Med. Genet., 1965, 2, 233. 12. REED W. - Dystrophic epidermolysis bullosa with epidermal neo-
plasms with emphasis on a dermal collagen defect. Birth Defect, 1975, 11,153.
13. GIPSON M. - Squamous cell carcinoma in epidermolysis bullosa dystrophica. Hand, 1975, 7, 179.
14. DUPREE E., HODGES F., SIMON J. - Epidermolysis bullosa of the esophagus. Am. J. Dis. Child, 1969, 117, 349.
15. MICHAELSON J. - Vitamin E trealrnent of epidermolysis bullosa. Arch. Dermatol., 1974, 109, 67.
16. KELLY R., KOFF H., ROTHAUS K., CARTER M., ARTUSIO J. - Brachial plexus anesthesia in eight patient with recessive @stro- phic epidermolysis bullosa. Anesth. Analg., 1987, 66, 1318.
17. LADD A., KIBELE A., GIBBONS S. - Surgical treatment and postoperative splinting of recessive dystrophic epidermolysis bullosa, a~ Hand Surg., 1996, 21,888.
18. DONATI L., KLINGER M., CAMPIGLIO G.L. - Wound healing: an up-to date. In : MOODY F., MONTORSI W., MONTORSI M., Advances in Surgery. New York, Raven Press, 1991
19. DONATI L., MAGLIACANI G., BORMIOLI M., SIGNORINI M., PREIS F. - Clinical experience with keratinocytes grafts. Burns, 1992, 18 Suppl., 19.
20. REDDY A., WONG D. - Epidermolysis bullosa: a review of anes- thetic problems and case reports. Can. Anaesth. Soc. J., 1972, 19, 536.
21. JAMES I., WARK H. - Airway management during anesthesia in patients with epidermolysis bullosa dystrophica. Anesthesiology, 1982, 56, 323.
22. LEE C., NAGEL E. - Anesthetic management of patient with rece- sive epidermolysis bullosa dystrophica. Anesthesiology, 1971,122.
23. PAJARDI G., SIGNORINI M., RAFANELLI G., DONATI L. - L'epidermolisi bollosa congenita : nostro protocollo nel tratta- mentto globale dell'arto superiore. Riv. It. Chit. Plast., 1993, 25 (Suppl), 299
24. ZAREM H., PEARSON R., LEAF N. - Surgical management of hand deformities in recessive dystrophic epidermolysis bullosa. Br. J. Plast. Surg., 1974, 27, 176.
25. REES T., S W I N Y A R D C. - Rehabilitative digital surgery in epidermolysis bullosa. Plast. Reconstr. Surg., 1967, 40, 169.
C A M P I G L I O G.L . , P A J A R D I G. , R A F A N E L L I G. - U n nouveau protocole de t ra i tement des atteintes de la main dans l '6p idermolyse bulleuse dystrophique r6cessive. (En Anglais).
A n n C h i r M a i n ( A n n H a n d S u r g ) , 1997, 16, n ° 2, 91-101.
RI~SUMt~ : La forme r6cessive de l'6pidermolyse bulleuse dystrophique provoque de graves d6forma- tions de la main avec importantes limitations fonctio- nelles. Typiquement le pouce est r6tract6 en adduction, la premi6re commissure est ferm6e, la paume et les doigts sont r6tract6s en flexion et les espaces inter- digitaux ont disparu (pseudo-syndactylie). Ce travail prdsente notre exp6rience avec un protocole fond6 sur l'association des techniques d6velopp6es internatio-
~v
C A M P I G L I O G.L. , P A J A R D I G. , R A F A N E L L I G. - U n n u e v o p r o t o c o l o de t r a t a m i e n t o de las d e f o r m a c i o n e s de la m a n o en la e p i d e r m 6 1 i s i s a m p o l l a r d i s t r d f i c a r e c e s i v a (13 casos). A n n C h i t M a i n ( A n n H a n d S u r g ) , 1997, 16, n ° 2, 91-101.
RESUMEN : La forma recesiva de la epiderm61isis ampollar distr6fica provoca graves deformaciones de la mano con una limitaci6n funcional importante. Tipicamente el pulgar se presenta con una contractura en adducci6n, la primer comisura se encuentra cer- rada, la palma y los dedos con una retraccidn en flexidn y los espacios interdigitales desaparacen (seudo sindactilia). Este trabajo presenta nuesta expe- riencia de un protocolo basado en la asociaci6n de
r
100 RECESSIVE DYSTROPHIC EPIDERMOL YSIS BULLOSA
ANNALES DE CHIRURGIE
DE LA MAIN 1997, ~ ou ~ s u P ~ u ~
16, n ° 2 ANNALS OF HAND AND UPPER LIMB
SURGERY
nalement : anesth6sie du plexus brachial avec sddation /~ la k6tamine, appareillage dynamique et couverture des 16sions avec k6ratinocytes allog6niques cultiv6s in vitro. Les r6sultats obtenus dans le premier groupe de 13 patients ont montr6 une bonne toldrance au trai- tement, aucune compl ica t ion anesth6sique et une am61ioration des d6formations de la main. Le recul fi longue terme a montr6 une rechute dans les 2 ans dans 2 cas, entre 2 et 4 ans dans 7 cas et apr6s 4 ans dans 6 cas. En conclusion, une attitude chirurgicale agres- sive avec une rd6ducation adapt6e permettent d'obte- nir une bonne rdcup6ration des fonctions de la main et un allongement substantiel du d61ai des in6vitables rechutes.
MOTS-CLt~S : t~pidermolyse bulleuse. - Chirurgie de la main. - Attelle.
t6cnicas desarrolladas internacionalmente: anestesia del plexo braquial y sedacidn con ketamina, ortesis dinfimicas y cubrimiento de las lesiones con keratino- citos aldgenos cultivados in vi tro. Los resultados obte- nidos en el primer grupo de 13 pacientes mostr6 una buena tolerancia al tratamiento, ninguna complicacidn anest6sica y una neta mejoria de las deformaciones de la mano. E1 seguimiento a largo plazo muestra una recaida de dos casos en dos afios, 7 casos entre 2 y 4 afios y 6 casos despu6s del cuarto afio. En conclu- sidn, una actitud quirfirgica agresiva con una reha- bilitacidn adecuada permitirfin obtener una buena recuperaci6n de las funciones de la mano y un prolon- gamiento sustancial de las inevitables recaidas.
PALABRAS-CLAVE : Epiderm61isis ampollar. - Cirugia de la mano. - F6rula,
CAMPIGLIO G.L., P A J A R D I G.,. RAFANELLI G. - Ann Chir Main (Ann Hand Surg), 1997, 16, n ° 2, 91-101.