a polymorphic mir-155 binding site in agtr1 is associated with cardiac hypertrophy in friedreich...
TRANSCRIPT

Journal of Molecular and Cellular Cardiology 51 (2011) 848–854
Contents lists available at SciVerse ScienceDirect
Journal of Molecular and Cellular Cardiology
j ourna l homepage: www.e lsev ie r.com/ locate /y jmcc
Original article
A polymorphic miR-155 binding site in AGTR1 is associated with cardiac hypertrophyin Friedreich ataxia
Matthew Kelly a,b, Richard D. Bagnall a, Roger E. Peverill c, Lesley Donelan c, Louise Corben d,Martin B. Delatycki d,e, Christopher Semsarian a,b,f,⁎a Agnes Ginges Centre for Molecular Cardiology, Centenary Institute, Sydney, New South Wales, Australiab Sydney Medical School, University of Sydney, New South Wales, Australiac MonashHEART and Monash Cardiovascular Research Centre, Southern Clinical School, Monash University, Melbourne, Victoria, Australiad Murdoch Childrens Research Institute, Victoria, Australiae Clinical Genetics, Austin Health, Victoria, Australiaf Department of Cardiology, Royal Prince Alfred Hospital, Sydney, New South Wales, Australia
⁎ Corresponding author at: Agnes Ginges Centre for MInstitute, Locked Bag 6, NewtownNSW2042, Australia. Te9565 6101.
E-mail address: [email protected] (C. Se
0022-2828/$ – see front matter © 2011 Elsevier Ltd. Aldoi:10.1016/j.yjmcc.2011.07.001
a b s t r a c t
a r t i c l e i n f oArticle history:Received 24 May 2011Received in revised form 22 June 2011Accepted 5 July 2011Available online 12 July 2011
Keywords:Friedreich ataxiaCardiac function and structureGenesRenin–Angiotensin–Aldosterone systemmicroRNA
Friedreich ataxia (FRDA) is an autosomal recessive neurodegenerative condition with a heterogeneous cardiacphenotype caused primarily by an expanded GAA trinucleotide repeat in the frataxin gene (FXN). FXN isimportant inmitochondrial iron efflux, sensitivity to oxidative stress, and cell death. The number of GAA repeatson the smaller FXN allele (GAA1) only accounts for a portion of the observed variability in cardiac phenotype.Genetic modifying factors, such as single nucleotide polymorphisms (SNPs) in genes of the Renin–Angiotensin–Aldosterone system (RAAS), may contribute to phenotype variability. This study investigated genetic variabilityin the angiotensin-II type-1 receptor (AGTR1), angiotensin-converting enzyme (ACE), and ACE2 genes as cardiacphenotype modifying factors in FRDA patients. Comprehensive review of the AGTR1, ACE and ACE2 genesidentified twelve haplotype tagging SNPs. Correlation of these SNPs with left ventricular internal diameter indiastole (LVIDd), interventricular septalwall thickness (SWT) and left ventricularmass (LVM)was examined in alarge Australian FRDA cohort (n=79) with adjustments performed for GAA repeats, age, sex, body surface areaand diastolic blood pressure. A significant inverse relationship was observed between GAA1 and LVIDd(p=0.010) but notwithSWTor LVMafter adjustment for covariates. TheAGTR1polymorphismrs5186wasmorecommon in FRDA patients than in a control population (p=0.002). Using a recessivemodel of inheritance, the Callele of rs5186 was associated with a significant increase in SWT (p=0.003) and LVM (p=0.001). Thisfunctional polymorphism increases expression of AGTR1 by altering the binding site for miR-155, a regulatorymicroRNA. No significant associations with left ventricular structure were observed for the remaining RAASpolymorphisms. TheAGTR1polymorphism rs5186 appears tomodify the FRDAcardiac phenotype independentlyofGAA1. This study supports the role of RAAS polymorphismsasmodifiers of cardiac phenotype in FRDApatients.
olecular Cardiology, Centenaryl.:+612 9565 6195; fax:+612
msarian).
l rights reserved.
© 2011 Elsevier Ltd. All rights reserved.
1. Introduction
Friedreich ataxia (FRDA) is an autosomal recessive neurodegen-erative disease arising from mutations in both alleles of the frataxingene (FXN), with a reported prevalence of 1 in 29000, making it themost common inherited ataxia [1,2]. In approximately 97% of casesthe mutant alleles have an expansion of a GAA trinucleotide repeat inintron 1 of FXN that reduces the amount of frataxin available to assistwith mitochondrial iron efflux and increases sensitivity to oxidative
stress, resulting in cell damage and death due to excess production offree radicals [1,3–5].
Aswell as the neurological features of the disease, a large proportionof FRDA patients develop abnormalities of cardiac structure or function.The most common observations are increased thickness of the leftventricular wall [6–12], reduced left ventricular cavity size [10,12,13]and increased left ventricularmass index (LVMI) [10–12].Most patientshave a normal ejection fraction [7,11,13], but a proportion of patientsdevelop left ventricular wall thinning, dilatation and a reduction inejection fraction [14,15]. Heart failure and cardiac arrhythmias arethought to be the most important causes of death in FRDA [16,17]. Theseverity of cardiac involvement in patients with FRDA is highly variable[7,14], suggesting that there are factors capable ofmodifying the cardiacphenotype. These modifying factors could be environmental and/orgenetic, andmayact either byexacerbating or protectingagainst disease[18].

849M. Kelly et al. / Journal of Molecular and Cellular Cardiology 51 (2011) 848–854
One such geneticmodifying factor is the number of GAA repeats onthe smaller FXN allele (GAA1). Previous studies have reported apositive correlation of GAA1 with the presence of cardiac structuralchange in FRDA [3,19,20] and increases in interventricular septal wallthickness (SWT) [6–9,11] and left ventricular mass (LVM) [7,9,13].While most studies have reported a more important role for GAA1,associations between the number of GAA repeats on the larger FXNallele (GAA2) with age of disease onset [19,21,22], SWT [11] and thepresence of cardiac disease [19,20] have also been reported. However,FXN allele GAA repeat length only accounts for a portion of theobserved variability of cardiac abnormalities (up to 20%) [11,19–22],suggesting there are other contributing factors yet to be identified.
The Renin–Angiotensin–Aldosterone system (RAAS) is a well-established mediator of cardiac growth, and functions as thepredominant system used by the body to maintain blood pressurehomeostasis. This is mediated primarily through the activation of theangiotensin-II type 1 receptor (AT1R) by angiotensin-II, which resultsin the activation of several pro-hypertrophic signaling cascades [23].Consequently, the components of the RAAS capable of influencing theproduction or activity of angiotensin-II are biologically plausiblecandidate modifiers of cardiac hypertrophy in diseases with a cardiacphenotype, such as FRDA [24]. These include AGTR1, which encodesthe AT1R, as well as ACE and ACE2, which encode the convertingenzymes of the RAAS, angiotensin converting enzyme (ACE) and itscounter-regulatory homolog ACE2 [25]. Several studies have investi-gated polymorphisms in the genes encoding these key RAAS proteinsas potential markers or modifiers of disease severity in othercardiovascular diseases [24,26–28].
This study sought to investigate the association between geneticvariability of the AGTR1, ACE and ACE2 genes and cardiac phenotype inFRDA patients by examining the correlation between several poly-morphisms in these genes and three echocardiographic measures ofcardiac structure previously shown to be abnormal in FRDA — leftventricular internal diastolic diameter (LVIDd), SWT and LVM.
2. Materials and methods
2.1. Study populations
Patients were recruited from amultidisciplinary FRDA clinic whichsees all individuals with FRDA who request to be seen. Approximatelytwo thirds of attendees are from the states of Victoria and New SouthWales, Australia with the other third being from other states oroverseas. The clinic sees individuals with the full range of thephenotypic spectrum. Clinical evaluation included a detailed physicalexamination, ECG and echocardiography. All participants werehomozygous for an expanded GAA repeat within intron 1 of FXN;patients with point mutations were excluded. Two patients wereexcluded, one due to the presence of aortic valvular disease and onedue to previous myocardial infarction. The study protocol wasapproved by the Southern Health Human Research and EthicsCommittee and all patients gave informed consent. Echocardiographicfindings on a subgroup (41/79) of the current study cohort have beenpreviously reported [12]. The control population used in this studyconsisted of 170 predominantly Caucasian individuals from Sydney,Australia who did not suffer from any cardiac-related health problemsat the time of blood collection.
2.2. Echocardiography
Transthoracic echocardiography was performed using a Sonos5500 ultrasound machine (Philips, Amsterdam, The Netherlands) andmeasurements were performed off-line using Xcelera V1.2 L4 SP2(Philips, Amsterdam, The Netherlands). Nearly all studies wereperformed by the one echocardiographer (LD). M-mode images ofthe left ventricle were obtained in the parasternal long axis view just
distal to the mitral valve leaflet tips after alignment of the cursorperpendicular to the left ventricular wall. 2-D images were used tofacilitate identification of the endocardium and standard M-modemeasurements of LVIDd and SWT were performed [29,30]. LVM wascalculated using the modified formula of Devereux et al.[31] andcorrected for body surface area (BSA) as LVM index (LVMI). Relativewall thickness (RWT) was calculated as two times the posterior wallthickness (PWT) divided by LVIDd. Four- and two-chamber 2-dimensional loops of left ventricular contraction were recorded andused for measurement of left ventricular end-diastolic volume(LVEDV) and ejection fraction using the biplane method of discs.Left ventricular length (LVL) was measured as the distance betweenthe plane of the mitral annulus and the apical endocardium in the twoand four-chamber views at end-diastole, using the longest dimensionobserved from these two views.
2.3. Genetic analysis
Genomic DNA was extracted [32] and the number of GAA repeatsin the FXN gene was measured [33] as described previously, withGAA1 representing the shorter allele and GAA2 representing thelonger allele. Analysis of the linkage disequilibrium (LD) structure ofthe AGTR1, ACE and ACE2 genes was performed using the HapMapPhase II project data from CEPH Caucasian trios [34]. The haplotypetagging SNPs that defined the underlying haplotype structures wereidentified using pairwise tagging with r2 thresholds of 0.8 and minorallele frequency thresholds of 0.05 using the Haploview 4.2 software(version 12.2.0) [35,36]. The AGTR1, ACE and ACE2 genes had five, twoand three tag SNPs selected, respectively, which captured themajorityof the common haplotype variation within these genes (Fig. 1). TheAGTR1 SNP rs5186 was also examined based on multiple previouslyreported associations with several cardiovascular diseases [37–42].
Genotyping of SNPs was performed using the TaqMan 5′ nucleaseactivity assay (Applied Biosystems, USA), according to the manufac-turer's recommendations. Briefly, the reaction mixture consisted of10 ng DNA, 1× Express qPCR Supermix with premixed ROX (Invitro-gen), and 1× SNP-specific TaqMan probe, made up to a final volume of5 μL with triple distilled water. PCR amplification was performed at95 °C for 10 min, followed by 40 thermal cycles of 95 °C for 15 s, and60 °C for 1 min. Fluorescence was measured for FAM (excitationwavelength 488 nm, emission wavelength 518 nm) and VIC (excita-tion wavelength 488 nm, emission wavelength 552 nm) using a7900HT Fast Real-Time PCR System (Applied Biosystems, USA). Datawere gathered and analyzed using SDS version 2.4 software (AppliedBiosystems, USA).
In addition to the selected tag SNPs, an insertion/deletion (I/D)polymorphism in the ACE gene (ACE I/D) was genotyped by PCR asdescribed previously, whereby the insertion (I) and deletion (D)alleles correspond to a 480 bp and 193 bp amplicon, respectively [43].
2.4. Statistical analysis
Statistical analyses were performed using PASW Statistics 17.0 forMacintosh (SPSS Inc. Chicago, IL, USA).Deviation fromHardy–Weinbergequilibrium was assessed using the χ2 goodness of fit test with onedegree of freedom. All data are expressed asmean±standard deviation,unless noted otherwise. Differences in categorical and continuousvariables between cohorts were compared using the χ2-test andindependent samples t-test, respectively. The relationship of GAA1and GAA2 with LVIDd, SWT and LVM was evaluated using multiplelinear regression,with adjustment performed for age and factors knownto influence left ventricular structure (sex, BSA and diastolic bloodpressure). The relations of GAA1 with LVEDV and LVL were alsoanalyzed to assess for consistency with findings obtained for LVIDd.
The association of individual polymorphisms with LVIDd, SWT andLVM was assessed by univariate general linear model analysis with
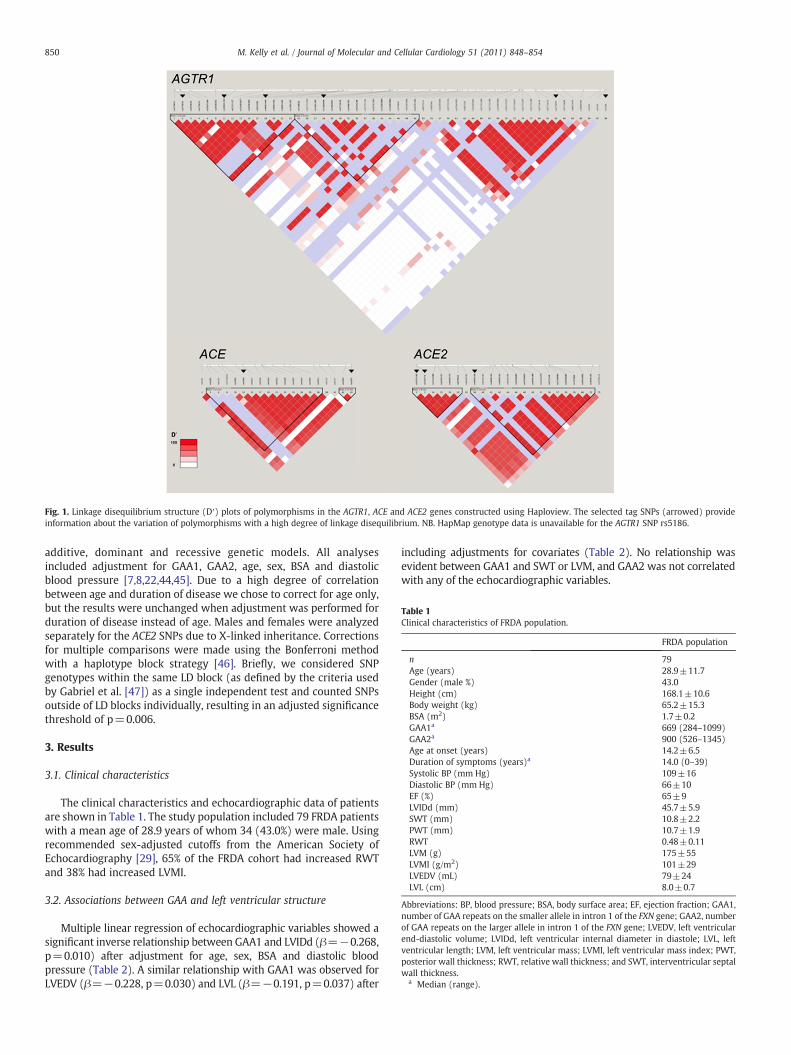
Fig. 1. Linkage disequilibrium structure (D′) plots of polymorphisms in the AGTR1, ACE and ACE2 genes constructed using Haploview. The selected tag SNPs (arrowed) provideinformation about the variation of polymorphisms with a high degree of linkage disequilibrium. NB. HapMap genotype data is unavailable for the AGTR1 SNP rs5186.
Table 1Clinical characteristics of FRDA population.
FRDA population
n 79Age (years) 28.9±11.7Gender (male %) 43.0Height (cm) 168.1±10.6Body weight (kg) 65.2±15.3BSA (m2) 1.7±0.2GAA1a 669 (284–1099)GAA2a 900 (526–1345)Age at onset (years) 14.2±6.5Duration of symptoms (years)a 14.0 (0–39)Systolic BP (mm Hg) 109±16Diastolic BP (mm Hg) 66±10EF (%) 65±9LVIDd (mm) 45.7±5.9SWT (mm) 10.8±2.2PWT (mm) 10.7±1.9RWT 0.48±0.11LVM (g) 175±55LVMI (g/m2) 101±29LVEDV (mL) 79±24LVL (cm) 8.0±0.7
Abbreviations: BP, blood pressure; BSA, body surface area; EF, ejection fraction; GAA1,number of GAA repeats on the smaller allele in intron 1 of the FXN gene; GAA2, numberof GAA repeats on the larger allele in intron 1 of the FXN gene; LVEDV, left ventricularend-diastolic volume; LVIDd, left ventricular internal diameter in diastole; LVL, leftventricular length; LVM, left ventricular mass; LVMI, left ventricular mass index; PWT,posterior wall thickness; RWT, relative wall thickness; and SWT, interventricular septalwall thickness.
a Median (range).
850 M. Kelly et al. / Journal of Molecular and Cellular Cardiology 51 (2011) 848–854
additive, dominant and recessive genetic models. All analysesincluded adjustment for GAA1, GAA2, age, sex, BSA and diastolicblood pressure [7,8,22,44,45]. Due to a high degree of correlationbetween age and duration of disease we chose to correct for age only,but the results were unchanged when adjustment was performed forduration of disease instead of age. Males and females were analyzedseparately for the ACE2 SNPs due to X-linked inheritance. Correctionsfor multiple comparisons were made using the Bonferroni methodwith a haplotype block strategy [46]. Briefly, we considered SNPgenotypes within the same LD block (as defined by the criteria usedby Gabriel et al. [47]) as a single independent test and counted SNPsoutside of LD blocks individually, resulting in an adjusted significancethreshold of p=0.006.
3. Results
3.1. Clinical characteristics
The clinical characteristics and echocardiographic data of patientsare shown in Table 1. The study population included 79 FRDA patientswith a mean age of 28.9 years of whom 34 (43.0%) were male. Usingrecommended sex-adjusted cutoffs from the American Society ofEchocardiography [29], 65% of the FRDA cohort had increased RWTand 38% had increased LVMI.
3.2. Associations between GAA and left ventricular structure
Multiple linear regression of echocardiographic variables showed asignificant inverse relationship between GAA1 and LVIDd (β=−0.268,p=0.010) after adjustment for age, sex, BSA and diastolic bloodpressure (Table 2). A similar relationship with GAA1 was observed forLVEDV (β=−0.228, p=0.030) and LVL (β=−0.191, p=0.037) after
including adjustments for covariates (Table 2). No relationship wasevident between GAA1 and SWT or LVM, and GAA2 was not correlatedwith any of the echocardiographic variables.

Table 2Association between GAA1 and echocardiographic measures of left ventricularstructure.
GAA1 standardized beta coefficient p-value
SWT (mm) 0.047 0.680LVIDd (mm) −0.268 0.010⁎
LVM (g) −0.093 0.363LVEDV (mL) −0.228 0.030⁎
LVL (cm) −0.191 0.037⁎
⁎ pb0.05.
851M. Kelly et al. / Journal of Molecular and Cellular Cardiology 51 (2011) 848–854
3.3. Genotype frequencies of RAAS polymorphisms
Minor allele frequencies of all polymorphisms in the control andFRDA populations are shown in Table 3. All polymorphisms were inHardy–Weinberg equilibrium in both populations, with the exceptionof the ACE2 SNP rs233575 in FRDA patients (p=0.02), which wasexcluded from further analysis (Table 3). The C allele of rs5186 inAGTR1 was significantly more frequent in the FRDA population thancontrols (p=0.002) (Table 3). There was no significant difference inallele frequency observed for the remaining SNPs in AGTR1 or those inACE and ACE2 (Table 3).
3.4. Associations between RAAS polymorphisms and left ventricularstructure
An association with greater SWT was observed for the C allele ofrs5186 using an additive and recessive genetic model (p=0.008 andp=0.003, respectively) (Table 4). The association observed for therecessive model remained significant following correction for multi-ple comparisons. The C allele of rs5186 was also significantlyassociated with LVM using an additive and recessive model(p=0.002 and p=0.001, respectively) (Table 4). GAA1 did notcontribute significantly to the association observed for SWT or LVM.No significant association was observed between rs5186 genotypeand LVIDd (Table 4).
Table 3Minor allele frequency of polymorphisms in the AGTR1, ACE and ACE2 genes in the FRDA p
Polymorphism Control
n(AA) n(Aa) n(aa) MAF HWE
AGTR1rs275652 (A/C) 117 51 2 0.16±0.02 0.256rs10935724 (A/G) 82 73 15 0.30±0.03 1.000rs4681440 (C/T) 127 39 4 0.14±0.02 0.531rs1492099 (G/A) 128 38 4 0.14±0.02 0.514rs275649 (G/A) 106 56 8 0.21±0.02 0.820rs5186 (A/C) 102 60 8 0.22±0.02 1.000
ACErs4309 (C/T) 48 83 39 0.47±0.03 0.761rs4363 (A/G) 43 88 39 0.49±0.03 0.759ACE I/D (I/D) 41 87 41 0.50±0.03 0.760
ACE2 malesrs233575 (T/C) 53 – 31 0.37±0.05 –
rs2074192 (C/T) 55 – 29 0.35±0.05 –
rs4646156 (T/A) 57 – 27 0.32±0.05 –
ACE2 femalesrs233575 (T/C) 40 35 11 0.33±0.04 0.468rs2074192 (C/T) 25 46 15 0.44±0.04 0.516rs4646156 (T/A) 40 33 13 0.34±0.04 0.160
Abbreviations: HWE, Hardy–Weinberg equilibrium p-value; MAF, minor allele frequency (bby ‘a’.⁎ pb0.05.⁎⁎ pb0.01.
Trends towards increased LVMwere observed for males with the Aallele of ACE2 polymorphism rs4646156 (p=0.046) and patients withthe I/I allele of the ACE I/D polymorphism (p=0.034), however, thesedid not remain significant following correction for multiple compar-isons. The remaining AGTR1, ACE and ACE2 polymorphisms were notassociated with LVIDd, SWT or LVM (Table 4).
4. Discussion
We have used a comprehensive tag SNP approach to investigatethe association of genetic variability in three important genes of theRAAS with measures of cardiac phenotype severity in FRDA, namelyLVIDd, SWT and LVM. The genes selected for investigation wereAGTR1, which encodes AT1R, the predominant angiotensin-II receptorin the cardiovascular system, and the ACE and ACE2 genes, whichencode the converting enzymes directly involved in the productionand degradation of angiotensin-II. We have identified rs5186, a SNP inAGTR1, as a potential modifier of the cardiac phenotype in a largepopulation of FRDA patients.
The majority of FRDA patients in this study had an elevated RWT,while a lesser proportion demonstrated an elevated LVMI. Theexplanation for this difference is that an increase in wall thicknessin FRDA is commonly accompanied by a decrease in left ventricularsize [6,8,12,13], in which case an increase in wall thickness will notnecessarily result in an increase in LVM. While an increase in RWTwith normal LVMI (concentric remodeling) is a common finding inhypertension [48], it is unclear if this represents an early stage ofhypertensive heart disease or whether it may be a patient or agespecific pattern of the hypertrophic process. An additional factor inFRDA, where previous studies have reported an inverse relationshipbetween age and LVMI [11,12], is that a higher LVMI may lead todecreased survival and that patients with an increased LVMI maytherefore be less represented in any cohort study. Moreover, not onlyis it not understood whether there are histopathological differencesbetween the different geometric patterns in hypertension, there iseven less information available about what underlies the changes inleft ventricular structure seen in FRDA.
opulation and the control population.
FRDA
n(AA) n(Aa) n(aa) MAF HWE χ2
p-value
49 27 2 0.20±0.03 0.722 0.31338 30 10 0.32±0.04 0.304 0.69456 19 3 0.16±0.03 0.398 0.51855 21 2 0.16±0.03 1.000 0.46143 31 4 0.25±0.03 0.766 0.34330 42 7 0.35±0.04 0.219 0.002⁎⁎
23 42 10 0.41±0.04 0.237 0.21722 39 18 0.53±0.04 1.000 0.44125 40 12 0.43±0.04 1.000 0.166
18 – 16 0.47±0.09 – 0.14922 – 12 0.35±0.08 – 0.91019 – 15 0.44±0.09 – 0.082
21 24 0 0.27±0.04 0.020⁎ 0.2828 26 10 0.52±0.05 0.363 0.216
18 24 3 0.33±0.04 0.313 0.875
ased on control population). Major allele represented by ‘A’, minor allele represented

Table 4Association of AGTR1, ACE and ACE2 polymorphisms with echocardiographic measures of left ventricular structure.
Polymorphism Genotype p-value
Additive Dominant Recessive
AGTR1rs275652 AA AC CC
LVIDd (mm) 4.6±0.6 4.6±0.5 4.6±0.9 0.983 0.859 0.924SWT (mm) 10.6±2.5 11.0±1.7 10.3±1.0 0.779 0.628 0.683LVM (g) 172±59 183±47 166±76 0.840 0.771 0.654
rs10935724 AA AC CCLVIDd (mm) 4.5±0.7 4.6±0.4 4.8±0.5 0.263 0.918 0.111SWT (mm) 10.7±1.7 11.1±2.7 10.0±2.4 0.411 0.784 0.164LVM (g) 170±49 183±62 174±54 0.925 0.905 0.690
rs4681440 CC CT TTLVIDd (mm) 4.5±0.6 4.6±0.4 5.1±0.3 0.244 0.374 0.108SWT (mm) 11.0±2.2 10.4±2.0 9.1±1.7 0.196 0.130 0.180LVM (g) 178±57 173±53 164±24 0.718 0.435 0.645
rs1492099 GG GA AALVIDd (mm) 4.6±0.6 4.6±0.5 4.6±0.9 0.975 0.847 0.927SWT (mm) 10.7±2.4 11.0±1.7 10.3±1.0 0.853 0.785 0.683LVM (g) 172±56 186±53 166±76 0.698 0.549 0.654
rs275649 GG GA AALVIDd (mm) 4.7±0.6 4.4±0.6 4.8±0.7 0.207 0.131 0.628SWT (mm) 10.7±2.4 11.0±2.0 10.2±0.9 0.713 0.786 0.481LVM (g) 177±55 175±56 175±60 0.897 0.783 0.682
rs5186 AA AC CCLVIDd (mm) 4.5±0.6 4.6±0.6 4.9±0.9 0.830 0.585 0.521SWT (mm) 10.8±2.6 10.6±1.6 11.7±2.8 0.008⁎ 0.459 0.003⁎⁎
LVM (g) 175±65 170±47 208±48 0.002⁎⁎ 0.451 0.001⁎⁎
ACErs4309 CC CT TT
LVIDd (mm) 4.6±0.5 4.5±0.6 4.7±0.8 0.139 0.382 0.178SWT (mm) 10.9±1.7 10.6±1.9 11.2±4.0 0.411 0.914 0.207LVM (g) 182±43 166±53 192±80 0.115 0.547 0.084
rs4363 GG GA AALVIDd (mm) 4.6±0.5 4.5±0.6 4.8±0.6 0.337 0.716 0.131SWT (mm) 11.0±1.7 10.4±1.9 11.2±3.1 0.264 0.673 0.194LVM (g) 181±47 164±51 193±68 0.180 0.905 0.088
ACE I/D DD ID IILVIDd (mm) 4.7±0.4 4.4±0.6 4.8±0.7 0.231 0.436 0.238SWT (mm) 11.0±1.7 10.4±1.8 11.6±3.7 0.176 0.923 0.082LVM (g) 188±45 159±48 202±80 0.047⁎ 0.616 0.034⁎
ACE2 malesrs2074192 C T
LVIDd (mm) 4.6±0.4 5.0±0.5 0.268 – –
SWT (mm) 12.0±2.7 10.8±1.0 0.164 – –
LVM (g) 204±65 207±37 0.485 – –
rs4646156 T ALVIDd (mm) 4.8±0.5 4.7±0.4 0.600 – –
SWT (mm) 10.9±1.2 12.5±3.0 0.065 – –
LVM (g) 195±45 218±68 0.046⁎ – –
ACE2 femalesrs2074192 CC CT TT
LVIDd (mm) 4.7±0.7 4.5±0.7 4.1±0.4 0.235 0.106 0.297SWT (mm) 9.8±0.8 10.3±2.0 9.9±2.0 0.791 0.709 0.670LVM (g) 160±36 159±46 129±28 0.439 0.371 0.243
rs4646156 TT TA AALVIDd (mm) 4.5±0.5 4.4±0.7 4.6±0.3 0.620 0.933 0.329SWT (mm) 10.0±2.0 10.2±1.8 10.7±1.2 0.889 0.846 0.631LVM (g) 154±50 151±37 166±32 0.889 0.827 0.635
Dominant and recessive with respect to the minor allele in the control population. Data are presented as mean±SD.⁎ pb0.05 (significant following Bonferroni correction).⁎⁎ pb0.006 (significant following Bonferroni correction).
852 M. Kelly et al. / Journal of Molecular and Cellular Cardiology 51 (2011) 848–854
There is evidence from a number of studies that GAA1 influences leftventricular structure in FRDA, although results have not been consistent[49]. In this cohort, GAA1 was found to be independently and inverselyassociated with LVIDd, while there was no relation of GAA1 with eitherSWT or LVM. The observed association between GAA1 and smaller leftventricular sizewas supportedbyadditional analyses thatdemonstratedsimilar inverse associations of GAA1 with the related, but independent,echocardiographic measures of LVEDV and LVL. While previous studies
have reported associations of GAA1 with both SWT and LVM [7,9], thishas not been a universal finding [8,11] and one MRI study has alsoreported an inverse relationship between GAA1 and LVEDV [13].
In contrast with the GAA1 findings in this cohort, the rs5186 C allelewas found to be significantly associatedwith increases in SWTand LVM.The rs5186 SNP is a functional A/C polymorphism that occurs in thetarget sequence of a regulatory microRNA, miR-155, in the 3′untranslated region of AGTR1 (Fig. 2) [50,51]. In the presence of the A

Fig. 2. Interaction of rs5186 andmiR-155. In the presence of the A allelemiR-155 regulates the production of AT1R by AGTR1. The rs5186 C allele interrupts base-pair complimentarityin the miR-155 target site, resulting in increased levels of AT1R (Adapted from Sethupathy et al., 2007) [51].
853M. Kelly et al. / Journal of Molecular and Cellular Cardiology 51 (2011) 848–854
allele, miR-155 downregulates the expression of AGTR1, resulting inreduced production of AT1R. However, the rs5186 C allele interruptsbase-pair complimentarity between miR-155 and the cis-regulatorytarget site, decreasing the ability of miR-155 to bind, thereby increasingthe expression of AT1R [50,51]. Previous studies of rs5186 have reportedpredominantly negative implications of the C allele, including associ-ations with increased degree of cardiac hypertrophy in patients withhypertension and hypertrophic cardiomyopathy [39], as well as morefrequent development of hypertension [38,41], diastolic heart failure[42],myocardial infarction [40] and oxidative stress in heart failure [37].
The echocardiographic measures of left ventricular structureassociated with GAA1 were different to those associated withrs5186, suggesting that these genes modify the cardiac phenotypeof FRDA by independent mechanisms. This is not surprising given thedifferent function of these genes. GAA1 is inversely correlated withthe amount of frataxin produced, with lower frataxin levels likely tolead to mitochondrial dysfunction and cardiomyocyte death [5,49].Therefore, one explanation for the reduction in chamber size could bea reduction in myocyte number and an accompanying increase incardiac fibrosis. In contrast, rs5186 indirectly influences hypertrophicsignaling cascades activated by AT1R, suggesting the observed cardiachypertrophy in FRDA may develop as a result of pathologicalcardiomyocyte hypertrophy [23]. However, AT1R signaling has alsobeen linked to both oxidative stress and cardiac fibrosis, so this maybe a common mechanism by which these genetic factors modify thecardiac phenotype [37,52,53].
An unexpected and intriguing finding of this study was that the Callele of rs5186 was more common in this cohort of FRDA patientsthan in a healthy control population. In addition, the rs5186polymorphism was more common in this FRDA cohort than severalother studies that have examined this SNP [37–41,51]. Combinedwiththe observed associations of the C allele with increased SWT and LVM,the significantly greater frequency of rs5186 in FRDA patients may beof particular importance. Based on the previous reports of rs5186associating with negative outcomes in several cardiovascular diseasesit may have been expected that the increased frequency of the C allelein the FRDA population would be detrimental and result in a moresevere phenotype [37–42]. However, the increase in frequency of theC allele in FRDA patients is more consistent with a protective effect ofrs5186, resulting in increased survival and therefore overrepresenta-tion of the allele in the survivors available for participation in thisstudy. That is, the rs5186 polymorphism isn't more common in theFRDA population at birth, but the prohypertrophic cardiac effects ofthe C allele confer a survival advantage, resulting in an enrichedpopulation in a cohort in which some of the group has already died. Tothe best of our knowledge this would be the first report of a beneficialeffect of the rs5186 polymorphism. Further investigation of theprevalence and cardiovascular effects of rs5186 in other large FRDApopulations is required. Future studies of this nature should also
assess the activity of miR-155 in FRDA patients, as it is the likelymechanism by which rs5186 modifies the cardiac phenotype.
There is currently no treatment proven to slow or prevent diseaseprogression or cause regression of the pathological features in FRDA[10,54,55]. This study provides some evidence that the RAAS may beinvolved in the development of the cardiac phenotype in FRDA, the mostcommoncauseofdeath inFRDApatients. Therefore,whilenot a treatmentfor the underlyingmitochondrial iron trafficking deficiency, theremay besome therapeutic benefit in administering pharmacological treatmentsthat modulate the RAAS, such as AT1R antagonists and ACE inhibitors,agents which are commonly used in heart failure patients with otheretiologies [55].
The design of this study has limitations commonly encountered inthe study of rare genetic diseases. Although this is a relatively largeand well characterized FRDA cohort the small sample size limits thestatistical power of the study to detect the small contribution of singleSNPs to the complex cardiac phenotype. This was compounded inassessing the ACE2 gene, which is X-linked, since the analysis had tobe performed in males and females separately, further reducing thecohort sizes. Ideally the study findings should be replicated in anindependent cohort, however, a suitable replication cohort withprospectively collected echocardiography data could not be found.Further, there was an absence of comprehensive clinical data in ourcontrol population. There were also limitations associated with usingM-mode echocardiography to assess left ventricular size and LVM[56]. However, while cardiac MRI is more accurate, it is not alwaysfeasible and the increased accuracy of MRI in individual subjects is lessimportant in a cohort study than in an interventional study.
5. Conclusions
In summary, rs5186, a functional AGTR1 polymorphism, had anincreased frequency in a large Australian FRDA population andshowed an association with increased SWT and LVM. This polymor-phism appears to modify the FRDA cardiac phenotype in a differentway to small FXN allele repeat length, which was associated with areduction in left ventricular chamber size in this cohort. This studysupports the potential modifying role of polymorphisms in the RAASin the development of the cardiac phenotype in FRDA patients as wellas the potential role of modulation of RAAS as a therapeutic option inFRDA patients. A greater understanding of the factors capable ofmodifying the cardiac phenotype in FRDA is likely to improve riskstratification and treatment strategies in patients with FRDA.
Disclosures
None declared.

854 M. Kelly et al. / Journal of Molecular and Cellular Cardiology 51 (2011) 848–854
References
[1] Cossee M, Schmitt M, Campuzano V, Reutenauer L, Moutou C, Mandel JL, et al.Evolution of the Friedreich's ataxia trinucleotide repeat expansion: founder effectand premutations. Proc Natl Acad Sci USA 1997 Jul 8;94(14):7452–7.
[2] Campuzano V, Montermini L, Molto MD, Pianese L, Cossee M, Cavalcanti F, et al.Friedreich's ataxia: autosomal recessive disease caused by an intronic GAA tripletrepeat expansion. Science 1996 Mar 8;271(5254):1423–7.
[3] Durr A, Cossee M, Agid Y, Campuzano V, Mignard C, Penet C, et al. Clinical andgenetic abnormalities in patients with Friedreich's ataxia. N Engl J Med 1996 Oct17;335(16):1169–75.
[4] Epplen C, Epplen JT, Frank G, Miterski B, Santos EJ, Schols L. Differential stabilityof the (GAA)n tract in the Friedreich ataxia (STM7) gene. Hum Genet 1997Jun;99(6):834–6.
[5] Wong A, Yang J, Cavadini P, Gellera C, Lonnerdal B, Taroni F, et al. The Friedreich'sataxia mutation confers cellular sensitivity to oxidant stress which is rescued bychelators of iron and calcium and inhibitors of apoptosis. Hum Mol Genet 1999Mar;8(3):425–30.
[6] Bit-Avragim N, Perrot A, Schols L, Hardt C, Kreuz FR, Zuhlke C, et al. The GAA repeatexpansion in intron 1 of the frataxin gene is related to the severity of cardiacmanifestation in patients with Friedreich's ataxia. J MolMed 2001;78(11):626–32.
[7] Dutka DP, Donnelly JE, Nihoyannopoulos P, Oakley CM, Nunez DJ. Markedvariation in the cardiomyopathy associated with Friedreich's ataxia. Heart 1999Feb;81(2):141–7.
[8] Dutka DP, Donnelly JE, Palka P, Lange A, Nunez DJ, Nihoyannopoulos P.Echocardiographic characterization of cardiomyopathy in Friedreich's ataxiawith tissue Doppler echocardiographically derived myocardial velocity gradients.Circulation 2000 Sep 12;102(11):1276–82.
[9] Isnard R, Kalotka H, Durr A, Cossee M, Schmitt M, Pousset F, et al. Correlationbetween left ventricular hypertrophy and GAA trinucleotide repeat length inFriedreich's ataxia. Circulation 1997 May 6;95(9):2247–9.
[10] Lagedrost SJ, Sutton MS, Cohen MS, Satou GM, Kaufman BD, Perlman SL, et al.Idebenone in Friedreich ataxia cardiomyopathy-results from a 6-month phase IIIstudy (IONIA). Am Heart J 2011 Mar;161(3):639–45 e1.
[11] Meyer C, Schmid G, Gorlitz S, Ernst M, Wilkens C, Wilhelms I, et al.Cardiomyopathy in Friedreich's ataxia-assessment by cardiac MRI. Mov Disord2007 Aug 15;22(11):1615–22.
[12] Mottram PM, Delatycki MB, Donelan L, Gelman JS, Corben L, Peverill RE. Earlychanges in left ventricular long-axis function in Friedreich ataxia: Relation withthe FXN gene mutation and cardiac structural change. JASE 2011;24(7):782–9.
[13] Rajagopalan B, Francis JM, Cooke F, Korlipara LV, Blamire AM, Schapira AH, et al.Analysis of the factors influencing the cardiac phenotype in Friedreich's ataxia.Mov Disord 2010 May 15;25(7):846–52.
[14] Casazza F, Morpurgo M. The varying evolution of Friedreich's ataxia cardiomy-opathy. Am J Cardiol 1996 Apr 15;77(10):895–8.
[15] Child JS, Perloff JK, Bach PM,Wolfe AD, Perlman S, Kark RA. Cardiac involvement inFriedreich's ataxia: a clinical study of 75 patients. J Am Coll Cardiol 1986 Jun;7(6):1370–8.
[16] De Michele G, Perrone F, Filla A, Mirante E, Giordano M, De Placido S, et al. Age ofonset, sex, and cardiomyopathy as predictors of disability and survival in Friedreich'sdisease: a retrospective study on 119 patients. Neurology 1996 Nov;47(5):1260–4.
[17] Hewer RL. Study of fatal cases of Friedreich's ataxia. Br Med J 1968 Sep 14;3(5619):649–52.
[18] Kelly M, Semsarian C. Multiple mutations in genetic cardiovascular disease: amarker of disease severity? Circ Cardiovasc Genet 2009;2:182–90.
[19] Filla A, De Michele G, Cavalcanti F, Pianese L, Monticelli A, Campanella G, et al. Therelationship between trinucleotide (GAA) repeat length and clinical features inFriedreich ataxia. Am J Hum Genet 1996 Sep;59(3):554–60.
[20] Monros E, Molto MD, Martinez F, Canizares J, Blanca J, Vilchez JJ, et al. Phenotypecorrelation and intergenerational dynamics of the Friedreich ataxia GAAtrinucleotide repeat. Am J Hum Genet 1997 Jul;61(1):101–10.
[21] Lamont PJ, Davis MB, Wood NW. Identification and sizing of the GAA trinucleotiderepeat expansion of Friedreich's ataxia in 56 patients. Clinical and geneticcorrelates. Brain 1997 Apr;120(Pt 4):673–80.
[22] Montermini L, Richter A, Morgan K, Justice CM, Julien D, Castellotti B, et al.Phenotypic variability in Friedreich ataxia: role of the associated GAA tripletrepeat expansion. Ann Neurol 1997 May;41(5):675–82.
[23] Paul M, Poyan Mehr A, Kreutz R. Physiology of local renin–angiotensin systems.Physiol Rev 2006 Jul;86(3):747–803.
[24] Marian AJ. Modifier genes for hypertrophic cardiomyopathy. Curr Opin Cardiol2002 May;17(3):242–52.
[25] Burrell LM, Johnston CI, Tikellis C, Cooper ME. ACE2, a new regulator of the renin–angiotensin system. Trends Endocrinol Metab 2004 May-Jun;15(4):166–9.
[26] Kaufman BD, Auerbach S, Reddy S, Manlhiot C, Deng L, Prakash A, et al. RAAS genepolymorphisms influence progression of pediatric hypertrophic cardiomyopathy.Hum Genet 2007 Dec;122(5):515–23.
[27] Ortlepp JR, Vosberg HP, Reith S, Ohme F, Mahon NG, Schroder D, et al. Geneticpolymorphisms in the renin–angiotensin–aldosterone system associated withexpression of left ventricular hypertrophy in hypertrophic cardiomyopathy: astudy of five polymorphic genes in a family with a disease causing mutation in themyosin binding protein C gene. Heart 2002 Mar;87(3):270–5.
[28] Perkins MJ, Van Driest SL, Ellsworth EG, Will ML, Gersh BJ, Ommen SR, et al. Gene-specific modifying effects of pro-LVH polymorphisms involving the renin–angiotensin–aldosterone system among 389 unrelated patients with hypertrophiccardiomyopathy. Eur Heart J 2005 Nov;26(22):2457–62.
[29] Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al.Recommendations for chamber quantification: a report from the AmericanSociety of Echocardiography's Guidelines and Standards Committee and theChamber Quantification Writing Group, developed in conjunction with theEuropean Association of Echocardiography, a branch of the European Society ofCardiology. J Am Soc Echocardiogr 2005 Dec;18(12):1440–63.
[30] Sahn DJ, DeMaria A, Kisslo J, Weyman A. Recommendations regarding quantita-tion in M-mode echocardiography: results of a survey of echocardiographicmeasurements. Circulation 1978 Dec;58(6):1072–83.
[31] Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, et al.Echocardiographic assessment of left ventricular hypertrophy: comparison tonecropsy findings. Am J Cardiol 1986 Feb 15;57(6):450–8.
[32] Chiu C, Tebo M, Ingles J, Yeates L, Arthur JW, Lind JM, et al. Genetic screening ofcalcium regulation genes in familial hypertrophic cardiomyopathy. J Mol CellCardiol 2007 Sep;43(3):337–43.
[33] Delatycki MB, Paris DB, Gardner RJ, Nicholson GA, Nassif N, Storey E, et al. Clinicaland genetic study of Friedreich ataxia in an Australian population. Am JMed Genet1999 Nov 19;87(2):168–74.
[34] The International HapMap Project. Nature 2003 Dec 18;426(6968):789–96.[35] Barrett JC, Fry B, Maller J, Daly MJ. Haploview: analysis and visualization of LD and
haplotype maps. Bioinformatics 2005 Jan 15;21(2):263–5.[36] de Bakker PI, Yelensky R, Pe'er I, Gabriel SB, Daly MJ, Altshuler D. Efficiency and
power in genetic association studies. Nat Genet 2005 Nov;37(11):1217–23.[37] Cameron VA, Mocatta TJ, Pilbrow AP, Frampton CM, Troughton RW, Richards AM,
et al. Angiotensin type-1 receptor A1166C gene polymorphism correlates withoxidative stress levels in human heart failure. Hypertension 2006 Jun;47(6):1155–61.
[38] Nalogowska-Glosnicka K, Lacka BI, Zychma MJ, Grzeszczak W, Zukowska-Szczechowska E, Poreba R, et al. Angiotensin II type 1 receptor gene A1166Cpolymorphism is associated with the increased risk of pregnancy-inducedhypertension. Med Sci Monit 2000 May-Jun;6(3):523–9.
[39] OsteropAP, KofflardMJ, Sandkuijl LA, ten Cate FJ, KramsR, SchalekampMA, et al. AT1receptorA/C1166 polymorphism contributes to cardiac hypertrophy in subjectswithhypertrophic cardiomyopathy. Hypertension 1998 Nov;32(5):825–30.
[40] Tiret L, Bonnardeaux A, Poirier O, Ricard S, Marques-Vidal P, Evans A, et al.Synergistic effects of angiotensin-converting enzyme and angiotensin-II type 1receptor gene polymorphisms on risk of myocardial infarction. Lancet 1994 Oct1;344(8927):910–3.
[41] Wang WY, Zee RY, Morris BJ. Association of angiotensin II type 1 receptor genepolymorphism with essential hypertension. Clin Genet 1997 Jan;51(1):31–4.
[42] Wu CK, Tsai CT, Chang YC, Luo JL,Wang YC, Hwang JJ, et al. Genetic polymorphismsof the angiotensin II type 1 receptor gene and diastolic heart failure. J Hypertens2009 Mar;27(3):502–7.
[43] Doolan G, Nguyen L, Chung J, Ingles J, Semsarian C. Progression of left ventricularhypertrophy and the angiotensin-converting enzyme gene polymorphism inhypertrophic cardiomyopathy. Int J Cardiol 2004 Aug;96(2):157–63.
[44] Hammond IW, Devereux RB, Alderman MH, Laragh JH. Relation of blood pressureand body build to left ventricular mass in normotensive and hypertensiveemployed adults. J Am Coll Cardiol 1988 Oct;12(4):996–1004.
[45] Lorenz CH,Walker ES, Morgan VL, Klein SS, Graham Jr TP. Normal human right andleft ventricular mass, systolic function, and gender differences by cine magneticresonance imaging. J Cardiovasc Magn Reson 1999;1(1):7–21.
[46] Nicodemus KK, Liu W, Chase GA, Tsai YY, Fallin MD. Comparison of type I errorfor multiple test corrections in large single-nucleotide polymorphism studiesusing principal components versus haplotype blocking algorithms. BMC Genet2005;6(Suppl 1):S78.
[47] Gabriel SB, Schaffner SF, Nguyen H, Moore JM, Roy J, Blumenstiel B, et al. Thestructure of haplotype blocks in the human genome. Science 2002 Jun21;296(5576):2225–9.
[48] Ganau A, Devereux RB, Roman MJ, de Simone G, Pickering TG, Saba PS, et al.Patterns of left ventricular hypertrophy and geometric remodeling in essentialhypertension. J Am Coll Cardiol 1992 Jun;19(7):1550–8.
[49] Delatycki MB, Williamson R, Forrest SM. Friedreich ataxia: an overview. J MedGenet 2000 Jan;37(1):1–8.
[50] Martin MM, Buckenberger JA, Jiang J, Malana GE, Nuovo GJ, Chotani M, et al. Thehuman angiotensin II type 1 receptor +1166 A/C polymorphism attenuatesmicrorna-155 binding. J Biol Chem 2007 Aug 17;282(33):24262–9.
[51] Sethupathy P, Borel C, Gagnebin M, Grant GR, Deutsch S, Elton TS, et al. HumanmicroRNA-155 on chromosome 21 differentially interacts with its polymorphictarget in the AGTR1 3′ untranslated region: a mechanism for functional single-nucleotide polymorphisms related to phenotypes. Am J Hum Genet 2007Aug;81(2):405–13.
[52] McEwan PE, Gray GA, Sherry L, Webb DJ, Kenyon CJ. Differential effects ofangiotensin II on cardiac cell proliferation and intramyocardial perivascularfibrosis in vivo. Circulation 1998 Dec 15;98(24):2765–73.
[53] Ramires FJ, Sun Y, Weber KT. Myocardial fibrosis associated with aldosterone orangiotensin II administration: attenuation by calcium channel blockade. J Mol CellCardiol 1998 Mar;30(3):475–83.
[54] Delatycki MB. Evaluating the progression of Friedreich ataxia and its treatment.J Neurol 2009 Mar;256(Suppl 1):36–41.
[55] Schulz JB, Boesch S, Burk K, Durr A, Giunti P, Mariotti C, et al. Diagnosis andtreatment of Friedreich ataxia: a European perspective. Nat Rev Neurol 2009Apr;5(4):222–34.
[56] Myerson SG, Montgomery HE, World MJ, Pennell DJ. Left ventricular mass:reliability of M-mode and 2-dimensional echocardiographic formulas. Hyperten-sion 2002 Nov;40(5):673–8.