a preliminary report on the treatment of kala-azar with ... filea preliminary report on the treat-...
TRANSCRIPT

A PRELIMINARY REPORT ON THE TREAT- MENT OF K ALA-AZAR WITH INTRAVENOUS
INJECTION OF METALLIC ANTIMONY. ^ 13Y Rai U. N. BRAHMAOHARI BAHADUR, MA, M.D,
Ph.D.,
Teacher of Medicine, Campbell Medical School, Calcutta.
The use of metallic antimony in a state of
finest sub-division in the treatment of kala-azar has not been noted by any previous observer. In a disease like kala-azar in which the parasites reside in such organs as the spleen and the bone marrow and in which very few parasites are found in the peripheral circulation, the use of the
soluble salts of antimony may be followed by such quick elimination of the drug that it may be excreted before exerting any marked influence on the parasites in the spleen and the bone
marrow. In the treatment of the allied disease of trypanosomiasis by intravenous injection of
tartar emetic or other soluble salts of antimony, it has been found that though they quickly free the peripheral blood from trypanosomes, still the parasites remain in the internal organs. So far,
therefore, the treatment of trypanosomiasis by means of intravenous injection of soluble salts of antimony has not been a permanent success. In kala-azar, in which the parasites live mostly in the internal organs, the same line of treatment may, from these theoretical considerations, be not expected to do much good. However, the treatment of kala-azar with tartar emetic and other soluble salts of antimony will form the subject of a future communication, though it may be remarked here, in passing, that good results with tartar emetic have been recently reported by several observers. The present paper is a prelimi- nary report, but the results obtained so far certainly justify further investigations. The method of administration is the author's
own and is described as follows :? An all-glass 10 cc. syringe is fitted with a three-
way stop-cock, the remaining two ends of which are fitted to a platinum needle and a rubber tubing attached to the nozzle of a piece of glass tube respectively. A stout hypodermic needle with a specially constructed blunt canula inside may be used in place of an ordinary one. This canula when pushed through the needle will prevent the puncture of the vein a second time during the process of injection of the metallic antimony, (see Figure). One grain of metallic antimony is made into a thoroughly homogeneous paste with sufficient liquid glucose in a glass mortar and then mixed with 20 cc. normal saline. (The glucose added is just sufficient to make a 5 per cent, solution with the 20 cc. normal saline.) The stop-cock is so arranged that the syringe
may be made to communicate alternately with the needle or the glass tube by turning the stop-cock. Half the suspension is now sucked into the glass syringe, and after being freed from any bubbles of air, it is injected into a vein of the forearm. The glass tube is now filled with a portion of the remaining suspension, which is sucked into the glass syringe after freeing the rubber tubing of any air bubbles, and then the suspension is again injected. In this way the whole of the suspension is injected into the vein. Any sediment of antimony left inside the syringe is subsequently mixed with normal saline contain- ing 5 per cent, glucose, and then injected into the vein. This process is repeated several times till no antimony is left inside the syringe. About 40 to 45 cc. of normal saline is required to inject 1 ^ 1| grs. of metallic antimony. In all the cases recorded below, the diagnosis was made by the presence of Leishman-Donovan bodies in the splenic blood. The first two cases were at first treated with
tartar emetic and Plimmer's salt (Antimonyl Sodae Tartars). Then after some days they were treated with intravenous injection of metallic antimony.
456 THE INDIAN MEDICAL GAZETTE. [Dec., 1916.
Case No. 4 was treated with intravenous injec- tion of metallic antimony and electargol. This
patient had marked jaundice with oedema of the
extremities, and there was a very large amount of albumen in the urine. These have completely disappeared during treatment. Case No. 5 had ccincrum oris on admission. This has disappear- ed after treatment.
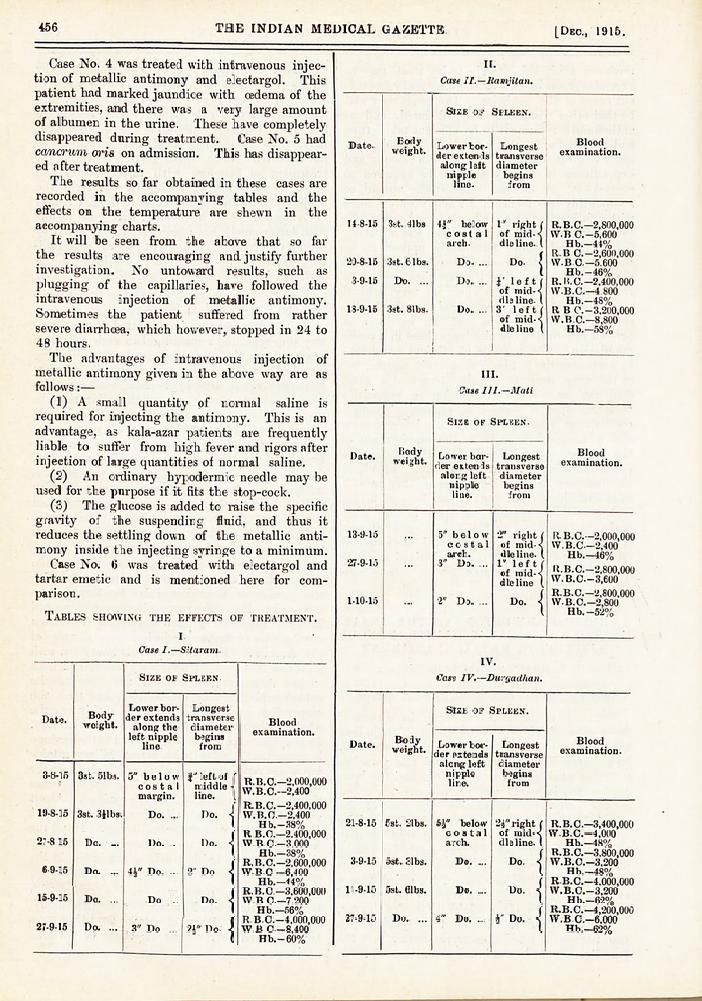
The results so far obtained in these cases are
recorded in the accompanying tables and the
effects on the temperature are shewn in the
accompanying charts. It will be seen from the above that so far
the results are encouraging and justify further investigation. No untoward results, such as
plugging of the capillaries, have followed the
intravenous injection of metallic antimony. Sometimes the patient suffered from rather
severe diarrhoea, which however, stopped in 24 to 48 hours. The advantages of intravenous injection of
metallic antimony given in the above way are as
follows:?
(1) A small quantity of normal saline is
required for injecting the antimony. This is an
advantage, as kala-azar patients are frequently liable to suffer from high fever and rigors after
injection of large quantities of normal saline.
(2) An ordinary hypodermic needle may be used for the purpose if it fits the stop-cock.
(3) The glucose is added to raise the specific gravity of the suspending fluid, and thus it
reduces the settling down of the metallic anti-
mony inside the injecting syringe to a minimum. Case No. 6 was treated with electargol and
tartar emetic and is mentioned here for com-
parison.
Tables showing the effects of treatment.
i
Case I.?Silaram.
Date.
3-8-15
19-8-15
27-8 15
69-15
15-9-15
27-9-15
Body weight.
3st. 51bs.
3st. 3$lbs.
Do. ...
Do. ...
Do. ...
Do. ...
Size of Spleen.
Lower bor- der extends along the
left nipple line
5" below costal
margin.
Do. ...
Do. .
ih" Do. ...
Do ..
3" Do ...
Longest transverse diameter
begins from
rleft of r middle -! line. I
?{ ?{
{ {
? Do. |
I)o,
Do
2" Do
Do
Blood examination.
R.B.C.?2,000,000 W.B.C.?2,400
R.B.C.?2,400,000 \V. B.C.?2,400
H b.?38% U B.C.?2.400,000 W.BC?3.000
Hb.?38% R. B.C.?2,600,000 YV.B.C ?6,400
Hb.?<4% R.B.C ?3,600,000 W B C?7.200
Hb.?56% R.BC.?4,000,000 W.B C?8,400
Hb.?60%
II.
Case II.?Ramjitan.
Date- Body weight.
Size of Spleen.
Lower bor- der extends
along left nipple line-
Longest Bi ??i transverse examination.
diameter begins from
14-8-15
20-8-15
3-9-15
18-9-15
3st. 41bs
3st. 6 lbs.
Do. ...
3st. 81bs.
4J" below costal arch.
Do. ...
Do. ...
Do. ...
1" right of mid- dle line.
? left of mid- dle line- s' left of mid-' die line
?ht (
?.1 (
\ it i
Si
R. B.C.?2,800.000 VV.B C.-5,600
Hb.?44% R.B C.-2,600.000 W.BC.?5.600
Hb. ?46% R.K C.?2,400,000 W.B.C.?4 800
Hb.?48% R B C.-3,200,000 W.B.C.?8,800
Hb.?58%
III.
Case 111.?Mali
Date. Body weight.
Size of Spleen-
Lower bor- der extends
along left nipple line.
Longest transverse diameter
begins from
Blood examination.
13-9-15
27-9-15
1-10-15
5" below costal arch.
3" Do. ...
2" Do. ...
2" right of m die line 1" left of mid- dle line
ight ( nid- < ine. (.
Do.
R- B.C.?2,000,000 W. B.C?2,400
Hb.?46% R. B.C.?2,800,000 W. B.C.?3,600
R.B.C.?2,800,000 W. B.C. ?2,800
Hb. ?52%
IV.
Case IV.?Durgadhan.
Date. Body weight.
Size of Spleen.
Lower bor- der extends
along left nipple line.
Longest transverse diameter begins from
Blood examination.
21-8-15
3-9-15
11-9-15
27-9-15
5st. 2tbs.
5st. 31bs.
5st. 61bs.
Do. ...
5g" below costal arch.
Do. ...
Do. ...
4" Do. ...
2i" right ( of mid-< die line. (
Do
Do
h" Do.
{ ?{
{
R. B.C.?3,400,000 YV.B.C.?4,000
Hb.?48% R. B.C.?3,800,000 VV. B.C.?3,200
Hb.?48% R B.C.?4,000,000 W.B.C.?3,200
Hb.?62% R.B.C.?4,200,000 W.BC.?6,000
Hb.?62%

TREATMENT OF KALA-AZAR WITH INTRAVENOUS INJECTION OF METALLIC ANTIMONY. By Rai U. N. BRAHMACHARI BAHADUR, m.a., m.d., Ph.D.,
Teacher of Medicine, Campbell Medical School, Calcutta.
CASE I. CASE I.
CASE II. CASE II.

TREATMENT OF KALA-AZAR WITH INTRAVENOUS INJECTION
OF METALLIC ANTIMONY.
By Rai U. N. BRAHMACHARI BAHADUR, h.a,, m.d., ph.D?
Teacher of Medicine, Campbell Medical School, Calcutta.
i. Lii
Apparatus for intravenous injection of Metallic Antimony. Apparatus for intravenous injection of Metallic Antimony.

TREATMENT OF KALA-AZAR WITH INTRAVENOUS INJECTION OF METALLIC ANTIMONY. Br Rai U. N. BRAHMACHARI BAHADUR, m.a., m.d., Ph.D.,
Teacher of Medicine, Campbell Medical School, Calcutta. CASE III. CASE III.
CASE IV. CASE IV.

TREATMENT OF KALA-AZAR WITH INTRAVENOUS INJECTION OF
METALLIC ANTIMONY.
By Rai U. N. BRAHMACHARI BAHADUR, m.a., m.d., Ph.D.,
Teacher of Medicine, Campbell Medical School, Calcutta.
DATE
TEMPERATURE
Cent. Fahr.
IJH3 15
m.e
13-9
15
M.E
CASE V.
14-9 15-9 16-9 17-9 I8J3 I9jj> 2CH3 2Jh9 22^9 23;9 2?9 25j9 26-9|27-9 IeF 15 15 15 15 15 15 15 lb 15 15 15 19 15
M.E M.E M.E M.E M.E M.E M.E M.E M.E M.E M.E M.E M.E M.E
41 106
>05
40 IO 4
103
39 102
10!
38
37
97
Pulse.
r??p- fe Bowels. ;
-JN ft 7^1 ? | ?
CASE V.
CASE VI. CASE VI.

Dec., 1915.J CLINICAL NOTES ON KALA-AZAR. 457
V.
Case V.?Kubi
Date.
18 9-15
27-9 15
Body weight.
Size of Spleen. examination.
a i * u -?.f (\ R.B.C.-2,400,000 Spleen felt just be- J , W R C-_4 800 low costal arch )j Hb.-50%
Spleen cannot be f felt below costals arch. I
R.B.C.?2,800,000 \V. B.C.?5,600
Hb.?52%
VI.
Case VI ?Narayan.
Date. Body weight.
Size of Spleen.
Lower bor- der extends along left nipple line.
4-9 15 1st. Gibs. 5-' below costal arch.
11-9-15 j ... ! AV Do. ...
18-9-15 1st. 4?lbs
2-10-15 Do. ...
4" Do.
Do.
Longest transverse diameter begins from
left of ( middles line. (.
Blood examination.
U" Do.
2' Do.
Do.
R.B. 0.-2,800,000 VV.B.C.?1,600
Hb.?46% 11. B.C.?2,600,000 VV. B.C.?4,400
Hb.?50% It B.C.?2,600,000 W.B.C.?4,000
Hb.?54% ;R B.C.?3,800,000 W.B C.-6.400
Hb. ?70%
N.B.? This case was treated with electargol and tartar emetic.