a prospective randomized controlled study to assess …
TRANSCRIPT

A PROSPECTIVE RANDOMIZED CONTROLLED
STUDY TO ASSESS THE EFFICIENCY OF ACTIVE
SELF LIGATING BRACKET SYSTEM Vs
CONVENTIONAL BRACKET SYSTEM.
Dissertation submitted to
THE TAMIL NADU Dr. M.G.R.MEDICAL UNIVERSITY
In partial fulfillment for the degree of
MASTER OF DENTAL SURGERY
BRANCH V
ORTHODONTICS AND DENTOFACIAL ORTHOPEDICS
APRIL-2016





ACKNOWLEDGEMENT
For days I had created a script in my head for this section. I really
could not wait to start writing this page, precisely because it marks the end of
my dissertation but, now I am at my wits end. None the less, I believe this is a
good time as any to show my deep sense of gratitude to the people who matter
the most to me.
I am forever indebted and owe my gratitude to my beloved mentor and
guide, Prof. Dr. N.R. Krishnaswamy, M.D.S, M.Ortho (RCS,Edin)
,D.N.B.(Ortho), Diplomate of Indian Board of Orthodontics, Professor and
Head of Department of Orthodontics, Ragas Dental College and Hospital,
Chennai for his immense patience, guidance and the support that he lent me
during this study. He has always been an epitome of perfection and has
encouraged me in many ways throughout the duration of the course to become
a better person and doctor. I am truly blessed to have spent time under his
tutelage.
I am highly grateful to Prof. Dr. M.K. Anand, M.D.S, for always
leading me to the correct direction and helping me to look for answers to my
never ending questions. I thank him for his unconditional support.
I would like to thank Dr. Kavitha, M.D.S (Sr. Lecturer) for her
profound interest, wise counsel and never ending willingness to render
generous help to me in giving this work a proper shape.

I would also like to sincerely acknowledge Dr. Shahul (Professor),
Dr. JayaKumar (Professor), Dr. Sriram (Professor), Dr. Shakeel (Reader),
Dr. Rekha (Reader), Dr. Shobana (Reader), Dr.Arathi (Sr.Lecturer),
Dr.Sraboni (Sr. Lecturer) and Dr. Rachel (Sr. Lecturer) for their support and
professional assistance throughout my post graduate course.
My sincere thanks to Prof. Mr. Kanakraj, Chairman &
Dr. S. Ramachandran, Principal, Ragas Dental College for providing me with
an opportunity to utilize the facilities available in this institution in order to
conduct this study.
My heartfelt thanks to my wonderful batchmates, Dr. Arpitha, Dr.Ravi
Teja, Dr. Diwakar, Dr. Mahalaxmi, Dr. Revathi, Dr. Sharanya,
Dr. Anushya, who were cheerfully available at all times to help me. Their
support and friendship helped me these past few years and I deeply appreciate
it.
I would also like to extend my gratitude to my juniors, Dr. Preethi R,
Dr. Preethi G, Dr. Evan, Dr. VeeraShankar, Dr. Rajesh, Dr. Vidhu, Dr.
Vineesha, Dr. Dhanalakshmi, Dr. Rishi, Dr. Swati, Dr. Aparna, Dr. Charles,
Dr. Harish, Dr. Sam, Dr. Gopi, Dr. Mathew for their support and cooperating
with me to conduct this study on their patients.

I would like to thank Mr. Ashok for helping me with the technical
work and Mr. Bhaskar, Sister Lakshmi, Sister Deviyani, Sister Kanaka,
Mrs. Ameena for their co-operation and help during my course of study.
I am blessed to have got this opportunity to thank my sister Ms Ahana
Ganguly for being my pillar of strength and always having my back and
protecting me from all the troubles I keep falling into. I am forever indebted to
her for being my comfort zone. Special thanks to my brother Mr. Sreyon
Chatterjee for his timely advise and help with all the technical support that I
needed.
Life is incomplete without the presence of true friends, they show you
the spark when the days turn gloomy and dull. I thank all my friends,
especially, Dr. Ashita Talwar, Dr. Megha Bhola, Dr. Anuj Kumar, Dr.
Deepak Singh, Ms. Shreyashi Das and Ms. Suparna Biswas for their
unwavering trust and whole hearted support in all my endeavors throughout
my life.
I dedicate this study to my father Dr. Syamal Ganguly, for his
unending trust and faith in my work and to my mother Prof. Dr. Urmi
Ganguly, for her constant encouragement and always standing by me. Words
cannot express my gratitude to my grandmother Mai, who always believed
that its never too late to fulfill our dreams. I am extremely blessed to have had
all these beautiful people in my life and I thank thee Almighty for it.

CONTENTS
S .No. TITLE PAGE NO.
1. INTRODUCTION 1
2. REVIEW OF LITERATURE 6
3. MATERIALS & METHODS 38
4. RESULTS 39
5. DISCUSSION 43
6. SUMMARY & CONCLUSION 60
7. BIBLIOGRAPHY 62
8. ANNEXURE -

Introduction

Introduction
1
INTRODUCTION
The systematic evolution of various dental materials has led to a
constant pursuit of technological advances in the field of orthodontics.
Appliance biocompatibility, treatment time and efficiency and patient
acceptance are the major confronting factors for the success of orthodontic
treatment.35
The first phase of fixed appliance orthodontic treatment is concerned
with tooth alignment, but the effectiveness of this process is dependent on
several variables. Clearly, the underlying tissue biology will play a major
significant role in the response of the periodontium to the applied orthodontic
force that provides the fundamental mechanism which allows tooth movement
through the alveolar bone.51
Although the biologic factors are largely beyond the control of the
orthodontist, more direct influence is possible achievable with the choice of
bracket system and arch wire.
When using pre adjusted edgewise brackets, important factors that
determine the rate of tooth alignment includes the bracket slot dimension, the
associated inter bracket span,51 and the choice of archwire.19,32,51
Frictional forces generated between bracket and arch wire also have a
significant effect on tooth movement.4 Friction is influenced by the physical
Introduction
2
characteristics of the archwire and bracket material, and the method of
attachment between arch wire and bracket slot.31,12
Conventionally ligated edgewise brackets incur increased levels of
frictional resistance via the elastomeric attachment between bracket and
archwire.6,7,26 To reduce unwanted friction, various types of self-ligating
bracket systems have been developed. Therefore, any appliance system that
can increase the rate of tooth alignment is a potential clinical advancement.
It has been more than 70 years since Dr. Jacob Stolzenberg described a
self-ligating edgewise bracket and the recent proliferation of various bracket
types represents a minority of the versions that have been patented since that
time.26
Proposed limitations of conventional ligating brackets include
higher frictional values, failure to maintain full arch wire engagement, force
decay of elastics, impeded oral hygiene and time consuming clinical
procedures.19
Self ligating brackets claim to overcome these drawbacks by providing
a more certain full arch wire engagement, reduced friction between bracket
and arch wire, with faster arch wire removal and ligation and lesser chair side
time.19 Reduced friction between arch wire and self ligating bracket
have been quoted by numerous authors compared with conventional

Introduction
3
brackets.51,19 Anchorage conservation with self ligating brackets is mainly due
to lower forces per unit area applied.32
Self ligating brackets have a mechanical built in device into the bracket
to close off the bracket slot. They offer better patient acceptance than steel
wire ligatures. The precision arm or the sliding fourth wall accurately locks
the archwire within the dimensions of the bracket slot ensuring complete
archwire engagement and controlled tooth movement.
Self ligating brackets (SLB) are broadly classified into Passive, Active
and Interactive and Self –ligating brackets. Active brackets, with the labial
fourth wall consists of a spring clip which is in contact with the arch wire.
These brackets express greater torque control. In the Active SLB system,
friction is produced as a result of the clip pressing against the archwire.19 In
passive SLB system, the slot is transformed into a tube by means of the labial
fourth wall that does not come into contact with the archwire. However, the
term “passive” is somewhat of a misnomer because it is passive only when
teeth are ideally aligned in 3 dimensions (torque, angulation, and in-out), and
an undersized wire would not touch the walls of the bracket slot.8
In Interactive bracket system, the clip is passive with the initial lower
dimensional wires and as the dimension of the arch wire increases the clip
actively engages the arch wire and express greater torque control, which is
required in the retraction and finishing stages of treatment.4

Introduction
4
Examples of active bracket is, SPEED (Strite Industries, Cambridge,
Ontario, Canada). Examples in the passive group are the Damon bracket
(Ormco.Glendora, Calif) and the SmartClip bracket (3M Unitek, Monrovia,
Calif).5 The In-Ovation “R” (GAC International, Bohemia, NY) and Time
(American Orthodontics, Sheboygan, Wis) are the SL systems which claim to
be interactive, but, as per Kusy31 all bracket systems—conventional, and SL
active and passive are interactive to some degree, meaning that the wire
probably touches some aspect of the bracket throughout treatment.
Bracket manufactures promote patient comfort as an advantage of self
ligating brackets in spite of the lack of concurrence in scientific literature;
more constant pain for conventional ligation.12
It has been also proposed that some self-ligating appliances might
increase the inter molar widths.6,7 The available evidence on the efficiency of
self-ligating brackets derives from a limited number of prospective and
randomized clinical trials; some have indicated differences in final molar
widths, and some have shown no differences between self-ligating and
conventional appliances.
Recently a concept termed as Dual activation system has been
introduced wherein, the anterior SLB are active in configuration and the
posterior brackets are passive in configuration.

Introduction
5
To the best of our knowledge, no previous in vivo studies have
compared the alignment efficiency and the arch dimensional changes with use
the of Dual activation self ligating bracket concept.
Thus, the purpose of this study was to compare the alignment
efficiency, the transverse arch dimensional changes and the torque expression
between Dual activation self ligating bracket system and Conventional bracket
system.

Review of Literature

Review of literature
6
REVIEW OF LITERATURE
Jacob Stolzenburg (1935),26 first introduced self ligating bracket
system and described the features of Russell Lock attachment which are
generally smoother for the patients as there are no steel ligatures present for
archwire engagement. The precision arm or the fourth sliding wall completely
secures the arch wire within the dimensions of the slot providing robust
ligation mechanism and controlled tooth movement.
Tweed (1943)65 in his philosophy of orthodontic treatment said that the
main goal is to preserve the anchorage, right from the start of the treatment
and to prevent the major reciprocal reaction that occurs during retraction stage.
Shivapuja (1994)52 in his comparative study on the effect of self
ligation bracket and conventional bracket ligation system found that the self
ligation system displayed a significantly lower level of frictional resistance,
less chairside time and improved infection control compared to ceramic or
metal brackets.
Tselepis M, West VC, Brockhurst P (1994)60 Compared the dynamic
frictional resistance between orthodontic bracket system and arch wires, arch
wire material, bracket material, bracket to arch wire angulation and
lubrication. The frictional force levels involved in sliding a ligated arch wire
through a bracket slot was measured with an universal testing machine. Of the
four factors investigated by him, all were found to have significant influence

Review of literature
7
on friction. The polycarbonate brackets showed the highest friction and the
stainless steel brackets showed the least. Friction is increased with the bracket
to arch wire angulation. Saliva lubrication reduced the friction significantly. A
range of 0.9-6.8 N frictional force levels were recorded. The actual force
values recorded were most useful for comparing the relative influence of the
factors tested for friction, rather than a quantitative assessment of friction in
vivo. The force levels observed suggest that friction maybe a significant
influence on the amount of applied force required to move a tooth in the
mouth.
Dwight H Damon (1998)10 compared the friction produced by three
types of conventional twin brackets with three self ligating brackets. When a
0.019 x 0.025 inch stainless steel wire were drawn through the bracket, a
conventional twin ligated bracket system with elastic modules produced 388 to
609 times the friction of passive self ligated brackets produced. Conventional
twins with metal ligatures had friction values more than 300 times compared
to the passive self ligating brackets. The active brackets produced 216 times
the friction of a passive self-ligating bracket.
Luca Pizzoni et al (1998)33 studied the frictional resistance
encountered in two self ligating bracket systems (Speed, Damon SL) and two
conventional brackets (Dentauram). These brackets were tested with four
wires (Stainless steel, Beta titanium-round and rectangular). The result showed
that round wires had a lower friction than rectangular wires. Beta titanium had

Review of literature
8
higher friction than stainless steel. The self ligating brackets had markedly
lower friction than conventional brackets at all angulations. It was concluded
that the selection of bracket design, wire material and wire cross section
significantly influences the forces acting in a continuous arch system.
Kapur et al (1998)29 conducted a study to compare the kinetic
frictional force of a new self ligating bracket (Damon SL) with that of a
conventional bracket. The results he revealed were that the self ligating
brackets had lower kinetic friction coefficient. They concluded that self
ligating brackets could offer a substantial clinical advantage to orthodontists
employing sliding mechanics.
Profit and Fields (2000)48 discussed the methods of anchorage
control. The extent to which anchorage should be reinforced depends on the
tooth movement that is desired. For significant differential tooth movement,
the ratio of periodontal ligament area in the anchorage unit to periodontal
ligament area in the tooth movement unit should be at least 2 to 1 without
friction, 4 to 1 with friction. Anything less produces something close to
reciprocal movement. A common way to improve the anchorage control is to
pit resistance of a group of teeth against the movement of a single tooth, rather
than dividing the arch into more or less equal segments. For all four extraction
cases with maximum anchorage consideration the three possible approaches
for space closure are:

Review of literature
9
1. One step closure with friction less appliance
2. A two step closure sliding the canine along the arch wire, then
retracting the incisors( like original Tweed technique)
3. Two step closure, tipping the anterior segment with some friction,
the uprighting the tipped teeth ( as in Begg technique)
Mc Laughin, Bennet and Trevisi (2001)36 discussed about the play of
the archwire placed in the bracket slot. When an undersized wire is placed in a
0.022” slot that is using a 0.019 x 0.025 inch wire as the final dimension wire
there will be slop or play of 10 degree between the slot and arch wire.
Harradine (2003)20 reported that currently available self ligating
brackets offer the valuable combination of low friction and secure full bracket
engagement. These developments offer the possibility of a significant
reduction in average treatment times and also in anchorage requirements,
particularly in cases requiring large tooth movements.
Srinivas (2003)53 has demonstrated that passive self-ligating
appliances use less anchorage than conventional appliances. This supports the
reduction in the use of anchorage devices experienced by users of passive self-
ligation. Use of intraoral expansion auxiliaries such as quad helixes or W-
springs because the force of the archwire is not transformed or absorbed by the
ligatures and the necessary expansion can be achieved by the force of the
archwires. Need for extractions to facilitate orthodontic mechanics because
alignment is not hindered by frictional resistance from ligatures and can

Review of literature
10
therefore be largely achieved with small diameter copper nickel titanium
archwires. Tooth alignment therefore places minimal stress on the
periodontium as it occurs and so the possibility of iatrogenic damage to the
periodontium is reduced. In addition, a passive edgewise self-ligation system
provides three key features:
Very low levels of static and dynamic friction
Rigid ligation due to the positive closure of the slot by the gate or slide
Control of tooth position because there is an edgewise slot of adequate
width and depth.
Miles P. G et al (2006)38 compared the effectiveness and comfort of
Damon 2 brackets and conventional twin brackets during initial alignment.
Comfort on the lips, more esthetic look, and bracket failure rates were also
recorded. The twin bracket was more uncomfortable with the initial arch wire.
However, at 10 weeks, substantially more patients reported discomfort with
the Damon 2 bracket when engaging the arch wire. Patients preferred the look
of twin bracket over the Damon 2 and more SLB debonded during the study.
He concluded that Damon 2 brackets was no better during initial alignment
than a conventional bracket.
Turnbull. N.R, David J Birne,(2007)62 in their prospective clinical
study, authors assessed the relative speed of arch wire changes in a patient,
comparing self ligating brackets with conventional elastomeric ligation
methods, and further assessed this in relation to the stage of orthodontic

Review of literature
11
treatment represented by different wire sizes and types. The time taken to
remove and ligate arch wires for 131 consecutive patients treated with either
self ligating or conventional brackets was prospectively assessed. The main
outcome measure was the time to remove or place elastomeric ligatures or
open/close self ligating for two matched groups of fixed appliance patients:
Damon 2 SLB and a conventional mini twin bracket. The relative effects of
various wire sizes and materials on ligation times were investigated. The study
was carried out by one operator. Authors found that ligation of an arch wire
was approximately twice as quick with self ligating brackets. Opening a
Damon slide was on average 1 second quicker per bracket than removing
elastic modules from the mini twin brackets, and closing a slide was 2 seconds
faster per bracket. This difference in ligation time became more marked for
larger wire sizes used in later treatment stages.
Pandis. N and Argy Polychronopoulou (2007)45 investigated the
duration of mandibular crowding alleviation with self ligating brackets
(Damon 2) compared with the conventional appliances (Microarch) and the
accompanying dental effects. Fifty four subjects were selected from a pool of
patients. Lateral cephalometric radiographs were used to assess the alteration
of mandibular incisor position before and after alignment. He concluded that
overall, no difference in the time required to correct mandibular crowding with
Damon 2 and conventional brackets was observed because in conventional
cases the stress exerted by the elastomeric modules and wire ligature adjacent

Review of literature
12
to the bracket sides, precluding free sliding of the wire into the slot walls and
adversely affecting movement rate. When the crowding and space in the arch
increases there is no difference found between the systems.
Daniel Rinchusea and Peter G Miles (2007)8 elucidated that the
ligation force is not transmitted to the tooth but is counteracted by the equal
and opposite force of the self ligating brackets against the arch wire. A module
exerting 50g force pulling the wire into the base of the slot is the load or
normal force, so it is pertinent in friction when sliding but does not place a
direct force on the tooth. The deflection of the arch wire exerts the force on the
tooth. Friction, which impedes the sliding movements is determined by
multiplying the coefficient of friction of the materials in contact by the normal
force, which is the force of ligation. Therefore, friction is directly proportional
to the force of ligation. The force applied to the tooth comes from the
deflection of the arch wire, so if the module does not deflect the arch wire,
then it is passive and no force is applied to the tooth. This normal force is
avoided by using a Damon or a Smart Clip bracket or passive ligation only
when the brackets and wire are ideally aligned. Any deflection of the arch wire
that engages the bracket due to rotation, tip or torque creates a normal force
and therefore classical friction. If this deflection is greater, eventually binding
and notching occur; these event cannot be avoided by any bracket design
whatsoever. So, a possible SLB in future could be a combination bracket with
both a spring clip and a passive slide. It could be also tied conventionally. If

Review of literature
13
low resistance to sliding is desired, the passive slide could be used, but, if high
resistance to sliding is appropriate, then the active spring clip could be used.
For example, the passive slide to reduce frictional resistance could be used in
the initial stages of treatment, and the spring clip can be utilized later in
treatment for three dimensional control. Therefore, this bracket system could
take advantage of an active spring clip or a passive slide at the orthodontist’s
discretion. Keeping in mind this idea, the clinician could determine the
particular needs and vary the type of control for each tooth. Another
possibility he stated was that of a hybrid system in various combinations of
conventional brackets and ligation, SL spring clip and SL passive slide
brackets that could be integrated into the patient’s treatment by using the same
slot size for all teeth. For instance, in the extraction space closure method of
Gianelly, with crimpable hooks and the anterior brackets could have been
conventional brackets and ligation or an active SL clip for 3D tooth control,
whereas, the posterior teeth could have passive SLB to reduce friction for
space closure by sliding. The conventional bracket, spring clip and
passive slide scheme could be modified for extraction and non-extraction
patients. Perhaps for certain non-extraction cases, all teeth could have brackets
with spring clip. Depending on the desired choice, SLB could be used
selectively with conventional brackets. For example, SLB could be used only
on teeth distal to extraction sites when closing the spaces by sliding or distal to
open coil springs when opening spaces.

Review of literature
14
Harradine (2008)19 stated that self ligating brackets do not require an
elastic or wire ligature systems, but have an in built mechanism that can be
opened and closed to secure the arch wire. Author explained the uses of self
ligating bracket and various designs of self ligating brackets. The advantages
are full arch wire engagement, reduced friction between bracket and the arch
wire, optimal oral hygiene, less chair side assistance and faster arch wire
removal and no meticulous ligation method. Most of the brackets have a metal
face to the bracket slot that is opened and closed with an instrument or using
finger tip. The difference between active and passive clips in terms of alloy of
which its made of, the friction and torque which alters the treatment
efficiency. In Ovation-R brackets the bracket width was reduced and this
narrower width was effective in terms of greater inter bracket span. The
disadvantages of the bracket system is that it is difficult to visualize the
gingival end of lower arch and make sit difficult to open. The lacebacks,
underties and elastomerics placed behind the arch wire also competes for
space with the bracket clips.
Paul Scott and Andrew T. Dibiase (2008)49 compared the efficiency
of mandibular tooth alignment and the clinical effectiveness of a self ligating
and a conventional pre adjusted edgewise orthodontic bracket system. It is a
multicenter randomized clinical trial. Sixty two subjects with mandibular
incisor irregularities of 5 to 12mm and a prescribed extraction pattern
including the mandibular first premolars were randomly allocated to treatment

Review of literature
15
with Damon 3 self ligating Vs Synthesis conventionally ligated brackets. Fully
ligated 0.014-inch Nickle Titanium arch wires were used first in both groups,
followed by a sequence of 0.014 x 0.025 inch and 0.018 x 0.025 inch Nickle
Titanium, and 0.019 x 0.025 inch stainless steel. Study casts were taken at the
start of treatment (T1), the first arch wire change (T2), and the placement of
the final 0.019 x 0.025 inch stainless steel arch wire (T3). Cephalometric
lateral skull and long cone periapical radiographs of the mandibular incisors
were taken at T1 and T3. Authors concluded that there is no significant
difference was noted in the initial rate of alignment for either bracket system.
Alignment was associated with an increase inter canine width, a reduction in
arch length, and proclination of the mandibular incisors for both appliances,
but the differences were not significant.
Hisham M. Badawi and Roger W. Toogood (2008)25 measured the
difference in third-order moments that can be delivered by engaging
0.019 x 0.025-in stainless steel archwires to active self-ligating brackets
(In-Ovation, GAC) and 2 passive self-ligating brackets (Damon2, Ormco and
Smart Clip, 3M Unitek). A bracket/wire assembly torsion device was
developed. This novel apparatus can apply torsion to the wire while
maintaining perfect vertical and horizontal alignment between the wire and the
bracket. A multi-axis force/torque transducer was used to measure the moment
of the couple (torque), and a digital inclinometer was used to measure the
torsion angle. Fifty maxillary right central incisor brackets from each of the

Review of literature
16
4 manufacturers were tested. Conclusions drawn were that the active
self-ligating brackets seemed to have better torque control, due to a direct
result of their active clip forcing the wire into the bracket slot. The amount of
arch wire bracket slop was considerably less for active self-ligating brackets
than passive self-ligating brackets. The active self-ligating brackets expressed
higher torque values than the passive self-ligating brackets at clinically usable
torsion angles (0°-35°). The passive self-ligating brackets produced lower
moments at low torsion angles and started producing higher moments at high
torsion that cannot be used clinically. The clinically applicable range of torque
activation was greater for the active self-ligating brackets than for the passive
self-ligating brackets. All the brackets showed significant variations in the
torque expressed; this seemed to be attributed to the variation in bracket slot
dimensions. Damon2 and Speed brackets were relatively more consistent than
Smart Clip and In-Ovation brackets.
Harradine (2008)19 stated that a combination of low friction and
secure full engagement is particularly useful in the alignment of very irregular
teeth and the resolution of severe rotations, where the capacity of the wire to
release from binding and slide through the brackets of the rotated and adjacent
teeth would be expected to significantly facilitate alignment. Low friction
therefore permits rapid alignment and more certain space closure, whereas the
secure bracket engagement permits full engagement with severely displaced
teeth and full control while sliding teeth along an archwire. It is this feature

Review of literature
17
that greatly facilitates the alignment of crowded teeth, which have to push
each other along the archwire to gain alignment.
Tae – kyung Kim, Ki-Dal Kim (2008)57 compared the frictional force
generated by various combinations of SLB types, arch wire sizes, and alloy
types and the amount of displacement during the initial leveling phase of
orthodontic treatment, by using a custom-designed typhodont system. Two
passive (Damon 2 and Damon 3), and 3 active SLBs (Speed, In-Ovation R,
Time 2), and Smart Clip were tested with 0.014-in and 0.016-in austenitic
nickel-titanium and copper-nickel-titanium arch wires. To simulate
malocclusion status, the maxillary canines were displaced vertically, and
mandibular lateral incisors horizontally from their ideal positions up to 3mm
with 1mm intervals. Two conventional brackets (Mini Diamond MD and
Clarity CL) were used as controls. Frictional forces were least in Damon and
IN-Ovation R brackets in the typodont, regardless of arch wire size and alloy
type. The A-Ni-Ti wire showed significantly lower frictional forces than Cu-
Ni-Ti wire of the same size. As the amounts of vertical displacement of the
maxillary canine and horizontal displacement of the mandibular incisors were
increased, frictional forces also increased.
David Birnie (2008)23 stated that The Damon philosophy is based on
the principle of using just enough force to initiate tooth movement-the
threshold force. The underlying principle behind the threshold force is that it
must be low enough to prevent occluding the blood vessels in the periodontal
Review of literature
18
membrane to allow the cells and the necessary biochemical messengers to be
transported to the site where bone resorption and apposition will occur and
thus permit tooth movement. A passive self-ligation mechanism has the lowest
frictional resistance of any ligation system. Thus the forces generated by the
archwire are transmitted directly to the teeth and supporting structures without
absorption or transformation by the ligature system.
Compared with conventional pre-adjusted edgewise appliances, it is
suggested that the use of passive self-ligation results in a significant reduction
in the use of anchorage devices because the frictional resistance generated by
ligatures is not present.
Jeffrey L. Berger (2008)2 showed the basis for the SPEED Design. In
1970, Dr. G. Herbert Hanson invented a miniaturized self-ligating bracket with
a super elastic nickel titanium spring clip to entrap the archwire. This flexible
spring clip can occupy either of two resting positions: “slot closed” to capture
the archwire, or “slot open” to release the arch-wire. The spring clip is also
capable of storing energy, which is gently released as corrective tooth
movement occurs. active spring clip. This fully pre-adjusted edgewise
appliance, was available in both 0.018” and 0.022” slot size. Benefits for the
clinician include:
Highly flexible nickel titanium spring clip provides precise 3-D
tooth control,
Minimal friction during sliding mechanics

Review of literature
19
Extended range of activation due to energy stored in spring
clip,
Large interbracket span,
Spring clip will not fatigue or plastically deform under normal
treatment conditions.
John R. Valant (2008)64 described a system which is interactive, that
is, they can exhibit either passive or active properties during any stage of
treatment at the discretion and direction of the clinician. There were principle
problems with a bracket system which is entirely active or passive, such as
difficulties in either achieving complete rotational corrections or maintaining
them once corrected, Inadequate torque control, Patient discomfort, Lessened
levels of hygiene due to bracket size and profile. This bracket system and its
mode of function, appeared to incorporate all of the desirable features that
were lacking in the systems previously used:
Minimal force and friction (passive) in the early stage of treatment
Torque and rotational control (active) in the middle and finishing
stages of treatment
Low profile (low in-out relationships)
An interactive mechanism has the inherent capacity to interact with
different arch wires in varying degrees and the amounts of force, friction, and
control that it can express. Furthermore, it is differentiated from an active
mechanism by virtue of the physical design and positional relationship of the

Review of literature
20
wire restraining and controlling element. Interactive clips are fabricated to
allow for varying degrees of contact with the archwires. As the wire
dimensions change, there is a gradual level of contact (variable amounts of
force and control) between the archwire and the clip. For example, in the Time
system, when 0.016 smaller round wires are used, the appliance is passive and
yields very low levels of friction and force. However, when larger rectangular
wires (eg, 0.017 x 0.025) are placed, the appliance becomes active in that it is
then able to control and finalize rotations and torque.
Padhraig S, Fleming, Andrew. T.DiBase (2009)41 compared the
efficiency of mandibular arch alignment in three dimensions with self ligating
bracket system (SmartClip) and a conventional pre-adjusted edgewise twin
bracket (Victory) in non-extraction patients. This was a prospective,
randomized, controlled clinical trial. Sixty-six consecutive patients satisfied
the inclusion criteria and were enrolled in the study. Pre treatment mandibular
arch irregularity were measured by using a co-ordinate measuring machine. A
0.016-in round martensitic active nickel-titanium aligning arch wire was
placed in all the subjects. Mandibular arch irregularity was re-measured after 8
weeks later and found that the bracket type had little influence on arch
efficiency. Authors concluded that efficiency of alignment in the mandibular
arch in non-extraction patients is independent of bracket type. Alignment
efficiency is largely influenced by initial irregularity.

Review of literature
21
Padhraig S, Fleming, Andrew. T.DiBase (2009)42 compared the
effects of two pre adjusted appliances on angular and linear changes of the
mandibular incisors, and transverse mandibular arch dimensional changes over
a minimum of 30 weeks. Sixty six consecutive patients allocated to treatment
with a SLB (Smartclip) and conventional pre adjusted edgewise brackets
(Victory). Initial study models and cephalograms were obtained within a
month of starting the study. All subjects received treatment with the following
arch wire sequence: 0.016-in round, 0.017 x 0.025-in rectangular,
0.019 x 0.025-in rectangular martensitic active nickel-titanium arch wires and
0.019 x 0.025-in stainless steel arch wires. Final records, including study
models and a lateral cephalograms, were collected after a minimum of
30 weeks after initial appliance placement. Lateral cephalograms were
assessed for treatment related changes in mandibular incisor inclination and
position. Transverse dimensional changes in intercanine, and intermolar
distances, and the amount of crowding alleviated during the study period were
assessed by comparison of pre treatment and post treatment models. There was
little difference overall in the pattern of arch alignment and leveling related to
the two PEA. However, there was a statistically greater increase in intermolar
width in the group treated with SLB, although the difference was only
0.91mm.
Padhraig S.Fleming,a Andrew T.DiBiase,b and RobertT.Lee43
tested the hypotheses that treatment with 2 fixed orthodontic appliances

Review of literature
22
(SmartClip andVictory;3MUnitek, Monrovia, Calif) would result in no
difference in (1)the duration of orthodontic treatment or (2) the number of
visits required. They randomly allocated Sixty-six patients into two groups
comprising of self ligating and conventional system. The duration of treatment
and the number of visits required in addition to the initial and final peer
assessment rating (PAR)scores were recorded. The number of teeth extracted
during treatment and the frequency of mechanical eruption of canines were
also noted. They found that in the Fifty-four participants who completed the
study. The duration of treatment was 3months greater in the group treated with
SmartClip. However, bracket type had no statistical influence on treatment
duration (P = 0.076), total visits required(P=0.184), or percentage PAR score
reduction(P= 0.255).they concluded the study saying that the self-ligating
bracket systems used in the trial neither improved the efficiency of fixed
appliance treatment nor resulted in fewer treatment visits.
Pandis. N and Argy Polychronopoulou (2010)46 compared the time
required to complete the alignment of crowded maxillary anterior teeth (canine
to canine) between Damon MX and In-Ovation R self ligating brackets, the
amount of crowding of the maxillary anterior dentition was assessed by using
the irregularity index. The number of days required to completely alleviate the
maxillary anterior crowding in the two groups were investigated. An analysis
of each protocol was performed. He concluded that there is no difference in
crowding alleviation was found between In-Ovation R and Damon MX.

Review of literature
23
Stephanie Shih-Hsuan Chen, a Geoffrey Michael Greenlee (2010)54
did a systematic review to identify and review the orthodontic literature with
regard to the efficiency, effectiveness, and stability of treatment with self
ligating brackets compared with conventional brackets. Self ligating appears to
have a significant advantage with regard to chair side time, based on several
cross- sectional studies. Analysis also showed a small, but statistically
significant difference in mandibular incisor proclination. No other differences
in treatment time and occlusal characteristics after treatment were found
between the two systems that are supported by the current evidence.
Retraction efficiency is not significantly efficient compared to conventional.
Long term studies are required with the greater sample size for better
understanding of the efficiency of self ligating brackets.
Padhraig S. Fleminga; Ama Johalb (2010)32 evaluated the clinical
differences in relation to the use of self ligating brackets in orthodontics. Six
RCTs and eleven CCT were identified from the electronic databases which
investigated the influence of bracket type on alignment efficiency, subjective
pain experience, bond failure rate, arch dimensional changes, rate of
orthodontic space closure, periodontal outcomes, and root resorption were
selected. Both authors were involved in validity assessment, and data
extraction. Meta analysis of the influence of bracket type on subjective pain
experience failed to demonstrate a significant advantage for either type of
appliance. Authors concluded that it was difficult to assess the efficiency at

Review of literature
24
this stage because there is insufficient high quality evidence to support the use
of self ligating brackets over conventional bracket system.
Emily Ong and Hugh McCallum (2010)11 compared the efficiency of
self ligating and conventionally ligated bracket system during the first
20weeks of extraction treatment. Fifty consecutive patients who had premolar
extractions in the maxillary and/or mandibular arch, 0.022 x 0.028-in slot
brackets, and similar arch wire sequences were studied. Forty four arches
received Damon 3MX brackets, and 40 arches received Victory Series or Mini
Diamond brackets. The models were evaluated for anterior arch alignment,
extraction spaces, and arch dimensions at pre treatment (T0), 10weeks (T1),
and 20weeks (T2). They concluded that there were no significant differences
between the self ligating and conventionally ligated groups at 20 weeks in
irregularity scores. There were no significant differences in passive extraction
space closures between the groups.
Nicholas Pandis, Argy Polychronopoulou (2010)46 conducted a study
to investigate the effect of treatment of mandibular crowding with self-ligating
and conventional brackets on dental arch variables and they selected fifty-six
patients who satisfied the inclusion criteria of non-extraction treatment in the
mandibular or maxillary arches, eruption of all mandibular teeth, no spaces
and an irregularity index greater than 2 mm in the mandibular arch, and no
adjunct treatment such as extra or intraoral appliances. The patients were

Review of literature
25
assigned to two groups: one group received treatment with the self-ligating
bracket and the other with a conventional edgewise appliance. Lateral
cephalometric radiographs were obtained at the beginning (T1) and end (T2)
of treatment were used to assess the alteration in mandibular incisor
inclination, and measurements of inter canine and inter molar widths were
made on dental casts to investigate changes associated with the correction.
Results showed an alignment-induced increase in the proclination of the
mandibular incisors was observed for both groups; no difference was
identified between self-ligating and conventional brackets with respect to this
parameter. Likewise, an increase in inter canine and inter molar widths was
noted for both bracket groups; the self-ligating group showed a higher
intermolar width increase than in the conventional group
PM Cattaneo, M Treccani, LHS Cevidanes, B Melsen (2011)40
evaluated the transversal tooth movements and buccal bone modeling of
maxillary lateral segments achieved with active or passive self-ligating bracket
systems in a randomized clinical trial. Sixty-four patients, with Class I, II, and
mild Class III malocclusions, were randomly assigned to treatment with
passive (Damon 3 MX) or active (In-Ovation R) SLBs. Impressions and cone-
beam CT-scans were taken before (T0) and after treatment (T1). Displacement
of maxillary canines, premolars and molars, and buccal alveolar bone
modeling were blindly assessed. Twenty-one patients in the Damon and 20 in
the In-Ovation group completed treatment according to the prescribed
protocol. Transversal expansion of the upper arch was achieved by buccal

Review of literature
26
tipping in all but one patient in each group. There were no statistical
significant difference in inter-premolar bucco-lingual inclination between the
two groups from T0 to T1. The bone area buccal to the 2nd premolar
decreased on average of 20% in the Damon and 14% in the In-Ovation group.
Only few patients exhibited widening of the alveolar process. They concluded
saying that the anticipated translation and buccal bone modeling using active
or passive SLBs could not be confirmed in the majority of the cases.
Individual pre-treatment factors, like initial teeth inclination and occlusion,
seemed to be important in determining the final outcome of the individual
treatment, and CBCT-technology combined with digital casts was important to
analyze 3D treatment outcomes both at dental and bone level in large study
groups.
Andrew T. DiBiase, Inas H. Nasr (2011)9 conducted a prospective
randomized clinical trial comparing the effect of bracket type on the duration
of orthodontic treatment and the occlusal outcome as measured by the peer
assessment rating (PAR) where sixty-two subjects with a mean pre treatment
PAR score of 39.40, along with mandibular irregularity from 5 to 12 mm, and
subjects who were prescribed extractions including mandibular first premolars
were randomly allocated to treatment with either the Damon3 self-ligated or
the Synthesis conventional ligated pre adjusted bracket systems (both, Ormco,
Glendora, Calif). An identical archwire sequence was used in both groups
excluding the finishing archwires: 0.014-in, 0.014 x 0.025-in, and

Review of literature
27
0.018 x 0.025 in copper-nickel-titanium aligning archwires, followed by 0.019
x 0.025-in stainless steel working archwires. Data collected at the start of
treatment and after appliance removal included dental study casts, total
duration of treatment, number of visits, number of emergency visits and
breakages during treatment, and number of failed appointments. Accounting
for pretreatment and in-treatment covariates, bracket type had no effect on the
overall treatment duration, number of visits, or overall percentage of reduction
in PAR scores. The time spent in space closure had an effect on treatment
duration, and the pretreatment PAR score influenced only the reduction in
PAR as a result of treatment. Thus, the use of Damon3 bracket does not reduce
overall treatment time or total number of visits, or result in a better occlusal
outcome when compared with conventional ligated brackets in the treatment
of extraction patients with crowding.
Johansson and Fredrik Lundström (2012)28 conducted a prospective
and randomized study of the efficiency of orthodontic treatment with self-
ligating edgewise brackets (SL; Time2 brand, American Orthodontics) and
conventional edgewise twin brackets (CE; Gemini brand, 3M). The
participants were treated by one of three specialists in orthodontics and with
continuous instructions alternately by five orthodontic assistants according to
our normal treatment routine (ie, modified 0.0220 MBT pre adjusted edgewise
technique). The treatments were evaluated in terms of overall treatment time,
number of visits, and treatment outcome using the Index of Complexity,
Outcome and Need (ICON). The number of emergency appointments, number

Review of literature
28
of archwires, overjet, relative space, and extractions at treatment start were
noted. After dropouts, the analyzed material consisted of 44 patients treated
with SL and 46 patients treated with conventional. It was found that were no
statistically significant differences between the SL and CE groups in terms of
mean treatment time in months (20.4 Vs 18.2), mean number of visits
(15.5 Vs 14.1), mean ICON scores after treatment (13.2 Vs 11.9), or mean
ICON improvement grade (7.9 Vs 9.1) thereby, they concluded saying that
orthodontic treatment with SL brackets does not reduce treatment time or
number of appointments and does not affect post treatment ICON scores or
ICON improvement grade compared with CE brackets.
Prettymana et al (2012)47 evaluated the significant clinical differences
between self-ligating brackets and conventional brackets during orthodontic
treatment, as perceived by orthodontists. They conducted a survey to assess
how SLB was compared to CB in terms of orthodontists’ perceptions
(n= 430).
Results showed that Self Ligating Brackets were preferred during the
initial stage of treatment based on the shorter adjustment appointments and
faster initial treatment progress they provided (P =0.001). On the other hand,
practitioners preferred CB during the finishing and detailing stages of
treatment (P =0.001). CB were also preferred over SLB because they were
cheaper.
Nigel Harradine (2013)22 summarized the advantages of self ligation
system thus, contribuiting to increased efficiency of the brackets. The

Review of literature
29
advantages included full secured ligation without the problems of force decay
in elastomeric modules, faster ligation and arch wire removal which saves
upto 9 minutes per visit compared to the conventional, rapidity of treatment
due to lower resistance to sliding inside the bracket slot.
Padhraig S. Fleminga and Kevin O’Brien (2013)14 contradicted the
advantages put forth by other authors saying that there was no significant time
difference for slide closure and replacement of ligatures and it is controversial
to say that self ligating brackets helps in faster alignment or in rapid space
closure.
Pandis and Padhraig S. Fleming (2014)15 did a network meta
analysis on the Initial orthodontic alignment effectiveness with self-ligating
and conventional appliances and the NMA results indicated that the
conventional appliances perform better in terms of alignment efficiency
compared with all other systems, with greater mean improvements of 0.03,
0.08, and 0.17 mm per month compared with In-Ovation-R, Damon, and
Smart-Clip, respectively.
Goldie Songra,a Matthew Clover(2014)17 compared the time to
initial alignment and extraction space closure using conventional brackets and
active and passive self-ligating brackets. They selected one hundred
adolescent patients 11 to 18 years of age undergoing maxillary and mandibular
fixed appliance therapy after the extraction of 4 premolars who were
randomized with stratification of 2 age ranges (11-14 and 15-18 years) and
3 maxillo mandibular plane angles (high, medium, and low) with an allocation

Review of literature
30
ratio of 1:2:2. Allocation was to 1 of 3 treatment groups: conventional
brackets, active self-ligating, or passive self ligating brackets. All subjects
were treated with the same arch wire sequence and space-closing mechanics.
Labial-segment alignment and space closure were measured on study models
taken every 12 weeks throughout treatment. Results demonstrated a significant
effect of bracket type on the time to initial alignment (P = 0.001), which was
shorter with the conventional brackets than either of the self-ligating brackets.
There was no statistically significant difference between any of the 3 bracket
types with respect to space closure. Space-closure times were shorter in the
mandible, except for the Damon 3MX bracket (Ormco, Orange, Calif), where
active and total space-closure times were shorter in the maxilla. The following
conclusions that were drawn from this study was
1. There was no statistically significant difference in the time to initial
alignment between active and passive self-ligating brackets. The time
to alignment was significantly shorter with conventional brackets.
2. There was no significant difference in the time to passive, active, or
total space closure among all bracket types.
3. There was a statistically significant difference in the time to initial
alignment between the mandible and the maxilla, with a shorter time to
alignment in the maxilla.
4. There was a statistically significant difference in space closure with
time between the mandible and the maxilla.

Review of literature
31
Megha Anand,a David L. Turpin (2015)63 did a retrospective cohort
study to assess the effects and efficiency of selfligating brackets compared
with conventional brackets along with a secondary purpose was to identify the
pretreatment factors associated with the choice of self-ligating or conventional
brackets. The subjects were treated by 2 private practitioners who used both
self-ligating and conventional brackets in their practices. The self ligating
subjects were consecutively identified (treatment completed between January
2011 and April 2012), and then an age- and sex-matched control group was
chosen from the same office. The outcome measures were changes in arch
dimensions, changes in mandibular incisor inclinations, final peer assessment
rating (PAR) scores, percentages of PAR reduction, overall treatment times,
total number of visits, and number of emergency visits. The final sample
comprised 74 patients. Results found were that the practitioners had
significant differences for several treatment parameters; therefore, the data
from the 2 clinicians were analyzed separately. For clinician 1, no significant
differences were observed between the self-ligating and conventional groups,
other than increased arch length in the self-ligating group. The self-ligation
patients treated by clinician 2 demonstrated significant increases in transverse
dimensions, lower percentages of reduction in PAR scores, shorter treatment
times, fewer visits, and more wire-sliding emergencies than the conventional
bracket group. Therefore, the study suggested that the bracket system, per se,
may not have a major effect on arch dimensions, mandibular incisor
inclinations, occlusal outcomes and treatment efficiency and it is possible that

Review of literature
32
the variations in these parameters may depend more on patient characteristics,
such as initial crowding or military population, or on treatment choices made
by the clinician, such as arch wire sequence and form, mechanic.

Materials and Methods

Materials and Methods
33
MATERIALS AND METHODS
Sixteen consecutive patients who met the selection criteria were
included in the study conducted in the Dept. of Orthodontics, Ragas Dental
College & Hospital, Chennai.
The inclusion criteria for all sixteen patients were as follows:
1. Age criteria: 14 to 25 years old having permanent dentition of either
gender.
2. Angles Class I, Class II Division 1 and Bi-dento alveolar
malocclusion requiring all first bicuspid extraction followed by fixed
orthodontic therapy.
3. Patients with Little’s irregularity index score of ≥ 2 for dental
crowding.
4. Group A anchorage.
5. First and second molars to be banded or bonded in maxillary and
mandibular arch.
Patients with previous history of orthodontic treatment, any missing
tooth other than third molars, with cleft lip and palate or any craniofacial
deformity or temporo-mandibular dysfunction were excluded from the study.
Four patients failed to keep up with the appointments and were excluded from
the study.

Materials and Methods
34
Twelve patients were randomly divided into two groups of six each:
Group A and Group B
Group A patients were bonded with Self Ligating pre-adjusted
edgewise, Roth 0.022 slot brackets (Dual activation Empower; American
Orthodontics, Sheboygan, WI,USA) and Group B patients was bonded with
Conventional pre-adjusted edgewise Roth 0.022 slot brackets (Mini Master
series; American Orthodontics, Sheboygan, WI,USA), which were positioned
using Boon’s gauge in the upper and lower arches. The first and second molars
were banded or bonded with Roth’s prescription with weldable or bondable
buccal tube and lingual sheath were used in the first molars for placement of
transpalatal arch if required.
Arch form used in the study was the Type III Arch form (American
Orthodontics, Sheboygan, WI,USA).
Leveling and aligning was done using a specific archwire sequence:
1. 0.016” round thermal NiTi
2. 0.018” round stainless steel with reverse curve
3. 0.019 x 0.025” NiTi
All the arch wires were to be changed only after it sits passively in the
bracket slots. All subjects were reviewed after an interval of 4 weeks. Once
the level slot alignment was achieved with 0.019x0.025” NiTi wire, the

Materials and Methods
35
0.019 x 0.025” stainless steel wire was inserted when it passively fitted into
the bracket slot.
Stainless steel ligatures or elastomeric modules were used to secure
archwire into the conventional brackets. Arch wires were disengaged by
cutting the ligatures or removing the modules. For the self ligating brackets,
the clip was opened and closed using the manufacturer-recommended
instrument (Hu Friedy clip appliance wire disengagement hand instrument;
American Orthodontics, Sheboygan, WI,USA)
A set of study models and lateral cephalograms were taken at the
beginning of the treatment (T0) and at the end of Leveling and aligning stage
(T2). To calculate the alignment efficiency a set of models were taken at the
time of placement of 0.018 inch stainless steel wire (T1).
All the lateral cephalograms were traced by the same investigator.
All the study models were evaluated by using Little’s irregularity index with a
digital Verneir caliper (Insize Digital Caliper, series 1112, resolution to
0.01mm) to quantify the alignment of the six anterior teeth of maxillary and
mandibular arches.
Inter canine width and Inter second premolar width were measured
from the cusp tips of the canines and second premolars respectively on the
study models using a digital Verneir caliper. Measurements were not taken

Materials and Methods
36
from the gingival margin because the quality of the gingival impression was
inconsistent.
Intermolar widths were measured from the mesial occlusal pits of the
mandibular and maxillary first molars.
The study models were measured with digital Vernier calipers with
sharpened tips that were accurate to 0.01 mm. All model measurements were
made by the principal researcher.
Landmarks and Reference planes used:
NASION (N)- The most anterior point of the fronto-nasal suture in the median
plane
SELLA (S)- the midpoint of the hypophyseal fossa. It is a constructed point in
the median plane.
S-N PLANE- it’s the cranial line between the center of sella tursica and the
anterior point of the anterior point of the fronto-nasal suture (nasion). It
represents the anterior cranial base. (Steiner’s analysis)
POINT B- It is the most posterior point in the concavity between the chin and
the mandibular process.
MANDIBULAR PLANE- A line drawn from anatomic gonion to gnathion.
Materials and Methods
37
STATISTICAL ANALYSIS
Descriptive and analytical statistical analyses were performed with
SPSS software package (SPSS for Windows XP,version 21.0, Chicago). For
each variable measured on the study models and on the lateral cephalograms,
the Mean and Standard deviation were calculated.
Wilcoxon Signed Rank Test which is a non parametric test, was done
to compare the irregularity index at T0 (before treatment), at T1 (at the time of
placement of 0.018 inch stainless steel) and at T2 (at the time of placement of
0.019 x 0.025 inch stainless steel wire) in each Self Ligating (Group A) and
Conventional (Group B) brackets.
Mann Whitney U Test (non parametric test), was done to evaluate the
alignment efficiency at T0 (before treatment), at T1 (at the time of placement
of 0.018 inch stainless steel) and at T2( at the time of placement of
0.019 x 0.025 inch stainless steel wire) between Self Ligating (Group A) and
Conventional (Group B) brackets.
Parametric Paired T-Test was done to evaluate the torque expression
in each Self Ligating (Group A) and Conventional (Group B) brackets at
initial and final alignment.
Paired t-Test was done to evaluate the amount of arch expansion at
Inter Canine, Inter Premolar and Inter Molar regions, for each Self Ligating
(Group A) and Conventional (Group B) brackets at T0 (before treatment), at

Materials and Methods
38
T1 (at the time of placement of 0.018 inch stainless steel) and at T2( at the
time of placement of 0.019 x 0.025 inch stainless steel wire).
Independent T Test was done to compare the amount of torque
expression at initial and final alignment between Self Ligating (Group A) and
Conventional (Group B) brackets.
Independent T Test was done to compare the amount of arch
expansion at Inter Canine, Inter Premolar and Inter Molar regions, for each of
the Self Ligating (Group A) and Conventional (Group B) brackets at T0
(before treatment), at T1 (at the time of placement of 0.018 inch stainless
steel) and at T2( at the time of placement of 0.019 x 0.025 inch stainless steel
wire).
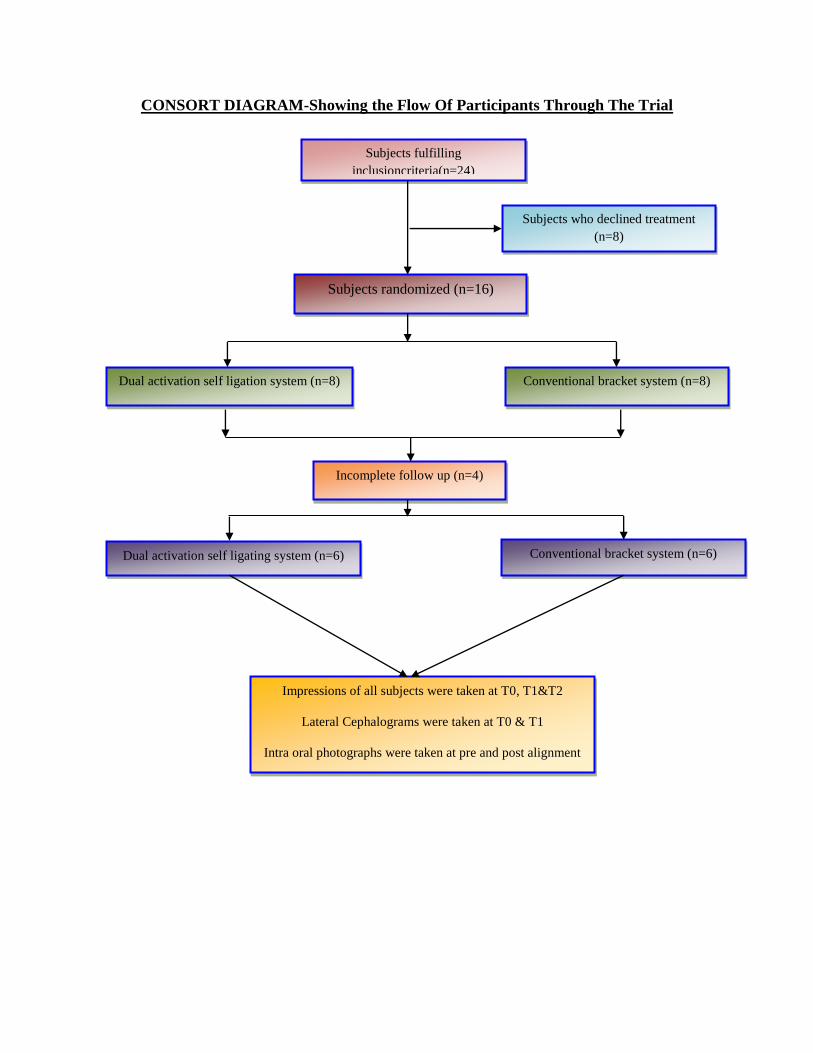
CONSORT DIAGRAM-Showing the Flow Of Participants Through The Trial
Subjects fulfilling
inclusioncriteria(n=24)
Subjects who declined treatment
(n=8)
Subjects randomized (n=16)
Dual activation self ligation system (n=8) Conventional bracket system (n=8)
Incomplete follow up (n=4)
Dual activation self ligating system (n=6) Conventional bracket system (n=6)
Impressions of all subjects were taken at T0, T1&T2
Lateral Cephalograms were taken at T0 & T1
Intra oral photographs were taken at pre and post alignment

Figures

Figures
Figure1. Dual Activation Self Ligating Bracket System
Figure 2. Conventional Bracket System

Figures
CALCULATION FOR IRREGULARITY INDEX MEASURED AT T0,T1&T2
Figure 3a. Study Group Mandibular T0 Figure 3b.Control Group Mandibular
Irregularity Index Irregularity Index T0
Figure 4a. Study Group Mandibular Irregularity Figure 4b.Control Group Mandibular Irregularity
Index T1 Index T1
Figure 5a. Study Group Mandibular Figure 5b. Study Group Mandibular
Irregularity Index T2 Irregularity Index T2
SAMPLE CONTROL

Figures
MEASUREMENTS FOR TRANSVERSE DIMENSIONAL CHANGES
Figure 6. Study Group Mandibular Inter Canine Width T0
Figure 7. Study Group Mandibular Inter Second Premolar Width T1
Figure 8. Study Group Mandibular Inter Second Molar Width T2

Figures
Figure 9a.
CEPHALOMETRIC RADIOGRAPH TO MEASURE TORQUE EXPRESSION
AT T0 (STUDY GROUP)

Figures
Figure 9b.
CEPHALOMETRIC RADIOGRAPH TO MEASURE TORQUE EXPRESSION
AT T1 (STUDY GROUP)

Figures
Figure 10a.
CEPHALOMETRIC RADIOGRAPH TO MEASURE TORQUE EXPRESSION
AT T0 (CONTROL GROUP)

Figures
Figure 10b.
CEPHALOMETRIC RADIOGRAPH TO MEASURE TORQUE EXPRESSION
AT T1 (CONTROL GROUP)

Results

Results
39
RESULTS
This study comprised of 12 patients who were divided into two groups,
Group A and Group B, each having 6 patients respectively. The mean age of
the patients was 16.8 ± 4 years in both the groups.
The irregularity index of the sample between the three time frames
were evaluated. (Table Ib). Results showed that there was a statistically
significant difference in the alignment of maxillary arch from T0 to T1
(p<0.024) and T0 to T2 (p<0.020) and mandibular arch from T0 to T1
(p<0.027) and T0 to T2 (p<0.024). However, no statistically significant
difference was there for both maxillary and mandibular arches in the time
frame of T1 to T2. Therefore, the major alignment difference is seen from T0-
T1 (Table Ib).
The irregularity index of the control group were tabulated in (Table Ic)
which showed that there was a statistically significant difference in the
alignment of maxillary arch from T0 to T1 (p<0.026) and from T0 to T2
(p<0.026). In the mandibular arch, statistically significant difference is seen
between T0 to T1 (p<0.026) and from T0 to T2 (p<0.27). However, no
statistically significant difference was found in maxillary arch in the time
frame of T2 to T1. Therefore, the maximum amount of alignment was seen
from T0-T1 (Table Ic).

Results
40
The comparison of the irregularity scores between sample and control
was evaluated (Table Id). Results showed that there was a statistically
significant difference at the start of the study T0 (p<0.045) with the sample
group having a higher irregularity score than the control. However, no
statistically significant difference was found between the sample and the
control over the two time frames; it showed that the irregularity score was
higher for sample, in the time period T0-T2. Hence, the sample group showed
better alignment efficiency than the control group (Table Id).
Amount of time taken for Alignment between sample and control was
evaluated (Table IIb). Results showed that there was a statistically significant
difference in alignment time taken for maxillary and mandibular arch between
T1 to T2 (p<0.026). No satistically significant difference was found between
other time periods. In total time taken, a significant difference (p<0.016) was
found between the sample and the control with a mean difference of 3 weeks.
(Table IIb).
The amount of torque expression in the sample group between pre (T0)
and post alignment (T2) was tabulated in (Table IIIa.) There was no
statistically significant difference in lower incisor to nasion-point B in the
angular measurements (p>0.084) though there was a mean decrease of 5° in
the post alignment values (Table IIIa).

Results
41
Amount of torque expression for Control group between pre (T0) and
post alignment stage (T1) were tabulated (Table IIIb). Results showed that
there was no statistically significant difference in the torque expression for
lower incisor to point B in the angular measurements (p>0.310) though there
was a mean decrease of 2° in the post alignment values (Table IIIb).
Amount of Torque expression between the Sample and Control groups
were tabulated in table IIIc. Results showed no statistically significant
difference in the amount of torque expression for mandibular incisors in the
post alignment phase between sample and control with the p value of p>0.091
(Table IIIc).
The intercanine width of the sample and control group is evaluated
(Table IVa). Results showed no statistical significant difference in the sample
group.
The inter premolar width of the sample and control group is evaluated
(Table IVb). Results showed no statistical significant difference in the sample
group.
The inter molar width of the sample and control group were evaluated
(Table IVc). Results showed no statistically significant difference in the
sample and control group for maxillary and mandibular arches.

Results
42
The intercanine width between the sample and the control over the
three time frames was tabulated (Table IVd). Results showed that there was no
statistically significant difference in the inter canine width between TO, T1
and T2 in both maxillary and mandibular arches.
The inter Premolar width between the sample and the control over
the three time frames were tabulated in the (Table IVe). Results showed that
there was no statistically significant difference in the inter Premolar width
between TO, T1 and T2 in both maxillary and mandibular arches.
The inter Molar width between the sample and the control over the
three time frames were tabulated (Table IVf.) Results showed that there was
no statistically significant difference in the inter Molar width between TO, T1
and T2 in both maxillary and mandibular arches.
So, there was no statistically significant difference in the amount of
transverse dimensions measured in the regions of inter canine, inter premolar
and inter molar both in the maxillary and mandibular arches for both samples
and control.

Tables &Graphs

Tables and Graphs
TABLE Ia. DESCRIPTIVE STATISTICS FOR IRREGULARITY
INDEX:
Measure Statistic Group
Sample Control Total
Maxilla
(mm) - T0
N 6 6 12
Mean 4.37 3.17 3.77
Std. Dev 0.9 0.98 1.09
1st Quartile 4 2 3.5
Median 4 3.5 4
3rd
Quartile 4 4 4
Maxilla
(mm) - T1
N 6 6 12
Mean 0.5 0.58 0.54
Std. Dev 0.84 0.66 0.72
1st Quartile 0 0 0
Median 0 0.5 0
3rd
Quartile 1 1 1
Maxilla
(mm)-T2
N 6 6 12
Mean 0 0 0
Std. Dev 0 0 0
1st Quartile 0 0 0
Median 0 0 0
3rd
Quartile 0 0 0

Tables and Graphs
Measure Statistic Group
Sample Control Total
Mandible
(mm) - T0
N 6 6 12
Mean 4 4.75 4.37
Std. Dev 1.26 1.6 1.43
1st Quartile 4 4 4
Median 4 5 4
3rd
Quartile 4 6 5.5
Mandible
(mm) - T1
N 6 6 12
Mean 0.67 1.17 0.92
Std. Dev 0.52 0.98 0.79
1st Quartile 0 0 0
Median 1 1.5 1
3rd
Quartile 1 2 1.5
Mandible
(mm) - T2
N 6 6 12
Mean 0 0 0
Std. Dev 0 0 0
1st Quartile 0 0 0
Median 0 0 0
3rd
Quartile 0 0 0

Tables and Graphs
TABLE IB. WILCOXON SIGNED RANKS TEST TO COMPARE THE
IRREGULARITY INDEX IN EACH SAMPLE GROUP BETWEEN
T0,T1&T2.
Measures Z-Value P-Value
Maxilla (mm) - T1 - Maxilla (mm) - T0 2.264 0.024
Maxilla (mm) - T2 - Maxilla (mm) - T0 2.333 0.020
Maxilla (mm) - T2 - Maxilla (mm) - T1 1.342 0.180
Mandible (mm) - T1 - Mandible (mm) - T0 2.214 0.027
Mandible (mm) - T2 - Mandible (mm) - T0 2.264 0.024
Mandible (mm) - T2 - Mandible (mm) - T1 2.000 0.046
TABLE IC. WILCOXON SIGNED RANKS TEST TO COMPARE THE
IRREGULARITY INDEX IN EACH CONTROL GROUP BETWEEN
T0,T1 & T2
Measures Z-Value P-Value
Maxilla (mm) - T1 - Maxilla (mm) - T0 2.232 0.026
Maxilla (mm) - T2 - Maxilla (mm) - T0 2.232 0.026
Maxilla (mm) - T2 - Maxilla (mm) - T1 1.633 0.102
Mandible (mm) - T1 - Mandible (mm) - T0 2.226 0.026
Mandible (mm) - T2 - Mandible (mm) - T0 2.207 0.027
Mandible (mm) - T2 - Mandible (mm) - T1 1.890 0.059
TABLE ID. COMPARISION OF IRREGULARITY INDEX BETWEEN
SAMPLE AND CONTROL USING MANN-WHITNEY TEST AT T0, T1
& T2
Measures Z-Value P-Value
Maxilla (mm) - T0 2.006 0.045
Maxilla (mm) - T1 0.360 0.719
Maxilla (mm) - T2 0.000 1.000
Mandible (mm) - T0 1.169 0.242
Mandible (mm) - T1 1.024 0.306
Mandible (mm) - T2 0.000 1.000

Tables and Graphs
TABLE IIA. DESCRIPTIVE STATISTICS FOR TIME TAKEN
FOR ALIGNMENT
Measure Statistic Group
Sample Control Total
Time taken
T0-T1 Max
N 6 6 12
Mean 10.67 13.33 12
Std. Dev 2.07 3.27 2.95
1st Quartile 8 12 10
Median 12 14 12
3rd Quartile 12 16 14
Time taken
T1-T2 Max
N 6 6 12
Mean 8 11.33 9.67
Std. Dev 2.53 1.63 2.67
1st Quartile 8 12 8
Median 8 12 10
3rd Quartile 8 12 12
Measure Statistic Group
Sample Control Total
Time taken
T0-T1 Mand
N 6 6 12
Mean 10.67 13.33 12
Std. Dev 2.07 3.27 2.95
1st Quartile 8 12 10
Median 12 14 12
3rd Quartile 12 16 14
Time Taken
T1-T2 Mand
N 6 6 12
Mean 8 11.33 9.67
Std. Dev 2.53 1.63 2.67
1st Quartile 8 12 8
Median 8 12 10
3rd Quartile 8 12 12
Total time
taken (weeks)
N 6 6 12
Mean 18.67 24.67 21.67
Std. Dev 3.27 3.01 4.33
1st Quartile 16 24 18
Median 18 24 22
3rd Quartile 20 28 24

Tables and Graphs
TABLE IIB. TIME TAKEN FOR ALIGNMENT USING MANN-
WHITNEY TEST FOR SAMPLES AND CONTROLS
Measures Z-Value P-Value
Time taken T0-T1 Max 1.563 0.118
Time taken T1-T2 Max 2.227 0.026
Time taken T0-T1 Mand 1.563 0.118
Time Taken T1-T2 Mand 2.227 0.026
Total time taken (weeks) 2.403 0.016

Tables and Graphs
RESULTS FOR TORQUE EXPRESSION
Paired samples T-Test to compare mean values of torque expression
between initial and final alignment in each Group
TABLE IIIA. GROUP: SAMPLE
Pair Measure N Mean Std. Dev t-Value P-
Value
Pair 1 IMPA-PRE 6 104.67 8.914 1.464 0.203
IMPA-POST 6 99.83 6.369
Pair 2 Lower Incisor to NB-PRE 6 36.00 6.066
2.150 0.084 Lower Incisor to NB-POST 6 32.50 4.722
Paired samples T-Test to compare mean values values of torque
expression between initial and final alginment in each Group
TABLE IIIB. GROUP: CONTROL
Pair Measure N Mean Std. Dev t-
Value
P-
Value
Pair 1 IMPA-PRE 6 111.67 3.830 1.536 0.185
IMPA-POST 6 108.33 8.641
Pair 2 Lower Incisor to NB-PRE 6 41.83 4.708
1.130 0.310 Lower Incisor to NB-
POST 6 39.83 8.353

Tables and Graphs
COMPARISON OF AMOUNT OF TORQUE EXPRESSION BETWEEN
GROUP A AND GROUP B:
TABLE IIIC. INDEPENDENT SAMPLES T-TEST TO COMPARE
MEAN VALUES OF TORQUE EXPRESSION BETWEEN SAMPLES
AND CONTROLS
Measure Group N Mean Std. Dev t-Value P-
Value
IMPA-PRE Sample 6 104.67 8.914 1.767 0.108
Control 6 111.67 3.830
IMPA-POST Sample 6 99.83 6.369 1.940 0.081
Control 6 108.33 8.641
Lower Incisor to NB-
PRE
Sample 6 36.00 6.066 1.861 0.092
Control 6 41.83 4.708
Lower Incisor to NB-
POST
Sample 6 32.50 4.722 1.872 0.091
Control 6 39.83 8.353

Tables and Graphs
RESULTS FOR TRANSVERSE DIMENSION.
TABLE IVA. PAIRED SAMPLES T-TEST TO COMPARE MEAN
VALUES OF INTER CANINE WIDTH BETWEEN T0,T1 & T2 IN
EACH GROUP: INTERCANINE WIDTH
Group Measurements N Mean Std. Dev t-Value P-Value
Sample
Pair 1 Maxilla (mm) - T0 6 36.3500 2.19049 0.908 0.405
Maxilla (mm) - T1 6 36.8833 1.02810
Pair 2 Maxilla (mm) - T0 6 36.3500 2.19049 0.776 0.473
Maxilla (mm) - T2 6 36.8233 .97336
Pair 3 Maxilla (mm) - T1 6 36.8833 1.02810 0.718 0.505
Maxilla (mm) - T2 6 36.8233 .97336
Pair 4 Mandible (mm) - T0 6 27.2683 1.46477 0.146 0.889
Mandible (mm) - T1 6 27.3600 1.13763
Pair 5 Mandible (mm) - T0 6 27.2683 1.46477 1.892 0.117
Mandible (mm) - T2 6 28.3283 1.41120
Pair 6 Mandible (mm) - T1 6 27.3600 1.13763 2.137 0.086
Mandible (mm) - T2 6 28.3283 1.41120
Control
Pair 1 Maxilla (mm) - T0 6 35.4333 2.48659 1.267 0.261
Maxilla (mm) - T1 6 36.0083 1.76436
Pair 2 Maxilla (mm) - T0 6 35.4333 2.48659 1.612 0.168
Maxilla (mm) - T2 6 36.2767 1.51191
Pair 3 Maxilla (mm) - T1 6 36.0083 1.76436 1.376 0.227
Maxilla (mm) - T2 6 36.2767 1.51191
Pair 4 Mandible (mm) - T0 6 26.2167 2.12553 3.179 0.025
Mandible (mm) - T1 6 27.7283 1.74809
Pair 5 Mandible (mm) - T0 6 26.2167 2.12553 3.894 0.011
Mandible (mm) - T2 6 28.2667 1.29915
Pair 6 Mandible (mm) - T1 6 27.7283 1.74809 2.476 0.056
Mandible (mm) - T2 6 28.2667 1.29915

Tables and Graphs
TABLE IVB. PAIRED SAMPLES T-TEST TO COMPARE MEAN
VALUES OF INTER PREMOLAR WIDTH BETWEEN T0,T1 & T2 IN
EACH GROUP :
Group Measurements N Mean Std. Dev t-Value P-Value
Sample
Pair 1 Maxilla (mm) - T0 6 45.5967 2.84119 0.949 0.386
Maxilla (mm) - T1 6 46.2250 1.29536
Pair 2 Maxilla (mm) - T0 6 45.5967 2.84119 0.272 0.796
Maxilla (mm) - T2 6 45.7600 2.08179
Pair 3 Maxilla (mm) - T1 6 46.2250 1.29536 0.919 0.400
Maxilla (mm) - T2 6 45.7600 2.08179
Pair 4 Mandible (mm) - T0 6 39.0417 4.58573 0.337 0.750
Mandible (mm) - T1 6 38.7150 2.82849
Pair 5 Mandible (mm) - T0 6 39.0417 4.58573 0.209 0.843
Mandible (mm) - T2 6 38.8667 2.81435
Pair 6 Mandible (mm) - T1 6 38.7150 2.82849 0.397 0.708
Mandible (mm) - T2 6 38.8667 2.81435
Control
Pair 1 Maxilla (mm) - T0 6 45.4717 2.28963 6.534 0.001
Maxilla (mm) - T1 6 47.4617 1.98365
Pair 2 Maxilla (mm) - T0 6 45.4717 2.28963 5.838 0.002
Maxilla (mm) - T2 6 47.9550 2.02477
Pair 3 Maxilla (mm) - T1 6 47.4617 1.98365 2.419 0.060
Maxilla (mm) - T2 6 47.9550 2.02477
Pair 4 Mandible (mm) - T0 6 38.0517 1.96486 4.553 0.006
Mandible (mm) - T1 6 40.3650 1.43581
Pair 5 Mandible (mm) - T0 6 38.0517 1.96486 4.264 0.008
Mandible (mm) - T2 6 40.6567 1.51373
Pair 6 Mandible (mm) - T1 6 40.3650 1.43581 2.139 0.085
Mandible (mm) - T2 6 40.6567 1.51373

Tables and Graphs
TABLE IVC. PAIRED SAMPLES T-TEST TO COMPARE MEAN
VALUES OF INTER MOLAR WIDTH BETWEEN T0,T1,T2
IN EACH GROUP
Group Measurements N Mean Std. Dev t-Value P-Value
Sample
Pair 1 Maxilla (mm) - T0 6 44.0900 2.51114 0.383 0.718
Maxilla (mm) - T1 6 44.3417 1.75065
Pair 2 Maxilla (mm) - T0 6 44.0900 2.51114 1.269 0.260
Maxilla (mm) - T2 6 45.6167 3.51761
Pair 3 Maxilla (mm) - T1 6 44.3417 1.75065 0.828 0.445
Maxilla (mm) - T2 6 45.6167 3.51761
Pair 4 Mandible (mm) - T0 6 39.0583 3.86050 0.029 0.978
Mandible (mm) - T1 6 39.0850 2.72118
Pair 5 Mandible (mm) - T0 6 39.0583 3.86050 0.184 0.862
Mandible (mm) - T2 6 39.2617 2.52716
Pair 6 Mandible (mm) - T1 6 39.0850 2.72118 0.649 0.545
Mandible (mm) - T2 6 39.2617 2.52716
Control
Pair 1 Maxilla (mm) - T0 6 45.3900 2.25904 0.859 0.430
Maxilla (mm) - T1 6 44.7900 3.06267
Pair 2 Maxilla (mm) - T0 6 45.3900 2.25904 0.083 0.937
Maxilla (mm) - T2 6 45.3533 2.58197
Pair 3 Maxilla (mm) - T1 6 44.7900 3.06267 2.103 0.089
Maxilla (mm) - T2 6 45.3533 2.58197
Pair 4 Mandible (mm) - T0 6 38.5417 2.00847 0.168 0.873
Mandible (mm) - T1 6 38.6117 2.11353
Pair 5 Mandible (mm) - T0 6 38.5417 2.00847 0.231 0.826
Mandible (mm) - T2 6 38.6517 2.20760
Pair 6 Mandible (mm) - T1 6 38.6117 2.11353 0.371 0.726
Mandible (mm) - T2 6 38.6517 2.20760

Tables and Graphs
TABLE IVD INDEPENDENT SAMPLES T-TEST TO COMPARE
MEAN VALUES OF INTER CANINE WIDTH BETWEEN SAMPLES
AND CONTROLS
Width Measure Group N Mean Std. Dev t-
Value
P-
Value
INTER
CANINE
WIDTH
Maxilla (mm) - T0 Sample 6 36.3500 2.19049 0.678 0.513
Control 6 35.4333 2.48659
Maxilla (mm) - T1 Sample 6 36.8833 1.02810 1.050 0.319
Control 6 36.0083 1.76436
Maxilla (mm) - T2 Sample 6 36.8233 .97336 0.745 0.474
Control 6 36.2767 1.51191
Mandible (mm) - T0 Sample 6 27.2683 1.46477 0.998 0.342
Control 6 26.2167 2.12553
Mandible (mm) - T1 Sample 6 27.3600 1.13763 0.433 0.674
Control 6 27.7283 1.74809
Mandible (mm) - T2 Sample 6 28.3283 1.41120 0.079 0.939

Tables and Graphs
TABLE IVE INDEPENDENT SAMPLES T-TEST TO COMPARE
MEAN VALUES OF INTER PREMOLAR WIDTH BETWEEN
SAMPLES AND CONTROLS
Width Measure Group N Mean Std. Dev t-
Value
P-
Value
INTER
PREMOLAR
WIDTH
Maxilla (mm) - T0 Sample 6 45.5967 2.84119 0.084 0.935
Control 6 45.4717 2.28963
Maxilla (mm) - T1 Sample 6 46.2250 1.29536 1.279 0.230
Control 6 47.4617 1.98365
Maxilla (mm) - T2 Sample 6 45.7600 2.08179 1.851 0.094
Control 6 47.9550 2.02477
Mandible (mm) -
T0
Sample 6 39.0417 4.58573 0.486 0.637
Control 6 38.0517 1.96486
Mandible (mm) -
T1
Sample 6 38.7150 2.82849 1.274 0.231
Control 6 40.3650 1.43581
Mandible (mm) -
T2
Sample 6 38.8667 2.81435 1.372 0.200

Tables and Graphs
TABLE IVF INDEPENDENT SAMPLES T-TEST TO COMPARE
MEAN VALUES OF INTER MOLAR WIDTH BETWEEN SAMPLES
AND CONTROLS
Width Measure Group N Mean Std. Dev t-
Value
P-
Value
INTER
MOLAR
WIDTH
Maxilla (mm) - T0 Sample 6
44.090
0 2.51114
0.943 0.368 Control
6 45.390
0 2.25904
Maxilla (mm) - T1 Sample 6
44.341
7 1.75065
0.311 0.762 Control
6 44.790
0 3.06267
Maxilla (mm) - T2 Sample 6
45.616
7 3.51761
0.148 0.885 Control
6 45.353
3 2.58197
Mandible (mm) - T0 Sample 6
39.058
3 3.86050
0.291 0.777 Control
6 38.541
7 2.00847
Mandible (mm) - T1 Sample 6
39.085
0 2.72118
0.336 0.743 Control
6 38.611
7 2.11353
Mandible (mm) - T2 Sample 6
39.261
7 2.52716 0.445 0.666

GRAPH 1
4.37
0.50
0.00
4.00
0.67
0.00 0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
Maxilla - T0 Maxilla - T1 Maxilla - T2 Mandible - T0 Mandible - T1 Mandible - T2
Me
an
va
lue
Mean Irregularity Index (mm) in Sample. Table No.Ib

GRAPH 2
3.17
0.58
0.00
4.75
1.17
0.00 0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
Maxilla - T0 Maxilla - T1 Maxilla - T2 Mandible - T0 Mandible - T1 Mandible - T2
Me
an
va
lue
Mean Irregularity Index (mm) in Control. Table No. Ic

GRAPH 3
4.37
0.50
0.00
4.00
0.67
0.00
3.17
0.58
0.00
4.75
1.17
0.00 0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
Maxilla - T0 Maxilla - T1 Maxilla - T2 Mandible - T0 Mandible - T1 Mandible - T2
Me
an
va
lue
Comparision of Mean Irregularity Index (mm). Table No.Id Sample
Control
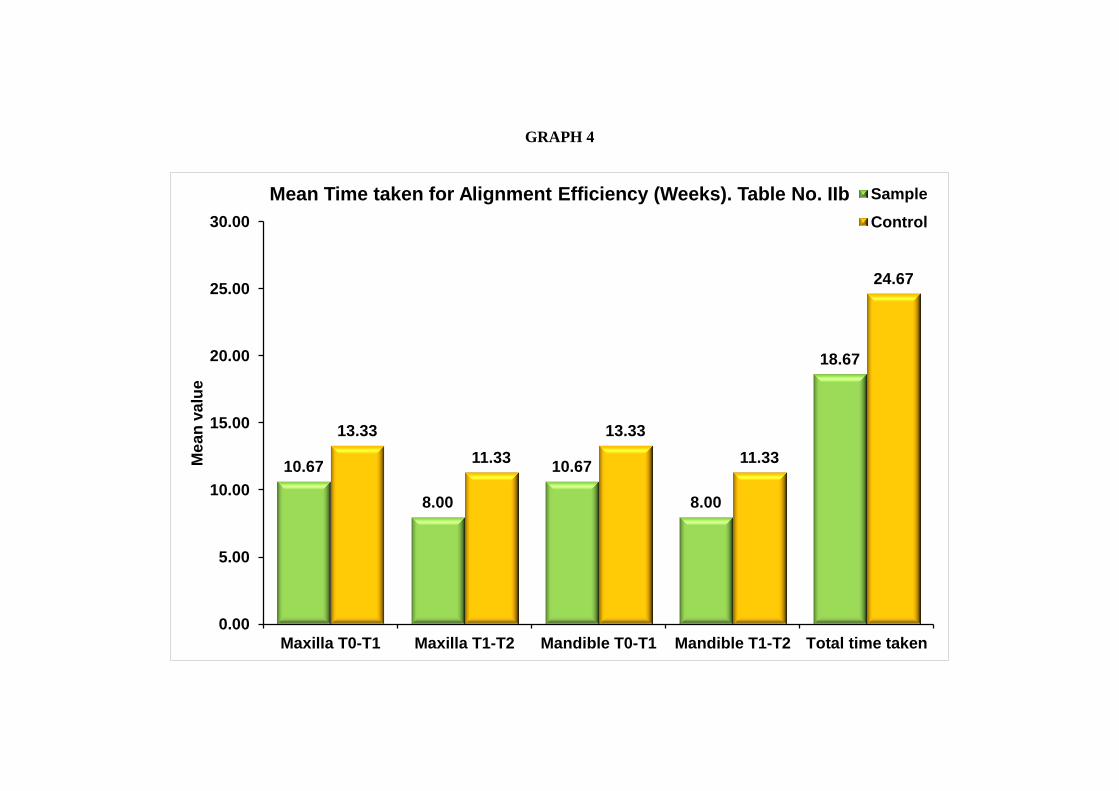
GRAPH 4
10.67
8.00
10.67
8.00
18.67
13.33
11.33
13.33
11.33
24.67
0.00
5.00
10.00
15.00
20.00
25.00
30.00
Maxilla T0-T1 Maxilla T1-T2 Mandible T0-T1 Mandible T1-T2 Total time taken
Me
an
va
lue
Mean Time taken for Alignment Efficiency (Weeks). Table No. IIb Sample
Control

GRAPH 5
104.67 99.83
36.00 32.50
111.67 108.33
41.83 39.83
0.00
20.00
40.00
60.00
80.00
100.00
120.00
IMPA-PRE IMPA-POST Lower Incisor toNB-PRE
Lower Incisor toNB-POST
Me
an
va
lue
Comparision of Mean Torque Expression. Table No.IIIc Sample
Control

GRAPH 6
36.35 36.88 36.82
27.27 27.36 28.33
35.43 36.01 36.28
26.22 27.73 28.27
0.00
10.00
20.00
30.00
40.00
50.00
60.00
Maxilla - T0 Maxilla - T1 Maxilla - T2 Mandible - T0 Mandible - T1 Mandible - T2
Me
an
va
lue
Comparision of Mean Inter Canine Width (mm). Table No. IVd Sample
Control

GRAPH 7
45.60 46.23 45.76
39.04 38.72 38.87
45.47 47.46 47.96
38.05 40.37 40.66
0.00
10.00
20.00
30.00
40.00
50.00
60.00
Maxilla - T0 Maxilla - T1 Maxilla - T2 Mandible - T0 Mandible - T1 Mandible - T2
Me
an
va
lue
Comparision of Mean Inter Premolar Width (mm). Table No.IVe Sample
Control

GRAPH 8
44.09 44.34 45.62
39.06 39.09 39.26
45.39 44.79 45.35
38.54 38.61 38.65
0.00
10.00
20.00
30.00
40.00
50.00
60.00
Maxilla - T0 Maxilla - T1 Maxilla - T2 Mandible -T0
Mandible -T1
Mandible -T2
Me
an
va
lue
Comparision of Mean Inter Molar Width (mm). Table no. IVf Sample
Control

Discussion

Discussion
43
DISCUSSION
Self-ligating bracket system has gained immense popularity in the last
few years. The proponents of the system claim that the SLBs is more effective
and efficient than the Conventional bracket system. The low friction which is a
hallmark of the self ligating brackets is supposed to encourage faster
alignment, without taxing the anchorage, with less need for extraction and in
fewer appointments. Efficiency is said to be influenced by three key factors:-
efficiency of the mechanics used, decreased chair time per office visit, and
fewer appointments to complete treatment.61
The term “self-ligating bracket” (SL bracket) is used for those type of
fixed orthodontic brackets that incorporate a locking mechanism (such as a
ring, spring, or door mechanism) that holds the arch-wire in the bracket slot.34
Self-ligating orthodontic brackets have a relatively long history,
but their development can best be viewed against the background of an
almost universal use of metal and elastomeric ligatures. Elastomeric ligation
gives unreliable archwire control, there is force decays therefore, tooth control
is not optimal,19
both wire and elastomeric ligatures sometimes may become
displaced.19
The other drawbacks of elastomerics include high friction,
increased chair side time and an added oral hygiene challenge.58
Wire ligation
is better in every respect, but it is very time consuming, has inconsistent force
application and the wire ends can cause trauma to patient and operator.58
Discussion
44
In contrast to this, the self ligating brackets are supposed to offer a
number of advantages such as:-19
Secured Robust Ligation, Full Bracket
Engagement, Low Friction, Increased efficiency, Maintenance of Optimal Oral
Hygiene, Comfortable for the Patient and Longer appointment intervals10,21
Wire ligatures provide suitable robust ligation, whereas elastomeric ligatures
undergo force decay if left for too long without being renewed, which calls for
frequent patient recalls.21
A study by Harradine, did quantify the loss of
elastomeric ligatures, finding 15 lost ligatures in 25 consecutively seen
patients in a 12-month treatment period.42
Full Bracket Engagement is a great advantage if the arch wire can be
fully engaged in the bracket slot and maintained there with certainty.23
Most of
the self-ligating brackets have mechanisms to deliver this advantage and
would ensure full engagement of all archwires and eliminate the need to regain
control of the teeth when full engagement is lost.42
In a study by Mezomo,35
where canine retraction was done with 0.018-in stainless steel wires, self
ligating brackets were found to provide better rotational control of the canine
than conventionally ligated brackets.
Wire ligatures do not stretch to an extent that engagement once
achieved at ligation is subsequently lost, so they can meet this requirement.
Elastomerics are worse since they may frequently exert insufficient force to
fully engage even a flexible wire and on subsequent degradation of their
elastic property may cause a significant loss of engagement as the elastomeric

Discussion
45
stretches.23
Typically elastomeric chains and ligatures suffer more than 50%
degradation in force in the first 24 hours21
when tested under in vitro
experimental environments. Twin brackets with the ability to “figure 8” the
elastomerics are a significant help in this respect but at the cost of increased
friction.58
Wire ligatures produce substantially lower friction forces than
elastomerics.52
However, the forces generated by wire ligation still reach high
and very variable levels 42
relative to those force levels that are thought to be
optimal for tooth movement. Most tooth movements involve relative
movement between the arch wire and the bracket.
Friction produced between the bracket and the arch wire must be
overcome before the intended tooth-moving forces can have their effect.19
Frictional forces arising from the method of ligation offers additional
resistance to this relative movement. Correspondingly much higher forces
must be applied and this has two related potential effects that inhibit tooth
movement. First, the total effective force is much more difficult to assess and
is more likely to be undesirably higher than force levels best suited to create
the optimal biologic response. Second, the binding forces are higher both
between bracket and wire and also at the contacts between irregular adjacent
teeth. And such binding forces also inhibit the required relative movement.19
Friction is the only source of resistance to sliding, when drawing arch
wires through well-aligned brackets friction has consistently been measured as

Discussion
46
much lower in the self- ligating brackets than in the conventionally ligated
brackets.2,22,29,33,37,52,55,56,59
Studies typically report values of almost zero with self-ligating
brackets and values from 43 to 98 g per bracket for various elastomeric-arch
wire combinations.30
The original motive of developing self-ligating brackets was to speed
the process of arch wire ligation.22
Maijer R, Harradine et al have shown self-
ligating brackets to save up to 9 minutes per visit compared with wire ligation
and approximately 2 minutes compared with elastomeric ligation.21,52
Several consecutive case series studies have found that treatment with
self-ligating brackets was quicker, required fewer visits, and resulted in better
final alignment and occlusion than treatment with conventional appliances 6,62
Two recent systematic reviews have concluded that there is insufficient
evidence to support the view that treatment with self-ligating brackets results
in fewer visits or shorter treatment time. 43,54
Manufacturers claim that treatment with self-ligating brackets is less
painful and it has put forth two explanations: the forces on the teeth are lower
because lighter arch wires can be used with equal effectiveness, and the teeth
move more readily in response to the applied forces because of decreased
resistance to sliding.22

Discussion
47
Yamaguchi M et al, conducted a split-mouth study to examine the
measure of pain with the help of the level of the neuropeptidase substance P in
gingival crevicular fluid, which is a marker of inflammation and associated
pain resulting from orthodontic forces and, found that treatment with self-
ligating brackets significantly lowered the levels of Substance P and
inflammation when compared with conventional ligation at 24 hours after arch
wire placement.68
Repeated claims of more efficient treatment have been made; which
have been contradicted by the findings from few randomized trials.9,13,28
Similarly, there appears to be little basis for the claim that self-ligating
brackets induce distinctive arch dimensional changes.44
Padhraig S. Fleming
conducted a randomized controlled trial, and found no differences in
maxillary arch dimensional changes or molar and incisor inclination changes
after alignment with passive self-ligating brackets, active self-ligation, or
conventional brackets.44
Interest in self ligating brackets has grown in the recent years. There
are essentially two main types of self-ligating brackets, based on the designing
of the locking mechanism and the dimensions of the slot: active brackets and
passive brackets.
In passive systems (such as the Damon System. ORMCO, A Company,
Orange, CA), the slot is locked with a rigid locking mechanism. Once it is
engaged, the bracket is effectively turned into a tube, ideally allowing arch

Discussion
48
wires to slide freely within the tube.34
In active systems (such as Quick,
Forestadent Ltd., Germany; and SPEED, Cambridge), the locking mechanism
generally consists of a flexible but resilient clip that can actively engages the
wire into the bracket slot once the arch wire reaches a certain size of
deflection. 52?
Active self ligating brackets such as, SPEED (Strite Industries,
Cambridge, Ontario, Canada), and Quick brackets(Forestadent Ltd., Germany)
have a sliding spring clip, (type of clip search) which encroaches on the slot
from the labial aspect, potentially placing an active force on the arch wire.
These brackets are all correctly described as having potentially active clips. In
contrast, the passive self ligating brackets such as the Damon brackets
(ORMCO, A Company, Orange, CA) have a slide which opens and closes
vertically and creates a passive labial surface to the slot with no intention
or ability to encroach upon the slot and store force by deflection of a
metal clip.58
A third type of bracket system has been added called the Interactive
self ligating brackets such as the InOvation R bracket (GAC, International,
Bohemia, NY, USA) which can exhibit either passive or active properties
during any stage of treatment at the discretion and direction of the clinician.64
They exhibit minimal force and friction (passive) in the early stage of
treatment .Torque and rotational control (active) in the middle and finishing
stages of treatment.66

Discussion
49
In the search of a possible ideal Self Ligating bracket, a combination
bracket with both a spring clip and a passive slide was pondered upon. If low
resistance to sliding is desired, the passive slide could be used, and, if high
resistance to sliding is appropriate, then the active spring clip could be used.8
Gianelly reported that in the extraction space-closure method, with
crimp-on hooks and molars, the anterior brackets could have conventional
brackets or an Self Ligating active clip for 3D control, whereas the posterior
teeth could have passive Self Ligating brackets to reduce friction for space
closure by sliding.18
Based on this concept, the Dual Activation Self Ligating Bracket
system was introduced in the market by American Orthodontics. They have a
unique system wherein, the anterior brackets are of the Intractive while, the
posteriors are passive self ligating bracket system. It claims to passively hold
the smaller archwires and actively engage the larger dimensional wires for
lower ligation force in the early treatment stage with proper torque and
rotational control during working and finishing stages.
A number of factors in addition to bracket type might be expected to
influence the time for initial alignment of the labial-segment teeth, including
the degree of initial mal-alignment of arch, arch wire engagement, arch-wire
sequence, and the presence or absence of extraction spaces.17

Discussion
50
Very low classical friction with various designs of Self Ligating
brackets has been clearly demonstrated within the literature with passive
ligation being superior to active ligation in this regard.33
However, the
assumption has been made that along with low friction in vitro comes more
rapid alignment and a reduction in treatment time in vivo.33
P.G.Miles38
found
that during the initial alignment phase of treatment, the passive system had 0.2
mm greater irregularity index score, so clinically it did not perform any better
than the conventional twin bracket.
The aim and objective of our study, was to assess the alignment
efficiency with the Dual activation bracket system. To our knowledge, all the
current evidence as far as bracket types influencing the rapidity of alignment is
confined to either active, passive or interactive bracket systems. Hence, the
need to assess the efficiency of the Dual activation brackets was designed and
the results were compared with the efficiency of the Conventional Pre adjusted
edgewise system.
Our study used Dual activation self ligating bracket system with the
interactive brackets in the anterior and passive self ligating brackets in the
posterior teeth. This refers to the fact that round wires less than 0.020 inches in
diameter sit passively in the slots of the anterior brackets, with no force being
delivered from the clip or the fourth wall.19
Any arch wire with a bucco-
lingual dimension larger than 0.020 inches will receive a greater amount of
force from the actively displaced clip, thereby delivering exceptional torque

Discussion
51
and rotation control during working and finishing stages. Whereas , the
posterior passive brackets offers low ligation forces throughout all the stages
of treatment.
Studies done by Henao et al24
found that the bracket is passive for
0.014 inches and 0.016 inches wires and as the dimension of the wire
increased the clip actively engaged the wire into the slot. This is because the
horizontal gingival wall is reduced and therefore, the dimension is reduced to
0.019 inch width and not 0.028 inch. In this regard, the dual activation bracket
systems have a better three dimensional control compared to passive self-
ligation system. However, as noted, the passive self ligation brackets produce
less frictional force compared to active self ligating brackets.53
Some of the other claims made by the proponents of the passive self
ligation system is that a majority of cases can be treated without extraction.
The combination of low force and low friction along with altered
biomechanical response which supposedly widens the arches. Thereby,
eliminating or at the best reducing the need for extraction in borderline
extraction cases. The passive widening of the arches is also supposed to reduce
the possibility of incisors flaring thereby, offering excellent torque control.
Thus, this study was done to compare the alignment efficiency of Dual
activation self ligating brackets (Empower Dual Activation, American
Orthodontics, Sheboygan, WI,USA) and conventional bracket (MiniMaster
Series, American Orthodontics, Sheboygan, WI,USA); along with changes in

Discussion
52
transverse dimensions and the torque expression between both the bracket
systems.
The alignment efficiency was assessed by using the Little’s Irregularity
Index50
measured on the study models of both upper and lower arches. In
addition, changes in arch width by using dental casts was also studied;
mandibular incisor inclination was measured from cephalometric lateral skull
radiographs.
There is a relative lack of evidence comparing the efficiency of SL and
CL brackets in extraction patients because most studies have investigated
mixed samples. Only 2 clinical trials have compared SL and CL brackets
solely in extraction patients.39,49
The prospective study included Sixteen subjects, with total number of
ten female subjects and six male subjects with mean age of 16.8±4 years
having only permanent dentition with Angle's class I Malocclusion or Bi-dento
alveolar malocclusion. The subjects were randomly divided into Group A and
Group B. Patients were selected based on their irregularity index scores of
≥ 4mm requiring all first bicuspid extractions. At the start of treatment four
subjects were eliminated from the study due to failure to keep up with the
appointments.
Plaster study models and lateral cephalometric radiographs were taken
at three time points: before the start of the treatment (T0), at the time of

Discussion
53
placement of 0.018 inch stainless steel wire (T1) and at the time of placement
of a 0.019 x 0.025 inch stainless steel wire which sits passively in the
arches (T2).
The treatment began with an initial archwire of 0.016-in round thermal
nickel titanium (Type III arch form, American Orthodontics,
Sheboygan,WI,USA), followed by 0.018-in- stainless steel (Type III arch
form, American Orthodontics, Sheboygan,WI,USA) ; then 0.019 x 0.025 in
nickle titanium wire (Type III arch form, American Orthodontics,
Sheboygan,WI,USA) followed by 0.019 x 0.025 in-stainless steel wire (Type
III arch form, American Orthodontics, Sheboygan,WI,USA). The patients
were reviewed every 4 weeks; and the first archwire/ all the archwires was left
in place until the teeth were passively engaged in all bracket slots before
proceeding to the second archwire. The total time taken from the time of
bonding T0 and advancing to T2 were noted in weeks to check for the
efficiency of the brackets.
The treatment efficiency of the Dual activation self ligating brackets
are discussed under the following headings:-
Alignment efficiency
Amount of Arch Expansion
Torque expression.

Discussion
54
Non Parametric Mann Whitney test was done to assess the amount of
difference in the irregularity score between the sample and the control in the
mentioned time frames. A Wilcoxon signed ranked test was done to evaluate
the alignment efficiency between the sample and the control.
Alignment efficiency:
All study models were evaluated by using Little’s irregularity index50
to quantify the alignment of the six anterior teeth. The study models were
evaluated using a digital vernier caliper over three time frames. The
measurements were made in duplicate, and the average of the 2 readings was
taken to a resolution of 0.01 mm.44
The time frames were as: T0 was at the
beginning of the treatment; followed by T1 which was at the time of
placement of a 0.018 inch stainless steel wire and T2 was at the time of
placement of a 0.019 x 0.025 inch stainless steel wire.
The results showed that although the irregularity score was high for the
sample at the start of the study, there was no statistical significant difference
between the sample and the control at T1 and T2 indicating rapid treatment by
the self ligating bracket system. The alignment time taken for maxillary and
mandibular arches between T1 to T2 which shows that Self ligating brackets
has faster initial alignment than the conventinal group with a mean difference
of 3.3 weeks. A statistically significant difference of 6 week was seen in the
total time taken showing lesser time taken for alignment in the Self ligating
group.

Discussion
55
In a study by Pandis et al45
moderate crowding of < 5 was alleviated
about 2.7 times faster with Self ligating brackets than with conventional
appliances. This difference could be because of the substantially greater free
play of the self-ligating brackets, an effect that facilitates unhindered labial
movement of the crown. Whereas , an elastomeric module or steel ligatures act
as obstacles because of the stress they exert on the wire adjacent to the bracket
sides, precluding free sliding of the wire into the slot walls and adversely
affecting movement rate.45
For moderate crowding with an irregularity index of ≤ 5 mm, there is
some evidence that the self ligating brackets can produce faster alignment,
although this becomes marginally insignificant for more severe crowding.45
The combination of low friction and secure full engagement is particularly
useful, in the alignment of very irregular teeth and the resolution of severe
rotations, where the capacity of the wire to slide through the brackets of the
rotated and adjacent teeth significantly facilitates alignment. This relationship
between friction and derotation has been described and quantified by Koenig
and Burstone,4 and the potential adverse forces shown to be very large. Low
friction, therefore, permits rapid alignment and more certain space closure,
whilst the secure bracket engagement permits full engagement with severely
displaced teeth and full control, whilst sliding teeth along an archwire.
The treatment times in both groups in this study were comparable with
average orthodontic treatment time. Statistically significant difference is seen

Discussion
56
in the total time taken showing lesser time taken for alignment in the Self
ligating group. Therefore, accounting for confounding pretreatment and in-
treatment factors, in our sample the use of self-ligated brackets offered mild
advantage in reducing treatment time for initial alignment. The claims22
relating to treatment efficiency of the Self ligating bracket have been justified
by our investigation. Advocates of this appliance emphasized the importance
of the clinicians embracing this philosophy, allowing the light-force, low-
friction system to achieve physiologic adaption, aligning crowded arches and
avoiding the use of auxiliaries, such as headgear or palatal expansion devices.
In our study, all patients had first premolars extracted, and none of the samples
had anchorage reinforcement at any stage during treatment.
Transverse dimensional changes:
Inter canine widths and Inter second premolar widths were measured
from the cusp tips of the canines and second premolars. Measurements were
not taken from the gingival margin because the quality of the gingival
impression was inconsistent. Inter molar widths were measured from the
central and mesial occlusal pits of the mandibular and maxillary first molars
because this area of the impression was clearer than the cusps.11.
All
measurements were done using digital Vernier caliper with sharpened tips that
were accurate to 0.01 mm.

Discussion
57
In this study, no statistical significant difference was found between the
two groups for inter canine, inter second premolar and inter molar widths
which showed that no arch expansion has taken place.
Padhraig S. Fleming 44
observed that significant changes occurred in
the premolar region with up to 4.51 mm of expansion with Damon Q in the
first premolar region. The changes were slightly greater than those reported by
Franchi et al 16
in a prospective follow-up of 20 patients treated with fixed
appliances with low-friction ligatures over the initial six months of treatment.
Franchi et al reported that expansion ranging from 1.71 to 3.65 mm for
maxillary transverse dimensions with increases peaking in the premolar
region. The reasons for relatively large dimensional increases in Fleming’s44
study can be related to the use of Damon archwires, whereas Tru-arch medium
form wires were used by Franchi et al. Its a known fact, that Damon arch
wires have a broad arch form shape, particularly in the buccal segments, and
that could have contributed to the amount of expansion reported.44
Moreover,
a previous randomized study by Cattaneo et al40
had combined the use of
Damon wires and brackets, but the narrower wires with active self-ligating
brackets, reported similar levels of first premolar expansion with mean values
of 4.5 and 4.3 mm in the active and passive groups, respectively. Slightly
greater amounts of inter molar (0.9 mm) and inter second premolar expansion
(0.7 mm) were noted with the Damon system, however, suggesting that any
effect of the broadened archwire might be exerted farther posteriorly.

Discussion
58
Torque expression:
Angular changes in axial inclination of the long axis of the mandibular
incisor relative to the mandibular plane were measured by assessing the lateral
cephalograms. Radiographs were traced and measured as serial pairs.
Results showed no statistically significant difference in the amount of
torque expression of mandibular incisor in both linear and angular
measurements.
N. Pandis, S Strigou, T Eliades65
tested the hypothesis that the
engagement mode of wire to bracket affects the buccolingual inclination of
maxillary incisors in extraction and non extraction treatment with self ligating
and conventional brackets and they concluded that self ligating brackets seem
to be equally efficient in delivering torque to maxillary incisors relative to
conventional brackets in extraction and non extraction cases.
Studies have depicted mandibular incisor proclination in both self
ligation and conventional groups had no statistical significant difference [Jiang
and Fu,27
; Scott et al.,49
; Fleming et al.42
;Pandis et al46
], indicating that the
mechanism for relieving crowding involves incisor proclination and transverse
expansion through tipping of posterior teeth, which is similar for conventional
and self-ligating brackets. A study by Cattaneo et al.40
, using CBCT was done
to compare the labio lingual inclination of mandibular incisors relative to the

Discussion
59
occlusal plane between active and passive self-ligating brackets and confirmed
a significant proclination of mandibular anterior teeth, thereby rejecting the
claim of torque control by self-ligating systems The meta-analysis including
three of these studies showed that self-ligating brackets had 1.5 degrees less
proclination that was statistically significant, although it may not be a
clinically significant change.63
The present study evaluated the efficiency of self ligating brackets and
conventional brackets only in the transverse plane and sagittal plane. Vertical
changes have not been addressed. Other possible confounding factors could
include the lack of using a cone beam CT to evaluate the arch width changes
and the cortical bone thickness in terms of expansion. Moreover, it has been
postulated that light continuous forces with reduced friction produces 1.8
times greater tooth movement compared to light dissipating or heavy forces.67
Therefore, further studies with more sample size and CBCT scans are
needed to investigate the transverse dimensional changes of dual activation
self ligating brackets compared to conventional brackets and their overall
treatment efficiency.

Summary and Conclusion

Summary and Conclusion
60
SUMMARY AND CONCLUSION
The purpose of this study was to determine the alignment efficiency of
Self Ligating brackets compared to the conventional bracket system.
Twelve consecutive patients who met the selection criteria were
included in the study from a pool of patients satisfying the following inclusion
criteria: all first bicuspid extraction in the maxillary and mandibular arches;
permanent dentition; irregularity index of greater than 2 and no therapeutic
intervention planned with any other extra oral or intra oral appliance. The
patients were randomly divided into two groups of six each- SLB group
(Empower Dual Activation, American Orthodontics, Sheboygan, WI,USA)
and Conventional group (Mini Master Series, American Orthodontics,
Sheboygan, WI,USA), both with Roth 0.022 –in slots. The irregularity index
of both maxillary and mandibular arches were normalized between the groups,
and the time taken for alignment was estimated in weeks. The time points of
the protocol were set as T0-start of the treatment; T1- at the time of placement
of 0.018-in stainless steel arch wire; T2- at the time of placement of 0.019 x
0.025-in stainless steel arch wire passively in the arch. Study models were
taken at each of the time points. Treatment duration was assessed by data
modeling with the Mann Whitney U test. Lateral cephalometric radiographs
were used to assess the alteration of mandibular incisor position before and
after alignment. Measurements of inter canine, inter second premolar and inter
molar widths were also made on the dental study models to evaluate the

Summary and Conclusion
61
transverse dimensional changes associated with the bracket systems. Paired T-
Tests were used to assess the torque expression and the transverse changes
between the two groups. The tests suggested that there was statistical
significance in torque expression between pre and post alignment and no
changes was observed in inter canine, inter second premolar and inter molar
regions.
The following conclusions can be made from the present study:
1. There was a statistically significant difference in the initial alignment
between the dual activation system and the conventional bracket
system, where the dual activation system showed rapid alignment in
the maxillary and mandibular arches.
2. No difference in the quantum of transverse dimensions was observed
between the dual activation system and the conventional system in the
regions of inter canine, inter premolar and inter molar.
3. No difference was noted in the amount of anterior torque expression in
between the two bracket systems.
The limitations of the study are the fact that the sample size needs to be further
enhanced to assess the amount of arch expansion brought about by the self
ligation system and the lack of Cone Beam CT decreases the strength of the
study as a clearer picture of the amount of change seen in the buccal and
palatal cortical bone thickness would reveal us the amount of expansion
achieved by the bracket systems.

Bibliography
Bibliography

Bibliography
BIBLIOGRAPHY
1. Bland JM, Altman DG. Statistical methods for assessing agreement
between two methods of clinical measurement. Lancet 1986;1:
307-10.
2. Berger JL. The influence of the SPEED bracket's self-ligating design
on force levels in tooth movement: a comparative in vitro study. Am J
Orthod Dentofacial Orthop 1990;97:219-28.
3. Budd S , John Daskalogiannakis and Bryan D. Tompson- A
study of the frictional characteristics of four commercially available
self-ligating bracket systems. European Journal of Orthodontics 30
(2008) 645–653.
4. Burstone.C.J and Koenig 1989 – Force systems from an Ideal arch-
Large delfection considerations. The Angle Orthodontist: September
1989, Vol. 59, No. 1, pp.11-16.
5. Chen S S-H, Greenlee MG, Kim JE, Smith CL, Huang GJ-
Systematic review of self ligating brackets. Am J Orthod Dentofacial
Orthop 2010;137:726.el-726.el8.
6. Damon DH. The rationale, evolution and clinical application of the
self-ligating bracket. Clin Orthod Res 1998;1:52-61.
7. Damon DH. The Damon low-friction bracket: a biologically
compatible straight-wire system. J ClinOrthod 1998;32:670-80.
62

Bibliography
8. Daniel J. Rinchuse and Peter G. Miles -Self-ligating brackets:
Present and future;Am J Orthod DentofacialOrthop 2007;132:216-22.
9. DiBiase AT, Nasr IH, Scott P, Cobourne MT. Duration of treatment
and occlusal outcome using Damon3 self-ligated and conventional
orthodontic bracket systems in extraction patients: a prospective
randomized clinical trial. Am J Orthod Dentofacial Orthop
2011;139:e111-6.
10. Eberting JJ, Straja SR, Tuncay OC. Treatment time, outcome,and
patient satisfaction comparisons of Damon and conventional brackets.
Clin Orthod Res 2001;4:228-34.
11. Emily Ong and Hugh McCallum- Efficiency of self ligating vs
conventionally ligated brackets during initial alignment.Am J Ortho
Dentofacial Orthop 2010;138:e1-138-e7.
12. Fleming, A.T. DiBiase, G. Sarri, and R.T. Lee- Pain Experience
during Initial Alignment with a Self-Ligating and a Conventional
Fixed Orthodontic Appliance System; The Angle Orthodontist 2009;
Vol. 79, No. 1, pp. 46–50; P.S.
13. Fleming PS, DiBiase AT, Lee RT.- Randomized clinical trial of
orthodontic treatment efficiency with self-ligating and conventional
fixed orthodontic appliances. Am J Orthod Dentofacial Orthop
2010;137:738-42.

Bibliography
14. Fleming and Kevin O’Brien-Self-ligating brackets do not increase
treatment efficiency. Am J Orthod Dentofacial Orthop 2013;143:
10-9.
15. Fleming, Pandis, - Initial orthodontic alignment effectiveness with
self-ligating and conventional appliances: A network meta-analysis in
practice. Am J Orthod Dentofacial Orthop 2014 ;145:S152-63.
16. Franchi L, Baccetti T, Camporesi M, Lupoli M. Maxillary arch
changes during leveling and aligning with fixed appliances and low-
friction ligatures. Am J Orthod Dentofacial Orthop 2006; 130:88-91.
17. Goldie Songra, Matthew Clover, Nikki E. Atack, Paul Ewings,
Martyn Sherriff, Jonathan R. Sandy,and Anthony J.- Comparative
assessment of alignment efficiency and space closure of active and
passive self-ligating vs conventional appliances in adolescents:A
single-center randomized controlled trial. Am J Ortho
DentofacialOrthop2014;145:569-78.
18. Gianelly AA. Bidimensional technique: theory and Practice.2000.
GAC International; New York: p. 46-7.
19. Harradine-.The History and Development of Self-Ligating
Brackets.Semin Orthod 2008;14:5-18
20. Harradine N.W.T- Current Products and Practices Self ligating
brackets: Where are we now? Journal of Orthodontics, Vol 30,
2003;262-273.

Bibliography
21. Harradine NWT. Self-ligating brackets and treatment efficiency.Clin
Orthod Res 2001;4:220-7.
22. Harradine-Self-ligating brackets increase treatment efficiency. Am J
Orthod Dentofacial Orthop 2013;143:10-9.
23. Harradine and David Birnie- self ligating brackets: theory and
practice.2006.
24. Henao S.P, Kusy RP- Frictional evaluations of dental typodont
model using four self ligating designs and a conventional design.
Angle orthod 2005;75(1):75-85.
25. Hisham M. Badawi, Roger W. Toogood, Jason P. R. Carey,
GiseonHeo, and Paul W.Major- Torque expression of self-ligating
brackets: Am J Orthod Dentofacial Orthop2008;133:721-8.
26. Jacob .Stolzenberg – The Russell attachment and its improved
advantages. Int J Ortho Dent.
27. Jiang RP, Fu MK- Non-extraction treatment with self-ligating and
conventional brackets. 2008, 43(8):459-463.
28. Johansson K, Lundstr€om F. Orthodontic treatment efficiency with
self ligating and conventional edgewise twin brackets: a prospective
randomized clinical trial. Angle Orthod 2012;82:929-34.
29. Kapur R, Sinha PK, Nanda RS- Frictional resistance of the Damon
SL bracket- Journal of Clinical Orthodontics 1998;32:485-489.

Bibliography
30. Khambay B, Millett D, McHugh S. Evaluation of methods of
archwire ligation on frictional resistance. Eur J Orthod 2004;26:
327-32.
31. Kusy RP, Whitley JQ- Influence of archwire and bracket
dimensions on sliding mechanics: derivations and determinations of
the critical contact angles for binding. Eur J Orthod 1999;21:199-208.
32. Lotfus B P,Artun J Nicholls T A, Stoner J A. Evaluation of
friction during tooth movement in various bracket-arch wire
combinations. American Journal of Orthodontics and Dentofacial
Orthopedics1999 116: 336-345.
33. Luca Pizzoni – frictional forces related to self ligating brackets;
European Journal of Orthodontics 1998;20:283-291
34. Ludwig, Dirk Bister, Sebastian Baumgaertel - Self-Ligating
Brackets in Orthodontics.2012. chpt 1. Pg 13.
35. Mauricio mezomo - Maxillary canine retraction with Self ligating
brackets. Angle Orthodontist 2011;81;292-297.
36. McLaughin, Bennet and Trevisi JH. Systemized orthodontic
treatment mechanics;2001:16-17.
37. Meling TR, Ødegaard J, Holthe K, Segner D. The effect of friction
on the bending stiffness of orthodontic beams: a theoretical and in
vitro study. Am J Orthod Dentofacial Orthop 1997;112:41-9.

Bibliography
38. Miles P.G and Weyant R.J- A clinical trial of Damon 2 v/s
conventional twin brackets during initial alignment. Angle
Orthodontist. 2006;76;480-485
39. Miles PG. Self-ligating Vs conventional twin brackets during en-
masse space closure with sliding mechanics. Am J Orthod Dentofacial
Orthop 2007;132:223-5.
40. PM Cattaneo, M Treccani, K Carlsson, T Thorgeirsson, LHS
Cevidanes, B Melsen- Transversal maxillary dento-alveolar changes
in patients treated with active and passive self-ligating brackets: a
randomized clinical trial using CBCT-scans and digital models.
Orthod Craniofac Res 2011;14:222–233
41. Padhraig S, Fleming, Andrew. T. DiBase- comparison of
mandibular arch changes during alignment and leveling with 2 pre
adjusted edgewise appliance. Am J Ortho DentofacialOrthop
2009;136:340-7.
42. Padhraig S, Fleming, Andrew. T.DiBase – efficiency of mandibular
arch alignment with 2 pre adjusted edgewise appliance.Am J Ortho
DentofacialOrthop 2009;135:597-602
43. Padhraig S. Fleminga; AmaJohalb- Self ligating brackets in
orthodontics. A systematic review. Angle orthodontist 2010;80:
575-584
44. Padhraig S. Fleming, Robert T. Lee, Valeria Marinho, and
AmaJohal- Comparison of maxillary arch dimensional changes with

Bibliography
passive and active self-ligation and conventional brackets in the
permanent dentition: A multicenter, randomized controlled trial. Am J
Ortho DentofacialOrthop2013;144:185-93
45. Pandis. N and ArgyPolychronopoulou- Self ligating v/s
conventional brackets in the treatment of mandibular crowding: A
prospective clinical trial of treatment duration and dental effects. Am
J Ortho DentofacialOrthop 2007;132:208-15
46. Pandis. N and ArgyPolychronopoulou- Active or passive self
ligating brackets? A randomized controlled trial of comparative
efficiency in resolving maxillary anterior crowding in adolescents.
Am J Ortho DentofacialOrthop 2010;137:12-13
47. Prettymana; Al M. Bestb; Steven J. Lindauerc - Self-ligating vs
conventional brackets as perceived by orthodontists Angle Orthod.
2012.
48. Profit and Fields HW- Contemporary Orthodontics 3rd
ed. St. Louis;
Mo CV Mosby 2000:348.
49. Paul Scott and Andrew T. Dibiase- Alignment efficiency of Damon
3 self ligating and conventional orthodontic bracket systems: A
randomized clinical trial. Am J Ortho Dentofacial Orthop2008;
134:470.e1-470.e8.
50. Robert M. little - The Irregularity Index: A quantitative score of
mandibular anterior alignment. Vol 68

Bibliography
51. Sandy JR, Farndale RW, Meikle MC. Recent advances in
understanding mechanically induced bone remodeling and their
relevance to orthodontic theory and practice. Am J Orthod Dento
facialOrthop 1993;103:212-22.]
52. Shivpuja PK, Berger J- A comparative study of conventional
ligation and self ligating bracket systems. Am J Ortho
DentofacialOrthop 1994; 106: 472-480
53. Srinivas S: Comparison of canine retraction with self-ligated and
conventional ligated brackets—a clinical study. Thesis in fulfillment
of postgraduate degree, Tamilnadu University, Chennai, India, 2003
54. Stephanie Shih-Hsuan Chen, a Geoffrey Michael Greenlee-
Syatematic review of self ligating brackets .Am J Ortho
DentofacialOrthop 2010;137:726.e1-726.e18.
55. Sims APT, Waters NE, Birnie DJ, Pethybridge RJ. A comparison
of the forces required to produce tooth movement in vitro using two
self-ligating brackets and a pre-adjusted bracket employing two types
of ligation. Eur J Orthod 1993;15:377-85.
56. Sims APT, Waters NE, Birnie DJ. A comparison of the forces
required to produce tooth movement ex vivo through three types of
preadjusted brackets when subjected to determined tip or torque
values. Br J Orthod 1994;21:367-73.
57. Tae- kyungkim, ki-dal Kim- comparison of frictional forces during
intial leveling stages in various combinations of self ligating brackets

Bibliography
and arch wires with a custom designed typodont system. Am J Ortho
DentofacialOrthop 2008;133:187.e15-187.e24.
58. Theodore Eliades, Nikolaos Pandis - Self-Ligation in Orthodontics
2009 chap1. Page 31.
59. Thomas S, Birnie DJ, Sherriff M. A comparative in vitro study of
the frictional characteristics of two types of self ligating brackets and
two types of preadjusted edgewise brackets tied with elastomeric
ligatures. Eur J Orthod 1998;20:589-96.
60. Tselepis M, Brockhurst P, West VC- The dynamic frictional
resistance between orthodontic brackets and arch wires- Am J Ortho
DentofacialOrthop 1994; 106(2):131-138.
61. Trevisi. H and Fredrik Bergstrand-The SmartClip Self-Ligating
Appliance System. Semin Orthod 2008;14:87-100.
62. Turnbull . N.R, David J Birne- Treatment efficiency of
conventional v/s self ligating brackets: effects of arch wire sizes and
material. Am J Ortho DentofacialOrthop 2007;131: 395-99.
63. Turpin David, Megha Anand- Restrospective Investigation of the
Effects and efficiency of Self ligating and conventional brackets. Am
J Ortho DentofacialOrthop 2015;148:67-75.
64. Tweed .C.H- Clinical Orthodontics .St.Louis, MO: CV Mosby;1966.

Bibliography
65. T.Eliades ,Pandis N, Strigou S- Maxillary incisor torque with
conventional and self-ligating brackets: a prospective clinical trial.
Orthod Craniofac Res. 2006 Nov;9(4):193-8.
66. Valant John R. -Time: A Self-Ligating Interactive Bracket System.
Semin Orthod 2008;14:46-53.
67. Warita. H. et al: A study on experimental tooth movement with NiTi
alloy orthodontic wires: comparision between light continuous forces
and light dissipating forces. 1996;55:515-527.
68. Yamaguchi M, Takizawa- The Damon system and release of
substance P in the Gingival crevicular fluid during orthodontic tooth
movement in adults. World J Ortho;10:141-146.

