a prospective study of hypodermoclysis performed by
TRANSCRIPT

570 Journal of Pain and Symptom Management Vol. 52 No. 4 October 2016
Brief Report
A Prospective Study of Hypodermoclysis Performed by
Caregivers in the Home Setting
Marieberta Vidal, MD, David Hui, MD, Janet Williams, and Eduardo Bruera, MDUniversity of Texas M. D. Anderson Cancer Center, Houston, Texas, USAAbstract
Context. Decreased oral intake is very common at the end of life. Dehydration can aggravate symptoms, such as fatigue,myoclonus, and confusion. Intravenous hydration at home can be logistically difficult and expensive. Hypodermoclysis is easy
to provide and inexpensive; however, it is rarely used to provide hydration at the end of life in the home setting.
Objectives. The purpose of this study was to determine if caregivers were capable of administering hypodermoclysis in the
home hospice setting.
Methods. All caregivers underwent a 45-minute training session on hypodermoclysis administration and assessment of
infusion site delivered by a specially trained nurse. Caregivers received daily calls and on-site evaluation on Day 8.
Results. A total of 21 patient/caregivers dyads were admitted to this preliminary study: 10 (48%) female patients and 16
(76%) female caregivers. All patients had advanced cancer, receiving hospice care at home. All caregivers who received
training were able to start the infusion. The infusion was facilitated by gravity or weight. Side effects were minimal with one
(5%) because of the care of the needle and leakage.
Conclusion. This preliminary study suggests that subcutaneous hydration could be administered by caregivers at home with
minimal burden, equipment, and technical support. J Pain Symptom Manage 2016;52:570e574 � 2016 Published by Elsevier
Inc. on behalf of American Academy of Hospice and Palliative Medicine.
Key Words
Hypodermoclysis, hydration, palliative care, EOL, delirium
IntroductionIn the United States, when oral intake is insufficient
to maintain adequate hydration, most patients withadvanced cancer in traditional hospitals receive paren-teral fluids.1,2 In contrast, advanced cancer patientsreceiving home hospice care almost never receiveparenteral fluid.3,4 Specialists in hospice care argueagainst parenteral fluids and for a less aggressiveapproach to patient care. Furthermore, the per diemhospice funding mechanism makes the administrationof parenteral fluid difficult to finance. Our group haspreviously summarized these arguments for andagainst hydration in terminally ill patients.5e7 The de-cision to give artificial hydration remains highly polar-ized and needs to be personalized.
Address correspondence to: Marieberta Vidal, MD, University ofTexas M. D. Anderson Cancer Center, 1515 HolcombeBoulevard, Houston, TX 77030, USA. E-mail: [email protected]
� 2016 Published by Elsevier Inc. on behalf of American Academy ofHospice and Palliative Medicine.
Artificial hydration has traditionally been givenintravenously and usually with a peripheral line. Theperipheral intravenous (IV) route for hydration maybe problematic for terminally ill cancer patients andposes a potential problem in the home care setting.8,9
Specifically, disadvantages of the IV route for hydra-tion in such patients includes pain associated with nee-dle insertion, the need for frequent site changes,difficulty in finding venous access, the need for immo-bilization of the arm, impediments to mobility, the riskof increasing agitation and accidental catheterremoval in patients with delirium, the need for hospi-talization, high cost, and need for specific training insurveillance and care of complications, such as throm-bophlebitis and infection.10
Accepted for publication: April 29, 2016.
0885-3924/$ - see front matterhttp://dx.doi.org/10.1016/j.jpainsymman.2016.04.009

Vol. 52 No. 4 October 2016 571Hypodermoclysis in the Home Setting
Hypodermoclysis has a low incidence of adverse ef-fects, generally related with local effects, such asswelling, localized pain, and erythema.11,12 Hypoder-moclysis involves the simple and minimally distressfulprocedure of inserting a butterfly needle subcutane-ously and attaching a line for fluids to be administeredvia an infusion pump or gravity in the homesetting.8,10,13,14 In ambulatory patients, the abdomen,upper chest, and area above the breast may be usedas the subcutaneous infusion site. In bedridden pa-tients, preferred sites are the thighs, abdomen, andouter aspects of the upper arm.15e18 In a prospectivestudy conducted at a palliative care unit, the meanduration of a subcutaneous site for the administrationof narcotics was seven days.7 Other potential advan-tages of hypodermoclysis are that it is easy to managein the home care setting and that the tubing can beconnected and disconnected from the needle by pri-mary caregivers after minimal training, it does notrequire expensive and complex infusion pumps, andit has the capability of intermittent administration.
Despite good evidence to support the benefits ofsubcutaneous absorption,7 this once popular routeof fluid administration in the 1940s and 1950s hasmostly been replaced by IV infusion and is rarelyused today in acute care settings in the UnitedStates.13 As a result, many physicians, nurses, patients,and caregivers are unfamiliar with this safe and effec-tive technique. Other than a small report of three pa-tients,19 we identified no studies that specificallyexamined the feasibility of administering hypoder-moclysis by caregivers in the home hospice setting. Abetter understanding of the feasibility of administra-tion of hypodermoclysis can pave the way for routineadoption of this intervention at home. The purposeof this study was to determine if caregivers werecapable of administering hypodermoclysis in thehome hospice setting.
MethodsThis prospective study was an extension of a ran-
domized placebo-controlled trial on parenteral hydra-tion in patients receiving care under one of fourHouston area hospices (Houston Hospice, Odyssey-Conroe Hospice Health Care, Odyssey-HoustonHealth Care, Silverado, and Vitas Hospice Care). Inthe primary study, eligible patients are randomizedto receive either 1000 mL (hydration group) or100 mL (placebo group) of normal saline daily for14 days (35). On completion of that study, patientand caregivers who wished to continue with hydrationwere enrolled onto this extension study. Eligibilitycriteria for the extension study included 1) havingcaregiver who is a spouse, adult child, relative, or
significant other who resides with the patient or pro-vides daily visits, 2) the primary caregiver agreed tobe trained and give fluids, 3) the primary caregivermeets a competency checklist of performing subcu-taneous hydration. This study was reviewed andapproved by the Institutional review Board of theMD Anderson Cancer Center. For all the participants,either the patient or the patient’s power of attorney (ifpatient was unable to consent) signed an informedconsent.
Study DesignPatients received 1000 mL normal saline subcutane-
ously each day by gravity until the patient or primarycaregiver elected to discontinue the hydration or untilthe patient died. The research nurses from theDepartment of Palliative Care and Rehabilitation Med-icine at MD Anderson Cancer Center were responsiblefor the infusions and follow-up assessments during thefirst seven days.The research nurses provided training to family
caregivers and any hospice nurse not yet familiarwith the subcutaneous route. The training was con-ducted according to a set of standardized hypoder-moclysis instructions, which comprised the followingsteps: 1) identification of the needed materials, 2)orientation about hand-washing and procedure clean-liness, 3) preparation of IV tubing and bag, 4) flush-ing, 5) administration of the fluid, 6) assessment ofinfusion site and measuring the amount of fluid given(Appendix A). The training took place in the patient’shome on the day of study registration. It was a one-to-one session that lasted approximately 60 minutes.When requested by the primary caregiver, we providededucation of hypodermoclysis to other adult membersof the household. However, the assessment was onlyconducted in the designated primary caregiverbecause this caregiver was the primary subject forour study. Caregivers were oriented to administer1000 mL of normal saline (0.9% sodium chloride)by gravity or pressure (using body weight method,sitting on, or recumbent over the bag) (AppendixA). A competency checklist (Appendix B) of perform-ing subcutaneous hydration needed to be 100% metbefore caregivers were able to administer fluids inde-pendently. The research nurse called the caregiverdaily, including weekends, to discuss logistics andany concerns. Discussion may involve the reason forfluid discontinuation including logistic reasons forthe caregiver like too stressful, health issues, changein caregiver, etc. Also patient-related reasons like pa-tient refusal, pain, unresponsiveness, actively dyingor perceived futility were addressed.All caregiver received a weekly on-site evaluation by
the research nurse, with as-needed visits in between totroubleshoot. The butterfly needle was placed by the

Table 1Patient and Caregivers Characteristics (n ¼ 21)
Demographics Patients, n (%) Caregivers, n (%)
Age (median, range) 67 (60, 78) 57 (50e66)Gender
Female 10 (48%) 16 (76%)Male 11 (52%) 5 (24%)
EthnicityWhite 9 (43%) 9 (43%)African American 8 (38%) 8 (38%)Hispanic 4 (19%) 4 (19%)
Relationship to patientSpouse 12 (57%)Child 7 (33%)Relative 2 (8%)
Marital statusMarried 15 (71%)Divorced 3 (14%)Single 2 (9%)
Employment statusFull time 4 (19%)Part time 3 (14%)Retired 4 (19%)Unemployed 4 (19%)Other/homemaker 3 (14%)
Level of educationHigh school 6 (29%)Some college/Junior 4 (19%)College graduate 7 (33%)Graduate work 1 (5%)
DiagnosisBreast 1 (5%)Gynecological 2 (10%)Gastrointestinal 9 (43%)Prostate 1 (5%)Lung 2 (10%)Urinary 1 (5%)Skin 2 (10%)Other 3 (14%)
Table 2Infusion Characteristics/Outcomes
Day 1e4(n ¼ 74)
Day 5e7(n ¼ 44)
Duration of daily infusion(hours), median (IQR)
13 (9e14) 17 (11e23)
Method of infusionGravity 68 (92%) 43 (98%)Weight applied to bag þ gravity 4 (5%) 2 (5%)Discontinued infusions 2 (3%) 1 (2%)Reasons for discontinuation
Logistic 0 0Perceived futility 1 (1%) 1 (2%)Side effects 1 (1%)Death 0 0
Caregiver Assessment ofDifficulty Day 8 (n ¼ 18) None At All
A Littleor SomeDifficulty
A Lot ofDifficult
Connecting the bag 18 (100%)Connecting the tubing 18 (100%)Disconnecting the tubing 18 (100%)Get fluid flow 17 (90%) 1 (6%) 1 (6%)Assess infusion site 18 (95%) 1 (6%)Overall difficulty 18 (95%) 1 (6%)Overall stress 18 (100%)
IQR ¼ interquartile range.
Table 3Nurse Assessment of Local toxicity
Toxicities
Days 1e4(n ¼ 76)a
Infusions
Days 5e7(n ¼ 44)a
Infusions
Needle displacement 4 (5%) 1 (2%)Leakage 4 (5%) 0Swelling >0 7 (9%) 3 (7%)Discomfort >0 9 (12%) 5 (11%)Pain >0 3 (4%) 4 (9%)Redness >0 1 (1%) 1 (2%)Itchy >0 4 (5%) 5 (11%)Other >0 1 (1%) 0
aNumber of infusions.
572 Vol. 52 No. 4 October 2016Vidal et al.
research nurse. In the event of side effects that neededon-site intervention, the research nurse visited the pa-tient and took necessary actions to address the issue. Ifthe butterfly needle had to be removed or changed,the research nurse provided further education to thecaregiver.
We collected information on patient and caregiversdemographics. Caregivers received daily phone callsfrom research nurses to assess the following: theamount of fluid given, the duration of infusion, themethod used, infusion sites, related issues includingneedle displacement, leakage, swelling, pain, discom-fort, itching, bruising or any other problems, and theneed for a research nurse visit. The caregiver rates thesymptoms of swelling, discomfort, pain, redness, itch,bruising, and others on a scale of 0 to 10, with 10 beingthe worst possible symptom and 0 no symptoms. Forneedle displacement and leakage, the answer was yes/no. The patients enrolled in the study continue theirroutine care by their hospice physicians and nurses.
Statistical AnalysisWe analyzed the study data by infusion. We summa-
rized the data with descriptive statistics, including
means, medians, interquartile ranges, standard devia-tions, and percentages. To determine the frequenciesof the variables, we used SPSS predictive analyticsoftware.
ResultsA total of 21 patient/caregiver dyads were admitted
to this preliminary study: 10 (48%) patients and 16(76%) caregivers were women. All patients hadadvanced cancer and were receiving hospice care athome. Most patients were married (71%) and theircaregiver was the spouse (57%). The rest of the demo-graphics are described in Table 1.The infusion characteristics are listed in Table 2.
The infusion duration varied between nine to 23 hourswith a median of 13 hours for the first four days and17 hours for the last three days. The majority of the
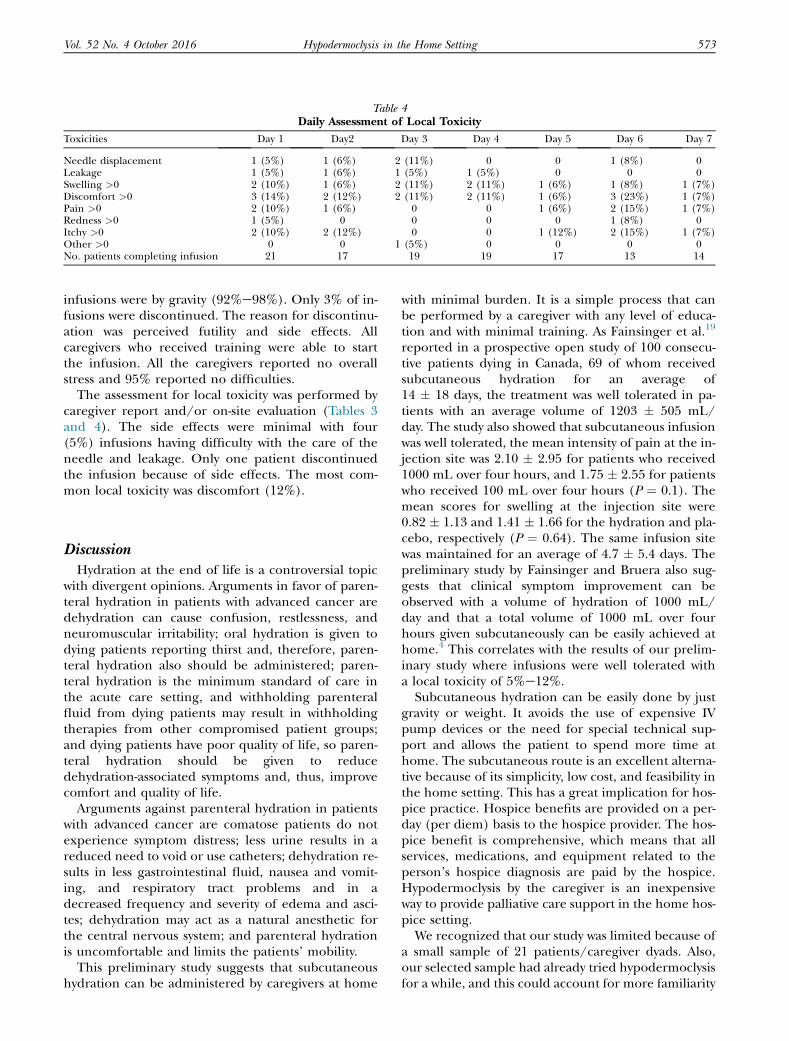
Table 4Daily Assessment of Local Toxicity
Toxicities Day 1 Day2 Day 3 Day 4 Day 5 Day 6 Day 7
Needle displacement 1 (5%) 1 (6%) 2 (11%) 0 0 1 (8%) 0Leakage 1 (5%) 1 (6%) 1 (5%) 1 (5%) 0 0 0Swelling >0 2 (10%) 1 (6%) 2 (11%) 2 (11%) 1 (6%) 1 (8%) 1 (7%)Discomfort >0 3 (14%) 2 (12%) 2 (11%) 2 (11%) 1 (6%) 3 (23%) 1 (7%)Pain >0 2 (10%) 1 (6%) 0 0 1 (6%) 2 (15%) 1 (7%)Redness >0 1 (5%) 0 0 0 0 1 (8%) 0Itchy >0 2 (10%) 2 (12%) 0 0 1 (12%) 2 (15%) 1 (7%)Other >0 0 0 1 (5%) 0 0 0 0No. patients completing infusion 21 17 19 19 17 13 14
Vol. 52 No. 4 October 2016 573Hypodermoclysis in the Home Setting
infusions were by gravity (92%e98%). Only 3% of in-fusions were discontinued. The reason for discontinu-ation was perceived futility and side effects. Allcaregivers who received training were able to startthe infusion. All the caregivers reported no overallstress and 95% reported no difficulties.
The assessment for local toxicity was performed bycaregiver report and/or on-site evaluation (Tables 3and 4). The side effects were minimal with four(5%) infusions having difficulty with the care of theneedle and leakage. Only one patient discontinuedthe infusion because of side effects. The most com-mon local toxicity was discomfort (12%).
DiscussionHydration at the end of life is a controversial topic
with divergent opinions. Arguments in favor of paren-teral hydration in patients with advanced cancer aredehydration can cause confusion, restlessness, andneuromuscular irritability; oral hydration is given todying patients reporting thirst and, therefore, paren-teral hydration also should be administered; paren-teral hydration is the minimum standard of care inthe acute care setting, and withholding parenteralfluid from dying patients may result in withholdingtherapies from other compromised patient groups;and dying patients have poor quality of life, so paren-teral hydration should be given to reducedehydration-associated symptoms and, thus, improvecomfort and quality of life.
Arguments against parenteral hydration in patientswith advanced cancer are comatose patients do notexperience symptom distress; less urine results in areduced need to void or use catheters; dehydration re-sults in less gastrointestinal fluid, nausea and vomit-ing, and respiratory tract problems and in adecreased frequency and severity of edema and asci-tes; dehydration may act as a natural anesthetic forthe central nervous system; and parenteral hydrationis uncomfortable and limits the patients’ mobility.
This preliminary study suggests that subcutaneoushydration can be administered by caregivers at home
with minimal burden. It is a simple process that canbe performed by a caregiver with any level of educa-tion and with minimal training. As Fainsinger et al.19
reported in a prospective open study of 100 consecu-tive patients dying in Canada, 69 of whom receivedsubcutaneous hydration for an average of14 � 18 days, the treatment was well tolerated in pa-tients with an average volume of 1203 � 505 mL/day. The study also showed that subcutaneous infusionwas well tolerated, the mean intensity of pain at the in-jection site was 2.10 � 2.95 for patients who received1000 mL over four hours, and 1.75 � 2.55 for patientswho received 100 mL over four hours (P ¼ 0.1). Themean scores for swelling at the injection site were0.82 � 1.13 and 1.41 � 1.66 for the hydration and pla-cebo, respectively (P ¼ 0.64). The same infusion sitewas maintained for an average of 4.7 � 5.4 days. Thepreliminary study by Fainsinger and Bruera also sug-gests that clinical symptom improvement can beobserved with a volume of hydration of 1000 mL/day and that a total volume of 1000 mL over fourhours given subcutaneously can be easily achieved athome.4 This correlates with the results of our prelim-inary study where infusions were well tolerated witha local toxicity of 5%e12%.Subcutaneous hydration can be easily done by just
gravity or weight. It avoids the use of expensive IVpump devices or the need for special technical sup-port and allows the patient to spend more time athome. The subcutaneous route is an excellent alterna-tive because of its simplicity, low cost, and feasibility inthe home setting. This has a great implication for hos-pice practice. Hospice benefits are provided on a per-day (per diem) basis to the hospice provider. The hos-pice benefit is comprehensive, which means that allservices, medications, and equipment related to theperson’s hospice diagnosis are paid by the hospice.Hypodermoclysis by the caregiver is an inexpensiveway to provide palliative care support in the home hos-pice setting.We recognized that our study was limited because of
a small sample of 21 patients/caregiver dyads. Also,our selected sample had already tried hypodermoclysisfor a while, and this could account for more familiarity

574 Vol. 52 No. 4 October 2016Vidal et al.
with the process. There is a need for further studies inthis area to validate outcomes with a larger sample.
Disclosures and AcknowledgmentsThis research received no specific funding/grant
from any funding agency in the public, commercial,or not-for-profit sectors. The authors declare no con-flicts of interest.
References
1. MacDonald N, Fainsinger R. Indications and ethical con-siderations in the hydration of patients with advanced can-cer. In: Bruera E, Higginson I, eds. Cachexia-anorexia incancer patients. New York: Oxford University Press, 1996:94e109.
2. Bruera E, Belzile M, Watanabe S, Fainsinger RL. Volumeof hydration in terminal cancer patients. Support Care Can-cer 1996;4:147e150.
3. Dunphy K, Finlay I, Rathbone G, Gilbert J, Hicks F. Rehy-dration in palliative and terminal care: if notdwhy not? Pall-iat Med 1995;9:221e228.
4. Fainsinger RL, Bruera E. Hypodermoclysis (HDC) forsymptom control vs. the Edmonton injector (EI). J PalliatCare 1991;7:5e8.
5. Fainsinger RL, Bruera E. The management of dehydra-tion in terminally ill patients. J Palliat Care 1995;10:55e59.
6. Schen RJ. Subcutaneous infusions in the elderly. Br MedJ (Clin Res Ed) 1981;282:823e824.
7. Bruera E, Sala R, Rico MA, et al. Effects of parenteral hy-dration in terminally ill cancer patients: a preliminary study.J Clin Oncol 2005;23:2366e2371.
8. Steiner N, Bruera E. Methods of hydration in palliativecare patients. J Palliat Care 1998;14:6e13.
9. Dalal S, Bruera E. Dehydration in cancer patients: totreat or not to treat. J Support Oncol 2004;2:467e479. 483.
10. Fainsinger RL. Dehydration and rehydration. In:Bruera E, Higginson I, Ripamonti C, von Gunten C, eds.Textbook of palliative medicine. London: Hodder Arnold,,2006:727e735.
11. Frisoli JA, de Paula AP, Feldman D, Nasri F. Subcutane-ous hydration by hypodermoclysis. A practical and low costtreatment for elderly patients. Drugs Aging 2000;16:313e319.
12. Berger EY. Nutrition by hypodermoclysis. J Am GeriatrSoc 1984;32:199e203.
13. Slesak G, Schnurle JW, Kinzel E, Jakob J, Dietz PK. Com-parison of subcutaneous and intravenous rehydration ingeriatric patients: a randomized trial. J Am Geriatr Soc2003;51:155e160.
14. Farrand S, Campbell AJ. Safe, simple subcutaneous fluidadministration. Br J Hosp Med 1996;55:690e692.
15. Lipschitz S, Campbell AJ, Roberts MS, et al. Subcutane-ous fluid administration in elderly subjects: validation of anunder-used technique. J Am Geriatr Soc 1991;39:6e9.
16. Bruera E, Legris MA, Kuehn N, Miller MJ. Hypoder-moclysis for the administration of fluids and narcotic analge-sics in patients with advanced cancer. J Pain SymptomManage 1990;5:218e220.
17. Schen RJ, Singer-Edelstein M. Hypodermoclysis. JAMA1983;250:1694e1695.
18. Waller A, Carolin NL. Subcutaneous infusions. In:Waller A, Carolin NL, eds. Handbook of palliative care incancer. Boston: Butterworth Heinemann, 1996:449e456.
19. Sato K, Karino M, Nishi T, et al. Three elderly patientcases maintained by home hypodermoclysisda practical hy-drating method performed by family members. Gan To Ka-gaku Ryoho 2008;35:185e187.

Vol. 52 No. 4 October 2016 574.e1Hypodermoclysis in the Home Setting
Appendix A
HypodermoclysisHypodermoclysis is a way for a patient to receive fluid that has been lost through vomiting, diarrhea, or sweat-
ing. It is usually used when the patient is too sick to eat or drink. Using a subcutaneous injection (an injectionwhere the needle is inserted just under the skin), a caregiver may give a patient saline or another solution.
Equipment
You will receive supplies or instructions on whereto purchase supplies from your hospice nurse. Collectand organize the supplies on a clean, dry surface. Youwill need the following:
� Hypodermoclysis solution as ordered by the physician� Intravenous (IV) tubing set� Seventy percent isopropyl alcohol swab� Hammer, nail, and coat hanger (depending on how thepatient is receiving the injection)
� Pillow and tray (depending on how the patient isreceiving the injection)
Before You Begin
1. Wash your hands, and close the clamp on the IV tubing. Remove the plastic tab from part at the bottom of the IV bag. Youmay not touch the port after it is opened.
2. Remove the plastic cover from the tubing spike and insert it into the port. You may not touch the IV tubing spike. If you dotouch the spike, it will be contaminated, and then you must start over using a new sterile set.

574.e2 Vol. 52 No. 4 October 2016Vidal et al.
3. Finally, squeeze the drip chamber of the IV tubing to fill half of the chamber. Open the clamp, and fill the tubing withfluid. Then, close the clamp when the tubing is full.
4. Check the skin where the needle is located. Make sure that there is no pain, redness, swelling, or leaking from the skin.

Vol. 52 No. 4 October 2016 574.e3Hypodermoclysis in the Home Setting
Procedure Instructions
5. Wipe the heparin lock with the alcohol wipe. Remove the cap from the tubing and insert it into the butterfly tubing. Makesure that the connection is tight.
MethodsThere are two methods available for you to administer fluiddthe gravity method and the body weight method.
Choose the method that is easier and more comfortable for the patient.

574.e4 Vol. 52 No. 4 October 2016Vidal et al.
The gravity method uses the force of gravity to drain fluid out of the IV fluid bag and into the patient. (Thepatient may sit or lie down.)
The body weight method uses force from the patient sitting on the IV fluid bag to push fluid into the patient.(The patient must be able to sit and stand repeatedly for this method. If the patient cannot, then someone elsemay follow the steps for sitting on the IV bag for the patient.)
Gravity Method
Continued From Step 56. One way to hang the bag is with a coat hanger, hammer, and nail.
7. Start the infusion fluid and regulate the infusion rate so that the patient receives no more than 500 cubic centimeters (cc)per hour (cc/hr). The clamp may be opened, and gravity will cause the fluid to flow.

Vol. 52 No. 4 October 2016 574.e5Hypodermoclysis in the Home Setting
8. Skip to Observation section of these instructions.
Body Weight Method
Continued From Step 56. Place the fluid bag on a hard surface horizontally, like on a chair. Place a pillow on top of the bag. Place a tray on top of thepillow. (You may use another hard, flat surface like a board if you do not have a tray.) The patient should then sit on thetray. (Someone else may follow the steps for sitting and standing if the patient cannot do this.)
7. Open the clamp halfway. After 10 minutes have passed, stand up and remove the tray and pillow. Pick up the IV fluid bagand hold it with both hands at eye level. If the patient has received more than 100 cc of fluid, then close the clamp slightlyby turning a half-turn down. If the patient has received less than 100 cc of fluid, then open the clamp slightly by turning ahalf-turn up.

574.e6 Vol. 52 No. 4 October 2016Vidal et al.
8. Replace the bag on the chair, the pillow on top of the bag, and the tray on top of the pillow. The patient (or helping per-son) should resume sitting on the bag.
9. Repeat Steps 7 and 8 until the patient has received 600 cc of fluid.
10. After the patient has received 600 cc of fluid or after 90 minutes have passed, close the clamp slightly by turning ahalf-turn down.

Vol. 52 No. 4 October 2016 574.e7Hypodermoclysis in the Home Setting
11. Close the clamp completely. Disconnect the IV fluid bag from the administration set. The site will appear somewhatswollen but should not be painful.
12. Your physician or nurse will indicate if more or less amount of fluid may be needed according to patient’s medicalcondition.

574.e8 Vol. 52 No. 4 October 2016Vidal et al.
ObservationObserve the site every eight hours or as needed for redness, bruising, swelling, tenderness, leaking, or apus-like discharge.If you have questions or experience any problems, contact your hospice nurse.

Vol. 52 No. 4 October 2016 574.e9Hypodermoclysis in the Home Setting
Appendix B
Today’s date:____________Patient number ____________Caregiver number ____________Protocol Acc# ____________
Caregiver Subcutaneous Hydration Checklist
Equipment Solution
IV tubing set
Alcohol swab
IV pole/other device
Flush syringe
Preparation
Wash Hands
Clamp IV tubing
Remove plastic tab of the IV bagwithout contamination
Remove plastic cover from tubingspike without contamination
Insert tubing spike into the port of IV bag
Prime the tubing
Assess skin
Procedures
Wipe heparine lock with the alcohol wipe
Remove the cap from the tubing
Insert IV tubing into the butterfly tubing
Check for tightness
Flush the butterfly tubing
Regulate the infusion rate
Close the clamp at the end of infusion
Disconnect the IV fluid bag fromthe butterfly tubing
Measure the amount of fluid given
IV ¼ intravenous.