a rapidly emerging sub-specialty requires dedicated ... · a rapidly emerging sub-specialty...
TRANSCRIPT


A rapidly emerging sub-specialty
Requires dedicated training and consistent
exposure to become proficient
That being said…
› We as general sonographers often encounter
MSK in our day-to-day exams
› This lecture will cover a few generalist exam
scenarios where some basic MSK knowledge
can go a long way in understanding the clinical
picture.

Superficial masses
Achilles Tendon
Baker’s cyst
Peripheral nerves

Our lumps and bumps exams
Keys to assessment:
› Patient history
› Location
› Morphology
Size
Vascularity

Patient History: › Clinical questions:
How long have you had it?
Was there an injury?
Has it changed in size? (bigger or smaller)
It is painful?
The answers to these questions plus the imaging characteristics give the radiologist an index of suspicion about a given mass and which recommendations to make as to follow up.

Location:
› Tissue Layers
Skin: made up of epidermis and dermis
Subcutaneous tissue aka hypodermis or fat
layer
Muscle

Skin
› Thin and hyperechoic
› Lesions involving the skin layer often need
imaging with a standoff pad to optimize focal
zone and appreciate
outward mass effect
› Warts, calluses,
hemangiomas

Fat layer
› Variable in thickness
› Made up of ‘fat islands’, connective tissue,
blood vessels and lymphatic channels
› Common location
for lipomas, abcesses,
hematomas, bursitis
and ganglions.

Muscle layer › Generally hypoechoic with echogenic fascial
lines though muscle; can become echogenic with disuse and atrophy.
› Exhibits a striated pattern in long axis and well formed muscle fibers are capable of demonstrating anisotropy (change in echogenicity based on angle of insonation)
› Masses can form a mass effect upon the adjacent muscle or can directly invade/arise from the muscle
Side-to-side comparison most beneficial
Be aware of tissue/fascial planes


Morphology: › Sonographers are already well equipped to
describe the characteristics of any lesion they find
Cystic vs solid
Ill-defined vs well circumscribed,
Heterogenous vs homogenous
Presence of any vascularity
Size
What can be improved upon is describing the location of these superficial masses › Subcutaneous vs intra-muscular
› Any invasion into surrounding tissue?

› Lipomas
Variable in size and echogenicity (echogenic –
isoechoic)
Most frequently subcutaneous but can also be
intra-muscular in origin
Note should be made of lipomas that are
growing, painful and/or exhibit internal
vascularity – may need follow up

Subcutaneous
lipoma


Intra-
Muscular
Lipoma


› Focal fluid
Abcess
Hematoma
Bursitis
Inflammation of a bursal sac of synovial fluid
Ganglions/Synovial cysts
Caused by leakage of fluid from a joint or tendon sheath
into the surrounding tissue

Very similar imaging characteristics › Often an irregular subcutaneous fluid collection
Abscess – simple fluid or debris filled, may contain air or exhibit increased peripheral vascularity
Hematoma – variety of appearances depending on stage, can look simple or solid or combined
Patient history key › Abscess – red, inflamed skin, possible open
wound and discharge
› Hematoma – history of trauma, likely bruising and pain over site

Subcutaneous
Hematoma
(history of injury)

Bursal sacs lie through out the body offering
cushion and protection against friction.
Inflammation of this sac leads to excess
synovial fluid = fluid collection
Patient history
› Pain
› Possible swelling
› Often chronic, variable in severity

Painful swelling around
the knee
- No hx of trauma
- Not a hematoma
- Not assoc w/ the joint
- Not a ganglion
Bursitis

- Most often associated with tendons/joints of the
hands and feet
- Predominately cystic, may have a thickened
rim/septations which may have increased vascularity

- Demonstrate the origin if
possible
- Often change in size
- Can be painful

› Nerve tumors
Painful, results in numbness or tingling
Probe pressure reproduces symptoms
Can often be seen to directly arise from an
adjacent nerve
Has a ‘tail’ or trumpeted ends

Nerve
Nerve splaying around
the lesion

Nerve
Nerve splaying around
the lesion

Only in long axis
can you determine
that this lesion is
arising from the
nerve

› Mysterious masses
Asymmetric tissue layers Often fat but no focal lipoma
Compare side to side to appreciate layer differences
Muscle hernia Often due to a weakness or defect in the fascia
Dynamic scanning a must
Nothing Patients often palpate ‘lumps’ where there is no
corresponding abnormality – often palpating normal muscle anatomy, etc
Compare side to side

Patient complaint:
Lump over scapula
on left
Lump was her
scapula – more
outwardly
prominent

Herniation of
muscle thru
fascial defect
Normal

Dynamic scanning shows mass change with muscle contraction

Patients who complained of a ‘fullness’ or asymmetry
to their back
Unable to palpate specific mass at time of exam,
panoramic reveals equal tissue planes

› Other….
Numerous superficial mass types (benign and
cancerous) – ultrasound alone cannot distinguish
(may need MRI and/or biopsy)
Ultrasound can start the analysis
Solid vs. cystic
Vascular?
Invasive?

When in doubt:
Measure, color, clip
and give rough location

Superficial masses
Achilles Tendon
Baker’s cyst
Peripheral nerves

In regards to emergent requests post trauma; Query Tear › Often come from emergency departments and
to a lesser extent GP’s offices
Where possible these patients are being sent to dedicated MSK centers as many radiologists prefer to have them performed/read by MSK specialized staff.
However, this is not always feasible – there is a finite surgical window to consider (7-10 days)
These patients can’t necessarily wait to be shuffled around and re-booked.

› Achilles used to be done under general
ultrasound before MSK became its own field
› Can and is being done under general if the
technologist is able and the radiologist is willing
› Following a few key points when evaluating the
Achilles eliminates many possible pitfalls and
results in more consistent results.

Anatomy: Attaches the gastroc
(medial and lateral heads) and soleus muscles to the calcaneus
Broad and thin proximally at its origin mid calf – overlying the soleus muscle
Thickens and becomes fully formed distally, inserting on the posterior calcaneus

Key exam features
› Is there a tear? Evaluate the Achilles tendon in long and short axis
Majority of traumatic tears occur between the distal soleus and the calcaneus
Therefore most helpful to start where its normal (the
calcaneus) and work your way up.
A torn tendon retracts causing thickening and
heterogeneity to the torn ends (often includes
shadowing)
Debris and hemorrhage fills the gap *will have no
normal linear strands

Normal
Achilles
Torn Achilles Tendenotic Achilles
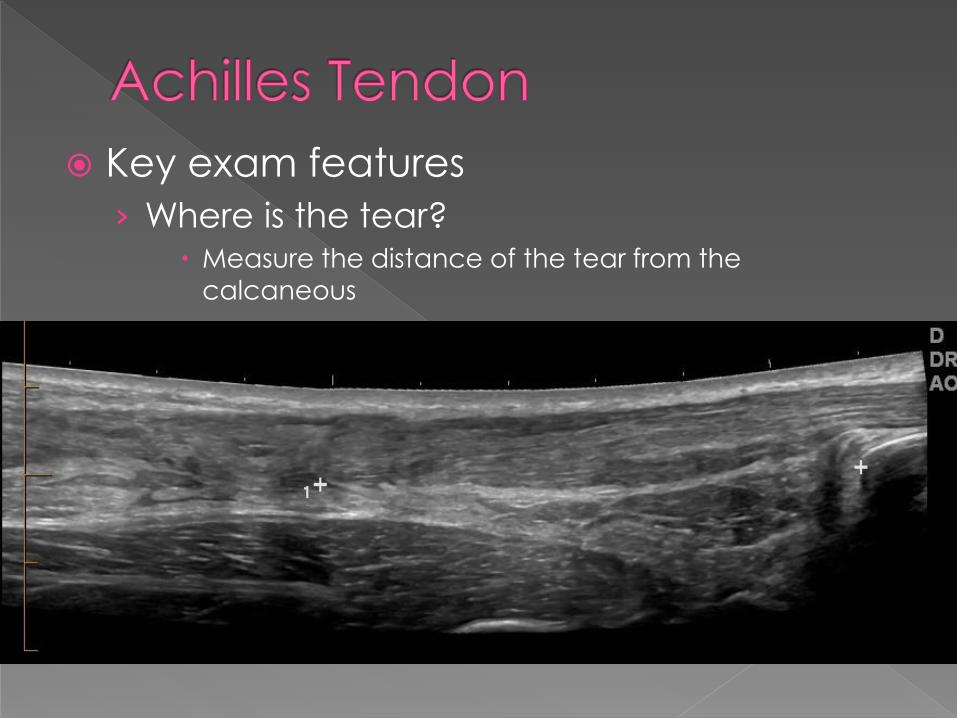
Key exam features
› Where is the tear? Measure the distance of the tear from the
calcaneous


Key exam features › Complete or partial tear?
Sweep side to side in long axis through the tear to look for any residual fibers
Take long and short axis clips through the tear to demonstrate the changes more clearly
› Functional tests:
Squeezing the calf = moves the proximal stump while the distal stump remains motionless = complete tear
Plantar/dorsi-flex the foot = moves the distal stump while the proximal stump remains motionless = complete tear

Normal Long Axis Achilles
Complete tear with
hematoma filling gap

Normal Short Axis
Achilles
Complete tear with
hematoma filling gap

Partial tear of Achilles.
Could be mistaken
for a complete tear in
long axis.

Key exam features
› Measure the tear
Long axis most important surgically
Can gently plantar/dorsi-flex the foot to help
define the edges of the tear
Measure the gap in neutral and again with
plantar flexion
Some tears are treated with a boot instead of surgery
if the tendon ends are closely approximated with
plantar flexion
Short axis measure if tear is partial



Not everyone has one
Lies adjacent and medial to the achilles
Most easily identifiable in short axis by
scanning the achilles over the soleus
muscle and focusing on the medial border
› Appears as a small, separate oval structure in
the same fascial plane
PITFALL:
› An intact plantaris tendon can mimic intact
medial achilles fibers


Can be used surgically to help repair the
achilles
Check if the patient has one
› Does it bridge the tear?

Can occur simultaneously with an
achilles tear or mimic an achilles tear by
presenting with similar symptoms
Medial gastrocnemius most commonly
torn
› Feels like a kick or shot to the calf
› Patient has focal pain over the medial calf
Distal soleus may also be partially torn
with a high achilles tear

Anatomy

› Muscle fibers like tendon fibers should be linear
› Musculo-tendinous junctions should be sharp and angular
› Muscles should
have thin fascial
planes separating
them



› Tears:
Bunching and curling of muscle fibers Often with hematoma formation in the acute phase
*Compare to opposite side for confirmation*
Medial gastroc
tears often involve a
fascial tear/separation
from the soleus with
hematoma tracking
up the calf between
the two muscles

› How to document:
Image the distal musculo-tendinous junctions of
medial/lateral gastroc and soleous in both planes
*Scan through the muscle*
Measure any hematoma formation in three planes
Document any suspected muscle tears with static
and clip imaging
Patient can always be rescanned at a dedicated
MSK facility if clarification is needed but finding the
problem is the first step.

Long axis imaging of
the medial gastroc on the
same patient
SWEEP THROUGH
THE MUSCLE!


› While non-surgical, these tears can cause
significant pain and weakness causing the
patient to require a course of rest and
sometimes physio to ensure proper healing
› Missing these tears results the patient in trying to
resume activity too soon on the basis of a
normal achilles exam.

Superficial masses
Achilles Tendon
Baker’s cyst
Peripheral nerves

Cause of posterior knee pain and swelling
Often found incidentally during the course of a DVT study
Occasionally cystic collections at the back of the leg are not Baker’s cysts, many are similarly benign synovial cysts of the knee joint but rarely they can be a sarcoma
Simple land marking of these posterior cysts can ensure that we don’t make that miss-diagnosis.

Posterior knee
anatomy
The neck of a
Baker’s cyst originates
from between the
medial gastroc muscle
and semimembanous
tendon at the medial
aspect of the post knee


Originate lateral to semimembranosus tendon
And medial to
medial gastroc muscle

Key exam features:
› Identify fluid collection
Can be simple or complex
Can be multi loculated
Can extend superiorly or inferiorly from the
knee joint or both
› Measure in three planes
› PUT ON COLOR


Key exam features:
› Verify location
Axial plane
Follow the medial border of the medial
gastroc up to the knee joint
The cyst should originate from between the medial
gastroc muscle and semimembranosus tendon
(hamstring).
› Cysts/masses in any other location must be
considered to not be Baker’s cysts


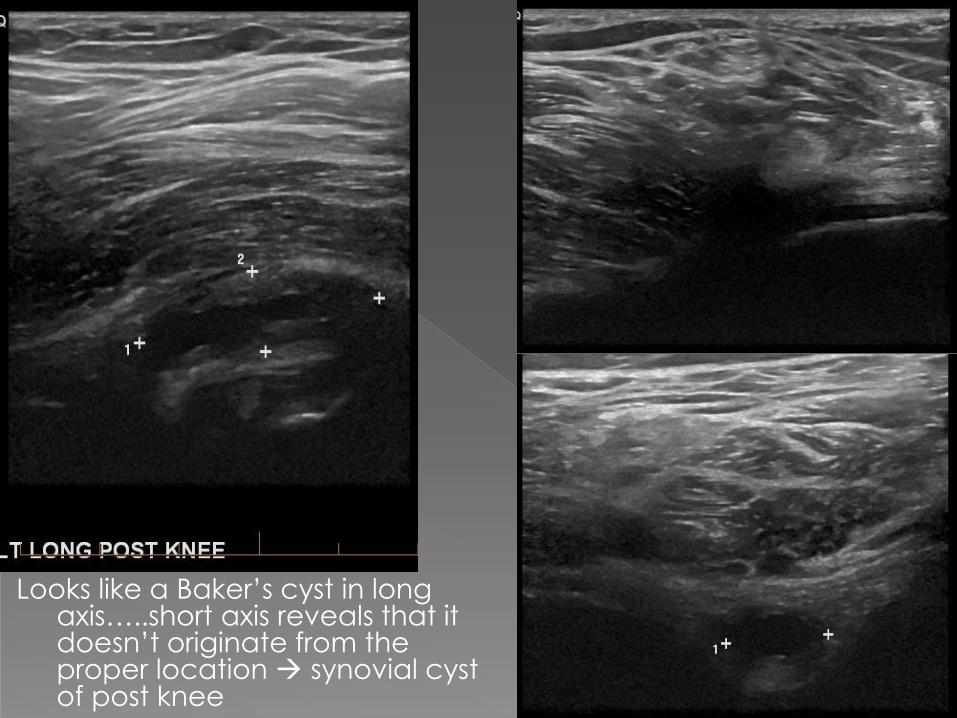
Looks like a Baker’s cyst in long axis…..short axis reveals that it doesn’t originate from the proper location synovial cyst of post knee

3yo with a Baker’s cyst
that was compressing
his popliteal vein with
leg extension

Superficial masses
Achilles Tendon
Baker’s cyst
Peripheral nerves

Neurovascular bundle:
› Consist of a nerve, artery, vein and lymphatics that travel together in the body.
› Example: brachial,
posterior tibial, etc.

Brachial neurovascular bundle
› Most problematic in terms of upper limb
venous ultrasounds to assess for clot.
› Many venous anatomical variations in the upper limb
Duplicated axillary vein
Variable origin of basilic vein
Single brachial vein

Brachial neurovascular bundle › The median nerve also courses alongside the
brachial artery and can easily be mistaken for a thrombosed brachial vein - especially in a case where only one brachial vein exists. (leading to a diagnosis of DVT where none exists)
› This can be avoided by learning to recognize peripheral nerves and their locations in the body.

Are most easily recognized in cross section
Have a ‘pediatric ovary’ appearance by being comprised of multiple small hypoechoic fascicles separated by echogenic fascia.
These fascicles can become dilated and therefore resemble a thrombosed vein as they are without flow and are non-compressible.

Normal neurovascular bundle

Long axis nerve
- can be difficult to differentiate from surrounding tissue
- can still appreciate echogenic fascia separating the fascicles – more uniform than a thrombosis

Thickened hypoechoic nerve (on the right) adj. to an artery (veins compressed in this view)
Nerve would not show flow – could be mistaken for a thrombosed vein

Test Time…
Basilic Vein
Brachial A Brachial V
Nerve or Vein?

Look for the ‘ovary’, try scanning up and down the
upper arm – no matter the venous configuration,
Every person will have a median nerve
Basilic Vein
Brachial A
Brachial V
Median Nerve
