a review of the prescribing capability of speech ... · a review of the prescribing capability of...
TRANSCRIPT

A review of the prescribing capability of speech pathologists, dietitians and
psychologists
This report has been prepared on behalf of the Allied Health Professions’ Office of Queensland by the School of Clinical Sciences,
Queensland University of Technology
Professor Lisa Nissen
Karen Bettenay

Page | 2 A review of the prescribing capability of speech pathologists, dietitians and psychologists
CContents Executive Summary ........................................................................................................................... 4
Terminology and Definitions ............................................................................................................ 10
List of tables and figures .................................................................................................................. 12
List of Abbreviations ........................................................................................................................ 14
1. Introduction ............................................................................................................................. 15
2. Non-Medical Prescribing in Australia ........................................................................................ 15
2.1 Drivers for non-medical prescribing .................................................................................. 15
2.1.1 Population growth........................................................................................................ 15
2.1.2 Ageing population ........................................................................................................ 15
2.1.3 Chronic disease and multiple morbidities ..................................................................... 16
3. The Health Professionals Prescribing Pathway .......................................................................... 16
4. National Prescribing Competencies .......................................................................................... 17
5. Allied Health Prescribing in Queensland ................................................................................... 18
6. Speech Pathology ..................................................................................................................... 19
6.1 Background Information .................................................................................................. 19
6.1.1 National Bodies/Registration ........................................................................................ 19
6.1.2 Education and Training ................................................................................................. 19
6.1.3 Current Prescribing Status ............................................................................................ 19
6.1.4 Prescribing potential .................................................................................................... 19
6.2 Prescribing Competence in Speech Pathology .................................................................. 20
6.2.1 Speech pathology training requirements and professional standards which define professional capability .............................................................................................................. 20
6.3 Speech Pathology Competency Mapping .......................................................................... 20
6.3.1 Methodology................................................................................................................ 20
6.3.2 Results ......................................................................................................................... 21
6.3.3 Discussion .................................................................................................................... 48
6.4 Recommendations ........................................................................................................... 50
7. Dietetics and Nutrition ............................................................................................................. 52
7.1 Background Information .................................................................................................. 52
7.1.1 National Bodies/Registration ........................................................................................ 52
7.1.2 Education and Training ................................................................................................. 52
7.1.3 Current Prescribing Status ............................................................................................ 53
7.1.4 Prescribing potential .................................................................................................... 53
7.2 Prescribing Competence in Dietetics ................................................................................ 53

Page | 3 A review of the prescribing capability of speech pathologists, dietitians and psychologists
7.2.1 Dietitian training requirements and professional standards which define professional capability .................................................................................................................................. 53
7.3 Dietetic Competency Mapping ......................................................................................... 54
7.3.1 Methodology................................................................................................................ 54
7.3.2 Results ......................................................................................................................... 54
7.3.3 Discussion .................................................................................................................... 81
7.4 Recommendations ........................................................................................................... 84
8 Psychology ............................................................................................................................... 85
8.1 Background information................................................................................................... 85
8.1.1 National Bodies/Registration ........................................................................................ 85
8.1.2 Education and Training ................................................................................................. 86
8.1.3 Areas of endorsement of registration ........................................................................... 88
8.1.4 Current Prescribing Status ............................................................................................ 88
8.1.5 Prescribing Potential .................................................................................................... 88
8.2 Prescribing Competence in Psychology ............................................................................. 89
8.2.1 Psychology training requirements and professional standards which define professional capability .................................................................................................................................. 89
8.3 Psychology Competency Mapping .................................................................................... 90
8.3.1 Methodology................................................................................................................ 90
8.3.2 Results ......................................................................................................................... 91
8.3.3 Discussion .................................................................................................................. 119
8.4 Recommendations ......................................................................................................... 121
9 References ............................................................................................................................. 123
Appendix A: Speech Pathology Mapping ........................................................................................ 126
Appendix B Dietitian Mapping ....................................................................................................... 178
Appendix C: Psychology Mapping .................................................................................................. 216

Page | 4 A review of the prescribing capability of speech pathologists, dietitians and psychologists
EExecutive Summary Introduction
Prescribing is a complex task which involves a combination of specific skills, knowledge and behaviours and includes both cognitive and decision making steps.
In order to safeguard patient safety, it is necessary to ensure that any health professional authorised to prescribe is competent to do so. This report aims to review current capabilities of speech pathologists, dietitians and psychologists, and determine competency areas that require additional training before a prescribing role can be considered.
Background
The role and authorisation to prescribe in Australia has traditionally been held by medical and dental practitioners. Over the last few years a number of other health professions have gained authority to prescribe under state legislation. Drivers for non-medical prescribing include a growing and ageing population, increase in the incidence of chronic disease states and increasing use of multiple drugs to treat such diseases.
In order to provide a nationally consistent approach to non-medical prescribing in Australia, Health Workforce Australia published the Health Professionals Prescribing Pathway (HPPP) in 2013(1). This pathway provided a prescribing framework for non-medical prescribers and defined three safe prescribing models:
Autonomous prescribing Prescribing under supervision Prescribing via a structured prescribing arrangement
In addition to establishing a prescribing pathway for non-medical prescribers, it is imperative to establish safe and effective prescribing practice and ensure that all practitioners are competent in their prescribing role. In 2012 the National Prescribing Service (NPS) published ‘Competencies Required to Prescribe Medicines -Putting quality use of medicines into practice’, this national Prescribing Competencies Framework is tailored specifically to the Australian healthcare system(2). The framework has seven competency areas, each of which is divided into elements which describe the specific processes, actions and tasks that health professionals carry out when prescribing. The elements are further broken down to performance criteria which describe observable behaviours or results that are expected of competent prescribers(2).
The Ministerial Taskforce on health practitioner expanded scope of practice: final report (3), found that allied health professionals within Queensland Health were not performing the full range of duties and tasks appropriate to their level of education and training, and that expanding the scope of practice of allied health professionals could improve patient access to services and outcomes for the community. The report detailed a number of areas that scope of practice could be extended, including prescribing, and gave a number of allied health prescribing examples.
In Queensland the authority to prescribe is legislated under the Health (Drugs and Poisons) Regulation 1996 (HDPR)(4). Any prescribing by allied health professionals in Queensland, not already authorised under the HDPR, must be undertaken within a formal research framework. Approval of the Chief Health Officer, under section 18 of the HDPR, must be obtained to enable individual health

Page | 5 A review of the prescribing capability of speech pathologists, dietitians and psychologists
professionals to prescribe. The Allied Health Professions’ Office of Queensland have developed a framework which describes the process by which such trials can be implemented(5).
In order to consider the prescribing potential of the speech pathologist, dietitian and psychologist and to identify options in Queensland relating to prescribing authority, it is necessary to review the current status of each discipline’s qualifications, and evaluate their capacity to provide the skills, knowledge and behaviours necessary to become a competent prescriber. If the current training requirements and professional standards for speech pathologists, dietitians and psychologists are mapped against the Prescribing Competencies Framework, it will be possible to evaluate the current prescribing capability and identify any gaps in capability that may need to be addressed.
Project Methodology
Program of study requirements for each discipline were reviewed, and relevant professional and practice standards were identified. These standards were mapped against individual performance criteria for every element within the Prescribing Competencies Framework. Each performance criteria was described as being covered sufficiently, partly or not covered by the discipline specific standards.
In addition, the performance criteria of the Prescribing Competencies Framework were mapped against the HPPP models of prescribing. This made it possible to identify the competency expectations dependent on the model of prescribing. By comparing this to the discipline specific mapping it was possible to identify current gaps in practice for each of the disciplines under each prescribing model.
To provide additional education and training information relevant to the review, the learning objectives from a representative program of study for each discipline were also mapped against the Prescribing Competencies Framework elements.
It should be noted that the education requirement for general registration as a psychologist is a 6 year sequence of study that can be achieved by a number of different routes. For the purpose of this report the Master’s degree route to general registration and the four year accredited sequence of study followed by a two year Board approved internship (4 + 2) were the only two training and education options reviewed.
Results
As would be expected, mapping for each discipline varied. There were, however, common areas that mapped well, and common areas where gaps in practice were potentially identified.
Areas that mapped well include:
Communication style and therapeutic partnership with patients and carers Respect for the person being treated Provision of information to, and collaboration with, other health professionals Clinical examination and interpretation of findings Synthesising information from assessment and developing possible diagnoses Recognising when non pharmacological treatment is appropriate Referral when treatment is outside scope of practice Developing a treatment plan in partnership with the person Development of a review plan

Page | 6 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Working within scope of practice Knowledge and compliance with professional standards and codes of conduct Accountability for patient care
Ares that did not map well include:
Ascertaining that information has been understood correctly Confirming understanding of information provided by other health professionals Application of Quality Use of Medicine (QUM) principles Obtaining approval for medicine use Providing appropriate medicine orders Stopping or modifying current treatment Ensuring all parties have a common understanding of therapeutic goals and their management Ensuring the person understands the treatment plan and how to use medicines safely and
effectively Identifying if the person requires a comprehensive medicines review Interpretation and application of guidelines and protocols
Mapping of the HPPP models of prescribing to the Prescribing Competencies Framework indicates that the requisite competencies to prescribe safely and appropriately are dependent on the model of prescribing in use. The number of competencies required to prescribe under supervision or autonomously is greater than those required to prescribe via a structured prescribing arrangement.
The mapping of learning outcomes again varied between disciplines but the following could not be identified across any of the professions reviewed:
Element 4.1: Provides clear instructions to other health professionals who dispense, supply, or administer medicines prescribed for the person
Element 5.1: Obtains information to assess the person’s response to treatment Element 5.2: Works in partnership with the person and other health professionals to address
issues arising from the review Element H1.6: Addresses the potential for bias in prescribing decisions Element H2.1: Obtains consent to provide clinical services to the person
Element H1.4 (practices quality use of medicines principles) could not be identified in the learning outcomes of speech pathology, dietetics or the 4+2 study route for psychology, but could be identified in the Masters’ route to psychology registration.
Mapping of the learning objectives for the representative pre-entry program of study provided limited information to assess graduate capability with respect to prescribing. The learning objectives are quite broad in their statements and, without review of individual lectures and tutorials, it is impossible to say to what extent they map with the Prescribing Competencies Framework. Mapping at an element level rather than a performance criteria level is also less specific; not all performance criteria within the element may be covered by the learning objectives. This mapping does, however, give an indication of the current coverage of the Prescribing Competencies Framework by an accredited program of study.

Page | 7 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Discussion
The prescribing capability assumptions made in the mapping process are based purely on information obtained from discipline specific professional and practice standards, and not on review of actual practice. It is likely that some of the prescribing activities that do not map well are undertaken in actual practice but, due to their lack of documentation in the professional standards, are perceived not to map to the Prescribing Competencies Framework. However, there were identified gaps in practice, specifically relating to medicines, which are likely to fall outside of the current scope of practice, and should be targeted for additional education and assessment.
The requisite competencies for safe and effective prescribing differ, dependent on the model of prescribing to be used. The number of competencies required to prescribe under supervision or autonomously is greater than those required to prescribe via a structured prescribing arrangement. The additional training required to achieve prescribing competence, dependent on the model of prescribing, was identified for each profession. Although there were slight variations between professions, common training requirements to prescribe via a structured training arrangement would include:
Medication history taking training, including adherence assessment Interpretation and application of guidelines and protocols appropriate to model of
prescribing QUM principles appropriate to model of prescribing Knowledge of potential adverse reactions and errors of medicines to be prescribed Identification of potential problems with existing medicines and cessation or adjustment as
appropriate Legislation, policies and procedures applicable to model of prescribing Writing of medicine orders appropriate to model of prescribing Recording keeping with respect to medicine use Review of medicine therapy Identification of person’s need for comprehensive medicines review Communication with the person regarding medicine choice, safe and effective use of the
medicine and experience with medicine use Consulting other health professionals with respect to medicine choice
Common additional training requirements to prescribe autonomously or under supervision include:
Knowledge of pharmacology, clinical medicine and therapeutics Access, interpretation, evaluation and application of medicine information to inform
evidence based decision making Identification of appropriate medicine options for both the condition and the person being
treated Tailoring of medicine to the person’s needs Consideration of cost of medicines to be prescribed Implication to the wider community with respect to prescribing Communication with the person with respect to opinions and preferences regarding
medicines and the treatment plan Communication with respect to medicines options and reaching agreement with the person

Page | 8 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Ethical issues with respect to prescribing Provision of verbal orders appropriate for model of prescribing if required Obtaining approval for medicine use if required
The training required to prescribe via a structured prescribing arrangement could be incorporated into pre-entry programs of study with minimal adjustment. Authority to prescribe under supervision or autonomously requires additional training, which could be provided in the way of postgraduate training with appropriate assessment and credentialing to ensure competency. The majority of the competencies are not profession specific, so there is the possibility of the development of a generic allied health prescribing course, which could be provided in combination with workplace supervision and mentoring in order to train and subsequently assess allied health prescribers. Over time it may be possible to incorporate all aspects of prescribing into pre-entry programs of study.
In order to progress the introduction of speech pathology, dietitian and psychology prescribing, processes around the accreditation of prescribing training programs and recognition of prescriber status need to be developed. The Australian Health Practitioner Regulation Agency (AHPRA) has established a Prescribing Working Group whose aim is to ‘develop a governance framework and other resources to support the development and review of national board regulatory policy relating to prescribing of scheduled medicines’(6). This working group provides a useful mechanism to facilitate active collaboration between health professions and the Health Profession Accreditation Councils’ Forum, which is working with its members to develop accreditation processes.
Recommendations:
If prescribing is to occur in these disciplines, consideration needs to be given to the process by which individual health professionals are recognised as competent to prescribe.
As discussed previously, in Queensland the authority to prescribe is legislated under the Health (Drugs and Poisons) Regulation 1996 (HDPR) therefore, amendments to the regulation would be required to authorise specific allied health professions to prescribe. As a temporary measure, prescribing could occur within Queensland under the section 18 approval process, which has been used previously to authorise prescribing trials in pharmacy and physiotherapy.
In addition, if prescribing is to occur at a national level, professional standards should be revised to include prescribing competencies. Amendments to the relevant medicines regulation in each state and territory would also be required.
In order to progress prescribing for speech pathology and dietetics it is recommended that the respective professional bodies:
Develop or adopt an accreditation framework and use it to accredit prescribing training programs
Establish a process for credentialing health practitioners within their profession to prescribe, dependent on completion of an accredited prescribing program of study
To maintain continuing professional development standards and currency of practice, only Certified Practising Speech Pathologists and Accredited Practising Dietitians should be credentialed to prescribe.
In order to progress psychology prescribing it is recommended that:

Page | 9 A review of the prescribing capability of speech pathologists, dietitians and psychologists
The Australian Psychology Accreditation Council (APAC) develops or adopts an accreditation framework and uses it to accredit prescribing training programs suitable for psychology prescribing
The Psychology Board of Australia (PsyBA) seeks Australian Health Workforce Ministerial Council approval, under section 14 of the National Law, to enable the Board to endorse the registration of a psychologist for scheduled medicines
The Psychology Board of Australia (PsyBA) approves, under section 35(1)(d) of the National Law, an accredited program of study as providing qualifications for endorsement

Page | 10 A review of the prescribing capability of speech pathologists, dietitians and psychologists
TTerminology and Definitions Prescribing
There are many definitions of prescribing; some having a legislative basis and some a more practice oriented focus. For the purpose of this document we will use the definition of prescribing from the Health Professionals Prescribing Pathway (HPPP), which defines prescribing as ‘an iterative process involving the steps of information gathering, clinical decision-making, communication and evaluation, which results in the initiation, continuation or cessation of a medicine’(1).
Medicines
In the broadest sense, a medicine includes any chemical substance given with the intention of preventing, diagnosing curing, controlling or alleviating disease or otherwise enhancing the physical or mental welfare of people(7). This includes prescription, non-prescription and complementary health care products, irrespective of the administered route.
The scheduling of medicines is a national classification system that controls how medicines and poisons are available to the public. All medicines and chemical are classified in the Standard for the Uniform Scheduling of Medicines and Poisons(8). In terms of therapeutics the main schedules are as follows:
Schedule 2: Pharmacy medicine-Substances, the safe use of which may require advice from a pharmacist and which should be available from a pharmacy or, where a pharmacy service is not available, from a licensed person.
Schedule 3: Pharmacist only medicine- Substances, the safe use of which requires professional advice but which should be available to the public from a pharmacist without a prescription.
Schedule 4: Prescription only medicine-Substances, the use or supply of which should be by or on the order of persons permitted by State or Territory legislation to prescribe and should be available from a pharmacist on prescription.
Schedule 8: Controlled drug-Substances which should be available for use but require restriction of manufacture, supply, distribution, possession and use to reduce abuse, misuse and physical or psychological dependence.
Medicines that have no restriction to their availability are called unscheduled medicines.
Authority to prescribe granted under the Health Drugs and Poisons Regulation1996 relates only to scheduled medicines.
From now on, this document will use the term ‘scheduled medicines’ to refer to those medicines regulated by the Health Drugs and Poisons Regulation 1996.
Prescription
A prescription is the direction or instruction from a prescriber to issue and administer a medicine. Although a prescription may initially be issued as a verbal order, in order to comply with legislative and regulatory requirements, this will typically be followed with a written instruction that bears the prescriber’s signature (this may be in handwritten or electronic format). The term prescription has a legal implication and it implies that a prescriber takes responsibility for the clinical care of that patient.

Page | 11 A review of the prescribing capability of speech pathologists, dietitians and psychologists
For this document, the term ‘prescription’ will refer to the written order for a scheduled medicine (whether handwritten or electronic) with the understanding that this may sometimes manifest as a verbal order in the first instance.
Scope of Practice
The area and extent of practice for an individual health professional, usually defined by a regulator, a profession or employer, after taking into consideration the health professional’s education, training, experiences, expertise and demonstrated competency(1).
Prescribing Competencies Framework
At a national level prescribing capability is described in the framework produced by the National Prescribing Service (NPS) ‘Competencies Required to Prescribe Medicines -Putting quality use of medicines into practice’(2). This framework describes competencies required to ‘prescribe medicines judiciously, appropriately, safely and effectively in the Australian healthcare system’ and, for the purposes of this paper, will be referred to as the ‘Prescribing Competencies Framework’.
Competencies
The knowledge skills and behaviours needed to adequately perform the function(2).

Page | 12 A review of the prescribing capability of speech pathologists, dietitians and psychologists
LList of tables and figures
Tables
Table 1 Speech pathology mapping summary: extent to which the Prescribing Competencies Framework is covered by the speech pathology standards
24
Table 2 Relationship between the Prescribing Competencies Framework, the HPPP prescribing models and the professional standards for speech pathologists
30
Table 3 Dietetic mapping summary: extent to which the Prescribing Competencies Framework is covered by the dietetic standards
55
Table 4 Relationship between the Prescribing Competencies Framework, the HPPP prescribing models and the professional standards for dietitians
63
Table 5 Psychology Standards/guidelines that can be used to map psychologist entry level competence against the Prescribing Competencies Framework
90
Table 6 Psychology mapping summary: extent to which the Prescribing Competencies Framework is covered by the psychology standards
92
Table 7 Relationship between the Prescribing Competencies Framework, the HPPP prescribing models and the professional standards and entry level competencies for psychologists
103
Table A1
Mapping of the Prescribing Competencies Framework against the Speech Pathology Australia (SPA) Competency-based Occupational Standards (CBOS) for Speech Pathologist Entry Level 2011 and Code of Ethics
126
Table A2
Mapping of the Prescribing Competencies Framework (Element Level) against Curriculum Learning Outcomes for Bachelor of Speech Pathology (Honours), University of Queensland
156
Table A3 Table A3: Analysis of additional training required to achieve prescribing competence in speech pathologists dependent on the HPPP model of prescribing
170
Table B1
Mapping of the Prescribing Competencies Framework against the Dietitians Association of Australia National (DAA) Competency standards for Dietitians in Australia (2015) and Statement of Ethical Practice
178
Table B2
Mapping of the Prescribing Competencies Framework (Element Level) against Curriculum Learning Outcomes for Bachelor of Nutrition and Dietetics, QUT
200
Table B3 Table B3: Analysis of additional training required to achieve prescribing competence in dietitians dependent on the HPPP model of prescribing
207
Table C1
Mapping of the Prescribing Competencies Framework against the National Practice Standards for the Mental Health Workforce and the Australian Psychological Society Code of Ethics
216

Page | 13 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Table C2
Mapping of the Prescribing Competencies Framework Against The Psychology Board Of Australia (PsyBA) Guidelines For 4+2 Internship Programs for Provisional Psychologists and Supervisors, Australian Psychology Accreditation Council (APAC) Accreditation Standard for Programs of Study in Psychology (Second Consultation Draft) and PsyBA National Psychology Examination Curriculum
244
Table C3
Mapping of the Prescribing Competencies Framework (Element Level) against Curriculum Learning Outcomes for Bachelor of Behavioural Science (Psychology) + Bachelor of Behavioural Science (Honours Psychology) + Master of Clinical Psychology, QUT
295
Table C4 Analysis of additional training required to achieve prescribing competence in psychologists dependent on the HPPP model of prescribing
313
Figures
Figure 1 Education and Training options for general registration as a Psychologist in Australia
87
Page | 14 A review of the prescribing capability of speech pathologists, dietitians and psychologists
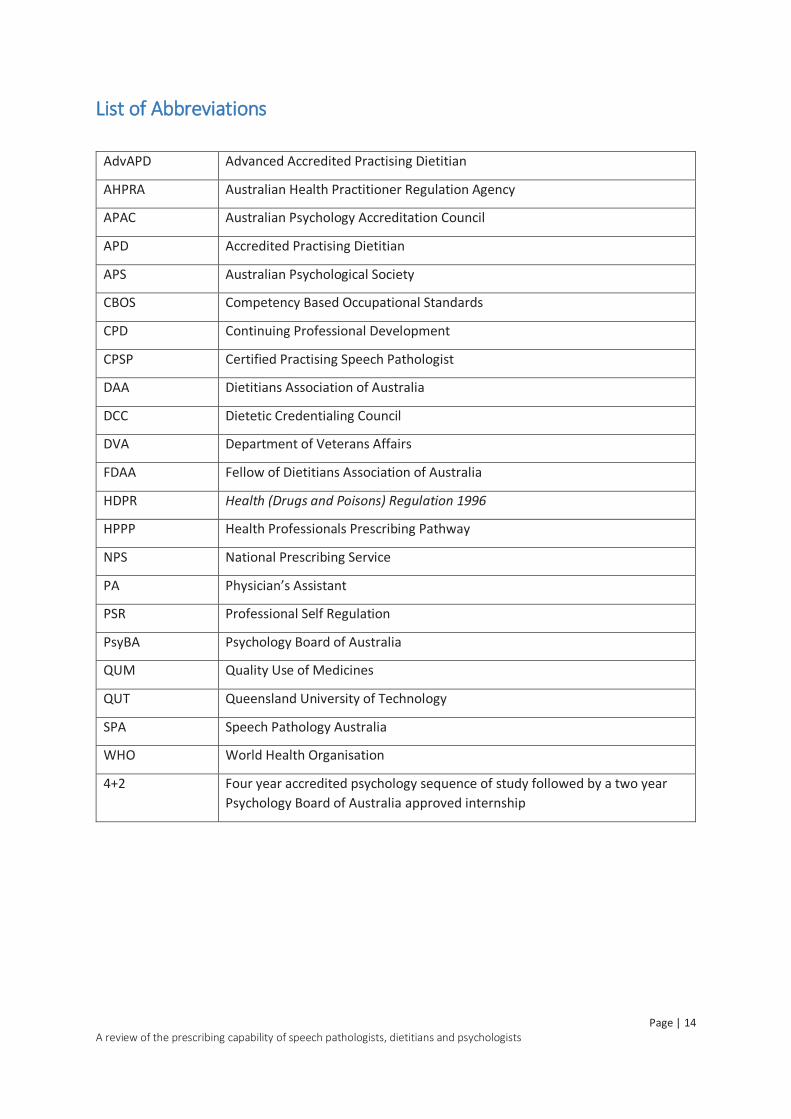
LList of Abbreviations
AdvAPD Advanced Accredited Practising Dietitian
AHPRA Australian Health Practitioner Regulation Agency
APAC Australian Psychology Accreditation Council
APD Accredited Practising Dietitian
APS Australian Psychological Society
CBOS Competency Based Occupational Standards
CPD Continuing Professional Development
CPSP Certified Practising Speech Pathologist
DAA Dietitians Association of Australia
DCC Dietetic Credentialing Council
DVA Department of Veterans Affairs
FDAA Fellow of Dietitians Association of Australia
HDPR Health (Drugs and Poisons) Regulation 1996
HPPP Health Professionals Prescribing Pathway
NPS National Prescribing Service
PA Physician’s Assistant
PSR Professional Self Regulation
PsyBA Psychology Board of Australia
QUM Quality Use of Medicines
QUT Queensland University of Technology
SPA Speech Pathology Australia
WHO World Health Organisation
4+2 Four year accredited psychology sequence of study followed by a two year Psychology Board of Australia approved internship

Page | 15 A review of the prescribing capability of speech pathologists, dietitians and psychologists
11. Introduction Prescribing is a complex task which involves a combination of specific skills, knowledge and behaviours and includes both cognitive and decision making steps.
Podiatrists and optometrists have held prescribing authority in Australia for a number of years, and there is growing evidence that extending the scope of practice of other allied health professionals, to include prescribing, will benefit the patient(1, 3, 9).
In order to safeguard patient safety, it is necessary to ensure that any health professional authorised to prescribe is competent to do so. The national Prescribing Competencies Framework (2) provides a valuable standard against which prescribing competence can be assessed.
This report aims to review current capabilities of speech pathologists, dietitians and psychologists, and determine competency areas that require additional training before a prescribing role can be considered.
2. Non-Medical Prescribing in Australia The role and authorisation to prescribe in Australia has traditionally been held by medical and dental practitioners. Over the last few years, a number of other health professions have gained authority to prescribe under state legislation.
2.1 Drivers for non-medical prescribing 2.1.1 Population growth
The estimated Australian population on 31 March 2015 was 23,714,300; a growth of 1.4% in a year(10).This population is projected to increase to between 36.8 and 48.3 million by 2061(11).
With a growing population comes increased healthcare needs and prescribing. In 2011–12 Australia spent around $140.2 billion on health, with $18.8 billion being spent on medications. Interestingly, health expenditure has grown faster than population growth with expenditure increased from $4,276 per person in 2001–02 to $6,230 in 2011–12(12).
2.1.2 Ageing population
Between 1994 and 2014 the proportion of the Australian population aged 65 years and over increased from 11.8% to 14.7%, and the population over 85 years almost doubled from 1% in 1994 to 1.9% in 2014(13). These numbers are projected to increase; with the proportion of the population aged over 65 being 22%, and over 85 being 5%, by 2061(11). This ageing population is projected to have implications in many areas, including health. Challenges to the healthcare system include changing health profiles, increased demand for health service use and rising health costs. Not only will there be growth in age related health problem such as dementia, arthritis and cancer, but an increase in diseases such as type 2 diabetes, as the ‘younger’ population, who have a higher incidence of lifestyle related disease, enter the 65 and over age bracket(12).

Page | 16 A review of the prescribing capability of speech pathologists, dietitians and psychologists
22.1.3 Chronic disease and multiple morbidities
In 2007-08, 35% of the population of Australia has at least one chronic disease, and 2% of the population reported four or more concurrent conditions. The likelihood of having a chronic disease increases with age, as does the likelihood of having multiple chronic conditions, with 8% of the population over 65 reporting four or more chronic conditions(14).
3. The Health Professionals Prescribing Pathway With increases in population, aged patients and multiple chronic disease states, there is a growing demand for healthcare. One way to meet this demand is by both optimising and extending the scope of practice of health professionals. One such possible area of extension is prescribing, and a number of health professionals, for example optometrists, podiatrists and nurse practitioners, have already been granted prescribing authority.
With the expansion of prescribing rights to non-medical prescribers, there is a need to ensure that health professionals authorised to prescribe are trained in such a way that they become safe, effective and appropriate prescribers. In order to provide a nationally consistent approach to non-medical prescribing in Australia, Health Workforce Australia published the Health Professionals Prescribing Pathway (HPPP)(1).
The HPPP outlines a prescribing framework that is applicable to health professionals registered under the National Registration and Accreditation Scheme, other than medical practitioners, and addresses five steps to safe and competent prescribing.
1. Complete education and training 2. Obtain recognition from the National Board of competence to prescribe 3. Ensure authorisation to prescribe 4. Maintain and enhance competence to prescribe 5. Prescribe medicines within scope of practice The pathway also defines three safe prescribing models by health professionals:
1. Autonomous prescribing
Prescribing occurs where a prescriber undertakes prescribing within their scope of practice without the approval or supervision of another health professional. The prescriber has been educated and authorised to autonomously prescribe in a specific area of clinical practice. Although the prescriber may prescribe autonomously, they recognise the role of all members of the health care team and ensure appropriate communication occurs between team members and the person taking medicine.
An example of autonomous prescribing is an optometrist with a scheduled medicines endorsement, who is authorised to independently write a PBS prescription for a medicine from the Optometry Board of Australia approved list of schedule 4 medicines. This can occur without supervision of a medical practitioner or use of a pre-agreed prescribing guideline, protocol or standing order.
2. Prescribing under supervision
Prescribing occurs where a prescriber undertakes prescribing within their scope of practice under the supervision of another authorised health professional. The supervised prescriber has been

Page | 17 A review of the prescribing capability of speech pathologists, dietitians and psychologists
educated to prescribe, and has a limited authorisation to prescribe medicines that is determined by legislation, requirements of the National Board and policies of the jurisdiction, employer or health service. The prescriber and supervisor recognise their role in their health care team and ensure appropriate communication occurs between team members and the person taking medicine.
An example of prescribing under supervision is a physician’s assistant (PA), working in a remote regional hospital, writing an inpatient prescription in accordance with an endorsed Practice Plan, which has been developed by the PA’s principal and secondary supervising medical practitioners.
3. Prescribing via a structured prescribing arrangement
Prescribing occurs where a prescriber with a limited authorisation to prescribe medicines by legislation, requirements of the National Board and policies of the jurisdiction or health service prescribes medicines under a guideline, protocol or standing order. A structured prescribing arrangement should be documented sufficiently to describe the responsibilities of the prescriber(s) involved and the communication that occurs between team members and the person taking medicine.
An example of prescribing under a structured prescribing arrangement is a paramedic administering a scheduled medicine, in response to an emergency situation, in accordance with a Queensland Ambulance Service Drug Therapy Protocol.
It is important to note that health professionals may work within more than one model of prescribing in their clinical practice.
44. National Prescribing Competencies In addition to establishing a prescribing pathway for non-medical prescribers, it is imperative to establish safe and effective prescribing practice and ensure that all practitioners are competent in their prescribing role.
Guidance to prescribing has previously been provided in the form of such publications as the World Health Organisation’s (WHO)‘Guide to Good Prescribing’(15). In 2012 the National Prescribing Service (NPS) published ‘Competencies Required to Prescribe Medicines -Putting quality use of medicines into practice’. Although it uses the WHO manual as a basis, this national Prescribing Competencies Framework is tailored specifically to the Australian healthcare system(2).
The Prescribing Competencies Framework aims to describe foundation competencies for autonomous prescribing; describing the knowledge, skills and behaviours that practitioners, who work to an acceptable standard, are expected to demonstrate. The framework has seven competency areas; five of which are related directly to prescribing and two horizontal competency areas which detail general professional competencies. The horizontal competency areas describe activities that the health practitioner should incorporate during the prescribing process.
Each competency area is divided into elements, which describe the specific processes, actions and tasks that health professionals carry out when prescribing. The elements are further broken down to performance criteria, which describe observable behaviours or results that are expected of competent prescribers(2). Individual performance criteria have evidence examples which can assist in the assessment of prescribing performance.
Page | 18 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Whilst it is not the intention of the Prescribing Competencies Framework to act as a curriculum, it provides a useful standard, and could be used in the development of prescriber training programs or to assess prescribing performance.
55. Allied Health Prescribing in Queensland In Queensland the authority to prescribe is legislated under the Health (Drugs and Poisons) Regulation 1996 (HDPR)(4). Under this legislation podiatrists and optometrists already have limited prescribing authority. Optometrists who have a scheduled medicines endorsement to their general registration are authorised, under the Ocular Therapeutics Protocol(16), to prescribe those topical drugs specified by the Optometry Board of Australia. The qualifications and requirements for endorsement, as well as the list of drugs, are stated in the Optometry Board of Australia’s Endorsement for scheduled medicines registration standard(17).
Similarly in Queensland, podiatrists with a scheduled medicines endorsement to their general registration are authorised to prescribe from a list of medicines defined in appendix 2C of the HDPR ‘Restricted drugs and poisons for endorsed podiatrists and trainee endorsed podiatrists’(4). The qualifications and requirements for endorsement are detailed in the Podiatry Board of Australia’s Endorsement for scheduled medicines registration standard(18).
Physiotherapists in Queensland are authorised to administer a schedule 2 poison, but not to prescribe any medicine or poison. The Physiotherapy Board of Australia is, however, investigating the possibility of application to the Australian Health Workforce Ministerial Council for approval of physiotherapy endorsement to registration to prescribe scheduled medicines(19).
There is also evidence of pharmacists moving into the prescribing arena in Queensland. Hale et al have published two trials involving pharmacist prescribing in a preadmission clinic (20, 21).
The Ministerial Taskforce final report on health practitioner expanded scope of practice(3), found that allied health professionals within Queensland Health were not performing the full range of duties and tasks appropriate to their level of education and training. The report detailed a number of areas that scope of practice could be extended, including prescribing, and gave a number of allied health prescribing examples.
Queensland Health have further supported the development of allied health prescribing through the provision of scholarship funding for Queensland Health employees to undertake an Allied Health Prescribing Training Program(22). The program, run as a pilot by Queensland University of Technology (QUT)(23), was designed to educate allied health professionals to undertake prescribing in a range of trials that are currently underway in Queensland. The course consists of two modules; ‘Introduction to clinical therapeutics for prescribers’ and ‘Prescribing and Quality Use of Medicine’.
Any prescribing by allied health professionals in Queensland, not already authorised under the HDPR, must be undertaken within a formal research framework. Approval of the Chief Health Officer, under section 18 of the HDPR, must be obtained to enable individual health professionals to prescribe. The Allied Health Professions’ Office of Queensland have developed a framework, which describes the process by which such trials can be implemented(5).

Page | 19 A review of the prescribing capability of speech pathologists, dietitians and psychologists
6. Speech Pathology 6.1 Background Information
The number of speech pathologists in Australia is estimated to be over 7,000(24). Whilst workforce shortages were experienced for a number of years at the start of the millennium, the latest skill shortage occupational report from March 2014 lists speech pathology as ‘no shortage’. The same document also shows an increase in the number of commencements and completions for domestic students in speech pathology higher education(25).
6.1.1 National Bodies/Registration
There is no speech pathology board established under the National Law(26), and hence no legal requirement for speech pathologists to be registered in Australia.
National representation is provided by Speech Pathology Australia (SPA), which is the major body for speech pathologists in Australia, with over 6,500 members(27). SPA has a number of functions including advocacy, representation to government and key stakeholders, governance of ethical and clinical standards of members and provision of professional development activities.
SPA is a self-regulating body and is committed to ensuring a high standard of ethical and clinical practice by its members. A regulatory framework is provided in the form of professional standards, a Code of Ethics and a Professional Self-Regulation (PSR) program. The PSR program encourages members to take responsibility for their own continuing professional development (CPD), and enables members to accrue points for CPD activities undertaken. Practising SPA members who meet the requirements of the PSR program can earn status as a Certified Practising Speech Pathologist (CPSP).
6.1.2 Education and Training
SPA is the accrediting body for programs of study leading to the speech pathology qualification in Australia.
The profession of speech pathology can be entered via one of two routes; completion of a four year accredited undergraduate Bachelor degree, or a two year accredited postgraduate Master’s degree. Both routes produce entry level graduates, who are sufficiently competent to provide patient services, commensurate with an entry level practitioner, without any period of formal internship or supervision.
6.1.3 Current Prescribing Status
Speech pathologists currently have no prescribing authority in Queensland or Australia.
6.1.4 Prescribing potential
There are a number of medicines that speech pathologists could potentially prescribe within their scope of practice, these include the following:
Oral antifungal agents such as nystatin for the treatment of oral candidiasis in radiation oncology patients, and amphotericin B for the prevention and treatment of candida infections in laryngectomy patients
Topical anaesthetics such as lignocaine for changing voice prostheses or passing nasendoscopes

Page | 20 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Topical corticosteroids such as Kenacomb®(triamcinolone, neomycin, nystatin and gramicidin) ointment to treat granulation tissue around tracheoesophageal puncture/voice prosthesis for laryngectomy patients
6.2 Prescribing Competence in Speech Pathology
In order to consider the prescribing potential of the speech pathologist, and to identify options in Queensland relating to prescribing authority, it is necessary to review the current status of speech pathology qualifications and evaluate their capacity to provide the skills, knowledge and behaviours necessary to become a competent prescriber. As discussed previously, such competence is described in the Prescribing Competencies Framework. If the current training requirements and professional standards for speech pathologists are mapped against the Prescribing Competencies Framework, it will be possible to evaluate the current prescribing capability of speech pathologists and identify any gaps in capability that may need to be addressed.
6.2.1 Speech pathology training requirements and professional standards which define professional capability
All entry level degree programs in Australia, accredited by SPA, are assessed against the 2011 Competency Based Occupational Standards for Speech Pathologists (CBOS 2011)(28). In order to be accredited, speech pathology programs of study have to demonstrate that their graduates attain these competencies. The standards detail the knowledge, skills and professional standards required for entry level practice. All practising speech pathologists should, therefore, have minimum standards of practice commensurate with CBOS 2011.
In addition to the CBOS 2011, SPA also produces the speech pathology Code of Ethics, this document contains the principles, values and standards that define acceptable professional behaviour(29). SPA member speech pathologists are expected to ‘read, understand and apply the Code of Ethics within all professional interactions’.
These two professional standards define the competencies and practice requirements of a speech pathologist. It is, therefore, reasonable to assume that if both CBOS 2011 and the Code of Ethics are mapped against the Prescribing Competencies Framework, a clearer picture of prescribing readiness will emerge.
6.3 Speech Pathology Competency Mapping
6.3.1 Methodology
Both the CBOS 2011 and the SPA Code of Ethics were mapped against individual performance criteria for every element within the Prescribing Competencies Framework. This mapping is shown in table A1, appendix A. The comments section of the table denotes whether statements identified in either one or both of the professional standards can be considered to map completely, partly, or not at all with the Prescribing Competencies Framework. The comments section is colour coded as follows:
Green denotes that a particular prescribing competency performance criterion maps well, and is covered sufficiently by either one or both of the standards
Orange denotes that the particular prescribing competency performance criterion is covered partly by either one or both of the standards

Page | 21 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Red denotes that the particular prescribing competency performance criterion cannot be identified in either of the standards
To provide additional education and training information relevant to the review, the learning objectives from a SPA accredited speech pathology program of study were also mapped against the Prescribing Competencies Framework elements. Learning objectives from The University of Queensland Bachelor of Speech Pathology (Honours) were mapped as a representative program of study.
6.3.2 Results
PProfessional Standards Mapping
Table 1 provides a summary of the mapping results. The table shows competencies from the Prescribing Competencies Framework separated into different categories, and indicates which of the prescribing competencies within each category are covered completely, partly, or not at all by the speech pathology standards. It should be noted that the capability assumptions made in the mapping process are based purely on information obtained from the speech pathology standards, and not on review of actual practice.
Interaction and communication with patients
Prescribing competencies relating to communication style and therapeutic partnership with patients and carers map well, as do the prescribing competencies relating to respect for the patient and providing clear written and verbal information to enable informed decision making.
Competencies that are not covered by the speech pathology standards are exploring and responding to patient concerns, considering the power differential between the health professional and the patient and ascertaining that information has been understood correctly.
Interaction and communication with other health professionals
Prescribing competencies relating to provision of information to, and collaboration with, other health professionals map well. Competencies not covered are responding appropriately to communication and confirming understanding of information provided by other health professionals.
Assessment and diagnosis
Assessment and diagnosis competencies are generally covered well by speech pathology standards. Prescribing competencies only partly covered include reviewing and interpreting information from the person’s heath record and obtaining information from the patient. The speech pathology standards do not detail the specifics of the information to be obtained from the patient such as medicines, allergies, alcohol and substance abuse; information that is vital when prescribing a medicine.
The only prescribing competency not covered in this category was the assessment of a patient’s risk factors for poor adherence.

Page | 22 A review of the prescribing capability of speech pathologists, dietitians and psychologists
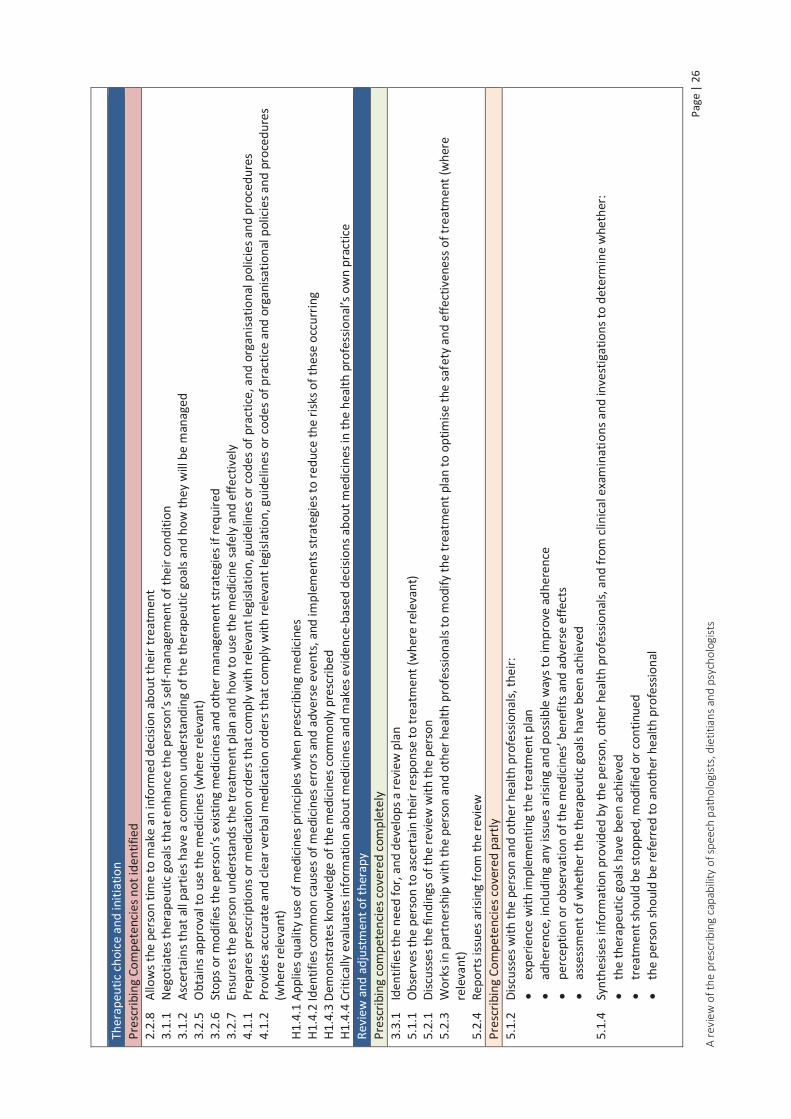
Therapeutic choice and initiation
Competencies that map completely include recognising when non pharmacological treatment is appropriate, supplementing verbal with written information, referral when treatment is outside scope of practice and developing a treatment plan in partnership with the patient.
Whilst the speech pathology standards detail planning and implementation of interventions, many of the prescribing competencies in his category are only partly covered, because they specifically relate to selection of medicine. These include identification of suitable medicine options, discussion of medicine options with the patient, reaching agreement with the patient about medicine choice and consulting other health professionals about potential medicines. In addition, the prescribing competency relating to recognising when it is clinically appropriate not to intervene is only partly covered by the speech pathology standards.
Not surprisingly, prescribing competencies specifically relating to medicine selection and ordering were not identified in the speech pathology standards. These include medicine information and knowledge, application of Quality Use of Medicines (QUM) principles, obtaining approval for medicine use and providing appropriate medication orders. Other competencies unable to be identified relate to interaction with the patient regarding initiation of medicine. These include negotiating therapeutic goals that facilitate self-management, allowing the patient time to make a decision, stopping or modifying existing medicines and ensuring patient understanding of therapeutic goals, management and how to use the medicine safely and effectively.
Review and adjustment of therapy
Prescribing competencies covered well in this category are development of a review plan, observation of patient response to therapy, discussing review findings with the patient, modification of the treatment plan if necessary and reporting issues arising from the review.
Partly covered prescribing competencies are; discussing response to treatment with the patient and other health professionals, and synthesising information obtained regarding the response to determine whether any changes to therapy were required.
Prescribing competencies unable to be identified in the speech pathology standards are obtaining additional information to assess response to therapy, identifying if the patient requires a comprehensive medicines review and organising the next review.
Legal and professional requirements
Prescribing competencies relating to scope of practice, professional standards, codes of conduct and accountability map completely with the speech pathology standards.
Competencies that map partly include maintenance of records, adherence to requirements for consent, demonstrating respect for scope of practice of other health professionals and implementing strategies to address potential prescribing bias. The prescribing competency relating to ongoing professional development with respect to prescribing practices maps partly. Although the speech pathology standards cover CPD requirements, prescribing is currently not within scope of practice, so is not covered by CPD statements. If prescribing becomes an activity within scope of practice, then this competency will map fully.

Page | 23 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Legal and professional competencies that could not be identified in the speech pathology standards are those relating to knowledge and compliance with legislation, policies and procedures relating to prescribing. In addition competencies relating to interpretation and application of guidelines and protocols, and contribution to the improvement of policies and procedures relating to medicines use, did not map.

Page
| 2
4 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Tabl
e 1:
Spe
ech
path
olog
y m
appi
ng su
mm
ary:
ext
ent t
o w
hich
the
Pres
crib
ing
Com
pete
ncie
s Fra
mew
ork
is co
vere
d by
the
spee
ch p
atho
logy
stan
dard
s
Inte
ract
ion
and
com
mun
icatio
n w
ith p
atie
nts
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
1.1.
1
Uses
app
ropr
iate
com
mun
icat
ion
stra
tegi
es to
est
ablis
h a
ther
apeu
tic p
artn
ersh
ip w
ith th
e pe
rson
H2
.2.1
Invo
lves
the
pers
on’s
fam
ily o
r car
ers i
n th
e co
nsul
tatio
n w
here
app
ropr
iate
H2
.2.3
Est
ablis
hes a
ther
apeu
tic p
artn
ersh
ip th
at a
ccor
ds w
ith th
e pr
efer
ence
s exp
ress
ed b
y th
e pe
rson
H2
.3.1
Res
pect
s the
per
son’
s val
ues,
belie
fs, a
nd e
xper
ienc
es
H2.3
.2 R
espe
cts t
he p
erso
n’s p
rivac
y an
d co
nfid
entia
lity
H2.3
.3 R
espe
cts t
he p
erso
n’s h
ealth
care
dec
ision
s H2
.4.1
Ass
esse
s the
per
son’
s pre
ferr
ed la
ngua
ge, c
omm
unica
tion
styl
e, c
omm
unic
atio
n ca
pabi
litie
s, an
d he
alth
lite
racy
, and
adj
usts
the
heal
th p
rofe
ssio
nal’s
ow
n co
mm
unic
atio
n st
yle
to in
tera
ct e
ffect
ivel
y w
ith th
em
H2.4
.3 P
rovi
des c
lear
and
app
ropr
iate
writ
ten
and
verb
al in
form
atio
n to
the
pers
on to
ena
ble
them
to m
ake
info
rmed
choi
ces a
nd a
chie
ve o
ptim
al h
ealth
out
com
es
Pres
crib
ing
Com
pete
ncie
s cov
ered
par
tly
Nil
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d H2
.2.2
Exp
lore
s and
resp
onds
app
ropr
iate
ly to
the
pers
on’s
conc
erns
and
exp
ecta
tions
rega
rdin
g:
th
e co
nsul
tatio
n
thei
r hea
lth
th
eir o
wn
role
and
that
of h
ealth
pro
fess
iona
ls in
man
agin
g th
eir h
ealth
the
heal
th p
rofe
ssio
nal’s
scop
e of
pra
ctic
e
the
use
of m
edici
nes a
nd o
ther
trea
tmen
ts to
mai
ntai
n th
eir h
ealth
H2
.4.2
Con
sider
s the
pot
entia
l iss
ue o
f per
ceiv
ed p
ower
diff
eren
ces b
etw
een
the
heal
th p
rofe
ssio
nal a
nd th
e pe
rson
H2
.4.4
Asc
erta
ins t
hat t
he in
form
atio
n pr
ovid
ed h
as b
een
rece
ived
and
und
erst
ood
corr
ectly
In
tera
ctio
n an
d co
mm
unica
tion
with
oth
er h
ealth
pro
fess
iona
ls Pr
escr
ibin
g co
mpe
tenc
ies c
over
ed c
ompl
etel
y 4.
2.1
Pr
ovid
es in
form
atio
n fo
r col
labo
ratio
n to
mem
bers
of i
nter
-pro
fess
iona
l hea
lthca
re te
ams b
oth
with
in fa
ciliti
es a
nd th
e co
mm
unity
H2
.5.1
Eng
ages
in o
pen,
inte
ract
ive
disc
ussio
ns w
ith o
ther
hea
lth p
rofe
ssio
nals
invo
lved
in c
arin
g fo
r the
per
son
H2.5
.4 P
rovi
des c
lear
ver
bal a
nd w
ritte
n in
form
atio
n to
oth
er h
ealth
pro
fess
iona
ls by
secu
re m
eans
whe
n im
plem
entin
g ne
w tr
eatm
ents
with
med
icine
s or m
odify
ing
exist
ing
trea
tmen
t pla
ns
Pres
crib
ing
Com
pete
ncie
s cov
ered
par
tly
Nil
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d H2
.5.2
Con
firm
s tha
t the
ir ow
n un
ders
tand
ing
of in
form
atio
n pr
ovid
ed b
y ot
her h
ealth
pro
fess
iona
ls is
corr
ect
H2.5
.3 R
espo
nds a
ppro
pria
tely
to co
mm
unic
atio
n in
itiat
ed b
y ot
her h
ealth
pro
fess
iona
ls

Page
| 2
5 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Asse
ssm
ent a
nd d
iagn
osis
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
1.2.
1
Cond
ucts
an
asse
ssm
ent t
hat i
s app
ropr
iate
to b
oth
the
heal
th p
rofe
ssio
nal’s
scop
e of
pra
ctic
e an
d th
e pe
rson
’s cli
nica
l con
text
1.
2.5
As
cert
ains
that
suffi
cien
t inf
orm
atio
n ha
s bee
n ob
tain
ed a
bout
the
pers
on’s
co-e
xist
ing
cond
ition
s and
curr
ent t
reat
men
ts to
iden
tify
poss
ible
risk
s and
co
ntra
indi
catio
ns fo
r tre
atm
ent
1.2.
6
Perf
orm
s clin
ical
exa
min
atio
ns th
at a
re w
ithin
the
heal
th p
rofe
ssio
nal’s
ow
n sc
ope
of p
ract
ice a
nd re
leva
nt to
the
pers
on’s
prob
lem
and
inte
rpre
ts th
e fin
ding
s of t
hese
ex
amin
atio
ns
1.3.
1
Synt
hesis
es in
form
atio
n fr
om th
e co
mpr
ehen
sive
asse
ssm
ent a
nd d
evel
ops p
rovi
siona
l and
diff
eren
tial d
iagn
oses
1.
3.2
De
velo
ps a
dia
gnos
tic st
rate
gy a
nd p
erfo
rms r
elev
ant i
nves
tigat
ions
1.
3.3
Ex
plai
ns th
e cli
nica
l iss
ues a
nd th
eir i
mpl
icat
ions
to th
e pe
rson
Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed p
artly
1.
2.2
Re
view
s and
inte
rpre
ts in
form
atio
n in
the
pers
on’s
heal
th re
cord
s 1.
2.3
O
btai
ns re
leva
nt in
form
atio
n fro
m th
e pe
rson
abo
ut th
eir m
edici
nes,
and
thei
r med
ical
and
clin
ical
hist
ory,
incl
udin
g th
eir c
o-ex
istin
g co
nditi
ons,
trea
tmen
ts, a
lcoho
l an
d su
bsta
nce
use,
alle
rgie
s and
socia
l con
text
Pr
escr
ibin
g Co
mpe
tenc
ies n
ot id
entif
ied
1.2.
4
Asse
sses
the
pers
on’s
risk
fact
ors f
or p
oor a
dher
ence
; for
exa
mpl
e so
cial i
sola
tion,
phy
sical
impa
irmen
t, co
gniti
ve im
pairm
ent o
r dist
urba
nce,
low
Eng
lish
prof
icien
cy,
low
hea
lth li
tera
cy, f
inan
cial
disa
dvan
tage
Th
erap
eutic
cho
ice
and
initi
atio
n Pr
escr
ibin
g co
mpe
tenc
ies c
over
ed c
ompl
etel
y 2.
1.2
Re
cogn
ises w
hen
it is
clini
cally
app
ropr
iate
to im
plem
ent n
on-p
harm
acol
ogica
l tre
atm
ents
2.
2.7
Su
pple
men
ts v
erba
l inf
orm
atio
n w
ith w
ritte
n in
form
atio
n ab
out t
he co
nditi
on a
nd tr
eatm
ent o
ptio
ns (w
here
app
ropr
iate
) 2.
2.9
Re
fers
the
pers
on fo
r fur
ther
ass
essm
ent o
r tre
atm
ent w
hen
the
suita
ble
trea
tmen
t opt
ions
are
out
side
the
heal
th p
rofe
ssio
nal’s
ow
n sc
ope
of p
ract
ice
3.2.
4
Deve
lops
the
trea
tmen
t pla
n in
par
tner
ship
with
the
pers
on
Pres
crib
ing
Com
pete
ncie
s cov
ered
par
tly
2.1.
1
Reco
gnise
s whe
n it
is cli
nica
lly a
ppro
pria
te n
ot to
inte
rven
e; fo
r exa
mpl
e, in
cas
es w
here
the
signs
and
sym
ptom
s are
like
ly to
reso
lve
with
out t
reat
men
t 2.
2.1
In
tegr
ates
kno
wle
dge
of p
harm
acol
ogy,
oth
er b
iom
edic
al sc
ienc
es, c
linica
l med
icine
, and
ther
apeu
tics a
nd id
entif
ies m
edici
nes s
uita
ble
for t
reat
ing
the
cond
ition
2.
2.2
O
btai
ns, i
nter
pret
s, an
d ap
plie
s cur
rent
evi
denc
e an
d in
form
atio
n ab
out m
edici
nes t
o in
form
dec
ision
s abo
ut in
corp
orat
ing
med
icine
s int
o th
e pe
rson
’s tr
eatm
ent p
lan
2.2.
3
Iden
tifie
s med
icine
s opt
ions
that
are
like
ly to
pro
vide
ther
apeu
tical
ly e
ffect
ive
and
safe
trea
tmen
t and
tailo
rs th
e m fo
r the
per
son
2.2.
4
Cons
ider
s the
cost
and
affo
rdab
ility
of t
he m
edici
nes t
o th
e pe
rson
2.
2.5
Co
nsid
ers t
he im
plica
tions
to th
e w
ider
com
mun
ity o
f usin
g a
part
icul
ar m
edic
ine
to tr
eat t
he p
erso
n 2.
2.6
Di
scus
ses t
he tr
eatm
ent o
ptio
ns a
nd m
edici
nes w
ith th
e pe
rson
, con
sider
ing:
the
prio
ritie
s for
trea
ting
thei
r cur
rent
con
ditio
n an
d co
-exi
stin
g co
nditi
ons;
thei
r re
adin
ess t
o ad
dres
s the
curr
ent c
ondi
tion;
thei
r exp
ecta
tions
of t
reat
men
t 3.
2.1
Ex
plor
es th
e pe
rson
’s op
inio
ns a
nd p
refe
renc
es co
ncer
ning
med
icine
s and
the
trea
tmen
t pla
n 3.
2.2
Co
nsul
ts o
ther
hea
lth p
rofe
ssio
nals
abou
t pot
entia
l med
icin
es a
nd th
e tr
eatm
ent p
lan
3.2.
3
Reac
hes a
gree
men
t with
the
pers
on a
bout
med
icine
s to
be u
sed
to tr
eat t
heir
cond
ition
Page
| 2
6 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Ther
apeu
tic c
hoic
e an
d in
itiat
ion
Pr
escr
ibin
g Co
mpe
tenc
ies n
ot id
entif
ied
2.2.
8
Allo
ws t
he p
erso
n tim
e to
mak
e an
info
rmed
dec
ision
abo
ut th
eir t
reat
men
t 3.
1.1
Ne
gotia
tes t
hera
peut
ic go
als t
hat e
nhan
ce th
e pe
rson
’s se
lf-m
anag
emen
t of t
heir
cond
ition
3.
1.2
As
cert
ains
that
all
part
ies h
ave
a co
mm
on u
nder
stan
ding
of t
he th
erap
eutic
goa
ls an
d ho
w th
ey w
ill b
e m
anag
ed
3.2.
5
Obt
ains
app
rova
l to
use
the
med
icine
s (w
here
rele
vant
) 3.
2.6
St
ops o
r mod
ifies
the
pers
on’s
exist
ing
med
icine
s and
oth
er m
anag
emen
t str
ateg
ies i
f req
uire
d 3.
2.7
En
sure
s the
per
son
unde
rsta
nds t
he tr
eatm
ent p
lan
and
how
to u
se th
e m
edici
ne sa
fely
and
effe
ctiv
ely
4.1.
1
Prep
ares
pre
scrip
tions
or m
edic
atio
n or
ders
that
com
ply
with
rele
vant
legi
slatio
n, g
uide
lines
or c
odes
of p
ract
ice, a
nd o
rgan
isatio
nal p
olici
es a
nd p
roce
dure
s 4.
1.2
Pr
ovid
es a
ccur
ate
and
clear
ver
bal m
edica
tion
orde
rs th
at co
mpl
y w
ith re
leva
nt le
gisla
tion,
gui
delin
es o
r cod
es o
f pra
ctice
and
org
anisa
tiona
l pol
icies
and
pro
cedu
res
(whe
re re
leva
nt)
H1.4
.1 A
pplie
s qua
lity
use
of m
edici
nes p
rinci
ples
whe
n pr
escr
ibin
g m
edici
nes
H1.4
.2 Id
entif
ies c
omm
on c
ause
s of m
edici
nes e
rror
s and
adv
erse
eve
nts,
and
impl
emen
ts st
rate
gies
to re
duce
the
risks
of t
hese
occ
urrin
g H1
.4.3
Dem
onst
rate
s kno
wle
dge
of th
e m
edic
ines
com
mon
ly p
resc
ribed
H1
.4.4
Crit
ically
eva
luat
es in
form
atio
n ab
out m
edici
nes a
nd m
akes
evi
denc
e-ba
sed
decis
ions
abo
ut m
edici
nes i
n th
e he
alth
pro
fess
iona
l’s o
wn
prac
tice
Revi
ew a
nd a
djus
tmen
t of t
hera
py
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
3.3.
1
Iden
tifie
s the
nee
d fo
r, an
d de
velo
ps a
revi
ew p
lan
5.1.
1
Obs
erve
s the
per
son
to a
scer
tain
thei
r res
pons
e to
trea
tmen
t (w
here
rele
vant
) 5.
2.1
Di
scus
ses t
he fi
ndin
gs o
f the
revi
ew w
ith th
e pe
rson
5.
2.3
W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
mod
ify th
e tr
eatm
ent p
lan
to o
ptim
ise th
e sa
fety
and
effe
ctiv
enes
s of t
reat
men
t (w
here
re
leva
nt)
5.2.
4
Repo
rts i
ssue
s aris
ing
from
the
revi
ew
Pres
crib
ing
Com
pete
ncie
s cov
ered
par
tly
5.1.
2
Disc
usse
s with
the
pers
on a
nd o
ther
hea
lth p
rofe
ssio
nals,
thei
r:
expe
rienc
e w
ith im
plem
entin
g th
e tr
eatm
ent p
lan
ad
here
nce,
inclu
ding
any
issu
es a
risin
g an
d po
ssib
le w
ays t
o im
prov
e ad
here
nce
pe
rcep
tion
or o
bser
vatio
n of
the
med
icine
s’ be
nefit
s and
adv
erse
effe
cts
as
sess
men
t of w
heth
er th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
5.1.
4
Synt
hesis
es in
form
atio
n pr
ovid
ed b
y th
e pe
rson
, oth
er h
ealth
pro
fess
iona
ls, a
nd fr
om cl
inica
l exa
min
atio
ns a
nd in
vest
igat
ions
to d
eter
min
e w
heth
er:
th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
trea
tmen
t sho
uld
be st
oppe
d, m
odifi
ed o
r con
tinue
d
the
pers
on sh
ould
be
refe
rred
to a
noth
er h
ealth
pro
fess
iona
l

Page
| 2
7 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Revi
ew a
nd a
djus
tmen
t of t
hera
py
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d 5.
1.3
O
btai
ns a
dditi
onal
info
rmat
ion
to a
sses
s whe
ther
the
ther
apeu
tic g
oals
have
bee
n ac
hiev
ed b
y ex
amin
ing
the
pers
on, r
eque
stin
g in
vest
igat
ions
, and
inte
rpre
ting
the
findi
ngs (
whe
re re
leva
nt)
5.2.
2
Iden
tifie
s if t
he p
erso
n re
quire
s a co
mpr
ehen
sive
med
icin
es re
view
5.
2.5
Or
gani
ses t
he n
ext r
evie
w
Lega
l and
pro
fess
iona
l req
uire
men
ts
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
H1.2
.1 D
emon
stra
tes k
now
ledg
e of
and
com
plia
nce
with
:
prof
essio
nal s
tand
ards
code
s of c
ondu
ct
sc
ope
of p
ract
ice st
atem
ents
or g
uide
lines
H1.2
.2 P
ract
ices w
ithin
the
limits
of t
he h
ealth
pro
fess
iona
l’s o
wn
educ
atio
n, tr
aini
ng a
nd sc
ope
of p
ract
ice
H1.2
.4 A
ccep
ts re
spon
sibili
ty a
nd is
acc
ount
able
for t
he ca
re p
rovi
ded
to th
e pe
rson
Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed p
artly
H1
.1.2
Mai
ntai
ns a
ccur
ate
and
com
plet
e re
cord
s of:
th
e co
nsul
tatio
n
clin
ical
exa
min
atio
ns a
nd in
vest
igat
ion
resu
lts
ris
k fa
ctor
s for
med
icine
s misa
dven
ture
the
pers
on’s
decis
ion
to d
eclin
e tr
eatm
ent (
whe
re re
leva
nt)
ch
ange
s to
the
pers
on’s
med
icine
s man
agem
ent p
lan,
inclu
ding
the
ratio
nale
beh
ind
thes
e ch
ange
s
the
revi
ew p
lan,
reco
mm
enda
tions
, and
dat
e fo
r nex
t rev
iew
outc
omes
of t
reat
men
t
H1.2
.3 D
emon
stra
tes r
espe
ct fo
r the
scop
e of
pra
ctice
of o
ther
hea
lth p
rofe
ssio
nals
and
thei
r con
trib
utio
n w
ithin
a co
llabo
rativ
e ca
re m
odel
, par
ticul
arly
that
of t
he p
erso
n’s
mai
n he
alth
care
pro
vide
r H1
.5.1
Eng
ages
in o
ngoi
ng p
rofe
ssio
nal d
evel
opm
ent a
nd e
duca
tion
to im
prov
e pr
escr
ibin
g pr
actic
es
H1.6
.1 Im
plem
ents
stra
tegi
es to
add
ress
influ
ence
s tha
t may
bia
s pre
scrib
ing
deci
sions
, inc
ludi
ng:
m
arke
ting
influ
ence
s
Poss
ible
per
sona
l, pr
ofes
siona
l or f
inan
cial
gai
n
Conf
licts
of i
nter
est
Th
e he
alth
pro
fess
iona
l’s o
wn
belie
fs, v
alue
s, an
d ex
perie
nces

Page
| 2
8 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
H2
.1.1
Adh
eres
to le
gisla
tive
and
wor
kpla
ce re
quire
men
ts fo
r obt
aini
ng a
nd re
cord
ing
cons
ent f
or:
Ac
cess
ing
heal
th re
cord
s
obta
inin
g in
form
atio
n fr
om, a
nd p
rovi
ding
info
rmat
ion
to, o
ther
hea
lth p
rofe
ssio
nals
co
nduc
ting
a cli
nica
l exa
min
atio
n
prov
idin
g cli
nica
l ser
vice
s
the
pote
ntia
l ben
efits
and
har
ms
Lega
l and
pro
fess
iona
l req
uire
men
ts
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d H1
.1.1
Dem
onst
rate
s kno
wle
dge
of, a
nd co
mpl
ies w
ith, l
egisl
atio
n, re
gula
tions
, and
com
mon
law
app
licab
le to
pre
scrib
ing
(as f
urth
er d
efin
ed b
y th
e kn
owle
dge
subs
ectio
n of
th
is co
mpe
tenc
y ar
ea)
H1.3
.1 D
emon
stra
tes k
now
ledg
e of
and
com
plie
s with
nat
iona
l, st
ate
and
terr
itory
, and
facil
ity p
olic
ies a
nd p
roce
dure
s in
rela
tion
to p
resc
ribin
g H1
.3.2
Dem
onst
rate
s app
ropr
iate
pro
fess
iona
l jud
gem
ent w
hen
inte
rpre
ting
and
appl
ying
gui
delin
es a
nd p
roto
cols
to th
e pe
rson
’s sit
uatio
n H1
.3.3
Con
trib
utes
to th
e im
prov
emen
t of p
olic
ies a
nd p
roce
dure
s for
the
judi
ciou
s, ap
prop
riate
, saf
e an
d ef
fect
ive
use
of m
edici
nes
Page | 29 A review of the prescribing capability of speech pathologists, dietitians and psychologists
LLearning Outcomes Mapping The learning outcomes were mapped at an element level to provide additional information regarding pre-entry education and training. The results of the mapping for the University of Queensland Bachelor of Speech Pathology (Honours) program of study are shown in table A2, appendix A.
The following Prescribing Competencies Framework elements were not identified in the learning objectives:
Element 4.1: Provides clear instructions to other health professionals who dispense, supply, or administer medicines prescribed for the person
Element 5.1: Obtains information to assess the person’s response to treatment
Element 5.2: Works in partnership with the person and other health professionals to address issues arising from the review
Element H1.4: Practices quality use of medicines principles
Element H1.6: Addresses the potential for bias in prescribing decisions
Element H2.1: Obtains consent to provide clinical services to the person
Mapping speech pathology prescribing capability against Prescribing Models To provide additional information to identify the prescribing capabilities of speech pathologists, the performance criteria of the Prescribing Competencies Framework were mapped against the HPPP models of prescribing. The results from the speech pathology mapping were then included to create a summary table (table 2).This table builds a clearer picture of the competency expectations dependent on the prescribing model, and indicates current gaps in speech pathology prescribing competence.

Page
| 3
0 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Tabl
e 2:
Rel
atio
nshi
p be
twee
n th
e Pr
escr
ibin
g Co
mpe
tenc
ies F
ram
ewor
k, th
e HP
PP p
resc
ribin
g m
odel
s and
the
prof
essio
nal s
tand
ards
for s
peec
h pa
thol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Com
pete
ncy
Area
1 U
nder
stan
ds th
e pe
rson
and
thei
r clin
ical n
eeds
Elem
ent 1
.1 E
stab
lishe
s a th
erap
eutic
par
tner
ship
with
the
pers
on a
nd a
colla
bora
tive
rela
tions
hip
with
oth
er h
ealth
pro
fess
iona
ls
1.1.
1 Us
es a
ppro
pria
te
com
mun
icat
ion
stra
tegi
es to
es
tabl
ish a
ther
apeu
tic p
artn
ersh
ip
with
the
pers
on
Elem
ent 1
.2 P
erfo
rms a
com
preh
ensiv
e m
edic
ines
ass
essm
ent t
o ob
tain
info
rmat
ion
to u
nder
stan
d th
e pe
rson
’s cl
inica
l nee
ds a
nd co
ntex
t
1.2.
1 Co
nduc
ts a
n as
sess
men
t tha
t is
appr
opria
te to
bot
h th
e he
alth
pr
ofes
siona
l’s sc
ope
of p
ract
ice a
nd
the
pers
on’s
clini
cal c
onte
xt
1.2.
2 Re
view
s and
inte
rpre
ts
info
rmat
ion
in th
e pe
rson
’s he
alth
re
cord
s
Not
es
In
dica
tes a
per
form
ance
crit
erio
n co
nsid
ered
ess
entia
l for
that
mod
el o
f pre
scrib
ing
In
dica
tes a
per
form
ance
crit
erio
n no
t con
sider
ed e
ssen
tial f
or th
at m
odel
of p
resc
ribin
g
# Ac
cord
ing
to re
leva
nt le
gisla
tion.
Not
e ac
cord
ing
to th
e Pr
escr
ibin
g Co
mpe
tenc
ies F
ram
ewor
k, a
pre
scrip
tion
may
pro
vide
an
orde
r to
adm
inist
er, r
athe
r th
an d
ispen
se.

Page
| 3
1 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
1.2.
3 O
btai
ns re
leva
nt in
form
atio
n fr
om th
e pe
rson
abo
ut th
eir
med
icin
es, a
nd th
eir m
edic
al a
nd
clin
ical
hist
ory,
inclu
ding
thei
r co-
exist
ing
cond
ition
s, tr
eatm
ents
, al
coho
l and
subs
tanc
e us
e, a
llerg
ies
and
soci
al co
ntex
t
1.2.
4 As
sess
es th
e pe
rson
’s ris
k fa
ctor
s for
poo
r adh
eren
ce; f
or
exam
ple
soci
al is
olat
ion,
phy
sical
im
pairm
ent,
cogn
itive
impa
irmen
t or
dist
urba
nce,
low
Eng
lish
prof
icien
cy,
low
hea
lth li
tera
cy, f
inan
cial
di
sadv
anta
ge
1.2.
5 As
cert
ains
that
suffi
cient
in
form
atio
n ha
s bee
n ob
tain
ed a
bout
th
e pe
rson
’s co
-exi
stin
g co
nditi
ons
and
curr
ent t
reat
men
ts to
iden
tify
poss
ible
risk
s and
cont
rain
dica
tions
fo
r tre
atm
ent
1.2.
6 Pe
rform
s clin
ical
exa
min
atio
ns
that
are
with
in th
e he
alth
pr
ofes
siona
l’s o
wn
scop
e of
pra
ctice
an
d re
leva
nt to
the
pers
on’s
prob
lem
an
d in
terp
rets
the
findi
ngs o
f the
se
exam
inat
ions

Page
| 3
2 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Elem
ent 1
.3 G
ener
ates
and
exp
lore
s pos
sible
dia
gnos
es
1.3.
1 Sy
nthe
sises
info
rmat
ion
from
th
e co
mpr
ehen
sive
asse
ssm
ent a
nd
deve
lops
pro
visio
nal a
nd d
iffer
entia
l di
agno
ses
1.3.
2 De
velo
ps a
dia
gnos
tic st
rate
gy
and
perf
orm
s rel
evan
t inv
estig
atio
ns
1.3.
3 Ex
plai
ns th
e cli
nica
l iss
ues a
nd
thei
r im
plica
tions
to th
e pe
rson
Com
pete
ncy
Area
2 T
reat
men
t opt
ions
: Un
ders
tand
s the
trea
tmen
t opt
ions
and
how
they
supp
ort t
he p
erso
n’s c
linica
l nee
d
Elem
ent 2
.1 C
onsid
ers n
on-p
harm
acol
ogica
l tre
atm
ent o
ptio
ns su
itabl
e fo
r tre
atin
g th
e pe
rson
and
thei
r con
ditio
n
2.1.
1 Re
cogn
ises w
hen
it is
clini
cally
ap
prop
riate
not
to in
terv
ene;
for
exam
ple,
in ca
ses w
here
the
signs
an
d sy
mpt
oms a
re li
kely
to re
solv
e w
ithou
t tre
atm
ent

Page
| 3
3 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
2.1.
2 Re
cogn
ises w
hen
it is
clini
cally
ap
prop
riate
to im
plem
ent n
on-
phar
mac
olog
ical t
reat
men
ts
Elem
ent 2
.2 Id
entif
ies a
ppro
pria
te m
edici
nes o
ptio
ns th
at ca
n be
inco
rpor
ated
into
the
pers
on’s
trea
tmen
t pla
n
2.2.
1 In
tegr
ates
kno
wle
dge
of
phar
mac
olog
y, o
ther
bio
med
ical
sc
ienc
es, c
linica
l med
icine
, and
th
erap
eutic
s and
iden
tifie
s med
icine
s su
itabl
e fo
r tre
atin
g th
e co
nditi
on
✗
2.2.
2 O
btai
ns, i
nter
pret
s, an
d ap
plie
s cu
rren
t evi
denc
e an
d in
form
atio
n ab
out m
edici
nes t
o in
form
dec
ision
s ab
out i
ncor
pora
ting
med
icine
s int
o th
e pe
rson
’s tr
eatm
ent p
lan
✗
2.2.
3 Id
entif
ies m
edic
ines
opt
ions
th
at a
re li
kely
to p
rovi
de
ther
apeu
tical
ly e
ffect
ive
and
safe
tr
eatm
ent a
nd ta
ilors
them
for t
he
pers
on
✗
2.2.
4 Co
nsid
ers t
he co
st a
nd
affo
rdab
ility
of t
he m
edici
nes t
o th
e pe
rson
✗

Page
| 3
4 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
2.2.
5 Co
nsid
ers t
he im
plic
atio
ns to
th
e w
ider
com
mun
ity o
f usin
g a
part
icula
r med
icine
to tr
eat t
he
pers
on
✗
2.2.
6 Di
scus
ses t
he tr
eatm
ent o
ptio
ns
and
med
icine
s with
the
pers
on,
cons
ider
ing:
the
prio
ritie
s for
tr
eatin
g th
eir c
urre
nt c
ondi
tion
and
co-e
xist
ing
cond
ition
s; th
eir r
eadi
ness
to
add
ress
the
curr
ent c
ondi
tion;
th
eir e
xpec
tatio
ns o
f tre
atm
ent
2.2.
7 Su
pple
men
ts v
erba
l inf
orm
atio
n w
ith w
ritte
n in
form
atio
n ab
out t
he
cond
ition
and
trea
tmen
t opt
ions
(w
here
app
ropr
iate
)
2.2.
8 Al
low
s the
per
son
time
to m
ake
an in
form
ed d
ecisi
on a
bout
thei
r tr
eatm
ent
2.2.
9 Re
fers
the
pers
on fo
r fur
ther
as
sess
men
t or t
reat
men
t whe
n th
e su
itabl
e tr
eatm
ent o
ptio
ns a
re
outs
ide
the
heal
th p
rofe
ssio
nal’s
ow
n sc
ope
of p
ract
ice

Page
| 3
5 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Com
pete
ncy
Area
3 S
hare
d de
cisio
n m
akin
g: W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
to d
evel
op a
nd im
plem
ent a
trea
tmen
t pla
n
Elem
ent 3
.1 N
egot
iate
s the
rape
utic
goal
s with
the
pers
on
3.1.
1 Ne
gotia
tes t
hera
peut
ic go
als
that
enh
ance
the
pers
on’s
self-
man
agem
ent o
f the
ir co
nditi
on
✗
3.1.
2 As
cert
ains
that
all
part
ies h
ave
a co
mm
on u
nder
stan
ding
of t
he
ther
apeu
tic g
oals
and
how
they
will
be
man
aged
Elem
ent 3
.2 W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
sele
ct m
edic
ines
and
to ta
ilor a
nd im
plem
ent a
trea
tmen
t pla
n
3.2.
1 Ex
plor
es th
e pe
rson
’s op
inio
ns
and
pref
eren
ces c
once
rnin
g m
edic
ines
and
the
trea
tmen
t pla
n
✗
3.2.
2 Co
nsul
ts o
ther
hea
lth
prof
essio
nals
abou
t pot
entia
l m
edic
ines
and
the
trea
tmen
t pla
n
3.2.
3 Re
ache
s agr
eem
ent w
ith th
e pe
rson
abo
ut m
edici
nes t
o be
use
d to
tr
eat t
heir
cond
ition
✗
3.2.
4 De
velo
ps th
e tr
eatm
ent p
lan
in
part
ners
hip
with
the
pers
on
✗

Page
| 3
6 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
3.2.
5 O
btai
ns a
ppro
val t
o us
e th
e m
edic
ines
(whe
re re
leva
nt)
✗ ✗
3.2.
6 St
ops o
r mod
ifies
the
pers
on’s
exist
ing
med
icine
s and
oth
er
man
agem
ent s
trat
egie
s if r
equi
red
3.2.
7 En
sure
s the
per
son
unde
rsta
nds
the
trea
tmen
t pla
n an
d ho
w to
use
th
e m
edic
ine
safe
ly a
nd e
ffect
ivel
y
Elem
ent 3
.3 D
evel
ops a
revi
ew p
lan
tailo
red
to th
e pe
rson
’s ne
eds
3.3.
1 Id
entif
ies t
he n
eed
for,
and
deve
lops
a re
view
pla
n
Com
pete
ncy
Area
4 C
o-or
dina
tion:
Com
mun
icate
s the
trea
tmen
t pla
n cle
arly
to o
ther
hea
lth p
rofe
ssio
nals
Elem
ent 4
.1 P
rovi
des c
lear
inst
ruct
ions
to o
ther
hea
lth p
rofe
ssio
nals
who
disp
ense
, sup
ply,
or a
dmin
ister
med
icine
s pre
scrib
ed fo
r the
per
son
4.1.
1 Pr
epar
es p
resc
riptio
ns o
r m
edic
atio
n or
ders
that
com
ply
with
re
leva
nt le
gisla
tion,
gui
delin
es o
r co
des o
f pra
ctice
, and
org
anisa
tiona
l po
licie
s and
pro
cedu
res

Page
| 3
7 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
4.1.
2 Pr
ovid
es a
ccur
ate
and
clear
ve
rbal
med
icatio
n or
ders
that
com
ply
with
rele
vant
legi
slatio
n, g
uide
lines
or
code
s of p
ract
ice
and
orga
nisa
tiona
l pol
icies
and
pr
oced
ures
(whe
re re
leva
nt)
✗ #
#
Elem
ent 4
.2 P
rovi
des i
nfor
mat
ion
abou
t med
icin
es a
nd th
e tr
eatm
ent p
lan
with
the
pers
on’s
cons
ent t
o ot
her h
ealth
pro
fess
iona
ls w
ho p
rovi
de ca
re to
the
pers
on
4.2.
1 Pr
ovid
es in
form
atio
n fo
r co
llabo
ratio
n to
mem
bers
of i
nter
-pr
ofes
siona
l hea
lthca
re te
ams b
oth
with
in fa
ciliti
es a
nd th
e co
mm
unity
Com
pete
ncy
Area
5 M
onito
rs a
nd re
view
s: M
onito
rs a
nd re
view
s the
per
son’
s res
pons
e to
trea
tmen
t
Elem
ent 5
.1 O
btai
ns in
form
atio
n to
ass
ess t
he p
erso
n’s r
espo
nse
to tr
eatm
ent
5.1.
1 O
bser
ves t
he p
erso
n to
as
cert
ain
thei
r res
pons
e to
trea
tmen
t (w
here
rele
vant
)
5.1.
2 Di
scus
ses w
ith th
e pe
rson
and
ot
her h
ealth
pro
fess
iona
ls, th
eir:
ex
perie
nce
with
impl
emen
ting
the
trea
tmen
t pla
n
adhe
renc
e, in
cludi
ng a
ny is
sues
ar
ising
and
pos
sible
way
s to
impr
ove
adhe
renc
e

Page
| 3
8 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
pe
rcep
tion
or o
bser
vatio
n of
the
med
icin
es’ b
enef
its a
nd a
dver
se
effe
cts
as
sess
men
t of w
heth
er th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
5.1.
3 O
btai
ns a
dditi
onal
info
rmat
ion
to a
sses
s whe
ther
the
ther
apeu
tic
goal
s hav
e be
en a
chie
ved
by
exam
inin
g th
e pe
rson
, req
uest
ing
inve
stig
atio
ns, a
nd in
terp
retin
g th
e fin
ding
s (w
here
rele
vant
)
5.1.
4 Sy
nthe
sises
info
rmat
ion
prov
ided
by
the
pers
on, o
ther
hea
lth
prof
essio
nals,
and
from
clin
ical
exam
inat
ions
and
inve
stig
atio
ns to
de
term
ine
whe
ther
:
th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
trea
tmen
t sho
uld
be st
oppe
d,
mod
ified
or c
ontin
ued
th
e pe
rson
shou
ld b
e re
ferr
ed to
an
othe
r hea
lth p
rofe
ssio
nal

Page
| 3
9 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Elem
ent 5
.2 W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
add
ress
issu
es a
risin
g fro
m th
e re
view
5.2.
1 Di
scus
ses t
he fi
ndin
gs o
f the
re
view
with
the
pers
on
5.2.
2 Id
entif
ies i
f the
per
son
requ
ires
a co
mpr
ehen
sive
med
icine
s rev
iew
5.2.
3 W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
mod
ify th
e tr
eatm
ent p
lan
to
optim
ise th
e sa
fety
and
effe
ctiv
enes
s of
trea
tmen
t (w
here
rele
vant
)
5.2.
4 Re
port
s iss
ues a
risin
g fr
om th
e re
view
5.2.
5 O
rgan
ises t
he n
ext r
evie
w
Com
pete
ncy
Area
H1
Prof
essio
nal:
Prac
tices
pro
fess
iona
lly
Elem
ent H
1.1
Prac
tices
with
in th
e ap
plic
able
legi
slativ
e an
d re
gula
tory
fram
ewor
ks
H1.1
.1 D
emon
stra
tes k
now
ledg
e of
, an
d co
mpl
ies w
ith, l
egisl
atio
n,
regu
latio
ns, a
nd co
mm
on la
w
appl
icabl
e to
pre
scrib
ing
(as f
urth
er
defin
ed b
y th
e kn
owle
dge
subs
ectio
n of
this
com
pete
ncy
area
)

Page
| 4
0 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
H1.1
.2 M
aint
ains
acc
urat
e an
d co
mpl
ete
reco
rds o
f:
th
e co
nsul
tatio
n
clin
ical
exa
min
atio
ns a
nd
inve
stig
atio
n re
sults
risk
fact
ors f
or m
edici
nes
misa
dven
ture
the
pers
on’s
decis
ion
to d
eclin
e tr
eatm
ent (
whe
re re
leva
nt)
ch
ange
s to
the
pers
on’s
med
icine
s m
anag
emen
t pla
n, in
cludi
ng th
e ra
tiona
le b
ehin
d th
ese
chan
ges
th
e re
view
pla
n,
reco
mm
enda
tions
, and
dat
e fo
r ne
xt re
view
outc
omes
of t
reat
men
t
Elem
ent H
1.2
Prac
tices
acc
ordi
ng to
pro
fess
iona
l sta
ndar
ds, c
odes
of c
ondu
ct, a
nd w
ithin
the
heal
th p
rofe
ssio
nal’s
ow
n sc
ope
of p
ract
ice
H1.2
.1 D
emon
stra
tes k
now
ledg
e of
an
d co
mpl
ianc
e w
ith:
pr
ofes
siona
l sta
ndar
ds
co
des o
f con
duct
scop
e of
pra
ctice
stat
emen
ts o
r gu
idel
ines

Page
| 4
1 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
H1.2
.2 P
ract
ices w
ithin
the
limits
of
the
heal
th p
rofe
ssio
nal’s
ow
n ed
ucat
ion,
trai
ning
and
scop
e of
pr
actic
e
H1.2
.3 D
emon
stra
tes r
espe
ct fo
r the
sc
ope
of p
ract
ice o
f oth
er h
ealth
pr
ofes
siona
ls an
d th
eir c
ontr
ibut
ion
with
in a
col
labo
rativ
e ca
re m
odel
, pa
rticu
larly
that
of t
he p
erso
n’s m
ain
heal
thca
re p
rovi
der
H1.2
.4 A
ccep
ts re
spon
sibili
ty a
nd is
ac
coun
tabl
e fo
r the
car
e pr
ovid
ed to
th
e pe
rson
Elem
ent H
1.3
Prac
tices
with
in th
e ap
plic
able
fram
ewor
ks o
f the
hea
lthca
re se
ttin
g an
d sy
stem
H1.3
.1 D
emon
stra
tes k
now
ledg
e of
an
d co
mpl
ies w
ith n
atio
nal,
stat
e an
d te
rrito
ry, a
nd fa
cility
pol
icies
and
pr
oced
ures
in re
latio
n to
pre
scrib
ing
H1.3
.2 D
emon
stra
tes a
ppro
pria
te
prof
essio
nal j
udge
men
t whe
n in
terp
retin
g an
d ap
plyi
ng g
uide
lines
an
d pr
otoc
ols t
o th
e pe
rson
’s sit
uatio
n

Page
| 4
2 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
H1.3
.3 C
ontr
ibut
es to
the
impr
ovem
ent o
f pol
icies
and
pr
oced
ures
for t
he ju
dici
ous,
appr
opria
te, s
afe
and
effe
ctiv
e us
e of
m
edic
ines
✗
Elem
ent H
1.4
Prac
tices
qua
lity
use
of m
edici
nes p
rinci
ples
H1.4
.1 A
pplie
s qua
lity
use
of
med
icin
es p
rinci
ples
whe
n pr
escr
ibin
g m
edici
nes
H1.4
.2 Id
entif
ies c
omm
on c
ause
s of
med
icin
es e
rror
s and
adv
erse
eve
nts,
and
impl
emen
ts st
rate
gies
to re
duce
th
e ris
ks o
f the
se o
ccur
ring
H1.4
.3 D
emon
stra
tes k
now
ledg
e of
th
e m
edic
ines
com
mon
ly p
resc
ribed
H1.4
.4 C
ritica
lly e
valu
ates
in
form
atio
n ab
out m
edici
nes a
nd
mak
es e
vide
nce-
base
d de
cisio
ns
abou
t med
icine
s in
the
heal
th
prof
essio
nal’s
ow
n pr
actic
e
✗

Page
| 4
3 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Elem
ent H
1.5
Dem
onst
rate
s a co
mm
itmen
t to
cont
inua
l qua
lity
impr
ovem
ent o
f the
hea
lth p
rofe
ssio
nal’s
ow
n pr
escr
ibin
g
H1.5
.1 E
ngag
es in
ong
oing
pr
ofes
siona
l dev
elop
men
t and
ed
ucat
ion
to im
prov
e pr
escr
ibin
g pr
actic
es
Elem
ent H
1.6
Addr
esse
s the
pot
entia
l for
bia
s in
pres
crib
ing
deci
sions
H1.6
.1 Im
plem
ents
stra
tegi
es to
ad
dres
s inf
luen
ces t
hat m
ay b
ias
pres
crib
ing
decis
ions
, inc
ludi
ng:
M
arke
ting
influ
ence
s
Poss
ible
per
sona
l, pr
ofes
siona
l or
finan
cial g
ain
Co
nflic
ts o
f int
eres
t
The
heal
th p
rofe
ssio
nal’s
ow
n be
liefs
, val
ues,
and
expe
rienc
es
✗
Com
pete
ncy
Area
H2
Com
mun
icate
s: Co
mm
unica
tes a
nd co
llabo
rate
s effe
ctiv
ely
with
the
pers
on a
nd o
ther
hea
lth p
rofe
ssio
nals
Elem
ent H
2.1
Obta
ins c
onse
nt to
pro
vide
clin
ical s
ervi
ces t
o th
e pe
rson
H2.1
.1 A
dher
es to
legi
slativ
e an
d w
orkp
lace
requ
irem
ents
for o
btai
ning
an
d re
cord
ing
cons
ent f
or:
ac
cess
ing
heal
th re
cord
s

Page
| 4
4 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
ob
tain
ing
info
rmat
ion
from
, and
pr
ovid
ing
info
rmat
ion
to, o
ther
he
alth
pro
fess
iona
ls
cond
uctin
g a
clini
cal e
xam
inat
ion
pr
ovid
ing
clini
cal s
ervi
ces
th
e po
tent
ial b
enef
its a
nd h
arm
s of
trea
tmen
t
the
finan
cial a
spec
ts o
f the
tr
eatm
ent
Elem
ent H
2.2
Ackn
owle
dges
the
pers
on, t
heir
fam
ily, a
nd ca
rers
as i
nteg
ral t
o ca
re a
nd co
llabo
rate
s to
achi
eve
optim
al h
ealth
out
com
es
H2.2
.1 In
volv
es th
e pe
rson
’s fa
mily
or
care
rs in
the
cons
ulta
tion
whe
re
appr
opria
te
H2.2
.2 E
xplo
res a
nd re
spon
ds
appr
opria
tely
to th
e pe
rson
’s co
ncer
ns a
nd e
xpec
tatio
ns re
gard
ing:
the
cons
ulta
tion
th
eir h
ealth
thei
r ow
n ro
le a
nd th
at o
f hea
lth
prof
essio
nals
in m
anag
ing
thei
r he
alth
the
heal
th p
rofe
ssio
nal’s
scop
e of
pr
actic
e

Page
| 4
5 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
th
e us
e of
med
icine
s and
oth
er
trea
tmen
ts to
mai
ntai
n th
eir
heal
th
H2.2
.3 E
stab
lishe
s a th
erap
eutic
pa
rtne
rshi
p th
at a
ccor
ds w
ith th
e pr
efer
ence
s exp
ress
ed b
y th
e pe
rson
Elem
ent H
2.3
Resp
ects
the
pers
on
H2.3
.1 R
espe
cts t
he p
erso
n’s v
alue
s, be
liefs
, and
exp
erie
nces
H2.3
.2 R
espe
cts t
he p
erso
n’s p
rivac
y an
d co
nfid
entia
lity
H2.3
.3 R
espe
cts t
he p
erso
n’s
heal
thca
re d
ecisi
ons
Elem
ent H
2.4
Com
mun
icate
s effe
ctiv
ely
with
the
pers
on u
sing
appr
opria
te co
mm
unic
atio
n sk
ills t
o en
able
the
safe
use
of m
edici
nes
H2.4
.1 A
sses
ses t
he p
erso
n’s
pref
erre
d la
ngua
ge, c
omm
unic
atio
n st
yle,
com
mun
icatio
n ca
pabi
litie
s, an
d he
alth
lite
racy
, and
adj
usts
the
heal
th p
rofe
ssio
nal’s
ow
n co
mm
unic
atio
n st
yle
to in
tera
ct
effe
ctiv
ely
with
them
H2.4
.2 C
onsid
ers t
he p
oten
tial i
ssue
of
per
ceiv
ed p
ower
diff
eren
ces

Page
| 4
6 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
betw
een
the
heal
th p
rofe
ssio
nal a
nd
the
pers
on
H2.4
.3 P
rovi
des c
lear
and
app
ropr
iate
w
ritte
n an
d ve
rbal
info
rmat
ion
to th
e pe
rson
to e
nabl
e th
em to
mak
e in
form
ed ch
oice
s and
ach
ieve
opt
imal
he
alth
out
com
es
H2.4
.4 A
scer
tain
s tha
t the
in
form
atio
n pr
ovid
ed h
as b
een
rece
ived
and
und
erst
ood
corr
ectly
Elem
ent H
2.5
Colla
bora
tes w
ith o
ther
hea
lth p
rofe
ssio
nals
to a
chie
ve o
ptim
al h
ealth
out
com
es fo
r the
per
son
H2.5
.1 E
ngag
es in
ope
n, in
tera
ctiv
e di
scus
sions
with
oth
er h
ealth
pr
ofes
siona
ls in
volv
ed in
carin
g fo
r th
e pe
rson
H2.5
.2 C
onfir
ms t
hat t
heir
own
unde
rsta
ndin
g of
info
rmat
ion
prov
ided
by
othe
r hea
lth
prof
essio
nals
is co
rrec
t
H2.5
.3 R
espo
nds a
ppro
pria
tely
to
com
mun
icat
ion
initi
ated
by
othe
r he
alth
pro
fess
iona
ls

Page
| 4
7 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
spee
ch p
atho
logi
st
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
spee
ch
path
olog
ist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
spee
ch p
atho
logi
st
H2.5
.4 P
rovi
des c
lear
ver
bal a
nd
writ
ten
info
rmat
ion
to o
ther
hea
lth
prof
essio
nals
by se
cure
mea
ns w
hen
impl
emen
ting
new
trea
tmen
ts w
ith
med
icin
es o
r mod
ifyin
g ex
istin
g tr
eatm
ent p
lans

Page | 48 A review of the prescribing capability of speech pathologists, dietitians and psychologists
6.3.3 Discussion
The Competency-based Occupational Standards for speech pathologists and the Code of Ethics provide a comprehensive description of the capabilities of an entry level speech pathologist. Minor adjustments to include reference regarding medicines could improve mapping in areas such as obtaining information from the patient as well as therapeutic selection and implementation.
It is likely that some of the prescribing activities that do not map well are undertaken in actual practice but, due to their lack of documentation in the professional standards, are perceived not to map to the Prescribing Competencies Framework. These include the following:
Allows the person time to make an informed decision about their treatment Negotiates therapeutic goals that enhance the person’s self-management of their condition Ascertains that all parties have a common understanding of the therapeutic goals and how they
will be managed Organises the next review Considers the potential issue of perceived power differences between the health professional
and the person Ascertains that the information provided has been received and understood correctly Confirms that their own understanding of information provided by other health professionals is
correct Responds appropriately to communication initiated by other health professionals
Areas that do not map well, and are likely to fall outside of the current scope of practice should be targeted for additional education and assessment, these include the following:
Medication and allergy history taking Adherence assessment Medication selection competencies
o Identification of safe, appropriate, effective medicine options o Stopping or modifying existing medicines if required o Medication knowledge o QUM principles
Medication orders Legislative requirements relating to medicines
Mapping of the learning objectives for the representative pre-entry program of study provided limited information to assess graduate capability with respect to prescribing. The learning objectives are quite broad in their statements and, without review of individual lectures and tutorials, it is impossible to say to what extent they map with the Prescribing Competencies Framework. Mapping at an element level rather than a performance criteria level is also less specific; not all performance criteria within the element may be covered by the learning objectives. This mapping does, however, give an indication of the coverage of the Prescribing Competencies Framework by a SPA accredited program of study.
Some of the elements which could not be identified in the learning objectives such as obtaining consent and obtaining information to assess the person’s response to treatment are likely to be covered in clinical placements. Other such as providing instruction to other health professionals who

Page | 49 A review of the prescribing capability of speech pathologists, dietitians and psychologists
dispense, supply, or administer medicines prescribed for the person or practicing quality use of medicines principles are clearly outside of current scope and would require an addition to the curriculum.
As indicated in table 2, the requisite competencies for safe and effective prescribing differ dependent on the model of prescribing to be used. The number of competencies required to prescribe under supervision or autonomously is greater than those required to prescribe via a structured prescribing arrangement. This information can be used to identify the additional training that would be required to achieve speech pathology prescribing competence dependent on the model of prescribing. Table A3, appendix A shows the competencies not met or only partly met by the speech pathology standards and indicates the additional training required dependent on the prescribing model. The additional training required for prescribing under a structured prescribing arrangement is as follows:
Medication history taking training, including adherence assessment Interpretation and application of guidelines and protocols appropriate to model of
prescribing QUM principles appropriate to model of prescribing Knowledge of the medicines to be prescribed (including potential adverse reactions and
errors) Identification of potential problems with existing medicines and cessation or adjustment as
appropriate Obtaining and recording consent for medicine use Legislation, policies and procedures applicable to model of prescribing Writing of medicine orders appropriate to model of prescribing Recording keeping with respect to medicine use Review of medicine therapy Identification of person’s need for comprehensive medicines review Communication with the person regarding medicine choice, safe and effective use of the
medicine and experience with medicine use Consulting other health professionals with respect to medicine choice
To prescribe under supervision or autonomously the following additional training to that described above is required:
Knowledge of pharmacology, clinical medicine and therapeutics Access, interpretation, evaluation and application of medicine information to inform
evidence based decision making Identification of appropriate medicine options for both the condition and the person being
treated Tailoring of medicine to person’s needs Consideration of cost of medicines to be prescribed Implication to the wider community with respect to prescribing Communication with the person with respect to opinions and preferences regarding
medicines and the treatment plan Communication with respect to medicines options and reaching agreement with the person Ethical issues with respect to prescribing Provision of verbal orders if required appropriate for model of prescribing
Page | 50 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Obtaining approval for medicine use if required
There are a number of routes by which competency to prescribe could be achieved. The competencies to prescribe via a structured prescribing arrangement could be incorporated into pre-entry programs of study with minimal adjustment. Authority to prescribe under supervision or autonomously requires additional training, which could be provided in the way of postgraduate training with appropriate assessment to ensure competency. The majority of the competencies are not profession specific, so there is the possibility of the development of a generic allied health prescribing course. This could be provided in combination with workplace supervision and mentoring, to train and subsequently assess speech pathology prescribers. Over time it may be possible to incorporate all aspects of prescribing into pre-entry programs of study.
In order to progress the introduction of speech pathologist prescribing of scheduled medicines within scope of practice, processes around the accreditation of prescribing training programs and recognition of prescriber status need to be developed.
In December 2013, following the development of the Prescribing Competencies Framework and the HPPP, the Health Profession Accreditation Councils’ Forum released a position statement ‘Development of Prescribing Standards and Accreditation Processes’(30). The position statement acknowledged the Prescribing Competencies Framework as the nationally recognised standard for prescribing, and stated that standards for prescribing education and training programs of study must align to the framework. The document also stated ‘The Forum is working with its Members to ensure efficient and effective accreditation processes are developed at the same time respecting the diversity of approaches of individual accreditation councils to these processes’.
In addition AHPRA has established a Prescribing Working Group whose aim is to ‘develop a governance framework and other resources to support the development and review of national board regulatory policy relating to prescribing of scheduled medicines’(6). This working group provides a useful mechanism to facilitate active collaboration between health professions and the Forum, with a view to consistency of accreditation. Whilst SPA is neither a member body of the Forum or AHPRA, it is possible that they could adopt any accreditation framework that is developed and use it to accredit prescribing training programs suitable for speech pathology prescribing. Alternatively SPA could independently develop their own accreditation standards. As an ongoing goal the Prescribing Competencies Framework should be embedded in any prescribing accreditation standards developed. This approach is evidenced in the 2015 Nurse Practitioner and Endorsement for Scheduled Medicines for Midwives Accreditation Standards, both of which require a map of subjects against the Prescribing Competencies Framework(31, 32).
6.4 Recommendations
If speech pathology prescribing is to occur, consideration needs to be given to the process by which speech pathologists are recognised as competent to prescribe. As discussed previously, in Queensland the authority to prescribe is legislated under the Health (Drugs and Poisons) Regulation 1996 (HDPR), therefore, amendments to the regulation would be required to authorise speech pathologists to prescribe. As a temporary measure, prescribing could occur within Queensland under the section 18 approval process, which has been used previously to authorise prescribing trials in pharmacy and physiotherapy.

Page | 51 A review of the prescribing capability of speech pathologists, dietitians and psychologists
If speech pathology prescribing is to occur at a national level, professional standards should be revised to include prescribing competencies. Amendments to the relevant medicines regulation in each state and territory would also be required.
In order to progress speech pathology prescribing it is recommended that SPA:
Develop or adopt an accreditation framework and use it to accredit prescribing training programs suitable for speech pathology prescribing
Establish a process to credential speech pathologists to prescribe, dependent on completion of an accredited prescribing program of study. In order to maintain continuing professional development standards and currency of practice, only Certified Practising Speech Pathologists should be credentialed to prescribe

Page | 52 A review of the prescribing capability of speech pathologists, dietitians and psychologists
7. Dietetics and Nutrition 7.1 Background Information
In Australia the title of dietitian is differentiated from other occupations in the nutrition industry such as nutritionist. A dietitian is defined as having ‘undertaken a course of study that included substantial theory and supervised and assessed professional practice in clinical nutrition, medical nutrition therapy and food service management’(33).Whilst all dietitians can, therefore, be considered as nutritionists, a nutritionist cannot use the title dietitian without an approved dietetic qualification. For the purpose of this report the profession of dietetics alone will be reviewed.
The total number of dietitians in Australia is unclear as the 2011 Australian Bureau of Statistics consensus did not allow for differentiation between the terms dietitian and nutritionist. Whilst 6,200 people reported having a bachelor or postgraduate degree as their highest level of qualification in nutrition and dietetics, only 2,832 reported dietitian as their occupation(34).
7.1.1 National Bodies/Registration
There is no dietetic board established under the National Law(26), and hence no legal requirement for dietitians to be registered in Australia.
National representation is provided by the Dietitians Association of Australia (DAA), which is the major body for dietitians in Australia, with over 5,700 members(35). DAA has a number of functions including advocacy, professional representation, accreditation, education and provision of professional development activities.
DAA is a self-regulating body and is committed to ensuring a high standard of ethical and clinical practice by its members. A regulatory framework is provided in the form of professional standards, a Code of Professional Conduct and Statement of Ethical Practice. In addition DAA has a credentialing program for dietitians; the Accredited Practising Dietitian (APD) program. This program, which is administered by the Dietetic Credentialing Council (DCC), provides the only national credential which is recognised by the Australian Government, state governments and private health insurers. In order to become an APD a dietitian must complete an initial provisional year, which involves completion of CPD and having an APD mentor for at least 52 weeks. In addition a minimum of 30 hours of CPD must be completed per year on an ongoing basis(36). It is not mandatory for dietitians holding the APD credential to be members of DAA.
DAA have previously submitted a response to the Health Workforce Australia HPPP project indicating that self-regulated professions should have access to the HPPP.
7.1.2 Education and Training
DAA is the accrediting body for programs of study leading to the dietetic qualification in Australia, with the Australian Dietetics Council providing governance to the accreditation process. Only graduates from accredited dietetic programs are allowed to become members of DAA and join the APD program.
A dietetic qualification can be achieved by completion of a four year accredited undergraduate Bachelor degree, or a two year accredited postgraduate Master’s degree. Both routes produce entry

Page | 53 A review of the prescribing capability of speech pathologists, dietitians and psychologists
level graduates who are sufficiently competent to provide patient services, commensurate with an entry level practitioner, without any period of formal internship or supervision.
7.1.3 Current Prescribing Status
Dietitians currently have no prescribing authority in Australia. In some organisations dietitians are already involved in the ordering of unscheduled medicines such as phosphate binders for chronic renal disease, and total parenteral nutrition.
7.1.4 Prescribing potential
Dietitians who have the management of diabetes within their scope of practice, may be given authority to prescribe scheduled medicines that are relevant to the management of diabetes. Such prescribing would be similar to that in New Zealand where Registered Nurses specialising in diabetes are authorised to prescribe a range of medicines from the following classes(37, 38):
Insulin Metformin Sulphonylureas Statins Angiotensin receptor blockers Diuretics Angiotensin converting enzyme inhibitors Calcium channel blockers Aspirin
Dietitians practising in the area of cystic fibrosis management may be able to prescribe pancreatic enzyme replacement therapy (whilst the 10,000 units preparation is unscheduled, the higher 25,000 units and 40, 000 units preparations are both schedule 4). The 2014 DAA cystic fibrosis role statement states that whilst prescribing pancreatic enzymes is not an activity APDs working in this area usually undertake, there is the potential for extended scope of dietetic practice in the future(39).
7.2 Prescribing Competence in Dietetics
In order to consider the prescribing potential of the dietitian, and to identify options in Queensland relating to prescribing authority, it is necessary to review the current status of dietetic qualifications and evaluate their capacity to provide the skills, knowledge and behaviours necessary to become a competent prescriber. As discussed previously, such competence is described in the Prescribing Competencies Framework. If the current training requirements and professional standards for dietitians are mapped against the framework, it will be possible to evaluate the current prescribing capability of dietitians and identify any gaps in capability that may need to be addressed.
7.2.1 Dietitian training requirements and professional standards which define professional capability
All entry level degree programs in Australia, accredited by DAA, are assessed against the recently revised DAA National Competency Standards for Dietitians in Australia(40). All dietetic programs of study have to demonstrate their graduates attain these competencies in order to be accredited. The Standards detail the knowledge, skills and professional standards required for entry level practice.

Page | 54 A review of the prescribing capability of speech pathologists, dietitians and psychologists
All practising dietitians should, therefore, have minimum standards of practice commensurate with the National Competency Standards.
In addition to the National Competency Standards, DAA also produces the Code of Professional Conduct and Statement of Ethical Practice(41, 42). The Code of Professional Conduct sets minimum national standards for accountable conduct. The values and principles underpinning these standards are defined in the Statement of Ethical Practice. Note the DAA produces two versions of each document. The version for members with Australian recognised dietetic qualifications and non-members with APD status (i.e. relevant to dietitians) is the version that will be referred to within this report.
Together the National Competency Standards and the Statement of Ethical Practice define the competencies and practice requirements of a dietitian. It is, therefore, reasonable to assume that if both the standards are mapped against the Prescribing Competencies Framework, a clearer picture of prescribing readiness will emerge.
7.3 Dietetic Competency Mapping
7.3.1 Methodology
Both the National Competency Standards for Dietitians in Australia and the DAA Statement of Ethical Practice were mapped against individual performance criteria for every element within the Prescribing Competencies Framework. The mapping is shown in table B1, appendix B. The comments section of the table denotes whether statements identified in either one or both of the professional standards can be considered to map completely, partly, or not at all with the Prescribing Competencies Framework. The comments section is colour coded as follows:
Green denotes that a particular prescribing competency performance criterion maps well, and is covered sufficiently by either one or both of the standards
Orange denotes that the particular prescribing competency performance criterion is covered partly by either one or both of the standards
Red denotes that the particular prescribing competency performance criterion cannot be identified in either of the standards
To provide additional education and training information relevant to the review, the learning objectives from a DAA accredited dietetic program of study were also mapped against the Prescribing Competencies Framework elements. Learning objectives from Queensland University of Technology (QUT) Bachelor of Nutrition and Dietetics were mapped as a representative program of study.
7.3.2 Results
PProfessional Standards Mapping
Table 3 provides a summary of the mapping results. The table shows competencies from the Prescribing Competencies Framework separated into different categories, and indicates which of the prescribing competencies within each category are covered completely, partly, or not at all by the dietetic standards. It should be noted that the capability assumptions made in the mapping process are based purely on information obtained from the dietetic standards, and not on review of actual practice.

Page
| 5
5 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Tabl
e 3:
Die
tetic
map
ping
sum
mar
y: e
xten
t to
whi
ch th
e Pr
escr
ibin
g Co
mpe
tenc
ies F
ram
ewor
k is
cove
red
by th
e di
etet
ic st
anda
rds
Inte
ract
ion
and
com
mun
icatio
n w
ith p
atie
nts
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
1.1.
1
Uses
app
ropr
iate
com
mun
icat
ion
stra
tegi
es to
est
ablis
h a
ther
apeu
tic p
artn
ersh
ip w
ith th
e pe
rson
H2
.2.3
Est
ablis
hes a
ther
apeu
tic p
artn
ersh
ip th
at a
ccor
ds w
ith th
e pr
efer
ence
s exp
ress
ed b
y th
e pe
rson
H2
.3.1
Res
pect
s the
per
son’
s val
ues,
belie
fs, a
nd e
xper
ienc
es
H2.3
.2 R
espe
cts t
he p
erso
n’s p
rivac
y an
d co
nfid
entia
lity
H2.3
.3 R
espe
cts t
he p
erso
n’s h
ealth
care
dec
ision
s H2
.4.1
Ass
esse
s the
per
son’
s pre
ferr
ed la
ngua
ge, c
omm
unica
tion
styl
e, c
omm
unic
atio
n ca
pabi
litie
s, an
d he
alth
lite
racy
, and
adj
usts
the
heal
th p
rofe
ssio
nal’s
ow
n co
mm
unic
atio
n st
yle
to in
tera
ct e
ffect
ivel
y w
ith th
em
Pres
crib
ing
Com
pete
ncie
s cov
ered
par
tly
H2.2
.1 In
volv
es th
e pe
rson
’s fa
mily
or c
arer
s in
the
cons
ulta
tion
whe
re a
ppro
pria
te
H2.2
.2 E
xplo
res a
nd re
spon
ds a
ppro
pria
tely
to th
e pe
rson
’s co
ncer
ns a
nd e
xpec
tatio
ns re
gard
ing:
the
cons
ulta
tion
th
eir h
ealth
thei
r ow
n ro
le a
nd th
at o
f hea
lth p
rofe
ssio
nals
in m
anag
ing
thei
r hea
lth
th
e he
alth
pro
fess
iona
l’s sc
ope
of p
ract
ice
th
e us
e of
med
icine
s and
oth
er tr
eatm
ents
to m
aint
ain
thei
r hea
lth
H2.4
.3 P
rovi
des c
lear
and
app
ropr
iate
writ
ten
and
verb
al in
form
atio
n to
the
pers
on to
ena
ble
them
to m
ake
info
rmed
choi
ces a
nd a
chie
ve o
ptim
al h
ealth
out
com
es
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d H2
.4.2
Con
sider
s the
pot
entia
l iss
ue o
f per
ceiv
ed p
ower
diff
eren
ces b
etw
een
the
heal
th p
rofe
ssio
nal a
nd th
e pe
rson
H2
.4.4
Asc
erta
ins t
hat t
he in
form
atio
n pr
ovid
ed h
as b
een
rece
ived
and
und
erst
ood
corr
ectly
In
tera
ctio
n an
d co
mm
unica
tion
with
oth
er h
ealth
pro
fess
iona
ls Pr
escr
ibin
g co
mpe
tenc
ies c
over
ed c
ompl
etel
y 4.
2.1
Pr
ovid
es in
form
atio
n fo
r col
labo
ratio
n to
mem
bers
of i
nter
-pro
fess
iona
l hea
lthca
re te
ams b
oth
with
in fa
ciliti
es a
nd th
e co
mm
unity
Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed p
artly
H2
.5.1
Eng
ages
in o
pen,
inte
ract
ive
disc
ussio
ns w
ith o
ther
hea
lth p
rofe
ssio
nals
invo
lved
in c
arin
g fo
r the
per
son
H2.5
.4 P
rovi
des c
lear
ver
bal a
nd w
ritte
n in
form
atio
n to
oth
er h
ealth
pro
fess
iona
ls by
secu
re m
eans
whe
n im
plem
entin
g ne
w tr
eatm
ents
with
med
icine
s or m
odify
ing
exist
ing
trea
tmen
t pla
ns
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d H2
.5.2
Con
firm
s tha
t the
ir ow
n un
ders
tand
ing
of in
form
atio
n pr
ovid
ed b
y ot
her h
ealth
pro
fess
iona
ls is
corr
ect
H2.5
.3 R
espo
nds a
ppro
pria
tely
to co
mm
unic
atio
n in
itiat
ed b
y ot
her h
ealth
pro
fess
iona
ls

Page
| 5
6 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Asse
ssm
ent a
nd d
iagn
osis
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
1.2.
6
Perf
orm
s clin
ical
exa
min
atio
ns th
at a
re w
ithin
the
heal
th p
rofe
ssio
nal’s
ow
n sc
ope
of p
ract
ice a
nd re
leva
nt to
the
pers
on’s
prob
lem
and
inte
rpre
ts th
e fin
ding
s of
thes
e ex
amin
atio
ns
1.3.
1
Synt
hesis
es in
form
atio
n fr
om th
e co
mpr
ehen
sive
asse
ssm
ent a
nd d
evel
ops p
rovi
siona
l and
diff
eren
tial d
iagn
oses
Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed p
artly
1.
2.1
Co
nduc
ts a
n as
sess
men
t tha
t is a
ppro
pria
te to
bot
h th
e he
alth
pro
fess
iona
l’s sc
ope
of p
ract
ice
and
the
pers
on’s
clini
cal c
onte
xt
1.2.
2
Revi
ews a
nd in
terp
rets
info
rmat
ion
in th
e pe
rson
’s he
alth
reco
rds
1.2.
3
Obt
ains
rele
vant
info
rmat
ion
from
the
pers
on a
bout
thei
r med
icine
s, an
d th
eir m
edic
al a
nd cl
inic
al h
istor
y, in
clud
ing
thei
r co-
exist
ing
cond
ition
s, tr
eatm
ents
, al
coho
l and
subs
tanc
e us
e, a
llerg
ies a
nd so
cial c
onte
xt
1.2.
4
Asse
sses
the
pers
on’s
risk
fact
ors f
or p
oor a
dher
ence
; for
exa
mpl
e so
cial i
sola
tion,
phy
sical
impa
irmen
t, co
gniti
ve im
pairm
ent o
r dist
urba
nce,
low
Eng
lish
prof
icien
cy, l
ow h
ealth
lite
racy
, fin
anci
al d
isadv
anta
ge
1.3.
3
Expl
ains
the
clini
cal i
ssue
s and
thei
r im
plic
atio
ns to
the
pers
on
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d 1.
2.5
As
cert
ains
that
suffi
cien
t inf
orm
atio
n ha
s bee
n ob
tain
ed a
bout
the
pers
on’s
co-e
xist
ing
cond
ition
s and
curr
ent t
reat
men
ts to
iden
tify
poss
ible
risk
s and
co
ntra
indi
catio
ns fo
r tre
atm
ent
1.3.
2
Deve
lops
a d
iagn
ostic
stra
tegy
and
per
form
s rel
evan
t inv
estig
atio
ns
Ther
apeu
tic c
hoic
e an
d in
itiat
ion
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
2.1.
2
Reco
gnise
s whe
n it
is cli
nica
lly a
ppro
pria
te to
impl
emen
t non
-pha
rmac
olog
ical t
reat
men
ts
2.2.
9
Refe
rs th
e pe
rson
for f
urth
er a
sses
smen
t or t
reat
men
t whe
n th
e su
itabl
e tr
eatm
ent o
ptio
ns a
re o
utsid
e th
e he
alth
pro
fess
iona
l’s o
wn
scop
e of
pra
ctic
e 3.
1.1
Ne
gotia
tes t
hera
peut
ic go
als t
hat e
nhan
ce th
e pe
rson
’s se
lf-m
anag
emen
t of t
heir
cond
ition
3.
2.4
De
velo
ps th
e tr
eatm
ent p
lan
in p
artn
ersh
ip w
ith th
e pe
rson
Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed p
artly
2.
2.1
In
tegr
ates
kno
wle
dge
of p
harm
acol
ogy,
oth
er b
iom
edic
al sc
ienc
es, c
linica
l med
icine
, and
ther
apeu
tics a
nd id
entif
ies m
edici
nes s
uita
ble
for t
reat
ing
the
cond
ition
2.
2.2
O
btai
ns, i
nter
pret
s, an
d ap
plie
s cur
rent
evi
denc
e an
d in
form
atio
n ab
out m
edici
nes t
o in
form
dec
ision
s abo
ut in
corp
orat
ing
med
icine
s int
o th
e pe
rson
’s tr
eatm
ent p
lan
2.2.
4
Cons
ider
s the
cost
and
affo
rdab
ility
of t
he m
edici
nes t
o th
e pe
rson
2.
2.6
Di
scus
ses t
he tr
eatm
ent o
ptio
ns a
nd m
edici
nes w
ith th
e pe
rson
, con
sider
ing:
the
prio
ritie
s for
trea
ting
thei
r cur
rent
con
ditio
n an
d co
-exi
stin
g co
nditi
ons;
thei
r re
adin
ess t
o ad
dres
s the
curr
ent c
ondi
tion;
thei
r exp
ecta
tions
of t
reat
men
t 2.
2.7
Su
pple
men
ts v
erba
l inf
orm
atio
n w
ith w
ritte
n in
form
atio
n ab
out t
he co
nditi
on a
nd tr
eatm
ent o
ptio
ns (w
here
app
ropr
iate
) 3.
2.1
Ex
plor
es th
e pe
rson
’s op
inio
ns a
nd p
refe
renc
es co
ncer
ning
med
icine
s and
the
trea
tmen
t pla
n 3.
2.2
Co
nsul
ts o
ther
hea
lth p
rofe
ssio
nals
abou
t pot
entia
l med
icin
es a
nd th
e tr
eatm
ent p
lan

Page
| 5
7 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Ther
apeu
tic c
hoic
e an
d in
itiat
ion
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d 2.
1.1
Re
cogn
ises w
hen
it is
clini
cally
app
ropr
iate
not
to in
terv
ene;
for e
xam
ple,
in c
ases
whe
re th
e sig
ns a
nd sy
mpt
oms a
re li
kely
to re
solv
e w
ithou
t tre
atm
ent
2.2.
3
Iden
tifie
s med
icine
s opt
ions
that
are
like
ly to
pro
vide
ther
apeu
tical
ly e
ffect
ive
and
safe
trea
tmen
t and
tailo
rs th
e m fo
r the
per
son
2.2.
5
Cons
ider
s the
impl
icatio
ns to
the
wid
er co
mm
unity
of u
sing
a pa
rtic
ular
med
icin
e to
trea
t the
per
son
2.2.
8
Allo
ws t
he p
erso
n tim
e to
mak
e an
info
rmed
dec
ision
abo
ut th
eir t
reat
men
t 3.
1.2
As
cert
ains
that
all
part
ies h
ave
a co
mm
on u
nder
stan
ding
of t
he th
erap
eutic
goa
ls an
d ho
w th
ey w
ill b
e m
anag
ed
3.2.
3
Reac
hes a
gree
men
t with
the
pers
on a
bout
med
icine
s to
be u
sed
to tr
eat t
heir
cond
ition
3.
2.5
O
btai
ns a
ppro
val t
o us
e th
e m
edici
nes (
whe
re re
leva
nt)
3.2.
6
Stop
s or m
odifi
es th
e pe
rson
’s ex
istin
g m
edici
nes a
nd o
ther
man
agem
ent s
trat
egie
s if r
equi
red
3.2.
7
Ensu
res t
he p
erso
n un
ders
tand
s the
trea
tmen
t pla
n an
d ho
w to
use
the
med
icine
safe
ly a
nd e
ffect
ivel
y 4.
1.1
Pr
epar
es p
resc
riptio
ns o
r med
icat
ion
orde
rs th
at c
ompl
y w
ith re
leva
nt le
gisla
tion,
gui
delin
es o
r cod
es o
f pra
ctice
, and
org
anisa
tiona
l pol
icies
and
pro
cedu
res
4.1.
2
Prov
ides
acc
urat
e an
d cle
ar v
erba
l med
icatio
n or
ders
that
com
ply
with
rele
vant
legi
slatio
n, g
uide
lines
or c
odes
of p
ract
ice a
nd o
rgan
isatio
nal p
olici
es a
nd
proc
edur
es (w
here
rele
vant
) H1
.4.1
App
lies q
ualit
y us
e of
med
icine
s prin
cipl
es w
hen
pres
crib
ing
med
icine
s H1
.4.2
Iden
tifie
s com
mon
cau
ses o
f med
icine
s err
ors a
nd a
dver
se e
vent
s, an
d im
plem
ents
stra
tegi
es to
redu
ce th
e ris
ks o
f the
se o
ccur
ring
H1.4
.3 D
emon
stra
tes k
now
ledg
e of
the
med
icin
es c
omm
only
pre
scrib
ed
H1.4
.4 C
ritica
lly e
valu
ates
info
rmat
ion
abou
t med
icine
s and
mak
es e
vide
nce-
base
d de
cisio
ns a
bout
med
icine
s in
the
heal
th p
rofe
ssio
nal’s
ow
n pr
actic
e Re
view
and
adj
ustm
ent o
f the
rapy
Pr
escr
ibin
g co
mpe
tenc
ies c
over
ed c
ompl
etel
y 3.
3.1
Id
entif
ies t
he n
eed
for,
and
deve
lops
a re
view
pla
n 5.
2.3
W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
mod
ify th
e tr
eatm
ent p
lan
to o
ptim
ise th
e sa
fety
and
effe
ctiv
enes
s of t
reat
men
t (w
here
rele
vant
) Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed p
artly
5.
1.1
O
bser
ves t
he p
erso
n to
asc
erta
in th
eir r
espo
nse
to tr
eatm
ent (
whe
re re
leva
nt)
5.1.
2
Disc
usse
s with
the
pers
on a
nd o
ther
hea
lth p
rofe
ssio
nals,
thei
r:
expe
rienc
e w
ith im
plem
entin
g th
e tr
eatm
ent p
lan
ad
here
nce,
inclu
ding
any
issu
es a
risin
g an
d po
ssib
le w
ays t
o im
prov
e ad
here
nce
pe
rcep
tion
or o
bser
vatio
n of
the
med
icine
s’ be
nefit
s and
adv
erse
effe
cts
as
sess
men
t of w
heth
er th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
5.
1.4
Sy
nthe
sises
info
rmat
ion
prov
ided
by
the
pers
on, o
ther
hea
lth p
rofe
ssio
nals,
and
from
clin
ical e
xam
inat
ions
and
inve
stig
atio
ns to
det
erm
ine
whe
ther
:
the
ther
apeu
tic g
oals
have
bee
n ac
hiev
ed
tr
eatm
ent s
houl
d be
stop
ped,
mod
ified
or c
ontin
ued
th
e pe
rson
shou
ld b
e re
ferr
ed to
ano
ther
hea
lth p
rofe
ssio
nal
5.2.
1
Disc
usse
s the
find
ings
of t
he re
view
with
the
pers
on
5.2.
5
Orga
nise
s the
nex
t rev
iew
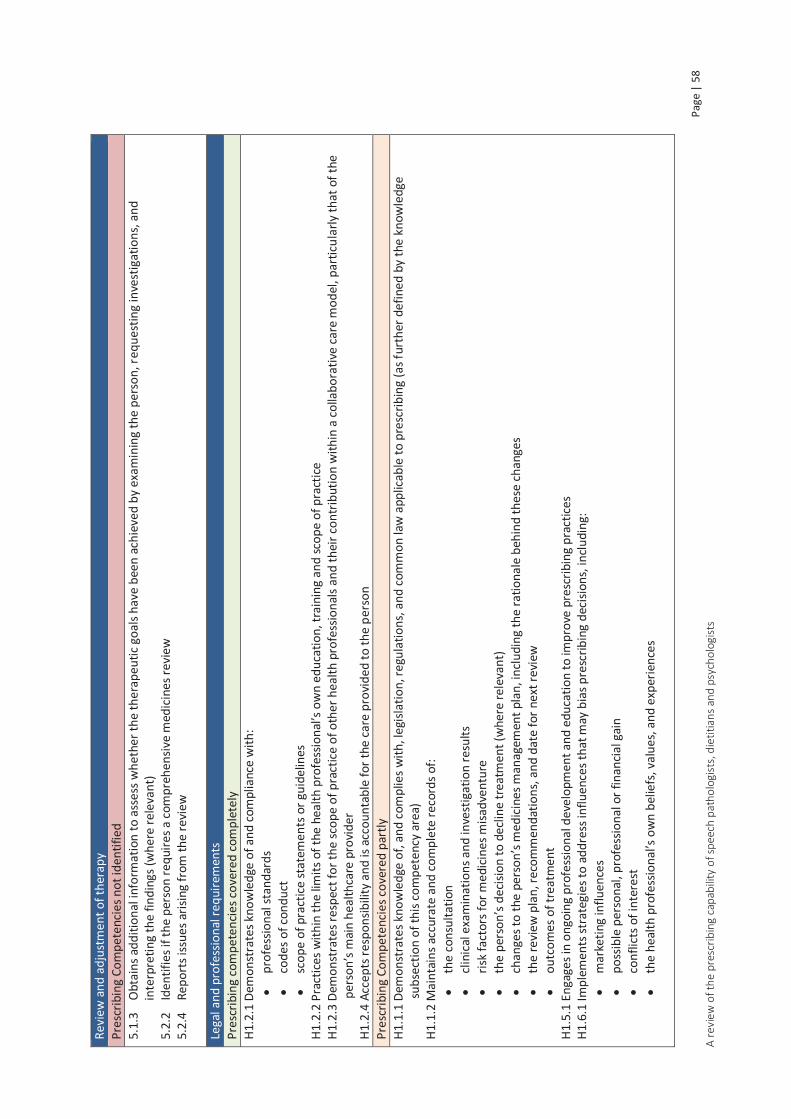
Page
| 5
8 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Revi
ew a
nd a
djus
tmen
t of t
hera
py
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d 5.
1.3
O
btai
ns a
dditi
onal
info
rmat
ion
to a
sses
s whe
ther
the
ther
apeu
tic g
oals
have
bee
n ac
hiev
ed b
y ex
amin
ing
the
pers
on, r
eque
stin
g in
vest
igat
ions
, and
in
terp
retin
g th
e fin
ding
s (w
here
rele
vant
) 5.
2.2
Id
entif
ies i
f the
per
son
requ
ires a
com
preh
ensiv
e m
edic
ines
revi
ew
5.2.
4
Repo
rts i
ssue
s aris
ing
from
the
revi
ew
Lega
l and
pro
fess
iona
l req
uire
men
ts
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
H1.2
.1 D
emon
stra
tes k
now
ledg
e of
and
com
plia
nce
with
:
prof
essio
nal s
tand
ards
code
s of c
ondu
ct
sc
ope
of p
ract
ice st
atem
ents
or g
uide
lines
H1
.2.2
Pra
ctice
s with
in th
e lim
its o
f the
hea
lth p
rofe
ssio
nal’s
ow
n ed
ucat
ion,
trai
ning
and
scop
e of
pra
ctice
H1
.2.3
Dem
onst
rate
s res
pect
for t
he sc
ope
of p
ract
ice o
f oth
er h
ealth
pro
fess
iona
ls an
d th
eir c
ontr
ibut
ion
with
in a
colla
bora
tive
care
mod
el, p
artic
ular
ly th
at o
f the
pe
rson
’s m
ain
heal
thca
re p
rovi
der
H1.2
.4 A
ccep
ts re
spon
sibili
ty a
nd is
acc
ount
able
for t
he ca
re p
rovi
ded
to th
e pe
rson
Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed p
artly
H1
.1.1
Dem
onst
rate
s kno
wle
dge
of, a
nd co
mpl
ies w
ith, l
egisl
atio
n, re
gula
tions
, and
com
mon
law
app
licab
le to
pre
scrib
ing
(as f
urth
er d
efin
ed b
y th
e kn
owle
dge
subs
ectio
n of
this
com
pete
ncy
area
) H1
.1.2
Mai
ntai
ns a
ccur
ate
and
com
plet
e re
cord
s of:
th
e co
nsul
tatio
n
clin
ical
exa
min
atio
ns a
nd in
vest
igat
ion
resu
lts
ris
k fa
ctor
s for
med
icine
s misa
dven
ture
the
pers
on’s
decis
ion
to d
eclin
e tr
eatm
ent (
whe
re re
leva
nt)
ch
ange
s to
the
pers
on’s
med
icine
s man
agem
ent p
lan,
incl
udin
g th
e ra
tiona
le b
ehin
d th
ese
chan
ges
th
e re
view
pla
n, re
com
men
datio
ns, a
nd d
ate
for n
ext r
evie
w
ou
tcom
es o
f tre
atm
ent
H1.5
.1 E
ngag
es in
ong
oing
pro
fess
iona
l dev
elop
men
t and
edu
catio
n to
impr
ove
pres
crib
ing
prac
tices
H1
.6.1
Impl
emen
ts st
rate
gies
to a
ddre
ss in
fluen
ces t
hat m
ay b
ias p
resc
ribin
g de
cisio
ns, i
nclu
ding
:
mar
ketin
g in
fluen
ces
po
ssib
le p
erso
nal,
prof
essio
nal o
r fin
ancia
l gai
n
conf
licts
of i
nter
est
th
e he
alth
pro
fess
iona
l’s o
wn
belie
fs, v
alue
s, an
d ex
perie
nces

Page
| 5
9 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Lega
l and
pro
fess
iona
l req
uire
men
ts
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d H1
.3.1
Dem
onst
rate
s kno
wle
dge
of a
nd c
ompl
ies w
ith n
atio
nal,
stat
e an
d te
rrito
ry, a
nd fa
cility
pol
icie
s and
pro
cedu
res i
n re
latio
n to
pre
scrib
ing
H1.3
.2 D
emon
stra
tes a
ppro
pria
te p
rofe
ssio
nal j
udge
men
t whe
n in
terp
r etin
g an
d ap
plyi
ng g
uide
lines
and
pro
toco
ls to
the
pers
on’s
situa
tion
H1.3
.3 C
ontr
ibut
es to
the
impr
ovem
ent o
f pol
icie
s and
pro
cedu
res f
or th
e ju
dici
ous,
appr
opria
te, s
afe
and
effe
ctiv
e us
e of
med
icine
s H2
.1.1
Adh
eres
to le
gisla
tive
and
wor
kpla
ce re
quire
men
ts fo
r obt
aini
ng a
nd re
cord
ing
cons
ent f
or:
ac
cess
ing
heal
th re
cord
s
obta
inin
g in
form
atio
n fr
om, a
nd p
rovi
ding
info
rmat
ion
to, o
ther
hea
lth p
rofe
ssio
nals
co
nduc
ting
a cli
nica
l exa
min
atio
n
prov
idin
g cli
nica
l ser
vice
s
the
pote
ntia
l ben
efits
and
har
ms o
f tre
atm
ent
th
e fin
ancia
l asp
ects
of t
he tr
eatm
ent
Page | 60 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Interaction and communication with patients
Prescribing competencies relating to communication style and therapeutic partnership with patients map well, as do the prescribing competencies relating to respect for the patient.
Prescribing competencies that map partly are involving the patient’s family or carers in the consultation, exploring and responding to patient concerns and providing clear written and verbal information to enable informed decision making.
Competencies that are not covered by the dietetic standards are considering the power differential between the health professional and the patient, and ascertaining that information has been understood correctly.
Interaction and communication with other health professionals
The prescribing competency relating to provision of information for collaboration with other health professionals maps completely with the dietetic standards.
Prescribing competencies that map partly are engaging in open discussion with, and providing clear written and verbal information to, other health professionals.
Competencies that are not covered are responding appropriately to communication and confirming understanding of information provided by other health professionals.
Assessment and diagnosis
Prescribing competencies relating to assessment and diagnosis that map completely are performing relevant clinical examinations within scope of practice, and synthesising assessment information to develop provisional and differential diagnoses.
The dietetic standards are quite broad in description, and the lack of detail means several competencies in this category only map partly. These include conducting an appropriate assessment, reviewing and interpreting information in the person’s health records and obtaining information from the patient. The dietetic standards do not detail the specifics of the information to be obtained from the patient such as medicines, allergies, alcohol and substance abuse; information that is vital when prescribing a medicine. Other competencies that map partly are assessing risk factors for non-adherence and explaining the clinical issues and implications to the patient.
Prescribing competencies not covered in this category are ascertaining sufficient information has been obtained, and developing a diagnostic strategy and performing relevant investigations.
Therapeutic choice and initiation
Prescribing competencies that map completely include recognising when non pharmacological treatment is appropriate, referral when treatment is outside scope of practice, negotiating therapeutic goals that enhance self-management and developing a treatment plan in partnership with the patient.
Some of the prescribing competencies in this category are only partly covered because they specifically relate to selection of medicine. These include; integrating knowledge to identify medicine options, obtaining and interpreting medicines information, considering medicines cost and affordability, discussion of medicine options and treatment preference with the patient, consulting

Page | 61 A review of the prescribing capability of speech pathologists, dietitians and psychologists
other health professionals about potential medicines and supplementing verbal with written information about potential medicines.
Not surprisingly, prescribing competencies specifically relating to medicine selection and ordering, such as medicine information and knowledge, application of Quality Use of Medicines (QUM) principles, obtaining approval for medicine use and providing appropriate medication orders, were not identified in the dietetic standards.
Other competencies not identified related to interaction with the patient regarding initiation of medicine. These include allowing the patient time to make a decision, reaching agreement with the patient regarding medicine choice, stopping or modifying existing medicines and ensuring patient understanding of therapeutic goals, management and how to use the medicine safely and effectively. In addition the prescribing competency relating to recognising when it is clinically appropriate not to intervene was not identified in the dietetic standards.
Review and adjustment of therapy
The national competency standard ‘Implements, evaluates and adapts nutrition care plans/programs/services’ covers much of this category, but lack of specificity limits close mapping to the Prescribing Competencies Framework.
Prescribing competencies fully covered are identifying the need for, and developing a review plan, and working in partnership with the patient and other health professionals to modify the treatment plan.
Prescribing competencies partly covered include observing the patient, discussing treatment response and using information gained to determine treatment success/need for adjustment. Other prescribing competencies partly covered are discussing the findings with the patient and organising the next review.
Competencies not identified in the dietetic standards are obtaining additional information to assess response, reporting issues arising from the review and identifying the need for a comprehensive medicines review.
Legal and professional requirements
Prescribing competencies relating to scope of practice, professional standards, codes of conduct and accountability map completely with the dietetic standards, as does demonstrating respect for the scope of practice of other health professionals.
Competencies that map partly include knowledge and compliance with legislation applicable to prescribing, maintenance of records and implementing strategies to address potential prescribing bias. The prescribing competency relating to ongoing professional development with respect to prescribing practices maps partly. Although the dietetic standards cover CPD requirements, prescribing is currently not within scope of practice, so is not covered by CPD statements. If prescribing becomes an activity within scope of practice, then this competency will map fully.
Prescribing competencies not identified in the dietetic standards include knowledge and compliance with policies and procedures in relation to prescribing, and adherence to requirements for consent. In addition competencies relating to interpretation and application of guidelines and protocols, and contribution to the improvement of policies and procedures relating to medicines use, did not map.

Page | 62 A review of the prescribing capability of speech pathologists, dietitians and psychologists
LLearning Outcomes Mapping
The learning outcomes were mapped at an element level to provide additional information regarding undergraduate education and training. The results of the mapping for the QUT Bachelor of Nutrition and Dietetics program of study are shown in table B2, appendix B.
The following Prescribing Competencies Framework elements were not identified in the learning objectives:
Element 3.2: Works in partnership with the person and other health professionals to select medicines and to tailor and implement a treatment plan
Element 3.3: Develops a review plan tailored to the person’s needs
Element 4.1: Provides clear instructions to other health professionals who dispense, supply, or administer medicines prescribed for the person
Element 4.2: Provides information about medicines and the treatment plan with the person’s consent to other health professionals who provide care to the person
Element 5.1: Obtains information to assess the person’s response to treatment
Element 5.2: Works in partnership with the person and other health professionals to address issues arising from the review
Element H1.1: Practices within the applicable legislative and regulatory frameworks
Element H1.4: Practices quality use of medicines principles
Element H1.6: Addresses the potential for bias in prescribing decisions
Element H2.1: Obtains consent to provide clinical services to the person
Element H2.2” Acknowledges the person, their family, and carers as integral to care and collaborates to achieve optimal health outcomes
Mapping dietetic prescribing capability against Prescribing Models
To provide additional information to identify the prescribing capabilities of dietitians, the performance criteria of the Prescribing Competencies Framework were mapped against the HPPP models of prescribing. The results from the dietetic mapping were then included to create a summary table (table 4). This table builds a clearer picture of the competency expectations dependent on the prescribing model, and indicates current gaps in dietetic prescribing competence.

Page
| 6
3 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Tabl
e 4:
Rel
atio
nshi
p be
twee
n th
e Pr
escr
ibin
g Co
mpe
tenc
ies F
ram
ewor
k, th
e HP
PP p
resc
ribin
g m
odel
s and
the
prof
essio
nal s
tand
ards
for d
ietit
ians
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
Com
pete
ncy
Area
1 U
nder
stan
ds th
e pe
rson
and
thei
r clin
ical n
eeds
Elem
ent 1
.1 E
stab
lishe
s a th
erap
eutic
par
tner
ship
with
the
pers
on a
nd a
colla
bora
tive
rela
tions
hip
with
oth
er h
ealth
pro
fess
iona
ls
1.1.
1 Us
es a
ppro
pria
te
com
mun
icat
ion
stra
tegi
es to
es
tabl
ish a
ther
apeu
tic p
artn
ersh
ip
with
the
pers
on
Elem
ent 1
.2 P
erfo
rms a
com
preh
ensiv
e m
edic
ines
ass
essm
ent t
o ob
tain
info
rmat
ion
to u
nder
stan
d th
e pe
rson
’s cl
inica
l nee
ds a
nd co
ntex
t
1.2.
1 Co
nduc
ts a
n as
sess
men
t tha
t is
appr
opria
te to
bot
h th
e he
alth
pr
ofes
siona
l’s sc
ope
of p
ract
ice a
nd
the
pers
on’s
clini
cal c
onte
xt
1.2.
2 Re
view
s and
inte
rpre
ts
info
rmat
ion
in th
e pe
rson
’s he
alth
re
cord
s
NNot
es
In
dica
tes a
per
form
ance
crit
erio
n cco
nsid
ered
ess
entia
l for
that
mod
el o
f pre
scrib
ing
In
dica
tes a
per
form
ance
crit
erio
n nno
t ccon
sider
ed e
ssen
tial f
or th
at m
odel
of p
resc
ribin
g
# Ac
cord
ing
to re
leva
nt le
gisla
tion.
Not
e ac
cord
ing
to th
e Pr
escr
ibin
g Co
mpe
tenc
ies
Fram
ewor
k, a
pre
scrip
tion
may
pro
vide
an
orde
r to
adm
inist
er, r
athe
r tha
n di
spe n
se.

Page
| 6
4 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
1.2.
3 O
btai
ns re
leva
nt in
form
atio
n fr
om th
e pe
rson
abo
ut th
eir
med
icin
es, a
nd th
eir m
edic
al a
nd
clin
ical
hist
ory,
inclu
ding
thei
r co-
exist
ing
cond
ition
s, tr
eatm
ents
, al
coho
l and
subs
tanc
e us
e, a
llerg
ies
and
soci
al co
ntex
t
1.2.
4 As
sess
es th
e pe
rson
’s ris
k fa
ctor
s for
poo
r adh
eren
ce; f
or
exam
ple
soci
al is
olat
ion,
phy
sical
im
pairm
ent,
cogn
itive
impa
irmen
t or
dist
urba
nce,
low
Eng
lish
prof
icien
cy,
low
hea
lth li
tera
cy, f
inan
cial
di
sadv
anta
ge.
1.2.
5 As
cert
ains
that
suffi
cient
in
form
atio
n ha
s bee
n ob
tain
ed a
bout
th
e pe
rson
’s co
-exi
stin
g co
nditi
ons
and
curr
ent t
reat
men
ts to
iden
tify
poss
ible
risk
s and
cont
rain
dica
tions
fo
r tre
atm
ent
1.2.
6 Pe
rform
s clin
ical
exa
min
atio
ns
that
are
with
in th
e he
alth
pr
ofes
siona
l’s o
wn
scop
e of
pra
ctice
an
d re
leva
nt to
the
pers
on’s
prob
lem
an
d in
terp
rets
the
findi
ngs o
f the
se
exam
inat
ions

Page
| 6
5 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
Elem
ent 1
.3 G
ener
ates
and
exp
lore
s pos
sible
dia
gnos
es
1.3.
1 Sy
nthe
sises
info
rmat
ion
from
th
e co
mpr
ehen
sive
asse
ssm
ent a
nd
deve
lops
pro
visio
nal a
nd d
iffer
entia
l di
agno
ses
1.3.
2 De
velo
ps a
dia
gnos
tic st
rate
gy
and
perf
orm
s rel
evan
t inv
estig
atio
ns
1.3.
3 Ex
plai
ns th
e cli
nica
l iss
ues a
nd
thei
r im
plica
tions
to th
e pe
rson
Com
pete
ncy
Area
2 T
reat
men
t opt
ions
: Un
ders
tand
s the
trea
tmen
t opt
ions
and
how
they
supp
ort t
he p
erso
n’s c
linic
al n
eed
Elem
ent 2
.1 C
onsid
ers n
on-p
harm
acol
ogica
l tre
atm
ent o
ptio
ns su
itabl
e fo
r tre
atin
g th
e pe
rson
and
thei
r con
ditio
n
2.1.
1 Re
cogn
ises w
hen
it is
clini
cally
ap
prop
riate
not
to in
terv
ene;
for
exam
ple,
in ca
ses w
here
the
signs
an
d sy
mpt
oms a
re li
kely
to re
solv
e w
ithou
t tre
atm
ent
2.1.
2 Re
cogn
ises w
hen
it is
clini
cally
ap
prop
riate
to im
plem
ent n
on-
phar
mac
olog
ical t
reat
men
ts

Page
| 6
6 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
Elem
ent 2
.2 Id
entif
ies a
ppro
pria
te m
edici
nes o
ptio
ns th
at ca
n be
inco
rpor
ated
into
the
pers
on’s
trea
tmen
t pla
n
2.2.
1 In
tegr
ates
kno
wle
dge
of
phar
mac
olog
y, o
ther
bio
med
ical
sc
ienc
es, c
linica
l med
icine
, and
th
erap
eutic
s and
iden
tifie
s med
icine
s su
itabl
e fo
r tre
atin
g th
e co
nditi
on
✗
2.2.
2 O
btai
ns, i
nter
pret
s, an
d ap
plie
s cu
rren
t evi
denc
e an
d in
form
atio
n ab
out m
edici
nes t
o in
form
dec
ision
s ab
out i
ncor
pora
ting
med
icine
s int
o th
e pe
rson
’s tr
eatm
ent p
lan
✗
2.2.
3 Id
entif
ies m
edic
ines
opt
ions
th
at a
re li
kely
to p
rovi
de
ther
apeu
tical
ly e
ffect
ive
and
safe
tr
eatm
ent a
nd ta
ilors
them
for t
he
pers
on
✗
2.2.
4 Co
nsid
ers t
he co
st a
nd
affo
rdab
ility
of t
he m
edici
nes t
o th
e pe
rson
✗
2.2.
5 Co
nsid
ers t
he im
plic
atio
ns to
th
e w
ider
com
mun
ity o
f usin
g a
part
icula
r med
icine
to tr
eat t
he
pers
on
✗

Page
| 6
7 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
2.2.
6 Di
scus
ses t
he tr
eatm
ent o
ptio
ns
and
med
icine
s with
the
pers
on,
cons
ider
ing:
the
prio
ritie
s for
tr
eatin
g th
eir c
urre
nt c
ondi
tion
and
co-e
xist
ing
cond
ition
s; th
eir r
eadi
ness
to
add
ress
the
curr
ent c
ondi
tion;
th
eir e
xpec
tatio
ns o
f tre
atm
ent
2.2.
7 Su
pple
men
ts v
erba
l inf
orm
atio
n w
ith w
ritte
n in
form
atio
n ab
out t
he
cond
ition
and
trea
tmen
t opt
ions
(w
here
app
ropr
iate
)
2.2.
8 Al
low
s the
per
son
time
to m
ake
an in
form
ed d
ecisi
on a
bout
thei
r tr
eatm
ent
2.2.
9 Re
fers
the
pers
on fo
r fur
ther
as
sess
men
t or t
reat
men
t whe
n th
e su
itabl
e tr
eatm
ent o
ptio
ns a
re
outs
ide
the
heal
th p
rofe
ssio
nal’s
ow
n sc
ope
of p
ract
ice

Page
| 6
8 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
Com
pete
ncy
Area
3 S
hare
d de
cisio
n m
akin
g: W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
to d
evel
op a
nd im
plem
ent a
trea
tmen
t pla
n
Elem
ent 3
.1 N
egot
iate
s the
rape
utic
goal
s with
the
pers
on
3.1.
1 Ne
gotia
tes t
hera
peut
ic go
als
that
enh
ance
the
pers
on’s
self-
man
agem
ent o
f the
ir co
nditi
on
✗
3.1.
2 As
cert
ains
that
all
part
ies h
ave
a co
mm
on u
nder
stan
ding
of t
he
ther
apeu
tic g
oals
and
how
they
will
be
man
aged
Elem
ent 3
.2 W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
sele
ct m
edic
ines
and
to ta
ilor a
nd im
plem
ent a
trea
tmen
t pla
n
3.2.
1 Ex
plor
es th
e pe
rson
’s op
inio
ns
and
pref
eren
ces c
once
rnin
g m
edic
ines
and
the
trea
tmen
t pla
n
✗
3.2.
2 Co
nsul
ts o
ther
hea
lth
prof
essio
nals
abou
t pot
entia
l m
edic
ines
and
the
trea
tmen
t pla
n
3.2.
3 Re
ache
s agr
eem
ent w
ith th
e pe
rson
abo
ut m
edici
nes t
o be
use
d to
tr
eat t
heir
cond
ition
✗
3.2.
4 De
velo
ps th
e tr
eatm
ent p
lan
in
part
ners
hip
with
the
pers
on
✗

Page
| 6
9 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
3.2.
5 O
btai
ns a
ppro
val t
o us
e th
e m
edic
ines
(whe
re re
leva
nt)
✗ ✗
3.2.
6 St
ops o
r mod
ifies
the
pers
on’s
exist
ing
med
icine
s and
oth
er
man
agem
ent s
trat
egie
s if r
equi
red
3.2.
7 En
sure
s the
per
son
unde
rsta
nds
the
trea
tmen
t pla
n an
d ho
w to
use
th
e m
edic
ine
safe
ly a
nd e
ffect
ivel
y
Elem
ent 3
.3 D
evel
ops a
revi
ew p
lan
tailo
red
to th
e pe
rson
’s ne
eds
3.3.
1 Id
entif
ies t
he n
eed
for,
and
deve
lops
a re
view
pla
n
Com
pete
ncy
Area
4 C
o-or
dina
tion:
Com
mun
icate
s the
trea
tmen
t pla
n cle
arly
to o
ther
hea
lth p
rofe
ssio
nals
Elem
ent 4
.1 P
rovi
des c
lear
inst
ruct
ions
to o
ther
hea
lth p
rofe
ssio
nals
who
disp
ense
, sup
ply,
or a
dmin
ister
med
icine
s pre
scrib
ed fo
r the
per
son
4.1.
1 Pr
epar
es p
resc
riptio
ns o
r m
edic
atio
n or
ders
that
com
ply
with
re
leva
nt le
gisla
tion,
gui
delin
es o
r co
des o
f pra
ctice
, and
org
anisa
tiona
l po
licie
s and
pro
cedu
res

Page
| 7
0 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
4.1.
2 Pr
ovid
es a
ccur
ate
and
clear
ve
rbal
med
icatio
n or
ders
that
com
ply
with
rele
vant
legi
slatio
n, g
uide
lines
or
code
s of p
ract
ice
and
orga
nisa
tiona
l pol
icies
and
pr
oced
ures
(whe
re re
leva
nt)
✗ #
#
Elem
ent 4
.2 P
rovi
des i
nfor
mat
ion
abou
t med
icin
es a
nd th
e tr
eatm
ent p
lan
with
the
pers
on’s
cons
ent t
o ot
her h
ealth
pro
fess
iona
ls w
ho p
rovi
de ca
re to
the
pers
on
4.2.
1 Pr
ovid
es in
form
atio
n fo
r co
llabo
ratio
n to
mem
bers
of i
nter
-pr
ofes
siona
l hea
lthca
re te
ams b
oth
with
in fa
ciliti
es a
nd th
e co
mm
unity
Com
pete
ncy
Area
5 M
onito
rs a
nd re
view
s: M
onito
rs a
nd re
view
s the
per
son’
s res
pons
e to
trea
tmen
t
Elem
ent 5
.1 O
btai
ns in
form
atio
n to
ass
ess t
he p
erso
n’s r
espo
nse
to tr
eatm
ent
5.1.
1 O
bser
ves t
he p
erso
n to
as
cert
ain
thei
r res
pons
e to
trea
tmen
t (w
here
rele
vant
)
5.1.
2 Di
scus
ses w
ith th
e pe
rson
and
ot
her h
ealth
pro
fess
iona
ls, th
eir:
ex
perie
nce
with
impl
emen
ting
the
trea
tmen
t pla
n
adhe
renc
e, in
cludi
ng a
ny is
sues
ar
ising
and
pos
sible
way
s to
impr
ove
adhe
renc
e

Page
| 7
1 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
pe
rcep
tion
or o
bser
vatio
n of
the
med
icin
es’ b
enef
its a
nd a
dver
se
effe
cts
as
sess
men
t of w
heth
er th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
5.1.
3 O
btai
ns a
dditi
onal
info
rmat
ion
to a
sses
s whe
ther
the
ther
apeu
tic
goal
s hav
e be
en a
chie
ved
by
exam
inin
g th
e pe
rson
, req
uest
ing
inve
stig
atio
ns, a
nd in
terp
retin
g th
e fin
ding
s (w
here
rele
vant
)
5.1.
4 Sy
nthe
sises
info
rmat
ion
prov
ided
by
the
pers
on, o
ther
hea
lth
prof
essio
nals,
and
from
clin
ical
exam
inat
ions
and
inve
stig
atio
ns to
de
term
ine
whe
ther
:
th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
trea
tmen
t sho
uld
be st
oppe
d,
mod
ified
or c
ontin
ued
th
e pe
rson
shou
ld b
e re
ferr
ed to
an
othe
r hea
lth p
rofe
ssio
nal

Page
| 7
2 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
Elem
ent 5
.2 W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
add
ress
issu
es a
risin
g fro
m th
e re
view
5.2.
1 Di
scus
ses t
he fi
ndin
gs o
f the
re
view
with
the
pers
on
5.2.
2 Id
entif
ies i
f the
per
son
requ
ires
a co
mpr
ehen
sive
med
icine
s rev
iew
5.2.
3 W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
mod
ify th
e tr
eatm
ent p
lan
to
optim
ise th
e sa
fety
and
effe
ctiv
enes
s of
trea
tmen
t (w
here
rele
vant
)
5.2.
4 Re
port
s iss
ues a
risin
g fr
om th
e re
view
5.2.
5 O
rgan
ises t
he n
ext r
evie
w
Com
pete
ncy
Area
H1
Prof
essio
nal:
Prac
tices
pro
fess
iona
lly
Elem
ent H
1.1
Prac
tices
with
in th
e ap
plic
able
legi
slativ
e an
d re
gula
tory
fram
ewor
ks
H1.1
.1 D
emon
stra
tes k
now
ledg
e of
, an
d co
mpl
ies w
ith, l
egisl
atio
n,
regu
latio
ns, a
nd co
mm
on la
w
appl
icabl
e to
pre
scrib
ing
(as f
urth
er

Page
| 7
3 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
defin
ed b
y th
e kn
owle
dge
subs
ectio
n of
this
com
pete
ncy
area
) H1
.1.2
Mai
ntai
ns a
ccur
ate
and
com
plet
e re
cord
s of:
th
e co
nsul
tatio
n
clin
ical
exa
min
atio
ns a
nd
inve
stig
atio
n re
sults
risk
fact
ors f
or m
edici
nes
misa
dven
ture
the
pers
on’s
decis
ion
to d
eclin
e tr
eatm
ent (
whe
re re
leva
nt)
ch
ange
s to
the
pers
on’s
med
icine
s m
anag
emen
t pla
n, in
cludi
ng th
e ra
tiona
le b
ehin
d th
ese
chan
ges
th
e re
view
pla
n,
reco
mm
enda
tions
, and
dat
e fo
r ne
xt re
view
outc
omes
of t
reat
men
t
Elem
ent H
1.2
Prac
tices
acc
ordi
ng to
pro
fess
iona
l sta
ndar
ds, c
odes
of c
ondu
ct, a
nd w
ithin
the
heal
th p
rofe
ssio
nal’s
ow
n sc
ope
of p
ract
ice
H1.2
.1 D
emon
stra
tes k
now
ledg
e of
an
d co
mpl
ianc
e w
ith:
pr
ofes
siona
l sta
ndar
ds
co
des o
f con
duct
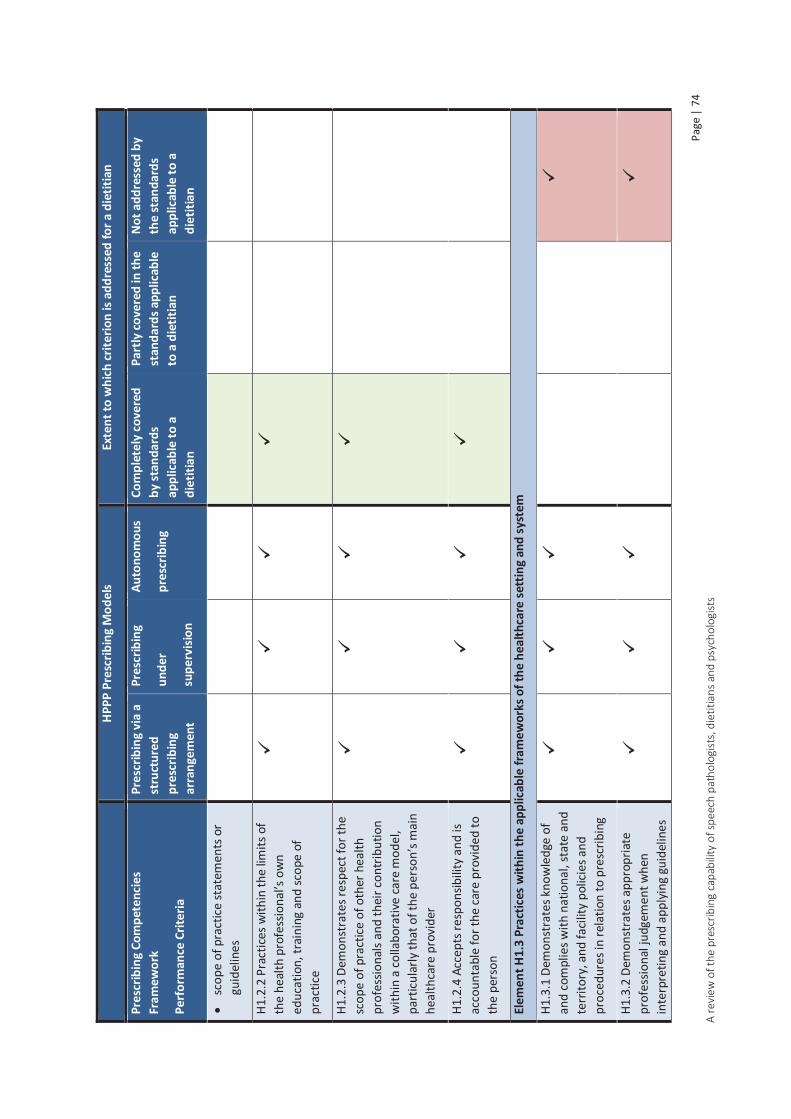
Page
| 7
4 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
sc
ope
of p
ract
ice st
atem
ents
or
guid
elin
es
H1.2
.2 P
ract
ices w
ithin
the
limits
of
the
heal
th p
rofe
ssio
nal’s
ow
n ed
ucat
ion,
trai
ning
and
scop
e of
pr
actic
e
H1.2
.3 D
emon
stra
tes r
espe
ct fo
r the
sc
ope
of p
ract
ice o
f oth
er h
ealth
pr
ofes
siona
ls an
d th
eir c
ontr
ibut
ion
with
in a
col
labo
rativ
e ca
re m
odel
, pa
rticu
larly
that
of t
he p
erso
n’s m
ain
heal
thca
re p
rovi
der
H1.2
.4 A
ccep
ts re
spon
sibili
ty a
nd is
ac
coun
tabl
e fo
r the
car
e pr
ovid
ed to
th
e pe
rson
Elem
ent H
1.3
Prac
tices
with
in th
e ap
plic
able
fram
ewor
ks o
f the
hea
lthca
re se
ttin
g an
d sy
stem
H1.3
.1 D
emon
stra
tes k
now
ledg
e of
an
d co
mpl
ies w
ith n
atio
nal,
stat
e an
d te
rrito
ry, a
nd fa
cility
pol
icies
and
pr
oced
ures
in re
latio
n to
pre
scrib
ing
H1.3
.2 D
emon
stra
tes a
ppro
pria
te
prof
essio
nal j
udge
men
t whe
n in
terp
retin
g an
d ap
plyi
ng g
uide
lines

Page
| 7
5 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
and
prot
ocol
s to
the
pers
on’s
situa
tion
H1.3
.3 C
ontr
ibut
es to
the
impr
ovem
ent o
f pol
icies
and
pr
oced
ures
for t
he ju
dici
ous,
appr
opria
te, s
afe
and
effe
ctiv
e us
e of
m
edic
ines
✗
Elem
ent H
1.4
Prac
tices
qua
lity
use
of m
edici
nes p
rinci
ples
H1.4
.1 A
pplie
s qua
lity
use
of
med
icin
es p
rinci
ples
whe
n pr
escr
ibin
g m
edici
nes
H1.4
.2 Id
entif
ies c
omm
on c
ause
s of
med
icin
es e
rror
s and
adv
erse
eve
nts,
and
impl
emen
ts st
rate
gies
to re
duce
th
e ris
ks o
f the
se o
ccur
ring
H1.4
.3 D
emon
stra
tes k
now
ledg
e of
th
e m
edic
ines
com
mon
ly p
resc
ribed
H1.4
.4 C
ritica
lly e
valu
ates
in
form
atio
n ab
out m
edici
nes a
nd
mak
es e
vide
nce-
base
d de
cisio
ns
✗

Page
| 7
6 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
abou
t med
icine
s in
the
heal
th
prof
essio
nal’s
ow
n pr
actic
e
Elem
ent H
1.5
Dem
onst
rate
s a co
mm
itmen
t to
cont
inua
l qua
lity
impr
ovem
ent o
f the
hea
lth p
rofe
ssio
nal’s
ow
n pr
escr
ibin
g
H1.5
.1 E
ngag
es in
ong
oing
pr
ofes
siona
l dev
elop
men
t and
ed
ucat
ion
to im
prov
e pr
escr
ibin
g pr
actic
es
Elem
ent H
1.6
Addr
esse
s the
pot
entia
l for
bia
s in
pres
crib
ing
deci
sions
H1.6
.1 Im
plem
ents
stra
tegi
es to
ad
dres
s inf
luen
ces t
hat m
ay b
ias
pres
crib
ing
decis
ions
, inc
ludi
ng:
m
arke
ting
influ
ence
s
poss
ible
per
sona
l, pr
ofes
siona
l or
finan
cial g
ain
co
nflic
ts o
f int
eres
t
the
heal
th p
rofe
ssio
nal’s
ow
n be
liefs
, val
ues,
and
expe
rienc
es
✗
Com
pete
ncy
Area
H2
Com
mun
icate
s: Co
mm
unic
ates
and
col
labo
rate
s effe
ctiv
ely
with
the
pers
on a
nd o
ther
hea
lth p
rofe
ssio
nals
Elem
ent H
2.1
Obta
ins c
onse
nt to
pro
vide
clin
ical s
ervi
ces t
o th
e pe
rson
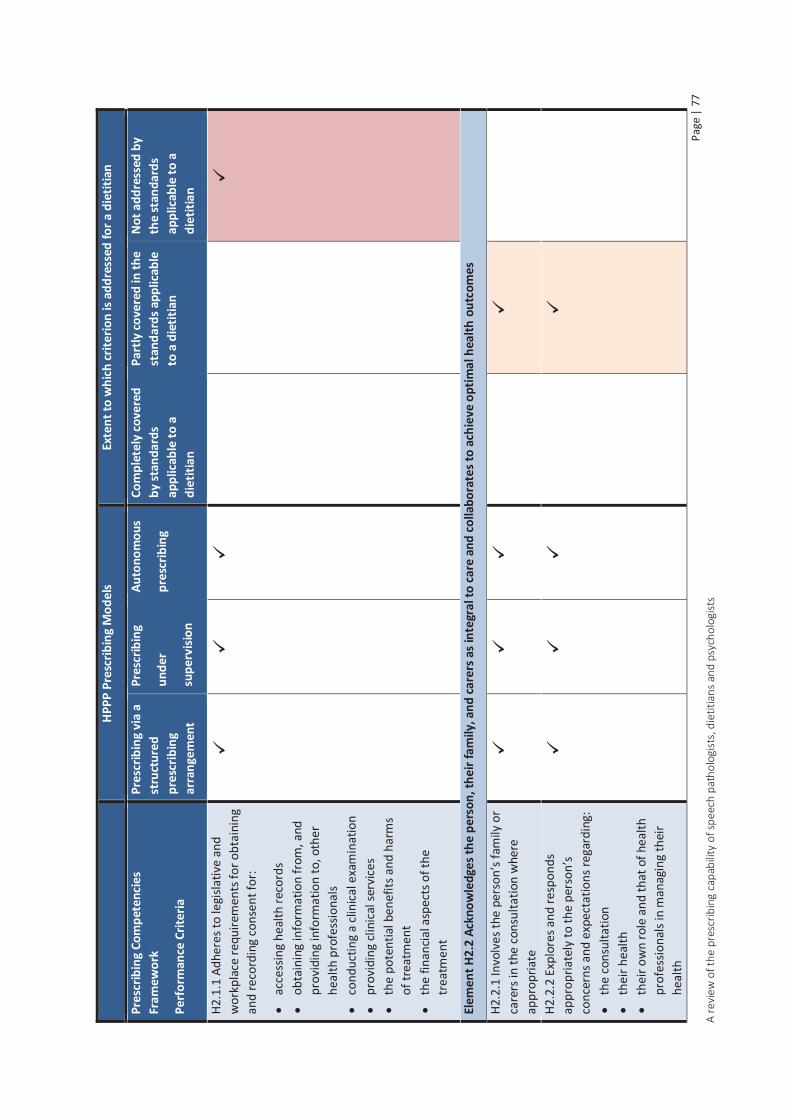
Page
| 7
7 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
H2.1
.1 A
dher
es to
legi
slativ
e an
d w
orkp
lace
requ
irem
ents
for o
btai
ning
an
d re
cord
ing
cons
ent f
or:
ac
cess
ing
heal
th re
cord
s
obta
inin
g in
form
atio
n fr
om, a
nd
prov
idin
g in
form
atio
n to
, oth
er
heal
th p
rofe
ssio
nals
co
nduc
ting
a cli
nica
l exa
min
atio
n
prov
idin
g cli
nica
l ser
vice
s
the
pote
ntia
l ben
efits
and
har
ms
of tr
eatm
ent
th
e fin
ancia
l asp
ects
of t
he
trea
tmen
t
Elem
ent H
2.2
Ackn
owle
dges
the
pers
on, t
heir
fam
ily, a
nd ca
rers
as i
nteg
ral t
o ca
re a
nd co
llabo
rate
s to
achi
eve
optim
al h
ealth
out
com
es
H2.2
.1 In
volv
es th
e pe
rson
’s fa
mily
or
care
rs in
the
cons
ulta
tion
whe
re
appr
opria
te
H2.2
.2 E
xplo
res a
nd re
spon
ds
appr
opria
tely
to th
e pe
rson
’s co
ncer
ns a
nd e
xpec
tatio
ns re
gard
ing:
the
cons
ulta
tion
th
eir h
ealth
thei
r ow
n ro
le a
nd th
at o
f hea
lth
prof
essio
nals
in m
anag
ing
thei
r he
alth

Page
| 7
8 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
th
e he
alth
pro
fess
iona
l’s sc
ope
of
prac
tice
th
e us
e of
med
icine
s and
oth
er
trea
tmen
ts to
mai
ntai
n th
eir
heal
th
H2.2
.3 E
stab
lishe
s a th
erap
eutic
pa
rtne
rshi
p th
at a
ccor
ds w
ith th
e pr
efer
ence
s exp
ress
ed b
y th
e pe
rson
Elem
ent H
2.3
Resp
ects
the
pers
on
H2.3
.1 R
espe
cts t
he p
erso
n’s v
alue
s, be
liefs
, and
exp
erie
nces
H2.3
.2 R
espe
cts t
he p
erso
n’s p
rivac
y an
d co
nfid
entia
lity
H2.3
.3 R
espe
cts t
he p
erso
n’s
heal
thca
re d
ecisi
ons
Elem
ent H
2.4
Com
mun
icate
s effe
ctiv
ely
with
the
pers
on u
sing
appr
opria
te co
mm
unic
atio
n sk
ills t
o en
able
the
safe
use
of m
edici
nes
H2.4
.1 A
sses
ses t
he p
erso
n’s
pref
erre
d la
ngua
ge, c
omm
unic
atio
n st
yle,
com
mun
icatio
n ca
pabi
litie
s, an
d he
alth
lite
racy
, and
adj
usts
the
heal
th p
rofe
ssio
nal’s
ow
n

Page
| 7
9 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
com
mun
icat
ion
styl
e to
inte
ract
ef
fect
ivel
y w
ith th
em
H2.4
.2 C
onsid
ers t
he p
oten
tial i
ssue
of
per
ceiv
ed p
ower
diff
eren
ces
betw
een
the
heal
th p
rofe
ssio
nal a
nd
the
pers
on
H2.4
.3 P
rovi
des c
lear
and
app
ropr
iate
w
ritte
n an
d ve
rbal
info
rmat
ion
to th
e pe
rson
to e
nabl
e th
em to
mak
e in
form
ed ch
oice
s and
ach
ieve
opt
imal
he
alth
out
com
es
H2.4
.4 A
scer
tain
s tha
t the
in
form
atio
n pr
ovid
ed h
as b
een
rece
ived
and
und
erst
ood
corr
ectly
Elem
ent H
2.5
Colla
bora
tes w
ith o
ther
hea
lth p
rofe
ssio
nals
to a
chie
ve o
ptim
al h
ealth
out
com
es fo
r the
per
son
H2.5
.1 E
ngag
es in
ope
n, in
tera
ctiv
e di
scus
sions
with
oth
er h
ealth
pr
ofes
siona
ls in
volv
ed in
carin
g fo
r th
e pe
rson
H2.5
.2 C
onfir
ms t
hat t
heir
own
unde
rsta
ndin
g of
info
rmat
ion
prov
ided
by
othe
r hea
lth
prof
essio
nals
is co
rrec
t

Page
| 8
0 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for a
die
titia
n
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r
supe
rvisi
on
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
diet
itian
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
die
titia
n
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
diet
itian
H2.5
.3 R
espo
nds a
ppro
pria
tely
to
com
mun
icat
ion
initi
ated
by
othe
r he
alth
pro
fess
iona
ls
H2.5
.4 P
rovi
des c
lear
ver
bal a
nd
writ
ten
info
rmat
ion
to o
ther
hea
lth
prof
essio
nals
by se
cure
mea
ns w
hen
impl
emen
ting
new
trea
tmen
ts w
ith
med
icin
es o
r mod
ifyin
g ex
istin
g tr
eatm
ent p
lans

Page | 81 A review of the prescribing capability of speech pathologists, dietitians and psychologists
7.3.3 Discussion
The National Competency Standards for Dietitians in Australia and the Statement of Ethical Practice are not as comprehensive as other allied health standards, particularly in relation to assessment, diagnosis and monitoring of therapy. It is likely that many of the prescribing activities that do not map well are undertaken in actual practice, but due to their lack of documentation in the professional standards, are perceived not to map to the Prescribing Competencies Framework. These include the following:
Reviews and interprets information in the person’s health records Performs relevant clinical examinations within scope of practice Develops a diagnostic strategy and performs relevant investigations Explains the clinical issues and implications to the person Allows the person time to make an informed decision about their treatment Ascertains that all parties have a common understanding of the therapeutic goals and how they
will be managed Ascertains that the information provided has been received and understood correctly Organises the next review Considers the potential issue of perceived power differences between the health professional
and the person Confirms that their own understanding of information provided by other health professionals is
correct Responds appropriately to communication initiated by other health professionals
Areas that do not map well, and are likely to fall outside of the current scope of practice should be targeted for additional education and assessment, these include the following:
Medication and allergy history taking Adherence assessment Medication selection competencies
o Identification of safe, appropriate, effective medicine options o Stopping or modifying existing medicines if required o Medication knowledge o QUM principles
Medication orders Ensuring the person understands the treatment plan and how to use the medicine safely and
effectively Legislative requirements relating to medicines
Mapping of the learning objectives for the representative undergraduate program of study provided limited information to assess graduate capability with respect to prescribing. The learning objectives are quite broad in their statements and, without review of individual lectures and tutorials, it if impossible to say to what extent they map with the Prescribing Competencies Framework. Mapping at an element level rather than a performance criteria level is also less specific; not all performance criteria within the element may be covered by the learning objectives. This mapping does, however, give an indication of the coverage of Prescribing Competencies Framework by a DAA accredited program of study. It also appears that areas not well covered in the professionals standards, for
Page | 82 A review of the prescribing capability of speech pathologists, dietitians and psychologists
example medication orders, assessing response to treatment, quality use of medicines and medicine legislation are also not covered in the learning objectives.
Some of the elements which could not be identified in the learning objectives such as obtaining consent and obtaining information to assess the person’s response to treatment are likely to be covered in clinical placements. Other such as providing instruction to other health professionals who dispense, supply, or administer medicines prescribed for the person or practicing quality use of medicines principles are clearly outside of current scope and would require an addition to the curriculum.
As indicated in table 4, the requisite competencies for safe and effective prescribing differ dependent on the model of prescribing to be used. The number of competencies required to prescribe under supervision or autonomously is greater than those required to prescribe via a structured prescribing arrangement. This information can be used to identify the additional training that would be required to achieve dietetic prescribing competence dependent on the model of prescribing. Table B3, appendix B shows the competencies not met or only partly met by the dietetic standards and indicates the additional training required dependent on the prescribing model. The additional training required for prescribing under a structured prescribing arrangement is as follows:
Medication history taking training, including adherence assessment and ascertaining that sufficient information has been obtained
Interpretation and application of guidelines and protocols appropriate to model of prescribing
QUM principles appropriate to model of prescribing Knowledge of the medicines to be prescribed (including potential adverse reactions and
errors) Identification of potential problems with existing medicines and cessation or adjustment as
appropriate Obtaining and recording consent for medicine use Legislation, policies and procedures applicable to model of prescribing Writing of medicine orders appropriate to model of prescribing Recording keeping with respect to medicine use Review of medicine therapy and reporting of issues arising from the review Identification of person’s need for comprehensive medicines review Communication with the person regarding medicine choice, safe and effective use of the
medicine and experience with medicine use Provision of verbal and written medicines information to facilitate informed choice Consulting other health professionals with respect to medicine choice Provision of written and verbal medicines information to other health professionals
To prescribe under supervision or autonomously the following additional training to that described above is required:
Knowledge of pharmacology, clinical medicine and therapeutics Access, interpretation, evaluation and application of medicine information to inform
evidence based decision making Identification of appropriate medicine options for both the condition and the person being
treated

Page | 83 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Tailoring of medicine to the person’s needs Consideration of cost of medicines to be prescribed Implication to the wider community with respect to prescribing Communication with the person with respect to opinions and preferences regarding
medicines and the treatment plan Communication with respect to medicines options and reaching agreement with the person Ethical issues with respect to prescribing Provision of verbal orders if required appropriate for model of prescribing Obtaining approval for medicine use if required
There are a number of routes by which competency to prescribe could be achieved. The competencies to prescribe via a structured prescribing arrangement could be incorporated into pre-entry programs of study with minimal adjustment. Authority to prescribe under supervision or autonomously requires additional training, which could be provided in the way of postgraduate training with appropriate assessment and credentialing to ensure competency. The majority of the competencies are not profession specific, so there is the possibility of the development of a generic allied health prescribing course. This could be provided in combination with workplace supervision and mentoring, to train and subsequently assess dietetic prescribers. Over time it may be possible to incorporate all aspects of prescribing into pre-entry programs of study.
In order to progress the introduction of dietitian prescribing of medicines within scope of practice, processes around the accreditation of prescribing training programs and recognition of prescriber status need to be developed.
In December 2013, following the development of the Prescribing Competencies Framework and the HPPP, the Health Profession Accreditation Councils’ Forum released a position statement ‘Development of Prescribing Standards and Accreditation Processes’(30). The position statement acknowledged the Prescribing Competencies Framework as the nationally recognised standard for prescribing, and stated that standards for prescribing education and training programs of study must align to the framework. The document also stated ‘The Forum is working with its Members to ensure efficient and effective accreditation processes are developed at the same time respecting the diversity of approaches of individual accreditation councils to these processes’.
In addition AHPRA has established a Prescribing Working Group whose aim is to ‘develop a governance framework and other resources to support the development and review of national board regulatory policy relating to prescribing of scheduled medicines’(6). This working group provides a useful mechanism to facilitate active collaboration between health professions and the Forum, with a view to consistency of accreditation. Whilst DAA is neither a member body of the Forum or AHPRA, it is possible that they could adopt any accreditation framework that is developed and use it to accredit prescribing training programs suitable for dietetic prescribing. Alternatively DAA could independently develop their own accreditation standards. As an ongoing goal the Prescribing Competencies Framework should be embedded in any prescribing accreditation standards developed. This approach is evidenced in the 2015 Nurse Practitioner and Endorsement for Scheduled Medicines for Midwives Accreditation Standards, both of which require a map of subjects against the Prescribing Competencies Framework(31, 32).

Page | 84 A review of the prescribing capability of speech pathologists, dietitians and psychologists
7.4 Recommendations
If dietetic prescribing is to occur, consideration needs to be given to the process by which dietitians are recognised as competent to prescribe.
As discussed previously, in Queensland the authority to prescribe is legislated under the Health (Drugs and Poisons) Regulation 1996 (HDPR), therefore, amendments to the regulation would be required to authorise dietitians to prescribe. As a temporary measure, prescribing could occur within Queensland under the section 18 approval process, which has been used previously to authorise prescribing trials in pharmacy and physiotherapy.
If dietetic prescribing is to occur at a national level, professional standards should be revised to include prescribing competencies. Amendments to the relevant medicines regulation in each state and territory would also be required.
In order to progress dietetic prescribing it is recommended that DAA:
Develop or adopt an accreditation framework and use it to accredit prescribing training programs suitable for dietetic prescribing
Establish a process to credential dietitians to prescribe, dependent on completion of an accredited prescribing program of study. In order to maintain continuing professional development standards and currency of practice, only Accredited Practising Dietitians should be credentialed to prescribe

Page | 85 A review of the prescribing capability of speech pathologists, dietitians and psychologists
8 Psychology 8.1 Background information
As of March 2015 there were 26,528 practising psychologists with general registration in Australia(43). The latest skill shortage occupational report for psychologists in Australia lists the February 2014 labour market rating as ‘no shortage’. The same document also shows a strong increase in the number of students commencing and completing higher education psychology qualifications(44).
8.1.1 National Bodies/Registration
General Registration
In Australia the psychology profession is regulated by the National Law(26). All psychologists are required to be registered with the Psychology Board of Australia (PsyBA), supported by the Australian Health Practitioner Regulation Agency (AHPRA).
The education and training requirement for general registration is a six year sequence. This comprises of a four year accredited sequence of study such as an honours degree, followed by an accredited postgraduate degree such as a Masters, or a period of supervised practice as a provisional psychologist. The PsyBA approved qualifications that lead to general registration are, therefore, as follows:
a) An accredited Master’s degree; or b) A five year accredited sequence of study followed by a one year Board approved internship
(5+1); or c) A four year accredited sequence of study followed by a two year Board approved internship
(4+2); or d) A qualification that in the Board’s opinion is substantially equivalent to either (a), (b) or (c).
In addition to the completion of an approved qualification, an applicant also has to sit the national psychology examination, (unless specific exemptions apply), before applying for general registration.
The Australian Psychology Society
The Australian Psychological society (APS) is the largest professional body for psychologists in Australia, with over 21,000 members(45). It has a number of functions including advocacy, representation of its members to the public and other professions, provision of information and professional development activities(46).
There are various levels of memberships available:
Associate Membership-open to all psychologists who have completed an accredited 4-year sequence of study
Membership-open to psychologists who have completed an accredited 6-year sequence of study in psychology (4 years undergraduate plus 2 years or more postgraduate)
Fellowship-existing APS members must be nominated by an APS Fellow and have a minimum of 10 years’ experience in psychological work or study subsequent to being elected to the grade of Member. The candidate must also have made a substantial contribution to the activities of the Society for a minimum of 5 years and have and advanced knowledge of

Page | 86 A review of the prescribing capability of speech pathologists, dietitians and psychologists
psychology and have made significant contribution to advancement of knowledge, professional practice and education of others
In addition there are student and affiliate membership categories
The APS were asked to participate in the HPPP project, and submitted a response to Health Workforce Australia’s consultation paper in May 2012(47).
8.1.2 Education and Training
The Australian Psychology Accreditation Council (APAC) is the accreditation authority responsible for accrediting education providers and programs of study for the psychology professions.
As discussed above, the education requirement for general registration as a psychologist is a 6 year sequence of study that can be achieved by a number of different routes. The education and training options are illustrated in Figure 1 (note: not all available psychology course titles in Australia are included):

Page | 87 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Figure 1 Education and Training options for general registration as a Psychologist in Australia

Page | 88 A review of the prescribing capability of speech pathologists, dietitians and psychologists
88.1.3 Areas of endorsement of registration
The PsyBA allows for subsequent endorsement of registration in the following areas of practice(48):
Clinical neuropsychology Clinical psychology Community psychology Counselling psychology Educational and developmental psychology Forensic psychology Health psychology Organisational psychology Sport and exercise psychology
Endorsement of registration facilitates recognition of practitioners who have an additional qualification and advanced supervised practice in a specific field of psychology.
There are two pathways for obtaining endorsement:
The standard pathway
a) Completion of an APAC accredited Masters in one of the approved areas of practice, and a registrar program consisting of a minimum of two years of approved, supervised full-time equivalent practice with a PsyBA approved supervisor or
b) Completion of an APAC accredited Doctorate in one of the approved areas of practice, and a registrar program consisting of a minimum one year of approved, supervised, full-time equivalent practice with a PsyBA approved supervisor or
c) Another qualification that, in the Board’s opinion, is substantially equivalent to (a) or (b).
The non-standard pathway
For applicants who have not completed a PsyBA registrar program including overseas trained applicants and applicants applying under transition provisions.
8.1.4 Current Prescribing Status
Psychologists currently have no prescribing authority in Australia. At an international level a number of countries have attempted to promote prescribing rights for psychologists, but have often met with resistance from psychiatrists. Only a small number of states in the United States have gained prescriptive authority(47, 49).
8.1.5 Prescribing Potential
Psychologist prescribing in Australia would improve access to psychoactive scheduled medicines in areas where doctor shortages are common, for example rural and remote areas. Improved access would also benefit the patient who is assessed as requiring a scheduled medicine as an adjunct to psychology treatment. For example a psychologist may prescribe an antidepressant to a patient they are treating with cognitive behavioural therapy. Prescribing by the psychologist would ensure the patient receives the medicine in a timely fashion, without multiple visits to health care practitioners, and facilitates regular medication monitoring, titration and review.

Page | 89 A review of the prescribing capability of speech pathologists, dietitians and psychologists
88.2 Prescribing Competence in Psychology
In order to consider the prescribing potential of the psychologist, and to identify options in Queensland relating to prescribing authority, it is necessary to review the current status of psychology qualifications and evaluate their capacity to provide the skills, knowledge and behaviours necessary to become a competent prescriber. As discussed previously, such competence is described in the Prescribing Competencies Framework. If the current training requirements and professional standards for psychologists are mapped against the framework, it will be possible to evaluate the current prescribing capability of psychologists, and identify any gaps in capability that may need to be addressed. For the purpose of this report the Master’s degree route to general registration and the four year accredited sequence of study followed by a two year Board approved internship (4 + 2) are the only two training and education options to be reviewed.
8.2.1 Psychology training requirements and professional standards which define professional capability
A discussed previously, APAC accredit programs of study leading to psychology qualifications. The APAC accreditation standard for the psychology profession is currently under review. Submissions to the Second Consultation Draft have closed, but the draft document provides a useful insight into changes in the accreditation requirements for psychology programs of study(49). The draft APAC standard details program of study requirements as follows:
Master’s degree (Australian Qualification Framework Level 9)
The Program of Study includes coverage of all content required to support achievement of each of the Core Competencies for the Entry Level Practitioner set out in Appendix C of the standard
The Program of Study incorporates all of the guiding principles and standards of the current version of the National Practice Standards for the Mental Health Workforce(50)
The Program of Study includes advanced training in ethics and ethical psychological practice, including the code of ethics currently adopted by the PsyBA, and the current version of the Australian Code for the Responsible Conduct of Research
Fourth year program of study (Australian Qualification Framework Level 8)
The Program of Study includes advanced training in research methods, including coverage of each of the content areas listed in A2.1, A2.2 and A2.3 of Appendix A (Graduate Attributes for the Australian Undergraduate Psychology Program)
The Program of Study incorporates coverage of the guiding principles of the current version of the National Practice Standards for the Mental Health Workforce
The Program of Study includes advanced training in ethics and ethical psychological practice including the code of ethics currently adopted by the PsyBA and the current version of the Australian Code for the Responsible Conduct of Research
In addition to the APAC requirements for the fourth year of the undergraduate degree, it is also important to consider the training requirements of the two year Board approved internship, which is a pre-requisite to registration via this training route. The PsyBA has produced ‘Guidelines for 4 + 2 internship programs for provisional psychologists and supervisors’(51),which detail the core capabilities for the internship program. Within this document the term capability refers to ‘the range of knowledge, skills and expertise expected of and demonstrated by a six-year trained psychologist’.

Page | 90 A review of the prescribing capability of speech pathologists, dietitians and psychologists
National Psychology Examination
Once the approved psychology education and training requirements have been satisfied, candidates are required to pass the National Psychology Examination in order to gain general registration. The examination curriculum(52)is designed to test the eight entry level core competencies that are described in the PsyBA internship program guidelines.
Summary of professional and training standards which define entry level capability with respect to prescribing competence
Review of the Australian Code for the Responsible Conduct of Research showed the document provides no information relevant to the psychologist’s competence to prescribe. It was, therefore, decided not to include it in any prescribing competency mapping.
Taking the preceding information into consideration, table 5 details the key documents that can be used to map psychologist entry level competence against the Prescribing Competencies Framework.
Table 5: Psychology Standards/guidelines that can be used to map psychologist entry level competence against the Prescribing Competencies Framework
Psychology General Registration Entry Route
Standards/Guidelines Master’s 4 + 2
National Practice Standards for the Mental Health Workforce
APS Code of Ethics
APAC Core Competencies of the entry level practitioner (appendix C of the draft APAC standard)
PsyBA Guidelines for 4 + 2 internship programs for provisional psychologists and supervisors
National psychology examination curriculum
88.3 Psychology Competency Mapping
8.3.1 Methodology
The mapping for psychology was divided into two separate processes. Professional Standards mapping was achieved by mapping the National Practice Standards for the Mental Health Workforce and the APS Code of Ethics against individual performance criteria for every element within the Prescribing Competencies Framework. These professional standards are relevant to both the Master’s and the 4 + 2 route to general registration. The results are shown in table C1, appendix C. The comments section of the table denotes whether statements identified in either one or both of the professional standards can be considered to map completely, partly or not at all with the Prescribing Competencies Framework. The comments section is colour coded as follows:

Page | 91 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Green denotes that a particular prescribing competency performance criterion maps well, and is covered sufficiently by either one or both of the standards
Orange denotes that the particular prescribing competency performance criterion is covered partly by either one or both of the standards
Red denotes that the particular prescribing competency performance criterion cannot be identified in either of the standards
In addition entry level practitioner competency was assessed by mapping the APAC Core Competencies of the entry level practitioner (appendix C of the draft APAC standard), the PsyBA Guidelines for 4 + 2 internship programs for provisional psychologists and supervisors and the National psychology examination curriculum. The results of this mapping are shown in table C2, appendix C.
To provide additional education and training information relevant to the review, the learning objectives from APAC accredited psychology programs of study, leading to general registration, were also mapped against the Prescribing Competencies Framework elements. Learning objectives from the following representative programs of study were mapped:
Bachelor of Behavioural Science (Psychology), Queensland University of Technology (QUT) Bachelor of Behavioural Science (Honours Psychology), QUT Graduate Diploma in behavioural Science, QUT Master of Clinical Psychology, QUT
88.3.2 Results
Professional Standards and Entry Level Competency Mapping
Table 6 provides a combined summary of the professional standards and entry level competency mapping results. The table shows competencies from the Prescribing Competencies Framework separated into different categories, and indicates which of the prescribing competencies within each category are covered completely, partly, or not at all by the psychology standards. It should be noted that the capability assumptions made in the mapping process are based purely on information obtained from the psychology standards, and not on review of actual practice.

Page
| 9
2 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Tabl
e 6:
Psy
chol
ogy
map
ping
sum
mar
y: e
xten
t to
whi
ch th
e Pr
escr
ibin
g Co
mpe
tenc
ies F
ram
ewor
k is
cove
red
by th
e ps
ycho
logy
stan
dard
s
Mas
ter’s
4
+ 2
Inte
ract
ion
and
com
mun
icatio
n w
ith p
atie
nts
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
1.1.
1
Uses
app
ropr
iate
com
mun
icat
ion
stra
tegi
es to
est
ablis
h a
ther
apeu
tic
part
ners
hip
with
the
pers
on
H2.2
.1 In
volv
es th
e pe
rson
’s fa
mily
or c
arer
s in
the
cons
ulta
tion
whe
re a
ppro
pria
te
H2.2
.3 E
stab
lishe
s a th
erap
eutic
par
tner
ship
that
acc
ords
with
the
pref
eren
ces
expr
esse
d by
the
pers
on
H2.3
.1 R
espe
cts t
he p
erso
n’s v
alue
s, be
liefs
, and
exp
erie
nces
H2
.3.2
Res
pect
s the
per
son’
s priv
acy
and
conf
iden
tialit
y H2
.3.3
Res
pect
s the
per
son’
s hea
lthca
re d
ecisi
ons
H2.4
.1 A
sses
ses t
he p
erso
n’s p
refe
rred
lang
uage
, com
mun
icatio
n st
yle,
co
mm
unic
atio
n ca
pabi
litie
s, an
d he
alth
lite
racy
, and
adj
usts
the
heal
th
prof
essio
nal’s
ow
n co
mm
unica
tion
styl
e to
inte
ract
effe
ctiv
ely
with
them
H2
.4.2
Con
sider
s the
pot
entia
l iss
ue o
f per
ceiv
ed p
ower
diff
eren
ces b
etw
een
the
heal
th p
rofe
ssio
nal a
nd th
e pe
rson
H2
.4.3
Pro
vide
s cle
ar a
nd a
ppro
pria
te w
ritte
n an
d ve
rbal
info
rmat
ion
to th
e pe
rson
to e
nabl
e th
em to
mak
e in
form
ed c
hoice
s and
ach
ieve
opt
imal
he
alth
out
com
es
1.1.
1
Uses
app
ropr
iate
com
mun
icat
ion
stra
tegi
es to
est
ablis
h a
ther
apeu
tic
part
ners
hip
with
the
pers
on
H2.2
.1 In
volv
es th
e pe
rson
’s fa
mily
or c
arer
s in
the
cons
ulta
tion
whe
re a
ppro
pria
te
H2.2
.3 E
stab
lishe
s a th
erap
eutic
par
tner
ship
that
acc
ords
with
the
pref
eren
ces
expr
esse
d by
the
pers
on
H2.3
.1 R
espe
cts t
he p
erso
n’s v
alue
s, be
liefs
, and
exp
erie
nces
H2
.3.2
Res
pect
s the
per
son’
s priv
acy
and
conf
iden
tialit
y H2
.3.3
Res
pect
s the
per
son’
s hea
lthca
re d
ecisi
ons
H2.4
.1 A
sses
ses t
he p
erso
n’s p
refe
rred
lang
uage
, com
mun
icatio
n st
yle,
co
mm
unic
atio
n ca
pabi
litie
s, an
d he
alth
lite
racy
, and
adj
usts
the
heal
th
prof
essio
nal’s
ow
n co
mm
unica
tion
styl
e to
inte
ract
effe
ctiv
ely
with
them
H2
.4.2
Con
sider
s the
pot
entia
l iss
ue o
f per
ceiv
ed p
ower
diff
eren
ces b
etw
een
the
heal
th p
rofe
ssio
nal a
nd th
e pe
rson
H2
.4.3
Pro
vide
s cle
ar a
nd a
ppro
pria
te w
ritte
n an
d ve
rbal
info
rmat
ion
to th
e pe
rson
to e
nabl
e th
em to
mak
e in
form
ed c
hoice
s and
ach
ieve
opt
imal
he
alth
out
com
es
Pres
crib
ing
Com
pete
ncie
s cov
ered
par
tly
H2.2
.2 E
xplo
res a
nd re
spon
ds a
ppro
pria
tely
to th
e pe
rson
’s co
ncer
ns a
nd
expe
ctat
ions
rega
rdin
g:
th
e co
nsul
tatio
n
thei
r hea
lth
th
eir o
wn
role
and
that
of h
ealth
pro
fess
iona
ls in
man
agin
g th
eir h
ealth
the
heal
th p
rofe
ssio
nal’s
scop
e of
pra
ctic
e
the
use
of m
edici
nes a
nd o
ther
trea
tmen
ts to
mai
ntai
n th
eir h
ealth
H2.2
.2 E
xplo
res a
nd re
spon
ds a
ppro
pria
tely
to th
e pe
rson
’s co
ncer
ns a
nd
expe
ctat
ions
rega
rdin
g:
th
e co
nsul
tatio
n
thei
r hea
lth
th
eir o
wn
role
and
that
of h
ealth
pro
fess
iona
ls in
man
agin
g th
eir h
ealth
the
heal
th p
rofe
ssio
nal’s
scop
e of
pra
ctic
e
the
use
of m
edici
nes a
nd o
ther
trea
tmen
ts to
mai
ntai
n th
eir h
ealth
Pr
escr
ibin
g Co
mpe
tenc
ies n
ot id
entif
ied
H2.4
.4 A
scer
tain
s tha
t the
info
rmat
ion
prov
ided
has
bee
n re
ceiv
ed a
nd u
nder
stoo
d co
rrec
tly
H2.4
.4 A
scer
tain
s tha
t the
info
rmat
ion
prov
ided
has
bee
n re
ceiv
ed a
nd u
nder
stoo
d co
rrec
tly

Page
| 9
3 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Mas
ter’s
4
+ 2
Inte
ract
ion
and
com
mun
icatio
n w
ith o
ther
hea
lth p
rofe
ssio
nals
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
4.2.
1
Prov
ides
info
rmat
ion
for c
olla
bora
tion
to m
embe
rs o
f int
er-p
rofe
ssio
nal
heal
thca
re te
ams b
oth
with
in fa
ciliti
es a
nd th
e co
mm
unity
H2
.5.1
Eng
ages
in o
pen,
inte
ract
ive
disc
ussio
ns w
ith o
ther
hea
lth p
rofe
ssio
nals
invo
lved
in ca
ring
for t
he p
erso
n H2
.5.3
Res
pond
s app
ropr
iate
ly to
com
mun
icat
ion
initi
ated
by
othe
r hea
lth
prof
essio
nals
H2.
5.4
Prov
ides
clea
r ver
bal a
nd w
ritte
n in
form
atio
n to
oth
er h
ealth
pro
fess
iona
ls by
secu
re m
eans
whe
n im
plem
entin
g ne
w tr
eatm
ents
with
med
icin
es o
r m
odify
ing
exist
ing
trea
tmen
t pla
ns
4.2.
1
Prov
ides
info
rmat
ion
for c
olla
bora
tion
to m
embe
rs o
f int
er-p
rofe
ssio
nal
heal
thca
re te
ams b
oth
with
in fa
ciliti
es a
nd th
e co
mm
unity
H2
.5.1
Eng
ages
in o
pen,
inte
ract
ive
disc
ussio
ns w
ith o
ther
hea
lth p
rofe
ssio
nals
invo
lved
in ca
ring
for t
he p
erso
n H2
.5.4
Pro
vide
s cle
ar v
erba
l and
writ
ten
info
rmat
ion
to o
ther
hea
lth p
rofe
ssio
nals
by se
cure
mea
ns w
hen
impl
emen
ting
new
trea
tmen
ts w
ith m
edic
ines
or
mod
ifyin
g ex
istin
g tr
eatm
ent p
lans
Pres
crib
ing
Com
pete
ncie
s cov
ered
par
tly
Nil
Nil
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d H2
.5.2
Con
firm
s tha
t the
ir ow
n un
ders
tand
ing
of in
form
atio
n pr
ovid
ed b
y ot
her
heal
th p
rofe
ssio
nals
is co
rrec
t
H2.5
.2 C
onfir
ms t
hat t
heir
own
unde
rsta
ndin
g of
info
rmat
ion
prov
ided
by
othe
r he
alth
pro
fess
iona
ls is
corr
ect
H2.5
.3 R
espo
nds a
ppro
pria
tely
to co
mm
unic
atio
n in
itiat
ed b
y ot
her h
ealth
pr
ofes
siona
ls As
sess
men
t and
dia
gnos
is Pr
escr
ibin
g co
mpe
tenc
ies c
over
ed c
ompl
etel
y
1.2.
1
Cond
ucts
an
asse
ssm
ent t
hat i
s app
ropr
iate
to b
oth
the
heal
th
prof
essio
nal’s
scop
e of
pra
ctice
and
the
pers
on’s
clini
cal c
onte
xt
1.2.
2
Revi
ews a
nd in
terp
rets
info
rmat
ion
in th
e pe
rson
’s he
alth
reco
rds
1.2.
5
Asce
rtai
ns th
at su
ffici
ent i
nfor
mat
ion
has b
een
obta
ined
abo
ut th
e pe
rson
’s co
-exi
stin
g co
nditi
ons a
nd cu
rren
t tre
atm
ents
to id
entif
y po
ssib
le ri
sks a
nd
cont
rain
dica
tions
for t
reat
men
t 1.
2.6
Pe
rfor
ms c
linic
al e
xam
inat
ions
that
are
with
in th
e he
alth
pro
fess
iona
l’s
own
scop
e of
pra
ctice
and
rele
vant
to th
e pe
rson
’s pr
oble
m a
nd in
terp
rets
th
e fin
ding
s of t
hese
exa
min
atio
ns
1.3.
1
Synt
hesis
es in
form
atio
n fr
om th
e co
mpr
ehen
sive
asse
ssm
ent a
nd d
evel
ops
prov
ision
al a
nd d
iffer
entia
l dia
gnos
es
1.3.
2
Deve
lops
a d
iagn
ostic
stra
tegy
and
per
form
s rel
evan
t inv
estig
atio
ns
1.3.
3
Expl
ains
the
clini
cal i
ssue
s and
thei
r im
plic
atio
ns to
the
pers
on
1.2.
1
Cond
ucts
an
asse
ssm
ent t
hat i
s app
ropr
iate
to b
oth
the
heal
th
prof
essio
nal’s
scop
e of
pra
ctice
and
the
pers
on’s
clini
cal c
onte
xt
1.2.
5
Asce
rtai
ns th
at su
ffici
ent i
nfor
mat
ion
has b
een
obta
ined
abo
ut th
e pe
rson
’s co
-exi
stin
g co
nditi
ons a
nd cu
rren
t tre
atm
ents
to id
entif
y po
ssib
le ri
sks a
nd
cont
rain
dica
tions
for t
reat
men
t 1.
2.6
Pe
rfor
ms c
linic
al e
xam
inat
ions
that
are
with
in th
e he
alth
pro
fess
iona
l’s
own
scop
e of
pra
ctice
and
rele
vant
to th
e pe
rson
’s pr
oble
m a
nd in
terp
rets
th
e fin
ding
s of t
hese
exa
min
atio
ns
1.3.
1
Synt
hesis
es in
form
atio
n fr
om th
e co
mpr
ehen
sive
asse
ssm
ent a
nd d
evel
ops
prov
ision
al a
nd d
iffer
entia
l dia
gnos
es
1.3.
2
Deve
lops
a d
iagn
ostic
stra
tegy
and
per
form
s rel
evan
t inv
estig
atio
ns
1.3.
3
Expl
ains
the
clini
cal i
ssue
s and
thei
r im
plic
atio
ns to
the
pers
on

Page
| 9
4 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Mas
ter’s
4
+ 2
Asse
ssm
ent a
nd d
iagn
osis
Pres
crib
ing
Com
pete
ncie
s cov
ered
par
tly
1.2.
3
Obt
ains
rele
vant
info
rmat
ion
from
the
pers
on a
bout
thei
r med
icine
s, an
d th
eir m
edica
l and
clin
ical
hist
ory,
incl
udin
g th
eir c
o-ex
istin
g co
nditi
ons,
trea
tmen
ts, a
lcoho
l and
subs
tanc
e us
e, a
llerg
ies a
nd so
cial c
onte
xt
1.2.
4
Asse
sses
the
pers
on’s
risk
fact
ors f
or p
oor a
dher
ence
; for
exa
mpl
e so
cial
isola
tion,
phy
sical
impa
irmen
t, co
gniti
ve im
pairm
ent o
r dist
urba
nce,
low
En
glish
pro
ficie
ncy,
low
hea
lth li
tera
cy, f
inan
cial d
isadv
anta
ge
1.2.
3
Obt
ains
rele
vant
info
rmat
ion
from
the
pers
on a
bout
thei
r med
icine
s, an
d th
eir m
edica
l and
clin
ical
hist
ory,
inclu
ding
thei
r co-
exist
ing
cond
ition
s, tr
eatm
ents
, alco
hol a
nd su
bsta
nce
use,
alle
rgie
s and
socia
l con
text
1.
2.4
As
sess
es th
e pe
rson
’s ris
k fa
ctor
s for
poo
r adh
eren
ce; f
or e
xam
ple
socia
l iso
latio
n, p
hysic
al im
pairm
ent,
cogn
itive
impa
irmen
t or d
istur
banc
e, lo
w
Engl
ish p
rofic
ienc
y, lo
w h
ealth
lite
racy
, fin
ancia
l disa
dvan
tage
Pr
escr
ibin
g Co
mpe
tenc
ies n
ot id
entif
ied
1.
2.2
Re
view
s and
inte
rpre
ts in
form
atio
n in
the
pers
on’s
heal
th re
cord
s
Ther
apeu
tic ch
oice
and
initi
atio
n Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed c
ompl
etel
y
2.1.
2
Reco
gnise
s whe
n it
is cli
nica
lly a
ppro
pria
te to
impl
emen
t non
-ph
arm
acol
ogica
l tre
atm
ents
2.
2.7
Su
pple
men
ts v
erba
l inf
orm
atio
n w
ith w
ritte
n in
form
atio
n ab
out t
he
cond
ition
and
trea
tmen
t opt
ions
(whe
re a
ppro
pria
te)
2.2.
9
Refe
rs th
e pe
rson
for f
urth
er a
sses
smen
t or t
reat
men
t whe
n th
e su
itabl
e tr
eatm
ent o
ptio
ns a
re o
utsid
e th
e he
alth
pro
fess
iona
l’s o
wn
scop
e of
pr
actic
e 3.
1.1
Ne
gotia
tes t
hera
peut
ic go
als t
hat e
nhan
ce th
e pe
rson
’s se
lf-m
anag
emen
t of
thei
r con
ditio
n 3.
2.4
De
velo
ps th
e tr
eatm
ent p
lan
in p
artn
ersh
ip w
ith th
e pe
rson
H1
.4.3
Dem
onst
rate
s kno
wle
dge
of th
e m
edic
ines
com
mon
ly p
resc
ribed
2.1.
2
Reco
gnise
s whe
n it
is cli
nica
lly a
ppro
pria
te to
impl
emen
t non
-ph
arm
acol
ogica
l tre
atm
ents
2.
2.7
Su
pple
men
ts v
erba
l inf
orm
atio
n w
ith w
ritte
n in
form
atio
n ab
out t
he
cond
ition
and
trea
tmen
t opt
ions
(whe
re a
ppro
pria
te)
2.2.
9
Refe
rs th
e pe
rson
for f
urth
er a
sses
smen
t or t
reat
men
t whe
n th
e su
itabl
e tr
eatm
ent o
ptio
ns a
re o
utsid
e th
e he
alth
pro
fess
iona
l’s o
wn
scop
e of
pr
actic
e 3.
1.1
Ne
gotia
tes t
hera
peut
ic go
als t
hat e
nhan
ce th
e pe
rson
’s se
lf-m
anag
emen
t of
thei
r con
ditio
n 3.
2.4
De
velo
ps th
e tr
eatm
ent p
lan
in p
artn
ersh
ip w
ith th
e pe
rson
H1
.4.3
Dem
onst
rate
s kno
wle
dge
of th
e m
edic
ines
com
mon
ly p
resc
ribed
Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed p
artly
2.
2.1
In
tegr
ates
kno
wle
dge
of p
harm
acol
ogy,
oth
er b
iom
edic
al sc
ienc
es, c
linica
l m
edic
ine,
and
ther
apeu
tics a
nd id
entif
ies m
edici
nes s
uita
ble
for t
reat
ing
the
cond
ition
2.
2.2
O
btai
ns, i
nter
pret
s, an
d ap
plie
s cur
rent
evi
denc
e an
d in
form
atio
n ab
out
med
icin
es to
info
rm d
ecisi
ons a
bout
inco
rpor
atin
g m
edici
nes i
nto
the
pers
on’s
trea
tmen
t pla
n 2.
2.3
Id
entif
ies m
edici
nes o
ptio
ns th
at a
re li
kely
to p
rovi
de th
erap
eutic
ally
ef
fect
ive
and
safe
trea
tmen
t and
tailo
rs th
em fo
r the
per
son
2.2.
4
Cons
ider
s the
cost
and
affo
rdab
ility
of t
he m
edici
nes t
o th
e pe
rson
2.2.
1
Inte
grat
es k
now
ledg
e of
pha
rmac
olog
y, o
ther
bio
med
ical
scie
nces
, clin
ical
med
icin
e, a
nd th
erap
eutic
s and
iden
tifie
s med
icine
s sui
tabl
e fo
r tre
atin
g th
e co
nditi
on
2.2.
2
Obt
ains
, int
erpr
ets,
and
appl
ies c
urre
nt e
vide
nce
and
info
rmat
ion
abou
t m
edic
ines
to in
form
dec
ision
s abo
ut in
corp
orat
ing
med
icine
s int
o th
e pe
rson
’s tr
eatm
ent p
lan
2.2.
3
Iden
tifie
s med
icine
s opt
ions
that
are
like
ly to
pro
vide
ther
apeu
tical
ly
effe
ctiv
e an
d sa
fe tr
eatm
ent a
nd ta
ilors
them
for t
he p
erso
n

Page
| 9
5 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Mas
ter’s
4
+ 2
2.2.
6
Disc
usse
s the
trea
tmen
t opt
ions
and
med
icine
s with
the
pers
on,
cons
ider
ing:
the
prio
ritie
s for
trea
ting
thei
r cur
rent
con
ditio
n an
d co
-ex
istin
g co
nditi
ons;
thei
r rea
dine
ss to
add
ress
the
curr
ent c
ondi
tion;
thei
r ex
pect
atio
ns o
f tre
atm
ent
3.1.
2
Asce
rtai
ns th
at a
ll pa
rtie
s hav
e a
com
mon
und
erst
andi
ng o
f the
ther
apeu
tic
goal
s and
how
they
will
be
man
aged
3.
2.1
Ex
plor
es th
e pe
rson
’s op
inio
ns a
nd p
refe
renc
es co
ncer
ning
med
icine
s and
th
e tr
eatm
ent p
lan
3.2.
2
Cons
ults
oth
er h
ealth
pro
fess
iona
ls ab
out p
oten
tial m
edic
ines
and
the
trea
tmen
t pla
n 3.
2.3
Re
ache
s agr
eem
ent w
ith th
e pe
rson
abo
ut m
edici
nes t
o be
use
d to
trea
t th
eir c
ondi
tion
2.2.
6
Disc
usse
s the
trea
tmen
t opt
ions
and
med
icine
s with
the
pers
on,
cons
ider
ing:
the
prio
ritie
s for
trea
ting
thei
r cur
rent
con
ditio
n an
d co
-ex
istin
g co
nditi
ons;
thei
r rea
dine
ss to
add
ress
the
curr
ent c
ondi
tion;
thei
r ex
pect
atio
ns o
f tre
atm
ent
3.1.
2
Asce
rtai
ns th
at a
ll pa
rtie
s hav
e a
com
mon
und
erst
andi
ng o
f the
ther
apeu
tic
goal
s and
how
they
will
be
man
aged
3.
2.1
Ex
plor
es th
e pe
rson
’s op
inio
ns a
nd p
refe
renc
es co
ncer
ning
med
icine
s and
th
e tr
eatm
ent p
lan
3.2.
3
Reac
hes a
gree
men
t with
the
pers
on a
bout
med
icine
s to
be u
sed
to tr
eat
thei
r con
ditio
n
Ther
apeu
tic ch
oice
and
initi
atio
n Pr
escr
ibin
g Co
mpe
tenc
ies n
ot id
entif
ied
2.1.
1
Reco
gnise
s whe
n it
is cli
nica
lly a
ppro
pria
te n
ot to
inte
rven
e; fo
r exa
mpl
e, in
ca
ses w
here
the
signs
and
sym
ptom
s are
like
ly to
reso
lve
with
out
trea
tmen
t 2.
2.5
Co
nsid
ers t
he im
plica
tions
to th
e w
ider
com
mun
ity o
f usin
g a
part
icul
ar
med
icin
e to
trea
t the
per
son
2.2.
8
Allo
ws t
he p
erso
n tim
e to
mak
e an
info
rmed
dec
ision
abo
ut th
eir
trea
tmen
t 3.
2.5
O
btai
ns a
ppro
val t
o us
e th
e m
edici
nes (
whe
re re
leva
nt)
3.2.
6
Stop
s or m
odifi
es th
e pe
rson
’s ex
istin
g m
edici
nes a
nd o
ther
man
agem
ent
stra
tegi
es if
requ
ired
3.2.
7
Ensu
res t
he p
erso
n un
ders
tand
s the
trea
tmen
t pla
n an
d ho
w to
use
the
med
icin
e sa
fely
and
effe
ctiv
ely
4.1.
1
Prep
ares
pre
scrip
tions
or m
edic
atio
n or
ders
that
com
ply
with
rele
vant
le
gisla
tion,
gui
delin
es o
r cod
es o
f pra
ctice
, and
org
anisa
tiona
l pol
icies
and
pr
oced
ures
4.
1.2
Pr
ovid
es a
ccur
ate
and
clear
ver
bal m
edica
tion
orde
rs th
at co
mpl
y w
ith
rele
vant
legi
slatio
n, g
uide
lines
or c
odes
of p
ract
ice a
nd o
rgan
isatio
nal
polic
ies a
nd p
roce
dure
s (w
here
rele
vant
) H1
.4.1
App
lies q
ualit
y us
e of
med
icine
s prin
cipl
es w
hen
pres
crib
ing
med
icine
s
2.1.
1
Reco
gnise
s whe
n it
is cli
nica
lly a
ppro
pria
te n
ot to
inte
rven
e; fo
r exa
mpl
e, in
ca
ses w
here
the
signs
and
sym
ptom
s are
like
ly to
reso
lve
with
out
trea
tmen
t 2.
2.4
Co
nsid
ers t
he co
st a
nd a
fford
abili
ty o
f the
med
icine
s to
the
pers
on
2.2.
5
Cons
ider
s the
impl
icatio
ns to
the
wid
er co
mm
unity
of u
sing
a pa
rtic
ular
m
edic
ine
to tr
eat t
he p
erso
n 2.
2.8
Al
low
s the
per
son
time
to m
ake
an in
form
ed d
ecisi
on a
bout
thei
r tr
eatm
ent
3.2.
2
Cons
ults
oth
er h
ealth
pro
fess
iona
ls ab
out p
oten
tial m
edic
ines
and
the
trea
tmen
t pla
n 3.
2.5
O
btai
ns a
ppro
val t
o us
e th
e m
edici
nes (
whe
re re
leva
nt)
3.2.
6
Stop
s or m
odifi
es th
e pe
rson
’s ex
istin
g m
edici
nes a
nd o
ther
man
agem
ent
stra
tegi
es if
requ
ired
3.2.
7
Ensu
res t
he p
erso
n un
ders
tand
s the
trea
tmen
t pla
n an
d ho
w to
use
the
med
icin
e sa
fely
and
effe
ctiv
ely
4.1.
1
Prep
ares
pre
scrip
tions
or m
edic
atio
n or
ders
that
com
ply
with
rele
vant
le
gisla
tion,
gui
delin
es o
r cod
es o
f pra
ctice
, and
org
anisa
tiona
l pol
icies
and
pr
oced
ures
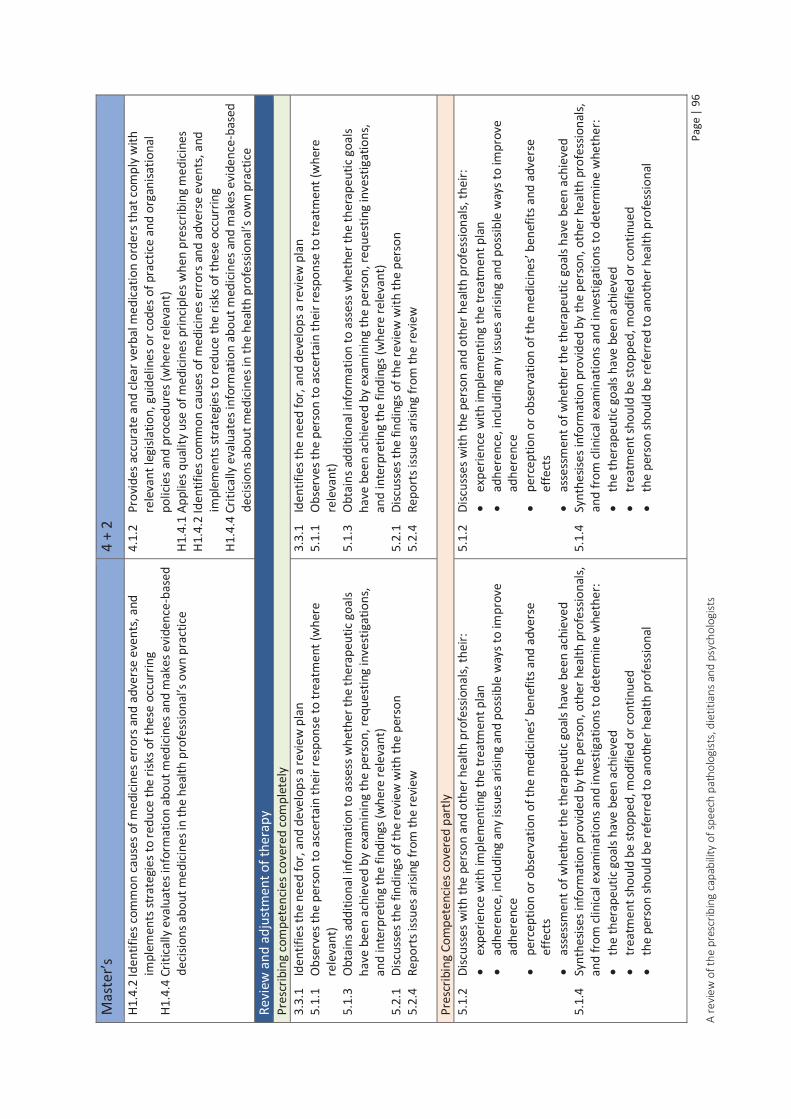
Page
| 9
6 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Mas
ter’s
4
+ 2
H1.4
.2 Id
entif
ies c
omm
on c
ause
s of m
edici
nes e
rror
s and
adv
erse
eve
nts,
and
impl
emen
ts st
rate
gies
to re
duce
the
risks
of t
hese
occ
urrin
g H1
.4.4
Crit
ically
eva
luat
es in
form
atio
n ab
out m
edici
nes a
nd m
akes
evi
denc
e-ba
sed
deci
sions
abo
ut m
edici
nes i
n th
e he
alth
pro
fess
iona
l’s o
wn
prac
tice
4.1.
2
Prov
ides
acc
urat
e an
d cle
ar v
erba
l med
icatio
n or
ders
that
com
ply
with
re
leva
nt le
gisla
tion,
gui
delin
es o
r cod
es o
f pra
ctice
and
org
anisa
tiona
l po
licie
s and
pro
cedu
res (
whe
re re
leva
nt)
H1.4
.1 A
pplie
s qua
lity
use
of m
edici
nes p
rinci
ples
whe
n pr
escr
ibin
g m
edici
nes
H1.4
.2 Id
entif
ies c
omm
on c
ause
s of m
edici
nes e
rror
s and
adv
erse
eve
nts,
and
impl
emen
ts st
rate
gies
to re
duce
the
risks
of t
hese
occ
urrin
g H1
.4.4
Crit
ically
eva
luat
es in
form
atio
n ab
out m
edici
nes a
nd m
akes
evi
denc
e-ba
sed
deci
sions
abo
ut m
edici
nes i
n th
e he
alth
pro
fess
iona
l’s o
wn
prac
tice
Revi
ew a
nd a
djus
tmen
t of t
hera
py
Pres
crib
ing
com
pete
ncie
s cov
ered
com
plet
ely
3.3.
1
Iden
tifie
s the
nee
d fo
r, an
d de
velo
ps a
revi
ew p
lan
5.1.
1
Obs
erve
s the
per
son
to a
scer
tain
thei
r res
pons
e to
trea
tmen
t (w
here
re
leva
nt)
5.1.
3
Obt
ains
add
ition
al in
form
atio
n to
ass
ess w
heth
er th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
by
exam
inin
g th
e pe
rson
, req
uest
ing
inve
stig
atio
ns,
and
inte
rpre
ting
the
findi
ngs (
whe
re re
leva
nt)
5.2.
1
Disc
usse
s the
find
ings
of t
he re
view
with
the
pers
on
5.2.
4
Repo
rts i
ssue
s aris
ing
from
the
revi
ew
3.3.
1
Iden
tifie
s the
nee
d fo
r, an
d de
velo
ps a
revi
ew p
lan
5.1.
1
Obs
erve
s the
per
son
to a
scer
tain
thei
r res
pons
e to
trea
tmen
t (w
here
re
leva
nt)
5.1.
3
Obt
ains
add
ition
al in
form
atio
n to
ass
ess w
heth
er th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
by
exam
inin
g th
e pe
rson
, req
uest
ing
inve
stig
atio
ns,
and
inte
rpre
ting
the
findi
ngs (
whe
re re
leva
nt)
5.2.
1
Disc
usse
s the
find
ings
of t
he re
view
with
the
pers
on
5.2.
4
Repo
rts i
ssue
s aris
ing
from
the
revi
ew
Pres
crib
ing
Com
pete
ncie
s cov
ered
par
tly
5.1.
2
Disc
usse
s with
the
pers
on a
nd o
ther
hea
lth p
rofe
ssio
nals,
thei
r:
expe
rienc
e w
ith im
plem
entin
g th
e tr
eatm
ent p
lan
ad
here
nce,
inclu
ding
any
issu
es a
risin
g an
d po
ssib
le w
ays t
o im
prov
e ad
here
nce
pe
rcep
tion
or o
bser
vatio
n of
the
med
icine
s’ be
nefit
s and
adv
erse
ef
fect
s
asse
ssm
ent o
f whe
ther
the
ther
apeu
tic g
oals
have
bee
n ac
hiev
ed
5.1.
4
Synt
hesis
es in
form
atio
n pr
ovid
ed b
y th
e pe
rson
, oth
er h
ealth
pro
fess
iona
ls,
and
from
clin
ical
exa
min
atio
ns a
nd in
vest
igat
ions
to d
eter
min
e w
heth
er:
th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
trea
tmen
t sho
uld
be st
oppe
d, m
odifi
ed o
r con
tinue
d
the
pers
on sh
ould
be
refe
rred
to a
noth
er h
ealth
pro
fess
iona
l
5.1.
2
Disc
usse
s with
the
pers
on a
nd o
ther
hea
lth p
rofe
ssio
nals,
thei
r:
expe
rienc
e w
ith im
plem
entin
g th
e tr
eatm
ent p
lan
ad
here
nce,
inclu
ding
any
issu
es a
risin
g an
d po
ssib
le w
ays t
o im
prov
e ad
here
nce
pe
rcep
tion
or o
bser
vatio
n of
the
med
icine
s’ be
nefit
s and
adv
erse
ef
fect
s
asse
ssm
ent o
f whe
ther
the
ther
apeu
tic g
oals
have
bee
n ac
hiev
ed
5.1.
4
Synt
hesis
es in
form
atio
n pr
ovid
ed b
y th
e pe
rson
, oth
er h
ealth
pro
fess
iona
ls,
and
from
clin
ical
exa
min
atio
ns a
nd in
vest
igat
ions
to d
eter
min
e w
heth
er:
th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
trea
tmen
t sho
uld
be st
oppe
d, m
odifi
ed o
r con
tinue
d
the
pers
on sh
ould
be
refe
rred
to a
noth
er h
ealth
pro
fess
iona
l

Page
| 9
7 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Mas
ter’s
4
+ 2
Revi
ew a
nd a
djus
tmen
t of t
hera
py
Pres
crib
ing
Com
pete
ncie
s not
iden
tifie
d 5.
2.2
Id
entif
ies i
f the
per
son
requ
ires a
com
preh
ensiv
e m
edic
ines
revi
ew
5.2.
3
Wor
ks in
par
tner
ship
with
the
pers
on a
nd o
ther
hea
lth p
rofe
ssio
nals
to
mod
ify th
e tr
eatm
ent p
lan
to o
ptim
ise th
e sa
fety
and
effe
ctiv
enes
s of
trea
tmen
t (w
here
rele
vant
) 5.
2.5
Or
gani
ses t
he n
ext r
evie
w
5.2.
2
Iden
tifie
s if t
he p
erso
n re
quire
s a co
mpr
ehen
sive
med
icin
es re
view
5.
2.3
W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
m
odify
the
trea
tmen
t pla
n to
opt
imise
the
safe
ty a
nd e
ffect
iven
ess o
f tr
eatm
ent (
whe
re re
leva
nt)
5.2.
5
Orga
nise
s the
nex
t rev
iew
Le
gal a
nd p
rofe
ssio
nal r
equi
rem
ents
Pr
escr
ibin
g co
mpe
tenc
ies c
over
ed c
ompl
etel
y H1
.2.1
Dem
onst
rate
s kno
wle
dge
of a
nd c
ompl
ianc
e w
ith:
pr
ofes
siona
l sta
ndar
ds
co
des o
f con
duct
scop
e of
pra
ctice
stat
emen
ts o
r gui
delin
es
H1.2
.2 P
ract
ices w
ithin
the
limits
of t
he h
ealth
pro
fess
iona
l’s o
wn
educ
atio
n,
trai
ning
and
scop
e of
pra
ctice
H1
.2.3
Dem
onst
rate
s res
pect
for t
he sc
ope
of p
ract
ice o
f oth
er h
ealth
pr
ofes
siona
ls an
d th
eir c
ontr
ibut
ion
with
in a
colla
bora
tive
care
mod
el,
part
icula
rly th
at o
f the
per
son’
s mai
n he
alth
care
pro
vide
r H1
.2.4
Acc
epts
resp
onsib
ility
and
is a
ccou
ntab
le fo
r the
care
pro
vide
d to
the
pers
on
H2.1
.1 A
dher
es to
legi
slativ
e an
d w
orkp
lace
requ
irem
ents
for o
btai
ning
and
re
cord
ing
cons
ent f
or:
Ac
cess
ing
heal
th re
cord
s
obta
inin
g in
form
atio
n fr
om, a
nd p
rovi
ding
info
rmat
ion
to, o
ther
hea
lth
prof
essio
nals
co
nduc
ting
a cli
nica
l exa
min
atio
n
prov
idin
g cli
nica
l ser
vice
s
the
pote
ntia
l ben
efits
and
har
ms
H1.2
.1 D
emon
stra
tes k
now
ledg
e of
and
com
plia
nce
with
:
prof
essio
nal s
tand
ards
code
s of c
ondu
ct
sc
ope
of p
ract
ice st
atem
ents
or g
uide
lines
H1
.2.2
Pra
ctice
s with
in th
e lim
its o
f the
hea
lth p
rofe
ssio
nal’s
ow
n ed
ucat
ion,
tr
aini
ng a
nd sc
ope
of p
ract
ice
H1.2
.3 D
emon
stra
tes r
espe
ct fo
r the
scop
e of
pra
ctice
of o
ther
hea
lth
prof
essio
nals
and
thei
r con
trib
utio
n w
ithin
a co
llabo
rativ
e ca
re m
odel
, pa
rticu
larly
that
of t
he p
erso
n’s m
ain
heal
thca
re p
rovi
der
H1.2
.4 A
ccep
ts re
spon
sibili
ty a
nd is
acc
ount
able
for t
he ca
re p
rovi
ded
to th
e pe
rson
H2
.1.1
Adh
eres
to le
gisla
tive
and
wor
kpla
ce re
quire
men
ts fo
r obt
aini
ng a
nd
reco
rdin
g co
nsen
t for
:
Acce
ssin
g he
alth
reco
rds
ob
tain
ing
info
rmat
ion
from
, and
pro
vidi
ng in
form
atio
n to
, oth
er h
ealth
pr
ofes
siona
ls
cond
uctin
g a
clini
cal e
xam
inat
ion
pr
ovid
ing
clini
cal s
ervi
ces
th
e po
tent
ial b
enef
its a
nd h
arm
s Pr
escr
ibin
g Co
mpe
tenc
ies c
over
ed p
artly
H1
.1.1
Dem
onst
rate
s kno
wle
dge
of, a
nd co
mpl
ies w
ith, l
egisl
atio
n, re
gula
tions
, an
d co
mm
on la
w a
pplic
able
to p
resc
ribin
g (a
s fur
ther
def
ined
by
the
know
ledg
e su
bsec
tion
of th
is co
mpe
tenc
y ar
ea)
H1.1
.1 D
emon
stra
tes k
now
ledg
e of
, and
com
plie
s with
, leg
islat
ion,
regu
latio
ns,
and
com
mon
law
app
licab
le to
pre
scrib
ing
(as f
urth
er d
efin
ed b
y th
e kn
owle
dge
subs
ectio
n of
this
com
pete
ncy
area
)

Page
| 9
8 A
revi
ew o
f the
pre
scrib
ing
capa
bilit
y of
spee
ch p
atho
logi
sts,
die
titia
ns a
nd p
sych
olog
ists
Mas
ter’s
4
+ 2
H1.1
.2 M
aint
ains
acc
urat
e an
d co
mpl
ete
reco
rds o
f:
the
cons
ulta
tion
cl
inic
al e
xam
inat
ions
and
inve
stig
atio
n re
sults
risk
fact
ors f
or m
edici
nes m
isadv
entu
re
th
e pe
rson
’s de
cisio
n to
dec
line
trea
tmen
t (w
here
rele
vant
)
chan
ges t
o th
e pe
rson
’s m
edici
nes m
anag
emen
t pla
n, in
cludi
ng th
e ra
tiona
le b
ehin
d th
ese
chan
ges
th
e re
view
pla
n, re
com
men
datio
ns, a
nd d
ate
for n
ext r
evie
w
ou
tcom
es o
f tre
atm
ent
H1.3
.1 D
emon
stra
tes k
now
ledg
e of
and
com
plie
s with
nat
iona
l, st
ate
and
terr
itory
, an
d fa
cilit
y po
licie
s and
pro
cedu
res i
n re
latio
n to
pre
scrib
ing
H1.3
.3 C
ontr
ibut
es to
the
impr
ovem
ent o
f pol
icie
s and
pro
cedu
res f
or th
e ju
dicio
us, a
ppro
pria
te, s
afe
and
effe
ctiv
e us
e of
med
icine
s H1
.5.1
Eng
ages
in o
ngoi
ng p
rofe
ssio
nal d
evel
opm
ent a
nd e
duca
tion
to im
prov
e pr
escr
ibin
g pr
actic
es
H1.1
.2 M
aint
ains
acc
urat
e an
d co
mpl
ete
reco
rds o
f:
the
cons
ulta
tion
cl
inic
al e
xam
inat
ions
and
inve
stig
atio
n re
sults
risk
fact
ors f
or m
edici
nes m
isadv
entu
re
th
e pe
rson
’s de
cisio
n to
dec
line
trea
tmen
t (w
here
rele
vant
)
chan
ges t
o th
e pe
rson
’s m
edici
nes m
anag
emen
t pla
n, in
cludi
ng th
e ra
tiona
le b
ehin
d th
ese
chan
ges
th
e re
view
pla
n, re
com
men
datio
ns, a
nd d
ate
for n
ext r
evie
w
ou
tcom
es o
f tre
atm
ent
H1.3
.1 D
emon
stra
tes k
now
ledg
e of
and
com
plie
s with
nat
iona
l, st
ate
and
terr
itory
, an
d fa
cilit
y po
licie
s and
pro
cedu
res i
n re
latio
n to
pre
scrib
ing
H1.3
.3 C
ontr
ibut
es to
the
impr
ovem
ent o
f pol
icie
s and
pro
cedu
res f
or th
e ju
dicio
us, a
ppro
pria
te, s
afe
and
effe
ctiv
e us
e of
med
icine
s H1
.5.1
Eng
ages
in o
ngoi
ng p
rofe
ssio
nal d
evel
opm
ent a
nd e
duca
tion
to im
prov
e pr
escr
ibin
g pr
actic
es
Le
gal a
nd p
rofe
ssio
nal r
equi
rem
ents
Pr
escr
ibin
g Co
mpe
tenc
ies n
ot id
entif
ied
H1.3
.2 D
emon
stra
tes a
ppro
pria
te p
rofe
ssio
nal j
udge
men
t whe
n in
terp
retin
g an
d ap
plyi
ng g
uide
lines
and
pro
toco
ls to
the
pers
on’s
situa
tion
H1.6
.1 Im
plem
ents
stra
tegi
es to
add
ress
influ
ence
s tha
t may
bia
s pre
scrib
ing
deci
sions
, inc
ludi
ng:
m
arke
ting
influ
ence
s
Poss
ible
per
sona
l, pr
ofes
siona
l or f
inan
cial
gai
n
Conf
licts
of i
nter
est
Th
e he
alth
pro
fess
iona
l’s o
wn
belie
fs, v
alue
s, an
d ex
perie
nces
H1.3
.2 D
emon
stra
tes a
ppro
pria
te p
rofe
ssio
nal j
udge
men
t whe
n in
terp
retin
g an
d ap
plyi
ng g
uide
lines
and
pro
toco
ls to
the
pers
on’s
situa
tion
H1.6
.1 Im
plem
ents
stra
tegi
es to
add
ress
influ
ence
s tha
t may
bia
s pre
scrib
ing
deci
sions
, inc
ludi
ng:
m
arke
ting
influ
ence
s
Poss
ible
per
sona
l, pr
ofes
siona
l or f
inan
cial
gai
n
Conf
licts
of i
nter
est
Th
e he
alth
pro
fess
iona
l’s o
wn
belie
fs, v
alue
s, an
d ex
perie
nces

Page | 99 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Interaction and communication with patients
Prescribing competencies relating to communication style and therapeutic partnership with patients and carers map well. Competencies relating to respect for the patient, consideration of power differential and providing clear written and verbal information to enable informed decision making are also completely covered by the psychology standards.
The prescribing competency regarding exploring and responding to patient concerns is partly covered by the psychology standards. The competency relating to ascertaining that information has been received and understood correctly is not covered.
Interaction and communication with other health professionals
Prescribing competencies relating to provision of information to, and collaboration with, other health professionals map well.
The prescribing competency relating to responding appropriately to communication initiated by other health professionals is covered completely by the APAC core competencies, but not by any of the other standards. The prescribing competency relating to confirming understanding of information provided by other health professionals was not identified in any of the psychology standards.
Assessment and diagnosis
Assessment and diagnosis competencies are generally covered well by psychology standards. Review and interpretation of information in the person’s health records is covered completely by the APAC core competencies, but not by any of the other standards.
The prescribing competency regarding obtaining information from the patient maps partly. Psychology standards do not detail the specifics of information required such as medicines, allergies, alcohol and substance abuse; information that is vital when prescribing a medicine. Assessment of a patient’s risk factors for poor adherence also maps partly to the psychology standards.
Therapeutic choice and initiation
Prescribing competencies that map completely include recognising when non pharmacological treatment is appropriate, supplementing verbal with written information, referral when treatment is outside scope of practice, negotiating therapeutic goals that enhance the person’s self-management, developing a treatment plan in partnership with the patient and knowledge of medicines commonly prescribed.
Whilst the psychology standards detail planning and implementation of interventions, many of the prescribing competencies in his category are only partly covered, because they specifically relate to selection of medicine. These include identification of suitable medicine options, discussion of medicine options with the patient and reaching agreement with the patient about medicine choice. The prescribing competencies regarding consideration of cost and affordability of medicines and consulting other health professionals about potential medicines map partly to the APAC core competencies, but cannot be identified in any other psychology standards.
Not surprisingly, prescribing competencies specifically relating to medicine selection and ordering were not identified in the psychology standards. These included critically evaluating medicines information, implications to the wider community of using a particular medicine, application of

Page | 100 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Quality Use of Medicines (QUM) principles, identification of medicine errors and adverse events, obtaining approval for medicine use and providing appropriate medication orders. Other competencies not identified relate to interaction with the patient regarding initiation of medicine. These include allowing the patient time to make a decision, stopping or modifying existing medicines and ensuring patient understanding of therapeutic goals, management and how to use the medicine safely and effectively. In addition the prescribing competency relating to recognising when it is clinically appropriate not to intervene was not identified by any of the psychology standards.
Review and adjustment of therapy
Prescribing competencies covered well in this category are development of a review plan, observation of patient response to therapy, obtaining additional information to assess response to therapy, discussing review findings with the patient and reporting issues arising from the review.
The prescribing competency relating to discussing response to therapy with the person and other health professionals is partly covered in the psychology standards, as is that relating to synthesising the information obtained to determine whether changes to therapy are required.
Prescribing competencies not covered by the psychology standards are identifying if the patient requires a comprehensive medicines review, working with the person and other health professionals to modify the treatment plan and organising the next review.
Legal and professional requirements
Prescribing competencies that map completely with the psychology standards include those relating to scope of practice, professional standards, code of conduct, demonstrating respect for scope of practice of other health professionals, accountability and obtaining and recording patient consent.
Competencies that map partly include knowledge and compliance with legislation, policies and procedures relating to prescribing, contribution to the improvement of policies and procedures relating to medicines use and maintenance of records. The prescribing competency relating to ongoing professional development with respect to prescribing practices maps partly. Although the psychology standards cover CPD requirements, prescribing is currently not within scope of practice, so is not covered by CPD statements. If prescribing becomes an activity within scope of practice, then this competency will map fully.
Legal and professional competencies not identified in the psychology standards are those relating to interpretation and application of guidelines and protocols, and implementation of strategies to reduce prescribing bias.
Mapping Differences between the Masters and 4+2 entry route competency standards
Regardless of the education and training pathway to general registration, there is an assumption that the competency of entry level psychologists should be the same, and the respective standards should reflect this. Whilst the standards for the Masters and 4 + 2 entry route to general registration were very similar in their mapping, there were minor differences. This was due to the different ways activities were described in the APAC core competencies and the PsyBA 4 + 2 Internship program training objectives. The following competencies were covered completely by the Master’s route competencies, but not identified in the 4 + 2 competencies:
1.2.2 Reviews and interprets information in the person’s health records

Page | 101 A review of the prescribing capability of speech pathologists, dietitians and psychologists
2.2.4 Considers the cost and affordability of the medicines to the person
3.2.2 Consults other health professionals about potential medicines and the treatment plan
H2.5.3 Responds appropriately to communication initiated by other health professionals
LLearning Outcomes Mapping
The representative learning outcomes were mapped at an element level to provide additional information regarding undergraduate education and training. The results of the mapping for the QUT psychology programs of study are shown in table C3, appendix C.
The following Prescribing Competencies Framework elements were not identified in any of the combined learning objectives for programs of study leading to general registration via the Master’s or the 4 + 2 route:
Bachelor of Science (Psychology) + Honours/Diploma (4years)
Element 2.1: Considers non-pharmacological treatment options suitable for treating the person and their condition (identified in elective subject only)
Element 3.1: Negotiates therapeutic goals with the person
Element 3.2: Works in partnership with the person and other health professionals to select medicines and to tailor and implement a treatment plan
Element 3.3: Develops a review plan tailored to the person’s needs
Element 4.1: Provides clear instructions to other health professionals who dispense, supply, or administer medicines prescribed for the person
Element 5.1: Obtains information to assess the person’s response to treatment
Element 5.2: Works in partnership with the person and other health professionals to address issues arising from the review
Element H1.3: Practices within the applicable frameworks of the healthcare setting and system (identified in elective subject only)
Element H1.4: Practices quality use of medicines principles (identified in elective subject only)
Element H1.5: Demonstrates a commitment to continual quality improvement of the health professional’s own prescribing (identified in elective subject only)
Element H1.6: Addresses the potential for bias in prescribing decisions
Element H2.1: Obtains consent to provide clinical services to the person
Element H2.2: Acknowledges the person, their family, and carers as integral to care and collaborates to achieve optimal health outcomes
Bachelor of Science (Psychology) + Honours/Diploma +Masters of Clinical Psychology course (6 years)
Element 3.1: Negotiates therapeutic goals with the person
Element 3.2: Works in partnership with the person and other health professionals to select medicines and to tailor and implement a treatment plan

Page | 102 A review of the prescribing capability of speech pathologists, dietitians and psychologists
Element 3.3: Develops a review plan tailored to the person’s needs
Element 4.1: Provides clear instructions to other health professionals who dispense, supply, or administer medicines prescribed for the person
Element 5.1: Obtains information to assess the person’s response to treatment
Element 5.2: Works in partnership with the person and other health professionals to address issues arising from the review
Element H1.3: Practices within the applicable frameworks of the healthcare setting and system (identified in elective subject only)
Element H1.5: Demonstrates a commitment to continual quality improvement of the health professional’s own prescribing (identified in elective subject only)
Element H1.6: Addresses the potential for bias in prescribing decisions
Element H2.1: Obtains consent to provide clinical services to the person
Element H2.2: Acknowledges the person, their family, and carers as integral to care and collaborates to achieve optimal health outcomes
MMapping psychology prescribing capability against Prescribing Models
To provide additional information to identify the prescribing capabilities of psychologists, the performance criteria of the Prescribing Competencies Framework were mapped against the HPPP models of prescribing. The results from the psychology mapping were then included to create a summary table (table 7). This table builds a clearer picture of the competency expectations dependent on the prescribing model, and indicates current gaps in psychology prescribing competence.

Page
| 1
03
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
Tabl
e 7:
Rel
atio
nshi
p be
twee
n th
e Pr
escr
ibin
g Co
mpe
tenc
ies F
ram
ewor
k, th
e HP
PP p
resc
ribin
g m
odel
s and
pro
fess
iona
l sta
ndar
ds a
nd e
ntry
leve
l co
mpe
tenc
ies f
or p
sych
olog
ists
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Co
mpe
tenc
y Ar
ea 1
Und
erst
ands
the
pers
on a
nd th
eir c
linica
l nee
ds
Elem
ent 1
.1 E
stab
lishe
s a th
erap
eutic
par
tner
ship
with
the
pers
on a
nd a
colla
bora
tive
rela
tions
hip
with
oth
er h
ealth
pro
fess
iona
ls
1.1.
1 Us
es a
ppro
pria
te
com
mun
icat
ion
stra
tegi
es to
es
tabl
ish a
ther
apeu
tic p
artn
ersh
ip
with
the
pers
on
M
aste
rs
4 +
2
Elem
ent 1
.2 P
erfo
rms a
com
preh
ensiv
e m
edic
ines
ass
essm
ent t
o ob
tain
info
rmat
ion
to u
nder
stan
d th
e pe
rson
’s cl
inica
l nee
ds a
nd co
ntex
t
1.2.
1 Co
nduc
ts a
n as
sess
men
t tha
t is
appr
opria
te to
bot
h th
e he
alth
pr
ofes
siona
l’s sc
ope
of p
ract
ice a
nd
the
pers
on’s
clini
cal c
onte
xt
M
aste
rs
4 +
2
1.2.
2 Re
view
s and
inte
rpre
ts
info
rmat
ion
in th
e pe
rson
’s he
alth
re
cord
s
M
aste
rs
4 +
2
Not
es
In
dica
tes a
per
form
ance
crit
erio
n co
nsid
ered
ess
entia
l for
that
mod
el o
f pre
scrib
ing
In
dica
tes a
per
form
ance
crit
erio
n no
t con
sider
ed e
ssen
tial f
or th
at m
odel
of p
resc
ribin
g
# Ac
cord
ing
to re
leva
nt le
gisla
tion.
Not
e ac
cord
ing
to th
e Pr
ecrib
ing
Com
pete
ncie
s Fra
mew
ork,
a p
resc
riptio
n m
ay p
rovi
de a
n or
der t
o ad
min
ister
, rat
her
than
disp
ense
. M
aste
rs
Psyc
holo
gist
s ach
ievi
ng g
ener
al re
gist
ratio
n fo
llow
ing
com
plet
ion
of a
n ac
redi
ted
Mas
ters
deg
ree
4 +
2 Ps
ycho
logi
sts
achi
evin
g ge
nera
l reg
istra
tion
follo
win
g co
mpl
etio
n of
an
accr
edite
d 4
year
sequ
ence
of s
tudy
+ 2
yea
r Psy
BA a
ppro
ved
inte
rnsh
ip

Page
| 1
04
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
1.
2.3
Obt
ains
rele
vant
info
rmat
ion
from
the
pers
on a
bout
thei
r m
edic
ines
, and
thei
r med
ical
and
cl
inic
al h
istor
y, in
cludi
ng th
eir c
o-ex
istin
g co
nditi
ons,
trea
tmen
ts,
alco
hol a
nd su
bsta
nce
use,
alle
rgie
s an
d so
cial
cont
ext
Mas
ters
4
+ 2
1.2.
4 As
sess
es th
e pe
rson
’s ris
k fa
ctor
s for
poo
r adh
eren
ce; f
or
exam
ple
soci
al is
olat
ion,
phy
sical
im
pairm
ent,
cogn
itive
impa
irmen
t or
dist
urba
nce,
low
Eng
lish
prof
icien
cy,
low
hea
lth li
tera
cy, f
inan
cial
di
sadv
anta
ge.
Mas
ters
4
+ 2
1.2.
5 As
cert
ains
that
suffi
cient
in
form
atio
n ha
s bee
n ob
tain
ed a
bout
th
e pe
rson
’s co
-exi
stin
g co
nditi
ons
and
curr
ent t
reat
men
ts to
iden
tify
poss
ible
risk
s and
cont
rain
dica
tions
fo
r tre
atm
ent
M
aste
rs
4 +
2
1.2.
6 Pe
rform
s clin
ical
exa
min
atio
ns
that
are
with
in th
e he
alth
pr
ofes
siona
l’s o
wn
scop
e of
pra
ctice
an
d re
leva
nt to
the
pers
on’s
prob
lem
an
d in
terp
rets
the
findi
ngs o
f the
se
exam
inat
ions
M
aste
rs
4 +
2

Page
| 1
05
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
El
emen
t 1.3
Gen
erat
es a
nd e
xplo
res p
ossib
le d
iagn
oses
1.3.
1 Sy
nthe
sises
info
rmat
ion
from
th
e co
mpr
ehen
sive
asse
ssm
ent a
nd
deve
lops
pro
visio
nal a
nd d
iffer
entia
l di
agno
ses
M
aste
rs
4 +
2
1.3.
2 De
velo
ps a
dia
gnos
tic st
rate
gy
and
perf
orm
s rel
evan
t inv
estig
atio
ns
M
aste
rs
4 +
2
1.3.
3 Ex
plai
ns th
e cli
nica
l iss
ues a
nd
thei
r im
plica
tions
to th
e pe
rson
M
aste
rs
4 +
2
Com
pete
ncy
Area
2 T
reat
men
t opt
ions
: Un
ders
tand
s the
trea
tmen
t opt
ions
and
how
they
supp
ort t
he p
erso
n’s c
linic
al n
eed
Elem
ent 2
.1 C
onsid
ers n
on-p
harm
acol
ogica
l tre
atm
ent o
ptio
ns su
itabl
e fo
r tre
atin
g th
e pe
rson
and
thei
r con
ditio
n
2.1.
1 Re
cogn
ises w
hen
it is
clini
cally
ap
prop
riate
not
to in
terv
ene;
for
exam
ple,
in ca
ses w
here
the
signs
an
d sy
mpt
oms a
re li
kely
to re
solv
e w
ithou
t tre
atm
ent
M
aste
rs
4 +
2
2.1.
2 Re
cogn
ises w
hen
it is
clini
cally
ap
prop
riate
to im
plem
ent n
on-
phar
mac
olog
ical t
reat
men
ts
M
aste
rs
4 +
2

Page
| 1
06
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
El
emen
t 2.2
Iden
tifie
s app
ropr
iate
med
icine
s opt
ions
that
can
be in
corp
orat
ed in
to th
e pe
rson
’s tr
eatm
ent p
lan
2.2.
1 In
tegr
ates
kno
wle
dge
of
phar
mac
olog
y, o
ther
bio
med
ical
sc
ienc
es, c
linica
l med
icine
, and
th
erap
eutic
s and
iden
tifie
s med
icine
s su
itabl
e fo
r tre
atin
g th
e co
nditi
on
✗
Mas
ters
4
+ 2
2.2.
2 O
btai
ns, i
nter
pret
s, an
d ap
plie
s cu
rren
t evi
denc
e an
d in
form
atio
n ab
out m
edici
nes t
o in
form
dec
ision
s ab
out i
ncor
pora
ting
med
icine
s int
o th
e pe
rson
’s tr
eatm
ent p
lan
✗
Mas
ters
4
+ 2
2.2.
3 Id
entif
ies m
edic
ines
opt
ions
th
at a
re li
kely
to p
rovi
de
ther
apeu
tical
ly e
ffect
ive
and
safe
tr
eatm
ent a
nd ta
ilors
them
for t
he
pers
on
✗
Mas
ters
4
+ 2
2.2.
4 Co
nsid
ers t
he co
st a
nd
affo
rdab
ility
of t
he m
edici
nes t
o th
e pe
rson
✗
Mas
ters
4 +
2
2.2.
5 Co
nsid
ers t
he im
plic
atio
ns to
th
e w
ider
com
mun
ity o
f usin
g a
part
icula
r med
icine
to tr
eat t
he
pers
on
✗
M
aste
rs
4 +
2

Page
| 1
07
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
2.
2.6
Disc
usse
s the
trea
tmen
t opt
ions
an
d m
edici
nes w
ith th
e pe
rson
, co
nsid
erin
g: t
he p
riorit
ies f
or
trea
ting
thei
r cur
rent
con
ditio
n an
d co
-exi
stin
g co
nditi
ons;
thei
r rea
dine
ss
to a
ddre
ss th
e cu
rren
t con
ditio
n;
thei
r exp
ecta
tions
of t
reat
men
t
Mas
ters
4
+ 2
2.2.
7 Su
pple
men
ts v
erba
l inf
orm
atio
n w
ith w
ritte
n in
form
atio
n ab
out t
he
cond
ition
and
trea
tmen
t opt
ions
(w
here
app
ropr
iate
)
M
aste
rs
4 +
2
2.2.
8 Al
low
s the
per
son
time
to m
ake
an in
form
ed d
ecisi
on a
bout
thei
r tr
eatm
ent
M
aste
rs
4 +
2
2.2.
9 Re
fers
the
pers
on fo
r fur
ther
as
sess
men
t or t
reat
men
t whe
n th
e su
itabl
e tr
eatm
ent o
ptio
ns a
re
outs
ide
the
heal
th p
rofe
ssio
nal’s
ow
n sc
ope
of p
ract
ice
M
aste
rs
4 +
2
Com
pete
ncy
Area
3 S
hare
d de
cisio
n m
akin
g: W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
to d
evel
op a
nd im
plem
ent a
trea
tmen
t pla
n
Elem
ent 3
.1 N
egot
iate
s the
rape
utic
goal
s with
the
pers
on
3.1.
1 Ne
gotia
tes t
hera
peut
ic go
als
that
enh
ance
the
pers
on’s
self-
man
agem
ent o
f the
ir co
nditi
on
✗
M
aste
rs
4 +
2

Page
| 1
08
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
3.
1.2
Asce
rtai
ns th
at a
ll pa
rtie
s hav
e a
com
mon
und
erst
andi
ng o
f the
th
erap
eutic
goa
ls an
d ho
w th
ey w
ill
be m
anag
ed
Mas
ters
4
+ 2
Elem
ent 3
.2 W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
sele
ct m
edic
ines
and
to ta
ilor a
nd im
plem
ent a
trea
tmen
t pla
n 3.
2.1
Expl
ores
the
pers
on’s
opin
ions
an
d pr
efer
ence
s con
cern
ing
med
icin
es a
nd th
e tr
eatm
ent p
lan
✗
Mas
ters
4
+ 2
3.2.
2 Co
nsul
ts o
ther
hea
lth
prof
essio
nals
abou
t pot
entia
l m
edic
ines
and
the
trea
tmen
t pla
n
Mas
ters
4 +
2
3.2.
3 Re
ache
s agr
eem
ent w
ith th
e pe
rson
abo
ut m
edici
nes t
o be
use
d to
tr
eat t
heir
cond
ition
✗
Mas
ters
4
+ 2
3.2.
4 De
velo
ps th
e tr
eatm
ent p
lan
in
part
ners
hip
with
the
pers
on
✗
M
aste
rs
4 +
2
3.2.
5 O
btai
ns a
ppro
val t
o us
e th
e m
edic
ines
(whe
re re
leva
nt)
✗ ✗
M
aste
rs
4 +
2 3.
2.6
Stop
s or m
odifi
es th
e pe
rson
’s ex
istin
g m
edici
nes a
nd o
ther
m
anag
emen
t str
ateg
ies i
f req
uire
d
M
aste
rs
4 +
2
3.2.
7 En
sure
s the
per
son
unde
rsta
nds
the
trea
tmen
t pla
n an
d ho
w to
use
th
e m
edic
ine
safe
ly a
nd e
ffect
ivel
y
M
aste
rs
4 +
2

Page
| 1
09
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
El
emen
t 3.3
Dev
elop
s a re
view
pla
n ta
ilore
d to
the
pers
on’s
need
s
3.3.
1 Id
entif
ies t
he n
eed
for,
and
deve
lops
a re
view
pla
n
M
aste
rs
4 +
2
Com
pete
ncy
Area
4 C
o-or
dina
tion:
Com
mun
icate
s the
trea
tmen
t pla
n cle
arly
to o
ther
hea
lth p
rofe
ssio
nals
Elem
ent 4
.1 P
rovi
des c
lear
inst
ruct
ions
to o
ther
hea
lth p
rofe
ssio
nals
who
disp
ense
, sup
ply,
or a
dmin
ister
med
icine
s pre
scrib
ed fo
r the
per
son
4.1.
1 Pr
epar
es p
resc
riptio
ns o
r m
edic
atio
n or
ders
that
com
ply
with
re
leva
nt le
gisla
tion,
gui
delin
es o
r co
des o
f pra
ctice
, and
org
anisa
tiona
l po
licie
s and
pro
cedu
res
M
aste
rs
4 +
2
4.1.
2 Pr
ovid
es a
ccur
ate
and
clear
ve
rbal
med
icatio
n or
ders
that
com
ply
with
rele
vant
legi
slatio
n, g
uide
lines
or
code
s of p
ract
ice
and
orga
nisa
tiona
l pol
icies
and
pr
oced
ures
(whe
re re
leva
nt)
✗ #
#
M
aste
rs
4 +
2
Elem
ent 4
.2 P
rovi
des i
nfor
mat
ion
abou
t med
icin
es a
nd th
e tr
eatm
ent p
lan
with
the
pers
on’s
cons
ent t
o ot
her h
ealth
pro
fess
iona
ls w
ho p
rovi
de ca
re to
the
pers
on
4.2.
1 Pr
ovid
es in
form
atio
n fo
r co
llabo
ratio
n to
mem
bers
of i
nter
-pr
ofes
siona
l hea
lthca
re te
ams b
oth
with
in fa
ciliti
es a
nd th
e co
mm
unity
M
aste
rs
4 +
2

Page
| 1
10
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Co
mpe
tenc
y Ar
ea 5
Mon
itors
and
revi
ews:
Mon
itors
and
revi
ews t
he p
erso
n’s r
espo
nse
to tr
eatm
ent
Elem
ent 5
.1 O
btai
ns in
form
atio
n to
ass
ess t
he p
erso
n’s r
espo
nse
to tr
eatm
ent
5.1.
1 O
bser
ves t
he p
erso
n to
as
cert
ain
thei
r res
pons
e to
trea
tmen
t (w
here
rele
vant
)
M
aste
rs
4 +
2
5.1.
2 Di
scus
ses w
ith th
e pe
rson
and
ot
her h
ealth
pro
fess
iona
ls, th
eir:
ex
perie
nce
with
impl
emen
ting
the
trea
tmen
t pla
n
adhe
renc
e, in
cludi
ng a
ny is
sues
ar
ising
and
pos
sible
way
s to
impr
ove
adhe
renc
e
perc
eptio
n or
obs
erva
tion
of th
e m
edic
ines
’ ben
efits
and
adv
erse
ef
fect
s
asse
ssm
ent o
f whe
ther
the
ther
apeu
tic g
oals
have
bee
n ac
hiev
ed
Mas
ters
4
+ 2
5.1.
3 O
btai
ns a
dditi
onal
info
rmat
ion
to a
sses
s whe
ther
the
ther
apeu
tic
goal
s hav
e be
en a
chie
ved
by
exam
inin
g th
e pe
rson
, req
uest
ing
inve
stig
atio
ns, a
nd in
terp
retin
g th
e fin
ding
s (w
here
rele
vant
)
M
aste
rs
4 +
2
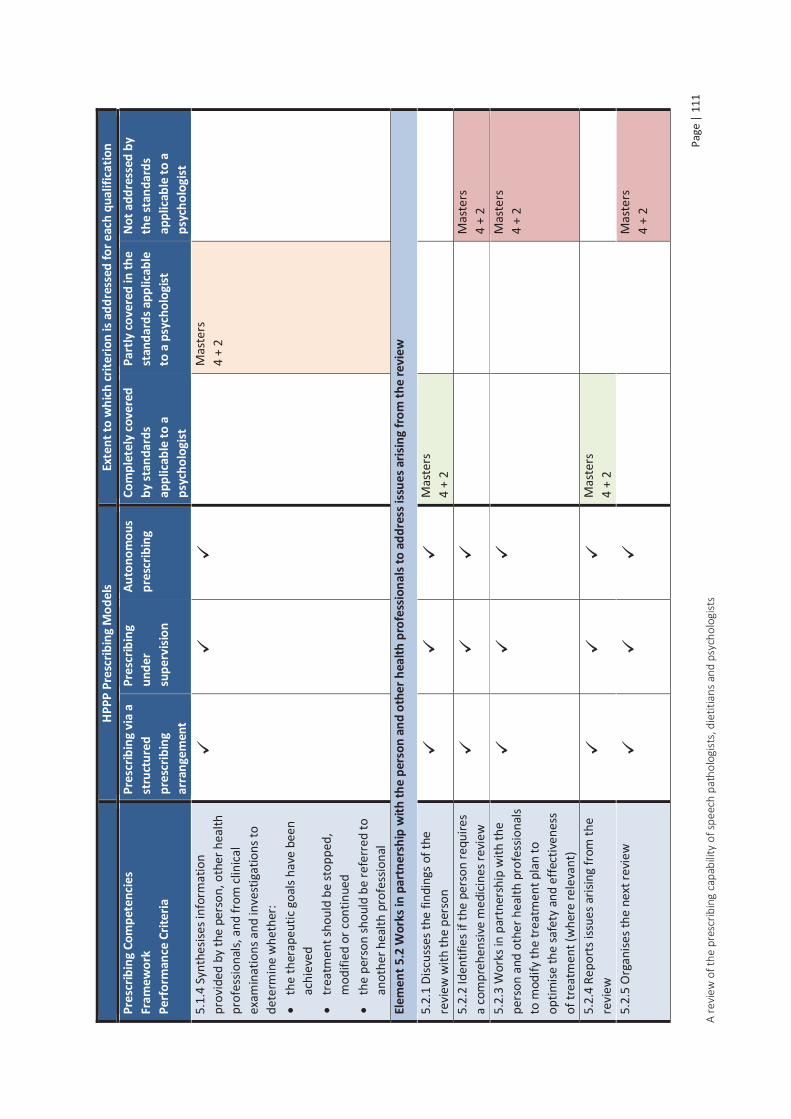
Page
| 1
11
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
5.
1.4
Synt
hesis
es in
form
atio
n pr
ovid
ed b
y th
e pe
rson
, oth
er h
ealth
pr
ofes
siona
ls, a
nd fr
om cl
inica
l ex
amin
atio
ns a
nd in
vest
igat
ions
to
dete
rmin
e w
heth
er:
th
e th
erap
eutic
goa
ls ha
ve b
een
achi
eved
trea
tmen
t sho
uld
be st
oppe
d,
mod
ified
or c
ontin
ued
th
e pe
rson
shou
ld b
e re
ferr
ed to
an
othe
r hea
lth p
rofe
ssio
nal
Mas
ters
4
+ 2
Elem
ent 5
.2 W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
add
ress
issu
es a
risin
g fro
m th
e re
view
5.2.
1 Di
scus
ses t
he fi
ndin
gs o
f the
re
view
with
the
pers
on
M
aste
rs
4 +
2
5.2.
2 Id
entif
ies i
f the
per
son
requ
ires
a co
mpr
ehen
sive
med
icine
s rev
iew
Mas
ters
4
+ 2
5.2.
3 W
orks
in p
artn
ersh
ip w
ith th
e pe
rson
and
oth
er h
ealth
pro
fess
iona
ls to
mod
ify th
e tr
eatm
ent p
lan
to
optim
ise th
e sa
fety
and
effe
ctiv
enes
s of
trea
tmen
t (w
here
rele
vant
)
M
aste
rs
4 +
2
5.2.
4 Re
port
s iss
ues a
risin
g fr
om th
e re
view
Mas
ters
4
+ 2
5.2.
5 O
rgan
ises t
he n
ext r
evie
w
M
aste
rs
4 +
2

Page
| 1
12
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Co
mpe
tenc
y Ar
ea H
1 Pr
ofes
siona
l: Pr
actic
es p
rofe
ssio
nally
Elem
ent H
1.1
Prac
tices
with
in th
e ap
plic
able
legi
slativ
e an
d re
gula
tory
fram
ewor
ks
H1.1
.1 D
emon
stra
tes k
now
ledg
e of
, an
d co
mpl
ies w
ith, l
egisl
atio
n,
regu
latio
ns, a
nd co
mm
on la
w
appl
icabl
e to
pre
scrib
ing
(as f
urth
er
defin
ed b
y th
e kn
owle
dge
subs
ectio
n of
this
com
pete
ncy
area
)
Mas
ters
4
+ 2
H1.1
.2 M
aint
ains
acc
urat
e an
d co
mpl
ete
reco
rds o
f:
the
cons
ulta
tion
cl
inic
al e
xam
inat
ions
and
in
vest
igat
ion
resu
lts
ris
k fa
ctor
s for
med
icine
s m
isadv
entu
re
th
e pe
rson
’s de
cisio
n to
dec
line
trea
tmen
t (w
here
rele
vant
)
chan
ges t
o th
e pe
rson
’s m
edici
nes
man
agem
ent p
lan,
inclu
ding
the
ratio
nale
beh
ind
thes
e ch
ange
s
the
revi
ew p
lan,
re
com
men
datio
ns, a
nd d
ate
for
next
revi
ew
ou
tcom
es o
f tre
atm
ent
Mas
ters
4
+ 2

Page
| 1
13
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
El
emen
t H1.
2 Pr
actic
es a
ccor
ding
to p
rofe
ssio
nal s
tand
ards
, cod
es o
f con
duct
, and
with
in th
e he
alth
pro
fess
iona
l’s o
wn
scop
e of
pra
ctice
H1.2
.1 D
emon
stra
tes k
now
ledg
e of
an
d co
mpl
ianc
e w
ith:
pr
ofes
siona
l sta
ndar
ds
co
des o
f con
duct
scop
e of
pra
ctice
stat
emen
ts o
r gu
idel
ines
M
aste
rs
4 +
2
H1.2
.2 P
ract
ices w
ithin
the
limits
of
the
heal
th p
rofe
ssio
nal’s
ow
n ed
ucat
ion,
trai
ning
and
scop
e of
pr
actic
e
M
aste
rs
4 +
2
H1.2
.3 D
emon
stra
tes r
espe
ct fo
r the
sc
ope
of p
ract
ice o
f oth
er h
ealth
pr
ofes
siona
ls an
d th
eir c
ontr
ibut
ion
with
in a
col
labo
rativ
e ca
re m
odel
, pa
rticu
larly
that
of t
he p
erso
n’s m
ain
heal
thca
re p
rovi
der
M
aste
rs
4 +
2
H1.2
.4 A
ccep
ts re
spon
sibili
ty a
nd is
ac
coun
tabl
e fo
r the
car
e pr
ovid
ed to
th
e pe
rson
M
aste
rs
4 +
2
Elem
ent H
1.3
Prac
tices
with
in th
e ap
plic
able
fram
ewor
ks o
f the
hea
lthca
re se
ttin
g an
d sy
stem
H1.3
.1 D
emon
stra
tes k
now
ledg
e of
an
d co
mpl
ies w
ith n
atio
nal,
stat
e an
d te
rrito
ry, a
nd fa
cility
pol
icies
and
pr
oced
ures
in re
latio
n to
pre
scrib
ing
Mas
ters
4
+ 2

Page
| 1
14
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
H1
.3.2
Dem
onst
rate
s app
ropr
iate
pr
ofes
siona
l jud
gem
ent w
hen
inte
rpre
ting
and
appl
ying
gui
delin
es
and
prot
ocol
s to
the
pers
on’s
situa
tion
M
aste
rs
4 +
2
H1.3
.3 C
ontr
ibut
es to
the
impr
ovem
ent o
f pol
icies
and
pr
oced
ures
for t
he ju
dici
ous,
appr
opria
te, s
afe
and
effe
ctiv
e us
e of
m
edic
ines
✗
Mas
ters
4
+ 2
Elem
ent H
1.4
Prac
tices
qua
lity
use
of m
edici
nes p
rinci
ples
H1.4
.1 A
pplie
s qua
lity
use
of
med
icin
es p
rinci
ples
whe
n pr
escr
ibin
g m
edici
nes
M
aste
rs
4 +
2
H1.4
.2 Id
entif
ies c
omm
on c
ause
s of
med
icin
es e
rror
s and
adv
erse
eve
nts,
and
impl
emen
ts st
rate
gies
to re
duce
th
e ris
ks o
f the
se o
ccur
ring
M
aste
rs
4 +
2
H1.4
.3 D
emon
stra
tes k
now
ledg
e of
th
e m
edic
ines
com
mon
ly p
resc
ribed
Mas
ters
4
+ 2
H1.4
.4 C
ritica
lly e
valu
ates
in
form
atio
n ab
out m
edici
nes a
nd
mak
es e
vide
nce-
base
d de
cisio
ns
abou
t med
icine
s in
the
heal
th
prof
essio
nal’s
ow
n pr
actic
e
✗
M
aste
rs
4 +
2

Page
| 1
15
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
El
emen
t H1.
5 De
mon
stra
tes a
com
mitm
ent t
o co
ntin
ual q
ualit
y im
prov
emen
t of t
he h
ealth
pro
fess
iona
l’s o
wn
pres
crib
ing
H1.5
.1 E
ngag
es in
ong
oing
pr
ofes
siona
l dev
elop
men
t and
ed
ucat
ion
to im
prov
e pr
escr
ibin
g pr
actic
es
Mas
ters
4
+ 2
Elem
ent H
1.6
Addr
esse
s the
pot
entia
l for
bia
s in
pres
crib
ing
deci
sions
H1.6
.1 Im
plem
ents
stra
tegi
es to
ad
dres
s inf
luen
ces t
hat m
ay b
ias
pres
crib
ing
decis
ions
, inc
ludi
ng:
m
arke
ting
influ
ence
s
poss
ible
per
sona
l, pr
ofes
siona
l or
finan
cial g
ain
co
nflic
ts o
f int
eres
t
the
heal
th p
rofe
ssio
nal’s
ow
n be
liefs
, val
ues,
and
expe
rienc
es
✗
M
aste
rs
4 +
2
Com
pete
ncy
Area
H2
Com
mun
icate
s: Co
mm
unic
ates
and
col
labo
rate
s effe
ctiv
ely
with
the
pers
on a
nd o
ther
hea
lth p
rofe
ssio
nals
Elem
ent H
2.1
Obta
ins c
onse
nt to
pro
vide
clin
ical s
ervi
ces t
o th
e pe
rson
H2.1
.1 A
dher
es to
legi
slativ
e an
d w
orkp
lace
requ
irem
ents
for o
btai
ning
an
d re
cord
ing
cons
ent f
or:
ac
cess
ing
heal
th re
cord
s
obta
inin
g in
form
atio
n fr
om, a
nd
prov
idin
g in
form
atio
n to
, oth
er
heal
th p
rofe
ssio
nals
M
aste
rs
4 +
2
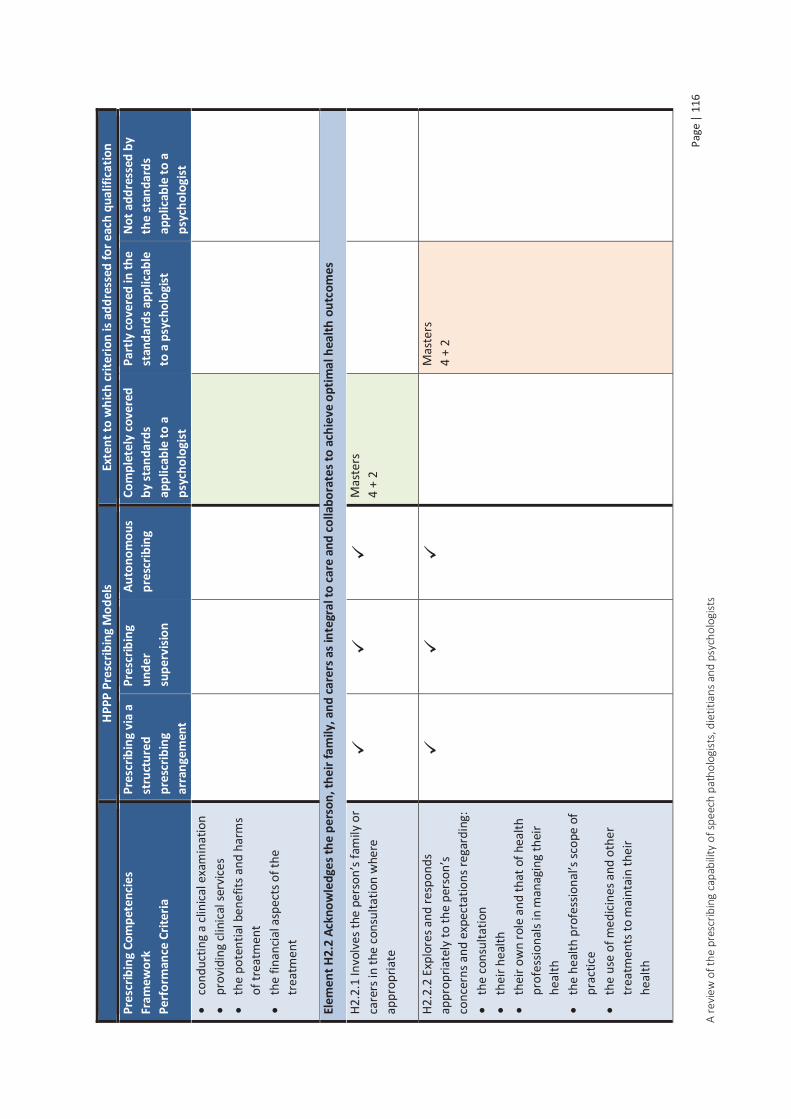
Page
| 1
16
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
cond
uctin
g a
clini
cal e
xam
inat
ion
pr
ovid
ing
clini
cal s
ervi
ces
th
e po
tent
ial b
enef
its a
nd h
arm
s of
trea
tmen
t
the
finan
cial a
spec
ts o
f the
tr
eatm
ent
El
emen
t H2.
2 Ac
know
ledg
es th
e pe
rson
, the
ir fa
mily
, and
care
rs a
s int
egra
l to
care
and
colla
bora
tes t
o ac
hiev
e op
timal
hea
lth o
utco
mes
H2.2
.1 In
volv
es th
e pe
rson
’s fa
mily
or
care
rs in
the
cons
ulta
tion
whe
re
appr
opria
te
M
aste
rs
4 +
2
H2.2
.2 E
xplo
res a
nd re
spon
ds
appr
opria
tely
to th
e pe
rson
’s co
ncer
ns a
nd e
xpec
tatio
ns re
gard
ing:
the
cons
ulta
tion
th
eir h
ealth
thei
r ow
n ro
le a
nd th
at o
f hea
lth
prof
essio
nals
in m
anag
ing
thei
r he
alth
the
heal
th p
rofe
ssio
nal’s
scop
e of
pr
actic
e
the
use
of m
edici
nes a
nd o
ther
tr
eatm
ents
to m
aint
ain
thei
r he
alth
Mas
ters
4
+ 2

Page
| 1
17
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
H2
.2.3
Est
ablis
hes a
ther
apeu
tic
part
ners
hip
that
acc
ords
with
the
pref
eren
ces e
xpre
ssed
by
the
pers
on
M
aste
rs
4 +
2
Elem
ent H
2.3
Resp
ects
the
pers
on
H2.3
.1 R
espe
cts t
he p
erso
n’s v
alue
s, be
liefs
, and
exp
erie
nces
Mas
ters
4
+ 2
H2.3
.2 R
espe
cts t
he p
erso
n’s p
rivac
y an
d co
nfid
entia
lity
M
aste
rs
4 +
2
H2.3
.3 R
espe
cts t
he p
erso
n’s
heal
thca
re d
ecisi
ons
M
aste
rs
4 +
2
Elem
ent H
2.4
Com
mun
icate
s effe
ctiv
ely
with
the
pers
on u
sing
appr
opria
te co
mm
unic
atio
n sk
ills t
o en
able
the
safe
use
of m
edici
nes
H2.4
.1 A
sses
ses t
he p
erso
n’s
pref
erre
d la
ngua
ge, c
omm
unic
atio
n st
yle,
com
mun
icatio
n ca
pabi
litie
s, an
d he
alth
lite
racy
, and
adj
usts
the
heal
th p
rofe
ssio
nal’s
ow
n co
mm
unic
atio
n st
yle
to in
tera
ct
effe
ctiv
ely
with
them
M
aste
rs
4 +
2
H2.4
.2 C
onsid
ers t
he p
oten
tial i
ssue
of
per
ceiv
ed p
ower
diff
eren
ces
betw
een
the
heal
th p
rofe
ssio
nal a
nd
the
pers
on
M
aste
rs
4 +
2
H2.4
.3 P
rovi
des c
lear
and
app
ropr
iate
w
ritte
n an
d ve
rbal
info
rmat
ion
to th
e pe
rson
to e
nabl
e th
em to
mak
e
M
aste
rs
4 +
2

Page
| 1
18
A re
view
of t
he p
resc
ribin
g ca
pabi
lity
of sp
eech
pat
holo
gist
s, d
ietit
ians
and
psy
chol
ogist
s
HP
PP P
resc
ribin
g M
odel
s Ex
tent
to w
hich
crite
rion
is ad
dres
sed
for e
ach
qual
ifica
tion
Pres
crib
ing
Com
pete
ncie
s Fr
amew
ork
Perf
orm
ance
Crit
eria
Pres
crib
ing
via
a st
ruct
ured
pr
escr
ibin
g ar
rang
emen
t
Pres
crib
ing
unde
r su
perv
ision
Auto
nom
ous
pres
crib
ing
Com
plet
ely
cove
red
by st
anda
rds
appl
icab
le to
a
psyc
holo
gist
Part
ly co
vere
d in
the
stan
dard
s app
licab
le
to a
psy
chol
ogist
Not
add
ress
ed b
y th
e st
anda
rds
appl
icab
le to
a
psyc
holo
gist
in
form
ed ch
oice
s and
ach
ieve
opt
imal
he
alth
out
com
es
H2.4
.4 A
scer
tain
s tha
t the
in
form
atio
n pr
ovid
ed h
as b
een
rece
ived
and
und
erst
ood
corr
ectly
M
aste
rs
4 +
2
Elem
ent H
2.5
Colla
bora
tes w
ith o
ther
hea
lth p
rofe
ssio
nals
to a
chie
ve o
ptim
al h
ealth
out
com
es fo
r the
per
son
H2.5
.1 E
ngag
es in
ope
n, in
tera
ctiv
e di
scus
sions
with
oth
er h
ealth
pr
ofes
siona
ls in
volv
ed in
carin
g fo
r th
e pe
rson
M
aste
rs
4 +
2
H2.5
.2 C
onfir
ms t
hat t
heir
own
unde
rsta
ndin
g of
info
rmat
ion
prov
ided
by
othe
r hea
lth
prof
essio
nals
is co
rrec
t
M
aste
rs
4 +
2
H2.5
.3 R
espo
nds a
ppro
pria
tely
to
com
mun
icat
ion
initi
ated
by
othe
r he
alth
pro
fess
iona
ls
M
aste
rs
4 +
2
H2.5
.4 P
rovi
des c
lear
ver
bal a
nd
writ
ten
info
rmat
ion
to o
ther
hea
lth
prof
essio
nals
by se
cure
mea
ns w
hen
impl
emen
ting
new
trea
tmen
ts w
ith
med
icin
es o
r mod
ifyin
g ex
istin
g tr
eatm
ent p
lans
M
aste
rs
4 +
2

Page | 119 A review of the prescribing capability of speech pathologists, dietitians and psychologists
88.3.3 Discussion
The psychology professional and entry level competency standards provide a comprehensive description of the capabilities of an entry level psychologist. Minor adjustments to include reference regarding medicines could improve mapping in areas such as obtaining information from the patient, as well as therapeutic selection and implementation.
It is likely that some of the prescribing activities that do not map well are undertaken in actual practice, but due to their lack of documentation in the standards, are perceived not to map to the Prescribing Competencies Framework. These include the following:
Allows the person time to make an informed decision about their treatment Works in partnership with the person and other health professionals to modify the treatment
plan Organises the next review Ascertains that the information provided has been received and understood correctly Confirms that their own understanding of information provided by other health professionals is
correct Responds appropriately to communication initiated by other health professionals
Areas that do not map well, and are likely to fall outside of the current scope of practice should be targeted for additional education and assessment, these include the following:
Medication and allergy history taking Medication selection competencies
o Identification of safe, appropriate, effective medicine options o Stopping or modifying existing medicines if required o QUM principles o Identification of medicines errors and adverse events
Medication orders Legislative requirements relating to medicines
Mapping of the learning objectives for the representative undergraduate programs of study provided limited information to assess graduate capability with respect to prescribing. The learning objectives are quite broad in their statements and, without review of individual lectures and tutorials, it if impossible to say to what extent they map with the Prescribing Competencies Framework. Mapping at an element level rather than a performance criteria level is also less specific; not all performance criteria within the element may be covered by the learning objectives. This mapping does, however, give an indication of the coverage of the Prescribing Competencies Framework by APAC accredited programs of study.
Some of the elements which could not be identified in the learning objectives are likely to be covered in clinical placements. These include negotiating of therapeutic goals, developing a review plan, assessing response to treatment, addressing issues arising from the review, obtaining consent and acknowledging and collaborating with the person and their family. Others such as providing instruction to other health professionals who dispense, supply, or administer medicines prescribed for the person or practicing quality use of medicines principles are clearly outside of current scope and would require an addition to the curriculum.

Page | 120 A review of the prescribing capability of speech pathologists, dietitians and psychologists
As indicated in table 7, the requisite competencies for safe and effective prescribing differ dependent on the model of prescribing to be used. The number of competencies required to prescribe under supervision or autonomously is greater than those required to prescribe via a structured prescribing arrangement. This information can be used to identify the additional training that would be required to achieve psychology prescribing competence, dependent on the model of prescribing. Table C4, appendix C shows the competencies not met or only partly met by the psychology standards and indicates the additional training required, dependent on the prescribing model. The additional training required for prescribing under a structured prescribing arrangement is as follows:
Medication history taking training, including adherence assessment Interpretation and application of guidelines and protocols appropriate to model of
prescribing QUM principles appropriate to model of prescribing Identification of common errors and potential adverse reactions associated with medicines
to be prescribed Identification of potential problems with existing medicines and cessation or adjustment as
appropriate Legislation, policies and procedures applicable to model of prescribing Writing of medicine orders appropriate to model of prescribing Recording keeping with respect to medicine use Review of medicine therapy Identification of person’s need for comprehensive medicines review Communication with the person regarding medicine choice, safe and effective use of the
medicine and experience with medicine use Consulting other health professionals with respect to medicine choice
To prescribe under supervision or autonomously the following additional training to that described above is required:
Knowledge of pharmacology, clinical medicine and therapeutics Access, interpretation, evaluation and application of medicine information to inform
evidence based decision making Identification of appropriate medicine options for both the condition and the person being
treated Tailoring of medicine to the person’s needs Consideration of cost of medicines to be prescribed Implication to the wider community with respect to prescribing Communication with the person with respect to opinions and preferences regarding
medicines and the treatment plan Communication with respect to medicines options and reaching agreement with the person Ethical issues with respect to prescribing Provision of verbal orders if required appropriate for model of prescribing Obtaining approval for medicine use if required
There are a number of routes by which competency to prescribe could be achieved. The competencies to prescribe via a structured prescribing arrangement could be incorporated into pre-entry programs of study with minimal adjustment. Authority to prescribe under supervision or

Page | 121 A review of the prescribing capability of speech pathologists, dietitians and psychologists
autonomously requires additional training which could be provided in the way of postgraduate training, with appropriate assessment and credentialing to ensure competency. The APS stated in response to the HWA consultation paper on the HPPP, that they had already developed the course content of a post graduate psychotherapy course, indicating their intention to implement a psychology prescribing program of study(47). However, the majority of the competencies are not profession specific, so there is the possibility of the development of a generic allied health prescribing course. This could be provided in combination with workplace supervision and mentoring, to train and subsequently assess psychology prescribers. Over time it may be possible to incorporate all aspects of prescribing into pre-entry programs of study.
In order to progress the introduction of psychologist prescribing of medicines within scope of practice, processes around the accreditation of prescribing training programs and recognition of prescriber status need to be developed.
In December 2013, following the development of the Prescribing Competencies Framework and the HPPP, the Health Profession Accreditation Councils’ Forum released a position statement ‘Development of Prescribing Standards and Accreditation Processes’(30). The position statement acknowledged the Prescribing Competencies Framework as the nationally recognised standard for prescribing, and stated that standards for prescribing education and training programs of study must align to the framework. The document also stated ‘The Forum is working with its Members to ensure efficient and effective accreditation processes are developed at the same time respecting the diversity of approaches of individual accreditation councils to these processes’.
In addition AHPRA has established a Prescribing Working Group whose aim is to ‘develop a governance framework and other resources to support the development and review of national board regulatory policy relating to prescribing of scheduled medicines’(6). This working group provides a useful mechanism to facilitate active collaboration between health professions and the Forum, with a view to consistency of accreditation. The APS have previously stated that whilst a consistent approach to accreditation of prescribing education would be beneficial within professions, it would not be beneficial across professions given the varying complexity of prescription medicines(47). However, APAC is a member body of the Forum leaving it well placed to inform the development of, and subsequently adopt, any accreditation framework that is developed.
Alternatively APAC could independently develop their own accreditation standards. As an ongoing goal the Prescribing Competencies Framework should be embedded in any prescribing accreditation standards developed. This approach is evidenced in the 2015 Nurse Practitioner and Endorsement for Scheduled Medicines for Midwives Accreditation Standards, both of which require a map of subjects against the Prescribing Competencies Framework(31, 32).
8.4 Recommendations
If psychologist prescribing is to occur, consideration needs to be given to the process by which psychologists are recognised as competent to prescribe.
As discussed previously, in Queensland the authority to prescribe is legislated under the Health (Drugs and Poisons) Regulation 1996 (HDPR) therefore, amendments to the regulation would be required to authorise psychologists to prescribe. As a temporary measure, prescribing could occur

Page | 122 A review of the prescribing capability of speech pathologists, dietitians and psychologists
within Queensland under the section 18 approval process, which has been used previously to authorise prescribing trials in pharmacy and physiotherapy.
In addition, if psychology prescribing is to occur at a national level, professional standards should be revised to include prescribing competencies. Amendments to the relevant medicines regulation in each state and territory would also be required.
In order to progress psychology prescribing it is recommended that:
APAC develops or adopts an accreditation framework and uses it to accredit prescribing training programs suitable for psychology prescribing
The PsyBA seeks Australian Health Workforce Ministerial Council approval, under section 14 of the National Law, to enable the Board to endorse the registration of a psychologist for scheduled medicines
The PsyBA approves, under section 35(1)(d) of the National Law, an accredited program of study as providing qualifications for endorsement

Page | 123 A review of the prescribing capability of speech pathologists, dietitians and psychologists
99 References 1. Health Workforce Australia. Health Professionals Prescribing Pathway (HPPP) Project Final
Report. Adelaide: Health Workforce Australia, 2013. 2. NPS: Better choices Better health. Competencies required to prescribe medicines: puting
quality use of medicines into practice. Sydney: National Prescribing Service Limited; 2012. 3. Allied Health Professions’ Office of Queensland. Ministerial Taskforce on health practitioner
expanded scope of practice: final report. Brisbane: Queensland Government; 2014. 4. Health (Drugs and Poisons) Regulation 1996 (2014). 5. Allied Health Professions' Office of Queensland. A framework for allied health professional
prescribing trials within Queensland Health. State of Queensland (Queensland Health); 2014. 6. Prescribing Working Group - Forum of Chairs’ Workforce Reform Committee. Terms of
Reference. Australian Health Practitioner Regulation Agency; 2014. 7. Australian Pharmaceutical Advisory Council. Guiding principles to achieve continuity in
medication management. Canberra: Australian Pharmaceutical Advisory Council; 2005. 8. Poisons Standard July 2015. 9. Nissen L, Kyle G, Stowasser D, Lum E, Jones A, McLean C. Non-Medical Prescribing. An
exploration of likely nature of, and contingencies for, developing a nationally consistent approach to prescribing by non-medical health professionals. 2010.
10. Australian Bureau of Statistics. Australian Demographic Statistics, Dec 2014: Australian Bureau of Statistics; 2014 [cited 20.07.2015]. Available from: http://www.abs.gov.au/ausstats/[email protected]/mf/3101.0.
11. Australian Bureau of Statistics. Main Features, Population Projections, Australia, 2012 (base) to 2101: Australian Bureau of Statistics; 2013 [cited 18.02.2015]. Available from: http://www.abs.gov.au/ausstats/[email protected]/Lookup/3222.0main+features32012%20(base)%20to%202101.
12. Australian Institute of Health and Welfare. Australia’s Health 2014. Canberra: Australian Institute of Health and Welfare; 2014.
13. Australian Bureau of Statistics. Population by Age and Sex, Australia, States and Territories: Australian Bureau of Statistics; 2014 [cited 18.02.2015]. Available from: http://www.abs.gov.au/ausstats/[email protected]/0/1CD2B1952AFC5E7ACA257298000F2E76?OpenDocument.
14. Australian Institute of Health and Welfare. Australia's Health 2012. Canberra: Australian Institute of Health and Welfare; 2012.
15. de Vries T, Henning R, Hogerzeil H, Fresle D. Guide to Good Prescribing: a practice manual. Geneva: World Health Organization Action Programme on Essential Drugs; 1994.
16. Queensland Health. Ocular Therapeutics Protocol - Optometrists Queensland Government; 2010.
17. Optometry Board of Australia. Endorsement for scheduled medicines registration standard. Optometry Board of Australia; 2010.
18. Podiatry Board of Australia. Endorsement for scheduled medicines registration standard. Podiatry Board of Australia; 2010.
19. Physiotherapy Board of Australia. Newsletter Issue 9-August 2014. Endorsements to prescribe scheduled medicines: Allied Health Professionals Registration Authority; 2014 [cited 16.06.2015]. Available from: http://www.physiotherapyboard.gov.au/News/Newsletters/August-2014.aspx.
20. Hale AR, Coombes ID, Stokes J, et al. Perioperative medication management: expanding the role of the preadmission clinic pharmacist in a single centre, randomised controlled trial of collaborative prescribing. BMJ Open. 2013;3:e003027.doi:10.1136/bmjopen-2013-.
21. Hale AH, Gibbs H, Coombes ID, et al. Pharmacist prescribing of venous thromboembolism prophylaxis in a surgical pre-admission clinic. Anaesth Intensive Care. 2014;42(4):519-20.

Page | 124 A review of the prescribing capability of speech pathologists, dietitians and psychologists
22. Allied Health Profession's Office of Queensland. Allied Health Professional Prescribing Training– Scholarship Funding for enrolment at QUT 2014: Queensland Government; 2014 [cited 22.06.2015]. Available from: http://www.australiandoctor.com.au/getmedia/d9c47c4d-88c7-4b7f-86cf-3009167c8063/Allied_health_QUT_prescribing_training.aspx.
23. Nissen L, Patounas M, Martelli J. Australia’s first Allied Health Prescribing Program – exploring participants understanding and confidence in clinical therapy choices for patient management: QUT; 2014 [cited 22.06.2015]. Available from: http://eprints.qut.edu.au/79554/.
24. Speech Pathology Australia. Education and Careers: Speech Pathology Australia; 2014 [cited 10.06.2015]. Available from: http://www.speechpathologyaustralia.org.au/index.php?option=com_content&view=article&id=174&Itemid=863.
25. Australian Government Department of Employment. ANZSCO 2527-12 Australia Speech Pathologist Australian Government Department of Employment; 2014 [cited 10.06.2015]. Available from: http://docs.employment.gov.au/system/files/doc/other/252711speechpathologistaus.pdf.
26. Health Practitioner Regulation National Law Act 2009 (Qld). 27. Speech Pathology Australia. Annual Report 2014. Melbourne: The Speech Pathology
Association of Australia Limited; 2015. 28. Speech Pathology Australia. Competency-based Occupational Standards for Speech
Pathologists. Entry Level. Melbourne: The Speech Pathology Association of Australia Limited; 2011.
29. Speech Pathology Australia. Code of Ethics. Melbourne: The Speech Pathology Association of Australia Limited; 2010.
30. Health Professions Accreditation Councils' Forum. Position Statement: Development of Prescribing Standards and Accreditation Processes: Health Professions Councils; 2013 [cited 15.07.2015]. Available from: http://www.healthprofessionscouncils.org.au/files/afd81a04d2f04a9cd00b4c4ba3481c93f1ffc5d2_original.pdf.
31. Australian Nursing and Midwifery Accreditation Council. Nurse Practitioner Accreditation Standards. Canberra: Australian Nursing and Midwifery Accreditation Council; 2015.
32. Australian Nursing and Midwifery Accreditation Council. Accreditation standards for programs leading to endorsement for scheduled medicines for midwives. Canberra: Australian Nursing and Midwifery Accreditation Council; 2015.
33. Dietitians Association of Australia. Distinction between dietitian and nutritionist Deakin: Dietitians Association of Australia; [cited 11.06.2015]. Available from: http://daa.asn.au/?page_id=1132.
34. Health Workforce Australia. Australia’s Health Workforce Series- Dietitians in Focus. Adelaide: Health Workforce Australia, 2014.
35. Dietitians Association of Australia. 2014 Annual Report. Deakin: Dietitians Association of Australia, 2015.
36. Dietitians Association of Australia. APD Program Deakin: Dietitians Association of Australia; [cited 11.06.2015]. Available from: http://daa.asn.au/for-health-professionals/apd-program/.
37. Medicines (Designated Prescriber—Registered Nurses Practising in Diabetes Health) Regulations 2011.
38. Budge C, Snell H. Registered Nurse Prescribing in Diabetes Care: 2012 Managed National Roll Out-Project Report. Dunedin: Society for the Study of Diabetes; 2013.
39. Dietitans Association of Australia. Role Statement for Accredited Practising Dietitians Practising in the Area of Cystic Fibrosis. 2014.

Page | 125 A review of the prescribing capability of speech pathologists, dietitians and psychologists
40. Dietitians Association of Australia. National Competency Standards for Dietitians in Australia. Dietitians Association of Australia; 2015.
41. Dietitians Association of Australia. Code of Professional Conduct for members with Australian recognised dietetic qualifications, and non-members with APD status. Dietitians Association of Australia; 2013.
42. Dietitians Association of Australia. Statement of Ethical Practice For members with Australian recognised dietetic qualifications, and non-members with APD status Dietitians Association of Australia; 2013.
43. Psychology Board of Australia. Psychology registrant data: March 2015. Melbourne: Psychology Board of Australia; 2015.
44. Australian Government Department of Employment. ANZSCO 2723 Psychologists: Australian Government Department of Employment; 2014 [cited 11.06.2015]. Available from: https://docs.employment.gov.au/node/34189.
45. Australian Psychological Society. About the APS: The Australian Psychological Society Limited; 2015 [cited 18.5.2015]. Available from: http://www.psychology.org.au/about-the-APS/?utm_source=FixedNav&utm_medium=Click&utm_campaign=About%2BUs.
46. Australian Psychological Society. APS Strategic Plan 2012-2014. Flinders Lane: Australian Psychological Society Limited; 2012.
47. Australian Psychological Society. The Australian Psychological Society’s Response to Health Workforce Australia’s Consultation Paper on a Health Professional Prescribing Pathway in Australia. Melbourne: The Australian Psychological Society Limited; 2012.
48. Psychology Board of Australia. Area of practice endorsements registration standard. Psychology Board of Australia; 2011.
49. Australian Psychology Accreditation Council. Second Consultation Draft: Accreditation Standard For Programs Of Study In Psychology: Australian Psychology Accreditation Council; 2014. Available from: http://admin.psychologycouncil.org.au/Assets/Files/APAC_Accreditation_Standard_for_Programs_of_Study_in_Psychology_2nd_Consultation_Draft_27_May_2014.pdf.
50. Victorian Government Department of Health. National practice standards for the mental health workforce 2013. Melbourne: Victorian Government Department of Health; 2013.
51. Psychology Board of Australia. Guidelines for 4+2 internship programs for provisional psychologists and supervisors. Melbourne: Psychology Board of Australia; 2013.
52. Psychology Board of Australia. National psychology examination curriculum. Melbourne: Psychology Board of Australia; 2012.