a senior management course for health managers in kenya unit 1.5: role of regional integration in...
TRANSCRIPT

A Senior Management Course for Health Managers in Kenya
Unit 1.5: Role of Regional Integration in Health System
Management
2ND EDITION July 2014
Purpose
•This unit helps participants to understand the importance of regional and international partnerships, health laws and declarations to Kenyan health system
By the end of this unit, the participants should be able to:
•Describe the role of aid effectiveness and other international declarations to health system management
•Explain the importance of regional integration and partnerships in health systems management
Objectives
3

This unit will cover the following topics:
•Aid effectiveness and other international declarations
•Role of regional integration in health systems management.
Overview
4
International Laws and Declarations in Health

Activity 1.3.5.1 Group work (40 minutes)
Work in groups to outline main challenges with application of health laws at national and county
levels – 20 minutes.
a) Select one specific law or regulation;
b) Describe the challenges of its application at national or county levels.
Present in plenary for 20 minutes
Copy to TLA 1.3.4

Public Health Law
• Concerns legal powers and duties of the State to assure the conditions for people to be healthy (e.g., to identify, prevent, and ameliorate risks to health in the population).
• Gives limitations on the power of the State to constrain the autonomy, privacy, liberty, proprietary, or other legally protected interests of individuals for the protection or promotion of community health.
7
Examples of International Public Health Laws
1. The WHO Framework Convention on Tobacco Control (WHO FCTC);
2. Trade-Related Aspects of Intellectual Property Rights (TRIPS);
3. World Trade Organization's (WTO) Agreement on TRIPS;
4. International Health Regulations;
5. The 2006 Maputo Plan of Action (commitment to the provision of reproductive health), the Roll Back Malaria Campaign. 8

1. The WHO Framework Convention on Tobacco Control (WHO FCTC)
•1st treaty negotiated under the auspices of the WHO.
•Reaffirms the right of all people to the highest standard of health.
•Asserts the importance of demand reduction strategies as well as supply issues.
•The WHO FCTC was developed in response to the globalisation of the tobacco epidemic.
9

TRIPS (Cont’d)
•Paragraph 6 of the Declaration on the TRIPs Agreement and Public Health allows countries to export patented medicines to third world countries with no manufacturing capacity in the pharmaceutical sector, by making use of compulsory licences;
•Ensures provision of cheap medicines to poor people, transfer of technology and regional cooperation.
10

2. Trade-Related Aspects of Intellectual Property Rights (TRIPS)
• Balances between providing incentives for future inventions/creation and allowing people to use existing inventions and creations;
• The agreement covers a wide range of subjects:
— copyright and trademarks;
— integrated circuit designs and trade secrets;
— patents for pharmaceuticals and other products are only part of the agreement.
11

3. The International Health Regulations (IHR)
•Adopted by the 22nd World Health Assembly on 25th July 1991;
•It represents a revised and consolidated version of the previous International Sanitary Regulations.
12

Purpose of International Health Regulations
•Ensure the maximum security against the international spread of diseases with minimum interference with world traffic;
•Strengthen the use of epidemiological principles as applied internationally, to detect, reduce or eliminate the sources from which infection spreads;
•Improve sanitation in and around ports and airports;
•Prevent the spread of vectors.
13

Declarations and Commitments: Aid Effectiveness- Paris Declaration of 2005
•‘Aid effectiveness’ refers to the efficacy of official development assistance (ODA) in achieving economic development in recipient nations.
•The member states reaffirmed their commitments to increase efforts in harmonisation, alignment and managing aid for results with a set of monitorable actions and indicators.
14

Declarations and Commitments: Aid Effectiveness- Paris Declaration of 2005 (Cont’d)
The key elements are:
• Ownership - Developing countries set their own strategies for poverty reduction, improve their institutions and tackle corruption;
• Alignment - Donor countries align behind these objectives and use local systems;
• Harmonisation - Donor countries coordinate, simplify procedures and share information to avoid duplication.15
Declarations and Commitments: Aid Effectiveness- Paris Declaration of 2005 (Cont’d)
•Results - Developing countries and donors shift focus to development results and results get measured.
•Mutual Accountability - Donors and partners are accountable for development results.
16
Declarations and Commitments: Primary Health Care
•The ICPHCHSA meeting in Ouagadougou, April 2008, reaffirmed the principles of the Declaration of Alma-Ata of September 1978, particularly in regard to:
—Health as a fundamental human right and the responsibility that governments have for the health of their people;
—Need for accelerated action by African governments, partners and communities to improve health;
17
Declarations and Commitments: Primary Health Care (Cont’d)
• The importance of the involvement, participation and empowerment of communities in health development;
• Recognition of the importance of a concerted partnership with civil society, private sector and development partners.
18

Declarations and Commitments: Health MDGS
•The 2001 Abuja Declaration (commitment to allocation of 15% of the national budget to health care).
•MDGs were endorsed by UN member countries to set out targets to be reached by 2015. The following relate to health:
– MDG 4: Reduce child mortality;
– MDG 5: Improve maternal health;
– MDG 6: Combat HIV/AIDS, malaria and other diseases.
19

Declarations and Commitments: Infectious Diseases
•Leaders of G8 countries, in 2000 meeting in Okinawa, Japan, committed to the need to mobilise resources for Aids, Malaria, TB and other infectious diseases.
•African leaders at a summit held in Abuja, Nigeria in April 2001, committed to fighting these diseases by increasing budget allocation to health to 15% of the national budget .
•Global fund was created in 2001 to provide a new channel for resources mobilised.
20

REGIONAL INTERGRATION AND PARTNERSHIPS

Agreements among geographically proximate countries to reduce/remove tariff and non-tariff barriers to free flow of:
• goods;
• services;
• factors of production.
What is regional integration?
22

•Integration helps overcome fragmentation;
•Creates larger markets to permit economies of scale, wider competition and increased foreign investment;
•Accelerates opening of economies to the rest of the world;
•Enhances credibility of health sector reforms through lock-in policy mechanisms;
•Strengthens unity for international negotiations;
•Reduces/resolves inter-state conflicts.
Why regional integration?
23

•An intergovernmental organisation comprising five countries in East Africa: Burundi, Kenya, Rwanda, Tanzania and Uganda;
•Was founded in 1967, collapsed in 1977, and revived on 7th July 2000;
•Is an integral part of the African Economic Community;
•Treaty establishing the EAC that relates to regional integration in the health sector was signed in 1999 and became operational on 7th July 2000;
•Articles 108 and 118 of the Treaty, mandates the Community to, among other tasks, coordinate the prevention and control of human and animal trans-boundary diseases (TBDs).
The East African Community (EAC)
24

•The health sub-sector is under the Social Sector.
•The goal of EAC Regional Plan of Action for the Prevention and Control of Human and Animal TBDs, 2007 - 2012 is:
–safeguard human and animal health;
–protect the socio - economic welfare of the East African people.
•A multi-sectoral regional technical team of experts coordinates the emergency preparedness and response to emerging and re-emerging human and animal TBDs in the region.
Areas of Co-operation in the Health Sub-Sector
25
1. The East Africa Community Health Systems, Research and Policy Unit;
2. The Disease Prevention and Control Unit, under the overall coordination of the Animal and Human Health Desks of the EAC Secretariat;
3. East Africa Regional integrated e-Health management information system.
Regional Coordination Mechanisms
26

•Spearheads regional integration in the area of:
–Health systems development and strengthening;
–Health research;
–Policy formulation and practice among the EAC member states.
•Coordinates and lobbies the EAC member states to invest in human resources in the provision of safe, quality, affordable and efficient health care services.
1. The East Africa Community Health Systems, Research and Policy Unit
27

Addresses the following key strategic interventions: •Establishing EAC regional information exchange system for communicable and non-communicable diseases;•Establishing a supranational regional reference public health laboratory and strengthening national public health laboratories;•Strengthening promotive, preventive, curative and rehabilitative health services for non-communicable diseases;•Strengthening the capacity of partner states to diagnose and treat non-communicable diseases.
2. The Disease Prevention and Control Unit
28

•Components of the Regional Integrated Network:
–e-Health Management Information System (e-HMIS);
–geographical information system (GIS); and
–accompanying ICT infrastructure for e-Health and telemedicine practice.
•Aims to enhance the quality of health data to facilitate timely flow and sharing of information to improve the health of the entire East African population.
3. Regional Integrated e-Health Management Information System
29
Keep processes simple
Drivers of satisfaction in EACs:•Improved timeliness•Going extra mile•Fairness•Knowledgeable staff
Collaboration – across channels and departments
Protect privacy & security of information
Centre of excellence institutions
Increase education & awareness
Deliver better services than private sector
Improve access-common freedoms in FTA
Offer more online, but don’t eliminate choice
Identify critical issues, challenges & way forward
“The bigger, the better” concept. What works?
Health Services Expectations from the EAC
30
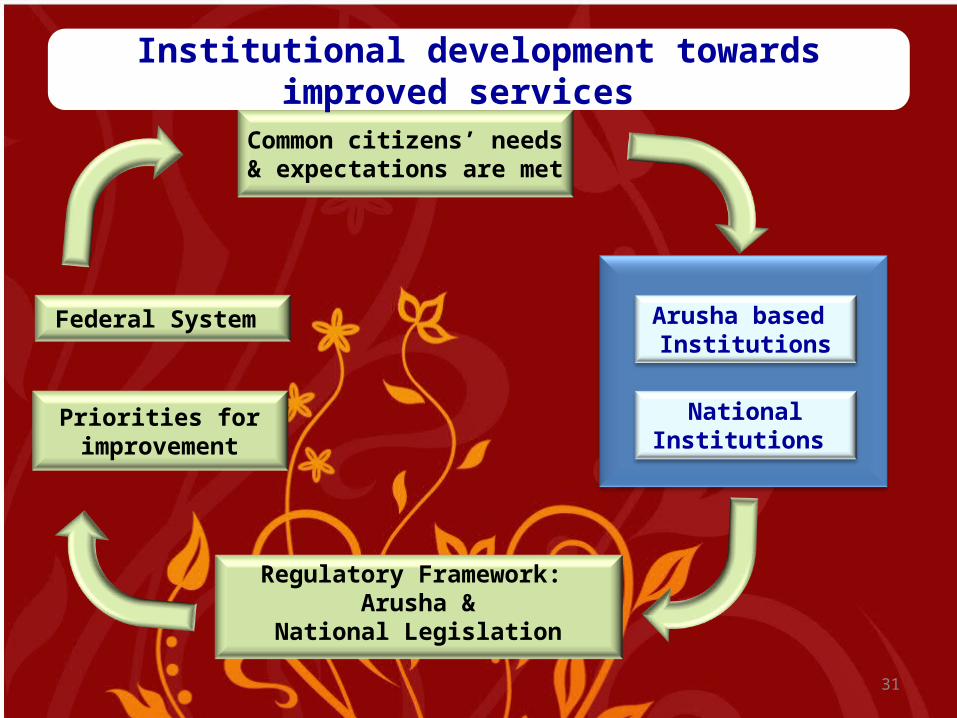
Common citizens’ needs & expectations
are met
Federal System Arusha based Institutions
National Institutions
Regulatory Framework: Arusha &
National Legislation
Priorities for improvement
Institutional development towards improved services
31
