a. service specifications service anticipatory care ...€¦ · the anticipatory care ces aims to...
TRANSCRIPT

1
SCHEDULE 2 – THE SERVICES
A. Service Specifications
Service Specification No.
Service Anticipatory Care Community Enhanced Service
(Incorporating End Of Life Care)
Commissioner Lead
Provider Lead
Period 1st April 2019 – 31st March 2020
Date of Review March 2020
1. Background
The Anticipatory Care CES aims to embed high quality care planning as an essential element of providing proactive and integrated care to patients who might otherwise be at risk of admission. It also supports effective care planning for end-of-life patients and those in care homes. Care planning is led by GP practices but may be undertaken in conjunction with multi-disciplinary teams working at a network or cluster level. Having reviewed the successes and limitations of previous years’ specifications, the service specification now focuses on the following areas:
A. Achieving and maintaining good quality care planning and addressing the needs of patients highlighted by other services as requiring a new or improved care plan.
B. Delivering a 20% reduction in Non-Elective Admissions for a targeted cohort of patients who have had three or more admissions in the previous year.
C. Care planning for new care home patients
D. Effective care planning for End of Life patients
2. Outcomes
2.1 NHS Outcomes Framework Domains & Indicators
Nationally, the NHS requires CCGs to commission services which will contribute to the
achievement of the objectives of the NHS Outcomes framework. Below it can be demonstrated that this CES scheme aims to tackle all five domains of the outcome framework.
Domain 1 Preventing people from dying prematurely
Domain 2 Enhancing quality of life for people with long-term conditions
Domain 3 Helping people to recover from episodes of ill-health or

2
following injury
Domain 4 Ensuring people have a positive experience of care
Domain 5 Treating and caring for people in safe environment and protecting them from avoidable harm
2.2 Local Outcomes
Anticipatory Care
This service aims:
To embed good practice in the creation and maintenance of care plans for all patients who could benefit from such a plan, thereby avoiding unnecessary non-elective admissions.
To deliver a 20% reduction in non-elective admissions amongst patients who have had three or more non-elective admissions in the previous 12 months.
To avoid unnecessary admissions amongst patients in care homes.
To underpin the further development of multidisciplinary integrated care teams as part of the emerging primary care networks as well as the use of IPA and other population health management tools to identify patients for whom care planning may be appropriate.
This service supports the delivery of the system operating plan and aligns with local ICS priorities.
End of Life
The service aims to support delivery of care in accordance with the Gold Standards Framework, a model to proactively manage palliative care in primary care settings. It is built around regular multidisciplinary meetings that identify and address the needs of palliative care patients and their carers.
3. Details of service
A. Achieving and maintaining good quality care planning and addressing the needs of patients highlighted by other services as requiring a new or improved care plan.
A.1 Service description/pathway
Practices providing the CES will be expected to routinely identify patients needing care plans. Before developing a care plan they should ensure that the patient is asked for consent to share their information with other healthcare providers (BHFT, Westcall, RBH, SCAS etc). Care plans may be developed by the practice themselves or through a multidisciplinary integrated care team working at a network or cluster level. Where such a team is developing and updating care plans, practices should be actively involved in this process including through GPs and other healthcare professionals attending or dialling into meetings.
Care plans should be stored on the practice’s clinical system and uploaded to Adastra. They should be updated on an ongoing basis and at least every 6 months by the practice itself or

3
through the multidisciplinary integrated care team. Multidisciplinary care teams may also support the identification of patients for care planning through local intelligence and use of the IPA and other population health management tools (which may also be used by individual practices if they wish to do so). Whilst the number of patients appropriate for care planning will vary depending on demographics, data from this year and previous year’s CESs will be used to benchmark typical levels of care planning. Number of care plans and any variations in that will be discussed at locality meetings.
Practices should ensure that carers (including care home staff)/relatives are involved in the care planning process and that documents are shared as appropriate.
The following supporting documents and videos will be available at the following link:
http://www.members.berkshirewestccg.nhs.uk/index.php/corporate/berkswest-primary-care/ces-service-specs
Anonymised example of a good and a bad care plan
***2016-17 Care Planning Training Slide Pack***
Making the best use of Care Plans, WestCall, Adastra and the URL
Advanced Care Planning - Rapid Response and Treatment Team (RRAT)
Practices will be expected to review their care plans against the guidance in order to achieve good care planning for patients. To further support identification of the most appropriate patients and quality care planning, practices will be expected to review the following further information on a quarterly basis:
Review the care plan of patients highlighted by SCAS and Westcall as requiring practice attention (lack of a care plan, poor quality etc.) This information will be provided to practices on an ongoing basis where such patients are identified.
Review the care plans of patients flagged by SCAS as frequent callers. These will be patients who have:
o Called 999 10+ times each quarter and/or o Called 111 20+ times each quarter
Data regarding this will be provided to practices directly each quarter by SCAS.
Review the care plans of patients flagged by Westcall as frequent callers (typically 20+ calls). This information will be provided to practices on an ongoing basis where patients are identified.
Review on a quarterly basis any patients highlighted by the locality urgent care GP leads following the review of pseudonymised information provided by Westcall on the presence and quality of care plans for recently deceased patients. Practices should compile any lessons learnt that will support any improvement in the quality of care plans going forward and share those with colleagues from other practices at a Locality Council meeting for discussion and benchmarking.
B. Delivering a 20% reduction in Non-Elective Admissions for a targeted cohort of patients who have had three or more admissions in the previous year.

4
B.1 Service description/Pathway
Practices will be provided with a list of patients who have had three or more Non-Elective
admissions between 1st April 2018 to 31st March 2019. GPs and appropriate clinical staff
(including members of the wider integrated multidisciplinary care team where appropriate)
should perform a review of each patient on the list provided and review each admission to see
if interventions or support in the community could have prevented the admission and whether
having these interventions in place could prevent future admission. Where care plans are
already in place these will need to be reviewed and updated as required. If a care plan is not in
place and if appropriate, i.e the patient has a condition/s that means they are at risk of further
admissions it is expected that one should be developed.
The review should be discussed with the patient and carer/relative and advice offered on services that are available to support them and any appropriate actions identified and agreed should be taken forward by the practice staff and recorded on the care plan. The new or updated care plan should be uploaded to Adastra as above.
The practice or the multidisciplinary integrated care team should monitor the patient through the year and keep a record of any changes that may happen to the patient and their circumstances, including noting any admissions, and whether these were also potentially avoidable. The care plan should be updated when any meaningful changes occur.
Where this part of the specification is delivered through an integrated multidisciplinary care team, practices should be actively involved including through GPs and other healthcare professionals attending or dialling into meetings.
From the above cohort those patients who would be eligible to receive flu immunisations in the winter period of 2019-20 this should be offered immunisation in the early part of the flu season, subject to vaccine availability.
C. To avoid unnecessary admissions amongst patients in care homes.
C.1 Service description/Pathway
New Care Home Residents should have face to face care planning with a member of the practice clinical team completed within 8 weeks of arrival. The plan should be developed and updated in accordance with the above guidance on quality care planning and should be uploaded to Adastra.
Practices are encouraged to have a nominated clinician at the practice to provide care to the care home residents. Practices are also expected to work with CCG Care Home Pharmacists to implement recommended changes to medications.
GPs may wish to consider working collaboratively with other practices to provide this service, where there are multiple practices covering one care home.

5
A copy of the care plan is to be shared with the care home and, where appropriate, with the patient’s family.
Care Home staff will be provided with a direct access number through to the practice should they need to speak to a member of the practice team urgently.
The practice will ensure that care home patients receive flu immunisation (unless declined by
patient) offer this in the early part of the flu season 2019-20, subject to vaccine availability. The
responsibly for administering the flu immunisation to Care Home/Nursing Home
patients/residents remains with the GP practice. A practice member should also have a
discussion with the resident/carer/relative around consent for them to have prophylaxis in the
event of a flu outbreak at the home. If consent is given, this should be documented in the
resident’s care plan. GP Practices might want to link with process put in place by Public Health.
For the purposes of this CES, when referring to Care Home Residents, this encompasses Residential Care Homes, Nursing Homes, Hospice Care, Care-led establishments where patients are residing, that is not their family home eg. Learning Disability Homes. This excludes residents of Ravenswood in Wokingham whose care is supported with another CES.
D. End of Life – To ensure effective care planning for End of Life patients
D.1 Service description/care pathway
Under this CES Practices should:
D.1.1 Learning and training
Be committed to continued development relevant to patients covered using practice-based learning including after death reviews and reviews of significant events.
Ensure clinicians have continuing medical experience, training and competence as necessary to enable then to deliver the service.
Ensure attendance by at least one GP from each practice at an annual training session for End of Life, and evidence of cascading learning from this training to others in the practice.
D.1.2 EOL palliative care register
Identify all patents, including those in residential and nursing homes, approaching end of life, and place them on their palliative care register, with confirmation that the appropriate GSF steps have been taken, or will be at appropriate times. The number of patients on the register is expected to be 1% of the practice list size.
Patients’ details held on the palliative care register will be reviewed regularly and will update the Adastra template where necessary. Diagnosis should be separately identified on the register
D.1.3 Care Plans

6
Prepare a plan of care for these identified patients, building on any care plan previously in place. This plan should include (if appropriate):
o Details of their named doctor and key worker o Resuscitation status o Medical records updated o Preferred place of Care/ Death identified and recorded o Details of symptoms and problems regular assessed, recorded and discussed o Clear actions to be taken
Transfer information to the Out-of-Hours team via Westcall using the EoL Adastra template. It is expected that when Respect forms become more readily used and available electronically they will be the form of choice for both care planning and end of life decisions however until that time the current electronic care plan and DNR forms will continue to be used and uploaded to Adastra.
Identify and support carers as appropriate during the patient’s illness and notify relevant professionals of patient death within one working day.
D.1.4 Reviews
Conduct 2 reviews of all patients placed on the palliative care register:
o Review 1 to include the care of those patients who have died to identify ways of further improving care (review to include patients who have died in the period but were not placed on the register).
o Review 2 to look at the learning from review 1 and ensure that actions have been taken and best practice is embedded.
o Multi-disciplinary reviews will be held monthly where possible.
D.1.5 Death of a patient
Demonstrate evidence that carers have been contacted following the death of a patient on the register if practicable and relevant, and have been given the opportunity to comment on the care received.
Demonstrate evidence that future practice has been amended where appropriate as a result, or that comments have been passed to the appropriate agency.
D.2 Complaints Deal with any complaint received from patients about the service as per their internal complaints policy. All complaints relating to the service to be reported to the CCG and to include a copy of the response letter sent to the complainant.
Applicable Service Standards
Applicable Service Standards
http://www.nice.org.uk/
GSF http://www.goldstandardsframework.org.uk/
Population Covered
This service covers all patients under the care of GPs in Berkshire West CCG.
7
Eligibility
To be eligible to provide this CES, the practice must be providing a full range of core GMS services in accordance with established practice in Berkshire West CCG.
To sign up to this CES practices are required to complete and return Annex A by 19th April 2019.
Interdependence with other services/providers
Where possible, the practice must ensure that it works in partnership with other local health and social care providers to provide the best possible service and outcomes for patients. The service is intended to support the further development of integrated multidisciplinary care teams working at a network or cluster level and many elements of the service may be delivered through these teams with appropriate engagement by the GP practice.
5. Audit Requirements
Audit requirements are linked to payment and are set out below.
8
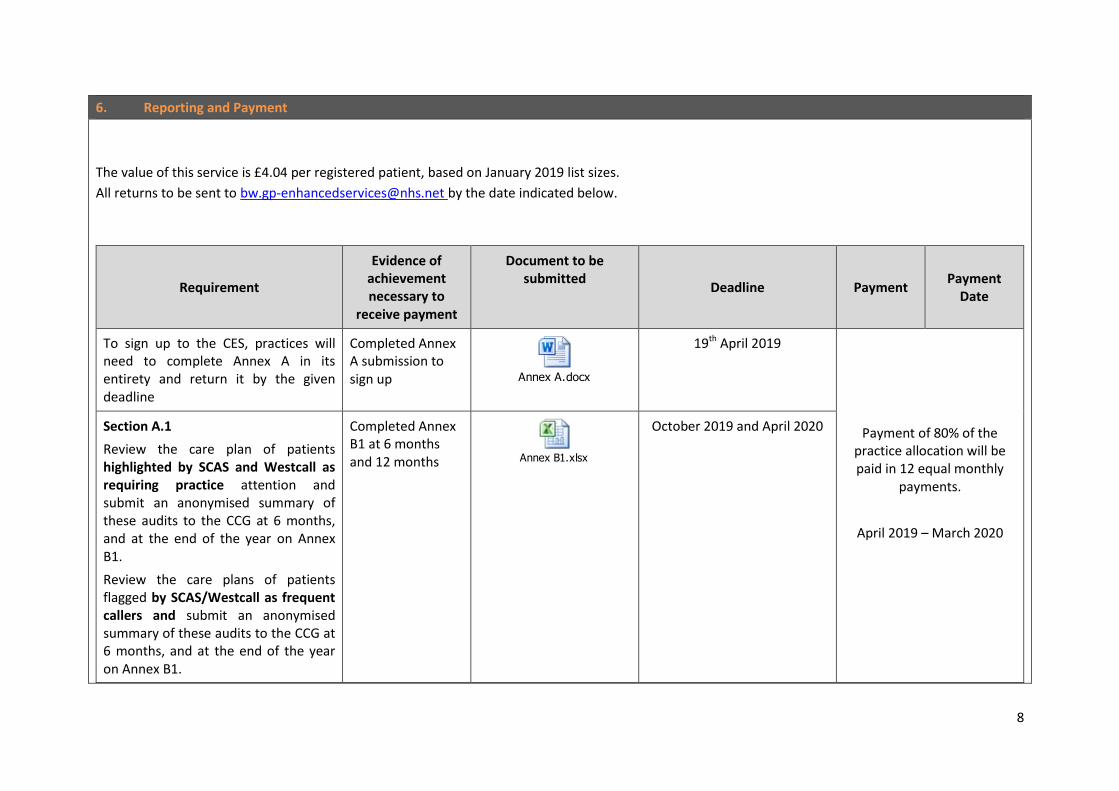
6. Reporting and Payment
The value of this service is £4.04 per registered patient, based on January 2019 list sizes.
All returns to be sent to [email protected] by the date indicated below.
Requirement
Evidence of achievement necessary to
receive payment
Document to be submitted
Deadline Payment Payment
Date
To sign up to the CES, practices will need to complete Annex A in its entirety and return it by the given deadline
Completed Annex A submission to sign up Annex A.docx
19th April 2019
Payment of 80% of the practice allocation will be paid in 12 equal monthly
payments.
April 2019 – March 2020
Section A.1
Review the care plan of patients highlighted by SCAS and Westcall as requiring practice attention and submit an anonymised summary of these audits to the CCG at 6 months, and at the end of the year on Annex B1.
Review the care plans of patients flagged by SCAS/Westcall as frequent callers and submit an anonymised summary of these audits to the CCG at 6 months, and at the end of the year on Annex B1.
Completed Annex B1 at 6 months and 12 months Annex B1.xlsx
October 2019 and April 2020

9
Review on a quarterly basis any patients highlighted by the locality urgent care GP leads and submit an anonymised summary of these audits to the CCG at 6 months, and at the end of the year on Annex B1.
NB - The number of care plans will be checked against the patients list and discussed at locality meetings. It is anticipated that the number of care plans at any practice would be typically around 2% of the practice’s population.
Section A.1
Audit of Care Plans of deceased patients
Practices will compile any lessons learnt that will support any improvement in the quality of care plans going forward and share those with colleagues from other practices at a Locality Council meeting for discussion and benchmarking.
Minutes of the locality meetings to tick that each practice has fulfilled this part of the requirements for the CES. Minutes of the meeting to go to Primary Care for learning.
Minutes of the locality meetings to tick that each practice has fulfilled this part of the requirements for the CES. Minutes of the meeting to go to Primary Care
October 2019 and April 2020

10
Section B.1
NEL monitoring
Practices will be provided with a list of patients who have had three or more Non-Elective admissions between 1st April 2018 to 31st March 2019. The practices will submit details of these reviews on Annex B in October 2019 and April 2020.
Completed Annex B submission
Annex B.xlsx
By 24th April 2020
Section C.1
Completion of the EOL annual audit
Practices are required to complete and return an annual audit as part of the claim for payment.
The audit return will be reviewed by the Palliative Care Lead for Berkshire West. The review will cover the processes for identification of palliative care patients, their needs assessment and the care provided as well as review of changes implemented as a result of significant event reviews after death, particularly of patients who did not achieve their preferred place of care at time of death.
NB - No payment will be made if
Completed Annex C submission
Annex C.docx

11
annual training has not been completed by the nominated GP, or other agreed Healthcare Professional and cascaded within the practice.
Section B.1
Reduction in practice NEL admissions which leads to an overall CCG reduction in NEL admissions for specific cohort of patients.
NEL admission data provided by CSU
During Q1 2020-21 the CCG will review the number of admissions for these patients from 1st April 2019 to 31st March 2020 against the previous year’s data. For localities that show a 20% total reduction in Non-Elective Admissions for their patient cohort there will be a further achievement payment. It is anticipated that 10% of this will be achieved through natural ‘churn’ with the remaining 10% being delivered as a result of the interventions described in this service. Practices who do not engage with the required returns process for this CES will not receive the locality achievement payment.
June 2020 20% of the budget
June 2020
Section D
Provide monthly details of all new Care Home patients between 1st April 2019 – 31st March 2020 including evidence that face to face planning has occurred.
Completed Annex D submission
Annex D.docx
Monthly completion £100 per new care
home patient
Monthly on receipt of Annex D

12
To ensure that the quality of care planning is being maintained the CCG Primary Care Team will co-ordinate randomized PPV, to assess practice care plans.
The CCG Primary Care Team will seek assurance from practices regarding activity around addressing patients highlighted through 999/111/Westcall as requiring practice attention.
Should a practice not provide the requested returns and audits, the CCG will look to reclaim funds paid to the practice; the practice will also not qualify to receive the 20% end of year payment. Significant variance from local benchmarked care plan numbers will also be investigated further with the practice concerned with the potential to make a financial adjustment should care planning activity be much lower than expected.