a study on vande mataram scheme in ahmedabad district
TRANSCRIPT

A study
on
Vande Mataram Scheme
in
Ahmedabad District
By
Indian Association of Preventive & Social Medicine
(Gujarat Chapter)
With Support of
Commisionerate of Health
(Health, Medical Services & Medical Education)

ACKNOWLEDGEMENT
Before starting this study is teamwork, and contributed by numerous people at one
or another point of time. Inputs from each are very important and vital however
more little it may be.
We would first of all like to acknowledge Dr. Dhananjay Bhatt, Additional
Director, Family Welfare, Gujarat State for inviting the organising and providing
an opportunity to observe and study one of the important health activities of the
Government.
We are also grateful to all people of 30 clusters, beneficiaries of the Vande
Mataram Scheme and registered Vande Mataram Doctors for sparing their valuable
time and providing information to our investigators.
We also extend our gratitude of thanks to Dr. Desai, Chief District Health Officer,
Ahmedabad and his office staffs for making the baseline information on the
scheme available to us.
We also thank interns doctors, B. J. Medical College, Ahmedabad for
enthusiastically participate in the study and collecting information without
tiredness.
We thank all staff member of Community Medicine Department, B.J.Medical
College, Ahmedabad who have provided the base and extended support at every
juncture of study.
Finally, we extend our feeling of gratitude to all members of the team who have
worked hard on the behalf of the organization to make it reality to put this report in
your hand.
Dr. B. S. Bhavsar, President Dr. K. N. Sonaliya, Secretary
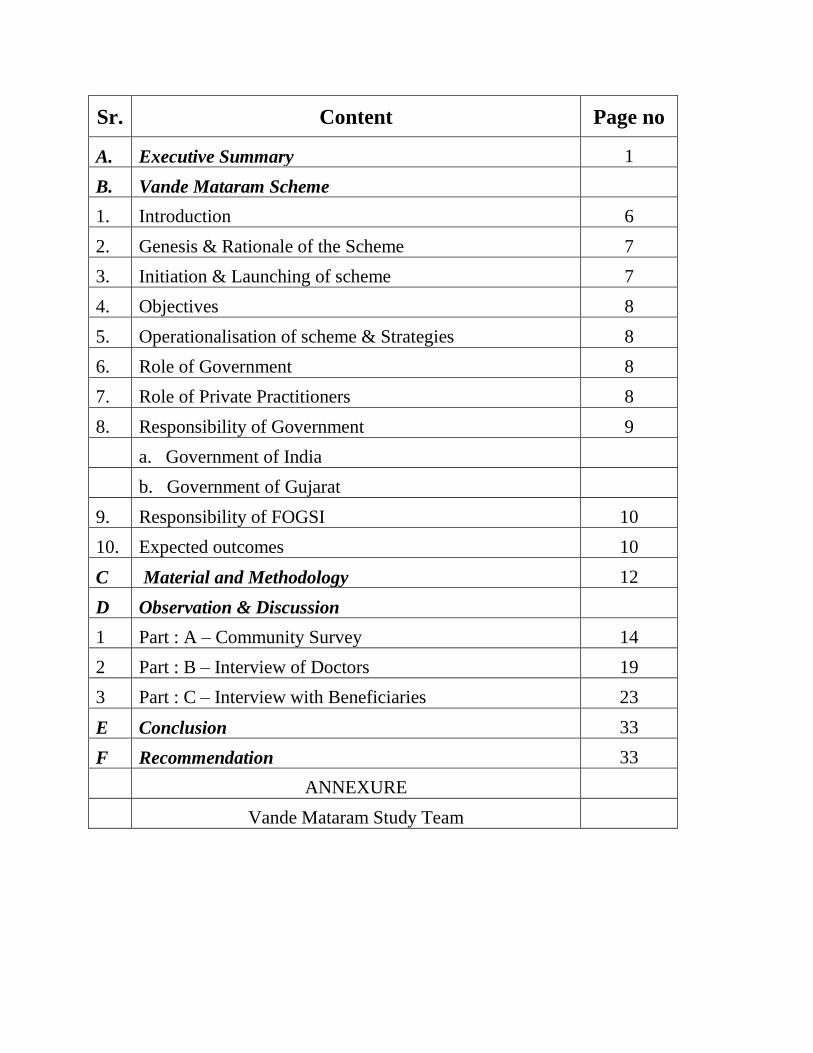
Sr. Content Page no
A. Executive Summary 1
B. Vande Mataram Scheme
1. Introduction 6
2. Genesis & Rationale of the Scheme 7
3. Initiation & Launching of scheme 7
4. Objectives 8
5. Operationalisation of scheme & Strategies 8
6. Role of Government 8
7. Role of Private Practitioners 8
8. Responsibility of Government 9
a. Government of India
b. Government of Gujarat
9. Responsibility of FOGSI 10
10. Expected outcomes 10
C Material and Methodology 12
D Observation & Discussion
1 Part : A – Community Survey 14
2 Part : B – Interview of Doctors 19
3 Part : C – Interview with Beneficiaries 23
E Conclusion 33
F Recommendation 33
ANNEXURE
Vande Mataram Study Team

1
Introduction
Vande Mataram “a programme dedicated” to mothers was launched on 9th February 2004 with
the objective to improve the access of safe motherhood services and to reduce the maternal
and neonatal deaths significantly. To fulfill these objectives, Obstetricians and Gynecologists of
public and private facilities and NGOs are included. This programme was started with the
objectives to bring the change in health seeking behavior utilizing resources/trained workforce
available in private sector, improving the acceptance and access to family planning methods,
detection and management of RTI/STI cases in pregnant women, improving institutional delivery
and strengthen public private partnership.
The Vande Mataram Scheme envisages…..
a. Provision of free OPD services including ante natal check up to all pregnant women and
b. Family planning counseling to new mothers on the 9th of every month
………by private obstetricians and gynecologists
Thus, aims to reduce maternal deaths significantly. In addition, the public facilities of
Government will also observe 9th of every month as Vande Mataram Day and render special
priority to expectant mothers in public sector, Government facilities. The scheme, which is a step
towards public-private and civil society partnership, will be a voluntary scheme under the
auspicious of the FOGSI, eventually such gynecologists / Lady doctors who are not members of
FOGSI will also be able to participate
Material and Methods :-
The study was conducted in Ahmedabad district (city area + Rural area ) in December 2004 in
two phases and three parts.
Phase I :-
A : Community Survey
30 cluster sampling technique (Ward / PHC is cluste unit taken)
Probable / prospective beneficiaries women (360) and women of reproductive age
group (600) were interviewed.
Phase II :-
B : Vande Mataram Doctor’s Interview
30 doctors were randomly selected (33% of total registration) and interviewed.
C : Beneficiary’s interview :
90 beneficiaries (10% of cumulative beneficiaries) randomly selected and interviewed.
Executive Summary
2
Analysis : -
Data was entered in Microsoft Access and analysis was done in SPSS.
Salient observations :
Total 960 women (360 pregnant / postnatal and 600 non pregnant women) of
reproductive age group were studied out of 30 clusters. 71 % of the women were
from 21 – 30 years age group.
Only 3.2 % were aware about the Vande Mataram Scheme.
Health workers were the source of information in most of the cases.
6.67 % was the utilization rate of Vande Mataram scheme.
Most of the beneficiaries had undergone ante-natal check-ups.
Almost 90 % underwent urine, Hemoglobin, B.P. examination and taken T.T and
IFA tablets.
Out of 60 postnatal women 16.67 % underwent postnatal check-ups.
Note : Out of total women who were aware about scheme 93 % and 100% who had
utilisized were reported from the one cluster in community survey.
A. Community Survey
3
Average service utilization is 5.1 beneficiaries per doctor for last 11 months (i.e. since
inception of the scheme.
Monthly average of service utilization is 0.47 beneficiaries /per doctor i.e.around one
patient per two months.
93 % of the doctors believes the scheme is not adequately utilized by the
66.6% doctors have received “Vande Matamram LOGO Board’ and all of them have
displayed it.
Most of the doctors (>80%) were satisfied with the regularity and adequacy of the supply
of ANC cards and IFA tablets and FP devices.
60 % doctors felt that the scheme is good.
70 % of the doctors were of the opinion that more awareness should be generated to
improve the scheme.
Among the registered beneficiaries almost half were in 25-29 years of age group.
99 % of the beneficiaries were housewives.
71 % of the beneficiaries were educated upto or beyond higher secondary level.
66.66% of the beneficiaries belonged to Class II or class III socio economical status.
Doctors were the source of information for the 90 % of the beneficiaries.
39 % of the beneficiaries were primi-gravida.
Almost 92 % of the beneficiaries availed the antenatal services of the scheme rest has
utilized for Family Planning consultation.
All of them were given the ANC card by doctor but only 10 % of the beneficiaries
showed the card to the card to the investigators at the time of visit.
32.7% had expressed satisfaction with the service while Majority 66.7% found the
programme to be O.K i.e. average.
All the beneficiaries were willing to motivate other females to avail the services
82 % of the beneficiaries wanted that their delivery should be conducted at private
hospital.
Part B: Doctor’s Interview :
Part C: Beneficiary’s Interview
4
Discussion and derivations : -
1. It was perceived as a good scheme by both, provider i.e. volunteered doctors and
beneficiaries and adequately support in terms of the supply from the government
sector, very poor awareness and utilization rate of the scheme was noted.
2. For gross inadequate utilization two key reasons can be traced.
a. Lack of awareness about existence of the scheme.
b. Not practicing the key principle of the scheme by Vande Mataram
Doctor i.e. free consultation for Antenatal care and family planning
services to all the eligible mothers on 9th of each month in their private
practice.
3. More than 80% of doctors has expressed satisfaction about regularity and
adequacy of the supply. Regularity shows the better fulfillment of the responsibility
by the Government but adequacy should be viewed under the light of low
utilisation of the services.

5
Recommendations:
1. It is required to reimbibe the key concept of providing free of cost consultation and
family planning services to all eligible mothers coming on 9th of the months, In the
registered doctors by health officials, since it has got tremendous implications on
success. For that regular meetings with private practitioners should be carried out by
them.
2. FOGSI is the key organisation in institution of this scheme, their interest, involvement,
and active participation should be revived to strengthen the Private sector’s
contribution.
3. Lack of awareness is the presently first and foremost bottleneck observed in the
implementation of the programme and which needs to be taken up vigorously.
4. As it was envisages under the scheme that District collector should give
advertisements on every 9th of month in local newspapers highlighting the features
and name of the doctors registered under. This operational guidelines was also
seems to be not in practice and need to be initiated and make it regular.
5. As it was suggested in the operational guidelines, practice of regular review at the
end of three months should be reinstituted at State, district level together by both
partners.
* * * * * * * *

6
Introduction :
In any community, mothers and children constitute a “priority group” and are considered as
“special risk group”. From a study carried out jointly by WHO and UNICEF on maternal
mortality, it is estimated that 99 % of maternal deaths occur in developing countries. India is
among those countries, which have very high maternal mortality. High maternal mortality
reflects inadequacy of health care services for mothers.
Maternal Mortality in India is estimated to be 407 in 1998 (SRS-RGI). This is significantly higher
compared to even the countries like Sri Lanka where it is about 60. The tenth Plan target is to bring
it down to less than 200 by the year 2007.
In the world as a whole, the problem of maternal mortality is principally one of applying existing
obstetric knowledge through Antenatal, Intra-natal and post-natal services rather than developing
new skills. Antenatal care is the care of woman during pregnancy. The primary aim of antenatal
care is to achieve at the end of pregnancy a healthy mother and a healthy baby. For achieving
this outcome, Government has introduced several health programmes time and again. Child
Survival and Safe Motherhood programme was started in August 1992. With additional
components this programme was renamed as Reproductive and Child Health programme in
1997.
Thus Maternal mortality in India is unacceptably high and is one of the main concerns of the Deptt.
of Family Welfare. Availability and accessabily to the antenatal, natal and postnatal care to all
mothers is the major approch and key bottneck for reducing the the maternal mortality in India.
Their are multitude of health care providers such as Ministry of Health, Municipality, Private
Sector, NGOs etc. with ill defined roles and poor coordination. A well coordinated effort
involving both public sector and the NGOs can help address a number of crucial issues for
effective functioning of reproductive and child health programme. NGOs can play an important
role in identifying the neediest hidden pockets. National Health Policy 2002 welcomes the
participation of private sector in all areas of health activities whether primary, secondary or
tertiary.
VANDE MATRAMA SCHEME
7
Genesis of Vande Matram Scheme
Currently, the Government health care system have only limited numbers of gynecologists. Against
the 3043 CHCs in the country there are only 780 Obstetricians and Gynecologists for providing
safe motherhood services.
With a view to obviate the problem of lack of Gynecologists, it is proposed to take up the scheme
titled “Vande Matram” for providing free safe motherhood services including immediate post natal
care on a fixed date of every month by all Gynecologist both in public and private facilities including
NGOs.
Federation of Obstetrics and Gynecological Society of India (FOGSI) which has 18,000
Obstetricians and Gynecologists on its roll as its members has responded to the call of Smt.
Sushma Swaraj, then Minister of Health and Family Welfare of India to come forward and render
antenatal/ postnatal service on the 9th of every month free of cost. Thus, the concept of Public
Private Partnership is actualised in the area of Maternal Care.
Rationale of the scheme :
Data on major causes of maternal mortality is available from the SRS of the registrar General of
India. The major causes of maternal mortality are ante and Postpartum hemorrhage, anaemia,
Obstructed labour, hypertensive disorders, post partum sepsis and unsafe abortions and quick
repeated pregnancies. Deaths due to anaemia, obstructed labour, Hypertensive disorders and sepsis
are preventable with provision of adequate antenatal care, referral and timely treatment of
complications of pregnancy. District household survey (1998 – 99) shows that about 33% pregnant
women avail of even a single antenatal check up. Thus the need to find an alternative measure to
provide safe motherhood service to all, pregnant women is sought, through the Vande Mataram
Scheme by involving the private practitioners and making their experties and services accessuble
free of cost to the mothers on a specific identified day of a month.
Initiation of the scheme :
Immediately meetings with local members of FOGSI and also other obstetricians and gynaccologists
from the private and public sector working in your district, and below levels was called.
They were informed about the Vande Mataram Scheme and persuaded to participate in the scheme.
Number of the copies on the detail of scheme were printed and distribute to Doctors, NGOs and
others
In order to ensure that all probable benificiaries do come to know who the volunteer Vande
Mataram doctors are, the District IEC fund was utilized for appropriate insertions/advertisements
highlighting the scheme in local hews papers most popularly read in your district on 9th of February,
2004 i.e. day the scheme come into existence.
Launching of the shceme :
The Vande Mataram Scheme was formally launched on 9th of February, 2004 at Ahmedabad by then
Cetral Health Minisiter and several public functions were also organised at different district head
quarters in the state and thoughout country.

8
Objectives of the scheme:
1. To bring about the change in health seeking behaviour of and for expectant and new mothers
and to creat awareness in the family and community the need for safe motherhood.
2. To involve and utilize the vast resourccs and specialist/trained workforce available in the
private sector and the private sector infrastructure for providing obstetric care on the 9th of
every month.
3. To improve the acceptance and access to family planning methods through improved family
planning counseling during both antenatal and postnatal period.
4. To detect for management of RTI/STI cases in pregnant women.
5. To improve institutional delivery.
6. To reduce the incidence and prevalence of nutritional anaemia in pregnant women.
7. To strengthen public, private and civil society partnership.
Strategy & Operational Guidelines:
The scheme is in the pursuance of public-private and civil society partnership. It is
a voluntary scheme under the auspicious of the FOGSI, eventually such
gynecologists/Lady doctors who are not members of FOGSI will also be able to
participate.
It proposes to involve practicing Obstetricians and Gynecologists from the Government sector, the
private sector including NGOs for providing the free Services at their clinics or by visiting the
nearest CHC/ Public hospital.
The Scheme envisages….
Role of Private Obstetrician & Gynecologist ….
1. Gynecologists /Lady doctors will provide
a). free antenatal/post natal services for pregnant women/new mothers and
b) family planning services to new mothers………
………on the 9 of every month.
2. Refer such women which is requiring treatment for complications if necessary, to pre identified
and designated centres.
Role of Government……
1. Public facilities of Government will also observe 9th of every month as Vande Mataram Day and
render special priority to expectant mothers in public sector, Government facilities.
2. In case some Gynecologists/lady doctors in private sector volunteer, they may be permitted to
visit nearby CHC/FRU/Sub-district hospital for this purpose.

9
Operationalisation of the scheme :
Responsibility of Government :
The Government of India
1 To develop a suitable communication package for creating awareness amongst the people about
the scheme.
3. To give a LOGO BOARD to identified volunteer doctors through district from the fund of the
Department of Family Welfare or any other fund at district disposal.
4. To supply IFA Tablets to Vande Matram doctor for distribution to pregnant Women.
5. To supply Contraceptives including IUD to Vande Matram doctor for free distribution.
6. To provide Vande Mataram enrollment cards to registered doctors so that antenatal cases may
be issued the same.
7. To ensure availability of supplly to the enrolled Vande Mataram doctors through local health
authroity.
8. To recognize the participating gynecologists/Lady doctors by giving a certificate recognizing
their participation and permitting them to display that they are providing free/voluntary
services as part of RCH programme.
Extension of responsibity in future :
9. Government has proposed to extend legal and insurance /indemnity protection to the
participatingng doctors to ensure that they do not face any adverse consequence due to
Consumer Protection Act while delivering the service under scheme.
10. To devlop and implement a scheme whereby compensations/ transaction costs permitted for
family planning procedures like Tubectomy, vasectomy and insertion of IUD currently available
at Govermnent, institutions will be available for Vande Mataram Doctors also.
State Governments
1. State Governments and FOGSI will identify State and District coordinators for this scheme.
2. All hospitals/FRUs in the Government sector will be issued instructions to give priority to Vande
Mataram card holders.
3. District Collectors to give advertisement every month in the local newspapers highlighting the
Scheme and giving the names of newly enrolled Vande Mataram Doctors.
4. Adequate number of iron folic acid tablets will be provided to the hospitals and clinics by the
State/Districts.
5. Contraceptives for free distribution, IUD for birth spacing and sterilization for permanent
methods.
6. To ensure that the supplies are sent to the Vande Mataram Doctors and the Doctor is not made
to waste his time by being asked to come to the Govt. supply points.
10
7. To hold fortnight motivational enrollment meetings in the districts till 8th of April, 2004 so
that maximirn participation can is secured. Thereafter, Chief Medical Officer and district
authority cn cominue to propagate the scheme and enroll more doctors.
8. District Collector to publish periodic small advertisements on 9h of every month in local
newspapers, informing about the newly enrolled doctors to the public and also the main message
of the scheme.
9. To invite local NGOs to locate and motivate private doctors to enroll.
FOGSI
1. The FOGSI will involve all the 167 local societies in each of which they will initially identify at
least two volunteer specialists.
2. Such identified volunteer specialists will provide free services on the 9th of every month to all
antenatal cases.
3. Initially the free service will include only antenatal / post natal examination and counseling/
advice regarding contraceptive, diet, immunization, delivery etc.
4. Complicated cases will be suitably advised regarding further management and institutional
delivery.
Expected Outcome of the scheme :
Public Private and civil society partnership will improve, improvement in acceptance of spacing and
family planning methods leading to reduction in unwanted pregnancy, Reduction of maternal and
nenatal deaths and wide recognition that safe motherhood needs medical care and antenatal
checkup.
Review :
The scheme will be reviewed every three months with objective to further improvement.

11
1. Assessing the awareness of scheme
among the prospective/probable
beneficiaries,
2. Knowing the utilization rate.
3. To find out bottlenecks in the
implementation of the scheme.
4. Satisfaction level among beneficiaries.
Objectives :

12
The study was conducted in the Ahmedabad district (city area + Rural area),
covering a population of 50,00,000. In rural areas, PHC areas where doctors
are registered were included for the study.
Study Period :- The study was carried out in December 2005.
Sampling Methodology :- The study was carried out in two phases.
Part I :- Community Survey (Probable/eligible prospective beneficiaries)
30 cluster sampling was used. Ward / PHC were used as a cluster unit.
Their population were listed and 30 clusters were selected from them.
360 i.e. eligible mothers (pregnant / mother with child of two months
age) and 600 women of reproductive age. The 360 women was calculated
out by considering 50% utilisation rate and 10% allowable error. Total
960 (360 pregnant / postnatal + 600 non-pregnant women) were
interviewed. 32 women (12 pregnant / postnatal women + 20 non-
pregnant) were taken up from each of the cluster. (Annexure : II)
Part II :- Interview of doctors registered under scheme
30% of the total registered i.e. 30 doctors were randomly selected
and interviewed. (Annexure : II)
Part III :- Interview of beneficiaries
Approximately 900 beneficiaries have been registered in Ahmedabad
district since its inception i.e Feb 2004. 10 % (90) of the total registered
beneficiaries were interviewed at their residence. 3 beneficiaries
registered under 30 doctors were selected for the interview. (Annexure :
III)
Materials and Method

13
Study instrument :-
A pre-designed and pre-tested proforma was used. Separate proformas were used for
probable beneficiaries, Doctors and registered beneficiaries.
Analysis : -
Data was entered in Microsoft Access and analysis was done in SPSS.

14
Part A : Community Survey
Total 960 women (360 eligible beneficiaries and 600 non pregnant women of
reproductive age group) were studied from 3697 households of 30 clusters. To
get 360 eligible beneficiaries 4763 women of reproductive age group were
contacted.
Table : 1. Age group of studied women
Sr. Age group No
(n=960)
%
(100%)
1 < 20 112 11.67%
2 21 to 30 684 71.25%
3 31 to 40 137 14.27%
4 > 41 27 2.81%
Majority of them were (71 % ) from 21-30 years age group, while 14.27% were
from 31 to 40 years of age group and 11.67% were below the age of 20 years.
Out of 360 eligible women 300 women were currently in antenatal period while
60 women were in their post natal period. (Table:1)
OBSERVATIONS & FINDINGS

15
Table : 2. Knowledge regarding Vande Mataram Scheme
Knowledge
(n=960)
Yes* NO
No 31 929
% 3.20% 96.80%
Source of information
Health
worker
Neighbor Others
No 29 1 1
% 93.55% 3.23% 3.23%
* Out of total 29 were reported from the one cluster only.
Out of total 960 women studied, 96.80% women had denied the knowledge about the scheme.
Only 3.20% had heard about the Vande Mataram scheme, out of them 93.55% got the
knowledge through Health worker, and rest had got the information through neighbor or other
source. (Table : 2)
When the women who had who had knowledge about the scheme were asked about their
willingness to avail the service, 93.55 % had expressed readiness to utilize/or had utilized
services. 7% woman were not in favor of utilizing the scheme. Since the can afford the services
the had denied to avail the service under the scheme (Table : 3)
16
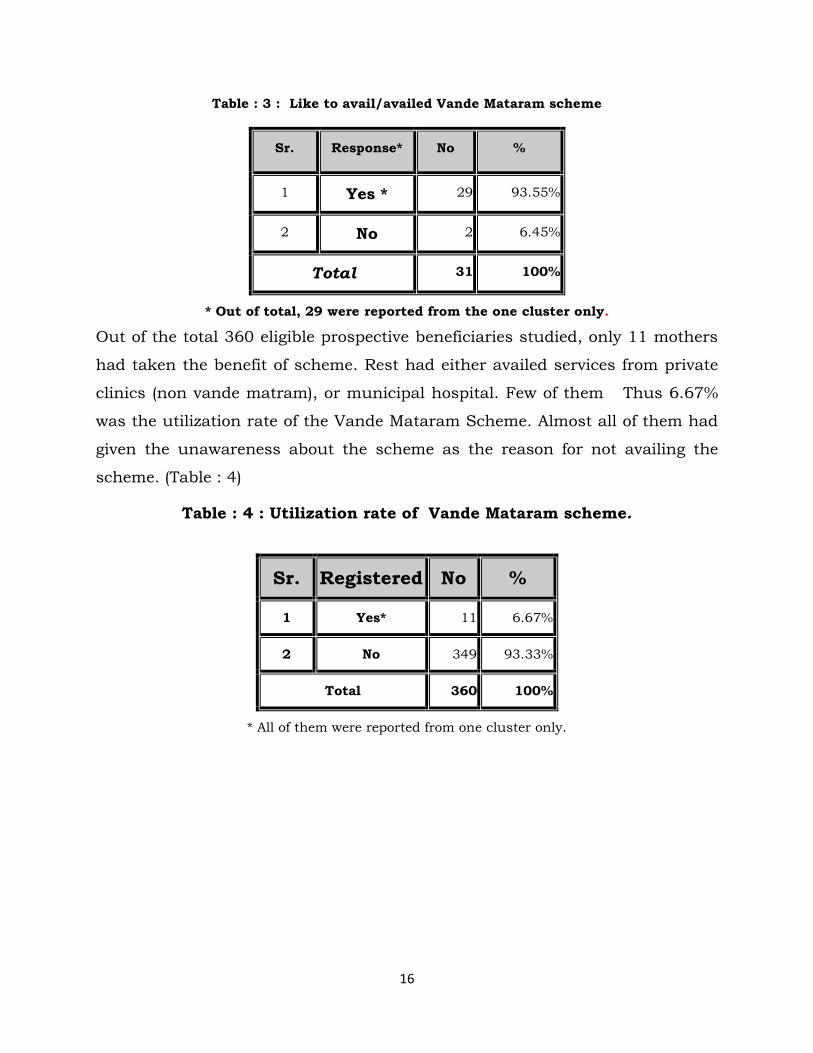
Table : 3 : Like to avail/availed Vande Mataram scheme
Sr. Response* No %
1 Yes * 29 93.55%
2 No 2 6.45%
Total 31 100%
* Out of total, 29 were reported from the one cluster only.
Out of the total 360 eligible prospective beneficiaries studied, only 11 mothers
had taken the benefit of scheme. Rest had either availed services from private
clinics (non vande matram), or municipal hospital. Few of them Thus 6.67%
was the utilization rate of the Vande Mataram Scheme. Almost all of them had
given the unawareness about the scheme as the reason for not availing the
scheme. (Table : 4)
Table : 4 : Utilization rate of Vande Mataram scheme.
Sr. Registered No %
1 Yes* 11 6.67%
2 No 349 93.33%
Total 360 100%
* All of them were reported from one cluster only.
17
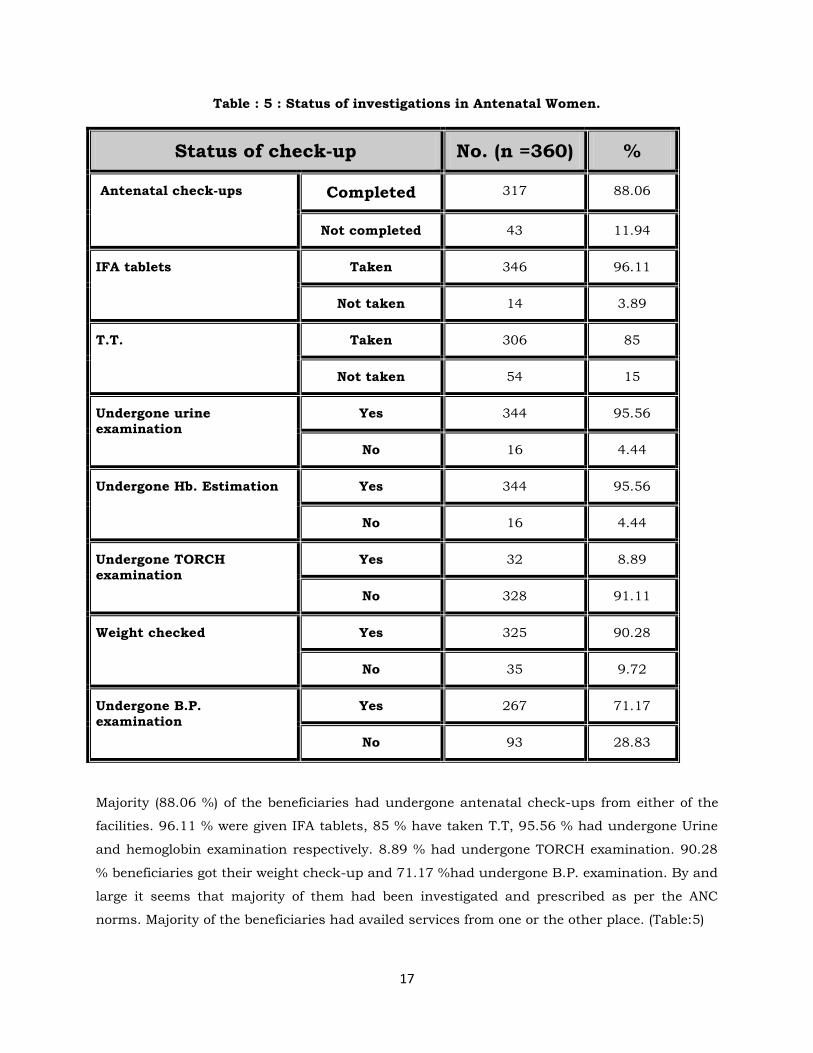
Table : 5 : Status of investigations in Antenatal Women.
Status of check-up No. (n =360) %
Antenatal check-ups Completed 317 88.06
Not completed 43 11.94
IFA tablets Taken 346 96.11
Not taken 14 3.89
T.T. Taken 306 85
Not taken 54 15
Undergone urine
examination
Yes 344 95.56
No 16 4.44
Undergone Hb. Estimation Yes 344 95.56
No 16 4.44
Undergone TORCH
examination
Yes 32 8.89
No 328 91.11
Weight checked Yes 325 90.28
No 35 9.72
Undergone B.P.
examination
Yes 267 71.17
No 93 28.83
Majority (88.06 %) of the beneficiaries had undergone antenatal check-ups from either of the
facilities. 96.11 % were given IFA tablets, 85 % have taken T.T, 95.56 % had undergone Urine
and hemoglobin examination respectively. 8.89 % had undergone TORCH examination. 90.28
% beneficiaries got their weight check-up and 71.17 %had undergone B.P. examination. By and
large it seems that majority of them had been investigated and prescribed as per the ANC
norms. Majority of the beneficiaries had availed services from one or the other place. (Table:5)

18
Table : 6 : Status of check-up in postnatal women.
Undergone Postnatal check-up
No. (n = 60) %
Yes 10 16.67
No 50 83.33
Sixty women were in their postnatal period. Out of the them women only 16.67 % had
undergone postnatal check-ups and a huge portion (83.33 %)of the women had not undergone
postnatal check-ups. This suggests that enough awareness about the importance of antenatal
check is present and good practice is also existing but need and importance of post natal
examination are yet not realized in the community. (Table :6)

19
Part B : Survey of registered doctors.
Total 154 women were registered with the 30 interviewed doctors since the initiation of the
scheme. It comes around total average 5.1 beneficiaries last taken the services per doctor for
last 11 months i.e. since inception of the scheme and one mother is taking the benefit of
scheme in two months per doctor. (Monthly average per doctor is 0.47, i.e. nearly half-patient
per doctor/month). As per the operational guidelines to all antenatal and postnatal mothers
have be provided free of cost consultation on 9th of each month, but based on this figure, it
seems that this practice is not followed at the clinics on designated date of month.
Table : 7 : Doctor’s view on utilization of the Scheme
Utilization No. %
Adequate 2 6.67
Inadequate 28 93.33
Total 30 100
When asked about the their views on utilization of the scheme 93.37% had
agreed about the low utilisation of the scheme, while 7 % of the doctors had
expressed that the scheme is being utilized adequately. (Table :7)
20
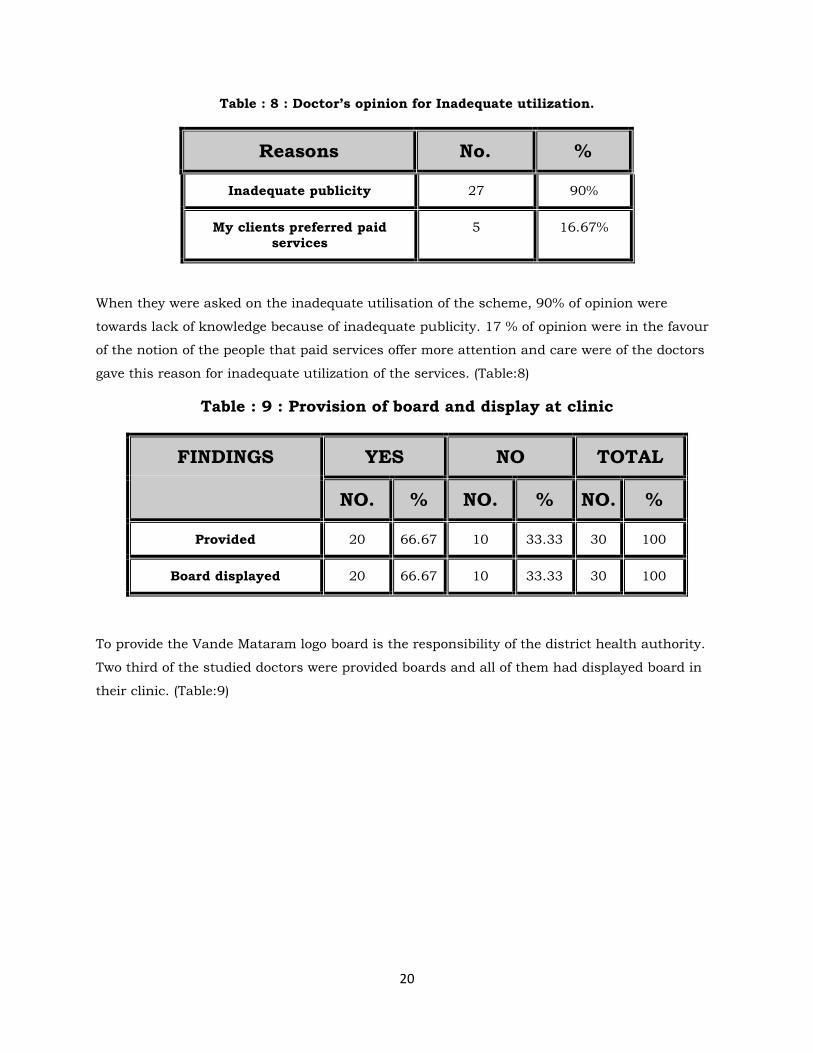
Table : 8 : Doctor’s opinion for Inadequate utilization.
Reasons No. %
Inadequate publicity 27 90%
My clients preferred paid
services
5 16.67%
When they were asked on the inadequate utilisation of the scheme, 90% of opinion were
towards lack of knowledge because of inadequate publicity. 17 % of opinion were in the favour
of the notion of the people that paid services offer more attention and care were of the doctors
gave this reason for inadequate utilization of the services. (Table:8)
Table : 9 : Provision of board and display at clinic
FINDINGS YES NO TOTAL
NO. % NO. % NO. %
Provided 20 66.67 10 33.33 30 100
Board displayed 20 66.67 10 33.33 30 100
To provide the Vande Mataram logo board is the responsibility of the district health authority.
Two third of the studied doctors were provided boards and all of them had displayed board in
their clinic. (Table:9)

21
Table : 10 : Supply of FP devices /ANC card / IFA tablets
Supply REGULAR IRREGULAR TOTAL
NO. % NO. % NO. %
FP devices 28 93.33 2 6.67 30 100
ANC card 24 80 6 20.00 30 100.
IFA tablets 26 86.67 4 13.33 30 100.
As per the operational guidelines district health officials have to provide FP
devises, ANC card and Iron Folic Acid tables in order these can be supplied to
Vande Mataram Beneficiaries free of cost. Most of doctors were satisfied with
regularity and adequacy of supplies of Family Planning Devices, ANC card and
IFA tablets. (Table : 10 & 11)
Table : 11 : FP DEVICES / ANC CARD / IFA TABLETS
Supply ADEQUATE INADEQUATE TOTAL
NO. % NO. % NO. %
FP devices 27 90 3 10 30 100
ANC card 24 80 6 20 30 100
IFA tablets 25 83.33 5 16.67 30 100

22
Majorities of the doctors were of expressed that it is a good scheme but only
35.48 % were feeling that it is not adequately utilized. Only 3.23 % doctors
were having dissatisfaction with the scheme due to poor supply of the logistics.
(Table : 12)
Table : 12 : Experience of Doctors regarding the Scheme .
Experience/opinion* NO. %
Good scheme 19 61.29
Not properly utilized by beneficiaries 11 35.48
Poor supply 1 3.23
Total 30 100.00
* Multiple answers.
Table : 13 : Suggestions by the Doctors to improve the scheme.
Suggestions to improve NO. %
Publicity / awareness 16 69.57%
Supply of logistic 3 13.04%
Regular follow up by government 2 8.70%
Day should be changed 1 4.35%
Involvement of more doctors 1 4.35%
*Multiple answers.
Majority (70 %) of the suggestion were in favour of increasing awareness while
13 % suggestion were towards ensuring adequate supply of logistics to improve
the utilization of the scheme. 8.7% suggestion do asked the greater
involvement of Government and rest suggestions were in foavour of changing
the day and increasing the involvement of doctor. (Table:13)

23
Part C : Interview of registered Beneficiaries.
Three beneficiaries from the list of each selected doctors were chosen randomly. They were
visited and their place and detail interview were taken. All the beneficiaries availed the services
at the private hospital of the registered doctors and all were examined by the specialists.
Table : 14 : Age – Group of the registered beneficiaries.
AGE – GROUP
(IN YEARS)
NO. %
20-24 35 38.9
25-29 50 55.6
30-34 5 5.6
Total 90 100.0
Almost half of the beneficiaries were in 25 – 29 years age-group while around 39 % of the
beneficiaries were in 20-24 years age-group and only 5.6% were 30 or above the 30 years of
their age. (Table : 14)
Table : 15 : Occupation of the registered beneficiaries.
Occupation NO. %
Housewife 89 98.9
Labourer 1 1.1
Total 90 100.0
Most (99 %) of the beneficiaries were housewives. Only 1 % of the beneficiaries were labourers.
Not a single woman was reported professional/employed. (Table : 15)

24
Table : 16 : Literacy Status of the registered beneficiaries.
Literacy Status NO. %
Illiterate 4 4.4
Primary 6 6.7
Secondary 16 17.8
Higher secondary 30 33.3
Graduate 34 37.8
Total 90 100
Majority (71.1 %) of the beneficiaries were educated up to or beyond higher secondary level.
Only 4.4 % beneficiaries were illiterates. Education is related to the utilization of services and
this may be the reason for availing the health service. (Table : 16)
Table : 17 : Literacy Status of the husband of the beneficiaries.
Literacy status No. %
Illiterate 2 2.2
Primary 1 1.1
Higher Secondary 15 16.7
Graduate 62 68.9
Post graduate 4 4.4
Professional 6 6.7
Total 90 100.0
Almost 70 % of the beneficiaries’ husband were graduates. This may be the motivating factor
for their wives for availing the health services. Also, education of husband is linked with
income generation which is anther factor for choosing type of the facility and availing the
services. (Table: 17)

25
Table : 18 : Socioeconomic status of the beneficiaries.
Socioeconomic status No. %
Class I 26 28.90
Class II 48 53.33
Class III 12 13.33
Class IV 4 4.44
Total 90 100.00
Almost half of the beneficiaries belonged to Class II socioeconomic status and 13.33% were
from the belonging to the Class III. These are the middle and lower middle class people.
Together they constitute 66.66% of the total. One third of the beneficiaries belonged to Class I
socioeconomic status. Only 4 % beneficiaries were from Class IV socioeconomic status. These
is the group which was targeted to take maximum benefit of the scheme but found very small
proportion of the beneficiaries. (Table : 18)

26
Table : 19 : Source of information regarding Vande Mataram Scheme
Source of information NO. %
Doctors 80 88.9
Pamphlets – Posters 3 3.3
Beneficiaries 7 7.8
Total 90 100.0
Majority (88.9 % ) of the beneficiaries came to know about the scheme through Doctors. Only
few (7 %) beneficiaries got the information through already registered beneficiaries. Thus
mouth to mouth publicity was noted weak in the spreading the words about the scheme, while
other mass media had non-significant role. (Table : 19)
Table : 20 : Order of pregnancy
Order of pregnancy NO. %
1 35 38.9
2 33 36.7
3 18 20.0
4 4 4.4
Total 90 100.0
39 % of the beneficiaries were primigravida. The reason may be that those females who became
pregnant for the first time may be more conscious regarding their child and were availing the
services provided by the specialists. (Table : 20)

27
Table : 21 : Family size (No of living children) of the beneficiaries.
Family Size NO. %
0 36 40.0
1 32 35.6
2 18 20.0
3 3 3.3
4 1 1.1
Total 90 100.00
Majority (95.6 %) of the beneficiaries had children ranging from nil to two. Only few (1.1 %) of
the beneficiaries had four children. (Table:21)
Table : 22 : Bad obstetric history
Bad obstetric
history
NO. %
Yes Caesarian section 1 1.1
Spontaneous
abortion
1 1.1
No 88 97.8
Total 90 100.0
Only 2 % of the beneficiaries had bad obstetric history. One beneficiary had past history of
spontaneous abortion and one had past history of Caesarian section. (Table : 22)
28
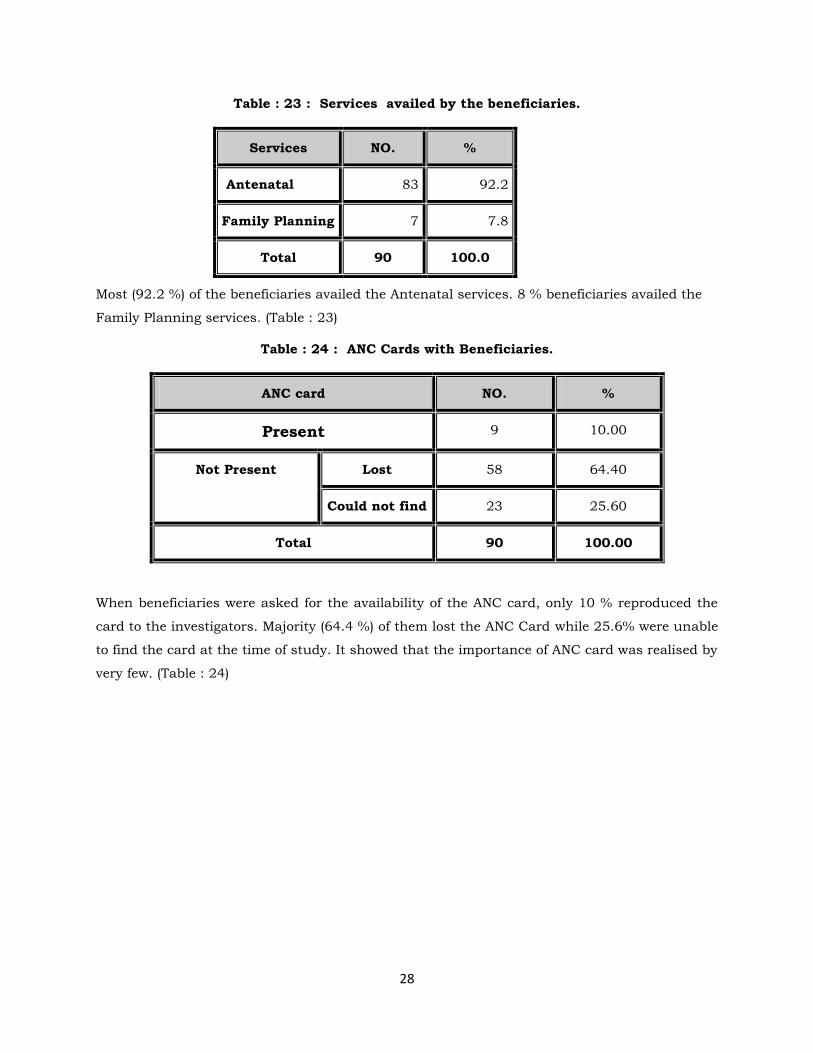
Table : 23 : Services availed by the beneficiaries.
Services NO. %
Antenatal 83 92.2
Family Planning 7 7.8
Total 90 100.0
Most (92.2 %) of the beneficiaries availed the Antenatal services. 8 % beneficiaries availed the
Family Planning services. (Table : 23)
Table : 24 : ANC Cards with Beneficiaries.
ANC card NO. %
Present 9 10.00
Not Present Lost 58 64.40
Could not find 23 25.60
Total 90 100.00
When beneficiaries were asked for the availability of the ANC card, only 10 % reproduced the
card to the investigators. Majority (64.4 %) of them lost the ANC Card while 25.6% were unable
to find the card at the time of study. It showed that the importance of ANC card was realised by
very few. (Table : 24)
29
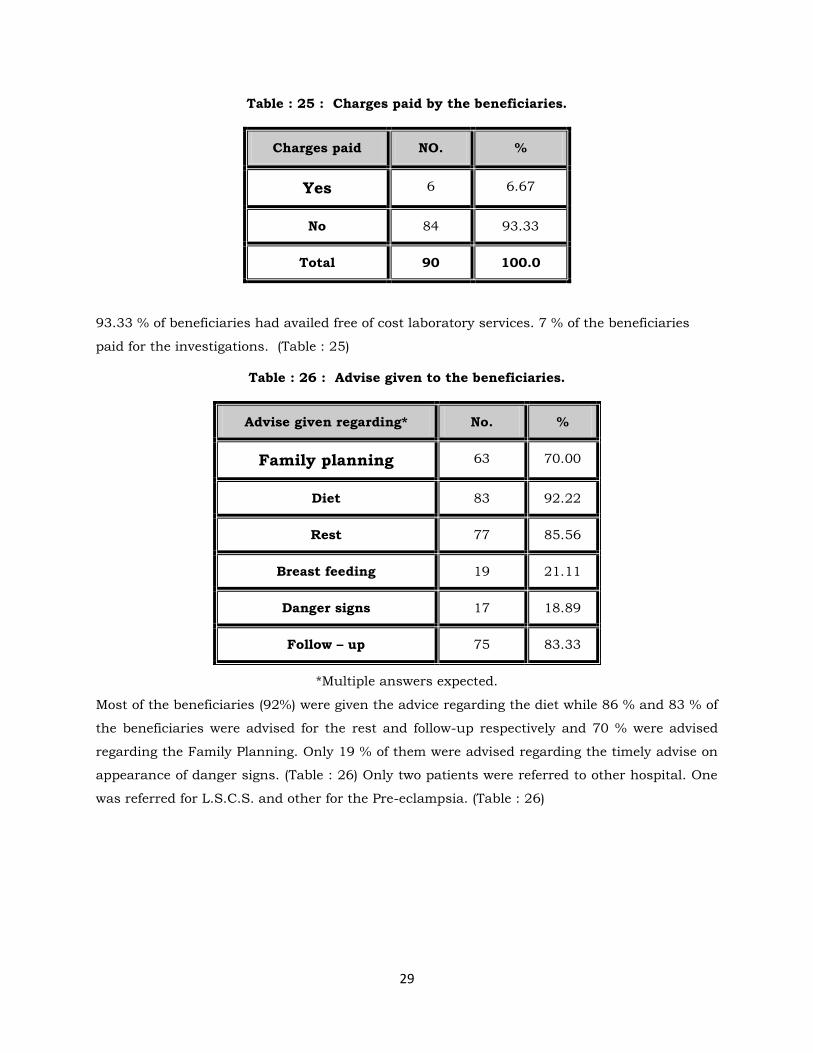
Table : 25 : Charges paid by the beneficiaries.
Charges paid NO. %
Yes 6 6.67
No 84 93.33
Total 90 100.0
93.33 % of beneficiaries had availed free of cost laboratory services. 7 % of the beneficiaries
paid for the investigations. (Table : 25)
Table : 26 : Advise given to the beneficiaries.
Advise given regarding* No. %
Family planning 63 70.00
Diet 83 92.22
Rest 77 85.56
Breast feeding 19 21.11
Danger signs 17 18.89
Follow – up 75 83.33
*Multiple answers expected.
Most of the beneficiaries (92%) were given the advice regarding the diet while 86 % and 83 % of
the beneficiaries were advised for the rest and follow-up respectively and 70 % were advised
regarding the Family Planning. Only 19 % of them were advised regarding the timely advise on
appearance of danger signs. (Table : 26) Only two patients were referred to other hospital. One
was referred for L.S.C.S. and other for the Pre-eclampsia. (Table : 26)

30
Table : 27 : Satisfaction among the beneficiaries
Experience No %
Satisfied* Check-up done nicely
Check-up done by the
specialist
Check-up done free of cost
Check-up done regularly
Advise regarding F.P.
Programme is given
27
26
15
4
8
Total 32.2
Not satisfied 1 1.1
O.K. 60 66.7
Total 90 100.0
*Multiple answers.
Out of the total surveyed beneficiaries one third of the beneficiaries were satisfied with the
programme. Most (66.7 %) of the beneficiaries found the programme to be O.K. i.e. average.
Only 1.1 % were not satisfied with the programme that too because of inconvenient timings to
them. (Table : 27)
Table : 28 : Recommendation to other females to avail the services.
Recommendation NO. %
Yes 89 98.89
No 1 1.11
Total 90 100.0
Almost all of the beneficiaries replied that they will motivate other females to take the benefit of
Vande Mataram Scheme. Surprisingly one beneficiary replied that she will not motivate other
females to avail the services under this scheme. (Table : 28)

31
Table : 29 : Preference for place of delivery.
Place of delivery NO. %
Private Hospital 74 82.22
PHC 8 8.89
Not applicable (postnatal
women)
6 6.67
At home 2 2.22
Total 90 100.0
Majority (82.22 %) of beneficiaries replied that they will give preference to the private hospital
for their delivery while 9 % gave PHC as their preference for the delivery. Surprisingly 2 % of
the beneficiaries were interested in the home delivery. (Table : 29)
Several important suggestions given by beneficiaries to improve the scheme were :-
1. Adequate and appropriate publicity of the programme should be done through print
and press media.
2. There should be involvement of more doctors.
3. The programme should be properly implemented.
4. Adequate and appropriate advice should be given to the patients by the Doctors.
32
A cross-sectional study was carried out in December 2004 to study the Vande Mataram Health
Scheme. The study was carried out in 3 phases. In the first phase the probable / prospective
beneficiaries were interviewed to know the utilization rate of beneficiaries. In second phase
doctors registered in the scheme were interviewed. In the third phase beneficiaries registered in
the scheme were interviewed. Total 960 women (360 pregnant / postnatal and 600 non
pregnant women) of reproductive age group were studied. 71 % of the women were from 21 –
30 years age group. Only 3.2 % were aware about the Vande Mataram Health Scheme. Health
workers were the source of information in most of the cases. 6.67 % was the utilization rate of
Vande Mataram Health scheme. Most of the beneficiaries had undergone ante-natal check-ups.
Almost 90 % underwent urine, Hemoglobin, B.P. examination and taken T.T and IFA tablets.
Out of 60 postnatal women 16.67 % underwent postnatal check-ups.
Average registration of the beneficiaries came out to be 5.1 since last 11 months of the starting
of the scheme. According to 93 % of the doctors, the scheme is not adequately utilized by the
beneficiaries, reason being the inadequate publicity. Board for the awareness of the scheme
was displayed by those doctors who were provided with the board. Majority of the doctors were
satisfied with the regularity and adequacy of the supply of FP devices, ANC cards and IFA
tablets. 60 % doctors felt that the scheme is good. 70 % of the doctors were of the opinion that
more awareness should be generated to improve the scheme.
Among the registered beneficiaries almost half were in 25-29 years of age group. 99 % of
the beneficiaries were housewives. 71 % of the beneficiaries were educated up to or beyond
higher secondary level. Almost 70 % beneficiaries’ husbands were graduates. Doctors were the
source of information for the 90 % of the beneficiaries. 39 % of the beneficiaries were primi-
gravida. 2 % of the beneficiaries were having bad obstetric history. Almost 90 % of the
beneficiaries availed the antenatal services of the scheme. Only 10 % of the beneficiaries
showed the card to the card to the investigators at the time of visit. All the beneficiaries availed
the services at the private hospital of the registered doctors. Majority of the beneficiaries found
the programme to be O.K. All the beneficiaries were willing to motivate other females to avail
the services. 82 % of the beneficiaries wanted that their delivery should be conducted at private
hospital.
SUMMARY

33
As any new programme takes time for fulfilling its objectives, this scheme will also take time for
its effective utilization. According to the survey, the scheme was perceived as a good scheme by
both providers i.e. volunteered doctors and beneficiaries.
1. It is required to reimbibe the key concept of providing free of cost consultation and family
planning services to all eligible mothers coming on 9th of the months, In the registered
doctors by health officials, since it has got tremendous implications on success. For that
regular meetings with private practitioners should be carried out by them.
2. FOGSI is the key organisation in institution of this scheme, their interest, involvement,
and active participation should be revived to strengthen the Private sector’s
contribution.
3. Lack of awareness is the presently first and foremost bottleneck observed in the
implementation of the programme and which needs to be taken up vigorously.
4. As it was envisages under the scheme that District collector should give advertisements
on every 9th of month in local newspapers highlighting the features and name of the
doctors registered under. This operational guideline was also seems to be not in
practice and need to be initiated and make it regular.
5. As it was suggested in the operational guidelines, practice of regular review at the end
of three months should be reinstituted at State, district level together by both partners.
6. Thus lack of awareness is the presently first and foremost bottleneck observed in the
implementation of the programme and which need to be taken up vigorously. Also it is
observed that the all patients coming on 9th of the months are not consulted free of cost
which was the key guidelines under the scheme with tremendous implications on
success. It is required to re-imbibe this concept in the registered doctors for improving
the utilization of scheme.
* * * * * * * * * * * *
CONCLUSION & RECOMMENDATIONS

34
QUESTIONNAIRE FOR THE WOMEN OF REPRODUCTIVE AGE GROUP
( PROSPECTIVE BENEFICIARIES)
Cluster No. :- Locality :- Dist :- Ahmedabad
Details Married women
(18–45 yrs)
Pregnant
& women
with child
of 2 months
Women number in cluster 1 2 3 4 5 6 7 8
(1). Age (in Years)
(2). Knowledge regarding any programme for mothers Yes / No
(3). Knowledge regarding Vande Mataram Scheme Yes / No
(3) a. If Yes,
(i) From where did you get the information ?Advertisement = 1,
Neighbours = 2, Health workers = 3, From registered beneficiaries = 4,
others = 5.
(i) What is the Programme about ? Related to pregnant women = 1, Related
to women of reproductive age group = 2, Related to children = 3,
Others = 4.
(ii) Programme is executed at :- Private Hospital (multi-speciality hospital)
=1,
Private Clinic = 2, CHC = 3, Sub-district hospital = 4, PHC : 5, Others =
6.
(iii)Frequency of Check-up :- Weekly = 1, Fortnightly = 2, Monthly = 3,
Others = 4.
(iv)By whom check-up is done ? Private obstetrician = 1, Govt. Obstetrician
= 2,
Medical Officer = 3, General Practitioner = 4, Others = 5.
(v) What investigations are carried out ? Hb. = 1, Urine Albumin & Sugar =
2,
Blood grouping & Cross-matching = 3, Torch infections = 4, Weight =
5,
B.P. = 6, Others =7.
(vi) Is it free of cost ? Yes / No
(vii) Are IFA tablets provided free of cost ? Yes / No
(viii) Are FP services available free of cost ? Yes / No
(ix) Are complicated cases referred ? Yes / No
(x) Is treatment for RTI / STDs given ? Yes / No
(xi) Would you like to avail the services provided in this programme ?
Yes / No
Annexure : I

35
Women number in cluster (cont..) 1 2 3 4 5 6 7 8
Further Questions applicable for pregnant women 6 , 7 & 8
(xi) Do you avail the services under the Vande Mataram Scheme ? Yes/No
If No, Reasons :- Don’t Know = 1, It consumes lot of
time = 2, Charges are taken = 3, Approach is not proper = 4,
Behaviour is not good = 5, Timings are not convenient = 6, Place of
check-up is too far = 7, others = 8
(4) Place of diagnosis of pregnancy :- At home by using kit = 1, Private
Obstetrician = 2, Govt. Hospital = 3, Trust hospital = 4 , Vande Mataram
Scheme = 4, PHC = 5, Municipal Hospital =6, Others = 7.
(5) Place of registration : Private Obstetrician : 1, Govt. Hospital : 2, Trust
hospital : 3, Vande Mataram Scheme : 4, PHC : 5, Municipal hospital = 6,
Others = 7.
(6) No. of Antenatal check-ups till now
(7) Have you taken IFA tablets ? Yes / No
(8) Have you taken T.T ? Yes / No
(9) Which investigations have been carried out ? Hb. = 1, Urine Albumin &
Sugar
= 2, Blood grouping & Cross-matching = 3, Torch infections = 4, Weight =
5,
B.P. = 6, Others =7.
Questions for postnatal mothers
(10) Have you undergone postnatal check-ups ?
If Yes, how many times ?
(11) Have you been given advise regarding FP ? Yes / No
No. of Household visited :-
Name of the Investigator :- Sign of the Investigator :-
Date :- Dec 2004

36
Interview with the Doctors volunteered in the scheme
Sr. No. : - __ __ Date of Interview :-
Details Feb Mar Apr May June Jul Aug Sep Oct Nov Dec
Beneficiaries
registered
IFA used
FP devices
Referred
RTI / STDs
* Write down the number or not applicable
General Information of Doctor
Name of the Doctor :
Qualification : Passed in (MD/DGO ) : ____________
Address :-
Ward/PHC area :
Date/month of registration to scheme :
Days and Time of service:-
Services provide at: Own Clinic /Govt. hosp / Trust (NGOs) hosp. /
Other (Specify) ____________________
Annexure : II

37
Q-1. According to you whether scheme is utilized by beneficiaries
adequately or not? Yes / No
If not reasons:
1. Inadequate publicity by Govt. 2. My clients prefer paid services
3. Others (Specify): __________________________
Q-2. Doctor’s Experience and opinion about scheme:
_____________________________________________________________
Q-3. Doctor’s Suggestion to improve the scheme:
_____________________________________________________________
Q-4: Weather the board for the scheme is provided by the CDHO?
Yes / No
Q-5. Whether board of Vande Mataram Scheme displayed or not:-
Yes / No
Q-6. What is the trend of supply of FP devices from CDHO :-
Regular / Irregular Adequate / Inadequate:
Q-7. What is the trend of supply of ANC card from CDHO :-
Regular / Irregular, Adequate / Inadequate:
Q-8. What is the trend of supply of IFA from CDHO:-
Regular / Irregular Adequate / Inadequate
Name & Sign of the investigator : ______________________________

38
PROFORMA FOR THE BENEFICIARIES
Q-1. Profile of the beneficiaries :-
(i) Name : ________________________________________________________
(ii) Address : ______________________________________________________
______________________________________________________
(iii) Ward/PHC: _____
(iv) Age : __ __ years
(v) Occupation :-
Housewife = 1, Labourer = 2, Private employee = 3, Govt. employee = 4,
Professional = 5, Business = 6, Skilled worker = 7,
Others = 8 (Specify) _________________________________________
(vi) Education :-
Illiterate = 1, Primary = 2, Secondary = 3, Higher Secondary = 4, Graduate = 5,
Post-graduate = 6, Professional = 7, Other = 8 (Specify) __________________
(vii) Education of the husband :-
Illiterate = 1, Primary = 2, Secondary = 3, Higher Secondary = 4, Graduate = 5,
Post graduate = 6, Professional = 7, Other = 8 (Specify)__________________
(viii) Total Family Members :- __ __
(ix) Total Family Income :- __ __ __ __ __ /month
(x) Socioeconomic status :- Class I / II / III / IV / V
(xi) Order of pregnancy : 1/ 2 / 3 / 4 / > 5
(xii) Family size ( No. of living children) :- ___
(xiii) Past Obstetric history : -
Still Birth = 1, Caesarian Section = 2, Spontaneous abortion = 3,
Hemorrhage = 4, Not Applicable = 5
(xiv) In case of Second Gravida or more, Where she has availed the previous services :-
Private Hospital = 1, Private clinic = 2, Government Hospital = 3, Municipal Hospital
= 4, Trust Hospital = 5,
Others = 6 (Specify) _____________________
(xv) Date of LMP : __ __ / __ __ / 2004
(xvi) Due date of delivery : __ __ / __ __ / 2004
(xvii) No. of Ante natal check-ups undergone till now (Taken/Due) :- __ / __
Annexure : III
39
Q-2 Show the ANC Card given by practitioners? Shown / Not shown.
If not shown, Reasons for non availability of the card :-
Lost = 1,could not, Find = 2, Others=3(specify)_________________________
(i) From where did you get the information about Vande Mataram Scheme ? Newspapers
= 1, Doctors = 2, TV = 3, Radio = 4, Pamplets-posters = 5, Beneficiaries = 6, Person
other than beneficiaries = 6,
Others = 7 (Specify) _____________________________________________
(ii) Date on which the Services you have availed : : __ __ / __ __ / 2004
(iii) Which Services did you avail ?
Antenatal = 1, Postnatal =2, Family Planning = 3
(iv) Where did you avail services?
CHC = 1, Private hospital = 2, FRU = 3, Sub-district Hospital = 4, Others = 5.
(v) How many times have you availed services?
Once = 1,Twice = 2, Thrice = 3, More than three times = 4.
(vi) By whom the check-up is done ?
Specialist = 1, MBBS doctor = 2, Nurse = 3, Paramedical personnel = 4,
Others = 5 (Specify)_________________________________________________
(vii) Which investigations have been carried out ?
Hb. = 1, Urine Albumin & Sugar = 2, Blood grouping & Cross-matching = 3,
Torch infections = 4, Weight = 5, B.P. = 6,
Others =7 (Specify) _______________________________
(viii) Had you paid any charges ? Yes/ No
(ix) How much you paid : ______________
(x) Reasons for paying charges :-
For check-up = 1, For investigations = 2, for medicines = 3
(xi) IFA tablets received? Yes/ No, If yes how many :
(xii) What advices you have been given ?
FP = 1, Diet = 2, Rest = 3, BF = 4, Danger signs = 5, Follow-up = 6,
Others = 7 (Specify) ____________________________

40
Q-3. Your experience regarding the programme?
Highly satisfied = 1, Satisfied = 2, Not satisfied = 3, OK = 4, Not replied = 5,
Others = 6 (Specify) ___________________
(a) If Satisfied/highly satisfied reasons;
(i) Check-up is done nicely
(ii) Check-up is carried out by the specialist
(iii) Is is free of cost
(iv) It is done regularly
(v) Advise regarding the selection of family planning devices is given
(vi) Others (specify) ________________________
(b) If No, reasons
(i) Place of check-up is too far ?
(ii) It consumes lot of time ?
(iii) Charges are taken ?
(iv) Check-up is not done properly?
(v) Behavior is not good ?
(vi) Timings are not convenient ?
(vii) Others (specify) ________________________
Q-4. Will you recommend other females to avail the services under this programme ?
Yes / No
Q-5. Where would you like your delivery to be conducted ?
Home = 1, Private hospital = 2, CHC = 3, FRU = 4, PHC = 5,
Not applicable in case of postnatal mothers = 6.
Q-6. Are you been referred to any other hospital during pregnancy ? Yes / No
Reason for referral : ____________________________________________________
Q-7. Are you been given treatment for any infection during pregnancy ? Yes / No
Q-8. Your feed back on the Scheme : ____________________________________________
__________________________________________________________________________
___________________________________________________________________________
Q-9. Your suggestion to improve the Scheme : -____________________________________
___________________________________________________________________________
___________________________________________________________________________
Name & Signature of investigator : Date :- -- / -- / ----

41
Sr. Clusters
(Wards/PHC) 1 Aamraivadi
2 Behrampura
3 Gomtipur
4 Jamalpur
5 Jetalpur
6 Kaligam
7 Khadia
8 Khokhara
9 Kubernagar
10 Madhupura
11 Maninagar
12 Memnagar
13 Naranpura
14 Naroda
15 Naroda Muthiya
16 Navrangpura
17 Nikolgam
18 Odav
19 Ognaj
20 Old Vadaj
21 Rakhiyal
22 Ranip
23 Sabarmati
24 Saraspur
25 Sardarnagar
26 Shahpur
27 Thakorbapanagar
28 Vasna
29 Vatva
30 Vejalpur
(Total population = 40,52,777, Cluster Interval 1,5,093/-)
Total 51 units (44 wards and 7 PHC areas. i.e. areas where Private Gynecologist have enrolled in Vande Mataram Scheme.) were considered for cluster selection.
Annexure : IV

42
TEAM* FOR VANDE MATARAM SCHEME STUDY
Project Guide Dr. B. S. Bhavsar,
President, IAPSM-GC &
Professor & Head
Chief coordinator Dr. K. N. Sonaliya Secretary IAPSM-GC & Assistant Professor
Principal Investigator Dr. A. M. Kadri Joint secretary IAPSM-GC & Assistant professor
Co-Investigator & Project Coordinator
Dr. Shikha Jain Assistant professor
Co-Investigator & Co-Coordinator
Dr. Sunil Nayak Final Year Resident
Asst project Coordinator
Dr. Chintul Shah Final Year Resident
Performa Design Dr. Dr. B. S. Bhavsar, Dr. G. K Kedia Dr. M. K. Lala Dr. A. Bhagyalaxmi Dr. A. M. Kadri Dr. Atul Trivedi Dr. Shikha Jain Dr. Sunil Nayak Dr. Chintul Shah
Faculties of Department of B.J.Medical College
Field Investigators Dr. Nital D. Patel Dr. Avni N. Suthar Dr. Kiran C. Patel Dr. Jayshree M. Patel Dr. Bhumi Meghpara Dr. Nisarg Patel Dr. Sapra Dalpat Dr. Arpit Sharma Dr. Rakesh Tank Dr. Nikhil Chaudhari Dr. Maulik Jethva Dr. Dipak G. Patel
All interns
Data Entry Mr. Narendra Parmar Ms. Finomina
Sanitary Inspector Laboratory Technician
Analysis & Report writing
Dr. A. M. Kadri Dr. Shikha Jain Dr. Mitesh Patel Dr. Sunil Nayak
Assistant Professor Assistant Professor Assistant Professor Final Year Resident
Finance Dr. Atul Trivedi Treasure, IAPSM-GC & Assistant Professor