a systematic review and meta-analysis of ciprofloxacin
TRANSCRIPT

A systematic review and meta-analysis of ciprofloxacin resistance in community and
hospital acquired E. coli UTI
Oyebola Fasugba1, Anne Gardner1, Brett Mitchell1, 2 , George Mnatzaganian1
1Faculty of Health Sciences, Australian Catholic University2Discipline of Nursing and Lifestyle Research Centre, Avondale College
1

Disclosure
• Ms Oyebola Fasugba, Prof Anne Gardner and A/Prof Brett
Mitchell are members of ACIPC
• A/Prof Brett Mitchell is Interim Editor-in-Chief
Infection, Disease and Health and Prof Anne Gardner is
on the Editorial board
• A/Prof Brett Mitchell is a member of the scientific
organising committee.
• Dr George Mnatzaganian has no conflicts of interests
2

Introduction
• Ciprofloxacin is the most frequently prescribed
fluoroquinolone for UTIs
• Not recommended for first-line treatment of UTI (Antibiotic Expert Groups,
2014; Gupta et al., 2011, Kurutepe et al., 2005)
• Fluoroquinolones ranked as one of the highest priority
critically important antimicrobials (AGISAR, 2012)
• Evidence shows increasing urinary E. coli resistance to
ciprofloxacin (Mcquiston Haslund et al., 2013)
• Lack of quantitative syntheses of overall ciprofloxacin
resistant E. coli UTI rates3
Aim
Systematically review the literature and conduct a
meta-analysis of observational studies published in
the last eleven years investigating ciprofloxacin
resistance in community-acquired and hospital-
acquired Escherichia coli urinary tract infection
4

Significance
• Expand understanding of antimicrobial resistance in urinary E. coli infections
• Provide information on global ciprofloxacin
resistance
• Provide a baseline for future interventions to be measured
• Highlight the methodological challenges of conducting research in this field
5

Methods
• Systematic review with meta-analyses
• Protocol registered (PROSPERO; registration number:
CRD42014014473)
• Electronic searches of 6 databases - MEDLINE, PubMed,
EMBASE, CINAHL, Scopus and Cochrane (2004-2014)
• Search terms: ‘resistance’, ‘urinary tract infection’ and
‘Escherichia coli’
6

MethodsInclusion criteria Exclusion criteria
Observational studies (cross sectional, cohort and case control)
Papers published over 11 years ago
Studies reporting ciprofloxacin resistance rates in E. coli UTI
Non-peer reviewed literature
Studies using CDC criteria formicrobiologically confirmed UTI (≥105
colony forming unit/ml)
Papers written in languages other than English
Hospital – studies with samples obtained after 48 hours of admission or within 48 hours of discharge
Setting (hospital or community) not clearly defined in study
Community- studies with samples from outpatients; general practices; emergency departments; within 48 hours of admission; nursing homes/aged care
7

Methods
• Quality and risk of bias (ROB) assessed using modified
version of Newcastle-Ottawa Scale (Wells et al., 2014)
• Pooled proportions & 95% confidence intervals
calculated using random effects meta-analysis model (Cooper
et al., 2009; DerSimonian & Laird, 1986)
• Degree of heterogeneity assessed using I2 statistic (Cooper et al.,
2009)
• Meta-regression and sub-group analyses to investigate
heterogeneity
• Funnel plots to investigate publication bias8

Results
• Of the identified 1134 papers, 53 were eligible for
inclusion
• Comprised 3 hospital and 51 community acquired
E. coli UTI studies
• 80% of studies were cross sectional
• Duration of studies ranged from 2 to 84 months
• <50% provided demographic data on participants
9
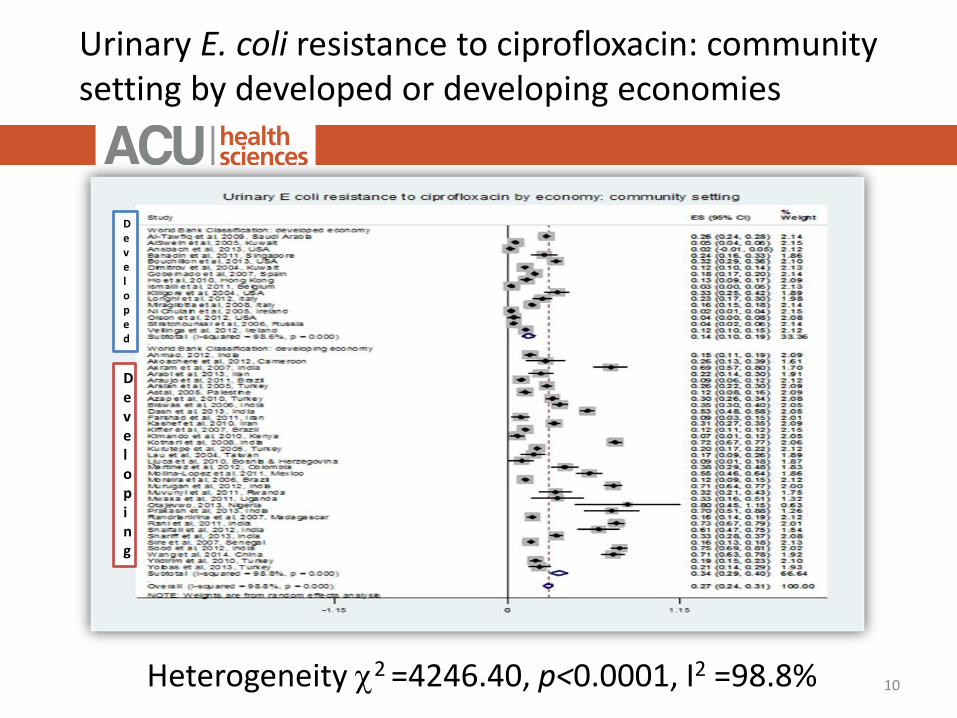
Urinary E. coli resistance to ciprofloxacin: community setting by developed or developing economies
Heterogeneity 2 =4246.40, p<0.0001, I2 =98.8% 10
Developing
Developed

Heterogeneity 2 =0.89, p = 0.641, I2 < 0.01% 11
Urinary E. coli resistance to ciprofloxacin: hospital setting
Results
Pooled resistance
hospital = 0.38 (0.36-0.41)
community = 0.27 (0.24-0.31)
P<0.001
12

Results
n=47, rs = 0.4313, P = 0.00313

Discussion
• Higher hospital than community resistance comparable
to individual studies
• Significantly higher resistance in developing compared to
developed countries attributed to over the counter use
of antibiotics
• Significant rise in resistance over time likely due to
increase in the use of FQs over the years
14

Limitations
• Poor quality of many studies retrieved resulted in a large
number being excluded
• Using the CDC criteria for definition of laboratory
diagnosed UTIs may have limited the number of hospital
acquired UTI studies
• Wide variation of resistance estimates between studies
and inclusion of studies having substantial clinical and
methodological heterogeneity
15

Implications and Conclusion
• Ciprofloxacin as empirical therapy for UTI should be
reconsidered
• Efforts should be made to limit its use to clinical
conditions for which there are clear therapeutic
indications
• Policy restrictions on ciprofloxacin use should be
enhanced especially in developing countries
16

Citation
Fasugba, O., Gardner, A., Mitchell, B. & Mnatzaganian, G. (2015). Ciprofloxacin resistance in community- and hospital-acquired Escherichia coli urinary tract infections: a systematic review and meta-analysis of observational studies. BMC Infectious Diseases (in press)
17

Acknowledgements
Thanks to supervisors
Thanks to Associate Professor Elizabeth McInnes
& Dr Verena Schadewaldt
Ms Fasugba is supported by an Australian Catholic
University Postgraduate Award
18

References
Antibiotic Expert Groups. (2014). Therapeutic guidelines: antibiotic. Version 15. Melbourne: Therapeutic Guidelines Limited. Retrieved from http://www.tg.org.au/?sectionid=41.
Cooper, H., Hedges, L. V., & Valentine, J. C. (2009). The handbook of research synthesis and meta-analysis: Russell Sage Foundation.
DerSimonian, R., & Laird, N. (1986). Meta-analysis in clinical trials. Controlled clinical trials, 7(3), 177-188. Gupta, K., Hooton, T. M., Naber, K. G., Wullt, B., Colgan, R., Miller, L. G., . . . Schaeffer, A. J. (2011). International clinical practice
guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clinical infectious diseases, 52(5), e103-e120.
Kurutepe, S., Surucuoglu, S., Sezgin, C., Gazi, H., Gulay, M., & Ozbakkaloglu, B. (2005). Increasing antimicrobial resistance inEscherichia coli isolates from community-acquired urinary tract infections during 1998-2003 in Manisa, Turkey. Japanese Journal of Infectious Diseases, 58(3), 159-161.
Mcquiston Haslund, J., Rosborg Dinesen, M., Sternhagen Nielsen, A. B., Llor, C., & Bjerrum, L. (2013). Different recommendationsfor empiric first-choice antibiotic treatment of uncomplicated urinary tract infections in Europe. Scandinavian journal of primary health care, 31(4), 235-240.
Wells, G., Shea, B., O’connell, D., Peterson, J., Welch, V., Losos, M., & Tugwell, P. (2014). The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses Retrieved 10 November 2014, from http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
WHO Advisory Group on Integrated Surveillance of Antimicrobial Resistance (AGISAR). (2012). Critically Important Antimicrobials for Human Medicine-3rd Revision. Geneva: World Health Organisation Retrieved from http://apps.who.int/iris/bitstream/10665/77376/1/9789241504485_eng.pdf.
19
