aac accepts, published online ahead of print on 19 november 2012...
TRANSCRIPT
1
Limited Activity of Miltefosine in Murine Models of Cryptococcal 1 Meningoencephalitis and Disseminated Cryptococcosis 2
Nathan P. Wiederhold1,2, Laura K. Najvar1,3, Rosie Bocanegra1,3, William R. 3 Kirkpatrick1,3, Tania C. Sorrell4,5,6, Thomas F. Patterson1,3 4
1University of Texas Health Science Center at San Antonio, San Antonio, TX, USA 5 2University of Texas at Austin College of Pharmacy, Austin, TX, USA 6 3South Texas Veterans Health Care Administration, San Antonio, TX, USA 7 4Sydney Emerging Infections and Biosecurity Institute, Sydney, Australia 8 5University of Sydney, Sydney, Australia 9 6Westmead Millennium Institute, Sydney, Australia 10 Running Title: Miltefosine against Cryptococcal Meningoencephalitis and 11 Cryptococcosis 12 Keywords: Miltefosine, cryptococcal meningoencephalitis, cryptococcosis, 13 Cryptococcus neoformans 14 Abstract Word Count: 216 Manuscript Word Count: 3006 15 Corresponding Author: 16 Nathan P. Wiederhold, Pharm.D. 17 UTHSCSA, PERC MSC 6220 18 7703 Floyd Curl Drive 19 San Antonio, TX 78229 20 Phone: 210-567-8340 21 Fax: 210-567-8328 22 Email: [email protected] 23
Copyright © 2012, American Society for Microbiology. All Rights Reserved.Antimicrob. Agents Chemother. doi:10.1128/AAC.01624-12 AAC Accepts, published online ahead of print on 19 November 2012
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

2
ABSTRACT: 24 Miltefosine is an alkyl phosphocholine with good oral bioavailability and in vitro 25 activity against Cryptococcus species that has gained interest as an additional agent for 26 cryptococcal infections. Our objective was to further evaluate the in vivo efficacy of 27 miltefosine in experimental in vivo models of cryptococcal meningoencephalitis and 28 disseminated cryptococcosis. Mice were infected intracranially or intravenously with 29 either C. neoformans USC1597 or H99. Miltefosine treatment (1.8 - 45 mg/kg orally 30 once daily) began either 1 hour or 1 day post-inoculation. Fluconazole (10 mg/kg orally 31 twice daily) or amphotericin B deoxycholate (3 mg/kg intraperitoneally once daily) 32 served as positive controls. In our standard models, miltefosine did not result in 33 significant improvements in survival or reductions in fungal burden against either C. 34 neoformans isolate. There was a trend towards improved survival with miltefosine 7.2 35 mg/kg against disseminated cryptococcosis with the H99 strain, but only at a low 36 infecting inoculum. In contrast, both fluconazole and amphotericin B significantly 37 improved survival in mice with cryptococcal meningoencephalitis and disseminated 38 cryptococcosis due to USC1597. Amphotericin B also improved survival against both 39 cryptococcal infections caused by H99. Combination therapy with miltefosine 40 demonstrated neither synergy nor antagonism in both models. These results demonstrate 41 limited efficacy of miltefosine and suggest caution with the potential use of this agent for 42 the treatment of C. neoformans infections. 43 44 45 46
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

3
INTRODUCTION 47 Cryptococcal meningoencephalitis remains a substantial infectious disease 48 challenge. Populations at risk for infections caused by Cryptococcus neoformans include 49 HIV/AIDS patients, recipients of solid organ or hematopoietic stem cells transplants, as 50 well as those receiving high dose chemotherapy or some other immunocompromised 51 condition (6, 19). The Centers for Disease Control and Prevention have estimated that in 52 HIV/AIDS patients the global burden of cryptococcosis is 1 million cases annually (18), 53 while other studies have reported the three month mortality for the treatment of acute 54 cryptococcal meningoencephalitis to be approximately 20% (11, 16). Effective treatment 55 is available in the United States and other developed countries, and includes amphotericin 56 B and flucytosine as induction therapy followed by fluconazole (19). However, 57 intravenous medications as well as oral flucytosine may not be available in less 58 developed areas, and the use of high dose oral fluconazole is not as effective as induction 59 therapy with amphotericin B (15, 20). Thus, there is a clinical need for new or alternative 60 strategies, including agents that may be administered orally, for the treatment of 61 cryptococcal meningoencephalitis. 62 Miltefosine (hexadecylphosphocholine) is an alkyl phosphocholine that has been 63 used in the treatment of leishmaniasis, including New World cutaneous, mucocutaneous, 64 and visceral disease (3, 4, 12, 22-26). Miltefosine can be administered by mouth, and 65 good oral bioavailability (82 - 94%) has been reported in rats and dogs (21). Recently, 66 this agent has gained interest as a potent therapeutic against invasive mycoses, including 67 cryptococcal infections as in vitro studies have demonstrated potent activity against C. 68 neoformans and dermatophytes (28, 29). In one case report, miltefosine in combination 69
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

4
with voriconazole and terbinafine was successfully used to treat a child with 70 Scedosporium prolificans osteomyelitis (13). Improvements in survival and reductions in 71 tissue fungal burden with the oral administration of miltefosine were also reported in a 72 murine model of disseminated cryptococcosis (29). Based on the preliminary in vitro data 73 that demonstrated activity against C. neoformans and in vivo efficacy against 74 disseminated cryptococcosis, we sought to further evaluate the effectiveness of 75 miltefosine in our murine model of cryptococcal meningoencephalitis, both as 76 monotherapy and in combination with other antifungals. Studies were also conducted to 77 further characterize the efficacy of this agent against disseminated cryptococcosis. 78 MATERIALS AND METHODS 79 Isolates and Antifungal Agents. Cryptococcus neoformans clinical isolate 80 USC1597 and H99 were used throughout this study. Each isolate was subcultured at 81 least twice on Sabouraud dextrose agar (SDA) (Remel, Inc., Lenexa, KS) before each in 82 vitro and in vivo experiment. Prior to inoculation, the isolates were grown in brain heart 83 infusion broth overnight at 37°C with shaking. The cells were then collected by 84 centrifugation, and were washed three times in sterile saline. The inocula concentrations 85 were determined with a hemocytometer, and viability was confirmed by plating serial 86 dilutions and enumeration of colony forming units (CFU). The clinically available 87 intravenous formulations of fluconazole (Pfizer, Inc., New York, NY) and amphotericin 88 B deoxycholate (X-Gen Pharmaceuticals, Big Flats, NY) were used in all studies and 89 were prepared according to the package inserts. Miltefosine powder was obtained from 90 Cayman Chemical Company (Ann Arbor, MI) and was dissolved in physiologic saline 91 prior to each experiment. 92
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

5
Susceptibility Testing. Susceptibility testing was done by broth microdilution in 93 accordance with the CLSI M27-A3 methodology in RPMI 1640 growth medium buffered 94 with 0.165M morpholinepropanesulfonic acid (MOPS; pH 7.0) (7). Stock solutions of 95 were prepared in water (fluconazole and amphotericin B deoxycholate) or RPMI 1640 96 (miltefosine). Aliquots of each agent (0.1 mL) at 2X concentrations were dispensed into 97 96 well microdilution trays. C. neoformans cells in RPMI were added (final inocula 0.5-98 2.5 x 103 cells/mL) and the trays were incubated at 35°C. Final antifungal concentrations 99 ranged from 0.125 - 64 µg/mL for miltefosine and fluconazole, and from 0.03 to 16 100 µg/mL for amphotericin B. The MICs for fluconazole were read at 50% reduction in 101 turbidity as compared to growth control at 72 hours. For amphotericin B and miltefosine, 102 MICs were determined as 100% inhibition relative to growth controls. In later 103 experiments, 5% (50 mg/mL) bovine serum albumin (Equitech Bio, Inc. Kerrville, TX) 104 was added to the RPMI medium to assess the effects of protein binding on the in vitro 105 potency of miltefosine. 106
Animal Model. Previously described murine models of cryptococcal 107 meningoencephalitis and disseminated cryptococcosis were utilized for all studies (8, 9, 108 27, 29). Immunocompetent outbred ICR mice (Harlan) weighing approximately 25 109 grams were housed five mice per cage and had access to food and water ad libitum. To 110 establish cryptococcal meningoencephalitis, mice were anesthetized using isoflurane, and 111 C. neoformans at 1500 - 2600 cells/mouse was delivered in a 0.06 mL volume through a 112 27-gauge needle fastened to a tuberculin syringe with a cuff to prevent penetration of 113 more than 1 mm. A midline puncture through the cranial vault approximately 6 mm 114 posterior to the orbit was made and the inoculum was injected after which the mice were 115
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

6
allowed to recover. To establish disseminated cryptococcosis, mice were inoculated 116 intravenously via the lateral tail vein with C. neoformans over a range of inocula in 117 different experiments (4.0 x 103 - 6.1 x 105 cells/mouse) delivered in a 0.2 mL volume of 118 sterile saline. This study was approved by the Institutional Animal Care and Use 119 Committee at the University of Texas Health Science Center at San Antonio, and all 120 animals were maintained in accordance with the American Association for Accreditation 121 of Laboratory Animal Care (17). 122 Antifungal Treatment. Antifungal therapy with miltefosine was initiated either 123 1 hour or 1 day post-inoculation at doses ranging between 1.8 - 60 mg/kg once daily by 124 oral gavage. Amphotericin B was initiated either 1 hour or 1 day post-inoculation at a 125 dose of 3 mg/kg once daily by intraperitoneal injection, while fluconazole was initiated 1 126 day post-inoculation in all experiments at a dose of 10 mg/kg once daily by oral gavage. 127 Between 8 - 20 mice were included per dosage group of each antifungal in each 128 experiment. The duration of therapy for each agent in each study is specified in the 129 Results section. 130 Outcome Measures. Survival and brain tissue fungal burden were used to 131 measure the in vivo efficacy of antifungal therapy. In the survival experiments, mice 132 were followed off therapy to either day 21 or day 30 post-inoculation, and any animal 133 that appeared moribund was humanely euthanized. In tissue burden experiments, brain 134 tissues were aseptically collected one day after treatment stopped in order to measure 135 fungal burden. Brains were weighed and then homogenized in sterile saline with a tissue 136 homogenizer. Serial dilutions were prepared in sterile saline and plated on SDA. After 137
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

7
48 - 72 hours of incubation, colonies were counted and the number of CFU per gram of 138 tissue for each animal was calculated. 139 Statistics. Survival was plotted by Kaplan-Meier analysis, and the log-rank and 140 Fisher’s exact test were used to assess for significant differences in median survival and 141 percent survival, respectively. Differences in tissue fungal burden were assessed using 142 ANOVA with Tukey’s post-test for multiple comparisons. A p-value of < 0.05 was 143 considered statistically significant. 144 RESULTS 145 Susceptibility. Miltefosine demonstrated in vitro activity against C. neoformans 146 USC1597 and H99 (MIC 1 μg/mL and 0.5 μg/mL, respectively) in RPMI. Fluconazole 147 was active against each C. neoformans isolate (MIC against USC1597 1 μg/mL & H99 2 148 μg/mL), and amphotericin B also demonstrated potent activity against both isolates (MIC 149 0.25 μg/mL). In contrast to the activity observed in RPMI for miltefosine, the potency of 150 this agent was significantly reduced with the addition of 5% BSA (MIC >64 μg/mL). 151 Cryptococcal Meningoencephalitis Caused by C. neoformans USC1597. The 152 objective of this study was to evaluate the in vivo efficacy of miltefosine against 153 cryptococcal meningoencephalitis, and the initial experiments utilized the fully 154 susceptible C. neoformans isolate (USC1597) to establish infection. Monotherapy with 155 miltefosine at doses ranging from 5 to 60 mg/kg/ day, amphotericin B 3 mg/kg/day, or 156 fluconazole 10 mg/kg twice daily were initiated one day post challenge, and each agent 157 was continued for 10 days in the survival arm and for seven days in the fungal burden 158 arm. Miltefosine did not lead to a survival advantage at doses as high as 45 mg/kg as the 159 median survival (range 13.5 - 23.5 days) and percent survival (0 - 10%) as each dose did 160
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

8
not differ significantly from untreated controls (19 days and 10.5%) (Figure 1A & B). In 161 contrast, median survival was significantly prolonged with fluconazole and amphotericin 162 B (29 and > 30 days, respectively) compared to controls and each miltefosine dose (p < 163 0.05 for all comparisons). In addition, amphotericin B significantly improved the 164 percentage of animals surviving to day 30 (95%; p < 0.05) (Figure 1B). Although 165 therapy with miltefosine 60 mg/kg was initially tried, mice were unable to tolerate a dose 166 this high as several died following a single administration, therefore, this dose was 167 discontinued. Combination therapy with miltefosine was also ineffective. Neither a 168 survival advantage or disadvantage was observed with miltefosine 45 mg/kg plus 169 amphotericin B or fluconazole as the median and percent survival values for these 170 combinations were similar to those observed with monotherapy with these antifungals 171 (Figure 1C). 172 Since the marked survival advantage observed with daily administration of 173 amphotericin B may have masked any benefit of combination therapy, we also evaluated 174 daily high dose miltefosine with a short course of this polyene. In this experiment, both 175 miltefosine 45 mg/kg and amphotericin B were initiated 1 hour post challenge, and 176 amphotericin B was discontinued after two doses. Even when therapy was initiated 177 shortly after intracranial challenge no improvement in survival was observed with 178 miltefosine monotherapy as the median and percent survival values (17.5 days and 0%) 179 were similar to untreated controls (15.5 days and 0%) (Figure 1D). In contrast, 180 monotherapy with a short course of amphotericin B still resulted in longer survival 181 compared to controls and miltefosine (24 days; p < 0.01). Similar to the previous results, 182 miltefosine combination therapy did not lead to a significant benefit compared to 183
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
9
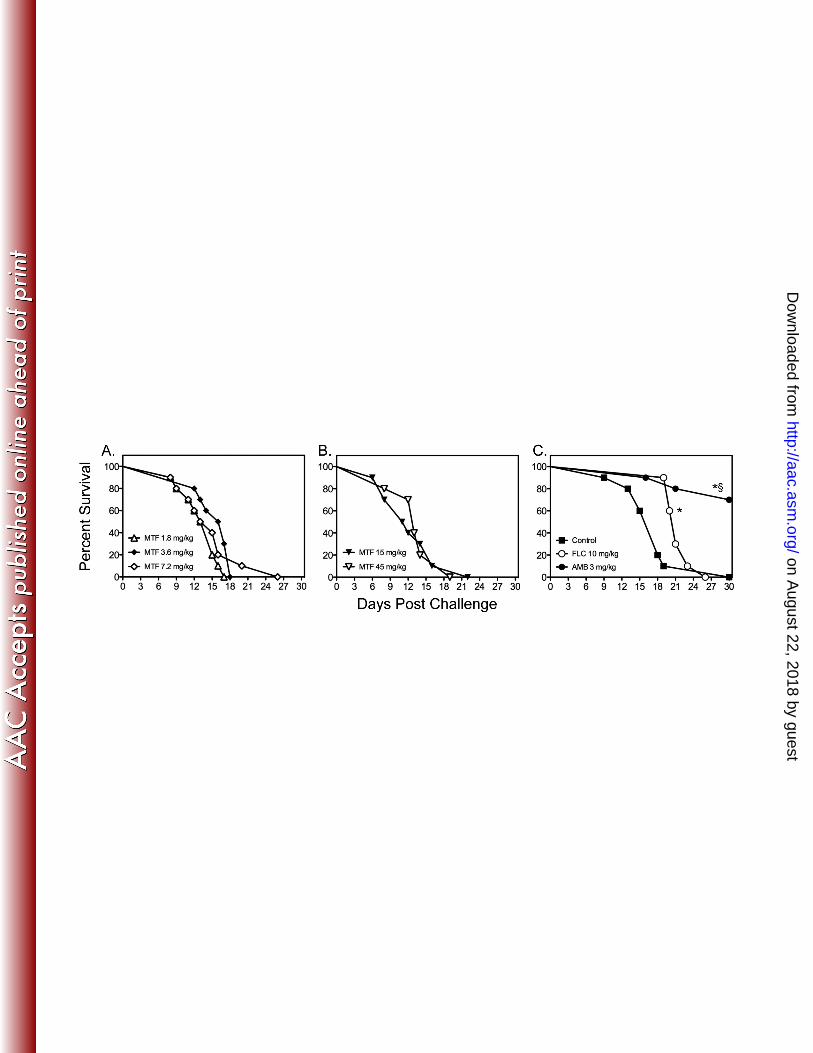
amphotericin B alone (median survival 21.5 days). The lack of efficacy of miltefosine 184 was also evident in the brain tissue fungal burden results (Table 1). No reductions in 185 fungal burden were observed in any miltefosine monotherapy group compared to 186 untreated controls. In contrast, significant reductions were observed in mice that received 187 fluconazole or amphotericin B as well as in those that received combination therapy. 188 Futhermore, the addition of miltefosine did not result in further reductions in fungal 189 burden compared to fluconazole or amphotericin B alone. 190 Cryptococcal Meningoencephalitis Caused by C. neoformans H99. Since the 191 previous study that reported in vivo efficacy of miltefosine against disseminated 192 cryptococcosis used a different C. neoformans strain (H99), we also evaluated the 193 effectiveness of this agent against cryptococcal meningoencephalitis caused by this 194 isolate. As shown in Figure 2, miltefosine was also ineffective against CNS infection 195 caused by H99. No improvements in survival were observed when miltefosine was 196 initiated 1 hour after inoculation at lower doses (1.8 - 7.2 mg/kg/day through day 4, 197 Figure 2A), or when higher doses with a longer period of administration were used (15 & 198 45 mg/kg/day through day 10, Figure 2B). In contrast, both amphotericin B and 199 fluconazole resulted in significant improvements in survival (median survival 21 and >30 200 days, respectively, Figure 2C) compared to untreated controls (18 days; p < 0.05) and 201 each miltefosine dose (range 11.5 - 16.5 days; p < 0.0001). The percentage of animals 202 surviving to day 30 was also significantly higher in animals treated with amphotericin B 203 compared to all other groups (70% vs. 0%; p < 0.001). 204 Disseminated Cryptococcosis Caused by C. neoformans USC1597 and H99. 205 We also evaluated the efficacy of miltefosine for the treatment of disseminated 206
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

10
cryptococcosis following intravenous challenge. In these experiments, miltefosine (1.8 - 207 45 mg/kg/day) was initiated one hour after inoculation, while fluconazole and 208 amphotericin B were started 1 day after infection. As seen against cryptococcal 209 meningoencephalitis, miltefosine did not improve survival at any dose tested (median 210 survival range 10 - 14 days) compared to untreated controls (12 days; Figure 3A & B). 211 Survival was significantly improved with fluconazole and amphotericin B (>21 days for 212 both agents; p < 0.0001). Combination therapy also did not significantly improve 213 survival compared to amphotericin B alone (Figure 3C). Furthermore, no significant 214 reductions in fungal burden were observed within the lungs or brain tissue with high dose 215 miltefosine (45 mg/kg) as monotherapy (Table 1), nor did combination therapy result in 216 further reductions in fungal burden compared to amphotericin B monotherapy. 217 We also tested the effectiveness of miltefosine against disseminated 218 cryptococcosis caused by C. neoformans H99. As shown in Figure 4, miltefosine and 219 fluconazole did not improve survival compared to untreated controls, while amphotericin 220 B significantly improved survival versus all other groups. As these results were in 221 contrast to what was previously reported in a similar model of disseminated 222 cryptococcosis, we also evaluated the effects of different infecting inocula levels on the 223 survival of untreated controls. As expected, the higher inocula (4.7 x 104 and 5.9 x 105 224 cells/mouse) resulted in 100% mortality early during the course of infection (Figure 5A). 225 As the survival curve for the 4.8 x 103 cells/mouse inoculum was similar to that observed 226 in untreated controls in the previous study that reported in vivo efficacy for miltefosine 227 (29), we also tested the effectiveness of this agent at this lower infecting inoculum. 228 Interestingly, a trend towards improved survival was observed with miltefosine 7.2 229
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

11
mg/kg/day versus untreated controls (17.5 vs. 20.5 days, respectively; p = 0.09), which 230 was in agreement with the results of the previous study. This suggests that the in vivo 231 efficacy of this agent may be inoculum-dependent. 232 DISCUSSION 233 Miltefosine, an alkyl phosphocholine, has been used as therapy for various forms 234 of leishmaniasis, and has recently garnered attention for its potential use against invasive 235 fungal infections, including cryptococcosis. Current interest in this agent is due to the in 236 vitro activity against Cryptococcus species and dermatophytes, and the clinical success 237 that was reported in one patient treated with miltefosine in combination with other 238 antifungal agents for Scedosporium prolificans osteomyelitis (13, 28). Additionally, 239 studies have also reported in vivo efficacy of miltefosine monotherapy in a murine model 240 of disseminated cryptococcosis and as well as meningitis due to Naegleria fowleri (14, 241 29). The mechanism by which miltefosine inhibits fungi has also been elucidated. 242 Following incorporation into yeast, miltefosine rapidly penetrates the mitochondrial inner 243 membrane where it inhibits cytochrome c oxidase and disrupts membrane potential 244 leading to apoptosis-like cell death (30). 245 Cryptococcal meningoencephalitis is a common manifestation of disseminated 246 disease caused by C. neoformans, and there is a clear need to develop new antifungal 247 agents as well as evaluate available drugs for the treatment of this invasive mycosis; as 248 such, we sought to evaluate the efficacy of miltefosine in our established murine model 249 of this CNS infection. Based on the in vitro activity that we observed and that reported 250 by others, as well as previous reports of in vivo efficacy, we expected to see benefit with 251 the use of this agent. However, the results were negative in the majority of our 252
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

12
experiments, as miltefosine monotherapy did not improve survival our animal models of 253 cryptococcal meningoencephalitis or disseminated cryptococcosis caused by two 254 different C. neoformans isolates. In contrast, efficacy was observed with the clinically 255 available antifungals fluconazole and amphotericin B. In addition, miltefosine failed to 256 reduce fungal burden within the brains or lungs of these animals, and did not improve the 257 effectiveness of therapy when used in combination. The exact reason for this lack of in 258 vivo efficacy in our models is unclear as in vitro activity was observed using the CLSI 259 methodology for antifungal susceptibility testing against yeasts. Furthermore, the MIC 260 values we observed against the two C. neoformans isolates were in agreement to those 261 reported by others (29). However, the in vitro potency of this agent was significantly 262 reduced when albumin was added to the growth medium. Miltefosine is highly protein 263 bound (~95%) (2, 10), which could partially explain the lack of in vivo activity we 264 observed, as there may be only a small fraction of unbound drug available to inhibit the 265 organism at the site of infection. In addition, the effectiveness against disseminated 266 cryptococcosis appeared to be dependent on the size of the infecting inoculum as a trend 267 towards improved survival was observed when a lower inoculum was used to establish 268 infection. The clinical relevance of this finding is unknown, but it is noteworthy that 269 miltefosine lacked activity when mice were challenged with our standard inocula in the 270 cryptococcal meningoencephalitis and disseminated cryptococcosis models while the 271 clinically available agents fluconazole and amphotericin B remained effective. 272 A limitation of this study is that we did not evaluate the pharmacokinetics of 273 miltefosine in these animal models, nor did we evaluate different dosing strategies in an 274 effort to potentially improve efficacy. Thus, it is unknown whether effective 275
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
13
concentrations were achieved either within the bloodstream or at the sites of infection, 276 including the CNS. However, other investigators have reported favorable 277 pharmacokinetics for miltefosine in mice and other animal, including good oral 278 bioavailability (82% to 95%), a long terminal half-life (range 73 to 104 hours), with 279 extensive tissue distribution, including the brain (1, 5, 21). In addition, peak miltefosine 280 serum concentrations above the MICs for the two C. neoformans isolates used in our 281 study and high AUC values have been reported in mice that received doses similar to 282 those we tested (1). Furthermore, in our initial experiment with miltefosine, acute 283 toxicity was observed in several mice following a single dose of 60 mg/kg. Thus, it is 284 unlikely that the concentrations that we achieved were suboptimal. 285 Although the results of this study do not eliminate the potential utility of 286 miltefosine for the treatment of invasive fungal infections, including those caused by 287 Cryptococcus species, caution is warranted. Additional concerns that may limit the 288 clinical use of this agent include dose-limiting side effects (i.e., nausea, vomiting, and 289 loss of appetite) reported in humans as well as the embryotoxic and teratogenic effects 290 that have been observed in animals (21). Further work is also needed in order to 291 determine the potential role of miltefosine in the treatment of invasive mycoses prior to 292 the wide spread clinical use of this agent. 293 294 ACKNOWLEDGEMENTS 295 The authors would like to thank Marcos Olivo with his assistance with the animal models. 296 This work was supported by a contract from the National Institutes of Health / National 297
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

14
Institute of Allergy and Infectious Diseases (N01-AI-25475) to TFP. TCS is a Sydney 298 Medical School Foundation Fellow. 299 300 TRANSPARENCY DECLARATION 301 NPW has received research support from Pfizer, Schering-Plough, Merck, Basilea, and 302 Astellas, and has served on advisory boards for Merck, Astellas, Toyama, and Viamet. 303 TFP has received research grants to UT Health Science Center San Antonio from Astellas, 304 Basilea, Merck, and Pfizer, and as a consultant for Astellas, Basilea, Merck, Pfizer, and 305 Toyama. All other authors: no conflicts. 306 307 REFERENCES 308 1. Arndt, D., R. Zeisig, I. Fichtner, A. D. Teppke, and A. Fahr. 1999. 309
Pharmacokinetics of sterically stabilized hexadecylphosphocholine liposomes 310 versus conventional liposomes and free hexadecylphosphocholine in tumor-free 311 and human breast carcinoma bearing mice. Breast Cancer Res Treat 58:71-80. 312
2. Berman, J., A. D. Bryceson, S. Croft, J. Engel, W. Gutteridge, J. Karbwang, H. 313 Sindermann, J. Soto, S. Sundar, and J. A. Urbina. 2006. Miltefosine: issues to be 314 addressed in the future. Trans R Soc Trop Med Hyg 100 Suppl 1:S41-44. 315
3. Bhattacharya, S. K., T. K. Jha, S. Sundar, C. P. Thakur, J. Engel, H. Sindermann, 316 K. Junge, J. Karbwang, A. D. Bryceson, and J. D. Berman. 2004. Efficacy and 317 tolerability of miltefosine for childhood visceral leishmaniasis in India. Clin 318 Infect Dis 38:217-221. 319
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

15
4. Bhattacharya, S. K., P. K. Sinha, S. Sundar, C. P. Thakur, T. K. Jha, K. Pandey, V. 320 R. Das, N. Kumar, C. Lal, N. Verma, V. P. Singh, A. Ranjan, R. B. Verma, G. 321 Anders, H. Sindermann, and N. K. Ganguly. 2007. Phase 4 trial of miltefosine for 322 the treatment of Indian visceral leishmaniasis. J Infect Dis 196:591-598. 323
5. Breiser, A., D. J. Kim, E. A. Fleer, W. Damenz, A. Drube, M. Berger, G. A. 324 Nagel, H. Eibl, and C. Unger. 1987. Distribution and metabolism of 325 hexadecylphosphocholine in mice. Lipids 22:925-926. 326
6. Chayakulkeeree, M., and J. R. Perfect. 2006. Cryptococcosis. Infect Dis Clin 327 North Am 20:507-544, v-vi. 328
7. CLSI. 2008. Reference method for broth dilution antifungal susceptibility testing 329 of yeasts; Approved standard - Third Edition (M27-A3). Clinical and Laboratory 330 Standards Institute, Wayne, PA. 331
8. Diamond, D. M., M. Bauer, B. E. Daniel, M. A. Leal, D. Johnson, B. K. Williams, 332 A. M. Thomas, J. C. Ding, L. Najvar, J. R. Graybill, and R. A. Larsen. 1998. 333 Amphotericin B colloidal dispersion combined with flucytosine with or without 334 fluconazole for treatment of murine cryptococcal meningitis. Antimicrob Agents 335 Chemother 42:528-533. 336
9. Ding, J. C., M. Bauer, D. M. Diamond, M. A. Leal, D. Johnson, B. K. Williams, 337 A. M. Thomas, L. Najvar, J. R. Graybill, and R. A. Larsen. 1997. Effect of 338 severity of meningitis on fungicidal activity of flucytosine combined with 339 fluconazole in a murine model of cryptococcal meningitis. Antimicrob Agents 340 Chemother 41:1589-1593. 341
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

16
10. Dorlo, T. P., P. P. van Thiel, A. D. Huitema, R. J. Keizer, H. J. de Vries, J. H. 342 Beijnen, and P. J. de Vries. 2008. Pharmacokinetics of miltefosine in Old World 343 cutaneous leishmaniasis patients. Antimicrob Agents Chemother 52:2855-2860. 344
11. Dromer, F., S. Mathoulin-Pelissier, O. Launay, and O. Lortholary. 2007. 345 Determinants of disease presentation and outcome during cryptococcosis: the 346 CryptoA/D study. PLoS Med 4:e21. 347
12. Jha, T. K., S. Sundar, C. P. Thakur, P. Bachmann, J. Karbwang, C. Fischer, A. 348 Voss, and J. Berman. 1999. Miltefosine, an oral agent, for the treatment of Indian 349 visceral leishmaniasis. N Engl J Med 341:1795-1800. 350
13. Kesson, A. M., M. C. Bellemore, T. J. O'Mara, D. H. Ellis, and T. C. Sorrell. 351 2009. Scedosporium prolificans osteomyelitis in an immunocompetent child 352 treated with a novel agent, hexadecylphospocholine (miltefosine), in combination 353 with terbinafine and voriconazole: a case report. Clin Infect Dis 48:1257-1261. 354
14. Kim, J. H., S. Y. Jung, Y. J. Lee, K. J. Song, D. Kwon, K. Kim, S. Park, K. I. Im, 355 and H. J. Shin. 2008. Effect of therapeutic chemical agents in vitro and on 356 experimental meningoencephalitis due to Naegleria fowleri. Antimicrob Agents 357 Chemother 52:4010-4016. 358
15. Larsen, R. A., M. A. Leal, and L. S. Chan. 1990. Fluconazole compared with 359 amphotericin B plus flucytosine for cryptococcal meningitis in AIDS. A 360 randomized trial. Ann Intern Med 113:183-187. 361
16. Lortholary, O., G. Poizat, V. Zeller, S. Neuville, A. Boibieux, M. Alvarez, P. 362 Dellamonica, F. Botterel, F. Dromer, and G. Chene. 2006. Long-term outcome of 363
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

17
AIDS-associated cryptococcosis in the era of combination antiretroviral therapy. 364 AIDS 20:2183-2191. 365
17. NAS. 1996. Guide for the care and use of laboratory animals. National Academy 366 Press, Washington, D.C. 367
18. Park, B. J., K. A. Wannemuehler, B. J. Marston, N. Govender, P. G. Pappas, and 368 T. M. Chiller. 2009. Estimation of the current global burden of cryptococcal 369 meningitis among persons living with HIV/AIDS. AIDS 23:525-530. 370
19. Perfect, J. R., W. E. Dismukes, F. Dromer, D. L. Goldman, J. R. Graybill, R. J. 371 Hamill, T. S. Harrison, R. A. Larsen, O. Lortholary, M. H. Nguyen, P. G. Pappas, 372 W. G. Powderly, N. Singh, J. D. Sobel, and T. C. Sorrell. 2010. Clinical practice 373 guidelines for the management of cryptococcal disease: 2010 update by the 374 Infectious Diseases Society of America. Clin Infect Dis 50:291-322. 375
20. Saag, M. S., W. G. Powderly, G. A. Cloud, P. Robinson, M. H. Grieco, P. K. 376 Sharkey, S. E. Thompson, A. M. Sugar, C. U. Tuazon, J. F. Fisher, and et al. 1992. 377 Comparison of amphotericin B with fluconazole in the treatment of acute AIDS-378 associated cryptococcal meningitis. The NIAID Mycoses Study Group and the 379 AIDS Clinical Trials Group. N Engl J Med 326:83-89. 380
21. Sindermann, H., and J. Engel. 2006. Development of miltefosine as an oral 381 treatment for leishmaniasis. Trans R Soc Trop Med Hyg 100 Suppl 1:S17-20. 382
22. Soto, J., B. A. Arana, J. Toledo, N. Rizzo, J. C. Vega, A. Diaz, M. Luz, P. 383 Gutierrez, M. Arboleda, J. D. Berman, K. Junge, J. Engel, and H. Sindermann. 384 2004. Miltefosine for new world cutaneous leishmaniasis. Clin Infect Dis 385 38:1266-1272. 386
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
18
23. Soto, J., J. Toledo, P. Gutierrez, R. S. Nicholls, J. Padilla, J. Engel, C. Fischer, A. 387 Voss, and J. Berman. 2001. Treatment of American cutaneous leishmaniasis with 388 miltefosine, an oral agent. Clin Infect Dis 33:E57-61. 389
24. Soto, J., J. Toledo, L. Valda, M. Balderrama, I. Rea, R. Parra, J. Ardiles, P. Soto, 390 A. Gomez, F. Molleda, C. Fuentelsaz, G. Anders, H. Sindermann, J. Engel, and J. 391 Berman. 2007. Treatment of Bolivian mucosal leishmaniasis with miltefosine. 392 Clin Infect Dis 44:350-356. 393
25. Sundar, S., T. K. Jha, C. P. Thakur, J. Engel, H. Sindermann, C. Fischer, K. Junge, 394 A. Bryceson, and J. Berman. 2002. Oral miltefosine for Indian visceral 395 leishmaniasis. N Engl J Med 347:1739-1746. 396
26. Sundar, S., F. Rosenkaimer, M. K. Makharia, A. K. Goyal, A. K. Mandal, A. 397 Voss, P. Hilgard, and H. W. Murray. 1998. Trial of oral miltefosine for visceral 398 leishmaniasis. Lancet 352:1821-1823. 399
27. Thompson, G. R., 3rd, N. P. Wiederhold, L. K. Najvar, R. Bocanegra, W. R. 400 Kirkpatrick, J. R. Graybill, and T. F. Patterson. 2012. A murine model of 401 Cryptococcus gattii meningoencephalitis. J Antimicrob Chemother 67:1432-1438. 402
28. Tong, Z., F. Widmer, T. C. Sorrell, Z. Guse, K. A. Jolliffe, C. Halliday, O. C. Lee, 403 F. Kong, L. C. Wright, and S. C. Chen. 2007. In vitro activities of miltefosine and 404 two novel antifungal biscationic salts against a panel of 77 dermatophytes. 405 Antimicrob Agents Chemother 51:2219-2222. 406
29. Widmer, F., L. C. Wright, D. Obando, R. Handke, R. Ganendren, D. H. Ellis, and 407 T. C. Sorrell. 2006. Hexadecylphosphocholine (miltefosine) has broad-spectrum 408
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
19
fungicidal activity and is efficacious in a mouse model of cryptococcosis. 409 Antimicrob Agents Chemother 50:414-421. 410
30. Zuo, X., J. T. Djordjevic, J. Bijosono Oei, D. Desmarini, S. D. Schibeci, K. A. 411 Jolliffe, and T. C. Sorrell. 2011. Miltefosine induces apoptosis-like cell death in 412 yeast via Cox9p in cytochrome c oxidase. Mol Pharmacol 80:476-485. 413
414 415 416 417 418 419 420 421 422 423 424 425 426 427 428 429 430 431
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

20
FIGURE AND TABLE LEGENDS 432 Figure 1. Survival curves in mice inoculated intracranially with C. neoformans 433 USC1597 at 1900 - 2800 colony-forming units (CFU)/animal. Antifungal monotherapy 434 therapy with miltefosine (MTF), fluconazole (FLC), amphotericin B (AMB) or 435 combination therapy began one day post challenge (A, B, & C) and continued for 10 days. 436 N = 19 - 20 mice per group for untreated controls, FLC, and AMB, and 8 - 10 mice per 437 MTF dose. The early initiation of MTF and AMB or combination therapy at 1 hour post 438 challenge was also evaluated (D). Daily MTF therapy continued for 10 days and AMB 439 was administered for only 2 doses. N = 9 - 10 mice per group. *P-value < 0.05 for 440 median survival compared to untreated controls. §P-value < 0.05 for percent survival at 441 study endpoint compared to untreated controls. 442 Figure 2. Survival curves in mice inoculated intracranially with C. neoformans H99 at 443 1335 colony-forming units CFU/animal. Antifungal therapy with miltefosine (MTF) 444 began 1 hour following infection, while therapy with fluconazole (FLC) and 445 amphotericin B (AMB) was initiated 1 day post challenge. Therapy with MTF at doses 446 of 1.8, 3.6, & 7.2 mg/kg (A) continued through day 4, and therapy with MTF at 15 & 45 447 mg/kg (B), or FLC and AMB (C) continued through day 10. N = 10 mice per group. *P-448 value < 0.05 for median survival compared to untreated controls. §P-value < 0.05 for 449 percent survival at study endpoint compared to untreated controls. 450 Figure 3. Survival curves in mice inoculated intravenously with C. neoformans 451 USC1597 at 0.54 - 1.6 x 105 CFU/animal. In the monotherapy experiment (A & B), 452 miltefosine (MTF) began 1 hour post challenge, while fluconazole (FLC) and 453 amphotericin B (AMB) were initiated 1 day post challenge. Therapy with MTF at doses 454
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

21
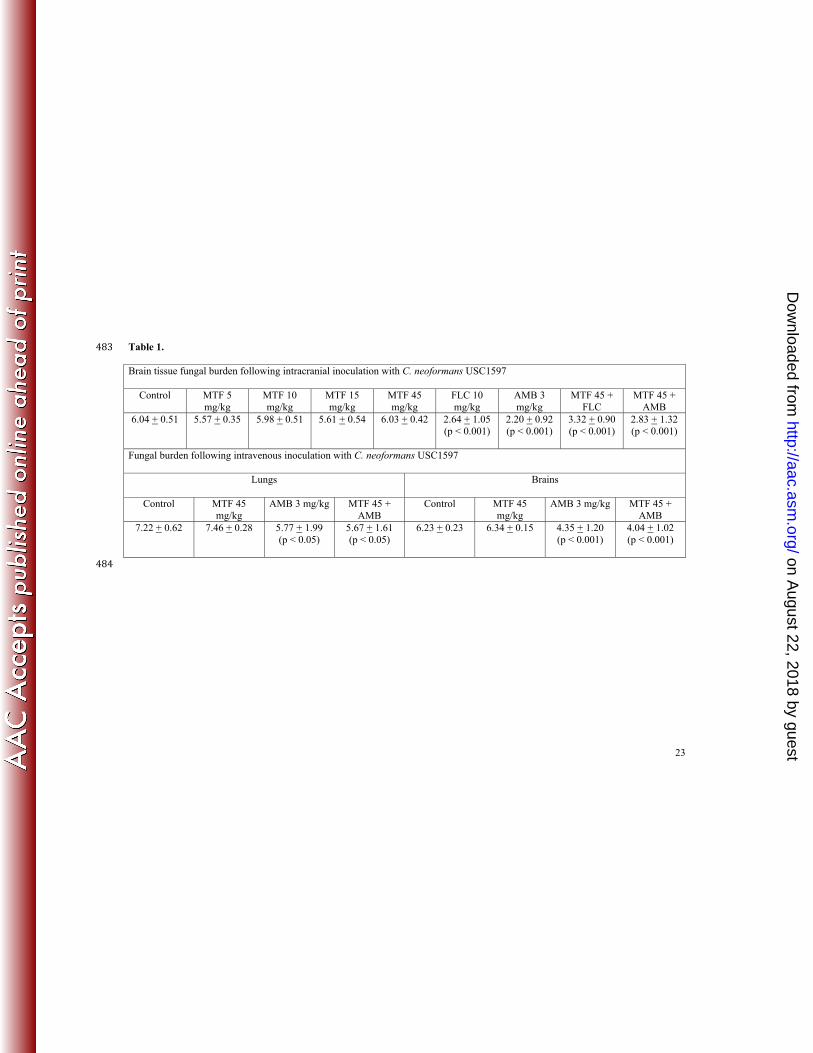
of 1.8, 3.6, & 7.2 mg/kg continued through day 4, and therapy with MTF at 15 & 45 455 mg/kg, FLC, and AMB continued through day 10. For combination therapy experiment 456 (C - E), MTF 45 mg/kg was combined with AMB. N = 10 mice per group. *P-value < 457 0.05 for median survival compared to untreated controls. §P-value < 0.05 for percent 458 survival at study endpoint compared to untreated controls. 459 Figure 4. Survival curves in mice inoculated intravenously with C. neoformans H99 at 460 0.54 - 6.1 x 105 CFU/animal. Treatment with miltefosine (MTF) began 1 hour post 461 challenge, while fluconazole (FLC) and amphotericin B (AMB) were started 1 day after 462 infection. Therapy with MTF at doses of 1.8, 3.6, & 7.2 mg/kg continued through day 4, 463 and therapy with MTF at 15 & 45 mg/kg, FLC, and AMB continued through day 10. N = 464 10 mice per group. *P-value < 0.05 for median survival compared to untreated controls. 465 §P-value < 0.05 for percent survival at study endpoint compared to untreated controls. 466 Figure 5. Survival curves in untreated mice challenged intravenously with C. 467 neoformans H99 at different inoculum levels (A), or with a single inoculum (4.0 x 103 468 CFU/animal) and treated with miltefosine (MTF) (B). MTF was initiated 1 hour post 469 challenge and continued through day 4. N = 10 mice per group. 470 Table 1. Fungal burden (mean + SD log10 CFU/gram) in the brains or lungs of mice with 471 cryptococcal meningoencephalitis or disseminated cryptococcosis following intracranial 472 or intravenous inoculation with C. neoformans USC1597. In the cryptococcal 473 meningoencephalitis model, antifungal therapy with miltefosine (MTF), fluconazole 474 (FLC), or amphotericin B (AMB) was continued through day 7, and brains were collected 475 on day 8 for fungal burden quantification. N = 19 - 20 mice per group for untreated 476 controls, FLC, and AMB, and 8 - 10 mice per MTF dose. In the disseminated 477
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

22
cryptococcosis model, MTF therapy was continued through day 7 while AMB was 478 administered for 2 doses. The lungs and brains were collected on day 8 for fungal burden 479 quantification (CFU/g of tissue). N = 10 mice per group. P-value versus untreated 480 controls and all miltefosine monotherapy. 481 482
on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
23
Table 1. 483 Brain tissue fungal burden following intracranial inoculation with C. neoformans USC1597
Control MTF 5 mg/kg
MTF 10 mg/kg
MTF 15 mg/kg
MTF 45 mg/kg
FLC 10 mg/kg
AMB 3 mg/kg
MTF 45 + FLC
MTF 45 + AMB
6.04 + 0.51 5.57 + 0.35 5.98 + 0.51 5.61 + 0.54 6.03 + 0.42 2.64 + 1.05 (p < 0.001)
2.20 + 0.92 (p < 0.001)
3.32 + 0.90 (p < 0.001)
2.83 + 1.32 (p < 0.001)
Fungal burden following intravenous inoculation with C. neoformans USC1597
Lungs
Brains
Control MTF 45 mg/kg
AMB 3 mg/kg MTF 45 + AMB
Control MTF 45 mg/kg
AMB 3 mg/kg MTF 45 + AMB
7.22 + 0.62
7.46 + 0.28 5.77 + 1.99 (p < 0.05)
5.67 + 1.61 (p < 0.05)
6.23 + 0.23 6.34 + 0.15 4.35 + 1.20 (p < 0.001)
4.04 + 1.02 (p < 0.001)
484 on August 22, 2018 by guest
http://aac.asm.org/
Dow
nloaded from