abc consulting and management brochure, 2015
TRANSCRIPT

Advisory Board
Consulting and Management

Image credits: Cover and page 1, iStock; all others by Nini Jin, The Advisory Board Company.

Advisory Board Consulting and Management | 1
We specialize in transforming health care across the major areas where our clients are focused: growth, margins, physician alignment, and the transition to value—and everything in between.
Partner with people who transform health care.

2 | The Advisory Board Company
Health care is in the midst of transformation. With an eye on the horizon, we’ve spent over five years transforming ourselves to better serve our health care partners during this time.
Transforming ahead of the curve

Advisory Board Consulting and Management | 3
evolving to meet emerging DEMANDS
1998Southwind Health Partners, LLC, is founded by John Deane. It grows over 10 years to become the leading firm in physician alignment and employment.
2009The Advisory Board Company acquires Southwind Health Partners, retaining 100% of the consulting team and legacy leadership team, who continue to oversee Advisory Board Consulting and Management.
PHYSICIAN ALIGNMENT
2009Recognizing the shift occurring in the industry, we become pioneers in developing the clinically integrated network. That was just the start. Over the next five years, we continue to add new capabilities to support the development of all value-based programs, such as advanced primary care, accountable care organizations, and population health management.
TRANSITION TO VALUE
2014Support for our clients’ growth initiatives has always been a part of our services. Over time, we see that our clients need help identifying the strategies that would ensure their growth in a changing, more consumer-driven market. To address this need, we launch a new corporate strategy offering fueled by top-rate talent.
GROWTH
2012As industry and market changes increased their threat to health system margins, we revitalize our hospital-focused consulting services with margins in mind. Merging hospital and physician alignment services, and with an eye toward the transition to value, we begin offering comprehensive support to help health systems achieve sustainable margins.
MARGINS
2015 Recognizing the huge investments being made in IT, we acquire Clinovations, a physician-led consulting practice focused on ensuring that health systems see the return on their investments. With the Clinovations team, we provide implementation strategy and planning, in addition to clinical workflow and technology optimization.

4 | The Advisory Board Company
strong, action-oriented approachextensive knowledge
consistent, predictable, and positive resultsfacilitating transformation, driving value
deep relationships500 + management consultants
Develop deep relationships rooted in trust, with clients, physicians, employees, and other stakeholders
Communicate bilingually to translate needs between clinicians and administrators, and to ensure full transparency
Create positive change through innovation and a strong, action-oriented approach
Retain talent with deep, extensive knowledge in health care, including trends, strategies, and operating principles
Deliver consistent, predictable, and positive results for every engagement
Maintain integrity, as paramount, in every interaction
steadfast COMMITMENT to core principles

Advisory Board Consulting and Management | 5
operators and clinicianshospital, physician practice, payer,
and accountable care settingintegrity and innovation
full transparency2,000 + engagements —50 states
unmatched bench STRENGTH
Averaging 20 years of experience in health care leadership, our team of over 500 includes both management executives and clinicians who have completed more than 2,000 engagements for clients in all 50 states.
We have subject matter experts in operational and clinical areas, with experience in the hospital, physician practice, payer, and accountable care settings.
Most importantly, however, our management consultants are skilled in transformation. Tackling extensive change is our true specialty, and why we can drive value for a 5:1 average ROI.

6 | The Advisory Board Company
We’re not vendors. We’re partners. Our success depends on yours, so we stay right beside you until we reach your goal.
partnership-driven ENGAGEMENTS
Introducing Advisory Board Consulting and Management | 7
Partnership is defined as taking part in an activity with another or others, especially in a business or company with shared risks and profits.
That is precisely what our consulting and management services are designed to be—a partnership. We make it our mission to arm your team with the knowledge and skills needed to maintain results and continue making progress long after our exit.
We partner with clients as strategists, analysts, implementation leaders, and interim executives. With a management model that has been in place for nearly 20 years, we know what it takes to design a partnership that can truly transform.

8 | The Advisory Board Company
effecting positive TRANSFORMATION
Helping you transformto face health care’s most robust challenges—while providing support for every problem, at every level.

ACOs • Advanced Primary Care Practice • Capacity
and Patient Flow • Care Management Program • Clinical
Care Models • Clinical Integration • Co-management
• Community Health Needs Assessment • Corporate
Strategy • Cost per Episode • EHR Optimization • Fair
Market Value • Health Insurance Exchanges • ICD-10
• IT Investment • Mergers and Acquisitions • Network
Development • Patient Access • Patient Experience •
Payment Transformation • Physician Compensation •
Physician Employment • Physician Needs Assessment
• Population Health • Referral Management • Regional
Partnerships • Retail Partnerships • Revenue Maximization •
Supply Costs • Variation • Workforce Management • P
Clinical Documentation • Clinical Workflow • Co-management •
Cost per Episode • Mergers and Acquisitions • Referral
Management • Retail Partnerships • Health Insurance
Access • Referral Management • Revenue Maximization
PHYSICIANALIGNMENT
MARGINS
TRANSITION TO VALUE
GROWTH
Introducing Advisory Board Consulting and Management | 9

10 | The Advisory Board Company
PHYSICIAN ALIGNMENT isn’t about collecting relationships. It’s about transforming them.

Advisory Board Consulting and Management | 11
CLIENT PROFILES
PHYSICIAN ALIGNMENT TRANSITION TO VALUE MARGINS GROWTH
As health systems have evolved, the physician relationship has taken on both new complexity and significance. Separate structures and multiple alignment models are often at play in one entity, and bringing harmony to this discord is one of the paramount challenges in health care today.
Innovation stalls when physician alignment is conducted as a transaction. But health systems can prosper when physicians are empowered as leaders and partners, working collectively to achieve a common vision.
A culture and care delivery model that is driven by those relationships positions the enterprise for excellence. We work side-by-side with physicians and corporate leadership to design and operationalize better systems and stronger brands.
Consolidated legacy medical groups from acquired health systems into a single, integrated multispecialty group practice.
Transformed physician alignment processes
Developed and employed a clinical integration strategy aimed at creating physician loyalty by driving cost reductions, growth, and commercial business.
Developed CI programs with 2,300+ participating physicians
Quickly established a new base of pediatric physicians and surgeons to support the revitalization of a children’s hospital after a long-term affiliate disengaged for a competing initiative.
Built an integrated pediatric delivery network
Created a consistent, high-quality patient experience throughout the entire system by aligning physicians and staff on operations, customer service, branding, and management.
Improved patient standards by 38%
Large academic medical center
Large health system, serving more than 6 million annually
Community children’s hospital
Private, not-for-profit academic medical center
12 | The Advisory Board Company
1. The network isn’t truly physician-led The legal rules for organizing CI networks require that physicians take a leadership role in the network, although the hospital can set up the infrastructure and the network itself can provide administrative support. This can be a tricky balance to achieve, because too much independence can lead to redundancy or even rivalry among care management efforts. In some markets, we’ve seen big inefficiencies develop when the CI network is not sufficiently aligned with health system administrators and other system-affiliated physician entities, such as employed medical groups. However, the CI network needs to be sufficiently independent and physician-led that physicians want to participate. So when a health system sets up a CI network, they also need to make sure that there are true physician champions, including independent physicians, not just at the table but driving the discussion. Otherwise, it could be a great party, but nobody will come. As I’ve told more than one client: “If these physicians were natural joiners, they would have joined something already!”
2. The CI network never gets appropriate contracts—and the hospital doesn’t help A CI network works only if payers or employers agree to provide performance-based incentives to the network. And the reality is, not every market has payers or employers eager to create those kinds of contracts. How can CI networks thrive in a market that isn’t on the forefront of value-based reimbursement? Many health systems start by creating incentives around caring for their own employee population. But beyond that, the health
system needs to help bring payers to the table—and be willing to use their analytics, their expertise, and even concessions on other contract terms to get a favorable CI contract in place. When my Advisory Board colleagues and I work with health systems on clinical integration strategy, we typically create a thorough economic analysis to understand the full impact of the CI network. That way, the health system can make an informed decision about how hard to fight, and which CI terms to fight for, in the context of overall payer contracting negotiations.
3. The financial case for the CI network relies too heavily on shared savings contracts Although we haven’t seen many shared savings-related failures yet, the reality of shared savings programs, including MSSP, is that not all participants will be able to generate the anticipated savings. Across the next several years, CI networks that are banking on shared savings payments to bolster the case for participation are likely to see physicians back out if the shared savings payments don’t live up to initial projections. We advise CI programs to think about shared savings as “maybe money”—nice if it materializes, but not what anyone should be relying on to get, or keep, physicians engaged in performance improvement efforts. The good news is that each of these failure points is preventable with planning, effort, and commitment. But health systems court disappointment when they create a clinically integrated network without sufficiently engaging physicians, committing to drum up the necessary contracts, or preparing for the dangers of risk-based contracts.
Why good clinical integration networks fail—and what to do about it
BY LAURIE SPRUNG, PHD, EXECUTIVE VICE PRESIDENT
CLINICAL INTEGRATION IS ONE OF THE FEW EFFECTIVE models we’ve found for getting physicians and hospitals to work together on improving care and to be rewarded for their success. Not all CI networks that look good on paper end up succeeding in the real world, though. Here are three reasons we see good CI networks fail—and how to position yourself for the best chance of success.
Our perspective on the issues affecting PHYSICIAN ALIGNMENT

Advisory Board Consulting and Management | 13
The biggest mistake health systems make in acquiring physician practices
BY ANTHONY D’EREDITA, EXECUTIVE VICE PRESIDENT
WHEN I WORK WITH HEALTH SYSTEMS on acquiring physician practices, the biggest mistake I see them make is to ignore the culture of the practices they’re looking to acquire. In fact, I’ve had clients do this intentionally, because they believe that giving the practices “autonomy” is more important than cultural integration.
They couldn’t be more wrong. Culture is the most effective tool a health system can use to ensure return on investment in acquired physician practices.
When I say culture, I’m not talking about dress code or taste in music. I mean the shared values, expectations, and identity that determine how practices work together. When you acquire a practice, you’re acquiring an entity that most likely has its own characteristics that define its culture. And they may or may not blend well with yours.
Quantifying cultureCulture is often talked about, but mostly as a “soft” attribute. But culture is a tangible, quantifiable thing. It defines all of the big ticket items that impact the medical group’s financial performance and its revenue contributions to the health system at large.
I had one health system client that pursued acquisitions without prioritizing cultural fit. The newly acquired practices did not share the same cultural value of expanded operating hours, a previous staple of the acquiring entity. As a result, they eroded patient access channels. After significantly slowing new patient growth, the practice is now undergoing the painful process modifying physician behavior and post-integration cultural assimilation.
Another recent client assumed employment would address “leakage” and clinical coordination to keep costs within the health system’s lower cost structure. When that didn’t happen, it contributed to an increase in cost, which jeopardized a new shared savings incentive program. To fix the issue, we had to bring their cultural values around clinical integration front and center. Over time the clinical coordination increased as culture assimilated.
My final example is a positive situation in which the client tested the cultural fit of a prospective orthopedic partner. They explored a few key strategic objectives such as standardized order sets and care protocols within an established program. When the practice refused, the client prioritized cultural fit over potential short-term program expansion, so they aligned with other community physician and grew the program in both a clinically integrated and cost-effective manner.
A final and less quantifiable contribution is physician engagement and leadership. Integrating your recently acquired practices to create a comprehensive care delivery system requires change, and peer-to-peer facilitated change management is a far better method. And when physicians truly feel like part of the system, things that seem like complex issues naturally fall into place.
Center your acquisition strategy on cultureMaking culture an important part of the acquisition process requires knowing what your culture is, being able to articulate it so others understand it, and making an assessment of cultural fit an explicit part of the acquisition process.
In their study High-Performance Medical Group, Health Care Advisory Board researchers identified a number of tactics for ensuring cultural fit, tactics that really ought to be used more broadly. For example, the Gundersen Lutheran health system in Wisconsin created a “Medical Group Compact” document that articulates the health system’s cultural priorities and how that translated to physician behavior.
Another health system, Minneapolis-based Fairview, actually created an assessment tool for scoring potential practice acquisitions on different attributes of cultural fit.
Health systems need a physician acquisitions strategy that’s more than purchasing and aggregating practices. Creating a comprehensive culture and expanding that culture once it’s established, should drive your M&A strategy.

14 | The Advisory Board Company
The key to success in health care’s TRANSITION TO VALUE is knowing how to transform at the core, without dismantling the whole structure.

Advisory Board Consulting and Management | 15
CLIENT PROFILES
PHYSICIAN ALIGNMENT TRANSITION TO VALUE MARGINS GROWTH
The stakes are high on the path to value, where the challenge is to find solid financial footing without dropping the ball on current revenue. Many organizations invest in technology, staff, and contracting strategies—components of population health management. But disparate pieces won’t add up to a holistic and integrated model.
Organizations need to understand how transformation efforts will impact financial performance, with a plan to pace out new initiatives over time. They require a tailored framework for care delivery that fits within the local market—and that sets them up for future growth.
Partner with a team that travels with ease across payer, physician, and patient worlds—and that identifies the no-regrets investments while crafting a blueprint for transition to a new model.
Developed a clinically integrated network, and created a population health services organization to serve the CI network and other key stakeholders in an effort to maximize the health system’s market position, ROI, and overall care delivery.
Identified $60M opportunity in transition to value
Created a new NEQCA-affiliated physician enterprise and supportive management services organization to integrate its best-of-class population health resources with best-of-class practice management infrastructure.
Redesigned hospital-based outpatient clinic operations
Enhanced patient care and improved physician recruitment, retention, and alignment by establishing a patient centered medical home, CI network, and sustainable ACO strategy.
Decreased inpatient admissions by 15% in one year
Developed a population health services organization to support the system and its various business units, and revised the existing care delivery model to manage the population served.
Built the infrastructure for population health management
Integrated health system
Top academic medical center
Regional health system
Pilot program focused on patient care

16 | The Advisory Board Company
What 650,000 air miles taught Jim Bonnette about accountable care
Q&A WITH JIM BONNETTE, MD, EXECUTIVE VICE PRESIDENT
Q: Can you talk a bit about your background? It’s awfully diverse—you got into health care as a physician, initially.
JB: I began practicing as an internist in California, which was for a long time a hotbed of managed care. And when things got bad in the 1990s, I got the worst of it. I saw it both from the practicing side as well as having been at an HMO. That helped me get a better perspective on care delivery—namely, what was effective and what wasn’t working.
Q: You’re not just a MD, of course. You’ve also been a consultant and executive, too.
JB: Throughout my career, I’ve worked in supply chain, clinical IT, and risk-management capacities, among other areas. I’ve had exposure to many different opportunities for change. In my last position, I built out a team of consultants across international offices over a period of three years. We did work all across the U.S. for accountable care and different care model implementations, and then did the same kind of work in the United Kingdom, France, Singapore, Indonesia, Saudi Arabia, Kuwait, and South America.
Q: That sounds like a lot of travel.
JB: I flew 650,000 miles last year...a bit too many.
Q: On your trips abroad, did you see one country that stood out as a leader in accountable care?
JB: I’ve seen good things in each country, but nobody’s got a complete system. Some things that are workable in certain cultures aren’t workable in ours, and vice versa. There are two common underlying problems, however. First, every country has a rate of growth of their expenditure in health care that they can’t tolerate. Second, the way we train our doctors here in the United States does not encourage or enable physicians to manage populations with chronic problems. No country that I’ve seen has set up effective systems to really manage chronically ill patients. None. But we have really good examples in the U.S., where we’ve experimented and created incredibly effective ways to care for people with chronic diseases. They are models that can be replicated, it’s just that most systems don’t know how to do it.
Q: Of course, health care leaders have always cared about planning and forecasting. Can you explain what’s different about setting a strategy today?
JB: In the current health care climate, hospitals and health systems are being pushed to make one change after another. It’s not enough to simply react to each new challenge. Those executives are looking to map out a long-term, cohesive plan for how to deal with the changing market. That’s the work Advisory Board Consulting and Management is really designed to do—build a road map for any organization grappling with the change in our industry. Given that we [in the health care sector] all buy into the necessity for change, leaders need to start asking, “In my organization, what do I have to do to get from where we are to where we need to be?”
Q: What about hospitals that hesitate to move toward accountable care?
JB: When I was talking about this stuff 10 years ago, I was getting all kinds of pushback. Funny, but now I don’t ever get anyone pushing back about the need to do it. What I get now are questions about how to do it. I typically recommend the patient-centered discussion: How do we best serve a population of patients?
Our perspective on the issues affecting TRANSITION TO VALUE

Advisory Board Consulting and Management | 17
How math makes population health more digestible
BY LAURIE SPRUNG, PHD, EXECUTIVE VICE PRESIDENT AND ERIC PASSON, EXECUTIVE VICE PRESIDENT
OUR CLIENTS ARE AT VARIOUS STAGES of population health management. Some are currently doing nothing, because their region isn’t experiencing any change. Others are trying to lay the groundwork and plan for a transition, but there’s no significant movement. Then there are more progressive systems that either want to get ahead of the movement, or have competitive issues that necessitate risk-based contracts.
What we’re finding across these health systems isn’t a need for innovation in clinical work. Clinicians are doing that.
What the health system needs now is to understand the math behind population health management. Or rather, what’s the economic model that will support population health goals without depleting the fee-for-service business that drives margins today?
Understand your population targetsThe first step to understanding the right economic model is to identify the right populations—or subsets of your whole population—to target. With that understanding, you can identify the resources you need to respond to the target populations, which includes organizing physicians and other caregivers around their conditions.
We were working with a client in the Southeast—a large health system that serves a population of over 1 million—that was trying to get a handle on population health management. We started with one of the most effective ways a health system can begin population health management, which is to look at its self-insured population. But we didn’t stop there.
After digging deeper to better understand and quantify the financial impact of a population health strategy, we discovered the system simply needed to focus on 3.2% of its self-insured population, or just over 400 individuals. That’s a much easier way to think about caring for a population of over 1 million people. When we presented these findings, the response was,
“We can deal with that.”
The health system’s employees are an ideal starting point, because they’re already at risk for those lives and the data for that population is easily accessible. To identify the 3.2%, we leveraged paid claims data to get a comprehensive view of the issues facing the health system, and analyzed that data from a payer, patient, and provider perspective by integrating data on both hospital cost and utilization.
This provided insight into which percentage of the population was responsible for the majority of the health system’s costs. From there, we were able to identify the high-risk patients in that smaller percentage.
Time your population health strategyWith the right population targets, you can project the financial impact of any demand destruction resulting from fewer inpatient admissions within those populations. That leads to the second objective of the math exercise: to pace the execution of your population health strategy based on what your health system can withstand financially.
The result of our math exercise was an opportunity analysis that showed the impact on the health system’s bottom line if it opted to transition at a slower pace or at a more aggressive pace. This way, the health system could determine when, how much, and where they could invest in developing the physician network, building the technology infrastructure, and adding the operational resources needed.
Impacting these smaller population health management targets allows systems to showcase their value proposition to payers, employers, and patients who are scrutinizing performance more than ever before. That’s when you can begin negotiating risk-based contracts and reaping financial gains from your progress.
Negotiating for value-based contracts or risk-based contracts is new to many of our clients, and we do a lot of work to help them understand how to accomplish their value-based care goals in a way that is financially manageable.

18 | The Advisory Board Company
Improving MARGINS through housekeeping is baseline. Turning them into market advantage is the new basis of competition.

Advisory Board Consulting and Management | 19
CLIENT PROFILES
PHYSICIAN ALIGNMENT TRANSITION TO VALUE MARGINS GROWTH
Improving margins is no longer just an exercise in cost management. In a world where we are competing on value, margins and cost performance can elevate providers of choice from the rest.
All health systems strive to cut expenses and uncover revenue cycle opportunities. But fewer also approach margins more broadly, beyond the books—extending accountability across the value chain to better manage episodes.
By reducing care variation and enhancing performance and quality—within the hospital and across ambulatory sites—health systems can improve margins while gaining an edge among payers and consumers alike. We work with clients to uncover system-wide value, and leverage margins as a competitive advantage.
Maintained financial sustainability for the system by deploying interim management in accounts receivable to improve point-of-service cash collections, payment integrity, and patient access.
Identified $11.5M in revenue cycle opportunity
Addressed root processes—ranging from admissions and bed assignments to patient transfers and case management—to “hardwire” margin improvement.
Achieved $12M+ in total financial improvement
Uncovered revenue by maximizing departmental resources, creating criteria to triage accounts, and designing reports to track denials and recoveries.
Generated $3.4M in untapped revenue within nine months
Led the turnaround of an integrated medical group by engaging physicians in leadership and governance, redesigning the professional fee revenue cycle, and realigning physician incentives in a new compensation plan.
Effected more than $20M in annual improvement
Regional, not-for-profit health care system
600 bed flagship hospital
400+ bed medical complex
Small, for-profit integrated health system

20 | The Advisory Board Company
How our clients are looking at margin improvement today—and how they ought to be
Q&A WITH JOHN JOHNSTON, SENIOR VICE PRESIDENT
Q: For the past several years, hospital executives have been focused on the idea of “Medicare breakeven,” or performing at a level to generate a positive operating margin at Medicare reimbursement rates. Are your clients still thinking about their margins in the same way?
JJ: Medicare will continue to be the main payer for hospitals, and it drives rates and models other payers adopt. Therefore, hospital leaders will keep looking at operating margins in the context of Medicare reimbursement. But actual Medicare breakeven is also a long way off for most organizations. While it is a priority, and hospital leaders are working to move in that direction, they’re doing so in a way that prioritizes “front burner” issues, such as Medicare rate cuts, reimbursement policy changes, and risk readiness.
Q: For your clients who are actively working toward Medicare breakeven, are there common threads across each of them?
JJ: One common thread is that most of my hospital clients had already begun tightening up cost discipline over the past two to three years, but they did so in traditional ways: improving labor productivity, lowering supply cost, and reducing physician practice subsidy. Those efforts were effective to the extent that they prevented their situation from worsening, but they weren’t quite enough to bend the cost curve in the out years. There is also a common thread among a subset of our clients who’ve been fortunate to have a good payer mix. Because they have been able to maintain stronger margins over the past few years, they’re having a harder time making adjustments to cost structure. Culturally they have not yet become accustomed to the frequency of change other hospitals have had to experience.
Q: For hospitals on the other end of the spectrum, ones that are struggling today, what advice are you giving them to get on a path to sustainability?
JJ: The first step for that group is to create a 12- to 18-month business plan to recast their cost structure while better positioning the organization for risk. It’s important for struggling hospitals to go down both paths simultaneously. If not, they risk staying two steps behind the market. This means taking a very purposeful approach to care redesign. Everyone should have a plan. It gives hospital leaders a framework for guiding their employees, physicians, and even their boards down a road that is difficult to navigate. The most forward-thinking organizations are not waiting on margins to drop—they are implementing a plan now, while they have time. One organization that comes to mind is Alexian Brothers Health System in Chicago. They have a very strong business plan to move to Medicare breakeven. Their plan has become a new way of doing business, and as a result they are seeing physicians, managers, and staff all move in the same direction.
Q: This is a turbulent time in the health care industry. Should hospital leaders be optimistic about the future of health care?
JJ: If hospitals approach their margin improvement efforts in the right way, they should have the resources to continue building a system that will enable hospitals, physicians, and caregivers to work collaboratively for the wellness of the patient. Hospitals have always treated sickness, but we also need to help patients avoid getting to the point of requiring hospitalization. Finally we are moving to a reimbursement model that supports providers to maintain a patient’s wellness, which is exciting and new. We just have to figure out how to get there in a financially sustainable way.
Our perspective on the issues affecting MARGINS

Advisory Board Consulting and Management | 21
Point-of-service collections start with you: 4 ways to get your staff on board
BY JAMES GREEN, MANAGING PARTNER
“This isn’t what I signed up for.”IN MY WORK helping organizations improve their front-end collections, I hear this phrase a lot.
I get it. Most employees come to a hospital to help patients. They often feel they didn’t sign up to collect money, and many staff haven’t had adequate training to do so. What’s more, no one wants to upset patients or drive them away.
And yet, I’ve seen the best of the best help their staff do more than just tolerate asking for point-of-service collections. How do they get their teams excited about this effort? Here are four strategies I’ve found that are keys to optimizing your up-front collections:
1. Hardwire a culture around up-front collections— from the top down First and foremost, it’s essential to establish a hardwired culture around up-front collections. Point-of-service collections is not optional—it’s the new standard. That message needs to come from the top down, “We are going to start collecting at the point-of-service. We’re going to ask every patient, every time.” Next, it’s critical to align your processes and policies to back up your message. Set an organizational goal and then set managers’ and staff’s goals accordingly. Update key job descriptions to ensure point-of-service collections language is included. Consider updating performance review grids to include POS collections performance criteria. Make whatever updates you need to ensure that everyone is on board. Lastly, organizations doing this well have a formal accountability structure, so ensure everyone involved in the point-of-service collections initiative understands how their role contributes to the organization’s success, set measurable targets for each key staff member involved, and hardwire routine report outs on progress to-date against goals—across individuals, departments, and organization-wide.
2. Focus on education Let’s face it: asking a patient for money can be uncomfortable. But with training, even the most timid registration staff member can master this skill. Train your staff to think about the discussion around point-of-service collections as more than just collecting payment. It’s about educating the patient, explaining
what their benefits are and what payment options they have. To boost staff confidence, give your employees a sample script to guide these types of conversations and educate them on the different types of patient out-of-pocket obligations (copay vs. co-insurance, deductible, out-of-pocket max, etc.). Once your staff feels empowered to address these point-of-service collections head-on, your patients will be better educated about their financial responsibility, and increased up-front revenue capture will follow.
3. Plan your community outreach Once you’ve got your organization fully on board, it’s time to think about how best advertise the point-of-service collections initiative within your community. Take the time to decide the most appropriate way to announce your new policies to ensure you set patient expectations. Then, think through how best to market your new policies to focus on the positive aspects of up-front collections. Lastly, consider the patient’s perspective—would you want to be surprised with a collection attempt on your date of service, or would you prefer to know your out-of-pocket obligation ahead of time? The majority of patients prefer the latter whenever possible, so consider pre-registration strategies, such as outbound calls 3-5 days prior to service, to further get the word out.
4. Remember the benefit to the patient Price shopping is growing rapidly as we move into an era of increased price transparency. If you can provide a timely, accurate estimate to patients, you’re well prepared for price-sensitive patients. There’s something else that we all can relate to—nothing kicks you when you’re down quite like a surprisingly large bill. By sharing an estimate at the point of service, your patients have a reasonable idea of what they can expect to pay, before they even receive care. Even more, they can sit down with a financial counselor to arrange an ideal payment plan prior to service if they anticipate difficulty in paying the full amount at once.
Giving your patients those options should make you feel better, not worse, about the care you provide.
That, after all, is what you signed up for.
22 | The Advisory Board Company
Scale is measured by increasing your coverage on a map. GROWTH is measured by expanding your consumer relevance.

Advisory Board Consulting and Management | 23
Today’s retail health care market has drastically changed the rules of the game, redefining the very basics of growth. Until recently, growth was about scale—a “land grab” to get bigger for the sake of your business.
But growth today comes from building a relevant network that appeals to different types of consumers, on issues like cost, quality, and clinical scope.
The potential upside is great, but many organizations lack the underlying foundation to sustain their investments in growth. We help health systems design a consumer-oriented growth strategy, and sustain value and relevance over time.
PHYSICIAN ALIGNMENT TRANSITION TO VALUE MARGINS GROWTH
CLIENT PROFILES
Implemented an aggressive growth strategy for the employed physician enterprise, including acquisition support, physician alignment, and organizational structure redesign.
Expanded physicians’ geographic reach
Deployed block scheduling processes to optimize surgery flow, allowing for more surgeons and more volume—all without having to build out additional ORs.
Increased surgical volumes by 10%
Developed and implemented an ACO and CI network, overseeing the alignment of physicians as well as resulting partnerships that expanded capabilities and capacity.
Yielded first market share gains in 30 years
Broadened and improved the availability of patient services by merging three competing cardiology practices into a single operating entity that bridged ambulatory and acute care services.
Merged 90+ physicians and surgeons
Five hospital, not-for-profit health system
Not-for-profit community health system
Competitive ACO and CI network
Small, acute care hospital undergoing acquisition

24 | The Advisory Board Company
The #1 reason why hospital deals fail—and how to make sure yours doesn’t
BY THOMAS CASSELS, EXECUTIVE DIRECTOR
WITH THE U.S. HEALTH CARE SYSTEM in the midst of a significant period of consolidation, we’re getting more questions about hospital M&A strategy than ever before. Many of you are concerned about getting the details of the transaction process right—ensuring that you choose the right partner, conducting extensive due diligence, and so on.
And while those factors are certainly crucial, we believe that what happens once the ink has dried is just as important as the steps leading up to the deal itself.
Understanding the value of integrationData has shown that many hospital mergers fall short of achieving their original goals. Few deals improve care quality, and an alarming proportion of newly acquired hospitals—about 1 in 5—actually start to lose money within two years of the transaction.
There’s a strong consensus across a range of industries that post-merger integration, which includes the way you align processes as well as people, is the largest determinant of a deal’s success.
10 tactics to guide post-merger integrationIn our study of the top performers, here’s what they do to ensure success in their integration efforts:
1. Begin integration planning long before deal closure. Rather than holding off until the deal closes, begin the planning process as early as possible. Ideally, high-level integration planning begins as soon as you start evaluating specific targets.
2. Immediately identify a dedicated integration leader. While the existing leadership team will certainly contribute to the integration process, the most successful institutions select an individual to lead integration efforts on a full-time basis.
3. Assemble a distinct integration team. Because the transaction process also warrants full-time staffing, pull together a separate integration team to ensure sufficient focus on the integration process and enable integration planning to begin early.
4. Use early wins to establish credibility and build momentum. Early successes boost morale in a time of uncertainty, enabling the system to create the momentum it needs to pursue more challenging goals across the long term.
5. Pick your battles with IT integration. IT poses one of the most significant challenges to the integration process. Best-in-class institutions stage the IT integration process, prioritizing efforts based on the needs of the deal at hand.
6. Over-communicate the benefits of integration. A comprehensive communication plan boosts morale and ensures that integration plans roll down to all appropriate constituencies.
7. Establish baseline targets at the outset. Success across the long term depends on your rigor in monitoring your integration efforts. Identify performance measures early on, ideally during the goal-setting process.
8. Instill accountability through defined scorekeeping. Once you’ve identified baseline targets, designate scorekeepers and create a clear evaluation process to establish accountability throughout the organization.
9. Create clear pathways to readjust the integration plan. The most effective systems establish standardized processes for gathering and disseminating best practices to target areas of underperformance.
10. Hardwire learning processes to inform future integration. Retain best practices by establishing a permanent integration team or—for those who cannot justify this investment—by ensuring the business development team is involved throughout the process.
Our perspective on the issues affecting GROWTH
Advisory Board Consulting and Management | 25
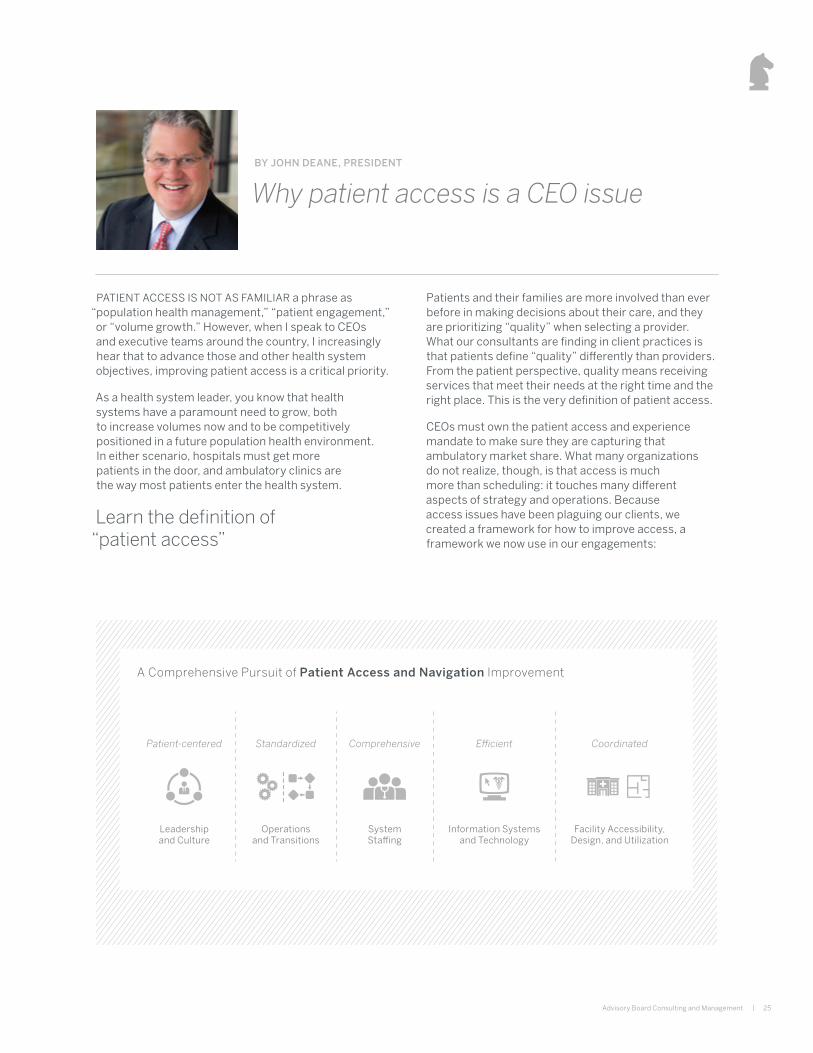
Why patient access is a CEO issueBY JOHN DEANE, PRESIDENT
PATIENT ACCESS IS NOT AS FAMILIAR a phrase as “population health management,” “patient engagement,” or “volume growth.” However, when I speak to CEOs and executive teams around the country, I increasingly hear that to advance those and other health system objectives, improving patient access is a critical priority.
As a health system leader, you know that health systems have a paramount need to grow, both to increase volumes now and to be competitively positioned in a future population health environment. In either scenario, hospitals must get more patients in the door, and ambulatory clinics are the way most patients enter the health system.
Learn the definition of “patient access”
Patients and their families are more involved than ever before in making decisions about their care, and they are prioritizing “quality” when selecting a provider. What our consultants are finding in client practices is that patients define “quality” differently than providers. From the patient perspective, quality means receiving services that meet their needs at the right time and the right place. This is the very definition of patient access.
CEOs must own the patient access and experience mandate to make sure they are capturing that ambulatory market share. What many organizations do not realize, though, is that access is much more than scheduling: it touches many different aspects of strategy and operations. Because access issues have been plaguing our clients, we created a framework for how to improve access, a framework we now use in our engagements:
A Comprehensive Pursuit of Patient Access and Navigation Improvement
Leadership and Culture
Patient-centered
Facility Accessibility, Design, and Utilization
Coordinated
System Staffing
Comprehensive
Operations and Transitions
Standardized
Information Systems and Technology
Efficient

Advisory Board Consulting and Management takes a multidisciplinary approach to every engagement by integrating operational and strategic consulting with industry-leading research and technology. The mission of our team is to help your organization improve performance, culture, and the patient experience—and enable sustainable, positive transformation.
For more information about our services, visit us at advisory.com/consulting.
PHYSICIAN ALIGNMENT
Transform your physician relationshipsfor an integrated, coordinated, and high-performing network.
advisory.com/consulting/alignment
MARGINS
Improve financial performance while gaining market advantage with payers and consumers.
advisory.com/consulting/margins
TRANSITION TO VALUE
Invest in the right care models and payment programs, with the tools to sustain them.
advisory.com/consulting/value
GROWTH
Build a consumer-relevant network to compete and grow in today’s retail marketplace.
advisory.com/consulting/growth
additional RESOURCES
26 | The Advisory Board Company

Consulting and Management
28 | The Advisory Board Company
firm SUMMARY
FOR MORE THAN THREE DECADES, The Advisory Board Company has been helping health care get better. We aren’t just a global research, technology, and consulting firm. We are a performance improvement partner for 180,000 leaders in 4,500+ organizations across health care and higher education. Through our membership model, we collaborate with executives and their teams to find and implement the best solutions to their toughest challenges. But it’s not enough just to know the right answer—we need to solve real-world problems. That’s why we create performance technology products that tell members where their biggest improvement opportunities are, and how to get results.
That’s why our expert researchers analyze thousands of case studies every year to find and share proven best practices.
That’s why our talent development team offers hands-on training to cultivate leaders and drive workforce engagement.
And, that’s why our seasoned consultants provide hands-on support and guidance in health care organizations around the world.

Learn more about the Consulting and Management team
advisory.com/consulting/experts

3102 West End Avenue, Suite 800, Nashville TN 37203
P 615.385.2126 | F 615.620.5020advisory.com/consulting
29983