abdominal pain- all quadrants- case based learning
TRANSCRIPT
CASE BASED LEARNING
ABDOMINAL PAIN
INTRODUCTION
Dr.B.Selvaraj MS;Mch;FICS;
Professor of Surgery
Melaka Manipal Medical College
Melaka 75150 Malaysia
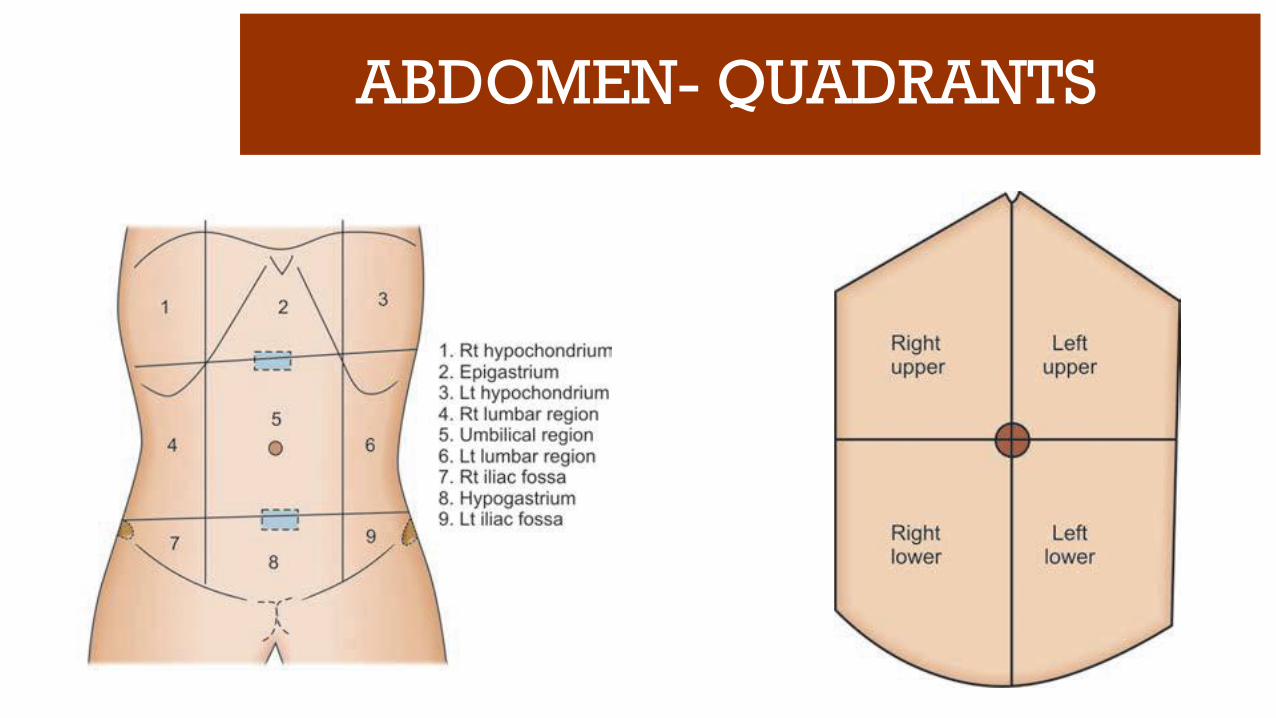
ABDOMEN- QUADRANTS
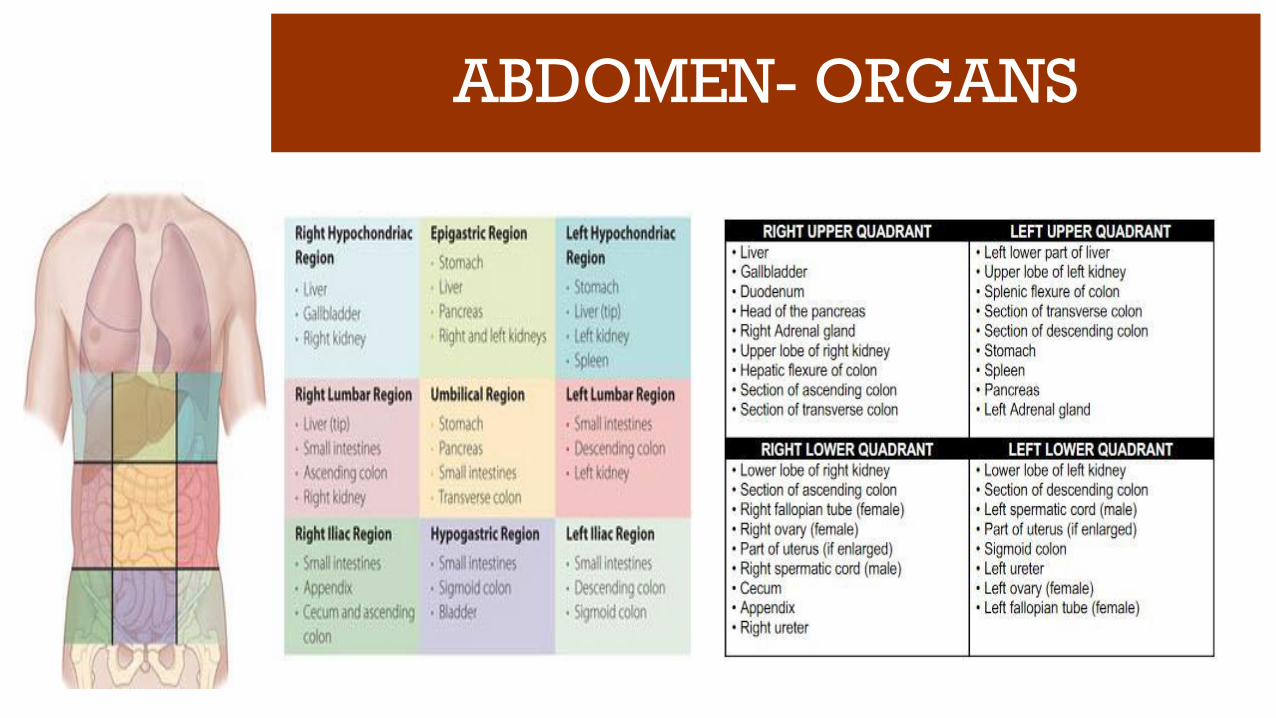
ABDOMEN- ORGANS

ABDOMINAL PAIN- CAUSES

ABDOMINAL PAIN- CAUSES
Inflammation of a viscus
Perforation of a viscus
Obstruction of a viscus
Infarction of a viscus
Intra-abdominal hemorrhage or retroperitoneal hemorrhage
Extra-abdominal or medical causes for acute abdominal pain like lower lobe
pneumonia and inferior wall MI

ABDOMINAL PAIN- HISTORY
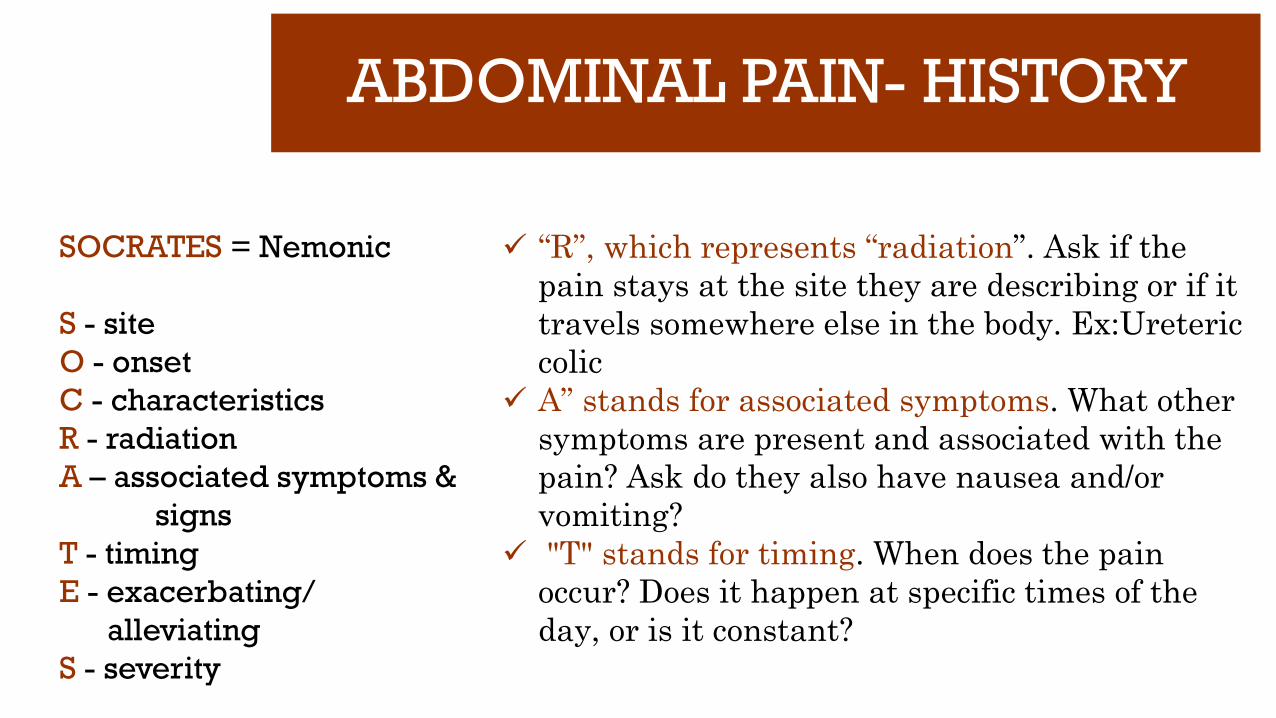
SOCRATES = Nemonic
S - site
O - onset
C - characteristics
R - radiation
A – associated symptoms &
signs
T - timing
E - exacerbating/
alleviating
S - severity
“S” stands for “site”. Which region/quadrant? Is
it a general sense of overall discomfort? The site
of pain helps you fine tune your subsequent
physical exam and diagnostic decision making.
“O” stands for “onset”. When did the pain start?
Acute or insidious?
“C” stands for “characteristics”. The pain may
be sharp, dull, heavy, etc. or a combination of
descriptions.
ABDOMINAL PAIN- HISTORY
SOCRATES = Nemonic
S - site
O - onset
C - characteristics
R - radiation
A – associated symptoms &
signs
T - timing
E - exacerbating/
alleviating
S - severity
“R”, which represents “radiation”. Ask if the
pain stays at the site they are describing or if it
travels somewhere else in the body. Ex:Ureteric
colic
A” stands for associated symptoms. What other
symptoms are present and associated with the
pain? Ask do they also have nausea and/or
vomiting?
"T" stands for timing. When does the pain
occur? Does it happen at specific times of the
day, or is it constant?

ABDOMINAL PAIN- HISTORY
SOCRATES = Nemonic
S - site
O - onset
C - characteristics
R - radiation
A – associated symptoms &
signs
T - timing
E - exacerbating/
alleviating
S - severity
“E” represents “exacerbating” factors; grouped
within this is also alleviating factors. The
patient should be probed as to what makes their
pain better or worse. Certain physical positions,
medications, etc. These factors can all provide
historical clues about the root cause.
“S” stands for “severity”. In most hospitals this
is formulated on a 1 to 10 scale with 10 being
the most severe pain they’ve ever experienced.

ABDOMINAL PAIN
Somatic pain:
Originate from abdominal wall and parietal peritoneum
Sharper and more distinct
Better localized
Sensitive to cutting,tearing, burning and crushing
Visceral pain:
Originate from internal organs and visceral peritoneum
Achy and crampy
Variable localization and sensation
Not sensitive to cutting, tearing, burning or crushing
Sensitive to stretching of walls of hollow organs and capsule of solid organs

ABDOMINAL PAIN
Shifting pain: Ex: Periumbilical pain shifting to RLQ in Ac.appendicitis
Radiating pain: Ex: Pain radiating from loin to groin in ureteric colic
Reffered pain: Ex: Pain felt at Lt shoulder in case of splenic rupture
ABDOMINAL PAIN- GRADING
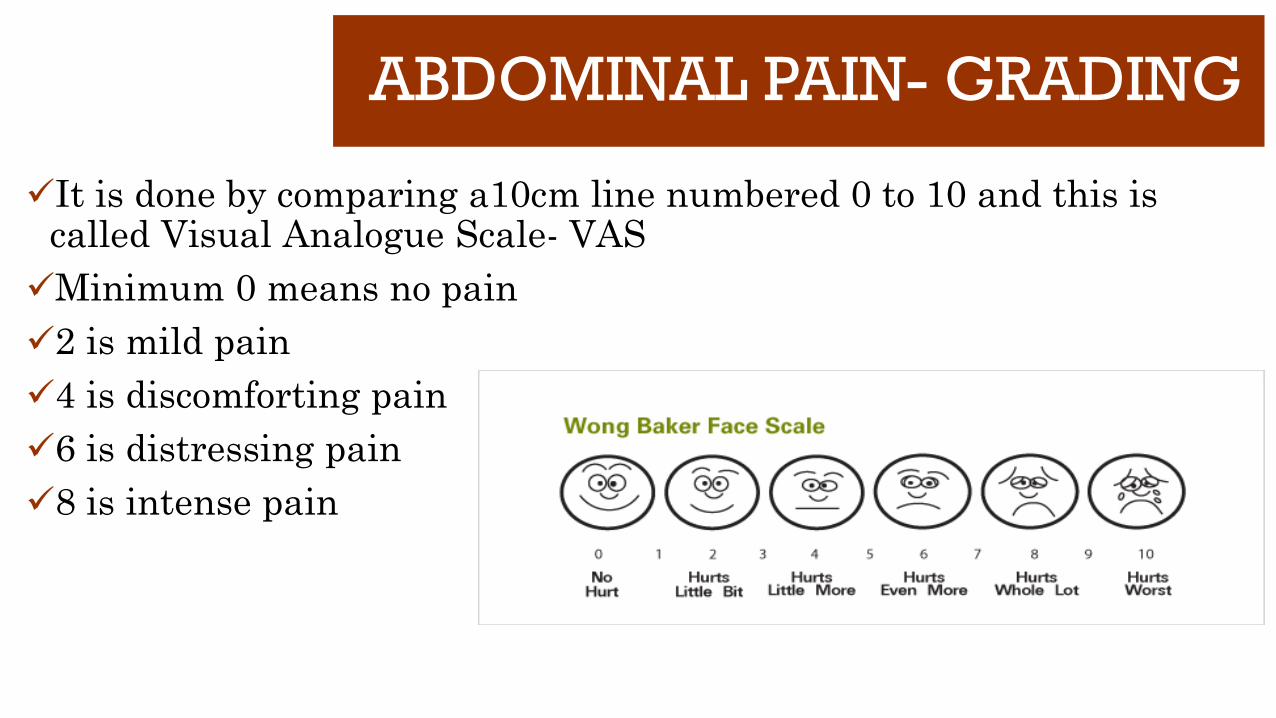
It is done by comparing a10cm line numbered 0 to 10 and this is called Visual Analogue Scale- VAS
Minimum 0 means no pain
2 is mild pain
4 is discomforting pain
6 is distressing pain
8 is intense pain


CASE BASED LEARNING
ABDOMINAL PAINRLQ PAIN
Dr.B.Selvaraj MS;Mch;FICS;
Professor of SurgeryMelaka Manipal Medical College
Melaka 75150 Malaysia

ABDOMINAL PAIN- RLQ PAINA 28-year-old female presents with a 2-day hx of vague periumbilicalpain. Today the patient has lower abdominal pain (right greater than left), which is associated with new onset of urinary frequency. She also vomited twice today. She is sexually active and her menstrual cycle tends to be irregular. Her last menstrual period was 6 weeks ago (2 weeks late).
VS: T = 100.2, HR = 90, BP = 110/68.Labs: H/H = 12.0/36.3, WBC = 11,300, U/A: 5 RBCs, 10–15 WBCs
Physical examination: RLQ tenderness, guarding, and rebound.Pelvic examination without cervical motion tenderness
What would be your differential dx and plan for further evaluation?

RLQ PAIN- Differential Diagnosis
D/D in Adult males

RLQ PAIN- Differential Diagnosis
D/D in Females
D/D in Children

ABDOMINAL PAIN- RLQ PAIN This patient has the characteristic prodrome for appendicitis with periumbilical pain
migrating to the RLQ and associated with localized peritoneal findings. Check the β-hCG before proceeding with appendectomy particularly in light of the patient’s
delayed menstrual period. Ectopic pregnancy must be r/o. The abnormal U/A result may relate to bladder irritation from an inflamed appendix or
represent the additional problem of a UTI. Though the clinical picture is most consistent with appendicitis, preoperative USG/CT Abd
should be done if the β-hCG is normal.
Diagnostic Priorities: Ac Appendicitis, R/O UTI and ectopic pregnancy.

RLQ PAIN- Ac. Appendicitis History- Symptoms • Anorexia (hamburger sign), nausea, vomiting • Vague periumbilical pain that shifts to the RLQ- “ Murphy’s Triad” Physical Exam- Signs • McBurney’s point tenderness and rebound tenderness • Cutaneous hyperesthesia, Rovsing’s, psoas, and obturator signs Laboratory • Elevated WBC with left shift • C-reactive protein • Pregnancy test • Urinalysis: sterile pyuria

RLQ PAIN- Ac. Appendicitis Diagnosis • Oftentimes is a clinical diagnosis Pathophysiology • Closed-loop obstruction • Fecolith in adults, lymphoid hyperplasia in children Imaging • None needed with classic H&P and leukocytosis • US: women and children • Avoid CT in children (increased risk of malignancy) and pregnancy (risk to fetus) • CT: if diagnosis is equivocal in men and nonpregnant women • MRI: pregnant women Management • Appendectomy (open or laparoscopic)
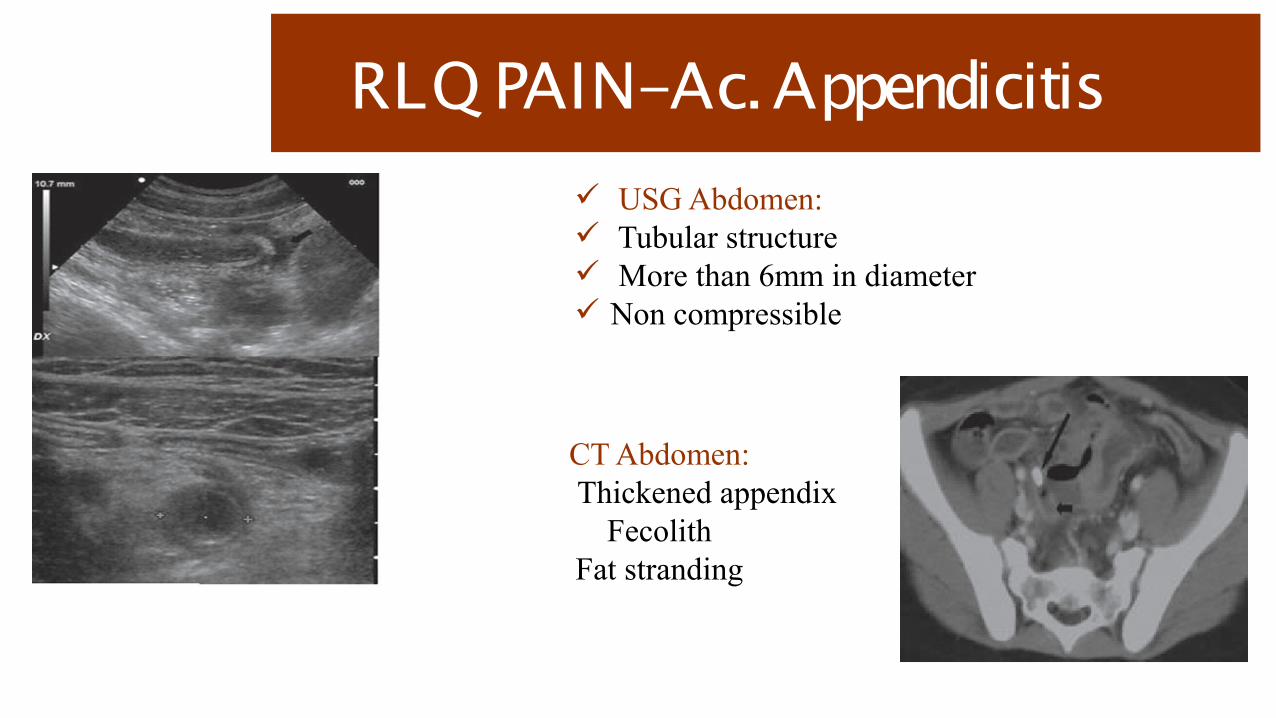
RLQ PAIN- Ac. Appendicitis USG Abdomen: Tubular structure More than 6mm in diameter Non compressible
CT Abdomen: Thickened appendix
FecolithFat stranding

ALVARADO SCORING

Ac. Appendicitis- Algorithm


CASE BASED LEARNING
ABDOMINAL PAINRUQ PAIN- 1
Dr.B.Selvaraj MS;Mch;FICS;
Professor of SurgeryMelaka Manipal Medical College
Melaka 75150 Malaysia

ABDOMINAL PAIN- RUQ PAIN
HISTORY:A 40-year-old moderately obese female presents to the emergency department with a 1-day history of constant epigastric and right upper quadrant (RUQ) pain. She describes the severity of the pain as a 7 out of 10. The pain began after eating fried pork. She reports that the pain also seems to affect the right side of her back near her scapula. She feels nauseated and has vomited twice. She has had similar pain, but of lesser severity, about once a month for the past year. The pain comes on after eating fried or spicy foods, but previously it has resolved after an hour. She is gravida six and para six.

ABDOMINAL PAIN- RUQ PAINOn physical examination, her temperature is 100 °F, heart rate is 110/min, and her blood pressure is 120/80 mmHg. She has marked tenderness in the RUQ of the abdomen to palpation. When the RUQ is palpated while she is taking a deep breath, she abruptly ceases inspiration secondary to pain Murphy’s Sign+ve
Laboratory values are significant for WBC count of 14 × 10 3 /μL (normal 4.1–10.9 × 10 3 /μL), Total Bilirubin 1.0 mg/dL (0.1–1.2 mg/dl), Alkaline phosphatase70 units/L (33–131 u/L), Amylase 60 units/L (30–110 u/L), and Lipase 30 units/L (7–60 u/L).
What would be your differential dx and plan for further evaluation?

RUQ PAIN- Differential Diagnosis

ABDOMINAL PAIN- RUQ PAIN
With her current history of severe persistent abdominal pain following ingestion of fatty foods, nausea and vomiting, and associated right upper quadrant tenderness to palpation, the etiology is most likely of biliary origin.
The patient’s prior history is consistent with symptomatic cholelithiasis With a positive Murphy’s sign, fever, tachycardia, and elevated WBC count, the most likely
current diagnosis is acute cholecystitis. With a normal total bilirubin and alkaline phosphatase, choledocholithiasis and acute
cholangitis are less likely. Similarly, a normal amylase and lipase rule out gallstone pancreatitis.

RUQ PAIN- Ac. Cholecystitis History • RUQ pain in obese, multiparous female Physical Exam • Murphy’s sign for acute cholecystitis Pathology/Pathophysiology • Acute cholecystitis triggered by persistent cystic duct obstruction by gallstone Diagnosis • RUQ US: gallstones, pericholecystic fluid, thickened gallbladder wall, and sonographic
Murphy’s sign • HIDA scan if RUQ ultrasound is nondiagnostic • KUB not helpful: only 10 % of gallstones are radio-opaque
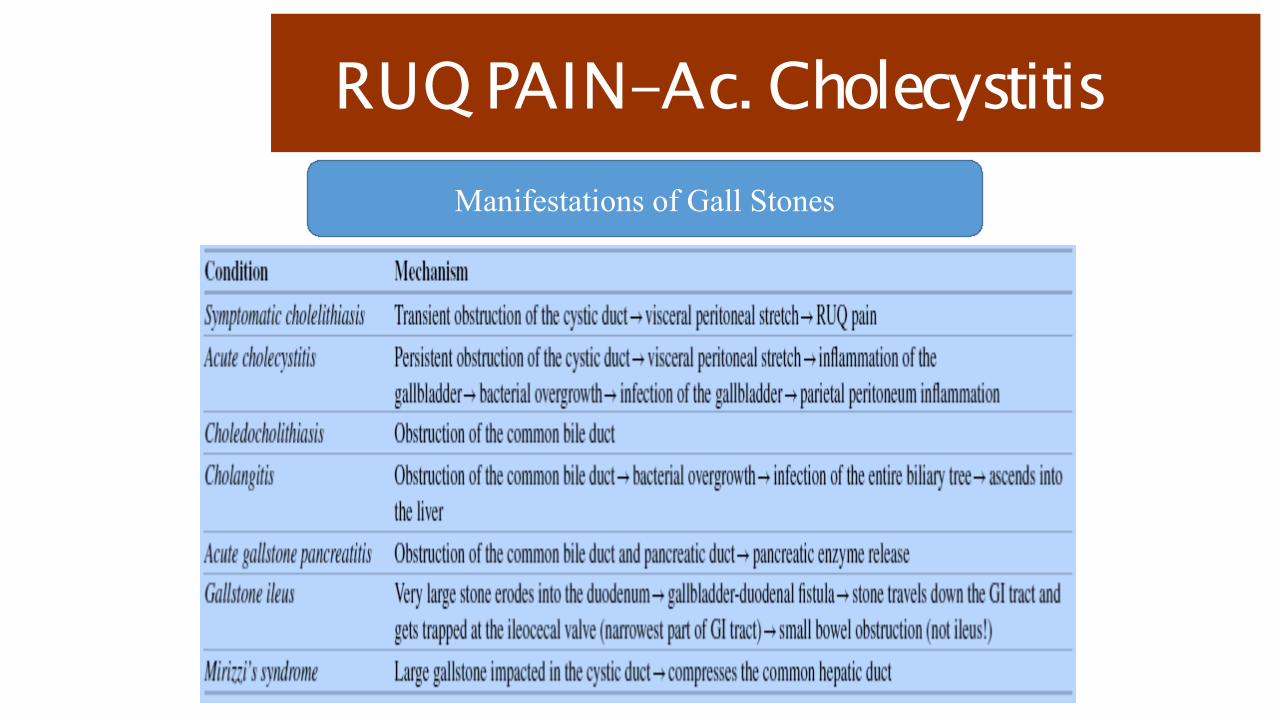
RUQ PAIN- Ac. CholecystitisManifestations of Gall Stones

RUQ PAIN- Ac. Cholecystitis
Biliary Colic Vs Ac Cholecystitis

RUQ PAIN- Ac. Cholecystitis Management • Asymptomatic gallstones: cholecystectomy not indicated • Symptomatic cholelithiasis (biliary colic): elective lap cholecystectomy • Acute cholecystitis: urgent (within 48 h) lap cholecystectomy • Acute acalculous cholecystitis: cholecystostomy tube if critically ill • Emphysematous cholecystitis: emergent cholecystectomy • Gallstone ileus: remove large impacted gallstone from terminal ileum (leave gallbladder
alone) Postoperative • If a patient presents within the first week after cholecystectomy with abdominal pain,
distention, and anorexia, consider a biloma (cystic duct stump leak, CBD injury) • Cystic duct stump leak readily treated with ERCP and stenting of the sphincter of Oddi • CBD injury may require hepaticojejunostomy/choledochojejunostomy
RUQ PAIN- Ac. Cholecystitis Additional Important Facts • Ursodeoxycholic acid could be employed as conservative management for patients with
cholelithiasis • Calcified gallbladder (porcelain): increased risk of malignancy, perform cholecystectomy • Choledochal cysts are congenital dilations of the biliary tree; prone to cholangitis, risk of
associated malignancy, need to excise (if intrahepatic ducts are involved (Caroli’s disease), and may need liver transplantation
• Hemolytic anemia in childhood: high risk of black pigment gallstones • Gallbladder cancer: associated with gallstones • Gallbladder polyps: > 1 cm suspicious for cancer; >2 cm high likelihood of cancer

RUQ PAIN- Ac. CholecystitisCholesterol gallstones form
when the concentration of cholesterol in the bile exceeds its solubility
Black stones are often associated with hemolytic disease
Brown stones usually are associated with bacterial infection and parasites
“Gall Stone is the tombstone erected in the memory of dead bacteria
inside”

RUQ PAIN- Ac. Cholecystitis
USG Abdomen:Hyperechoic Gall stone shadow
Posterior acoustic shadowingGB wall thickness > 3mms
Pericholecystic fluid collection
HIDA Scan:Fig 1: Visualisation of GB
Fig 2: Non visualization of GB- Acute Cholecystitis


CASE BASED LEARNING
ABDOMINAL PAINRUQ PAIN- 2
Dr.B.Selvaraj MS;Mch;FICS;
Professor of SurgeryMelaka Manipal Medical College
Melaka 75150 Malaysia

ABDOMINAL PAIN- RUQ PAINHISTORY:A 40-year-old female presents with a 24 hour history of right upper quadrant (RUQ) and epigastric pain, associated with nausea and vomiting. She has had similar pain in the past, particularly after eating greasy foods. According to her family, over the last few hours, the patient has become slightly confused. Past medical history is negative.
PHYSICAL EXAM:Temperature of 102.5 °F, a heart rate of 110 beats/min, respiratory rate of 16/min, and a blood pressure of 90/60mmHg. She is moderately tender in the RUQ to deep palpation. She has slight scleral icterus. She has noted dark- colored Urine. The remainder of her abdominal exam is negative.

ABDOMINAL PAIN- RUQ PAINLaboratory Values:White blood count of 15 × 10 3 /μL (normal 4.1–10.9 × 10 3 /μL), Total bilirubin of 4.0 mg/dl (0.1–1.2 mg/dl),Alkaline phosphatase (AP) of 350 μ/L (33–131 μ/L), Aspartate aminotransferase (AST) of 300 μ/L (5–35 μ/L) Alanine aminotransferase (ALT) of 280 μ/L (7–56 μ/L), Gamma-glutamyl transpeptidase (GGT) of 330 μ/L (8–88 μ/L), Amylase of 100 μ/L (30–110 μ/L). Urine is positive for bilirubin.
What would be your differential dx and plan for further evaluation?

RUQ PAIN- Differential Diagnosis

ABDOMINAL PAIN- RUQ PAIN The most likely diagnosis in a patient with a 1-day history of RUQ pain worsened with
greasy foods, nausea, jaundice, and fever is acute cholangitis secondary to gallstone impaction Charcot’s Triad
Additionally, she has leukocytosis, hypotension, altered mental status, elevated bilirubin, and deranged liver function tests, all of which are consistent with the suppurative cholangitis Reynold’s Pentad
The Tokyo guidelines have been proposed as diagnostic criteria for acute cholangitis. Patients should have evidence of systemic inflammation (fever and/or leukocytosis), cholestasis (jaundice and/or abnormal liver enzymes), and biliary obstruction (dilated bile ducts on ultrasound).
RUQ PAIN- Ascending CholangitisHistory and Physical• Charcot’s triad RUQ pain, fever and jaundice• Reynold’s pentad + hypotension and altered mental status• Look for evidence of SIRS• Elderly patients may be hypothermic and leukopenic (are relatively immunosuppressed)
Etiology/Pathophysiology• Biliary obstruction with bacterial infection• Bacteria enter bile either via bloodstream from the portal vein or retrograde from the duodenum• Most commonly caused by gallstone obstruction of the distal CBD• Other causes: biliary stricture, cancer, parasites• Suppurative cholangitis: acute cholangitis complicated by septic shock

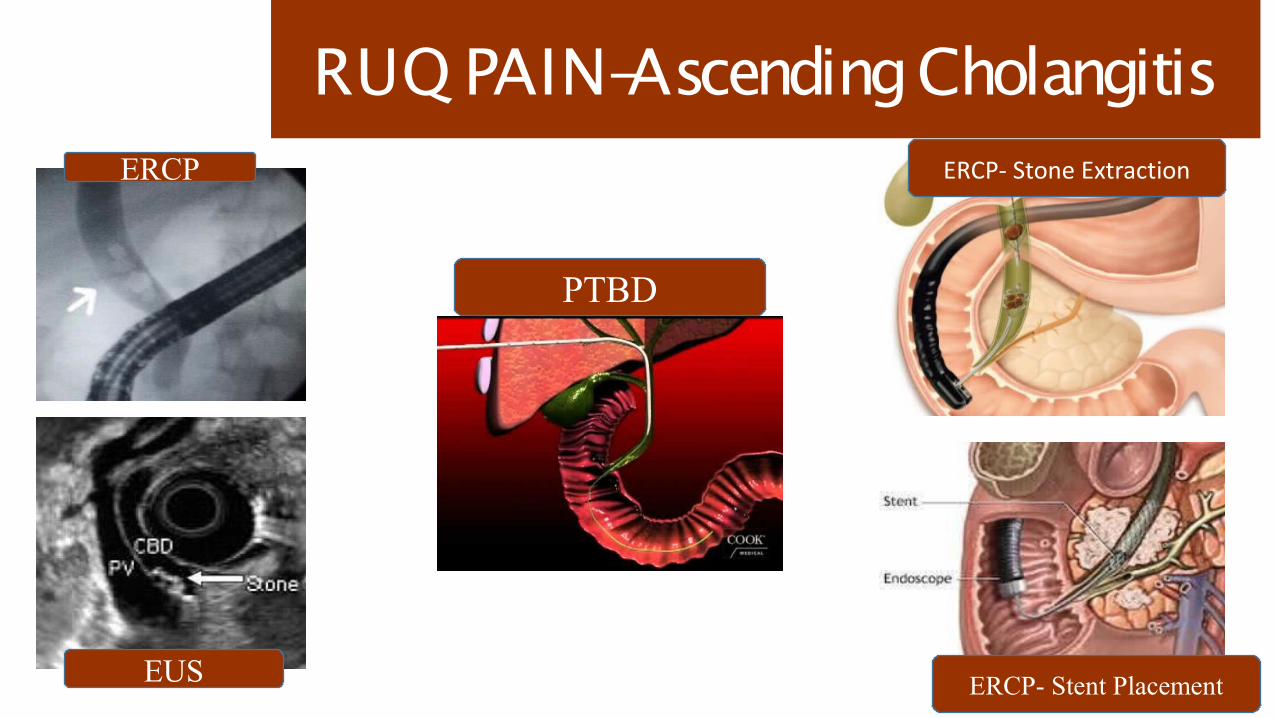
RUQ PAIN- Ascending Cholangitis Diagnosis• Elevated WBC• AP, ALT, AST, GGT rise proportion• US: dilated CBDManagement• Aggressive IV fluids, blood cultures, broad-spectrum antibiotics• Admit to ICU• Urgent biliary decompression via ERCP• PTC if ERCP fails PTBD• Open surgery (insert T-tube into CBD) if PTC fails• Cholecystectomy after sepsis resolves to prevent further biliary complicationsWatch Out• The diagnosis of acute cholangitis may be missed in the elderly and immunosuppressed (e.g. steroids)• Think sclerosing cholangitis if also having symptoms of IBD

RUQ PAIN-Ascending cholangitis
RUQ PAIN-Ascending Cholangitis
PTBD
ERCP
EUS
ERCP- Stone Extraction
ERCP- Stent Placement


CASE BASED LEARNING
ABDOMINAL PAIN
EPIGASTRIC PAIN- 1
Dr.B.Selvaraj MS;Mch;FICS;
Professor of Surgery
Melaka Manipal Medical College
Melaka 75150 Malaysia

ABDOMINAL PAIN-EPIGASTRIC PAIN- 1
HISTORY:
A 56-year-old male with a history of gastroesophageal reflux disease (GERD),
hypertension, and diabetes presents to the emergency room complaining of severe
upper central abdominal pain. The patient reports epigastric pain for months, but it
has just acutely become intolerable over the last 8 hrs. He states that the chronic
pain has been a “gnawing” pain that comes on after eating. He thought he was just
having some indigestion and would take some antacids for relief. Late last night,
the pain became excruciating and now he is having trouble moving.

ABDOMINAL PAIN- RUQ PAIN
On physical examination, blood pressure is 130/70 mmHg, heart rate is
110 bpm, and temperature is 101.5 °F. He appears to be in severe distress
secondary to pain. The patient refuses to straighten his legs because it hurts too
much. He almost jumps off of the table when you press on his abdomen. He has
diffuse guarding and rebound tenderness.
Laboratory values: WBC of 15 (normal 4.1–10.9 × 10 3 /μL), BUN of 35 (7–20
mg/dL), creatinine of 1.8 (0.5–1.4 mg/dL), serum amylase of 70 (30–110 μ/L), and
lipase of 60 (7–60 u/L).
An upright CXR demonstrates free air under the right diaphragm.
What would be your differential dx and plan for further evaluation?

Epigastric Pain- Differential Diagnosis

ABDOMINAL PAIN-Epigastric Pain
✓ The free air under the diaphragm indicates that the patient has a perforated
viscus.
✓ This is supported by evidence of diffuse peritonitis on physical exam.
✓ The most common causes of free air under the diaphragm are perforated ulcers
and perforated diverticulitis.
✓ Given the longstanding history of epigastric pain relieved by antacids, the most
likely diagnosis is a perforated ulcer
Epigastric Pain- DU perforation
✓ History and Physical:
✓ Sudden onset severe epigastric pain that becomes diffuse
✓ History of peptic ulcer disease (PUD), H. pylori, smoking, chronic NSAID use
✓ Evidence of SIRS
✓ Patient lying motionless in bed
✓ Abdominal guarding, rigidity, and rebound tenderness
✓ Pathophysiology:
✓ Acid hypersecretion, defective mucosal defense or H.Pylori infection
✓ Five types of gastric ulcers- Modified Johnson’s classification
✓ Type I ulcers are on the lesser curve of the stomach
✓ Type II ulcers are in the stomach and duodenum
✓ Type III ulcers are pre-pyloric
✓ Type IV ulcers are located proximally near the cardia
✓ Type V ulcers are anywhere secondary to NSAID use

Epigastric Pain- DU perforation
✓ Workup:
✓ Leukocytosis with left shift
✓ Upright CXR: free air under diaphragm
✓ CT with oral gastrografin
✓ Management:
✓ Duodenal perforation
✓ – Primary closure with an omental patch
✓ Gastric perforation
✓ – Primary closure, biopsy, omental patch vs. wedge resection
✓ – Must rule out malignancy
✓ Triple therapy: clarithromycin, amoxicillin, and a PPI for 14 days (if H. pylori
positive)
✓ Additional acid reduction surgery rarely needed

Epigastric Pain- DU perforation
Pneumoperitoneum DU Perforation Graham’s Patch- Omentopexy


CASE BASED LEARNING
ABDOMINAL PAIN
EPIGASTRIC PAIN- 2
Dr.B.Selvaraj MS;Mch;FICS;
Professor of Surgery
Melaka Manipal Medical College
Melaka 75150 Malaysia

ABDOMINAL PAIN-Epigastric PainHISTORY:
A 41-year-old woman presents to the emergency department complaining of severe
and continuous epigastric pain for the past 24 hours. The pain radiates straight
through to her back. She has had progressive nausea with vomiting. The vomitus is
bile stained without blood. She has had similar but less severe episodes in the past,
usually after eating heavy meals, but they always resolved within a few hours. She is
married, with two children, and does not consume any alcohol.
PHYSICAL EXAM:
On exam, she is afebrile, heart rate is 115/min, blood pressure is 128/86 mmHg, and
she has a normal respiratory rate. Her abdomen is not distended. She has no
surgical scars on her abdomen and no obvious masses visible. She has no bruising
around her umbilicus or along her flank. Bowel sounds are hypoactive. She has
marked tenderness to palpation in her epigastrium, without guarding or rebound.
The remainder of her abdomen is soft and non-tender to palpation. No masses or
organomegaly are appreciated.

ABDOMINAL PAIN-Epigastric Pain
Laboratory Values:
WBC count of 17.2 × 10 3 cells/μL (normal 4.1–10.9 × 10 3 cells/uL),
Amylase of 1,545 u/L (normal 30–110 u/L),
Lipase of 1,134 u/L (normal 7–60 u/L),
ALT of 245 u/L (7–56 u/L), AST of 263 u/L (5–35 u/L),
Serum glucose of 156 mg/dl (65–110 mg/dL), and LDH 180 u/L (0–250 u/L)
An abdominal series demonstrates gas throughout the small and large bowel,
and a focal dilated loop of proximal small bowel without air fluid levels- sentinel
loop++. There is no free air under the diaphragm.
What would be your differential dx and plan for further evaluation?

EPIGASTRIC PAIN-Differential Diagnosis

ABDOMINAL PAIN-Epigastric Pain
✓ Diagnosis most probably Acute Pancreatitis
✓ This patient has the classic presentation which consists of epigastric abdominal
pain radiating straight through to the back with nausea and vomiting.
✓ She has had prior episodes of pain, which have resolved within a few hours,
after eating heavy meals, which is characteristic of symptomatic gallstones.
✓ Since the vast majority of pancreatitis cases are due to gallstones or alcohol and
this patient does not consume alcohol, we can conclude that her symptoms are
most likely related to gallstones.
✓ Finally, the amylase and lipase are elevated

Epigastric Pain-Acute Pancreatitis
History and Physical
• Nonsurgical conditions that mimic an acute abdomen: gastroenteritis, acute
adrenal insufficiency, sickle cell crisis, diabetic ketoacidosis, acute porphyria, pelvic
inflammatory disease, kidney stones, and pyelonephritis
• Patients with pancreatitis typically present with epigastric pain radiating to the
back, nausea, vomiting, anorexia, fever,tachycardia.
Pathophysiology
• The initial event in pancreatitis is the inappropriate activation of pancreatic
enzymes
• Gallstones and alcohol are the most common causes of acute pancreatitis
Epigastric Pain-Acute Pancreatitis
Diagnosis
• Most cases can be diagnosed with just a history, physical, and abnormal
amylase/lipase
• Ranson criteria are used to predict severity based on parameters during initial
admission and at 48 hours after
Workup
• Amylase/lipase levels do not correlate with severity of pancreatitis
• In the absence of a history of alcohol abuse, start with a RUQ ultrasound to look
for gallstones

Epigastric Pain-Acute Pancreatitis
Management
• Patients should initially be managed conservatively with IV fluids, NPO, and
narcotic analgesia
• Gallstones
– urgent ERCP if concomitant cholangitis
– early cholecystectomy if mild pancreatitis
– late cholecystectomy if severe pancreatitis
• If patients do not clinically improve after 3 days of conservative management, get
a CT scan with contrast to look for any underlying complications (i.e., necrosis)
• Begin enteral nutrition in patients with prolonged NPO status or in severe acute
pancreatitis
• Refractory persistent abdominal pain is the main indication for surgery in chronic
pancreatitis

Epigastric Pain-Acute Pancreatitis
“I GET SMASHED”:
Idiopathic
Gallstones
Ethanol
Trauma
Scorpion bite
Mumps (viruses)
Autoimmune
Steroids
Hyperlipidemia
ERCP
Drugs
• Systemic
– Early (1st week)
– Multi-organ failure
• Local
– Late (3 weeks)
– Pancreatic abscess
– Pancreatic pseudocyst
– Pancreatic necrosis
Etiology Complications

Acute Pancreatitis- Ranson’s Scoring
At Admission After 48 hrs
“GA LAW (Georgia law)”:
Glucose >200
Age > 55
LDH > 350
AST > 250
WBC > 16,000
“C HOBBS (Calvin and
Hobbes)”:
Calcium <8 mg/dL
Hct drop of >10%
O2 <60 (PaO2)
Base deficit >4
Bun >5 increase
Sequestration >6 L

Acute Pancreatitis-Glasgow- Imrie Scoring

Acute Pancreatitis-Balthazar Scoring

Acute Pancreatitis-BISAP Scoring

Acute Pancreatitis- AXR

Acute Pancreatitis- CECT
CECT: Acute Pancreatitis
Diffusely enlarged pancreas with low density from edema
Phlegmon / Inflammatory MassWhite arrowheads: PhlegmonBlack arrowhead: Pancreatic calcificationLarge Arrow: Peripancreatic fascial infiltration
Acute Pancreatitis / Pancreatic NecrosisArrow: No enhancement of pancreas with IV contrastArrowheads: Normal enhancement in the tail of Pancreas.


CASE BASED LEARNING
ABDOMINAL PAINLLQ Pain - 1
Dr.B.Selvaraj MS;Mch;FICS;
Professor of SurgeryMelaka Manipal Medical College
Melaka 75150 Malaysia

ABDOMINAL PAIN-LLQ PainHISTORY:A 55-year-old obese female presents with a 2-day history of left lower quadrant pain, nausea, anorexia, and low-grade fever. The patient states that the pain is constant, moderately severe, and does not radiate anywhere. No H/O aggravating/relieving factors. She denies vomiting and bloody or black stools and has no recent change in bowel habits, though she says she’s been constipated most of her life. She has noted similar pain in the past,but never this severe, and has never sought medical attention before. She has never had a screening colonoscopy or prior surgery. PHYSICAL EXAM:Abdominal exam reveals mild distention, no surgical scars, and no masses. Bowel sounds are absent. The left lower quadrant is moderately tender to palpation with guarding and no rebound tenderness. Rectal exam is unremarkable. Pelvic exam reveals no cervical motion tenderness and no adnexal masses. LABS: TWBC- 16,000; Hb-13Gm; Hct- 39% What would be your differential dx and plan for further evaluation?

LLQ PAIN- Differential Diagnosis

ABDOMINAL PAIN-LLQ Pain Diagnosis most probably Acute Diverticulitis Given the patient’s left lower quadrant (LLQ) pain and tenderness on exam, associated with
fever and leukocytosis, acute diverticulitis is the most likely diagnosis. Obesity, diet low in fiber and high in fat and red meat, and advanced age are risk factors for the
formation of diverticulosis. Rectal diverticula are extremely rare. It is hypothesized that they almost never occur because
the taenia coli, the longitudinal bands of smooth muscle along the colon, unite into a circumferential band around the rectum, thereby eliminating points of weakness that precede a diverticulum.

LLQ Pain-Acute DiverticulitisHistory and Physical• Major risk factors are obesity, advanced age, and diet low in fiber, high in fat and red meat• Diverticulitis is a clinical diagnosis (LLQ pain and tenderness, fever, leukocytosis)Pathophysiology• The sigmoid colon is the most common site• Complicated diverticulitis: abscess, free perforation, fistula, stricture, and obstructionDiagnosis• CT scan is the first-line imaging modality• Avoid barium enema and colonoscopy in acute presentation because of increased risk of
perforation• Determine if complicated or uncomplicated and with or without SIRS

LLQ Pain-Acute Diverticulitis Management • Uncomplicated diverticulitis without SIRS – Treated as outpatient – Oral antibiotics and clear liquids • Uncomplicated diverticulitis with SIRS – Admit to hospital – NPO, IV fluids, IV antibiotics, and analgesia – Follow up with colonoscopy 4–6 weeks after acute episode to rule out malignancy and Inflammatory Bowel Disease.

LLQ Pain-Acute Diverticulitis
Management • Complicated diverticulitis usually requires surgery– Resect the affected colon and construct end colostomy if urgent– Sigmoid colectomy with primary anastomosis if not urgent
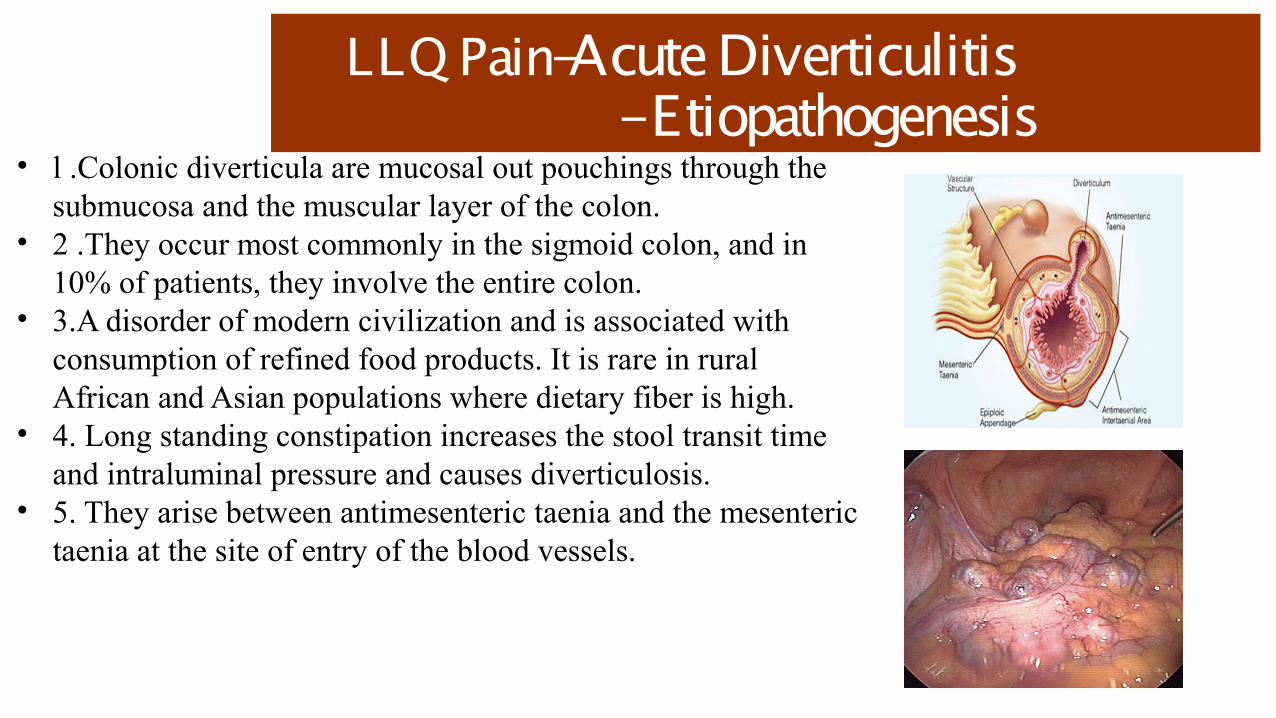
LLQ Pain-Acute Diverticulitis - Etiopathogenesis
• l .Colonic diverticula are mucosal out pouchings through the submucosa and the muscular layer of the colon.
• 2 .They occur most commonly in the sigmoid colon, and in 10% of patients, they involve the entire colon.
• 3.A disorder of modern civilization and is associated with consumption of refined food products. It is rare in rural African and Asian populations where dietary fiber is high.
• 4. Long standing constipation increases the stool transit time and intraluminal pressure and causes diverticulosis.
• 5. They arise between antimesenteric taenia and the mesenteric taenia at the site of entry of the blood vessels.


CASE BASED LEARNING
ABDOMINAL PAINLLQ PAIN- 2
Dr.B.Selvaraj MS;Mch;FICS;
Professor of SurgeryMelaka Manipal Medical College
Melaka 75150 Malaysia

ABDOMINAL PAIN- LLQ PainHISTORY:An 80-year-old male presents with severe abdominal distention and no bowel movement or gas per rectum for 3 days, as well as recent onset of vomiting. He has Parkinson’s disease and chronic constipation and lives in a nursing home. His medications include levodopa and benztropine, which he has been taking for several years.PHYSICAL EXAM:Patient’s vital signs are T 37°C, heart rate 90/min, blood pressure 116/70 mmHg, and respiratory rate 22/min. Patient is tachypnic but nontoxic, with mental status unaltered. His abdomen is severely distended. He does not have any abdominal surgical scars. He is tympanitic but has no significant tenderness to palpation. There are no palpable hernias, and rectal exam demonstrates an absence of stoolwith no palpable masses or strictures.

ABDOMINAL PAIN- LLQ PainLABS:BUN 26 mg/dL; Creatinine 1.4 mg/dL, Electrolytes within normal limits, TWBC:6800/dL; ABG- pH 7.48//PaCO2 30//PaO2 80//HCO3 24//SpO2 99 %.IMAGING:Plain upright abdominal radiograph shows a massively dilated loop of sigmoid with the apex pointing toward the right upper quadrant, consistent with the “coffee bean” or “bent-inner tube” sign; upright chest radiograph shows no free air under the diaphragm.What would be your differential dx and plan for further evaluation?

LLQ PAIN- Differential Diagnosis

ABDOMINAL PAIN-LLQ Pain
Diagnosis most probably Sigmoid Volvulus The massive, slowly progressive abdominal distention, combined with obstipation, and X-ray
findings are consistent with large bowel obstruction. The radiologic appearance is most consistent with a sigmoid volvulus.
Large bowel obstruction-LBO- is more likely to be associated with more pronounced distention, less or late onset vomiting, and decreased bowel sounds.
Small bowel obstruction- SBO- SBOs tend to be associated with more pronounced vomiting. In an early SBO, bowel sounds are hyperactive, with “rushes and tinkles”- Borborygmi. In late SBO- absent bowel sounds- silent abdomen.

LLQ Pain- Sigmoid VolvulusHistory and Physical • LBO – gradual and severe abdominal distention, obstipation, and vomiting• Uncomplicated volvulus – normal vitals, normal mental status, and non-tender abdomen• Complicated volvulus – severe abdominal pain, fever, tachycardia, toxic appearance, peritoneal signs, and leukocytosis• Look for abdominal scars and hernias and perform a rectal exam to assess other differential diagnoses Etiology/Risk Factors:• Most common causes of LBO: Cancer, Diverticulitis & Volvulus• Sigmoid Volvulus – acquired stretching of the sigmoid– Neuropsychiatric disease, institutionalization, chronic constipation, long-term anticholinergic use, highfiber diet, and pregnancy• Cecal Volvulus – congenital failure of fixation of the cecum

LLQ Pain- Sigmoid VolvulusDiagnosis• Compared to LBO, SBO has faster onset and more likely to cause vomiting and high-pitched bowel sounds• Patients with Ogilvie’s syndrome are more likely to be already hospitalized and bedridden, often in the postoperative setting• Abdominal X-ray– Sigmoid volvulus –“coffee bean”, “omega”, or “bent inner tube”, “kidney-bean” sign– Cecal volvulus –“comma” or “kidney bean” sign- Human embryo sign• CT scan if equivocal X-ray findings• Contrast enema may be diagnostic (“bird’s beak” sign) and therapeutic in reducing the volvulus– Water-soluble contrast (Gastrografin) rather than barium, to avoid peritonitis and scarring in case of perforation– Bowel wall thickening, mesenteric edema, pneumatosis, and portal venous gas suggest ischemic bowel

LLQ Pain- Sigmoid Volvulus
Management• Therapy differs based on the location and severity of complication– Uncomplicated sigmoid volvulus – endoscopic detorsion followed by semi-elective resection– Complicated sigmoid volvulus – no detorsion attempted; emergent laparotomy with resection– Cecal volvulus – no detorsion attempted; take to OR for right colectomy• Complications of surgery – wound infection, anastomotic leak, and recurrence. Without detorsion or resection – ischemia,perforation, and sepsis
