ability management program - western forest … · findings will be shared with senior management...
TRANSCRIPT
ABILITY MANAGEMENT PROGRAM
Western Forest Products Inc. – Ability Management Program Page 2 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
PROCESSES AND PROCEDURES included:
Ability Management Process Stay at Work Process Return to Work Process Workplace Accommodation Process
1. POLICY STATEMENT
a. Western Forest Products Inc. (WFP) is committed to ensuring a loss control prevention program is in place as part of its Integrated Healthy Workplace Management System. The Ability Management Program (Program) is intended to provide support to all employees who become unable to perform regular work safely as a result of injury/illness, by ensuring a timely and safe return to productive work regardless of the nature of injury/illness.
2. PURPOSE
a. The purpose of this Program is to:
i. To ensure consistent and effective administration of the Program.
ii. To establish service wide responsibilities and accountabilities as it relates to on the job discomfort and absences due to sickness and disability.
iii. To ensure all employees who are absent due to occupational and/or non-occupational
injury/illness are provided with proactive and appropriate services to promote a speedy recovery and an early, safe return to work.
iv. To ensure consistency and continuity of services between all programs and services
available to WFP employees. 3. SCOPE
a. All WFP employees are eligible to participate in the Program regardless of the nature or cause of injury/illness.
4. PROJECTED OUTCOMES AND PROGRAM EVALUATION
a. It is anticipated that lost time and associated costs (i.e. Insurance premiums) will decrease.
b. The Program will also capture data to monitor lost time, injury and disability trends. The
Ability Management Coordinator (AMC) will be responsible for the execution of this task.
Western Forest Products Inc. – Ability Management Program Page 3 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
c. The Program will be reviewed at minimum, on an annual basis, or sooner as directed by the Corporate Manager – Health and Safety, to determine effectiveness of current processes and to identify any emerging injury and disability patterns.
i. The review will be undertaken by the following parties:
o the Corporate Manager - Health and Safety,
o the AMC, and,
o a Union appointed representative.
d. Feedback from employees will be sought via internal satisfaction surveys on an annual
basis. Findings will be shared with senior management as well as external service providers as required.
5. DEFINITIONS
a. Disability: Any restrictions or lack (resulting from an impairment) of ability to perform an activity in the manner or within the ranges considered normal and customary for an individual.
b. Non-Occupational Injury/Illness: Refers to injuries and illnesses that occur outside of the
workplace and not as a result of work.
c. Occupational Injury/Illness: Refers to injuries and illnesses that are directly resultant of work tasks or occurring on the worksite.
d. Modified Work: Refers to any changes made to an employee’s normal and customary job
duties due to an illness or injury. This includes temporary and permanent changes, as well as changes to work schedule and work tasks.
e. Transitional Work: Refers to the use of modified work with increases in job tasks and/or
work hours at specific timelines, with the goal of returning the employee back to full pre-disability work duties.
6. ROLES and RESPONSIBILITIES
a. Senior Management
i. Will provide support and encourage the development of joint Program initiatives and approaches including providing information and assistance in training and development, facilitative services and sharing of information and best practices.
b. Ability Management Coordinator
i. Is responsible for the development and implementation of the Program, including
monitoring injury and disability trends, ensuring policies and procedures are up to date with legislation and industry standards, ensuring supervisor/manager and
Western Forest Products Inc. – Ability Management Program Page 4 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
employees are adequately trained and educated in participating in the Program, and liaising with external service providers and insurers to maintain quality service to employees.
ii. Will provide support to affected employees in accessing benefits or obtaining
appropriate healthcare and/or rehabilitation assistance. The AMC will also ensure the appropriate referrals are made to external service providers and insurers.
iii. Will coordinate and participate in Return to Work (RTW) meetings, including ensuring
all appropriate participants are in attendance, and all information relevant to return to work is gathered and made available. The AMC will also ensure the agreed upon Return to Work Plan (RTWP) is documented and endorsed by the employee and the supervisor/manager.
iv. Will ensure all work accommodations and RTWPs do not endanger the health and
safety of the employee, coworkers or others.
v. Will coordinate any independent assessments (e.g. ergonomic, medical, functional abilities evaluations).
vi. Will treat all documents with confidentiality and uphold the privacy of the employee.
c. Supervisor
i. Is responsible for ensuring the appropriate forms are completed and referrals are
made in a timely manner once an injury/illness has been reported. The Workplace Injury Package (WIP) should be provided to the injured/ill employee by the supervisor where appropriate (ie if First Aid not sought). o The WIP contains the following:
(a) WSBC Form 6 (Occupational injuries) (b) Functional Abilities Assessment form (c) Offer of modified work / Identification of available tasks
ii. Is responsible for providing accurate information on the affected employee’s job tasks.
iii. Will work with the affected employee, the AMC and all other involved stakeholders in
developing appropriate Stay at Work (SAW) and RTWPs. This includes identifying appropriate alternate duties / workplace accommodations.
iv. Will maintain open communication with the affected employee in a caring and
supportive manner during RTW coordination.
v. Will ensure co-workers are advised as needed regarding workplace accommodations and RTWPs. Supervisors will also accept concerns from co-employees and address accordingly to ensure health and safety is maintained while the returning employee is supported.
Western Forest Products Inc. – Ability Management Program Page 5 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
vi. Will meet with the employee regularly throughout the RTWP to monitor progress. All concerns that arise should be reported to the AMC for further review to monitor progress to ensure safe work duties.
d. Injured/Ill Employee
i. Will report discomfort, injuries and illnesses as a soon as possible to the manager/supervisor and First Aid Attendant (if work related).
ii. Will ensure the appropriate forms and documentation are completed and submitted in
a timely manner.
iii. Is responsible for participating in all SAW, RTW and work accommodation efforts by attending any meetings and providing all relevant information to involved stakeholders, including the manager/supervisor, treating physician, the AMC and the Union representative, where applicable. Relevant information includes any requests for work accommodations, functional and cognitive abilities and RTW prognosis.
iv. Must comply with treatment as recommended by his/her health care provider team.
This includes attending all medical and rehabilitation appointments as well as any independent assessments.
v. Is responsible for applying safe work practices and notifying the manager/supervisor
and/or the AMC of any concerns or change in status during the RTW or work accommodation period.
vi. Maintain all performance expectations while participating in a work accommodation
program or during the SAW / RTW period.
e. Co-workers
i. Co-workers are expected to support employees participating in work accommodation or during the SAW / RTW period by: o Supporting employees by understanding the purpose of the Program, o Knowing the scope of safe duties for the affected employee o Communicating any concerns or safety issues with the manager/supervisor.
f. Union Representative
i. Participate in RTW meetings as needed to assist in identifying safe and appropriate
workplace accommodations.
ii. Support the employee by advising him/her of their rights and responsibilities.
iii. Participate in Joint Committee Meetings as required to provide feedback on the development of the Program and its services.
Western Forest Products Inc. – Ability Management Program Page 6 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
g. Joint Ability Management Committee
i. Will involve the participation of a Senior Operating Manager or designate, a Senior Union Representative, the Operational AM lead, and as required, the AMC.
ii. Will meet regularly to review Program issues and outcomes, as well as on an ad hoc
basis to address any individual RTW cases.
iii. Will ensure the Program is conspicuously posted or otherwise made available to workers in physical or electronic format.
o Other possible methods may include handouts, manuals or reference materials.
iv. Will identify available alternate or modified duties specific to their operation.
o Alternate duties may include a range of standard opportunities and/or a list of
functionally acceptable restrictions.
(a) This list / document can be considered as the Offer of Modified Work as referenced in Section 14. Forms.
v. Will communicate all potential IM cases to the AMC.
h. First Aid Attendants
i. As the first point of contact for any work-related injuries, the First Aid Attendant will
assist the injured employee with processing the appropriate paperwork to report the incident.
ii. Will provide the injured employee with the WIP.
iii. Will advise the supervisor/manager of an incident or injury in a timely manner.
i. Human Resources
i. Advise on accommodation requests which may cause “undue hardship” as defined by
the BC Human Rights Code.
ii. Advise re other issues that may arise that pertain to Labour agreements and law.
j. Medical Practitioner
i. Complete Functional Abilities Assessment (FAA) form (included in the WIP) to accurately communicate employee’s physical abilities.
k. WorkSafeBC
i. Work cooperatively within the parameters of the Program to ensure a timely return to
work for injured employees.
Western Forest Products Inc. – Ability Management Program Page 7 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
7. BENEFITS
a. Short Term Disability Benefits
i. Contact the Benefits Administrator (Duncan HR Office) for further information on how to initiate a claim.
b. Long Term Disability Benefits
i. Contact the Benefits Administrator for further information on how to initiate a claim.
c. Employee and Family Assistance Program (EFAP)
i. WFP offers EFAP services for its employees through the local Assessment &
Resource services providers (ie Upper Island ARS, South Island ARS, etc.).
ii. Contact one of your local EFAP representatives for more information. 8. ABILITY MANAGEMENT PROCESS
a. Non-Occupational Illness/Injury
i. Employees who are absent from work for more than three (3) consecutive shifts may be requested to submit a completed FAA form within five (5) business days to the Operational AM lead.
ii. The purpose of the FAA is to:
o Provide information on the employee’s current functional abilities to assist in
identifying suitable job tasks, whether modified, temporary or permanent;
o Ensure the employee has sought appropriate medical attention and is compliant with treatment recommendations; and
o Provide information on the employee’s RTW prognosis.
iii. Employees are expected to fully participate in the Ability Management process which
includes ongoing communication with the supervisor/manager and the AMC, as well as being compliant with the rehabilitation/treatment plan and all RTW efforts.
iv. When during the course of case management, the employee is medically cleared to
RTW, the AMC will notify the immediate supervisor/manager upon receipt of the RTW information and RTW coordination will begin.
b. Occupational Injury/Illness
i. At the onset of injury, or as soon as medically possible, the employee must report the
incident to the supervisor/manager and see a First Aid Attendant so a First Aid Report can be filed. Should the employee require medical attention off-site, the employee will be provided with a WIP.
Western Forest Products Inc. – Ability Management Program Page 8 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
ii. The WIP must be completed by the employee and physician and forwarded to the supervisor/manager, and as required, the AMC for ongoing management. Should the injured employee require modified work duties, or remains absent from work; an updated FAA form will be required every two (2) weeks.
iii. WFP initiates contact with WorkSafeBC via its submission of the Form 7.
iv. Once the injured employee is cleared to return to work, RTW coordination will begin.
9. STAY AT WORK PROCESS
a. The SAW process is accessible to all employees who are experiencing discomfort that prohibits them from performing their regular duties. The goal of the SAW process is to safely facilitate full recovery by temporarily modifying the employee’s duties.
10. RETURN TO WORK PROCESS
a. The RTW process is accessible to all employees who are absent from work due to injury/illness, regardless of the nature of the medical condition. The goal of the RTW process is to safely assist the injured/ill employee back to his/her pre-disability regular job duties and hours. WFP understands that in some cases, the safest method is to implement a plan where the employee begins working on a modified work schedule and/or modified job tasks, with gradual increases in the job demands until all components of the pre-disability job are achieved.
b. All employees who are absent from work for more than three (3) consecutive shifts, as a
result of injury/illness, must provide written documentation from the treating physician stating the employee’s medical fitness to return to work.
c. Should the employee require modified job tasks or partial work hours, recommendations
endorsed by the physician or healthcare provider must be submitted to the supervisor/manager and the Operational AM lead on the FAA form. A RTW meeting between the employee, the supervisor/manager, the Operational AM lead (and the AMC as required) will be held to coordinate a RTWP. Where applicable or if requested by either party, the Union AM Committee representative may be present.
d. A finalized Plan will be documented on the RTWP form, must be signed by the employee,
and supervisor/manager, and must be within the employee’s current physical capabilities.
e. If necessary, the supervisor/manager may need to discuss the RTWP with co-workers to ensure health and safety is maintained. Co-workers are responsible for adhering to all health and safety guidelines and advise the supervisor/manager of any concerns with the Plan through the duration of the Plan. Co-workers are also expected to be supportive and respectful of the returning employee’s RTWP.
f. During the RTWP, the injured/ill employee is responsible for advising the
supervisor/manager of any changes to the employee’s medical status that may affect the duration of the Plan and any potential safety concerns or issues related to the Plan. An
Western Forest Products Inc. – Ability Management Program Page 9 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
additional RTW meeting may be required to revise the Plan. The employee is expected to continue with treatment and rehabilitation recommendations throughout the duration of the Plan; however, appointments should be scheduled outside of the planned work hours wherever possible.
11. WORKPLACE ACCOMMODATION
a. WFP is committed to maintaining the health and safety of all employees and to the prevention of disability-related absences. As such, WFP is able to accommodate employees who require a temporary or permanent change to his/her job tasks or schedule due to medical reasons up to the point of “undue hardship”, as defined by the BC Human Rights Code.
b. Requests for workplace accommodations do not need to follow an injury/illness-related
absence; requests for accommodation may be used as a preventative initiative to avoid any lost time (ie SAW).
c. Identifying and implementing suitable workplace accommodations is an individualized
process where the company and Union where applicable, remove barriers in the workplace that prevent the employee from participating in equal employment.
d. The identification of appropriate workplace accommodations involves the participation of
the employee, the supervisor/manager, the AMC, the union representative and the employee’s medical team.
e. Appropriate accommodations may include modifications to the work schedule, job tasks,
equipment, workstation, policy or procedure, and/or implementation of assistive devices.
f. If necessary, specialists will be consulted to ensure safety, necessity and possible solutions.
g. During an accommodation, the employee is responsible for identifying and communicating
any concerns, changes to their functional capacity, and/or any amending recommendations from their medical team. Failure to do so may result in delay of identifying appropriate solutions and may pose a health and safety risk to the employee and others.
h. Temporary Accommodations
i. Refers to modified work tasks or work schedule that is assigned to the employee for a
defined period of time.
ii. Temporary accommodations may be used to assist the employee in a transitional work plan that safely returns the employee back to pre-disability job tasks.
iii. In cases where it is deemed the employee requires permanent accommodations,
temporary accommodations can be used in the interim while a permanent solution is coordinated.
Western Forest Products Inc. – Ability Management Program Page 10 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
i. Permanent Accommodations
i. Once it is deemed that an employee’s condition is permanent or long term, with no improvement in the foreseeable future, permanent accommodations may be considered.
ii. The following criteria must be met:
o The employee cannot perform the essential duties of his/her own job even with
modifications to the job;
o Employee is qualified to perform the alternate job;
o Employee is able to perform the essential duties of the alternate job;
o Accommodation does not infringe on collective agreement wording, unless approved by a union representative; and
o A vacancy is available.
j. Order of Identifying Accommodations
i. Employee’s own job with modifications;
ii. Temporary accommodation within the same department and same job grade;
iii. Temporary accommodation within same department, but with different job grade;
iv. Temporary accommodation in a different department, but with same job grade;
v. Temporary accommodation in a different department, but with different job grade;
vi. Permanent accommodation in the same or different department with same job grade;
vii. Permanent accommodation in the same or different department with lower job grade;
viii. Permanent accommodation with a reduced job status (e.g. full time to part time); and
ix. Should no work accommodation be made and there is no reasonable prospect of the
employee returning to work in any capacity in the foreseeable future, the employee’s employment with WFP will be reviewed. Termination may be considered, subject to any collective agreement article, the Employment Standards Act, BC Human Rights Code and any other applicable legislation.
12. CONFIDENTIALITY
a. WFP is cognizant of the privacy and confidentiality of its employees and understands the sensitive nature of the flow of information and documentation.
Western Forest Products Inc. – Ability Management Program Page 11 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
b. The Program will be executed in accordance with the Personal Information Protection of Electronic Documents Act (PIPEDA) and WFP’s Employee Privacy Policy, and any other corporate, legal and/or regulatory document and data retention policies.
13. REFERENCES
a. Employee Privacy Policy
b. Occupational Health and Safety Policy 14. FORMS
a. Functional Abilities Assessment (FAA) form
b. WSBC Form 6 (Occupational Claims)
c. Offer of Modified Work
d. Return to Work Plan (RTWP) form 15. PROCESS FLOW CHARTS
a. See following pages
Western Forest Products Inc. – Ability Management Program Page 12 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
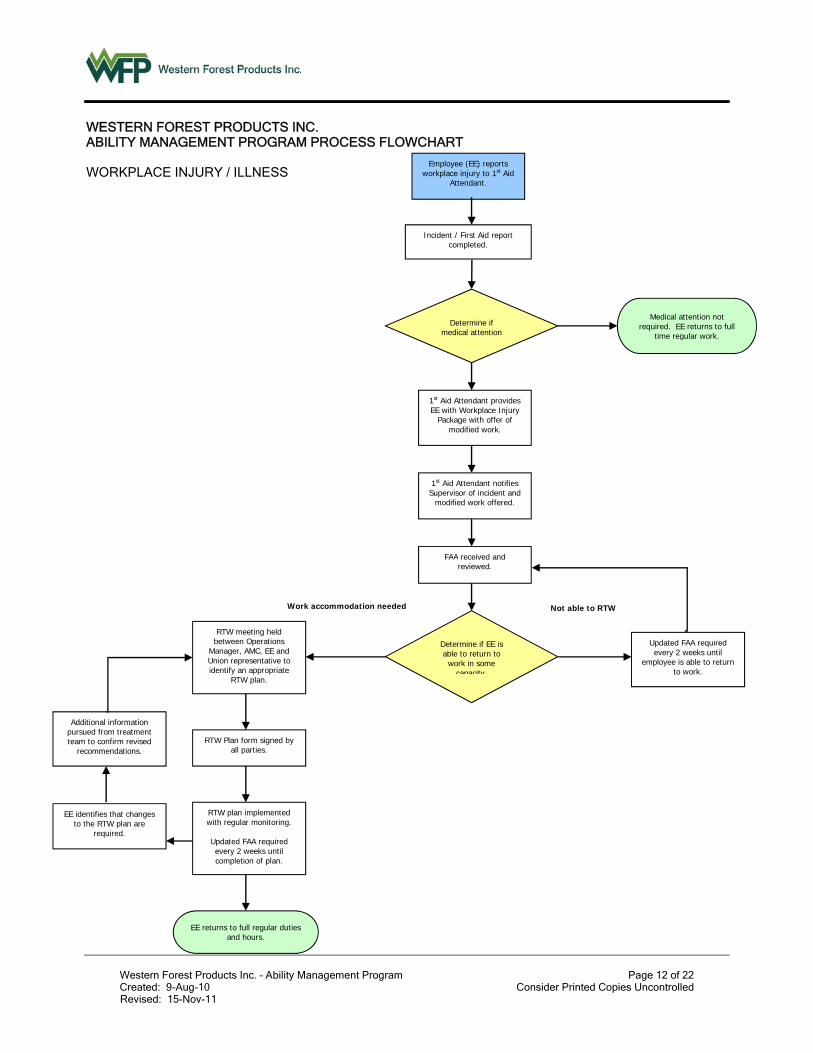
WESTERN FOREST PRODUCTS INC. ABILITY MANAGEMENT PROGRAM PROCESS FLOWCHART WORKPLACE INJURY / ILLNESS
Work accommodation needed
Additional information pursued from treatment team to confirm revised
recommendations.
EE identifies that changes to the RTW plan are
required.
RTW meeting held between Operations
Manager, AMC, EE and Union representative to identify an appropriate
RTW plan.
RTW Plan form signed by all parties.
RTW plan implemented with regular monitoring.
Updated FAA required every 2 weeks until completion of plan.
EE returns to full regular duties and hours.
Employee (EE) reports workplace injury to 1st Aid
Attendant.
1st Aid Attendant provides EE with Workplace Injury
Package with offer of modified work.
Incident / First Aid report completed.
FAA received and reviewed.
Determine if EE is able to return to
work in some capacity
Medical attention not required. EE returns to full
time regular work.
Determine if medical attention
d
1st Aid Attendant notifies Supervisor of incident and
modified work offered.
Updated FAA required every 2 weeks until
employee is able to return to work.
Not able to RTW
Western Forest Products Inc. – Ability Management Program Page 13 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
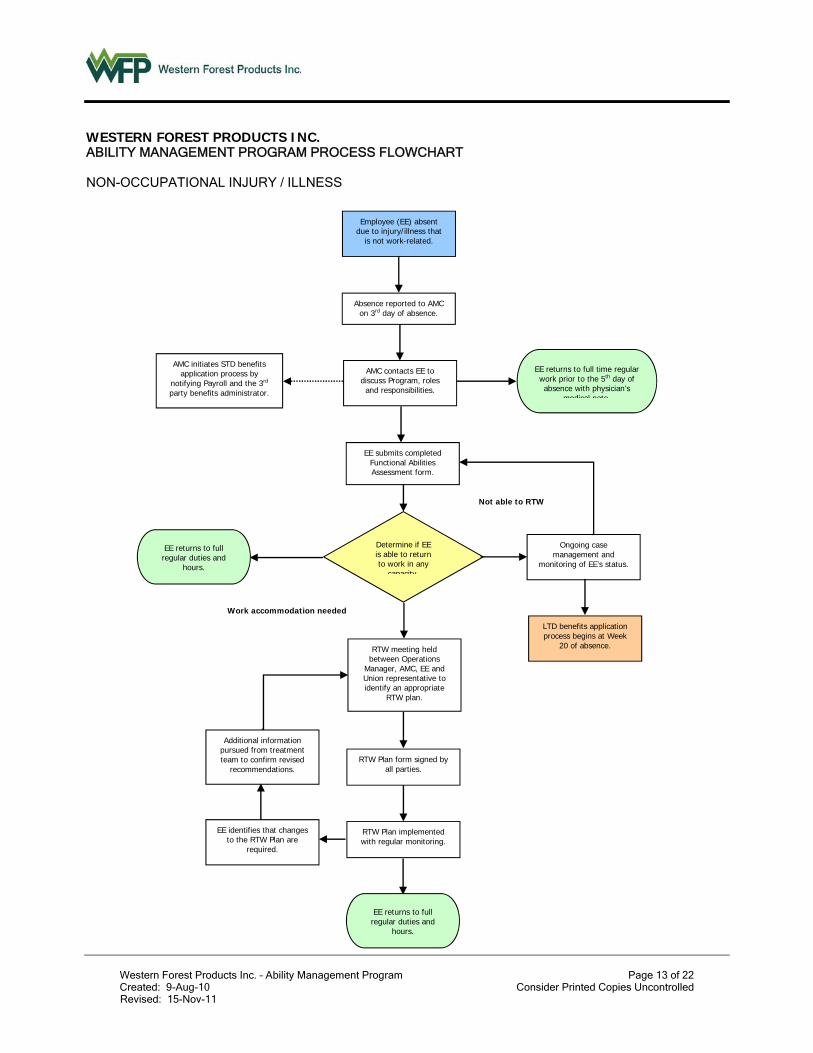
WESTERN FOREST PRODUCTS INC. ABILITY MANAGEMENT PROGRAM PROCESS FLOWCHART NON-OCCUPATIONAL INJURY / ILLNESS
Employee (EE) absent due to injury/illness that
is not work-related.
Absence reported to AMC on 3rd day of absence.
AMC contacts EE to discuss Program, roles and responsibilities.
EE submits completed Functional Abilities Assessment form.
AMC initiates STD benefits application process by
notifying Payroll and the 3rd party benefits administrator.
Ongoing case management and
monitoring of EE’s status.
Determine if EE is able to return to work in any
capacity
LTD benefits application process begins at Week
20 of absence.
Work accommodation needed
Not able to RTW
EE returns to full time regular work prior to the 5th day of absence with physician’s
medical note
Additional information pursued from treatment team to confirm revised
recommendations.
EE identifies that changes to the RTW Plan are
required.
RTW meeting held between Operations
Manager, AMC, EE and Union representative to identify an appropriate
RTW plan.
RTW Plan form signed by all parties.
RTW Plan implemented with regular monitoring.
EE returns to full regular duties and
hours.
EE returns to full regular duties and
hours.

Western Forest Products Inc. – Ability Management Program Page 14 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
This page intentionally left blank
Western Forest Products Inc. – Ability Management Program Page 15 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
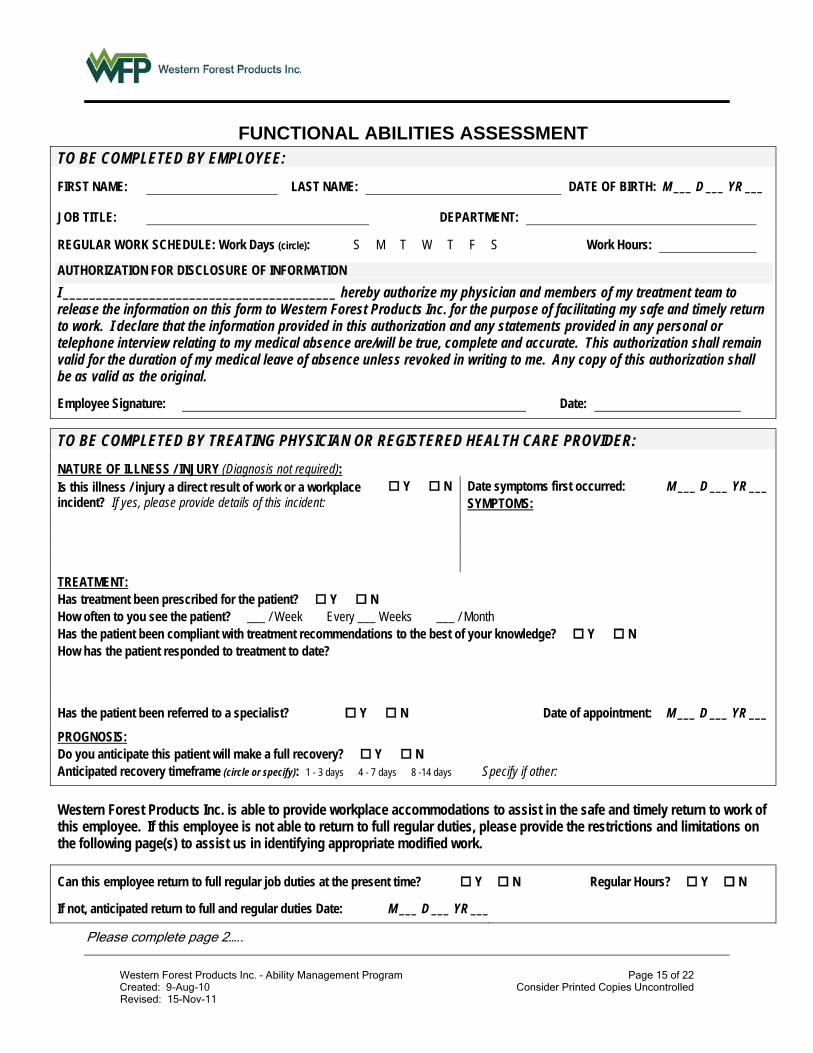
FUNCTIONAL ABILITIES ASSESSMENT TO BE COMPLETED BY EMPLOYEE:
FIRST NAME: LAST NAME: DATE OF BIRTH: M ___ D ___ YR ___
JOB TITLE: DEPARTMENT:
REGULAR WORK SCHEDULE: Work Days (circle): S M T W T F S Work Hours:
AUTHORIZATION FOR DISCLOSURE OF INFORMATION
I _________________________________________ hereby authorize my physician and members of my treatment team to release the information on this form to Western Forest Products Inc. for the purpose of facilitating my safe and timely return to work. I declare that the information provided in this authorization and any statements provided in any personal or telephone interview relating to my medical absence are/will be true, complete and accurate. This authorization shall remain valid for the duration of my medical leave of absence unless revoked in writing to me. Any copy of this authorization shall be as valid as the original.
Employee Signature: Date:
TO BE COMPLETED BY TREATING PHYSICIAN OR REGISTERED HEALTH CARE PROVIDER:
NATURE OF ILLNESS / INJURY (Diagnosis not required): Is this illness / injury a direct result of work or a workplace incident? If yes, please provide details of this incident:
Y N Date symptoms first occurred: SYMPTOMS:
M ___ D ___ YR ___
TREATMENT: Has treatment been prescribed for the patient? Y N How often to you see the patient? ___ / Week Every ___ Weeks ___ / Month Has the patient been compliant with treatment recommendations to the best of your knowledge? Y N How has the patient responded to treatment to date?
Has the patient been referred to a specialist? Y N Date of appointment: M ___ D ___ YR ___
PROGNOSIS: Do you anticipate this patient will make a full recovery? Y N Anticipated recovery timeframe (circle or specify): 1 - 3 days 4 - 7 days 8 -14 days Specify if other:
Western Forest Products Inc. is able to provide workplace accommodations to assist in the safe and timely return to work of this employee. If this employee is not able to return to full regular duties, please provide the restrictions and limitations on the following page(s) to assist us in identifying appropriate modified work.
Can this employee return to full regular job duties at the present time? Y N Regular Hours? Y N
If not, anticipated return to full and regular duties Date: M ___ D ___ YR ___
Please complete page 2…..
Western Forest Products Inc. – Ability Management Program Page 16 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
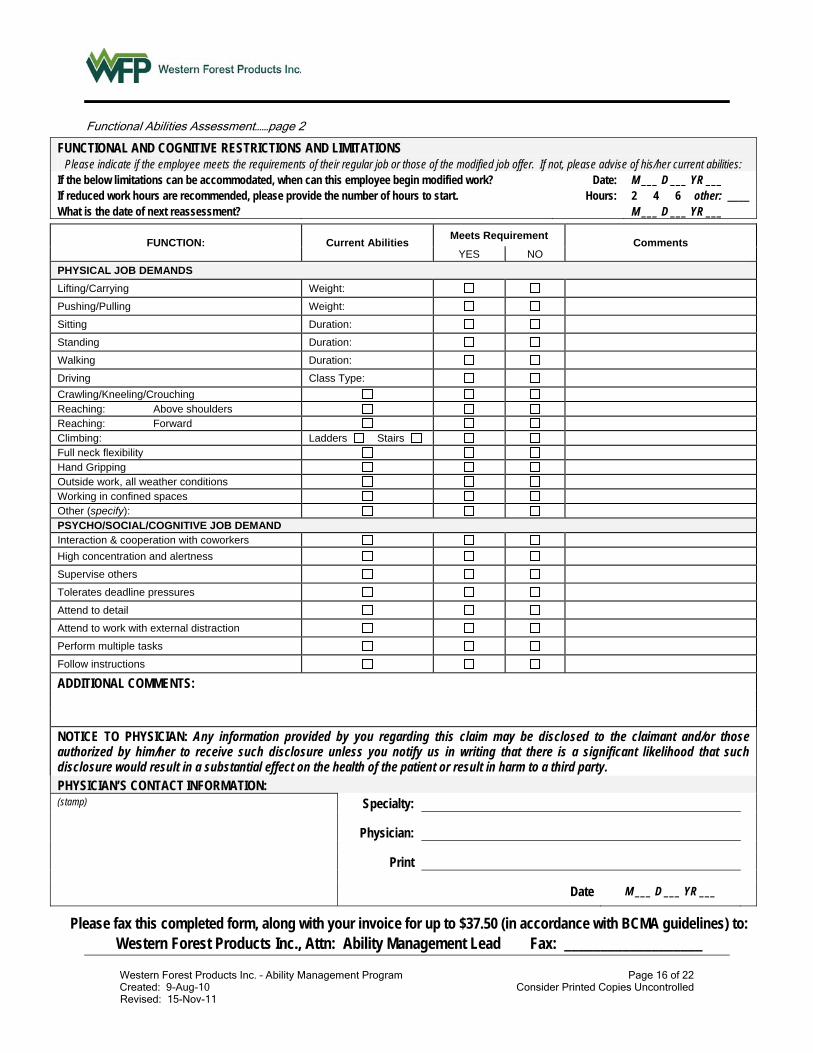
Functional Abilities Assessment……page 2
FUNCTIONAL AND COGNITIVE RESTRICTIONS AND LIMITATIONS Please indicate if the employee meets the requirements of their regular job or those of the modified job offer. If not, please advise of his/her current abilities:
If the below limitations can be accommodated, when can this employee begin modified work? Date: M ___ D ___ YR ___ If reduced work hours are recommended, please provide the number of hours to start. Hours: 2 4 6 other: ____ What is the date of next reassessment? M ___ D ___ YR ___
FUNCTION: Current Abilities Meets Requirement
Comments YES NO
PHYSICAL JOB DEMANDS
Lifting/Carrying Weight:
Pushing/Pulling Weight:
Sitting Duration:
Standing Duration:
Walking Duration:
Driving Class Type:
Crawling/Kneeling/Crouching Reaching: Above shoulders Reaching: Forward Climbing: Ladders Stairs Full neck flexibility Hand Gripping Outside work, all weather conditions Working in confined spaces Other (specify): PSYCHO/SOCIAL/COGNITIVE JOB DEMAND Interaction & cooperation with coworkers
High concentration and alertness
Supervise others
Tolerates deadline pressures
Attend to detail
Attend to work with external distraction
Perform multiple tasks
Follow instructions
ADDITIONAL COMMENTS:
NOTICE TO PHYSICIAN: Any information provided by you regarding this claim may be disclosed to the claimant and/or those authorized by him/her to receive such disclosure unless you notify us in writing that there is a significant likelihood that such disclosure would result in a substantial effect on the health of the patient or result in harm to a third party. PHYSICIAN’S CONTACT INFORMATION: (stamp) Specialty:
Physician:
Date M ___ D ___ YR ___
Please fax this completed form, along with your invoice for up to $37.50 (in accordance with BCMA guidelines) to: Western Forest Products Inc., Attn: Ability Management Lead Fax: ___________________
Western Forest Products Inc. – Ability Management Program Page 17 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
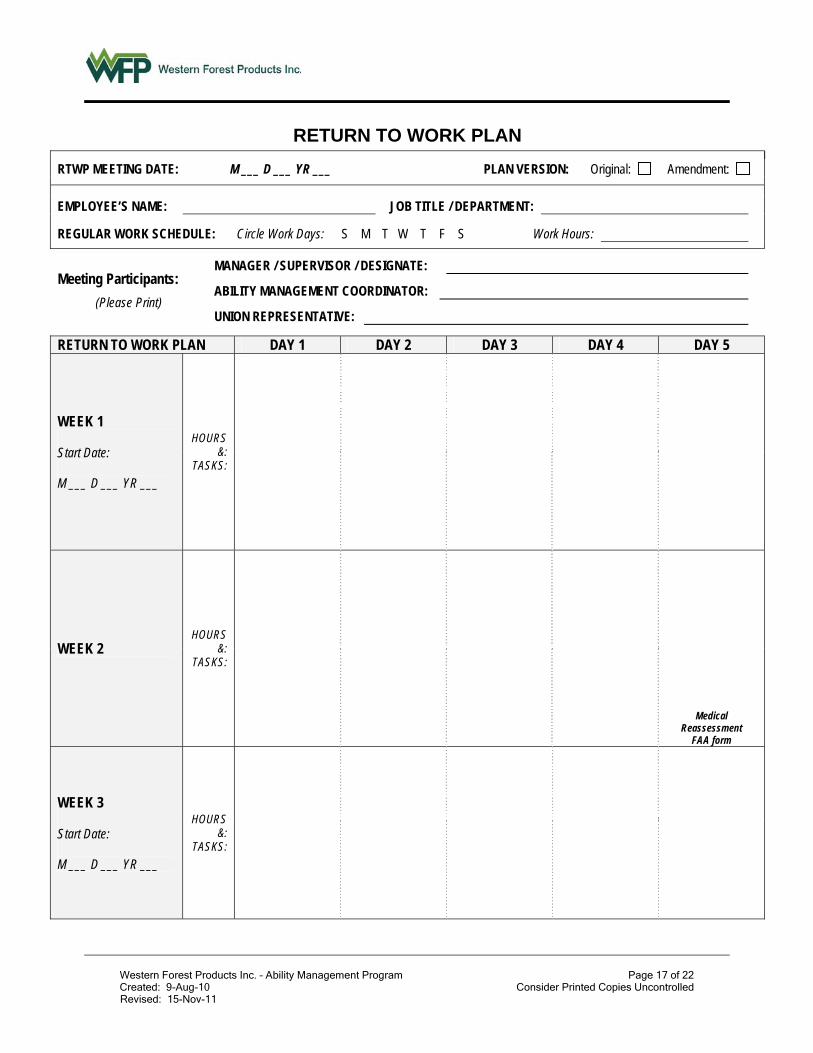
RETURN TO WORK PLAN
RTWP MEETING DATE: M ___ D ___ YR ___ PLAN VERSION: Original: Amendment:
EMPLOYEE’S NAME: JOB TITLE / DEPARTMENT:
REGULAR WORK SCHEDULE: Circle Work Days: S M T W T F S Work Hours:
Meeting Participants:
(Please Print)
MANAGER / SUPERVISOR / DESIGNATE:
ABILITY MANAGEMENT COORDINATOR:
UNION REPRESENTATIVE:
RETURN TO WORK PLAN DAY 1 DAY 2 DAY 3 DAY 4 DAY 5
WEEK 1 Start Date: M ___ D ___ YR ___
HOURS &:
TASKS:
WEEK 2 HOURS
&: TASKS:
Medical Reassessment
FAA form
WEEK 3 Start Date: M ___ D ___ YR ___
HOURS &:
TASKS:
Western Forest Products Inc. – Ability Management Program Page 18 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
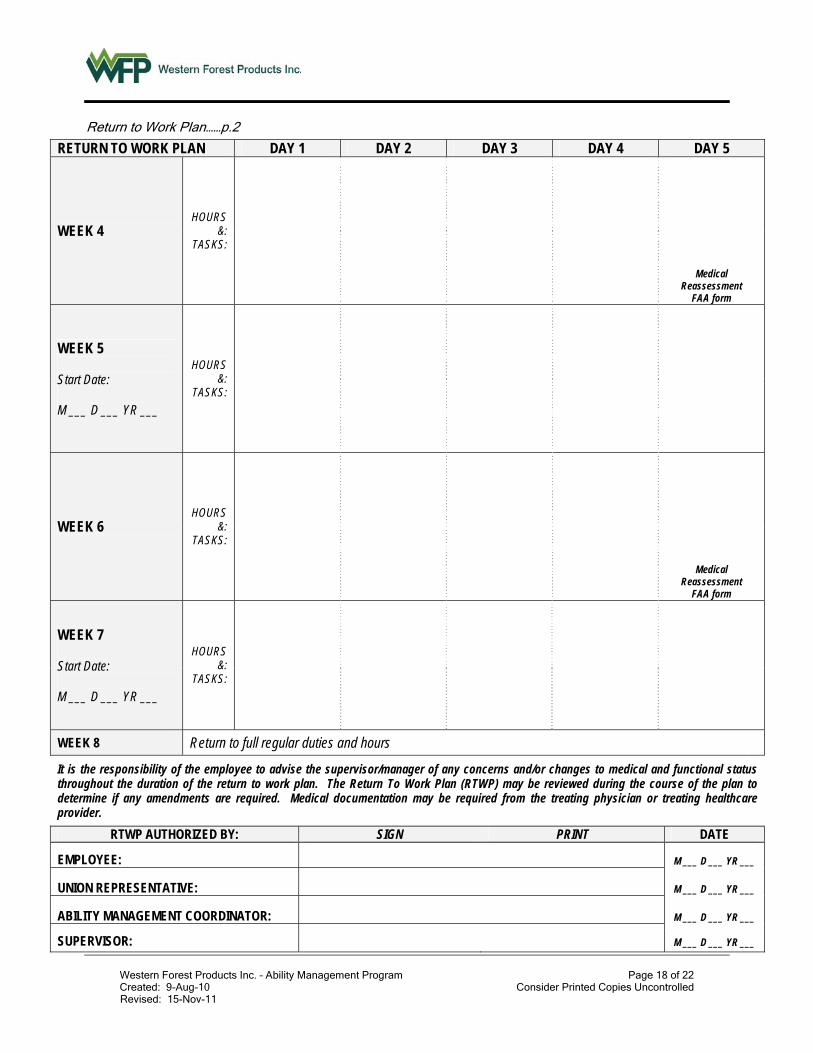
Return to Work Plan……p.2
RETURN TO WORK PLAN DAY 1 DAY 2 DAY 3 DAY 4 DAY 5
WEEK 4 HOURS
&: TASKS:
Medical Reassessment
FAA form
WEEK 5 Start Date: M ___ D ___ YR ___
HOURS &:
TASKS:
WEEK 6 HOURS
&: TASKS:
Medical Reassessment
FAA form
WEEK 7 Start Date: M ___ D ___ YR ___
HOURS &:
TASKS:
WEEK 8 Return to full regular duties and hours
It is the responsibility of the employee to advise the supervisor/manager of any concerns and/or changes to medical and functional status throughout the duration of the return to work plan. The Return To Work Plan (RTWP) may be reviewed during the course of the plan to determine if any amendments are required. Medical documentation may be required from the treating physician or treating healthcare provider.
RTWP AUTHORIZED BY: SIGN PRINT DATE
EMPLOYEE: M ___ D ___ YR ___
UNION REPRESENTATIVE: M ___ D ___ YR ___
ABILITY MANAGEMENT COORDINATOR: M ___ D ___ YR ___
SUPERVISOR:
M ___ D ___ YR ___
Western Forest Products Inc. – Ability Management Program Page 19 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
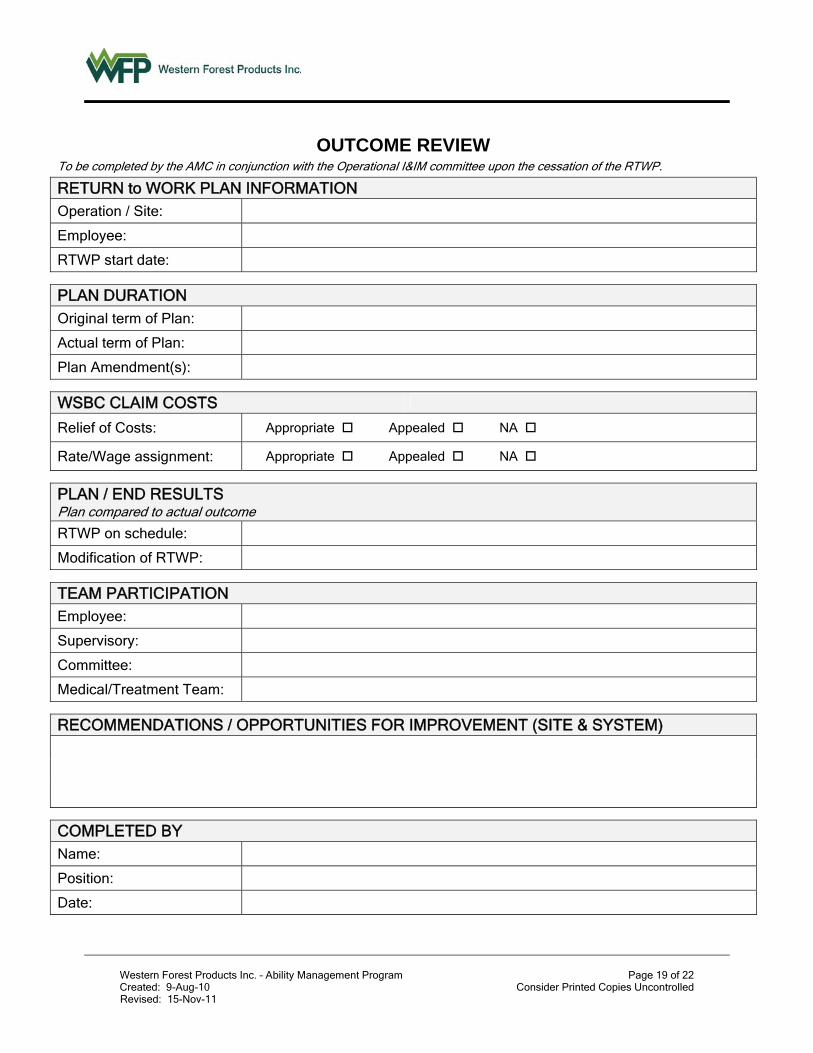
OUTCOME REVIEW To be completed by the AMC in conjunction with the Operational I&IM committee upon the cessation of the RTWP.
RETURN to WORK PLAN INFORMATION Operation / Site: Employee: RTWP start date:
PLAN DURATION Original term of Plan: Actual term of Plan: Plan Amendment(s):
WSBC CLAIM COSTS
Relief of Costs: Appropriate Appealed NA
Rate/Wage assignment: Appropriate Appealed NA
PLAN / END RESULTS Plan compared to actual outcome
RTWP on schedule: Modification of RTWP:
TEAM PARTICIPATION Employee: Supervisory: Committee: Medical/Treatment Team:
RECOMMENDATIONS / OPPORTUNITIES FOR IMPROVEMENT (SITE & SYSTEM)
COMPLETED BY Name: Position: Date:

Western Forest Products Inc. – Ability Management Program Page 20 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
This page intentionally left blank
Western Forest Products Inc. – Ability Management Program Page 21 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
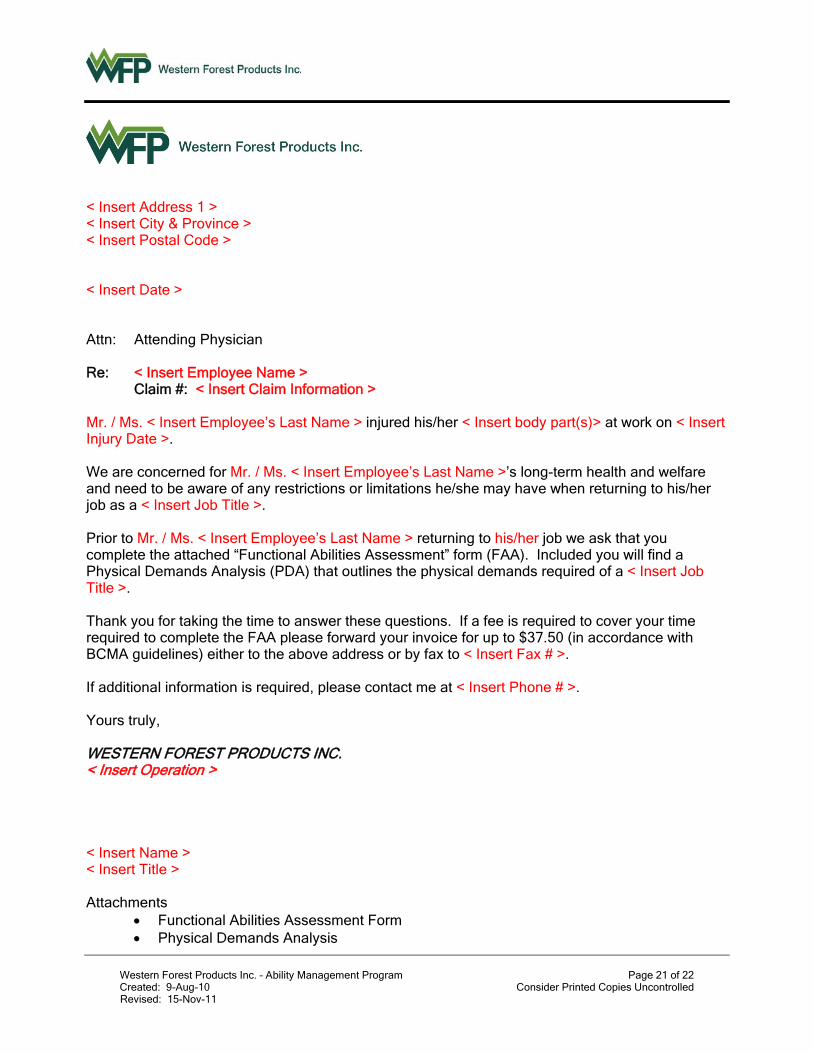
< Insert Address 1 > < Insert City & Province > < Insert Postal Code > < Insert Date > Attn: Attending Physician Re: < Insert Employee Name >
Claim #: < Insert Claim Information > Mr. / Ms. < Insert Employee’s Last Name > injured his/her < Insert body part(s)> at work on < Insert Injury Date >. We are concerned for Mr. / Ms. < Insert Employee’s Last Name >’s long-term health and welfare and need to be aware of any restrictions or limitations he/she may have when returning to his/her job as a < Insert Job Title >. Prior to Mr. / Ms. < Insert Employee’s Last Name > returning to his/her job we ask that you complete the attached “Functional Abilities Assessment” form (FAA). Included you will find a Physical Demands Analysis (PDA) that outlines the physical demands required of a < Insert Job Title >. Thank you for taking the time to answer these questions. If a fee is required to cover your time required to complete the FAA please forward your invoice for up to $37.50 (in accordance with BCMA guidelines) either to the above address or by fax to < Insert Fax # >. If additional information is required, please contact me at < Insert Phone # >. Yours truly, WESTERN FOREST PRODUCTS INC. < Insert Operation > < Insert Name > < Insert Title > Attachments
Functional Abilities Assessment Form Physical Demands Analysis
Western Forest Products Inc. – Ability Management Program Page 22 of 22 Created: 9-Aug-10 Consider Printed Copies Uncontrolled
Revised: 15-Nov-11
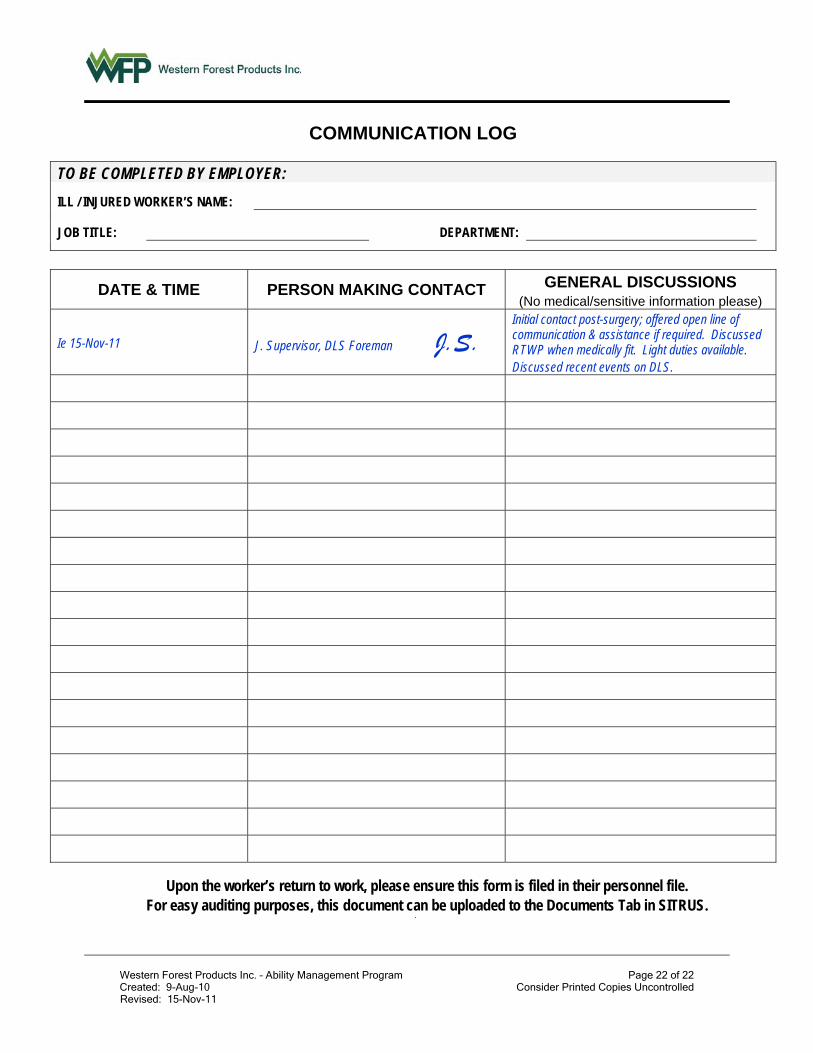
COMMUNICATION LOG
TO BE COMPLETED BY EMPLOYER:
ILL / INJURED WORKER’S NAME:
JOB TITLE: DEPARTMENT:
DATE & TIME PERSON MAKING CONTACT GENERAL DISCUSSIONS (No medical/sensitive information please)
Ie 15-Nov-11 J. Supervisor, DLS Foreman J.S. Initial contact post-surgery; offered open line of communication & assistance if required. Discussed RTWP when medically fit. Light duties available. Discussed recent events on DLS.
Upon the worker’s return to work, please ensure this form is filed in their personnel file. For easy auditing purposes, this document can be uploaded to the Documents Tab in SITRUS.