abruptio placenta vld
TRANSCRIPT

ABRUPTIO PLACENTAEABRUPTIO PLACENTAE
• DR V L DESHMUKH
• ASSO PROF
• DEPT OBGY
• GMCH A,BAD
Abruptio PlacentaeAbruptio Placentae
• Abruptio – tearing away from
• Placentae – placenta
• It is a Latin word
Synonyms Synonyms
• Accidental Haemorrhage (Great Britain)
• Ablatio Placentae
• Premature separation of placenta
Definition:
• It is one form of Antepartum Haemorrhage
where bleeding occurs due to premature
separation of normally situated placenta.

a) Retreoplacental haematomo b) Revealed c) Concealed d) Mixed
1. Revealed : Most common
Blood loss is visible as the blood drops down
between membrane & decidua & come out
through cervical canal.
2. Concealed : Rare
a) Effusion of blood behind the placenta but its
margins still remain adherent
b) Placenta completely separated but
membranes intact
c) Blood enter amniotic sac after breaking
membranes
d) Fetal Head closely applied to lower uterine
segment.
1. Mixed – quite common
- Some amount of blood is inside & some
expelled.
Incidence
- 1 in 150 deliveries

• Perinatal mortality – 15 – 20%
• Maternal mortality – 2 – 5 %
Etiology:
a) Maternal Hypertension: 44% of all cases
mechanism- Spasm of vessels in utero
placental bed i.e. of decidual spiral artery
causes endothelial damage & rupture of
vessels leading to haemorrhage.


b) Maternal trauma – 1.5 – 9.5 %
- Motor vehicle accidents (MVA)
- Assaults, falls.
c) Foetal trauma –
- Attempted external cephalic version
- Needle puncture at amniocentesis
d) Cigarette Smoking –
- Decidual necrosis

e) Cocaine abuse – Onset of labour with
placental abruption in 4 of 23 women
immediately after IV self infection of cocaine.
f) Short umbilical cord – Mechanical pull during
labour.
g) Sudden Uterine decompression
1. Delivery of first baby of twins
2. PROM
3. Sudden escape of liquor amni in hydramnios.
h) Advanced Maternal age
i) Thrombophilias
j) Folic acid deficiency
k) Sick placenta
l) Retroplacental fibromyoma
m) Idiopathic
n) Recurrence increase 10 fold.

Pathogenesis:
• Initiated by Haemorrhage into decidua basalis.
• The decidua splits leaving thin layer adherent
to the myometrium
• Subsequently there is development of decidual
Haematoma that leads to separation
compression & ultimate destruction of
placenta.
• Sometimes
– Decidual spiral artery rupture RP Haematoma separation of placenta inability of uterus to contract& control the torn vessels.
– Changes in other organs• Liver – Fibrin knots
• Kidney – Acute cortical necrosis or acute tubular necrosis, proteinurea.
• Blood coagulopathy – Due to excess consumption of plasma fibrinogen due DIC & RP bleeding.

Investigation :
• For evaluation of haemostatic system in
patients with abruptio placentae, most
laboratories use DIC profile.
• It includes
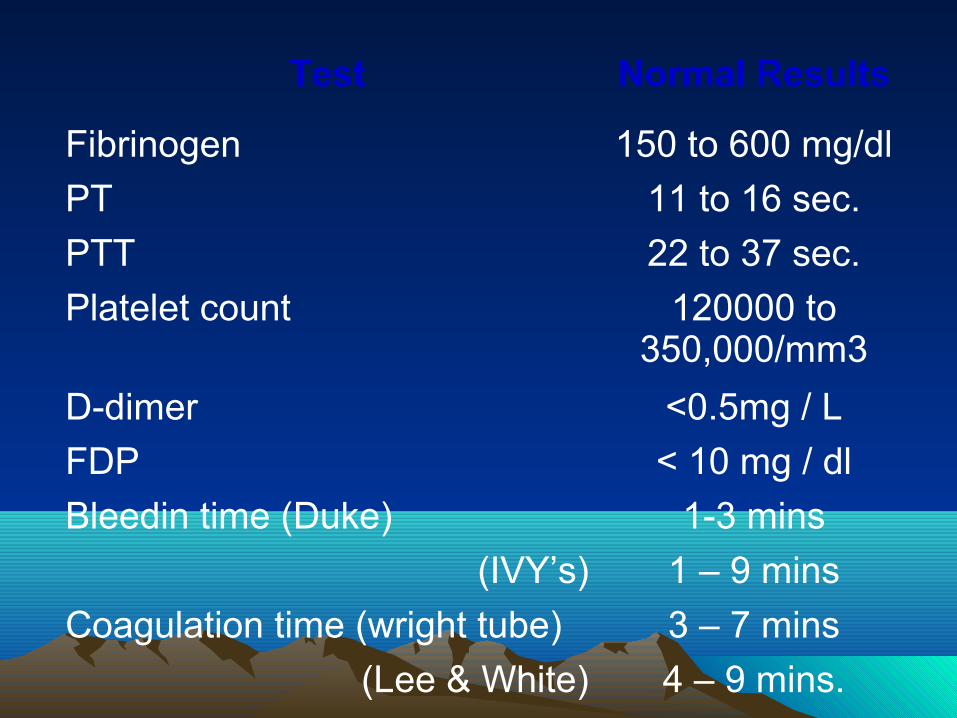
Test Normal Results
Fibrinogen 150 to 600 mg/dl
PT 11 to 16 sec.
PTT 22 to 37 sec.
Platelet count 120000 to 350,000/mm3
D-dimer <0.5mg / L
FDP < 10 mg / dl
Bleedin time (Duke) 1-3 mins
(IVY’s) 1 – 9 mins
Coagulation time (wright tube) 3 – 7 mins
(Lee & White) 4 – 9 mins.

• Clot observation test (weiner)
– 5 ml of venous blood placed in 15 ml dry test
tube & kept at 370C
– CT < 6min, fibrinogen level > 150 mg%
no clot < 30 min,fibrinogen level < 100 mg %
• FDP
– Latex agglutination test
– In DIC > 80 ug / ml
• D-dimer
– Specific component of fibrin break down
– Latex agglutination method.
– In DIC > 200 mg / L
• Estimation of fibrinogen
– Blood sample collected in EDTA vial critical
level 100 mg %
Diagnosis of abruptio placentae is more clinical Diagnosis of abruptio placentae is more clinical rather than USG findings.rather than USG findings.
S/S Frequency
Vaginal bleeding 78%
Uterine tenderness /back pain
66%
Fetal distress 60%
High frequency contractions 17%
Hypertonus 17%
Idiopathic preterm labour 22%
Dead fetus 15%


• Classification of placental abruption is based
on extent of separation (ie, partial vs complete)
and location of separation (ie, marginal vs
central). Clinical characteristics include the
following:
Class 0 is asymptomatic. Diagnosis is made
retrospectively by finding an organized blood
clot or a depressed area on a delivered
placenta.

Class 1 is mild and represents approximately 48%
of all cases. Characteristics include the
following:
• No vaginal bleeding to mild vaginal bleeding
• Slightly tender uterus
• Normal maternal BP and heart rate
• No coagulopathy
• No fetal distress

Class 2 is moderate and represents approximately 27% of
all cases Characteristics include the following:
• No vaginal bleeding to moderate vaginal Bleeding
• Moderate-to-severe uterine tenderness with possible
tetanic contractions
• Maternal tachycardia with orthostatic changes in BP
and heart rate
• Fetal distress
• Hypofibrinogenemia (ie, 50-250 mg/dL)

Class 3 is severe and represents approximately
24% of all cases. Characteristics include the
following:
• No vaginal bleeding to heavy vaginal bleeding
• Very painful tetanic uterus
• Maternal shock
• Hypofibrinogenemia (ie, <150 mg/dL)
• Coagulopathy
• Fetal death

• Role of USG in Abruptio placentae – – locate RP clot (20-25%)
• Estimation of blood loss– Wt. of RP clot in gm x 3
• Pain due to RP clot causing intravasation of
blood & disruption of myometrial fibres.
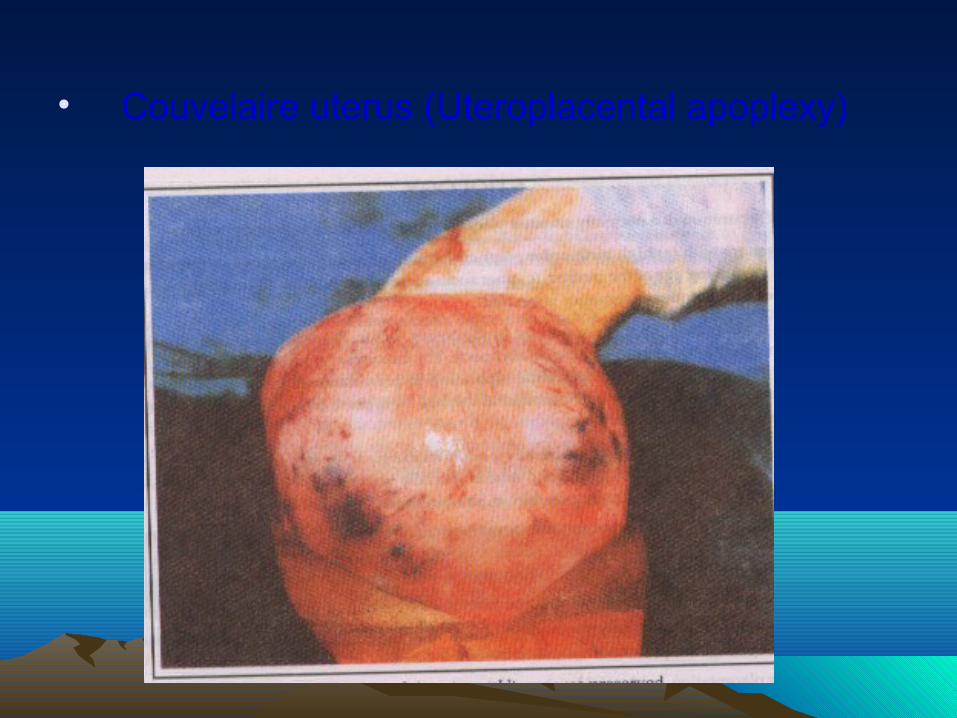
• Couvelaire uterus (Uteroplacental apoplexy)

Microscopic appearance
• Due to more severe & wide spread extravasation of blood into the uterine musculature & beneath the uterine serosa.
• Occasionally seen beneath the tubal serosa, connective tissue of broad ligament, substance of ovaries & in peritoneal cavity

• Incidence (unpredictable)
• Myometrial Haemotomas seldom interfere with
uterine contractions to cause PPH.
• Hence not indication for hysterectomy.
• Naked eye appearance uterus of dark port
wine colour.