abs lab 8. extraperitoneal abdominal viscera page … 5...anatomic exposures in vascular surgery....
TRANSCRIPT

ABS Lab 8. Extraperitoneal Abdominal Viscera Page 8‐1
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
BWH 2015 GENERAL SURGERY RESIDENCY PROCEDURAL ANATOMY COURSE
5. ABDOMINOPELVIC VASCULAR PROCEDURES
CONTENTS 5.1 ORGANIZATION OF THE RETROPERITONEUM ........................................................................................... 2
5.2 ABDOMINAL AORTA ................................................................................................................................... 6
5.3 ABDOMINOPELVIC VASCULAR PROCEDURES ......................................................................................... 10
RETROPERITONEAL APPROACH TO THE ABDOMINAL AORTA (AND DISTAL DESCENDING THORACIC AORTA) .................................................................................................................................................... 10
LEFT VISCERAL MEDIAL ROTATION (MATTOX MANEUVER) FOR TRANSPERITONEAL SUPRARENAL AORTIC CONTROL ................................................................................................................................... 13
TRANSPERITONEAL APPROACH TO THE ABDOMINAL AORTA FOR INFRARENAL CONTROL ................. 13
OPEN ABDOMINAL AORTIC ANEURYSM REPAIR .................................................................................... 15
COMMON, INTERNAL, AND EXTERNAL ILIAC ARTERY (CIA, IIA, EIA) EXPOSURE AND BYPASS .............. 21
AORTOFEMORAL BYPASS ....................................................................................................................... 23
SMA EXPOSURE (“FINDING THE SMA”) .................................................................................................. 24
SMA EMBOLECTOMY .............................................................................................................................. 27
SMA BYPASS ............................................................................................................................................ 28
CONTROL OF THE PORTAL VEIN ............................................................................................................. 29
RIGHT MEDIAL VISCERAL ROTATION (CATTELL‐BRAASCH MANEUVER) ................................................ 30
CONTROL OF THE (INFRA‐ AND RETROHEPATIC) IVC ............................................................................. 31
5.4 RETROPERITONEAL TRAUMA ZONES ....................................................................................................... 34
5.5 POSTERIOR ABDOMINAL WALL ............................................................................................................... 36

ABS Lab 8. Extraperitoneal Abdominal Viscera Page 8‐1
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
BWH 2015 GENERAL SURGERY RESIDENCY PROCEDURAL ANATOMY COURSE
5. ABDOMINOPELVIC VASCULAR PROCEDURES
March 12, 2015
OBJECTIVES FOR LABORATORY 5
After successfully completing Laboratory 5, you will be able to do the following.
SKILLS OBJECTIVES
1. Review positioning and incisions to access the abdominal aorta, including midline and retroperitoneal (“hockeystick”) incisions and the portions of the aorta optimally visualized via each
2. Review how to rapidly perform right medial visceral rotation (Cattell‐Brasch maneuver) and left medial visceral rotation (Mattox maneuver) performed in laboratory 3
3. Perform transperitoneal aortic exposure and obtain supraceliac, infrarenal, transhiatal thoracic aortic control
4. Perform open abdominal aortic aneurysm repair and proximal anastomosis for aortobifemoral (ABF) bypass
5. Locate the superior mesenteric artery (SMA) and perform SMA embolectomy and bypass
6. Expose the common, external, and internal iliac arteries and perform bypasses to each
7. Perform maneuvers to control hemorrhage from portal vein and retrohepatic inferior vena cava injuries
KNOWLEDGE OBJECTIVES
1. Describe the composition of the perirenal fascia and its role in organizing the retroperitoneum.
2. Explain the embryonic basis for the arterial supply of the gastrointestinal system in the adult. Describe the foregut, midgut, and hindgut, and the unpaired branch of the aorta supplying each embryonic division.
3. Contrast the structures supplied by paired versus unpaired branches of the abdominal aorta. Contrast the venous drainage pathways of structures supplied by paired versus unpaired branches of the abdominal aorta
4. Describe the trauma zones useful for characterizing retroperitoneal hematomata.
SUGGESTED READINGS
Cronenwett JL, Johnston KW. Rutherford’s Vascular Surgery. Saunders, an imprint of Elsevier, Inc., Philadelphia, PA. 2014.
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Zollinger R Jr., Ellison E. Zollinger’s Atlas of Surgical Operations, 9th Ed. McGraw Hill, New York. 2010.
Hirshberg A, Mattox KL. Top Knife: The Art & Craft of Trauma Surgery. tfm Publishing Ltd, Nr Shrewsbury, UK. 2005.

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐2
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
5. ABDOMINOPELVIC VASCULAR PROCEDURES 5.1 ORGANIZATION OF THE RETROPERITONEUM
The retroperitoneum is the region of extraperitoneal connective tissue posterior to the peritoneal sac. The retroperitoneum is continuous anteriorly with the preperitoneal connective tissue of the anterolateral abdominal wall and inferiorly with the infraperitoneal connective tissue surrounding the pelvic viscera (Figure 5‐1). The retroperitoneum lies between the lining deep fascia over the posterior abdominal wall muscles and diaphragm and the parietal peritoneum forming the posterior portion of the peritoneal sac. Structures in the retroperitoneum include the abdominal aorta and its branches, the inferior vena cava and its tributaries; the adrenal (suprarenal) glands; the kidneys and ureters; clusters of abdominal lymph nodes surrounding the vessels; and autonomic nerves supplying the abdominal and pelvic organs.
Two types of retroperitoneal fascia
The variety of retroperitoneal fasciae and ligaments can be divided into two basic types.
1. Lining deep fascia (somatic fascia) covering muscles. The lining deep fascia of the abdominopelvic cavity forms a continuous layer distinguished by regional muscle names. The lining deep fasciae of the retroperitoneum are the quadratus lumborum fascia, psoas fascia, diaphragmatic fascia, iliac fascia, and transversalis fascia. The medial arcuate ligament and lateral arcuate ligament are thickened portions of the psoas fascia and the quadratus lumborum fascia that provide attachment for the posterior muscle fibers of the diaphragm lateral to the crura. The phrenoesophageal ligament is an upward extension of the inferior diaphragmatic fascia that attaches to the wall of the esophagus superior to the esophageal hiatus.
2. Condensations of collagen and elastic fibers within the retroperitoneal loose connective tissue given descriptive or eponymous names. All loose connective tissue consists primarily of adipocytes, tough collagen fibers, and elastic fibers. In certain regions, collagen fibers and elastic fibers within the loose connective tissue condense to form demonstrable named fasciae or ligaments. Named condensations of retroperitoneal loose connective tissue include the perirenal fascia surrounding the kidney and perirenal fat, the ligament of Trietz attaching the duodenojejunal junction to the deep fascia of the right diaphragmatic crus, and the phrenicosplenic ligament attaching the splenic capsule to the deep fascia covering the inferior surface of the diaphragm.
In the abdomen, the term ligament is also used to describe remnants of embryonic structures, such as the ligamentum teres, or double layered peritoneal reflections such as the triangular and coronary ligaments of the liver or the splenorenal ligament.
Perirenal fascia
The perirenal fascia is a demonstrable condensation of collagen fibers surrounding the perirenal space (Figure 5‐1) within the retroperitoneum. The anterior and posterior layers of the perirenal fascia are continuous. The anterior layer of the perirenal fascia (Gerota fascia) extends across the midline; the posterior layer of the perirenal fascia (Zuckerkandl fascia) fuses posteriorly with the deep fascia covering the posterior abdominal wall muscles and spine. The lateroconal fascia extends laterally from the junction between the anterior and posterior layers of the perirenal fascia to fuse with the transversalis fascia on the inner surface of the anterolateral abdominal wall.
The perirenal fascia encloses the perirenal space. The perirenal space contains perirenal fat and the adrenal glands, kidneys, proximal ureters, aorta and initial portions of its branches, and inferior vena and terminal portions of its tributaries.
The pararenal space lies outside the perirenal space and contains pararenal fat (Figure 5‐1).

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐3
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Figure 5‐1. Retroperitoneal structures and organization. (Modified from Netter Atlas of Human Anatomy, 5th Edition.
Philadelphia: Elsevier, 2010.)

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐4
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Three ways to be retroperitoneal
During embryonic development, the urogenital system and major blood vessels developed within the retroperitoneal connective tissue.
1. ‘Primarily retroperitoneal’ organs include the major blood vessels, kidneys, ureters, gonads, and adrenals. The ‘primarily retroperitoneal’ organs developed in the retroperitoneum and stayed there despite subsequent developmental events.
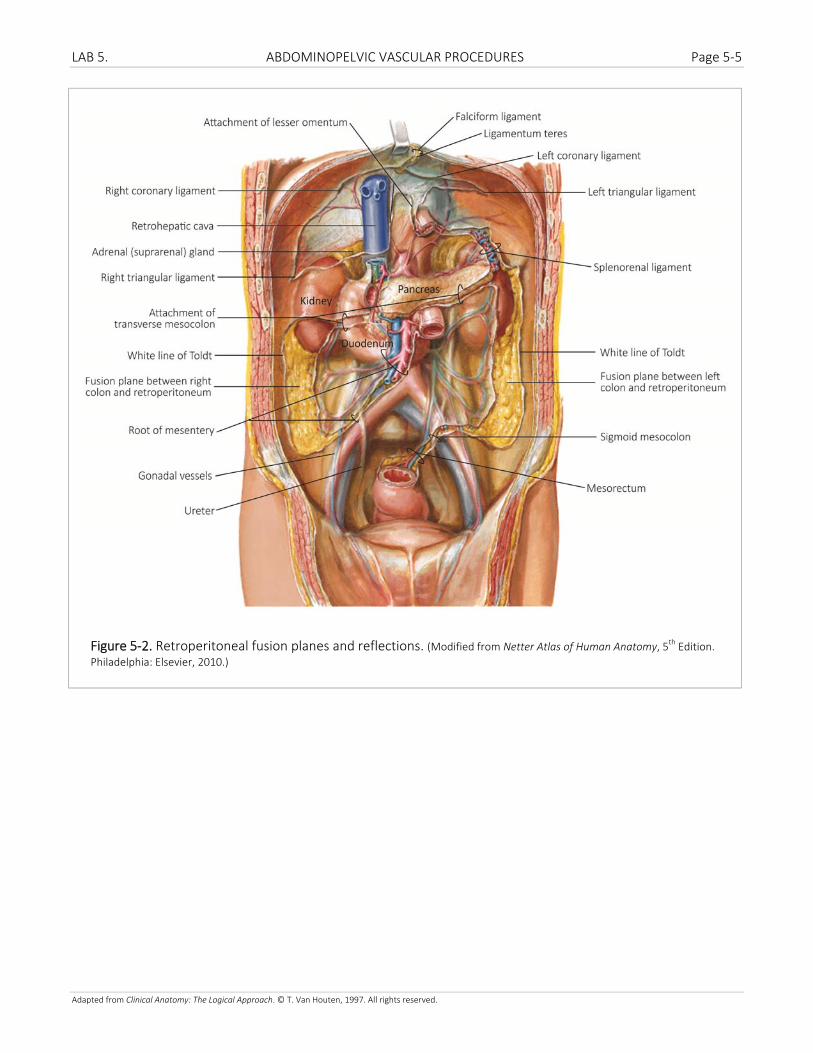
During the early stages of embryonic development, the gastrointestinal system and spleen developed between the two layers of the dorsal mesentery, and the entire gastrointestinal tract and spleen were ‘intraperitoneal’. The dorsal mesentery also provided pathways for neurovascular structures to travel between the retroperitoneum and the ‘intraperitoneal’ gastrointestinal organs and spleen. Two waves of contact between regions of the gastrointestinal organs and the posterior parietal peritoneum altered this simple configuration (Figure 5‐2).
2. The first wave of ‘secondarily retroperitoneal’ organs includes the second, third, and fourth parts of the duodenum and the pancreas proximal to the tail. The duodenum and pancreas came to rest against the posterior parietal peritoneum during the rotation of the stomach and the early elongation and rotation of the intestines. Fusion between the posterior parietal peritoneum and the visceral peritoneum and mesenteries of the duodenum and pancreas is relatively complete. Although the duodenum can be mobilized more easily, mobilization of the pancreas is difficult and carries a higher risk of bleeding, and fluids leaking from pancreatic tissues spread readily through the retroperitoneal loose connective tissue.
3. The second wave of ‘secondarily retroperitoneal’ organs includes the left (ascending) colon and right (descending) colon. The left and right colon came to rest against the posterior parietal peritoneum as the intestines returned to the abdomen following their herniation into the umbilicus. Although fusion between the posterior parietal peritoneum and the visceral peritoneum and mesenteries of the left and right colon occurred, a well‐defined ‘bloodless’ fusion plane persists, separating the left and right colonfrom the rest of the retroperitoneum. The left and right colon are relatively easy to mobilize without risk of significant bleeding. One exception occurs in portal hypertension, however, as portal‐systemic shunts occur across the fusion plane.
LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐5
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Figure 5‐2. Retroperitoneal fusion planes and reflections. (Modified from Netter Atlas of Human Anatomy, 5th Edition.
Philadelphia: Elsevier, 2010.)

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐6
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
5.2 ABDOMINAL AORTA
Unpaired branches of the abdominal aorta
Unpaired branches of the abdominal aorta supply unpaired abdominal organs of the gastrointestinal tract. The median sacral artery is an unfortunate exception to this rule (Figure 5‐3).
Branches of the celiac axis supply foregut structures including the stomach, first part of the duodenum, liver, gallbladder, and pancreas. A branch of the celiac axis also supplies the spleen.
Branches of the superior mesenteric artery supply midgut derivatives including the remainder of the duodenum, the jejunum, the ileum, the ascending colon, most of the transverse colon.
Branches of the inferior mesenteric artery supply hindgut derivatives including the splenic flexure of the transverse colon, descending colon, sigmoid colon, and proximal rectum.
Portal vein tributaries receive blood from all organs supplied by unpaired branches of the aorta (except the median sacral artery) (Figure 5‐3).

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐7
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Figure 5‐3. Unpaired branches of the abdominal aorta and hepatic portal tributaries. (Modified from Netter
Atlas of Human Anatomy, 5th Edition. Philadelphia: Elsevier, 2010.)

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐8
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Paired branches of the abdominal aorta supply the diaphragm and trunk wall or paired adrenal or urogenital
organs (Figure 5‐4).
Paired somatic branches of the abdominal aorta include the inferior phrenic arteries supplying the diaphragm and the paired segmental subcostal arteries and lumbar arteries 1‐4 supplying the trunk wall. The anastomoses between the subcostal and lumbar arteries and the superior and inferior epigastric arteries provides an important collateral arterial pathway.
Paired visceral branches of the abdominal aorta include the renal arteries, adrenal arteries, and gonadal arteries.
Inferior caval tributaries receive blood from all regions supplied by paired branches of the abdominal aorta. Caval‐caval anastomoses are found both anteriorly (subcostal and lumbar veins to superior and inferior epigastric veins) and posteriorly (subcostal and intercostal veins to ascending lumbar veins). The ascending lumbar veins are continuous superiorly with the azygos system in the chest.
Both the left testicular vein and left adrenal vein drain into the left renal vein (Figure 8‐8). The right testicular vein and right adrenal vein drain directly into the inferior vena cava.
Surgical approach to the abdominal aorta. There are two options for surgical exposure of the abdominal aorta: (1) transperitoneal and (2) retroperitoneal. The two are equivalent in many circumstances (data on outcomes are conflicting), but each may be favored in the following situations:
Transperitoneal
‐ Emergent cases (e.g. ruptured AAA)
‐ Need to address or assess nonvascular intra‐abdominal viscera
‐ Exposure of the right renal, external iliac, internal iliac, and femoral arteries
Retroperitoneal
‐ Exposure of the visceral, supraceliac, or distal descending thoracic segments of the aorta
‐ Hostile abdomens
‐ Obese patients
Due to previous dissections, we will not be performing the retroperitoneal approach. However, one should be familiar with how it is performed …

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐9
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Figure 5‐4 Paired branches of the aorta and caval tributaries. (Modified from Netter Atlas of Human Anatomy, 5th
Edition. Philadelphia: Elsevier, 2010.)
LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐10
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
RETROPERITONEAL APPROACH TO THE ABDOMINAL AORTA (AND DISTAL DESCENDING THORACIC AORTA)
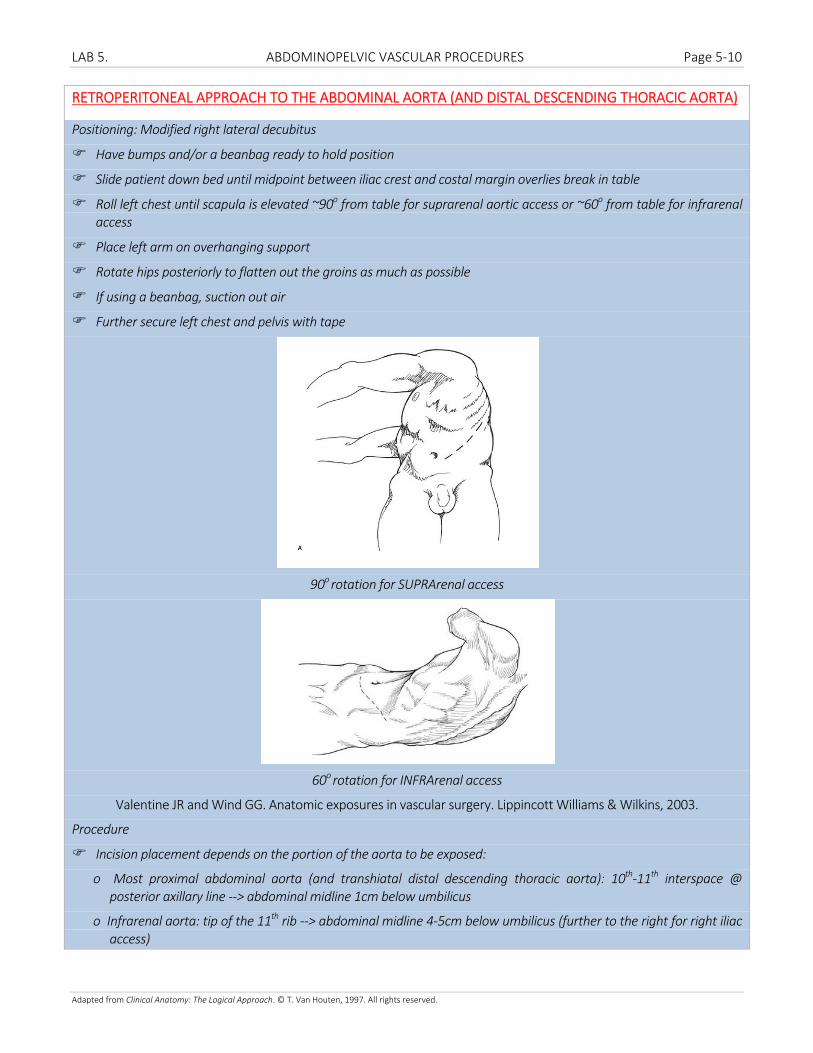
Positioning: Modified right lateral decubitus
Have bumps and/or a beanbag ready to hold position
Slide patient down bed until midpoint between iliac crest and costal margin overlies break in table
Roll left chest until scapula is elevated ~90o from table for suprarenal aortic access or ~60o from table for infrarenal access
Place left arm on overhanging support
Rotate hips posteriorly to flatten out the groins as much as possible
If using a beanbag, suction out air
Further secure left chest and pelvis with tape
90o rotation for SUPRArenal access
60o rotation for INFRArenal access
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Procedure
Incision placement depends on the portion of the aorta to be exposed:
o Most proximal abdominal aorta (and transhiatal distal descending thoracic aorta): 10th‐11th interspace @ posterior axillary line ‐‐> abdominal midline 1cm below umbilicus
o Infrarenal aorta: tip of the 11th rib ‐‐> abdominal midline 4‐5cm below umbilicus (further to the right for right iliac access)

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐11
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Incise the layers of the abdominal wall with electrocautery (left rectus abdominis will need to be divided)—avoid entry into the peritoneum medially
Ligate the epigastric vessels coursing anterior to the posterior rectus sheath
Excise the 11th or 12th rib with a rib cutter to improve lateral exposure
Bluntly dissect the peritoneal sac from the abdominal wall moving in a lateral to medial direction
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Use a self‐retaining retractor to facilitate exposure
Continue blunt dissection posteriorly along the psoas muscle (see “POSTERIOR ABDOMINAL WALL” below)
If exposure of the suprarenal aorta is desired (e.g. visceral segment)
o Open the anterior renal fascia and continue your dissection plane posterior to Gerota’s fascia
o Ligate a lumbar branch coursing to the left renal vein
o Mobilize the left kidney medially
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
o Carefully dissect out the left renal artery (the left renal vein has been swept medially and no longer crosses your field as it does when the kidney is left in situ)
o Further exposure of the celiac artery and descending thoracic aorta can be obtained by incising the median arcuate ligament and left crus

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐12
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
o Circumferential control is usually not attempted due to risk of injury to underlying venous structures; instead dissect anteriorly and posteriorly for clamp application
If exposure of the infrarenal aorta is desired, continue your dissection anterior to Gerota’s fascia and leave the left kidney in situ
o In this case the left ureter should be left along the posterior abdominal wall or it will obscure exposure of the juxtarenal aorta
Cronenwett JL, Johnston KW. Rutherford’s Vascular Surgery. Saunders, an imprint of Elsevier, Inc., Philadelphia, PA. 2014.
o Full mobilization of the peritoneal sac off the aorta with the left kidney left in situ requires (1) ligation of the IMA near the anterior abdominal wall (preserve length for possible reimplantation), and (2) ligation of the left gonadal vein which empties into the left renal vein
o Control of the right CIA requires rightward extension of the lower incision beyond the midline whereas control of the right EIA usually requires a separate right lower quadrant incision (alternatively right iliac control may be achieved by transaortic balloon occlusion)
Tranperitoneal access to the aorta may be achieved by (1) performing the Mattox maneuver (suprarenal aorta), or (2) targeted mobilization of the ligament of Treitz and incision of the posterior peritoneum (infrarenal aorta). For example, the former would be appropriate for management of a traumatic zone I supramesocolic

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐13
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
retroperitoneal hematoma in which there is concern for supraceliac aortic injury or in other situations where access to the suprarenal aorta is required.
LEFT VISCERAL MEDIAL ROTATION (MATTOX MANEUVER) FOR TRANSPERITONEAL SUPRARENAL AORTIC CONTROL
Please review this maneuver in Laboratory 3. Abdominal visceral procedures
Mattox maneuver, suprarenal aortic control: http://www.surgicalcore.org/videoplayer/510000039/50
Alternative for rapid supraceliac control: http://www.surgicalcore.org/videoplayer/510000038/50
TRANSPERITONEAL APPROACH TO THE ABDOMINAL AORTA FOR INFRARENAL CONTROL
Generous midline incision from xiphoid to pubis
Laparotomy as discussed in laboratory 1
Retract to the right and cephalad the greater omentum, transverse colon, and small bowel and use a self‐retaining retractor to preserve your exposure
Incise the ligament of Treitz and mobilize the 4th portion of the duodenum
Continue to incise the posterior peritoneum traveling caudally and to the right overlying the abdominal aorta while avoiding injury to the IMA and autonomic nerves
Alternatively, the exposure may be performed from inferior to superior
Cronenwett JL, Johnston KW. Rutherford’s Vascular Surgery. Saunders, an imprint of Elsevier, Inc., Philadelphia, PA. 2014.

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐14
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Meticulously ligate lymphatics along the anterior aorta to avoid chyle leak
If juxtarenal clamp application is required, the left renal vein may obstruct access to the aorta at that level. You have 2 options:
o Retract the left renal vein cephalad: this requires ligation of its gonadal, adrenal, and lumbar branches to avoid their avulsion during renal vein mobilization
o Divide the left renal vein: In this case the aforementioned branches must be preserved to ensure adequate outflow from the kidney
Cronenwett JL, Johnston KW. Rutherford’s Vascular Surgery. Saunders, an imprint of Elsevier, Inc., Philadelphia, PA. 2014.
Transperitoneal exposure of the infrarenal aorta: http://www.surgicalcore.org/videoplayer/510000040/50

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐15
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
OPEN ABDOMINAL AORTIC ANEURYSM REPAIR
Procedure
If access to the more distal common iliac arteries is necessary (e.g. concomitant common iliac aneurysms), the appropriate visceral mobilizations (see “COMMON ILIAC ARTERY (CIA) EXPOSURE …” below) should be undertaken prior to evisceration/packing of the bowel
Expose the aorta as discussed above (see “RETROPERITONEAL APPROACH TO THE ABDOMINAL AORTA …” , “LEFT VISCERAL MEDIAL ROTATION (MATTOX MANEUVER) FOR TRANSPERITONEAL SUPRARENAL AORTIC CONTROL”, or “TRANSPERITONEAL APPROACH TO THE ABDOMINAL AORTA FOR INFRARENAL CONTROL”)
Divide and ligate the IMA proximally at its takeoff from the aorta to preserve length should reimplantation be required
o Potential indications for reimplantation of the IMA
Significant SMA disease
Bilateral hypogastric artery occlusions
Large IMA
Prior colectomy
Sluggish or no back‐bleeding from an IMA that is known to be patent (from preop imaging, etc.; IMA stump pressure >40mmHg is felt by some to indicate adequate collateral circulation)
Colonic ischemia after IMA clamping/division intraop
Expose the common iliac arteries for clamp placement. Posterior dissection and circumferential control is usually not necessary and risks injuring the underlying veins

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐16
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
o The ureters must be identified and preserved during CIA exposure
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
The anesthesiologist is instructed to administer systemic heparin
An aortic clamp and curved clamps for the common iliac arteries are selected and applied once heparinization is therapeutic
A longitudinal arteriotomy is made in the aneurysm sac

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐17
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Cronenwett JL, Johnston KW. Rutherford’s Vascular Surgery. Saunders, an imprint of Elsevier, Inc., Philadelphia, PA. 2014.
Mural thrombus is evacuated and backbleeding from lumbar arteries controlled with full‐thickness horizontal mattress or figure‐of‐8 sutures
The aneurysm sac is opened and the proximal aortic and distal aortic or iliac cuffs (depending on whether a tube graft or bifurcated graft will be used) are prepared
Proximal anastomosis: end‐to‐end graft‐to‐aorta
o 3‐0 Prolene
o Needles should traverse the aorta inout to prevent raising of an intimal flap and outin on the graft
o Start at the posterior midline

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐18
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
o Continuous sutures can be run from the posterior midline to the anterior midline, or—to prevent purse‐stringing—a second double‐armed suture can be placed in the anterior midline and each arm can meet the posterior sutures more laterally
o Upon completion of the anastomosis, the graft is clamped, and the aortic clamp released to check for hemostasis
Distal anastomosis: end‐to‐end graft‐to‐aorta or each limb of a bifurcated graft to the common iliac arteries
o Technique is similar to the proximal anastomosis except that 4‐0 Prolene is often used on the iliac arteries

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐19
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
o Prior to completion of the suture line, the clamp on the graft stemming antegrade flow from the aorta should be released to flush clot and debris out of the arterial system and prevent “trashing” of the lower extremity vasculature with emboli
o Once the anastomotic sutures have been tied down, close communication with anesthesia is critical to allow adequate volume resuscitation and monitoring of chemistries as the distal clamp is relieved restoring antegrade flow to each lower extremity (or both for a tube graft)
o Note that it is possible to perform end‐of‐graft to side‐of‐iliac artery anastomoses (e.g. if iliac occlusions are present) in which case (1) the proximal iliac at the site of transection of the aneurysmal sac should be oversewn and (2) care should be taken to ensure that the ureter remains anterior to the graft to prevent compression and ureteral obstruction. Specific techniques of end‐to‐side vascular anastomoses are discussed in laboratory 6.

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐20
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
The aneurysm sac should be closed over the graft, in particular the proximal aortic suture line to decrease the risk of aortoenteric fistula/erosion
o A tongue of greater omentum can be interposed between the graft and overlying viscera if the aneurysm sac cannot be closed
Be sure to check the appearance of the sigmoid colon and reimplant the IMA if the indications above exist
Distal pulses should be checked prior to the completion of the operation
Open AAA repair: http://accesssurgery.mhmedical.com.ezp‐prod1.hul.harvard.edu/MultimediaPlayer.aspx?MultimediaID=5481801

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐21
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
COMMON, INTERNAL, AND EXTERNAL ILIAC ARTERY (CIA, IIA, EIA) EXPOSURE AND BYPASS
Retroperitoneal exposure
Position: Supine with rolled towel under hip or with hips over break in bed and table jack‐knifed
Incision from the lateral border of the rectus ~2‐3 fingerbreadths superior to the inguinal ligament midaxillary line halfway between the costal margin and iliac crest
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
o If only the external iliac artery needs to be exposed, a smaller incision from the lateral rectus sheath to a point 2cm superior to the anterior iliac spine, running 2cm superior and parallel to the inguinal ligament usually suffices
Ligate the superficial epigastric and circumflex iliac arteries
Deepen the incision through the transversalis fascia being sure not to enter the peritoneal cavity
Strip the peritoneal sac from the pelvic wall starting laterally and continuing medially
The ipsilateral ureter should be swept medially with the peritoneal sac
Identify the external iliac artery distally and trace it proximally to identify the common and internal segments and obtain proximal and distal control
Transperitoneal exposure
This is usually performed at the time of operation for other traumatic injuries or during aneurysmal disease for the aorta; thus positioning and incision are usually contingent on the other procedures planned
Right iliac arteries
o Retract the large and small bowel as described for transperitoneal infrarenal aortic exposure above
o Incise the peritoneum starting at the ligament of Treitz and traveling toward the patient’s right to avoid injuring the IMA as discussed
o Extend the peritoneal incision further inferolaterally over the right common iliac artery
o Bluntly dissect the periadventitia about the right common iliac artery up to the aortic bifurcation

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐22
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
o Cautiously encircle the CIA with a vessel loop so as not to injure the underlying common iliac vein
o Continue the dissection distally toward the CIA’s bifurcation into the IIA and EIA—the right ureter lies in this plane and should be cautiously mobilized and retracted laterally
o Dissect out the IIA and EIA and cautiously encircle, being sure not to injure the corresponding posteromedial veins
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Left iliac arteries: 2 approaches exist, (1) medial, and (2) lateral
o Medial approach: laterally retract the area of incised peritoneum over the aortic bifurcation to visualize the iliac arteries
Further incision of the peritoneum in this area should be avoided in men or injury to sympathetic nerves may result in sexual dysfunction (a lateral approach may be required if visualization is inadequate)
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐23
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
o Lateral approach: retract the sigmoid colon medially, mobilize as discussed previously, and continue dissection in the avascular plane posterior to the sigmoid and its mesentery to expose the left iliac arteries (avoid injury to the ureter)
Cronenwett JL, Johnston KW. Rutherford’s Vascular Surgery. Saunders, an imprint of Elsevier, Inc., Philadelphia, PA. 2014.
Bypass
Creation of an anastomosis with the iliac arteries is similar to other running end‐of‐graft to side‐of‐native artery and end‐of‐grant to end‐of‐native artery vascular anastomoses. Refer to “SMA BYPASS” below and “OPEN ABDOMINAL AORTIC ANEURYSM REPAIR” above for general instruction on each of these techniques. Typically 4‐0 Prolene is used to sew to the iliac arteries.
As discussed above, care should be taken to ensure that the ureter remains anterior to the graft to prevent compression and ureteral obstruction
Retroperitoneal right iliac artery exposure: http://www.surgicalcore.org/videoplayer/510000043/50
AORTOFEMORAL BYPASS
Proximal anastomosis with the abdominal aorta is similar to the proximal anastomosis for “OPEN ABDOMINAL AORTIC ANEURYSM REPAIR” above, although end‐of‐graft to side‐of‐aorta anastomoses can also be fashioned with oversewing of the aortic stump. Please refer to Laboratory 6 for the complete procedure including common, superficial, and deep femoral artery exposure and distal anastomosis.
Aortofemoral bypass: http://accesssurgery.mhmedical.com.ezp‐prod1.hul.harvard.edu/MultimediaPlayer.aspx?MultimediaID=5481792
Locating the superior mesenteric artery (SMA) is a critical skill for general and vascular surgeons alike given the importance of this maneuver in the assessment of the vessel’s patency in cases of suspected acute mesenteric ischemia. Bypass and embolectomy are frequently required for thrombotic and embolic occlusions, respectively. At its origin off of the visceral segment of the abdominal aorta, the SMA lies within centimeters of the celiac axis’ origin at the level of the L1 vertebra, just beyond the diaphragmatic hiatus. Exposure of the SMA within the intestinal mesentery can be achieved via the anterior or lateral approach; the former is more rapid and adequate for embolectomy, while the latter is required for retrograde bypass (to prevent the bypass graft from crossing the duodenum.)
LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐24
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
SMA EXPOSURE (“FINDING THE SMA”)
Origin off of aorta
Supine
Midline incision from xiphoid to pubis
Assess the condition of midgut structures in all procedures involving the SMA
Retract bowel caudally
Place a self‐retaining retractor
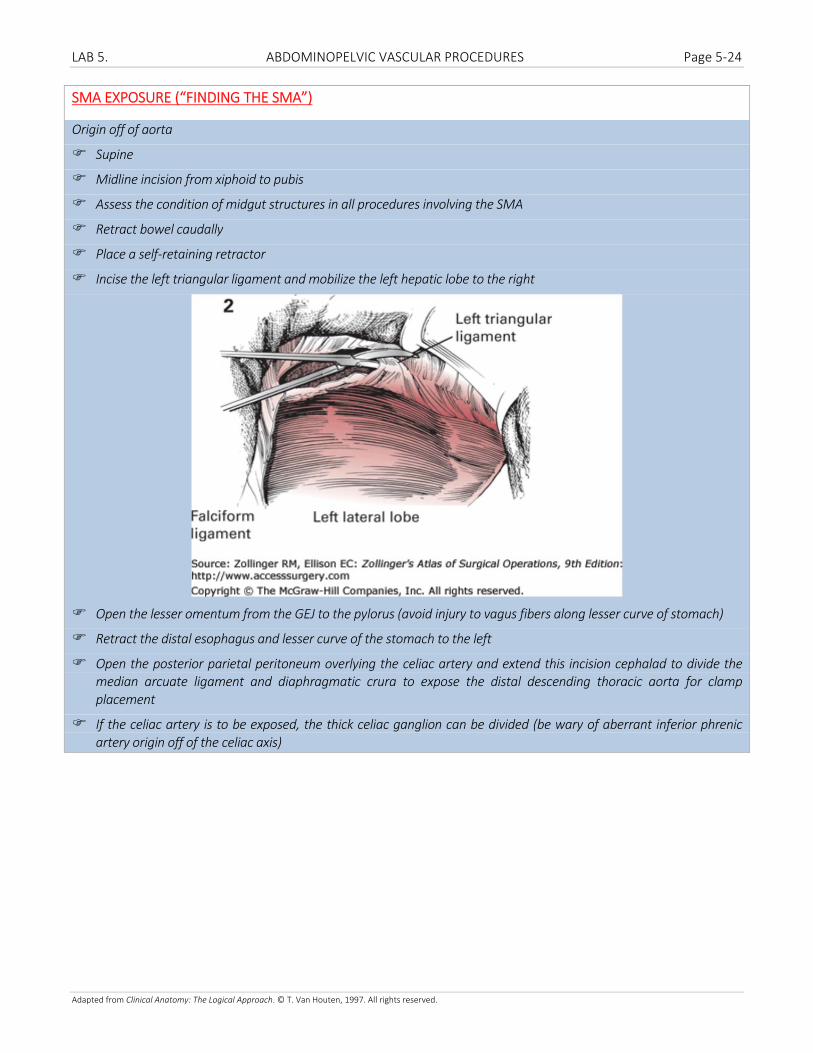
Incise the left triangular ligament and mobilize the left hepatic lobe to the right
Open the lesser omentum from the GEJ to the pylorus (avoid injury to vagus fibers along lesser curve of stomach)
Retract the distal esophagus and lesser curve of the stomach to the left
Open the posterior parietal peritoneum overlying the celiac artery and extend this incision cephalad to divide the median arcuate ligament and diaphragmatic crura to expose the distal descending thoracic aorta for clamp placement
If the celiac artery is to be exposed, the thick celiac ganglion can be divided (be wary of aberrant inferior phrenic artery origin off of the celiac axis)

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐25
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
As shown above, the superior border of the pancreas obstructs access to the origin of the SMA, and must be mobilized
o Stay along the aorta as you mobilize the pancreas as (1) lateral dissection or retraction can avulse the splenic artery tributaries to the pancreatic parenchyma, (2) the left renal vein crosses the aorta to join the IVC through the crook formed by the takeoff of the SMA
Once adequately mobilized, retract the superior border of the pancreas and splenic vein caudally to expose the SMA
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Within small bowel mesentery: Anterior approach
Supine
Midline incision from xiphoid to pubis
Assess the condition of midgut structures in all procedures involving the SMA
LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐26
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Elevate the transverse colon and greater omentum, retract and pack the small bowel to the right
Place a self‐retaining retractor
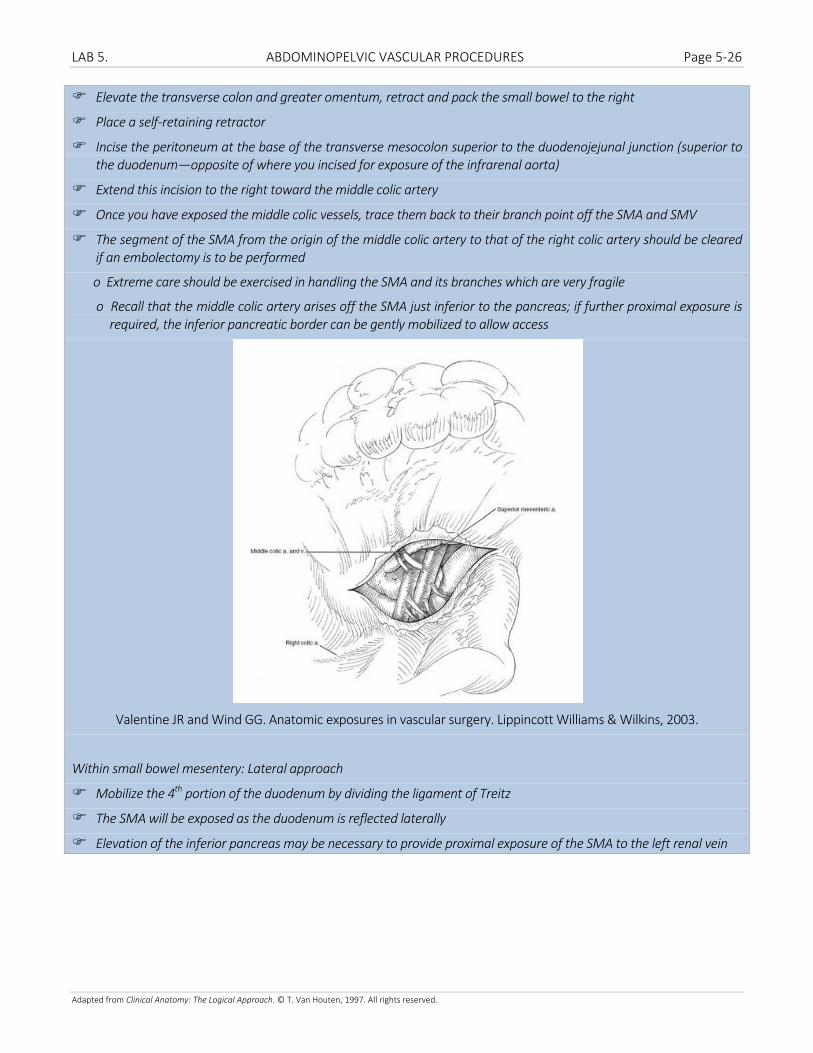
Incise the peritoneum at the base of the transverse mesocolon superior to the duodenojejunal junction (superior to the duodenum—opposite of where you incised for exposure of the infrarenal aorta)
Extend this incision to the right toward the middle colic artery
Once you have exposed the middle colic vessels, trace them back to their branch point off the SMA and SMV
The segment of the SMA from the origin of the middle colic artery to that of the right colic artery should be cleared if an embolectomy is to be performed
o Extreme care should be exercised in handling the SMA and its branches which are very fragile
o Recall that the middle colic artery arises off the SMA just inferior to the pancreas; if further proximal exposure is required, the inferior pancreatic border can be gently mobilized to allow access
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Within small bowel mesentery: Lateral approach
Mobilize the 4th portion of the duodenum by dividing the ligament of Treitz
The SMA will be exposed as the duodenum is reflected laterally
Elevation of the inferior pancreas may be necessary to provide proximal exposure of the SMA to the left renal vein

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐27
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
SMA EMBOLECTOMY
Procedure
Expose the SMA within the bowel mesentery using the anterior approach discussed above
Isolate the middle and right colic as well as jejunal branches
Administer intravenous heparin
For very small caliber SMA a longitudinal arteriotomy should be made, otherwise in most cases a transverse arteriotomy is made
Pass a 3‐4Fr Fogarty balloon proximally, inflate and withdraw gently until high pressure, pulsatile antegrade flow is restored
Pass a 2‐3Fr Fogarty balloon distally until pulsatile backbleeding is restored
Cronenwett JL, Johnston KW. Rutherford’s Vascular Surgery. Saunders, an imprint of Elsevier, Inc., Philadelphia, PA. 2014.
tPA or other thrombolytics can be administered intra‐arterially
Perform a patch angioplasty if a longitudinal arteriotomy was used; else close primarily

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐28
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
SMA BYPASS
Retrograde bypass: Right common iliac artery‐to‐SMA distal to occlusion
Expose the SMA within the bowel mesentery using the lateral approach discussed above
Graft selection
o No bowel soilage: 6‐8mm Dacron/ringed PTFE
o Bowel soilage: SFV, GSV
Sufficient graft length should be selected to allow a “lazy C” configuration to prevent kinking
Proximal anastomosis: End of graft‐to‐side of SMA or end‐to‐end anastomoses can be used (latter shown below)
Distal anastomosis: End of graft‐to‐side of right common iliac artery
Cronenwett JL, Johnston KW. Rutherford’s Vascular Surgery. Saunders, an imprint of Elsevier, Inc., Philadelphia, PA. 2014.
Other options for SMA bypass: (1) Retrograde bypass from the infrarenal aorta to the SMA just distal to the thrombotic occlusion, (2) Retrograde bypass from the left common iliac artery to the SMA just distal to the thrombotic occlusion, (3) Antegrade bypass from the supraceliac aorta to the SMA distal to the thrombotic occlusion
Always assess bowel viability when performing procedures on the SMA
o Allow 20‐30 minutes of reperfusion prior to making a final decision
o Evidence of adequate perfusion
Pulse in the mesenteric arcade
Pink bowel wall color
Peristalsis
Pulsatile Doppler signal from antimesenteric border of bowel
Bleeding from cut surfaces (if small bowel resection is undertaken)
An omental flap can be brought through the transverse mesocolon to provide coverage of prosthetic graft material
Return for 2nd look laparotomy

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐29
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
CONTROL OF THE PORTAL VEIN
Pringle maneuver
Divide the hepatoduodenal ligament lateral to the portal triad
Place a finger through the gastroepiploic foramen of Winslow into the lesser sac
Place a vascular clamp from right to left across the portal triad using the digit in the lesser sac to guide the posterior tine
Exposure of portal vein
Approach the the portal vein from the right posterior aspect of the hepatoduodenal ligament to avoid injury to avoid blood vessels and lymphatics that run along its anterior aspect
Incise the peritoneum overlying the posterior portal vein (at the lip of the foramen of Winslow) from the liver hilum to the head of the pancreas

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐30
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Encircle the portal vein and branches
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Repair of injuries can be performed by lateral venorrhaphy (running 4‐0 or 5‐0 Prolene), end‐to‐end anastomosis, interposition grafting, splenic vein transposition, venovenous shunt from SMV, or ligation
RIGHT MEDIAL VISCERAL ROTATION (CATTELL‐BRAASCH MANEUVER)
Please review this maneuver in Laboratory 3. Abdominal visceral procedures

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐31
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
CONTROL OF THE (INFRA‐ AND RETROHEPATIC) IVC
Infrahepatic IVC: retroperitoneal approach
Position: Supine with right flank elevated 15‐20o on rolled sheets
Prep/drape: Lower chest, abd, right flank
Incision: Right flank incision from tip of 11th rib to border of right rectus just superior to level of the umbilicus
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Dissect the layers of the abdominal wall down through the transversalis fascia being cautious not to enter the peritoneum
Separate the peritoneum off of the overlying fascia starting laterally and continuing medially
Bluntly dissect the right colon (secondarily retroperitoneal) from psoas muscle and reflect medially with the peritoneum
The right ureter should be swept medially with the peritoneal sac
Obtain distal control of the IVC above the highest lumbar vein and proximal control above the iliac confluence
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Infrahepatic IVC: transperitoneal approach
Position: Supine
Prep/drape: Lower chest, abd, right flank
Incision: Midline incision (right subcostal incision can be used in non‐traumatic cases)
Pack the small bowel in the left abdomen
Perform a right medial visceral rotation (Cattell‐Braasch maneuver) as discussed in “Laboratory 3. Abdominal visceral procedures” to expose the infrahepatic IVC from the iliac vein confluence to the caudate lob

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐32
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Areolar tissue and lymphatics should be cleared from the anterior and lateral surfaces of the IVC
Posterior lumbar veins should be ligated prior to mobilization of the IVC to prevent their avulsion
The right adrenal vein should be controlled prior to encircling the IVC above the renal veins
Avoid excessive mobilization of the suprarenal IVC as this segment is relatively fixed by the renal veins
Retrohepatic IVC
Position: Supine
Prep/drape: Entire chest and lower neck and abdomen
Incision: Midline incision—extension to median sternotomy may be necessary if suprahepatic IVC exposure becomes necessary
Enter the peritoneal cavity
Pack the abdomen to allow resuscitation before proceeding, if necessary
Elevate the costal margins with self‐retaining retractors
Divide the right triangular ligament and mobilize the right liver medially

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐33
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.
Smaller hepatic vein branches from the posterior right and caudate liver lobes should be ligated to avoid troublesome bleeding
If control of the main hepatic veins is necessary, divide the falciform and coronary ligaments and retract the liver caudally to expose the suprahepatic (still subdiaphragmatic) IVC and the hepatic vein‐IVC confluence, and encircle the 3 main hepatic veins near their junction with the IVC
Valentine JR and Wind GG. Anatomic exposures in vascular surgery. Lippincott Williams & Wilkins, 2003.

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐34
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
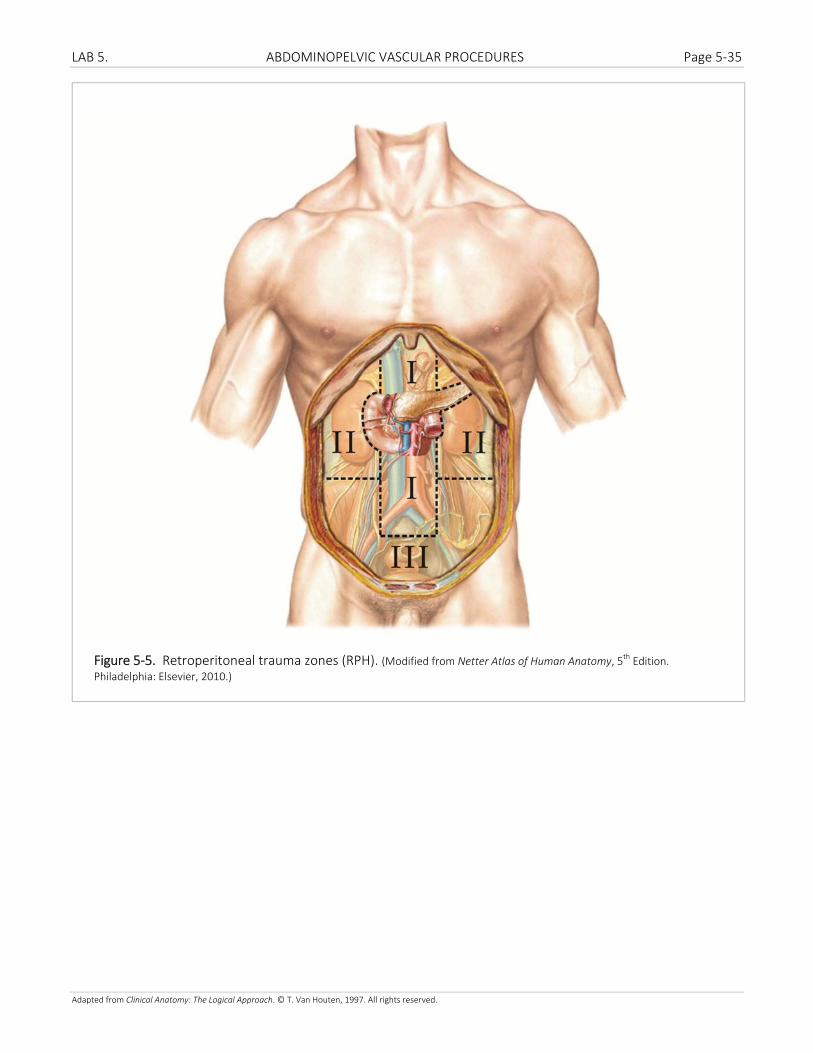
5.3 RETROPERITONEAL TRAUMA ZONES Three retroperitoneal zones are defined for characterizing retroperitoneal hemorrhage (RPH) (Figure 5‐5).
Zone 1. Zone 1 extends from the esophageal hiatus of the diaphragm to the sacral promontory. Zone I non‐vascular structures include the ‘secondarily retroperitoneal’ pancreas and the 2nd, 3rd, and 4th portions of the duodenum. Zone I vascular structures include the aorta, inferior vena cava, celiac trunk, superior mesenteric artery, inferior mesenteric artery, and the origins of the renal vessels. RPH localized to the upper Zone 1 implies injury to the great vessels.
Zone 2. Paired Zone 2 extends from the lateral diaphragm to the iliac crest. Zone 2 structures include the adrenal
glands, kidneys, ureters, and renal vessels at the kidney hilum.
Zone 3. Zone 3 includes the pelvic extraperitoneum. Zone 3 structures include the iliac vessels, rectum, bladder
and distal ureters, and the male and female pelvic viscera.
LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐35
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Figure 5‐5. Retroperitoneal trauma zones (RPH). (Modified from Netter Atlas of Human Anatomy, 5th Edition.
Philadelphia: Elsevier, 2010.)

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐36
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
5.4 POSTERIOR ABDOMINAL WALL
Posterior abdominal wall boundaries and layers. The posterior abdominal wall is the region between the 12th rib superiorly, iliac crest inferiorly, and anterolateral abdominal wall muscles laterally (Figure 5‐6). From superficial to deep, the layers of the posted prior abdominal wall include skin; subcutaneous fat; investing deep fascia; ribs, spine, and associated muscles; and lining deep fascia facing the abdominal cavity.
Posterior abdominal wall muscles. Functionally, the posterior abdominal wall muscles are spinal muscles. Contraction produces motion at the fibrocartilaginous intervertebral joints and synovial plane facet joints between individual vertebrae and between the ribs and spine.
The posterior spinal muscles (erector spinae group) extend and/or laterally bend the spine. The anterior spinal muscles (psoas major and quadratus lumborum) flex and/or laterally bend the spine, and the inconstant psoas minor muscle is a weak spinal flexor. Inferiorly the psoas major and iliacus muscles join to form the iliopsoas muscle, the most powerful hip flexor.
Lining deep fascia over the posterior abdominal wall. The deep fascia surrounding the posterior abdominal wall muscles is a continuation of the thoracolumbar fascia. Like the anterolateral abdominal wall muscles, the posterior abdominal wall muscles are covered with investing fascia on their outer surfaces and lining fascia on their deep surfaces.
The lining deep fascia of the abdominopelvic cavity forms a continuous layer over the inferior surface of the diaphragm, posterior abdominal wall muscles, anterolateral abdominal wall muscles, and deep surfaces of the muscles of the pelvic sidewalls and pelvic floor. The anatomic continuity of the lining deep fascia is obscured by the practice of applying different names to the fascia as it covers individual muscles. For example, the lining deep fascia is psoas fascia where it covers the deep surface of the psoas muscles, quadratus lumborum fascia where it covers the deep surface of the quadratus lumborum muscle, and transversalis fascia where it covers the deep surface of the transversus abdominis muscle. The lining fascia of the abdominal wall attaches to the periosteum of the spine and iliac crest, then continues into the pelvis to form a continuous layer over the muscles of the pelvic sidewalls and pelvic floor (obturator fascia, piriformis fascia, and so on). Superiorly, the lining deep fascia of the abdominopelvic cavity forms the diaphragmatic fascia over the inferior surface of the diaphragm. Local thickenings of lining deep fascia form the medial arcuate ligament at the border between the diaphragmatic and psoas fascia and the lateral arcuate ligament at the border between the diaphragmatic fascia and quadratus lumborum fascia.
Identifying posterior abdominal wall muscles
Identify the iliac crest of the pelvis. Superior to the iliac crest, identify the quadratus lumborum muscle and follow it to its attachment on rib 12 (Figure 8‐9). Medial to quadratus lumborum, identify the psoas major muscle. Verify the origin of psoas major from the bodies and transverse processes of the lumbar vertebrae. If present, identify the tendon of the small, inconstant psoas minor muscle anterior to psoas major. Inferior to the iliac crest, identify the iliacus muscle at its origin from the iliac fossa.
Return to the diaphragm and, on its inferior surface, identify the central tendon, peripheral muscular portion, left crus, and right crus. Identify the caval foramen, esophageal hiatus, and aortic hiatus and the structures passing through them (Figure 8‐9).
Identify two condensations of the lining deep fascia, the lateral arcuate ligament, a dense connective tissue thickening, where the diaphragm arches over the quadratus lumborum muscle, and the medial arcuate ligament where the diaphragm arches over the psoas major muscle.

LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐37
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
Figure 5‐6 Posterior abdominal wall nerves. (Modified from Netter Atlas of Human Anatomy, 5th Edition. Philadelphia:
Elsevier, 2010.)
LAB 5. ABDOMINOPELVIC VASCULAR PROCEDURES Page 5‐38
Adapted from Clinical Anatomy: The Logical Approach. © T. Van Houten, 1997. All rights reserved.
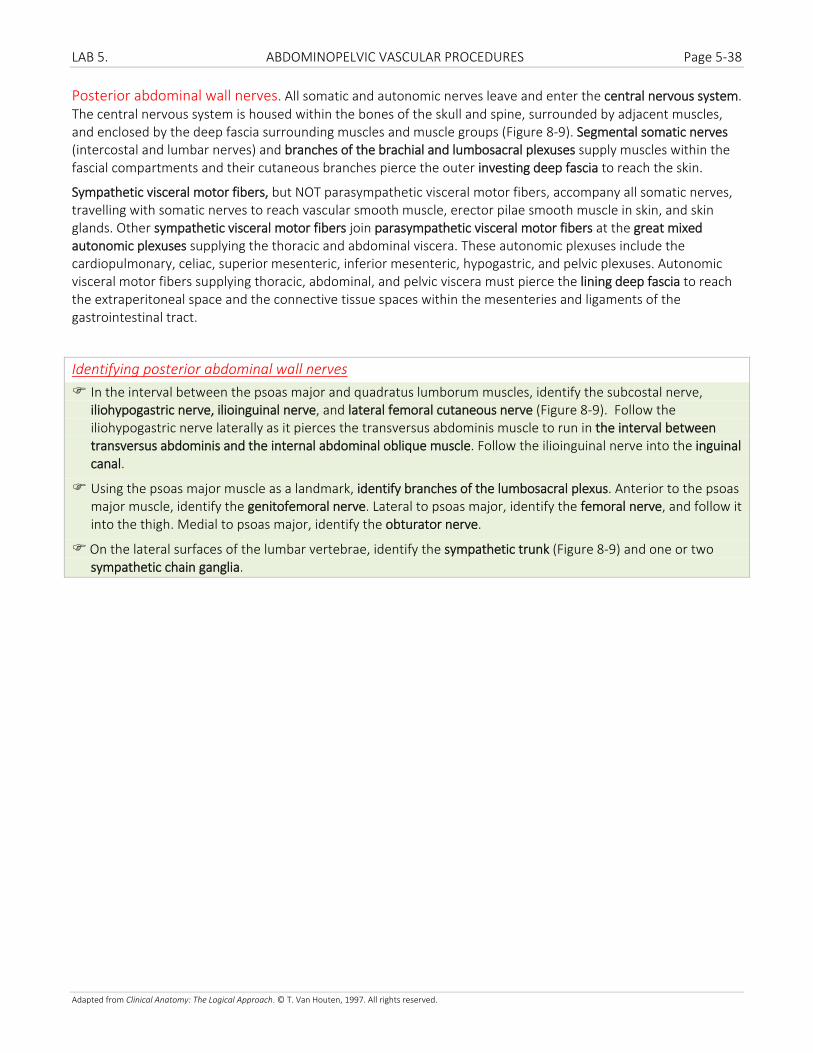
Posterior abdominal wall nerves. All somatic and autonomic nerves leave and enter the central nervous system. The central nervous system is housed within the bones of the skull and spine, surrounded by adjacent muscles, and enclosed by the deep fascia surrounding muscles and muscle groups (Figure 8‐9). Segmental somatic nerves (intercostal and lumbar nerves) and branches of the brachial and lumbosacral plexuses supply muscles within the fascial compartments and their cutaneous branches pierce the outer investing deep fascia to reach the skin.
Sympathetic visceral motor fibers, but NOT parasympathetic visceral motor fibers, accompany all somatic nerves, travelling with somatic nerves to reach vascular smooth muscle, erector pilae smooth muscle in skin, and skin glands. Other sympathetic visceral motor fibers join parasympathetic visceral motor fibers at the great mixed autonomic plexuses supplying the thoracic and abdominal viscera. These autonomic plexuses include the cardiopulmonary, celiac, superior mesenteric, inferior mesenteric, hypogastric, and pelvic plexuses. Autonomic visceral motor fibers supplying thoracic, abdominal, and pelvic viscera must pierce the lining deep fascia to reach the extraperitoneal space and the connective tissue spaces within the mesenteries and ligaments of the gastrointestinal tract.
Identifying posterior abdominal wall nerves
In the interval between the psoas major and quadratus lumborum muscles, identify the subcostal nerve, iliohypogastric nerve, ilioinguinal nerve, and lateral femoral cutaneous nerve (Figure 8‐9). Follow the iliohypogastric nerve laterally as it pierces the transversus abdominis muscle to run in the interval between transversus abdominis and the internal abdominal oblique muscle. Follow the ilioinguinal nerve into the inguinal canal.
Using the psoas major muscle as a landmark, identify branches of the lumbosacral plexus. Anterior to the psoas major muscle, identify the genitofemoral nerve. Lateral to psoas major, identify the femoral nerve, and follow it into the thigh. Medial to psoas major, identify the obturator nerve.
On the lateral surfaces of the lumbar vertebrae, identify the sympathetic trunk (Figure 8‐9) and one or two sympathetic chain ganglia.