absite review conference topicmonth head and neck / breastaugust 09 alimentarysept 09 alimentary /...
TRANSCRIPT
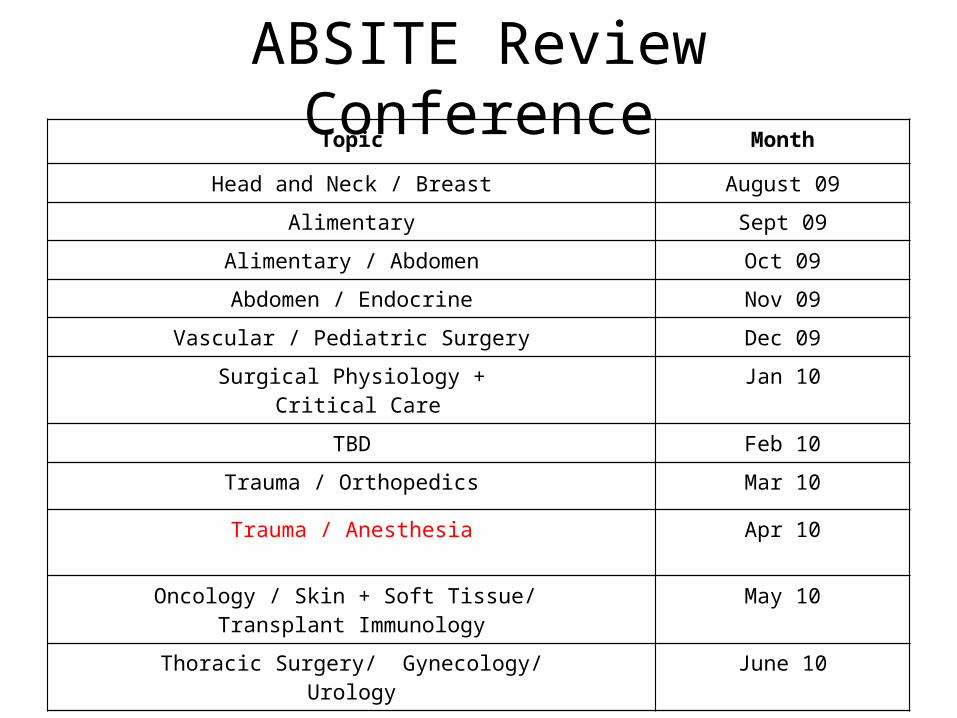
ABSITE Review ConferenceTopic Month
Head and Neck / Breast August 09
Alimentary Sept 09
Alimentary / Abdomen Oct 09
Abdomen / Endocrine Nov 09
Vascular / Pediatric Surgery Dec 09
Surgical Physiology + Critical Care
Jan 10
TBD Feb 10
Trauma / Orthopedics Mar 10
Trauma / Anesthesia Apr 10
Oncology / Skin + Soft Tissue/ Transplant Immunology
May 10
Thoracic Surgery/ Gynecology/Urology
June 10
Trauma/ Anesthesia
You start to perform your Kocher maneuver in the above patient and find that the 1st and 2nd portions of the duodenum are completely blown out proximal to the common bile duct. The most appropriate next step is:
a) Whipple
b) Oversew proximal and distal portions of the duodenum, then gastrojejunostomy
c) Proximal duodenojejunstomy and distal duodenojejunostomy
d) Place drains
Trauma/ Anesthesia
Answer B.
For an injury that is proximal to the ampulla of Vater, you can staple off the proximal and distal ends of the duodenal injury and perform a gastrojejunostomy. You can do this because the ampulla of Vater is not involved and will still drain distally. Food will pass via the gastrojejunsotomy.
Remember to widely drain.
If the injury involves the duodenum distal to the ampulla of Vater, a duodenojejunostomy is needed to control biliary flow. If the ampulla itself is destroyed (functional Whipple), you can place drains initially if the patient is unstable but the patient will need to return for a formal Whipple.
Trauma/ Anesthesia
All of the following are indications for angiogram of an extremity except:
a) Injury to anatomically related nerve
b) History of large severe blood loss from the injury
c) Large hematoma
d) Active hemorrhage
Trauma/ Anesthesia
Answer D. Active hemorrhage is an indication to go to the OR, not get an angiogram.Major (Hard) signs of vascular injury
Active hemorrhage present
Pulse deficit
Expanding or pulsatile hematoma
Distal ischemia
Bruit or thrill present
Treatment for any of the above is to go to OR for exploration.
Minor (Soft) signs of vascular injury
History of hemorrhage at the scene
Anatomically related nerve deficit
A large stable hematoma
Injury close to a major artery (GSW to the medial thigh)
ABI < 0.9
Unequal pulses
Diagnosis for any of the above is to go to angiography.

Trauma/ Anesthesia
You perform a DPL on a patient involved in a motor vehicle accident which is positive. The patient has remained hypotensive despite blood resuscitation. The patient has a blown pupil on the right. The most appropriate next step is:
a) Head CT
b) Abdominal CT
c) Head and Abdominal CT
d) OR
Trauma/ Anesthesia
Answer D.
A positive DPL in a hypotensive patient mandates operative exploration. In the ABC’s scheme, C (circulation) must be addressed before addressing the head injury.

Trauma/ Anesthesia
While in the OR, this patient should undergo:
a) Laparotomy only
b) Laparotomy followed by head CT
c) Laparotomy and Burr hole placement
d) Burr hole placement only
Trauma/ Anesthesia
Answer C.
While in the OR, you should place a Burr hole to decompress the side with the blown pupil. This is placed 5 cm anterior and 5 cm superior to the external auditory canal (frontal bone).
Another option would be to place an ICP bolt and check the pressure, with placement of a Burr hole is the pressure is elevated (although just doing the Burr hole is probably the best treatment).

WHERE TO MAKE THE FIRST BURR HOLE?• If fracture crosses a vessel, make the hole there.• If patient has an obvious scalp injury, start in the center.• If there is no fracture line or obvious scalp injury, make the first hole in the
classical position.• If the first hole is negative, make the next one in the parietal region, and
then one in the frontal region. • If this too is negative, repeat the same three holes in the same order on
the other side.
• Occasionally, you will have to make six holes; only if all six are negative can you be sure that there is no clot above a patient’s tentorium- “woodpecker method”
• Only when you have reached the dura will you see if the bleeding is epidural or subdural.
• Do NOT make a burr hole over a major sinus.

Trauma/ Anesthesia
A 25 year old man in a MVA will open his eyes only to painful stimuli, does not form words but mumbles, and withdraws to pain. The patients Glasgow Coma Scale is:
a) 10
b) 8
c) 6
d) 4
Trauma/ Anesthesia
Answer B.
Opens eyes (2), Incomprehensible sounds(2), Withdraws from pain (4)Eye opening
4 Spontaneous
3 Opens to command
2 Opens eyes to pain
1 No response
Verbal response
5 Appropriate and oriented
4 Confused but responds
3 Inappropriate words with speech
2 Incomprehensible sounds
1 No response
Motor function
6 Follows commands
5 Localizes to pain site
4 Withdraws from pain
3 Flexion with painful stimuli (decorticate)
2 Extension with painful stimuli (decerebrate)
1 No response to painful stimuli
Trauma/ Anesthesia
The above patient is having difficulty maintaining his airway so you intubate him. Head CT shows loss of sulci and compression of cisterns so you place an ICP monitoring catheter. All of the following are true of cerebral perfusion except:
a) In general, a cerebral perfusion pressure of 70 is sufficient
b) Cerebral perfusion pressure = Mean arterial pressure – intracranial pressure
c) Mannitol can help lower ICP
d) Hypoventilation benefits these patients
Trauma/ Anesthesia
Answer D.
In general, a CPP > 60 is sufficient. Mannitol helps increase cerebral perfusion bu drawing water from the brain thereby decreasing ICP. Mild hyperventilation (pCO2 30-35) helps by causing mild cerebral vascocontriction which limits brain edema.
Trauma/ Anesthesia
A 27 year old man is in the ICU 6 hours after splenectomy following a MVA. The patient has a prolonged transport time and received 20 units of blood prior to arrival. Currently, his peak airway pressures are 65 (plateaus 50), his abdomen is distended, he is not making any urine, and his bladder pressure is 40. His CVP is 18. The most appropriate maneuver in this patient is:
a) Increase PEEP
b) Volume resuscitation
c) Decompressive laparotomy
d) CT scan
Trauma/ Anesthesia
Answer C.
The patient has classic signs of abdominal compartment syndrome. Objectively, a bladder pressure > 25-30 suggests abdominal compartment syndrome. Decreased urine output from IVC compression results in decreased cardiac output. Elevated ventilatory pressures are coexistent. Treatment of abdominal compartment syndrome is decompressive laparotomy.

Trauma/ Anesthesia
Trauma/ Anesthesia
Malignant hyperthermia is most commonly related to a defective receptor (ryanodine receptor) on the sarcoplasmic reticulum that controls calcium release. The 1st sign of malignant hyperthermia after receiving succinylcholine in the intubated patient is:
a) Fever
b) Rigors
c) Increase in end tidal CO2
d) Tachycardia

Trauma/ Anesthesia
Answer C.
Trauma/ Anesthesia
The most appropriate step in the treatment of malignant hyperthermia is:
a) Dantrolene
b) Dopamine
c) Dobutamine
d) Lasix and potassium
Trauma/ Anesthesia
Answer A.
Malignant hyperthermia can be triggered by either volatile gaseous inhalation anesthetics (sevoflurane, isoflurane, halothane, enflurane, etc.) or succinylcholine.
The defect is in calcium metabolism which causes a prolonged muscle excitation- contraction syndrome.
In an intubated patient, the first sign is a rise in the end tidal CO2. Other signs include tachycardia, fever, rigidity, acidosis, and hyperkalemia.
Treatment includes stopping the precipitating anesthetic or paralytic, dantrolene (which decouples the excitation complex), cooling blankets, HCO3- (alkalinize), glucose, and oxygen.
Trauma/ Anesthesia
Drop in end tidal CO2
Disconnection from the ventilator
Pulmonary embolus
CO2 embolus
Trauma/ Anesthesia
Rise in end tidal CO2
Most common cause is alveolar hypoventilation (atelectasis). Others include lung injury, absorption of CO2 with laparoscopy, shivering, hyperthermia, catecholamine release, thyroid storm, inadequate fresh gas flow, exhausted soda lime
Hypoventilation, which may result from increased resistance to air flow in external anesthesia equipment (rebreathing of CO2), the tracheal tube (kinking, obstruction with secretions, and herniated or ruptured cuff), or the tracheobronchial tree (laryngospasm or bronchospasm)
Trauma/ Anesthesia
Cis-atracurium (Nimbex) is metabolized by:
a) Liver
b) Kidney
c) Plasma cholinesterase
d) Hoffman degradation
Trauma/ Anesthesia
Answer D.
Cis-atricurium is degraded by Hoffman degradation which makes it ideal for patients with either renal failure or liver failure.
Trauma/ Anesthesia
Two days after a severe inhalational injury, you have trouble oxygenating your patient so you decide to paralyze her with pancuronium. The most common side effect of pancuronium is:
a) Fever
b) Hypotension
c) Increased Intracranial Pressure
d) Tachycardia
Trauma/ Anesthesia
Answer D.
The most common side effect of pancuronium (non-depolarizing muscle relaxant) is tachycardia.
Trauma/ Anesthesia
A 52 year old woman undergoes a routine low anterior resection for colon cancer and has a temperature of 104.0 six hours post-op. you look at her wound and it is purple around the edges and there seems to be some gray drainage. The most appropriate next step is:
a) Cefazolin
b) Ceftriaxone
c) Zosyn
d) Re-exploration
Trauma/ Anesthesia
Answer D.
Trauma/ Anesthesia
The most likely organism in the above scenario is:
a) Staph aureus
b) Clostridum perfringens
c) Enterococcus
d) E. Coli
Trauma/ Anesthesia
Answer B.
Clostridium perfringens wound infection is rare but it needs to be recognized. Patients who have high fever immediately post-op need to have their dressing removed and their wound inspected. If wound drainage appears or there is surrounding skin changes, the patient should immediately be taken back to the OR for wide debridement. The patient is at high risk for developing necrotizing fascitis and/or myonecrosis.
Beta-hemolytic group A strep is also a potential source of early invasive wound infection early post-op.
Penicillin is the classic treatment of choice for both clostridium perfringens and beta-hemolyttic group A strep but in reality you would start a broad spectrum antibiotic until you knew what the organism was.
Trauma/ Anesthesia
The muscles that are the 1st to relax with paralytics are the:
a) Neck muscles and face
b) Diaphragm muscles
c) Extremities
d) Abdominal Wall
Trauma/ Anesthesia
Answer A.
Trauma/ Anesthesia
The muscles that are the last to relax with paralytics and the 1st to recover are the:
a) Neck muscles and face
b) Diaphragm muscles
c) Extremities
d) Abdominal Wall Muscles
Trauma/ Anesthesia
Answer B.
The muscles of the neck and face are the 1st to relax with paralytics and the last to recover. The diaphragm muscles are the last to relax and the 1st to recover.
Trauma/ Anesthesia
The various inhaled anesthetics have different biological characteristics. A low minimum alveolar concentration (MAC) of an inhaled anesthetic indicates:
a) A less potent anesthetic
b) A more lipid soluble anesthetic
c) A very fast onset
d) A large amount of anesthetic is required for induction
Trauma/ Anesthesia
Answer B.
The minimum alveolar concentration of an inhaled anesthetic is the amount of anesthetic for which only 50% of patients will move with incision.
A low MAC = more lipid soluble = more potent anesthetic.
Speed of induction is inversely proportional to solubility.
A high alveloar concentration = less lipid soluble = less potent = faster onset.
Nitrous oxide is the fastest working inhaled anesthetic but also has a high MAC.
Trauma/ Anesthesia
Severe hallucinations are a common side effect of:
a) Ketamine
b) Etomidate
c) Propofol
d) Sodium thiopental
Trauma/ Anesthesia
Answer A.
Severe hallucinations are a side effect of ketamine.
Trauma/ Anesthesia
Non-depolarizing paralytics can be reversed with:
a) Beta-blocker
b) Alpha blocker
c) Calcium
d) Neostigmine
Trauma/ Anesthesia
Answer D.
Non-depolarizing paralytics competitively block acetylcholine receptors. If you block acetylcholinesterase, you get build up of acetylcholine which will compete against the non-depolarizing paralytic.
Neostigmine is an inhibitor of acetylcholinesterase.
Trauma/ Anesthesia
Of the anesthetic agents listed below, the one most likely to case an allergic reaction is:
a) Lidocaine
b) Bupivicaine
c) Mepivicaine
d) Procaine
Trauma/ Anesthesia
Answer D.
Procaine is an ester type anesthetic along with cocaine and tetracaine. They are more likely to cause allergic reactions because of their PABA analogue.
Amide type local anesthetics all have an “i” in the first portion of their names such as lidocaine, bupivicaine, and mepivicaine. These rarely cause allergic reactions.
Trauma/ Anesthesia
All of the following are true of local anesthetics except:
a) These agents work by increasing the action potential threshold in peripheral nerves
b) Work better in acidic environments
c) Can cause seizures
d) Ester based local anesthetics have increased allergic reactions compared to amide based anesthetics
Trauma/ Anesthesia
Answer B.
Local anesthetics work by raising the action potential threshold (makes it harder to have an action potential occur so pain sensation is not tranmitted). Local anesthetics work very poorly in acidic environments (which makes it hard to anesthetize infected wounds).

Trauma/ Anesthesia
Helpful hints to make local anesthetic more comfortable • Use smaller gauge needles (higher numbers)• Elective procedures: 27 to 30 gauge needl• Avoid using anything larger than a 25 gauge needle• Infiltrate skin slowly• Inject through wound edge if possible• Warm Xylocaine to body temperature• Be generous with local anesthetic• Use Buffered Lidocaine (Bicarbonate 1 part to Xylocaine 9 part ratio)• Cool skin before injection (Ice, Liquid Nitrogen, frigiderm)• Consider topical anesthetic use before injection

Trauma/ Anesthesia
Topical pre-anesthetics• Ethyl Chloride Spray: Do not use with electrocautery, 1-2 seconds of anesthesia• Lidocaine-Epinephrine-Tetracaine (LET): Indicated for open wounds• EMLA cream (Eutactic Mixture of Local Anesthetic): Indicated in closed wounds, Apply ointment under Occlusion, Use 90 minutes prior to injection• Iontophoresis: Lidocaine sponges applied to intact skin, DC current applied to electrodes, Onset within 10 minutes and duration of 15 minutes, Penetration depth of 1-2 cm• Lidocaine 4% in liposomal matrix (ELA-Max): Similar application as with EMLA cream• Anesthetic Patch (Lidoderm)
Trauma/ Anesthesia
Amide and Ester anesthetic metabolism and excretion.
Metabolized by liver
Excreted by kidney
Dose calculations
Solution of 0.5%: 5 mg/ml
Solution of 1%: 10 mg/ml
Solution of 2%: 20 mg/ml
Trauma/ Anesthesia
Local Anesthetics: Short acting Amide Anesthetics
Local Lidocaine (Xylocaine) 1% or 2%
Onset: 2 minutes
Duration: 1.5 to 2 hours
Max dose: 4 mg/kg to 280 mg (14 ml 2%, 28 ml 1%)
Mepivacaine (Carbocaine) 1%
Onset: 3 to 5 minutes
Duration: 1.5 to 2 hours
Max dose: 4 mg/kg up to 280 mg (28 ml))
Prilocaine (Citanest) 1%
Onset: 2 minutes
Duration: 1 hour
Max dose: 7 mg/kg up to 500 mg (50 ml)

Trauma/ Anesthesia
Local Anesthetics: Long acting Amide Anesthetics
Lidocaine with Epinephrine 1:100,000 or 1:200,000
Onset: 2 minutes
Duration: 2 to 6 hours
Max dose: 7 mg/kg to 500 mg (25 ml 2%, 50 ml 1%)
Bupivacaine (Marcaine) 0.25%
Onset: 5 minutes
Duration: 2 to 4 hours
Max dose: 2.5 mg/kg up to 175 mg (50 ml)
Etidocaine (Duranest) 0.5% or 1%
Max dose: 4 mg/kg to 280 mg (25 ml 1%, 50 ml 0.5%)

Trauma/ Anesthesia
Histamine release is characteristic of:
a) Demerol
b) Fentanyl
c) Sufentanil
d) Morphine
Trauma/ Anesthesia
Answer D.
Morphine has a characteristic histamine release which can cause hypotension.
Trauma/ Anesthesia
An overdose of Fentanyl is treated with:
a) Flumazenil
b) Narcan
c) Neostigmine
d) Edrophonium
Trauma/ Anesthesia
Answer B.
All narcotic agents (Morphine, Fentanyl, Demerol, Sufentanil) overdoses can be treated with Narcan (naloxone).
Trauma/ Anesthesia
Narcan Dosing•IV is most effective. IM or SC administration may be necessary if the IV route is not available. •An initial dose of 0.4 mg to 2 mg of NARCAN may be administered intravenously. •May be repeated at two- to three-minute intervals. •If no response is observed after 10 mg, the diagnosis of opioid-induced or partial opioid-induced toxicity should be questioned.
Trauma/ Anesthesia
A severe overdose of Ativan is treated with:
a) Flumazenil
b) Narcan
c) Neostigmine
d) Edrophonium

Trauma/ Anesthesia
Answer A.
Severe overdoses of benzodiazepines (Ativan, Valium, Versed) are treated with Flumazenil.

Trauma/ Anesthesia
Flumazenil Dosing• Recommended initial dose of ROMAZICON is 0.2 mg (2 mL) administered intravenously over 15 seconds. • If the desired level of consciousness is not obtained after waiting an additional 45 seconds, a second dose of 0.2 mg (2 mL) can be injected and repeated at 60-second intervals where necessary (up to a maximum of 4 additional times) to a maximum total dose of 1 mg (10 mL). •The dosage should be individualized based on the patient's response, with most patients responding to doses of 0.6 mg to 1 mg.
Trauma/ Anesthesia
A patient undergoing a left lower lobectomy has an epidural placed containing morphine and bupivicaine. All of the following are true about the epidural except:
a) Respiratory depression is most likely due to the morphine
b) Hypotension and bradycardia are most likely due to the bupivicaine
c) Epidurals are well tolerated in patients with hypertrophic cardiomyopathy
d) Spinal headaches can often be treated with a blood patch
Trauma/ Anesthesia
Answer C.
HCM is a contraindication to epidurals because they cause a decrease in afterload which can be catastrophic in dilated cardiomyopathy (the ventricle collapses at the level of the septum).
Hypotension and bradycardia with epidurals are almost always related to the local anesthetic. (Sympathectomy and decrease venous return)
Trauma/ Anesthesia
Answer C.
Morphine administered by epidural does not cause hypotension. CSF does not contain mast cells that release histamine.
Respiratory depression is related to morphine in epidurals. Many centers place Dilaudid in epidurals to avoid this side effect.
Trauma/ Anesthesia
Prior to performing a lung resection, the anesthesiologist attempts to intubate the patient but is not sure if the tube is in the trachea. The best determinant of esophageal versus tracheal intubation is:
a) Breath sounds
b) Gastric sounds
c) Grade of the view of the vocal cords
d) End tidal CO2
Trauma/ Anesthesia
Answer D.
End tidal CO2 monitoring is the most sensitive test as to whether or not the endotracheal tube is placed correctly.
Observational methods to confirm correct tube placement
Direct visualization of the tube passing through the vocal cords, Clear and equal bilateral breath sounds on auscultation of the chest, Absent sounds on auscultation of the epigastrium, Equal bilateral chest rise with ventilation, Fogging of the tube, An absence of stomach contents in the tube
Instruments to confirm correct tube placement
Colorimetric end tidal CO2 detector, Waveform capnography, Self inflating esophageal bulb, Pulse oximetry- delay in fall of saturation, especially if pre-oxygenated, Esophageal Detection Device (ODD)

Trauma/ Anesthesia
A 65 year old man on dialysis for renal failure undergoes an elective AAA repair. The patients ASA class is:
a) II
b) III
c) IV
d) V
Trauma/ Anesthesia
Answer B.
Class I: Healthy
Class II: Mild disease without limitation (HTN, DM, Obesity, Smoker)
Class III: Severe Disease (Stable angina, previous MI, moderate COPD)
Class IV: Severe Disease with Constant Threat to Life (Unstable Angina, Renal or Liver Failure, Severe COPD)
Class V: Moribund Patient that will not survive without surgery (Ruptured AAA, Saddle Pulmonary Embolus)
Class VI: Organ Donor

Trauma/ Anesthesia
Trauma/ Anesthesia