absite review: inguinal and femoralinguinal and … hernias.pdfabsite review: inguinal and...
TRANSCRIPT
ABSITE Review:Inguinal and FemoralInguinal and Femoral HerniasSybile Val M.D.SUNY Downstate Medical CenterSUNY Downstate Medical CenterDepartment of SurgeryJune 27, 2008
www.downstatesurgery.org
Obj tiObjectivesCorrectly identify anatomical landmarksCorrectly identify anatomical landmarks intra-operativelyDiff ti t b t f l d i i lDifferentiate between femoral and inguinal herniasUnderstand different approaches at surgical repairCompare operative approaches
www.downstatesurgery.org
Q tiQuestions1. From which muscle layer is the inguinal ligament y g g
derived? a. Transversus abdominusb. External obliquec. Internal obliqued. None of the above
2. What are the borders of the femoral canal? a. External oblique, femoral vein, empty spaceb. external oblique, femoral vein, empty space iliopubic tract and
f l ifemoral veinc. iliopubic, cooper’s, femoral vein and junction of iliopubic and
cooper’s ligamentd None of the aboved. None of the above
www.downstatesurgery.org
Q tiQuestions3 A McVay repair3. A McVay repair
a. May be used to repair femoral herniasb. Entails suturing Poupart’s to the conjoined tendonc. Is no longer performedd. Does not require a relaxing incision
4 TAPP4. TAPPa. Is contraindicated in the elderlyb. Requires traversing the peritoneal cavityc. Is totally extraperitoneald. Has a low learning curve
www.downstatesurgery.org
Q tiQuestions5 The base of Hasselbach’s triangle is5. The base of Hasselbach’s triangle is
a. Derived from the external obliqueb. Cooper’s ligamentc. There is no based. The inferior epigastric
www.downstatesurgery.org
I t d tiIntroduction
In the US ~1 million abdominal wall hernia repairs/yearp y
750,000 – inguinal25,000 - femoral25,000 femoral
www.downstatesurgery.org
I t d tiIntroductionFrom latin word meaning ruptureFrom latin word meaning ruptureDefinition: Abnormal protrusion
Occur at sites where the aponeurosis and fascia are not covered by striated muscle
Male preponderance (7:1)Presentation:
Groin bulge/painRight more common than leftg
www.downstatesurgery.org
I t d tiIntroduction
Risk Factors:AgeOb itObesityCOPDChronic constipationChronic constipationStrainingPregnancyAscitesPeritoneal dialysis
www.downstatesurgery.org
I i l H iInguinal HerniaDirectIndirect Direct
Weakness in the transversalis fascia
IndirectMost common typeWeakness in the transversalis fascia
Due to “wear and tear”Weakness in the internal inguinal ringAssociated with patent
i liprocessus vaginalis
www.downstatesurgery.org
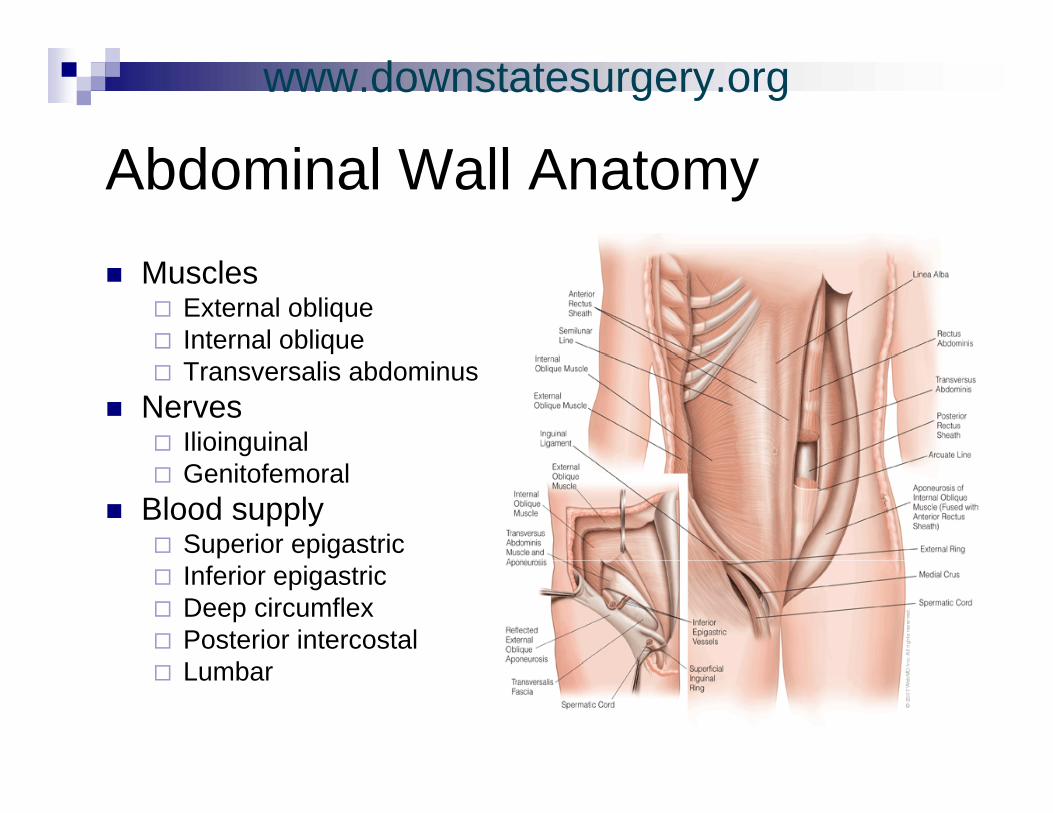
Abd i l W ll A tAbdominal Wall AnatomyMuscles
External obliqueInternal obliqueTransversalis abdominus
NervesIlioinguinalGenitofemoral
Blood supplySuperior epigastricInferior epigastricDeep circumflexPosterior intercostal L bLumbar
www.downstatesurgery.org
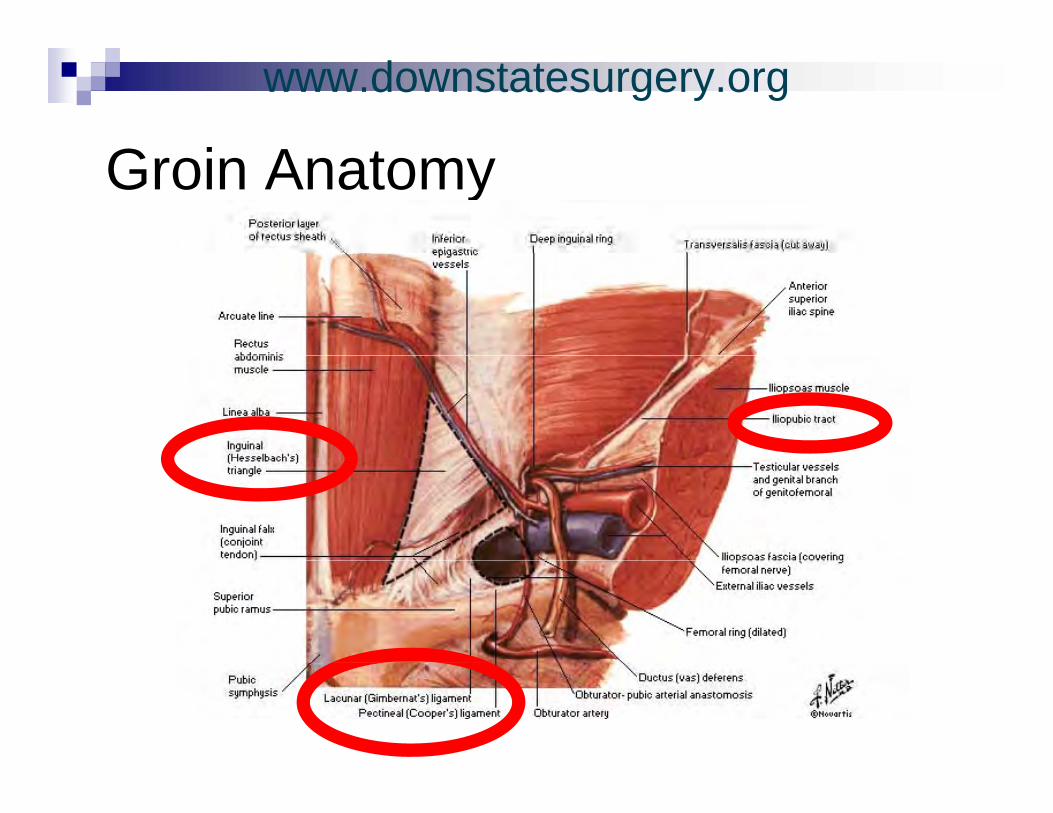
G i A tGroin Anatomy
www.downstatesurgery.org
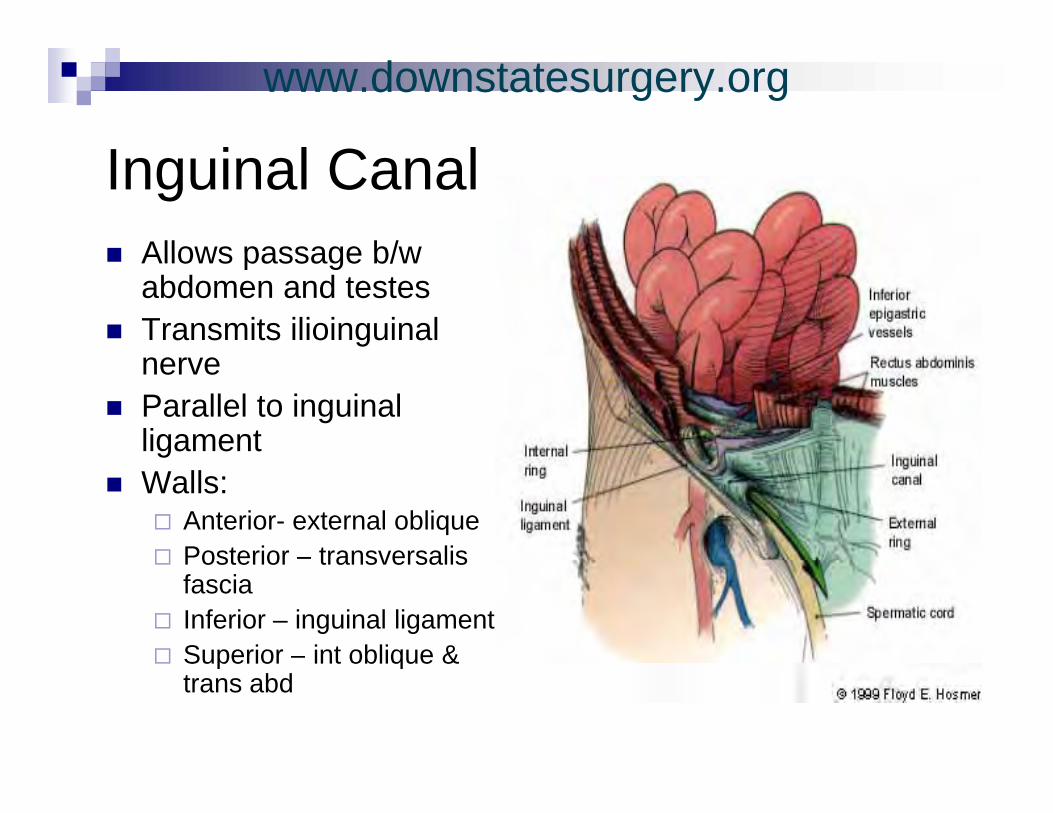
I i l C lInguinal CanalAllows passage b/wAllows passage b/w abdomen and testesTransmits ilioinguinal nerveParallel to inguinal ligamentWalls:
Anterior- external obliquePosterior – transversalisPosterior transversalis fasciaInferior – inguinal ligamentSuperior – int oblique &Superior int oblique & trans abd
www.downstatesurgery.org
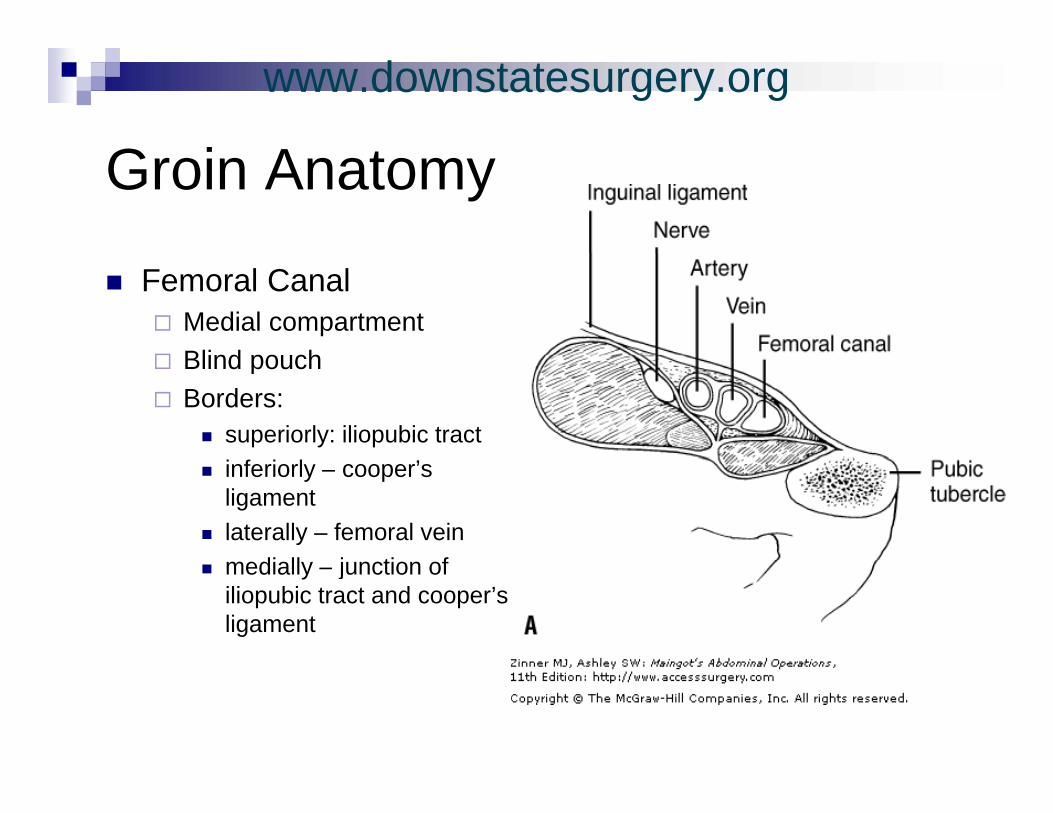
G i A tGroin Anatomy
Femoral CanalMedial compartmentBlind pouchBlind pouchBorders:
superiorly: iliopubic tractinferiorly – cooper’s ligamentlaterally – femoral vein
di ll j ti fmedially – junction of iliopubic tract and cooper’s ligament
www.downstatesurgery.org
O ti R iOperative RepairIndicated for all symptomatic herniasBased on surgeon’s experienceMay be:
Via anterior or posterior approachP iPrimary:
Preferred in presence of contaminationBest choice in female patientspAccomplished using: Bassini, McVay or Shouldice technique
www.downstatesurgery.org

O ti R iOperative Repair
Prosthetic Mesh Repair technique:Onlay versus preperitonealMesh bridges inguinal defectForeign body reaction incitedCommon strategy entails:
Minimal tissue dissection Anchoring of mesh with interrupted suturesg p
www.downstatesurgery.org
O ti R iOperative Repair
Laparoscopic technique:Based on reconstruction of weakened posterior abdominal wallSteep learning curveTwo approaches:Two approaches:
Totally extraperitonealTransabdominal preperitoneal (Intraperitoneal Onlay Mesh)
www.downstatesurgery.org
Hi t i l R iHistorical Review
Edoardo Bassini (1844-1924)Father of modern hernia repair
Performed and published a novel anatomical dissection (1884)
Repair empasized:Repair empasized:High ligation Reconstruction of the inguinal floorgOpening the transversalis fascia
Preparation for deep repair in three layer repair
www.downstatesurgery.org
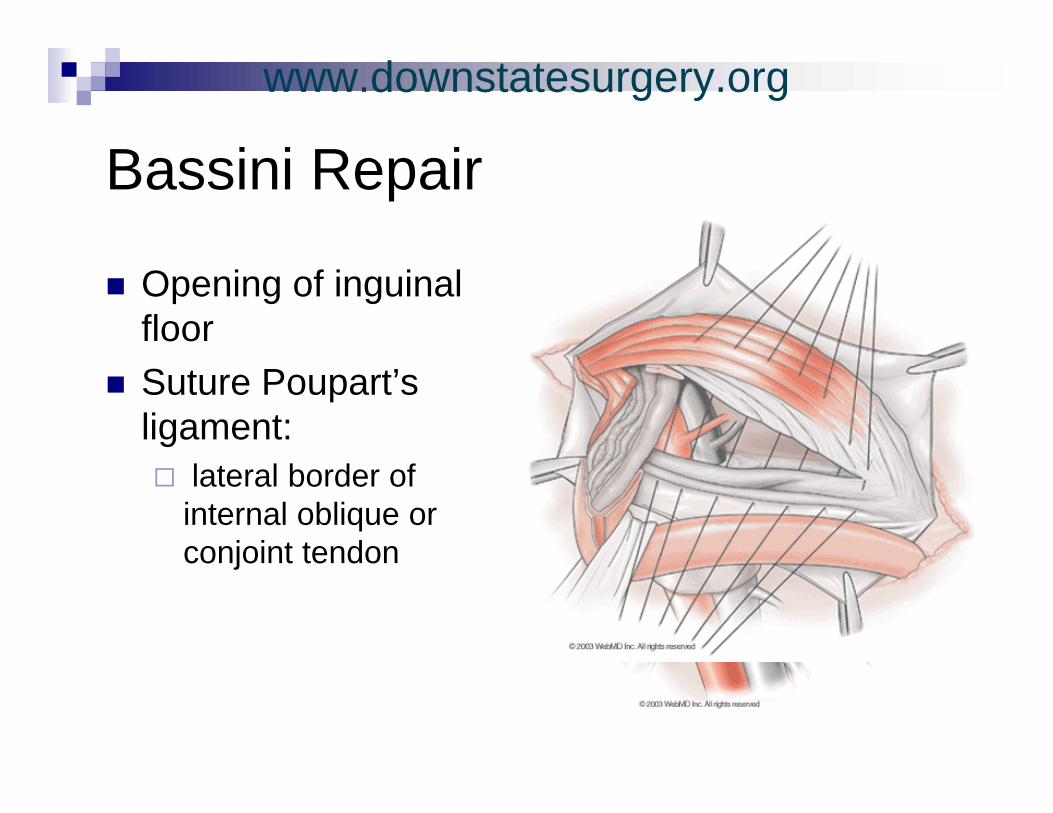
B i i R iBassini Repair
Opening of inguinal floorSuture Poupart’s ligament:
lateral border of internal oblique or conjoint tendonconjoint tendon
www.downstatesurgery.org
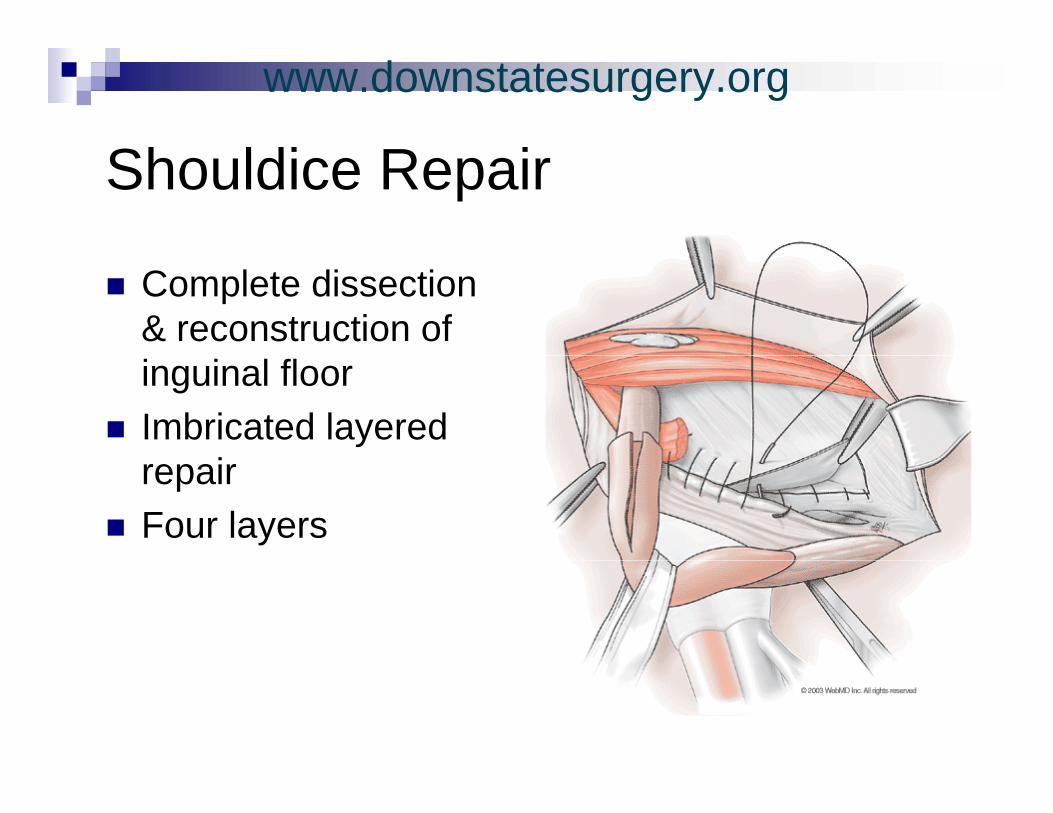
Sh ldi R iShouldice Repair
Complete dissection & reconstruction of inguinal floorImbricated layered
irepairFour layers
www.downstatesurgery.org
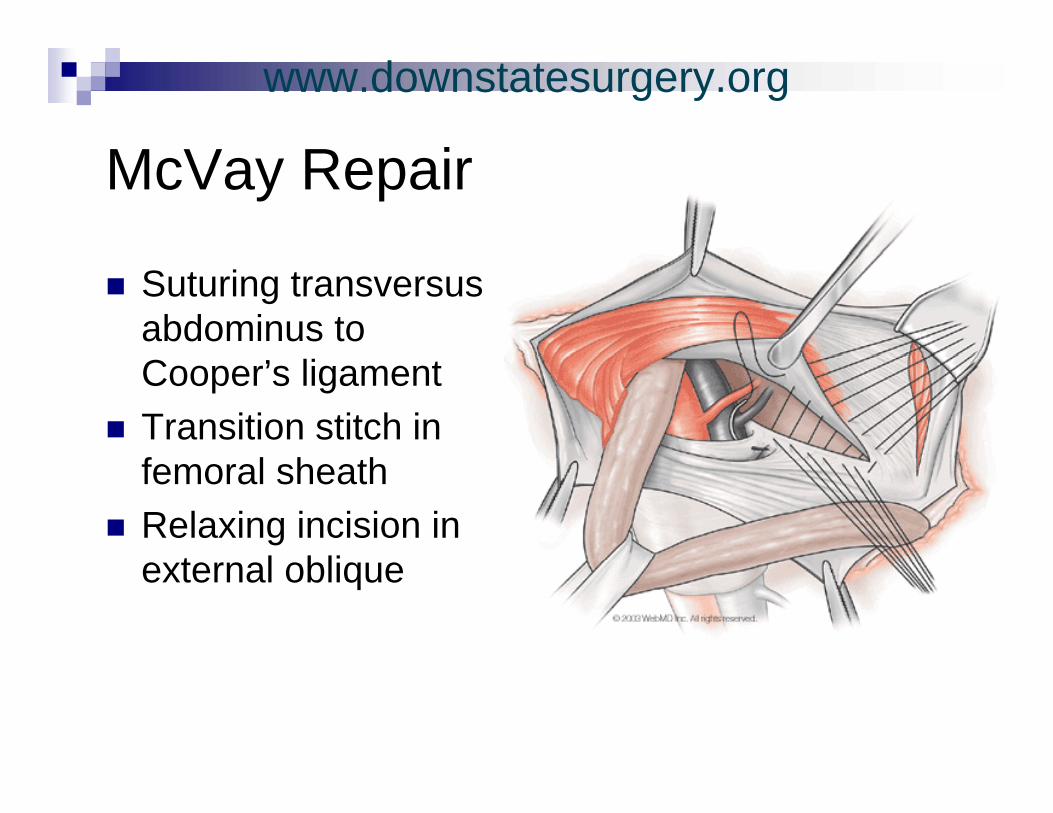
M V R iMcVay Repair
Suturing transversus abdominus to Cooper’s ligamentTransition stitch in f l h thfemoral sheathRelaxing incision in
t l bliexternal oblique
www.downstatesurgery.org
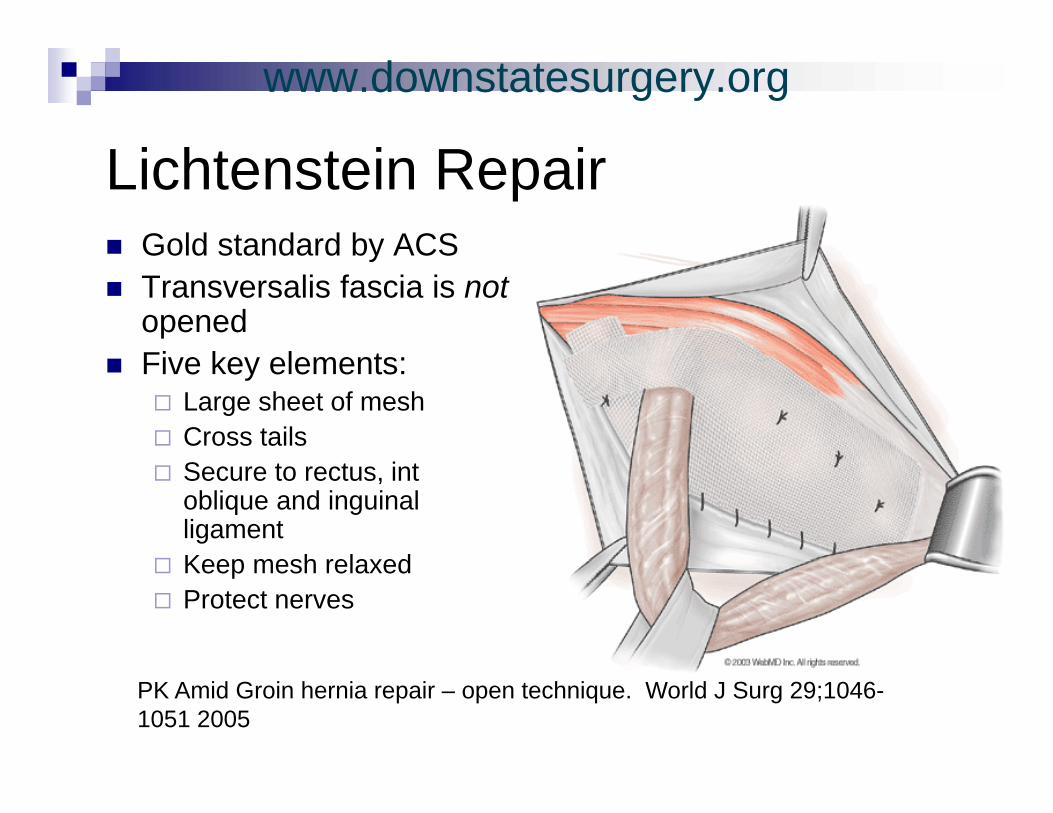
Li ht t i R iLichtenstein RepairGold standard by ACSGold standard by ACSTransversalis fascia is notopenedFi k l tFive key elements:
Large sheet of meshCross tailsSecure to rectus, int oblique and inguinal ligamentKeep mesh relaxedKeep mesh relaxedProtect nerves
PK Amid Groin hernia repair – open technique. World J Surg 29;1046-1051 2005
www.downstatesurgery.org
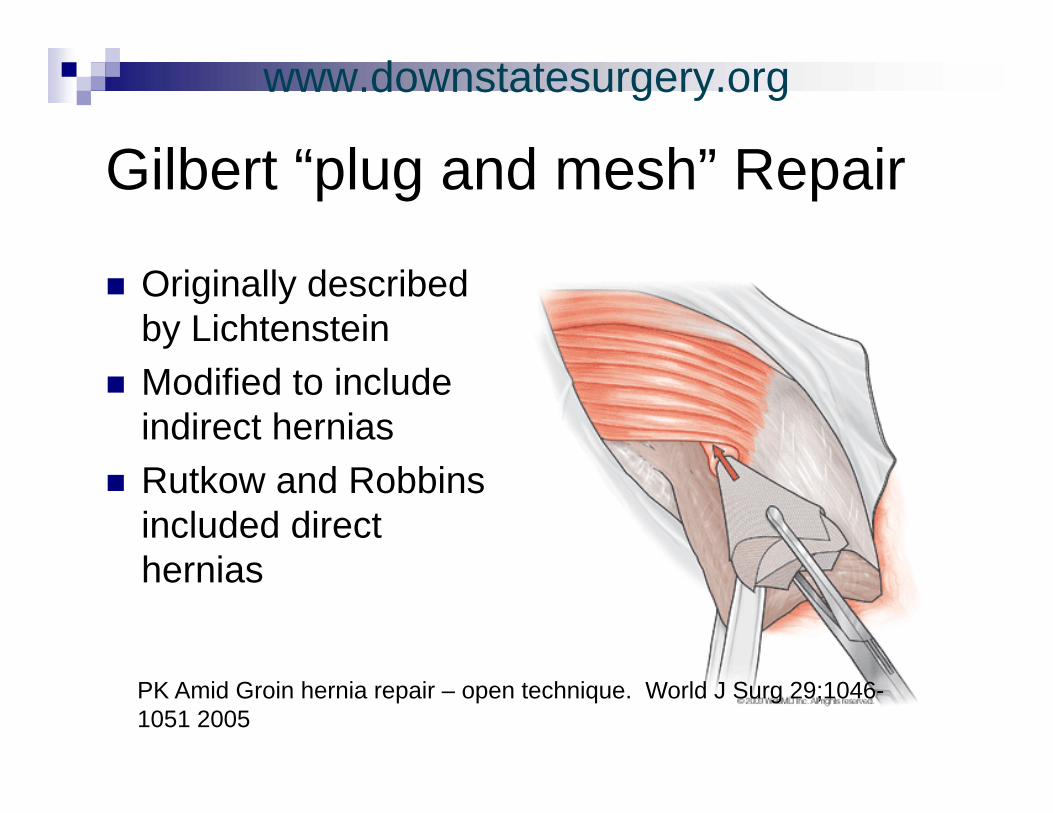
Gilb t “ l d h” R iGilbert “plug and mesh” Repair
Originally described by LichtensteinModified to include indirect herniasRutkow and Robbins included direct h ihernias
PK Amid Groin hernia repair – open technique. World J Surg 29;1046-1051 2005
www.downstatesurgery.org
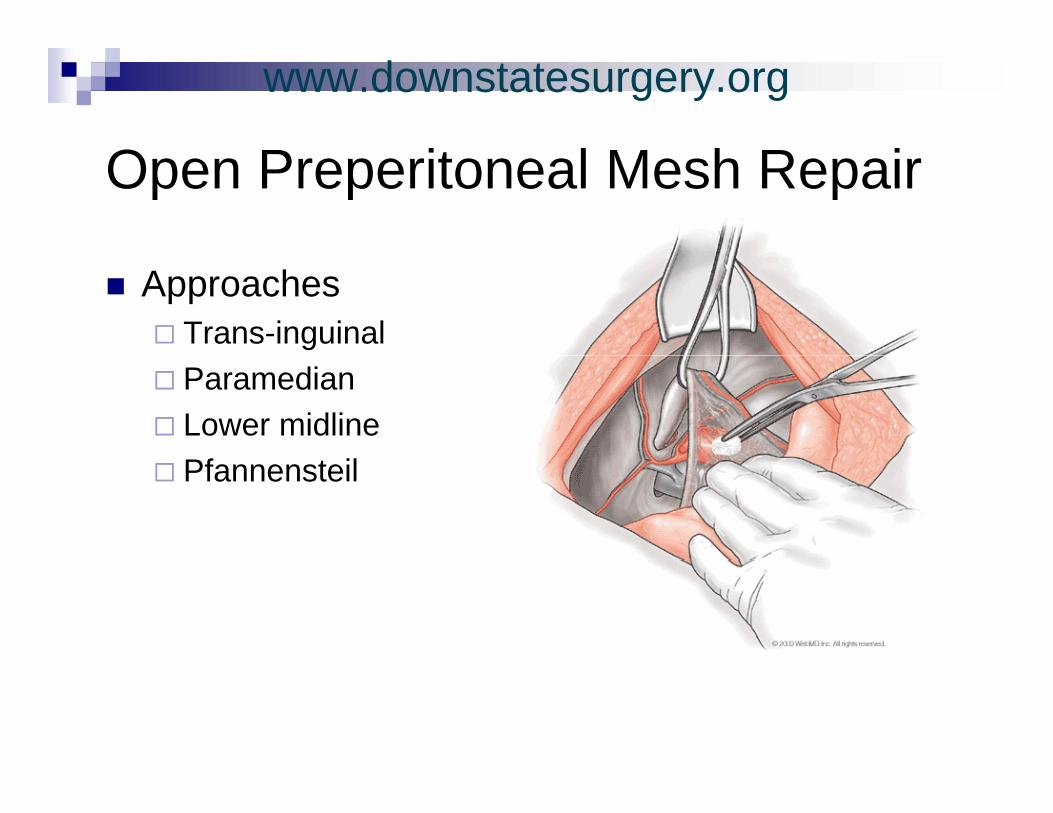
O P it l M h R iOpen Preperitoneal Mesh Repair
ApproachesTrans-inguinalParamedianLower midlinePfannensteil
www.downstatesurgery.org
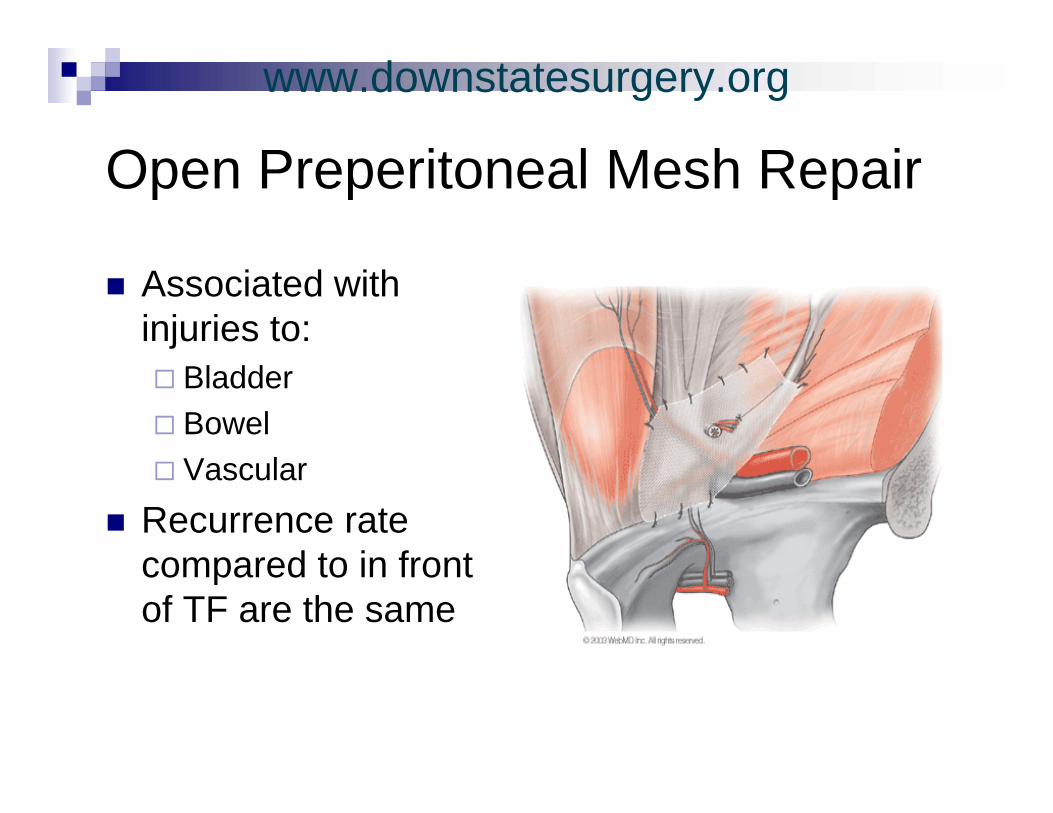
O P it l M h R iOpen Preperitoneal Mesh Repair
Associated with injuries to:
BladderBowelV lVascular
Recurrence rate compared to in frontcompared to in front of TF are the same
www.downstatesurgery.org
PHS S t R iPHS System Repair
Combines Lichtenstein and preperitoneal repair2 layers:
Deep Superficial
www.downstatesurgery.org
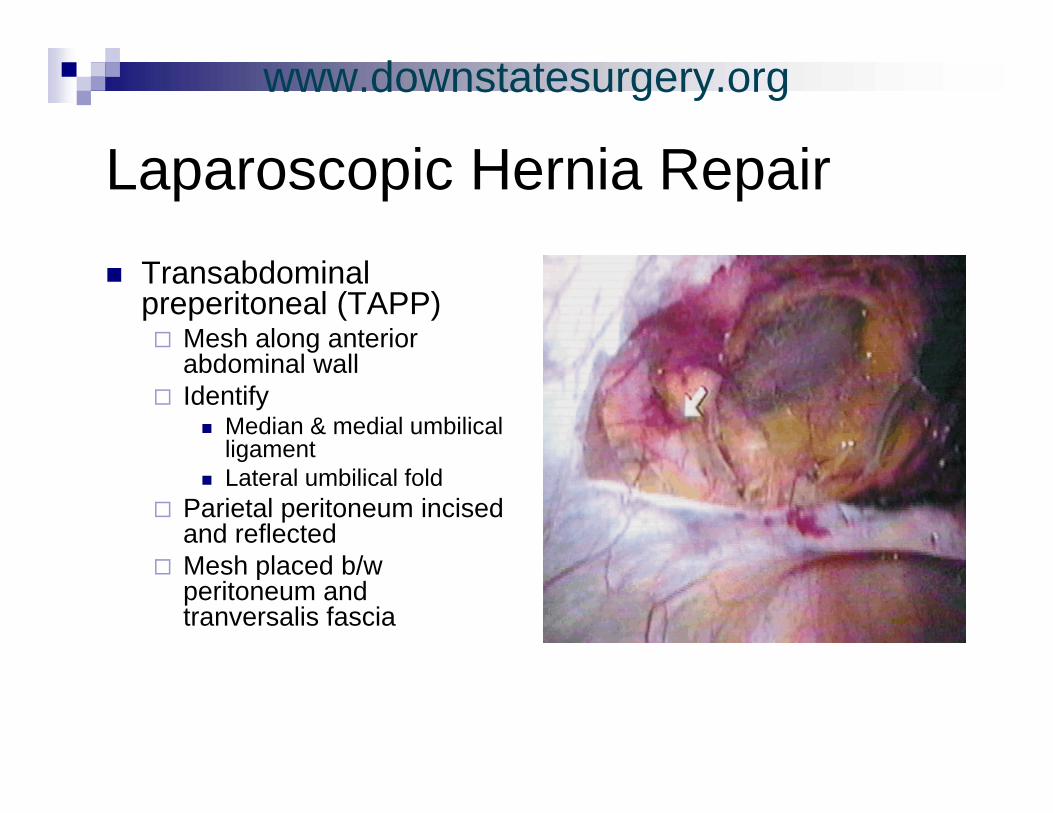
L i H i R iLaparoscopic Hernia RepairTransabdominal preperitoneal (TAPP)
Mesh along anterior bd i l llabdominal wall
IdentifyMedian & medial umbilical ligamentgLateral umbilical fold
Parietal peritoneum incised and reflectedMesh placed b/Mesh placed b/w peritoneum and tranversalis fascia
www.downstatesurgery.org
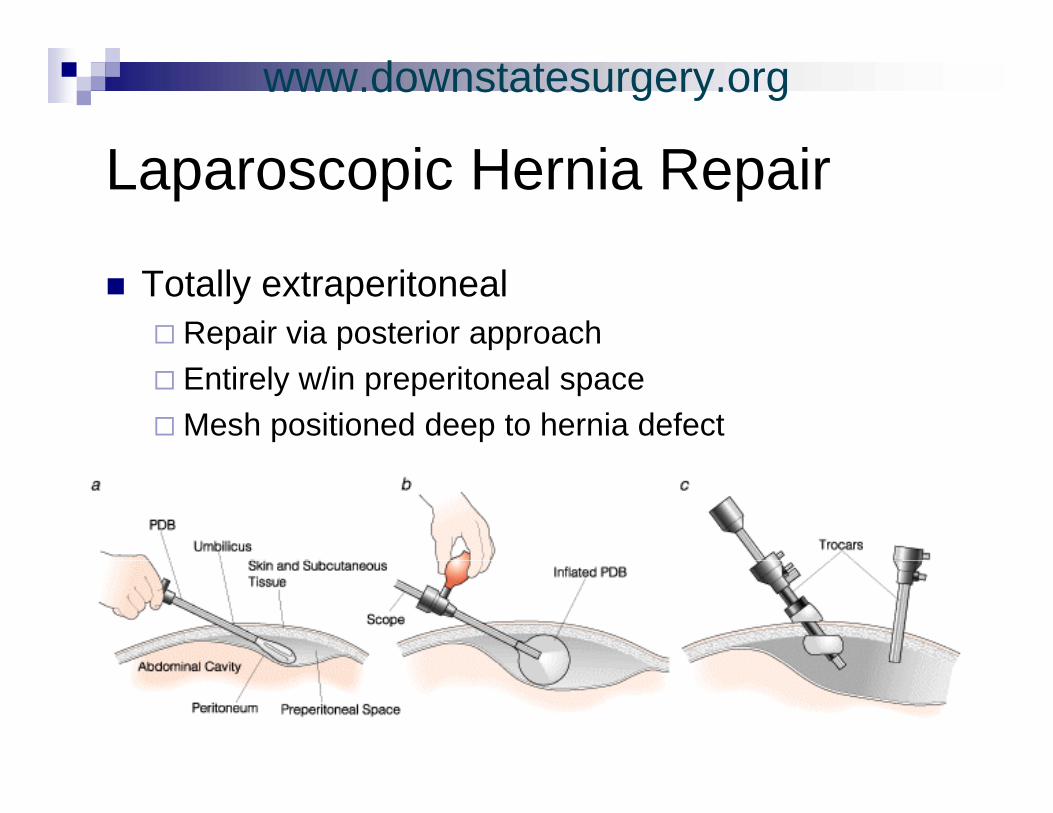
L i H i R iLaparoscopic Hernia Repair
Totally extraperitonealRepair via posterior approachEntirely w/in preperitoneal spaceMesh positioned deep to hernia defect
www.downstatesurgery.org
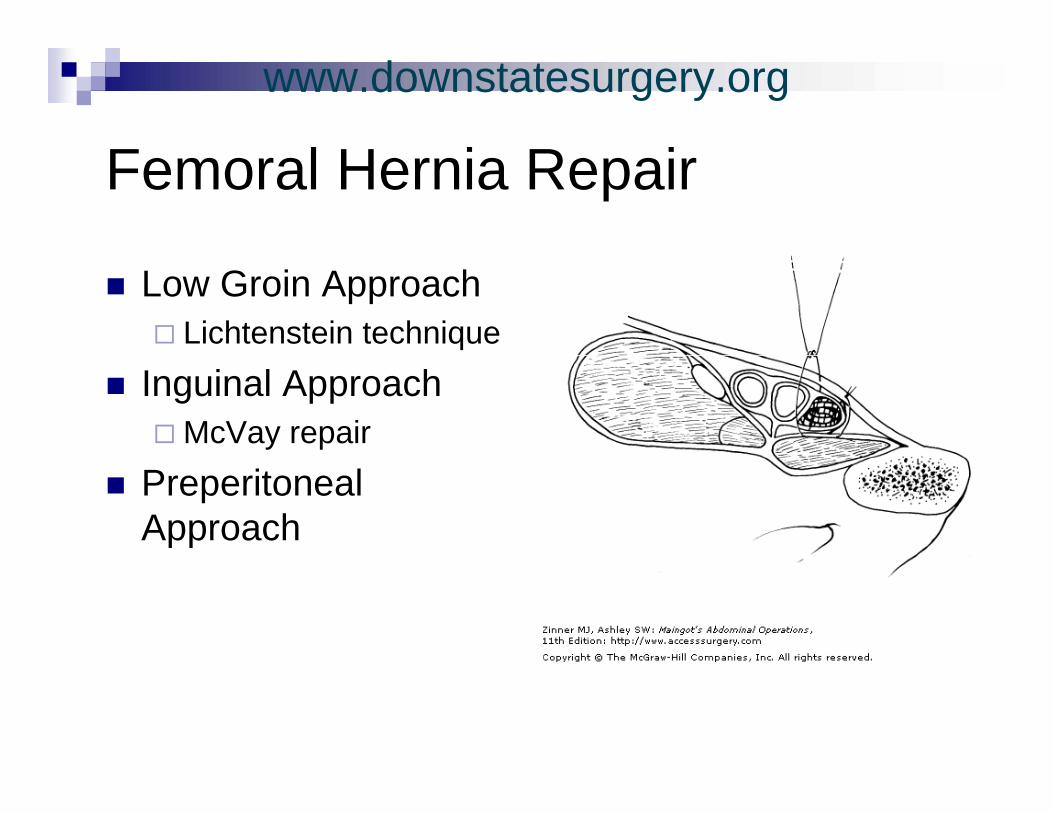
F l H i R iFemoral Hernia Repair
Low Groin ApproachLichtenstein technique
Inguinal ApproachMcVay repair
Preperitoneal Approach
www.downstatesurgery.org
C li tiComplications
RecurrencePostherniorrhaphy
HemorrhageOsteitis pubisp y
painIschemic orchitis
pInfectionProsthesis-related
Testicular atrophy complication
www.downstatesurgery.org
Q ti f th hQuestions of the hour…
1. Is there a superior open repair technique?q
2. Is laparoscopic repair superior to open repair?repair?
3. Chronic pain, is it avoidable?
www.downstatesurgery.org
Open vs. Open
SS Awad et al. Improved outcomes with the prolene hernia system mesh p p ycompared to the time-honored Lichtenstein onlay mesh repair for inguinal hernia repair. Am J of Surgery 2007;193:697-701
www.downstatesurgery.org
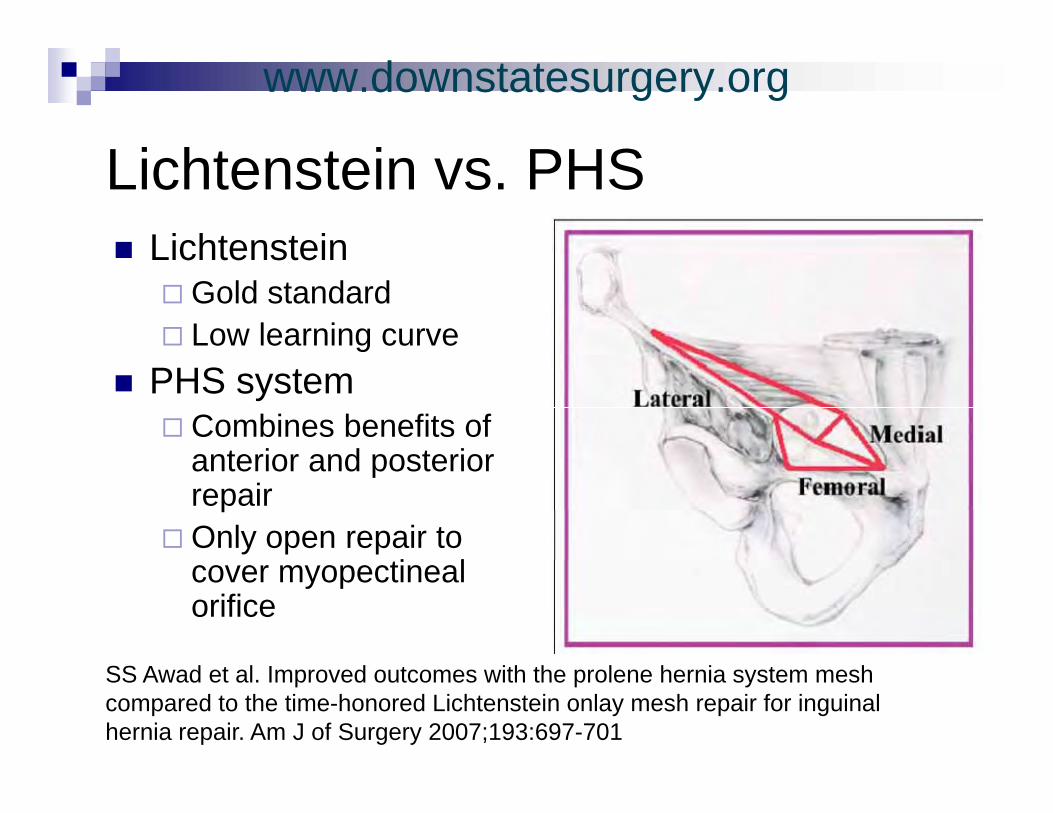
Li ht t i PHSLichtenstein vs. PHSLichtensteinLichtenstein
Gold standardLow learning curve
PHS systemCombines benefits of anterior and posterioranterior and posterior repairOnly open repair to
ti lcover myopectineal orifice
SS Awad et al. Improved outcomes with the prolene hernia system mesh compared to the time-honored Lichtenstein onlay mesh repair for inguinal hernia repair. Am J of Surgery 2007;193:697-701
www.downstatesurgery.org
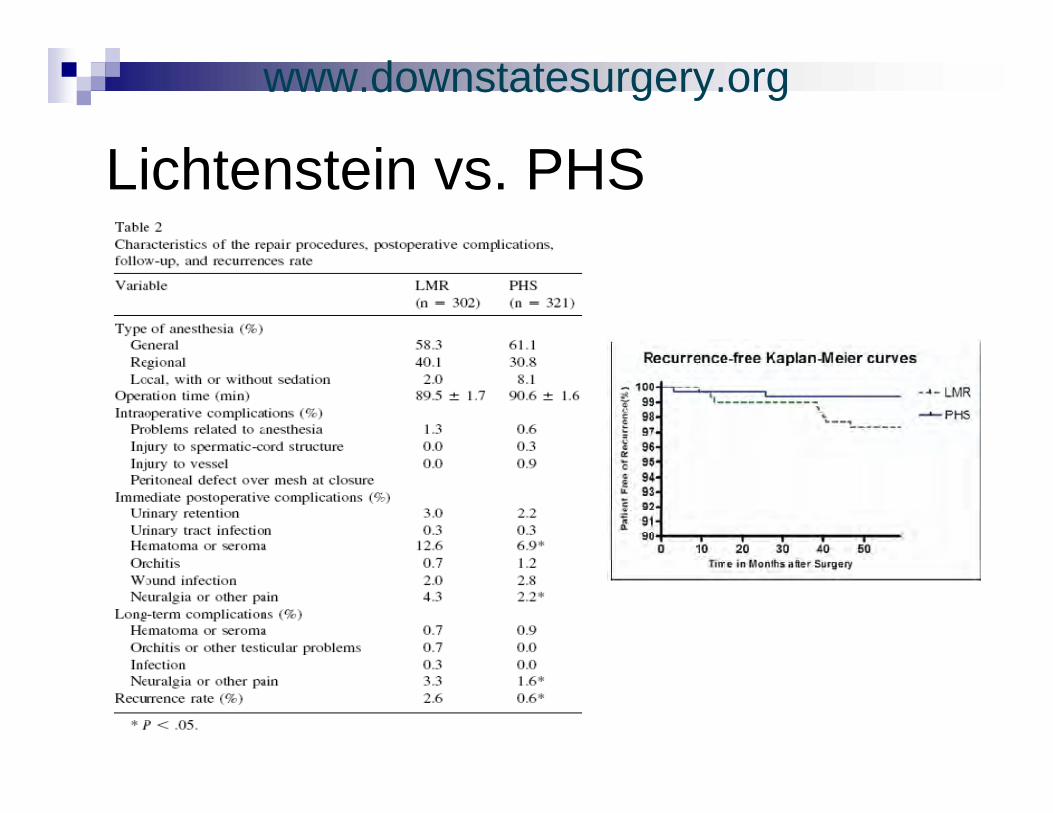
Li ht t i PHSLichtenstein vs. PHSRetrospective study with 622 ptsRetrospective study with 622 pts
321 – PHS repair302 LMR302 – LMR
Follow up was 20 monthsAssessed:
Difference in operating timeComplicationsRecurrence
SS Awad et al. Improved outcomes with the prolene hernia system mesh compared to the time-honored Lichtenstein onlay mesh repair for inguinal hernia repair. Am J of Surgery 2007;193:697-701
www.downstatesurgery.org
Li ht t i PHSLichtenstein vs. PHS
www.downstatesurgery.org
Li ht t i PHSLichtenstein vs. PHSConclusion:Conclusion:
PHS was superior to LMR due to:Lower recurrence ratesLower recurrence ratesDecreased complicationsLess post operative painp p pEarlier return to normal activity
SS Awad et al. Improved outcomes with the prolene hernia system mesh p p ycompared to the time-honored Lichtenstein onlay mesh repair for inguinal hernia repair. Am J of Surgery 2007;193:697-701
www.downstatesurgery.org
Open vs. Laparoscopic
Neumayer L, Giobbie-Hurder A, jonasson O, et al. Veterans Affairs Cooperative Studies Program 456 Investigators. Open mesh versus laparoscopic mesh repair of inguinal hernia. N Engl J Med 2004; 350:1819-27
www.downstatesurgery.org
The data showsThe data shows…Laparoscopic approach gaining popularity
Prelim recurrence rates ranged from 3-10%Benefits included
Less PainQuicker return to activityQuicker return to activity
Subsided enthusiasm due to:High costSteep learning curvep gSerious complicationsNeed for general anesthesia
TAPP versus TEP:TEP preferred because:
Wide exposureAvoids abdominal entryAssociated with decrease post-op painAssociated with decrease post-op painFaster post-operative recovery
www.downstatesurgery.org
Open versus LaparoscopicOpen versus LaparoscopicGoal:
Examine perioperative outcomes and complications in both TEP and open mesh repair
345 patients345 patients198 – open mesh repair147 – TEP repair
F ll th thFollow up: three monthsCompared:
Operative timeOperative timeComplications
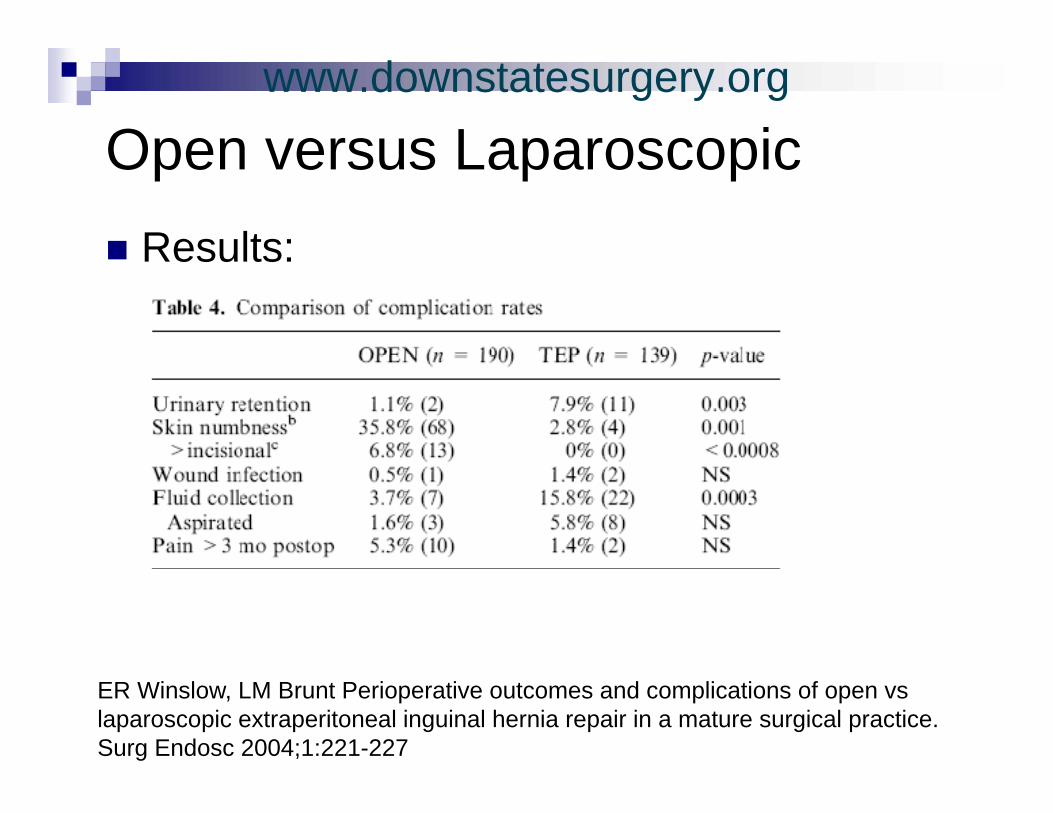
ER Winslow, LM Brunt Perioperative outcomes and complications of open vs laparoscopic extraperitoneal inguinal hernia repair in a mature surgical practice. Surg Endosc 2004;18:221-227
www.downstatesurgery.org
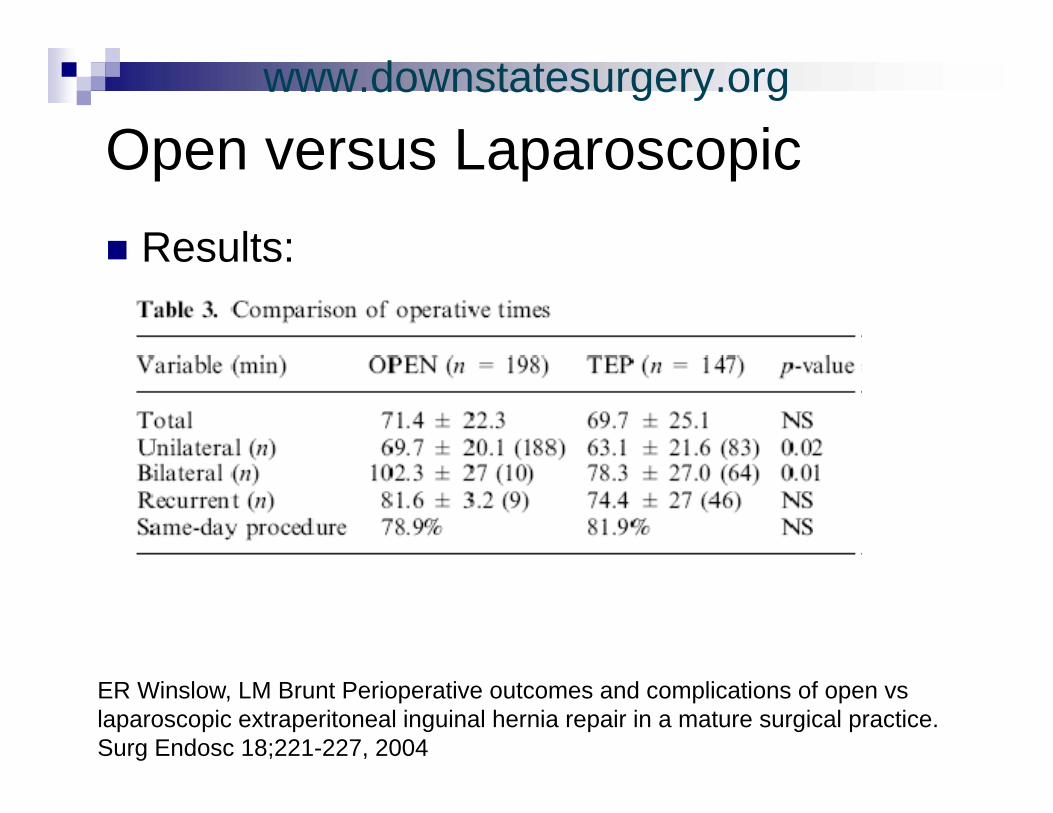
Open versus LaparoscopicOpen versus LaparoscopicResults:Results:
ER Winslow, LM Brunt Perioperative outcomes and complications of open vs laparoscopic extraperitoneal inguinal hernia repair in a mature surgical practice. Surg Endosc 18;221-227, 2004
www.downstatesurgery.org
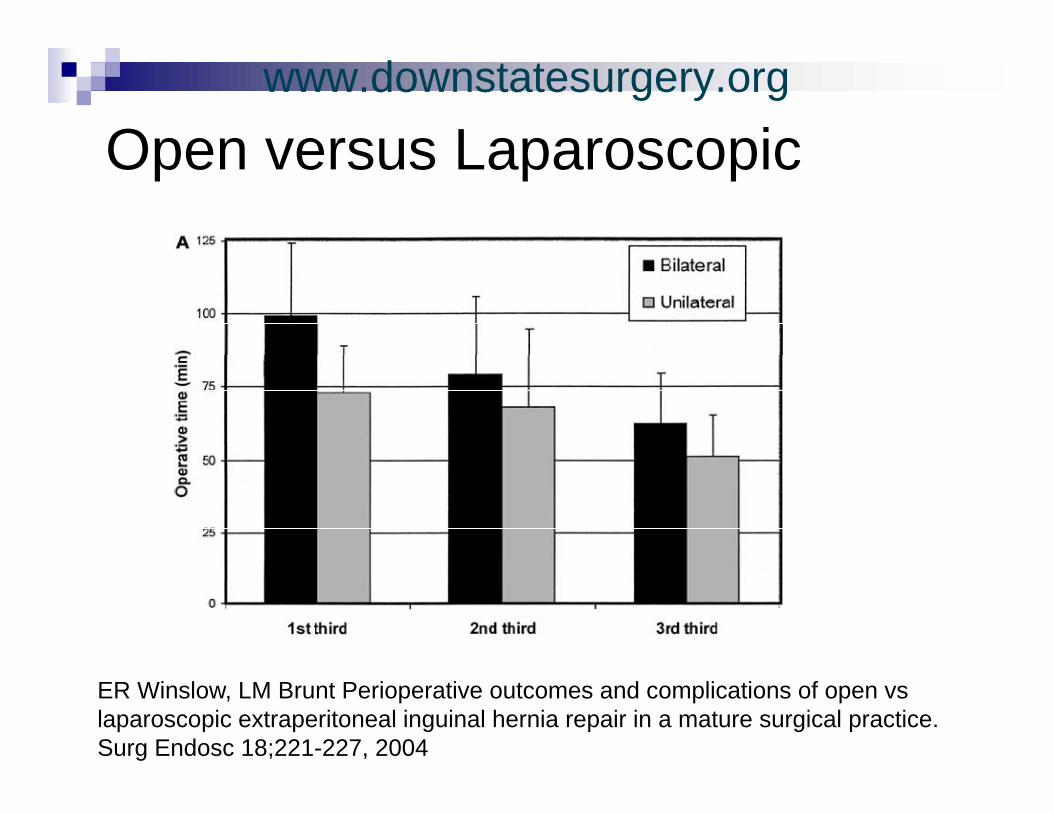
Open versus LaparoscopicOpen versus Laparoscopic
ER Winslow, LM Brunt Perioperative outcomes and complications of open vs laparoscopic extraperitoneal inguinal hernia repair in a mature surgical practice. Surg Endosc 18;221-227, 2004
www.downstatesurgery.org
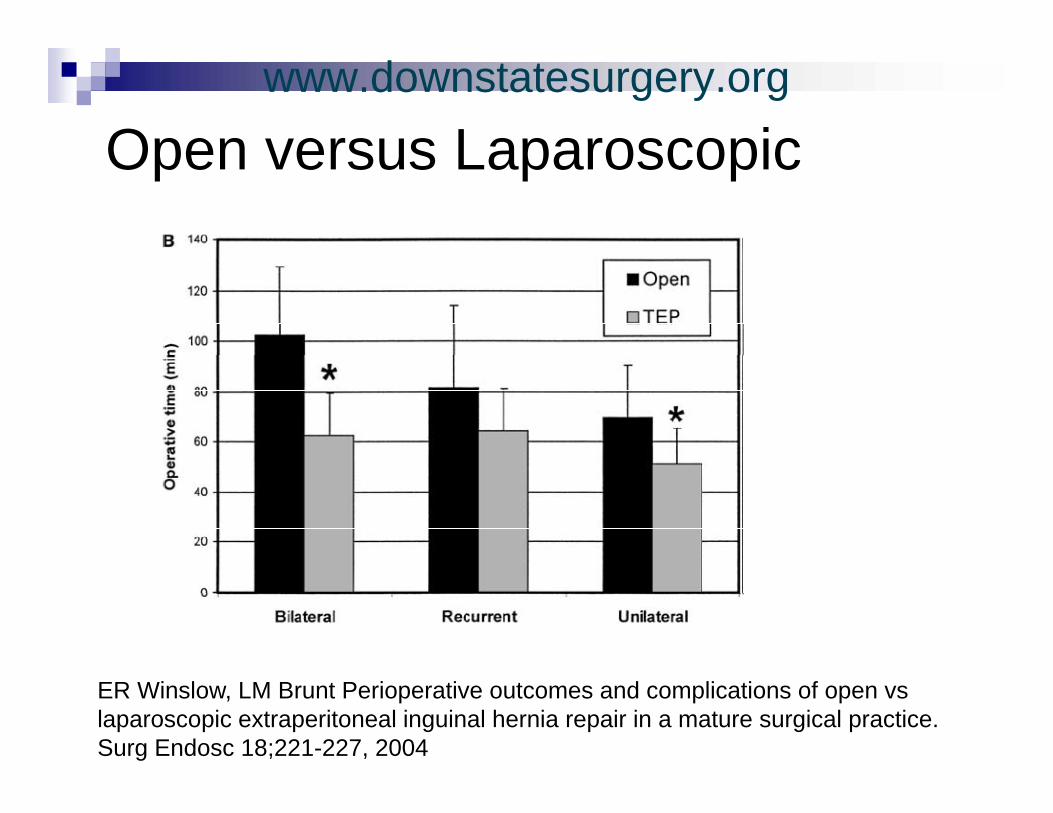
Open versus LaparoscopicOpen versus Laparoscopic
ER Winslow, LM Brunt Perioperative outcomes and complications of open vs laparoscopic extraperitoneal inguinal hernia repair in a mature surgical practice. Surg Endosc 18;221-227, 2004
www.downstatesurgery.org
Open versus LaparoscopicOpen versus LaparoscopicResults:Results:
ER Winslow, LM Brunt Perioperative outcomes and complications of open vs laparoscopic extraperitoneal inguinal hernia repair in a mature surgical practice. Surg Endosc 2004;1:221-227
www.downstatesurgery.org
Open versus LaparoscopicOpen versus LaparoscopicConclusion:Conclusion:
TEP repairs can be performed efficiently and without major complicationswithout major complicationsOperative times are shorter in the hands of experienced surgeonsexperienced surgeonsTEP associated with lower rate of post-operative numbness and prolonged groin painp p g g p
ER Winslow, LM Brunt Perioperative outcomes and complications of open vs laparoscopic extraperitoneal inguinal hernia repair in a mature surgical practice. Surg Endosc 2004;18:221-227
www.downstatesurgery.org
Open versus Laparoscopic
Prospective randomized controlled trial
Open versus Laparoscopic
Prospective, randomized controlled trialConducted b/w 1996-1997Follow up: 7.3 years168 patients:p
81 – TEP87 - Lichtenstein87 Lichtenstein
Hallen et al Laparoscopic extraperitoneal inguinal hernia repair versus openHallen et al. Laparoscopic extraperitoneal inguinal hernia repair versus open mesh repair:long term follow-up of a randomized controlled trial. SURGERY 2008;143:313-317
www.downstatesurgery.org
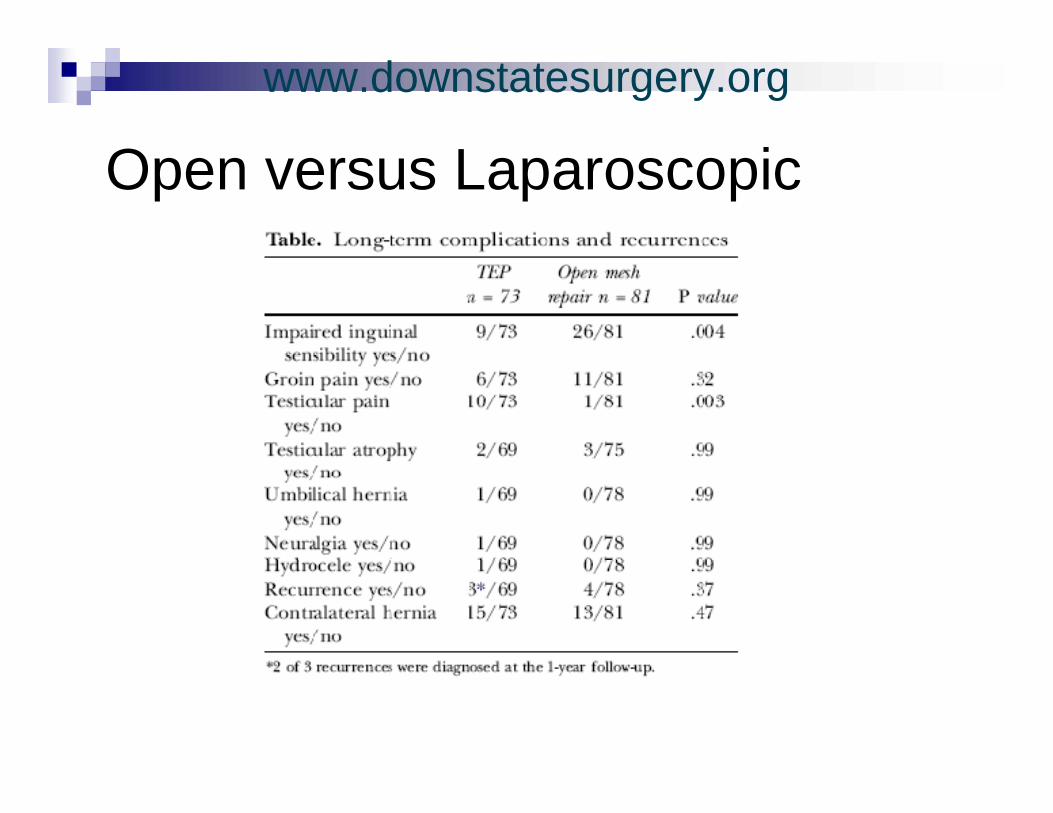
O L iOpen versus Laparoscopic
www.downstatesurgery.org
O L iConclusion:
Open versus LaparoscopicConclusion:
Long term cure of hernia in patient with lap or open hernia repair is excellentope e a epa s e ce eIndividualized hernia repair yields best results and is most cost effectiveTEP is an excellent method for individuals in a working population who require short convalescenceconvalescenceTEP advantageous in recurrent hernias
Hallen et al. Laparoscopic extraperitoneal inguinal hernia repair versus open mesh repair:long term follow-up of a randomized controlled trial. SURGERY 2008143:313-317
www.downstatesurgery.org
Ch i G i P iChronic Groin Pain
Potentially incapacitating complication Cause not clear: ? Nerve EntrapmentCause not clear: ? Nerve Entrapment
Ilioinguinal IliohypogastricIliohypogastric Genital branch of genitofemoral
R ti ti d di i i hRoutine preservation and division have been advocated
www.downstatesurgery.org
Prophylactic IlioinguinalProphylactic Ilioinguinal Neurectomy in Open Hernia Repair
Double blinded randomized controlled trial100 patients b/w 18-80yoa
50: whole ilioinguinal nerve excised50: nerve preserved
P i t i id f h i i t 6Primary outcome: incidence of chronic pain at 6 monthsSecondary outcome: incidence of groin numbnessy g
Follow up: 6 months
WL Mui et al “Prohylactic ilioinguinal neurctomy in open inguinal hernia repair” Annals of Surgery 244;1, 2006
www.downstatesurgery.org
Prophylactic IlioinguinalProphylactic Ilioinguinal Neurectomy in Open Hernia Repair
Results:No significant difference in:No significant difference in:
incidence of pain at 6 monthsIncidence of groin numbness and sensation changeQuality of life
WL Mui et al “Prohylactic ilioinguinal neurctomy in open inguinal hernia repair” Annals of Surgery 244;1, 2006
www.downstatesurgery.org
C l iConclusionLi ht t i ti t b t d dLichtenstein continues to be standard although PHS and laparoscopic techniques are gaining acceptanceare gaining acceptanceSurgeon experience is key to providing good hernia repairgood hernia repairLearning curve in laparoscopic hernia repair is steep however in hands of experiencedis steep however in hands of experienced surgeons outcome comparable to open repairrepair
www.downstatesurgery.org